
CONTENTS Dental Care -...
88
Indian Journal of Comprehensive Dental Care JULY- DEC 2016 • VOL 6 • ISSUE 2 IJCDC 760 Indian Journal of Comprehensive Dental Care CONTENTS ORIGINAL ARTICLES “A STUDY TO ASSESS THE ORAL HEALTH STATUS AND VARIOUS ORAL HYGIENE PRACTICES OF PATIENTS REPORTING TO SGRD DENTAL COLLEGE, AMRITSAR” 770 * A COMPARATIVE EVALUATION OF ACCURACY OF THE ROOT ZX ELECTRONIC APEX LOCATOR IN THE PRESENCE OF DIFFERENT IRRIGANTS 774 *Shantun Malhotra **Rajesh Khanna *** Kanwalpreet Kaur Bhullar **** Mohit Gautam EVALUATION OF REMINERALIZATION OF ENAMEL WITH TOPICAL APPLICATION OF CALCIUM PHOSPHATE BASED AGENTS: A QUANTITATIVE ENERGY DISPERSIVE X- RAY ANALYSIS USING SCANNING ELECTRON MICROSCOPY : AN IN-SITU STUDY 780 * Tawanpreet Kaur **Rajesh Khanna ***Rupam Kaur ****Aashish Handa PREVALENCE OF DENTAL ANOMALIES IN PATIENTS WITH CLEFT LIP AND PALATE 785 *Sukhdeep Singh Kahlon **Chetan Dev Singh Boparai ***Tahira kaur Bawa ****Sukhamrit Kaur A CLINICAL STUDY TO COMPARE VARIOUS BLOOD CELL PARAMETERS FOR ASSESSMENT 789 OF ANAEMIA OF CHRONIC DISEASE IN HEALTHY SUBJECTS AND CHRONIC PERIODONTITIS PATIENTS *Navkiran **Anooja Lall ***Ashish Verma ****Sahib Tej Singh CASE REPORTS MANAGEMENT OF AMELOGENESIS IMPERFECTA - AN ESTHETIC REHABILITATION 794 *Deepika Singla **Sonam Mahajan ***Manjot Singh ****Vanita *****Pardeep Mahajan ******Prashant Monga NON SURGICAL MANAGEMENT OF GRADE 3 MOBILE TEETH: A CASE REPORT 797 *Gunmeen Sadana **Manjul Mehra ***Rashu Grover ****Jasmeet Kaur OBTURATOR PROSTHESIS FOR REHABILITATION OF ACQUIRED MAXILLARY DEFECT 801 – A CASE REPORT * Akash Duggal **Aman Arora ***Parul Duggal ****Tarunpreet Kaur Gill THE DYNAMIC IMPRESSION TECHNIQUE FOR RESORBED RIDGES 804 *Aman Arora **Navdeep Attri ***Preeti Chawla Arora ****Aakash Duggal IMPLANT PLACEMENT WITH PREDICTABLE GBR IN LARGE BONY DEFECT- A CASE REPORT 807 *Ashish Verma **Sahib Tej Singh ***Harmandeep Singh ****Sukhpreet Singh *****Navdeep Singh MUCOUS MEMBRANE PEMPHIGOID – A CASE REPORT 811 *Isha Singla **Shambulingappa Pallagatti ***Soheyl Sheikh ****Deepak Gupta *****Simranpreet Saini ******Shiny Singh GIANT SUBMANDIBULAR GLAND SIALOLITH : A CASE REPORT 814 *Amneet Sandhu **Supreet Gill ***Parminder Singh ****Yashmeet Kaur Amaninder Kaur Randhawa **Gurpreet Kaur ***Satinder Singh Walia ****Gursimran Kaur
Transcript of CONTENTS Dental Care -...

Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2I J C D C
760Indian Journal of Comprehensive Dental Care
CONTENTS
ORIGINAL ARTICLES
“A STUDY TO ASSESS THE ORAL HEALTH STATUS AND VARIOUS ORAL HYGIENE PRACTICES OF PATIENTS REPORTING TO SGRD DENTAL COLLEGE, AMRITSAR” 770*
A COMPARATIVE EVALUATION OF ACCURACY OF THE ROOT ZX ELECTRONIC APEX LOCATOR IN THE PRESENCE OF DIFFERENT IRRIGANTS 774*Shantun Malhotra **Rajesh Khanna *** Kanwalpreet Kaur Bhullar **** Mohit Gautam
EVALUATION OF REMINERALIZATION OF ENAMEL WITH TOPICAL APPLICATION OF CALCIUM PHOSPHATE BASED AGENTS: A QUANTITATIVE ENERGY DISPERSIVE X- RAY ANALYSIS USING SCANNING ELECTRON MICROSCOPY : AN IN-SITU STUDY 780* Tawanpreet Kaur **Rajesh Khanna ***Rupam Kaur ****Aashish Handa
PREVALENCE OF DENTAL ANOMALIES IN PATIENTS WITH CLEFT LIP AND PALATE 785*Sukhdeep Singh Kahlon **Chetan Dev Singh Boparai ***Tahira kaur Bawa ****Sukhamrit Kaur
A CLINICAL STUDY TO COMPARE VARIOUS BLOOD CELL PARAMETERS FOR ASSESSMENT 789OF ANAEMIA OF CHRONIC DISEASE IN HEALTHY SUBJECTS AND CHRONIC PERIODONTITIS PATIENTS*Navkiran **Anooja Lall ***Ashish Verma ****Sahib Tej Singh
CASE REPORTS
MANAGEMENT OF AMELOGENESIS IMPERFECTA - AN ESTHETIC REHABILITATION 794*Deepika Singla **Sonam Mahajan ***Manjot Singh ****Vanita *****Pardeep Mahajan ******Prashant Monga
NON SURGICAL MANAGEMENT OF GRADE 3 MOBILE TEETH: A CASE REPORT 797*Gunmeen Sadana **Manjul Mehra ***Rashu Grover ****Jasmeet Kaur
OBTURATOR PROSTHESIS FOR REHABILITATION OF ACQUIRED MAXILLARY DEFECT 801 – A CASE REPORT* Akash Duggal **Aman Arora ***Parul Duggal ****Tarunpreet Kaur Gill
THE DYNAMIC IMPRESSION TECHNIQUE FOR RESORBED RIDGES 804*Aman Arora **Navdeep Attri ***Preeti Chawla Arora ****Aakash Duggal
IMPLANT PLACEMENT WITH PREDICTABLE GBR IN LARGE BONY DEFECT- A CASE REPORT 807*Ashish Verma **Sahib Tej Singh ***Harmandeep Singh ****Sukhpreet Singh *****Navdeep Singh
MUCOUS MEMBRANE PEMPHIGOID – A CASE REPORT 811*Isha Singla **Shambulingappa Pallagatti ***Soheyl Sheikh ****Deepak Gupta *****Simranpreet Saini ******Shiny Singh
GIANT SUBMANDIBULAR GLAND SIALOLITH : A CASE REPORT 814*Amneet Sandhu **Supreet Gill ***Parminder Singh ****Yashmeet Kaur
Amaninder Kaur Randhawa **Gurpreet Kaur ***Satinder Singh Walia ****Gursimran Kaur

I J C D C
761Indian Journal of Comprehensive Dental Care
CONTENTS
UNICYSTIC AMELOBLASTOMA: RAISING OBSCURITY IN PERIRADICULAR DIAGNOSIS 817- A CASE REPOR T*Ramandeep S Narang **Adesh S Manchanda ***Jaspreet Kaur
THREE DIMENSIONAL ARCH CONTROL WITH A UBIQUITOUS DEVICE- HYGIENIC RAPID EXPANDER 821*Shilpa Gupta Saini **Shaunak Vyas ***Navjot Singh Jassal ****Sanak Kaur Chattha
REVIEWS
COMPARISON OF THREE NEWER SURGICAL APPROACHES FOR THE MANAGEMENT OF RANULA 824*Nitin Verma **Jeevan Lata ***Sarita Mahajan
MANAGEMENT OF BISPHOSPHONATES INDUCED OSTEONECROSIS OF THE JAW 829- A SYSTEMATIC REVIEW*Vishal Mittal **Tejinder Kaur ***Amit Dhawan ****Jasmine Kaur *****Ramandeep S Bhullar
ENDODONTIC MANAGEMENT OF IMMATURE TEETH WITH NECROTIC PULP- SHIFTING FROM 835 APEXIFICATION TO REVASCULARIZATION*Gunmeen Sadana ** Sunil Gupta ***Teena Gupta ****Hashmit Kaur Rai
SOLAR ENERGY – ITS USE IN DENTISTRY 841*Harmanpreet Singh **Nidhi Gupta ***Preety Gupta ****Vikram Arora
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

I J C D C
762Indian Journal of Comprehensive Dental Care
DR SUKHDEEP SINGH KAHLON
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2
DR. RAJESH KHANNA
DR. KAVIPAL SINGH (Principal S.G.R.D.)
DR. KAMALDEEP SHARMA
DR. ADESH MANCHANDA

Indian Journal of Comprehensive Dental Care
I J C D CI J C D C
763
About the Journal
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2
www.ijcdc.com

I J C D C
764Indian Journal of Comprehensive Dental Care
Manuscripts must be prepared in accordance with "Uniform validation. Up to 400 words and 4 references.requirements for Manuscripts submitted to Biomedical Announcements of conferences, meetings, courses, awards, Journal" developed by International Committee of Medical and other items likely to be of interest to the readers should be Journal Editors (October 2001). The uniform requirements submitted with the name and address of the person from and specific requirement of ' Indian Journal of Comprehensive whom additional information can be obtained. Up to 100 Dental Care' are summarized below. Before sending a words. manuscript contributors are requested to check for the latest
Authorship criteriainstructions available. All persons designated as authors should qualify for The Editorial Processauthorship, and all those who qualify should be listed. Each
The manuscripts will be reviewed for possible publication with author should have participated sufficiently in the work to the understanding that they are being submitted to one take public responsibility for appropriate portions of the journal at a time and have not been published, simultaneously content. The first author should take responsibility for the submitted, or already accepted for publication elsewhere. integrity of the work as a whole, from inception to published The Editors review all submitted manuscripts initially. article. Manuscripts with insufficient originality, serious scientific Authorship credit should be based only onflaws, or absence of importance of message are rejected. The
1. Substantial contributions to conception and design, journal will not return the unaccepted manuscripts. or acquisition of data, or analysis and interpretation of data;
Other manuscripts are sent to two or more expert reviewers 2. Drafting the article or revising it critically for without revealing the identity of the authors to the reviewers. important intellectual content; and Within a period of six to eight weeks, the contributors will be
3. Final approval of the version to be published. informed about the rev iewers ' comments and Conditions 1, 2, and 3 must all be met. Acquisition of funding, acceptance/rejection of manuscript. Articles accepted would the collection of data, or general supervision of the research be copy edited for grammar, punctuation, print style, and group, by themselves, do not justify authorship.format. Page proofs will be sent to the first author, which has
to be returned within five days. Correction received after that The order of authorship on the byline should be a joint period may not be included. All manuscripts received are duly decision of the co-authors. Authors should be prepared to acknowledged. explain the order in which authors are listed. Once submitted
the order cannot be changed without written consent of all Types of Manuscripts and word limitsthe authors.Original research articlesFor a study carried out in a single institute, the number of Randomized controlled trials, intervention studies, studies of authors should not exceed six. For a case-report and for a screening and diagnostic test, outcome studies, cost review article, the number of authors should not exceed four. effectiveness analyses, case-control series, and surveys with For short communication, the number of authors should not high response rate. Up to 2500 words excluding references be more than three. A justification should be included, if the and abstract.number of authors exceeds these limits.
Short CommunicationOnly those who have done substantial work in a particular
Up to 1000 words excluding references and abstract and up to field can write a review article. A short summary of the work 5 references. done by the authors (s) in the field of review should Case reports accompany the manuscript. The journal expects the authors
to give post-publication updates on the subject of review. The New / interesting / very rare cases can be reported. Cases with update should be brief, covering the advances in the field after clinical significance or implications will be given priority, Up to the publication of article and should be sent as letter to editor, 2000 words excluding references and abstract and up to 10 as and when major development occur in the field. references.Sending the Manuscript to the JournalReview articlesArticles should be submitted online at Systemic critical assessments of literature and data sources.
Up to 3500 words excluding references and abstract.1. First Page File: Prepare the title page, covering Letter to the Editorletter, acknowledgement, etc., using a word processor
Should be short, decisive observation. They should not be program. All information which can reveal your identity preliminary observations that need a later paper for
Instructions to Authors
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

I J C D C
765Indian Journal of Comprehensive Dental Care
should be here. Do not zip the files. characters;
2. Article file: The main text of the article, beginning 4. Name of the authors (the way it should appear in the from Abstract till References (including tables) should be in journal), with his or her highest academic degree(s) and this file. Do not include any information such as institutional affiliation; acknowledgement, your names in page headers, etc., in this 5. The name of the department(s) and institution(s) to file. Do not zip the files. Limit the file size to 400 kb. Do not which the work should be attributed; incorporate images in the file. If the file size is large, graphs can
6. The name, address, phone numbers, facsimile be submitted as images separately without incorporating numbers, and e-mail address of the contributor responsible for them in the article file to reduce the size of the file. correspondence about the manuscript;
3. Images: Submit good quality color images. Size of 7. The total number of pages, total number of the image should be as less as possible. All image formats photographs and word counts separately for abstract and for the (jpeg, tiff, gif, bmp, png, eps, etc.) are acceptable; jpeg is most text (excluding the references and abstract). suitable. 8. Source(s) of support in the form of grants, equipment, 4. Legends: Legends for the figures/images should be drugs, or all of these; and included at the end of the article file. 9. If the manuscript was presented as part at a meeting, The authors' form and copyright transfer form has to be the organisation, place, and exact date on which it was read. submitted to the editorial office by post, in original with the Abstract Pagesignatures of all the authors within two weeks of online
submission. Images related to the articles should be sent in a The second page should carry the full title of the manuscript and 'compact disc' or as hard copies to the journal office at the an abstract (of no more than 150 words for case reports, brief time of acceptance of the manuscript. These images should of reports and 250 words for original articles). The abstract should high resolution and exceptional quality. be structured and state the Context (Background), Aims, Settings
and Design, Methods and Material, Statistical analysis used, Editorial officeResults and Conclusions. Below the abstract should provide 3 to DR SHANTUN MALHOTRA ( EDITOR-IN-CHIEF)10 key word.
SRI GURU RAM DAS INSTITUTE OF DENTAL SCIENCES & IntroductionRESEARCH, MALL MANDI, G.T.ROAD AMRITSAR-143006State the purpose of the article and summarize the rationale for PUNJABthe study or observation.
E-MAIL- [email protected] Ph.no- 09317741818 Methods
Preparation of the ManuscriptDescribe the selection of the observational or experimental
Microsoft Word must be used to submit a subjects (patients or laboratory animals, including controls) manuscript. The text must be double spaced with 1" margins clearly. Identify the age, sex, and other important characteristics and justified to the left-hand margin. Avoid using "styles" or of the subjects. Identify the methods, apparatus (give the document templates. The "Normal" Word format is manufacturer's name and address in parentheses), and recommended. (Arial 12 pt text is preferred.) The manuscripts procedures in sufficient detail. Give references to established should be typed in A4 size (212 × 297 mm) paper, with margins methods, including statistical methods; provide references and of 25 mm (1 inch) from all the four sides . The language should brief descriptions for methods that have been published but are be British English. Please number all pages. not well known; describe new or substantially modified The text of observational and experimental articles should be methods, give reasons for using them, and evaluate their divided into sections with the headings: Introduction, limitations. Identify precisely all drugs and chemicals used, Methods, Results, Discussion, References, Tables, Figures, including generic name(s), dose(s), and route(s) of Figure legends, and Acknowledgment. Do not make administration. Reports of randomised clinical trials should subheadings in these sections. present information on all major study elements, including the
protocol, assignment of interventions (methods of Title Pagerandomisation, concealment of allocation to treatment groups),
The title page should carry and the method of masking (blinding)1. Type of manuscript Ethics2. The title of the article, which should be concise, but When reporting experiments on human subjects, indicate informative; whether the procedures followed were in accordance with the 3. Running title or short title not more than 50 ethical standards of the responsible committee on human
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

I J C D C
766Indian Journal of Comprehensive Dental Care
experimentation (institutional or regional) and with the order). Identify references in text, tables, and legends by Arabic Helsinki Declaration of 1975, as revised in 2000 (available at numerals in superscript. References cited only in tables or figure http://www.wma.net/e/policy/17-c_e.html). Do not use legends should be numbered in accordance with the sequence patients' names, initials, or hospital numbers, especially in established by the first identification in the text of the particular illustrative material. When reporting experiments on animals, table or figure. Use the style of the examples below, which are indicate whether the institution's or a national research based on the formats used by the NLM in Index Medicus. The council's guide for, or any national law on the care and use of titles of journals should be abbreviated according to the style laboratory animals was followed. used in Index Medicus. Use complete name of the journal for
non-indexed journals. Avoid using abstracts as references. StatisticsInformation from manuscripts submitted but not accepted
When possible, quantify findings and present them with should be cited in the text as "unpublished observations" with appropriate indicators of measurement error or uncertainty written permission from the source. Avoid citing a "personal (such as confidence intervals). Report losses to observation communication" unless it provides essential information not (such as dropouts from a clinical trial). Put a general available from a public source, in which case the name of the description of methods in the Methods section. When data person and date of communication should be cited in are summarized in the Results section, specify the statistical parentheses in the text. For scientific articles, contributors methods used to analyse them. Avoid non-technical uses of should obtain written permission and confirmation of accuracy technical terms in statistics, such as 'random' (which implies a from the source of a personal communication. If the number of randomising device), 'normal', 'significant', 'correlations', and authors is more than six, list the first six authors followed by et al. 'sample'. Define statistical terms, abbreviations, and most
Journal referencessymbols. Use upper italics (P < 0.05). Standard journal articleResultsKulkarni SB, Chitre RG, Satoskar RS. Serum proteins in Present the results in logical sequence in the text, tables, and tuberculosis. J Postgrad Med 1960; 6:113-120. illustrations. Do not repeat in the text all the data in the tables
or illustrations; emphasise or summarise only important Volume with supplementobservations. Shen HM, Zhang QF. Risk assessment of nickel carcinogenicity Discussion and occupational lung cancer. Environ Health Perspect 1994; 102
Suppl 1:275-282. Emphasize the new and important aspects of the study and the conclusions that follow from them. Do not repeat in detail Issue with supplementdata or other material given in the Introduction or the Results Payne DK, Sullivan MD, Massie MJ. Women's psychological section. Include in the Discussion section the implications of reactions to breast cancer. Semin Oncol 1996; 23(1, Suppl 2):89-the findings and their limitations, including implications for 97. future research. Relate the observations to other relevant
Books and Other Monographsstudies. Personal author(s)In particular, contributors should avoid making statements on Ringsven MK, Bond D. Gerontology and leadership skills for economic benefits and costs unless their manuscript includes nurses. 2nd ed. Albany (NY): Delmar Publishers; 1996. economic data and analyses. Avoid claiming priority and
alluding to work that has not been completed. State new Editor(s), compiler(s) as authorhypotheses when warranted, but clearly label them as such.
Norman IJ, Redfern SJ, editors. Mental health care for elderly Recommendations, when appropriate, may be included.
people. New York: Churchill Livingstone; 1996.Acknowledgments
Chapter in a bookAs an appendix to the text, one or more statements should
Phillips SJ, Whisnant JP. Hypertension and stroke. In: Laragh JH, specify contributions that need acknowledging but do not
Brenner BM, editors. Hypertension: pathophysiology, diagnosis, justify authorship, such as general support by a departmental
and management. 2nd ed. New York: Raven Press; 1995. pp 465-chair; Acknowledgments of technical help; and
478. Acknowledgments of financial and material support, which
Tablesshould specify the nature of the support. This should be the last page of the manuscript. Tables should be self-explanatory and should not duplicate
textual material. References
Tables with more than 10 columns and 25 rows are not References should be numbered consecutively in the order in acceptable. which they are first mentioned in the text (not in alphabetic
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2I J C D C
767Indian Journal of Comprehensive Dental Care
Illustrations (Figures) While submitting a revised manuscript, contributors are requested to include, along with single copy of the final Figures should be numbered consecutively according to the revised manuscript, a photocopy of the revised manuscript order in which they have been first cited in the text. with the changes underlined in red and copy of the comments
Symbols, arrows, or letters used in photomicrographs should with the point to point clarification to each comment. The contrast with the background and should marked neatly with manuscript number should be mentioned without fail. transfer type or by tissue overlay and not by pen.
The authors' form and copyright transfer form has to be Titles and detailed explanations belong in the legends for submitted in original with the signatures of all the illustrations not on the illustrations themselves. contributors at the time of submission of revised copy.When graphs, scatter-grams or histograms are submitted the Article printing chargesnumerical data on which they are based should also be
Reprintssupplied. All authors will be sent reprints of journal issue free of cost and The photographs and figures should be trimmed to remove all additional copies can be purchased at Rs 500/ per copy .the unwanted areas. CopyrightsIf photographs of people are used, either the subjects must
not be identifiable or their pictures must be accompanied by The whole of the literary matter is the copyright of the written permission to use the photograph. Editorial Board. The Journal, however, grants to all users a
free, irrevocable, worldwide, perpetual right of access to, and If a figure has been published, acknowledge the original a license to copy, use, distribute, perform and display the work source and submit written permission from the copyright (either in pre-print or post-print format) publicly and to make holder to reproduce the material. A credit line should appear and distribute derivative works in any digital medium for any in the legend for figures for such figures. reasonable non-commercial purpose, subject to proper
The Journal reserves the right to crop, rotate, reduce, or attribution of authorship and ownership of the rights. The enlarge the photographs to an acceptable size. journal also grants the right to make small numbers of printed For online submission Refer to guideline at www.ijcdc.com copies for their personal non-commercial use.
Legends for Illustrations Contributors' Form Available at www.ijcdc.com
Type or print out legends (maximum 40 words, excluding the credit line) for illustrations using double spacing, with Arabic numerals corresponding to the illustrations.
When symbols, arrows, numbers, or letters are used to identify parts of the illustrations, identify and explain each one clearly in the legend.
Explain the internal scale and identify the method of staining in photomicrographs.
Protection of Patients' Rights to Privacy.
Identifying information should not be published in written descriptions, photographs, sonograms, CT scans, etc., and pedigrees unless the information is essential for scientific purposes and the patient (or parent or guardian) gives written informed consent for publication. When informed consent has been obtained, it should be indicated in the article and copy of the consent should be attached with the covering letter.
Sending a revised manuscript

Indian Journal of Comprehensive
Dental Care
JAN - JUNE. 2016 • VOL 5 • ISSUE 1I J C D C
768Indian Journal of Comprehensive Dental Care
From the Patron's Desk ………

Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2I J C D C
769Indian Journal of Comprehensive Dental Care
This issue brings forth a news of sad demise of a very dynamic and visionary personality,
Dr. Sumeet Kaur Sandhu (ex- principal and vice president of the Scientific Society of SGRDIDSR).
Dr. Sumeet was the guiding force behind the vision of formation of the body and always had an
encouraging 'pat on the back' ready for every academic endeavour that the society planned to execute
.With her untiring efforts and renowned persona we were able to execute many academic events in the
institution and also bring forth to the readers ,this publication which has helped a lot of researchers to get
their work published.
I hope her soul rest in peace and she keeps blessing us from her heavenly abode, to motivate us all in our
future endeavours as well.
As I feel its rightly said “ the tribe often feels that the visionary has turned his back on them, when infact
he's just turned his face towards the future”
Dr. Shantun Malhotra
Editor in chief
IJCDC
Editorial
“A STUDY TO ASSESS THE ORAL HEALTH STATUS AND VARIOUS ORAL HYGIENE PRACTICES OF PATIENTS REPORTING TO SGRD DENTAL COLLEGE,AMRITSAR”
ABSTRACT
This study was conducted to assess the oral health status , various oral hygiene
practices and to assess the knowledge regarding the use and importance of
fluoridated toothpaste in prevention of dental caries . The study was
conducted in the department of Oral medicine and Radiology at Sri Guru Ram
Das Institute of Dental sciences and Research Sri Amritsar. A total of 400
patients were enrolled in the study. The information was collected on a
structured format , which was analyzed using SPSS(Version 13). In the present
study we have found that overall dental health status of patients was poor and
they had very less knowledge about proper oral hygiene habits .The knowledge
about role of fluoridated toothpaste in prevention of dental caries was least , ie
only 0.5 % of all knew about it .
Keywords: oral health, hygine, fluoride
770
Corresponding author:Name: Dr. Amaninder K RandhawaAddress: Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.(M) 9876697694Email: [email protected]
1. MDS, Reader, Department of Public Health Dentistry, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
2. BDS, Lecturer, Department of Oral Medicine and Radiology, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
3. MDS, Reader, Department of Public Health Dentistry, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
4. BDS,Lecturer, Department of Public Health Dentistry, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
INTRODUCTION not timely intervened may lead to early bone loss and severe 4 periodontal disease . Nearly 19% of the population aged In a developing country like India , Prevalence and
5 between 65-74 years is edentulous. distribution of periodontal diseases , dental caries , oral
cancers , malocclusion and crippling nature of fluorosis have Another area of concern is tobacco abuse .Tobacco 1 led to a significant burden and economic loss Dental caries consumption is well established risk factors for .
2 development of oral cancer. Which is commonest cancer in is one of the most common cause of tooth loss and is found
India accounting for 50-70% of total cancer mortality. The universally irrespectively of age , gender, caste, creed or
present study was conducted in the department of Oral geographic location .The prevalence of dental caries in India 3 Medicine and Radiology of Sri Guru Ram Das institute of is 50-60%
Dental health sciences and Research Sri Amritsar to assess 4Periodontal disease affects 95-100% of population ,which is the oral health status and various oral hygiene practices and
initially painless, chronic , self destructive leading to gradual to assess the knowledge regarding the use and importance
tooth loss . Initially the disease is confined to gingiva which if
Indian Journal of Comprehensive Dental Care
I J C D C1. Amaninder Kaur Randhawa
2. Gurpreet Kaur
3. Satinder Singh Walia
4. Gursimran Kaur
Date of Submission : 4/2/16 Date of Acceptance : 21/2/16
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

Indian Journal of Comprehensive Dental Care
of fluoridated toothpaste in prevention of caries. once a day were maximum constituting 60.5 %(242),
whereas brushing twice a day were just 37.5%(150) (table 1, Materials and Method graph 1) . Regarding the use of oral hygiene aids and material
This study was conducted to assess the oral health status and used, toothbrush and toothpaste were used maximum various oral hygiene practices and to assess the knowledge constituting 94.75 %( 379) and 93.75 %(375)respectively regarding the use and importance of fluoridated toothpaste (table 2 graph 2). Horizontal method of tooth brushing was in prevention of caries the most commonly used method by majority of subjects
The study was conducted in the department of Oral medicine constituting 69.75 %(279) (table 3, graph 3). Regarding
and Radiology at Sri Guru Ram Das Institute of Dental changing of toothbrush majority of them were those who
sciences and Research Sri Amritsar. A total of 400 patients had no information about the time span of changing the
were enrolled in the study. The information regarding brush. 56.5% were those who believed that brush should be
demographic details, oral hygiene practices, oral health changed when the bristles are worn out (table4, graph 4) .
status was done on a structured format .Type III examination Regarding rinsing of mouth after any meal 45% constituted
was done on dental chair with illumination light, two mouth who rinsed sometimes, whereas 20.25% were those who
mirrors and a CPI probe . The study was conducted over a never rinsed their mouth . Out of all 2% agreed that they use
period of three months from June 2015 to august 2015 some kind of tobacco. Tooth pain has been the maximum
chief complaint of the patient for coming to the dental Results institute constituting 44.5%( table 5, graph5) Regarding
Among total patients the percentage of subjects brushing various dental problems mean DMFT came to be 11,
771
Table 1 : Showing frequency of toothbrushing
How many times do you brush your teeth no %age
1
Never
0 0
2
Once in a week
4 1%
3 More than once a week 4 1%
4 Once a day 242 60.5%
5 More than once a day 150 37.5%
Table 2: Showing various oral hygiene aids used
What oral hygiene aids do you use to clean teeth
no %age
1
Toothbrush
379 94.75
2
Finger
6 1.5
3 Neem stick 15 3.75
4 Salt/ash 2 0.5
5 Toothpaste 375 93.75
6 Tooth powder 20 5
7 Tobacco powder 0 0
8 Others 3 0.75
How do you brush your teeth no %age
1
Horizontal manner
279 69.75
2
Vertical manner
99 24.75
3 Circular motion 12 3
4 others 10 2.5
Table 3: Showing method of brushing used Table 4: Showing time span of changing the toothbrush
When do you change your brush No %age
1
Every month
0 0
2
After three months
113 28.25
3 Once a year 35 8.75
4 When bristles of brush are worn out 226 56.5
5 Not applicable 26 6.5
Table 5: Showing the chief complaint of the patient
What is your chief complaint no %age
1
Tooth pain
178 44.5
2
Carious tooth
42 10.5
3 Bleeding gums 13 3.25
4 Crowding of teeth 8 2
5 Tooth ulceration 6 1.5
6 Bad breath 3 0.75
7 others 150 37.5

Indian Journal of Comprehensive Dental Care
gingivitis constituted 67.5%. The knowledge about know proper type of brushing and how often brushing has to
fluoridated toothpaste and its role in prevention of dental be done probably they might have learnt through popular
caries was the least that is only 0.5%(graph 6). media but are not professionally educated. The prevalence of
oromucosal lesions was 5.25% which was found to be lower DISCUSSION6 7than Axell T etal and Macigo FG etal .The mean DMFT of the
Majority of the population ie more than 90% are using present study has come out to be 11 which was found to be
toothbrush and tooth paste to clean their teeth , and the 8 9higher to than reported by Sendilkumar , Benoit and S horizontal manner of brushing is the most commonly used . 10Saravasan . The overall prevalence of periodontal diseases This reveals that people know about brushing but they don't
772
Graph 1: showing frequency of toothbrushing Graph 2: showing brushing aid and brushing material used
Graph :3 showing method of toothbrushing used Graph 4: showing time duration of changing the toothbrush
Graph 5: showing the chief complaint of the patient Graph 6: showing knowledge about presence of fluoride in toothpaste

Indian Journal of Comprehensive Dental Care
was found to be 67.5% which was found to be lower than 7. Macigo FG ,Mwaniki DL and Guthua SW, ;prevalence of 11Athannnasulli etal but higher than reported by Macedo TC oral mucosal lesions in a Kenyan population with special
12 reference to oral leukoplakia :East African medical etal . In the present study just 0.5 % of patients were aware
journal 1995;72;12;778-782of the importance of fluoride in the toothpaste which was
very low in comparison to the study reported by Jensen 8. Sendilkumar B,KV Arun;Oral health status in East Coastal 13 14 15 etal , Hugosan etal , and Peterson etal Areas of Chennai Tamilnadu ; Journal of the Indian
Association of Public Health Dentistry 2002;11-15Conclusion :
9. Benoit V, Poul EP,and Seydou O, , Oral health status of In the present study we have found that overall dental health
children and adults in urban and rural areas of Burkina status of patients was poor and they had very less knowledge
Faso, African International dental journal (2004) 54, 83-about proper oral hygiene habits . To combat these problems
89a mass health education programme should be undertaken
to educate the population around , regarding oral health and 10. Saravasan s , kalyani v , vijayrani mp etal ; caries care and people should be motivated to utilize the services preavalence and treatment needs of rural school rendered by the college . Existing health care system of children in Chidambrum Taluk , Tamil Nadu , South India government can be utilized for effective referral of patient Journal Dental Research 2008;19(3) ;186-190 from rural places to dental college .
11. Athanassoul i T, Ko lets i –Kounar i H ,Mamai References HomataHPanagopoulus H; Oral health status of adult
population in Athens , Greece , Community dentistry 1. Shah N Oral and dental diseases : causes ,prevention and
and oral epidemiology 1990;17;82-4 treatment strategies NCMH Background Papers Burden
of Disease in India 2004 276-298 12. Macedo TC , Costa MC, Gomes FS, Vienna MI and Santos
CT : Factors related to periodontal disease in rural 2. Joshi N, Rajesh R, Sunitha M : Prevalence of dental caries
population , Brazilian Oral Research 2006 :20(3): 257-62among school children in Kulasekharam village : A
correlated prevalence survey J Indian Soc pedod Prev 13. Jensen O,Gabre P, Skold UM, Birkhed D : Is the use of Dent 2005 ;23(3);138-140 fluoride toothpaste optimal ?Knowledge,attitudes and
behavior concerning fluoride toothpaste and 3. Patro BK : Prevalence of dental caries among adults and
toothbrushing in different age groups in Sweden elderly in an urban resettlement colony of New Delhi
:Community Dentistry and Oral Epidemiology journal of dental research 2008 ;19;2;95-98
:2012:40:175-1844. WHO Global Oral Health Data Bank and WHO oral
14. Hugosan A, Koch G,Gothberg C,Lundin SA etal : oral health country area Profile program 2000
health of individuals aged 3-80 )years in Jonkoping 5. Shah N, Prakash H , Sunderum K etal , Edentulousness ,
,Sweden during 30 years (1973-2003).I. Review of denture wear and denture needs of elderly population –
findings on dental care habits and knowledge of oral a community based study Journal of oral rehabilitation
health .Swed Dent J 2005 :29:125-38;2004 ;31(5); 467 -476
15. Peterson PK, Aleksejuniene, Christenson LB, Eriksen HM 6. Axel T, Zain RB, Siwamongstham P etal ; Prevalence of
etal : Oral Health Behavior and attitudes of adults in oral soft tissue lesions in outpatients at two Malaysaian
Lithuania : acta odontol scand:58(2000):243-248and Thai dental schools ;Community dent Oral
Epidemiol 1990;18;95-99
773

A COMPARATIVE EVALUATION OF ACCURACY OF THE ROOT ZX ELECTRONIC APEX LOCATOR IN THE PRESENCE OF DIFFERENT IRRIGANTS
Abstract
Objective: The aim of this study is to evaluate the accuracy of Root ZX in
determining working length in presence of 2% chlorhexidine and 5% sodium
hypochlorite.
Material and Methods: Thirty extracted, single rooted, single canal human
teeth were used. Teeth were decoronated at CEJ and actual canal length
determined. Then working length measurements were obtained with Root ZX
in presence of 2% chlorhexidine and 5% NaOCl. The working length obtained
with Root ZX were compared with actual canal length and subjected to
statistical analysis.
Results: No statistical significant difference was found between actual canal
length and Root ZX measurements in presence of 2% chlorhexidine. Highly
statistical difference was found between actual canal length and Root ZX
measurements in presence of 5% of NaOCl, however all the measurements
were within the clinically acceptable range of ±0.5mm.
Conclusion: The accuracy of EL measurement of Root ZX within±0.5 mm of AL
was consistently high in the presence of 2% chlorhexidine and 5% sodium
hypochlorite.
Clinical significance: This study signifies the efficacy of ROOT ZX (Third
generation apex locator) as a dependable aid in endodontic working length.
Key words: Root ZX, working length, chlorhexidine, sodium hypochlorite.
774
Corresponding author:Name: Dr. Shantun Malhotra, Address: Department of Conservative Dentistry, SGRD Institute of Dental Sciences & Research , Amritsar-143001Email id: [email protected] (M) +919317741818
1. Reader, Department of Conservative Dentistry, SGRD Institute of Dental Sciences & Research , Amritsar
2. Professor & H.O.D., Department of Conservative Dentistry, SGRD Institute of Dental Sciences & Research , Amritsar
3. Professor, Department of Conservative Dentistry, SGRD Institute of Dental Sciences & Research , Amritsar
4. M . D. S . Re s i d e nt , D e p a r t m e nt o f Conservative Dentistry, SGRD Institute of Dental Sciences & Research , Amritsar
4Introduction variations that make its identification unpredictable.
The establishment of appropriate working length is one of Many methods have been put forward for determination of 5the most critical steps in endodontic therapy. Cleansing, the working length but with varying degree of accuracy.
shaping and obturation of the root canal systems cannot be Traditional methods for establishing the working length
accomplished perfectly unless the working length is include the use of radiography, anatomical averages and 1determined precisely. Working length (WL) is the distance knowledge of the anatomy, tactile sensation and paper
6from a coronal reference point to a point at which the canal point technique. However, the possibility of the 2preparation and obturation should terminate. radiographic distortion, operator measuring errors or use of
an improper radiographic technique can lead to faulty Establishing the working length at the apical constriction is 5
3 readings. considered ideal for endodontic treatment. The apical
constriction (minor apical diameter) is the narrowest apical In order to overcome these drawbacks, electronic apex
portion of the root canal with a variety of morphological locators have been introduced to determine the working
Indian Journal of Comprehensive Dental Care
I J C D C1 Shantun Malhotra2. Rajesh Khanna3. Kanwalpreet Kaur Bhullar4. Mohit Gautam
Date of Submission : 2/3/16 Date of Acceptance : 26/3/16
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2
Indian Journal of Comprehensive Dental Care
7length and form an important adjunct to radiography. The contact to the patient's lip or by an electrode held in the
use of electronic devices to determine the WL was proposed patient's hand. The electrical circuit is complete when the 8 endodontic instrument is advanced apically inside the root first by Custer (1918) , and the first electronic apex locator
canal until it touches periodontal tissue. The display on the (EAL) was developed following Suzuki's investigation of the 9 apex locator indicates that the apical area has been electrical resistance properties of oral tissues (Suzuki 1942).
11,12reached.Sunada in 1962 adopted the principle reported by Suzuki and
was the first to describe the detail of simple clinical device to The electrolytes in root canals are considered to be one of the 10measure working length in patients. main factors that affect the precision of measurements made
13,14 by certain EALs (Fan et al. 2006, Özsezer et al. 2007). All apex locators function by using the human body to
Consequently, it is important to understand the effects of the complete an electrical circuit. One side of the apex locator's
different irrigants that are used in root canal treatment on circuitry is connected to an endodontic instrument. The 15
other side is connected to the patient's body, either by a the accuracy of measurements made by EALs. The effect of
775
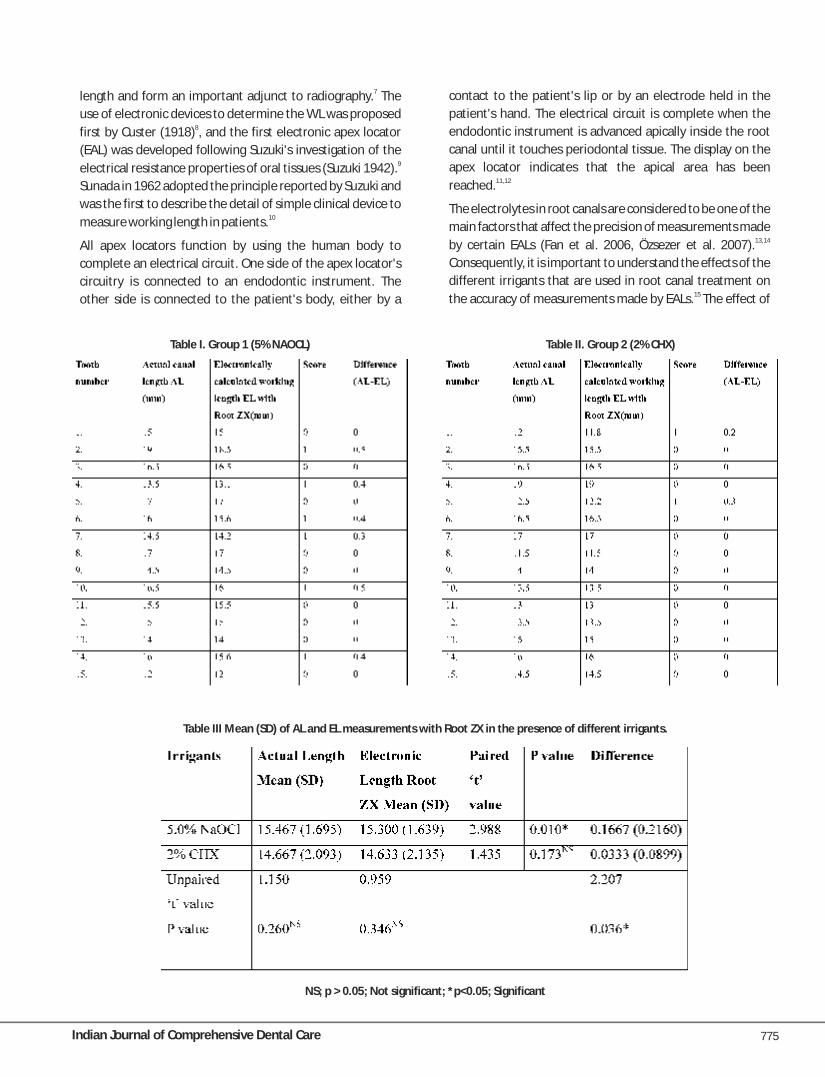
Table I. Group 1 (5% NAOCL) Table II. Group 2 (2% CHX)
Table III Mean (SD) of AL and EL measurements with Root ZX in the presence of different irrigants.
NS; p > 0.05; Not significant; *p<0.05; Significant

Indian Journal of Comprehensive Dental Care
different irrigants on the accuracy of EALs has been evaluated The EAL tested in this experiment was: Root ZX (J. Morita Mfg 16, 17(Kaufman et al. 2002, Erdemir et al. 2007). Corp., Japan). It was used according to manufacturer's
19instructions. Depending on the size of the canal, #15 or #20 However, few studies have focused on the influence of K-file (Mani Inc., Japan), was attached to the file holder and different irrigating solutions used along with electronic apex introduced into the canal. The meter's 0.5 mm reading was locator (Root ZX). Therefore, the purpose of this study was to set between the “APEX” and “1” (factory setting) as indicated compare the accuracy of electronic apex locator (Root ZX) in by a flashing bar and will be used for electronic the presence of commonly used irrigating solutions (Sodium measurements. The file was gently inserted into the root Hypochlorite and Chlorhexidine).canal until the “APEX” signal will be displayed. The file was
Materials and Methods: then gently retracted until the display showed a flashing
Thirty, straight, single-rooted permanent human teeth with image of the root canal and a flashing bar between APEX and
mature apices were selected for this study. The teeth were 1 (0.5 reading). The silicone stopper on the file will be
cleaned of calculus, soft tissues, and debris with hand carefully adjusted to a reference point, and the file was
instrumentation and stored in distilled water until used. withdrawn to measure the distance between the silicone
Teeth with resorption, curvatures, open apices, or stopper and the file tip and noted down. This was recorded as
radiographically invisible canals were excluded from the the electronically measured canal length (EL).
study. The electronically measured Working length (EL) was
The teeth were decoronated at the level of cementoenamel compared with the actual canal (AL) length measured
junction with a diamond disc to allow access to the root canal conventionally and scores were attributed to the resulting 20and to provide a stable reference for all measurements. The values .
coronal portion of each canal was preflared using sequential Comparison between the electronically measured Working
Gates Glidden drills #4, #3, and #2 (Mani Inc., Japan), length (EL) and the actual canal (AL). Score Situation
irrigated with saline and pulp extirpated with a barbed 0 Working Length (WL) equal to gold standard
broach.1 Working Length (WL) from 0.5 to 1mm shorter
Measurement of actual working length than gold standard
Teeth were numbered 1–30 and the actual canal length (AL) 2 Working Length (WL) > 1mm shorter than gold
was determined by introducing a size 10 or 15 k-file (Mani standard
Inc., Japan) into the canal until its tip emerged through the 3 Working Length (WL) exceeds gold standard
major apical foramen. The long axis of the tooth was placed The canal length was assessed for each tooth with individual perpendicular to the line of sight and the tip of the file was irrigants. The results obtained (in millimeters) were positioned tangential to the major apical foramen. After recorded. The difference between the median of electro-carefully adjusting the silicone stopper to the reference nically measured length (EL) and the AL was calculated for point, the file was withdrawn from the root canal, and the each tooth in the presence of all irrigating solutions. The distance between the file tip and silicone stopper was resulting difference in working length was noted down.measured with a scale to the nearest 0.5 mm; 0.5 mm was
subtracted from this length and recorded as AL. Results:
To simulate the periodontium, this study used the in vitro Table I and Table II show the actual working length obtained 18 model as designed by Donnelly. A polystyrene container (30 with conventional method and the electronically measured
ml) was filled with warmed gelatin solution and refrigerated working length obtained with Root Zx using different irrigants
for 2 hrs to set. The apical two thirds of the root was (5% NaOCl & 2% Chlorohexidine). It also indicates the score
embedded in gelatin, and the tooth was stabilized to the lid of given and the difference in working length obtained per
a container with auto-polymerizing resin. The lip electrode tooth.
was also placed in gelatin through another opening in the lid. The mean values of actual canal length and electronically
Working model for electronic working length determi- measured working length with Root ZX along with their
nation differences for two groups are given in table III. Table III
shows that the working length difference obtained by The irrigants tested will be: 5% sodium hypochlorite (NaOCl) different groups of irrigants is statistically significant as P and 2% chlorhexidine gluconate (CHX) The irrigant to be value = 0.036. It depicts that the difference in working length tested was introduced into the canal with a 23-guage needle.obtained with 5% NaOCl are significantly larger than those
776

Indian Journal of Comprehensive Dental Care
obtained with 2% Chlorohexidine. with that of the actual root canal length. In this in vitro study
electronic apex locator namely Root ZX was used to calculate Although statistically significant difference exists between the length of the root canal.the irrigants, the majority of the readings were within the
acceptable range of ±0.5 mm for Root ZX. However, there is still a concern as to whether high
electroconductive irrigants such as saline, anesthetic The results indicate that Root ZX is accurate within ±0.5mm solution, and sodium hypochlorite can affect the of these 100% of the time with two test irrigants.
25new-generation EALs performance.Discussion
The present study used an in vitro model as described by Establishment of the correct working length is an important
Donnelly to obtain accurate measurements. The advantages stage in root canal treatment, because sufficient evidence
of the model were its simplicity, ease of use and the ability to suggests that instrumentation either beyond or too short of
have strict control over the tested experimental condition. A 21apex can adversely affect success. disadvantage of the model is its inability to fully simulate in
18Historically, conventional radiography has been the primary vivo conditions.
means for determining the working length in endodontic The use of irrigating solutions is an important aspect of
therapy. However radiographs have inherent limitations like endodontic treatment. Sodium hypochlorite (NaOCl) is the
providing only two-dimensional images of three-most popular irrigating solution. NaOCl ionizes in water into
22dimensional objects. Na and the hypochlorite ion, OCl, establishing an equilibrium
The EAL is a device used to accurately determine the location with hypochlorous acid (HOCl). At acidic and neutral pH, 3 23of the apical foramen. Kuttler and Green have shown that chlorine exists predominantly as HOCl, whereas at high pH of
28 the apex coincides with the anatomical foramen no more 9 and above, OCl predominates. Hypochlorous acid is
than 50% of the time. This limits the usefulness of responsible for the antibacterial activity. NaOCl is commonly 24radiographs, even if the quality is excellent. An excellent used in concentrations between 0.5% and 6%. It is a potent
adjunct, therefore, is the use of an EAL. The first-generation antimicrobial agent, killing most bacteria instantly on direct
EALs were resistance-based and the second-generation EALs contact. It also effectively dissolves pulpal remnants and 5were impedance-based apex locators. The main collagen, the main organic components of dentin. Hypo-
shortcomings of these EALs included poor accuracy in the chlorite is the only root-canal irrigant of those in general use
presence of fluids and pulp tissue, and the need for that dissolves necrotic and vital organic tissue. It is difficult to 25calibration. The frequency-based third-generation EALs imagine successful irrigation of the root canal without
20have more powerful microprocessors and are able to process hypochlorite.
mathematical quotient and algorithm calculations required Chlorhexidine gluconate (CHX) is widely used in disinfection 26
29to give accurate readings. in dentistry because of its good antimicrobial activity. CHX is
Root ZX (J. Morita Mfg Corp., Kyoto, Japan) is a marketed as a water-based solution and as a gel (with
third-generation EAL that uses dual frequency and Natrosol). Some studies have indicated that the CHX gel has a
comparative impedance principle is based on the “ratio slightly better performance than the CHX liquid but the 30method” for measuring canal length. This method reasons for possible differences are not known. CHX
simultaneously measures the impedance values at two solutions in concentrations of 0.2–2% are considered 31frequencies (8 and 0.4 kHz) and calculates a quotient of toxicologically safe. However, there is paucity of research
32impedances. This quotient is expressed as a position of the regarding the accuracy of EAL in presence of Chlorhexidine. 27 file in the canal. Root ZX requires no calibration, and can be It is imperative that the clinician should be confident of the
5used when the canal is filled with a strong electrolyte. fact that irrigating solution is not effecting the accurateness 20of the apex locator.The fourth-generation apex locators do not process the
impedance information as a mathematical algorithm, but The study confirms that, Root ZX is 100% accurate within 0.5
instead they take the resistance and capacitance mm from the apical foramen. Thus, measurements attained
measurements separately and compare them with a within this tolerance are considered highly accurate.
database to determine the distance to the apex of the root According to this study, statistically significant difference was 26canal. found when measurements were done in canals irrigated
with 5% sodium hypochlorite. The possible reason for this However, only few investigations have been carried out to variation could be the higher electrical conductivity of compare the electronic root canal length measurements sodium hypochlorite.
777
Indian Journal of Comprehensive Dental Care
This study shows that Root ZX can reliably be used for
determining the position of the apical foramen in the
presence of above mentioned irrigating solutions.
Conclusion
It can be concluded that Root ZX can accurately determine
the root canal length within ±0.5 mm from the apical
constriction. Therefore it is clinically safe and accurate to use
Root ZX with the two mentioned irrigating solutions in this
study.
References
1. Inoue N, Skinner DH. A simple and accurate way of
measuring root canal length. J Endod. 1985; 11(10): 421
427.
2. Glossary. Contemporary terminology for Endodontics. Int Endod J. 2007; 40(5), 391–397.
6th ed. Chicago: American Association of Endodontists; 18. Donnelly JC. A simplified model to demonstrate the 1998. operation of electronic root canal measuring devices. J
3. Kuttler Y. Microscopic investigation of root apexes. J Am Endod. 1993; 19(11) :579-80.
Dent Assoc. 1955; 50(5): 544-552. 19. J Morita corp. Fully automatic root canal length
4. Nekoofar MH, Ghandi MM, Hayes SJ, Dummer PM. The measuring device. Root ZX operation instructions.
fundamental operating principles of electronic root 2000:1-9.
canal length measurement devices. Int Endod J. 2006; 20. Khattak O, Raidullah E, Francis ML. A comparative 39(8): 595-609. assessment of the accuracy of electronic apex locator
5. Ingle JI, Bakland LK. Endodontic cavity preparation. 5th (Root ZX ) in the presence of commonly used irrigating
ed. B.C. Decker: Elsevier Inc; 2002. p. 405-507 solutions. J Clin Exp Dent. 2014; 6(1): 41-46.
6. Plotino G, Grande NM, Brigante L, Lesti B, Somma F. Ex 21. Arora RK, Gulabivala K. An in vitro evaluation of the
vivo accuracy of three electronic apex locators: Root ZX, ENDEX and RCM mark II electronic apex locators in root
Elements Diagnostic Unit and Apex Locator and ProPex. canal with different contents. Oral Surg Oral Med Oral
Int Endod J. 2006; 39(5): 408-414. Pathol Oral Radiol Endod 1995; 79(4) :497-503.
7. Jain S, Kapur R. Comparative evaluation of accuracy of 22. Guise GM, Goodell GG, Imamura GM. In vitro
two electronic apex locators in the presence of various comparison of three electronic apex locators. J Endod.
irrigants: An in vitro study Contemp Clin Dent. 2012; 2010; 36(2): 279-281.
3(Supple 2):140-145 23. Green D. Stereomicroscopic study of 700 root apices of
8. Custer LE. Exact methods of locating the apical foramen. maxillary and mandibular posterior teeth. Oral Surg.
J Natl Dent Assoc 1918; 5(8): 815–819. 1960; 13(6): 728–733.
9. Suzuki K Experimental study on iontophoresis. 24. Olson AK, Goerig AC, Cavataio RE, Luciano J. The ability of
the radiograph to determine the location of the apical
foramen. Int Endod J. 1991; 24(1): 28–35.
25. Kim E, Lee SJ. Electronic apex locator. Dent Clin North
Am. 2004; 48(1): 35-54.
26. Gordon MPJ, Chandler NP. Electronic apex locators. Int
Endod J.2004; 37(7): 425-437.
27. Kobayashi C, Suda H. New electronic canal measuring
device based on the ratio method. J Endod. 1994; 20(3):
111-114.
28. Barrette WC Jr, Hannum DM, Wheeler WD, Hurst JK
General mechanism for the bacterial toxicity of
tubules. Int Endod J. 2006; 39(2): 127–135.
14. Özsezer E, Inan U, Aydin U. In vivo evaluation of ProPex
electronic apex locator. J Endod. 2007; 33(8): 974–977.
15. Duran-Sindreu F, Gomes S, Stöber E, Mercadé M, Jané L,
Roig M. In vivo evaluation of the iPex and Root ZX
electronic apex locators using various irrigants Int Endod
J. 2013; 46(8): 769-774.
16. Kaufman AY, Keila S, Yoshpe M. Accuracy of a new apex
locator: an in vitro study. Int Endod J. 2002; 35(2):
186–192.
17. Erdemir A, Eldeniz AU, Ari H, Belli S, Esener T. The
influence of irrigating solutions on the accuracy of the
electronic apex locator facility in the Tri Auto ZX
handpiece.
J Jpn
Stomatol Soc. 1942; 16: 411–417.
10. Sunada I. New method for measuring the length of the
root canal. J Dent Res. 1962; 41: 375-87.
11. Aurelio JA, Nahmias Y, Gerstein H. A model for
demonstrating an electronic canal length measuring
device. J Endod. 1983; 9(12) :568-569.
12. Nahmias Y, Aurelio JA, Gerstein H. An in vitro model for
evaluation of electronic root canal measuring devices. J
Endod. 1987;13(5): 209-14
13. Fan W, Fan B, Gutmann JL, Bian Z, Fan MW. Evaluation of
the accuracy of three electronic apex locators using glass
778

Indian Journal of Comprehensive Dental Care
hypochlorous acid: abolition of ATP production. 31. Yesilsoy C, Whitaker E, Cleveland D, Phillips E, Trope M.
Biochemistry. 1989; 28(23): 9172-9178. Antimicrobial and toxic effects of established and
potential root canal irrigants. J Endod. 1995; 21(10): 513-29. Russell AD, Day MJ. Antibacterial activity of 515.chlorhexidine. J Hosp Infect. 1993; 25(4): 229-238.
32. Jenkins JA, Walker WA, Schindler WG, Flores CH. An 30. Ferraz CC, Gomes BP, Zaia AA, et al. In vitro assessment of invitro evaluation of the accuracy of the Root ZX in the the antimicrobial action and the mechanical ability of presence of various irrigants. J Endod. 2001; 27(3): 209-chlorhexidine gel as an endodontic irrigant. J Endod. 211.2001; 27(7): 452-455.
779

EVALUATION OF REMINERALIZATION OF ENAMEL WITH TOPICAL APPLICATION OF CALCIUM PHOSPHATE BASED AGENTS: A QUANTITATIVE ENERGY DISPERSIVE X- RAY ANALYSIS USINGSCANNING ELECTRON MICROSCOPY: AN IN-SITU STUDYAbstract
This study quantitatively evaluated the remineralization potential of Casein
phosphopeptide-amorphous calcium phosphate, Casein phosphopeptide-
amorphous calcium phosphate containing 900 ppm fluoride and Novamin on
enamel subsurface lesions using scanning electron microscopy with energy
dispersive X-ray analysis (SEM-EDX). Forty five patients were divided equally
into three groups: group A, group B and group C (n=15), based on the
remineralizing agent that was used on the experimental demineralized tooth
slab. Casein Phosphopeptide-Amorphous Calcium Phosphate containing 900
ppm fluoride (CPP-ACPF) had significantly higher remineralization potential
than Novamin. However no statistically significant difference was found
between the remineralization potential of Casein Phosphopeptide-
Amorphous Calcium Phosphate (CPP-ACP) and Casein Phosphopeptide-
Amorphous Calcium Phosphate containing 900 ppm fluoride and between the
remineralization potential of Casein Phosphopeptide-Amorphous Calcium
Phosphate (CPP-ACP) and Novamin. It can be concluded that all the three
agents significantly remineralized the artificial enamel subsurface lesions.
Keywords: CPP-ACP, Novamin, demineralization, remineralisation, energy
dispersive X-ray analysis.
780
Corresponding author:Name: Dr. Tawanpreet KaurAddress: Sri Guru Ram Das Institute of DentalSciences and Research, Amritsar.
1. PG student, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
2. Professor & Head Deptt. of Conservative Dentistry and Endodontics, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
3. MDS, Reader, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
4. MDS, Reader, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
INTRODUCTION The minimal invasive approach focuses on the usage and
application of remineralizing agents to tooth structure Preservation of a healthy set of natural teeth for each (enamel and dentin lesions). These agents aim at controlling patient should be the objective of every dental surgeon. All the demineralization/ remineralization cycle, depending work in the health field is aimed at conservation of the
2upon the microenvironment around the tooth.human body and its function; similarly, dentistry's goal 1should be to preserve healthy, natural tooth structure. Casein phosphopeptide-amorphous calcium phosphate
(CPP-ACP), derived from milk protein casein, has been In the past, dentistry's approach towards management of a reported to reduce demineralization of the tooth structure caries lesion was focused primarily on operative treatment. and enhance remineralization. The anticariogenic potential An increased understanding of the caries process and and remineralizing effects have been shown in in-vitro and remineralization, and changes in caries prevalence has
3in situ studies. Also Bioactive glass (Novamin) in an aqueous catalyzed the evolution in caries management from G.V. 1 environment releases bioavailable calcium, sodium and Black's “extension for prevention” to “minimally invasive”.
Indian Journal of Comprehensive Dental Care
I J C D C1. Tawanpreet Kaur2. Rajesh Khanna3. Rupam Kaur4. Aashish Handa
Date of Submission : 28/8/15 Date of Acceptance : 1/10/15
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

Indian Journal of Comprehensive Dental Care
phosphate ions contributing to the remineralization 5mm×4mm×2mm in size, was cut into acrylic base to house 4process. the demineralized tooth slab (4mm×3mm×3mm). Both the
appliance and demineralized tooth slab were autoclaved Quantitative measurements of changes in a tooth's mineral before the tooth slab was subjected to remineralization content in a single caries lesion are desirable. One of the most procedure in the oral cavity of the patient. recent techniques is Scanning Electron Microscopy with an
5 Forty five patients were divided equally into three groups: Energy Dispersive X- ray analysis.
group A, group B and group C (n=15), based on the The remineralization potential of CPP-ACP has been remineralizing agent that was used on the experimental evaluated mainly in in-vitro conditions and rarely in the oral demineralized tooth slab.environment of the patients. Further, the remineralization
Group A: Casein phosphopeptide-Amorphous calcium potential of bioactive glass has so far not been evaluated and
phosphate (CPP-ACP) used as remineralizing agent (n=15).compared with CPP-ACP and CPP-ACP containing fluoride.
Therefore the objective of this study was to evaluate the Group B: Casein phosphopeptide-Amorphous calcium remineralization potential of three different calcium phosphate containing 900 ppm fluoride (CPP-ACPF) used as phosphate based remineralizing agents in the oral remineralizing agent (n=15).environment of the patients; so that caries process can be
Group C: Novamin containing dentifrice (Vantej) used as intervened at an early stage thus preserving maximum
remineralizing agent (n=15).amount of natural tooth structure.
The remineralising agent was applied three times a day for 3 MATERIALS AND METHOD
minutes for 14 days. The appliance was worn for a minimum The in-situ study was conducted on forty-five freshly of 10 hours during daytime. The subjects were instructed to extracted caries free premolars obtained from the patients remove their appliances while performing oral hygiene undergoing orthodontic treatment. Teeth with intrinsic procedures, eating, drinking and sleeping. After removing stains, teeth with any wasting diseases like attrition, the appliances, the patient was instructed to store the abrasion, erosion, teeth with developmental anomalies and appliance in a sealed plastic bag in a humidified environment teeth with any restoration were excluded from the study. until reinsertion. At the end of the14th day, the tooth slab
was removed from the appliance for further evaluation.The same forty-five patients from whom the premolars were
extracted were taken for this study. It was ensured that the The sound, demineralized and remineralized tooth slabs thus selected patients were not having any current caries activity, obtained from each tooth were then examined under periodontal disease, or any other oral pathology; none of Scanning Electron Microscope and Energy Dispersive X- Ray them were using antibiotics or other medications that affect analysis was used to measure mineral content. The calcium, salivary flow rate. Also the medical history of the patients phosphate and fluoride content, in percentage weight, thus was taken and the patients allergic to milk or milk products measured in sound, demineralized and remineralized tooth were not selected for the study. The treatment plan was slabs was tabulated and put to statistical analysis.explained to the patient and written consent from the
RESULTSpatient was taken for following the treatment regime.
Tables I, II and III depict the mean calcium, phosphate and The crown of each of these premolar teeth was then
fluoride content (in wt %) in sound, demineralised and sectioned to obtain total of three tooth slabs
remineralised enamel slabs in group I, II and III. (4mm×3mm×3mm). Out of the three slabs obtained from
ANOVA test showed that the difference in calcium content in each tooth, one tooth slab was kept, in a clean container in a remineralized enamel slabs between different groups was humidified environment, as a positive control. The rest of the statistically significant; p=0.049 (Table I). The difference in two tooth slabs were immersed in 20ml of a demineralizing phosphorus content in sound, demineralized and solution (solution containing 2.2mM KH PO , 50mM acetic 2 4
remineralized enamel slabs between different groups was acid and 2.2mMCaCl with pH adjusted to 4.4) for a period of 2
not statistically significant; p=0.614, p=0.493 and p=0.104 24 hours. Out of the two demineralized tooth slabs, one respectively (Table II). The difference in fluorine content in tooth slab was then kept, in a clean container in a humidified sound, demineralized and remineralized enamel slabs environment, as a negative control. The other demineralized between different groups was not statistically significant; slab was inserted / fixed into a removable appliance. p=0.476, p=0.857 and p=0.094 respectively (Table III).
A removable mid - palatal appliance was fabricated using DISCUSSIONself-cure acrylic resin extending from the first premolar
region to the first/second molar region. A rectangular trough, Casein (derived from the Latin word 'caseus' meaning
781

Indian Journal of Comprehensive Dental Care
transient increase in pH occurs that facilitates the
precipitation of calcium and phosphate from the particles
and from saliva to form a calcium phosphate (Ca-P) layer on
tooth surfaces. As the reactions and the deposition of Ca-P
complexes continue, this layer crystall izes into
hydroxycarbonate apatite, which is chemically and 7structurally similar to biological apatite.
Therefore the objective of this in situ study was to evaluate
the remineralisation potential of three different calcium-
phosphate based remineralising agents i.e. Casein
Phosphopeptide-Amorphous Calcium Phosphate (CPP-ACP),
Casein Phosphopeptide-Amorphous Calcium Phosphate
containing 900 ppm fluoride (CPP-ACPF) and Novamin.
In Group I, after remineralisation the calcium content
increased to 43.26 wt% from 40.31 wt %; phosphorus
content increased to 20.88 wt% from 18.79 wt %; whereas cheese) is the predominant phosphoprotein in bovine milk fluorine content increased to 3.09 wt% from 1.88 wt %. In and accounts for almost 80 percent of its total protein, Group II, after remineralisation the calcium content primarily as calcium phosphate stabilized micellular
6 increased to 43.61 wt% from 40.37 wt %; phosphorus complexes.content increased to 21.68 wt% from 19.15 wt %; whereas
The concept of casein phosphopeptide amorphous calcium fluorine content increased to 3.59 wt% from 2.02 wt %. In
phosphate as a remineralizing agent was first postulated in Group III, after remineralisation the calcium content
1998. The remineralization process involves diffusion of increased to 42.36 wt% from 40.24 wt %; phosphorus
calcium and phosphate ions through the protein/water-filled content increased to 21.00 wt% from 19.22 wt %; whereas
pores of the carious surface enamel into the body of the fluorine content increased to 3.11 wt% from 1.88 wt %. These
enamel lesion. Once in the body of the enamel lesion, these findings are in concurrence with the study by Narayana SS, et 2+calcium and phosphate species increase the activities of Ca 4al. (2014) who found that calcium, phosphorus and fluorine 3-and PO , thereby increasing the degree of saturation with 4 content in enamel slabs remineralized by CPP-ACP, CPP-ACPF
5respect to hydroxyapatite.and Novamin was higher as compared to their respective
Novamin is the trade name for a calcium sodium demineralized controls. These results are also in concurrence 5phosphosilicate bioactive glass. In aqueous environments, with the study by Hegde MN and Moany A. (2012) who
+such as saliva, sodium ions (Na ) in calcium sodium found that 10% CPP-ACP paste significantly remineralized the phosphosilicate particles immediately begin to exchange artificial enamel subsurface lesions in vitro and the with hydrogen cations (H+ or H O+). This rapid exchange of remineralization rates increased with the time for which the 3
2+ 3–ions allows calcium (Ca ) and phosphate (PO ) species to be enamel was exposed to the CPP-ACP paste. The 4
calcium/phosphate ratio increased from 1.6227 at the end of released from the particle structure. A modest localized,
782
Table-I
Statistical Analysis (anova Test) Of Calcium Content In Sound,
Demineralised And Remineralised Enamel Slabs
Of Different Groups Of Remineralizing Agents
Table-II
Statistical Analysis (anova Test) Of Phosphorus
Content In Sound, Demineralised And Remineralised
Enamel Slabs Of Different Groups Of Remineralizing Agents
Table-III
Statistical Analysis (anova Test) Of Fluorine Content In Sound,
Demineralised And Remineralised Enamel Slabs Of
Different Groups Of Remineralizing Agents

Indian Journal of Comprehensive Dental Care
th th7 day to 1.6947 at the end of 14 day; and was 1.9373 at the potential of CPP-ACP and CPP-ACPF (p=0.502). Also Shetty S, th 14
end of 35 day. These findings are further supported by et al. (2014) found statistically insignificant difference 8 between the remineralization potential of CPP-ACP and CPP-Grewal N, et al. (2013) who found that application of CPP-
ACPF (p=1.000).ACP for 14 days remineralized erosive enamel lesions.
15These findings are also in concurrence with those of Kumar Further, in a study Lata S, et al. (2010) found that the
9 combination of fluoride and CPP-ACP does not provide any VL, et al. (2008) who found that CPP-ACP showed higher
additive remineralization potential when compared to remineralization potential when used in combination with
fluoride varnish alone at the surface level. These results are fluoride (13% reduction in lesion depth) as compared to CPP 16
alone (10% reduction) or fluoride alone (7% reduction). further supported by Jayarajan J, et al. (2011) who found 10 that though CPP-ACPF showed marginally more amount of Moreover in an animal study, Reynolds EC, et al. (1995)
remineralization than CPP-ACP but the difference between showed that rats receiving 0.5% CPP-ACP plus 500 ppm
remineralization potential of CPP-ACPF and CPP-ACP was not fluoride had significantly lower caries scores than those
statistically significant (p<0.05).receiving either 0.5% CPP-ACP or 500 ppm fluoride alone.
However these findings are not in concurrence with the ANOVA test of statistical analysis shows that the difference in 17
calcium content in sound and demineralized enamel slabs study by Srinivasan N, et al. (2010) who found
between different groups was not statistically significant; remineralization effect of CPP-ACP with 900 ppm fluoride to
p=0.506 and p=0.962 respectively. However the difference in be superior to that of CPP-ACP alone. It was observed that
calcium content in remineralized enamel slabs between post-erosion, CPP-ACP increased surface microhardness by
different groups was statistically significant; p=0.049. Also 46.24% whereas CPP-ACPF increased surface microhardness
the difference in net gain in calcium content between by 64.25%. These findings are also not in concurrence with 18different groups was found to be statistically significant; Reynolds EC, et al. (2008) who found dentifrice with 2%
p=0.013. The difference in phosphorus content in sound, CPP-ACP plus 1100-ppm fluoride to be superior to CPP-ACP
demineralized and remineralized enamel slabs between alone or fluoride alone in promoting in-situ remineralization
different groups was not statistically significant; p=0.614, (P < 0.01). Further the results of the present study are also 19p=0.493 and p=0.104 respectively. However the difference in not in concurrence with Mehta AB, et al. (2014) who
net gain in phosphorus content between different groups compared the remineralization potential of Novamin and
was found to be statistically significant; p=0.037. The CPP-ACP and found Novamin to have higher (statistically
difference in fluorine content in sound, demineralized and significant) remineralization potential compared to CPP-ACP
remineralized enamel slabs between different groups was (p=0.013).
not statistically significant; p=0.476, p=0.857 and p=0.094 Therefore, it can be concluded that three different calcium respectively. Also the difference in net gain in fluorine phosphate based remineralizing agents i.e. Casein content between different groups was found to be not Phosphopeptide-Amorphous Calcium Phosphate (CPP-ACP), statistically significant; p=0.152. Casein Phosphopeptide-Amorphous Calcium Phosphate
These findings are in concurrence with the study by containing 900 ppm fluoride (CPP-ACPF) and Novamin do 11Krithikadatta J, et al. (2013) who found that fluoride have a remineralizing potential when applied for 14 days. But
incorporated in 10% CPP-ACP complex did not improve the there is insufficient clinical trial evidence (in quantity, quality
degree of remineralization when compared to 10% CPP-ACP or both) to make a recommendation regarding the long-term
used alone. The plausible hypothesis for this observation in effectiveness of Casein derivatives and Novamin in
10% CPP-ACP was attributed either to the presence of preventing caries in vivo.
fluoride ions in saliva or subjacent plaque that could have CONCLUSIONplayed a role in the formation of fluorapatite or to the pH
The following conclusions were drawn from the present range in the subjects being closed to neutral as at pH range study:from 7.0-6.0 CPP-ACPF and CPP-ACP solutions are found to
1. Casein Phosphopeptide-Amorphous Calcium Phosphate produce similar levels of remineralization. This hypothesis
containing 900 ppm fluoride (CPP-ACPF) had can explain the observations of the present study.
significantly higher remineralization potential than These findings are also in accordance with the study by 12 Novamin.
Mehta R, et al. (2013) who found no significant difference
2. However no statistically significant difference was found between the remineralization potential of CPP-ACP and CPP-13 between the remineralization potential of Casein ACPF after 14 days (p=0.21). Patil N, et al. (2013) also found
Phosphopeptide-Amorphous Calcium Phosphate (CPP-no significant difference between the remineralization
783

Indian Journal of Comprehensive Dental Care
ACP) and Casein Phosphopeptide-Amorphous Calcium Johnson IH, et al. Anticariogenicity of calcium phosphate
Phosphate containing 900 ppm fluoride and between complexes of tryptic casein phosphopeptides in the rat.
t h e re m i n e ra l i za t i o n p o t e n t i a l o f C a s e i n J Dent Res 1995; 74(6): 1272-1279.
Phosphopeptide-Amorphous Calcium Phosphate (CPP- 11. Krithikadatta J, Fredrick C, Abarajithan M, Kandaswamy ACP) and Novamin. D. Remineralisation of occlusal white spot lesion with a
3. Scanning Electron Microscope images revealed mineral combination of 10% CPP-ACP and 0.2% sodium fluoride
deposits on the surface of remineralized enamel slabs in evaluated using Diagnodent: a pilot study. Oral Health
all the three groups, thus indicating the remineralization Prev Dent 2013; 11(2): 191-196.
potential of these agents. 12. Mehta R, Nandlal B, Prashanth S. Comparative
REFERENCES evaluation of remineralization potential of casein
phosphopeptide-amorphous calcium phosphate and 1. Murdoch-Kinch CA and McLean ME. Minimally invasive casein phosphopeptide-amorphous calcium phosphate dentistry. J Am Dent Assoc 2003; 134(1): 87-95.fluoride on artificial enamel white spot lesion: an in vitro
2. Rao A and Malhotra N. The role of remineralizing agents light fluorescence study. Indian J Dent Res 2013; 24(6): in dentistry: a review. Compend Contin Educ Dent 2011; 681-689.32(6): 26-33.
13. Patil N, Choudhari S, Kulkarni S, Joshi SR. Comparative 3. Vashisht R, Indira R, Ramachandran S, Kumar A, evaluation of remineralizing potential of three agents on
Srinivasan MR. Role of casein phosphopeptide artificially demineralized human enamel: An in vitro amorphous calcium phosphate in remineralization of study. J Conserv Dent 2013; 16(2): 116-120.white spot lesions and inhibition of Streptococcus
14. Shetty S, Hegde MN, Bopanna TP. Enamel mutans? J Conserv Dent 2013; 16(4): 342-346.remineralization assessment after treatment with three
4. Narayana SS, Deepa VK, Ahamed S, Sathish ES, different remineralizing agents using surface Meyappan R, Satheesh Kumar KS. Remineralization microhardness: An in vitro study. J Conserv Dent 2014; efficiency of bioactive glass on artificially induced 17(1): 49-52.carious lesion an in-vitro study. J Indian Soc Pedod Prev
15. Lata S, Varghese NO, Varughese JM. Remineralization Dent 2014; 32(1): 19-25.potential of fluoride and amorphous calcium
5. Hegde MN and Moany A. Remineralization of enamel phosphate-casein phosphopeptide on enamel lesions: subsurface lesions with casein phosphopeptide- An in vitro comparative evaluation. J Conserv Dent 2010; amorphous calcium phosphate: A quantitative energy 13(1): 42-46.dispersive X-ray analysis using scanning electron
16. Jayarajan J, Janardhanam P, Jayakumar P, Deepika. microscopy: An in vitro study. J Conserv Dent 2012; Efficacy of CPP-ACP and CPP-ACPF on enamel 15(1): 61-67.remineralization-an in vitro study using scanning
6. White AJ, Gracia LH, Barbour ME. Inhibition of dental electron microscope and Diagnodent. Indian J Dent Res erosion by casein and casein-derived proteins. Caries 2011; 22(1): 77-82.Res 2011; 45(1): 13-20.
17. Srinivasan N, Kavitha M, Loganathan SC. Comparison of 7. Burwell AK, Litkowski LJ, Greenspan DC. Calcium sodium the remineralization potential of CPP-ACP and CPP-ACP
phosphosilicate (NovaMin): remineralization potential. with 900 ppm fluoride on eroded human enamel: An in Adv Dent Res 2009; 21(1): 35-39. situ study. Arch Oral Biol 2010; 55: 541-544.
8. Grewal N, Kudupudi V, Grewal S . Surface 18. Reynolds EC, Cai F, Cochrane NJ, Shen P, Walker GD, remineralization potential of casein phosphopeptide- Morgan MV, et al. Fluoride and casein phosphopeptide - amorphous calcium phosphate on enamel eroded by amorphous calcium phosphate. J Dent Res 2008; 87(4): cola-drinks: An in-situ model study. Contemp Clin Dent 344-348.2013; 4(3): 331-337.
19. Mehta AB, Kumari V, Jose R, Izadikhah V. 9. Kumar VL, Itthagarun A, King NM. The effect of casein Remineralization potential of bioactive glass and casein
phosphopeptide - amorphous calcium phosphate on phosphopeptide-amorphous calcium phosphate on remineralization of artificial caries- like lesions: an in initial carious lesion: An in-vitro pH-cycling study. J vitro study. Aust Dent J 2008; 53: 34-40. Conserv Dent 2014; 17(1): 3-7.
10. Reynolds EC, Cain CJ, Webber FL, Black CL, Riley PF,
784

PREVALENCE OF DENTAL ANOMALIES IN PATIENTS
WITH CLEFT LIP AND PALATE
ABSTRACT
Background: Cleft lip and palate is among the most common congenital human
malformations. When compared with the general population, subjects with a
cleft lip and palate have been found to have a higher prevalence of dental
anomalies.
Aims: The purpose of the following study is to investigate the frequency of
various dental anomalies in patients with unilateral and bilateral cleft lip and
palate, both inside and outside the cleft region, and the possible association
between the side of the cleft and the side of the dental anomalies.
Materials and method: 100 patients with cleft lip and palate with age ranging
from 8 to 25 years were included in the study. Diagnostic records, including
orthopantomograms, lateral cephalograms, dental casts and photographs
were evaluated for the prevalence rates of three different dental anomalies i.e.
missing, impacted and supernumerary teeth for each group.
Results: A significantly high proportion of subjects were having at least one
dental anomaly with the most prevalent being missing maxillary lateral incisors
in the cleft region. Missing, impacted as well as supernumerary teeth were
significantly higher in the cleft side of unilateral cleft lip and palate patients. In
bilateral cleft lip and palate patients missing and supernumerary teeth were
higher on both sides of the defect whereas impacted occurred only on one side
of the defect.
Conclusion: Thus, the management of dental anomalies should be central to
the treatment planning process of individuals with a cleft.
Keywords: cleft, lip, anomalies, orthodontics
785
Corresponding author:Name: Dr. Sukhdeep Singh KahlonAddress: Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar(M) 919888897473Email: [email protected]
1. MDS, Professor, & H.O.D., Sri Guru Ram Das Institute of Dental Sciences And Research, Amritsar.
2. MDS, Senior lecturer, Sri Guru Ram Das Institute of Dental Sciences And Research, Amritsar.
3. PG Student, Sri Guru Ram Das Institute of Dental Sciences And Research, Amritsar.
4. BDS, Lecturer, Sri Guru Ram Das Institute of Dental Sciences And Research, Amritsar.
INTRODUCTION dental arch in various cleft groups and found that a
significant proportion (96.7%) of subjects with the cleft had Cleft lip and palate (CLP) is among the most common 6at least one dental anomaly. Shapira et al found that in the congenital human malformations. Failure of fusion of the
cleft area, most developmental dental irregularities are maxillary and medial nasal prominences or between the related to the maxillary lateral incisors in both deciduous palatal processes results in clefts of varying extent,
1 and permanent dentition. Dental anomalies may be a unilaterally or bilaterally. It affects between 1 and 7 of 1000 2,3 complicating factor in dental as well as orthodontic newborns with higher frequency in Asian people.
treatment planning, hence a detailed examination to Compared to general population, CLP subjects have a higher determine the existence of anomalies is required before the prevalence of dental anomalies, such as variation in tooth initiation of orthodontic correction. This is especially true number and position and reduced tooth dimensions, most
4 5 with regard to orthodontic treatment that involves of which is localised in cleft area. Akcam et al investigated extractions, which relies on healthy remaining teeth and the frequency of various dental anomalies in the maxillary roots to accommodate force application.
Indian Journal of Comprehensive Dental Care
I J C D C1. 2. Chetan Dev Singh Boparai3. Tahira kaur Bawa4. Sukhamrit Kaur
Sukhdeep Singh Kahlon
Date of Submission : 3/3/16 Date of Acceptance : 16/3/16
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

Indian Journal of Comprehensive Dental Care 786
Table I Sample distribution according to gender Table II Sample distribution according to cleft type
Table III Prevalence of missing teeth according to gender
Table IV Prevalence of missing teeth according to side involved
Table V Prevalence of supernumerary teeth according to gender
Table VI Prevalence of supernumerary teeth according to side involved
Table VII Prevalence of impacted teeth according gender Table VIII Prevalence of impacted teeth according to side involved
AIM AND OBJECTIVES used for the observation purposes. Panormic, periapical and
occlusal radiographs were used to determine the presence or The purpose of the following study is to investigate the absence of teeth. All the radiographs were of diagnostic frequency of various dental anomalies in patients with clarity. Subjects who were a part of the study did not have unilateral and bilateral cleft lip and palate, both inside and clefts as a part of a craniofacial syndrome. outside the cleft region, and the possible association
between the side of the cleft and the side of the dental The following anomalies were investigated:
anomalies. 1. Missing/Agenesis: Congenital absence of a permanent
MATERIALS AND METHOD tooth or germ.
The sample consisted of 100 consecutive patients of repaired 2. Supernumerary teeth: Those that appear in addition to
cleft lip and palate with the age group ranging from 8 to 25 the regular number of teeth.
years. The subject distribution according to gender and mean 3. Impaction: A tooth that is not expected to erupt age is described in Table I. The patients were divided into 2 completely into its normal functional position based on groups, patients with bilateral and unilateral complete cleft clinical and radiographic assessment (Thilander and
7lip and palate as mentioned in Table II. Jakobsson, 1968).
Lateral cephalograms, OPGs, photos and dental casts were

Indian Journal of Comprehensive Dental Care
STATISTICAL ANALYSIS strongly with the severity of clefts, which was in accordance
to the present study which indicated that the number of A single observer analyzed the dental casts, photographs and subjects suffering from hypodontia was highest in bilateral radiographs. Student t test and Chi Square test were done to
9CLP subjects . No significant difference was found in determine the comparisons between cleft and non-cleft side prevalence of hypodontia between the sexes. 76.9 % of male data for both males and females. Statistical significance was subjects and 88.6 % female subjects suffered from set at p<0.05. hypodontia. These numbers are significantly greater than the
RESULTS 6findings of Shapira et al who reported the incidence of Results showed that missing teeth were found in 81% of the hypodontia at 46% in boys and 31% in girls. Also, maxillary cleft patients with a higher predilection in males (61.7%) lateral incisor was the most prevelant missing tooth followed compared to females (Table III). A significantly higher by the maxillary second pre molars. number of missing teeth were seen in the cleft side of ULCP
Supernumerary teeth were found in 10% of the subjects; patients (34.3% showed involvement on ipsilateral side, 10% 2which is almost double the 5.4% in the study of Kim et al . on contralateral side and 35.7% involving both sides) as
Also, supernumerary teeth occurred in the maxilla, depicted in Table IV and on both the sides in BCLP patients 10corresponding to the findings of Kraus et al , who proposed (83.3%). These values were statistically significant with p
that it occurred more frequently in maxillary lateral incisor value< 0.001.
region adjacent to the cleft followed by maxillary second pre Supernumerary teeth were seen in only 10% patients, more molars. commonly in UCLP patients with a higher incidence in males
Analysis of impacted teeth of the subjects showed that the (6%) as shown in Table V. Among the BCLP patients, 10%
highest prevalence was in the maxillary arch of both cases showed prevalence of supernumerary teeth with
unilateral and bilateral CLP subjects, mostly affecting involvement on both the sides. In ULCP patients, 4.3%
maxillary canines. The varying results reported in the showed involvement on ipsilateral side followed by 2.85% on
literature can be explained by the application of different contralateral side and 2.85% involving both sides (Table VI).
criteria in different studies and a lack of standardization of Impacted teeth were observed in 23% of the patients with a the data. However, a much greater sample size would be higher prevalence of 56.5% in UCLP female patients (Table necessary to draw more precise conclusions.VII). Among the BCLP patients, 10% cases showed
CONCLUSIONinvolvement on one side whereas 6.7% showed involvement
The most common dental anomaly in the cleft lip and palate on both the sides. In ULCP patients, 18.6% showed patient is that of missing tooth, the most common being involvement on ipsilateral side, 4.3% on contralateral side maxillary lateral incisor followed by maxillary second pre and 2.9% involving both sides (Table VIII).molar. Both supernumerary and impacted teeth occur mostly
DISCUSSIONin the maxillary arch with the maxillary canines as the most
Study of the most common patterns of dental anomalies frequently affected teeth in both types of clefts. No sex (shape, number and location) in subjects with complete differences were found in regard to the prevalence of unilateral cleft lip and palate, either in the cleft area missing, impacted or supernumerary teeth. Missing, (involving the permanent lateral incisor) or outside it, is impacted as well as supernumerary teeth were significantly important for accurate, timely and effective orthodontic higher in the cleft side of unilateral cleft lip and palate treatment planning. Also, the prevalence of dental anomalies patients. In bilateral cleft lip and palate patients missing and has been found to vary among different racial/ethnic groups. supernumerary teeth were higher on both sides of the defect The rate of overall dental anomalies has generally been whereas impacted occurred only on one side of the defect. found to be higher among cleft patients in comparison with The management of dental anomalies, which can easily be the general population, with anomalies most often located in detected by careful inspection of routine orthodontic
8the area of the cleft (Ribeiro et al., 2003) . This corresponds diagnostic records, should be taken into consideration in with the findings of the present study where a significant treatment planning of individuals with a cleft.portion of individuals with cleft (89%) found to have at least
REFERENCESone dental anomaly. In this present study, the prevalance of h
1. Altalibi, M., Saltaji, H., Edwards, R., Major, P.W., Flores-ypodontia was found to be 81% in cleft patients, which
Mir, C. Indices to assess malocclusions in patients with 6coincides with the findings of Shapira et al (77%) . Ranta
cleft lip and palate. Eur J Orthod. 2013;35:772–782.reported that the prevalence of hypodontia increases
787

Indian Journal of Comprehensive Dental Care
2. Kim, N.Y., Baek, S.H. Cleft sidedness and congenitally impaction of maxillary canines. Acta Odontologica
missing or malformed permanent maxillary lateral Scandinavica 26: 145–168.
incisors in Korean patients with unilateral cleft lip and 8. Ribeiro L L, DasNeves L T, Costa B, Gomide M R 2003 alveolus or unilateral cleft lip and palate. Am J Orthod Dental anomalies of the permanent lateral incisors and Dentofacial Orthop. 2006;130:752–758. prevalence of hypodontia outside the cleft area in
3. Jamilian, A., Nayeri, F., Babayan, A. Incidence of cleft lip complete unilateral cleft lip and palate. Cleft Palate
and palate in Tehran. J Indian Soc Pedod Prev Dent. Craniofacial Journal 40: 172–175.
2007;25:174–176. 9. Ranta R 1986 A review of tooth formation in children
4. Lourenço Ribeiro, L., Teixeira Das Neves, L., Costa, B., with cleft lip and palate. Am J Orthod Dentofacial
Ribeiro Gomide, M. Dental anomalies of the permanent Orthop. 90: 11–1.
lateral incisors and prevalence of hypodontia outside 10. Kraus, B.S., Jordan, R.E., Pruzansky, S. Dental the cleft area in complete unilateral cleft lip and palate. abnormalities in the deciduous and permanent Cleft Palate Craniofac J. 2003;40:172–175. dentitions of individuals with cleft lip and palate. J Dent
5. Akcam, M.O., Evirgen, S., Uslu, O., Memikoglu, U.T. Res. 1966;45:1736–1746.
Dental anomalies in individuals with cleft lip and/or
palate. Eur J Orthod. 2010;32:207–213.
6. Shapira, Y., Lubit, E., Kuftinec, M.M. Hypodontia in
children with various types of clefts. Angle
Orthod.2000;70:16–21.
7. Thilander B, Jakobsson S O 1968 Local factors in
788

A CLINICAL STUDY TO COMPARE VARIOUSBLOOD CELL PARAMETERS FOR ASSESSMENT OF ANAEMIA OF CHRONIC DISEASE IN HEALTHY SUBJECTS AND CHRONIC PERIODONTITIS PATIENTS
ABSTRACT
Periodontitis is an inflammatory disease of the supporting tissues of the tooth.
An immune response to bacteria and their products induces a major vascular
response, offering explanatory mechanisms for the interactions between
periodontal infection and a variety of systemic disorders. Therefore,
periodontitis results in low-grade systemic inflammation, may cause decreased
erythropoiesis and lower haemoglobin concentration.
Aims: This study is aimed at the assessment of various blood cell parameters in
healthy subjects and those with chronic periodontitis
Methods and Material: 100 patients with severe chronic periodontitis (test
group) and 100 periodontally healthy subjects (control group) in the age group
of 20-60 years participated in the study. The blood sample obtained by
venupuncture from antecubital fossa, was taken in anticoagulant coated
vacuum tubes. Measurement of all blood cell parameters was done.
Statistical analysis used: Mann Whitney U test and Pearson chi square test were
used.
Key-words: anaemia, chronic periodontitis, systemic inflammation
789
Corresponding author:Name: Dr. Navkiran,M.D.S., Dept of Periodontology, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsaremail: [email protected]
1. M.D.S., Professor and Head, Department of Periodontology, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar
2. M . D . S . S t u d e n t , D e p a r t m e n t o f Periodontology, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar
3. Reader, Department of Periodontology, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar
4. S e n i o r L e c t u r e r, D e p a r t m e n t o f Periodontology, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar
5. Name of the department and institution to which the work is attributed: Department of Periodontology, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
INTRODUCTION by periodontal tissues in response to bacterial infection,
suggesting that periodontitis may cause ACD. However, Periodontitis is an inflammatory disease of the supporting conflicting results have been reported regarding the tissues of the tooth caused by specific microorganisms in a
[5,6][1] association between the two.susceptible host. Studies have associated periodontitis
with various systemic conditions, indicating that The present clinical study is undertaken to compare the [3] periodontitis leads to low-grade systemic inflammation. various blood cell parameters in healthy subjects and those
with chronic periodontitis. Anaemia of chronic disease (ACD), is the anaemia occurring
in chronic infections that is not due to dysfunction of bone MATERIALS AND METHODS:
marrow cells or other diseases, and occurring despite the A total of 200 systemically healthy patients visiting the out [4]presence of adequate iron stores and vitamins. It is due to patient department of Sri Guru Ram Das Institute of Dental
the increased production of cytokines that mediate the Sciences and Research, Amritsar participated in the study. immune or inflammatory response, which are also released The following selection criteria were applied to the
Indian Journal of Comprehensive Dental Care
I J C D C1. 2. Anooja Lall3. Ashish Verma4. Sahib Tej Singh
Navkiran
Date of Submission : 13/1/16 Date of Acceptance : 22/1/16
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

Indian Journal of Comprehensive Dental Care 790
Males Females p value
n(200) 68
132
0.073Test (100) 28
72
Control (100) 40
60
Table 1. Demographic and characteristics of two study groups Table 2. Mean Gingival Index and Mean Plaque
Index values of two study groups
Test (100)
Control (100)
z value
p value
Mean GI
2.37±0.48
1.21±0.49
1.16
<0.05
Mean PI
2.25±0.43
1.35±0.49
1.5
<0.05
Table 3. Reference ranges, mean values, p values of all the blood parameters in both the study groups.
Range Test Control p value
Hb (mg/dl)
M: 13-18
F: 11.5-16.5
12.02±1.01
13.4±1.5
<0.05
RBC
(million/mm3)
M: 4.74-5.49
F: 4.14-4.79
4.5±0.19
4.6±0.41
<0.05
MCV (n)
80-100
83.4±1.5
85.4±3.8
0.43
MCH (mg/dl)
32-38
30.4±1.2
33.1±1.6
0.06
MCHC (%) 37-49 35.4±1.6 36.2±1.5 <0.05
TLC
(million/mm3)
4000-11000
9582.09±648.6
8950.3±859.
4
<0.05
N (%) 50-70
70.14±1.3
69.91±2.8
<0.05
E (%) 1-6
2.73±0.6
2.37±0.5
0.43
L (%) 30-40
38.15±2.7
36.67±2.4
<0.05
M (%) 2-10
1.84±0.7
1.81±0.67
0.2
BT (min) 1-5 2.15±0.5 2.25±0.38 0.81
CT (min) 2-7 4.35±0.4 4.31±0.4 0.57

Indian Journal of Comprehensive Dental Care
patients: RESULTS
Inclusion Criteria The present study showed the differences in the blood cell
parameters in healthy subjects and those with chronic 1. Patients aged 20-60 years of age.periodontitis. There were more females in both the groups.
2. Patients diagnosed with chronic periodontitis i.e. The study showed no significant gender predisposition probing depth ≥ 5mm. between male and female patient groups suffering from
Exclusion Criteria anaemia of chronic disease. (Table 1)
1. Those with acute or chronic medical conditions like The mean gingival and plaque index were significantly higher
bacterial, viral or fungal infections. in patients with chronic periodontitis as compared to
healthy group subjects. The mean gingival index of test 2. History of smokinggroup was 2.37 with a standard deviation of 0.48 i.e.
3. Any history of recent trauma or tooth extraction.2.37±0.48 as compared to control group which was
4. History of periodontal surgery or antibiotic uptake in 1.21±0.49, whereas the mean plaque index of test group was
last 3 months. 2.25±0.43 as compared to control group i.e. 1.35±0.49, both
the values being statistically significant. (Table 2)5. Pregnant/ lactating females.
The present study showed decrease in haemoglobin levels The study population was divided into two groups:and erythrocyte count in chronic periodontitis patients as
Group 1 (Control): Periodontally healthy subjectscompared to healthy subjects. The mean RBC count in test
Group 2 (Test): Those with moderate to severe periodontitis. group is 4.5±0.19 whereas it is 4.6±0.41 in control group (p
value <0.05), which is statistically significant. The mean Prior to the study, the design and purpose of the study was MCHC concentration of test group is 35.4±1.6, which is less explained to the patients, a detailed proforma was prepared, as compared to that of control group i.e. 36.2±1.5 (p value and informed consent was obtained from all subjects. A full <0.05), which is statistically significant. The mean MCH and mouth periodontal examination of all the subjects was done MCV values were almost similar in both the groups and were using the following clinical parameters:not statistically significant (p values 0.43 and 0.06 7Gingival Index (Loe and Silness, 1963)respectively).
Plaque Index (Turesky Gilmore modification of Quigley Hein The TLC count was increased in test group (9582.09±648.6)
8Plaque Index)as compared to control group (8950.3±859.4), with increase
Pocket probing depth (PPD) using calibrated William's in counts of neutrophils, lymphocytes and eosinophils. The probe) increase in neutrophil count was statistically significant
(70.14±1.3 in test group and 69.91±2.8 in control group) and Sample Collectionincrease in lymphocyte count was also significant
After recording the clinical parameters, 5 ml of venous blood statistically (38.15±2.7 in test group and 36.67±2.4 in control
was drawn under aseptic conditions, from the ante-cubital group). The increase in eosinophil count was not statistically
fossa. It was transferred immediately to EDTA significant (p value 0.2).
(ethylenediaminetetraacetic acid) containing vacutainers to (Table 3)be transported to the Medical Laboratory. The estimation of
the following haematological parameters was done: The present study showed decrease in levels of HB, RBC
count, MCHC and increase in TLC levels in periodontitis Haemoglobin (Hb), RBC count, Total Leukocyte Count (TLC), patients, as compared to healthy control group subjectsDifferential Leukocyte Count (DLC), Mean Corpuscular
Volume (MCV), Mean Corpuscular Haemoglobin (MCH), DISCUSSIONMean Corpuscular Haemoglobin Concentration (MCHC),
Various epidemiological studies showed that periodontitis is Bleeding Time (BT) , Clotting time (CT)
associated with an increased risk of systemic disorders like All the measurements were done using standardized and cardiovascular diseases, cerebrovascular ischemia, and
[9] automated procedures using Poch 100i. atherosclerosis, preterm low birth weight. The present
study was aimed at showing an association between chronic The data was collected and analysed using Mann Whitney U periodontitis and anaemia of chronic disease.test. Pearson Chi square test was also applied to study the
statistical significance between the blood parameters and In India, anaemia is more prevalent in females because of the periodontal variables. poor nutrition, increased menstrual losses, high incidence of
791

Indian Journal of Comprehensive Dental Care
tropical and intestinal infections, and other miscellaneous Due to stasis, the central stream of cells widens and the
factors. Females are also prone to hormonal imbalance peripheral zone becomes narrower because of plasma loss
during puberty, during the reproductive phase, and toward by exudation. After this margination, the neutrophils of
menopausal age. The microbial flora and host immune central column come close to the vessel wall as a result of
response are altered leading to exaggerated response of the redistribution. All consequences finally cause increase in [10] [17]periodontal tissues to local factors . The present study did neutrophils and leukocytes.
not show any significant association between any gender The results of the present clinical and haematological trial predilection and anaemia of chronic disease in male and indicates that chronic periodontitis may be considered to
[11] female patients (p 0.073). In a study by Virdi et al (2013) it have a tendency towards the development of anaemia, as it was observed that haematological values in females were may cause decrease in number of erythrocyte count, Hb, less as compared to males. The possible reason for this could decreased MCHC and an increase in the levels of be hormonal changes encountered in females during neutrophils, lymphocytes and total leukocyte count. Further pregnancy, lactation, menstrual cycle, reproduction etc. as longitudinal studies are needed to investigate the
[14]reported by Bentley ME and Griffiths PL in 2003. association of blood cell parameters with periodontitis.
The present study showed that there is decrease in values of CONCLUSIONhaemoglobin, RBC count and MCHC in patients with chronic
The present study showed a positive association between periodontitis as compared to periodontally healthy subjects.
the haematological parameters i.e. Hb, RBC, TLC, MCHC and These results are in accordance with the study of Virdi H
severity of chronic periodontal disease. It can be concluded [11](2013) , which showed that the mean values of that like any other chronic condition, periodontitits may
haemoglobin and red blood cell indices were significantly tend towards anaemia. Such a comparison can add to our
lower and the values of erythrocyte sedimentation rate knowledge regarding changes in blood parameters in
(ESR) were significantly higher in test group as compared to patients with chronic periodontitis. These blood cell
control group, suggesting a mild anaemia. parameters can be utilized as predictors or risk markers of
[2] [13]Studies by Hutter JW et al (2001) , Seigel EH (1945) , life-threatening systemic diseases and may give an early [12]Gokhale SR (2010) also indicated that periodontitis option for timely intervention and diagnosis.
patients have a lower hematocrit, lower numbers of REFERENCES
erythrocytes, lower haemoglobin levels and higher 1. Patel M, Shakir QJ, Shetty A. Interrelationship between erythrocyte sedimentation rates, hence indicating that
chronic periodontitis and anemia: a 6-month follow up chronic periodontitis can lead to anaemia. study. J Indian Soc Periodontol 2014;18:19-25.
All the processes involved in the development of ACD can be 2. Hutter JW, Van der Velden U, Varoufaki A, Huffels RA, attributed to the cytokines, including shortened red cell
Hoek FJ, Loos BG.Lower numbers of erythrocytes and survival, blunted erythropoietin response to anaemia, lower levels of hemoglobin in periodontitis patients impaired erythroid colony formation in response to compared to control subjects. J Clin Periodontol erythropoietin, and the abnormal mobilization of 2001;28:930-6.reticuloendothelial iron stores.
3. Scannapieco FA, Bush RB, Paju S. Associations between The present study results showed increase in levels of TLC, periodontal disease and risk for atherosclerosis, neutrophils, lymphocytes and eosinophils, which is in
[16] cardiovascular disease and stroke. A systematic review. correlation to the studies by Kolte R et al (2014) , [15] Ann Periodontol 2003;8:38-53.Agnihotram (2010) , which also showed increase in TLC
levels, neutrophils, lymphocytes count in chronic 4. Weiss G, Goodnough LT. Anemia of chronic disease. N periodontitis patients as compared to healthy control group Engl J Med 2005;352:1011-23.subjects.
5. Wakai K, Kawamura T, Umemura O, Hara Y, Machida J, It is justified by the fact that in early stages of periodontitis, Anno T, et al. Associations of medical status and physical the rate of blood flow is increased due to vasodilatation. But fitness with periodontal disease. J Clin Periodontol subsequently, there is a slowing and stasis of blood stream. 1999;26:664-72.With stasis, changes in normal axial flow of the blood in the
6. Havemose-Poulsen A, Westergaard J, Stoltze K, Skjodt H, microcirculation take place. The normal axial flow consists of
Danneskiold- Samsøe B, Locht H et al. Periodontal and central stream of cells comprising leukocytes and RBC, and
hematological characteristics associated with aggressive peripheral cell-free layer of plasma close to the vessel wall.
792
Indian Journal of Comprehensive Dental Care
periodontitis, juvenile idiopathic arthritis, and 13. Seigel EH. Total erythrocyte, leukocyte and differential
rheumatoid arthritis. J Periodontol 2006;77:280-8. white cell counts of blood in chronic periodontal disease.
J Dent Res 1945;24: 270.7. Loe H, Silness J. Periodontal diseases in pregnancy I.
Prevalence and severity. Acta Odontol Scand 14. Bentley ME, Griffiths PL. The burden of anemia among
1963;21:533-51. women in India. Eur J Clin Nutrition 2003; 57:52-60.
8. Breuer M, Cosgrove R. The relationship between 15. Agnihotram G, Mahesh Singh TR, et al. Study of clinical
gingivitis and plaque levels. J Periodontol 1989;60:172- parameters in chronic periodontitis. Int J Appl Biol
5. Pharm Technol 2010;1:1202-7
9. Scannapieco FA. Position paper of The American 16. Kotle R, Kotle A, Deshpande N. Assessment and
Academy of Periodontology: Periodontal disease as a comparison of anemia of chronic disease in healthy
potential risk factor for systemic diseases position paper. subjects and chronic periodontitis patients: A clinical
J Periodontol 1998;69:841-50. and haematological study. J Indian Soc Peridontol
2014;18:183-6.10. Amar S, Chung KM. Effects of hormonal variation on the
periodontium in women. Periodontol 2000 1994;6:79- 17. Noack B, Genco RJ, Trevisan M, Grossi S, Zambon JJ, De
87. Nardin E. Periodontal infections contribute to elevated
systemic C-reactive protein level. J Periodontol 2001;72: 11. Kaur Virdi, H. Hematological parameters- A diagnostic 1221-7.mirror for periodontics. Indian Journal of Dental
Sciences 2013;2:45-8.
12. Gokhale SR, Sumanth S, Padhye A. Evaluation of blood
parameters in patients with chronic peridoontitis for
signs of anemia. J Periodontol 2010;81:1202-6.
793

MANAGEMENT OF AMELOGENESIS IMPERFECTA
- AN ESTHETIC REHABILITATION
ABSTRACT
Amelogenesis imperfecta (AI) is a diverse collection of inherited diseases that
exhibit quantitative or qualitative tooth enamel defects in the absence of
systemic manifestations. Also known by varied names such as Hereditary
enamel dysplasia, Hereditary brown enamel, Hereditary brown opalescent
teeth, this defect is entirely ectodermal, since mesodermal components of the
teeth are basically normal. The AI trait can be transmitted by either autosomal
dominant, autosomal recessive, or X-linked modes of inheritance. Genes
implicated in autosomal forms are genes encoding enamel matrix proteins,
namely: enamelin and ameloblastin, tuftelin, MMP-20 and kallikrein – 4. This
case report deals with the treatment of Amelogenesis Imperfecta in 20 year old
patient.
Key words: Full Mouth rehabilitation, enamel, dental, genetic, inherited
Amelogenesis Imperfecta (AI)
794
Corresponding author:Name: . Sonam MahajanSenior Lecturer, Dept. Of Conservative Dentistry and EndodonticsGenesis Institute of Dental Sciences and Research, FerozepurContact- 08146774405Email id: [email protected]
1. Post Graduate Student Dept . Of Conservative Dentistry and Endodontics Genesis Institute of Dental Sciences and Research, Ferozepur
2. Senior Lecturer, Dept. Of Conservative Dentistry and Endodontics Genesis Institute of Dental Sciences and Research, Ferozepur
3. Post Graduate Student, Dept. Of Conservative Dentistry and Endodontics Genesis Institute of Dental Sciences and Research, Ferozepur
4. Dept. Of Conservative Dentistry and Endodontics, Genesis Institute of Dental Sciences and Research, Ferozepur
5. Professor and Head, Dept. Of Conservative Dentistry and Endodontics, Genesis Institute of Dental Sciences and Research, Ferozepur
6. Reader, Dept. Of Conservative Dentistry and Endodontics, Genesis Institute of Dental Sciences and Research, Ferozepur
2INTRODUCTION dentition with mutations in five genes—AMEL, ENAM, 3MMP20, KLK4, and FAM83H . Amelogenesis Imperfecta represents a group of conditions,
genomic in origin affecting the structure and clinical
appearance of the enamel of all or nearly all the teeth which
may be associated with morphologic or biochemical It is an exclusive ectodermal disturbance, related to 1changes elsewhere in the body . The term, AI was alterations in the organic enamel matrix which causes white
introduced by Weinmann and co-workers. It is a hereditary flecks, narrow horizontal bands, lines of pits, grooves, and defect of enamel affecting both the primary and permanent discoloration of the teeth varying from yellow to dark brown
Transmission of the gene is
autosomal dominant, recessive or X linked with an 4prevalence of 1:700 to 1:14,000 .
Indian Journal of Comprehensive Dental Care
I J C D C1. Deepika Singla2. Sonam Mahajan3. Manjot Singh4. Vanita5. Pardeep Mahajan6. Prashant Monga
Date of Submission : 2/1/16 Date of Acceptance : 20/1/16
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

Indian Journal of Comprehensive Dental Care
5,6prone to rapid wear and breakage . With generalized Of Dental Sciences and Research, Ferozepur with a chief
compromise of enamel, there is loss of vertical dimension as complaint of unesthetic smile due to discoloured & rough
well as lack of interproximal contacts, resulting in food front teeth. The family history revealed that her parents had
lodgement and problems associated with it. In most cases a consanguineous marriage (1st cousins) and there was no 3 history of any other members of the family having a similar the esthetic disability is striking . AI has been reported to be
discoloration of the teeth. No significant medical history was associated with other dental conditions such as recorded. Clinical examination of the patient revealed that Taurodontism, pulpal calcifications, multiple tooth there was thin enamel with dark brown pigmentation on the impactions, oligodontia, hyper-cementosis, distorted roots, facial surface, enamel pit defects and light brown bands on aberrant dentin formation and marked follicular hyperplasia
2,7,8,9 the incisal third of the maxillary anterior teeth (FIG 1).and malocclusion .
A treatment plan was developed with the following aims: to According to Witkop, AI can be classified into four main reduce the reported sensitivity of the teeth and to improve types: (1) hypoplastic;(2) hypomaturation; (3) hypocalcified;
2 the esthetics. Esthetic rehabilitation with All Ceramic Crowns and (4) hypomaturation-hypoplastic with taurodontism . was planned but due to financial issues PFM crowns were Each main type of AI may be further divided into several desired by the patient. Root canal treatment was performed subtypes, depending on clinical features and inheritance w.r.t 11,12,21,22 as there was insufficient tooth structure patterns. Other forms of enamel dysmineralization will and further reduction of tooth would lead to pulpal exhibit a pattern based upon the time of insult, thus affecting exposure. The tooth preparation was done for porcelain the enamel forming at the time. In contrast, AI will affect all fused to metal crowns on left and right maxillary incisors. The teeth similarly and can have a familial history. Fluorosis can prepared teeth were then restored with temporary heat cure mimic AI, but usually the teeth are not affected uniformly,
10 acrylic crowns for 3 months for evaluation of esthetic often sparing the premolars and second permanent molars . satisfaction of the patient. After 3 months, the temporary
The condition is a social hindrance to the patient and treating crowns were replaced by PFM crowns in the anterior teeth
such individuals brings drastic transformation in their (FIG 2).10psychosocial behaviour and approach towards life The DISCUSSIONtreatment of patients with AI should be planned taking both
the clinical and the emotional demands into consideration. The term “Amelogenesis Imperfecta” describes a diverse Therefore, the planning of esthetic restorations on the group of hereditary conditions primarily affecting the anterior teeth may not only preserve the tooth structure but quality and/or quantity of dental enamel. The affected teeth
11also eliminate the adverse social impact of their teeth . show a soft enamel of normal thickness that chips and wears 12,13easily and has a radiodensity similar to that of dentin . CASE REPORT
The results of clinical and radiographic evaluations indicated A 20-year-old female patient was referred to the Department that the patient in the present case had hypomaturation of Conservative Dentistry and Endodontics, Genesis Institute form of AI. All the teeth are misshapen, and spotted. The
.
795
FIG 1The exposed dentin was hypersensitive.
Patient had not undergone any restorative treatment for
esthetics before and now desired to improve the appearance of her anterior teeth.
From history & clinical examination it was diagnosed as – Amelogenesis imperfecta of
the Hypomature type.
FIG 2 Oral hygiene instructions were given and the patient was recalled after 1 month for follow
up. A follow up of 24 months showed that esthetic expectations of the patient were
completely fulfilled. Thus, with completion of the treatment, we could not only
conserve the remaining tooth structure but could also improve esthetics of the patient.

Indian Journal of Comprehensive Dental Care
insufficiency of the enamel makes the teeth extremely 5 Soares CJ, Fonseca RB, Martins LR, Giannini M. Esthetic
sensitive to contact and thermal stimuli. These problems rehabilitation of anterior teeth affected by enamel
combine to make early diagnosis essential and immediate hypoplasia: A case report. J Esthet Restor Dent 14,15treatment a necessity, even for the youngest patients . 2001;14:340-8
Currently, the cases of AI are restored with adhesive 6. Crabb JJ. The restoration of hypoplastic anterior teeth restorative techniques, overdentures, fixed partial dentures, using an acid-etched technique. J Dent 1975;3:121-4full porcelain crowns, porcelain fused-to metal crowns and
7. Desort KD. AI: the genetics, classification and treatment. inlay/onlay restorations constitute the contemporary J Prosthet Dent 1983;49:786-92. treatment modalities. However, full porcelain restorations
are becoming increasing popular, because of their inheriting 8. Lykogeorgos T, Duncan K, Crawford PJM, Aldrrd MJ.
eshthetics, excellent biocompatibility and improved physical Unusual manifestations in X-linked AI. Int J Paediatr Dent
properties. Moreover, the advances in the field of esthetic 2003;13:356-61.
dentistry, especially in bonding to dentin, help practitioners 9. Fritz GW. AI and multiple impactions. Oral Surg Oral Med 16,17,18to restore function and esthetics to an acceptable level . Oral Pathol. 1981;51:459-60
But, marginal adaptation and bonding problems have been 19 10. Guideline on Dental Management of Heritable Dental
pointed out as disadvantages of laminate veneers . Developmental Anomalies Reference manual, vol. 36 /
In the present case, metal-reinforced porcelain restorations no. 6 were preferred considering patient's socioeconomic status
11. Shah et al Dental Rehabilitation of Amelogenesis and to redouble the mechanical durability, recover esthetics
Imperfecta in the mixed Dentition, International Journal and protect the residual dentin.
Of Scientific Study, Vol.1, Issue 6, 2014 It is very important that the treatment plan is such
12. W.K. Seow. Clinical diagnosis and management strategies formulated that it prevents the development of
of amelogenesis imperfect variants. Pediatric dentistry psychological problems arising from the appearance of teeth
20 1993; 15:384-93affected by Amelogenesis Imperfecta . Following the
13. P.J.M Crawford ,m. Aldred, and a.Bloch-zupan. treatment, the psychological transformation of this 20 year Amelogenesis impeerfecta. Orphanet journal of rare old girl was spectacular as was evident from her confident diseases 2007;2:17smile during the follow up visits.
14. A.Sengun and F.Ozer. Restoring function and esthetics in CONCLUSIONa patient with amelogenesis imperfecta: a case report.
This clinical report describes the oral rehabilitation of a 20 Quintessence international 2002;33:199-204
year old girl patient affected by Hypomature Amelogenesis 15. D.J. Lamb. The treatment of amelogenesis imperfecta. Imperfecta. The treatment plan for cases of AI is related to
The Journal of Prosthetic Dentistry 1976;36:286-91many factors : the age of the patient, the socioeconomic
status of the patient, the type and severity of the disorder, 16. Gokce K, Canpolat C, Ozel E. Restoring function and and the intraoral situation at the time the treatment is esthetics in a patient with amelogenesis imperfecta: a planned. Thus, rehabilitation in this case included anterior case report. J Contemp Dent Prac 2007;8:0-101PFM crowns to eliminate tooth sensitivity, improve the
17. Christensen GJ. Porcelain-fused to–metal versus non esthetics and restore function.
metal crowns. J Am Dent Assoc 1990;130: 409-11REFERENCES:
18. Sengun A, Ozer F. Restoring function and esthetics in a 1. Aldred MJ, Crawford PJM, Savarirayan R: Amelogensis patient with amelogenesis imperfect: a case report.
imperfecta - a classification and catalogue for the 21st Quintessence Int 2002;33:199-204century. Oral Dis, 2003 9:19-23
19. Ozturk N, Sari Z, Ozturk B. An interdisciplinary approach 2. Witkop CJ. Amelogenesis imperfecta, dentinogenesis for restoring function and esthetics in a patient with
imperfecta, and dentin dysplasia revisited: Problems in amelogenesis imperfecta and malocclusion: a clinical classification. J Oral Pathol 1989; 17:547-53. report. J Prosthet Dent 2004;92:112-15
3. Tunkiwala et al. Conservative esthetic rehabilitation of a 20. I.C. Mackie, a. S. Blinkhorn. Amelogenesis imperfecta: young patient with Amelogenesis Imperfecta, early interception to prevent attrition. Dental update Conservative Restoration, vol.35, No.3, 2014, pp.175- 1991;18: 79-80182
4. Priyadarshini et al Full Mouth Rehabilitation of
amelogenesis Imperfecta- A case report, Endodontology,
150-155
796

NON SURGICAL MANAGEMENT OF GRADE 3 MOBILE TEETH: A CASE REPORT
ABSTRACT
The main goal of endodontic therapy is to eliminate or at least achieve a
significant reduction of microorganisms present in the root canal system. It is
well recognized that chemo-mechanical instrumentation alone is unable to
completely disinfect the root canal system. Use of intracanal medication with
antimicrobial activity between appointments has been recommended to
eliminate possible persistent microorganisms .Calcium hydroxide with its
antimicrobial property has been widely used as inter appointment intracanal
dressing. This paper presents a case report in which Calcium hydroxide was
used as an intracanal medicament for treatment of mobile teeth with
periapical abscess.
Keywords: mobility, calcium hydroxide, pedodontics
797
Corresponding author:Name: Dr. Gunmeen Sadana MDS, Professor and Head, Department of Paediatric and Preventive Dentistry, Sri Guru Ram Das Institute of Dental Sciences and Research, AmritsarEmail: [email protected]
1. MDS, Professor and Head, Department of Paediatric and Preventive Dentistry, Sri Guru Ram Das Institute of Dental Sciences and Research, Sri Amritsar
2. MDS, Reader, Department of Paediatric and Preventive Dentistry, Sri Guru Ram Das Institute of Dental Sciences and Research, Sri Amritsar
3. MDS, Reader, Department of Paediatric and Preventive Dentistry, Sri Guru Ram Das Institute of Dental Sciences and Research, Sri Amritsar
4. MDS Student, Department of Paediatric and Preventive Dentistry, Sri Guru Ram Das Institute of Dental Sciences and Research, Sri Amritsar
INTRODUCTION relation to muscle attachments. In the maxilla, periapical
abscesses drain through the palatal bone into the oral cavity Dentoalveolar abscesses are infections of dental origin, the or rarely into sinus maxillaris or the nasal cavity. The majority with an endodontic or a periodontal pocket origin. mandibular periapical abscess drains commonly through Periapical and periodontal abscesses may advance into
1the buccal bone into the oral cavity. combined periodontal endodontic lesions. Dental
abscesses and abscesses in general expand through tissue Pathology of the periapical abscess
providing least resistance by forming a sinus tract (fistula). — The pathological features of the periapical abscess In case of the periodontal abscess, drainage is most likely to depend on the microbial activity occurring in the apical part take place through the periodontal pocket since this is of the root canal, having little room for expansion except usually the path of least resistance. In case of a periapical through the apical foramen. abscess, the spread is primarily dictated by the thickness of
— The necrotic pulp of the root canal serves as an the overlying bone and the location of the abscess in 2,3important source of bacterial nutrition.
Indian Journal of Comprehensive Dental Care
I J C D C1. Gunmeen Sadana2. Manjul Mehra3. Rashu Grover4. Jasmeet Kaur
Date of Submission : 4/2/16 Date of Acceptance : 12/21/16
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

Indian Journal of Comprehensive Dental Care
Proteolytic bacteria predominate the root canal flora, which CASE REPORT
changes over time to a more anaerobic microbiota A 14 year old patient reported to the department of (microaerophilic streptococci of the "S. milleri" group (S. paediatric and preventive dentistry, Sri Guru Ram Das dental anginosus, S. Constellatus and S. intermedius),anaerobic college and research institute, Amritsar with the complaint streptococci {P. anaerobius and P. micros), gram-positive of mobile teeth with respect to lower anterior teeth region anaerobic rods {Eubacterium spp., Actinomyces spp. And since one year. On oral examination it was seen that the right Propionibacterium spp.) and gram-negative anaerobic rods lower central and lateral incisors and left central incisor were {Porphyromonas spp., Prevotella spp., Bacteroides grade 3 mobile and contacted the lingual cingulum of the spp),Campylobacter spp., Fusobacterium spp. and opposing upper anterior teeth on occlusion. On radiographic
1,4,5Treponema spp.) examination a periapical radiolucency was seen wrt
Even when the infection occurs outside the apical foramen 31,41,42 region (Figure 1). Clinical signs
and in the periapical tissues, immediate drainage is not ( progressive mobility, bone loss) were suggestive of trauma possible and ongoing tissue destruction and pus formation from occlusion. After relieving the occlusion, splinting may result. The abscess usually expands through the bone by followed by root canal treatment was planned for the a sinus tract formation.Microorganisms are the main involved teeth. Teeth were stabilised with a temporary splint etiology of apical inflammatory lesions, and the goal of using ligature wire (temporary splints are used to stabilise endodontic treatment is the prevention and control of pulpal the teeth during the treatment and can be used for 6 and periradicular infections. Various measures have been months). The teeth were isolated using cotton rolls. In the introduced to reduce the number of microorganisms from first visit, an access cavity was prepared with a straight line the root canal system, including various mechanical entry into the root canal using tapered fissure bur. The instrumentation techniques, irrigation regimes, and working length was established with one mm short of the intracanal medicaments. It is difficult to eliminate all radiographic apex (figure 2). Next, pulp extirpation and microorganisms from an infected root canal system by complete debridement of the canal was done followed by
6mechanical instrumentation alone. Thus, chemical copious irrigation with normal saline and 5% sodium irrigation and disinfection are necessary to remove hypochlorite. Open dressing was given to encourage the microorganisms, their byproducts, pulp tissue remnants, drainage. The patient was recalled next subsequent day and and other debris from the root canal. The use of intracanal copius irrigation with saline and 5% sodium hypochlorite medication with antimicrobial activity between was performed. After drying the canals with sterile paper appointments has been recommended to eliminate possible points calcium hydroxide paste was placed in the canals of persistent microorganisms, particularly in case of pulp the teeth. The access cavity was sealed with intermediate
7,8necrosis with periradicular bone loss.
798
Pre operative radiograph Pre operative photograph Figure 1
Working length was determined Calcium hydroxide dressing Figure 2
Obturation radiograph
Figure 3
1 year follow up radiograph and photograph
Figure 4

Indian Journal of Comprehensive Dental Care
restorative material and radiograph was taken. After 2 using an agar diffusion method. They found that Ca(OH)2
months, the teeth were asymptomatic .Obturation was effectively inhibited the growth of all three microorganisms
done with gutta percha using lateral condensation followed after 24 hours, but there was a difference in the sensitivity of by post endo restoration(figure 3) Splint was removed after 3 each microorganism, such that Streptococcus mutans was months from the first visit. Patient was recalled after one the most sensitive and E. faecalis was the least. Some have month from the removal of splint. And followed up every 6 studied Ca(OH)2, chlorhexidine (CHX), and their
15,16,17months for one year. (figure 4) mixtures. Basrani et al., Lin et al. and Ballal et al. found
DISCUSSION that the CHX gel was more effective than the Ca(OH)2 paste 18,19against E. faecalis and C. Albicans. In the present case no The main goal of endodontic therapy is to eliminate or at
carious lesion was present with periodontal attachment least achieve a significant reduction of microorganisms loss, the pulp necrosis might have occurred as a present in the root canal system. It is well recognized that consequence of an accidental trauma which had occurred chemo-mechanical instrumentation alone is unable to
9,10 due to biting on some hard object during chewing. These completely disinfect the root canal system . Use of hard objects are often present as impurities, like stones in intracanal medication with antimicrobial activity between the cereals and pulses. As a result of a severe impact injury appointments has been recommended to eliminate possible which may have been caused by a small hard object, the persistent microorganisms, particularly in case of pulp forces may have got concentrated at small points, resulting in necrosis with periradicular bone loss. Calcium hydroxide excessive pressure in the apical vessels, leading to an with its antimicrobial property has been widely used as inter
101 1 , 1 2 ischaemic infarction. Another cause may be due to trauma appointment intracanal dressing. It has been
from occlusion which may be primary or secondary or demonstrated that treatment with calcium hydroxide as an combined. Following calcium hydroxide dressing for 2 interim dressing in the presence of large and chronic months, the teeth were asymptomatic. Obturation was periapical lesions can create an environment more favorable done with gutta percha using lateral condensation . Splint to healing and encourage osseous repair. Most of the root was removed after 3 months from the first visit. Patient was canal microbes are unable to survive in the highly alkaline recalled after one month from the removal of splint. No environment provided by calcium hydroxide. Several mobility was present on oral examination. Radiographically , bacterial species commonly found in infected root canals are inter proximal bone formation was seen. Patient was eliminated after a short period when in direct contact with followed up every 6 months for one year. Clinically, teeth calcium hydroxide. Antimicrobial activity of calcium were asymptomatic with no mobility. Radiographically, hydroxide is related to release of hydroxyl ions in an aqueous intact lamina dura with normal interproximal bone is seen environment. Hydroxyl ions are highly oxidant-free radicals with complete periapical healing.that show extreme reactivity resulting in the damage to
bacterial cytoplasmic membrane, protein denaturation, and CONCLUSION
damage to Because the endodontic pathogens and their byproducts 9,13 bacterial DNA. It has been asserted that all biological may affect the integrity of the periodontium, they have to be
actions of calcium hydroxide progress by the ionic eliminated during root canal treatment. The placement of 14 calcium hydroxide paste benefits, because of its dissociation in calcium ion and hydroxyl ion (Estrela 1995) .
antibacterial, proteolytic and anti inflammatory properties. Calcium hydroxide is often used to effect periapical healing
by combination of its antimicrobial activity and its ability to BIBLIOGRAPHYpromote hard tissue formation and periodontal healing. A
1. Dahlén G. Microbiology and treatment of dental series of studies demonstrated the antimicrobial effect of
abscesses and periodontal-endodontic lesions. Ca(OH)2). Several researchers investigated the effect of root
Periodontol 2000. 2002;28:206-39.canal medicaments by a direct exposure, and they found that
2. Eabricius L, Dahlen G, Obman A, Moller A. Predominant Ca(OH)2 was effective in killing bacteria. Mehrvarzfar et al. indigenous oral bacteria isolated from infected root compared bioactive glass with Ca(OH)2 and found that both canals after varied times of closure. Scand I Dent Res exhibited antimicrobial effects against E. faecalis and that 1982: 90:134-144.Ca(OH)2 showed a superior disinfecting effect. Blanscet et al.
found that the higher the concentration of the Ca(OH)2 3. Sundqvist G. Ecolog)'of the root canal flora. J Endod paste was, the larger were the zones of inhibition observed. 1992:18: 427-430.Pavelic et al. evaluated the antimicrobial effect of Ca(OH)2 by
4. van Winkelboff A, Carlee A, de Graaff J. Baeteroides
799

Indian Journal of Comprehensive Dental Care
endodontalis and other black-pigmented Baeteroides
species in odontogenic ahscesses. Infect Immun 1985:
49: 494- 497.
5. van Winkelhoff AJ, van Steenhergen TJM, de Graaff J.
Tbe role of black-pigmented Baeteroides in human oral
infections. Clin Periodontol 1988: 15: 145-155.
13. Wood G. Pits, Fistula, and draining lesions (H. M.
cherrick, chaptered.): Differential diagnosis of oral
lesions. 3rd ed. St. Louis, MO: CV Mosby Co. 1985; 199-
201.
14. C. Estrela, “Two methods to evaluate the antimicrobial
action of calcium hydroxide paste,” Journal of
Endodontics, vol. 27, no. 12, pp. 720–723, 2001.6. Shuping GB, Orstavik D, Sigurdsson A, Trope M.
Reduction of intracanal bacteria using nickel-titanium 15. M e h r va r z fa r P, A k h ava n H , R a st ga r i a n H ,
rotary instrumentation and various medications. J Mohammadzade Akhlagi N, Soleymanpour R, Ahmadi A.
Endod 2000;26:751-755. An in vitro comparative study on the antimicrobial
effects of bioglass 45S5 vs. calcium hydroxide on 7. Walton RE. Intracanal medicaments. Dent Clin North Am Enterococcus faecalis. Iran Endod J 2011;6:29-33.1984;28:783-796.
16. Blanscet ML, Tordik PA, Goodell GG. An agar diffusion 8. Kim D, Kim E. Antimicrobial effect of calcium hydroxidecomparison of the antimicrobial effect of calcium as an intracanal medicament in root canaltreatment: ahydroxide at five different concentrations with three literature review - Part II. in vivo studies. Restor Dent different vehicles. J Endod 2008;34:1246-1248.Endod. 2015 May;40(2):97-103.
17. Pavelić B, Anić I, Najzar-Fleger D, Stilinović B, Temmer K. 9. Sheehan DJ, Potter BJ, Davis LS. Cutaneous Draining The antimicrobial efficiency of aqueous solutions of Sinus Tract of Odontogenic Origin: Unusual Presentation calcium hydroxide on Streptococcus mutans, of a Challenge Diagnosis. South Med J. 2005; 98(2): 250-Streptococcus faecalis and Candida albicans, in vitro. 2.Acta Stomatol Croat 1991;25:207-212.
10. GuptaR, PrakashV.NonSurgical Management of 18. Lin YH, Mickel AK, Chogle S. Effectiveness of selected Mandibular Molar with Multiple Intra-oral Sinus Tracts:
materials against Enterococcus faecalis: part 3. The A Case Report. J Clin Diagn Res.2013 Oct;7(10):2392-3.antibacterial effect of calcium hydroxide and
11. Mittal N, Gupta P. Management of Extra Oral Sinus chlorhexidine on Enterococcus faecalis. J Endod 2003; Cases: A clinical Dilemma. J Endod. 2004; 30(7): 541-7. 29:565-566.
12. Gandhi A, Kathuria A, Gandhi T. Endodontic-periodontal 19. Ballal V, Kundabala M, Acharya S, Ballal M. Antimicrobial management of two rooted maxillary lateral incisor action of calcium hydroxide, chlorhexidine and their associated with complex radicular lingual groove by combination on endodontic pathogens. Aust Dent J using spiral computed tomography as a diagnostic aid: a 2007;52:118-121.case report. Int Endod J. 2011; 44(6): 574-82.
800

OBTURATOR PROSTHESIS FOR REHABILITATIONOF ACQUIRED MAXILLARY DEFECT – A CASE REPORT
Abstract :
Malignancies are common in oral region which are treated through surgical
intervention. These surgical interventions sometimes lead to altered anatomy
and devastating effect on the patient's esthetics, self confidence, speech and
mastication. Rehabilitation of these acquired defects can be accomplished by
using various types of microvascular flaps or by prosthetic means. Surgery is
preferred means of treatment but it may not be feasible in many clinical
scenario. So prosthetic rehabilitation is best alternative. Prosthetic
rehabilitation of missing oral and extra oral structures should aim at restoration
of normal function of mastication, speech, swallowing, appearance etc. This
case report describes a case of acquired maxillary defect rehabilitated using an
interim obturator.
Key words: Obturator, Acquired palatal defect, Maxillectomy.
801
Corresponding author:Name: Dr. Akash DuggalAddress: Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.(M) 08054853531Email: [email protected]
1. Akash Duggal, MDS, Reader, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
2. Aman Arora, MDS, Reader, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
3. Parul Duggal, MDS, Oral Medicine and Radiology.
4. Tarunpreet Kaur Gill, Post Graduate Student, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
INTRODUCTION into nasal cavity, impaired mastication and deglutition. At
times it also affects the facial contour of the patient. Malignant neoplasm of upper gingiva and hard palate nearly Rehabilitation of these acquired maxillary defect can be account for 1-5% of total occurrence in the oral cavity. Two accomplished by using various types of flaps or by prosthetic thirds of the lesions which involve these areas are squamous means. Surgical reconstruction is the preferred treatment cell carcinomas.but it may not be feasible in many clinical scenario when
Most of these carcinomas invade the underlying bone when defect is large, chances of recurrence are there and there is diagnosed. The recommended treatment for these types of general disability of patient.lesion are alveolectomy, palatectomy, partial/ total
Prosthetic rehabilitation seems to be a better alternative. maxillectomy. These surgical defects can result in multiple The prosthesis that is fabricated to repair the defect is called problems as it disturbs both form and function of normal as a maxillary obturator. stomatognathic system.
According to Glossary of Prosthodontic terms, an obturator It results in hypernasal speech, regurgitation of food/fluid
Indian Journal of Comprehensive Dental Care
I J C D C1. 2. Aman Arora3. Parul Duggal4. Tarunpreet Kaur Gill
Akash Duggal
Date of Submission : 13/1/16 Date of Acceptance : 2/2/16
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

Indian Journal of Comprehensive Dental Care
is a prosthesis which is fabricated so as to cover or maintain confirmed that there will not be any further tissue changes
the integrity of the intra oral structures which may have been occurring or that the chances recurrence of tumor are
lost as a result of congential, acquired or developmental unlikely, which allows for a permanent prosthetic
disease process. rehabilitation.
Obturators for post surgical defect have been described to be The following case report describes a case of acquired
three types : (1) Surgical obturator (2)Interim Obturator (3) maxillary defect rehabilitated using Interim obturator.
Definitive obturator. CASE REPORT
The surgical obturator - It is a base plate type appliance which A 40 years old male patient (Figure 1) reported to the is constructed from the pre-operative impression cast and Department of Prosthodontics and Crown & Bridge with the inserted at the time of resection of the maxilla in the chief complaint of difficulty in speech and mastication. He operating room to serve as a matrix for keeping surgical was also concerned about esthetics due to acquired packing in place, reducing wound contamination by covering maxillary defect (Aramany Class VI). Patient had a history of the defect, preventing hematoma formation, aiding speech carcinoma and had undergone partial maxillectomy for and deglutition and providing psychological assurance to the resection of the same 2 and a half months ago. On intra-oral patient that rehabilitation has begun. The surgical obturator examination a defect was seen (Figure 2), which extended must not be removed for 7 - 10 days post-surgically. from second premolar region of first quadrant to second
The temporary / interim obturator - An interim obturator is a premolar region of second quadrant and involved the labial
maxillofacial prosthesis which is made following completion sulcus. First and second molars were present on both sides.
of initial healing after surgical resection of a portion or one Initial healing had taken place. An interim obturator was
side or both side maxillae; majority of times some or all teeth planned so that definitive treatment could be delayed until
in the region of the surgical defect are removed during sufficient healing occurs.
surgical procedure. It is provided after few weeks of the Moreover, patient can get accustomed to wearing a healing period. It aids in initial closure of the surgical defect prosthesis until a definitive obturator is fabricated. It was following initial healing. The interim obturator is a planned that acrylic teeth would be incorporated in the provisional prosthesis which is made when a clearly well prosthesis for esthetic purpose but those would be kept out defined surgical defect margin exists and no further surgical of occlusion so that minimum load is exerted on to the still procedures are planned. healing ridges and mucosa.
The definitive obturator - A definitive obturator is a Preliminary impressions were made with irreversible maxillofacial prosthesis that replaces part or all of the maxilla hydrocolloid (Algitex) and stone cast (Gypstone, Prevest, and associated lost teeth due to surgery or trauma. A DenPro) was obtained. (Figure 3)definitive obturator is fabricated only after it has been
Special trays were fabricated with autopolymerizing acrylic
802
Figure 7 : Denture insertionFigure 6 : Finsihed and polished prosthesis
Figure 5 : Investing of waxed up denture
Figure 4: Final cast
Figure 3: Preliminary castFigure 2 : Intra oral photograph of defect
Figure 1: Extra oral photograph of patient

Indian Journal of Comprehensive Dental Care
resin after blocking out undercuts. Border moulding was tissues and ridges. The purpose of interim prosthesis was to
done using low fusing compound and final impression was allow sufficient time so that the patient's awareness of
made with light bodied silicone (Zetaplus). Final cast was wearing a foreign object would decrease gradually with
poured in Type IV gypsum (Kalrock, Kalabhai). (Figure 4) increasing time. Apart from this, it shall also serve as a
diagnostic aid to test patient's ability to manage with the Undercuts were blocked with baseplate wax and obturator. autopolymerizing acrylic resin record bases were fabricated.
Occlusal rims were fabricated and jaw relations recorded. SUMMARY
Teeth arrangement and try-in was done. An interim obturator can be used to rehabilitate an acquired
maxillary defect, protecting it from fluid contamination and Wax-up was done and prostheses invested, dewaxed and resultant infection and aid speech and mastication till processed in conventional manner. (Figure 5)complete healing of the defect occur. Rehabilitation of
Prostheses was retrieved, finished and polished (Figure 6). individuals with acquired maxillary defects requires a Prosthesis was delivered (Figure 7) and patient was recalled sympathetic, patient and sequential approach whereby the after 24 hours, 1 week and 1 month. Patient was satisfied individual should be given time to adjust to the altered with the prosthesis and mentioned an improvement in anatomy of oral cavity and the prosthesis for a successful speech and mastication. prognosis.
DISCUSSION REFERENCES
Rehabilitation of maxillary defects very often puzzles the 1. Mukeshsoni, Jain Deshraj Interim Obturator clinicians as a great dilemma still exists whether to go for Rehabilitation of a Maxillary Defect –Case ReportIOSR surgical or prosthetic rehabilitation. Surgical rehabilitation is Journal of Dental and Medical Science ; Volume 14, Issue not done until the defect is stable and the lesion is less likely 2 Ver. VII (Feb. 2015), PP 01-03.to recur. Also it is not possible in each and every case to go for
2. Tirelli G, Rizzo R, Biasotto M, Di Lenarda R, Argenti B, surgical intervention.Gatto A, Bullo F. Obturator prostheses following palatal
The basic advantage of surgical reconstruction are resection: clinical cases. ActaOtorhinolaryngol Ital. 2010 permanent closure of oro-nasal communication. Problem Feb;30(1):33-39with this procedure are questionable prognosis of
3. Cordeiro PG, Santamaria E. A classification system and vascularized flap with autogenous bone graft particularly for algorithm for reconstruction of maxillectomy and very large defects because the vessels of the free flap are midfacial defects. PlastReconstrSurg 2000;105:2331-compromised with partial necrosis.2346
As reported by Corderio et al, there are systemic 4. Singh M, Bhushan A, Chand S Obturator prostheses for complications in 11.7% of patients and in 9.1% re-exploration
hemimaxi l lectomy pat ients Journal of Oral is necessary because the vessels of the free flap are Rehabilitation 2001 28; 821-829compromised with partial necrosis in 1.8% cases.
5. Mubashir A S et al Management of Post Surgical Defect in Other than this patient needs to be motivated for a second the Mandible with an Interim Obturator: A Case Report surgery and have to be convinced for another surgical wound Int J Oral Health Med Res | MAY- JUNE 2015 | VOL 2 | at donor's site for the graft.ISSUE 1
Prosthetic rehabilitation is seen to be a better alternative for 6. Ahmed Bilal Rehabilitation of surgically resected soft such cases.
palate with Interim Velopharyngeal Obturator. Advantage of of obturators include avoidance of any further International Journal of Oral and Craniofacial Science ; surgery, allowing the defect to keep under control in case of 2015; 1(2); 31-33recurrence of primary disease, provision for replacement of
teeth and can be planned at any time soon after surgical
resection. In this particular case, a temporary/ interim
obturator made up of heat polymerizing acrylic resin was
planned so that definitive treatment could be delayed until
sufficient healing occurs. Acrylic teeth were incorporated
into the prosthesis for esthetics and were kept out of
occlusion so that minimum load is transferred to underlying
803

THE DYNAMIC IMPRESSION TECHNIQUE
FOR RESORBED RIDGES
ABSTRACT
Resorbed mandibular ridge compromises the support, retention and stability
of complete dentures. An impression procedure should be such that it gains
maximum coverage. As osseous structures in resorbed ridges offer little
possibility of retention and stability and also the muscle attachments are
located near the crest of the residual ridge so dislocating effect is more. The
simplest approach is to extend the denture base adequately for proper use of
all available supporting tissues. To achieve this a good impression is required
that could be accurately recorded in the impression by means of dynamic
technique.
Key words: resorbed mandibular ridge, dynamic impression, tissue
conditioner.
804
Corresponding author:Name: Dr. Aman AroraAddress: Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.(M): 09855906097Email: [email protected]
1. Reader, Deptt Of Prosthodontics, Sri Guru Ram Das Institute of Dental Sciences and Research, Sri Amritsar
2. Post Graduate student, Deptt Of Prosthodontics, Sri Guru Ram Das Institute of Dental Sciences and Research, Sri Amritsar
3. Reader, Deptt. of Oral Medicine, Diagnosis & Radiology, Sri Guru Ram Das Institute of Dental Sciences and Research, Sri Amritsar
4. Reader, Deptt Of Prosthodontics, Sri Guru Ram Das Institute of Dental Sciences and Research, Sri Amritsar.
Introduction technique which uses tissue conditioner and final wash
impression made with light body elastomeric impression Complete dentures are primarily mechanical devices but material.since they function in the oral cavity, they must be fashioned
so that they are in harmony with the normal neuromuscular CASE REPORT
function. Residual ridge resorption is a complex biophysical A 65 years old male patient reported to the department of process and a common occurrence following extraction of prosthodontics and crown and bridge, with Chief Complaint teeth. Ridge atrophy is most dramatic during the first year of loose lower denture posing difficulty in eating and after tooth loss followed by a slower but more progressive speech. History of the patient revealed that the patient was rate of resorption thereafter. A definitive impression of an edentulous for past 3 years and had been wearing dentures edentulous arch can be challenging when the residual ridges for 2 years. He got 2 sets of dentures made but was not
1present are less than ideal . satisfied with any of them. He complained that the previous
This case report described closed mouth impression dentures were loose and he wanted a solution for the same.
Indian Journal of Comprehensive Dental Care
I J C D C1. 2. Navdeep Attri3. Preeti Chawla Arora4. Aakash Duggal
Aman Arora
Date of Submission : 11/1/16 Date of Acceptance : 24/1/16
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

Indian Journal of Comprehensive Dental Care
On intraoral examination it was found that the patient had patient (fig 7). Satisfactory results were achieved with few
completely edentulous maxillary and mandibular ridges with corrections and the patient adapted easily to the dynamic
severely resorbed flat mandibular ridge (fig 1). Preliminary denture.
impressions of maxillary and mandibular arches were made Discussionwith modeling compound impression material (fig 2).
The success of every complete denture relies on the Primary casts were obtained and custom trays were fulfillment of the three basic properties of retention, stability, fabricated. Border molding was done with type I low fusing
2and support . The degree of muscular activity and the region impression compound (DPI Pinnacle Tracing Sticks) and final to which the denture can be extended without displacement impressions made with zinc oxide eugenol impression paste are important aspects of any impression technique. For (DPI impression paste) in conventional manner. Master casts individuals with an accentuated bone resorption, it is difficult obtained (fig 3) and temporary record bases were to obtain good retention and stability of the complete constructed and occlusal rims were fabricated. After denture due to the presence of muscular insertions near the establishing the vertical dimension of occlusion, lower ridge crest or border, which might cause muscular-induced impression was again made by using 2 applications of tissue displacement of the denture. In these cases, dynamic conditioning material (Orthoplast Soft Liner), each
1impression technique is highly recommended . application allowed to remain in mouth for 8-10 minutes (fig
4) and patient was instructed to close in the predetermined In this particular case, the main aim of the impression
vertical dimension of occlusion and also patient was procedure was to gain maximum area of coverage as osseous
instructed to perform various functional movements (fig 5). structures offered little possibility of retention and stability
After each application impression removed from mouth and and also the muscle attachments were located near the crest
checked for any denuded areas and the areas were relieved. of the residual ridge so dislocating effect was more. For these
A final wash impression was made with light bodied reasons, the range of muscle action, as well as spaces into
elastomeric impression material (Photosil light body which the denture can be extended without dislocation,
polyvinyl Siloxane) (fig 6). could be accurately recorded in the impression by means of
dynamic methods.In this technique, a two step mandibular impression making
was planned. The first impression of the mandibular arch Dynamic dentures differ characteristically from conventional
with zinc oxide eugenol impression paste further enhanced dentures. The borders of the denture base from a dynamic
the retention and stability. The bases thus formed are used impression are longer lingually and buccally in relation to the
for making second impression i.e dynamic impression which amount of extension obtained from a conventional 3is more accurate. Further denture construction was done in impression . Lingual anterior area is a very critical area for
4conventional manner and denture was delivered to the good border seal and retention . Various functional
805
Fig 1- intraoral photograph of mandibular ridge
Fig 2-initial impressions Fig 3- master casts Fig 4-impression with tissue conditioner
Fig 5- dynamic impression made at predetermined vertical dimension
Fig 6- final wash impression made with elastomeric
impression material
Fig 7- denture insertion

Indian Journal of Comprehensive Dental Care
movements limit the flow of impression material in a Conclusion
downward direction but do not eliminate impression Prosthodontic rehabilitation of a patient with compromised material that is located horizontally under the tongue. This residual ridge in a conventional manner is a difficult task. material is retained and molded by the muscles thus, Modification in treatment procedure should be considered excluding dislocating effect in the sublingual region on the to fulfill the patient's functional demands. This technique completed denture. With the dynamic impressions, the recorded the maximum denture bearing surface area thus individual muscular pattern of each patient is recorded to a improving the retention and stability of the denture along larger extent than with conventional methods. The with comfort and confidence in the patient.advantages of dynamic impressions are : (1) avoidance of the
Referencesdislocating effect of the muscles on improperly formed
1) Comparison of Different Final Impression Techniques denture borders, and (2) complete utilization of the
for Management of Resorbed Mandibular Ridge, Case possibilities of active and passive tissue fixation of the
Reports in Dentistry Volume 2014.denture. These advantages are the direct result of the
impression material being shaped by the functional 2) Management of mandibular compromised ridge: a movements of the muscles and muscle attachments that literature review and case report. World journal of border the denture base. Since functional activity of muscles dentistry 2013.1)and muscle attachments exclusively shapes the dynamic
3) Dynamic impression methods, JPD 1965.impression, the arbitrary elements of conventional methods
3 4) Complete denture prosthodontics. A manual for clinical are reduced .thprocedures, Bernard Levin 17 edition.
To provide a compatible base material for contact with 5) Essentials of complete denture prosthodontics second dental model stone used for pouring the impression, final
edition by Sheldon Winkler.wash impression made with light bodied elastomeric
impression material to provide a clean release of the cast 6) Tissue Conditioners: A Review IOSR journal of dental 5material . Because of the flow and viscoelastic properties of and medical sciences 2015.
6tissue conditioning material the borders are molded well
during functional movements, also the material is easily
available, simple to use, less time consuming and pressure
areas can be identified and can be corrected. The only
disadvantage can be the cost of the material.
806

IMPLANT PLACEMENT WITH PREDICTABLE GBR IN
LARGE BONY DEFECT- A CASE REPORT
ABSTRACT
The replacement of missing teeth with implant borne restorations has become
a treatment modality accepted by the scientific community for fully and
partially edentulous patients. Advancement in the oral implant treatment
leads to predictable survival rates and create important treatment options
available. Bone defect associated with lost teeth in anterior maxilla will affect
both surgical placement of implant and subsequent prosthetics rehabilitation.
Bone defect correction can be carried on using variety of ways include barrier
membrane with guided bone regeneration, block grafts etc. This case report
describes the management of an anterior missing tooth following implant
placement and filling the labial bone defect using particulated bone graft and
membrane. After 3 months of healing esthetic crown was placed.
Keywords: Dental implant, Guided Tissue Regeneration(GTR) ,Bone graft
807
Corresponding author:Name: Dr. Ashish Verma, M.D.S., Dept of PeriodontologySri Guru Ram Das Institute of Dental Sciences and ResearchAmritsar.
1. Reader, Department of Periodontology, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
2. Senior Lecturer, Department of Period-ontology, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
3. M.D.S. Student, Department of Period-ontology, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
4 BDS Graduate, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar
5. BDS Graduate, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
INTRODUCTION The characteristics of the alveolar ridge play an important
decisive factor in the success of implant placement. The introduction of osseointegration by Branemark and co-Currently, however, implants are also being placed in sites workers and replacement of lost teeth by implants have with ridge defects of various dimensions utilizing the various revolutionized oral rehabilitation while significantly
1 reconstruction techniques using bone graft, guided bone advancing restorative dentistry . There are many patients regeneration orthognathic surgery or bone distraction.who present with missing teeth. In the anterior region, tooth
loss is most commonly a result of a traumatic injury or it is a Minor trauma causes loss of alveolus and gingiva. Major
congenital anomaly. Single missing posterior teeth are trauma can cause extensive vertical and horizontal bone 13usually caused by advanced caries or a failed endodontic loss . Restoration of missing anterior maxillary teeth is
procedure and occasionally by a congenital defect. There are challenging due to compromised esthetics associated with
several options available for the replacement of a single missing teeth itself in addition gradual alveolar bone 2 14missing tooth . resorption which will further compromise esthetics .
Indian Journal of Comprehensive Dental Care
I J C D C1. 2. Sahib Tej Singh3. Harmandeep Singh4. Sukhpreet Singh5. Navdeep Singh
Ashish Verma
Date of Submission : 13/1/16 Date of Acceptance : 22/1/16
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

Indian Journal of Comprehensive Dental Care
CASE REPORT description of the risks and benefits of the proposed
treatment was told followed by a written consent taken from Here is the presentation of a case where the missing the patient. maxillary right central incisor was restored by placement of
implant and simultaneous apisectomy procedure and use of The investigation included an intraoral periapical radiograph,
bone grafting was done with the adjacent tooth to remove orthopentomograph, blood tests which included
the periapical defect which was spreading towards the haemoglobin, bleeding time and clotting time
implant site. Dental History
A 25 year old male patient reported to the department of Questioning the patient reported that tooth 11 was Peridontology And Oral Implantology, Sri Guru Ramdas extracted in another hospital 1 year ago. And since then no Institute Of Dental Sciences And Research complaining of further treatment was done due to economical issues. missing upper anterior tooth 11 since 1 year. The tooth 11
Clinical Examinationwas extracted 1 year ago after accident which fractured the
Clinical examination was conducted, and thorough deep crown leaving the roots. The patient insisted for immediate
examination of both extra and intra oral examination of restoration to improve the function and esthetics.
reported the following:Conducting a thorough medical history, we found that the
Extra-oral: patient had a good physical condition and denied any
systematic diseases or any allergic diseases that were No gross facial asymmetry or swelling was detected. No relevant to dental treatment and he had no mucosal lesions, clicking of TMJ or limitation and deviation of opening.no bleeding disorder, no tobacco smoking, alcohol and drug
Intra-oral:abuse.
Hard tissue examination: reveals that tooth 11 was missing. He was informed of all the viable options to replace the
Evaluation of edentulous space shows that the quantity and missing right central incisor and a detailed written
808
IMPLANT PLACEMENT WITH PREDICTABLE GBR IN LARGE BONY DEFECT- A CASE REPORT
Figure 1.Periapical IOPA showing missing 11 and periapical lesion irt 12
Figure 2. Pre operative Orthopentomograph
Figure 3A midcrestal combined with
crevicular incisions were given on the implant site
to elevate a mucoperiosteal flap.
Figure4As the mucoperiosteal flap was
raised a labial bone defect was seen irt 12 extending over the region in
relation to 11
Figure5Corticotomy was done to remove the defect followed by curettage
of the periapical lesion .Apicectomy of the tooth 12 was done
Figure 6The speed was adjusted to
approx. 1300 rpm at the initial drill with an intermittent pressure
of 1 second on the bone and 1 to 2 seconds off the bone, under
copious sterile saline irrigation. The implant was placed with its
head at crest bone level, and then put the healing screw on
the abutment connection area.
Figure7Because of the lack of enough bone,
bone regeneration technique was used after implant placement.
Bone graft (Bio-oss) was used to fill the bone defect followed
by suturing
Figure 8
Post-operative IOPA was
done as shown in
Figure 9
After an uneventful healing period
of 4 months, stage 2 surgery of
uncovering of implant was done.
Healing abutments were screwed in.
At 2 weeks, impression was recorded
for full PFM crown . PFM crown was
cemented thereafter the laboratory
procedures

Indian Journal of Comprehensive Dental Care
quality of edentulous area (alveolar bone) was not good. many researches has reported that, the success and survival
There were obvious bone defect and labial ridge in form of rate of dental implant placed in anterior maxilla are almost 3concavity of 11 and 12 as seen on periapical xray and same to other segment of jaw .
orthopentomograph. The inter-alveolar spaces were However, there is often inadequate bone to receive and
enough for restoration.support implants. This can be the result of trauma,
Soft tissue examinations: The thickness of the soft tissue of periodontal disease, endodontic infection, post-extraction the edentulous ridge was assessed at different points of the ridge defects, disuse atrophy, etc. Successful implant edentulous space and it was about 2 mm measured by a placement in planed site required enough bone volume of graduated periodontal probe. The color and texture of sufficient density to enable an implant of the appropriate size
3mucosa was normal. No obvious mucosal lesions, fibrous to be placed in a desirable position and orientation .connective tissue displacement and other abnormities were
Placement of bone grafts in conjunction with endosseous detected. Periodontal status: Oral hygiene was good. No
dental implant shortens the treatment time without marginal gingival inflammation was detected. No
influencing the success rate or increase the complication . periodontal pockets were detected. No other tooth mobility
The interaction between the graft and the surrounding host was found. 9bone is very important and is the subject of much research .Before starting an implant surgery and as a part of treatment
In this present case report simultaneous GBR was performed plan process, the patient must have an initial radiographic
in the maxillary right central and lateral region during implant screening which in this case was intraoral peri-apical X-ray
placement achieving good primary implant fixation and graft (figure1) accomplished by intraoral long cone paralleling
stability.The necessity for augmenting the volume of bone is technique and a pre operative orthopentomograph.(figure2)
obvious in that implant stability requires optimum contact of The patient understanding of the financial, time, and
the implant with bone over a sufficiently large surface area to maintenance requirements were crucial, and these 10,11ensure good osseointegration . obligations were made clear to the patient before starting
The soft tissue characteristics are equally important as the the treatment and during subsequent appointments.adequate keratinized mucosa is known to absorb the
Before the surgery, all the supragingival and subgingival mechanical stress and retard the inflammatory process. This
calculus was removed and blood screening test were can be achieved by using the resorbable/nonresorbable
performed.barrier membranes and bone substitutes to enhance bone
The patient was informed about the common complications regeneration.of the implant surgery that could happen, and written
consent was taken.
The surgical stent was positioned and the implant site was
prepared with correct angulations and depth for implant
fixture. A 2mm diameter twist drill was used to drill to the
desired depth.
A small, sharp-tipped guiding drill was used to create a Various studies suggest that GBR results in rapid, clinically 12precise, minimally invasive initial penetration through the relevant bone closure of dental implant dehiscence defect
mucosa and into bone to locate the exact position of planed .In this case, on the buccal aspect of implant, a dehiscence implant. type defect with corono-apical and mesio-distal extension of
5 mm was found. The defect was clinically almost completely The osteotomy was started with the initial pilot drill and
restored with GBR. GBR concept advocates that the sequentially deepened with 2.0 and 2.5 mm diameter drills .
regeneration of osseous defects is predictably attained via DISCUSSION
the application of occlusive membrane which mechanically Management of an anterior missing tooth can pose a excludes non-osteogenic cell populations from the challenge to practitioners. Several options are available with surrounding soft tissues, thereby allowing osteogenic cell their own advantages and disadvantages. populations originating from the parent bone to inhabit the
Endosseous dental implants are a predictable modality of osseous wound. In this case of GBR we have used Bio-Oss
tooth replacement that can improve the dental health and biograft. There are numerous materials currently available
quality of life for many people. Different study conducted by for treating intrabony periodontal defects including
Guided Bone Regeneration is a surgical procedure that
utilizes barrier membranes to direct the growth of new bone
and gingival tissue at sites having insufficient volumes or
dimensions of bone. The present scenario focuses on the
application of guided bone regeneration to defective alveolar 5,6ridges facilitating the placement of implants .
809

Indian Journal of Comprehensive Dental Care
4autografts, allografts, xenografts and alloplasts .
The biological principle of GBR is highly predictable for ridge
enlargement or defect regeneration under the prerequisite
of a complication-free healing. The harmony of soft and hard
tissue was achieved by implant placement with bone
augmentation in aesthetically challenging situation. The
findings of this case report reveal that this treatment 7,8modality ie. GBR, leads to substantial clinical improvement .
Summary
In the restoration of the maxillary anterior region, the
surgeon may be required to use a variety of surgical
techniques to obtain a beneficial functional and esthetic 9. Boronat A, Carrillo C, Penarrocha M, Pennarocha M result. Specific attention must be given to both the hard and
.Dental implants placed simultaneously with bone grafts soft tissues of the periodontium in selecting those surgical in horizontal defects: a clinical retrospective study with procedures capable of enhancing esthetics in a particular 37 patients. Int J Oral Maxillofac Implants 2010; 25:189 clinical situation. Minor soft tissue manipulation may create 196.restorative opportunities otherwise not considered possible.
BIBLIOGRAPHY
1. Branemark PI, Adell R, Breine U et al. Intra-osseous
anchorage of dental prostheses.Experimental studies.
Scand J Plast Reconstr Surg 1969; 3(2):81–100
2. Tuna H , Uzun G , Keyf F. The single-tooth implant
treatment for maxillary central incisors loss after
trauma: case reports.Clinical dentistry and research
2011; 35(1): 47-52Cho KS, Choi SH, Han KH, Chai JK, Wikesjo UM, and Kim
3. Walid Al-Jallad, et al. Restoration of Missing Upper CK. Alveolar bone formation at dental implant
Anterior Teeth using Dental Implant Simultaneous with dehiscence defects following guided bone regeneration
Bone Grafting- A Case Report. J Dent Oral Health; 1: 1-8and xenogenic freeze-dried demineralized bone matrix.
4. Verma UP. Guided bone regeneration(GBR) for the Clinical Oral Implants Research, 1988 Dec; 9(6):419-28.treatment of implant dehiscence defect. IJCD JUNE,
13. Palmer RM, Palmer PJ, Newton JT. Dealing with esthetic 2011 2(3)
demands in the anterior maxilla. Periodontol 2003;
33:105-118.
14. Cawood JI, Howell RA. Reconstructive prosthetics
surgery:I. Anatomical considerations. Int J Oral
Maxillofacial Surg 1991; 20:75-82.
6. D. Lundgren, L. Sennerby, H. Falk, B. Friberg. The use of a
new bioresorbable barrier for guided bone regeneration
in connection with implant installation. Clinical Oral
Implants Research, 1994; 5:177–184
7. Roberto cocchetto, Giampaolo vincenzi.Delayed and
immediate loading of implants in the esthetic zone,
Practical proceed esthetic dentistry 2007; 22:3.
8. Sompop Bencharit, Debra Schardt-Sacco, Michael
B.Border, ColinP.Barbaro. Full Mouth Rehabilitation
with Implant-Supported Prostheses for Severe
Periodontitis: A Case Report, Open dentistry
journal,2010; 4:165-171.
10. Jun-Beom Park. Restoration of the maxillary anterior
tooth using immediate implantation with simultaneous
ridge augmentation. IJDR, 2010; 21:454-456.
11. Péter Windisch, Dóra Szendroi-Kiss, Attila Horváth,
Zsuzsanna Suba, István Gera, Anton Sculean.
Reconstructive periodontal therapy with simultaneous
ridge augmentation, Clincal Oral Investigation 2008; 12
(3): 257–264.
12.
5. D. Buser, U. Brägger, N. P. Lang, S. Nyman. Regeneration
and enlargement of jaw bone using guided tissue
regeneration, Clinical Oral Implants Research 1990; 1:
22–32.
810

MUCOUS MEMBRANE PEMPHIGOID
– A CASE REPORT
Abstract
Benign mucous membrane pemphigoid (MMP) is an autoimmune disease
characterized by chronic vesiculo-bullous eruptions, predominantly on
mucous membranes but occasionally on skin. The diagnosis is hard to achieve
due similarity in clinical picture with other vesiculobullous lesions like
pemphigus, bullous pemphigoid, etc., thereby, posing a diagnostic dilemma for
the clinician. Histopathology can confirm the diagnosis; however,
corticosteroids can be started to relieve the symptoms while confirmatory
reports are not available as it is common treatment for most of mucosal lesions.
After histopathology report, if diagnosis of MMP is established, anti-leprotic
drug can be started along with corticosteroids for better relief. We report a case
of mucous membrane pemphigoid in a 43 year-old female with difficulty in
eating food and pain in left and right side of mouth (buccal mucosa). Skin
lesions were also present on legs and shoulder. Oral mucosal lesions were
managed with anti-leprotic drug (Dapsone), topical and systemic
corticosteroids. Such approaches not only result in immediate relief of
symptoms and improved clinical outcomes but also provide a better quality of
life for the affected patients.
Keywords: mucous membrane pemphigoid, histopathology, corticosteroids
811
Corresponding author:Name: Dr. Isha Singla,M.D.S., Senior Lecturer, Department of Oral Medicine and Radiology, Adesh Institute of Dental Science and Research, Bathinda, Punjab (India)(M) 9463184517e mail: [email protected]
1. M.D.S., Senior Lecturer, Department of oral medicine and radiology, Adesh Institute of Dental Science and Research, Bathinda, Punjab.
2. M.D.S., Professor, Department of oral medicine and radiology, M.M. College of Dental Sciences and Research, Mullana, Ambala, Haryana
3. M.D.S., Professor, Department of oral medicine and radiology, M.M. College of Dental Sciences and Research, Mullana, Ambala, Haryana
4. M.D.S., Senior Lecturer, Department of oral medicine and radiology, M.M. College of Dental Sciences and Research, Mullana, Ambala, Haryana
5. Post Graduate Student, Department of oral medicine and radiology, M.M. College of Dental Sciences and Research, Mullana, Ambala, Haryana (India)
6. BDS Student. SGRD Institute of Dental Sciences & Research, Amritsar, Punjab. India
Introduction mucous membrane pemphigoid, linear IgA disease, chronic
bullous dermatosis of childhood, and epidermolysis bullosa Bullous diseases are divided into two form- either 2acquista. Benign mucous membrane pemphigoid is an pemphigus with intraepithelial separation of cells or
autoimmune disease characterized by chronic vesiculo-pemphigoid with subepithelial separation of cells. The bullous eruptions, predominantly on mucous membranes pemphigoid family of diseases is a part of the group of
3 but occasionally on skin. It is also known as Cicatricial autoimmune subepidermal/subepithelial bullous 1 pemphigoid. It has a chronic course and a tendency toward disorders.
scar formation. It occurs worldwide in the people of all The pemphigoid group encompasses bullous pemphigoid,
Indian Journal of Comprehensive Dental Care
I J C D C1. 2. Shambulingappa Pallagatti 3. Soheyl Sheikh4. Deepak Gupta5. Simranpreet Saini6. Shiny Singh
Isha Singla
Date of Submission : 12/1/16 Date of Acceptance : 21/2/16
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

Indian Journal of Comprehensive Dental Care
1races. in eating food and pain in left and right side of mouth (buccal
mucosa) since 2 months. It was associated with bleeding and Mucous membrane pemphigoid primarily affects middle-surrounding area was slightly inflamed. Her past aged adults and females are more commonly affected as
4 dental/medical history was unremarkable. Extraorally, lymph compared to males. It can affect any mucosal surface but the 5 nodes were not palpable.
oral mucosa is the most common site and the nose, 6 The intraoral examination revealed irregular ulcers oesophagus, larynx and genitals less frequently affected.
measuring 2 cm X 2 cm present on the left and right buccal Patients often present with the complaint of bleeding, pain, mucosa, covered with pseudomembrane and had an dysphagia and peeling of the mucosa but the most serious
5 erythmatous floor. On left side, it extended 2.5 cm from the complications of the disease result from scarring. Erosions angle of mouth to the posterior molar region and supero-and scarring of the mucosa might result in significant
6 inferiorly, it extended 1cm above and 0.5 cm below the line of morbidity and treatment is usually challenging. However, occlusion (Figure 1a). On right side, it was 2 cm from the oral lesions despite of being extremely painful, generally are angle of mouth to the posterior molar region and supero-self-limiting and do not result in scar formation or organ
4 inferiorly it extended 1.5 cm above and 1 cm below the dysfunction.occlusal line (Figure 1b). On physical examination, skin
Diagnosis is based on history, clinical presentation, lesions were also present on legs and shoulder (Figure 2). The
histopathological and immuno-fluoresence examinations. lesions on the skin were present as 0.5-1 cm in diameter
The management of a patient with mucous membrane ulcers covered with the scab. The surrounding area was
pemphigoid is complicated by the chronic nature of the normal. There were no signs observed or symptoms reported 5disease.by the patient on the ocular or genital mucosa.
Topical corticosteroids are the first line of treatment for oral The inspectory findings were confirmed. On palpation, oral
MMP, particularly for localized lesions. Extensive oral lesions lesions were tender and non-scrapable. Thin layer of
or spread of the disease to other mucous membranes require epithelium peeled away in an irregular pattern leaving the 7 prolonged administration of systemic corticosteroids.denuded base. The history and clinical findings of the patient
Alternatively, steroid-sparing drugs such as dapsone, helped form a provisional diagnosis of pemphigus. A
azathioprine, cyclophosphamide or intravenous differential diagnosis of mucous membrane pemphigoid and 7 immunoglobulins can be given.bullous pemphigoid was also considered due to similarity in
8 It has been reported in Indian literature frquently. However, clinical picture. An incisional biopsy was performed under we report a case of oral mucous membrane pemphigoid that local anaesthesia to establish a definitive diagnosis. was managed successfully with topical steroid
Empirical treatment was started with topical steroids hence (Triamcinolone acetonide 0.1%), systemic steroid and anti-
the patient was prescribed topical corticosteroids Kenacort leprotic drug (Dapsone). This case was reported because of
(0.1%Triamcinolone acetonomide) 3 times a day.difficulty in treatment approach of such patients. A different
Histopathologically, the features were consistent with those type of treatment plan was used which has been elaborated of pemphigoid (Figure 3). So other drugs were added to further. already existing regime of topical corticosteroids. Anti-
Case Reportleprotic drug (Dapsone) 150 mg/ day and systemic
A 43- year old female reported to the Department of Oral corticosteroid (6mg/day) were given to the patient. This was Medicine and Radiology with the chief complaint of difficulty followed by scaling and oral hygiene instructions. The patient
812
Figure 1a & 1b. Irregular ulcers on right & left side of buccal mucosa, covered with pseudomembrane and having an erythmatous floor
Figure 2: Extra-oral lesion on leg presenting as 0.5-1 cm in diameter ulcers
covered with the scab and surrounding normal area
Figure 3: Histopathological picture showing epithelial connective tissue interface
with subbasilar split.

Indian Journal of Comprehensive Dental Care
was reviewed every 2 weeks for three months. The skin and disease. This helped to manage the condition of the patient
oral lesions had subsided within 16 weeks of starting the in the present case as well. After confirmation of the
treatment. The patient was put on a maintenance dose of the diagnosis, other drugs can be added to the existing regime.
topical corticosteroids and reinforcement of oral hygiene This approach was followed in the above mentioned case
instructions were given. also. Such approaches will not only result in improved clinical
outcomes but also provide a better quality of life for the Discussionaffected patients. Clinical awareness amongst health
Cicatricial pemphigoid (CP) was first described by Cooper in professionals and early recognition of the lesion should be 9 91857. In 1911, Thost separated CP from pemphigus. The emphasized.
term mucous membrane pemphigoid was first introduced by 9 ReferencesLever in 1953. Cicatricial pemphigoid may remain localised
1. Mobini N, Nagarwalla N, Ahmed AR. Oral pemphigoid. to the oral cavity or it may be generalised. The most
Subset of cicatricial pemphigoid? Oral Surg Oral Med commonly involved sites are oral mucosa and ocular 10 Oral Pathol Oral Radiol Endod 1998; 85 :37-43. Eschle-involvement but in the case reported above, oral mucosa
Meniconi MEand skin were the involved sites.
2. Ahmad SR, Foster CS.Mucous membrane pemphigoid: History, clinical examination, histopathology and immuno-
an update. Curr Opin Ophthalmol 2005; 16:303-307. fluorescence are helpful in diagnosis. The present case was
Cheng YSdiagnosed on the basis of classical clinical features and 8histopathology. 3. Rees TD, Wright JM, Plemons JM. Childhood oral
pemphigoid: a case report and review of the literature. J Mucous membrane pemphigoid can be difficult to treat and 6 Oral Pathol Med 2001; 30:372-377.the results are often disappointing. It is difficult to treat and
results can be disappointing because the lesion can recur 4. Dayan S, Simmons RK, Ahmed AR. Contemporary issues anytime despite of proper following of regime by the patient. in the diagnosis of oral pemphigoid: a selective review of Early recognition and treatment can improve prognosis and the literature. Oral Surg Oral Med Oral Pathol Oral Radiol
8 avoid surgical intervention. Therapeutic regimens in mucous Endod 1999; 88:424-430. membrane pemphigoid are based primarily on clinical
5. Ciarrocca KN, Greenberg MS. A retrospective study of experience. Local therapy may be sufficient to control the
the management of oral mucous membrane disease, but systemic medications are indicated for severe
pemphigoid with dapsone. Oral Surg Oral Med Oral ocular, laryngeal or esophageal involvement as well as for
Pathol Oral Radiol Endod 1999; 88:159-163. Lee HY6 oral or cutaneous disease unresponsive to topical therapy.6. Blazek C, Beltraminelli H, Borradori L. Oral Mucous
Histopathologically, the mucous membrane pemphigoid Membrane Pemphigoid: Complete Response to Topical
shows a sub-epidermal vesicles with a dense inflammatory Tacrolimus. Acta Derm Venereol. 2011 May 20.
infiltrate in the dermis or submucosa with lymphocytes, 10 7. Assmann T, Becker J, Ruzicka T, Megahed M. Topical histocytes and plasma cell infiltrate. In the present case,
tacrolimus for oral cicatricial pemphigoid.Clinical and histopathological picture revealed parakeratinized stratified Experimental Dermatology 2004; 29: 673–687.squamous epithelium with underlying connective tissue. The
epithelial connective tissue interface was predominantly flat 8. Ramanan C, Ghorpade A, Das MN, Bose U, Banerjee AK. with subbasilar split in most areas. Connective tissue showed Cicatricial pemphigoid - A case report. Indian J Dermatol intense inflammatory infiltrate of predominantly plasma Venereol Leprol 2001; 67:212-213. Ojha Jcells. Numerous eosinophils and mast cells were also seen.
9. Bhattacharyya I, Stewart C, Katz J. Cicatricial pemphigoid These features are suggestive of benign mucous membrane
with severe gingival and laryngeal involvement in an 18-pemphigoid.
year-old female. Oral Surg Oral Med Oral Pathol Oral Conclusion Radiol Endod 2007; 104:363-367.
In the evaluation and treatment of mucous membrane 10. Sayegh H, Kawar J, Shokeh H. Cicatricial Pemphigoid: A pemphigoid, the extent of disease, co-morbidities and the case report. JRMS 2004; 11: 54-56age of the patient are important considerations. Appropriate
diagnosis and starting empirical treatment (with
corticosteroids), before a definitive diagnosis is established,
are important for managing this potentially debilitating
813
GIANT SUBMANDIBULAR GLAND SIALOLITH : A CASE REPORT
Abstract
Sialolithiasis is a common disease of salivary glands characterized by the
obstruction of salivary secretions by a calculus. Salivary stones may form in any
of the major or minor salivary glands or their excretory ducts. This is associated
with pain and inflammation, and in some occasions with an infection of the
affected gland. Size of the sialolith may range from 0.1mm to 30mm or even
bigger. Those salivary stones which exceed 15mm in any one dimension or 1gm
weight are classified as Giant sialoliths. Giant sialoliths are rarely reported, we
report here a case of giant sialolith of the submandibular gland duct.
Keywords: sialolith, saliva, surgery
814
Corresponding author:Name: AmneetSandhuAddress:Sri Guru Ram Das Institute of Dental Sciences and Research, AmritsarPhone No. 9872480636
1. M.D.S, Reader, Department of Oral and Maxillofacial Surgery, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
2. M.D.S, Consultant Oral and Maxillofacial Surgeon
3. Dr. Parminder Singh, M.D.S, Consultant Maxillofacial Surgeon, SGL hospital, Jalandhar
4. M.D.S, Reader, Department of Oral and Maxillofacial Surgery, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar
Introduction frequency of sialoliths is relatively high, the occurrence of
giant sialoliths larger than 1.5cm in any diameter is rare. Sialolithiasis is defined as the formation of calcific
concretions within the parenchyma or the ductal system of a This report describes a case of giant sialolith in a 35 year old
major or minor salivary gland. It constitutes one of the most male, addressing the clinical features, the diagnosis and the
common causes of dysfunction of the salivary glands. It surgery performed to restore the salivary flow.
occurs mainly in the submandibular gland (80-90%) and to a Case Reportlesser degree in the parotid gland (5-20%). The sublingual
1 A 35 year old male was referred to our center for evaluation and the minor salivary glands are rarely affected . It is
and management of pain and swelling in the right believed that salivary stones develop as a result of the
submandibular region. Pain was dull, intermittent and deposition of mineral salts around a nidus of mucus,
associated with meals. There was history of enlargement of 2bacteria or desquamated cells . The size of the calculi varies the pre-existing swelling during meals.
from less than 1mm to a few centimeters. Although the
Indian Journal of Comprehensive Dental Care
I J C D C1. Amneet Sandhu2. Supreet Gill3. Parminder Singh4. Yashmeet Kaur
Date of Submission : 28/12/15 Date of Acceptance : 2/1/16
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

Indian Journal of Comprehensive Dental Care
3On extraoral examination, there was a moderate sized 1gm weight . In this report clinical and radiological features
swelling in the right submandibular region. The swelling was of a giant sialolith, with dimensions of 39mmx11mm was
soft and tender on palpation with normal overlying skin. present. It was located in the wharton's duct opposing the
Intraorally there was considerable fullness along the course mandibular right premolar and first molar region. Large
of Wharton's duct on the right side. On bimanual palpation of sialoliths may lead to infection, suppuration and ulceration 5the floor of the mouth, a hard mass was felt in the premolar- on the floor of the mouth . The largest sialolith reported in
molar region. Milking of the gland produced very less saliva the literature was 70mm in the length of Wharton's duct and 6but a flow of pus. was described as having “Hen's Egg” size .
Computed Tomography scan (Axial section - Fig 1and Sagittal Traditional and recent etiopathogenicfactors include a
section - Fig 2) reveals a large radiopaque calculus lingual to reduced salivary flow rate, a change in pH, dehydration, duct
the body of mandible in the duct of right submandibular anomalies and the retrograde migration of food, bacteria or 7gland. foreign body from the oral cavity favoring stone formation .
Calculi may form in any of the salivary glands but On the basis of clinical and radiographic findings, a diagnosis submandibular gland is the most common by far (80-90%). of left submandibular gland duct sialolith was made. Factors responsible are: high mucin content of the saliva,
Since the size of the sialolith was large, transoral-tortuous course of wharton's duct, flow of saliva against
sialolithotomy was done under local anesthesia and proper gravity, high calcium content of saliva and more alkaline
antibiotic cover. The floor of the mouth was stabilized by firm 8saliva . All these features are unique to submandibular upward and medial pressure in the submandibular area and
gland. incision was made through the mucosa over the sialolith.
The clinical feature frequently encountered is the After careful mucosal dissection the submandibular duct was enlargement of the gland during eating. If the obstruction is identified and incised over the sialolith. The sialolith was not complete, this swelling gradually diminishes between exposed, mobilized and removed. The wound was closed at meals as the saliva is permitted to escape slowly from the the mucosal layer. The sialolith removed (Fig 3) measured duct around the obstructing stone. Complete obstruction is 39mm in length. The follow-up of six months showed no manifested clinically by swelling, redness and pain in the area complications and complete restoration of salivary flow. of the orifice of the excretory duct. This is followed by the
On the basis of clinical, radiological and histopathological acute symptoms of the gland. The pain is dull at first but
findings the diagnosis of giant submandibular salivary duct gradually becomes severe as pus starts to form and the gland
sialolith was confirmed. continues to perform its functional activity, causing an
Discussion increase in pressure. At this time the patient may become 2febrile and the gland is markedly enlarged and tender . In this The formation of calcific concretions in the salivary duct or
report the patient gave history of pre-prandial and glands is a common disorder, especially in the submandibular postprandial submandibular swelling since six months. Long glands. Most of the salivary calculi are small in size, in standing obstruction by a sialolith can cause severe damage contrast to those that reach several centimeters, which are to the acini of the gland, resulting in permanent decrease or reported as megaliths or giant calculi. Giant sialoliths are
1even absence of salivary flow .classified as those exceeding 15mm in any one dimension or
815
Fig 1. Axial CT scan showing a large calculus in the duct of right
submandibular gland.
Fig 2. Sagittal CT scan showing calculus in the right submandibular gland duct.
Fig 3.Surgically obtained sialolith

Indian Journal of Comprehensive Dental Care
Salivary calculi consist of laminated structure of concentric gland affected and stone location. The treatment objective is
shells of calcareous minerals with alternate layers of organic to restore the salivary flow. The sialolith should be removed
resinous material that also forms the outer covering. The with minimally invasive method, via transoralsialolithotomy
crystalline component appears to be composed of calcium to avoid morbidity associated with sialadenectomy.
phosphate in the form of hydroxyapatite and small amounts Intraglandularsialoliths necessitate sialadenectomy.
of magnesium, carbonate and ammonium ions. The organic Referencesmatrix is composed of various carbohydrates and amino
5 1. Lustmann J, Regev E, and Melamed Y. Sialolithiasis : A acids .
survey on 245 patients and a review of literature. Int. J. Ultrasonography (USG) is a method of choice in salivary flow Oral Maxillofac. Surg. 1990;19:135-138diagnostics. Its sensitivity in calculi detection amounts to
2. Carr SJ. Sialolith of unusual size and configuration: 94%, specificity – 100% and accuracy-96%. USG allows
Report of a case. Oral Surg Oral Med Oral Pathol. detection of non opaque calculi with sensitivity of 80-
1965;20: 709-712996% .Sialendoscopy allows the direct visualization of salivary 3. Bodner L and Beer-Sheva. Giant salivary gland calculi: duct lumen i.e. visualization of calculi, mucosal plugs, foreign
Diagnostic imaging and surgical management. Oral Surg body and polyps. It is mainly used in the treatment of Oral Med Oral Pathol Oral RadiolEndod. 2002; 94:320-inflammatory condition of the salivary glands and
10 323obstruction of the salivary ducts .
The treatment objective for giant sialoliths, as for the
standard sized sialoliths is restoration of normal salivary
secretion. Treatment options are transoralsialolithotomy,
interventional sialendoscopy, Extracorporeal short wave 4lithotripsy (ESWL) and resection of the gland . The giant 5. Deeb ME, Holte N and Gorlin RJ. Submandibular salivary
sialolith should be removed in a minimally invasive manner, gland sialoliths perforated through oral floor. Oral Surg. via a transoralsialolithotomy to avoid the morbidity 1981; 51: 134-139associated with sialadenectomy. Whenever the stone can be
6. Ledesma-Montes C, Garces-Ortiz M, Salcido-Garcia JF, palpated it is best to remove it through intraoral approach.
Hernandez-Flores F and Hernandez-Guerrero JC. Giant The cardinal rule when performing stone removal from
sialolith: Case report and review of the literature. J Oral wharton's duct is to first isolate the duct and then provide a
Maxillofac Surg. 2007; 65: 128-130longitudinal incision into the duct over the stone to retrieve
7. Capaccio P, Marciante GA, Gagguri M and Spadari F. it. Giant sialoliths are accompanied by long standing salivary Submandibular swelling: tooth or salivary stone. Indian gland sialadenitis resulting in a grossly fibrotic and poorly journal of dental research. 2013;24:381-383functioning gland. However, after elimination of the
obstruction, the apparent resiliency of submandibular gland 8. Arora V, Samadhani S and Bapan A.S. Stony Wharton's 11results in no adverse symptoms . ESWL is an effective non duct. Indian Journal of Otolaryngology and Head and
invasive alternate approach where the size of the calculi is neck Surgery. 2001; 53:242-243reduced to small fragments, the diameter of which does not
9. Yousem DM, Kraut MA and Chalian AA. Major Salivary 12block the flow of saliva and can be washed away . Gland
gland imaging. Radiology. 2002;216:19-29resection is only indicated when there is substantial mass
10. Rzymska-Grala I, Stopa Z, Grala B et al. Salivary Gland within the gland itself that is not surgically accessible calculi- Comtemprary methods of imaging. Pol J Radiol. intraorally and when there are small stones present in the 2010;75(3): 25-37vertical portion of wharton's duct from comma area to
11hilum . 11. Iqbal A, Gupta AK, Natu SS and Gupta AK. Unusually large
Sialolith of Wharton's duct. Ann Maxillofac Surg. 2012; Chronic infection, strictures and fistulas are the main 2: 70-73complications resulting from the presence of salivary
5calculus . 12. Andretta M, Tregnaghi A, Prosenikliev V and Staffieri A.
Current opinions in sialolithiasis diagnosis and Conclusiontreatment. ActaOtorhinolaryngol Ital. 2005;25:145-149
The submandibular gland is the largest contributor to
baseline salivary flow. There are various methods available
for the management of salivary stones depending on the
4. Bhullar, R. S., Dhawan, A., Bhullar, K., andMalhotra, S.
(2015). Giant submandibular gland duct sialolith
mimicking an impacted canine tooth.National Journal of
Maxillofacial Surgery, 6(1), 89.
816

UNICYSTIC AMELOBLASTOMA: RAISING OBSCURITY
IN PERIRADICULAR DIAGNOSIS - A Case Report
ABSTRACT:
Ameloblastoma is a benign tumor; whose importance lies in its potential to
grow to enormous size with resulting bone deformity. Unicystic
ameloblastoma (UA) is a less encountered variant of amelobastoma. The
neoplastic nature of the lesion becomes evident only when the enucleated
material is available for histologic examination. Although its predilection is for
the posterior mandibular region, but its presence in the periradicular area
mimicing a cyst and a granuloma cannot be overlooked upon. Despite the
clinical diagnosis of periapical disease of endodontic origin, a non endodontic
lesion may be present. Hence, lesions such as UA located on periapical area of a
tooth can lead to a pulp-periapical misdiagnosis, and should be considered in
differential diagnosis. This paper illustrates a case of unicystic ameloblastoma
present in the anterior maxillary region that clinically and radiographically
resembled an inflammatory pathosis, emphasizing the importance of correct
diagnosis and treatment.
KEYWORDS: Unicystic ameloblastoma, differential diagnosis, periapical lesion.
817
Corresponding author:Name: Dr. Adesh S Manchanda MDS, Reader, Department of Oral Pathology & Microbiology, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.e-mail: [email protected](M) : 07837060067
1. MDS, Professor, and Head Department of Oral Pathology & Microbiology, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
2. MDS, Reader, Department of Oral Pathology & Microbiology, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
3. BDS, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
INTRODUCTION its potential to grow to enormous size with resulting bone 2deformity. Unicystic ameloblastoma (UA) is a less Odontogenic tumours (OTs) are derived from epithelial or
encountered variant of amelobastoma and appears more mesenchymal elements, or both, that are part of the tooth frequently in the second or third decade with no sexual or forming apparatus. They are therefore exclusively found in racial predilection. Much confusion still exists when it comes the mandible and maxilla and must be considered in to the terminology used for UA. Some of the terms used for differential diagnosis of lesions involving these sites. Like this lesion prior to 1977, when Robinson and Martinez' neoplasms elsewhere in the body, OTs tend to mimic introduced the concept of UA, were cystic (intracystic) microscopically, the cell or tissue of origin. An understanding ameloblastoma, ameloblastoma associated with about the biologic behaviour of the various OTs is of dentigerous cyst, cystogenic ameloblastoma, extensive fundamental importance to the overall management of
1 dentigerous cyst with intracystic ameloblastic papilloma, patients.mura l amelob lastoma, dent igerous cyst wi th
Ameloblastoma is a benign tumor; whose importance lies in ameloblastomatous proliferation, and ameloblastoma
Indian Journal of Comprehensive Dental Care
I J C D C1. Ramandeep S Narang2. Adesh S Manchanda3. Jaspreet Kaur
Date of Submission : 11/1/16 Date of Acceptance : 21/2/16
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

Indian Journal of Comprehensive Dental Care
developing in a radicular (or "globulomaxillary") cyst. The cm, extending up to #11 tooth region medially and distally till
term unicystic is derived from the macro and microscopic #24. Hard tissue examination revealed caries present in
appearance, the lesion being essentially a well-defined, relation to #21 and #22. On radiographic examination, a
often large monocystic cavity with a lining, focally but rarely unilocular radioluceny of 2.5 x 2 cm in size was seen
entirely composed of odontogenic (ameloblastomatous) periapically in relation to #21 extending till #24 along with 3epithelium. the widening of periodontal ligament space of #21, #22 and
#23 (Figure 1). Aspiration cytology revealed few squamous The diagnosis of unicystic ameloblastoma is based on two cells in a background of inflammatory cells.features. First, the lesion must be unilocular (less commonly
multilocular), clinically and radiologically. Second, on Based on the clinical and radiographic examination a
microscopic examination it must appear as a single cystic provisional diagnosis of radicular cyst was given. In this case
lesion with the epithelial lining consisting of ameloblastoma. the focus was on radicular cyst which is a highly prevalent
If the lesion is small, it is commonly seen as an incidental periapical lesion associated with carious tooth, pulp necrosis,
finding on radiographs taken for other purposes, in these and infection. Other non inflammatory periapical lesions
circumstances, some lesions could remain undiagnosed in such as periapical cemento- osseous dysplasia, bone cyst, 4 odontogenic keratocyst, fibro-osseous neoplasm, the early stages of their development.
adenomatoid odontogenic tumor and ameloblastoma were UA is almost exclusively encountered asymptomatically in also considered in the differential diagnosis at a later stage. the posterior mandible, and its presence in the periradicular Surgical enucleation of the lesion under local anesthesia with area mimicing a cyst and a granuloma cannot be overlooked adrenaline was performed. A full thickness flap was raised, a upon. Despite the clinical diagnosis of periapical disease of window was made in the alveolar bone, the access was endodontic origin, a non endodontic lesion may be present. enlarged, and the entire lesion was enucleated. The excised Hence, lesions such as UA located on periapical area of a specimen was then submitted for histopathological tooth can lead to a pulp-periapical misdiagnosis, and should examination.be considered in differential diagnosis. The neoplastic nature
Histologically, the given section showed a cyst wall lined by of the lesion becomes evident only when the enucleated
ameloblastic epithelium which was disrupted in places. The material is available for histologic examination.
lining showed columnar basal cells with hyperchromatic This paper illustrates a case of unicystic ameloblastoma nuclei; nuclear palisading with polarization and cytoplasmic present in the anterior maxillary region that clinically and vacuolation with intercellular spacing; and a thin layer of radiographically resembled an inflammatory pathosis, stellate reticulum like cells. The stroma showed mild chronic emphasizing the importance of correct diagnosis and inflammatory cell infiltrate and areas of haemorrhage. Final treatment.diagnosis was made as unicystic ameloblastoma of the
CASE REPORT luminal variant (Figure 2(a) & (b)). Patient had an uneventful
A 28 year old female patient presented with a swelling in the postoperative recovery with no signs of recurrence during
upper left anterior region of maxilla. On extraoral the 1 year follow up examination.
examination, a single, non tender swelling about 2 x 2 cm in DISCUSSIONsize was observed on the left side of face. Intraoral
Unicystic ameloblastoma, a variant of ameloblastoma; examination revealed a soft, fluctuant swelling of size 2 x 2
818
Figure 1: Intraoral periapical radiograph showing a unilocular radiolucent
lesion involving the #21 tooth region to #24 tooth region.
Figure 2: (a) Ameloblastic epithelial lining with palisaded basal cell layer and stellate reticulum like cells (H & E; X10). (b) Ameloblastic epithelial lining showing showing nuclear
palisading, hyperchromatic nuclei with polarization and cytoplasmic vacuolation with intercellular spacing and stellate reticulum like cells H & E; X40).

Indian Journal of Comprehensive Dental Care
requires separate consideration based on clinical, periapical cyst but the microscopic examination showed an
radiological and pathologic features and in its response to entirely different picture, suggesting to the practitioner to
treatment. Whether UA originates de novo as a neoplasm or keep in mind the differential diagnosis of apical lesions, and
whether it is a result of neoplastic transformation of non the presence of a noncystic lesion.
neoplastic cyst epithelium has long been debated. Both On comparing UA with a solid multicystic ameloblastoma, mechanisms probably occur, but proof, which is involved in some authors believe that this lesion is less aggressive than
2individual patient, is virtually impossible to obtain. Clinically its solid or multicystic form and even curettage has been and radiologically UA shows characteristics of an performed as the indicated therapeutic approach. The age of odontogenic cyst like dentigerous, radicular, glandular the patient is another influencing factor related to the choice
13odontogenic cyst, but in histologic examination shows a of treatment. As UA tends to affect young adolescent typical ameloblastomatous epithelium lining part of the cyst patients, the concern to minimize surgical trauma and permit cavity, with or without luminal and/or mural tumor jaw function and tooth development to proceed reasonably
5proliferation. unimpaired should be one of the important aspects in tumor
Although, most studies on periradicular lesions focus on management. While conservative surgery seems to have
radicular cysts and granulomas which are highly prevalent been justified in preference to mutilating radical surgery for
periapical lesions, nevertheless, the occurrence of non the young patients, choice of treatment has to be considered
inflammatory pathoses in this area should always be kept in in conjunction with other clinical and pathological factors
mind from a differential diagnosis point of view. Radiolucent such as the size, location and growth pattern of the tumor.
lesions in the mandibular and maxillary areas surrounding Whatever surgical approach the surgeon decides to take,
the root apices might lead to a misdiagnosis of apical long term follow up is mandatory, as recurrence of unicystic 5periodontitis, and several other pathologies such as ameloblastoma may be long delayed.
periapical osseous dysplasia, simple bone cysts, giant cell The importance of UA is that it possesses a much better granulomas, keratocystic odontogenic tumors, UA's, and prognosis after enucleation or curettage than does the
6metastatic lesions. As these lesions present a different classic intraosseous ameloblastoma. Its recurrence rate after prognosis they should always be considered while arriving at these procedures is around 15%, whereas recurrence is a diagnosis. They are, however, rare. The unicystic much higher after curettage of classic intraosseous ameloblastoma presents a special concern in this respect, ameloblastomas. The reason for this better prognosis is that being locally aggressive and nonresponsive to root canal in many examples the ameloblastoma involves only the treatment or tooth extraction. epithelial lining of the cyst or projects into its lumen, and the
Generally, apical inflammatory lesions appear as radiolucent histopathological findings of the present case is in
images in intimate contact with the apical root. On concordance with it. These lesions, which are sometimes
radiographic examination, radicular cysts frequently show an referred to as luminal and intraluminal ameloblastomas,
oval outline with well-defined limits and uniform, respectively, are confined by the fibrous connective tissue
symmetrical concentric growth. Additionally, alveolar wall of the cyst and are consequently removed completely if 2cortical bone appears gradually dislocated from the insertion the cyst is enucleated.
point of the lesion on the dental apex. Although root CONCLUSIONresorption is frequently associated with chronic periapical
Unicystic ameloblastoma can be found at or near tooth lesions, it is not commonly seen in small lesions and is rarely 7,8 apices, simulating a radicular cyst or adenomatoid
advanced. Moreover, clinical manifestations of cystic odontogenic tumor or some other non inflammatory
lesions include slow asymptomatic growth, needle aspiration pathosis. So diagnosis should be based on correlation of 8,9usually liberates serous fluid.clinical, radiographic and histopathological features to clear
Some of these clinical and radiographic features are common any doubts regarding the ambiguous nature of such lesions 10to UA. Most UAs have been associated with an expansile which are found in the peri-radicular region.
unilocular radiolucency with root resorption but not with REFERENCES11,12cortical erosion and perforation. Moreover, pulp 1. Manchanda A, Narang R, Singh B. Odontogenic tumors: sensitivity testing is important for the differential diagnosis
pathogenesis and historical update-A review. Ind J Comp between apical lesions of endodontic and nonendodontic Dent Care 2014; 4: 76-82.origin. In the present case, carious #21 and #22 along with
the radiographic findings gave weightage to a diagnosis of 2. Paikkatt V, Sreedharan S. Unicystic ameloblastoma of the
819

Indian Journal of Comprehensive Dental Care
maxilla: a case report. J Indi Soci Pedo Prev Dent 2007; 8. Neville BW, Damm DA, Allen CM,Bouquot JE. Oral and nd25: 106-110. maxillofacial pathology 2002; Chapter 15, 2 edn.
Philadelphia, USA; WB Saunders compay, pp: 616-8.3. Philipsen HP, Reichert PA. Classification of odontogenic ndtumours. A historical review. J Oral Pathol Med 2006; 77- 9. Shear M. Cysts of the oral regions. Chapter 11, 2 edn.
85. Oxford, UK: Wright, pp: 281-97.
4. Cunha E, Fernandes A. Unicystic ameloblastoma: a 10. Eversole LR, Leider AS, Hansen LS. Ameloblastoma with
possible pitfall in periapical diagnosis. Int Endo J 2005; pronounced desmoplasia. J Oral Maxillofac Surg 1984;
38: 334-340. 42: 735-40.
5. Satyabhushan N. Un icyst i c amelob lastoma 11. L i TJ, Wu YT. Unicyst ic Ameloblastoma: a
masquerading as huge periapical lesion, both clinically clinicopathologic study of 33 Chinese patients. am j surg
and histopathologically: two case reports with review of pathol 2000; 24: 1385–92.
literature. J Clin Imag Sci 2013; 3: 9. 12. Li TJ, Kitano M, Arimura K, Sugihara K. Recurrence of
6. Gondak R. Unicystic ameloblastoma mimicking apical unicystic ameloblastom a: A case report and review of
periodontitis: a case series. J Endo 2013; 39: 145-147. the literature. Arch Pathol Lab Med 1998; 122: 371-74.
7. Wood NK, Goaz PW. Differential diagnosis of oral and 13. Robinson L, Martinez MG. unicystic ameloblastoma: A
maxillofacial lesions. Chapter 15, 3rd edn. St Louis, MO, prognostically distinct entity. Cancer 1977; 40: 2278-85.
USA: Mosby, pp: 320-56.
820

THREE DIMENSIONAL ARCH CONTROL WITH A UBIQUITOUS DEVICE- HYGIENIC RAPID EXPANDER
ABSTRACT
Hyrax appliance was primarily invented with the goal of expanding narrow
maxilla and correcting posterior crossbites, thereby correcting malocclusions
in transverse plane. With the passage of time, innovations and ideas have led
the orthodontists capable enough to use this appliance for correction of
malocclusion in not just transverse but vertical and anteroposterior planes as
well.
Usage of specific appliances for a particular malocclusion not only increases
inventory and cost factor but also creates dilemma in the mind of the
orthodontist. How comforting would it be to have one appliance which
answers to various questions that glares in an orthodontist's face. Hyrax is our
closest bet for such an appliance. For it can be used in conventional
orthodontics for expansion and molar distalisation, growth modulation
therapy in patients with face mask and surgical orthodontics as an alveolar
transport device and a distractor as well. This paper would throw light upon,
how a standard hyrax appliance could be used to correct malocclusions in all
three planes of space.
Keywords: orthodontics, expansion, hyrax
821
Corresponding author:Name: Dr. Shilpa Gupta SainiAddress: Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar(M) +919876873003e-mail: [email protected]
1. MDS, Reader, Deptt. of orthodontics, Sri Guru Ram Das Institute of Dental Sciences And Research, Amritsar
2. PG Student, Sri Guru Ram Das Institute of Dental Sciences And Research, Amritsar
3. PG Student, Sri Guru Ram Das Institute of Dental Sciences And Research, Amritsar
4. Lecturer, Sri Guru Ram Das Institute of Dental Sciences And Research, Amritsar
INTRODUCTION anchored in the patient's mouth and the screw is turned by
the patient. The activation protocol varies according to the HYRAX also known as hygienic rapid expander is an age of the patient. For a young growing patient two turns orthodontic appliance that was introduced to expand the each day for the first 4-5 days, one turn each day for the maxillary arch. Rapid maxillary expansion was first proposed remainder of RME treatment. For adults (non-growing) by Angle in the 19th century which led to introduction of a patients because of increased skeletal resistance, two turns series of expansion appliances during which hyrax was each day for the first 2 days, one turn each day for the next 5-developed with the main advantage of being completely
1 7 days and one turn every other day for the remainder of acrylic free . RME treatment. The force from the jack screw is transferred
Hyrax appliance comprises of a screw having mesial and through the framework, to the molars and subsequently the distal extensions; the distal extensions are soldered to the maxillary suture. The more frequently the screw is torque first molar bands, and the mesial extensions are snugly the greater the force.
2contoured and soldered to first bicuspids . The appliance is
Indian Journal of Comprehensive Dental Care
I J C D C1. Shilpa Gupta Saini2. Shaunak Vyas3. Navjot Singh Jassal4. Sanak Kaur Chattha
Date of Submission : 1/4/16 Date of Acceptance : 20/4/16
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

Indian Journal of Comprehensive Dental Care
The spectrum of hyrax as a treatment modality has been unilateral cleft lip and palate. Facial analysis showed a
widened off late with its usage in correction of concave profile with an evident scar in the repaired cleft
anteroposterior and vertical plane as well. Apart from being a region. Intraoral examination showed a retruded maxilla,
palatal expander it can also be used an alveolar bone class III malocclusion with a negative overjet and anterior 3,4,5 6,7transport device distractor , a distractor , a molar crossbite (figure 2a).
distaliser, and in growth modulation with a facemask The treatment objective in this patient was to improve his therapy. profile by forward positioning of the maxilla, correction of
Folllowing are the various case reports which highlight the the anterior crossbite so as to obtain optimal overjet and
ubiquitous usage of the hyrax appliance. overbite. Hyrax was taken up as the appliance of choice but
with a change in its orientation. It was placed Case Report 1-anteroposteriorly with its arms being soldered to bands on
A 14 year old male came with a chief complaint of inability to first premolar and first molar bilaterally. The change in close his teeth properly. He had a history of hypothyroidism direction of the hyrax screw was done to move the anterior and had been on medication for 2 years. On examination he segment of the maxillary complex in a forward position. This had a straight profile with retruded maxilla and an edge to modified hyrax appliance was cemented in the patients edge bite. Maxillary arch was constricted in the canine- maxillary arch and thereafter patient was referred to a premolar region which had brought his upper premolars into maxillofacial surgeon for carrying out vertical and horizontal crossbite [figure 1(a,b)]. osteotomy cuts in premolar-molar region. It was followed by
The treatment objective was to improve his profile and to a period of appliance activation.
correct the crossbite as well as to achieve enough space to After the treatment there was a remarkable improvement in relieve crowding in the maxillary arch. Hyrax was chosen patient's profile, with the correction of overjet and anterior upon as the appliance to bring about arch expansion in the crossbite (figure 2b).transverse plane of space. Appliance was delivered and
Case Report 3-activated according to the previously mentioned norms.
A 13 year old male reported with a chief complaint of reverse Positive results were noted in a span of 2 months with an closure of his upper front teeth during biting. On examination adequate increase in inter canine and intermolar widths he had a concave profile with an anteriorly divergent face, a (figure 1c). Crossbites were relieved in the premolar region.reverse overjet and crowding in upper anterior region with
Case Report 2- buccally placed canine (figure 3a). He was a vertical grower
A 21 year old male presented with the chief complaint of which was noted clinically and then confirmed
backwardly placed upper jaw with a history of repaired cephalometrically.
822
Figure 1a Profile View
Figure 1b Intraoral right buccal view
Figure 1c Maxillary occlusal view after correction
Figure 2a Overjet
Figure 2b Maxillary occlusal view after correction
Figure 3b Maxillary occlusal with appliance
Figure 3a Intraoral frontal view

Indian Journal of Comprehensive Dental Care
To correct the transverse malocclusion hyrax was again our 3) Yilmaz S, Kilic A.R., Keles A. and Efeoglu E.:
appliance of choice. But the vertical proportions had to be Reconstruction of an alveolar cleft for orthdonic tooth
controlled. Therefore, a bonded hyrax (figure 3b) was given in movement. Am J Orthod Dentofacial Orthop. 2000; 117
this case which has an advantage of keeping a check on the (2):156-63.
facial height. In addition to it, palatal expansion is conjoined 4) Dogan, Dolanmaz., Ali, Ihyd. Karaman., Ercan, Durmus., with a relative intrusion of maxillary molars which is followed and Siddik Malkoc.: Management of alveolar clefts using by a forward and upward rotation of mandible thereby dento –osseous transport distraction osteogenesis. The
8reducing the facial height . Angle Orthod. 2003; 73 (6): dec :723-729.
Again, satisfying results were obtained with correction of 5) VegaO, PérezD, PáramoV, FalcónJA new device for overjet and crossbite and keeping a check on the facial height alveolar bone transportation. CraniomaxillofacTrauma as well. Reconstr. 2011 Jun;4(2):91-106.
CONCLUSION 6) Showkatbakhsh R Pourdanesh F, Jamilian A, Ghorbani A,
Hyrax has been a leading treatment modality to correct Behnaz M. Hyrax application as a tooth-borne distractor
transverse discrepancies. With the advent of new for maxillary advancement. J Craniofac Surg. 2011
innovations it has now become a leader in correcting sagittal Jul;22(4):1361-6.
abnormalities along with controlling the vertical component. 7) Nair A Kumar JP, Venkataramana V, Yuvaraj A, Reddy VS, The Kumar SK DentoAlveolar distraction osteogenesis using
rigid intraoral tooth borne distraction device. J Int Oral
REFERENCES Health. 2014 Apr;6(2):106-13.
1) Kumar SA, Gurunathan D, Muruganandham, Sharma S. 8) Pinto FM, Pereira BL, Abi-Ramia,Stuani AS, Stuani MB,
Rapid Maxillary Expansion: A Unique Treatment Artese F. Vertical growth control during maxillary
Modality in Dentistry. J Clin Diagn Res. 2011 Aug, 5(4): expansion using a bonded Hyrax appliance. Dental Press
906-911. Hamula W J Orthod 2012 Jan-Feb;17(1):101-7
2) Hamula DW, Hurt A. The hygienic rapid palatal expander.
J Clin Orthod. 1998 Sep;32(9):562-7.
usage of hyrax is multidimensional with newer
techniques adding more luster to its treatment repertoire.
823

COMPARISON OF THREE NEWER SURGICAL APPROACHES FOR THE MANAGEMENT OF RANULA
ABSTRACT
Oral ranulas are caused by extravasation of mucus from the sublingual glands.
Excision of a sublingual gland, which has the least risk of recurrence (approx.
1%) is considered to be the best treatment, though it still leads to complications
such as dysesthesia of the tongue, damage to Wharton's duct, bleeding and
haematoma. The conventional method of searching for the submandibular
duct begins from the middle of the duct and the major problem is that the
middle part may or may not be deep. This can make it difficult to find the duct,
particularly after it has been displaced by extrusion of a cyst. Attempts to excise
the ranula in conjunction with the sublingual gland likely places the lingual
nerve and submandibular duct at even more risk due to more invasive
dissection. This necessitates the consideration of newer techniques which
decrease the risk of damage to these vital structures and prevents recurrence.
The rationale of the present article is to review the literature and compare the
results of three different approaches for the effective management of ranula.
Keywords: ranula, duct, excision
824
Corresponding author:Name: Dr. Nitin VermaAddress: Assistant Professor, Oral and Maxillofacial Surgeon, Punjab Govt. Dental College, Amritsar
1. Assistant Professor, Oral and Maxillofacial Surgeon, Punjab Govt. Dental College, Amritsar
2. Prof. and Head of the department , Oral and Maxillofacial Surgeon, Punjab Govt. Dental College, Amritsar
3. Post Graduate student, Oral and Maxillofacial Surgeon, Punjab Govt. Dental College, Amritsar
INTRODUCTION treatments, many patients have experienced recurrence
and sometimes larger lesions have occurred, e.g. conversion Mucoceles and ranulas are mucous retention phenomena, of a simple (superficial or oral) ranula into a plunging which develop from the extravasation or retention of
11-13(cervical, burrowing, diving, or suprahyoid) ranula . mucous after trauma to the sublingual gland or one of the 1-5 Despite high recurrence rates, marsupialisation is still minor salivary glands .The prevalence of ranula is about 0.2
suggested as the best choice in children because it is less cases per 1000 person and accounts for 6% of all oral 14, 15invasive than others . Sclerotherapy a non-surgical sialocysts. Clinicians have used several methods of
treatment for oral ranulas, has also been associated with treatment for oral and plunging ranulas. including 16high recurrence rate of 49% . However, the success of a marsupialisation, excision, excision of the ranula and
procedure used to treat a plunging ranula depends on drainage of the contents, total removal of the sublingual complete excision of the sublingual gland and drainage of its gland and evacuation of its contents intraorally, and yttrium-
10,176-10 contents . Excision of the sublingual gland is often scandium- gallium garnet laser . Despite these
regarded as uncomplicated, but the limited access and the
Indian Journal of Comprehensive Dental Care
I J C D C1. Nitin Verma 2. Jeevan lata 3. Sarita Mahajan
Date of Submission : 11/2/16 Date of Acceptance : 4/3/16
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

Indian Journal of Comprehensive Dental Care
fact that the operation involves displacement of two vital simplifies excision of the sublingual gland while protecting
structures make resection a difficult operation, often the submandibular duct. Modified L shaped incision makes 18, 19accompanied by complications . The conventional method dissection of the submandibular duct easier. It is an angular
of searching for the submandibular duct begins from the incision that starts from the lingual frenum, crosses the
middle of the duct , this can make it difficult to find the duct, sublingual caruncle, and bypasses the external side of the
particularly after it has been displaced by extrusion of a cyst. ipsilateral fold, until it reaches the distal end of the first molar
Attempts to excise the ranula in conjunction with the instead of making a conventional arc.
sublingual gland likely places the lingual nerve and The modified incision simplifies orientation for repair submandibular duct at even more risk due to more invasive containing the submandibular duct orifice (the sublingual
16dissection . This necessitates the consideration of newer caruncle). A thin mucosal flap is raised including the techniques which decrease the risk of damage to these vital submandibular duct, the position of which is fixed and structures and prevent recurrence. The rationale of the superficial, and it is easy to find. The most difficult step is present article is to review the literature and compare the separation of the flap just underneath the sublingual fold, results of three different approaches for the effective where multiple minor sublingual ducts tether the gland to management of ranula. the mucosa. The submandibular duct is raised with the
angular flap, because the integrity of its attachment to the A) The first approach studied was a two incision fistula 20 caruncle is maintained. In this approach, two key structures technique for the treatment of oral ranulas. It was
at risk in the procedure have been identified at an early stage conducted by the Independent Ethics Committee of the
in the dissection .After the superficial and medial surfaces Ninth People's Hospital of Shanghai Jiao Tong University
have been exposed, dissection of the deep and lateral School of Medicine on 12 patients. Twelve patients with oral
surfaces of the gland from their bed is relatively ranulas confirmed by fine needle aspiration cytology were
straightforward, and identification of the sublingual vessels enrolled and gave their consent to be treated by this new
is simplified. Careful separation and ligation is required for technique. Exclusion criteria included inflammation
the 1-2 large branches of the sublingual artery and vein detected by blood tests, malignancy of the head and neck,
before their entrance into the gland. The flap is repositioned and radiotherapy to the head and neck.
with a few sutures. A drain is tied to the teeth, and removed The aim of the operation was to make a fistula in the surface
on postoperative day 2.of the ranula to drain the retained mucus. Double incisions
They used the chi square test, the chi square test with a are made (8-15 mm long, and 2-3 mm wide) on the surface of
correction for continuity, and Fisher's exact test, as each cyst, depending on its size (Fig. 1A1).
applicable. Probabilities of less than 0.05 were accepted as After the mucus had drained, the incision was sutured with
significant. the middle mucosal strip in the cyst (Fig.1A2). The patients
Results: were placed on a liquid diet with regular oral rinses for 7 days,
and given prophylactic antibiotics for 3 days. No sublingual There were significant differences in postoperative bleeding gland was excised. The clinical outcomes and complications (p = 0.01), incidence of injury to the submandibular duct (p = were evaluated during a period that ranged from 8-24 0.03), incidence of ranula on the opposite side (p = 0.02), months. Nine ranulas became smaller and gradually duration of operation (p = 0.000), sex (p = 0.03), and volume disappeared, and there were no complications or injury to of intraoperative bleeding (p = 0.000). There were no other Wharton's duct. Three ranulas recurred, but disappeared significant differences.after a second operation. There were no cases of
c) Third approach studied was Anterograde excision of a dysaesthesia of the tongue, or limitation of movement of the
22sublingual gland .tongue as a result of the scar.
Author prospectively studied 50 consecutive patients with B) Second approach to treat oral ranulas is Modified L shaped
ranula who were treated by anterograde excision of the 21surgical approach for excision of the sublingual gland.sublingual gland between May 2012 and January 2015 at
The aim of this retrospective review was to present 1131 Sanming First Hospital, Sanming, Fujian, China. Patients with cases of ranula recorded at from 1981 to 2013. A total of 365 bilateral ranulas and those who had previously been treated patients were treated with the conventional approach, while for ranula were excluded. With the patient under general the other 766 have been treated since 1991 using the anaesthesia and nasotracheal intubation, a linear incision is modified approach. made 1 cm medial and parallel to, the ipsilateral mandible,
and extended from the orifice of Wharton's duct to the The modified L shaped incision is both viable and safe, and
825

Indian Journal of Comprehensive Dental Care
lingual side of the retromolar region. To control bleeding the the gland and the first crossing point of Wharton's duct and
site was infiltrated with a solution of lignocaine and the lingual nerve. It then continues anteriorly to create a
epinephrine. The mucosa was then incised, and blunt tunnel lateral to Wharton's duct. After the glandular tissue
dissection and mosquito haemostats used to expose the lateral to the tunnel had been incised completely without
lateral aspect of the sublingual gland. The posterior part of bleeding, Wharton's duct was exposed and the gland cut into
the gland was gripped with an Allis clamp and constant two parts: superior and inferior. The two parts were then
traction exerted in an anterior, superior, and medial direction opened laterally with Allis clampsor mosquito haemostats to
by the assistant, which exposes the loose areolar tissue expose the medial aspect of the gland, and give a wider
behind the gland. Smooth, blunt dissection was used in the surgical field to visualise and protect Wharton's duct and the
loose areolar tissue to identify Wharton's duct, the main lingual nerve (fig.4.)
trunk of the lingual nerve, the branches of the sublingual The inferior part of the gland is then removed anteriorly and artery and vein, the relations of the lingual nerve and the superior part of the gland is removed posteriorly. Wharton's duct, and the sublingual ganglion split from the Bartholin's duct is identified, ligated, and divided. The ranula main trunk of the lingual nerve (Figs. 3). is ruptured without excision and mucus drained naturally and
The sublingual ganglion and the branches of the sublingual suctioned. Finally, the surgical field is irrigated and inspected,
artery and vein were ligated and divided as close as possible followed by meticulous haemostasis. The incised mucosa is
to the posterior surface of the gland. To prevent damage to loosely sutured back, and a drain inserted through the
the lingual nerve, therefore, anterograde dissection of incision. Patients were recommended to take a liquid diet for
Wharton's duct was started between the posterior surface of 1 week. The drain was removed after 1–2 days.
826
20Fig.1 . Diagram of two incision fistula technique
21.Fig. 2 The conventional and modified
approaches. (A) conventional incision;
(B) modified L shaped incision
22Fig.3 . Before anterograde excision of the sublingual gland the important anatomical
structures and the first crossing point of Wharton's duct (WD) and the lingual nerve (LN) were identified in the space behind the
sublingual gland (G). B=branches of the sublingual artery and vein, SLG=sublingual
ganglion, and R=ranulas
22Fig. 4 . After the glandular tissue lateral to the tunnel has been incised completely
without loss of blood, Wharton's duct (WD) is exposed and the gland cut into two parts: superior (SP) and inferior (IP). LN=lingual
nerve and R=ranulas

Indian Journal of Comprehensive Dental Care
DISCUSSION noted that the space behind the gland itself contained
important anatomical structures, including Wharton's duct,
the main trunk of the lingual nerve, the branches of the sub-ut is still used lingual artery and vein, and the sublingual ganglion, together perhaps because of fear of potential surgical injury to with the first crossing point of Wharton's duct and the lingual adjacent structures when removing the sublingual gland or nerve, which was large. There is no risk of injury to the lingual because of preservation of the function of the gland nerve during anterograde dissection of Wharton's duct,
because at this point the lingual nerve is inferior or medial to Excision of the the duct, not lateral. The medial aspect of the gland, sublingual gland or ranula may carry the potential risk of Wharton's duct, and the lingual nerve are therefore exposed severe hemorrhage from the lingual and sublingual directly, a wider surgical field is provided, and a cleaner plane vasculature, lingual nerve damage, and duct severance.of dissection is achievable without bleeding. The medial
aspect of the gland can be dissected under direct vision, and
further dissection of the lingual nerve is not necessary, so the
risk of injury will be reduced.
CONCLUSION
Excision of a cyst, or a sublingual gland, or both, should not be
The two incision technique is simple and safe, but particular the first choice of treatment. For the management of ranula,
attention should be paid to avoiding injury to Wharton's duct first treatment of choice should be two incision operation.
and the lingual nerve. The width of the middle mucosal strip Since newer techniques (Both modified L shaped and
should depend on the thickness of the cyst's wall, and care anterograde approach ) have lesser chances of injury to
should be taken when inserting sutures to prevent tearing Wharton's duct and lingual nerve in comparison to
the mucosa. conventional approach. These should be considered when
excision of cyst or sublingual gland is to be done or The modified approach takes full advantage of 2 distinct management of recurrent ranula. However, Further studies anatomical characteristics that make it superior to the are still needed to evaluate its long term outcome of newer conventional approach. First, the submandibular duct that techniques.connects to its orifice –
REFERENCESthe sublingual caruncle can be found easily because of its
constant anatomical position. In addition, the front of the 1. Shear M: Cysts of the oral regions. Dental practitioner
submandibular duct, which is superficial and constant, can handbook No. 23 Bristol, England, John Wright & Sons
also be found easily. The modified L shaped incision which Ltd, 1976, pp 148-149
contains the sublingual caruncle in the angular mucosal flap, 2. Van Den Akker HP, Bays RA, Becker AE: Plunging or is a guide to finding the duct methodically from the front. cervical ranula. Review of the literature and report of 4 Because of these anatomical characteristics, the key step of cases. J Maxillofac Surg 6:286, 1978 dissecting submandibular duct turns out to be easy, leading
3. Araki H: An experimental study of oral mucous cyst to an appreciable reduction in injuries to the submandibular
formation. Jpn J Oral Maxillofac Surg 33:467, 1987 duct, the volume of operative bleeding, and the duration of
4. Crysdale WS, Mendelsohn JD, Conley S: Ranulas-the operation. The modified surgical approach has therefore
mucoceles of the oral cavity: Experience in 26 children. made an important contribution to speeding up the progress
Laryngoscope 98:296, 1988 of the operation and improving safety. There were no long
term complications involving the lingual or hypoglossal 5. Catone GA, Merrill RG, Henny FA: Sublingual gland nerves, and a low rate of recurrence, which might result from mucus- escape phenomenon-treatment by excision of the favourable exposure. sublingual gland. J Oral Surg 27:774, 1969
6. S. Garofalo, V. Briganti, S. Cavallaro, et al. Nickel
Gluconate-Mercurius Heel-Potentised Swine Organ
Preparations: a new therapeutical approach for the
primary treatment of pediatric ranula and intraoral
mucocele. Int J Pediatr Otorhinolaryngol, 71 (2007), pp. During Anterograde excision of the sublingual gland it is 247–255
Sclerotherapy and marsupialisation are less invasive than
excision, inspite the rate of recurrence is high b
Excision
of a sublingual gland, which has the least risk of recurrence, is
considered to be the best treatment. But
A
recent report has shown that a tunnel of mucosa was an 23effective approach for oral ranulas , but this method still
risks damaging Wharton's duct and nerve, and might even
lead to new ranulas. Keeping in mind potential risk involved
with these techniques ,consideration towards newer
techniques in the management of ranula has been given.
When compared the modified
angular incision containing the orifice of the submandibular 24duct with a square incision and square flap it was found that
it was less invasive, probably as a result of a combination of
mylohyoid dehiscence, racial predisposition, and previous 25trauma to the mouth or face or previous oral surgery .
.
827

Indian Journal of Comprehensive Dental Care
7. Y. Morita, K. Sato, M. Kawana, et al. Treatment of ranula- plunging ranula managed by the intraoral approach
excision of the sublingual gland versus marsupialization, Tohoku J Exp Med, 200 (2003), pp. 59–65
Auris Nasus Larynx, 30 (2003), pp. 311–314 18. Y.F. Zhao, Y. Jia, X.M. Chen, et al. Clinical review of 580
8. M. Zola, D. Rosenberg, K. Anakwa. Treatment of a ranula rannlas Oral Surg Oral Med Oral Pathol Oral Radial
using all Er, Cr: YSGG laser J Oral Maxillofac Surg, 64 Endod, 98 (2004), pp. 281–287
(2006), pp. 823–827 19. Y.F. Zhao, J. Jia, Y. Jia Complications associated with
9. H.D. Baurmash Treating oral ranula: another case snrgical management of ranulas J Oral MaxillofacSurg,
against blanket removal of the sublingual gland Br J Oral 63 (2005), pp. 51–54
Maxillofac Surg, 39 (2001), pp. 217–220 20. Shaoyi Wang, Zhiyuan Zhang, Chi Yang .Clinical
10. K.A. Al Ruhaimi. Recurrent plunging ranula of the neck evaluation of a two incision fistula technique for the
Saudi Med J, 34 (2013), pp. 313–315 treatment of oral ranulas British Journal of Oral and
Maxillofacial Surgery Volume 54, Issue 1, January 2016, 11. Kurozu T: Clinical and pathological studies of oral Pages 22–24mucous cyst. Jpn J Oral Maxillofac Surg 29:393, 1983
21. GuoRong Zhao, Ping Jib, HongWei Zhao, Yong Li, Ying Li, 12. Parekh D, Stewart M, Joseph C, et al: Plunging ranula: A Ping Liu, Lin Zeng, Fu Gui Zhang. Modified L shaped report of three cases and review of the literature. Br J surgical approach to excision of the sublingual gland Surg 74:307, 1987 British Journal of Oral and Maxillofacial Surgery Volume
13. Natiella JR, Meenaghan MA, Rosa RA, et al: Cryosurgery 53, Issue 8, October 2015, Pages 725–729of major and minor salivary gland: A light microscopic
22. Zhigang Liu, Bin Wang com . Anterograde excision of a evaluation in the Rhesus monkey. J Oral Pathol sublingual gland: new surgical technique for the 8:237,1979treatment of ranulas. British Journal of Oral and
14. H.D. Baurmash. A case against sublingual gland removal Maxillofacial Surgery 54 (2016) 151–154as primary treatment of ranulas J Oral Maxillofac Surg,
65 (2007), pp. 117–121
15. C. Mortellaro, S. Dall'Oca, A.G. Lucchina, et al.Sublingual
ranula: a closer look to its surgical management J
Craniofac Surg, 19 (2008), pp. 286–290
16. M.R. Patel, A.M. Deal, W.W. Shockley.Oral and plunging
ranulas: What is the most effective treatment
Laryngoscope, 119 (2009), pp. 1501–1509
17. H. Hidaka, T. Oshima, S. Kakehata, et al. Two cases of
23. Jia, L. Xing, F. Zhu, et al. Minimally invasive treatment of
oral ranula with a mucosal tunnel
24. C. Yates .A surgical approach to the sublingual salivary
gland
25. S. McKinstry, C. Lewis Bilateral plunging ranula: two case
reports and a review of the literature
Br J Oral Maxillofac
Surg, 53 (2015), pp. 138–141
Ann R Coll Surg Engl, 76 (1994), pp. 108–109
N Z Med J, 126
(2013), pp. 81–86
828

MANAGEMENT OF BISPHOSPHONATES INDUCED OSTEONECROSIS OF THE JAW- A SYSTEMATIC REVIEW
Abstract
Bisphosphonate–Induced Osteonecrosis of the Jaw (BIONJ) adversely affects
the quality of life, producing significant morbidity. Management of BIONJ has
centered on efforts to eliminate or reduce severity of symptoms, to slow or
prevent the progression of disease, and to eradicate diseased bone. The
staging system adopted by the American Academy of Oral and Maxillofacial
Surgeons (AAOMS) categorizes patients based on presence of exposed bone
and severity of signs and/or symptoms. Specific management regimens have
included medicinal management (chlorhexidine rinses, antibiotic therapy,
hyperbaric oxygen, vitamin E, teriparatide and non-surgical sequestrectomy)
and surgical debridement and/or resection of necrotic bone followed by
reconstruction.
Keywords: ostronecrosis, Bisphosphonates, antimicrobials, surgery
reconstruction
829
Corresponding author:Name: Dr. Tejinder KaurAddress: Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.(M) :9814010528e-mail: [email protected]
1. Post graduate student, Department of Oral and Maxillofacial Surgery Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar.
2. M.D.S, Professor, and Head of the Department Department of Oral and Maxillofacial Surgery Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar
3. M.D.S, Assoc. Professor, Department of Oral and Maxillofacial Surgery Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar
4. M.D.S, Assoc. Professor, Department of Oral and Maxillofacial Surgery Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar
5. MDS Professor and Dean Academics Department of OMFS, Sri Guru Ram Das Institute of Dental Sciences and Research, Amritsar
INTRODUCTION
Osteonecrosis, which is also known as avascular necrosis of
bone, aseptic necrosis, ischemic necrosis, is characterized by
the death of bone as a natural consequence of a wide variety used routinely to of systemic and local factors compromising the blood flow of
decrease osteoclast-mediated bone loss in osteoporosis, the bone. This disorder can be caused by an injury or factors multiple myeloma, Paget disease, and complications of such as hemoglobinopathies, anticardiolipin antibodies, metastatic diseasedefects in the thrombotic and fibrinolytic systems, fat
emboli, alcoholism, corticosteroids, radiation therapy and 1bisphosphonates. According to the American Academy of Oral and
Maxillofacial Surgeons (AAOMS), bisphosphonate-induced
osteonecrosis of the jaw (BIONJ) is defined by three main
characteristics: previous or current bisphosphonate
osteoradionecrosis. The clinical symptoms include pain,
fistula, exposed bone, and even extended bone destruction
and pathological bone fracture. Second type of
osteonecrosis has been observed to involve the jaws during
long term of antiresorptive bone treatment
. This type was first reported by Marx in 22003.
There are two principal groups of patients that are affected
with this disorder. The first group suffers from
Indian Journal of Comprehensive Dental Care
I J C D C1. Vishal Mittal2. Tejinder Kaur3. Amit Dhawan4. Jasmine Kaur5. Ramandeep S Bhullar
Date of Submission : 6/2/16 Date of Acceptance : 24/2/16
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

Indian Journal of Comprehensive Dental Care
therapy, exposed necrotic bone in the maxillofacial region vii. Caries
that has been persisted for more than 8 weeks, and no history viii. Periapical pathology.of radiation therapy to the jaws. If these three conditions are
ix. Extraction of tooth with poor prognosis.present, the diagnosis can be confirmed clinically. It is
6Treatment Goalsimportant to exclude local malignancy, trauma, periodontal
disease, and lingual-mandibular sequestration and The major goals of treatment for patients at risk of 3ulceration. developing or who have Bisphosphonate–Induced
Osteonecrosis of the Jaw are:BIONJ treatment has been challenging from the beginning as
there is no consensus regarding the clinical management of · Prioritization and support of continued oncologic patients with BIONJ because of incomplete understanding of treatment in patients receiving IV antiresorptive and the etio-pathogenesis of the disease. The AAOMS 2014 antiangiogenic therapy. Patients having malignant disease Position Paper on Medication-Related Osteonecrosis of the can benefit greatly from the therapeutic effect of Jaws states that the “Treatment objectives for patients with bisphosphonate therapy by controlling bone pain and an established diagnosis of BIONJ are to eliminate pain, reducing the incidence of other skeletal complications.control infection of the soft and hard tissue, and minimize the
· Preservation of quality of life through:progression or occurrence of bone necrosis.”
a) Patient education and reassurance.Different therapeutic approaches have been reported
b) Control of pain.including anti-microbial rinses, antibiotics, local
d e b r i d e m e n t a n d s u r g i c a l r e s e c t i o n , o r a c) Control of secondary infection.combinationthereof. However, since several recent studies d) Prevention of extension of lesion and development of have shown durable diseasefree status after surgical new areas of necrosis.resection of lesions of BIONJ.
MEDICAL MANAGEMENTThe aim of this review is to share different treatment
Treatment of BIONJ with medical therapy alone is most approachesto patients with BIONJ. Fundamentally, commonly employed for patients with less severe disease, treatment can be divided into medical and surgical therapies, those who decline surgery, or those whose comorbidities although a combination is often used. For purposes of clarity, preclude them from surgery. Medical therapies currently in in this review we employ the staging system and treatment use include topical, oral and intravenous antimicrobials, strategies (Table 1.) as described in the 2014 AAOMS position other medications and hyperbaric oxygen (HBO).paper.
ANTIMICROBIALSManagement Strategies for Patients Treated with
· Topical antimicrobialsBisphosphonates5 Chlorhexidine gluconate is a topical bactericidal and Marx R E. et al (2005) found a statistically significant, almost
bacteriostatic agent that has been shown to be effective in threefold reduction in the incidence of osteonecrosis in treatment of patients with BIONJ. Although the pathogenesis patients when preventive measures were applied. Treatment of BIONJ remains unclear, there is evidence that the oralflora, planning for patients who may be prescribed and more specifically bio films, contribute tothe disease bisphosphonate therapy should include thorough process. The use of chlorhexidine is thus rationalized by its examination of the oral cavity and a radiographic ability to decrease total bacterial counts, including assessment. It is important to identify both acute infection
3, 7potentially pathologic organisms.and sites of potential infection to prevent future sequelae
that could be exacerbated once drug therapies begin. · Oral antimicrobialsConsiderations during the clinical and radiographic
Antimicrobials are a mainstay in the management of assessment include:
BIONJ.Antimicrobial therapy is based on clinical observation i. Patient motivation and scientific literature suggesting that pathogenic bacteria
may contribute to BIONJ. Systemic antibiotics may decrease ii. Patient education regarding dental care
bacterial counts in the oral cavity, including pathogenic iii. Fluoride applicationorganisms. Selection of specific antibiotics should be based
iv. Chlorhexidine rinses on patient tolerance, compliance, and prior antibiotic v. Periodontal disease exposure. One should also consider therapies targeted
against common colonizers of BIONJ lesions, including vi. Presence of root fragments
830

Indian Journal of Comprehensive Dental Care
Bacteroide scapillosus, Coryne bacterium species, Fuso 2-week course for patients with persistent stage 1 disease 7, 8bacterium nucleatum, Gemella species, Klebsiell- and up to a 4- to 6-week course for more severe cases.
apneumoniae, Parv imonasmicra, Peptostreptoc Intravenous antimicrobialsoccusanaerobius, Porphyromonasas-accharolytica,
Intravenous antimicrobials may be of benefit in patients with Porphyromonasendodontalis, Porphyromonas gingival is,
pathogenic organisms resistant to oral agents and may Prevotella buccae, Prevotelladisiens, Prevotellainter media,
provide greater tissue penetration in certain cases.When all Prevotella species, Staphylococcus aureus, Staphylococcus
available oral agents have been exhausted and no less epidermidis, Strept ococcusagalactiae, Streptococcus
invasive option exists, it is mandatory to employ long-term anginosus, Streptococcus constellatus, Streptococcus mitis,
intravenous antimicrobials (6 weeks). In the future, it is and a-hemolytic Streptococcus. Over the years penicillin
conceivable that antimicrobial therapy may be more remainedthe first treatment of choice, in patients allergic to
effective in BIONJ treatment when combined with penicillin alternates are clindamycin, fluoroquinolones,
developing delivery mechanisms most capable of metronidazole and newly introduced sitafloxacin. Although
7penetrating biofilms.there is no data to clarify the most appropriate duration of Other Medicationsantibiotic therapy for BIONJ, but it is advisable to prescribe a
831
Table1. Staging of and treatment strategies for bisphosphonate-induced osteonecrosis of the jaw3, 4 (BIONJ) according to the American Association of Oral and Maxillofacial Surgeons (AAOMS).

Indian Journal of Comprehensive Dental Care
· Pentoxifylline and vitamin E offered when disease progresses to the point where 11symptoms are not controlled with medical therapies.The combination of pentoxifylline and vitamin E has been
used successfully in the treatment of jaw osteoradionecrosis A wide spectrum of disease is often seen with stage 2 BIONJ,
and BIONJ.Pentoxifylline, a xanthine derivative with an ranging from focal minimally symptomatic exposed bone to
excellent safety profile decreases inflammation and reduces severely painful widespread bone necrosis. It is thus difficult
blood viscosity by increasing erythrocyte deformability. to recommend a single surgical treatment approach in these
Vitamin E decreases tissue inflammation and fibrosis, and is a patients. Rather, the decision regarding operative
scavenger of free radicals capable of cellular injury. intervention depends on the patient's medical status,
Numerous reports supporting the role of both inflammation comorbidities, pain level, their treatment goals, and the 7, 12, 13and decreased vascularity as contributors to BIONJ make the extent of disease.
use of this relatively well tolerated drug combination a Treatment modalities for stage 2 BIONJrational choice.The duration of treatment has not been
Debridement, marginal resection and segmental resection clarified, but literature suggests that the benefits may are terms commonly seen in the literature describing surgical plateau after 2 to 3 years of use. The recommended dose of treatment of BIONJ. Debridement and marginal resection pentoxifylline is 400 mg sustained release twice daily and
7 both refer to removal of necrotic bone, primarily in the 1000 IU vitamin E daily.
alveolus, with the goal of maintaining an intact inferior · Teriparatide border of the mandible. Segmental resection, on the other
Teriparatide is a subcutaneously administered drug used hand, refers to en-bloc removal of involved bone, including
primarily in the treatment of osteoporosis. It retains the the inferior border of the mandible, with a resulting
anabolic effects of endogenous parathyroid hormone, continuity defect. Success rate vary widely in response to
including promotion of bone remodeling. Teriparatide is local debridement/marginal resection ranging from 15% to
thought to stimulate effectively osteoblast function and 100%.
proliferation, increase osseous cells ignaling and activate Success of debridement or marginal resection may also be osteoclasts. The safety, side effects, dosing, and duration of limited by the difficulty in differentiating healthy bone from therapy for the management of BIONJ are not known. diseased bone. Inadequate removal of affected bone has Currently, this agent is not frequently used in practice for been found to increase BIONJ recurrence. Because the extent treatment of BIONJ and it is important to note that of the osteonecrosis is often greater than what is seen teriparatideis contraindicated in patients with metastatic clinically, preoperative imaging with CT or cone beam CT, bone disease or osteosarcoma. Certainly, promising results bone scintigraphy, and/or MRI can also aid in determining the have been observed with this therapy and, given the limited type and extent of surgery and assist in identifying bony options available for treatment of BIONJ, its use should be margins. Intraoperative fluorescence-guided debridement
7,9,10considered and studied further. has been suggested to assist in differentiating necrotic from
· Hyperbaric Oxygen Therapy viable bone.
HBO therapy has been used for management Tetracycline is used as a bone label for this purpose because it
ofosteoradionecrosis of the jaw for many years and more is incorporated into sites of bone remodeling and thus will
recently has been applied to treatment of BIONJ. HBO only be seen in viable bone. The technique involves
provides greater oxygen to tissues with impaired preoperative administration of doxycycline (100 mg twice a
vascularization reverses impaired leukocyte function and day 10 days before surgery). A fluorescent light source is
also supplies reactive oxygen. All of these effects the applied to the affected region during debridement and areas
oretically contribute to improved wound healing and bone of necrotic bone are seen to fluoresce as a pale bluish-white 14turnover. HBO is seldom used asa singular treatment color whereas viable bone appears brightly fluorescent.
modality, but is morecommonly used as a surgical adjunct. During surgical debridement, extraction of any involved The clinical utility of HBO for management of BIONJ remains teeth is also indicated. It is better to debride diseased tissue
7unclear and it deserves further study. adequately, including removal of adjacent potentially
SURGICAL MANAGEMENT involved teeth, than leave the area inadequately treated to
preserve teeth. Any sharp bony spicules should be removed Focus in the surgical treatment of BIONJ is directed toward and extraction sockets and bony margins should be free of stage-specific therapeutic options. Patients with stage 0 and sharp edges to aid in achieving tension-free primary closure. stage 1 disease generally do not warrant surgical All resected hard and soft tissue should be sent for intervention. In general practice, surgical treatment is histopathological examination and culture sensitivity to
832

Indian Journal of Comprehensive Dental Care
allow directed postoperative antibiotic therapy. been divided into 4 basic categories by Marx R.E: 15, 1. Resections with immediate rigid plate fixation:Adjunctive treatments, including platelet-rich plasma
16 17 18,low-level laser therapy Hydroxyapatite composite , Indicated where reconstruction is required beyond a primary have been used in conjunction with surgical debridement to closure or more commonly in case of a continuity resection. improve postoperative healing. A systematic review of the Rigid plate fixation in this group should be precise and be
20literature on platelet concentrates concluded that it placed with the intent on long-term use.promotes gingival healing and acts as a barrier membrane
2. Resections with delayed rigid plate fixation:between the alveolar bone and the oral cavity.
Indicated in cases with high risk of secondary infection, high Hydroxyapatite composite focuses on the bone formation degree soft tissue loss and patient's debilitation from the and the angiogenesis by the grafting material, dual releasing malignancy. In such cases, it is very reasonable to accomplish simvastatin and bone derived fibroblast growth factor for the the required resection in a shorter focused surgery and plan further prevention of BIONJ. Low-level laser therapy to place a rigid plate later if and when the patient's local stimulates bone healing by increasing vascularity and
20tissue health and systemic conditions improve.osteoblastic differentiation, has been used in conjunction
with surgical debridement of osteonecrosis. However, rates 3. Resect ions with or without r ig id plate of healing after surgical debridement with and without low- reconstruction but requiring soft tissue replacement:level laser therapy are comparable and further research is
Indicated in cases with a significant loss of either mucosal needed to determine the value of low-level laser therapy. In
lining and/or skin due to the antiangiogenesis effect of the summary, in cases of stage 2 BIONJ when debridement and 20bisphosphonate.marginal resection is determined to be the indicated
20, 214. Delayed bone graft reconstruction (free fibula).treatment, the following principles should be applied:
Future Perspectives1. Appropriate preoperative imaging to assess the extent
of disease. Treatments modal i t ies l ike hematopoiet ic cel l
transplantation, Adipose-derived stem cells, plasma rich in 2. Removal of all necrotic bone and any involved teeth to growth factors, ozone and vitamin D supplementation have achieve disease-free bony margins.been advocated for the management of BIONJ, but all these
3. Removal of any sharp bony edges and spicules.modalities are under trial and need further research to
4. Achievement of a layered tension-free primary wound ensure as an optimal patient treatment protocol of BIONJ.closure whenever possible.
Conclusion5. Culture-directed postoperative antibiotic therapy until
Management of BIONJ presents a challenging clinical mucosal healing is seen.
dilemma. Mucosal coverage is the main goal of BIONJ 6. Restraint from wearing any oral prosthetic devices until treatment in order to prevent secondary infection. The
7complete mucosal healing is seen. management of BIONJ remains controversial, and there is no
definitive standard of care for this disease. Non-surgical, Treatment modalities for stage 3 BIONJconservative, and minimally invasive treatment regimens for
Patients with stage 3 BIONJ who present with extensive BIONJ are considered useful to control the disease, leading to
maxillofacial involvement may benefit from wide local predictable good results in cases of lower stages of BIONJ.
debridement or segmental resection of necrotic bone. This Further research is indicated particularly for higher stage
treatment is reserved for those with severe symptomatic BIONJ (refractory stage 3 lesions). BIONJ may also be
disease when other modalities have failed. Segmental approached with new adjunctive treatments such as laser
resection for treatment of stage 3 osteonecrosis of the jaw therapy, HBO, growth factors or hydroxyapatite composite in
followed by reconstruction has shown generally favorable order to ensure an optimal patient treatment protocol. The
outcomes with up to a 90% success rate. As with stage 2 application of adjunctive treatments remains an opinion-
disease, evidence of osteomyelitis at one of the resected based approach rather than an evidence-based one.
margins is a predictor for recurrent disease. Experiences with Controlled studies or clinical trials should be performed to
segmental resection in cases involving both the maxilla and evaluate these adjunctive treatments for BIONJ patients.
mandible has overall been positive with successful long term BIBLIOGRAPHYresolution of BIONJ without recurrence. The same treatment
principles outlined for stage 2 BIONJ also apply to patients 1. Gutta R, Louis PJ. Bisphosphonates and osteonecrosis of 7, 19with stage 3 disease. Reconstructive procedures for the jaws: Science and rationale. Oral surg Oral med Oral
Bisphosphonate-Induced Osteonecrosis of the Jaws have
833

Indian Journal of Comprehensive Dental Care
path Oral radiolendod 2007; 104:186-93 bisphosphonates-related osteonecrosis of the jaw
(BRONJ). Oral Oncology 50 (2014) 1049–10572. Marx R E. Pamidronate (aredia) and zoledronate
(zometa) induced avascular necrosis of The jaws: A 13. Reich W, Bilkenroth U, Schubert J, Wickenhauser C,
growing epidemic J Oral MaxillofacSurg 2003; 61:1115- Eckert A W, et al Surgical treatment of bisphosphonate-
1118. associated osteonecrosis: Prognostic score and long
term results, Journal of Cranio-Maxillo-Facial Surgery 3. Ruggiero SL, Dodson TB, Fantasia J, Goodday R, Aghaloo (2015), j.jcms.2015.07.035T, et al. American association of oral and maxillofacial
surgeon's position paper on bisphosphonate-related 14. Porcaro C, Amosso E, Scarpella R, Carini F Doxycycline
osteonecrosis of the jaws. J Oral MaxillofacSurg 2014; fluorescence-guided Er:YAG laser ablation combined
65: 369-376. with Nd:YAG/diode laser biostimulation for treating
bisphosphonate-related osteonecrosis of the jaw. Oral 4. R. Fliefel, M. Tro¨ltzsch, J. Ku¨hnisch, M. Ehrenfeld, S. Surgery, Oral Medicine, Oral Pathology and Oral Otto. Treatment strategies and outcomes of Radiology (2014),j.oooo.2014.04.014.bisphosphonate-related osteonecrosis of the jaw
(BRONJ) with characterization of patients: a systematic 15. Soydan SS, Uckan S. Management of bisphosphonate-
review. Int. J. Oral Maxillofac.Surg. 2015; 44: 568–585. related osteonecrosis of the jaw with a platelet-rich
fibrin membrane: Technical report. J Oral MaxillofacSurg 5. Marx RE, Sawatari Y, Fortin M, Broumand V. 2014; 72: 322-326.B i s p h o s p h o n a t e - I n d u c e d E x p o s e d B o n e
(Osteonecrosis/Osteopetrosis) of the Jaws: Risk Factors, 16. S. Bocanegra-Pe´rez, M. Vicente-Barrero, M. Knezevic, J.
Recognition, Prevention, and Treatment. J Oral M. Castellano-Navarro, E.Rodri´guez-Bocanegra, et al.
MaxillofacSurg 2005; 63: 1567–1575. Use of platelet-rich plasma in the treatment of
bisphosphonate-related osteonecrosis of the jaw. Int. J. 6. Yamashita J, McCauley LK. Antiresorptives and Oral Maxillofac.Surg. 2012; 41: 1410–1415.osteonecrosis of the jaw. J Evid Base Dent Pract 2012; S1:
233-247. 17. Vescovi P, Merigo E, Meleti M, Fornaini C, Nammour S, et
al Nd:YAG laser biostimulation of bisphosphonate-7. Williams W B, O'Ryan F Management of medication-associated necrosis of the jaw bone with and without related osteonecrosis of the jaw Oral Maxillofacial surgical treatment. British Journal of Oral and SurgClin N Am 27 (2015) 517–525.Maxillofacial Surgery 45 (2007) 628–632
8. Ikeda T, Kuraguchi J, Kogashiwa Y, Yokoi H, Satomi T et al. 18. Miyazawa A. Matsuno T., Asano K., Mataga I. Successful treatment of Bisphosphonate-Related
Development of the HA composite for the prevention of Osteonecrosis of the Jaw (BRONJ) patients with BRONJ. AAOMS 2014; 195-196.sitafloxacin: New strategies for the treatment of BRONJ.
Bone 73 (2015) 217–222. 19. Bodem J P, Schaal C, Kargus S, Saure D, Mertens C, et al.
Surgical management of Bisphosphonate-related 9. H. Kakehashi, T. Ando, T. Minamizato, Y. Nakatani, T. osteonecrosis of the jaw Stage II and III. Oral Surgery, Kawasaki, et al Administration of teriparatide improves Oral Medicine, Oral Pathology and Oral Radiology (2015) the symptoms of advanced bisphosphonate-related j.oooo.2015.10.033.osteonecrosis of the jaw: preliminary findings. Int. J. Oral
Maxillofac. Surg. 2015.07.018 20. Marx RE. Reconstruction of defects caused by
bisphosphonate-induced osteonecrosis of the jaws. J 10. E. H. Dayisoylu, F. C¸.Senel, C. U¨ngo¨r, E. Tosun, M. C¸ Oral MaxillofacSurg 2009; 67: 107-119.ankaya, et al The effects of adjunctive parathyroid
hormone injection on bisphosphonate-related 21. Nocini P.F., Bettini G, Ragazzo M, Blandamura S, Chiarini
osteonecrosis of the jaws: an animal study. Int. J. Oral L, et al. Vascularized fibula flap reconstruction of the
Maxillofac. Surg. 2013; 42: 1475–1480 mandible in bisphosphonate-related osteonecrosis.
EJSO 2009; 35: 373-379.11. Bodem J P, Kargus S, Engel M, Hoffmann J. Value of
nonsurgical therapeutic management of stage I
bisphosphonate-related osteonecrosis of the jaw.
Journal of Cranio-Maxillo-Facial Surgery (2015),
j.jcms.2015.05.019
12. Rupel K, Ottaviani G, Gobbo M, Contardo L, Tirelli G, et al.
A systematic review of therapeutical approaches in
834
ENDODONTIC MANAGEMENT OF IMMATURE TEETH WITH NECROTIC PULP- SHIFTING FROMAPEXIFICATION TO REVASCULARIZATION
Abstract
Immature permanent teeth that have lost vitality have traditionally been
treated by apexification. Through this technique, the formation of an apical
barrier to close the open apex is promoted so that the filling materials can be
confined to the root canal. Because tissue regeneration cannot be achieved
with apexification, a new technique called regenerative endodontic treatment
was presented recently to treat immature permanent teeth. Regenerative
endodontic treatment is a treatment procedure designed to replace damaged
pulp tissue with viable tissue which restores the normal function of the pulp-
dentin structure. After regenerative endodontic treatment, continued root
development and hard tissue deposition on the dentinal wall can occur under
ideal circumstances. In this review article, the rationale behind
revascularization is elaborated along with its protocol and the factors that
affect the outcome of the procedure.
Keywords: apexification, immature, revascularization
835
Corresponding author:Name: Dr. Gunmeen Sadana, MDS, Professor and Head, Department of Paediatric and Preventive Dentistry, Sri Guru Ram Das Institute of Dental Sciences and Research, AmritsarEmail: [email protected]
1. MDS, Professor and Head, Department of Paediatric and Preventive Dentistry, Sri Guru Ram Das Institute of Dental Sciences and Research, Sri Amritsar
2. MDS, Professor, Department of Paediatric and Preventive Dentistry, Sri Guru Ram Das Institute of Dental Sciences and Research, Sri Amritsar
3. MDS, Professor, Department of Paediatric and Preventive Dentistry, Sri Guru Ram Das Institute of Dental Sciences and Research, Sri Amritsar
4. MDS Student, Department of Paediatric and Preventive Dentistry, Sri Guru Ram Das Institute of Dental Sciences and Research, Sri Amritsar
Introduction unpredictability of apical closure and susceptibility of
cervical root fracture after prolonged exposure to Ca(OH)2Endodontic management of immature permanent teeth raised serious concern about the merits of this treatment with necrotic pulps and open apices has been a significant approach.challenge, owing to the presence of thin dentin walls and the
lack of a natural apical constriction that an obturation More recently, the traditional apexification procedure has
material can be placed against. For decades, such teeth have been modified by the introduction of artificial apical barrier
been treated by the apexification procedure, which involved methods with mineral trioxide aggregate (MTA). Although
placement of intracanal calcium hydroxide (Ca(OH) ) to this approach might considerably shorten the treatment 2
induce formation of a calcific barrier at the apex. Despite the period, improve patient compliance, and result in favorable
widespread use of the Ca(OH) based apexification healing of the periapical tissues, it still cannot stimulate the 2
development of apical closure and thickening of radicular technique, the lengthy treatment period that might require
dentin. multiple visits and renewal of the intracanal dressing,
Indian Journal of Comprehensive Dental Care
I J C D C1. Gunmeen Sadana2. Sunil Gupta3. Teena Gupta4. Hashmit Kaur Rai
Date of Submission : 3/2/16 Date of Acceptance : 16/2/16
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

Indian Journal of Comprehensive Dental Care
population doublings, and tissue regeneration capacity than
DPSCs. These evidences suggest that SCAP derived from a On the basis of these considerations, the fate of apexification developing tissue may be a superior cell source for tissue in future treatment protocols for necrotic immature
1 regeneration.permanent teeth seemed to be questionable indeed.5Protocol for Regenerative Endodontic Treatment ProcedureThe path of endodontic treatment took a sharp turn almost a
decade ago, when Iwaya et al showed that continued root Revascularization should include appropriate case selection,
development and apical closure in a necrotic immature tooth with a strict disinfection protocol and use of antimicrobial
were possible when successful disinfection of the root canal paste to achieve complete asepsis and blood clot formation 2was achieved. in canal space followed by placement of an MTA barrier, or
equivalent over blood clot with a final restoration and follow-However, it was in 2004, when Banchs and Trope published a up at regular intervals.case report describing a new treatment procedure for the
management of the open apex called “revascularization.” I) Case selection
The protocol differs from traditional apexification techniques Currently there is no evidence-based guideline to help in that disinfection of the canal is done with both sodium clinicians determine which condition of cases can be treated hypochlorite and chlorhexidine and a combination of three with this conservative approach. The presence of antibiotics (ciprofloxacin, metronidazole and minocycline). radiolucency at the periradicular region can no longer be Unlike traditional apexification or the use of apical barriers, used as a determining factor, nor is the vitality test as in both revascularization procedures allow for increase in both the situation, vital pulp tissue or apical papilla may still present in
3length of the root and root wall thickness. the canal and at the apex. Logically, any remnant of visible
soft tissue that can be visualized under the dental The current (2012) American Association of Endodontists'
microscopeGlossary of Endodontic Terms defines regenerative
endodontics as “biologically-based procedures designed to should give the clinician an incentive to take the conservative physiologically replace damaged tooth structures, including approach, even though the soft tissue may be purely dentin and root structures, as well as cells of the pulp-dentin granulation tissues. However, one can also not rule out the
4complex.” possibility that there are not any remaining pulp tissues in
the very apical part of the canal only because it cannot be It can safely be said that regenerative endodontics is a
detected clinically.treatment revolution in dentistry- the era in which root canal
therapy brings diseased teeth back to life, rather than leaving Although case reports on revascularization are largely from 5a “non- vital” or dead tooth in the mouth. teeth with incomplete apical closures, it has also been noted
6 that reimplantation of avulsed teeth with an apical opening Rationale of Regenerative Endodonticsof approximately 1.1 mm demonstrate a greater likelihood of
Regenerative endodontic treatment can occur in infected revascularization. This is mainly because in enlarged apical
immature permanent teeth because of mesenchymal stem foramen there is a high chance of survival of remaining vital
cells which exist in the apical papilla of immature teeth. pulp in the canal since open apex provides a good
These stem cells from the apical papilla (SCAP) are capable of communication from pulp space to the periapical tissues,
differentiating into odontoblast-like cells forming root therefore it may be possible for periapical disease to occur
dentin.while the pulp is only partially necrotic and infected. It is
Another type of mesenchymal cells, which are called dental necessary to promote vascularization and maintain initial cell pulp stem cells (DPSCs) were discovered and isolated earlier, viability via nutrient diffusion and oxygen supply. This finding have the ability to differentiate into odontoblast-like cells suggests that revascularization of necrotic pulps with fully and form dentin/pulp-like complex when implanted into formed (closed) apices might require instrumentation of the subcutaneous spaces of immunocompromised mice. tooth apex to approximately 1 to 2mm in apical diameter to
7allow systemic bleeding into root canal systems. Both SCAP and DPSCs are as potent in osteo/dentinogenic
differentiation as mesenchymal cells from bone marrows, Another obvious consideration is the duration of the whereas they are weaker in adipogenic potential. SCAP and infection. The longer the duration of infection lesser will be DPSCs show similar features, but they have some differences. the number of survived remaining pulp tissue and stem cells. SCAP show a significantly greater bromodeoxyuridine uptake Additionally, the longer the infection there is in the canal, the rate (an indication of cell proliferation), number of more likelihood of a deeper penetration of microbial colonies
836

Indian Journal of Comprehensive Dental Care
into dentinal tubules. This renders the disinfection more should be carried out for 30 min at every 5 minutes. This
difficult to accomplish. The technique also shows maximum continuous procedure completely disinfects the root canal,
positive outcome in young adults as younger adult patients as the survival of microorganisms or its toxins will prevent the
generally have a greater capacity for healing. revascularization procedure.
ii) Disinfection protocol In the next appointment, after 1 week irrigation of the canal
is again carried out for 15 min. If vital tissue is present in the A successful vital pulp treatment requires a good seal against canal the concentration of NaOCl used is 5.25% and if it is not bacteria, no severe inflammatory reactions, and stable present and revascularization is carried out by blood clot, haemodynamics within the pulp. Use of intracanal irrigants then the concentration used by most authors is 1.25-2.5%.with placement of antibiotics for several weeks as a means of
disinfection of the canal is a very important step to achieve Revascularization procedure has also been carried out only
revascularization. with the copious irrigation of the canal without
instrumentation. The noninstrumentation procedure using Calcium hydroxide Ca(OH) has been advocated as a root 2
6% NaOCl and 2% chlorhexidine coronal irrigation has shown canal disinfectant and for stimulation of hard tissue repair at to preserve the remaining vital dental pulp stem cells in the apex of infected immature teeth. Several favorable single step revascularization procedure. Hence it is believed biological properties have been attributed to it when used to be critical for pulp revascularization.clinically. It is antimicrobial, it has the ability to dissolve
However Rossi-Fedele et al have showed that formation of necrotic tissue in the root canal and it can induce apical
precipitate when chlorhexidine and NaOCl are mixed leading closure by hard tissue formation. It also acts as a 10to discoloration and other side effects. Combination of 17% physiochemical barrier, which precludes the proliferation of
EDTA with 6% NaOCl is safe till now and has shown to be residual microorganisms and prevents the reinfection of the
effective for regeneration of pulpal stem cells. root canal from the oral cavity.
Ethylenediaminetetraacetic acid (EDTA) very effectively However, a freshly mixed paste of Ca(OH) has a pH of 2
releases growth factors from human dentin as well as helps in approximately 12.5 and is potentially toxic to not only
11,12the survival of stem cells of apical papilla.8bacterial cells but human cells too. The use of Ca(OH) in 2
iii) The use of antimicrobial pasterevascularization is therefore not without criticism, which
are: As calcium hydroxide has its own disadvantages in
revascularization process, combination of antibiotic paste 1. Ca(OH) may destroy the ability to induce the nearby 2
has been used as an intracanal medicament. By using the undifferentiated cells to become odontoblasts and antibiotic paste, the pulp tissue is able to fill in the remaining damage the remaining pulp tissue, apical papilla and canal space. There is a particular combination of antibiotics HERS (Hertwig's epithelial root sheath).which effectively disinfects root canal systems and increases
2. Direct contact of Ca(OH) paste with the tissue which will 2 revascularization of avulsed and necrotic teeth. This induce the formation of a layer of calcific tissue which
combination includes metronidazol, minocycline and may occlude the pulp space, therefore preventing pulp
ciprofloxacin, which is known as triple antibiotic paste. The tissue from regeneration.
triple-antibiotics regimen was first tested by Sato et al. to be 133. Even if apexification with Ca(OH) is rendered successful 2 effective against the Escherichia coli infected dentin in vitro.
owing to its antibacterial properties, the procedure will The same research group also tested their bactericidal leave behind a short root with thin dentinal walls with a efficacy against microbes from carious dentin and infected
9high risk of root fracture. pulp. They found that the mixture of antibiotics is sufficiently
potent to eradicate the bacteria. The gentle treatment regimen is, therefore, an attempt to
conserve any viable tissues that may be remained in the canal The application of antibacterial drugs may represent one
system which harbor stem cells, i.e., SCAP in the apical papilla method of eradicating bacteria in root canal treatment. This
and DPSCs (dental pulp stem cells) in the pulp. Avoidance of concept is also known as Lesion Sterilization and Tissue
trauma to the tissue around the apex is advised. After proper Repair (LSTR) therapy. This technique has been developed
disinfection, the remnants of the survived HERS at the apices by Cariology Research Unit of Nigata University School of 14 of immature teeth may organize the apical mesodermal Dentistry, Japan. Composition and mixing instructions for
15tissue into root components. the tri-antibiotic paste is adapted from Hashino et al.
In the first appointment continuous irrigation with NaOCl Antibiotics (3M mix-MP) combines Ciprofloxacin 200mg,
837

Indian Journal of Comprehensive Dental Care
Metronidazole 500mg, Minocyclin 100mg and a carrier (MP): perception then treatment is administered with the addition
Macrogol ointment or Propylene glycol is used. The of evoking an intracanal blood clot. Induction of bleeding to
combination of drugs has been shown to penetrate facilitate healing is a common surgical procedure. It was first
efficiently through dentine from prepared root canals, proposed by Ostby in 1961 to induce hemorrhage and form
suggesting that topical application of the drug combination blood clot in the canal space of mature teeth in the hope to
may be potent in sterilizing lesions in root canal treatment. guide the tissue repair in the canal. Later in 1974 Myers and
Fountain attempted to regenerate dental pulp with blood Disadvantages of using antimicrobial pasteclot filled in the canal. The mechanism of how a blood clot
The concern of the antibiotic paste is that it may cause benefits the root canal revascularization is not entirely clear, bacterial resistance. Also, the paste contains both although the possible reasons could be that blood clot may bactericidal (metronidazol and ciprofloxacin) and act as a natural fibrin scaffold for cell attachment, bacteriostatic (minocycline) antibiotics. Additionally, proliferation, and differentiation to facilitate the minocycline may cause tooth discoloration. Reynolds et al regeneration and repair of tissues into the canal. SCAP cells have suggested that the discoloring effect of the minocycline from the apical papilla may migrate into the root canal and can be minimized by occluding the dentinal tubules in the produce dentin-pulp complex-like tissue and delivers pulp chamber with a bonding agent, then placing a root canal abundant growth factors within the blood clot, such as projector into the chamber, and filling the space between the platelet-derived growth factor which will aid in projector and the dentin with a flowable composite resin. revascularization.After the resin sets, the projector can be removed and the
Hemorrhage is induced by over instrumentation with either triple mix antibiotics paste can be placed into the canal in a endodontic files or an endodontic explorer penetrating backfill manner to the level of CEJ.slightly into the remaining pulp tissue or periapical tissue.
When discoloration occurs after using the triple antibiotic This procedure induces bleeding into the canal and the paste, internal bleaching can be performed during the follow bleeding is left for 15 minutes so that the blood would clot in up examinations when evidence of maturation of the tooth the canal and stopped at a level 3mm below CEJ. MTA is then has been observed. placed over the blood clot.
Cefaclor instead of minocycline can also be substituted in the At this point, it is unsure of which factors in the blood clot are 16paste to avoid discoloration. important. When these factors are isolated, they can be
In addition, the use of white MTA instead of grey MTA should incorporated into a synthetic scaffold that will be easier to for 9also be considered. clinicians to manipulate compared with a blood clot.
However platelet rich plasma as been tried as a successful iv) Blood clot formation in canal spaceclinical alternative. Ding et al. discussed the value of use of
Revascularization can be carried out with or without the PRP in whom it is difficult to produce bleeding in the canal formation of blood clot. As until now no guideline has been 17with a file. A recent case report has suggested the possibility proposed for revascularization, it is completely on the
of PRP as a potentially ideal scaffold for pulp revitalization in clinician to decide whether the canal should be instrumented 16tooth with necrotic pulp and a periapical lesion.for inducing blood clot or not depending on the visual or
v) MTA barrier, or equivalent, placed over blood clot, Final tactile perception of soft tissue remaining within the root restoration and follow-upcanal system. Lack of responsiveness to cold or electric
testing is not considered to be indication of loss of vitality, as Once the intracanal infection is controlled and a physical
scaffold to promote cell growth and differentiation has been most of the revascularization procedures are carried out in achieved, next important step is coronal seal to prevent immature tooth with open apex. Despite the preoperative reinfection. In revascularization after inducing blood clot, irresponsiveness of vitality testing of the tooth, if some MTA is placed over the clot. If revascularization is carried out vitality is noted during treatment either by sensitivity to without the use of blood clot then after drying the canal with instrumentation within the root canal system or by the visual paper point, MTA is placed carefully over the tissues in the or tactile perception of soft tissue remaining within the root root canal. A small piece of collacote may be placed at the canal system then blood clot is not induced within the canal pulp chamber to support the MTA cement which is to be space, as the remaining vital pulp supplies the stem cells and placed over it. This is followed by the placement of a wet growth factor responsible for revascularization.cotton pellet and temporary filling material. Patient is then
However if there is lack of evidence of residual vital pulp recalled after 2- 3 weeks and if the tooth is asymptomatic
tissue within the root canal system either by tactile or visual
838

Indian Journal of Comprehensive Dental Care
then the temporary filling material and the cotton pellet is emergence of this concept, clinicians should re- evaluate
replaced with a bonded resin restoration or glass ionomer existing modus operandi while developing the treatment of
cement. certain clinical cases. This is principally imperative while
dealing with immature teeth, as they still have growth left to The use of MTA is for its excellent microleakage-proof accomplish, hence, are more likely to carry potent stem cells property and biocompatibility. Additional placement with that enables the tissue to regenerate and repair better than glass ionomer/resin provides a double seal, further securing
5matured tissues.the sealing ability and the integrity of the filled access.
ReferencesThe tooth should be followed up periodically to observe the
maturation of the root. If after several rounds of intra-canal 1. Wigler R, Kaufman AY, Lin S, Steinbock N, Hazan-Molina
irrigation and medication the clinical symptoms show no sign H, Torneck CD. Revascularization: a treatment for
of improvement, i.e., persistent presence of sinus tract, permanent teeth with necrotic pulp and incomplete
swelling and/or pain, apexification procedure should then be root development. J Endod 2013 Mar;39(3):319-26.
carried out. If no signs of regeneration are present after 3 2. Iwaya SI, Ikawa M, Kubota M. Revascularization of an months, then more traditional treatment methods can be immature permanent tooth with apical periodontitis initiated. and sinus tract. Dent Traumatol 2001 Aug;17(4):185-7.
Factors that affect the results of regenerative endodontic 3. Banchs F, Trope M. Revascularization of immature 6treatment permanent teeth with apical periodontitis: new
There are some factors that affect the results of regenerative treatment protocol? J Endod 2004;30:196-200.
endodontic treatment. To achieve successful results of the 4. https://www.aae.org/uploadedfiles/ clinical_resources treatment procedure, a thorough understanding of these /guidelines_and_position_statements/scopeofendo_refactors is very important. gendo.pdf
The first factor is the disinfection of the canal. The absence of 5. Palit Madhu Chanda, Hegde KS, Bhat SS, Sargod SS, bacteria is critical for successful revascularization because Mantha S, Chattopadhyay S. Tissue engineering in the new tissue will stop at the level it meets bacteria in the endodontics: root canal revascularization. J Clin Pediatr canal space. In necrotic cases with apical periodontitis it must Dent 2014 Summer;38(4):291-7.be recognized that the vital tissue might not be normal pulp
6. Bin-Na Lee, Jong-Wook Moon, Hoon-Sang Chang, In-tissue, despite the fact that root development continues and Nam Hwang, Won-Mann Oh, Yun-han Hwang. A review dentine maturation occurs. In teeth with open apices and of the regenerative endodontic treatment procedure. necrotic pulps, it is possible that some vital pulp tissue and Restor Dent Endod. 2015 Aug; 40(3): 179–187.Hertwig's Epithelial Root Sheath remain. When the canal is
7. Torabinejad M, Chivian N. Clinical applications of mineral properly disinfected, the inflammatory process reverses and 9 trioxide aggregate. J Endod 1999;25:197–205.these tissues may proliferate.
8. Cvek M. Treatment of non-vital permanent incisors with The second factor is the apex diameter. A tooth with an open
calcium hydroxide: I—follow-up of periapical repair and apex allows the migration of mesenchymal stem cells into the
apical closure of immature roots. Odontol Revy root canal space, and this could allow host cell homing to
1972;23:27–44.form new tissue in the root canal space. An apical opening of
1.1 mm in diameter or larger is beneficial, with natural 9. Kleier DJ, Barr ES. A study of endodontically apexified regenerative endodontic treatment occurring in teeth. Endod Dent Traumatol 1991;7:112–7.approximately 18% to 34% of teeth with immature roots.
10. Rossi-Fedele G, Dogramaci EJ Guastalli AR, Steier L, de The third factor is the patient age. Several case reports of Figueiredo JA. Antagonistic interactions between regenerative endodontic treatment procedures have sodium hypochlorite, chlorhexidine, EDTA, and citric generally been limited to patients who are reaching acid. J Endod 2012;38(4):426-31.
3,18,19,20adolescence, mostly aged from 8 - 16 years. Based on 11. Hargreaves KM, Giesler T, Henry M, Wang Y.
these case reports, it would not be advisable to perform Regenerative potential of the young permanent tooth:
regenerative endodontic treatment procedures in children what does the future hold? J Endod 2008;34(7
younger than 8 years or older than 16 years. Suppl):S51-6.
Conclusion12. Galler KM, D'Souza RN, Federlin M, Cavender AC,
Regenerative endodontics is a concept and because of the
839

Indian Journal of Comprehensive Dental Care
Hartgerink JD, Hecker S, Schmalz G. Dentin conditioning 17. Ding RY, Cheung GS, Chen J, Yin XZ, Wang QQ, Zhang CF.
codetermines cell fate in regenerative endodontics. J Pulp revascularization of immature teeth with apical
Endod 2011;37(11):1536-41. periodontitis: a clinical study. J Endod 2009;35(5):745-9.
13. Sato I, Ando-Kurihara N, Kota K, Iwaku M, Hoshino E. 18. Shin SY, Albert JS, Mortman RE. One step pulp
Sterilization of infected root-canal dentine by topical revascularization treatment of an immature permanent
application of a mixture of ciprofloxacin, metronidazole tooth with chronic apical abscess: a case report. Int
and minocycline in situ. Int Endod J 1996;29:118 –24. Endod J 2009;42:1118-1126.
14. Takushige T, Cruz EV, Asgor Moral A, Hoshino E. 19. Garcia-Godoy F, Murray PE. Recommendations for using
Endodontic treatment of primary teeth using a regenerative endodontic procedures in permanent
combination of antibacterial drugs. Int Endod J immature traumatized teeth. Dent Traumatol
2004;37(2):132-8. 2012;28:33-41.
15. Hoshino E, Kurihara-Ando N, Sato I, et al. In-vitro 20. Chueh LH, Huang GT. Immature teeth with periradicular
antibacterial susceptibility of bacteria taken from periodontitis or abscess undergoing apexogenesis: a
infected root dentine to a mixture of ciprofloxacin, paradigm shift. J Endod 2006;32:1205-1213.
metronidazole and minocycline. Int Endod J
1996;29:125–30.
16. Kling M, Cvek M, Mejare I. Rate and predictability of pulp
revascularization in therapeutically reimplanted
permanent incisors. Endod Dent Traumatol
1986;2:83–89.
840

SOLAR ENERGY – ITS USE IN DENTISTRY
Abstract:
The global demand for energy is currently growing beyond the limits of
production. To meet future energy demands efficiently, an effective renewable
energy solution should be investigated. Although many renewable sources of
energy are available, yet solar energy is one of the promising option as it is
abundantly available to be tapped. Through this paper, an attempt has been
made to review the potential use of solar energy in dentistry.
Keywords: Solar energy, dentistry
841
Corresponding author:Name: Harmanpreet Singh, Address: Post graduate student, Department of Public Health Dentistry, Swami Devi Dyal Hospital and Dental College, Barwala, Panchkula.(M) : 09815121244Email: [email protected]
1. Post graduate student, Department of Public Health Dentistry, Swami Devi Dyal Hospital and Dental College, Barwala, Panchkula.
2. MDS, Professor and Head, Department of Public Health Dentistry, Swami Devi Dyal Hospital and Dental College, Barwala, Panchkula.
3. MDS, Senior Lecturer, Department of Public Health Dentistry, Swami Devi Dyal Hospital and Dental College, Barwala, Panchkula.
4. MDS, Senior Lecturer, Department of Public Health Dentistry, Swami Devi Dyal Hospital and Dental College, Barwala, Panchkula.
INTRODUCTION consumption and 100 times more the world's coal, gas and
oil reserves. Moreover, the solar energy is available all the In a country like India, where majority of the people are (2)day along to be tapped by anyone and that too free of cost. residing in the rural areas in which electricity is one of the
major problem, so to overcome the issue of the electricity Solar energy is produced by thermonuclear process leading
an alternate source of energy need to be investigated for to production of heat and electromagnetic radiations.
providing electricity to the people residing in those areas. Approximately 650,000,000 tons of hydrogen is converted (3)Renewable energy sources need to be explored. Solar into helium every second. Inspite of this, the solar
energy is one such source, as an amount of solar/sun energy radiation energy coming to earth is some 200,000,000 billon 2which strikes the earth surface is greater than annual global kWh. On a clear sunny day, between 800-1000 W/m (global
(1)energy consumption. It has been estimated that the solar radiation) reaches the ground as some of the radiations are (4)energy which is being received by the earth surface is more lost while penetrating the atmosphere. These solar
than 1500 times the world's commercial energy radiation thus can be converted into electricity by means of
Indian Journal of Comprehensive Dental Care
I J C D C1. Harmanpreet Singh2. Nidhi Gupta3. Preety Gupta4. Vikram Arora
Date of Submission : 16/1/16 Date of Acceptance : 24/2/16
Indian Journal of Comprehensive
Dental Care
JULY- DEC 2016 • VOL 6 • ISSUE 2

Indian Journal of Comprehensive Dental Care
(6)Photovolatic cells. Advantage of Using Soladey
Now a days, the solar energy is finding its way in day to day • The Ionic Process is activated simply by light and
use not only in urban areas but also in rural areas and far water
away places where availability of electricity is a problem. • Titanium dioxide rod produces ions to break down
Solar energy driven products provides a compelling solution plaque
for remote and off-grid communities, particularly rural areas • Requires little or no toothpasteof the developing countries, which may not have reliable
• Works on tough dental stains, encourages whiter access to consumables such as gas or may have only very (5) teethexpensive gas.
• Convenient to keep in your car, bag, and child's This article intends to review the potential usage of solar lunchbox so ideal for travel or where water is unavailableenergy in dentistry which ranges from mobile dental vans,
• Cleans and refreshes dentures and bracesdental instruments, oral hygiene maintenance, sterilization
of instruments, electricity for lights and air conditioners. • No electrical cords or batteries
Solar Powered Toothbrush • More effective for plaque removal than an ordinary
toothbrushA mechanical toothbrush powered by the sun. First invented
by Dr. Yoshinori Nakagaina (Japan) and first manufactured in • Ionic action in the saliva is naturally antibacterial the year 1980. Dr. Kunio Komiyama, a dentistry professor and continues after brushingemeritus at the university of Saskatchewan, designed the
• Brush handle and titanium dioxide rod can last a first model of solar powered toothbrush. Newer model of
lifetimelight-activated toothbrush, (Soladey-J3X) is incorporated
• Uses economical changeable brush heads.with a TiO semiconductor and a solar panel. It does not work 2
in the dark, though the brush needs about as much light as a Solar Powered Portable Dental Kit (Fig. 2)(6)solar-powered calculator would to operate.
Is a self contained portable dental system which is powered Mechanism of action of Soladey-J3X Ionic toothbrush (Fig. by solar energy. This helps a dental professional to provide 1) services in remote rural areas(as the kit contains chargeable
battery for micrometer-handpiece and foot control), high in When exposed to any light source (a fluorescent bathroom Himalayas or Amazon jungles. With this system, there is light, a plain light bulb, or sunlight), the photosensitive almost a minimal use of electricity as the power is supplied titanium rods inside Soladey-J3X converts light into by solar panels and there is no use of wall plugs. It is in use by negatively charged electrons (ions). The rods release these the US Army and US marine corps since 1995 and many ions, which blend with saliva to attract positive (hydrogen)
(9)humanitarian organizations.ions from the organic acid in the dental plaque causing its
decomposition. The reaction could also have an effect on Solar powered Autoclave (7) plaque formation. There is also evidence that the powdered
Mechanism of action :TiO2 semiconductor irradiated with visible light has a
Solar energy operated autoclaves are being developed which bactericidal effect against Escherichia coli and streptococcus (8) make use of broadband light absorbing particles mutans.
842
Legend to Fig. 1
Mechanism of action of Solar Powered Toothbrush
Source: http://www.connect-green.com/tag/solar/
Legend to Fig. 2
Solar Powered Dental Kit
Source: Brochure Bell dental products
Legend to Fig. 3
Solar powered dental van
Source: Dental Tribune; the world's dental
newspaper South African Edition – Oct 2013

Indian Journal of Comprehensive Dental Care
(Nanoparticles) such as metallic nanoshells, nanoshell Solar powered electricity
aggregates, and conductive carbon nanoparticles. These Solar powered electricity is the direct conversion of sunlight nanoparticles when dispersed in aqueous solution and into direct current (DC) electricity. Before it can be used in illuminated by sunlight, have been shown to convert homes and business (Clinic), it has to be changed into absorbed solar energy to steam at an efficiency of just over alternating current (AC) electricity using an inverter. The 80%, where less than 20% of the energy contributes to inverted/ changed current then travels from the inverter to heating the liquid volume. In the solar steam generation the building's fuse, and from there to the appliances that process, broadband light-absorbing nanoparticles create a need it. Energy storage (battery) is needed for night use large number of nucleation sites for steam generation within when no sunlight is there. PV panels use the photovoltaic the fluid. As the light is absorbed by a nanoparticle, effect to turn the sun's energy directly into electricity, which temperature difference between the nanoparticle and the can supplement or replace a building's usual supply. To surrounding fluid is established because of a reduced generate as much electricity as possible, PV panels need to thermal conductivity at the metal–liquid interface: this local spend as much time as possible in direct sunlight. A sloping,
(13)temperature increase may become sufficient to transform south-facing roof is the ideal place to mount a solar panel.the liquid in the direct vicinity of the nanoparticle into vapor.
Solar Hybrid Air Conditioner On sustained illumination, the vapor envelope surrounding
This refers to air conditioning (cooling) system that uses solar the nanoparticle grows, eventually resulting in buoyancy of
energy or off grid power supply. An air-conditioning system the nanoparticle–bubble complex. When this complex
utilizing solar energy (absorption cooling systems) would reaches the surface of the liquid, the vapor is released,
generally be more efficient, cost wise, if it was used to resulting in a vigorous non equilibrium steam generation that
provide both heating and cooling requirements in the does not require the bulk fluid temperature to have reached (14)(10) building it serves. Solar energy heats a fluid that provides its boiling point.
heat to the generator of an absorption chiller and is re-With nanoparticle dispersants, temperatures of both the circulated back to the collectors. The heat provided to the liquid and the steam increases far more rapidly than the generator drives a cooling cycle that produces chilled water. temperature of pure water, with the liquid water reaching The chilled water produced is used for cooling. Solar thermal 100°C more rapidly with nanoparticle dispersants than water energy can be used to efficiently cool in the summer, and also without nanoparticles. Using a solar concentrator (Fresnel heat domestic hot water and buildings in the winter. Efficient lens or dish mirror) to deliver sunlight into the nanoparticle-absorption chillers nominally require water of at least 190°F dispersed aqueous working fluid, this process is capable of
(15)(88°C).delivering steam at a temperature of 115–135°C into a 14.2-L (11) Sensitive dentistry clinic in Port Charlotte, Florida, United volume for a time period sufficient for sterilization.
States, became the first dental clinic to use solar energy Solar powered mobile dental and medical clinic (Fig. 3)system as cooling method. The five ton hybrid air
The seven-meter solar powered mobile dental truck is conditioning unit was installed, which comes with a rooftop designed to provide crucial health services to the people solar panel. With a typical air conditioning system, the living in rural areas and far off places of Africa. The truck has compressor accounts for most of the energy consumed. The compartments that help health professionals provide hybrid system uses its solar panel to collect the sun's heat, hearing diagnostics as well as eye and blood tests. It even has which is converted to energy that refrigerates and warms the a small dental clinic. The truck's dental clinic has a dental air, allowing it to completely bypass the compressor. It also chair, an x-ray unit, a water distiller and a needle incinerator. uses heat pump rather than the standard electric coils. Unlike Solar panels on the truck charge the truck's lighting and the a photovoltaic solar panel system, solar air conditioner TV that shows public information, videos to patients as they doesn't require constant direct sunlight and can run for four queue for medical services. It also relies on an inbuilt (16)days on just four solid hours of sun.generator to help power the truck's other equipment. Apart
Solar powered production of Plaster of Parisfrom providing health service, it also helps in providing
education to the people. This is done through a 12-meter Solar power is also finding its way in the production of plaster
solar-powered internet school that can accommodate at of paris. Solar energy provides the required heat for the
least 21 people. Twenty four solar panels provide nine hours calcination process. The plaster of paris produced with the
of power a day to this mobile classroom. It is equipped with help of solar energy is of much superior quality (in term of (12) whiteness and setting time) as the one produced in which laptops and even a 50-inch electronic board.
843

Indian Journal of Comprehensive Dental Care
heat source is wood, coal and diesel. This superior quality of dental plaque. Journal of the Osaka Odontological (17)plaster of paris will be very useful product in dentistry. Society. 1986; 49: 550-59.
Conclusion 9. Bel ldentalproducts: http://www.bdproducts.
qwestoffice.net/products_travelbell.php. last accessed Solar energy is an important part of life and has been since on feb 2015.the beginning of time. It is capable of producing the raw
power required to satisfy energy needs of the entire planet 10. Neumann O, et al. Solar vapor generation enabled by
with the advantage of being one of the least destructive nanoparticles. ACS Nano.2013; 7: 42–49.
energy source. Use of solar energy in dentistry has proven to 11. Neumann O, Ferontic C, Neumann AD, Dong A, Schell K, be promising. However, further studies are required to Lu B et al. Compact solar autoclave based on steam explore the hidden potential of solar energy in this field. generation using broadband light-harvesting Rferences nanoparticles. Proceedings of the National Academy of
1. Lewis N S. Toward cost-effective solar energy use. Science. 2013;110(29): 11677–81.
Science 2007; 315(5813): 798–01. 12. Jenkins C. Istrodent : A South African company leading
2. Gupta S K, Anand R S. Development of Solar Electricity the way in mobile health care. Dental Tribune-South
Supply System in India: An Overview. Journal of Solar African Edition, 2013; 1(3):1&3.
Energy Volume 2013;(2013) Article ID 632364:10 13. Devabhaktuni V , MansoorAlam , Depuru S S R , GreenII R
3. AIA Research Corporation; Solar Dwelling Design C, DouglasNims , CraigNear. Solar energy: Trends and
Concepts; U.S. Department of Housing and Urban enabling technologies. Renewable and Sustainable
Development, Washington D.C;1976 Energy Reviews. 19. 2013;555–564.
4. Thermal use of solar energy -Austrian Development 14. Mittal V, Kasana K S, Thaku N S. The study of solar
Corporation (2009). absorption air-conditioning systems. Journal of Energy
in Southern Africa. 2005; l 16(4): 59-66. Ice-cooling 5. Kaseman T, Boubour J, and Schuler D A. Validation of the System Reduces Environmental Burden”Efficacy of a Solar-Thermal Powered Autoclave System
for Off-Grid Medical Instrument Wet Sterilization. 15. The New Otani News. New Otani Co.,Ltd. 2000-06-28.
American Journal of Tropical Medicine and Hygiene. Retrieved 2007-11-08.
2012; 87 (4): 602–07. 16. Port Charlotte's Sensitive Dentistry uses Sun for AC. The
6. Uswak G, Hoover J, Lee J, Li J, Karunanayake C . A Double- Sun newspaper: Wednesday May5,2010.
blind Cross-over Study evaluating the Efficacy of a Light- 17. Acharya H N, Chandok A. Production of plater of paris activated Toothbrush. International Journal of using solar energy. International Journal of Engineering Experimental Dental Science. 2012; 1(2): 57-60 and Technology. 2013; 2 (4): 516-19.
7. Bhusari B M, Banavali K A, Kotak B. Light Energy
Conversion Toothbrush (Soladeytm) Towards a Super
Clean Mouth! : A Review. Journal of Dental and Medical
Sciences. 2013; 8(4): 30-32.
8. Kusunoki. K, Oku. T, Koni. H. A study on the effect of the
solar energy conversion toothbrush on the control of
844

Indian Journal of Comprehensive Dental Care 845
DENTAL DILEMMA-11
Dr. Adesh S Manchanda, Reader, Department of Oral Pathology & Microbiology, SGRD Institute of Dental Sciences and Research, Sri Amritsar
Dr. Balwinder Singh, Senior Lecturer, Department of Oral Medicine & Radiology, SGRD Institute of Dental Sciences and Research, Sri Amritsar.
Dr Ramandeep S Narang, Professor & Head, Department of Oral Pathology & Microbiology, SGRD Institute of Dental Sciences and Research, Sri Amritsar .
QUESTION:A 40 year old male complains of burning sensation and reddish white discoloration of the left commissural
region and buccal mucosa of the oral cavity (Figure 1) since 2 years. Patient gives a history of bidi smoking since
13 years. Histopathological examination revealed dysplastic features upto two third of the epithelium and
moderate inflammation in the connective tissue stroma. (Figure 2)
Identify the condition?
Figure 1 Figure 2
Answer to DENTAL DILEMMA 10 -: Adenomatoid Odontogenic Tumor

Indian Journal of Comprehensive Dental Care 846
Dr.Sumeet Sandhu, one of the most renowned Oral
and Maxillofacial Surgeons of this region, academician thpar excellence, was born on 7 February 1966 to S.
Balwant Singh and Mrs. Surinder Kaur Dhillon. After
finishing high school from Maharashtra, she did her
Bachelors' in Dental Surgery from Govt. Dental College,
Amritsar in 1983 followed by her Master's degree in
Maxillofacial Surgery in 1991 from the same Institute. Her
astute clinical acumen and teaching skills were beneficial for the patients and students
alike. She left her Government service to serve Sri Guru Ram Das Institute of Dental
Sciences & Research, Amritsar in 1997. She was instrumental in starting the Department
of Maxillofacial Surgery which was enhanced to a Post Graduate Department. under her
agesis.
She went on to become the Principal of Sri Guru Ram Das Institute of Dental Sciences
& Research, Amritsar on Ist June, 2015. She had to her credit numerous publications and
contributions at the National and International conferences. She was the brain behind the
inception of the “Punjab State Chapter of AOMSI” in 2011. It was under her able thguidance that the Institute 40 National Conference of AOMSI in November, 2015.
Rightly called “Mentor of Mentors”, she was loved and revered by one and all. She left for rdher heavenly abode on 23 April,2016. She is survived by her husband, a daughter and a
son.
In recognition of her contributions to the specialty, the national association has
dedicated a Panel discussion – Dr. Sumeet Sandhu Memorial Panel discussion” at the
national forum.



















