
Connect Spring 2013
28
-
Upload
eastern-health -
Category
Documents
-
view
223 -
download
1
description
Connect is a full-colour magazine published four times per year for Eastern Health employees. The publication’s content focuses on employees, concentrating on their roles, achievements, innovations and successes. The goal of the magazine is to tell stories that demonstrate how employees are achieving Eastern Health’s strategic directions, as well as the organization’s vision - Healthy People, Healthy Communities. The magazine is distributed to all Eastern Health employees either in print or electronically using a “digital reader” format. It is also be available to the general public, on-line, through the organization’s website. Newfoundland, Canada
Transcript of Connect Spring 2013


Meet Wayne. Wayne usually works inInfrastructure Support at the WaterfordHospital in St. John’s. He’s also a part-timeSanta and full-time Zumba enthusiast(“Heh, I lost 80 lbs dancing!”) with a greatsense of humour and a commitment toworking safely, each and every day. Waynesays, “We had a real laugh shooting these‘what not to do moments’ and I hope theyremind people just how silly we can besometimes when we don’t put safetyfirst!”
Spring 2013
Connect is published by the CorporateCommunications department of EasternHealth.
Connect is printed internally by PrintingServices.
Please address any comments orsuggestions to Susan Bonnell, Editor:
Corporate CommunicationsAdministrative OfficeWaterford Bridge RoadSt. John's, NL A1E 4J8
(709) [email protected]
125
16 22
Q U A L I T Y & S A F E T Y
5 Getting a Handle on Safety
8 Shared Approach + Shared Benefits =Safer Together
11 Buying Smart Means Buying Safe
12 The Sticking Point
16 …Alone Again, Naturally
18 Living the Values
22 Storm Troopers!Eastern Health Staff vs. 60 Centimetres
M Y S T O R Y
26 Safety...a Way of Life
SAFETY MOMENTS

Cover Photography by Phil SimmsOn the Cover: Pandora White, Ed Sears, Joy Maddiganand Wayne Humber
Contributors
1 Robyn LushCorporate Communications
2 Tom GoddenOccupational Health and Safety
3 Deborah CollinsCorporate Communications
4 Angela LawrenceCorporate Communications
5 Carl ThomasOccupational Health and Safety
6 Susan BonnellCorporate Communications
7 Kimberly WellsOccupational Health and Safety
8 Miranda BungayOccupational Health and Safety
9 Phil SimmsCorporate Communications
1
2
8
5
7
4
3
6
9
4
Both research and experience tell us: health careworkplaces are some of the most hazardous. Eachand every day, employees are exposed to
numerous risks, from chemical and drug exposures toradioactive material and x-ray hazards, from bloodborne pathogens and biological hazards to ergonomichazards like repetitive tasks and patient handling. Alsosad but true is the threat many of our employees face ofphysical and psychological violence.
Being safe is everyone’s responsibility, which is whywe have dedicated an entire issue of Connect to thisimportant issue. I hope you enjoy the stories in thisedition and that they have an impact on you and yoursafety mindset.
Safety must be embedded into every action we take,from the individual performing hand hygiene at theright time, to the leader making decisions with respect tostaffing levels, to the organization’s purchase of safetyequipment or the design of new buildings.
But we all know that safety doesn’t end with theemployee. The safety culture of our organization is a keydeterminant of both employee well-being and clientsafety; maintaining a safe workplace allows for increasedfocused on the quality of care we provide to our patients,residents and clients.
In our strategic plan, we identified the developmentof an integrated safety plan – bringing together bothsides of the equation – because we know that improvingsafety outcomes in any one area of the organizationcontributes to the safety of all. I’m proud to see that thisplan is now in place and work continues on thisimportant goal.
Our Quality and Risk Management Framework,Program Quality and Safety Committees, InfectionPrevention and Control strategies, Occurrence ReportingSystem and Occupational Health and Safety Committeesare all key components of a holistic approach to safety,but the real key to success is a just and trusting culturethat supports frequent reporting of incidents, accidentsand near misses.
Whether or not you sit on a committee or play a leadrole in safety, you are a member of the team that canimprove the workplace for our employees and protectthe quality of care we provide to the public.
Together, we can be a safe and supportive workplace. Together, we can be the definition of quality and
safety in one.
Message from the President and CEO

5Spring 2013
Q U A L I T Y & S A F E T Y
5
Getting aHandle onSAFETY
by DEBORAH COLLINSPhotography by Phil Simms
What do transfer belts, mechanical lifts,ceiling lifts, orange tubes and purplesheets have in common?
They are all devices used to move patientsand residents safely – protecting them and thehealth care staff who are moving them.
Safety has always been a key considerationwhile handling patients and residents in ourfacilities; however, as with all aspects of healthcare, ongoing advances in training andequipment translate into improvements as staffmove patients in their beds, from bed to chair,and assist with washing and dressing routines.
How are we making those improvements?Through the Eastern Health Safe Patient/ResidentHandling Program.
Piloted at Agnes Pratt Nursing Home, St.John’s in the spring of 2012, the program movedon to Golden Heights Manor, Bonavista in the fallof 2012 and is currently being implemented atHoyles-Escasoni Complex in St. John’s.Ultimately, the goal is to implement it at all ourlong-term care facilities, hospitals and healthcentres.PANDORA WHITE AND CLIENT

6
Q U A L I T Y & S A F E T Y
The program places equalimportance on the safety of bothpatient and care provider. Thisintegrated approach to safety inour hospitals and nursing homes isvery much in sync with EasternHealth’s new Integrated Safety Planas well as Together, We Can,Eastern Health’s Strategic Plan2011-2014, which identifies safetyand quality as a strategic priority.
Here’s one example of howthings have changed:
In the past, our employeecaregivers may have pivoted apatient from bed to chair and back.This practice relied heavily on useof good body mechanics. In thisscenario, a patient may besomewhat anxious as a successfultransfer depended on thecaregiver’s strength and ability.This particular task has been
replaced with use of ‘stand assistlifts.’ This piece of equipment usespatient’s abilities as well, and allowscaregivers to complete the tasksafely.
“This integrated approach tosafety is definitely better,” saysAruna Ralhan, Eastern Health’sRegional Ergonomics ProgramCoordinator, Occupational Health,Safety and Rehabilitation.
“The core of the program isthat the procedure or equipmentused will maximize the function ofthe patient or resident, whilebalancing it with the caregiver’ssafety. There is lot of emphasis onindividual assessment to choosethe right tools for the task at hand.”
Aruna says this programrepresents a change in thought andprocess and takes time andcontinuous re-enforcement.However, she adds that caregiversonly want to do their best for theirpatient or resident, and once theyrealize that this program focuseson that goal, it’s an easy sell.
Pandora White agrees. APersonal Care Assistant at theAgnes Pratt Nursing Home in St.John’s, she felt there was a definiteneed for this kind of program, butwondered how hard it might be to
integrate the new processes intoher daily routine.
“Now that it has been put intopractice, I feel it is one of the mostimportant and effective tools weuse,” she says. “The staff membersthat have received training have allcome back with positive outlooksand are working hard to practicesafe resident handling every day.”
The safe handling programmakes perfect sense in acute careas well. Often there is a quickchange in patient’s status, soongoing assessment to identify theright intervention and piece ofequipment - at any point of care -is essential to keep everyone safe.
Proper training andequipment for patients andresidents should also translate intofewer workplace injuries for staff,and in turn reduce staff shortages,which benefits everyone.
Families of patients andresidents also need to be educatedabout this change in practice. Butonce they know that the programfocuses on their loved one’scomfort, safety, and maximumfunction, while also ensuringcaregiver safety, their responseshave been quite positive.
“I think this program ensures
I feel it is one of the most importantand effective tools we use.
“
“

SAFETY MOMENT
Walk the TalkIn case you are thinking that falls are onlydangers to people who work on scaffolds andsteel girders high in the sky, think again. Mostfalls actually occur on the same level and arecaused by just tripping over an obstacle orslipping on something. If you see a hazard,address it.
� Keep walkways and floors free ofobstacles like boxes and cords. Food onthe floor has also caused serious falls.
� Flooring surfaces must be even andsecured. Watch out for loose tiles andraised carpeting.
� Don’t rush. Pay attention to your walkingsurfaces and take short, deliberate stepswhen walking on wet or slippery surfaces.Walk with your feet pointed slightlyoutward, and make wide turns at corners.
A R E N E W E D C O M M I T M E N T
7Spring 2013
The Safe Patient/ResidentHandling Program has threecomponents:
Patient/Resident Assessment
� Employees will assess patient/resident abilitieswithin 24 hours of admission
� Patient/resident handling and movementstatus is documented on the resident care plan
� Assessments are done on an ongoing basis toensure the most appropriate equipment andtechniques are used with thepatients/residents, as their individual abilitiesmay change over time
Safe Handling and MovementTechniques and Training
� Employees are trained in safe patient/residenthandling and movement techniques
� Employees are trained to identify risks andappropriate interventions for various scenarios
� More than one employee will often be requiredto safely handle and move a patient/resident
Safe Handling Equipment Use andTraining:
� Employees are trained in the use of equipmentfor the safe handling and movement of apatient/resident
� Safe handling equipment includes transferbelts, floor based mechanical lifts, ceiling lifts,and friction reducing devices such as orangetubes, purple sheets and draw sheets
a dignified and respectful approach to those weserve,” says Pandora. “It helps to ensure safety,comfort and consistency and has shown to be verybeneficial to both staff and residents. If wecontinue to implement these safe practices, I feelthe result will be a very positive one to allinvolved.” �
1
2
3

8
Q U A L I T Y & S A F E T Y
JOY MADDIGAN
There’s safety in numbers. This tried and true pieceof advice underlies Safer Together, Eastern Health’snew integrated safety plan.
The plan is based on the understanding that aneffective safety culture, the bedrock of a safe organization,is linked to all aspects of safety – patient safety, employeehealth and safety, as well as safe equipment, buildings, andpolicies. It follows that creating such a culture requires allhealth care professionals to work together towards acommon goal.
President and CEO Vickie Kaminski has seen adefinite shift in how safety is viewed in health care. As aSurveyor for Accreditation Canada, she has seen theseparate goals around patient and staff safety and qualityconverge in recent years.
“Client safety and employee safety have traditionallybeen viewed as distinct and separate entities,” she says,“with the result being that different safety processes oftencompete for the attention of managers and staff, when, inreality, many of the foundational elements to improve

9Spring 2013
A R E N E W E D C O M M I T M E N T
by DEBORAH COLLINSPhotography by Phil Simms
REGINA COADY
safety are the same for both clients and employees.”Safer Together is the organization’s first attempt to
formally align its safety resources and expertise in acomprehensive way. Joining forces and working in acomplementary and collaborative manner, will improvesafety for the benefit of both clients and employees.
“The Integrated Safety Plan is an excellentdemonstration of Eastern Health’s commitment to safetyand to working together,” says Regina Coady, Directorof Occupational Health, Safety and Rehabilitative Services.“We know there is a strong relationship between
workplace safety and patient, resident, client safety andthis plan provides a great foundation for strengthenedwork between all parties.”
While much work has been done to improve safety,there is more to do. The plan allows Eastern Health tobuild on initiatives in order to make safety an everydayreality. Its purpose is to improve client and employee safetyoutcomes by focusing on three fundamental directions: � Building an integrated safety strategy� Strengthening the culture of safety� Reducing harm and preventing injury

10
Bringing EasternHealth’s diverse safetymanagement systemstogether to develop acommon vision withshared, but distinct, goalswill be a new Safety Network.It will consist of a network of safetyprofessionals, including, but not limited toOccupational Health, Safety and Rehabilitation,Infection Prevention and Control, Clinical Services,Quality Patient Safety and Risk Management andHuman Resources.
This focused and shared attention to safety has thepotential to be a powerful catalyst for change when itcomes to improving Eastern Health’s safety culture, andbuilding on the progress already made.
Quality Perspectives, Quality SolutionsThe problem of risks and medical safety is a critical
issue squarely facing health care today. Over the pasttwo decades, there has been more recognition of theeffect that frequency of errors, health care associatedinfections and other failures have on the delivery ofhealth care.
Some of the most common adverse eventsexperienced by Canadian patients and clients includereceipt of a wrong medication or dose by a healthprofessional, health care associated infections, trips andfalls, in-hospital hip fractures, and adverse transfusionreactions.
The Canadian Patient Safety Institute, Safer Healthcare Now and Accreditation Canada help facilitate bestpractices in health organizations and Eastern Health isno exception. Major initiatives are underway in theareas of:� Medication Reconciliation
Goal: reduce medication errors during andfollowing an admission to hospital
� Ventilator Associated PneumoniaGoal: eliminate pneumonia in individuals using aventilator
� Stop Infection Now CollaborativeGoal: improve hand hygiene and environmentalcleanliness
� Surgical Site InfectionsGoal: reduce surgical site infections
� Central Line Infections Goal: reduce blood-borne infections associationwith use of a central line
� Acute Myocardial Infarction Care Goal: reduce mortality
� Venous Thrombolytic Embolus (VTE) InitiativeGoal: reduce/ prevent VTE
� Falls StrategyGoal: reduce falls and falls that cause harm
� MoreOB Goal: safe obstetrical experience for mother andbaby
Patients and clients have acknowledged EasternHealth’s efforts.
In the first Client Satisfaction/Experience of CareSurvey conducted by Eastern Health during 2011-2012,respondents rated ‘concern for safety’ consistently high,with an average score of 81.2 throughout acute careinpatient, outpatient services, and emergency services.
“These numbers are encouraging to the staff andphysicians at Eastern Health as we strive to providetimely and high quality care to the men, women andchildren that we serve,” said Joy Maddigan, Directorof Quality, Safety and Risk. “However, this feedbackfrom our clients also serves to hold us accountable inareas where improvement is needed, as we continue tomake safety a priority in the care we provide.” �
Q U A L I T Y & S A F E T Y
SAFETY MOMENT
Dress for SuccessWhat you wear on your feet is more than just afashion statement when it comes to safety. Besure to wear footwear that:
� Provides good traction
� Covers the entire foot (including the heelsand toes)
� Provides support and comfort for jobsthat require frequent standing or walking
� Is made of sturdy material to help protectthe feet against punctures, rolled ordropped objects, liquid or corrosive spills(mesh, canvas, cloth topsiders, clogs andcrocs are out!)
Elizabeth Lace is a Manager for MaterielsManagement on the Burin Peninsula. Amember of the Product Quality and Safety
Committee, Elizabeth says the team is alwayslooking at ways to improve the safety of staff andclients.
“Sometimes individuals come to us forassistance in investigating safer ways of doing thework we do,” she says, “and at other times we takethe lead and initiate projects.”
The committee consists of representativesfrom each of the various key disciplines withinEastern Health and is committed to improving theprocess of evaluation, implementation andeducation of products and equipment throughoutthe organization.
Their projects have included:� Support and implementation of safety
needle devices � The glove management program� The standardization and purchase of acute
care beds, long term care beds, critical carebeds, birthing beds, transport stretchers andlifts
—R. Lush
A R E N E W E D C O M M I T M E N T
Buying$martMeans Buying Safe
11Spring 2013
12
Q U A L I T Y & S A F E T Y
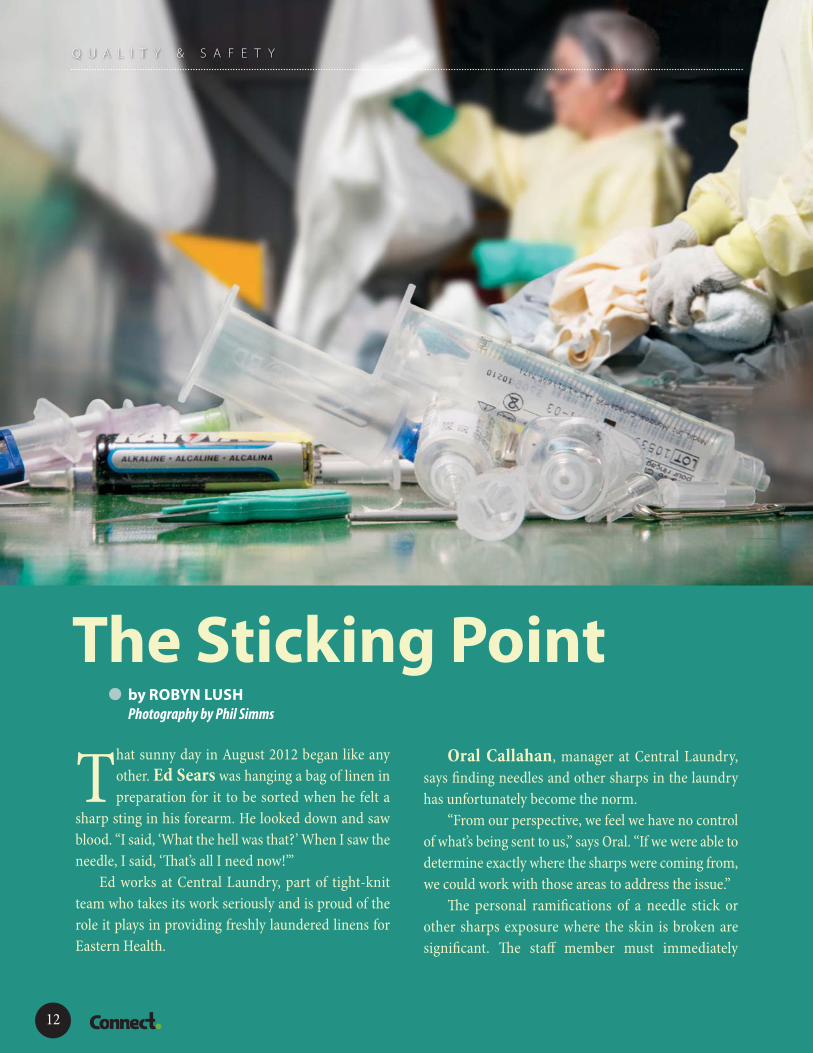
That sunny day in August 2012 began like anyother. Ed Sears was hanging a bag of linen inpreparation for it to be sorted when he felt a
sharp sting in his forearm. He looked down and sawblood. “I said, ‘What the hell was that?’ When I saw theneedle, I said, ‘That’s all I need now!’”
Ed works at Central Laundry, part of tight-knitteam who takes its work seriously and is proud of therole it plays in providing freshly laundered linens forEastern Health.
Oral Callahan, manager at Central Laundry,says finding needles and other sharps in the laundryhas unfortunately become the norm.
“From our perspective, we feel we have no controlof what’s being sent to us,” says Oral. “If we were able todetermine exactly where the sharps were coming from,we could work with those areas to address the issue.”
The personal ramifications of a needle stick orother sharps exposure where the skin is broken aresignificant. The staff member must immediately
The Sticking Pointby ROBYN LUSHPhotography by Phil Simms
administer first aid and then reportthe incident to an OccupationalHealth and Rehabilitationrepresentative. If the incidentoccurs after hours, they must go tothe nearest emergencydepartment.
And that’s just the beginning.As with all employees who
have experienced an occupationalexposure to blood borne pathogensand who cannot identify thesource, Ed faced six months offollow-up testing to ensure he wasnot infected with Hepatitis B,Hepatitis C or HIV.
It’s been a stressful situation forhim that has made a big impact onhis life.
“You gotta wait and see,” saysEd. “There’s a possibility I could’vebeen infected with AIDS. I was toldthe chances were slim, but it’salways there, in the back of mymind – what if?”
Cyril Howse, a 37-yearEastern Health veteran and amember of Central Laundry’sOH&S Committee, shows a displayboard they use at various EasternHealth sites during NorthAmerican Occupational Safety andHealth (NAOSH) Week. It haseverything from clamps to blades,and scalpels to needles, which haveall been found in laundry bags.
“We use this display to showstaff the surprising and serious
things we find,” says Cyril. “If theycan see the things we see, maybe itwill make them think twice whenit comes to properly disposingthese items.”
Having worked in several roleswithin Eastern Health, Cyril seeshow busy we’ve all become andfeels that is a contributing factor.
“Our organization has fantastic
ORAL CALLAHAN
13Spring 2013
A R E N E W E D C O M M I T M E N T
ED SEARS
CYRIL HOWSE

SAFETY MOMENT
Aware to Care Many accidents and injuries occur when youare distracted while working. Concentrate onthe work at hand, and keep your mind on yourwork.
� Set up your work station in a clearunobstructed location with good lighting,proper electrical circuits and away frombusy foot traffic that would causedistractions.
� Every day we make decisions we hope willmake the job faster and more efficient.Shortcuts that reduce your safety on thejob are not shortcuts, but an increasedchance for injury.
� Confidence is a good thing.Overconfidence can be too much of agood thing. Don’t start a task withincomplete instructions, and do ask aboutprocedures and safety precautions.
� Keep it clean. A well-maintained area setsa standard for others to follow.
141414
staff, from our doctors and nurses to housekeepingand laundry workers,” he says. “We are all dedicatedto the client, their safety and care. But we need to doa better job of thinking about each other, our fellowworker and how the work we do is connected. Whatwe do in laundry affects the comfort and safety of staffand patients who rely on our service. At the sametime, work done in a clinical setting has direct impacton the effectiveness and safety of the service weprovide.”
So what else can we do to ensure the safety ourco-workers and staff?
“Report, report, report,” stresses OccupationalHealth and Safety Manager Tom Godden. “Weneed staff to report safety hazards or incidents,otherwise we have no way of knowing how serious anissue is, how often it occurs, or potentially how toaddress it.”
“Not only that,” he adds, “we have a moralobligation to report because that same thing thathappened or almost happened to you could happento another employee. Yes, it takes time to file a report.And sometimes it seems like nothing changes. But itdoes matter. These reports do not disappear into thestratosphere – we see them, we act on them. “Staffsafety really matters.”
We need to do a better jobof thinking about eachother, our fellow workerand how the work we dois connected.
“ “
Q U A L I T Y & S A F E T Y

15Spring 2013
What can I do to prevent needle stickinjuries / BBF from occurring?
� Consider all sharps as potentially infectious andhandle them with care to prevent accidental exposure.
� Ensure prompt and proper disposal of sharpsfollowing use
� Do not leave used needles, lancets, or other sharps onclient’s beds, bedside tables or over bed tables.
� Do not stick used needles into the mattress of any bedor stretcher.
� Remove and change sharps containers when they arethree-quarters full – do not overfill!
What is considered to be a significantexposure?
� Needle stick injuries, sharps injuries, or human bites,where skin is obviously broken and usually bleedsafter the event (Percutaneous)
� Any contact with broken skin (Cutaneous)� Any contact with conjunctiva (eye membrane), or
mucous membranes of the nose or mouth (Mucosal)
What do I do if I have a significantexposure?
1. Administer First Aid:a. Percutaneous – allow immediate bleeding of
wound, wash injured area well with soap and waterand apply antiseptic, if available
b. Cutaneous – remove contaminated clothing, washarea well with soap and water and apply antiseptic,if available to open wounds
c. Mucosal – flush well with large amounts of water
2. Report the injury to the:a. Supervisor of the work areab. Occupational Health Nurse (OHN) at your facilityc. Emergency Room (after hours only)
3. The area supervisor or designate must completethe Occupational Health Source Risk Assessment Formand fax to Occupational Health at your facility.
4. Complete the Employee Incident / Accident Report
The full Blood Borne Pathogen policy can be found in thepolicy section of the intranet under global policies.
New Policy Directs Action After ExposureIndividuals with direct or indirect patient, resident, or client contact have an increased risk for potential exposure
to body fluids capable of transmitting blood borne pathogens. To help guide and inform staff, a new Blood BornePathogen policy has been developed for Eastern Health. Occupational Health Nurse Coordinator Karen Donovanhas been involved in drafting the policy. “To date this fiscal year,” she says, “there have been 179 exposures,79 per cent of which have been needle stick injuries. If safety-engineered sharps andappropriate personal protective equipment (PPE) were used, like face masks andeye shields, most cases of needle sticks and other blood exposures could beprevented. “However,” Karen says, “once exposed, the biggest issueis employees not knowing what steps to take. That’s where thepolicy and accompanying education pamphlet come in.” �
Once Exposed...
A R E N E W E D C O M M I T M E N T

16
Q U A L I T Y & S A F E T Y
16
…Alone Again,
TONY PENNEY

17Spring 2013
A R E N E W E D C O M M I T M E N T
17
An evening medicationdelivery to the home of aclient with both a mental
health and addictions diagnosis, oran impromptu counseling sessionin a car - during a transport to andfrom various appointments withclients; it’s all in a day’s work forTony Penney, an AddictionsSpecialist with Eastern Health’sMental Health and AddictionsProgram.
As a member of the program’sAssertive Community TreatmentTeam (ACTT), Tony works withdozens of clients living in andaround St. John’s who struggle witha variety of issues, such as multiplesubstance abuse, mental healthdiagnoses, housing challenges and,in some cases, criminal records.
“Even though we are in a‘helping profession,’ our assistancecan sometimes be viewed asintrusive by our clients,” Tony says.“It’s important to be aware of aclient’s mindset at any given time,and to be prepared for suddenchanges in behaviour in a one-on-one encounter, to ensure the safety
of both parties.” For this reason, Tony and his
co-workers follow standard safetyprocedures, which are simple buteffective:• Be familiar with client logs, or
records, so that you are awareof any recent incidents whichcould pose a risk
• Keep your cell phone charged• Maintain regular contact with
co-workers, informing themof your whereabouts
• Carry an emergency kit withfirst aid supplies, water, aflashlight and booster cables
• Always back into a client’sdriveway
• Keep your boots or shoes onin a client’s house
“You have to use commonsense,” Tony says. “All the safetypolicies in the world won’t matterif you don’t follow them. The risksare minimal, but you can’t be 100per cent sure of the client’sbehaviour; it could change in aninstant.”
“Safety - as a strategic priority
- extends beyond our buildings,especially to those who work aloneor in isolation,” says ReginaCoady, Director of OccupationalHealth and Rehabilitation Services.“They work in circumstanceswhere they cannot be seen or heardby a co-worker, when assistancewould not be readily available tothem in case of an emergency, or ifthey become injured or sick.”
Others who work alone includethe nurses in Public Health andHome and Community Care whomake home visits and theBehaviour Management Specialistswith the Community SupportsProgram, to name only a few.
While it is not alwayshazardous to work alone it can be,depending on the individualcircumstances. Employees whowork alone or in an isolated areaface an increased risk ofconfrontations or even violence.This can happen in a variety ofsettings: in emergencydepartments or psychiatric units,where frustration or aggression canerupt - or in long-term carefacilities, where many residentssuffer from dementia and mayexhibit aggressive behaviour.
Even though such incidents arenot that common, when they dooccur the consequences can beserious. The wide variety ofcircumstances makes it important
Naturallyby DEBORAH COLLINSwith CARL THOMAS and MIRANDA BUNGAYPhotography by Phil Simms


SAFETY MOMENT
Work. Rest. Repeat Muscles benefit from taking a break or restfrom what they are doing. That is, they are lesslikely to become fatigued or tired from being inthe same position or doing the same taskrepetitively. Short intervals for recuperationhelp muscles to sustain high levels of effortmore of the time. “Rest” does not need to be fora long time, or even away from work. Here aresome things to do on your break:
� Change your posture.
� Look away from where you are used tolooking, and let your eyes readjust for alittle while.
� Do a different task that uses differentmuscles.
� Taking appropriate short breaksthroughout your day may help to keepyour overall level of fatigue and burn out incheck.
Source: Safety Services Newfoundland andLabrador, 2010
19Spring 2013 19
to assess each situation individually to ensuremaximum safety for all involved.
The Newfoundland and LabradorOccupational Health and Safety Act andRegulations (2009) states that when a worker isassigned to work alone or in isolation, anassessment must be conducted to identify thepotential hazards and associated risks. EasternHealth’s Occupational Health, Safety and &Rehabilitation Department worked in consultationwith the Human Resources Program and PolicyDevelopment to develop the Working Alone or inIsolation policy. This policy includes all workingalone or in isolation situations for workersproviding community-based services.
Important safeguards are check in/check onprocedures, as well as emergency responseprotocol procedures to be followed should aworker fail to check in as scheduled. EasternHealth is also identifying providers of electroniclone-worker monitoring systems. These systemswork with cell phone technology to provide ameans of effective, efficient, and reliable check inprocesses for those working alone or in isolation.
Knowing that appropriate safety measuresare in place and emergency response protocols areready if and when they are needed frees our healthcare professionals to do what they do best –provide skilled and compassionate care.
“Although I am always on alert, I don’t worryabout safety while I’m treating a client,” says Tony.“If I’m consumed with worry, it may interfere withthe care I’m giving. While I must be aware of theclient’s frame of mind, I am also very aware thatmy clients’ complex needs have resulted in thembecoming marginalized and disenfranchised –and often very frustrated.
“I need to remain calm, even when theycannot. For safety’s sake.” �
A R E N E W E D C O M M I T M E N T



Storm Troopers! Eastern Health Staff VS. 60 Centimetres
Clearly, it takes more than blizzards, blackoutsand blocked driveways to keep Eastern Healthemployees from their posts. That much was
clear during ‘Snowmageddon’ - the winter blast that hitthe St. John’s area on Friday, January 11.
The phrase ‘essential employees’ has a specialsignificance in health care; hospitals and long-term carehomes don’t shut down in a storm. Patients andresidents still require round-the-clock care and ouremployees take their responsibilities very seriously. Weheard numerous stories about staff members whoeither arrived early, in anticipation of the storm, stayeduntil help arrived – or worked double shifts. Others,who weren’t even scheduled to work, offered to comein.
One nurse from Hoyles-Escasoni, who lives onehour from St. John’s, got a hotel room in the city onThursday night, and then headed to work on foot the
next morning!Down the road at the
Glenbrook Lodge, nursingcare teams and supportdepartments pulledtogether to ensure thatessential services wereprovided to all theresidents, waiting long after their shifts ended untiltheir replacements arrived.
Across town, at the Agnes Pratt Nursing Home, agroup of nurses set up beds in the Gathering Squareactivity area the night before to be available for workin the morning. Sharing their ‘dorm’ was the supportservices supervisor, and site administrator AnnetteMorgan, who says “staff made the best of achallenging time, and made it a great opportunity tospend some social time with their co-workers,
22
Q U A L I T Y & S A F E T Y
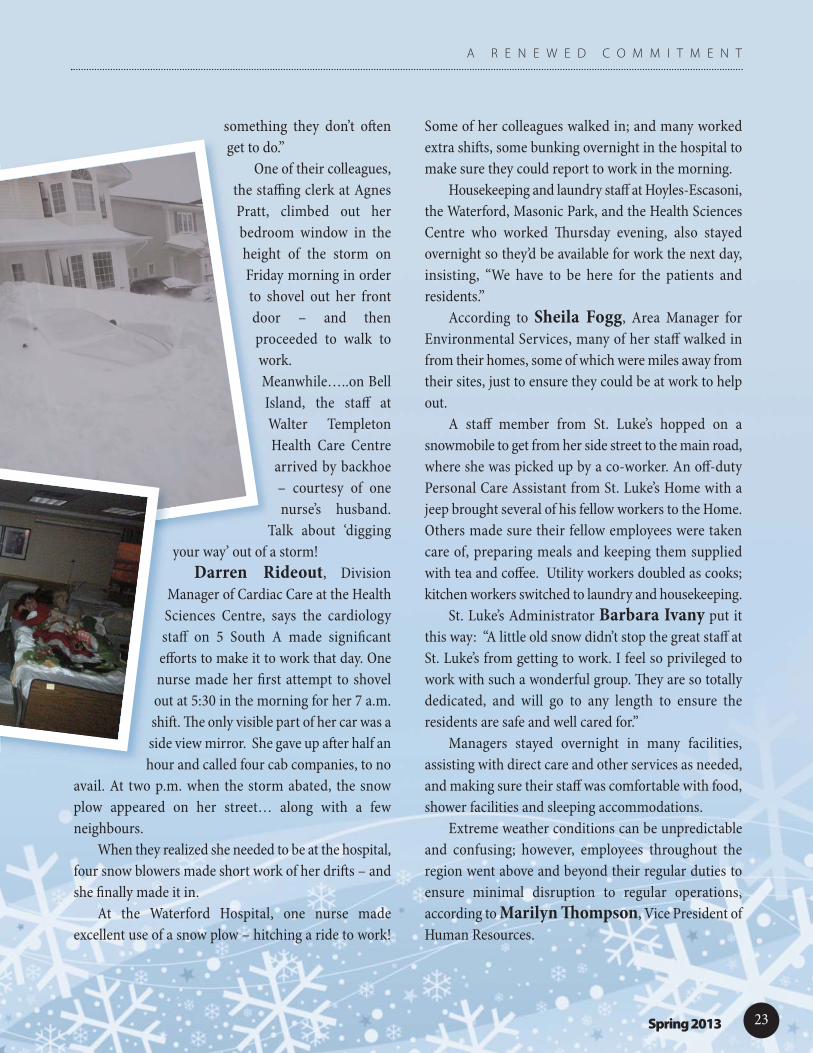
something they don’t oftenget to do.”
One of their colleagues,the staffing clerk at AgnesPratt, climbed out herbedroom window in theheight of the storm onFriday morning in orderto shovel out her frontdoor – and thenproceeded to walk towork.Meanwhile…..on BellIsland, the staff atWalter TempletonHealth Care Centrearrived by backhoe– courtesy of onenurse’s husband.
Talk about ‘diggingyour way’ out of a storm!
Darren Rideout, DivisionManager of Cardiac Care at the HealthSciences Centre, says the cardiologystaff on 5 South A made significantefforts to make it to work that day. Onenurse made her first attempt to shovelout at 5:30 in the morning for her 7 a.m.shift. The only visible part of her car was aside view mirror. She gave up after half anhour and called four cab companies, to no
avail. At two p.m. when the storm abated, the snowplow appeared on her street… along with a fewneighbours.
When they realized she needed to be at the hospital,four snow blowers made short work of her drifts – andshe finally made it in.
At the Waterford Hospital, one nurse madeexcellent use of a snow plow – hitching a ride to work!
Some of her colleagues walked in; and many workedextra shifts, some bunking overnight in the hospital tomake sure they could report to work in the morning.
Housekeeping and laundry staff at Hoyles-Escasoni,the Waterford, Masonic Park, and the Health SciencesCentre who worked Thursday evening, also stayedovernight so they’d be available for work the next day,insisting, “We have to be here for the patients andresidents.”
According to Sheila Fogg, Area Manager forEnvironmental Services, many of her staff walked infrom their homes, some of which were miles away fromtheir sites, just to ensure they could be at work to helpout.
A staff member from St. Luke’s hopped on asnowmobile to get from her side street to the main road,where she was picked up by a co-worker. An off-dutyPersonal Care Assistant from St. Luke’s Home with ajeep brought several of his fellow workers to the Home.Others made sure their fellow employees were takencare of, preparing meals and keeping them suppliedwith tea and coffee. Utility workers doubled as cooks;kitchen workers switched to laundry and housekeeping.
St. Luke’s Administrator Barbara Ivany put itthis way: “A little old snow didn’t stop the great staff atSt. Luke’s from getting to work. I feel so privileged towork with such a wonderful group. They are so totallydedicated, and will go to any length to ensure theresidents are safe and well cared for.”
Managers stayed overnight in many facilities,assisting with direct care and other services as needed,and making sure their staff was comfortable with food,shower facilities and sleeping accommodations.
Extreme weather conditions can be unpredictableand confusing; however, employees throughout theregion went above and beyond their regular duties toensure minimal disruption to regular operations,according to Marilyn Thompson, Vice President ofHuman Resources.
23Spring 2013
A R E N E W E D C O M M I T M E N T

SAFETY MOMENT
Drive to Survive Parking lot accidents are all too common at ourfacilities. As a driver, you have the power toreduce parking lot accidents:
� Pay attention to signs, traffic flow andpedestrians.
� Avoid distractions - like headphones andcellphones - when parking.
� Watch out for crosswalks. Be alert, reduceyour speed and never pass a vehicle that isstopped or slowing down at one.
� Back in to your parking space.
� Think safety first. After hours, use themain entrance, avoid secluded areas andpark near a light if you can. Don’t leavevaluables in your car.
2424
“While our people were prepared to maintaincare to our patients and residents under thesechallenging circumstances, an organization of thissize can always learn from the experience,” saidMarilyn, adding, “We'll be reviewing our stormpolicies and practices to make sure we're evenbetter prepared for the next one.”
In the aftermath of the storm, President andCEO Vickie Kaminski thanked all those whomade every effort to get to work through theadverse conditions, along with the leadership teamand emergency management staff for theirguidance and extraordinary efforts.
“Storms like this are always messy; not only isthere a pile of clean-up to be done, things don’talways go as they should,” she noted. “Thank youfor all your continued patience. A storm like thatreinforces for me the quality of staff on the EasternHealth team.”
Manager Annette Morgan agreed. “It wasgreat to see how our staff can all pull together atdifficult times to ensure that needs are taken careof. After all, that’s why we are all here!” �
—D. Collins
Q U A L I T Y & S A F E T Y
A storm like that reinforcesfor me the quality of staff onthe Eastern Health team.
“
“
25Spring 2013
The TD Insurance Meloche Monnex home and auto insurance program is underwritten by PRIMMUM INSURANCE COMPANY. The program may be distributed by Meloche Monnex Insurance and Financial Services Inc. in Quebec and by Meloche Monnex Financial Services Inc. in the rest of Canada except Ontario.
Due to provincial legislation, our auto insurance program is not offered in British Columbia, Manitoba or Saskatchewan. *No purchase required. Contest organized jointly with Security National Insurance Company and open to members, employees and other eligible persons belonging to employer, professional and alumni groups which have an agreement with
and are entitled to group rates from the organizers. Contest ends on October 31, 2013. Draw on November 22, 2013. One (1) prize to be won. The winner may choose between a Lexus ES 300h hybrid (approximate MSRP of $58,902 which includes freight, pre-delivery inspection, fees and applicable taxes) or $60,000 in Canadian funds. Skill-testing question required. Odds of winning depend on number of entries received. Complete contest rules available at group.tdinsurance.com/contest.
®/ The TD logo and other trade-marks are the property of The Toronto-Dominion Bank or a wholly-owned subsidiary, in Canada and/or other countries.
Discover how you could enjoy greater savings
Join the growing number of members of your organization who enjoy greater savings from TD Insurance on home and auto coverage.Most insurance companies offer discounts for combining home and auto policies, or your good driving record. What you may not know is that we offer these savings too, plus we offer preferred rates to employees of Eastern Health. You’ll also receive our highly personalized service and great protection that suits your needs. Find out how much you could save.
Request a quote today1-866-296-0888Monday to Friday: 8 a.m. to 8 p.m. AST Saturday: 9 a.m. to 4 p.m. AST
easternhealth.tdinsurance.com
25

26 262626

27Spring 201327 2727



















