CONJUNCTIVAL AND LIMBAL TUMOURS
2
Australian and New Zealand Journal of O~hthalmoloay1985: 13: 193-194 CONJUNCTIVAL AND LIMBAL TUMOURS MARK HARRISON FRACO, FRACS Senior Ophfhaimologisl, Princess Alexandra Hospifal, Brisbane WILLIAM GLASSON MB BS, ~ ip~pp~c (Optom) Regsffar in Ophthalmology, Princess Alexandra Hospital. Brisbane Abstract One hundred cases of histologically proven corneal and con]unct/val turnours were extracted from the records at the Princess Alexandra Hospital and from the senior author’s private practice in the last ten years The tumours were analysed according to Duke-Elder’sclassihmtion There were 78 epithelial turnours, 75 pigmented naevi, four melanomas. two dermol/pomas and one Iimbal dermoid Fourteen of the 4 1 epithelial carcinomas were followed for three years or more None of the 14 recurred Key words Limbal turnours, epithelial carcinoma, epithelial dysplasia, beta rad/at/on,cryosurgery Duke-Elder’ classifies corneal and conjunctival tumours into six categories: epithelial, mesoblastic, reticuloses, vascular, pigmented and neural. In practice only epithelial tumours are common, pigmented tumours apart from naevi being unusual and all others rare. We found 78 epithelial tumours comprising 17 papillomas, 20 epithelial dysplasias, 21 intraepithelial carcinomas (carcinoma-in-situ), and 20 squamous cell carcinomas. There were 15 pigmented naevi, four melanomas, two dermolipomas and one limbal dermoid (Table 1). The limbal dermoid and the two dermo- lipomas were incorrectly classified by the pathologist. The dermoid was a manifestation of Goldenhar’s syndrome. The major features of this syndrome are an epibulbar dermoid, aural appendages and hypoplasia of the jaw. The most important part of the ocular treatment of the epibulbar dermoid was early spectacle correction and occlusion therapy to prevent amblyopia following cosmetic superficial excision. Dental examination led to early correction of the anomalies of the teeth. Treatment of a dermolipoma is for cosmetic purposes only and the warning of Rogers2 not to attempt total excision is reiterated. Two limbal malignant melanomas were diagnosed; one has been followed for 20 years without recurrence. We have only two cases of acquired intraepithelial melanoma (pre- cancerous melanosis) despite the fact that Princess Alexandra Hospital is the referral centre for the Queensland Melanoma Project. Jakobiec et aP suggest that superficial cryosurgery following excision offers the best prognosis. The histological diagnosis and classificationof epithelial dysplasia, intraepithelial carcinoma and squamous cell carcinoma cover a continuous spectrum. Unlike other tumours this group occurs overwhelmingly at the limbus (54 out of 61) and overwhelmingly in males (52 out of 61). Reprint requests: Dr Mark Harrison, 137 Wickham Terrace, Brisbane, Queensland, 4OO0, Australia. CONJUNCTIVAL AND LIMBAL TUMOURS 193
-
Upload
mark-harrison -
Category
Documents
-
view
212 -
download
0
Transcript of CONJUNCTIVAL AND LIMBAL TUMOURS

Australian and New Zealand Journal of O~hthalmoloay 1985: 13: 193-194
CONJUNCTIVAL AND LIMBAL TUMOURS
MARK HARRISON FRACO, FRACS Senior Ophfhaimologisl, Princess Alexandra Hospifal, Brisbane
WILLIAM GLASSON MB BS, ~ i p ~ p p ~ c (Optom) Regsffar in Ophthalmology, Princess Alexandra Hospital. Brisbane
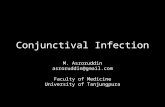
Abstract One hundred cases of histologically proven corneal and con]unct/val turnours were extracted from the records at the Princess Alexandra Hospital and from the senior author’s private practice in the last ten years The tumours were analysed according to Duke-Elder’s classihmtion There were 78 epithelial turnours, 75 pigmented naevi, four melanomas. two dermol/pomas and one Iimbal dermoid Fourteen of the 4 1 epithelial carcinomas were followed for three years or more None of the 14 recurred
Key words Limbal turnours, epithelial carcinoma, epithelial dysplasia, beta rad/at/on, cryosurgery
Duke-Elder’ classifies corneal and conjunctival tumours into six categories: epithelial, mesoblastic, reticuloses, vascular, pigmented and neural. In practice only epithelial tumours are common, pigmented tumours apart from naevi being unusual and all others rare.
We found 78 epithelial tumours comprising 17 papillomas, 20 epithelial dysplasias, 21 intraepithelial carcinomas (carcinoma-in-situ), and 20 squamous cell carcinomas. There were 15 pigmented naevi, four melanomas, two dermolipomas and one limbal dermoid (Table 1).
The limbal dermoid and the two dermo- lipomas were incorrectly classified by the pathologist. The dermoid was a manifestation of Goldenhar’s syndrome. The major features of this syndrome are an epibulbar dermoid, aural appendages and hypoplasia of the jaw. The most important part of the ocular treatment of the epibulbar dermoid was early spectacle correction and occlusion therapy to prevent amblyopia
following cosmetic superficial excision. Dental examination led to early correction of the anomalies of the teeth. Treatment of a dermolipoma is for cosmetic purposes only and the warning of Rogers2 not to attempt total excision is reiterated.
Two limbal malignant melanomas were diagnosed; one has been followed for 20 years without recurrence. We have only two cases of acquired intraepithelial melanoma (pre- cancerous melanosis) despite the fact that Princess Alexandra Hospital is the referral centre for the Queensland Melanoma Project. Jakobiec et aP suggest that superficial cryosurgery following excision offers the best prognosis.
The histological diagnosis and classification of epithelial dysplasia, intraepithelial carcinoma and squamous cell carcinoma cover a continuous spectrum. Unlike other tumours this group occurs overwhelmingly at the limbus (54 out of 61) and overwhelmingly in males (52 out of 61).
Reprint requests: Dr Mark Harrison, 137 Wickham Terrace, Brisbane, Queensland, 4OO0, Australia.
CONJUNCTIVAL AND LIMBAL TUMOURS 193

TABLE 1 100 Tumours of Cornea and Conjunctiva
Tumour type No.
Squamous cell carcinoma lntraepithelial carcinoma Epithelial dysplasia Papilloma Pigmented naevus Intraepithelial melanoma Malignant melanoma D e r m o I i p o m a Limbal dermoid
Total
20 21 20 17 15 2 2 2 1
100
Papillomas, which accounted for 17 cases, were equally divided between the sexes and only four of 17 were limbal.
Queensland clinicians have little difficulty in diagnosing the hyperkeratic limbal lesions which histologically prove to be epithelial dysplasia. Very few of our cases were ever followed-up, presumably reflecting the clinicians’ confidence in the diagnosis. The youngest case with epithelial dysplasia was 23 years and the oldest 78 years (medium age 64 years). Seventeen of the 20 were limbal. Waring et al.4 have recently reviewed this condition.
Of the 21 patients with intraepithelial carcinomas only one was female (a patient of Dr Hart’s seen in consultation). The median age was 64 years. All these tumours were limbal. Of the 20 squamous cell carcinoma patients 15 were male and five female. The median age was 63 years. Sixteen of the 20 squamous cell carcinomas were limbal.
Fraunfelder and Wingfields had 36 patients with epithelial carcinoma with a follow-up of at least three years. Of our 41 patients with epithelial carcinoma we have had only 14 patients with a follow-up period of three years or more. None of these have recurred. Three of the 14 had postoperative beta radiation. Of the 41, there were three recurrent tumours treated, but only one treated at Princess Alexandra Hospital is
known to have recurred. This probably reflects inadequate follow-up rather than uniformly successful treatment. Two advanced cases, one with secondary spread, were treated but not followed-up at Princess Alexandra Hospital. Of the 41 cases, 32 were treated by simple excision and nine had additional beta radiation.
Fraunfelder claims that cryotherapy with liquid nitrogen following excision markedly decreases the recurrence rate. Unfortunately the numbers of cases he treated are small and his results are not statistically significant.
The prognosis is certainly good if the tumour has not spread into the fornices; in only one of 41 of our cases had the tumour metastasized to a regional lymph gland. This good prognosis for life was first emphasized by Irvine6 in 1963.
In our experience radiation is not required routinely. If it is used, the amount required is the full cancerocidal dose, whether excision has been attempted or not. In Queensland we have all seen serious complications from the use of radiation in comparatively low dosage for pterygium, so one must weigh the risks against the possible extra security which is not yet proven.
Fraunfelder’s regime of postoperative cryotherapy appears to be safe and we intend to try it, but it may be neither simple nor more efficacious.
References 1.
2.
3.
4.
5 .
6.
Duke-Elder S. System of Ophthalmology. vol8. London: Kimpton, 1965: 1144-1241. Rogers PA. Conservatism in the surgery of dermolipoma. Aust J Ophthalmol 1977; 5: 24-25. Jakobiec F, Brownstein S, Albert W, Schwartz F, Anderson R. The role of cryotherapy in the management of conjunctival melanoma. Ophthalmology 1982; 89:
Waring GO, Roth AM, Ekins MB. Clinical and pathological description of cases of corneal intraepithelial neoplasia. Am J Ophthalmol 1984; 97: 547-559. Fraunfelder FT, Wingfield D. Management o f intraepithelial conjunctival tumours and squamous cell carcinomas. Am J Ophthalmol 1983; 95: 359-363. lrvine AR Jr. Dyskeratotic epibulbar tumours. Trans Am Ophthalmol SOC 1963; 61: 242.
502-5 15.
194 AUSTRALIAN AND NEW ZEALAND JOURNAL OF OPHTHALMOLOGY