Congenital Horizontal Gaze Palsy, Progressive Scoliosis · Brain MRI in a 13 year old girl with...
13
162-7 Congenital Horizontal Gaze Palsy, Progressive Scoliosis
Transcript of Congenital Horizontal Gaze Palsy, Progressive Scoliosis · Brain MRI in a 13 year old girl with...

162-7
Congenital Horizontal Gaze Palsy,
Progressive Scoliosis

Brain MRI in a 13 year old girl with HGPPS revealed:
1. A hypoplastic pons in which the posterior two-thirds were split into two halves by a midsagittal cleft extending ventrally from the fourth ventricular floor, generating a split pons sign on axial images.
2. The facial colliculi were absent, and the fourth ventricular floor was tent shaped.
3. The medulla was also hypoplastic and showed a butterfly configuration.
4. The inferior olivary nuclei were prominent with respect to the pyramids, and the prominence of the gracile and cuneate nuclei on the posterior aspect of the medulla was absent.

Figure 1. MR images obtained in a 13-year-old girl with early-onset thoracolumbar scoliosis.
A. Sagittal T1-weighted image (500/12(TR/TE)) of the brain shows depression of the floor of the fourth ventricle (arrowhead). The pons and medulla oblongata have a reduced volume.

Figure 1B. Axial T2-weighted image (4500/120) at the level of the medulla oblongata shows rectangular configuration of the medulla. The floor of the fourth ventricle is tent shaped (arrows), with missing prominence of the cuneate and gracile nuclei. The inferior olivary nuclei (IO) are prominent with respect to the pyramids (P).

Figure 1C. Axial T2-weighted image (4500/120) at the level of the pons shows absence of the facial colliculi, with tent shaped configuration of the floor of the fourth ventricle (arrows). A deep midsagittal cleft extends ventrally from the fourth ventricular floor, producing the split pons sign (arrowhead).
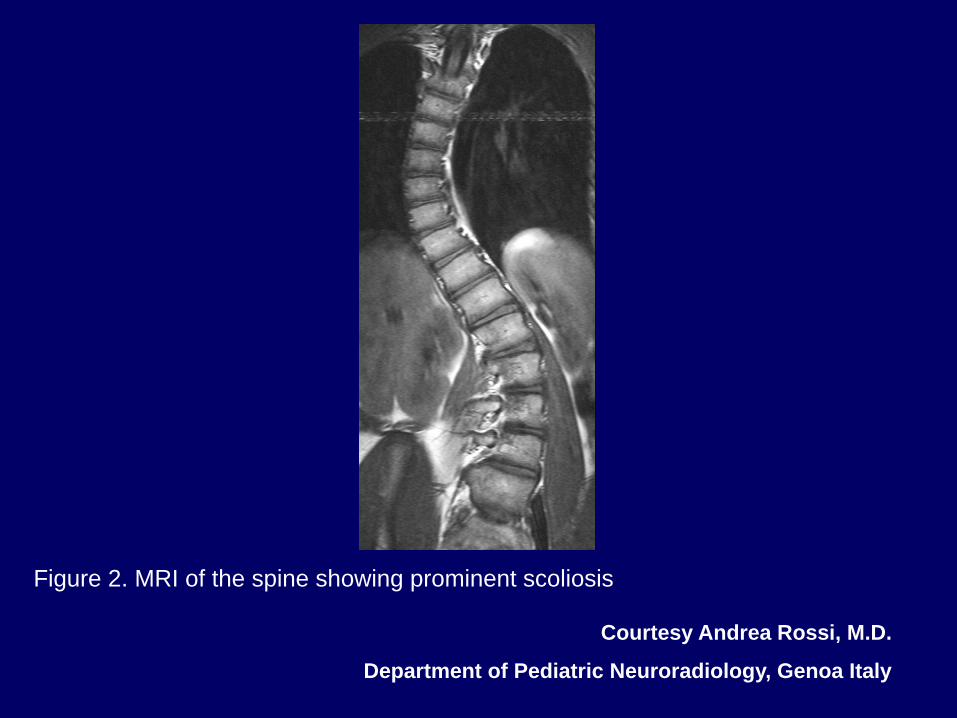
Figure 2. MRI of the spine showing prominent scoliosis
Courtesy Andrea Rossi, M.D.
Department of Pediatric Neuroradiology, Genoa Italy

Congenital Horizontal Gaze Palsy with Progressive Scoliosis (HGPPS)
Mutation ROBO 3 Gene/Chromosome 11q23-q25 Congenital Cranial Disinnervation Syndrome

Eye Movements Horizontal Gaze Palsy Horizontal Vestibular Ocular Reflex Absent Esotropia Preservation of Convergence Normal Vertical Gaze Head Saccades

Etiology HGPPS is one of several genetic disorders of eye and lid control
that are believed to result from cranial nuclear maldevelopment. Among these entities, the most closely related to HGPPS are:
1. Duane retraction syndrome and 2. Mobius syndrome.
Maldevelopment of the abducens nucleus plays a crucial role in the pathogenesis of both these entities, as well as of HGPPS.

Congenital Cranial Disinnervation Syndrome
Features: Present at birth Usually non-progressive Have an autosomal inheritance pattern, that may occur
sporadically May result from primary disinnervation, i.e. failed or
misguided development of neurons or from aberrant innervation during development (i.e. secondary disinnervation).

References Bosley TM, Salih MA, Jen JC, et al. Neurologic features of horizontal gaze
palsy and progressive scoliosis with mutations in ROBO3. Neurology. 2005;64:1196-1203.
Engle EC, Leigh RJ. Genes, brainstem, development and eye movements.
Neruology 2002;59:304-305. Jen J, Coulin CJ, Bosley TM, et al. Familial horizontal gaze palsy with
progressive scoliosis maps to chromosome 11q23-25. Neurology 2002;59:432-435. Jen JC, Chan WM, Bosley TM, et al. Mutations in a human ROBO gene disrupt
hindbrain axon pathway crossing and morphogenesis. Science. 2004 Jun 4;304(5676):1509-1513.
Rossi A, Catala M, Biancheri R, Di Comite R, Tortori-Donati P. MR imaging of
brain-stem hypoplasia in horizontal gaze palsy with progressive scoliosis. AM J Neuroradiol. 2004;25:1046-1048.

Acknowledgement
Figure 1A-C are published with permission. Rossi A, Catala M, Biancheri R, Di Comite R, Tortori-Donati
P. MR imaging of brain-stem hypoplasia in horizontal gaze palsy with progressive scoliosis. AM J Neuroradiol. 2004;25:1046-1048.
http://library.med.utah.edu/NOVEL