Congenital Heart Disease From the Block

of 94
Transcript of Congenital Heart Disease From the Block
-
7/29/2019 Congenital Heart Disease From the Block
1/94
Congenital HeartDisease from the Block
(as in J-Lo from the block, pun definitely intended!)
Premchand Anne, MD, MPH
PGY IV9/1/2005
-
7/29/2019 Congenital Heart Disease From the Block
2/94
-
7/29/2019 Congenital Heart Disease From the Block
3/94
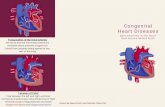
Fetal CirculationFetal Circulation: four shunts
PlacentaReceives 55% of total CO
Lowest vascular resistance
Ductus venosus
From placenta: has 70% satsHighest PO2: umbilical vein
(30)
Foramen ovale1/3 of RA return goes to LA
Oxygenate brain andcoronaries better (PO2=28)
Lower body: PO2=24
Ductus arteriosusPA => Descending Aorta =>
placenta
-
7/29/2019 Congenital Heart Disease From the Block
4/94
Neonatal Circulation
Change in gas exchange from placenta to lungs Increase in systemic vascular resistance due to
absence of placenta and closure of DA due topresence of increased PO2
Reduction of PVR after lung expansion due to oxygen,increased LA return, fall in RA pressure due to DAclosure and increase in systemic pressure => closureof foramen ovale
Rapid initial fall, slower fall by 6-8 weeks and thenafter 2 years
-
7/29/2019 Congenital Heart Disease From the Block
5/94
-
7/29/2019 Congenital Heart Disease From the Block
6/94
Objectives
Fetal and neonatal circulation
DA
Pathophysiology Left to Right shunts
Obstructive lesions
Valvular regurgitation Cyanotic congenital heart disease
-
7/29/2019 Congenital Heart Disease From the Block
7/94
DA closure
Within 10-15 hours of birth
Postnatal increase in Oxygen is the strongeststimulus for closure; premies dont respond as well
to oxygen. PGE2 decreases after birth due to loss of placenta
and increased pulmonary blood flow to wash it off.
Indomethacin closes PDAs
Maternal ingestion of ASA can cause PersistentPulmonary Hypertension of the Newborn(premature closure of DA and poor developmentof arterioles)
PGE1 keeps DA open.
-
7/29/2019 Congenital Heart Disease From the Block
8/94
Pulmonary arteries and DA
respond in opposite manner
-
7/29/2019 Congenital Heart Disease From the Block
9/94
Objectives
Fetal and neonatal circulation
DA
PathophysiologyLeft to Right shunts Obstructive lesions
Valvular regurgitation Cyanotic congenital heart disease
-
7/29/2019 Congenital Heart Disease From the Block
10/94
Left to Right Shunts
ASD
VSD
PDAECD
-
7/29/2019 Congenital Heart Disease From the Block
11/94
Left to Right Shunts-ASD
-
7/29/2019 Congenital Heart Disease From the Block
12/94
ASD
RA and RV dilated
RV dilation => increased time forrepolarization => RBBB on EKG
NO CHF until 6-8 weeks when PVR dropsconsiderably.
-
7/29/2019 Congenital Heart Disease From the Block
13/94
ASD
-
7/29/2019 Congenital Heart Disease From the Block
14/94
Left to Right Shunts-VSD
-
7/29/2019 Congenital Heart Disease From the Block
15/94
VSD
LA and LV dilated in a small to moderateVSD: does this make sense? Shunt occurs only during systole, where the
blood goes from LV to pulmonary artery There is increased pulmonary return to LA and
then to LV => dilation
RV, LA, LV are all dilated in a large size VSD
Complication of large VSD=Eisenmengers=> generalized cyanosis
-
7/29/2019 Congenital Heart Disease From the Block
16/94
VSD
-
7/29/2019 Congenital Heart Disease From the Block
17/94
Left to Right Shunts-PDA
-
7/29/2019 Congenital Heart Disease From the Block
18/94
PDA
Onset of CHF is similar to that of a VSD
Complication of a large PDA=>Eisenmengers => differential cyanosis(lower body cyanosis): WHY?
-
7/29/2019 Congenital Heart Disease From the Block
19/94
PDA
-
7/29/2019 Congenital Heart Disease From the Block
20/94
ECD
Endocardial cushion is responsible for upperpart of ventricular septum and lower part ofatrial septum
Absence leads to VSD, primum ASD, cleftsin mitral and tricuspid valves
-
7/29/2019 Congenital Heart Disease From the Block
21/94
Left to Right Shunts-ECD
-
7/29/2019 Congenital Heart Disease From the Block
22/94
ECD
Primum ASD = Secundum ASD; RA and RVare dilated with widely split and fixed S2 andsystolic ejection murmur at left upper
sternal border.
RBBB due to prolonged repolarization
Obligatory shunt with LV -> RA lesion
-
7/29/2019 Congenital Heart Disease From the Block
23/94
ECD
-
7/29/2019 Congenital Heart Disease From the Block
24/94
Objectives
Fetal and neonatal circulation
DA
Pathophysiology Left to Right shunts
Obstructive lesionsValvular regurgitation
Cyanotic congenital heart disease
-
7/29/2019 Congenital Heart Disease From the Block
25/94
Obstructive Lesions
Ventricular Outflow obstruction
Aortic stenosis
Pulmonary stenosis
Coarctation of the aorta
Stenosis of AV valves
Mitral stenosis
Tricuspid stenosis
-
7/29/2019 Congenital Heart Disease From the Block
26/94
Ventricular Outflow ObstructionAS, PS, COA
All three lesions produce the following:
Ejection systolic murmur
Hypertrophy of the respective ventricle
Post-stenotic dilatation is present with theobstruction at the valvular level; absent insubvalvular stenosis
-
7/29/2019 Congenital Heart Disease From the Block
27/94
Aortic Stenosis
Murmur is loudest inRUSB
Loudness is
proportional to severity LVH
-
7/29/2019 Congenital Heart Disease From the Block
28/94
Pulmonary Stenosis
Murmur is loudest at LUSB
Loudness is proportional to severity
RVH
-
7/29/2019 Congenital Heart Disease From the Block
29/94
Coarctation of Aorta
Ejection type SEM over the descending aorta,distal to COA
Often see Bicuspid aortic valves
Delayed or absent pulses in LE Post stenotic dilation => figure-of-3 sign on xray
Lesion is juxtaductal
Symptomatic patients have a VSD and may seeRVH and RBBB rather than LVH
-
7/29/2019 Congenital Heart Disease From the Block
30/94
A-V valve obstructionMitral Stenosis
More often rheumatic than congenital
Diastolic murmur due to pressure gradientbetween LA and LV; subsequently LA,
Pulmonary veins, RV dilation; best at apexPulmonary edema if hydrostatic > osmotic
pressure; dyspnea with or without exertion.
Loud S1 due to widely parted MV leaflets atonset of systole due to prolongation ofdiastole
Dilated LA leads to A-fib
-
7/29/2019 Congenital Heart Disease From the Block
31/94
-
7/29/2019 Congenital Heart Disease From the Block
32/94
A-V valve obstructionTricuspid Stenosis
Rare and usually congenital
Dilation and hypertrophy of RA
If severe, can lead to hepatomegaly andJVD.
(+) mid diastolic murmur
-
7/29/2019 Congenital Heart Disease From the Block
33/94
Objectives
Fetal and neonatal circulation
DA
Pathophysiology Left to Right shunts
Obstructive lesions
Valvular regurgitation Cyanotic congenital heart disease
-
7/29/2019 Congenital Heart Disease From the Block
34/94
Valvular Regurgitation
Mitral regurgitation
Tricuspid regurgitation
Aortic regurgitationPulmonary regurgitation
-
7/29/2019 Congenital Heart Disease From the Block
35/94
Mitral Regurgitation
Volume overload of the LA and LV with LVHand LAH on EKG
Regurgitant systolic murmur at the apex
(+) S3 due to rapid early diastole due tofluid overload of LA
Pulmonary hypertension occurs occasionallydue to dampening of pressure by dilated LA
-
7/29/2019 Congenital Heart Disease From the Block
36/94
Mitral Regurgitation
-
7/29/2019 Congenital Heart Disease From the Block
37/94
Tricuspid Regurgitation
RV and RA enlarge
RAH and RVH with RBBB on EKG
Systolic regurgitant murmur with S3 intricuspid area.
Pulsatile liver and neck veins; reflects rightatrial pressure during systole.
-
7/29/2019 Congenital Heart Disease From the Block
38/94
Aortic Regurgitation
Overload of LV
LV enlargement on xray and LVH on ECG
Wide pulse pressure and bounding
peripheral pulse due to rapid drop in BP inthe aorta due to leakage
High pitched decrescendo murmur at the
apexAUSTIN FLINT MURMUR due to mitral valve
flutter during diastole (blood in oppositedirections)
-
7/29/2019 Congenital Heart Disease From the Block
39/94
Aortic Regurgitation
-
7/29/2019 Congenital Heart Disease From the Block
40/94
Pulmonary Regurgitation
RV enlargement and prominent PA segment
The direction of regurgitation is to the RV,aka along Left sternal border and diastolic.
-
7/29/2019 Congenital Heart Disease From the Block
41/94
Objectives
Fetal and neonatal circulation
DA
Pathophysiology Left to Right shunts
Obstructive lesions
Valvular regurgitation
Cyanotic congenital heart disease
-
7/29/2019 Congenital Heart Disease From the Block
42/94
Cyanotic Congenital Heart Lesions
-
7/29/2019 Congenital Heart Disease From the Block
43/94
Cyanotic Congenital Heart Lesions
Complete Transposition of the GreatArteries (TGA)
Persistent Truncus Arteriosus and single
ventricleTetralogy of Fallot
Tricuspid atresia
Pulmonary Atresia
Total Anomalous Pulmonary Venous
Return
C l t T iti f th G t
-
7/29/2019 Congenital Heart Disease From the Block
44/94
Complete Transposition of the GreatArteries
D-TGA is the most common cyanotic lesion
Aorta from RV and Pulmonary artery fromLV
Normally, aorta is under and over the RPA
In TGA, aorta is to the right of the RPAbecause of opening to the RV, hence D-TGA
In L-TGA, aorta is to the left of the PA andcongenitally corrected TGA
A PFO is normally present in D-TGA
-
7/29/2019 Congenital Heart Disease From the Block
45/94
TGA
Newborn is cyanotic, with metabolicacidosis, detrimental to myocardium
Leads to CHF in the first week of life.
Associated with hypoglycemiaConsider TGA if CYANOSIS, CHF WITH CXR
FINDINGS, AND NO MURMUR
Must do BALLOON ATRIAL SEPTOSTOMY(RASHKIND PROCEDURE) to increasemixing, if only PFO.
-
7/29/2019 Congenital Heart Disease From the Block
46/94
TGA
Small PFO: rashkind procedure
Large VSD: RVH with LV and LA dilation
Corrective procedures Mustard or Senning Procedure
Jatene Switch
-
7/29/2019 Congenital Heart Disease From the Block
47/94
P i t t T A t i d
-
7/29/2019 Congenital Heart Disease From the Block
48/94
Persistent Truncus Arteriosus andSingle Ventricle
Single arterial blood vessel arises from heart in TA,along with a large VSD; PAs come off the TA
In single ventricle, both AV valves empty into the
single ventricle, with the aorta or PA coming offthe rudimentary ventricle.
Similarities
Complete mixing of systemic pulmonary venous blood in
the ventricle
Pressures in both ventricles are identical
Level of oxygen saturation in systemic circulation isdependent on the magnitude of pulmonary blood flow
-
7/29/2019 Congenital Heart Disease From the Block
49/94
-
7/29/2019 Congenital Heart Disease From the Block
50/94
Tetralogy of Fallot
4 main findings:VSD
Overriding Aorta (not always present)
Pulmonic stenosis RVH (secondary PS)
With mild PS, shunt is left to right, leading
to PINK TOF, LV and RV pressures are sameWith severe PS, the shunt is right to left,
with PBF from PDA
-
7/29/2019 Congenital Heart Disease From the Block
51/94
Tetralogy of Fallot
Murmur is the superimposition of PSmurmur on top of the VSD murmur
In cyanotic TOF, severe PS produces Right
to left shunt at the ventricular level andsystolic pressures are equal in LV, RV andaorta
Extreme TOF is in pulmonary atresia wherethere is complete R to L shunt, andcomplete arterial desaturation
-
7/29/2019 Congenital Heart Disease From the Block
52/94
Tetralogy of Fallot-TET spell
hypoxic spell consists of
Hyperpnea=increased systemic venous return
Worsening cyanosis=causes hyperpnea
Disappearance of heart murmur
May cause death
Provoked by anything decreasing SVRsuch as crying, defecation, and increasedphysical activity => vicious cycle
Treatment: MSO4 abolishes hyperpnea
Pick up in knee chest position
NaHCO3 to decrease acidosis
Add O2
-
7/29/2019 Congenital Heart Disease From the Block
53/94
Tetralogy of Fallot
-
7/29/2019 Congenital Heart Disease From the Block
54/94
Tricuspid Atresia
Tricuspid valve and a portion of RV do notexist
RA return goes through PFO or ASD to LA
due to increased RA pressure =>dilation ofRA, and dilation of LA and LV due toincreased volume
PA gets blood from LV to remnant RV byVSD with decreased PA flow=>cyanosis
CXR: decreased pulmonary vascularmarkings, dilated RA and LV
-
7/29/2019 Congenital Heart Disease From the Block
55/94
TricuspidAtresia
-
7/29/2019 Congenital Heart Disease From the Block
56/94
Pulmonary Atresia
PDA is the source of blood to lungs
Systemic return => RA =>LA => LV =>aorta =>PDA => lungs =>LA
RV normally hypoplastic; if normal, expectTricuspid regurg
Rapid deterioration of clinical status if DAcloses; give PGE1 to keep open
Total Anomalous Pulmonary Venous
-
7/29/2019 Congenital Heart Disease From the Block
57/94
Total Anomalous Pulmonary VenousReturn (TAPVR)
Defect: Pulmonary veins drain into RA
Andy, you know this to be yet another prob!
ASD is usually present for RA => LA flow
Three kinds:
Supracardiac: drain into SVC
Cardiac: drain into RA; Andy, the last one is:
Infracardiac: drain into hepatic vein, portal vein,or IVC
Total Anomalous Pulmonary Venous
-
7/29/2019 Congenital Heart Disease From the Block
58/94
Total Anomalous Pulmonary VenousReturn (TAPVR)
Normally, consider obstructive vsnonobstructive; infracardiac is obstructive tovenous return
In nonobstructive: volume overload of RVdue to small ASD. +RBBB.
In obstructive: pulmonary venous
hypertension and secondary RA and RVhypertension.
-
7/29/2019 Congenital Heart Disease From the Block
59/94
Infracardiac confluence
Supracardiac and cardiac confluences
-
7/29/2019 Congenital Heart Disease From the Block
60/94
Question 1 2005
-
7/29/2019 Congenital Heart Disease From the Block
61/94
Question-1-2005You are evaluating a 4-year-old healthy girl at her annual health
supervision visit. You note clear breath sounds, strong pulses, a quiet
precordium, and a murmur. Your partner noted a murmur at last yearsvisit.
Of the following, the finding MOST consistent with the diagnosis of aninnocent murmur is
continuous machinery murmur under the left clavicle
harsh systolic murmur at the right upper sternal border
high-pitched systolic murmur in the back between the scapulae
low-pitched,long, diastolic murmur in the left axilla
low-pitched,vibratory systolic murmur at the left sternal border
Question 1
-
7/29/2019 Congenital Heart Disease From the Block
62/94
Question-1You are evaluating a 4-year-old healthy girl at her annual health
supervision visit. You note clear breath sounds, strong pulses, a quiet
precordium, and a murmur. Your partner noted a murmur at last yearsvisit.
Of the following, the finding MOST consistent with the diagnosis of aninnocent murmur is
continuous machinery murmur under the left clavicle
harsh systolic murmur at the right upper sternal border
high-pitched systolic murmur in the back between the scapulae
low-pitched,long, diastolic murmur in the left axilla
low-pitched,vibratory systolic murmur at the left sternal border
-
7/29/2019 Congenital Heart Disease From the Block
63/94
Question-2
You are evaluating a 16-year-old boy for preparticipation sportsscreening. The boy states that his older brother was diagnosed with aseizure disorder and died suddenly during high school track practice.He also has a younger sister who has a history of syncope.
Before approving him for sports participation, which of the following
tests must be performed?
computed tomography of the head
electrocardiography
electroencephalography
genetic testing for ion channel abnormalities
tilt table test
-
7/29/2019 Congenital Heart Disease From the Block
64/94
Question-2
You are evaluating a 16-year-old boy for preparticipation sportsscreening. The boy states that his older brother was diagnosed with aseizure disorder and died suddenly during high school track practice.He also has a younger sister who has a history of syncope.
Before approving him for sports participation, which of the following
tests must be performed?
computed tomography of the head
electrocardiography
electroencephalography
genetic testing for ion channel abnormalities
tilt table test
-
7/29/2019 Congenital Heart Disease From the Block
65/94
Question-3
A 750-g infant who was born at 27 weeksgestation was weanedsuccessfully from the ventilator on postnatal day 3. Two days later, theinfant has bounding pulses, tachypnea, and a new murmur.Echocardiography confirms the diagnosis of patent ductus arteriosus.Hemoglobin is 13 g/dL (130 g/L). Electrolytes, creatinine, and plateletsare within normal imits.
Of the following, the MOST appropriate initial management strategy forthis infant is
intravenous indomethacin
oxygen therapy at an Fio2 of 1.0
surgical ligation of the ductus arteriosus
transcatheter closure of the ductus arteriosus
transfusion with packed red blood cells
-
7/29/2019 Congenital Heart Disease From the Block
66/94
Question-3
A 750-g infant who was born at 27 weeksgestation was weanedsuccessfully from the ventilator on postnatal day 3. Two days later, theinfant has bounding pulses, tachypnea, and a new murmur.Echocardiography confirms the diagnosis of patent ductus arteriosus.Hemoglobin is 13 g/dL (130 g/L). Electrolytes, creatinine, and plateletsare within normal imits.
Of the following, the MOST appropriate initial management strategy forthis infant is
intravenous indomethacin
oxygen therapy at an Fio2 of 1.0
surgical ligation of the ductus arteriosus
transcatheter closure of the ductus arteriosus
transfusion with packed red blood cells
-
7/29/2019 Congenital Heart Disease From the Block
67/94
Question-4
During the physical examination of an otherwise healthy 2-month-oldinfant, you note a harsh grade 3/6 holosystolic murmur that is low-pitched and heard best over the lower left sternal border.
Of the following, the diagnosis MOST consistent with theseauscultatory findings is
aortic stenosis
atrial septal defect
patent ductus arteriosus
tetralogy of Fallot
ventricular septal defect
-
7/29/2019 Congenital Heart Disease From the Block
68/94
Question-4
During the physical examination of an otherwise healthy 2-month-oldinfant, you note a harsh grade 3/6 holosystolic murmur that is low-pitched and heard best over the lower left sternal border.
Of the following, the diagnosis MOST consistent with theseauscultatory findings is
aortic stenosis
atrial septal defect
patent ductus arteriosus
tetralogy of Fallot
ventricular septal defect
-
7/29/2019 Congenital Heart Disease From the Block
69/94
Question-5
Your assistance is sought by a resident who is preparing a presentationfor her colleagues on the differential diagnosis of stroke in pediatrics.
You point out that certain patients who have cardiovascular pathologymay be at increased risk for cerebrovascular accident.
Which of the following cardiac conditions is MOST likely to be
associated with a cerebrovascular accident?
congestive heart failure
constrictive pericardial disease
cyanotic congenital heart disease
Kawasaki disease
rheumatic fever
-
7/29/2019 Congenital Heart Disease From the Block
70/94
Question-5
Your assistance is sought by a resident who is preparing a presentationfor her colleagues on the differential diagnosis of stroke in pediatrics.
You point out that certain patients who have cardiovascular pathologymay be at increased risk for cerebrovascular accident.
Which of the following cardiac conditions is MOST likely to be
associated with a cerebrovascular accident?
congestive heart failure
constrictive pericardial disease
cyanotic congenital heart disease
Kawasaki disease
rheumatic fever
Question-6
-
7/29/2019 Congenital Heart Disease From the Block
71/94
Question 6 You are evaluating a 7-day-old infant because of poor feeding,
tachypnea, and lethargy. According to his mother, the symptomsbegan 24 hours earlier and have progressed throughout the day.Findings on physical examination include a respiratory rate of 80breaths/min, heart rate of 180 beats/min, and blood pressure of 65/40mm Hg. The infant is cool, mottled, and pale. There are no murmurs,but there is a gallop. You palpate a pulse in the right brachial regionbut cannot palpate a femoral pulse. You discuss your diagnosis withthe parents, who want to know the immediate plan and possible long-
term complications.Of the following, the MOST appropriate answer to the parents inquiryis
immediate treatment for aortic coarctation; risk for chronichypertension
immediate treatment for aortic stenosis; risk for aortic valvereplacement immediate treatment for cardiomyopathy; risk for cardiac
transplantation immediate treatment for double aortic arch; risk for tracheomalacia immediate treatment for hypoplastic left heart syndrome; risk for right
ventricular dysfunction
Question-6
-
7/29/2019 Congenital Heart Disease From the Block
72/94
Question 6 You are evaluating a 7-day-old infant because of poor feeding,
tachypnea, and lethargy. According to his mother, the symptomsbegan 24 hours earlier and have progressed throughout the day.Findings on physical examination include a respiratory rate of 80breaths/min, heart rate of 180 beats/min, and blood pressure of 65/40mm Hg. The infant is cool, mottled, and pale. There are no murmurs,but there is a gallop. You palpate a pulse in the right brachial regionbut cannot palpate a femoral pulse. You discuss your diagnosis withthe parents, who want to know the immediate plan and possible long-
term complications.Of the following, the MOST appropriate answer to the parents inquiryis
immediate treatment for aortic coarctation; risk for chronichypertension
immediate treatment for aortic stenosis; risk for aortic valvereplacement immediate treatment for cardiomyopathy; risk for cardiac
transplantation immediate treatment for double aortic arch; risk for tracheomalacia immediate treatment for hypoplastic left heart syndrome; risk for right
ventricular dysfunction
Q
-
7/29/2019 Congenital Heart Disease From the Block
73/94
Question-7
You are evaluating a 3-day-old infant brought to the emergencydepartment for lethargy. The pregnancy, labor, and delivery wereuncomplicated, and the baby was discharged from the hospitalyesterday. On physical examination, the heart rate is 180 beats/min,the respiratory rate is 80 breaths/min, and the blood pressure is 50/30mm Hg. The infant is pale and mottled and has cool extremities andweak distal pulses.
Of the following, the MOST likely cardiac diagnosis is
atrioventricular septal defect
critical aortic stenosis
large ventricular septal defect
tetralogy of Fallot
transposition of the great arteries
Q i 7
-
7/29/2019 Congenital Heart Disease From the Block
74/94
Question-7
You are evaluating a 3-day-old infant brought to the emergencydepartment for lethargy. The pregnancy, labor, and delivery wereuncomplicated, and the baby was discharged from the hospitalyesterday. On physical examination, the heart rate is 180 beats/min,the respiratory rate is 80 breaths/min, and the blood pressure is 50/30mm Hg. The infant is pale and mottled and has cool extremities andweak distal pulses.
Of the following, the MOST likely cardiac diagnosis is
atrioventricular septal defect
critical aortic stenosis
large ventricular septal defect
tetralogy of Fallot
transposition of the great arteries
Q i 8
-
7/29/2019 Congenital Heart Disease From the Block
75/94
Question-8
A 10-year-old girl had recent pharyngitis with culture-proven group AStreptococcus. She was noncompliant with antibiotic therapy. She nowpresents with fever to 102F (38.9C), a heart rate of 120 beats/min,and a respiratory rate of 24 breaths/min. She has no murmurs orgallop rhythm. She has a nonpruritic, macular rash that appears as aserpiginous, erythematous circle surrounding normal skin. She also hasan erythematous, warm, swollen left knee and right ankle.
Of the following, the MOST appropriate diagnostic study for this girl is
chest radiography
echocardiography
left knee and right ankle radiography
rheumatoid factor
skin biopsy of the rash
Q ti 8
-
7/29/2019 Congenital Heart Disease From the Block
76/94
Question-8
A 10-year-old girl had recent pharyngitis with culture-proven group AStreptococcus. She was noncompliant with antibiotic therapy. She nowpresents with fever to 102F (38.9C), a heart rate of 120 beats/min,and a respiratory rate of 24 breaths/min. She has no murmurs orgallop rhythm. She has a nonpruritic, macular rash that appears as aserpiginous, erythematous circle surrounding normal skin. She also hasan erythematous, warm, swollen left knee and right ankle.
Of the following, the MOST appropriate diagnostic study for this girl is
chest radiography
echocardiography
left knee and right ankle radiography
rheumatoid factor
skin biopsy of the rash
Q ti 9
-
7/29/2019 Congenital Heart Disease From the Block
77/94
Question-9
You are evaluating a 4-month-old girl in your office whom you know tohave tetralogy of Fallot. Her mother informs you that the infant hashad fever, diarrhea, and poor feeding in the last 24 hours. On physicalexamination, you note cyanosis of the extremities and perioral area,tachypnea, hyperpnea, and a heart rate of 180 beats/min. You do nothear a murmur.
Of the following, the MOST appropriate management strategy is to administer antipyretics for fever
encourage oral intake of fluids
order echocardiography
place her in the knee-chest position with oxygen
reassure her mother because the murmur is gone
Q ti 9
-
7/29/2019 Congenital Heart Disease From the Block
78/94
Question-9
You are evaluating a 4-month-old girl in your office whom you know tohave tetralogy of Fallot. Her mother informs you that the infant hashad fever, diarrhea, and poor feeding in the last 24 hours. On physicalexamination, you note cyanosis of the extremities and perioral area,tachypnea, hyperpnea, and a heart rate of 180 beats/min. You do nothear a murmur.
Of the following, the MOST appropriate management strategy is to administer antipyretics for fever
encourage oral intake of fluids
order echocardiography
place her in the knee-chest position with oxygen
reassure her mother because the murmur is gone
Q ti 10 2004
-
7/29/2019 Congenital Heart Disease From the Block
79/94
Question-10-2004
A 14-year-old boy complains of fatigue, weight loss, and night sweatsover 2 months. His parents noted the recent onset of generalizedswelling of the face and neck that has a dusky color.
Of the following, the MOST useful diagnostic test for this boy is
chest radiography
computed tomography of the sinuses
cranial computed tomography
serum antinuclear antibody test
tuberculin skin test
Q ti 10 2004
-
7/29/2019 Congenital Heart Disease From the Block
80/94
Question-10-2004
A 14-year-old boy complains of fatigue, weight loss, and night sweatsover 2 months. His parents noted the recent onset of generalizedswelling of the face and neck that has a dusky color.
Of the following, the MOST useful diagnostic test for this boy is
chest radiography
computed tomography of the sinuses
cranial computed tomography
serum antinuclear antibody test
tuberculin skin test
Q ti 11
-
7/29/2019 Congenital Heart Disease From the Block
81/94
Question-11
A 16-year-old girl who has systemic lupus erythematosus has beenvomiting for 1 day after having vague abdominal discomfort associatedwith anorexia for 3 days. Physical examination reveals tachycardia,with a heart rate of 130 beats/min. All peripheral pulses diminish instrength when she inhales.
Of the following, the MOST important study to obtain initially is
abdominal computed tomography
chest radiography
electrocardiography
erythrocyte sedimentation rate
upper gastrointestinal radiographic series
Q ti 11
-
7/29/2019 Congenital Heart Disease From the Block
82/94
Question-11
A 16-year-old girl who has systemic lupus erythematosus has beenvomiting for 1 day after having vague abdominal discomfort associatedwith anorexia for 3 days. Physical examination reveals tachycardia,with a heart rate of 130 beats/min. All peripheral pulses diminish instrength when she inhales.
Of the following, the MOST important study to obtain initially is
abdominal computed tomography
chest radiography
electrocardiography
erythrocyte sedimentation rate
upper gastrointestinal radiographic series
Q ti 12
-
7/29/2019 Congenital Heart Disease From the Block
83/94
Question-12
An 11-year-old girl has a 1-week history of dyspnea, malaise, andfatigue. She developed vomiting after 24 hours of feeling abdominalfullness and discomfort. Physical examination reveals a blood pressureof 85/50 mm Hg, tachypnea, rales, hepatomegaly, and no cardiacmurmur. The heart rate by auscultation is 120 beats/min. Palpation ofthe pulses reveals a regular rate of 60 beats/min.
Of the following, the MOST likely diagnosis is acute
hepatitis
lobar pneumonia
myocarditis
pancreatitis
pericarditis
Q ti 12
-
7/29/2019 Congenital Heart Disease From the Block
84/94
Question-12
An 11-year-old girl has a 1-week history of dyspnea, malaise, andfatigue. She developed vomiting after 24 hours of feeling abdominalfullness and discomfort. Physical examination reveals a blood pressureof 85/50 mm Hg, tachypnea, rales, hepatomegaly, and no cardiacmurmur. The heart rate by auscultation is 120 beats/min. Palpation ofthe pulses reveals a regular rate of 60 beats/min.
Of the following, the MOST likely diagnosis is acute
hepatitis
lobar pneumonia
myocarditis
pancreatitis
pericarditis
Q estion 13
-
7/29/2019 Congenital Heart Disease From the Block
85/94
Question-13
Two weeks after having a perimembranous ventricular septal defectrepaired, a 4-year-old child presents with anorexia and occasionalvomiting. On physical examination, there is pallor of the lips, and thepulses are difficult to feel. The auscultated heart rate is 140 beats/min,but the heart rate by radial pulse is only 70 to 80 beats/min. There isno palpable radial pulse during the inspiratory phase of respiration.
Of the following, the intervention that is MOST likely to be effective is
direct current cardioversion
intravenous methylprednisolone
pericardiocentesis
thoracentesis
transvenous cardiac pacing
Question 13
-
7/29/2019 Congenital Heart Disease From the Block
86/94
Question-13
Two weeks after having a perimembranous ventricular septal defectrepaired, a 4-year-old child presents with anorexia and occasionalvomiting. On physical examination, there is pallor of the lips, and thepulses are difficult to feel. The auscultated heart rate is 140 beats/min,but the heart rate by radial pulse is only 70 to 80 beats/min. There isno palpable radial pulse during the inspiratory phase of respiration.
Of the following, the intervention that is MOST likely to be effective is
direct current cardioversion
intravenous methylprednisolone
pericardiocentesis
thoracentesis
transvenous cardiac pacing
Question 14
-
7/29/2019 Congenital Heart Disease From the Block
87/94
Question-14
An asymptomatic 4-year-old girl has long, spidery fingers and a pectuscarinatum deformity. Her height is at the 50th percentile and weight isat the 5th percentile. Cardiac auscultation reveals a systolic click thatoccurs later in systole with squatting and earlier with standing.
Of the following, the MOST likely finding on echocardiography wouldbe
bicuspid aortic valve
Ebstein anomaly of the tricuspid valve
idiopathic hypertrophic subaortic stenosis
mitral valve prolapse
sinus of Valsalva aneurysm
Question 14
-
7/29/2019 Congenital Heart Disease From the Block
88/94
Question-14
An asymptomatic 4-year-old girl has long, spidery fingers and a pectuscarinatum deformity. Her height is at the 50th percentile and weight isat the 5th percentile. Cardiac auscultation reveals a systolic click thatoccurs later in systole with squatting and earlier with standing.
Of the following, the MOST likely finding on echocardiography wouldbe
bicuspid aortic valve
Ebstein anomaly of the tricuspid valve
idiopathic hypertrophic subaortic stenosis
mitral valve prolapse
sinus of Valsalva aneurysm
Question 15
-
7/29/2019 Congenital Heart Disease From the Block
89/94
Question-15
A newborn who has cyanosis has pulse oximetry values of 95% inhead hood oxygen at 100% Fio2. Arterial blood gas from the rightradial artery shows: pH, 7.34; Po2, 65 torr; and Pco2, 38 torr.
Of the following, the MOST likely diagnosis is
coarctation of the aorta with bicuspid aortic valve
double-inlet single ventricle with mild pulmonic valve stenosis
pulmonary atresia with restrictive ductus arteriosus
transposition of the great vessels with restrictive foramen ovale
ventricular septal defect with mild pulmonic valve stenosis
Question 15
-
7/29/2019 Congenital Heart Disease From the Block
90/94
Question-15
A newborn who has cyanosis has pulse oximetry values of 95% inhead hood oxygen at 100% Fio2. Arterial blood gas from the rightradial artery shows: pH, 7.34; Po2, 65 torr; and Pco2, 38 torr.
Of the following, the MOST likely diagnosis is
coarctation of the aorta with bicuspid aortic valve
double-inlet single ventricle with mild pulmonic valve stenosis
pulmonary atresia with restrictive ductus arteriosus
transposition of the great vessels with restrictive foramen ovale
ventricular septal defect with mild pulmonic valve stenosis
Question 16
-
7/29/2019 Congenital Heart Disease From the Block
91/94
Question-16
Which of the following laboratory findings is either a majoror minor Jones criterion for the diagnosis of acuterheumatic fever?
decreased PR interval by electrocardiography
decreased serum complement
decreased serum haptoglobin
elevated antistreptolysin O titer
elevated C-reactive protein
Question 16
-
7/29/2019 Congenital Heart Disease From the Block
92/94
Question-16
Which of the following laboratory findings is either a majoror minor Jones criterion for the diagnosis of acuterheumatic fever?
decreased PR interval by electrocardiography
decreased serum complement
decreased serum haptoglobin
elevated antistreptolysin O titer
elevated C-reactive protein
Jones Criteria
-
7/29/2019 Congenital Heart Disease From the Block
93/94
Jones Criteria
Major JONES Joints
Obvious as in Carditis
Nodules
Erythema marginatum
Sydenhams Chorea
Minor criteria
Elevated acute phase reactants Increased PR interval
Arthralgias
fever
References
-
7/29/2019 Congenital Heart Disease From the Block
94/94
References