Congenital clubfoot
29
Congenital Clubfoot ( Talipes equinovarus ) Yasser Alwabli
Transcript of Congenital clubfoot
Congenital Clubfoot (Talipes equinovarus)
Yasser
Alwabli
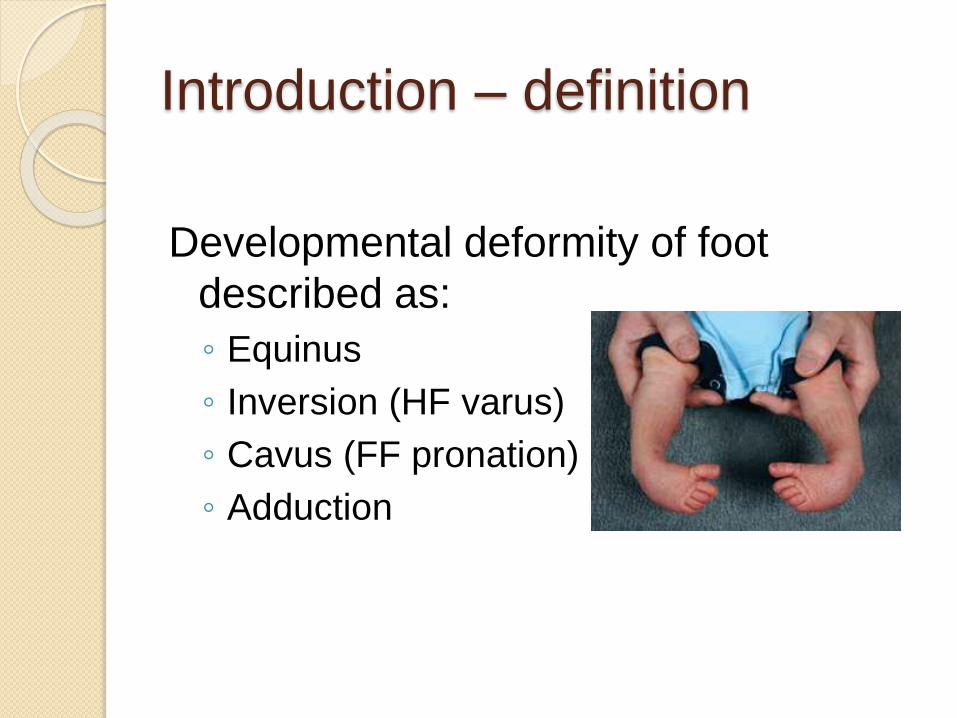
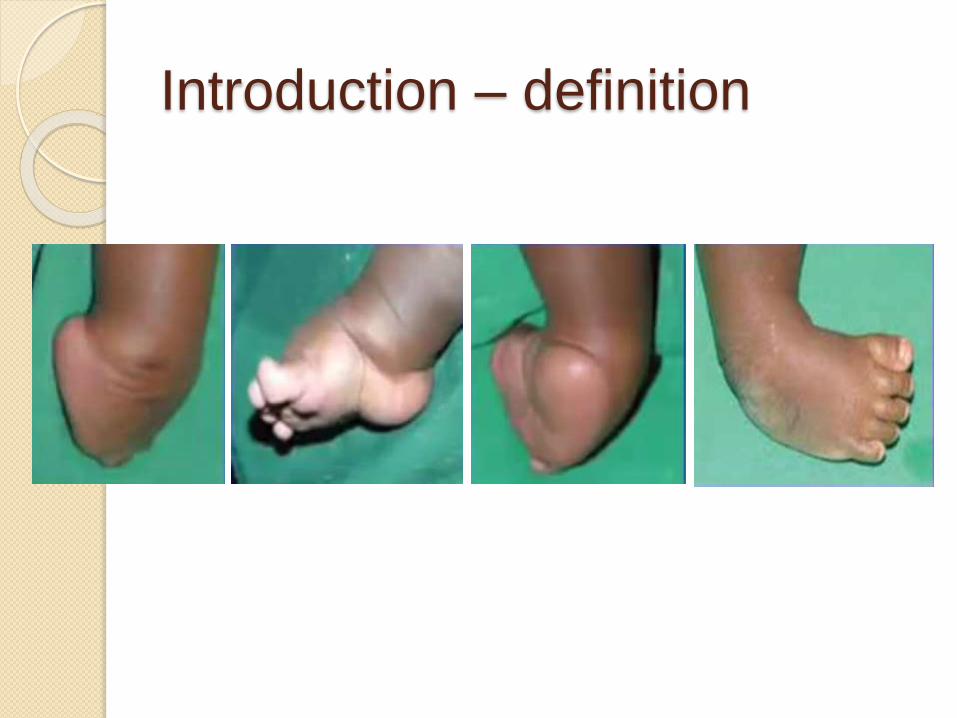
Introduction – definition
Developmental deformity of foot
described as:
◦ Equinus
◦ Inversion (HF varus)
◦ Cavus (FF pronation)
◦ Adduction
Introduction – definition
Epidemiology
1-2 in 1000
50% bilateral, Boys 2X
Associations (20%) - SP, CP, AG ? DDH (Paton RW, 2009)
Family studies:
◦ 30% in identical twins, one parent 3-4%
and two parents 30%
Etiology
Many theories:
◦ Mechanical, neuromuscular, vascular
deficiencies
◦ Polygenic multifactorial trait
◦ AD with incomplete penetrance
◦ Environmental – early amniocentesis,
maternal smoking
◦ Genetic – PITX1 gene
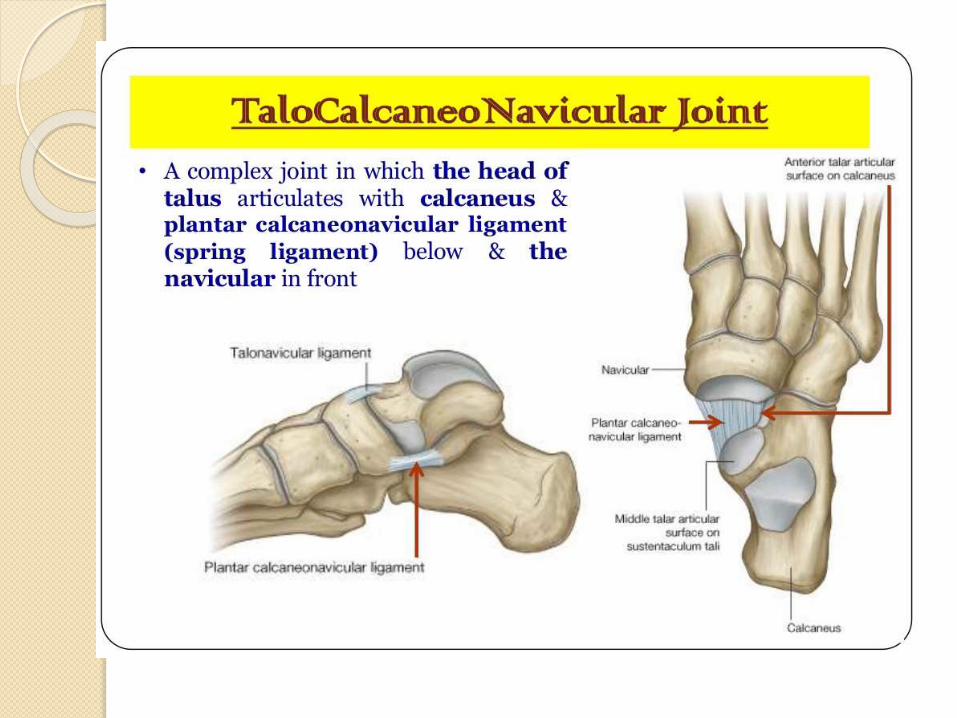
Pathoanatomy
Talocalcaneonavicular (TCN) joint
dislocation with soft tissue
contractures


Soft tissue contractures
Cavus (tight intrinsics, FHL, FDL)
Adductus (tight tibialis posterior)
Varus (tight tendoachilles, tibialis
posterior)
Equinus (tight tendoachilles)

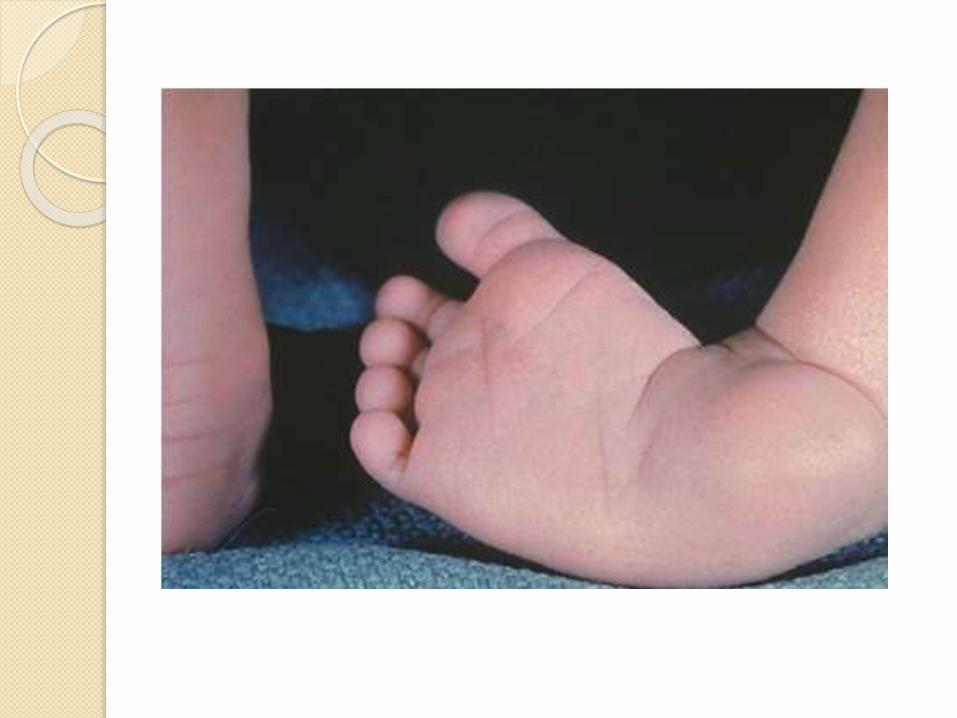
Clinically
Small foot
Small calf
Tibia - shortened
Medial and posterior foot skin creases
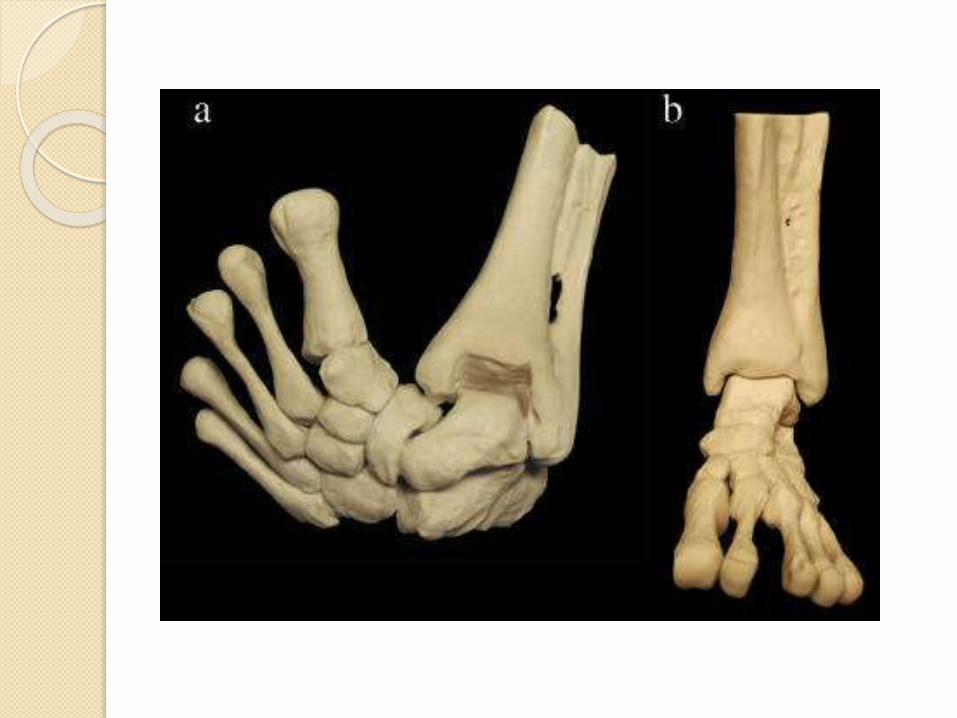
Foot deformities:
◦ Hindfoot - Equinus + Varus
◦ Midfoot - Cavus
◦ Forefoot - Adduction
Imaging
Antenatally – US
X-Rays – not routinely done
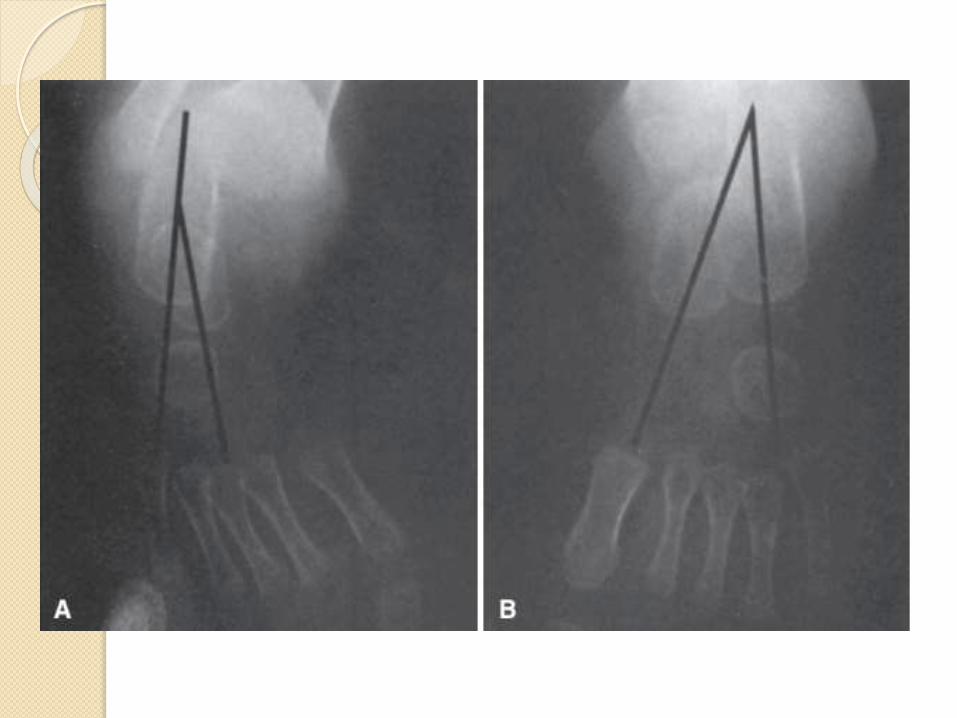
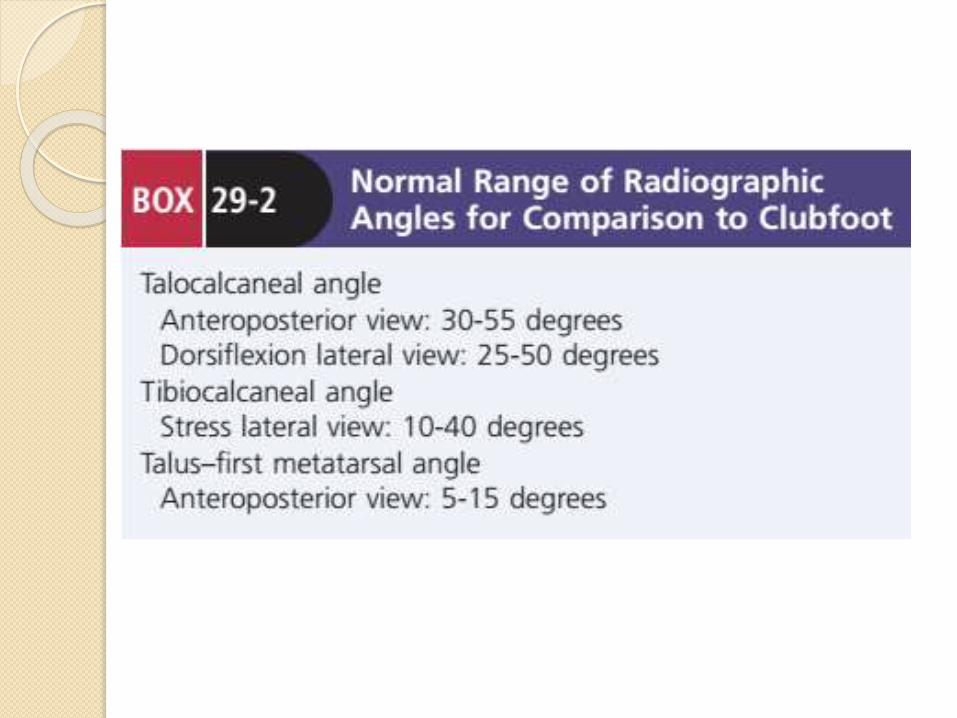
Views - AP and lateral in stress dorsiflexion. ◦ On AP view: Talocalcaneal angle (30-55˚) and the talo-first
metatarsal angle (5-15˚).
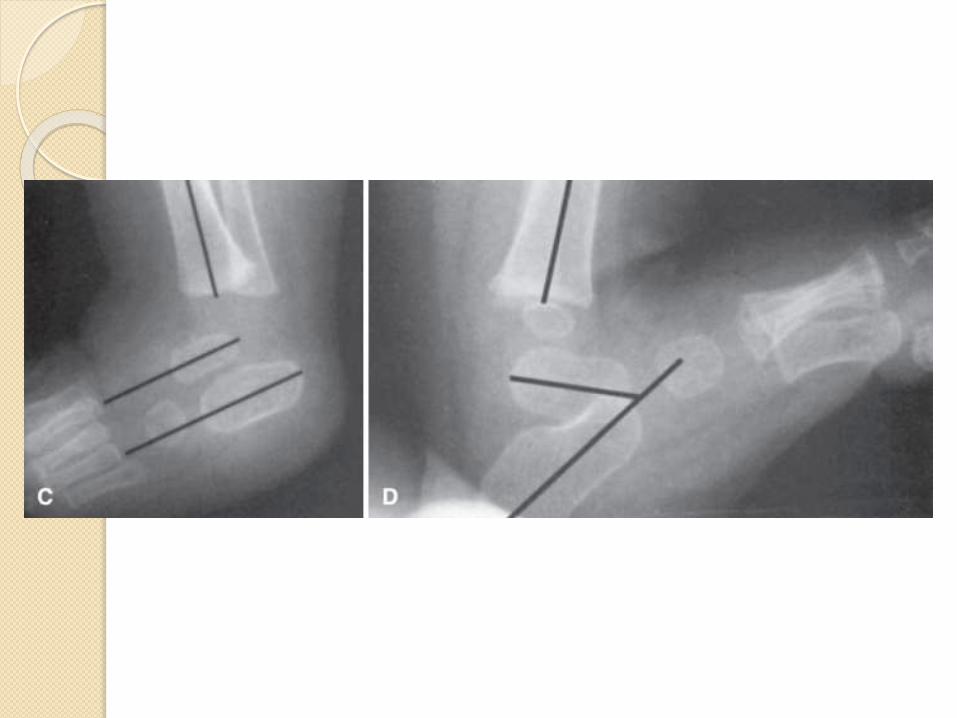
◦ Lateral view: Talocalcaneal angle (10-40˚) and the tibiocalcaneal
angle (10-20˚).
Hindfoot parallelism
All of these angles are decreased.
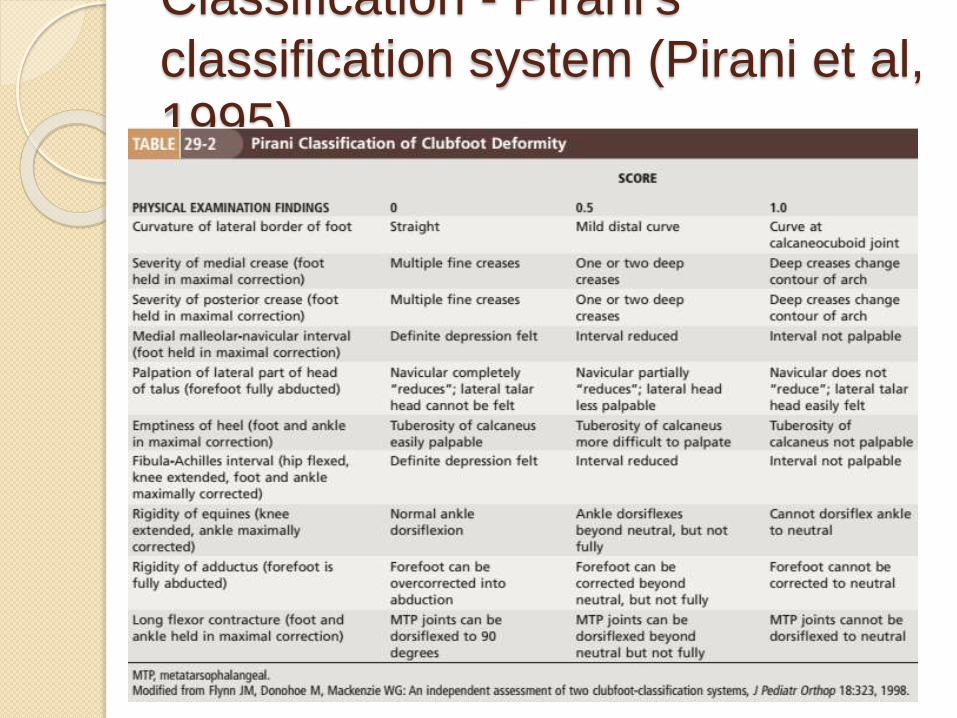
Classification - Pirani’s
classification system (Pirani et al,
1995)
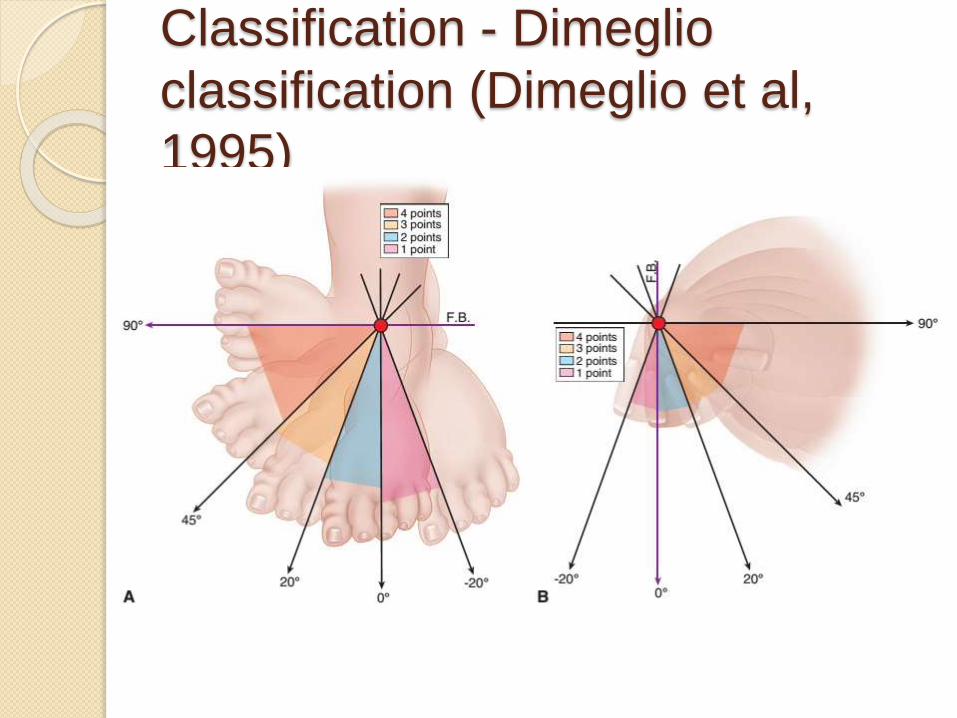
Classification - Dimeglio
classification (Dimeglio et al,
1995)

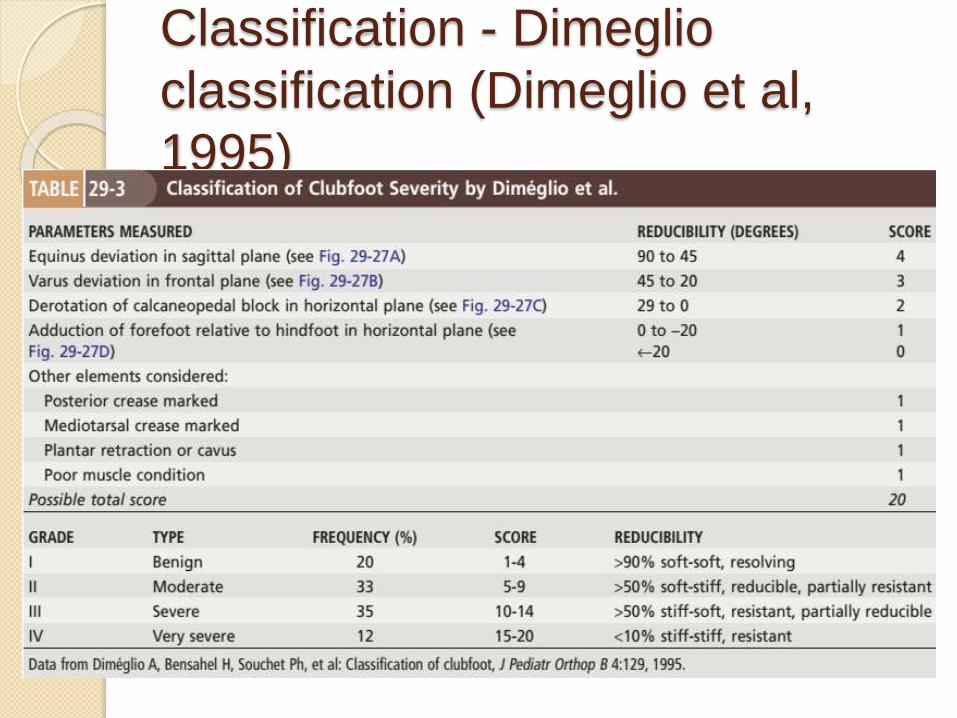
Classification - Dimeglio
classification (Dimeglio et al,
1995)
Classification - Dimeglio
classification (Dimeglio et al,
1995)
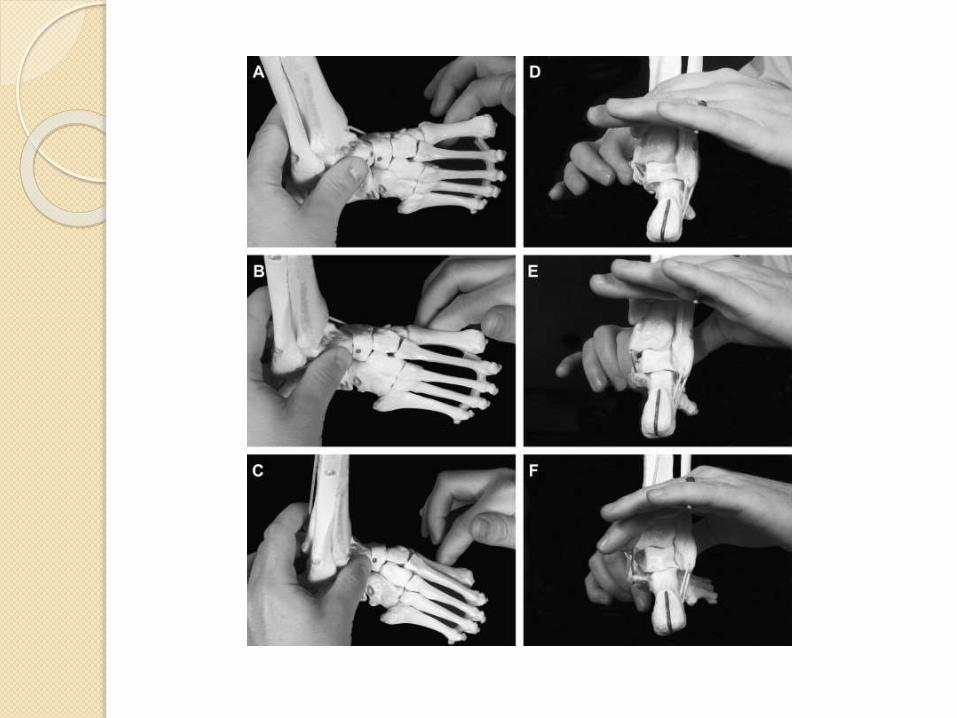
Treatment – Ponseti
technique Since 1950
POSNA members – 96.7% (2010)
Success rate – 90%
Timing – first weeks of life
Serial casting (average 4-5 casts)
Long leg cast
Dennis brown bar
Achilles tenotomy – 70%

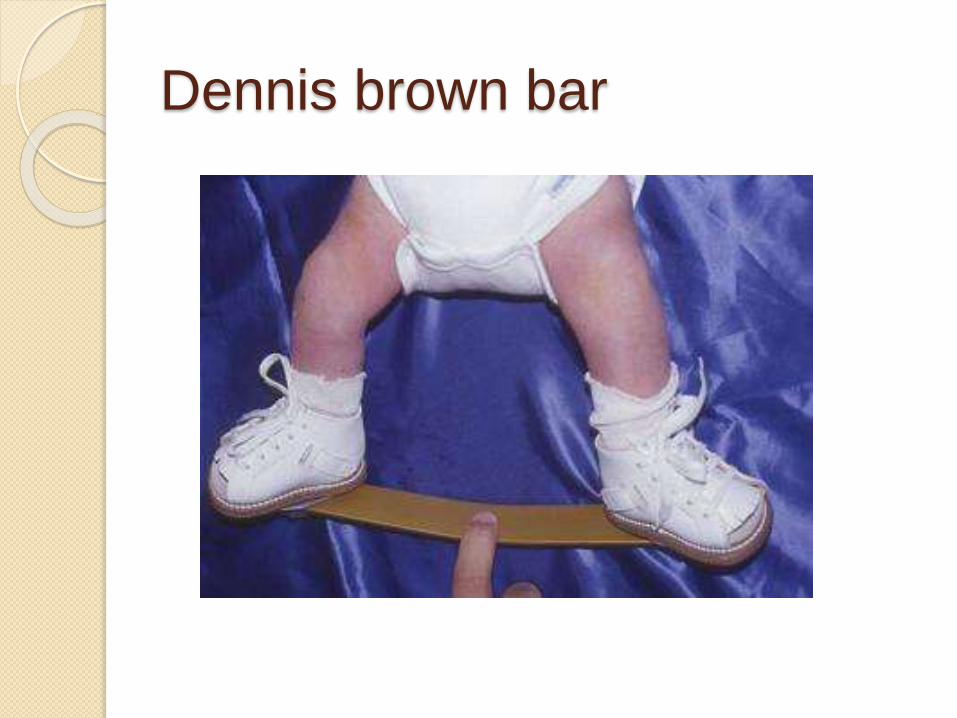
Dennis brown bar

Treatment – Ponseti
technique
Treatment - French technique
74% success rate
Daily manipulation by physiotherapist followed by immobilization with adhesive taping to maintain the correction achieved with stretching.
Daily for 2 months then 3/week till age 6 months.
If successful in achieving correction, parents continue both the home exercises and night splints until the child reaches walking age.
Treatment – surgical options
Posteromedial soft tissue release: Resistant cases
Delayed presentation
Syndrome-associated clubfoot
Medial opening or lateral column-
shortening osteotomy, or cuboidal
decancellation – older children 3-10
years
Tripe arthrodesis – refractory cases
Talectomy – salvage procedure
Complications
With nonoperative treatment:
◦ Relapse
◦ Dynamic supination
With operative treatment:
◦ Residual cavus
◦ Pes planus
◦ Intoeing gait
◦ Dorsal bunion