Confirmation of Tolosa-Hunt Syndrome via endoscopic biopsy ... · Campbell R, Okazaki H. Painful...
1
Confirmation of Tolosa-Hunt Syndrome via endoscopic biopsy of inflammation surrounding the orbital apex Amy Li Richter MD, Masayoshi Takashima MD Baylor College of Medicine Bobby R. Alford Department of Otolaryngology - Head and Neck Surgery Objectives Case Report 1) Review the criteria of diagnosing Tolosa- Hunt Syndrome (THS), a rare cause of painful ophthalmoplegia due to idiopathic granulomatous inflammation of the orbital apex or cavernous sinus. 2) Review the literature of THS and other surgical techniques used previously in the setting of THS. • History of present illness: BH is a 41 year old male with 2 week history of decreased vision, left eye pain, pressure headache. No light perception from his left eye for 5 days. • Surgical / social history: appendectomy, current 1/2 pack-per-day smoker, social drinker, no illicit drugs • Vital signs: Temperature 100.3F • Exam: • Eyes: No light perception in left eye, afferent pupillary defect in left eye, paralysis of extraocular movements (total loss of cranial nerves III, IV, VI), right eye normal • Neuro: Decreased sensation in left CN V2 • CBC, CMP, ESR, CRP, CSF, CTA, MRA, MRV all normal • MRI demonstrated abnormal enhancement in left orbital apex and cavernous sinus with extension along left infraorbital nerve into the left inferior orbital and pterygopalatine fissures. • CT demonstrated loss of fat planes in the left inferior orbital and pterygopalatine fissures and hyperostosis of the left sphenoid bone. 2004 THS International Headache Society criteria A. One or more episodes of unilateral orbital pain persisting for weeks if untreated B. Paresis of one or more of the third, fourth and/or sixth cranial nerves and/or demonstration of granulomatous inflammation by MRI or biopsy C. Paresis coincides with the onset of pain or follows it within 2 weeks D. Pain and paresis improve within 72h when treated adequately with corticosteroids E. Other causes have been excluded by appropriate investigations • One case per million per year, rare cause of painful ophthalmoplegia • Nonspecific inflammation of orbital apex, septa and wall of cavernous sinus: lymphocyte and plasma cell infiltration, giant cell granulomas, and proliferation of fibroblasts • Palsy of CN III, IV, VI, and superior divisions of CN V • Differential diagnosis includes tumors, vasculitis, basal meningitis, sarcoid, diabetes mellitus, and ophthalmoplegic ‘migraine’ • MRI demonstrates inflammation in the cavernous sinus, superior orbital fissure or orbit in 92% of cases • Diagnosis is a diagnosis of exclusion or demonstration of granuloma on MRI or granulomatous inflammation on histopathology • Treatment with steroids; steroid type, dosage, administration method, and duration are variable Imaging Image 1. Coronal fat suppressed MRI. Enhancement of extraocular muscles at orbital apex and extension into pterygopalatine fossa (arrow). Image 2. Axial fat suppressed MRI. Enhancement of extracranial optical nerve extending into inferior orbital fissure (arrow). Image 3. Coronal CT with contrast. Loss of fat planes in pterygopalatine fossa at sphenopalatine foramen (arrow). Surgical Approaches Background Pathology Fig 1. Pterygopalatine fossa • Biopsies performed of pterygopalatine fossa, pterygoid fossa, and sphenopalatine foramen • Figure 1 demonstrates chronic inflammation with distorted lymphocytes (arrowhead) and plasma cells and fibrosis • Figure 2 demonstrates chronic granulomatous inflammation with distorted lymphocytes surrounding fibrovascular bundles (arrowhead) • Endonasal endoscopic biopsy of inflammatory tissue at pterygopalatine fossa and sphenopalatine foramen was performed within 72 hours to confirm chronic granulomatous inflammation and rule out infectious and neoplastic etiology. • Steroids were initiated, and patient BH had resolution of his pain within 24 hours of starting high dose intravenous dexamethasone. He continued a several week course of oral steroids and continued to have gradual improvement of his ophthalmoplegia. At his one month follow up visit, he had significantly improved vision. Fig 2. Pterygoid fossa Discussion Fig 3. Sphenopalatine artery Fig 4. Pterygoid fossa Reference No Surgical approach Pathology Tolosa. 1954 1 Transfrontal intradural, autopsy Negative; non- specific periarterial granulation Hunt et al. 1961 1 Transfrontal parasellar Nonspecific inflammation Lakke. 1962 1 Frontotemporal craniotomy Nonspecific inflammation Schatz. 1972 2 Frontotemporal craniotomy to cavernous sinus Chronic inflammation, plasma cells, fibrosis; chronic granulomatous lesion Campbell et al. 1987 1 Autopsy Vasculitis and nongranulomatous inflammation Goadsby et al. 1989 1 Craniotomy Retroorbital granuloma Brown et al. 1990 1 Sublabial transseptal sphenoidotomy Nonspecific inflammation Yousem et al. 1990 3 Unspecified cavernous sinus biopsy Nonspecific inflammatory change Lance. 1991 1 Unspecified Lateral cavernous sinus granuloma Montecucco et al. 1993 1 Unspecified Mononuclear cells noncaseating granuloma Wasmeier et al. 2002 2 Transfrontal biopsy of medial rectus; transorbital exploration Granulocytic myositis; granulomatous inflammation at orbital apex References Brown J, Moster M, Kenning J, et al. The Tolosa-Hunt syndrome: A case report. Otolaryng Head Neck. 1990;102;402-4. Campbell R, Okazaki H. Painful ophthalmoplegia (Tolosa-Hunt variant): Autopsy findings in a patient with necrotizing intracavernous carotid vasculitis and inflammatory disease of the orbit. Mayo Clinic Proc. 1987;62:520-6. Goadsby P, Lance J. Clinicopathological correlation in a case of painful ophthalmoplegia: Tolosa-Hunt syndrome. J Neurol Neurosurg Psychiat. 1989;52:1290-3. Hunt W, Meagher J, LeFever J. Painful ophthalmoplegia: its relation to indolent inflammation of the cavernous sinus. Neurology. 1961;11:56-62. Kline L. The Tolosa-Hunt syndrome. Surv Ophthalmol. 1982;27:79-95. Lakke JPWF. Superior orbital fissure syndrome. Arch Neurol. 1962;7:289-300. Lance J. Solved and unsolved headache problems. Headache. 1991;31:439- 45. Montecucco C, Caporali R, Pacchetti C, et al. Is Tolosa-Hunt syndrome a limited form of Wegener’s granulomatosis? Br J Rheumatol. 1993;32:640-1. Schuknect B, Sturm V, Huisman TAGM, et al. Tolosa-Hunt syndrome: MR imaging features in 15 patients with 20 episodes of painful ophthalmoplegia. Eur J Radiol. 2009;69:445-53. Schatz N, Farmer P. THS: The pathology of painful ophthalmoplegia. In: Smith JL, et al. Neuro-ophthalmology Vol 6. St. Louis: Mosby Co. 1972;102-12. Tolosa E. Periarteritic lesions of the carotid siphon with the clinical features of a carotid infraclinoidal aneurysm. J Neurol Neurosurg Psychiat. 1954;17;300-2. Yousem D, Atlas S, Grossman R, et al. MR imaging of Tolosa-Hunt syndrome. Am J Roentgenol. 1990;154:167-70. Diagnostic Criteria Operative Biopsy Disclosure It is the policy of Baylor College of Medicine (Baylor) that the provider and faculty / presenters disclose any significant financial or other relationships with commercial companies whose products may be discussed in the activity, or the commercial supporters, if any. Baylor also requires that faculty disclose any unlabeled use or investigational use (not yet approved for any purpose) of pharmaceutical and medical device products. Amy Richter, M.D., and Masayoshi Takashima, M.D. reported nothing to disclose. • Historically, THS has been a diagnosis of exclusion. There are only 14 documented cases with histologic diagnosis, of which only one biopsy in vivo was performed via transnasal approach (sphenoidotomy) and only 50% demonstrated granuloma formation or granulomatous inflammation. Most cases of THS are confirmed by symptoms and granuloma on imaging. • Endonasal endoscopic biopsy of the peri-orbital apex proved to be a safe, low risk procedure to confirm THS and rule out dangerous causes of painful ophthalmoplegia, including malignancy.
Transcript of Confirmation of Tolosa-Hunt Syndrome via endoscopic biopsy ... · Campbell R, Okazaki H. Painful...

Confirmation of Tolosa-Hunt Syndrome via endoscopic
biopsy of inflammation surrounding the orbital apex Amy Li Richter MD, Masayoshi Takashima MD
Baylor College of Medicine Bobby R. Alford Department of Otolaryngology - Head and Neck Surgery
Objectives
Case Report
1) Review the criteria of diagnosing Tolosa-
Hunt Syndrome (THS), a rare cause of
painful ophthalmoplegia due to
idiopathic granulomatous inflammation
of the orbital apex or cavernous sinus.
2) Review the literature of THS and other
surgical techniques used previously in
the setting of THS.
• History of present illness: BH is a 41 year old male with 2 week history of decreased vision, left eye pain, pressure headache. No light perception from his left eye for 5 days.
• Surgical / social history: appendectomy, current 1/2 pack-per-day smoker, social drinker, no illicit drugs
• Vital signs: Temperature 100.3F
• Exam:
• Eyes: No light perception in left eye, afferent pupillary defect in left eye, paralysis of extraocular movements (total loss of cranial nerves III, IV, VI), right eye normal
• Neuro: Decreased sensation in left CN V2
• CBC, CMP, ESR, CRP, CSF, CTA, MRA, MRV all normal
• MRI demonstrated abnormal enhancement in left orbital apex and cavernous sinus with extension along left infraorbital nerve into the left inferior orbital and pterygopalatine fissures.
• CT demonstrated loss of fat planes in the left inferior orbital and pterygopalatine fissures and hyperostosis of the left sphenoid bone.
2004 THS International Headache Society criteria
A. One or more episodes of unilateral orbital pain
persisting for weeks if untreated
B. Paresis of one or more of the third, fourth and/or
sixth cranial nerves and/or demonstration of
granulomatous inflammation by MRI or biopsy
C. Paresis coincides with the onset of pain or follows
it within 2 weeks
D. Pain and paresis improve within 72h when
treated adequately with corticosteroids
E. Other causes have been excluded by appropriate
investigations
• One case per million per year, rare cause of painful ophthalmoplegia
• Nonspecific inflammation of orbital apex, septa and wall of cavernous sinus: lymphocyte and plasma cell infiltration, giant cell granulomas, and proliferation of fibroblasts
• Palsy of CN III, IV, VI, and superior divisions of CN V
• Differential diagnosis includes tumors, vasculitis, basal meningitis, sarcoid, diabetes mellitus, and ophthalmoplegic ‘migraine’
• MRI demonstrates inflammation in the cavernous sinus, superior orbital fissure or orbit in 92% of cases
• Diagnosis is a diagnosis of exclusion or demonstration of granuloma on MRI or granulomatous inflammation on histopathology
• Treatment with steroids; steroid type, dosage, administration method, and duration are variable
Imaging
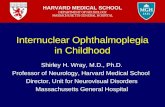
Image 1. Coronal fat suppressed MRI.
Enhancement of extraocular muscles
at orbital apex and extension into
pterygopalatine fossa (arrow).
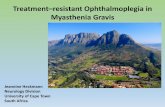
Image 2. Axial fat suppressed
MRI. Enhancement of extracranial
optical nerve extending into inferior
orbital fissure (arrow).
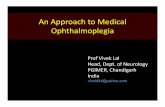
Image 3. Coronal CT with
contrast. Loss of fat planes in
pterygopalatine fossa at
sphenopalatine foramen (arrow).
Surgical Approaches
Background Pathology
Fig 1. Pterygopalatine fossa
• Biopsies performed of pterygopalatine fossa, pterygoid fossa, and sphenopalatine foramen
• Figure 1 demonstrates chronic inflammation with distorted lymphocytes (arrowhead) and plasma cells and fibrosis
• Figure 2 demonstrates chronic granulomatous inflammation with distorted lymphocytes surrounding fibrovascular bundles (arrowhead)
• Endonasal endoscopic biopsy of inflammatory tissue at pterygopalatine fossa and sphenopalatine foramen was performed within 72 hours to confirm chronic granulomatous inflammation and rule out infectious and neoplastic etiology.
• Steroids were initiated, and patient BH had resolution of his pain within 24 hours of starting high dose intravenous dexamethasone. He continued a several week course of oral steroids and continued to have gradual improvement of his ophthalmoplegia. At his one month follow up visit, he had significantly improved vision.
Fig 2. Pterygoid fossa
Discussion
Fig 3. Sphenopalatine artery Fig 4. Pterygoid fossa
Reference No Surgical
approach
Pathology
Tolosa.
1954
1 Transfrontal
intradural,
autopsy
Negative; non-
specific periarterial
granulation
Hunt et al.
1961
1 Transfrontal
parasellar
Nonspecific
inflammation
Lakke.
1962
1 Frontotemporal
craniotomy
Nonspecific
inflammation
Schatz.
1972
2 Frontotemporal
craniotomy to
cavernous
sinus
Chronic
inflammation,
plasma cells,
fibrosis; chronic
granulomatous
lesion
Campbell et
al. 1987
1 Autopsy Vasculitis and
nongranulomatous
inflammation
Goadsby et
al. 1989
1 Craniotomy Retroorbital
granuloma
Brown et al.
1990
1 Sublabial
transseptal
sphenoidotomy
Nonspecific
inflammation
Yousem et
al. 1990
3 Unspecified
cavernous
sinus biopsy
Nonspecific
inflammatory
change
Lance.
1991
1 Unspecified Lateral cavernous
sinus granuloma
Montecucco
et al. 1993
1 Unspecified Mononuclear cells
noncaseating
granuloma
Wasmeier
et al. 2002
2 Transfrontal
biopsy of
medial rectus;
transorbital
exploration
Granulocytic
myositis;
granulomatous
inflammation at
orbital apex
References Brown J, Moster M, Kenning J, et al. The Tolosa-Hunt syndrome: A case report.
Otolaryng Head Neck. 1990;102;402-4.
Campbell R, Okazaki H. Painful ophthalmoplegia (Tolosa-Hunt variant): Autopsy
findings in a patient with necrotizing intracavernous carotid vasculitis and
inflammatory disease of the orbit. Mayo Clinic Proc. 1987;62:520-6.
Goadsby P, Lance J. Clinicopathological correlation in a case of painful
ophthalmoplegia: Tolosa-Hunt syndrome. J Neurol Neurosurg Psychiat.
1989;52:1290-3.
Hunt W, Meagher J, LeFever J. Painful ophthalmoplegia: its relation to indolent
inflammation of the cavernous sinus. Neurology. 1961;11:56-62.
Kline L. The Tolosa-Hunt syndrome. Surv Ophthalmol. 1982;27:79-95.
Lakke JPWF. Superior orbital fissure syndrome. Arch Neurol. 1962;7:289-300.
Lance J. Solved and unsolved headache problems. Headache. 1991;31:439-
45.
Montecucco C, Caporali R, Pacchetti C, et al. Is Tolosa-Hunt syndrome a limited
form of Wegener’s granulomatosis? Br J Rheumatol. 1993;32:640-1.
Schuknect B, Sturm V, Huisman TAGM, et al. Tolosa-Hunt syndrome: MR
imaging features in 15 patients with 20 episodes of painful ophthalmoplegia.
Eur J Radiol. 2009;69:445-53.
Schatz N, Farmer P. THS: The pathology of painful ophthalmoplegia. In: Smith
JL, et al. Neuro-ophthalmology Vol 6. St. Louis: Mosby Co. 1972;102-12.
Tolosa E. Periarteritic lesions of the carotid siphon with the clinical features of a
carotid infraclinoidal aneurysm. J Neurol Neurosurg Psychiat. 1954;17;300-2.
Yousem D, Atlas S, Grossman R, et al. MR imaging of Tolosa-Hunt syndrome.
Am J Roentgenol. 1990;154:167-70.
Diagnostic Criteria
Operative Biopsy
Disclosure
It is the policy of Baylor College of Medicine (Baylor) that the provider
and faculty / presenters disclose any significant financial or other
relationships with commercial companies whose products may be
discussed in the activity, or the commercial supporters, if any. Baylor
also requires that faculty disclose any unlabeled use or investigational
use (not yet approved for any purpose) of pharmaceutical and medical
device products. Amy Richter, M.D., and Masayoshi Takashima, M.D.
reported nothing to disclose.
• Historically, THS has been a diagnosis of exclusion. There are only 14 documented cases with histologic diagnosis, of which only one biopsy in vivo was performed via transnasal approach (sphenoidotomy) and only 50% demonstrated granuloma formation or granulomatous inflammation. Most cases of THS are confirmed by symptoms and granuloma on imaging.
• Endonasal endoscopic biopsy of the peri-orbital apex proved to be a safe, low risk procedure to confirm THS and rule out dangerous causes of painful ophthalmoplegia, including malignancy.