Concussion treatment
24
IN- SERVICE CREATED & PRESENTED BY: SUSAN MILLER, SPT REGIS UNIVERSITY, APRIL 2015 Management & Treatment for Concussions
-
Upload
susan-miller -
Category
Documents
-
view
75 -
download
2
Transcript of Concussion treatment
I N - S E R V I C E C R E A T E D & P R E S E N T E D B Y :
S U S A N M I L L E R , S P T
R E G I S U N I V E R S I T Y , A P R I L 2 0 1 5
Management & Treatment for Concussions
Objectives
Overview of Concussion
Screen Tools: VOMS & BESS
Vestibular exercise program
What is a concussion?
According to Centers of Disease Control (CDC):
“A type of traumatic brain injury, or TBI, caused by a bump, blow or jolt to the head that can change the way your brain normally works. Concussions can also occur from a fall or blow to the body that causes the head and brain to move quickly back and forth.”
How can a concussion occur?
Head strikes a stationary item Head hitting ground/object
Head hitting an object during MVA
Object hitting the head I.E. - ball or stick during sports or human collision
Quick acceleration/deceleration of the head
These events cause Quick deceleration of the head
Shifting of brain tissue inside the skull
If Rotational force occurs LOC & nausea will occur
(Miranda, 2013)
What is affected from a concussion?
Reaction time & brain processing
Abnormal vestibular functioning Brain receives abnormal signals about position & movement of
head in space
Relies on visual input resulting in:
Fatigue
Difficulty with ADL’s
Eyestrain
Tension headaches
Dizziness
Sense of irritability
(Miranda, 2013)
Diagnosis of a concussion
Cannot be seen on CT or MRI Help rule out more series brain injuries (IC bleeding,
contusion, and/or lesions)
A Group of Symptoms will occur immediately or weeks to months after incident
Length of time for symptoms: Acute symptoms: 1-2 weeks following
Post Concussion Syndrome: 3-4 weeks to months
10-20%
(Johnston et al, 2004; Harmon et al, 2013; Miranda, 2013)
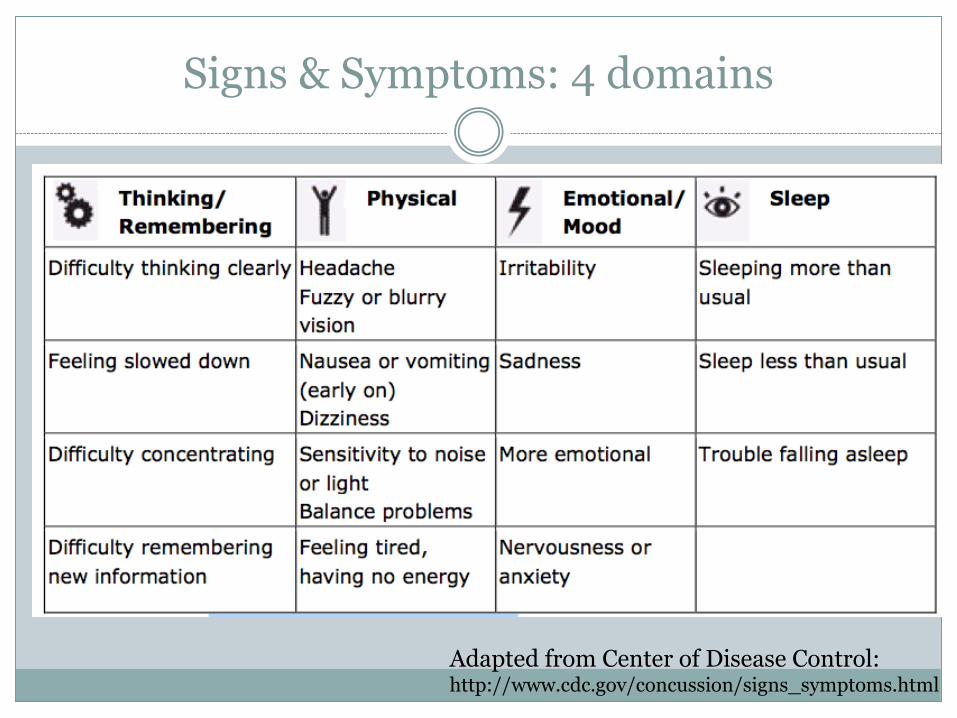
Signs & Symptoms: 4 domains
Adapted from Center of Disease Control:http://www.cdc.gov/concussion/signs_symptoms.html
Create a Multi-Disciplinary Team Approach
Team Includes: School Professionals
Physical Team: School nurse, certified athletic trainer, coach, & PE teacher, athletic director & other
Academic Tam: teacher, counselor, school psychologist, school social worker, and administrator and others
Medical Professionals
Doctor of Medicine (MD), Doctor of Osteopathic Medicine (DO), Nurse Practitioner (NP), Physician Assistant (PA), a licensed psychologist (with training in concussion management or a neuropsychologist
Family
Student, parents, guardians, grandparents, siblings, student’s peers
Adjunct team
Physical Therapist, Massage Therapist, Chiropractors & OT *
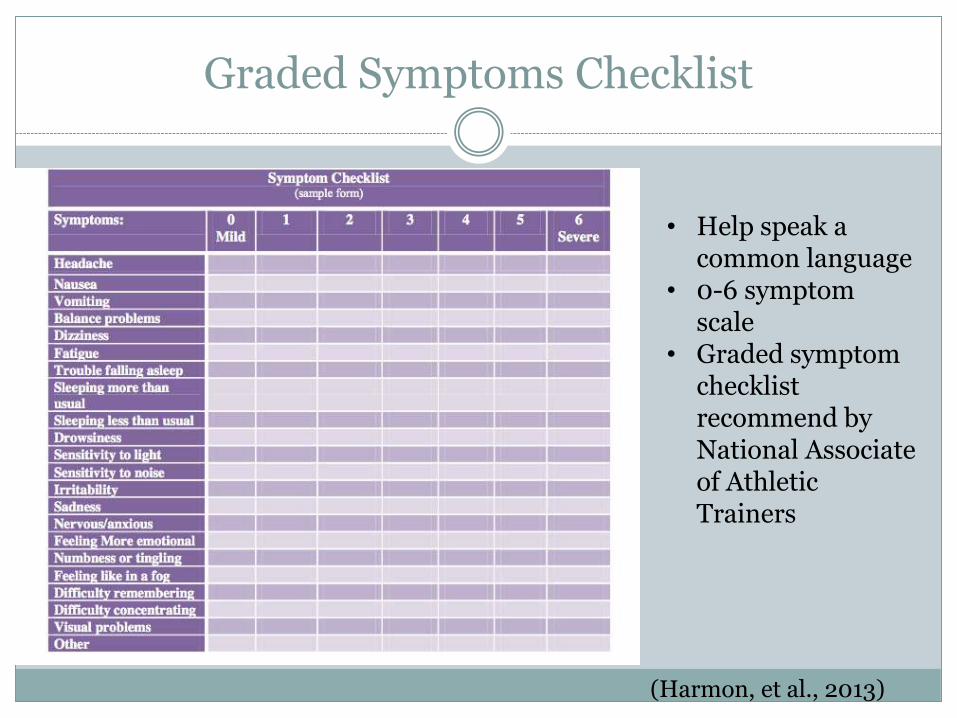
Graded Symptoms Checklist
• Help speak a common language
• 0-6 symptom scale
• Graded symptom checklist recommend by National Associate of Athletic Trainers
(Harmon, et al., 2013)
Determining Return to Play
Health care provider: Doctor of Medicine
Licensed Nurse Practitioner
Doctor of Osteopathic medicine
Licensed Physician Assistant
Licensed Doctor of Psychology w/ training in neuropsychology or concussion evaluation & management
Physical Therapist? Introduced in Feb. 2015 to House & Senate
SAFE PLAY Act (Supporting Athletes, Families and Educators to Protect Lives of Athletic Youth Act)
Concussion/Examination
History Cervical Evaluation VOMS* Ocular/Visual Assessment Gaze Stability Head Righting Neurologic Screen Cervicogenic Dizziness Balance Gait Assessment Exertion Response Positional Vertigo/Dizziness
Adapted from Kinetic Energy PT
Concussion Screening Tools
University of Pittsburgh Medical Center Vestibular/Ocular Motor Screening (UPMC VOMS)*
Balance Error Scoring System (BESS) test*
Computerized neurocognitive test (ImPACT)
UPMC VOMS
Develop to assess vestibular & ocular motor impairment
5 Domains: Smooth Pursuit
Horizontal & vertical saccades
Convergence
Horizontal & vertical Vestibular Ocular Motor Reflex (VOR)
Visual Motion Sensitivity (VMS)
Patients verbally rate changes: Headache, dizziness, nausea & fogginess Scale: 0 (none) to 10 (severe)
5 mins to administrate
See handout for test (Mucha, A. et al., 2014)
BESS test
Clinical balance test: 6 conditions (EO/EC), 3 stances, 2 surfaces (firm & foam); hands on hips for 20 s Feet together
Single leg
Tandem Stance
Total Errors: Lifting hands off hips
Opening eyes (in eyes closed conditions)
Leaning >30° of flexion/extension or adduction/abduction
Stepping out of position
Protracted time out of position
Acute Interventions
Physical:
Strategic rest periods: 15-20 min through the day
Sunglasses, quiet rooms, frequent breaks
Remove physical activity that provokes systems
Cognitive:
Reduce workload
Emotional:
Secondary depression & anxiety
Sleep/Energy:
Rest breaks; late start, early leave
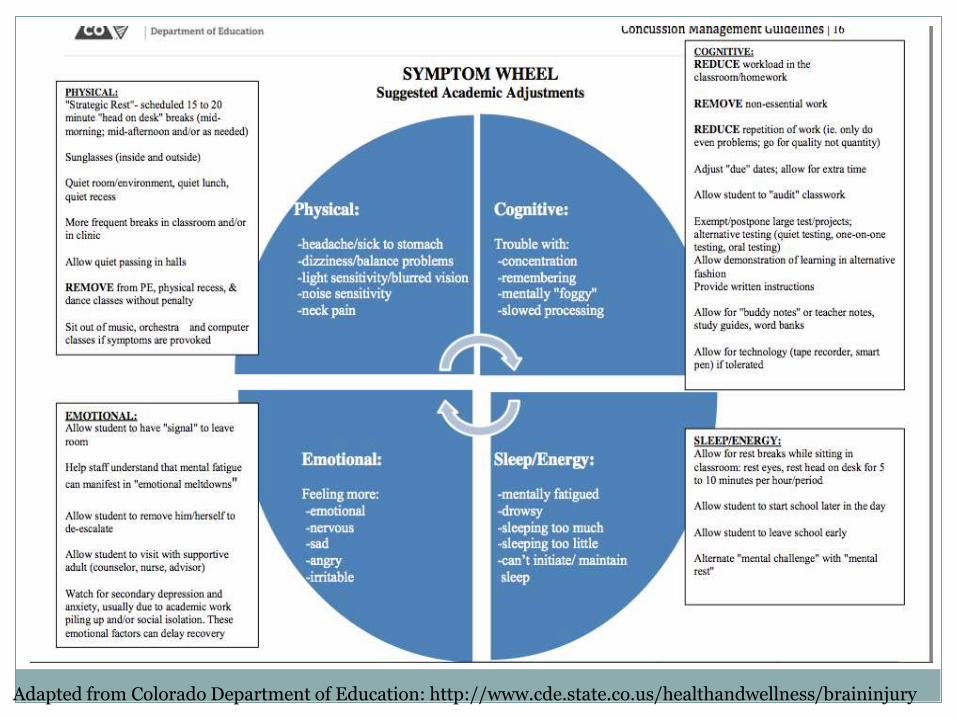
Adapted from Colorado Department of Education: http://www.cde.state.co.us/healthandwellness/braininjury
Vestibular Treatment for Concussions
Head trauma can cause inner ear damage
Resulting in balance & dizziness
Vestibular treatment can help improve sensory input for vestibular, visual, and proprioceptive systems
Vestibular Therapy:
EXERCISES
Vestibular Adaption exercise (Gaze Stability)
Vestibular stimulation (habituation)
Static & Dynamic Balance Cardiovascular
Manual Therapy- Cervical
Gaze Stability & Vestibular Adaption Exercises
VOR training
Includes movement of eyes that function to stabilize during head movement
Exercises Include:
X1 viewing
X2 viewing
Scanning exercises
Saccade Exercises
Positions:
Seated Standing Walking and/or Unstable Surfaces
Hand out & next slide for example
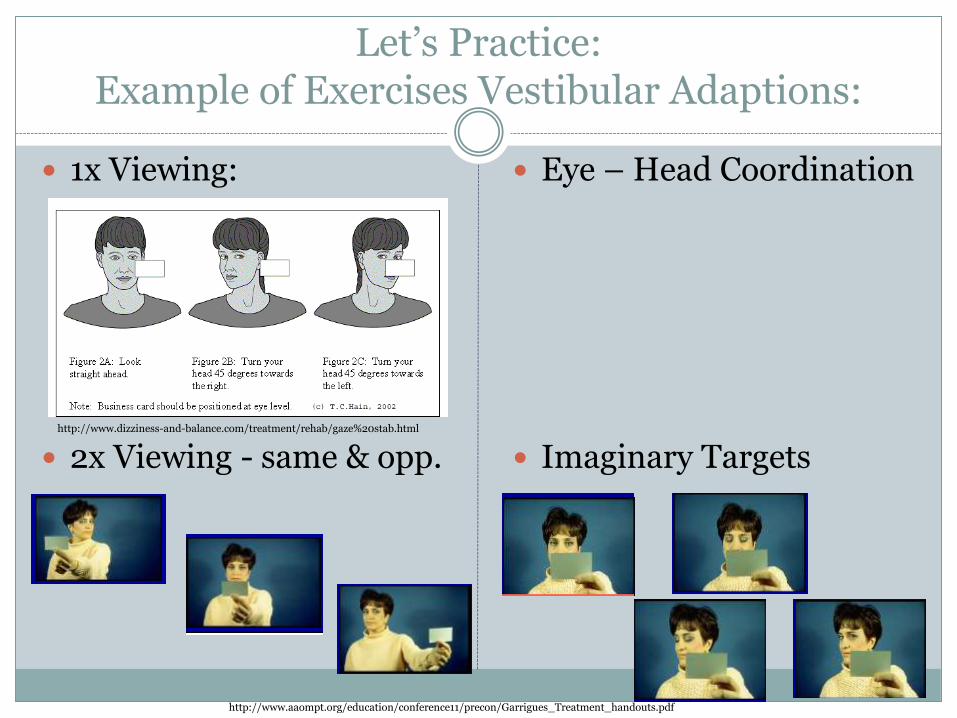
Let’s Practice: Example of Exercises Vestibular Adaptions:
1x Viewing:
2x Viewing - same & opp.
Eye – Head Coordination
Imaginary Targetshttp://www.dizziness-and-balance.com/treatment/rehab/gaze%20stab.html
3
VORx2 Imaginary Target Imaginary Target
Imaginary Target
Imaginary Target
Imaginary Target
Imaginary Target
Standing Static (Feet In Place)
• Upright
• Weight Shift
• Single Leg Stance
• Sit To Stand
• Rocker board
• 1 foot on step
3
VORx2 Imaginary Target Imaginary Target
Imaginary Target
Imaginary Target
Imaginary Target
Imaginary Target
Standing Static (Feet In Place)
• Upright
• Weight Shift
• Single Leg Stance
• Sit To Stand
• Rocker board
• 1 foot on step
3
VORx2 Imaginary Target Imaginary Target
Imaginary Target
Imaginary Target
Imaginary Target
Imaginary Target
Standing Static (Feet In Place)
• Upright
• Weight Shift
• Single Leg Stance
• Sit To Stand
• Rocker board
• 1 foot on step
3
VORx2 Imaginary Target Imaginary Target
Imaginary Target
Imaginary Target
Imaginary Target
Imaginary Target
Standing Static (Feet In Place)
• Upright
• Weight Shift
• Single Leg Stance
• Sit To Stand
• Rocker board
• 1 foot on step
http://www.aaompt.org/education/conference11/precon/Garrigues_Treatment_handouts.pdf
3
VORx2 Imaginary Target Imaginary Target
Imaginary Target
Imaginary Target
Imaginary Target
Imaginary Target
Standing Static (Feet In Place)
• Upright
• Weight Shift
• Single Leg Stance
• Sit To Stand
• Rocker board
• 1 foot on step
Vestibular Stimulation Exercises
Exercises to improve cervical ROM Flexion, extension, Rotation
Rotational exercises Picking items up from the ground
Exercises to improve static balance in the absence of vision
Motion Sensitivity exercise (Habituation) Based from Motion Sensitivity Score
Pick 4 positions that causes moderate level of symptoms
Pt. to repeat 2-3x’s
Hand out for test
Static & Dynamic Balance Exercises
Maintain Balance for 30s Static:
Eyes Open Closed
Firm surface Soft Surface
Different Stances: comfortable, narrow, tandem, single stance
Dynamic:
Walking w/ head movements: rotation, flexion, extension maintain direction & velocity of gait
Toss a ball to the patient while walking
Ambulation on unstable surface
Narrow BOS
(Kristjansson et al. 2009; Lee et al, 2013)
Manual Therapy - Cervical Cardiovascular
Soft Tissue Massage
Sub-occipital release
ROM exercise
Strengthening & improvement of posture (exercise & education)
Stationary Bike
Treadmill walking or jogging
Agility drills
Manual Therapy & Cardiovascular
(Schneider et al., 2014; Wells et al, 2015)
Exercise Program Progression
Type: Combo of cervical & vestibular training
Repetitions: 3-5 progressing towards 10
Duration: min. 6 -12 weeks
Until dizziness symptoms goes away altogether
Frequency: PT 1-2x/week; HEP 1-2x/day
Intensity: Should produce temporary increase in dizziness
Normal response & should try to work through these symptoms
(Schneider et al., 2014 Kristjansson et al. 2009)
References
Concussion Management Guidelines. Colorado Department of Education. http://www.cde.state.co.us/healthandwellness/concussionguidelines11-6-14 . Accessed on March 2015.
Harmon KG, Drezner JA, Gammons M, Guskiewicz KM, Halstead M, Herring SA, Kutcher JS, Pana A, Putukian M, Roberts WO. American Medical Society for Sports Medicine position statement: Concussion in sport. British Journal of Sports Medicine. 2013;47(1):15–26.
Heads Up Basic on Concussions. Center for Disease Control. http://www.cdc.gov/headsup/basics/concussion_whatis.html. March 2015.
Injury Prevention & Control: Traumatic Brain Injury. Center of Disease Control. http://www.cdc.gov/concussion/signs_symptoms.html. Accessed March 2015.
Johnston KM, Bloom GA, Ramsay J, Kissick J, Montgomery D, Foley D, Chen JK, Ptito A. Current concepts in concussion rehabilitation. Current Sports Medicine Reports. 2004;3(6):316–323.
Kristjannsson E, Treleaven J. Sensorimotor function and dizziness in neck pain: implications for assessment and management. J Orthop Sports Phys Ther. 2009; 39(5): 364-377.
Lee H, Sullivan, J, Schneiders A. The use of the dual-task paradigm in detecting gait performance deficits following a sports related concussion: A systematic and meta-analysis. J Sci and Med in Sp. 2013: (48) 2-7.
Miranda, N. Concussion: When Recovery Is Complicated By Vestibular Involvement and How Vestibular Rehabilitation Can Help. Vestibular Disorder Association. 2013.
Mucha, A. et al. Brief Vestibular and Ocular Motor Screening (VOMS) Assessment: Preliminary Finding in Patient following Sport-related Concussion. Am J Sports Med. Aug 2014
Schneider K, Meeuwissee W, Nettel-Aguirre A, Barlow K, Boyd L, Kang J, Emery C. Cervicovestibularrehabilitation in sport-related concussion: a randomized controlled trail. Br J Sports Med. 2014: (48) 1294-1298.
Vestibular Rehabilitation: Rehabilitation Options for Patients with Dizziness and Imbalance. American Speech-Language-Hearing Association. http://www.asha.org/aud/articles/vestibularrehab. Accessed March 2015.
Wells E, Goodkin H, Griesbach G. Challeneges in Determining the Role of Rest and Exercise in Management of Mild Traumatic Brain Injury. J Child Neuro. 2015: 1-7.