Computed Tomography of Facial Fractures€¦ · Describe the role of CT imaging in patient...
20
523CT RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5 CE Directed Reading F acial skeletal fractures are com- mon, and severe cases usually result from motor vehicle acci- dents, interpersonal violence, sports, or accidental falls. Precise visual- ization of the location, magnitude, and extent of fractures provides clinicians with a clearer picture of likely complica- tions and associated soft-tissue or senso- ry system damage, as well as details needed to plan surgical interventions. 1 There are alternative imaging modalities for assessing facial trauma, but multide- tector computed tomography (MDCT) imaging has become the standard choice for quick and accurate assessment of head and face trauma. This modality has revolutionized the detection and assess- ment of complex fracture patterns and the prediction of complications associat- ed with specific types, locations, and patterns of fractures. CT or MDCT of the face, head, and neck are now routine imaging examinations for patients with severe facial trauma. 1-4 Although MDCT offers superior visualization of fractures and other trauma associated with high-velocity impact injuries to the face and head, it is not superior to other imaging modalities for assessing minor damage to bones such as minimally displaced nasal bone fractures. In such cases, and particularly for children, MDCT is not recommended because of its relatively high radiation doses. The bones of children are not just smaller versions of the adult bones. Because of differences in the biology of bones, craniofacial morphology, and risk behaviors throughout the human lifespan, the patterns and associations of facial fractures vary importantly with age. Epidemiology Facial fractures account for more than 407 000 emergency department visits per year, representing nearly $1 billion a year in medical costs, with After completing this article, the reader should be able to: Summarize the skeletal anatomy of the face. List some leading causes of facial fractures. Explain the differences between children’s and adults’ facial skeletons and how facial fracture patterns change with age. Describe the role of CT imaging in patient assessment. Identify various types of facial fractures, including complex facial skeletal trauma and associated complications. Compare systems for classifying the severity of facial fractures. Discuss treatment techniques. Facial skeletal fractures are common, potentially serious, and frequently associated with other life-threatening conditions, such as traumatic brain injuries. Facial fractures can be simple or complex and sometimes involve serious complications. Computed tomography has revolutionized the rapid and precise assessment of craniofacial and neck fractures in patients with severe facial trauma. This article introduces readers to the epidemiology, skeletal anatomy and biomechanics, complications, and diagnostic imaging of facial fractures. In addition, this article describes efforts to develop and validate a quantitative scoring system for facial fracture severity and reviews treatment strategies for facial skeletal fractures. Bryant Furlow, BA Computed Tomography of Facial Fractures This article is a Directed Reading. Your access to Directed Reading quizzes for continuing education credit is determined by your membership status and CE preference. This symbol indicates that there is more content in the online version of this article.
Transcript of Computed Tomography of Facial Fractures€¦ · Describe the role of CT imaging in patient...

523CTRADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
CEDirected Reading
Facial skeletal fractures are com-mon, and severe cases usually result from motor vehicle acci-dents, interpersonal violence,
sports, or accidental falls. Precise visual-ization of the location, magnitude, and extent of fractures provides clinicians with a clearer picture of likely complica-tions and associated soft-tissue or senso-ry system damage, as well as details needed to plan surgical interventions.1 There are alternative imaging modalities for assessing facial trauma, but multide-tector computed tomography (MDCT) imaging has become the standard choice for quick and accurate assessment of head and face trauma. This modality has revolutionized the detection and assess-ment of complex fracture patterns and the prediction of complications associat-ed with specific types, locations, and patterns of fractures. CT or MDCT of the face, head, and neck are now routine imaging examinations for patients with severe facial trauma.1-4
Although MDCT offers superior visualization of fractures and other trauma associated with high-velocity impact injuries to the face and head, it is not superior to other imaging modalities for assessing minor damage to bones such as minimally displaced nasal bone fractures. In such cases, and particularly for children, MDCT is not recommended because of its relatively high radiation doses.
The bones of children are not just smaller versions of the adult bones. Because of differences in the biology of bones, craniofacial morphology, and risk behaviors throughout the human lifespan, the patterns and associations of facial fractures vary importantly with age.
EpidemiologyFacial fractures account for more
than 407 000 emergency department visits per year, representing nearly $1 billion a year in medical costs, with
After completing this article, the reader should be able to:Summarize the skeletal anatomy of the face. List some leading causes of facial fractures. Explain the differences between children’s and adults’ facial skeletons and how facial
fracture patterns change with age. Describe the role of CT imaging in patient assessment. Identify various types of facial fractures, including complex facial skeletal trauma and
associated complications. Compare systems for classifying the severity of facial fractures. Discuss treatment techniques.
Facial skeletal fractures are common, potentially serious, and frequently associated with other life-threatening conditions, such as traumatic brain injuries. Facial fractures can be simple or complex and sometimes involve serious complications. Computed tomography has revolutionized the rapid and precise assessment of craniofacial and neck fractures in patients with severe facial trauma. This article introduces readers to the epidemiology, skeletal anatomy and biomechanics, complications, and diagnostic imaging of facial fractures. In addition, this article describes efforts to develop and validate a quantitative scoring system for facial fracture severity and reviews treatment strategies for facial skeletal fractures.
Bryant Furlow, BA
Computed Tomography of Facial Fractures
This article is a Directed Reading. Your access to Directed Reading quizzes for continuing education credit is determined by your membership status and CE preference.
This symbol indicates that there is more content in the online version of this article.

CEDirected Reading
RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Computed Tomography of Facial Fractures
524CT
an average hospital stay of 6 days and hospitalization costs of $62 414, according to a nationwide database study published in 2011.5 Advances in diagnostic imaging—particularly the widespread adoption of MDCT capable of visualizing occult injuries to facial bones, sinuses, and soft tissues—have improved detec-tion of injuries that are frequently not apparent on clinical examination.6
The average age of facial fracture patients is 38 years, and men represent 68% of cases.5 Advances in automo-bile safety, including laminated windshields, seatbelts, and airbags, have reduced vehicular accident mortality rates and injuries to the eyes, the bones around the eyes, and the temporomandibular joints (TMJs).7
Particularly among adolescent boys and young men, interpersonal violence is a common cause of facial fractures.5,8 Alcohol consumption plays a major role in interpersonal violence resulting in facial fractures.8,9 Alcohol-involved interpersonal violence also is associated with more severe facial skeletal injuries than nonalcohol-associated violence. The relative risk of required surgical treatment was 60% higher when alcohol was involved in violence, according to a 2012 prospective British study.9
Midface fractures are commonly associated with accidental falls, particularly among elderly people.10 Horseback riding falls also are associated with midface fractures.11 Dog-bite injuries, especially among young children, can result in fractures of the nasal bones, orbital bones, cheek bones, and mandible; any dog attack involving bites to the face is an indication for diagnostic imaging to detect facial fractures.12
Workplace accidents resulting in facial fractures are more common among men and tend to be associated with construction jobs; falling objects at construction sites are associated with skeletal fractures in the mid-face and mandible.13
Facial fractures frequently are associated with soft-tissue and other skeletal trauma. When this trauma involves regions other than the face and head, it typi-cally reflects complex external blunt forces related to the cause of the injury, such as high-velocity automobile accidents or falls from heights that can cause multiple and widespread potentially life-threatening injuries, a condition called polytrauma.6,14 For example, patients with facial fractures sometimes also present with pul-monary and limb bone injuries.14,15
Not surprisingly, the same external blunt forces that fracture facial bones also frequently cause serious soft-tissue damage elsewhere in the face and head, either directly or indirectly. Associations have been identified that follow predictable patterns, reflecting the transmis-sion of external forces throughout the body during cer-tain types of impacts.7 Knowing about such associations can help clinicians look for injuries that are not initially obvious.7 For example, facial fractures in severe trauma patients frequently are associated with other traumatic head, brain, and upper cervical spinal injuries.5,7,15,16 Cervical spinal fractures accompanying upper midface fractures typically occur at lower levels of the cervical spine than cervical injuries that accompany mandibular fractures, which tend to be higher on the cervical spine.7
Dental injuries are another common association, affecting 15% of adult patients with facial fractures.6 Tooth trauma is most frequently seen in association with mandibular fractures.17
Despite the widespread belief that patients with facial fractures but no clinically obvious neurological abnormal-ities do not have severe intracranial hemorrhaging, a 2008 case-control study in Austria found that normal neuro-logical examination findings cannot independently rule out intracranial hemorrhage among patients with facial fractures. This is especially true in the presence of vomit-ing, nausea, or seizures.18 “In many cases, facial fractures distract attention from more critical, often life-threatening injuries,” the study’s authors warned.18
Complications arising directly from facial fractures also are common. Even simple nasal and mandible frac-tures, as well as complex midface trauma, can lead to significant blood loss.7 TMJ damage can make it painful and difficult to open one’s mouth or to chew. Fracturing or displacement of bones can cause shearing, herniation, or displacement of nerves, the eyes, and other soft tis-sues. Lateral blows to the face can, in rare cases, cause blindness or severe visual impairment.19 Extensive facial trauma and associated bleeding and swelling can compromise airways. Fractures to the bones that make up the orbital cavities can result in damage to the optic nerves or blood vessels, causing blindness or herniation of the globe (eye); zygomatic bone fractures can cause fractures to the orbital f loor, displacing the globe.7 Infection also can result from facial fractures and asso-ciated trauma.

CEDirected Reading
525CTRADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Furlow
Epidemiology of Pediatric vs Adult Facial FracturesOverall, facial fractures are less frequent among
children than adults.20 However, they tend to be more severe in children when they do occur. Head trauma in general is the leading cause of death from injury among children in the United States.20 According to a 2008 analysis of data from 277 000 pediatric patients from the National Trauma Data Bank, the leading causes of facial fractures among children were automobile acci-dents (55%), violence (12%), and falls (9%).20
Half of injuries resulting from child physical abuse involve the head and neck, although facial fractures are rare in abuse cases, representing less than 3% of cases.21,22 Physical trauma to the head and neck should be considered evidence of possible chronic child abuse when accompanied by signs of malnutrition, missing or broken teeth, fractures at different stages of healing, bruises, hand and object imprints, abrasions, or burns.22
The greater plasticity of children’s bones means they are more resistant to fracture than are adult bones, on average.17 Facial fracture–associated dental injuries are more severe, extensive, and common among children than among adults, affecting 29.5% of children with facial fractures due to automobile accidents or falls from heights.17 This is likely related to the greater forces nec-essary to cause facial fractures in children than adults. When researchers study children with facial fractures, they are almost by definition studying a patient popula-tion that experienced high-magnitude forces.17 Nearly one-third of children who receive a facial fracture diag-nosis simultaneously receive a concussion diagnosis, and a concomitant cranial fracture more than doubles the risk of concussion.23
Facial Skeletal Anatomy The skeleton of the head consists of 44 bony ele-
ments that fuse during early development to form the cranium (also known as the vault or braincase), the skull base, and the facial skeleton. The mandible connects to the skull at the TMJs. The rest of the bones of the head are fused or sutured together. During early devel-opment, the bones of the braincase and face emerge from 2 distinct embryonic tissues and are referred to as the neurocranium (vault) and viscerocranium (facial skeleton).24,25 The vault consists of 8 sutured bones that contain and protect the brain and brain stem from
external blunt forces. The skull base separates the brain from facial anatomies; its 5 bones are subdivided into anterior, middle, and posterior zones or regions.25
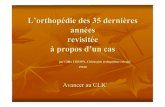
The human facial skeleton is composed of at least 14 interconnecting bones, not including the teeth, depending on how these fused bones and their sutures are delineated and counted. These include the frontal bone, nasal bones, temporals, sphenoidals, lacrimals, zygomatics, ethmoids, maxilla, vomer, and mandible (see Figure 1). These bones and their sutures repre-sent more than 180 anatomic contours and features, including crests, plates, spines, canals, arches, processes, and other structures. Together the structures form a complex scaffolding for muscle attachments and the functional units of the face, namely the eyes, upper respiratory airways (eg, the nasal cavity), the teeth, and the mouth.2,25
Interconnecting facial skeletal buttresses connect the face to the skull base, transferring and withstand-ing chewing and biting forces and external compressive forces to protect soft tissues, nerves, and the underlying sinus structures (see Figure 2).1 Within the network of buttresses are very thin bony sinus cavities. The surfaces of these intricately contoured air-containing skeletal cavities are covered with respiratory epithelial tissue. Among other functions, they moisten air inhaled through the nose.
Unlike facial skeletal buttresses, the delicate sinuses are not resistant to external blunt forces and have been
Figure 1. Bones of the human face. ©2010 ASRT. All rights reserved.
Nasal bone
Maxilla
Temporal boneLacrimal boneEthmoid bone
Sphenoid bone
VomerZygomatic bone
Mandible
Frontal bone

CEDirected Reading
RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Computed Tomography of Facial Fractures
526CT
likened to a “crumple zone.” Once crushed, they distort the shape and function of the face.7 The hypothesis that sinuses might function to reduce or prevent the transmis-sion of external forces through the face to the brain, simi-lar to engineered vehicle crumple zones, is controversial.7 For example, little evidence demonstrates that patients with only facial fractures experience less severe brain injuries than patients who have only skull injuries.7,26
The normal skeletal anatomy of the face frequently is classified into upper, middle, and lower partitions (see Figure 3).1 The upper facial skeleton includes the frontal bone and the frontal sinuses, encompassing the forehead down to the upper edges of the orbital cavity rims.1 The mandible or jawbone represents the lower facial skeleton. Between the 2 is the midface skeleton, which extends downward from the superior orbital rims and orbits and includes the nasal cavity and associated sinuses.1,27
The Midfacial SkeletonThe skeletal middle face includes the orbital cavities;
nasal cavity; and the maxillary, ethmoid, and sphe-noid—or midface—sinuses.1
The midface’s orbital cavities, or orbits, are conical spaces that contain the eyes and associated vasculature and nerves. The bony roof of the orbits includes the thick frontal bone. The curved inner medial and lateral walls of the orbits join the walls of adjacent sinuses.27 The thin bones of the maxillary sinus roof also function as a f loor for the orbits; blood vessels and nerves are situ-ated in canals and grooves that pass through the orbital f loor.27 Whereas the bone of the maxillary sinus roof is thin and relatively weak, other portions of the orbital walls and external rims, which are made up of thicker maxillary and zygomatic bones, are strong and more protective of the eyes.27 Between the orbits, the nasal
Figure 2. System of facial skeletal buttresses. Three-dimensional computed tomography (CT) images of an adult skull in frontal 3-D surface-rendered (A) and lateral oblique (B) orientations with color overlays show the superficial aspects of the horizontal and vertical facial skeletal buttresses and (in B) the sites of potential complications of fractures involving each buttress. The horizontal buttresses are the upper transverse maxillary (light green), lower transverse maxillary (green), upper transverse mandibular (gold), and lower transverse mandibular (purple) buttresses. The vertical buttresses are the medial maxillary (red), lateral maxillary (blue), posterior maxillary (magenta), and posterior vertical mandibular (purple) buttresses. Reprinted with permission from Winegar BA, Murillo H, Tantiwongkosi B. Spectrum of critical imaging findings in complex facial skeletal trauma. Radiographics. 2013;33(1):3-19.
A B

CEDirected Reading
527CTRADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Furlow
skeleton is made up of symmetrically paired nasal bones and the bony nasal septum situated between the maxilla and frontal bone and anterior to the nasal cavity.28
The curved zygomatic arches or processes are sym-metrically paired bones on the right and left halves of the face. The name of these bones was derived from zygoma, the Greek word for yoke, alluding to their function in keeping the eyes contained within the orbits.
Attached to the zygomatic processes are paired right and left maxillae, each of which represents 2 fused bones that create the palate or roof of the mouth, the nasal f loor and lateral walls, and orbital walls.25,27 The maxillae cover the region between the lower base of
the nostrils and the upper teeth and extend upward between the nose and the lower and inner edges of the orbits.
The Facial Skeletal ButtressesThe 8 paired skeletal buttresses of the face are regions
of increased bone thickness that support muscles, eyes, teeth, and the uppermost airways (see Figure 4).1,2
There are 4 paired vertical facial skeletal buttresses and 4 transverse buttresses, creating a cagelike array of thickened facial bones. All of the buttresses are linked, directly or indirectly, to the other buttresses, influenc-ing the transmission of external forces throughout the facial skeleton.2
Not surprisingly, the buttresses’ anatomy often is an important factor in treatment planning for facial fractures.2 For example, because of their increased bone thickness, buttresses are frequently sites of metal screw fixation during surgery for facial fractures.2
Sometimes, because the right- and left-face transverse buttresses meet in the midface to create a continuous buttress, they are referred to in the singular (eg, upper transverse mandibular buttress), whereas vertical but-tresses usually are referred to in the plural (eg, right and left buttresses). However, because all buttresses,
Figure 4. Illustration of an adult skull depicting the 4 paired ver-tical buttresses and 4 transverse buttresses, all of which exist in areas of the facial skeleton with relative increased bone thickness. Reprinted with permission from Hopper RA, Salemy S, Sze RW. Diagnosis of midface fractures with CT: what the surgeon needs to know. Radiographics. 2006;26(3):783-793.
Figure 3. Three-dimensional surface-rendered CT image of an adult skull with color overlays shows partition of the facial skeleton into upper (red), middle (blue), and lower (light green) thirds. This system is used by otolarynglogists to describe locations of fractures in the facial skeletal anatomy. Reprinted with permis-sion from Winegar BA, Murillo H, Tantiwongkosi B. Spectrum of critical imaging findings in complex facial skeletal trauma. Radiographics. 2013;33(1):3-19.

CEDirected Reading
RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Computed Tomography of Facial Fractures
528CT
whether vertical or transverse, are in reality paired and symmetrical features, the plural is used throughout this article.
Pediatric Facial Skeletal AnatomyThere are marked differences in the neuroanatomy
and facial skeletons of adults and children that affect patterns of facial skeletal trauma in these 2 popula-tions.20 Children’s underdeveloped facial skeletons are composed of less ossified, more f lexible bones than adult bones, with lower ratios of rigid cortical bone to interior cancellous (“spongy”) marrow-containing bone.20,29 This can lead to so-called green-stick or incomplete fractures in children. Although unerupted teeth in young children’s maxillae and mandibles might give those structures somewhat greater resistance to external compressive forces compared with older patients, the mandibles and other bones of children have a thinner cortex, leaving them less resistant, over-all, to fracture.20
In addition, the morphology of children’s skeletons is very different from adults; children have a larger cranium-to-face ratio and smaller, f latter midfaces and mandibles.21,29 The bony orbits represent a much larger proportion of children’s faces than adults’ faces, and children’s midfaces are relatively smaller. As a result, the midface fractures common among adolescents and adults are relatively rare among children.29
Children’s sinuses have fewer air cavities than those of adults.29 The sinuses mature slowly throughout child-hood and adolescence. Maxillary sinuses mature first, at tooth eruption. Ethmoid sinuses mature next, at puberty. The frontal sinuses mature in adulthood (see Figure 5).29
Facial Skeletal Trauma and Fracture Types
Facial fracture patterns reflect the location, direc-tion, and magnitude of traumatic forces.27 When forces are severe, the extent of underlying facial skeletal trauma is not always readily discernable from a visual assessment of external facial trauma.27 Midface frac-tures are common and frequently involve occult, serious soft-tissue damage; their management requires careful diagnostic imaging of the facial skeletal buttresses and soft tissues.2
CT imaging allows reconstruction of 2-D and 3-D images from multiple angles, thus allowing visualization of even subtle fractures that would be missed with tra-ditional radiography.2 Predicting clinical complications and planning treatment and surgery require a complete set of images and an understanding of the clinical asso-ciations of common facial fracture patterns.2
Pediatric Facial FracturesA common refrain in the facial fracture literature is
that “children are not just little adults.”21,30 The anatomic and biological differences between the facial skeletons of adults and children of different ages lead to distinct patterns of fractures, associated trauma, and brain involvement. These differing patterns create distinct management challenges.
Overall, pediatric fractures most frequently involve nasal trauma (50% of cases) and mandibular fractures ( 49% of cases).21 However, facial fracture patterns vary with the stage of craniofacial development and maturity.31
Children’s facial fractures are associated with higher mortality and morbidity rates.17,20 Children who sustain
Figure 5. Illustration depicting the development of the frontal and maxillary sinuses according to age in years. Increasing develop-ment of the paranasal sinuses is positively correlated with the prevalence of midfacial fractures in children. The sinuses reach their full size after puberty is complete. Reprinted with permission from Alcalá-Galiano A, Arribas-Garcia IJ, Martín-Pérez MA, Romance A, Montalvo-Moreno JJ, Juncos JM. Pediatric facial fractures: children are not just small adults. Radiographics. 2008;28(2):441-461.

CEDirected Reading
529CTRADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Furlow
facial fractures are significantly more likely to expe-rience traumatic brain injury, skull base fractures, cranial vault fractures, cervical spinal fractures, eye injuries, and facial soft-tissue injuries than are children who have traumatic injuries without facial fractures.20 Approximately 32% of children with facial fractures have a concomitant concussion, and the risk of concus-sion is doubled among children who sustain both facial and cranial fractures.23 Pediatric facial fractures are therefore an indication for concussion screening and neuroimaging.23
The nature of facial fractures changes with age throughout childhood.20 For example, midface fractures are more common among toddlers and infants than adolescents, while mandibular fractures are more com-mon among teens than young children.17 The orbits rep-resent a larger proportion of children’s faces than adults’ faces, and the frontal sinuses are immature. Together, these factors mean that the bony orbits are a common site of pediatric facial fractures.29 Blow-in superior orbit-al fractures are seen more often among younger chil-dren, whereas in later years, children are more likely to sustain fractures to the bones that make up the orbital f loors.29 Green-stick “trap-door” facial fractures of the
bony orbits can leave a bone fragment connected by a “hinge” to the orbital f loor, with the fragment initially protruding into the sinus (leading the eye to prolapse into the gap), and subsequently snapping back into place in a manner that entraps eye tissue in a prolapsed position (see Figure 6).21
Because children’s immature sinuses have fewer air cavities, frontal sinus fractures are relatively rare in children and tend to be associated with higher-velocity forces than the forces necessary to fracture adults’ fron-tal sinuses.29 When frontal sinus fractures do occur in children, they are frequently associated with severe and serious soft-tissue trauma, such as cerebrospinal f luid leaks and traumatic brain injuries.29
Sinus FracturesFrontal sinus fractures result from high-velocity
blunt trauma to the upper face. These fractures have become less frequent with the advent of automobile airbags.3 However, they still represent up to 15% of all facial fractures, are frequently accompanied by other craniofacial fractures, and can be fatal.32 The presence of frontal sinus fractures calls for careful neuroimaging assessment for traumatic brain injury, pneumocephalus
Figure 6. A-C. Computed tomographic diagnosis of nasofrontal outflow tract injury as noted by frontal sinus floor fractures (arrows). This is one criterion used in the diagnosis of outflow tract injury. When outflow tract injuries allow access to the brain vault, meningitis or brain infection can occur. C. A trap-door facial fracture (arrow). Reprinted with permission from Stanwix MG, Nam AJ, Manson PN, Mirvis S, Rodriguez ED. Critical computed tomographic diagnostic criteria for frontal sinus fractures. J Oral Maxillofac Surg. 2010;68(11):2714-2722.
A B C

CEDirected Reading
RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Computed Tomography of Facial Fractures
530CT
(the presence of air in the cranial vault), and facial imag-ing for other facial fractures.3,32
Because of MDCT’s precision, surgical interven-tions have become less frequent while monitoring with diagnostic imaging has become more common.3,32
Nevertheless, frontal sinus fractures can require quick surgical intervention, especially when they involve trauma to the nasofrontal outflow tract, which can become a conduit for infectious agents into the brain (see Figure 7). Closing this conduit to the brain in some cases requires surgical obliteration of the naso-frontal outflow tract, in addition to internal fixation of the fractured sinus.3,32 Pneumocephalus is an indication of severe injury and requires surgical intervention.3 Criteria for CT-based diagnosis of nasofrontal outflow tract injuries include fractures of the sinus f loor or the anterior or posterior table or obstruction of the outflow tract. Fractures of the anterior or posterior table are present in up to 91% of patients with outflow tract inju-ries.32 Fractures of the sinus f loor are identified in only 9% of patients with this type of injury.32 The presence of any one of these criteria carries up to a 300% increased likelihood of brain injury or other facial fractures.32 Anterior and posterior assessments include the degree of displacement associated with any fractures.3
Nasal FracturesNasal bones are more exposed than other facial
bones, and nasal fractures are the most common form of facial trauma, although in most cases these fractures result in minor displacements that can be readily reduced without open surgery or even radiography.28
Nasal bone fractures result from external blunt forces that impact the nose anteriorly or laterally.1 Type 1 nasal fractures involve trauma to, and displacement of, the anterior spine and bridge of the nose but do not involve the nasal septum; type 2 fractures also involve the septum.1 Type 3 nasal fractures are more serious and involve the bony orbits and other bone in addition to the nasal structures affected by type 1 and type 2 nasal fractures.1 Complications associated with type 1 fractures usually are merely aesthetic, but type 2 and 3 nasal fractures can lead to impaired nasal breathing. Clinical assessment is the norm for type 1 and 2 trau-ma, whereas imaging is indicated to evaluate suspected type 3 fractures.28
Orbital FracturesThe orbits and orbital rims are complex skeletal struc-
tures composed of surrounding bones and buttresses.28 Fractures of the orbital walls can be localized and simple, or they can be complex fractures extending beyond the orbits, such as those extending into or through the orbital rims. Both simple and complex orbital fractures can affect the position and integrity of the eyes, eye muscles,
Figure 7. CT images of the skull of an unrestrained passenger in a motor vehicle involved in a head-on collision with another vehicle. The patient has simultaneous anterior-posterior displaced fracture, axial image (A) and 3-D surface-rendered reconstruction (B). The patient meets all criteria for nasofrontal outflow tract injury, a risk factor for serious infectious complications: fracture of the floor (C, arrow) and (D) fracture of the anterior ethmoid cells (black arrow) and frank obstruction (white arrow). Reprinted with permission from Stanwix MG, Nam AJ, Manson PN, Mirvis S, Rodriguez ED. Critical computed tomographic diagnostic criteria for frontal sinus fractures. J Oral Maxillofac Surg. 2010;68(11):2714-2722.
Click here in the online version of this article to view a table of facial fracture types and classifications.
A
C
B
D

CEDirected Reading
531CTRADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Furlow
or optic nerves.28 As the name implies, simple blowout fractures occur when fractures in the orbital wall extend outward into the sinuses. Blow-in fractures are less fre-quent and occur when fractured bone intrudes into the orbital space inhabited by the eye.28 Blowout fractures affecting more than half of the orbital floor increase the risk of enophthalmos, or the sinking of the eye from its normal anatomic position.28
Orbital blowout fractures are sometimes classified into 3 categories33: Type I – trap-door fractures. Type II – separated bone fragments surrounding
displaced soft tissue. Type III – displaced bone surrounding displaced
soft tissue.
Mandibular FracturesMore frequently seen among children than adults,
simple mandibular fractures usually are condylar or subcondylar, affecting the TMJ region (see Figure 8).21 Children typically sustain a single mandibular fracture, whereas adults more frequently sustain multiple fractures to the jawbone.21 Condylar fractures occur bilaterally 20% of the time.21 Mandibular fractures, like facial trau-ma in general, frequently involve dental trauma. This can be particularly severe among children.17 Jaw injuries are a common type of facial fracture in automobile accidents.34
Complex Facial FracturesComplex facial fractures frequently occur in predict-
able patterns and can result when the midface is sub-jected to high-velocity external blunt forces.1 Complex facial fractures are uncommon in children, representing less than 10% of all pediatric facial fractures.17 Complex fractures involving damage to multiple facial skeletal buttresses can partly or completely dissociate the midfa-cial skeleton from the skull and frequently require rapid assessment and surgical intervention to reduce and fix fractured bones in place.1 Common complex patterns of facial fractures frequently involve orbital walls and rims.28
Le Fort Fractures
These fractures are named for the French surgeon René Le Fort, who first described them in 1901 based on experiments involving numerous cadaverous human heads and wooden clubs.1,28 There are 3 types of Le Fort
fracture patterns, elements of which can overlap (see Figure 9). Le Fort fractures are classified by the site and extent of fractures, using coronal and axial 2-D CT images and 3-D surface renderings.2
Nasoorbitoethmoid FracturesNasoorbitoethmoid (NOE) fractures result from
high-velocity blunt forces to the nose or the upper mid-face, causing fractures in the region where the transverse maxillary buttresses meet the medial maxillary buttress-es.1,2 Patients with NOE fractures typically present with reduced nose projection from the face and abnormal protrusion of the eye or eyes.1 NOE fractures are differ-entiated from simple nasal fractures by confirmation of involvement of the orbital walls and ethmoid sinuses.1,2
The Manson classification system identifies 3 types of NOE fractures28,35: Type I – a large single-segment fracture in the
medial orbital rim. Type II – comminution (severe, complex fractur-
ing into multiple small fragments) of the medial orbital rim but without damage to the tendon.
Type III – comminution, as in type II, but with damage to the tendon.
Figure 8. Three-dimensional CT surface-rendered image with color overlays showing the parts of the mandible in lateral orientation: the alveolar process (magenta), parasymphyseal region (blue), body (red), angle (green), ramus (yellow), coronoid process (orange), and condyle (purple). Reprinted with permis-sion from Winegar BA, Murillo H, Tantiwongkosi B. Spectrum of critical imaging findings in complex facial skeletal trauma. Radiographics. 2013;33(1):3-19.

CEDirected Reading
RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Computed Tomography of Facial Fractures
532CT
Zygomaticomaxillary Complex FracturesDirect blunt trauma to a zygomatic arch or upper
transverse maxillary buttress can cause simple fractures limited to the zygomatic bone.1 Fractures that extend into the orbital wall, in contrast, are termed zygomatico-maxillary complex (ZMC) fractures.
The zygomatic and maxillary sinus bones repre-sent much of the f loors and lateral walls of the bony orbits.2 These ZMCs involve the upper transverse maxillary buttresses and the lateral maxillary vertical buttresses. ZMC fractures, also known as tetrapod1 or quadripod fractures, extend through 4 zygomatic bone sutures: the zygomaticofrontal, zygomatico-maxillary, zygomaticotemporal, and, posteriorally, the zygomaticosphenoid sutures (see Figure 10).1 However, ZMC fractures represent a class of fracture patterns, and not all ZMC fractures involve all 4 of these sutures.28
ComplicationsThe fracturing and displacement of facial bones can
cause nerve damage and compress or damage soft tis-sues, frequently in ways that can be predicted by visu-alization of skeletal trauma.1,27 For example, cerebrospi-nal f luid leaks frequently accompany fractures of the central sinus walls.27 Because of the anatomic location of the frontal sinuses, sinus fractures can provide infec-tious organisms access to the brain, potentially causing brain abscess or meningitis.32
Fractures in the orbital wall can have profound implications for patients’ visual acuity and quality of life. Lateral orbital wall fractures can injure the eye, eye muscles, and optic nerves.1 Superior orbital fissure syndrome and orbital apex syndrome (also known as Jacod syndrome) sometimes result, albeit very rarely, when lateral maxillary buttress fractures extend into or through the superior orbital fissure or the adjacent orbital apex.1,36 Signs of these syndromes include oph-thalmoplegia (eye muscle paralysis), eye muscle weak-ness, drooping of the upper eyelid, fixed dilation of the eye, bulging of the eyes, and hypothesia (loss of touch sensation) in the face, upper eyelids, or forehead.36
Large orbital f loor blowout fractures can cause enophthalmos, or the downward displacement of the eye.28 Eye muscle or globe tissue can herniate into blowout fractures. Soft-tissue herniation associated with orbital f loor fractures can contribute to diplopia (bilateral eye misalignment and resulting double vision) and can cause intraorbital edema and hemorrhage in the days following traumatic injury.33 However, when diplopia persists longer than a few days after an injury, soft-tissue herniation is a more likely culprit than edema or hemorrhage.33 Fractures near the orbital apex are uncommon but potentially serious when involving the optic nerve.28
Soft-tissue damage resulting from facial bone frac-tures can include hematoma and herniation, which can complicate visualization of focal injuries.27 Type 2 and 3
Figure 9. Illustrations of Le Fort fracture patterns, types I, II, and III, that depict the classic fracture patterns described by René Le Fort in 1901. A. The horizontal plane of the Le Fort I fracture extends between the pterygoid plates of the sphenoid bone to the piriform aperture and lateral nasal wall. B. Le Fort II fractures propagate from the pterygoid plates posteriorly, through the orbital floor, to the nasofrontal suture. In bilateral but not unilateral/partial cases, this gives rise to the classic “pyramidal” pattern. C. Craniofacial disjunction, or Le Fort III fracture, involving total separation of the midface structures from the cranial base. This level of fracture propagates from the pterygoid plates, through the lateral orbital wall (fronto-zygomatic suture) by the orbital floor, to the nasofrontal suture. Reprinted with permission from Susanne Loomis, MS, FBCA, of REMS Media Services, Imaging, MGH.
A B C

CEDirected Reading
533CTRADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Furlow
nasal fractures can sometimes cause septal hematomas, which are more common among children.28 They also can cause abscesses or perforation, which can compli-cate breathing.1 Accumulations of mucus in the lacrimal sac or paranasal sinuses, called mucoceles, are a common complication of nasofrontal and frontal sinus trauma. Preventing mucocele formation is an indication for frontal sinus surgery following NOE fractures.2
Because of their thicker bone, facial skeletal buttresses are more resistant to fracturing. Although greater force is required to fracture buttresses than other components of the facial skeleton, such fractures do commonly result from high-velocity impact injuries due to sports, interper-sonal violence, and, particularly, automobile accidents. When they do occur, buttress fractures commonly are associated with soft-tissue injuries, which frequently are serious.1 For example, fractures of one or both of the pos-terior maxillary vertical buttresses can cause TMJ disloca-tion.1 Fractures of the upper and lower transverse man-dibular buttresses can cause nerve damage that results in loss of touch sensation in the lower lip, chin, or the tip or anterior portion of the tongue.1
Upper transverse maxillary buttress fractures are associated with the orbital complications described previously, such as displacement or herniation of the eye or associated soft tissues, as well as potentially devastating ruptures of the globe, orbital hematoma, tears in the optic muscle, and superior orbital fissure syndrome.1 Deformities of the globe’s overall shape (eg, the “f lat tire” sign) are visible on CT images and indi-cate globe rupture and trauma to the entire eye, includ-ing the cornea and retina, which can cause blindness (see Figure 11).1
Medial maxillary buttress fractures, which can be either solitary fractures or complex Le Fort or NOE fractures, require careful CT image analysis for assess-ment and surgical planning because these injuries can endanger the eyes; vasculature associated with the eyes, such as the ethmoid arteries; and supporting soft tis-sue, such as the canthal tendons.1 Cerebrospinal leaks also can result from medial maxillary buttress fractures, and as with frontal sinus fractures, these injuries carry the risk of infection when fractures affect the paranasal sinuses. Meningitis and cerebral or epidural abscess can result.1 Damaged lacrimal (tear) ducts and sacs are sur-gically repaired to correct their inflammation.1
Figure 10. Zygomaticomaxillary complex (ZMC) fracture pat-tern before and after internal fixation. A. Three-dimensional CT image of an adult face in oblique orientation depicts a right ZMC fracture with a nondisplaced zygomaticofrontal suture (green arrow), mildly displaced zygomaticomaxillary suture (blue arrow), and comminuted and displaced zygomatic arch extending through the zygomaticotemporal suture (red arrow); the zygomaticosphenoid suture was involved but is not depicted. A nondisplaced fracture of the base of the right coronoid process (arrowhead) also is depicted. B. Three-dimensional CT image in the same orientation demonstrates fixation of the zygomatico-maxillary and zygomaticotemporal sutures with plates and screws in place. Reprinted with permission from Winegar BA, Murillo H, Tantiwongkosi B. Spectrum of critical imaging findings in com-plex facial skeletal trauma. Radiographics. 2013;33(1):3-19.
A
B

CEDirected Reading
RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Computed Tomography of Facial Fractures
534CT
NOE fracture patterns often are associated with pro-truding eyes, telecanthus (abnormal distance between the eyes caused by tendon injury), and cerebrospinal f luid discharge from the nose.1
Pediatric ComplicationsRelatively little research has been published on
complications associated with facial fractures in chil-dren, partly because of poor standardization of defini-tions and reporting criteria and standards for adverse events.30 But pediatric complications are important because children’s faces are still developing; fractures can subtly or profoundly alter craniofacial development and adult facial appearance and function and have life-long implications for patients’ quality of life.30
Researchers at the Children’s Hospital of Pittsburgh in Pennsylvania developed a simple qualitative clas-sification system that identifies 3 broad, nonmutually exclusive types of complications that result from pediat-ric facial fractures30: Type 1 – complications “intrinsic to, or concomi-
tant with the fracture itself,” such as the loss of permanent teeth.
Type 2 – complications associated with medical interventions, such as loss of nerve function after reduction and internal fixation of a fragmented mandible, or surgical scars.
Type 3 – complications stemming from growth and development after the fracture and medical
treatment, such as asymmetric growth of the mandible resulting from a condylar (TMJ-region mandibular) fracture.
This classification scheme is based on experiences at the researchers’ hospital, and they acknowledged that no classification system, including theirs, has been tested and validated with longitudinal studies of large popula-tions of patients over time.30
Type 1 pediatric complications include eye trauma, with some studies suggesting that up to 24% of children sustaining orbital midfacial fractures suffer nerve and globe damage leading to blindness.30 As among adults, fractures at the orbital apex are a risk factor for optic nerve damage.
Facial lacerations are commonly and unsurprisingly associated with facial fractures and can scar children’s faces for life. Septal hematoma following pediatric nasal bone fractures is a potentially serious type 1 complica-tion that can lead to necrosis and infection if not quickly evacuated.28 In addition, septal hematomas can lead to a long-term “saddle nose” disfigurement if not evacuated quickly.28 Tooth injuries also commonly accompany facial fractures, including root and crown fractures.30 Type 1 and type 2 pediatric complications of the sensory nerves of the face include alterations of taste and smell, as well as nerve palsies associated with cranial nerves.30 TMJ ankylosis (impaired jaw movement) sometimes occurs as a type 1 or type 2 pediatric complication fol-lowing mandibular fractures; it is rarely associated with prolonged maxillomandibular fixation.30
Among children who have sustained facial fractures, surgical reduction and fixation lead to complications in fewer than 5% of cases.30 These complications can include infection, bilateral facial asymmetry, or scarring.
Patients who have suffered pediatric facial fractures should undergo surveillance throughout childhood to detect TMJ ankylosis, tooth loss, and type 3 developmen-tal complications, including facial asymmetries stemming from aberrations in facial bone development and growth.30
Computed Tomography Imaging of Facial Fractures
Diagnostic MDCT has higher sensitivity for detect-ing midface fractures than conventional radiography. MDCT examinations should be undertaken following a facility’s written standardized trauma assessment
Figure 11. Ruptured globe in a 43-year-old man. Unenhanced axial CT scan shows the “ flat tire” sign, which indicates an open-globe injury. Reprinted with permission from Kubal WS. Imaging of orbital trauma. Radiographics. 2008;28(6):1729-1739.

CEDirected Reading
535CTRADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Furlow
procedures.37 Scans might be limited to the face or include the entire head, neck, and cervical spine for patients with suspected polytrauma with signs of facial trauma.37 Trauma patients undergoing brain CT who have clinically identifiable facial trauma should undergo CT imaging of the face and the orbits.7 Any patient with severe facial trauma should undergo CT imaging of the face, orbits, and brain.7
CT scan acquisition direction typically is cranio-caudal.37 With a 16- or 64-channel MDCT scanner, scan parameters are 120 kV tube voltage, 115 mA, a 0.9 pitch, narrow acquisition slice thickness (eg, 0.65 mm on a 64-channel MDCT scanner38) and a gantry rota-tion time of 1 second.37,39 Reconstruction of multiplanar coronal, sagittal, and axial images using bone and soft-tissue algorithms at 1.25-mm slice thickness is under-taken for image interpretation.37
Three-dimensional image reconstructions usually are produced.37 Both 3-D volume and surface-rendered MDCT images are useful in diagnostic imaging and surgical planning for high-energy (eg, complex) facial fractures because they precisely visualize the location and extent of fractures.39 Conversely, 3-D volume-rendered images frequently poorly visualize low-energy simple fractures involving no major bone displacement, such as simple type 1 nasal fractures.28,39
When clinical examination indicates that a nasal fracture involves minimal displacement and is not likely to be accompanied by other facial fractures (such as type 1 nasal fractures resulting from low-velocity external blunt forces), diagnostic imaging usually is not indicated, particularly for children and adolescents.28 However, when other facial fractures are suspected (eg, type 3 nasal trauma with significant displacement), imaging usually is undertaken to con-firm the presence and extent of nasal bone and other fractures and to plan nasal reduction to avoid aesthetic and functional complications.39 Lateral radiographs of the nose sometimes are still undertaken for this purpose but have poor sensitivity (as low as 53%) for fracture detection.28 MDCT has far better sensitiv-ity, but concerns have been raised about the relatively high radiation dose associated with this modality and whether it is medically justified for investigating nasal bone fractures, particularly when clinical examination
suggests minimal fracture displacement.28,39 Because of the long-term hazards posed by radiation, unnecessary CT of the head and face should be avoided, particular-ly with children, in keeping with the as low as reason-ably achievable (ALARA) principle. Ultrasonography can be used as a nonionizing alternative to CT for confirming and characterizing lateral nasal wall frac-tures in children.39
When a nasal fracture is to be assessed in the course of CT imaging for other possible facial fractures or because the nasal fracture has caused significant dis-placement, however, MDCT sagittal multiplanar recon-struction images appear to offer better diagnostic preci-sion than axial CT images alone, particularly when used alongside axial images.39
CT is necessary for orbital fracture surgery planning to assess entrapped tissue positions, muscle anatomy, and fracture displacement.40 As is the case with other midface MDCT imaging applications, thin-section multiplanar images are used to evaluate orbital frac-tures. Orbital fractures are common in cases of midface trauma, including NOE and ZMC fractures. NOE fractures most frequently affect the medial orbital wall; ZMC fractures tend to occur in the orbital f loor and lateral wall.40 Le Fort type III craniofacial dissociation fractures affect the medial and lateral orbital wall and the posterior portion of the orbital f loor.40 Most orbital fracture planning images are 2-D reconstructions. Axial CT reconstructions are prepared for medial wall frac-tures to confirm increased orbital volume and enoph-thalmos and to visualize muscle entrapment by blow-in or blowout fractures.40 Two-dimensional CT images can be reconstructed to visualize fractures of the external orbital wall and orbital apex, the presence and exact locations of bone fragments, and the location of the optic nerve and any compression of the optic nerve by displaced portions of the fracture or fragments.40 Evidence of optic nerve involvement is an indication for emergency surgery to prevent blindness.40 Orbital roof fractures are assessed with 2-D axial and coronal reformatted CT images that visualize comminuted fractures of the frontal sinus; indications for referral to neurosurgery include orbital roof fractures associated with pneumocephalus, cerebrospinal f luid leaks, or hematomas within the cranial vault.40

CEDirected Reading
RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Computed Tomography of Facial Fractures
536CT
Soft-tissue wounds within the orbits, including laceration of the cornea, damage to the globe, and bleeding within the orbits, also can be assessed using MDCT imaging to confirm clinical and ophthalmologic examinations.40 Open-globe injury (ruptured eye) is indicated by changes in the external contour and volume of the affected eye (the “f lat tire” sign) and the presence of bone fragments or hyperdense foreign materials within the body of the orbits.40 (CT is sensitive in the detection of metal and bone, but glass and wood fragments might not be well visualized.40) Ocular lacerations cause f luid accumulations.40
As noted above, cerebrospinal f luid leaks, telecanthus, and optic nerve injury are complications of medial maxillary buttress fractures; these can be detected with coronal and axial CT reconstructions.1 Orbital apex fractures frequently are an indication for immediate surgical intervention.28
Suspected orbital trauma among children should be evaluated carefully for possible trap-door fractures in the orbital f loor, which can ensnare soft tissues and reduce the range of eye movement and function.28,33 When the bone has snapped back into place and trapped soft tissue, the only sign of a trap-door fracture is likely to be the snared soft tissue, such as optical muscle.28 Even in the absence of trap-door fractures, orbital f loor fracture and associated soft-tissue herniation are risk factors for diplopia. Larger fractures are more likely than medium or small fractures to cause diplopia.33 This non–trap-door orbital f loor fracture and herniation is seen in adults and can be detected on CT as multiple contact points between the eye muscle and the edge of the fracture.33 When orbital f loor fractures and soft-tissue herniation are not confirmed by CT, diplopia might be due to eye muscle or optic nerve injury.33
Injury Severity ScoresSeveral authors have proposed maxillofacial trauma
severity scores to replace local and regional descriptions of facial fractures and fracture patterns, to standardize currently qualitative and somewhat subjective descrip-tions of trauma severity, and to facilitate more uniform standards of care.41 No single test has gained universal acceptance or widespread use for guiding facial trauma
treatment, but proponents argue that such scores might prove to be valuable prognostic tools.41 The 4 validated scoring systems for complex craniofacial fractures are described in the Box.
Using multiplanar 2-D reformations and 3-D render-ings of archived CT data for 119 patients with facial trauma, British researchers tested all 4 severity scoring systems to develop a new proposed maxillofacial trauma scoring system called the ZS Scoring System.41 Only the proposed ZS model successfully discriminated between varying levels of trauma, the authors reported.41 This is likely in part because the 4 existing trauma scales did not sufficiently weight more severe fractures (assigning them a large enough number compared with less severe frac-tures).41 For example, the ZS score heavily weights bone fracture comminution and scores dental trauma, making it a more sensitive measure of high-velocity trauma.41
However, existing systems have other limitations. For example, the Maxillofacial Injury Severity Score scale does not include frontal or orbital fractures.41
Treatment of Facial FracturesSimple nasal fractures frequently are reduced
through nonsurgical manipulation.7 More serious facial trauma is triaged into 3 broad categories7:
Box
Validated Scoring Systems for Complex Craniofacial Fractures41
Facial Injury Severity Score – assigns weighted numerical scores for different fractures, the sum of which represents the final score.
Maxillofacial Injury Severity Score – assigns numerical scores to malocclusion, limited mouth opening, and magnitude of facial deformity, using components from the Abbreviated Injury Scale 1990, with predefined weighting of scores that assigns higher numbers, for example, to Le Fort III fractures than to isolated mandibular injuries.
Cooter and David Score – grades fractures on a scale of 0 to 3 for each of 20 craniofacial skeletal zones.
Facial Fracture Severity Score – similar to the Cooter and David Score system, the Facial Fracture Severity Score assigns numerical severity scores to 41 facial skeletal anatomies, the sum of which represents the final score.

CEDirected Reading
537CTRADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Furlow
Fractures or other injuries requiring immediate intervention to save the patient’s life or eyesight. Identifying these fractures might require immedi-ate CT scanning, particularly if injuries are sus-pected that could threaten the patient’s eyesight. High-speed MDCT allows single-scan acquisition of facial, skull base, intracranial, neck, and other anatomies, avoiding repeat imaging examinations and delayed care.7
Wounds requiring treatment within a few hours, such as contaminated wounds. These injuries are addressed once the patient has been stabilized.
Injuries that can wait 24 hours or more, if neces-sary, in the judgment of the clinician.
The third category includes definitive reduction and fixation of complex facial fractures, but the timing of these interventions is not widely agreed upon.7 No opti-mal time to repair has been identified, in part because no simple rule applies to complex patterns of facial trauma.7 Traditionally, such interventions were postponed until acute brain injuries and swelling had subsided, but in recent years, many hospitals have begun “early and total repair of facial injuries” within days of, or even on the day of, a patient’s admission to the emergency department.7
To minimize surgical scarring, internal reduction and fixation of mandibular and most midface trauma involves small skin incisions or surgical access through the mouth.7 Transoral miniplates and screws can be placed through the mouth or a very small transbuccal cheek incision.7 Orbital fixation often can be achieved transcutaneously through the lower eyelid or transconjunctivally.7
Endoscopy commonly is used for TMJ arthroscopy and treatment of condylar fractures as well as some isolated frontal sinus, orbital f loor, and zygomatic arch fractures.7
With more extensive or complex patterns of facial fractures, a coronal scalp f lap allows complete surgical access to and visualization of the upper face but carries a risk of nerve injury, diplopia, telecanthus, and scalp necrosis.7 Midface fractures might be accessed through a midfacial “degloving” procedure, an intraoral surgi-cal exposure of the anterior mandible.7 Traditionally, load-bearing plates have been used for fracture fixation, when buttresses such as mandibles allow implantation with screws.7 Miniplates can replace the temporary
larger plates, and unlike large traditional plates, mini-plates do not require removal later.7 Even smaller microplates and tiny screws have been developed for use with the orbital rim, nasal bones, and frontal sinus.7
Fixation with titanium pins and plates can restrict bone growth in pediatric patients, complicate imaging, and present long-term local biological hazards, such as possible carcinogenicity. Alternative biological absorb-able fixation device materials are in use, but questions have been raised about their safety.42 Absorbable mate-rial devices appear overall to involve a 20% higher com-plication rate than titanium among patients treated for maxillofacial fractures, according to one recent study.42
Conclusion Facial fractures are a common form of trauma and fre-
quently occur in complex patterns predictably associated with some types of soft-tissue damage and clinical compli-cations. Accurate classification of facial fractures is key to successful medical management.
MDCT has revolutionized the diagnostic assess-ment of facial trauma and associated head and neck injuries, allowing rapid acquisition of precise diagnos-tic images in a single examination that spares trau-matized patients repeated imaging examinations and allows more rapid and better informed treatment plan-ning. MDCT provides clinicians the accurate spatial information they need for successful surgical interven-tion, as well as information to help avoid unjustifiable interventions.
As always, however, the benefits of imaging must be balanced against the inherent risks of ionizing radiation, particularly for children. The ALARA principle must be observed for all patients. Simple, minimally displaced nasal fractures without other facial trauma, for example, are rarely an indication for MDCT examinations.
New Mexico–based medical writer and health care journalist Bryant Furlow, BA, is a regular contributor to Radiologic Technology, The Lancet Oncology, and other medical journals and medical news outlets. In addition to medical research and diagnostic imaging, he covers health care in rural and tribal communities.

CEDirected Reading
RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Computed Tomography of Facial Fractures
538CT
Reprint requests may be mailed to the American Society of Radiologic Technologists, Communications Department, 15000 Central Ave SE, Albuquerque, NM 87123-3909, or e-mailed to [email protected].
© 2014 American Society of Radiologic Technologists
References 1. Winegar BA, Murillo H, Tantiwongkosi B. Spectrum of
critical imaging findings in complex facial skeletal trauma. Radiographics. 2013;33(1):3-19. doi:10.1148/rg.331125080.
2. Hopper RA, Salemy S, Sze RW. Diagnosis of midface fractures with CT: what the surgeon needs to know. Radiographics. 2006;26(3):783-793. doi:10.1148/rg.263045710.
3. Echo A, Troy JS, Hollier LH. Frontal sinus fractures. Semin Plast Surg. 2010;24(4):375-382. http://www.ncbi.nlm.nih .gov/pmc/articles/PMC3324222/. Accessed July 9, 2013.
4. Scarfe WC. Imaging of maxillofacial trauma: evolution and emerging revolutions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100(2 Suppl):S75-S96.
5. Allareddy V, Allareddy ZV, Nalliah RP. Epidemiology of facial fracture injuries. J Oral Maxillofac Surg. 2011;69 (10):2613-2618. doi:10.1016.j.joms/2011.02.057.
6. Thorén H, Snäll J, Salo J, et al. Occurrence and types of asso-ciated injuries in patients with fractures of the facial bones. J Oral Maxillofac Surg. 2010;68(4):805-810. doi:10.1016/j.joms .2009.09.057.
7. Perry P. Maxillofacial trauma – developments, innovations and controversies. Injury Int J Care Injured. 2009;40:1252-1259.
8. Lee KH. Interpersonal violence and facial fractures. J Oral Maxillfac Surg. 2009;67(9):1878-1883.
9. O’Meara C, Witherspoon R, Hapangama N, Hyam DM. Alcohol and interpersonal violence may increase the severity of facial fracture. Br J Oral Maxillofac Surg. 2012;50(1):36-40.
10. Lee KH. Epidemiology of facial fractures secondary to acci-dental falls. Asian J Oral Maxillofac Surg. 2009;21:33-37.
11. Lee KH, Steenberg LJ. Equine-related facial fractures. Int J Oral Maxillofac Surg. 2008;37(11):999-1002. doi:10.1016/j /ijom2008.05.009.
12. Wei LA, Chen HH, Hink EM, Durairaj VD. Pediatric facial fractures from dog bites. Ophthal Plast Reconstr Surg. 2013;29(3):179-182. doi:10.1097/IOP.0b013e3182880114.
13. Lee KH, Chou HJ. Facial fractures in work-related injuries. Asian J Oral Maxillofac Surg. 2010;22:138-142.
14. Thorén H, Iso-Kungas P, Iizuka T, Lindqvist C, Törnwall J. Changing trends in causes and patterns of facial fractures in children. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107(3):318-324. doi:10.1016/j.tripleo.2008.09.024.
15. Alvi A, Doherty T, Lewen G. Facial fractures and concomitant injuries in trauma patients. Laryngoscope. 2003;113(1):102-106.
16. Costello BJ, Papadopoulos H, Ruiz R. Pediatric craniomaxil-lofacial trauma. Clin Pediatr Emerg Med. 2005;6(1):32-40.
17. Iso-Kungas P, Törnwall J, Suominen AL, Lindqvist C, Thorén H. Dental injuries in pediatric patients with facial fractures are frequent and severe. J Oral Maxillofac Surg. 2012;70(2):396-400. doi:10.1016/j.joms.2011.08.035.
18. Kloss F, Laimer K, Hohlrieder M, et al. Traumatic intra-cranial haemorrhage in conscious patients with facial fractures: a review of 1959 cases. J Cranio-Maxillofac Surg. 2008;36(7):372-377. doi:10.1016/j.jcms.2007.12.002.
19. MacKinnon CA, David DJ, Cooter RD. Blindness and severe visual impairment in facial fractures: an 11 year review. Br J Plast Surg. 2002;55(1):1-7. doi:10.1054/bjps.2001.3728.
20. Imahara SD, Hopper RA, Wang J, Rivara FP, Klein MB. Patterns and outcomes of pediatric facial fractures in the United States: a survey of the National Trauma Data Bank. J Am Coll Surg. 2008;207(5):710-716. doi:10.1016/j.jamcoll surg.2008.06.333.
21. Alcalá-Galiano A, Arribas-Garcia IJ, Martín-Pérez MA, Romance A, Montalvo-Moreno JJ, Juncos JM. Pediatric facial fractures: children are not just small adults. Radiographics. 2008;28(2):441-461. doi:10.1148/rg.282075060.
22. Ryan ML, Thorson CM, Otero CA, et al. Pediatric facial trauma: a review of guidelines for assessment, evalua-tion, and management in the emergency department. J Craniofac Surg. 2011;22(4):1183-1189. doi:10.1097/SCS .0b013e31821c0d52.
23. Afrooz PN, Grunwaldt LJ, Zanoun RR, et al. Pediatric facial fractures: occurrence of concussion and relation to fracture patterns. J Craniofac Surg. 2012;23(5):1270-1273.
24. Carlson BM. Head and neck. In: Carlson BM, ed. Human Embryology & Developmental Biology. 5th ed. Philadelphia, PA: Saunders; 2013:294-334.
25. Larheim TA, Westesson PL, Kakimoto N, Smith HJ. Maxillofacial imaging anatomy. In: Larheim TA, Westesson PL (eds). Maxillofacial Imaging. Berlin, Germany: Springer-Verlag; 2006:1-20.
26. Martin RCG, Spain DA, Richardson JD. Do facial fractures protect the brain or are they a marker for severe head injury? Am Surg. 2002;68(5):477-481.
27. Doland KD, Jacoby CG, Smoker WRK. The radiology of facial fractures. Radiographics. 1984;4(4):577-663. http://radiographics.rsna.org/content/4/4/577.abstract. Accessed July 16, 2013.
28. Casto AL, Priolo GD, Garufi A, et al. Imaging evaluation of facial complex strut fractures. Semin Ultrasound CT MRI. 2012;33(5):396-409. doi:10.1053/j.sult.2012.06.003.

CEDirected Reading
539CTRADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Furlow
29. Roeder RA, Thaller S. Unique features of the pediatric craniofacial anatomy. J Craniofac Surg. 2011;22(2):392-394. doi:10.1097/SCS.0b013e318208ba30.
30. Chao MT, Losee JE. Complications in pediatric facial frac-tures. Craniomaxillofac Trauma Reconstr. 2009;2(2):103-112.
31. Chan J, Putnam MA, Feustel PJ, Koltai PJ. The age dependent relationship between facial fractures and skull fractures. Int J Pediatr Otorhinolaryngol. 2004;68(7):877-881. doi:10.1016/j .ijporl.2004.01.021.
32. Stanwix MG, Nam AJ, Manson PN, Mirvis S, Rodriguez ED. Critical computed tomographic diagnostic criteria for frontal sinus fractures. J Oral Maxillofac Surg. 2010;68(11):2714-2722. doi:10.1016/j.joms.2010.05.019.
33. Shah HA, Shipchandler TZ, Sufyan AS, Nunery WR, Lee HBH. Use of fracture size and soft tissue herniation on computed tomography to predict diplopia in isolated orbital f loor fractures. Am J Otolaryngol – Head Neck Med Surg. 2013;34(6):695-698. doi:10.1016/j.amjoto.2013.02.006.
34. Sung EK, Nadgir RN, Sakai O. Computed tomographic imaging in head and neck trauma: what the radiologist needs to know. Semin Roentgenol. 2012;47(4):320-329. doi:1053/j .ro.2012.05.002.
35. Markowitz BL, Manson PN, Sargent L, et al. Management of the medial canthal tendon in nasoethmoid orbital fractures: the importance of the central fragment in classification and treatment. Plast Reconstr Surg. 1991;87(5):843-853.
36. Chen CT, Chen YR. Traumatic superior orbital fissure syndrome: current management. Craniomaxillofac Trauma Reconstr. 2010;3(1):9-16. http://www.ncbi.nlm.nih.gov/pmc /articles/PMC3052661/. Accessed July 8, 2013.
37. Sohns JM, Staab W, Sohns C, et al. Current perspective of multidetector computed tomography (MDCT) in patients after midface and craniofacial trauma. Clin Imag. 2013;37(4):728-733. doi:10.1016/j.clinimag.2012.11.002.
38. Avery LL, Susarla SM, Novelline RA. Multidetector and three-dimensional CT evaluation of the patient with max-illofacial injury. Radiol Clin N Am. 2011;49(1):183-203. doi:10.1016/j.rcl.2010.07.014.
39. Kim BH, Seo HS, Kim AY, et al. The diagnostic value of the sagittal multiplanar reconstruction CT images for nasal bone fractures. Clin Radiol. 2010;65(4):308-314. doi:10.1016/j .cread.2009.12.006.
40. Caranci F, Cicala D, Cappabianca S, Briganti F, Brunese L, Fonio P. Orbital fractures: role of imaging. Semin Ultrasound CT MRI. 2012;33(5):385-391. doi:10.1053/j.sult .2012.06.007.
41. Ahmad Z, Nouraei R, Holmes S. Towards a classification system for complex craniofacial fractures. Br J Oral Maxillofac Surg. 2012;50(6):490-494. doi:10.1016/j.bjoms.2011.09.018.
42. Yang L, Xu M, Jin X, et al. Complications of absorbable fixa-tion in maxillofacial surgery: a meta-analysis. PLoS One. 2013;8(6):e67449. doi:10.1371/journal.pone.0067449.

540CT RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Directed Reading Quiz
continued on next page
Read the preceding Directed Reading and choose the answer that is most correct based on the article.
To earn continuing education credit: Take this Directed Reading quiz online at www.asrt.org/drquiz. Or, transfer your responses to the answer sheet on Page 410M and mail to ASRT, PO Box 51870, Albuquerque, NM 87181-1870.
New and rejoining members are ineligible to take DRs from journal issues published prior to their most recent join date unless they have purchased access to the quiz from the ASRT. To purchase access to other quizzes, go to www.asrt.org/store.
*Your answer sheet for this Directed Reading must be received in the ASRT office on or before this date.
To earn continuing education credit: Take this Directed Reading quiz online at www.asrt.org/drquiz. Or, transfer your responses to the answer sheet on Page 544CT and mail to ASRT, PO Box 51870, Albuquerque, NM 87181-1870.
New and rejoining members are ineligible to take DRs from journal issues published prior to their most recent join date unless they have purchased access to the quiz from the ASRT. To purchase access to other quizzes, go to www.asrt.org/store.
*Your answer sheet for this Directed Reading must be received in the ASRT office on or before this date.
14803-04 1.5 Category A+ creditsExpires June 30, 2016*
Computed Tomography of Facial Fractures
1. The average patient with a facial fracture is a(n):a. preschooler injured on the playground.b. high school athlete who plays a contact sport.c. elderly woman with impaired balance.d. man in his late 30s.
2. In patients with facial fractures, intracranial hemorrhage can be ruled out based solely on normal neurological findings.a. trueb. false
3. Which of the following are possible complications in patients with facial fractures?
1. significant blood loss2. displacement of the eyes3. compromised airway
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
4. According to a 2008 analysis of the National Trauma Data Bank, which of the following is the leading cause of facial fractures among children in the United States?a. automobile accidentsb. child abusec. falls from heightsd. animal attacks
5. Among children who receive a diagnosis of facial fracture, one-third simultaneously receive a ______ diagnosis.a. collarbone fractureb. cranial fracturec. concussiond. hearing loss
6. The midface skeleton extends downward from the:a. frontal bone and frontal sinuses.b. mandible and nasal cavity.c. superior orbital rims and orbits and includes the
nasal cavity and associated sinuses.d. frontal and nasal sinuses.

RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Directed Reading Quiz
continued on next page
541CT
7. What is the term for the cagelike array of thickened facial bones that supports muscles, eyes, teeth, and the uppermost airways?a. facial skeletal buttressesb. zygomatic processesc. orbital cavitiesd. viscerocranium
8. Which of the following represents a much larger proportion of the facial skeleton in children than in adults?a. maxillab. mandiblec. bony orbitsd. sinuses
9. In younger children, ______ facial fractures are more common, whereas among older children ______ fractures are more common.a. orbital floor; blow-in superior orbitalb. blow-in superior orbital; orbital floorc. frontal sinus; blow-in superior orbitald. orbital floor; frontal sinus
10. Frontal sinus fractures are an indication for diagnostic imaging for which of the following conditions?a. enophthalmosb. diplopiac. ophthalmoplegiad. pneumocephalus
11. Among patients with frontal sinus fractures, up to 91% present with which of the following criteria for computed tomography (CT)–based diagnosis of nasofrontal outflow injuries?a. sinus floor fracturesb. pneumocephalusc. anterior or posterior table fracturesd. obstruction
12. Diagnostic imaging is indicated to evaluate suspected type ______ nasal fractures.a. 1b. 2c. 3d. 4
13. Blowout fractures affecting more than 50% of the orbital floor are a risk factor for which of the following conditions?a. enophthalmosb. diplopiac. ophthalmoplegiad. pneumocephalus
14. Simple (isolated) fractures of the ______ are more frequent among children than adults.a. maxillab. mandiblec. orbitsd. sinuses
15. Jaw injuries are a common type of facial fracture in ______ accidents.a. workplaceb. automobilec. home-basedd. horseback riding
16. Presentation with reduced nose projection from the face and abnormal protrusion of one or both eyes is typical of ______ fractures.a. Le Fortb. nasoorbitoethmoid c. zygomaticomaxillary complex d. “trap-door”
17. Which of the following is a sign of Jacod syndrome?a. enophthalmosb. diplopiac. ophthalmoplegiad. pneumocephalus

RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Directed Reading Quiz
542CT
18. When ______ persists beyond a few days after an injury, soft-tissue herniation is a more likely culprit than edema or hemorrhage.a. enophthalmosb. diplopiac. ophthalmoplegiad. pneumocephalus
19. A deformity of the globe’s overall shape, visible on CT scans, is called the ______ sign.a. “deflated balloon”b. “donut”c. “flat tire”d. “figure 8”
20. Which 16- or 64-channel multidetector CT scanning parameters are used for imaging the face, orbits, and brain?
1. 120 kV2. 115 mA3. 1-second gantry rotation time
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
21. CT is sensitive for detecting:1. bone.2. metal.3. glass.
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
22. Which of the following type of fracture is frequently an indication for immediate surgical intervention?a. orbital apexb. orbital ceilingc. lateral orbital walld. inferior orbital wall
23. Which of the following facial trauma severity models successfully discriminated between various levels of trauma, according to a recent study of multiplanar 2-D reformations and 3-D CT images?a. Facial Injury Severity Scoreb. Facial Fracture Severity Scorec. Cooter and David Scored. ZS Scoring System
24. What is the optimal timing for reduction and fixation of complex facial fractures?a. 24 to 48 hours after the injury b. 72 hours after swelling has subsidedc. as soon as possible after the patient is stabilizedd. no optimal time has been identified
25. Which of the following problems has been associated with titanium pins and plates used for facial fracture fixation?
1. restricted bone growth in pediatric patients
2. possible carcinogenicity3. imaging complications
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3