
Comprehensive systematic review summary: Disease-modifying...
13
SPECIAL ARTICLE Comprehensive systematic review summary: Disease-modifying therapies for adults with multiple sclerosis Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology Alexander Rae-Grant, MD, Gregory S. Day, MD, MSc, Ruth Ann Marrie, MD, PhD, Alejandro Rabinstein, MD, Bruce A.C. Cree, MD, PhD, MAS, Gary S. Gronseth, MD, Michael Haboubi, DO, June Halper, MSN, APN-C, MSCN, Jonathan P. Hosey, MD, David E. Jones, MD, Robert Lisak, MD, Daniel Pelletier, MD, Sonja Potrebic, MD, PhD, Cynthia Sitcov, Rick Sommers, LMSW, Julie Stachowiak, PhD, Thomas S.D. Getchius, Shannon A. Merillat, MLIS, and Tamara Pringsheim, MD, MSc Neurology ® 2018;90:789-800. doi:10.1212/WNL.0000000000005345 Correspondence American Academy of Neurology [email protected] Abstract Objective To review evidence on starting, switching, and stopping disease-modifying therapies (DMTs) for multiple sclerosis (MS) in clinically isolated syndrome (CIS), relapsing-remitting MS (RRMS), and progressive MS forms. Methods Relevant, peer-reviewed research articles, systematic reviews, and abstracts were identified (MEDLINE, CENTRAL, EMBASE searched from inception to November 2016). Studies were rated using the therapeutic classification scheme. Prior published Cochrane reviews were also used. Results Twenty Cochrane reviews and an additional 73 full-text articles were selected for data extraction through an updated systematic review (completed November 2016). For people with RRMS, many DMTs are superior to placebo (annualized relapses rates [ARRs], new disease activity [new MRI T2 lesion burden], and in-study disease progression) (see summary and full text publications). For people with RRMS who experienced a relapse on interferon-β (IFN-β) or glatiramer acetate, alemtuzumab is more effective than IFN-β-1a 44 μg subcutaneous 3 times per week in reducing the ARR. For people with primary progressive MS, ocrelizumab is probably more effective than placebo (in-study disease progression). DMTs for MS have varying adverse effects. In people with CIS, glatiramer acetate and IFN-β-1a subcutaneous 3 times per week are more effective than placebo in decreasing risk of conversion to MS. Cladribine, immunoglob- ulins, IFN-β-1a 30 μg intramuscular weekly, IFN-β-1b subcutaneous alternate day, and teri- flunomide are probably more effective than placebo in decreasing risk of conversion to MS. Suggestions for future research include studies considering comparative effectiveness, usefulness of high-efficacy treatment vs stepped-care protocols, and research into predictive biomarkers. RELATED ARTICLES Editorial Complexity of MS management in the current treatment era Page 761 Article Practice guideline recommendations summary: Disease- modifying therapies for adults with multiple sclerosis: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology Page 777 From the Department of Neurology (A.R.-G.), Cleveland Clinic, OH; Department of Neurology (G.S.D.), Charles F. and Joanne Knight Alzheimer Disease Research Center, Washington University in St. Louis, MO; Department of Community Health Sciences (R.A.M.), Max Rady College of Medicine, Rady Faculty of Health Sciences, University of Manitoba, Winnipeg, Canada; Department of Neurology (A.R.), Mayo Clinic, Rochester, MN; UCSF Weill Institute for Neurosciences, Department of Neurology (B.A.C.C.), University of California, San Francisco; Department of Neurology (G.S.G.), Kansas University Medical Center, Kansas City; Department of Neurology, School of Medicine (M.H.), University of Louisville, KY; Consortium of Multiple Sclerosis Centers (J.H.), Hackensack, NJ; Department of Neuroscience (J.P.H.), St. Luke’s University Health Network, Bethlehem, PA; Department of Neurology (D.E.J.), University of Virginia, Charlottesville; Consortium of Multiple Sclerosis Centers (R.L.), Hackensack, NJ; Department of Neurology, School of Medicine (R.L.), Wayne State University, Detroit, MI; Department of Neurology, Keck School of Medicine (D.P.), University of Southern California, Los Angeles; Neurology Department (S.P.), Southern California Permanente Medical Group, Kaiser, Los Angeles; National Multiple Sclerosis Society (C.S.), Arlington, VA; National Multiple Sclerosis Society (R.S.), New York, NY; Santa Fe (J.S.), NM; Heart Rhythm Society (T.S.D.G.), Washington, DC; American Academy of Neurology (S.A.M.), Minneapolis, MN; and Department of Clinical Neurosciences, Psychiatry, Pediatrics and Community Health Sciences, Cumming School of Medicine (T.P.), University of Calgary, Alberta, Canada. Go to Neurology.org/N for full disclosures. Funding information and disclosures deemed relevant by the authors, if any, are provided at the end of the article. Approved by the Guideline Development, Dissemination, and Implementation Subcommittee on October 9, 2017; by the AAN Practice Committee on October 21, 2017; and by the AAN Institute Board of Directors on March 6, 2018. Copyright © 2018 American Academy of Neurology 789 Copyright ª 2018 American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
Upload
hoangxuyen -
Category
Documents
-
view
215 -
download
0
Transcript of Comprehensive systematic review summary: Disease-modifying...

SPECIAL ARTICLE
Comprehensive systematic review summaryDisease-modifying therapies for adults withmultiple sclerosisReport of the Guideline Development Dissemination and ImplementationSubcommittee of the American Academy of Neurology
Alexander Rae-Grant MD Gregory S Day MD MSc Ruth Ann Marrie MD PhD Alejandro Rabinstein MD
Bruce AC CreeMD PhDMAS Gary S GronsethMDMichael Haboubi DO JuneHalperMSN APN-C MSCN
Jonathan P Hosey MD David E Jones MD Robert Lisak MD Daniel Pelletier MD Sonja Potrebic MD PhD
Cynthia Sitcov Rick Sommers LMSW Julie Stachowiak PhD Thomas SD Getchius Shannon AMerillat MLIS
and Tamara Pringsheim MD MSc
Neurologyreg 201890789-800 doi101212WNL0000000000005345
Correspondence
American Academy of
Neurology
guidelinesaancom
AbstractObjectiveTo review evidence on starting switching and stopping disease-modifying therapies (DMTs)for multiple sclerosis (MS) in clinically isolated syndrome (CIS) relapsing-remitting MS(RRMS) and progressive MS forms
MethodsRelevant peer-reviewed research articles systematic reviews and abstracts were identified(MEDLINE CENTRAL EMBASE searched from inception to November 2016) Studies wererated using the therapeutic classification scheme Prior publishedCochrane reviews were also used
ResultsTwenty Cochrane reviews and an additional 73 full-text articles were selected for data extractionthrough an updated systematic review (completed November 2016) For people with RRMSmany DMTs are superior to placebo (annualized relapses rates [ARRs] new disease activity[new MRI T2 lesion burden] and in-study disease progression) (see summary and full textpublications) For people with RRMS who experienced a relapse on interferon-β (IFN-β) orglatiramer acetate alemtuzumab is more effective than IFN-β-1a 44 μg subcutaneous 3 times perweek in reducing the ARR For people with primary progressive MS ocrelizumab is probablymore effective than placebo (in-study disease progression) DMTs for MS have varying adverseeffects In people with CIS glatiramer acetate and IFN-β-1a subcutaneous 3 times per week aremore effective than placebo in decreasing risk of conversion to MS Cladribine immunoglob-ulins IFN-β-1a 30 μg intramuscular weekly IFN-β-1b subcutaneous alternate day and teri-flunomide are probably more effective than placebo in decreasing risk of conversion to MSSuggestions for future research include studies considering comparative effectiveness usefulnessof high-efficacy treatment vs stepped-care protocols and research into predictive biomarkers
RELATED ARTICLES
EditorialComplexity of MSmanagement in the currenttreatment era
Page 761
ArticlePractice guidelinerecommendationssummary Disease-modifying therapies foradults with multiplesclerosis Report of theGuideline DevelopmentDissemination andImplementationSubcommittee of theAmerican Academy ofNeurology
Page 777
From the Department of Neurology (AR-G) Cleveland Clinic OH Department of Neurology (GSD) Charles F and Joanne Knight Alzheimer Disease Research Center WashingtonUniversity in St Louis MO Department of Community Health Sciences (RAM) Max Rady College of Medicine Rady Faculty of Health Sciences University of Manitoba WinnipegCanada Department of Neurology (AR) Mayo Clinic Rochester MN UCSF Weill Institute for Neurosciences Department of Neurology (BACC) University of California SanFrancisco Department of Neurology (GSG) Kansas University Medical Center Kansas City Department of Neurology School of Medicine (MH) University of Louisville KYConsortium of Multiple Sclerosis Centers (JH) Hackensack NJ Department of Neuroscience (JPH) St Lukersquos University Health Network Bethlehem PA Department of Neurology(DEJ) University of Virginia Charlottesville Consortium of Multiple Sclerosis Centers (RL) Hackensack NJ Department of Neurology School of Medicine (RL) Wayne StateUniversity Detroit MI Department of Neurology Keck School of Medicine (DP) University of Southern California Los Angeles Neurology Department (SP) Southern CaliforniaPermanente Medical Group Kaiser Los Angeles National Multiple Sclerosis Society (CS) Arlington VA National Multiple Sclerosis Society (RS) New York NY Santa Fe (JS) NMHeart Rhythm Society (TSDG) Washington DC American Academy of Neurology (SAM) Minneapolis MN and Department of Clinical Neurosciences Psychiatry Pediatrics andCommunity Health Sciences Cumming School of Medicine (TP) University of Calgary Alberta Canada
Go to NeurologyorgN for full disclosures Funding information and disclosures deemed relevant by the authors if any are provided at the end of the article
Approved by the Guideline Development Dissemination and Implementation Subcommittee on October 9 2017 by the AAN Practice Committee on October 21 2017 and by the AANInstitute Board of Directors on March 6 2018
Copyright copy 2018 American Academy of Neurology 789
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
This article summarizes the findings and conclusions of anAmerican Academy of Neurology (AAN) practice guidelineon the efficacy and safety of disease-modifying therapies(DMTs) in multiple sclerosis (MS) References e1 throughe49 cited here are available at linkslwwcomWNLA374 asa data supplement to this summary article
A companion article presents the recommendations andsuggestions for future research1 The complete practiceguideline (systematic review recommendations and sugges-tions for future research) is available at linkslwwcomWNLA429 as a data supplement to the companion recom-mendations article This guideline although not a formalupdate to the 2002 AAN guideline on DMTs2 replaces thatearlier guideline The complete guideline includes full detailsof the methodology used including risk of bias classificationfor each study confidence in the evidence determinationsand rationales for recommendation strength space restric-tions precluded more detailed description in this article
MS affects more than 400000 people in the United States andmore than 23 million people worldwide3 Since 1993 DMTshave been approved in the United States for treating relapsingforms of MS most of these therapies are approved for use inother countries Many additional medications have been usedoff-label for MS disease modification
Multiple newDMTs have become available since publication ofthe 2002 AAN practice guideline on DMTs in MS2 Cliniciansand people withMSmay now choose from several medicationswith differing mechanisms of action risk profiles and moni-toring requirements Before recommending a specific therapythe clinician must navigate these complexities while carefullybalancing the potential for therapeutic benefits of a medicationwith patient preferences monitoring recommendations drug-and individual-specific risk factors and concerns regarding thelong-term risk of MS-related disability and morbidity
The new practice guideline1 based on the systematic reviewsummarized here provides guidance concerning current issuessurrounding DMT for MS prescribing specifically addressing
the following questions pertinent to clinically isolated syn-dromes of demyelination (CIS) relapsing-remitting MS(RRMS) and progressive forms of MS (secondary progressiveMS [SPMS] and primary progressive MS [PPMS])
1 In people with RRMS are DMTs superior to placebo orother DMTs as measured by annualized relapse rates(ARRs) and the relative risk of relapse at 2 years
2 In people with RRMS are DMTs superior to placebo orother DMTs in reducingMRI-detected new disease activityas measured by newT2 lesion burden or atrophymeasures
3 In people with RRMS are DMTs superior to placebo orother DMTs in preventing disease progression asmeasured by in-study disease progression measures
4 In people with RRMS who experience disease activitywhile on a DMT is changing to a different DMT superiorto continuing the present DMT in terms of relapse rate andMRI-detected T2 or gadolinium-enhanced lesion activity
5 In people with progressive MS are DMTs superior toplacebo or other DMTs as measured by relapse rate or in-study disease progression
6 What are the adverse effects (AEs) of DMTs in peoplewith MS compared with placebo (AE-related discontin-uation and serious or life-threatening AEs)
7 In people with CIS are DMTs superior to placebo indecreasing the risk of conversion to MS
Description of the analytic processIn May 2015 the AAN guideline subcommittee recruiteda multidisciplinary panel to develop the guideline on whichthis systematic review is based The panel consists of 12 AANphysician and nurse members 2 representatives from theConsortium of Multiple Sclerosis Centers and 3 patientrepresentatives Two AAN staff representatives were alsoappointed to the panel Conflicts of interest were reviewed bythe panel leadership panelists with conflicts did not partici-pate in systematic review development
The practice guideline follows the methodologies described inthe 2011 edition of the AANrsquos guideline development processmanual as amended to include an updated classificationscheme for therapeutic studies a formalized prioritizationprocess for guideline topic nominations and a change in theorder of steps for the external (peer) review process4 Instituteof Medicine standards for systematic review and clinical prac-tice guideline development were adhered to throughout the
Supplemental DataPractice Guidelines
NPuborg77nyxt
GlossaryAAN = American Academy of Neurology AE = adverse effect ARR = annualized relapse rate CIS = clinically isolatedsyndromes DMT = disease-modifying therapy EDSS = Expanded Disability Status Scale HYP = high-yield process IFN-β = interferon-β IM = intramuscular MS = multiple sclerosis PPMS = primary progressive multiple sclerosis RCT =randomized controlled trial RRMS = relapsing-remitting multiple sclerosis SPMS = secondary progressive multiple sclerosis
790 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
development process including posting of the protocol anddraft document with recommendations for public review andactive solicitation of patient input56 For the systematic reviewthe panel used appropriate Cochrane reviews (assessed by 2panelists working independently of each other and using AMeasurement Tool to Assess Systematic Reviews quality)7 inaddition to treatment-specific systematic reviews Two non-conflicted panelists working independently reviewed abstractsfor article inclusion From their review full-text articles wereobtained for data extraction and risk of bias was established by2 panelists rating articles independently of each other Dataextraction was performed by the AAN staff guideline meth-odologist and confirmed by panel members The panel con-sidered data for efficacy outcomes from randomized controlledtrials (RCTs) For harms the panel considered data fromRCTs cohort studies case reports and case series Meta-analyses were performed when appropriate Before data anal-ysis the panel completed an anonymous survey to establish theminimal clinically meaningful difference for measures of DMTefficacy and AEs this information was used in the analyticportion of the guideline Conclusions were developed usinga modified Grading of Recommendations Assessment De-velopment and Evaluation process8
Analysis of evidenceTwenty Cochrane systematic reviews were identified and used inthe evidence review process These systematic reviews includeddata from 70 RCTs which were included in the panelrsquos evidencesynthesis For the update of the Cochrane reviews and de novosystematic review (completed November 2016) the combinedsearches yielded 4301 abstracts Each abstract was reviewed forrelevance by at least 2 panel members who deemed 284 asrelevant The corresponding articles were obtained for full-textreview by 2 panelists working independently of each other Anadditional 73 articles were identified for data extraction
All trials included individuals with MS aged 18 years or olderThe maximum age of participants varied across trials but wasusually between 50 and 60 years Most studies were 2 years inlength (range 6 monthsndash3 years) Trials occurred in multiplecountries worldwide Twenty-three DMTs were systemati-cally reviewed methotrexate cyclophosphamide pulsedcorticosteroids for disease modification interferon-β (IFN-β)(4 types IFN-β-1b subcutaneous alternate day IFN-β-1aintramuscular [IM] subcutaneous pegylated IFN sub-cutaneous every other week IFN-β-1a subcutaneous 3 timesper week) glatiramer acetate (3 types proprietary daily20-mg subcutaneous form proprietary 3-day-per-week 40-mgsubcutaneous form generic 20-mg subcutaneous daily form)natalizumab azathioprine teriflunomide mycophenolatemofetil rituximab ocrelizumab daclizumab mitoxantronealemtuzumab fingolimod dimethyl fumarate IV immuno-globulin for disease modification and cladribine
Safety note After US Food and Drug Administration (FDA)approval was received daclizumab (ZINBRYTA) was
voluntarily removed from the market onMarch 2 2018 by itsmanufacturers Biogen and AbbVie due to serious adverseevents in relapsing MS8a
The results of the systematic review support the followingevidence-based conclusions All recommendations are pro-vided in the companion publication1
1 In people with RRMS are DMTs superior toplacebo or other DMTs as measured by ARRsand the relative risk of relapse at 2 yearsFor this question figure 1 presents the data regarding ARRsand figure 2 presents the data on the relative risk of relapse at 2years The table shows the findings and conclusions for boththe ARRs and the relative risk of relapse at 2 years
2 In people with RRMS are DMTs superior toplacebo or other DMTs in reducing MRI newdisease activity as measured by new T2 lesionburden or atrophy measures
Risk of new or enlarging T2 lesionsThe following DMTs are more effective than placebo in re-ducing the risk of MRI-detected new or enlarging T2 lesions(high confidence) fingolimod910 IFN-β-1a 44 μg sub-cutaneous 3 times weekly11 and natalizumab12
Ocrelizumab13 is more effective than IFN-β-1a subcutaneous3 times per week in reducing the risk of new or enlarging T2lesions detected by MRI (high confidence)
Cladribine14 is probably more effective than placebo in re-ducing the risk of new or enlarging T2 lesions detected byMRI (moderate confidence)
The following DMTs are probably more effective than otherDMTs in reducing the risk of MRI-detected new or enlargingT2 lesions (moderate confidence) alemtuzumab (vs IFN-β-1a subcutaneous 3 times per week)15 fingolimod (vs IFN-β-1a IM once weekly)16 IFN-β-1a 44 μg subcutaneous3 times weekly (vs IFN-β-1a IM once weekly)17
IFN-β-1a subcutaneous 3 times per week is possibly no moreeffective than glatiramer acetate in decreasing the risk of MRI-detected new or enlarging T2 lesions (low confidence)18
There is insufficient evidence to determine the efficacy ofazathioprine comparedwith IFN-β19 in reducing the risk ofMRI-detected new or enlarging T2 lesions (very low confidence)
Reducing the volume or number of T2 lesionsThe following DMTs are more effective than placebo inreducing the volume or number of MRI-detected T2 lesions(high confidence) daclizumab high-yield process (HYP)20
dimethyl fumarate1821 glatiramer acetate18 IFN-β-1a30 μg IM weekly22 mitoxantrone23 natalizumab12 andpegylated IFN24 See the safety note on this page8a
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 791
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Rituximab25 and teriflunomide26 are probably more effectivethan placebo in reducing the volume or number of MRI-detected T2 lesions (moderate confidence)
The following DMTs are probably more effective thanother DMTs in reducing the volume or number of MRI-detected T2 lesions (moderate confidence) alemtuzumab
Figure 1 Outcome Annualized relapse rate relapsing-remitting multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit RM = raw mean difference UCL = upper confidence limit aVersus interferon-β-1a 44 μg 3 times perweek subcutaneously bSee safety note on page 7918a
Figure 2 Outcome Relative risk of relapse at 2 years relapsing-remitting multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit RR = risk ratio UCL = upper confidence limit aRelative to interferon alone bOutcome assessed at 18months cOutcome assessed at 1 year dSee safety note on page 7918a
792 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table Efficacy of disease-modifying therapies (DMTs) for reducing the annualized relapse rate (ARR) and risk of relapse at2 years
Confidencestrength
Reduction of the ARR Reduction of risk of relapse at 2 y
Compared withplacebo
Compared with otherDMTs Compared with placebo Compared with other DMTs
High Cladribine14e34 moreeffective
Alemtuzumab moreeffective than IFN-β-1asubcutaneous 3 times perwk1529
Daclizumab HYPa moreeffective (outcome measuredat 1 y)20
Alemtuzumab1529 more effective than IFN-β-1a subcutaneous 3 times per wk
Daclizumab HYPa moreeffective20
Azathioprine moreeffective thanβ-interferons19e35
Dimethyl fumarate1821 moreeffective
mdash
Dimethyl fumarate1821
more effectivebFingolimod more effectivethan IFN-β-1a IM once perwk16
Fingolimod910 more effective mdash
Fingolimod910e36 moreeffective
Ocrelizumab moreeffective than IFN-β-1asubcutaneous 3 times perwk13
Immunoglobulins3940 moreeffective
mdash
Glatiramer acetate1834e37 more effective
mdash IFN-β-1a IM once per wk2232
more effectivemdash
Natalizumab12 moreeffective
mdash IFN-β-1a subcutaneous 3times per wk11 more effective
mdash
Pegylated IFN24 moreeffective
mdash Mitoxantrone23 moreeffective
mdash
Teriflunomide26e38e39
more effectivemdash Natalizumab12 more effective mdash
mdash mdash Pegylated IFN more effective(outcome measured at 1 y)24
mdash
Moderate Azathioprine probablymore effectivee40
mdash Cladribine probably moreeffective14
Daclizumab HYPa probably more effectivethan IFN-β-1a IM once per wk (outcomemeasured at 3 y)27
IFN-β-1a IM once perwk22 probably moreeffective
mdash Glatiramer acetate probablymore effective183435
IFN-β-1b subcutaneousalternate daye1 probablymore effective
mdash IFN-β-1b subcutaneousalternate day probably moreeffectivee1
mdash
Pulsed corticosteroidsadded to IFN-β-1a36e41
probably more effective
mdash Pulsed corticosteroids addedto IFN-β-1ae41 probably moreeffective
mdash
mdash DaclizumabHYP27 IFN-β-1aonce perwk probablymoreeffectivea
Rituximab probably moreeffective (outcome measuredat 1 y)25
mdash
mdash mdash Teriflunomide26 probablymore effective
mdash
Low Cyclophosphamidee42
possibly more effectivemdash mdash Mycophenolate mofetil plus IFN-β-1a IM
weekly31e43 possibly no more effective thanIFN plus placebo (outcome measured at 1 y)
mdash mdash mdash Complex nonbiologic generic glatirameracetate (Glatopa)e44 possibly no moreeffective than glatiramer acetate (Copaxone)
mdash mdash mdash IFN-β-1a IM once weekly37 possibly no moreeffective than glatiramer acetate (Copaxone)
mdash mdash mdash IFN-β-1a subcutaneous 3 times weeklye45
possibly no more effective than glatirameracetate (Copaxone)
Continued
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 793
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
(vs IFN-β-1a subcutaneous 3 times per week)15 and dacli-zumab (vs IFN-β-1a IM once weekly)27 See safety note onpage 7918a
There is insufficient evidence to determine the efficacy ofmycophenolate mofetil vs IFN-β-1a once weekly for reducingthe volume or number of MRI-detected T2 lesions (very lowconfidence)28
There is insufficient evidence to determine the efficacy of pulsedcorticosteroids29 relative to placebo for reducing the volume ornumber of MRI-detected T2 lesions (very low confidence)
Reducing loss of parenchymal volumeOcrelizumab13 is more effective than IFN-β-1a 44 μg sub-cutaneous 3 times weekly in reducing loss of parenchymalvolume (high confidence)
Alemtuzumab is probably more effective than IFN-β-1a 44 μgsubcutaneous 3 times weekly29 in reducing loss of paren-chymal volume (moderate confidence)
Pulsed corticosteroids30 are probably more effective thanplacebo in reducing loss of parenchymal volume (moderateconfidence)
There is insufficient evidence to determine the efficacy of thefollowing DMTs relative to placebo in reducing loss of pa-renchymal volume (very low confidence) IFN-β-1a 30 μg IMweekly22 andmycophenolate mofetil added to IFN-β-1a 30 μgIM weekly31
3 In people with RRMS are DMTs superior toplacebo or other DMTs in preventing diseaseprogression as measured by in-study diseaseprogression measuresThe most consistently reported measure for in-studydisability progression was the proportion of people withMS with disability progression Disability progression wasdefined by an increase in the Expanded DisabilityStatus Scale (EDSS) of 1 point in those with a baselineEDSS score of 50 or lower or an increase of 05 point inthose with a baseline EDSS score of 55 or higher sustainedfor 3 or 6 months and detected over a 2-year study period(figure 3)
The following DMTs are more effective than placebo in re-ducing the risk of disability progression in people with RRMS(high confidence) daclizumab HYP20 dimethylfumarate1821 fingolimod910 IFN-β-1a 30 μg IM weekly2232
IFN-β-1a 44 μg subcutaneous 3 times weekly11 mitoxan-trone23 natalizumab12 pegylated IFN24 andteriflunomide2633 See safety note on page 7918a
The following DMTs are more effective than other DMTs inreducing the risk of disability progression in people withRRMS (high confidence) alemtuzumab (vs IFN-β-1a 44 μgsubcutaneous 3 times weekly) 1529 and ocrelizumab (vs IFN-β-1a 44 μg subcutaneous 3 times weekly)13
Cladribine14 is probably more effective than placebo in re-ducing the risk of disability progression in people with RRMS(moderate confidence)
Table Efficacy of disease-modifying therapies (DMTs) for reducing the annualized relapse rate (ARR) and risk of relapse at2 years (continued)
Confidencestrength
Reduction of the ARR Reduction of risk of relapse at 2 y
Compared withplacebo
Compared with otherDMTs Compared with placebo Compared with other DMTs
mdash mdash mdash IFN-β-1b subcutaneous alternate daye46e47
possibly no more effective than glatirameracetate (Copaxone)
Very low Azathioprine insufficientto support or refutee40
mdash Azathioprine insufficient tosupport or refutee40
mdash
Immunoglobulinsinsufficient to support orrefute3940e48e49
mdash Cyclophosphamideinsufficient to support orrefute (outcome measured at12 mo)e42
mdash
Pulsed corticosteroidsinsufficient to support orrefute30
mdash Methotrexate insufficient tosupport or refutee2
mdash
Rituximab insufficient tosupport or refute25
mdash Pulsed corticosteroidsinsufficient to support orrefute30
mdash
Abbreviations HYP = high-yield process IFN-β = interferon-β IM = intramusculara See safety note on page 7918ab Glatiramer acetate included as a reference comparator in a dimethyl fumarate study and not powered for study of noninferiority or superiority required byregulatory agency
794 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Daclizumab is probably more effective than IFN-β-1a 30 μgIM27 in reducing the risk of disability progression in people withRRMS (moderate confidence) See safety note on page 7918a
Pulsed corticosteroids30 are possibly more effective thanplacebo in reducing the risk of disability progression in peoplewith RRMS (low confidence)
The following DMTs are possibly no more effective thanplacebo in reducing the risk of disability progression in peoplewith RRMS (low confidence) glatiramer acetate183435 andpulsed corticosteroids added to IFN-β-1a IM once weekly36
Fingolimod is possibly no more effective than IFN-β-1a IMweekly in reducing the risk of disability progression over1 year (low confidence)16 See safety note on page 7918a
IFN-β-1a is possibly no more effective than glatiramer acetatein reducing the risk of disability progression over 3 years (lowconfidence)37
There is insufficient evidence to determine the efficacy of thefollowing DMTs compared with placebo in reducing the riskof disability progression in people with RRMS (very lowconfidence) azathioprine38 immunoglobulins3940 IFN-β-1bsubcutaneous alternate daye1 and methotrexatee2
IFN-β-1b alternate day is probably less effective than glatir-amer acetate in reducing the risk of disability progression over2 years (moderate confidence)e1
4 In peoplewith RRMSwho experience diseaseactivity while on a DMT is changing toa different DMT superior to continuing thepresent DMT in terms of relapse rate and MRI-detected T2 or gadolinium-enhancedlesion activityFor individuals with RRMS who experienced a relapse onIFN-β or glatiramer acetate alemtuzumab is more effectivethan IFN-β-1a 44 μg subcutaneous 3 times per week in re-ducing the ARR the relapse risk disability progression andrisk of new or enlarging T2 lesions over 2 years (highconfidence)15
In individuals with RRMS who experience 1 or more relapsesin the preceding 12 months on IFN-β adding natalizumab ismore effective than adding placebo in decreasing the risk ofrelapse over 2 years the ARR the risk of disability progressionover 2 years and the risk of new or enlarging T2 lesions at1 year (high confidence)e3
In individuals with RRMS who experienced one ormore relapses in the preceding 12 months on glatiramer ac-etate there is insufficient evidence to determine the efficacy ofnatalizumab added to glatiramer acetate compared with pla-cebo added to glatiramer acetate in decreasing the risk ofrelapse at 6 months (very low confidence)e4
Natalizumab added to glatiramer acetate is probably moreeffective than placebo added to glatiramer acetate in
Figure 3 Outcome Relative risk (RR) of in-study disability progression at 2 years relapsing-remitting multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aOutcome measured at 1 year bVersus interferon-β-1a cOutcomemeasured at 3 years dSee safety note on page 7918a
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 795
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
decreasing the cumulative number of new or enlarging T2lesions at 6 months (moderate confidence)e4
Note that natalizumab is not presently approvedrecommended as an add-on therapy to other DMTs owingto potential safety concerns associated with combined use ofthis medication
5 In people with progressive MS are DMTssuperior to placeboor otherDMTsasmeasuredby relapse rate or in-studydisease progression
Risk of relapseFigure 4 presents these data regarding risk of relapse IFN-β-1b subcutaneous alternate day (SPMS) is more effectivethan placebo in reducing the risk of relapse in people withprogressive MS (high confidence)e5e6
The following DMTs are probably more effective than placeboin reducing the risk of relapse in people with progressive MS(moderate confidence) IFN-β-1a 60 μg IM weekly (SPMS)e7
and mitoxantrone (worsening RRMS and SPMS)e8
There is insufficient evidence to determine the efficacy of thefollowing DMTs compared with placebo in reducing the riskof relapse in people with progressive MS (very low confi-dence) azathioprine38 immunoglobulinse9e10 and metho-trexate (chronic progressive MS older terminology that isundefined but included present PPMS and SPMS diseasetypes)e11 There is insufficient evidence to determine theefficacy of high-dose corticosteroids compared with low-dosecorticosteroidse12 in reducing the risk of relapse in peoplewith SPMS (very low confidence)
Disability progressionThe following DMTs are probably more effective than pla-cebo in reducing the risk of in-study disability progression inpeople with progressive MS (RRMS or SPMS moderateconfidence) mitoxantrone (worsening RRMS and SPMS)e13
and ocrelizumab (PPMS)e14
The following DMTs are possibly no more effective thanplacebo in reducing the risk of in-study disability progressionin people with progressive MS (low confidence) cladribine(SPMS)e15 fingolimod (PPMS)e16 glatiramer acetate(progressive forms of MSe17 and PPMSe18) IFN-β-1a 30 μgIM weekly (SPMSe7 and PPMSe19) IFN-β-1a subcutaneous 3times per week (SPMS)e20 IFN-β-1b subcutaneous alternateday (SPMSe5e6 and PPMSe21) and rituximab (PPMS)e22
There is insufficient evidence to determine the efficacy of thefollowing DMTs relative to placebo in reducing the risk of in-study disability progression in people with progressive MS(very low confidence) azathioprine38 corticosteroids addedto mitoxantronee23 cyclophosphamidee24e25 immunoglobu-linse9e10 and methotrexate (CPMS [PPMS])e11
There is insufficient evidence to determine the efficacy ofhigh-dose corticosteroids relative to low-dose cortico-steroidse26 in reducing the risk of in-study disability pro-gression in people with progressive MS (very lowconfidence)
6 What are the AEs of DMTs in people with MScompared with placebo (AE-relateddiscontinuation and serious or life-threatening AEs)A comprehensive review of adverse effects associated withDMTs is included in the full-text document (data supplementto the companion recommendations article linkslwwcomWNLA429) and table
7 In people with CIS are DMTs superior toplacebo in decreasing the risk of conversionto MSFigure 5 presents the data regarding risk of conversion to MSin people with CIS For individuals with CIS the followingDMTs are more effective than placebo in reducing the pro-portion of individuals converting to MS (high confidence)glatiramer acetatee27 and IFN-β-1a subcutaneous 3 timesweeklye28
Figure 4 Outcome Relative risk (RR) of relapse at 2 years secondary progressive multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aHigh-dose corticosteroids vs low-dose corticosteroids bOutcomemeasured at 3 years
796 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
For individuals with CIS the following DMTs are probablymore effective than placebo in reducing the proportion ofindividuals converting to MS (moderate confidence)cladribinee29 immunoglobulinse30 IFN-β-1a 30 μg IMweeklye31 IFN-β-1b subcutaneous alternate daye32 andteriflunomidee33
DiscussionMultiple DMTs are now approved for use in CIS or MSallowing people with MS and clinicians to consider DMTmechanism of action efficacy and AE profile in the decision-making process This systematic review was used to developa practice guideline for the use of DMT for MS acknowl-edging the limits of current evidence Measures of efficacysuch as long-term disability patient satisfaction quality of lifeand effects on MS symptoms may be important to thedecision-making process but ultimately remain inadequatelystudied Similarly there is a dearth of high-quality evidencepertaining to the comparative efficacy of specific DMTs orvarious treatment strategies (eg high-efficacy treatment vsstepped-care treatment protocols) Future studies addressingthese and other questions are needed to further informtreatment recommendations particularly those pertaining towhen to switch or stop DMTs
Author contributionsDr Rae-Grant study concept and design acquisition of dataanalysis or interpretation of data draftingrevising the man-uscript critical revision of the manuscript for important in-tellectual content study supervision Dr Day study conceptand design analysis or interpretation of data draftingrevisingthe manuscript critical revision of the manuscript for im-portant intellectual content Dr Marrie study concept anddesign acquisition of data analysis or interpretation of datadraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Rabinsteinanalysis or interpretation of data draftingrevising the man-uscript Dr Cree study concept and design draftingrevising
the manuscript critical revision of the manuscript forimportant intellectual content Dr Gronseth analysis orinterpretation of data critical revision of the manuscript forimportant intellectual content study supervisionDr Haboubi study concept and design analysis or in-terpretation of data draftingrevising the manuscriptJ Halper study concept and design draftingrevising themanuscript critical revision of the manuscript for importantintellectual content Dr Hosey critical revision of the man-uscript for important intellectual content Dr Jones studyconcept and design draftingrevising the manuscript criticalrevision of the manuscript for important intellectual contentDr Lisak study concept and design draftingrevising themanuscript critical revision of the manuscript for importantintellectual content Dr Pelletier study concept and designdraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Potrebicstudy concept and design acquisition of data analysis or in-terpretation of data draftingrevising the manuscript criticalrevision of the manuscript for important intellectual contentstudy supervision C Sitcov study concept and designdraftingrevising the manuscript critical revision of themanuscript for important intellectual content R Sommersdraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Stacho-wiak study concept and design draftingrevising the manu-script critical revision of the manuscript for importantintellectual content TSD Getchius study supervisionSA Merillat draftingrevising the manuscript study super-vision Dr Pringsheim study concept and design acquisitionof data analysis or interpretation of data draftingrevising themanuscript critical revision of the manuscript for importantintellectual content study supervision
AcknowledgmentThe authors thank the North American Research CommitteeonMultiple Sclerosis (NARCOMS) Registry for its assistancein administering an outcomes survey the results of whichwere included in this practice guideline NARCOMS issupported in part by the Consortium of Multiple SclerosisCenters (CMSC) and the Foundation of the CMSC
Figure 5 Outcome Relative risk (RR) of conversion to multiple sclerosis over 2 years
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aOutcome measured at 1 year bOutcome measured at 3 years
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 797
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study fundingThis practice guideline was developed with financial supportfrom the American Academy of Neurology (AAN) Authorswho serve as AAN subcommittee members or as method-ologists (AR-G GSD AR GSG MH SP TP) orwho are or were AAN staffmembers (TSDG SAM) werereimbursed by the AAN for expenses related to travel tosubcommittee meetings where drafts of manuscripts werereviewed All authors on the panel were reimbursed by theAAN for expenses related to travel to 2 in-person meetings
DisclosureA Rae-Grant receives royalties from 2 textbooks he haspublished 1 on neurology and 1 on multiple sclerosis (MS)organizes and receives honoraria for grand rounds and neu-rology review courses and is local primary investigator fora clinical trial with MedDay Pharmaceuticals for which hereceives no personal compensation A Rabinstein reports nodisclosures relevant to the manuscript B Cree has receivedcompensation for consulting from AbbVie Biogen EMDSerono GeNeuro GenzymeSanofi Aventis Novartis andShire has given expert testimony and prepared an affidavit formedical malpractice cases (1 or 2 per year) within his area ofexpertise and has acted as consultant in a legal proceeding forAcorda and Biogen G Gronseth serves as associate editor(level of evidence review) for Neurologyreg serves on the edi-torial advisory board for Neurology Now and is compensatedby the American Academy of Neurology (AAN) for meth-odologic activities G Day holds stock in ANI PharmaceuticalsM Haboubi has received travel reimbursement and honorariafor grand rounds presentations in Madisonville KY J Halperand J Hosey report no disclosures relevant to the manuscriptD Jones has received personal compensation for consultingfrom Biogen and Genzyme has received honoraria fromthe Consortium of Multiple Sclerosis Centers (CMSC) theMultiple Sclerosis Association of America (MSAA) and thePharmacy Quality Alliance has received institutional researchsupport from Biogen and the National MS Society (NMSS)has received salary support from the CMSC and has receivedtravel reimbursement from Biogen and Genzyme and fromthe AAN Can Do MS the CMSC and the MSAA R Lisakserved as the President of the CMSC and serves as a memberof the Board of the DMC Foundation has served on scientificadvisory boards for Mallinckrodt Syntimmune Celegeneand Alexion serves as chair of the adjudication committee ofa clinical trial (PAREXEL) has received funding for travelfrom the CMSC the GBSCIDP Foundation Internationalthe NMSS and Syntimmune for travel to consultants meet-ings has served as a journal editor for Clinical and Experi-mental Neuroimmunology andClinical Neuropharmacology hasreceived publishing royalties from Willey for InternationalNeurology A Clinical Approach has received honoraria fromMallinckrodt Syntimmune and Teva Pharmaceuticals andfrom the consulting agencies AlphaSights ClearViewHealthcare Partners GLC and Insights Consulting hasserved on a speakers bureau for Teva Pharmaceuticals for talks
unrelated to pharmaceuticals has received research supportfrom Mallinckrodt for investigator-initiated wet bench stud-ies and from Acorda Avanir Biogen Chugai GenentechMedImmune Novartis and Teva Pharmaceuticals for servingas a site investigator in multicenter trials has given experttestimony prepared an affidavit and acted as witness for TevaPharmaceuticals and has acted as an expert on a patent casefor Acorda Wayne State University has received financialcompensation from the NMSS for his salary as principle in-vestigator for a research grant RA Marrie receives researchgrants from nonprofit organizations including CanadianInstitutes of Health Research (CIHR) the CMSC Crohnrsquosand Colitis Canada the NMSS the Multiple Sclerosis Societyof Canada the Multiple Sclerosis Scientific Research Foun-dation and Research Manitoba and serves on the editorialboard of Neurology D Pelletier has served on scientific ad-visory boards for Biogen EMD Serono GenzymeSanofiAventis Hoffman LaRoche and Novartis has received re-search support for Biogen Genzyme Hoffman LaRoche andthe National Institute of Neurologic Disorders and Stroke ofthe NIH and has received honoraria for providing consultingservices at scientific advisory board meetings from BiogenEMD Serono GenzymeSanofi Aventis Hoffman LaRocheand Novartis S Potrebic received an honorarium from CDIQuality Institute PLE for participation in a headacheappropriate-use criteria panel for imaging and receives travelreimbursement from the AAN for attending AAN ResidencyIn-Service Training Examination Work Group meetingsAAN Axon Registry Committee meetings AAN GuidelineDevelopment Dissemination and Implementation Sub-committee meetings and the Guidelines International Net-work North America Evidence-based Guidelines AffectingPolicy Practice and Stakeholders (E-GAPPS) conference RSommers C Sitcov and J Stachowiak report no disclosuresrelevant to the manuscript T Getchius is a former AANemployee and reports no relevant disclosures S Merillatreports no disclosures relevant to the manuscript T Prings-heim has received research support from the CIHR and ShireCanada Inc Go to NeurologyorgN for full disclosures
DisclaimerClinical practice guidelines practice advisories systematicreviews and other guidance published by the AmericanAcademy of Neurology and its affiliates are assessments ofcurrent scientific and clinical information provided as an ed-ucational service The information (1) should not be con-sidered inclusive of all proper treatments methods of care oras a statement of the standard of care (2) is not continuallyupdated and may not reflect the most recent evidence (newevidence may emerge between the time information is de-veloped and when it is published or read) (3) addresses onlythe question(s) specifically identified (4) does not mandateany particular course of medical care and (5) is not intendedto substitute for the independent professional judgment of thetreating provider as the information does not account forindividual variation among people with MS In all cases theselected course of action should be considered by the treating
798 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
provider in the context of treating the individual patientUse of the information is voluntary AAN provides thisinformation on an ldquoas isrdquo basis and makes no warrantyexpressed or implied regarding the information AANspecifically disclaims any warranties of merchantability orfitness for a particular use or purpose AAN assumes noresponsibility for any injury or damage to persons or propertyarising out of or related to any use of this information or forany errors or omissions
Conflict of interest statementThe American Academy of Neurology (AAN) is committedto producing independent critical and truthful clinical prac-tice guidelines (CPGs) Significant efforts are made to mini-mize the potential for conflicts of interest to influence therecommendations of this CPG To the extent possiblethe AAN keeps separate those who have a financial stake inthe success or failure of the products appraised in the CPGsand the developers of the guidelines Conflict of interest formswere obtained from all authors and reviewed by an oversightcommittee prior to project initiation AAN limits the partic-ipation of authors with substantial conflicts of interest TheAAN forbids commercial participation in or funding ofguideline projects Drafts of the guideline have been reviewedby at least 3 AAN committees a network of neurologistsNeurologyreg peer reviewers and representatives from relatedfields The AAN Guideline Author Conflict of Interest Policycan be viewed at aancom For complete information on thisprocess access the 2011 AAN process manual as amended4
Received July 12 2017 Accepted in final form February 15 2018
References1 Rae-Grant A Day GS Marrie RA et al for the Guideline Development Dissemi-
nation and Implementation Subcommittee of the American Academy of NeurologyPractice guideline recommendations summary disease-modifying therapies for adultswith multiple sclerosis report of the Guideline Development Dissemination andImplementation Subcommittee of the American Academy of Neurology Neurology201890777ndash788
2 Goodin DS Frohman EM Garmany GP et al on behalf of the American Academy ofNeurology and the MS Council for Clinical Practice Guidelines Disease-modifyingtherapies in multiple sclerosis subcommittee of the American Academy of Neurologyand the MS Council for Clinical Practice Guidelines report of the Therapeutics andTechnology Assessment Subcommittee of the American Academy of Neurology andthe MS Council for Clinical Practice Guidelines Neurology 200258169ndash178
3 Browne P Chandraratna D Angood C et al Atlas of Multiple Sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
4 American Academy of Neurology Clinical Practice Guideline Process Manual 2011ed [online] St Paul The American Academy of Neurology 2011 Available at aancompolicy-and-guidelinesguidelinesabout-guidelines2 Accessed March 122016
5 Institute of Medicine Eden J Levit L Berg A Morton S editors Committee onStandards for Systematic Reviews of Comparative Effectiveness ResearchWashington DC National Academies Press 2011
6 Institute of Medicine Committee on Standards for Developing Trustworthy ClinicalPractice Guidelines Clinical Practice Guidelines We Can Trust Washington DCNational Academies Press 2011
7 Shea BJ Grimshaw JM Wells GA et al Development of AMSTAR a measurementtool to assess the methodological quality of systematic reviews BMC Med ResMethodol 2007710
8 Guyatt GH Oxman AD Schunemann HJ Tugwell P Knottnerus A GRADEguidelines a new series of articles in the Journal of Clinical Epidemiology J ClinEpidemiol 201164380ndash382
8a Biogen and AbbVie announce the voluntary worldwide withdrawal of marketingauthorizations for ZINBRYTAreg (daclizumab) for relapsing multiple sclerosis [press
release] Available at httpmediabiogencompress-releaseautoimmune-diseasesbiogenC2A0and-abbvie-announceC2A0-voluntaryC2A0worldwide-withdrawal-marketi Issued March 2 2018 Accessed March 5 2018
9 Kappos L Radue EW OrsquoConnor P et al A placebo-controlled trial of oral fingolimodin relapsing multiple sclerosis N Engl J Med 2010362387ndash401
10 Calabresi P Radue EW Goodin D et al Safety and efficacy of fingolimod in patientswith relapsing-remitting multiple sclerosis (FREEDOMS II) a double-blind rando-mised placebo-controlled phase 3 trial Lancet Neurol 201413545ndash556
11 PRISMS (Prevention of Relapses and Disability by Interferon Beta-la Subcutaneouslyin Multiple Sclerosis) Study Group Randomised double-blind placebo-controlledstudy of interferon beta-1a in relapsingremitting multiple sclerosis Lancet 19983521498ndash1504
12 Polman C OrsquoConnor PW Havdrova E et al A randomized placebo-controlled trialof natalizumab for relapsing multiple sclerosis N Engl J Med 2006354899ndash910
13 Hauser SL Bar-Or A Comi G et al for the OPERA I and OPERA II ClinicalInvestigators Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosisN Engl J Med 2017376221ndash234
14 Giovannoni G Comi G Cook S et al on behalf of the CLARITY Study Group Aplacebo-controlled trial of oral cladribine for relapsing multiple sclerosis N Engl JMed 2010362416ndash426
15 Cohen J Coles AJ Arnold DL et al CARE-MS I Investigators Alemtuzumab versusinterferon beta 1a as first-line treatment for patients with relapsing-remitting multiplesclerosis a randomised controlled phase 3 trial Lancet 20123801819ndash1828
16 Cohen J Barkhof F Comi G et al on behalf of the TRANSFORMS Study GroupOral fingolimod or intramuscular interferon for relapsing multiple sclerosis N Engl JMed 2010362402ndash415
17 Panitch H Goodin DS Francis G et al or the University of British Columbia MSMRI Research Group Randomized comparative study of interferon beta-1a treat-ment regimens in MS the EVIDENCE Trial Neurology 2002591496ndash1506
18 Fox R Miller DH Phillips JT et al on behalf of the CONFIRM Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 or glatiramer in multiple sclerosisN Engl J Med 20123671087ndash1097
19 Massacesi L Tramacere I Amoroso S et al Azathioprine versus beta interferons forrelapsing-remitting multiple sclerosis a multicentre randomized non-inferiority trialPLoS One 20149e113371
20 Gold R Giovannoni G Selmaj K et al on behalf of the SELECT Study Inves-tigators Daclizumab high-yield process in relapsing-remitting multiple sclerosis(SELECT) a randomised double-blind placebo-controlled trial Lancet 20133812167ndash2175
21 Gold R Kappos L Arnold DL et al on behalf of the DEFINE Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 for relapsing multiple sclerosisN Engl J Med 20123671098ndash1107
22 Vollmer T Sorensen PS Selmaj K et al on behalf of the BRAVO Study Group Arandomized placebo-controlled phase III trial of oral laquinimod for multiple scle-rosis J Neurol 2014261773ndash783
23 Millefiorini E Gasperini C Pozzilli C et al Randomized placebo-controlled trial ofmitoxantrone in relapsing-remitting multiple sclerosis 24-month clinical and MRIoutcome J Neurol 1997244153ndash159
24 Calabresi P Kieseier BC Arnold DL et al for the ADVANCE Study InvestigatorsPegylated interferon beta-1a for relapsing-remitting multiple sclerosis (ADVANCE)a randomised phase 3 double-blind study Lancet Neurol 201413657ndash665
25 Hauser SL Waubant E Arnold DL et al for the HERMES Trial Group B-celldepletion with rituximab in relapsing-remitting multiple sclerosis N Engl J Med 2008358676ndash688
26 OrsquoConnor P Wolinsky JS Confavreux C et al for the TEMSO Trial Group Ran-domized trial of oral teriflunomide for relapsing multiple sclerosis N Engl J Med20113651293ndash1303
27 Kappos L Wiendl H Selmaj K et al Daclizumab HYP versus interferon beta-1a inrelapsing multiple sclerosis N Engl J Med 20153731418ndash1428
28 Frohman EM Cutter G Remington G et al A randomized blinded parallel-grouppilot trial of mycophenolate mofetil (CellCept) compared with interferon beta-1a(Avonex) in patients with relapsing-remitting multiple sclerosis Ther Adv NeurolDisord 2010315ndash28
29 Coles A TwymanCL Arnold DL et al the CARE-MS II Investigators Alemtuzumab forpatients with relapsing multiple sclerosis after disease-modifying therapy a randomisedcontrolled phase 3 trial Lancet 2012801829ndash1839
30 Zivadinov R Rudick RA De Masi R et al Effects of IV methylprednisolone on brainatrophy in relapsing-remitting MS Neurology 2001571239ndash1247
31 Remington GM Treadaway K Frohman T et al A one-year prospective ran-domized placebo-controlled quadruple-blinded phase II safety pilot trial ofcombination therapy with interferon beta-1a and mycophenolate mofetil in earlyrelapsing-remitting multiple sclerosis (TIME MS) Ther Adv Neurol Disord 201033ndash13
32 Jacobs L Cookfair DL Rudick RA et al Intramuscular interferon beta-1a for diseaseprogression in relapsing multiple sclerosis Ann Neurol 199639285ndash294
33 Confavreux C OrsquoConnor P Comi G et al for the TOWER Trial Group Oralteriflunomide for patients with relapsing multiple sclerosis (TOWER) a randomiseddouble-blind placebo-controlled phase 3 trial Lancet Neurol 201413247ndash256
34 Johnson KP Brooks BR Cohen JA et al Copolymer 1 reduces relapse rate andimproves disability in relapsing-remitting multiple sclerosis results of a phase IIImulticenter double-blind placebo-controlled trial Copolymer 1 Multiple SclerosisStudy Group Neurology 1995451268ndash1276
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 799
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
35 Bornstein MB Miller A Slagle S et al A pilot trial of COP 1 in exacerbating-remittingmultiple sclerosis N Engl J Med 1987317408ndash414
36 Ravnborg M Sorensen PS Andersson M et al Methylprednisolone in combinationwith interferon beta-1a for relapsing-remitting multiple sclerosis (MECOMBINstudy) a multicentre double-blind randomized placebo-controlled parallel-groupstudy Lancet Neurol 20109672ndash680
37 Lublin FD Cofield SS Cutter GR et al on behalf of the CombiRx InvestigatorsRandomized study combining interferon and glatiramer acetate in multiple sclerosisAnn Neurol 201373327ndash340
38 Ellison G Myers LW Mickey MR et al A placebo-controlled randomized double-masked variable dosage clinical trial of azathioprine with and without methylpred-nisolone in multiple sclerosis Neurology 1989391018ndash1026
39 Fazekas F Deisenhammer F Stasser-Fuchs S Nahler G Mamoli B Randomisedplacebo-controlled trial of monthly intravenous immunoglobulin therapy in relapsing-remitting multiple sclerosis Austrian Immunoglobulin in Multiple Sclerosis StudyGroup Lancet 1997349598ndash593
40 Achiron A Gabbay U Gilad R et al Intravenous immunoglobulin treatment inmultiple sclerosis effect on relapses Neurology 199850398ndash402
Neurologyreg Online CME Program
Earn CME while reading Neurology This program is available only to online Neurology subscribers Read the articles markedCME go to Neurologyorg and click on CME This will provide all of the information necessary to get started TheAmerican Academy of Neurology (AAN) is accredited by the Accreditation Council for Continuing Medical Education(ACCME) to sponsor continuing medical education for physicians Neurology is planned and produced in accordance withthe ACCME Essentials For more information contact AAN Member Services at 800-879-1960
NeurologyorgN Offers Important Information to Patients and Their Families
The Neurologyreg Patient Page providesbull A critical review of ground-breaking discoveries in neurologic research that are written especially for patients and their familiesbull Up-to-date patient information about many neurologic diseasesbull Links to additional information resources for neurologic patients
All Neurology Patient Page articles can be easily downloaded and printed and may be reproduced to distribute for educational purposesClick on the lsquoPatientsrsquo link on the home page (NeurologyorgN) for a complete index of Patient Pages
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Audio summaries of current issues Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
800 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000005345201890789-800 Neurology
Alexander Rae-Grant Gregory S Day Ruth Ann Marrie et al Implementation Subcommittee of the American Academy of Neurology
with multiple sclerosis Report of the Guideline Development Dissemination and Comprehensive systematic review summary Disease-modifying therapies for adults
This information is current as of April 23 2018
ServicesUpdated Information amp
httpnneurologyorgcontent9017789fullincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl201804239017789DC1
Supplementary material can be found at
References httpnneurologyorgcontent9017789fullref-list-1
This article cites 37 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9017789fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2018 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

This article summarizes the findings and conclusions of anAmerican Academy of Neurology (AAN) practice guidelineon the efficacy and safety of disease-modifying therapies(DMTs) in multiple sclerosis (MS) References e1 throughe49 cited here are available at linkslwwcomWNLA374 asa data supplement to this summary article
A companion article presents the recommendations andsuggestions for future research1 The complete practiceguideline (systematic review recommendations and sugges-tions for future research) is available at linkslwwcomWNLA429 as a data supplement to the companion recom-mendations article This guideline although not a formalupdate to the 2002 AAN guideline on DMTs2 replaces thatearlier guideline The complete guideline includes full detailsof the methodology used including risk of bias classificationfor each study confidence in the evidence determinationsand rationales for recommendation strength space restric-tions precluded more detailed description in this article
MS affects more than 400000 people in the United States andmore than 23 million people worldwide3 Since 1993 DMTshave been approved in the United States for treating relapsingforms of MS most of these therapies are approved for use inother countries Many additional medications have been usedoff-label for MS disease modification
Multiple newDMTs have become available since publication ofthe 2002 AAN practice guideline on DMTs in MS2 Cliniciansand people withMSmay now choose from several medicationswith differing mechanisms of action risk profiles and moni-toring requirements Before recommending a specific therapythe clinician must navigate these complexities while carefullybalancing the potential for therapeutic benefits of a medicationwith patient preferences monitoring recommendations drug-and individual-specific risk factors and concerns regarding thelong-term risk of MS-related disability and morbidity
The new practice guideline1 based on the systematic reviewsummarized here provides guidance concerning current issuessurrounding DMT for MS prescribing specifically addressing
the following questions pertinent to clinically isolated syn-dromes of demyelination (CIS) relapsing-remitting MS(RRMS) and progressive forms of MS (secondary progressiveMS [SPMS] and primary progressive MS [PPMS])
1 In people with RRMS are DMTs superior to placebo orother DMTs as measured by annualized relapse rates(ARRs) and the relative risk of relapse at 2 years
2 In people with RRMS are DMTs superior to placebo orother DMTs in reducingMRI-detected new disease activityas measured by newT2 lesion burden or atrophymeasures
3 In people with RRMS are DMTs superior to placebo orother DMTs in preventing disease progression asmeasured by in-study disease progression measures
4 In people with RRMS who experience disease activitywhile on a DMT is changing to a different DMT superiorto continuing the present DMT in terms of relapse rate andMRI-detected T2 or gadolinium-enhanced lesion activity
5 In people with progressive MS are DMTs superior toplacebo or other DMTs as measured by relapse rate or in-study disease progression
6 What are the adverse effects (AEs) of DMTs in peoplewith MS compared with placebo (AE-related discontin-uation and serious or life-threatening AEs)
7 In people with CIS are DMTs superior to placebo indecreasing the risk of conversion to MS
Description of the analytic processIn May 2015 the AAN guideline subcommittee recruiteda multidisciplinary panel to develop the guideline on whichthis systematic review is based The panel consists of 12 AANphysician and nurse members 2 representatives from theConsortium of Multiple Sclerosis Centers and 3 patientrepresentatives Two AAN staff representatives were alsoappointed to the panel Conflicts of interest were reviewed bythe panel leadership panelists with conflicts did not partici-pate in systematic review development
The practice guideline follows the methodologies described inthe 2011 edition of the AANrsquos guideline development processmanual as amended to include an updated classificationscheme for therapeutic studies a formalized prioritizationprocess for guideline topic nominations and a change in theorder of steps for the external (peer) review process4 Instituteof Medicine standards for systematic review and clinical prac-tice guideline development were adhered to throughout the
Supplemental DataPractice Guidelines
NPuborg77nyxt
GlossaryAAN = American Academy of Neurology AE = adverse effect ARR = annualized relapse rate CIS = clinically isolatedsyndromes DMT = disease-modifying therapy EDSS = Expanded Disability Status Scale HYP = high-yield process IFN-β = interferon-β IM = intramuscular MS = multiple sclerosis PPMS = primary progressive multiple sclerosis RCT =randomized controlled trial RRMS = relapsing-remitting multiple sclerosis SPMS = secondary progressive multiple sclerosis
790 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
development process including posting of the protocol anddraft document with recommendations for public review andactive solicitation of patient input56 For the systematic reviewthe panel used appropriate Cochrane reviews (assessed by 2panelists working independently of each other and using AMeasurement Tool to Assess Systematic Reviews quality)7 inaddition to treatment-specific systematic reviews Two non-conflicted panelists working independently reviewed abstractsfor article inclusion From their review full-text articles wereobtained for data extraction and risk of bias was established by2 panelists rating articles independently of each other Dataextraction was performed by the AAN staff guideline meth-odologist and confirmed by panel members The panel con-sidered data for efficacy outcomes from randomized controlledtrials (RCTs) For harms the panel considered data fromRCTs cohort studies case reports and case series Meta-analyses were performed when appropriate Before data anal-ysis the panel completed an anonymous survey to establish theminimal clinically meaningful difference for measures of DMTefficacy and AEs this information was used in the analyticportion of the guideline Conclusions were developed usinga modified Grading of Recommendations Assessment De-velopment and Evaluation process8
Analysis of evidenceTwenty Cochrane systematic reviews were identified and used inthe evidence review process These systematic reviews includeddata from 70 RCTs which were included in the panelrsquos evidencesynthesis For the update of the Cochrane reviews and de novosystematic review (completed November 2016) the combinedsearches yielded 4301 abstracts Each abstract was reviewed forrelevance by at least 2 panel members who deemed 284 asrelevant The corresponding articles were obtained for full-textreview by 2 panelists working independently of each other Anadditional 73 articles were identified for data extraction
All trials included individuals with MS aged 18 years or olderThe maximum age of participants varied across trials but wasusually between 50 and 60 years Most studies were 2 years inlength (range 6 monthsndash3 years) Trials occurred in multiplecountries worldwide Twenty-three DMTs were systemati-cally reviewed methotrexate cyclophosphamide pulsedcorticosteroids for disease modification interferon-β (IFN-β)(4 types IFN-β-1b subcutaneous alternate day IFN-β-1aintramuscular [IM] subcutaneous pegylated IFN sub-cutaneous every other week IFN-β-1a subcutaneous 3 timesper week) glatiramer acetate (3 types proprietary daily20-mg subcutaneous form proprietary 3-day-per-week 40-mgsubcutaneous form generic 20-mg subcutaneous daily form)natalizumab azathioprine teriflunomide mycophenolatemofetil rituximab ocrelizumab daclizumab mitoxantronealemtuzumab fingolimod dimethyl fumarate IV immuno-globulin for disease modification and cladribine
Safety note After US Food and Drug Administration (FDA)approval was received daclizumab (ZINBRYTA) was
voluntarily removed from the market onMarch 2 2018 by itsmanufacturers Biogen and AbbVie due to serious adverseevents in relapsing MS8a
The results of the systematic review support the followingevidence-based conclusions All recommendations are pro-vided in the companion publication1
1 In people with RRMS are DMTs superior toplacebo or other DMTs as measured by ARRsand the relative risk of relapse at 2 yearsFor this question figure 1 presents the data regarding ARRsand figure 2 presents the data on the relative risk of relapse at 2years The table shows the findings and conclusions for boththe ARRs and the relative risk of relapse at 2 years
2 In people with RRMS are DMTs superior toplacebo or other DMTs in reducing MRI newdisease activity as measured by new T2 lesionburden or atrophy measures
Risk of new or enlarging T2 lesionsThe following DMTs are more effective than placebo in re-ducing the risk of MRI-detected new or enlarging T2 lesions(high confidence) fingolimod910 IFN-β-1a 44 μg sub-cutaneous 3 times weekly11 and natalizumab12
Ocrelizumab13 is more effective than IFN-β-1a subcutaneous3 times per week in reducing the risk of new or enlarging T2lesions detected by MRI (high confidence)
Cladribine14 is probably more effective than placebo in re-ducing the risk of new or enlarging T2 lesions detected byMRI (moderate confidence)
The following DMTs are probably more effective than otherDMTs in reducing the risk of MRI-detected new or enlargingT2 lesions (moderate confidence) alemtuzumab (vs IFN-β-1a subcutaneous 3 times per week)15 fingolimod (vs IFN-β-1a IM once weekly)16 IFN-β-1a 44 μg subcutaneous3 times weekly (vs IFN-β-1a IM once weekly)17
IFN-β-1a subcutaneous 3 times per week is possibly no moreeffective than glatiramer acetate in decreasing the risk of MRI-detected new or enlarging T2 lesions (low confidence)18
There is insufficient evidence to determine the efficacy ofazathioprine comparedwith IFN-β19 in reducing the risk ofMRI-detected new or enlarging T2 lesions (very low confidence)
Reducing the volume or number of T2 lesionsThe following DMTs are more effective than placebo inreducing the volume or number of MRI-detected T2 lesions(high confidence) daclizumab high-yield process (HYP)20
dimethyl fumarate1821 glatiramer acetate18 IFN-β-1a30 μg IM weekly22 mitoxantrone23 natalizumab12 andpegylated IFN24 See the safety note on this page8a
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 791
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Rituximab25 and teriflunomide26 are probably more effectivethan placebo in reducing the volume or number of MRI-detected T2 lesions (moderate confidence)
The following DMTs are probably more effective thanother DMTs in reducing the volume or number of MRI-detected T2 lesions (moderate confidence) alemtuzumab
Figure 1 Outcome Annualized relapse rate relapsing-remitting multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit RM = raw mean difference UCL = upper confidence limit aVersus interferon-β-1a 44 μg 3 times perweek subcutaneously bSee safety note on page 7918a
Figure 2 Outcome Relative risk of relapse at 2 years relapsing-remitting multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit RR = risk ratio UCL = upper confidence limit aRelative to interferon alone bOutcome assessed at 18months cOutcome assessed at 1 year dSee safety note on page 7918a
792 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table Efficacy of disease-modifying therapies (DMTs) for reducing the annualized relapse rate (ARR) and risk of relapse at2 years
Confidencestrength
Reduction of the ARR Reduction of risk of relapse at 2 y
Compared withplacebo
Compared with otherDMTs Compared with placebo Compared with other DMTs
High Cladribine14e34 moreeffective
Alemtuzumab moreeffective than IFN-β-1asubcutaneous 3 times perwk1529
Daclizumab HYPa moreeffective (outcome measuredat 1 y)20
Alemtuzumab1529 more effective than IFN-β-1a subcutaneous 3 times per wk
Daclizumab HYPa moreeffective20
Azathioprine moreeffective thanβ-interferons19e35
Dimethyl fumarate1821 moreeffective
mdash
Dimethyl fumarate1821
more effectivebFingolimod more effectivethan IFN-β-1a IM once perwk16
Fingolimod910 more effective mdash
Fingolimod910e36 moreeffective
Ocrelizumab moreeffective than IFN-β-1asubcutaneous 3 times perwk13
Immunoglobulins3940 moreeffective
mdash
Glatiramer acetate1834e37 more effective
mdash IFN-β-1a IM once per wk2232
more effectivemdash
Natalizumab12 moreeffective
mdash IFN-β-1a subcutaneous 3times per wk11 more effective
mdash
Pegylated IFN24 moreeffective
mdash Mitoxantrone23 moreeffective
mdash
Teriflunomide26e38e39
more effectivemdash Natalizumab12 more effective mdash
mdash mdash Pegylated IFN more effective(outcome measured at 1 y)24
mdash
Moderate Azathioprine probablymore effectivee40
mdash Cladribine probably moreeffective14
Daclizumab HYPa probably more effectivethan IFN-β-1a IM once per wk (outcomemeasured at 3 y)27
IFN-β-1a IM once perwk22 probably moreeffective
mdash Glatiramer acetate probablymore effective183435
IFN-β-1b subcutaneousalternate daye1 probablymore effective
mdash IFN-β-1b subcutaneousalternate day probably moreeffectivee1
mdash
Pulsed corticosteroidsadded to IFN-β-1a36e41
probably more effective
mdash Pulsed corticosteroids addedto IFN-β-1ae41 probably moreeffective
mdash
mdash DaclizumabHYP27 IFN-β-1aonce perwk probablymoreeffectivea
Rituximab probably moreeffective (outcome measuredat 1 y)25
mdash
mdash mdash Teriflunomide26 probablymore effective
mdash
Low Cyclophosphamidee42
possibly more effectivemdash mdash Mycophenolate mofetil plus IFN-β-1a IM
weekly31e43 possibly no more effective thanIFN plus placebo (outcome measured at 1 y)
mdash mdash mdash Complex nonbiologic generic glatirameracetate (Glatopa)e44 possibly no moreeffective than glatiramer acetate (Copaxone)
mdash mdash mdash IFN-β-1a IM once weekly37 possibly no moreeffective than glatiramer acetate (Copaxone)
mdash mdash mdash IFN-β-1a subcutaneous 3 times weeklye45
possibly no more effective than glatirameracetate (Copaxone)
Continued
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 793
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
(vs IFN-β-1a subcutaneous 3 times per week)15 and dacli-zumab (vs IFN-β-1a IM once weekly)27 See safety note onpage 7918a
There is insufficient evidence to determine the efficacy ofmycophenolate mofetil vs IFN-β-1a once weekly for reducingthe volume or number of MRI-detected T2 lesions (very lowconfidence)28
There is insufficient evidence to determine the efficacy of pulsedcorticosteroids29 relative to placebo for reducing the volume ornumber of MRI-detected T2 lesions (very low confidence)
Reducing loss of parenchymal volumeOcrelizumab13 is more effective than IFN-β-1a 44 μg sub-cutaneous 3 times weekly in reducing loss of parenchymalvolume (high confidence)
Alemtuzumab is probably more effective than IFN-β-1a 44 μgsubcutaneous 3 times weekly29 in reducing loss of paren-chymal volume (moderate confidence)
Pulsed corticosteroids30 are probably more effective thanplacebo in reducing loss of parenchymal volume (moderateconfidence)
There is insufficient evidence to determine the efficacy of thefollowing DMTs relative to placebo in reducing loss of pa-renchymal volume (very low confidence) IFN-β-1a 30 μg IMweekly22 andmycophenolate mofetil added to IFN-β-1a 30 μgIM weekly31
3 In people with RRMS are DMTs superior toplacebo or other DMTs in preventing diseaseprogression as measured by in-study diseaseprogression measuresThe most consistently reported measure for in-studydisability progression was the proportion of people withMS with disability progression Disability progression wasdefined by an increase in the Expanded DisabilityStatus Scale (EDSS) of 1 point in those with a baselineEDSS score of 50 or lower or an increase of 05 point inthose with a baseline EDSS score of 55 or higher sustainedfor 3 or 6 months and detected over a 2-year study period(figure 3)
The following DMTs are more effective than placebo in re-ducing the risk of disability progression in people with RRMS(high confidence) daclizumab HYP20 dimethylfumarate1821 fingolimod910 IFN-β-1a 30 μg IM weekly2232
IFN-β-1a 44 μg subcutaneous 3 times weekly11 mitoxan-trone23 natalizumab12 pegylated IFN24 andteriflunomide2633 See safety note on page 7918a
The following DMTs are more effective than other DMTs inreducing the risk of disability progression in people withRRMS (high confidence) alemtuzumab (vs IFN-β-1a 44 μgsubcutaneous 3 times weekly) 1529 and ocrelizumab (vs IFN-β-1a 44 μg subcutaneous 3 times weekly)13
Cladribine14 is probably more effective than placebo in re-ducing the risk of disability progression in people with RRMS(moderate confidence)
Table Efficacy of disease-modifying therapies (DMTs) for reducing the annualized relapse rate (ARR) and risk of relapse at2 years (continued)
Confidencestrength
Reduction of the ARR Reduction of risk of relapse at 2 y
Compared withplacebo
Compared with otherDMTs Compared with placebo Compared with other DMTs
mdash mdash mdash IFN-β-1b subcutaneous alternate daye46e47
possibly no more effective than glatirameracetate (Copaxone)
Very low Azathioprine insufficientto support or refutee40
mdash Azathioprine insufficient tosupport or refutee40
mdash
Immunoglobulinsinsufficient to support orrefute3940e48e49
mdash Cyclophosphamideinsufficient to support orrefute (outcome measured at12 mo)e42
mdash
Pulsed corticosteroidsinsufficient to support orrefute30
mdash Methotrexate insufficient tosupport or refutee2
mdash
Rituximab insufficient tosupport or refute25
mdash Pulsed corticosteroidsinsufficient to support orrefute30
mdash
Abbreviations HYP = high-yield process IFN-β = interferon-β IM = intramusculara See safety note on page 7918ab Glatiramer acetate included as a reference comparator in a dimethyl fumarate study and not powered for study of noninferiority or superiority required byregulatory agency
794 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Daclizumab is probably more effective than IFN-β-1a 30 μgIM27 in reducing the risk of disability progression in people withRRMS (moderate confidence) See safety note on page 7918a
Pulsed corticosteroids30 are possibly more effective thanplacebo in reducing the risk of disability progression in peoplewith RRMS (low confidence)
The following DMTs are possibly no more effective thanplacebo in reducing the risk of disability progression in peoplewith RRMS (low confidence) glatiramer acetate183435 andpulsed corticosteroids added to IFN-β-1a IM once weekly36
Fingolimod is possibly no more effective than IFN-β-1a IMweekly in reducing the risk of disability progression over1 year (low confidence)16 See safety note on page 7918a
IFN-β-1a is possibly no more effective than glatiramer acetatein reducing the risk of disability progression over 3 years (lowconfidence)37
There is insufficient evidence to determine the efficacy of thefollowing DMTs compared with placebo in reducing the riskof disability progression in people with RRMS (very lowconfidence) azathioprine38 immunoglobulins3940 IFN-β-1bsubcutaneous alternate daye1 and methotrexatee2
IFN-β-1b alternate day is probably less effective than glatir-amer acetate in reducing the risk of disability progression over2 years (moderate confidence)e1
4 In peoplewith RRMSwho experience diseaseactivity while on a DMT is changing toa different DMT superior to continuing thepresent DMT in terms of relapse rate and MRI-detected T2 or gadolinium-enhancedlesion activityFor individuals with RRMS who experienced a relapse onIFN-β or glatiramer acetate alemtuzumab is more effectivethan IFN-β-1a 44 μg subcutaneous 3 times per week in re-ducing the ARR the relapse risk disability progression andrisk of new or enlarging T2 lesions over 2 years (highconfidence)15
In individuals with RRMS who experience 1 or more relapsesin the preceding 12 months on IFN-β adding natalizumab ismore effective than adding placebo in decreasing the risk ofrelapse over 2 years the ARR the risk of disability progressionover 2 years and the risk of new or enlarging T2 lesions at1 year (high confidence)e3
In individuals with RRMS who experienced one ormore relapses in the preceding 12 months on glatiramer ac-etate there is insufficient evidence to determine the efficacy ofnatalizumab added to glatiramer acetate compared with pla-cebo added to glatiramer acetate in decreasing the risk ofrelapse at 6 months (very low confidence)e4
Natalizumab added to glatiramer acetate is probably moreeffective than placebo added to glatiramer acetate in
Figure 3 Outcome Relative risk (RR) of in-study disability progression at 2 years relapsing-remitting multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aOutcome measured at 1 year bVersus interferon-β-1a cOutcomemeasured at 3 years dSee safety note on page 7918a
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 795
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
decreasing the cumulative number of new or enlarging T2lesions at 6 months (moderate confidence)e4
Note that natalizumab is not presently approvedrecommended as an add-on therapy to other DMTs owingto potential safety concerns associated with combined use ofthis medication
5 In people with progressive MS are DMTssuperior to placeboor otherDMTsasmeasuredby relapse rate or in-studydisease progression
Risk of relapseFigure 4 presents these data regarding risk of relapse IFN-β-1b subcutaneous alternate day (SPMS) is more effectivethan placebo in reducing the risk of relapse in people withprogressive MS (high confidence)e5e6
The following DMTs are probably more effective than placeboin reducing the risk of relapse in people with progressive MS(moderate confidence) IFN-β-1a 60 μg IM weekly (SPMS)e7
and mitoxantrone (worsening RRMS and SPMS)e8
There is insufficient evidence to determine the efficacy of thefollowing DMTs compared with placebo in reducing the riskof relapse in people with progressive MS (very low confi-dence) azathioprine38 immunoglobulinse9e10 and metho-trexate (chronic progressive MS older terminology that isundefined but included present PPMS and SPMS diseasetypes)e11 There is insufficient evidence to determine theefficacy of high-dose corticosteroids compared with low-dosecorticosteroidse12 in reducing the risk of relapse in peoplewith SPMS (very low confidence)
Disability progressionThe following DMTs are probably more effective than pla-cebo in reducing the risk of in-study disability progression inpeople with progressive MS (RRMS or SPMS moderateconfidence) mitoxantrone (worsening RRMS and SPMS)e13
and ocrelizumab (PPMS)e14
The following DMTs are possibly no more effective thanplacebo in reducing the risk of in-study disability progressionin people with progressive MS (low confidence) cladribine(SPMS)e15 fingolimod (PPMS)e16 glatiramer acetate(progressive forms of MSe17 and PPMSe18) IFN-β-1a 30 μgIM weekly (SPMSe7 and PPMSe19) IFN-β-1a subcutaneous 3times per week (SPMS)e20 IFN-β-1b subcutaneous alternateday (SPMSe5e6 and PPMSe21) and rituximab (PPMS)e22
There is insufficient evidence to determine the efficacy of thefollowing DMTs relative to placebo in reducing the risk of in-study disability progression in people with progressive MS(very low confidence) azathioprine38 corticosteroids addedto mitoxantronee23 cyclophosphamidee24e25 immunoglobu-linse9e10 and methotrexate (CPMS [PPMS])e11
There is insufficient evidence to determine the efficacy ofhigh-dose corticosteroids relative to low-dose cortico-steroidse26 in reducing the risk of in-study disability pro-gression in people with progressive MS (very lowconfidence)
6 What are the AEs of DMTs in people with MScompared with placebo (AE-relateddiscontinuation and serious or life-threatening AEs)A comprehensive review of adverse effects associated withDMTs is included in the full-text document (data supplementto the companion recommendations article linkslwwcomWNLA429) and table
7 In people with CIS are DMTs superior toplacebo in decreasing the risk of conversionto MSFigure 5 presents the data regarding risk of conversion to MSin people with CIS For individuals with CIS the followingDMTs are more effective than placebo in reducing the pro-portion of individuals converting to MS (high confidence)glatiramer acetatee27 and IFN-β-1a subcutaneous 3 timesweeklye28
Figure 4 Outcome Relative risk (RR) of relapse at 2 years secondary progressive multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aHigh-dose corticosteroids vs low-dose corticosteroids bOutcomemeasured at 3 years
796 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
For individuals with CIS the following DMTs are probablymore effective than placebo in reducing the proportion ofindividuals converting to MS (moderate confidence)cladribinee29 immunoglobulinse30 IFN-β-1a 30 μg IMweeklye31 IFN-β-1b subcutaneous alternate daye32 andteriflunomidee33
DiscussionMultiple DMTs are now approved for use in CIS or MSallowing people with MS and clinicians to consider DMTmechanism of action efficacy and AE profile in the decision-making process This systematic review was used to developa practice guideline for the use of DMT for MS acknowl-edging the limits of current evidence Measures of efficacysuch as long-term disability patient satisfaction quality of lifeand effects on MS symptoms may be important to thedecision-making process but ultimately remain inadequatelystudied Similarly there is a dearth of high-quality evidencepertaining to the comparative efficacy of specific DMTs orvarious treatment strategies (eg high-efficacy treatment vsstepped-care treatment protocols) Future studies addressingthese and other questions are needed to further informtreatment recommendations particularly those pertaining towhen to switch or stop DMTs
Author contributionsDr Rae-Grant study concept and design acquisition of dataanalysis or interpretation of data draftingrevising the man-uscript critical revision of the manuscript for important in-tellectual content study supervision Dr Day study conceptand design analysis or interpretation of data draftingrevisingthe manuscript critical revision of the manuscript for im-portant intellectual content Dr Marrie study concept anddesign acquisition of data analysis or interpretation of datadraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Rabinsteinanalysis or interpretation of data draftingrevising the man-uscript Dr Cree study concept and design draftingrevising
the manuscript critical revision of the manuscript forimportant intellectual content Dr Gronseth analysis orinterpretation of data critical revision of the manuscript forimportant intellectual content study supervisionDr Haboubi study concept and design analysis or in-terpretation of data draftingrevising the manuscriptJ Halper study concept and design draftingrevising themanuscript critical revision of the manuscript for importantintellectual content Dr Hosey critical revision of the man-uscript for important intellectual content Dr Jones studyconcept and design draftingrevising the manuscript criticalrevision of the manuscript for important intellectual contentDr Lisak study concept and design draftingrevising themanuscript critical revision of the manuscript for importantintellectual content Dr Pelletier study concept and designdraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Potrebicstudy concept and design acquisition of data analysis or in-terpretation of data draftingrevising the manuscript criticalrevision of the manuscript for important intellectual contentstudy supervision C Sitcov study concept and designdraftingrevising the manuscript critical revision of themanuscript for important intellectual content R Sommersdraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Stacho-wiak study concept and design draftingrevising the manu-script critical revision of the manuscript for importantintellectual content TSD Getchius study supervisionSA Merillat draftingrevising the manuscript study super-vision Dr Pringsheim study concept and design acquisitionof data analysis or interpretation of data draftingrevising themanuscript critical revision of the manuscript for importantintellectual content study supervision
AcknowledgmentThe authors thank the North American Research CommitteeonMultiple Sclerosis (NARCOMS) Registry for its assistancein administering an outcomes survey the results of whichwere included in this practice guideline NARCOMS issupported in part by the Consortium of Multiple SclerosisCenters (CMSC) and the Foundation of the CMSC
Figure 5 Outcome Relative risk (RR) of conversion to multiple sclerosis over 2 years
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aOutcome measured at 1 year bOutcome measured at 3 years
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 797
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study fundingThis practice guideline was developed with financial supportfrom the American Academy of Neurology (AAN) Authorswho serve as AAN subcommittee members or as method-ologists (AR-G GSD AR GSG MH SP TP) orwho are or were AAN staffmembers (TSDG SAM) werereimbursed by the AAN for expenses related to travel tosubcommittee meetings where drafts of manuscripts werereviewed All authors on the panel were reimbursed by theAAN for expenses related to travel to 2 in-person meetings
DisclosureA Rae-Grant receives royalties from 2 textbooks he haspublished 1 on neurology and 1 on multiple sclerosis (MS)organizes and receives honoraria for grand rounds and neu-rology review courses and is local primary investigator fora clinical trial with MedDay Pharmaceuticals for which hereceives no personal compensation A Rabinstein reports nodisclosures relevant to the manuscript B Cree has receivedcompensation for consulting from AbbVie Biogen EMDSerono GeNeuro GenzymeSanofi Aventis Novartis andShire has given expert testimony and prepared an affidavit formedical malpractice cases (1 or 2 per year) within his area ofexpertise and has acted as consultant in a legal proceeding forAcorda and Biogen G Gronseth serves as associate editor(level of evidence review) for Neurologyreg serves on the edi-torial advisory board for Neurology Now and is compensatedby the American Academy of Neurology (AAN) for meth-odologic activities G Day holds stock in ANI PharmaceuticalsM Haboubi has received travel reimbursement and honorariafor grand rounds presentations in Madisonville KY J Halperand J Hosey report no disclosures relevant to the manuscriptD Jones has received personal compensation for consultingfrom Biogen and Genzyme has received honoraria fromthe Consortium of Multiple Sclerosis Centers (CMSC) theMultiple Sclerosis Association of America (MSAA) and thePharmacy Quality Alliance has received institutional researchsupport from Biogen and the National MS Society (NMSS)has received salary support from the CMSC and has receivedtravel reimbursement from Biogen and Genzyme and fromthe AAN Can Do MS the CMSC and the MSAA R Lisakserved as the President of the CMSC and serves as a memberof the Board of the DMC Foundation has served on scientificadvisory boards for Mallinckrodt Syntimmune Celegeneand Alexion serves as chair of the adjudication committee ofa clinical trial (PAREXEL) has received funding for travelfrom the CMSC the GBSCIDP Foundation Internationalthe NMSS and Syntimmune for travel to consultants meet-ings has served as a journal editor for Clinical and Experi-mental Neuroimmunology andClinical Neuropharmacology hasreceived publishing royalties from Willey for InternationalNeurology A Clinical Approach has received honoraria fromMallinckrodt Syntimmune and Teva Pharmaceuticals andfrom the consulting agencies AlphaSights ClearViewHealthcare Partners GLC and Insights Consulting hasserved on a speakers bureau for Teva Pharmaceuticals for talks
unrelated to pharmaceuticals has received research supportfrom Mallinckrodt for investigator-initiated wet bench stud-ies and from Acorda Avanir Biogen Chugai GenentechMedImmune Novartis and Teva Pharmaceuticals for servingas a site investigator in multicenter trials has given experttestimony prepared an affidavit and acted as witness for TevaPharmaceuticals and has acted as an expert on a patent casefor Acorda Wayne State University has received financialcompensation from the NMSS for his salary as principle in-vestigator for a research grant RA Marrie receives researchgrants from nonprofit organizations including CanadianInstitutes of Health Research (CIHR) the CMSC Crohnrsquosand Colitis Canada the NMSS the Multiple Sclerosis Societyof Canada the Multiple Sclerosis Scientific Research Foun-dation and Research Manitoba and serves on the editorialboard of Neurology D Pelletier has served on scientific ad-visory boards for Biogen EMD Serono GenzymeSanofiAventis Hoffman LaRoche and Novartis has received re-search support for Biogen Genzyme Hoffman LaRoche andthe National Institute of Neurologic Disorders and Stroke ofthe NIH and has received honoraria for providing consultingservices at scientific advisory board meetings from BiogenEMD Serono GenzymeSanofi Aventis Hoffman LaRocheand Novartis S Potrebic received an honorarium from CDIQuality Institute PLE for participation in a headacheappropriate-use criteria panel for imaging and receives travelreimbursement from the AAN for attending AAN ResidencyIn-Service Training Examination Work Group meetingsAAN Axon Registry Committee meetings AAN GuidelineDevelopment Dissemination and Implementation Sub-committee meetings and the Guidelines International Net-work North America Evidence-based Guidelines AffectingPolicy Practice and Stakeholders (E-GAPPS) conference RSommers C Sitcov and J Stachowiak report no disclosuresrelevant to the manuscript T Getchius is a former AANemployee and reports no relevant disclosures S Merillatreports no disclosures relevant to the manuscript T Prings-heim has received research support from the CIHR and ShireCanada Inc Go to NeurologyorgN for full disclosures
DisclaimerClinical practice guidelines practice advisories systematicreviews and other guidance published by the AmericanAcademy of Neurology and its affiliates are assessments ofcurrent scientific and clinical information provided as an ed-ucational service The information (1) should not be con-sidered inclusive of all proper treatments methods of care oras a statement of the standard of care (2) is not continuallyupdated and may not reflect the most recent evidence (newevidence may emerge between the time information is de-veloped and when it is published or read) (3) addresses onlythe question(s) specifically identified (4) does not mandateany particular course of medical care and (5) is not intendedto substitute for the independent professional judgment of thetreating provider as the information does not account forindividual variation among people with MS In all cases theselected course of action should be considered by the treating
798 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
provider in the context of treating the individual patientUse of the information is voluntary AAN provides thisinformation on an ldquoas isrdquo basis and makes no warrantyexpressed or implied regarding the information AANspecifically disclaims any warranties of merchantability orfitness for a particular use or purpose AAN assumes noresponsibility for any injury or damage to persons or propertyarising out of or related to any use of this information or forany errors or omissions
Conflict of interest statementThe American Academy of Neurology (AAN) is committedto producing independent critical and truthful clinical prac-tice guidelines (CPGs) Significant efforts are made to mini-mize the potential for conflicts of interest to influence therecommendations of this CPG To the extent possiblethe AAN keeps separate those who have a financial stake inthe success or failure of the products appraised in the CPGsand the developers of the guidelines Conflict of interest formswere obtained from all authors and reviewed by an oversightcommittee prior to project initiation AAN limits the partic-ipation of authors with substantial conflicts of interest TheAAN forbids commercial participation in or funding ofguideline projects Drafts of the guideline have been reviewedby at least 3 AAN committees a network of neurologistsNeurologyreg peer reviewers and representatives from relatedfields The AAN Guideline Author Conflict of Interest Policycan be viewed at aancom For complete information on thisprocess access the 2011 AAN process manual as amended4
Received July 12 2017 Accepted in final form February 15 2018
References1 Rae-Grant A Day GS Marrie RA et al for the Guideline Development Dissemi-
nation and Implementation Subcommittee of the American Academy of NeurologyPractice guideline recommendations summary disease-modifying therapies for adultswith multiple sclerosis report of the Guideline Development Dissemination andImplementation Subcommittee of the American Academy of Neurology Neurology201890777ndash788
2 Goodin DS Frohman EM Garmany GP et al on behalf of the American Academy ofNeurology and the MS Council for Clinical Practice Guidelines Disease-modifyingtherapies in multiple sclerosis subcommittee of the American Academy of Neurologyand the MS Council for Clinical Practice Guidelines report of the Therapeutics andTechnology Assessment Subcommittee of the American Academy of Neurology andthe MS Council for Clinical Practice Guidelines Neurology 200258169ndash178
3 Browne P Chandraratna D Angood C et al Atlas of Multiple Sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
4 American Academy of Neurology Clinical Practice Guideline Process Manual 2011ed [online] St Paul The American Academy of Neurology 2011 Available at aancompolicy-and-guidelinesguidelinesabout-guidelines2 Accessed March 122016
5 Institute of Medicine Eden J Levit L Berg A Morton S editors Committee onStandards for Systematic Reviews of Comparative Effectiveness ResearchWashington DC National Academies Press 2011
6 Institute of Medicine Committee on Standards for Developing Trustworthy ClinicalPractice Guidelines Clinical Practice Guidelines We Can Trust Washington DCNational Academies Press 2011
7 Shea BJ Grimshaw JM Wells GA et al Development of AMSTAR a measurementtool to assess the methodological quality of systematic reviews BMC Med ResMethodol 2007710
8 Guyatt GH Oxman AD Schunemann HJ Tugwell P Knottnerus A GRADEguidelines a new series of articles in the Journal of Clinical Epidemiology J ClinEpidemiol 201164380ndash382
8a Biogen and AbbVie announce the voluntary worldwide withdrawal of marketingauthorizations for ZINBRYTAreg (daclizumab) for relapsing multiple sclerosis [press
release] Available at httpmediabiogencompress-releaseautoimmune-diseasesbiogenC2A0and-abbvie-announceC2A0-voluntaryC2A0worldwide-withdrawal-marketi Issued March 2 2018 Accessed March 5 2018
9 Kappos L Radue EW OrsquoConnor P et al A placebo-controlled trial of oral fingolimodin relapsing multiple sclerosis N Engl J Med 2010362387ndash401
10 Calabresi P Radue EW Goodin D et al Safety and efficacy of fingolimod in patientswith relapsing-remitting multiple sclerosis (FREEDOMS II) a double-blind rando-mised placebo-controlled phase 3 trial Lancet Neurol 201413545ndash556
11 PRISMS (Prevention of Relapses and Disability by Interferon Beta-la Subcutaneouslyin Multiple Sclerosis) Study Group Randomised double-blind placebo-controlledstudy of interferon beta-1a in relapsingremitting multiple sclerosis Lancet 19983521498ndash1504
12 Polman C OrsquoConnor PW Havdrova E et al A randomized placebo-controlled trialof natalizumab for relapsing multiple sclerosis N Engl J Med 2006354899ndash910
13 Hauser SL Bar-Or A Comi G et al for the OPERA I and OPERA II ClinicalInvestigators Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosisN Engl J Med 2017376221ndash234
14 Giovannoni G Comi G Cook S et al on behalf of the CLARITY Study Group Aplacebo-controlled trial of oral cladribine for relapsing multiple sclerosis N Engl JMed 2010362416ndash426
15 Cohen J Coles AJ Arnold DL et al CARE-MS I Investigators Alemtuzumab versusinterferon beta 1a as first-line treatment for patients with relapsing-remitting multiplesclerosis a randomised controlled phase 3 trial Lancet 20123801819ndash1828
16 Cohen J Barkhof F Comi G et al on behalf of the TRANSFORMS Study GroupOral fingolimod or intramuscular interferon for relapsing multiple sclerosis N Engl JMed 2010362402ndash415
17 Panitch H Goodin DS Francis G et al or the University of British Columbia MSMRI Research Group Randomized comparative study of interferon beta-1a treat-ment regimens in MS the EVIDENCE Trial Neurology 2002591496ndash1506
18 Fox R Miller DH Phillips JT et al on behalf of the CONFIRM Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 or glatiramer in multiple sclerosisN Engl J Med 20123671087ndash1097
19 Massacesi L Tramacere I Amoroso S et al Azathioprine versus beta interferons forrelapsing-remitting multiple sclerosis a multicentre randomized non-inferiority trialPLoS One 20149e113371
20 Gold R Giovannoni G Selmaj K et al on behalf of the SELECT Study Inves-tigators Daclizumab high-yield process in relapsing-remitting multiple sclerosis(SELECT) a randomised double-blind placebo-controlled trial Lancet 20133812167ndash2175
21 Gold R Kappos L Arnold DL et al on behalf of the DEFINE Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 for relapsing multiple sclerosisN Engl J Med 20123671098ndash1107
22 Vollmer T Sorensen PS Selmaj K et al on behalf of the BRAVO Study Group Arandomized placebo-controlled phase III trial of oral laquinimod for multiple scle-rosis J Neurol 2014261773ndash783
23 Millefiorini E Gasperini C Pozzilli C et al Randomized placebo-controlled trial ofmitoxantrone in relapsing-remitting multiple sclerosis 24-month clinical and MRIoutcome J Neurol 1997244153ndash159
24 Calabresi P Kieseier BC Arnold DL et al for the ADVANCE Study InvestigatorsPegylated interferon beta-1a for relapsing-remitting multiple sclerosis (ADVANCE)a randomised phase 3 double-blind study Lancet Neurol 201413657ndash665
25 Hauser SL Waubant E Arnold DL et al for the HERMES Trial Group B-celldepletion with rituximab in relapsing-remitting multiple sclerosis N Engl J Med 2008358676ndash688
26 OrsquoConnor P Wolinsky JS Confavreux C et al for the TEMSO Trial Group Ran-domized trial of oral teriflunomide for relapsing multiple sclerosis N Engl J Med20113651293ndash1303
27 Kappos L Wiendl H Selmaj K et al Daclizumab HYP versus interferon beta-1a inrelapsing multiple sclerosis N Engl J Med 20153731418ndash1428
28 Frohman EM Cutter G Remington G et al A randomized blinded parallel-grouppilot trial of mycophenolate mofetil (CellCept) compared with interferon beta-1a(Avonex) in patients with relapsing-remitting multiple sclerosis Ther Adv NeurolDisord 2010315ndash28
29 Coles A TwymanCL Arnold DL et al the CARE-MS II Investigators Alemtuzumab forpatients with relapsing multiple sclerosis after disease-modifying therapy a randomisedcontrolled phase 3 trial Lancet 2012801829ndash1839
30 Zivadinov R Rudick RA De Masi R et al Effects of IV methylprednisolone on brainatrophy in relapsing-remitting MS Neurology 2001571239ndash1247
31 Remington GM Treadaway K Frohman T et al A one-year prospective ran-domized placebo-controlled quadruple-blinded phase II safety pilot trial ofcombination therapy with interferon beta-1a and mycophenolate mofetil in earlyrelapsing-remitting multiple sclerosis (TIME MS) Ther Adv Neurol Disord 201033ndash13
32 Jacobs L Cookfair DL Rudick RA et al Intramuscular interferon beta-1a for diseaseprogression in relapsing multiple sclerosis Ann Neurol 199639285ndash294
33 Confavreux C OrsquoConnor P Comi G et al for the TOWER Trial Group Oralteriflunomide for patients with relapsing multiple sclerosis (TOWER) a randomiseddouble-blind placebo-controlled phase 3 trial Lancet Neurol 201413247ndash256
34 Johnson KP Brooks BR Cohen JA et al Copolymer 1 reduces relapse rate andimproves disability in relapsing-remitting multiple sclerosis results of a phase IIImulticenter double-blind placebo-controlled trial Copolymer 1 Multiple SclerosisStudy Group Neurology 1995451268ndash1276
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 799
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
35 Bornstein MB Miller A Slagle S et al A pilot trial of COP 1 in exacerbating-remittingmultiple sclerosis N Engl J Med 1987317408ndash414
36 Ravnborg M Sorensen PS Andersson M et al Methylprednisolone in combinationwith interferon beta-1a for relapsing-remitting multiple sclerosis (MECOMBINstudy) a multicentre double-blind randomized placebo-controlled parallel-groupstudy Lancet Neurol 20109672ndash680
37 Lublin FD Cofield SS Cutter GR et al on behalf of the CombiRx InvestigatorsRandomized study combining interferon and glatiramer acetate in multiple sclerosisAnn Neurol 201373327ndash340
38 Ellison G Myers LW Mickey MR et al A placebo-controlled randomized double-masked variable dosage clinical trial of azathioprine with and without methylpred-nisolone in multiple sclerosis Neurology 1989391018ndash1026
39 Fazekas F Deisenhammer F Stasser-Fuchs S Nahler G Mamoli B Randomisedplacebo-controlled trial of monthly intravenous immunoglobulin therapy in relapsing-remitting multiple sclerosis Austrian Immunoglobulin in Multiple Sclerosis StudyGroup Lancet 1997349598ndash593
40 Achiron A Gabbay U Gilad R et al Intravenous immunoglobulin treatment inmultiple sclerosis effect on relapses Neurology 199850398ndash402
Neurologyreg Online CME Program
Earn CME while reading Neurology This program is available only to online Neurology subscribers Read the articles markedCME go to Neurologyorg and click on CME This will provide all of the information necessary to get started TheAmerican Academy of Neurology (AAN) is accredited by the Accreditation Council for Continuing Medical Education(ACCME) to sponsor continuing medical education for physicians Neurology is planned and produced in accordance withthe ACCME Essentials For more information contact AAN Member Services at 800-879-1960
NeurologyorgN Offers Important Information to Patients and Their Families
The Neurologyreg Patient Page providesbull A critical review of ground-breaking discoveries in neurologic research that are written especially for patients and their familiesbull Up-to-date patient information about many neurologic diseasesbull Links to additional information resources for neurologic patients
All Neurology Patient Page articles can be easily downloaded and printed and may be reproduced to distribute for educational purposesClick on the lsquoPatientsrsquo link on the home page (NeurologyorgN) for a complete index of Patient Pages
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Audio summaries of current issues Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
800 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000005345201890789-800 Neurology
Alexander Rae-Grant Gregory S Day Ruth Ann Marrie et al Implementation Subcommittee of the American Academy of Neurology
with multiple sclerosis Report of the Guideline Development Dissemination and Comprehensive systematic review summary Disease-modifying therapies for adults
This information is current as of April 23 2018
ServicesUpdated Information amp
httpnneurologyorgcontent9017789fullincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl201804239017789DC1
Supplementary material can be found at
References httpnneurologyorgcontent9017789fullref-list-1
This article cites 37 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9017789fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2018 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

development process including posting of the protocol anddraft document with recommendations for public review andactive solicitation of patient input56 For the systematic reviewthe panel used appropriate Cochrane reviews (assessed by 2panelists working independently of each other and using AMeasurement Tool to Assess Systematic Reviews quality)7 inaddition to treatment-specific systematic reviews Two non-conflicted panelists working independently reviewed abstractsfor article inclusion From their review full-text articles wereobtained for data extraction and risk of bias was established by2 panelists rating articles independently of each other Dataextraction was performed by the AAN staff guideline meth-odologist and confirmed by panel members The panel con-sidered data for efficacy outcomes from randomized controlledtrials (RCTs) For harms the panel considered data fromRCTs cohort studies case reports and case series Meta-analyses were performed when appropriate Before data anal-ysis the panel completed an anonymous survey to establish theminimal clinically meaningful difference for measures of DMTefficacy and AEs this information was used in the analyticportion of the guideline Conclusions were developed usinga modified Grading of Recommendations Assessment De-velopment and Evaluation process8
Analysis of evidenceTwenty Cochrane systematic reviews were identified and used inthe evidence review process These systematic reviews includeddata from 70 RCTs which were included in the panelrsquos evidencesynthesis For the update of the Cochrane reviews and de novosystematic review (completed November 2016) the combinedsearches yielded 4301 abstracts Each abstract was reviewed forrelevance by at least 2 panel members who deemed 284 asrelevant The corresponding articles were obtained for full-textreview by 2 panelists working independently of each other Anadditional 73 articles were identified for data extraction
All trials included individuals with MS aged 18 years or olderThe maximum age of participants varied across trials but wasusually between 50 and 60 years Most studies were 2 years inlength (range 6 monthsndash3 years) Trials occurred in multiplecountries worldwide Twenty-three DMTs were systemati-cally reviewed methotrexate cyclophosphamide pulsedcorticosteroids for disease modification interferon-β (IFN-β)(4 types IFN-β-1b subcutaneous alternate day IFN-β-1aintramuscular [IM] subcutaneous pegylated IFN sub-cutaneous every other week IFN-β-1a subcutaneous 3 timesper week) glatiramer acetate (3 types proprietary daily20-mg subcutaneous form proprietary 3-day-per-week 40-mgsubcutaneous form generic 20-mg subcutaneous daily form)natalizumab azathioprine teriflunomide mycophenolatemofetil rituximab ocrelizumab daclizumab mitoxantronealemtuzumab fingolimod dimethyl fumarate IV immuno-globulin for disease modification and cladribine
Safety note After US Food and Drug Administration (FDA)approval was received daclizumab (ZINBRYTA) was
voluntarily removed from the market onMarch 2 2018 by itsmanufacturers Biogen and AbbVie due to serious adverseevents in relapsing MS8a
The results of the systematic review support the followingevidence-based conclusions All recommendations are pro-vided in the companion publication1
1 In people with RRMS are DMTs superior toplacebo or other DMTs as measured by ARRsand the relative risk of relapse at 2 yearsFor this question figure 1 presents the data regarding ARRsand figure 2 presents the data on the relative risk of relapse at 2years The table shows the findings and conclusions for boththe ARRs and the relative risk of relapse at 2 years
2 In people with RRMS are DMTs superior toplacebo or other DMTs in reducing MRI newdisease activity as measured by new T2 lesionburden or atrophy measures
Risk of new or enlarging T2 lesionsThe following DMTs are more effective than placebo in re-ducing the risk of MRI-detected new or enlarging T2 lesions(high confidence) fingolimod910 IFN-β-1a 44 μg sub-cutaneous 3 times weekly11 and natalizumab12
Ocrelizumab13 is more effective than IFN-β-1a subcutaneous3 times per week in reducing the risk of new or enlarging T2lesions detected by MRI (high confidence)
Cladribine14 is probably more effective than placebo in re-ducing the risk of new or enlarging T2 lesions detected byMRI (moderate confidence)
The following DMTs are probably more effective than otherDMTs in reducing the risk of MRI-detected new or enlargingT2 lesions (moderate confidence) alemtuzumab (vs IFN-β-1a subcutaneous 3 times per week)15 fingolimod (vs IFN-β-1a IM once weekly)16 IFN-β-1a 44 μg subcutaneous3 times weekly (vs IFN-β-1a IM once weekly)17
IFN-β-1a subcutaneous 3 times per week is possibly no moreeffective than glatiramer acetate in decreasing the risk of MRI-detected new or enlarging T2 lesions (low confidence)18
There is insufficient evidence to determine the efficacy ofazathioprine comparedwith IFN-β19 in reducing the risk ofMRI-detected new or enlarging T2 lesions (very low confidence)
Reducing the volume or number of T2 lesionsThe following DMTs are more effective than placebo inreducing the volume or number of MRI-detected T2 lesions(high confidence) daclizumab high-yield process (HYP)20
dimethyl fumarate1821 glatiramer acetate18 IFN-β-1a30 μg IM weekly22 mitoxantrone23 natalizumab12 andpegylated IFN24 See the safety note on this page8a
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 791
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Rituximab25 and teriflunomide26 are probably more effectivethan placebo in reducing the volume or number of MRI-detected T2 lesions (moderate confidence)
The following DMTs are probably more effective thanother DMTs in reducing the volume or number of MRI-detected T2 lesions (moderate confidence) alemtuzumab
Figure 1 Outcome Annualized relapse rate relapsing-remitting multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit RM = raw mean difference UCL = upper confidence limit aVersus interferon-β-1a 44 μg 3 times perweek subcutaneously bSee safety note on page 7918a
Figure 2 Outcome Relative risk of relapse at 2 years relapsing-remitting multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit RR = risk ratio UCL = upper confidence limit aRelative to interferon alone bOutcome assessed at 18months cOutcome assessed at 1 year dSee safety note on page 7918a
792 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table Efficacy of disease-modifying therapies (DMTs) for reducing the annualized relapse rate (ARR) and risk of relapse at2 years
Confidencestrength
Reduction of the ARR Reduction of risk of relapse at 2 y
Compared withplacebo
Compared with otherDMTs Compared with placebo Compared with other DMTs
High Cladribine14e34 moreeffective
Alemtuzumab moreeffective than IFN-β-1asubcutaneous 3 times perwk1529
Daclizumab HYPa moreeffective (outcome measuredat 1 y)20
Alemtuzumab1529 more effective than IFN-β-1a subcutaneous 3 times per wk
Daclizumab HYPa moreeffective20
Azathioprine moreeffective thanβ-interferons19e35
Dimethyl fumarate1821 moreeffective
mdash
Dimethyl fumarate1821
more effectivebFingolimod more effectivethan IFN-β-1a IM once perwk16
Fingolimod910 more effective mdash
Fingolimod910e36 moreeffective
Ocrelizumab moreeffective than IFN-β-1asubcutaneous 3 times perwk13
Immunoglobulins3940 moreeffective
mdash
Glatiramer acetate1834e37 more effective
mdash IFN-β-1a IM once per wk2232
more effectivemdash
Natalizumab12 moreeffective
mdash IFN-β-1a subcutaneous 3times per wk11 more effective
mdash
Pegylated IFN24 moreeffective
mdash Mitoxantrone23 moreeffective
mdash
Teriflunomide26e38e39
more effectivemdash Natalizumab12 more effective mdash
mdash mdash Pegylated IFN more effective(outcome measured at 1 y)24
mdash
Moderate Azathioprine probablymore effectivee40
mdash Cladribine probably moreeffective14
Daclizumab HYPa probably more effectivethan IFN-β-1a IM once per wk (outcomemeasured at 3 y)27
IFN-β-1a IM once perwk22 probably moreeffective
mdash Glatiramer acetate probablymore effective183435
IFN-β-1b subcutaneousalternate daye1 probablymore effective
mdash IFN-β-1b subcutaneousalternate day probably moreeffectivee1
mdash
Pulsed corticosteroidsadded to IFN-β-1a36e41
probably more effective
mdash Pulsed corticosteroids addedto IFN-β-1ae41 probably moreeffective
mdash
mdash DaclizumabHYP27 IFN-β-1aonce perwk probablymoreeffectivea
Rituximab probably moreeffective (outcome measuredat 1 y)25
mdash
mdash mdash Teriflunomide26 probablymore effective
mdash
Low Cyclophosphamidee42
possibly more effectivemdash mdash Mycophenolate mofetil plus IFN-β-1a IM
weekly31e43 possibly no more effective thanIFN plus placebo (outcome measured at 1 y)
mdash mdash mdash Complex nonbiologic generic glatirameracetate (Glatopa)e44 possibly no moreeffective than glatiramer acetate (Copaxone)
mdash mdash mdash IFN-β-1a IM once weekly37 possibly no moreeffective than glatiramer acetate (Copaxone)
mdash mdash mdash IFN-β-1a subcutaneous 3 times weeklye45
possibly no more effective than glatirameracetate (Copaxone)
Continued
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 793
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
(vs IFN-β-1a subcutaneous 3 times per week)15 and dacli-zumab (vs IFN-β-1a IM once weekly)27 See safety note onpage 7918a
There is insufficient evidence to determine the efficacy ofmycophenolate mofetil vs IFN-β-1a once weekly for reducingthe volume or number of MRI-detected T2 lesions (very lowconfidence)28
There is insufficient evidence to determine the efficacy of pulsedcorticosteroids29 relative to placebo for reducing the volume ornumber of MRI-detected T2 lesions (very low confidence)
Reducing loss of parenchymal volumeOcrelizumab13 is more effective than IFN-β-1a 44 μg sub-cutaneous 3 times weekly in reducing loss of parenchymalvolume (high confidence)
Alemtuzumab is probably more effective than IFN-β-1a 44 μgsubcutaneous 3 times weekly29 in reducing loss of paren-chymal volume (moderate confidence)
Pulsed corticosteroids30 are probably more effective thanplacebo in reducing loss of parenchymal volume (moderateconfidence)
There is insufficient evidence to determine the efficacy of thefollowing DMTs relative to placebo in reducing loss of pa-renchymal volume (very low confidence) IFN-β-1a 30 μg IMweekly22 andmycophenolate mofetil added to IFN-β-1a 30 μgIM weekly31
3 In people with RRMS are DMTs superior toplacebo or other DMTs in preventing diseaseprogression as measured by in-study diseaseprogression measuresThe most consistently reported measure for in-studydisability progression was the proportion of people withMS with disability progression Disability progression wasdefined by an increase in the Expanded DisabilityStatus Scale (EDSS) of 1 point in those with a baselineEDSS score of 50 or lower or an increase of 05 point inthose with a baseline EDSS score of 55 or higher sustainedfor 3 or 6 months and detected over a 2-year study period(figure 3)
The following DMTs are more effective than placebo in re-ducing the risk of disability progression in people with RRMS(high confidence) daclizumab HYP20 dimethylfumarate1821 fingolimod910 IFN-β-1a 30 μg IM weekly2232
IFN-β-1a 44 μg subcutaneous 3 times weekly11 mitoxan-trone23 natalizumab12 pegylated IFN24 andteriflunomide2633 See safety note on page 7918a
The following DMTs are more effective than other DMTs inreducing the risk of disability progression in people withRRMS (high confidence) alemtuzumab (vs IFN-β-1a 44 μgsubcutaneous 3 times weekly) 1529 and ocrelizumab (vs IFN-β-1a 44 μg subcutaneous 3 times weekly)13
Cladribine14 is probably more effective than placebo in re-ducing the risk of disability progression in people with RRMS(moderate confidence)
Table Efficacy of disease-modifying therapies (DMTs) for reducing the annualized relapse rate (ARR) and risk of relapse at2 years (continued)
Confidencestrength
Reduction of the ARR Reduction of risk of relapse at 2 y
Compared withplacebo
Compared with otherDMTs Compared with placebo Compared with other DMTs
mdash mdash mdash IFN-β-1b subcutaneous alternate daye46e47
possibly no more effective than glatirameracetate (Copaxone)
Very low Azathioprine insufficientto support or refutee40
mdash Azathioprine insufficient tosupport or refutee40
mdash
Immunoglobulinsinsufficient to support orrefute3940e48e49
mdash Cyclophosphamideinsufficient to support orrefute (outcome measured at12 mo)e42
mdash
Pulsed corticosteroidsinsufficient to support orrefute30
mdash Methotrexate insufficient tosupport or refutee2
mdash
Rituximab insufficient tosupport or refute25
mdash Pulsed corticosteroidsinsufficient to support orrefute30
mdash
Abbreviations HYP = high-yield process IFN-β = interferon-β IM = intramusculara See safety note on page 7918ab Glatiramer acetate included as a reference comparator in a dimethyl fumarate study and not powered for study of noninferiority or superiority required byregulatory agency
794 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Daclizumab is probably more effective than IFN-β-1a 30 μgIM27 in reducing the risk of disability progression in people withRRMS (moderate confidence) See safety note on page 7918a
Pulsed corticosteroids30 are possibly more effective thanplacebo in reducing the risk of disability progression in peoplewith RRMS (low confidence)
The following DMTs are possibly no more effective thanplacebo in reducing the risk of disability progression in peoplewith RRMS (low confidence) glatiramer acetate183435 andpulsed corticosteroids added to IFN-β-1a IM once weekly36
Fingolimod is possibly no more effective than IFN-β-1a IMweekly in reducing the risk of disability progression over1 year (low confidence)16 See safety note on page 7918a
IFN-β-1a is possibly no more effective than glatiramer acetatein reducing the risk of disability progression over 3 years (lowconfidence)37
There is insufficient evidence to determine the efficacy of thefollowing DMTs compared with placebo in reducing the riskof disability progression in people with RRMS (very lowconfidence) azathioprine38 immunoglobulins3940 IFN-β-1bsubcutaneous alternate daye1 and methotrexatee2
IFN-β-1b alternate day is probably less effective than glatir-amer acetate in reducing the risk of disability progression over2 years (moderate confidence)e1
4 In peoplewith RRMSwho experience diseaseactivity while on a DMT is changing toa different DMT superior to continuing thepresent DMT in terms of relapse rate and MRI-detected T2 or gadolinium-enhancedlesion activityFor individuals with RRMS who experienced a relapse onIFN-β or glatiramer acetate alemtuzumab is more effectivethan IFN-β-1a 44 μg subcutaneous 3 times per week in re-ducing the ARR the relapse risk disability progression andrisk of new or enlarging T2 lesions over 2 years (highconfidence)15
In individuals with RRMS who experience 1 or more relapsesin the preceding 12 months on IFN-β adding natalizumab ismore effective than adding placebo in decreasing the risk ofrelapse over 2 years the ARR the risk of disability progressionover 2 years and the risk of new or enlarging T2 lesions at1 year (high confidence)e3
In individuals with RRMS who experienced one ormore relapses in the preceding 12 months on glatiramer ac-etate there is insufficient evidence to determine the efficacy ofnatalizumab added to glatiramer acetate compared with pla-cebo added to glatiramer acetate in decreasing the risk ofrelapse at 6 months (very low confidence)e4
Natalizumab added to glatiramer acetate is probably moreeffective than placebo added to glatiramer acetate in
Figure 3 Outcome Relative risk (RR) of in-study disability progression at 2 years relapsing-remitting multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aOutcome measured at 1 year bVersus interferon-β-1a cOutcomemeasured at 3 years dSee safety note on page 7918a
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 795
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
decreasing the cumulative number of new or enlarging T2lesions at 6 months (moderate confidence)e4
Note that natalizumab is not presently approvedrecommended as an add-on therapy to other DMTs owingto potential safety concerns associated with combined use ofthis medication
5 In people with progressive MS are DMTssuperior to placeboor otherDMTsasmeasuredby relapse rate or in-studydisease progression
Risk of relapseFigure 4 presents these data regarding risk of relapse IFN-β-1b subcutaneous alternate day (SPMS) is more effectivethan placebo in reducing the risk of relapse in people withprogressive MS (high confidence)e5e6
The following DMTs are probably more effective than placeboin reducing the risk of relapse in people with progressive MS(moderate confidence) IFN-β-1a 60 μg IM weekly (SPMS)e7
and mitoxantrone (worsening RRMS and SPMS)e8
There is insufficient evidence to determine the efficacy of thefollowing DMTs compared with placebo in reducing the riskof relapse in people with progressive MS (very low confi-dence) azathioprine38 immunoglobulinse9e10 and metho-trexate (chronic progressive MS older terminology that isundefined but included present PPMS and SPMS diseasetypes)e11 There is insufficient evidence to determine theefficacy of high-dose corticosteroids compared with low-dosecorticosteroidse12 in reducing the risk of relapse in peoplewith SPMS (very low confidence)
Disability progressionThe following DMTs are probably more effective than pla-cebo in reducing the risk of in-study disability progression inpeople with progressive MS (RRMS or SPMS moderateconfidence) mitoxantrone (worsening RRMS and SPMS)e13
and ocrelizumab (PPMS)e14
The following DMTs are possibly no more effective thanplacebo in reducing the risk of in-study disability progressionin people with progressive MS (low confidence) cladribine(SPMS)e15 fingolimod (PPMS)e16 glatiramer acetate(progressive forms of MSe17 and PPMSe18) IFN-β-1a 30 μgIM weekly (SPMSe7 and PPMSe19) IFN-β-1a subcutaneous 3times per week (SPMS)e20 IFN-β-1b subcutaneous alternateday (SPMSe5e6 and PPMSe21) and rituximab (PPMS)e22
There is insufficient evidence to determine the efficacy of thefollowing DMTs relative to placebo in reducing the risk of in-study disability progression in people with progressive MS(very low confidence) azathioprine38 corticosteroids addedto mitoxantronee23 cyclophosphamidee24e25 immunoglobu-linse9e10 and methotrexate (CPMS [PPMS])e11
There is insufficient evidence to determine the efficacy ofhigh-dose corticosteroids relative to low-dose cortico-steroidse26 in reducing the risk of in-study disability pro-gression in people with progressive MS (very lowconfidence)
6 What are the AEs of DMTs in people with MScompared with placebo (AE-relateddiscontinuation and serious or life-threatening AEs)A comprehensive review of adverse effects associated withDMTs is included in the full-text document (data supplementto the companion recommendations article linkslwwcomWNLA429) and table
7 In people with CIS are DMTs superior toplacebo in decreasing the risk of conversionto MSFigure 5 presents the data regarding risk of conversion to MSin people with CIS For individuals with CIS the followingDMTs are more effective than placebo in reducing the pro-portion of individuals converting to MS (high confidence)glatiramer acetatee27 and IFN-β-1a subcutaneous 3 timesweeklye28
Figure 4 Outcome Relative risk (RR) of relapse at 2 years secondary progressive multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aHigh-dose corticosteroids vs low-dose corticosteroids bOutcomemeasured at 3 years
796 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
For individuals with CIS the following DMTs are probablymore effective than placebo in reducing the proportion ofindividuals converting to MS (moderate confidence)cladribinee29 immunoglobulinse30 IFN-β-1a 30 μg IMweeklye31 IFN-β-1b subcutaneous alternate daye32 andteriflunomidee33
DiscussionMultiple DMTs are now approved for use in CIS or MSallowing people with MS and clinicians to consider DMTmechanism of action efficacy and AE profile in the decision-making process This systematic review was used to developa practice guideline for the use of DMT for MS acknowl-edging the limits of current evidence Measures of efficacysuch as long-term disability patient satisfaction quality of lifeand effects on MS symptoms may be important to thedecision-making process but ultimately remain inadequatelystudied Similarly there is a dearth of high-quality evidencepertaining to the comparative efficacy of specific DMTs orvarious treatment strategies (eg high-efficacy treatment vsstepped-care treatment protocols) Future studies addressingthese and other questions are needed to further informtreatment recommendations particularly those pertaining towhen to switch or stop DMTs
Author contributionsDr Rae-Grant study concept and design acquisition of dataanalysis or interpretation of data draftingrevising the man-uscript critical revision of the manuscript for important in-tellectual content study supervision Dr Day study conceptand design analysis or interpretation of data draftingrevisingthe manuscript critical revision of the manuscript for im-portant intellectual content Dr Marrie study concept anddesign acquisition of data analysis or interpretation of datadraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Rabinsteinanalysis or interpretation of data draftingrevising the man-uscript Dr Cree study concept and design draftingrevising
the manuscript critical revision of the manuscript forimportant intellectual content Dr Gronseth analysis orinterpretation of data critical revision of the manuscript forimportant intellectual content study supervisionDr Haboubi study concept and design analysis or in-terpretation of data draftingrevising the manuscriptJ Halper study concept and design draftingrevising themanuscript critical revision of the manuscript for importantintellectual content Dr Hosey critical revision of the man-uscript for important intellectual content Dr Jones studyconcept and design draftingrevising the manuscript criticalrevision of the manuscript for important intellectual contentDr Lisak study concept and design draftingrevising themanuscript critical revision of the manuscript for importantintellectual content Dr Pelletier study concept and designdraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Potrebicstudy concept and design acquisition of data analysis or in-terpretation of data draftingrevising the manuscript criticalrevision of the manuscript for important intellectual contentstudy supervision C Sitcov study concept and designdraftingrevising the manuscript critical revision of themanuscript for important intellectual content R Sommersdraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Stacho-wiak study concept and design draftingrevising the manu-script critical revision of the manuscript for importantintellectual content TSD Getchius study supervisionSA Merillat draftingrevising the manuscript study super-vision Dr Pringsheim study concept and design acquisitionof data analysis or interpretation of data draftingrevising themanuscript critical revision of the manuscript for importantintellectual content study supervision
AcknowledgmentThe authors thank the North American Research CommitteeonMultiple Sclerosis (NARCOMS) Registry for its assistancein administering an outcomes survey the results of whichwere included in this practice guideline NARCOMS issupported in part by the Consortium of Multiple SclerosisCenters (CMSC) and the Foundation of the CMSC
Figure 5 Outcome Relative risk (RR) of conversion to multiple sclerosis over 2 years
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aOutcome measured at 1 year bOutcome measured at 3 years
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 797
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study fundingThis practice guideline was developed with financial supportfrom the American Academy of Neurology (AAN) Authorswho serve as AAN subcommittee members or as method-ologists (AR-G GSD AR GSG MH SP TP) orwho are or were AAN staffmembers (TSDG SAM) werereimbursed by the AAN for expenses related to travel tosubcommittee meetings where drafts of manuscripts werereviewed All authors on the panel were reimbursed by theAAN for expenses related to travel to 2 in-person meetings
DisclosureA Rae-Grant receives royalties from 2 textbooks he haspublished 1 on neurology and 1 on multiple sclerosis (MS)organizes and receives honoraria for grand rounds and neu-rology review courses and is local primary investigator fora clinical trial with MedDay Pharmaceuticals for which hereceives no personal compensation A Rabinstein reports nodisclosures relevant to the manuscript B Cree has receivedcompensation for consulting from AbbVie Biogen EMDSerono GeNeuro GenzymeSanofi Aventis Novartis andShire has given expert testimony and prepared an affidavit formedical malpractice cases (1 or 2 per year) within his area ofexpertise and has acted as consultant in a legal proceeding forAcorda and Biogen G Gronseth serves as associate editor(level of evidence review) for Neurologyreg serves on the edi-torial advisory board for Neurology Now and is compensatedby the American Academy of Neurology (AAN) for meth-odologic activities G Day holds stock in ANI PharmaceuticalsM Haboubi has received travel reimbursement and honorariafor grand rounds presentations in Madisonville KY J Halperand J Hosey report no disclosures relevant to the manuscriptD Jones has received personal compensation for consultingfrom Biogen and Genzyme has received honoraria fromthe Consortium of Multiple Sclerosis Centers (CMSC) theMultiple Sclerosis Association of America (MSAA) and thePharmacy Quality Alliance has received institutional researchsupport from Biogen and the National MS Society (NMSS)has received salary support from the CMSC and has receivedtravel reimbursement from Biogen and Genzyme and fromthe AAN Can Do MS the CMSC and the MSAA R Lisakserved as the President of the CMSC and serves as a memberof the Board of the DMC Foundation has served on scientificadvisory boards for Mallinckrodt Syntimmune Celegeneand Alexion serves as chair of the adjudication committee ofa clinical trial (PAREXEL) has received funding for travelfrom the CMSC the GBSCIDP Foundation Internationalthe NMSS and Syntimmune for travel to consultants meet-ings has served as a journal editor for Clinical and Experi-mental Neuroimmunology andClinical Neuropharmacology hasreceived publishing royalties from Willey for InternationalNeurology A Clinical Approach has received honoraria fromMallinckrodt Syntimmune and Teva Pharmaceuticals andfrom the consulting agencies AlphaSights ClearViewHealthcare Partners GLC and Insights Consulting hasserved on a speakers bureau for Teva Pharmaceuticals for talks
unrelated to pharmaceuticals has received research supportfrom Mallinckrodt for investigator-initiated wet bench stud-ies and from Acorda Avanir Biogen Chugai GenentechMedImmune Novartis and Teva Pharmaceuticals for servingas a site investigator in multicenter trials has given experttestimony prepared an affidavit and acted as witness for TevaPharmaceuticals and has acted as an expert on a patent casefor Acorda Wayne State University has received financialcompensation from the NMSS for his salary as principle in-vestigator for a research grant RA Marrie receives researchgrants from nonprofit organizations including CanadianInstitutes of Health Research (CIHR) the CMSC Crohnrsquosand Colitis Canada the NMSS the Multiple Sclerosis Societyof Canada the Multiple Sclerosis Scientific Research Foun-dation and Research Manitoba and serves on the editorialboard of Neurology D Pelletier has served on scientific ad-visory boards for Biogen EMD Serono GenzymeSanofiAventis Hoffman LaRoche and Novartis has received re-search support for Biogen Genzyme Hoffman LaRoche andthe National Institute of Neurologic Disorders and Stroke ofthe NIH and has received honoraria for providing consultingservices at scientific advisory board meetings from BiogenEMD Serono GenzymeSanofi Aventis Hoffman LaRocheand Novartis S Potrebic received an honorarium from CDIQuality Institute PLE for participation in a headacheappropriate-use criteria panel for imaging and receives travelreimbursement from the AAN for attending AAN ResidencyIn-Service Training Examination Work Group meetingsAAN Axon Registry Committee meetings AAN GuidelineDevelopment Dissemination and Implementation Sub-committee meetings and the Guidelines International Net-work North America Evidence-based Guidelines AffectingPolicy Practice and Stakeholders (E-GAPPS) conference RSommers C Sitcov and J Stachowiak report no disclosuresrelevant to the manuscript T Getchius is a former AANemployee and reports no relevant disclosures S Merillatreports no disclosures relevant to the manuscript T Prings-heim has received research support from the CIHR and ShireCanada Inc Go to NeurologyorgN for full disclosures
DisclaimerClinical practice guidelines practice advisories systematicreviews and other guidance published by the AmericanAcademy of Neurology and its affiliates are assessments ofcurrent scientific and clinical information provided as an ed-ucational service The information (1) should not be con-sidered inclusive of all proper treatments methods of care oras a statement of the standard of care (2) is not continuallyupdated and may not reflect the most recent evidence (newevidence may emerge between the time information is de-veloped and when it is published or read) (3) addresses onlythe question(s) specifically identified (4) does not mandateany particular course of medical care and (5) is not intendedto substitute for the independent professional judgment of thetreating provider as the information does not account forindividual variation among people with MS In all cases theselected course of action should be considered by the treating
798 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
provider in the context of treating the individual patientUse of the information is voluntary AAN provides thisinformation on an ldquoas isrdquo basis and makes no warrantyexpressed or implied regarding the information AANspecifically disclaims any warranties of merchantability orfitness for a particular use or purpose AAN assumes noresponsibility for any injury or damage to persons or propertyarising out of or related to any use of this information or forany errors or omissions
Conflict of interest statementThe American Academy of Neurology (AAN) is committedto producing independent critical and truthful clinical prac-tice guidelines (CPGs) Significant efforts are made to mini-mize the potential for conflicts of interest to influence therecommendations of this CPG To the extent possiblethe AAN keeps separate those who have a financial stake inthe success or failure of the products appraised in the CPGsand the developers of the guidelines Conflict of interest formswere obtained from all authors and reviewed by an oversightcommittee prior to project initiation AAN limits the partic-ipation of authors with substantial conflicts of interest TheAAN forbids commercial participation in or funding ofguideline projects Drafts of the guideline have been reviewedby at least 3 AAN committees a network of neurologistsNeurologyreg peer reviewers and representatives from relatedfields The AAN Guideline Author Conflict of Interest Policycan be viewed at aancom For complete information on thisprocess access the 2011 AAN process manual as amended4
Received July 12 2017 Accepted in final form February 15 2018
References1 Rae-Grant A Day GS Marrie RA et al for the Guideline Development Dissemi-
nation and Implementation Subcommittee of the American Academy of NeurologyPractice guideline recommendations summary disease-modifying therapies for adultswith multiple sclerosis report of the Guideline Development Dissemination andImplementation Subcommittee of the American Academy of Neurology Neurology201890777ndash788
2 Goodin DS Frohman EM Garmany GP et al on behalf of the American Academy ofNeurology and the MS Council for Clinical Practice Guidelines Disease-modifyingtherapies in multiple sclerosis subcommittee of the American Academy of Neurologyand the MS Council for Clinical Practice Guidelines report of the Therapeutics andTechnology Assessment Subcommittee of the American Academy of Neurology andthe MS Council for Clinical Practice Guidelines Neurology 200258169ndash178
3 Browne P Chandraratna D Angood C et al Atlas of Multiple Sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
4 American Academy of Neurology Clinical Practice Guideline Process Manual 2011ed [online] St Paul The American Academy of Neurology 2011 Available at aancompolicy-and-guidelinesguidelinesabout-guidelines2 Accessed March 122016
5 Institute of Medicine Eden J Levit L Berg A Morton S editors Committee onStandards for Systematic Reviews of Comparative Effectiveness ResearchWashington DC National Academies Press 2011
6 Institute of Medicine Committee on Standards for Developing Trustworthy ClinicalPractice Guidelines Clinical Practice Guidelines We Can Trust Washington DCNational Academies Press 2011
7 Shea BJ Grimshaw JM Wells GA et al Development of AMSTAR a measurementtool to assess the methodological quality of systematic reviews BMC Med ResMethodol 2007710
8 Guyatt GH Oxman AD Schunemann HJ Tugwell P Knottnerus A GRADEguidelines a new series of articles in the Journal of Clinical Epidemiology J ClinEpidemiol 201164380ndash382
8a Biogen and AbbVie announce the voluntary worldwide withdrawal of marketingauthorizations for ZINBRYTAreg (daclizumab) for relapsing multiple sclerosis [press
release] Available at httpmediabiogencompress-releaseautoimmune-diseasesbiogenC2A0and-abbvie-announceC2A0-voluntaryC2A0worldwide-withdrawal-marketi Issued March 2 2018 Accessed March 5 2018
9 Kappos L Radue EW OrsquoConnor P et al A placebo-controlled trial of oral fingolimodin relapsing multiple sclerosis N Engl J Med 2010362387ndash401
10 Calabresi P Radue EW Goodin D et al Safety and efficacy of fingolimod in patientswith relapsing-remitting multiple sclerosis (FREEDOMS II) a double-blind rando-mised placebo-controlled phase 3 trial Lancet Neurol 201413545ndash556
11 PRISMS (Prevention of Relapses and Disability by Interferon Beta-la Subcutaneouslyin Multiple Sclerosis) Study Group Randomised double-blind placebo-controlledstudy of interferon beta-1a in relapsingremitting multiple sclerosis Lancet 19983521498ndash1504
12 Polman C OrsquoConnor PW Havdrova E et al A randomized placebo-controlled trialof natalizumab for relapsing multiple sclerosis N Engl J Med 2006354899ndash910
13 Hauser SL Bar-Or A Comi G et al for the OPERA I and OPERA II ClinicalInvestigators Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosisN Engl J Med 2017376221ndash234
14 Giovannoni G Comi G Cook S et al on behalf of the CLARITY Study Group Aplacebo-controlled trial of oral cladribine for relapsing multiple sclerosis N Engl JMed 2010362416ndash426
15 Cohen J Coles AJ Arnold DL et al CARE-MS I Investigators Alemtuzumab versusinterferon beta 1a as first-line treatment for patients with relapsing-remitting multiplesclerosis a randomised controlled phase 3 trial Lancet 20123801819ndash1828
16 Cohen J Barkhof F Comi G et al on behalf of the TRANSFORMS Study GroupOral fingolimod or intramuscular interferon for relapsing multiple sclerosis N Engl JMed 2010362402ndash415
17 Panitch H Goodin DS Francis G et al or the University of British Columbia MSMRI Research Group Randomized comparative study of interferon beta-1a treat-ment regimens in MS the EVIDENCE Trial Neurology 2002591496ndash1506
18 Fox R Miller DH Phillips JT et al on behalf of the CONFIRM Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 or glatiramer in multiple sclerosisN Engl J Med 20123671087ndash1097
19 Massacesi L Tramacere I Amoroso S et al Azathioprine versus beta interferons forrelapsing-remitting multiple sclerosis a multicentre randomized non-inferiority trialPLoS One 20149e113371
20 Gold R Giovannoni G Selmaj K et al on behalf of the SELECT Study Inves-tigators Daclizumab high-yield process in relapsing-remitting multiple sclerosis(SELECT) a randomised double-blind placebo-controlled trial Lancet 20133812167ndash2175
21 Gold R Kappos L Arnold DL et al on behalf of the DEFINE Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 for relapsing multiple sclerosisN Engl J Med 20123671098ndash1107
22 Vollmer T Sorensen PS Selmaj K et al on behalf of the BRAVO Study Group Arandomized placebo-controlled phase III trial of oral laquinimod for multiple scle-rosis J Neurol 2014261773ndash783
23 Millefiorini E Gasperini C Pozzilli C et al Randomized placebo-controlled trial ofmitoxantrone in relapsing-remitting multiple sclerosis 24-month clinical and MRIoutcome J Neurol 1997244153ndash159
24 Calabresi P Kieseier BC Arnold DL et al for the ADVANCE Study InvestigatorsPegylated interferon beta-1a for relapsing-remitting multiple sclerosis (ADVANCE)a randomised phase 3 double-blind study Lancet Neurol 201413657ndash665
25 Hauser SL Waubant E Arnold DL et al for the HERMES Trial Group B-celldepletion with rituximab in relapsing-remitting multiple sclerosis N Engl J Med 2008358676ndash688
26 OrsquoConnor P Wolinsky JS Confavreux C et al for the TEMSO Trial Group Ran-domized trial of oral teriflunomide for relapsing multiple sclerosis N Engl J Med20113651293ndash1303
27 Kappos L Wiendl H Selmaj K et al Daclizumab HYP versus interferon beta-1a inrelapsing multiple sclerosis N Engl J Med 20153731418ndash1428
28 Frohman EM Cutter G Remington G et al A randomized blinded parallel-grouppilot trial of mycophenolate mofetil (CellCept) compared with interferon beta-1a(Avonex) in patients with relapsing-remitting multiple sclerosis Ther Adv NeurolDisord 2010315ndash28
29 Coles A TwymanCL Arnold DL et al the CARE-MS II Investigators Alemtuzumab forpatients with relapsing multiple sclerosis after disease-modifying therapy a randomisedcontrolled phase 3 trial Lancet 2012801829ndash1839
30 Zivadinov R Rudick RA De Masi R et al Effects of IV methylprednisolone on brainatrophy in relapsing-remitting MS Neurology 2001571239ndash1247
31 Remington GM Treadaway K Frohman T et al A one-year prospective ran-domized placebo-controlled quadruple-blinded phase II safety pilot trial ofcombination therapy with interferon beta-1a and mycophenolate mofetil in earlyrelapsing-remitting multiple sclerosis (TIME MS) Ther Adv Neurol Disord 201033ndash13
32 Jacobs L Cookfair DL Rudick RA et al Intramuscular interferon beta-1a for diseaseprogression in relapsing multiple sclerosis Ann Neurol 199639285ndash294
33 Confavreux C OrsquoConnor P Comi G et al for the TOWER Trial Group Oralteriflunomide for patients with relapsing multiple sclerosis (TOWER) a randomiseddouble-blind placebo-controlled phase 3 trial Lancet Neurol 201413247ndash256
34 Johnson KP Brooks BR Cohen JA et al Copolymer 1 reduces relapse rate andimproves disability in relapsing-remitting multiple sclerosis results of a phase IIImulticenter double-blind placebo-controlled trial Copolymer 1 Multiple SclerosisStudy Group Neurology 1995451268ndash1276
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 799
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
35 Bornstein MB Miller A Slagle S et al A pilot trial of COP 1 in exacerbating-remittingmultiple sclerosis N Engl J Med 1987317408ndash414
36 Ravnborg M Sorensen PS Andersson M et al Methylprednisolone in combinationwith interferon beta-1a for relapsing-remitting multiple sclerosis (MECOMBINstudy) a multicentre double-blind randomized placebo-controlled parallel-groupstudy Lancet Neurol 20109672ndash680
37 Lublin FD Cofield SS Cutter GR et al on behalf of the CombiRx InvestigatorsRandomized study combining interferon and glatiramer acetate in multiple sclerosisAnn Neurol 201373327ndash340
38 Ellison G Myers LW Mickey MR et al A placebo-controlled randomized double-masked variable dosage clinical trial of azathioprine with and without methylpred-nisolone in multiple sclerosis Neurology 1989391018ndash1026
39 Fazekas F Deisenhammer F Stasser-Fuchs S Nahler G Mamoli B Randomisedplacebo-controlled trial of monthly intravenous immunoglobulin therapy in relapsing-remitting multiple sclerosis Austrian Immunoglobulin in Multiple Sclerosis StudyGroup Lancet 1997349598ndash593
40 Achiron A Gabbay U Gilad R et al Intravenous immunoglobulin treatment inmultiple sclerosis effect on relapses Neurology 199850398ndash402
Neurologyreg Online CME Program
Earn CME while reading Neurology This program is available only to online Neurology subscribers Read the articles markedCME go to Neurologyorg and click on CME This will provide all of the information necessary to get started TheAmerican Academy of Neurology (AAN) is accredited by the Accreditation Council for Continuing Medical Education(ACCME) to sponsor continuing medical education for physicians Neurology is planned and produced in accordance withthe ACCME Essentials For more information contact AAN Member Services at 800-879-1960
NeurologyorgN Offers Important Information to Patients and Their Families
The Neurologyreg Patient Page providesbull A critical review of ground-breaking discoveries in neurologic research that are written especially for patients and their familiesbull Up-to-date patient information about many neurologic diseasesbull Links to additional information resources for neurologic patients
All Neurology Patient Page articles can be easily downloaded and printed and may be reproduced to distribute for educational purposesClick on the lsquoPatientsrsquo link on the home page (NeurologyorgN) for a complete index of Patient Pages
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Audio summaries of current issues Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
800 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000005345201890789-800 Neurology
Alexander Rae-Grant Gregory S Day Ruth Ann Marrie et al Implementation Subcommittee of the American Academy of Neurology
with multiple sclerosis Report of the Guideline Development Dissemination and Comprehensive systematic review summary Disease-modifying therapies for adults
This information is current as of April 23 2018
ServicesUpdated Information amp
httpnneurologyorgcontent9017789fullincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl201804239017789DC1
Supplementary material can be found at
References httpnneurologyorgcontent9017789fullref-list-1
This article cites 37 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9017789fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2018 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

Rituximab25 and teriflunomide26 are probably more effectivethan placebo in reducing the volume or number of MRI-detected T2 lesions (moderate confidence)
The following DMTs are probably more effective thanother DMTs in reducing the volume or number of MRI-detected T2 lesions (moderate confidence) alemtuzumab
Figure 1 Outcome Annualized relapse rate relapsing-remitting multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit RM = raw mean difference UCL = upper confidence limit aVersus interferon-β-1a 44 μg 3 times perweek subcutaneously bSee safety note on page 7918a
Figure 2 Outcome Relative risk of relapse at 2 years relapsing-remitting multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit RR = risk ratio UCL = upper confidence limit aRelative to interferon alone bOutcome assessed at 18months cOutcome assessed at 1 year dSee safety note on page 7918a
792 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table Efficacy of disease-modifying therapies (DMTs) for reducing the annualized relapse rate (ARR) and risk of relapse at2 years
Confidencestrength
Reduction of the ARR Reduction of risk of relapse at 2 y
Compared withplacebo
Compared with otherDMTs Compared with placebo Compared with other DMTs
High Cladribine14e34 moreeffective
Alemtuzumab moreeffective than IFN-β-1asubcutaneous 3 times perwk1529
Daclizumab HYPa moreeffective (outcome measuredat 1 y)20
Alemtuzumab1529 more effective than IFN-β-1a subcutaneous 3 times per wk
Daclizumab HYPa moreeffective20
Azathioprine moreeffective thanβ-interferons19e35
Dimethyl fumarate1821 moreeffective
mdash
Dimethyl fumarate1821
more effectivebFingolimod more effectivethan IFN-β-1a IM once perwk16
Fingolimod910 more effective mdash
Fingolimod910e36 moreeffective
Ocrelizumab moreeffective than IFN-β-1asubcutaneous 3 times perwk13
Immunoglobulins3940 moreeffective
mdash
Glatiramer acetate1834e37 more effective
mdash IFN-β-1a IM once per wk2232
more effectivemdash
Natalizumab12 moreeffective
mdash IFN-β-1a subcutaneous 3times per wk11 more effective
mdash
Pegylated IFN24 moreeffective
mdash Mitoxantrone23 moreeffective
mdash
Teriflunomide26e38e39
more effectivemdash Natalizumab12 more effective mdash
mdash mdash Pegylated IFN more effective(outcome measured at 1 y)24
mdash
Moderate Azathioprine probablymore effectivee40
mdash Cladribine probably moreeffective14
Daclizumab HYPa probably more effectivethan IFN-β-1a IM once per wk (outcomemeasured at 3 y)27
IFN-β-1a IM once perwk22 probably moreeffective
mdash Glatiramer acetate probablymore effective183435
IFN-β-1b subcutaneousalternate daye1 probablymore effective
mdash IFN-β-1b subcutaneousalternate day probably moreeffectivee1
mdash
Pulsed corticosteroidsadded to IFN-β-1a36e41
probably more effective
mdash Pulsed corticosteroids addedto IFN-β-1ae41 probably moreeffective
mdash
mdash DaclizumabHYP27 IFN-β-1aonce perwk probablymoreeffectivea
Rituximab probably moreeffective (outcome measuredat 1 y)25
mdash
mdash mdash Teriflunomide26 probablymore effective
mdash
Low Cyclophosphamidee42
possibly more effectivemdash mdash Mycophenolate mofetil plus IFN-β-1a IM
weekly31e43 possibly no more effective thanIFN plus placebo (outcome measured at 1 y)
mdash mdash mdash Complex nonbiologic generic glatirameracetate (Glatopa)e44 possibly no moreeffective than glatiramer acetate (Copaxone)
mdash mdash mdash IFN-β-1a IM once weekly37 possibly no moreeffective than glatiramer acetate (Copaxone)
mdash mdash mdash IFN-β-1a subcutaneous 3 times weeklye45
possibly no more effective than glatirameracetate (Copaxone)
Continued
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 793
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
(vs IFN-β-1a subcutaneous 3 times per week)15 and dacli-zumab (vs IFN-β-1a IM once weekly)27 See safety note onpage 7918a
There is insufficient evidence to determine the efficacy ofmycophenolate mofetil vs IFN-β-1a once weekly for reducingthe volume or number of MRI-detected T2 lesions (very lowconfidence)28
There is insufficient evidence to determine the efficacy of pulsedcorticosteroids29 relative to placebo for reducing the volume ornumber of MRI-detected T2 lesions (very low confidence)
Reducing loss of parenchymal volumeOcrelizumab13 is more effective than IFN-β-1a 44 μg sub-cutaneous 3 times weekly in reducing loss of parenchymalvolume (high confidence)
Alemtuzumab is probably more effective than IFN-β-1a 44 μgsubcutaneous 3 times weekly29 in reducing loss of paren-chymal volume (moderate confidence)
Pulsed corticosteroids30 are probably more effective thanplacebo in reducing loss of parenchymal volume (moderateconfidence)
There is insufficient evidence to determine the efficacy of thefollowing DMTs relative to placebo in reducing loss of pa-renchymal volume (very low confidence) IFN-β-1a 30 μg IMweekly22 andmycophenolate mofetil added to IFN-β-1a 30 μgIM weekly31
3 In people with RRMS are DMTs superior toplacebo or other DMTs in preventing diseaseprogression as measured by in-study diseaseprogression measuresThe most consistently reported measure for in-studydisability progression was the proportion of people withMS with disability progression Disability progression wasdefined by an increase in the Expanded DisabilityStatus Scale (EDSS) of 1 point in those with a baselineEDSS score of 50 or lower or an increase of 05 point inthose with a baseline EDSS score of 55 or higher sustainedfor 3 or 6 months and detected over a 2-year study period(figure 3)
The following DMTs are more effective than placebo in re-ducing the risk of disability progression in people with RRMS(high confidence) daclizumab HYP20 dimethylfumarate1821 fingolimod910 IFN-β-1a 30 μg IM weekly2232
IFN-β-1a 44 μg subcutaneous 3 times weekly11 mitoxan-trone23 natalizumab12 pegylated IFN24 andteriflunomide2633 See safety note on page 7918a
The following DMTs are more effective than other DMTs inreducing the risk of disability progression in people withRRMS (high confidence) alemtuzumab (vs IFN-β-1a 44 μgsubcutaneous 3 times weekly) 1529 and ocrelizumab (vs IFN-β-1a 44 μg subcutaneous 3 times weekly)13
Cladribine14 is probably more effective than placebo in re-ducing the risk of disability progression in people with RRMS(moderate confidence)
Table Efficacy of disease-modifying therapies (DMTs) for reducing the annualized relapse rate (ARR) and risk of relapse at2 years (continued)
Confidencestrength
Reduction of the ARR Reduction of risk of relapse at 2 y
Compared withplacebo
Compared with otherDMTs Compared with placebo Compared with other DMTs
mdash mdash mdash IFN-β-1b subcutaneous alternate daye46e47
possibly no more effective than glatirameracetate (Copaxone)
Very low Azathioprine insufficientto support or refutee40
mdash Azathioprine insufficient tosupport or refutee40
mdash
Immunoglobulinsinsufficient to support orrefute3940e48e49
mdash Cyclophosphamideinsufficient to support orrefute (outcome measured at12 mo)e42
mdash
Pulsed corticosteroidsinsufficient to support orrefute30
mdash Methotrexate insufficient tosupport or refutee2
mdash
Rituximab insufficient tosupport or refute25
mdash Pulsed corticosteroidsinsufficient to support orrefute30
mdash
Abbreviations HYP = high-yield process IFN-β = interferon-β IM = intramusculara See safety note on page 7918ab Glatiramer acetate included as a reference comparator in a dimethyl fumarate study and not powered for study of noninferiority or superiority required byregulatory agency
794 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Daclizumab is probably more effective than IFN-β-1a 30 μgIM27 in reducing the risk of disability progression in people withRRMS (moderate confidence) See safety note on page 7918a
Pulsed corticosteroids30 are possibly more effective thanplacebo in reducing the risk of disability progression in peoplewith RRMS (low confidence)
The following DMTs are possibly no more effective thanplacebo in reducing the risk of disability progression in peoplewith RRMS (low confidence) glatiramer acetate183435 andpulsed corticosteroids added to IFN-β-1a IM once weekly36
Fingolimod is possibly no more effective than IFN-β-1a IMweekly in reducing the risk of disability progression over1 year (low confidence)16 See safety note on page 7918a
IFN-β-1a is possibly no more effective than glatiramer acetatein reducing the risk of disability progression over 3 years (lowconfidence)37
There is insufficient evidence to determine the efficacy of thefollowing DMTs compared with placebo in reducing the riskof disability progression in people with RRMS (very lowconfidence) azathioprine38 immunoglobulins3940 IFN-β-1bsubcutaneous alternate daye1 and methotrexatee2
IFN-β-1b alternate day is probably less effective than glatir-amer acetate in reducing the risk of disability progression over2 years (moderate confidence)e1
4 In peoplewith RRMSwho experience diseaseactivity while on a DMT is changing toa different DMT superior to continuing thepresent DMT in terms of relapse rate and MRI-detected T2 or gadolinium-enhancedlesion activityFor individuals with RRMS who experienced a relapse onIFN-β or glatiramer acetate alemtuzumab is more effectivethan IFN-β-1a 44 μg subcutaneous 3 times per week in re-ducing the ARR the relapse risk disability progression andrisk of new or enlarging T2 lesions over 2 years (highconfidence)15
In individuals with RRMS who experience 1 or more relapsesin the preceding 12 months on IFN-β adding natalizumab ismore effective than adding placebo in decreasing the risk ofrelapse over 2 years the ARR the risk of disability progressionover 2 years and the risk of new or enlarging T2 lesions at1 year (high confidence)e3
In individuals with RRMS who experienced one ormore relapses in the preceding 12 months on glatiramer ac-etate there is insufficient evidence to determine the efficacy ofnatalizumab added to glatiramer acetate compared with pla-cebo added to glatiramer acetate in decreasing the risk ofrelapse at 6 months (very low confidence)e4
Natalizumab added to glatiramer acetate is probably moreeffective than placebo added to glatiramer acetate in
Figure 3 Outcome Relative risk (RR) of in-study disability progression at 2 years relapsing-remitting multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aOutcome measured at 1 year bVersus interferon-β-1a cOutcomemeasured at 3 years dSee safety note on page 7918a
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 795
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
decreasing the cumulative number of new or enlarging T2lesions at 6 months (moderate confidence)e4
Note that natalizumab is not presently approvedrecommended as an add-on therapy to other DMTs owingto potential safety concerns associated with combined use ofthis medication
5 In people with progressive MS are DMTssuperior to placeboor otherDMTsasmeasuredby relapse rate or in-studydisease progression
Risk of relapseFigure 4 presents these data regarding risk of relapse IFN-β-1b subcutaneous alternate day (SPMS) is more effectivethan placebo in reducing the risk of relapse in people withprogressive MS (high confidence)e5e6
The following DMTs are probably more effective than placeboin reducing the risk of relapse in people with progressive MS(moderate confidence) IFN-β-1a 60 μg IM weekly (SPMS)e7
and mitoxantrone (worsening RRMS and SPMS)e8
There is insufficient evidence to determine the efficacy of thefollowing DMTs compared with placebo in reducing the riskof relapse in people with progressive MS (very low confi-dence) azathioprine38 immunoglobulinse9e10 and metho-trexate (chronic progressive MS older terminology that isundefined but included present PPMS and SPMS diseasetypes)e11 There is insufficient evidence to determine theefficacy of high-dose corticosteroids compared with low-dosecorticosteroidse12 in reducing the risk of relapse in peoplewith SPMS (very low confidence)
Disability progressionThe following DMTs are probably more effective than pla-cebo in reducing the risk of in-study disability progression inpeople with progressive MS (RRMS or SPMS moderateconfidence) mitoxantrone (worsening RRMS and SPMS)e13
and ocrelizumab (PPMS)e14
The following DMTs are possibly no more effective thanplacebo in reducing the risk of in-study disability progressionin people with progressive MS (low confidence) cladribine(SPMS)e15 fingolimod (PPMS)e16 glatiramer acetate(progressive forms of MSe17 and PPMSe18) IFN-β-1a 30 μgIM weekly (SPMSe7 and PPMSe19) IFN-β-1a subcutaneous 3times per week (SPMS)e20 IFN-β-1b subcutaneous alternateday (SPMSe5e6 and PPMSe21) and rituximab (PPMS)e22
There is insufficient evidence to determine the efficacy of thefollowing DMTs relative to placebo in reducing the risk of in-study disability progression in people with progressive MS(very low confidence) azathioprine38 corticosteroids addedto mitoxantronee23 cyclophosphamidee24e25 immunoglobu-linse9e10 and methotrexate (CPMS [PPMS])e11
There is insufficient evidence to determine the efficacy ofhigh-dose corticosteroids relative to low-dose cortico-steroidse26 in reducing the risk of in-study disability pro-gression in people with progressive MS (very lowconfidence)
6 What are the AEs of DMTs in people with MScompared with placebo (AE-relateddiscontinuation and serious or life-threatening AEs)A comprehensive review of adverse effects associated withDMTs is included in the full-text document (data supplementto the companion recommendations article linkslwwcomWNLA429) and table
7 In people with CIS are DMTs superior toplacebo in decreasing the risk of conversionto MSFigure 5 presents the data regarding risk of conversion to MSin people with CIS For individuals with CIS the followingDMTs are more effective than placebo in reducing the pro-portion of individuals converting to MS (high confidence)glatiramer acetatee27 and IFN-β-1a subcutaneous 3 timesweeklye28
Figure 4 Outcome Relative risk (RR) of relapse at 2 years secondary progressive multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aHigh-dose corticosteroids vs low-dose corticosteroids bOutcomemeasured at 3 years
796 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
For individuals with CIS the following DMTs are probablymore effective than placebo in reducing the proportion ofindividuals converting to MS (moderate confidence)cladribinee29 immunoglobulinse30 IFN-β-1a 30 μg IMweeklye31 IFN-β-1b subcutaneous alternate daye32 andteriflunomidee33
DiscussionMultiple DMTs are now approved for use in CIS or MSallowing people with MS and clinicians to consider DMTmechanism of action efficacy and AE profile in the decision-making process This systematic review was used to developa practice guideline for the use of DMT for MS acknowl-edging the limits of current evidence Measures of efficacysuch as long-term disability patient satisfaction quality of lifeand effects on MS symptoms may be important to thedecision-making process but ultimately remain inadequatelystudied Similarly there is a dearth of high-quality evidencepertaining to the comparative efficacy of specific DMTs orvarious treatment strategies (eg high-efficacy treatment vsstepped-care treatment protocols) Future studies addressingthese and other questions are needed to further informtreatment recommendations particularly those pertaining towhen to switch or stop DMTs
Author contributionsDr Rae-Grant study concept and design acquisition of dataanalysis or interpretation of data draftingrevising the man-uscript critical revision of the manuscript for important in-tellectual content study supervision Dr Day study conceptand design analysis or interpretation of data draftingrevisingthe manuscript critical revision of the manuscript for im-portant intellectual content Dr Marrie study concept anddesign acquisition of data analysis or interpretation of datadraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Rabinsteinanalysis or interpretation of data draftingrevising the man-uscript Dr Cree study concept and design draftingrevising
the manuscript critical revision of the manuscript forimportant intellectual content Dr Gronseth analysis orinterpretation of data critical revision of the manuscript forimportant intellectual content study supervisionDr Haboubi study concept and design analysis or in-terpretation of data draftingrevising the manuscriptJ Halper study concept and design draftingrevising themanuscript critical revision of the manuscript for importantintellectual content Dr Hosey critical revision of the man-uscript for important intellectual content Dr Jones studyconcept and design draftingrevising the manuscript criticalrevision of the manuscript for important intellectual contentDr Lisak study concept and design draftingrevising themanuscript critical revision of the manuscript for importantintellectual content Dr Pelletier study concept and designdraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Potrebicstudy concept and design acquisition of data analysis or in-terpretation of data draftingrevising the manuscript criticalrevision of the manuscript for important intellectual contentstudy supervision C Sitcov study concept and designdraftingrevising the manuscript critical revision of themanuscript for important intellectual content R Sommersdraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Stacho-wiak study concept and design draftingrevising the manu-script critical revision of the manuscript for importantintellectual content TSD Getchius study supervisionSA Merillat draftingrevising the manuscript study super-vision Dr Pringsheim study concept and design acquisitionof data analysis or interpretation of data draftingrevising themanuscript critical revision of the manuscript for importantintellectual content study supervision
AcknowledgmentThe authors thank the North American Research CommitteeonMultiple Sclerosis (NARCOMS) Registry for its assistancein administering an outcomes survey the results of whichwere included in this practice guideline NARCOMS issupported in part by the Consortium of Multiple SclerosisCenters (CMSC) and the Foundation of the CMSC
Figure 5 Outcome Relative risk (RR) of conversion to multiple sclerosis over 2 years
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aOutcome measured at 1 year bOutcome measured at 3 years
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 797
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study fundingThis practice guideline was developed with financial supportfrom the American Academy of Neurology (AAN) Authorswho serve as AAN subcommittee members or as method-ologists (AR-G GSD AR GSG MH SP TP) orwho are or were AAN staffmembers (TSDG SAM) werereimbursed by the AAN for expenses related to travel tosubcommittee meetings where drafts of manuscripts werereviewed All authors on the panel were reimbursed by theAAN for expenses related to travel to 2 in-person meetings
DisclosureA Rae-Grant receives royalties from 2 textbooks he haspublished 1 on neurology and 1 on multiple sclerosis (MS)organizes and receives honoraria for grand rounds and neu-rology review courses and is local primary investigator fora clinical trial with MedDay Pharmaceuticals for which hereceives no personal compensation A Rabinstein reports nodisclosures relevant to the manuscript B Cree has receivedcompensation for consulting from AbbVie Biogen EMDSerono GeNeuro GenzymeSanofi Aventis Novartis andShire has given expert testimony and prepared an affidavit formedical malpractice cases (1 or 2 per year) within his area ofexpertise and has acted as consultant in a legal proceeding forAcorda and Biogen G Gronseth serves as associate editor(level of evidence review) for Neurologyreg serves on the edi-torial advisory board for Neurology Now and is compensatedby the American Academy of Neurology (AAN) for meth-odologic activities G Day holds stock in ANI PharmaceuticalsM Haboubi has received travel reimbursement and honorariafor grand rounds presentations in Madisonville KY J Halperand J Hosey report no disclosures relevant to the manuscriptD Jones has received personal compensation for consultingfrom Biogen and Genzyme has received honoraria fromthe Consortium of Multiple Sclerosis Centers (CMSC) theMultiple Sclerosis Association of America (MSAA) and thePharmacy Quality Alliance has received institutional researchsupport from Biogen and the National MS Society (NMSS)has received salary support from the CMSC and has receivedtravel reimbursement from Biogen and Genzyme and fromthe AAN Can Do MS the CMSC and the MSAA R Lisakserved as the President of the CMSC and serves as a memberof the Board of the DMC Foundation has served on scientificadvisory boards for Mallinckrodt Syntimmune Celegeneand Alexion serves as chair of the adjudication committee ofa clinical trial (PAREXEL) has received funding for travelfrom the CMSC the GBSCIDP Foundation Internationalthe NMSS and Syntimmune for travel to consultants meet-ings has served as a journal editor for Clinical and Experi-mental Neuroimmunology andClinical Neuropharmacology hasreceived publishing royalties from Willey for InternationalNeurology A Clinical Approach has received honoraria fromMallinckrodt Syntimmune and Teva Pharmaceuticals andfrom the consulting agencies AlphaSights ClearViewHealthcare Partners GLC and Insights Consulting hasserved on a speakers bureau for Teva Pharmaceuticals for talks
unrelated to pharmaceuticals has received research supportfrom Mallinckrodt for investigator-initiated wet bench stud-ies and from Acorda Avanir Biogen Chugai GenentechMedImmune Novartis and Teva Pharmaceuticals for servingas a site investigator in multicenter trials has given experttestimony prepared an affidavit and acted as witness for TevaPharmaceuticals and has acted as an expert on a patent casefor Acorda Wayne State University has received financialcompensation from the NMSS for his salary as principle in-vestigator for a research grant RA Marrie receives researchgrants from nonprofit organizations including CanadianInstitutes of Health Research (CIHR) the CMSC Crohnrsquosand Colitis Canada the NMSS the Multiple Sclerosis Societyof Canada the Multiple Sclerosis Scientific Research Foun-dation and Research Manitoba and serves on the editorialboard of Neurology D Pelletier has served on scientific ad-visory boards for Biogen EMD Serono GenzymeSanofiAventis Hoffman LaRoche and Novartis has received re-search support for Biogen Genzyme Hoffman LaRoche andthe National Institute of Neurologic Disorders and Stroke ofthe NIH and has received honoraria for providing consultingservices at scientific advisory board meetings from BiogenEMD Serono GenzymeSanofi Aventis Hoffman LaRocheand Novartis S Potrebic received an honorarium from CDIQuality Institute PLE for participation in a headacheappropriate-use criteria panel for imaging and receives travelreimbursement from the AAN for attending AAN ResidencyIn-Service Training Examination Work Group meetingsAAN Axon Registry Committee meetings AAN GuidelineDevelopment Dissemination and Implementation Sub-committee meetings and the Guidelines International Net-work North America Evidence-based Guidelines AffectingPolicy Practice and Stakeholders (E-GAPPS) conference RSommers C Sitcov and J Stachowiak report no disclosuresrelevant to the manuscript T Getchius is a former AANemployee and reports no relevant disclosures S Merillatreports no disclosures relevant to the manuscript T Prings-heim has received research support from the CIHR and ShireCanada Inc Go to NeurologyorgN for full disclosures
DisclaimerClinical practice guidelines practice advisories systematicreviews and other guidance published by the AmericanAcademy of Neurology and its affiliates are assessments ofcurrent scientific and clinical information provided as an ed-ucational service The information (1) should not be con-sidered inclusive of all proper treatments methods of care oras a statement of the standard of care (2) is not continuallyupdated and may not reflect the most recent evidence (newevidence may emerge between the time information is de-veloped and when it is published or read) (3) addresses onlythe question(s) specifically identified (4) does not mandateany particular course of medical care and (5) is not intendedto substitute for the independent professional judgment of thetreating provider as the information does not account forindividual variation among people with MS In all cases theselected course of action should be considered by the treating
798 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
provider in the context of treating the individual patientUse of the information is voluntary AAN provides thisinformation on an ldquoas isrdquo basis and makes no warrantyexpressed or implied regarding the information AANspecifically disclaims any warranties of merchantability orfitness for a particular use or purpose AAN assumes noresponsibility for any injury or damage to persons or propertyarising out of or related to any use of this information or forany errors or omissions
Conflict of interest statementThe American Academy of Neurology (AAN) is committedto producing independent critical and truthful clinical prac-tice guidelines (CPGs) Significant efforts are made to mini-mize the potential for conflicts of interest to influence therecommendations of this CPG To the extent possiblethe AAN keeps separate those who have a financial stake inthe success or failure of the products appraised in the CPGsand the developers of the guidelines Conflict of interest formswere obtained from all authors and reviewed by an oversightcommittee prior to project initiation AAN limits the partic-ipation of authors with substantial conflicts of interest TheAAN forbids commercial participation in or funding ofguideline projects Drafts of the guideline have been reviewedby at least 3 AAN committees a network of neurologistsNeurologyreg peer reviewers and representatives from relatedfields The AAN Guideline Author Conflict of Interest Policycan be viewed at aancom For complete information on thisprocess access the 2011 AAN process manual as amended4
Received July 12 2017 Accepted in final form February 15 2018
References1 Rae-Grant A Day GS Marrie RA et al for the Guideline Development Dissemi-
nation and Implementation Subcommittee of the American Academy of NeurologyPractice guideline recommendations summary disease-modifying therapies for adultswith multiple sclerosis report of the Guideline Development Dissemination andImplementation Subcommittee of the American Academy of Neurology Neurology201890777ndash788
2 Goodin DS Frohman EM Garmany GP et al on behalf of the American Academy ofNeurology and the MS Council for Clinical Practice Guidelines Disease-modifyingtherapies in multiple sclerosis subcommittee of the American Academy of Neurologyand the MS Council for Clinical Practice Guidelines report of the Therapeutics andTechnology Assessment Subcommittee of the American Academy of Neurology andthe MS Council for Clinical Practice Guidelines Neurology 200258169ndash178
3 Browne P Chandraratna D Angood C et al Atlas of Multiple Sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
4 American Academy of Neurology Clinical Practice Guideline Process Manual 2011ed [online] St Paul The American Academy of Neurology 2011 Available at aancompolicy-and-guidelinesguidelinesabout-guidelines2 Accessed March 122016
5 Institute of Medicine Eden J Levit L Berg A Morton S editors Committee onStandards for Systematic Reviews of Comparative Effectiveness ResearchWashington DC National Academies Press 2011
6 Institute of Medicine Committee on Standards for Developing Trustworthy ClinicalPractice Guidelines Clinical Practice Guidelines We Can Trust Washington DCNational Academies Press 2011
7 Shea BJ Grimshaw JM Wells GA et al Development of AMSTAR a measurementtool to assess the methodological quality of systematic reviews BMC Med ResMethodol 2007710
8 Guyatt GH Oxman AD Schunemann HJ Tugwell P Knottnerus A GRADEguidelines a new series of articles in the Journal of Clinical Epidemiology J ClinEpidemiol 201164380ndash382
8a Biogen and AbbVie announce the voluntary worldwide withdrawal of marketingauthorizations for ZINBRYTAreg (daclizumab) for relapsing multiple sclerosis [press
release] Available at httpmediabiogencompress-releaseautoimmune-diseasesbiogenC2A0and-abbvie-announceC2A0-voluntaryC2A0worldwide-withdrawal-marketi Issued March 2 2018 Accessed March 5 2018
9 Kappos L Radue EW OrsquoConnor P et al A placebo-controlled trial of oral fingolimodin relapsing multiple sclerosis N Engl J Med 2010362387ndash401
10 Calabresi P Radue EW Goodin D et al Safety and efficacy of fingolimod in patientswith relapsing-remitting multiple sclerosis (FREEDOMS II) a double-blind rando-mised placebo-controlled phase 3 trial Lancet Neurol 201413545ndash556
11 PRISMS (Prevention of Relapses and Disability by Interferon Beta-la Subcutaneouslyin Multiple Sclerosis) Study Group Randomised double-blind placebo-controlledstudy of interferon beta-1a in relapsingremitting multiple sclerosis Lancet 19983521498ndash1504
12 Polman C OrsquoConnor PW Havdrova E et al A randomized placebo-controlled trialof natalizumab for relapsing multiple sclerosis N Engl J Med 2006354899ndash910
13 Hauser SL Bar-Or A Comi G et al for the OPERA I and OPERA II ClinicalInvestigators Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosisN Engl J Med 2017376221ndash234
14 Giovannoni G Comi G Cook S et al on behalf of the CLARITY Study Group Aplacebo-controlled trial of oral cladribine for relapsing multiple sclerosis N Engl JMed 2010362416ndash426
15 Cohen J Coles AJ Arnold DL et al CARE-MS I Investigators Alemtuzumab versusinterferon beta 1a as first-line treatment for patients with relapsing-remitting multiplesclerosis a randomised controlled phase 3 trial Lancet 20123801819ndash1828
16 Cohen J Barkhof F Comi G et al on behalf of the TRANSFORMS Study GroupOral fingolimod or intramuscular interferon for relapsing multiple sclerosis N Engl JMed 2010362402ndash415
17 Panitch H Goodin DS Francis G et al or the University of British Columbia MSMRI Research Group Randomized comparative study of interferon beta-1a treat-ment regimens in MS the EVIDENCE Trial Neurology 2002591496ndash1506
18 Fox R Miller DH Phillips JT et al on behalf of the CONFIRM Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 or glatiramer in multiple sclerosisN Engl J Med 20123671087ndash1097
19 Massacesi L Tramacere I Amoroso S et al Azathioprine versus beta interferons forrelapsing-remitting multiple sclerosis a multicentre randomized non-inferiority trialPLoS One 20149e113371
20 Gold R Giovannoni G Selmaj K et al on behalf of the SELECT Study Inves-tigators Daclizumab high-yield process in relapsing-remitting multiple sclerosis(SELECT) a randomised double-blind placebo-controlled trial Lancet 20133812167ndash2175
21 Gold R Kappos L Arnold DL et al on behalf of the DEFINE Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 for relapsing multiple sclerosisN Engl J Med 20123671098ndash1107
22 Vollmer T Sorensen PS Selmaj K et al on behalf of the BRAVO Study Group Arandomized placebo-controlled phase III trial of oral laquinimod for multiple scle-rosis J Neurol 2014261773ndash783
23 Millefiorini E Gasperini C Pozzilli C et al Randomized placebo-controlled trial ofmitoxantrone in relapsing-remitting multiple sclerosis 24-month clinical and MRIoutcome J Neurol 1997244153ndash159
24 Calabresi P Kieseier BC Arnold DL et al for the ADVANCE Study InvestigatorsPegylated interferon beta-1a for relapsing-remitting multiple sclerosis (ADVANCE)a randomised phase 3 double-blind study Lancet Neurol 201413657ndash665
25 Hauser SL Waubant E Arnold DL et al for the HERMES Trial Group B-celldepletion with rituximab in relapsing-remitting multiple sclerosis N Engl J Med 2008358676ndash688
26 OrsquoConnor P Wolinsky JS Confavreux C et al for the TEMSO Trial Group Ran-domized trial of oral teriflunomide for relapsing multiple sclerosis N Engl J Med20113651293ndash1303
27 Kappos L Wiendl H Selmaj K et al Daclizumab HYP versus interferon beta-1a inrelapsing multiple sclerosis N Engl J Med 20153731418ndash1428
28 Frohman EM Cutter G Remington G et al A randomized blinded parallel-grouppilot trial of mycophenolate mofetil (CellCept) compared with interferon beta-1a(Avonex) in patients with relapsing-remitting multiple sclerosis Ther Adv NeurolDisord 2010315ndash28
29 Coles A TwymanCL Arnold DL et al the CARE-MS II Investigators Alemtuzumab forpatients with relapsing multiple sclerosis after disease-modifying therapy a randomisedcontrolled phase 3 trial Lancet 2012801829ndash1839
30 Zivadinov R Rudick RA De Masi R et al Effects of IV methylprednisolone on brainatrophy in relapsing-remitting MS Neurology 2001571239ndash1247
31 Remington GM Treadaway K Frohman T et al A one-year prospective ran-domized placebo-controlled quadruple-blinded phase II safety pilot trial ofcombination therapy with interferon beta-1a and mycophenolate mofetil in earlyrelapsing-remitting multiple sclerosis (TIME MS) Ther Adv Neurol Disord 201033ndash13
32 Jacobs L Cookfair DL Rudick RA et al Intramuscular interferon beta-1a for diseaseprogression in relapsing multiple sclerosis Ann Neurol 199639285ndash294
33 Confavreux C OrsquoConnor P Comi G et al for the TOWER Trial Group Oralteriflunomide for patients with relapsing multiple sclerosis (TOWER) a randomiseddouble-blind placebo-controlled phase 3 trial Lancet Neurol 201413247ndash256
34 Johnson KP Brooks BR Cohen JA et al Copolymer 1 reduces relapse rate andimproves disability in relapsing-remitting multiple sclerosis results of a phase IIImulticenter double-blind placebo-controlled trial Copolymer 1 Multiple SclerosisStudy Group Neurology 1995451268ndash1276
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 799
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
35 Bornstein MB Miller A Slagle S et al A pilot trial of COP 1 in exacerbating-remittingmultiple sclerosis N Engl J Med 1987317408ndash414
36 Ravnborg M Sorensen PS Andersson M et al Methylprednisolone in combinationwith interferon beta-1a for relapsing-remitting multiple sclerosis (MECOMBINstudy) a multicentre double-blind randomized placebo-controlled parallel-groupstudy Lancet Neurol 20109672ndash680
37 Lublin FD Cofield SS Cutter GR et al on behalf of the CombiRx InvestigatorsRandomized study combining interferon and glatiramer acetate in multiple sclerosisAnn Neurol 201373327ndash340
38 Ellison G Myers LW Mickey MR et al A placebo-controlled randomized double-masked variable dosage clinical trial of azathioprine with and without methylpred-nisolone in multiple sclerosis Neurology 1989391018ndash1026
39 Fazekas F Deisenhammer F Stasser-Fuchs S Nahler G Mamoli B Randomisedplacebo-controlled trial of monthly intravenous immunoglobulin therapy in relapsing-remitting multiple sclerosis Austrian Immunoglobulin in Multiple Sclerosis StudyGroup Lancet 1997349598ndash593
40 Achiron A Gabbay U Gilad R et al Intravenous immunoglobulin treatment inmultiple sclerosis effect on relapses Neurology 199850398ndash402
Neurologyreg Online CME Program
Earn CME while reading Neurology This program is available only to online Neurology subscribers Read the articles markedCME go to Neurologyorg and click on CME This will provide all of the information necessary to get started TheAmerican Academy of Neurology (AAN) is accredited by the Accreditation Council for Continuing Medical Education(ACCME) to sponsor continuing medical education for physicians Neurology is planned and produced in accordance withthe ACCME Essentials For more information contact AAN Member Services at 800-879-1960
NeurologyorgN Offers Important Information to Patients and Their Families
The Neurologyreg Patient Page providesbull A critical review of ground-breaking discoveries in neurologic research that are written especially for patients and their familiesbull Up-to-date patient information about many neurologic diseasesbull Links to additional information resources for neurologic patients
All Neurology Patient Page articles can be easily downloaded and printed and may be reproduced to distribute for educational purposesClick on the lsquoPatientsrsquo link on the home page (NeurologyorgN) for a complete index of Patient Pages
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Audio summaries of current issues Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
800 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000005345201890789-800 Neurology
Alexander Rae-Grant Gregory S Day Ruth Ann Marrie et al Implementation Subcommittee of the American Academy of Neurology
with multiple sclerosis Report of the Guideline Development Dissemination and Comprehensive systematic review summary Disease-modifying therapies for adults
This information is current as of April 23 2018
ServicesUpdated Information amp
httpnneurologyorgcontent9017789fullincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl201804239017789DC1
Supplementary material can be found at
References httpnneurologyorgcontent9017789fullref-list-1
This article cites 37 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9017789fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2018 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
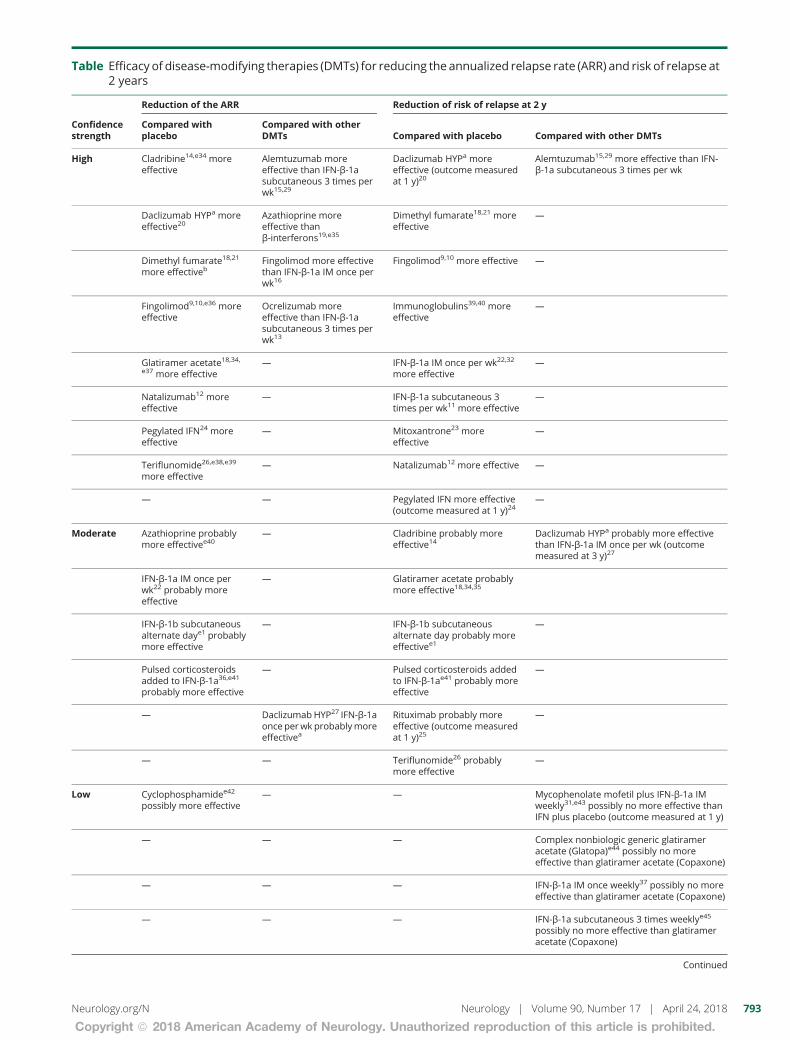
Table Efficacy of disease-modifying therapies (DMTs) for reducing the annualized relapse rate (ARR) and risk of relapse at2 years
Confidencestrength
Reduction of the ARR Reduction of risk of relapse at 2 y
Compared withplacebo
Compared with otherDMTs Compared with placebo Compared with other DMTs
High Cladribine14e34 moreeffective
Alemtuzumab moreeffective than IFN-β-1asubcutaneous 3 times perwk1529
Daclizumab HYPa moreeffective (outcome measuredat 1 y)20
Alemtuzumab1529 more effective than IFN-β-1a subcutaneous 3 times per wk
Daclizumab HYPa moreeffective20
Azathioprine moreeffective thanβ-interferons19e35
Dimethyl fumarate1821 moreeffective
mdash
Dimethyl fumarate1821
more effectivebFingolimod more effectivethan IFN-β-1a IM once perwk16
Fingolimod910 more effective mdash
Fingolimod910e36 moreeffective
Ocrelizumab moreeffective than IFN-β-1asubcutaneous 3 times perwk13
Immunoglobulins3940 moreeffective
mdash
Glatiramer acetate1834e37 more effective
mdash IFN-β-1a IM once per wk2232
more effectivemdash
Natalizumab12 moreeffective
mdash IFN-β-1a subcutaneous 3times per wk11 more effective
mdash
Pegylated IFN24 moreeffective
mdash Mitoxantrone23 moreeffective
mdash
Teriflunomide26e38e39
more effectivemdash Natalizumab12 more effective mdash
mdash mdash Pegylated IFN more effective(outcome measured at 1 y)24
mdash
Moderate Azathioprine probablymore effectivee40
mdash Cladribine probably moreeffective14
Daclizumab HYPa probably more effectivethan IFN-β-1a IM once per wk (outcomemeasured at 3 y)27
IFN-β-1a IM once perwk22 probably moreeffective
mdash Glatiramer acetate probablymore effective183435
IFN-β-1b subcutaneousalternate daye1 probablymore effective
mdash IFN-β-1b subcutaneousalternate day probably moreeffectivee1
mdash
Pulsed corticosteroidsadded to IFN-β-1a36e41
probably more effective
mdash Pulsed corticosteroids addedto IFN-β-1ae41 probably moreeffective
mdash
mdash DaclizumabHYP27 IFN-β-1aonce perwk probablymoreeffectivea
Rituximab probably moreeffective (outcome measuredat 1 y)25
mdash
mdash mdash Teriflunomide26 probablymore effective
mdash
Low Cyclophosphamidee42
possibly more effectivemdash mdash Mycophenolate mofetil plus IFN-β-1a IM
weekly31e43 possibly no more effective thanIFN plus placebo (outcome measured at 1 y)
mdash mdash mdash Complex nonbiologic generic glatirameracetate (Glatopa)e44 possibly no moreeffective than glatiramer acetate (Copaxone)
mdash mdash mdash IFN-β-1a IM once weekly37 possibly no moreeffective than glatiramer acetate (Copaxone)
mdash mdash mdash IFN-β-1a subcutaneous 3 times weeklye45
possibly no more effective than glatirameracetate (Copaxone)
Continued
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 793
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
(vs IFN-β-1a subcutaneous 3 times per week)15 and dacli-zumab (vs IFN-β-1a IM once weekly)27 See safety note onpage 7918a
There is insufficient evidence to determine the efficacy ofmycophenolate mofetil vs IFN-β-1a once weekly for reducingthe volume or number of MRI-detected T2 lesions (very lowconfidence)28
There is insufficient evidence to determine the efficacy of pulsedcorticosteroids29 relative to placebo for reducing the volume ornumber of MRI-detected T2 lesions (very low confidence)
Reducing loss of parenchymal volumeOcrelizumab13 is more effective than IFN-β-1a 44 μg sub-cutaneous 3 times weekly in reducing loss of parenchymalvolume (high confidence)
Alemtuzumab is probably more effective than IFN-β-1a 44 μgsubcutaneous 3 times weekly29 in reducing loss of paren-chymal volume (moderate confidence)
Pulsed corticosteroids30 are probably more effective thanplacebo in reducing loss of parenchymal volume (moderateconfidence)
There is insufficient evidence to determine the efficacy of thefollowing DMTs relative to placebo in reducing loss of pa-renchymal volume (very low confidence) IFN-β-1a 30 μg IMweekly22 andmycophenolate mofetil added to IFN-β-1a 30 μgIM weekly31
3 In people with RRMS are DMTs superior toplacebo or other DMTs in preventing diseaseprogression as measured by in-study diseaseprogression measuresThe most consistently reported measure for in-studydisability progression was the proportion of people withMS with disability progression Disability progression wasdefined by an increase in the Expanded DisabilityStatus Scale (EDSS) of 1 point in those with a baselineEDSS score of 50 or lower or an increase of 05 point inthose with a baseline EDSS score of 55 or higher sustainedfor 3 or 6 months and detected over a 2-year study period(figure 3)
The following DMTs are more effective than placebo in re-ducing the risk of disability progression in people with RRMS(high confidence) daclizumab HYP20 dimethylfumarate1821 fingolimod910 IFN-β-1a 30 μg IM weekly2232
IFN-β-1a 44 μg subcutaneous 3 times weekly11 mitoxan-trone23 natalizumab12 pegylated IFN24 andteriflunomide2633 See safety note on page 7918a
The following DMTs are more effective than other DMTs inreducing the risk of disability progression in people withRRMS (high confidence) alemtuzumab (vs IFN-β-1a 44 μgsubcutaneous 3 times weekly) 1529 and ocrelizumab (vs IFN-β-1a 44 μg subcutaneous 3 times weekly)13
Cladribine14 is probably more effective than placebo in re-ducing the risk of disability progression in people with RRMS(moderate confidence)
Table Efficacy of disease-modifying therapies (DMTs) for reducing the annualized relapse rate (ARR) and risk of relapse at2 years (continued)
Confidencestrength
Reduction of the ARR Reduction of risk of relapse at 2 y
Compared withplacebo
Compared with otherDMTs Compared with placebo Compared with other DMTs
mdash mdash mdash IFN-β-1b subcutaneous alternate daye46e47
possibly no more effective than glatirameracetate (Copaxone)
Very low Azathioprine insufficientto support or refutee40
mdash Azathioprine insufficient tosupport or refutee40
mdash
Immunoglobulinsinsufficient to support orrefute3940e48e49
mdash Cyclophosphamideinsufficient to support orrefute (outcome measured at12 mo)e42
mdash
Pulsed corticosteroidsinsufficient to support orrefute30
mdash Methotrexate insufficient tosupport or refutee2
mdash
Rituximab insufficient tosupport or refute25
mdash Pulsed corticosteroidsinsufficient to support orrefute30
mdash
Abbreviations HYP = high-yield process IFN-β = interferon-β IM = intramusculara See safety note on page 7918ab Glatiramer acetate included as a reference comparator in a dimethyl fumarate study and not powered for study of noninferiority or superiority required byregulatory agency
794 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Daclizumab is probably more effective than IFN-β-1a 30 μgIM27 in reducing the risk of disability progression in people withRRMS (moderate confidence) See safety note on page 7918a
Pulsed corticosteroids30 are possibly more effective thanplacebo in reducing the risk of disability progression in peoplewith RRMS (low confidence)
The following DMTs are possibly no more effective thanplacebo in reducing the risk of disability progression in peoplewith RRMS (low confidence) glatiramer acetate183435 andpulsed corticosteroids added to IFN-β-1a IM once weekly36
Fingolimod is possibly no more effective than IFN-β-1a IMweekly in reducing the risk of disability progression over1 year (low confidence)16 See safety note on page 7918a
IFN-β-1a is possibly no more effective than glatiramer acetatein reducing the risk of disability progression over 3 years (lowconfidence)37
There is insufficient evidence to determine the efficacy of thefollowing DMTs compared with placebo in reducing the riskof disability progression in people with RRMS (very lowconfidence) azathioprine38 immunoglobulins3940 IFN-β-1bsubcutaneous alternate daye1 and methotrexatee2
IFN-β-1b alternate day is probably less effective than glatir-amer acetate in reducing the risk of disability progression over2 years (moderate confidence)e1
4 In peoplewith RRMSwho experience diseaseactivity while on a DMT is changing toa different DMT superior to continuing thepresent DMT in terms of relapse rate and MRI-detected T2 or gadolinium-enhancedlesion activityFor individuals with RRMS who experienced a relapse onIFN-β or glatiramer acetate alemtuzumab is more effectivethan IFN-β-1a 44 μg subcutaneous 3 times per week in re-ducing the ARR the relapse risk disability progression andrisk of new or enlarging T2 lesions over 2 years (highconfidence)15
In individuals with RRMS who experience 1 or more relapsesin the preceding 12 months on IFN-β adding natalizumab ismore effective than adding placebo in decreasing the risk ofrelapse over 2 years the ARR the risk of disability progressionover 2 years and the risk of new or enlarging T2 lesions at1 year (high confidence)e3
In individuals with RRMS who experienced one ormore relapses in the preceding 12 months on glatiramer ac-etate there is insufficient evidence to determine the efficacy ofnatalizumab added to glatiramer acetate compared with pla-cebo added to glatiramer acetate in decreasing the risk ofrelapse at 6 months (very low confidence)e4
Natalizumab added to glatiramer acetate is probably moreeffective than placebo added to glatiramer acetate in
Figure 3 Outcome Relative risk (RR) of in-study disability progression at 2 years relapsing-remitting multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aOutcome measured at 1 year bVersus interferon-β-1a cOutcomemeasured at 3 years dSee safety note on page 7918a
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 795
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
decreasing the cumulative number of new or enlarging T2lesions at 6 months (moderate confidence)e4
Note that natalizumab is not presently approvedrecommended as an add-on therapy to other DMTs owingto potential safety concerns associated with combined use ofthis medication
5 In people with progressive MS are DMTssuperior to placeboor otherDMTsasmeasuredby relapse rate or in-studydisease progression
Risk of relapseFigure 4 presents these data regarding risk of relapse IFN-β-1b subcutaneous alternate day (SPMS) is more effectivethan placebo in reducing the risk of relapse in people withprogressive MS (high confidence)e5e6
The following DMTs are probably more effective than placeboin reducing the risk of relapse in people with progressive MS(moderate confidence) IFN-β-1a 60 μg IM weekly (SPMS)e7
and mitoxantrone (worsening RRMS and SPMS)e8
There is insufficient evidence to determine the efficacy of thefollowing DMTs compared with placebo in reducing the riskof relapse in people with progressive MS (very low confi-dence) azathioprine38 immunoglobulinse9e10 and metho-trexate (chronic progressive MS older terminology that isundefined but included present PPMS and SPMS diseasetypes)e11 There is insufficient evidence to determine theefficacy of high-dose corticosteroids compared with low-dosecorticosteroidse12 in reducing the risk of relapse in peoplewith SPMS (very low confidence)
Disability progressionThe following DMTs are probably more effective than pla-cebo in reducing the risk of in-study disability progression inpeople with progressive MS (RRMS or SPMS moderateconfidence) mitoxantrone (worsening RRMS and SPMS)e13
and ocrelizumab (PPMS)e14
The following DMTs are possibly no more effective thanplacebo in reducing the risk of in-study disability progressionin people with progressive MS (low confidence) cladribine(SPMS)e15 fingolimod (PPMS)e16 glatiramer acetate(progressive forms of MSe17 and PPMSe18) IFN-β-1a 30 μgIM weekly (SPMSe7 and PPMSe19) IFN-β-1a subcutaneous 3times per week (SPMS)e20 IFN-β-1b subcutaneous alternateday (SPMSe5e6 and PPMSe21) and rituximab (PPMS)e22
There is insufficient evidence to determine the efficacy of thefollowing DMTs relative to placebo in reducing the risk of in-study disability progression in people with progressive MS(very low confidence) azathioprine38 corticosteroids addedto mitoxantronee23 cyclophosphamidee24e25 immunoglobu-linse9e10 and methotrexate (CPMS [PPMS])e11
There is insufficient evidence to determine the efficacy ofhigh-dose corticosteroids relative to low-dose cortico-steroidse26 in reducing the risk of in-study disability pro-gression in people with progressive MS (very lowconfidence)
6 What are the AEs of DMTs in people with MScompared with placebo (AE-relateddiscontinuation and serious or life-threatening AEs)A comprehensive review of adverse effects associated withDMTs is included in the full-text document (data supplementto the companion recommendations article linkslwwcomWNLA429) and table
7 In people with CIS are DMTs superior toplacebo in decreasing the risk of conversionto MSFigure 5 presents the data regarding risk of conversion to MSin people with CIS For individuals with CIS the followingDMTs are more effective than placebo in reducing the pro-portion of individuals converting to MS (high confidence)glatiramer acetatee27 and IFN-β-1a subcutaneous 3 timesweeklye28
Figure 4 Outcome Relative risk (RR) of relapse at 2 years secondary progressive multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aHigh-dose corticosteroids vs low-dose corticosteroids bOutcomemeasured at 3 years
796 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
For individuals with CIS the following DMTs are probablymore effective than placebo in reducing the proportion ofindividuals converting to MS (moderate confidence)cladribinee29 immunoglobulinse30 IFN-β-1a 30 μg IMweeklye31 IFN-β-1b subcutaneous alternate daye32 andteriflunomidee33
DiscussionMultiple DMTs are now approved for use in CIS or MSallowing people with MS and clinicians to consider DMTmechanism of action efficacy and AE profile in the decision-making process This systematic review was used to developa practice guideline for the use of DMT for MS acknowl-edging the limits of current evidence Measures of efficacysuch as long-term disability patient satisfaction quality of lifeand effects on MS symptoms may be important to thedecision-making process but ultimately remain inadequatelystudied Similarly there is a dearth of high-quality evidencepertaining to the comparative efficacy of specific DMTs orvarious treatment strategies (eg high-efficacy treatment vsstepped-care treatment protocols) Future studies addressingthese and other questions are needed to further informtreatment recommendations particularly those pertaining towhen to switch or stop DMTs
Author contributionsDr Rae-Grant study concept and design acquisition of dataanalysis or interpretation of data draftingrevising the man-uscript critical revision of the manuscript for important in-tellectual content study supervision Dr Day study conceptand design analysis or interpretation of data draftingrevisingthe manuscript critical revision of the manuscript for im-portant intellectual content Dr Marrie study concept anddesign acquisition of data analysis or interpretation of datadraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Rabinsteinanalysis or interpretation of data draftingrevising the man-uscript Dr Cree study concept and design draftingrevising
the manuscript critical revision of the manuscript forimportant intellectual content Dr Gronseth analysis orinterpretation of data critical revision of the manuscript forimportant intellectual content study supervisionDr Haboubi study concept and design analysis or in-terpretation of data draftingrevising the manuscriptJ Halper study concept and design draftingrevising themanuscript critical revision of the manuscript for importantintellectual content Dr Hosey critical revision of the man-uscript for important intellectual content Dr Jones studyconcept and design draftingrevising the manuscript criticalrevision of the manuscript for important intellectual contentDr Lisak study concept and design draftingrevising themanuscript critical revision of the manuscript for importantintellectual content Dr Pelletier study concept and designdraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Potrebicstudy concept and design acquisition of data analysis or in-terpretation of data draftingrevising the manuscript criticalrevision of the manuscript for important intellectual contentstudy supervision C Sitcov study concept and designdraftingrevising the manuscript critical revision of themanuscript for important intellectual content R Sommersdraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Stacho-wiak study concept and design draftingrevising the manu-script critical revision of the manuscript for importantintellectual content TSD Getchius study supervisionSA Merillat draftingrevising the manuscript study super-vision Dr Pringsheim study concept and design acquisitionof data analysis or interpretation of data draftingrevising themanuscript critical revision of the manuscript for importantintellectual content study supervision
AcknowledgmentThe authors thank the North American Research CommitteeonMultiple Sclerosis (NARCOMS) Registry for its assistancein administering an outcomes survey the results of whichwere included in this practice guideline NARCOMS issupported in part by the Consortium of Multiple SclerosisCenters (CMSC) and the Foundation of the CMSC
Figure 5 Outcome Relative risk (RR) of conversion to multiple sclerosis over 2 years
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aOutcome measured at 1 year bOutcome measured at 3 years
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 797
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study fundingThis practice guideline was developed with financial supportfrom the American Academy of Neurology (AAN) Authorswho serve as AAN subcommittee members or as method-ologists (AR-G GSD AR GSG MH SP TP) orwho are or were AAN staffmembers (TSDG SAM) werereimbursed by the AAN for expenses related to travel tosubcommittee meetings where drafts of manuscripts werereviewed All authors on the panel were reimbursed by theAAN for expenses related to travel to 2 in-person meetings
DisclosureA Rae-Grant receives royalties from 2 textbooks he haspublished 1 on neurology and 1 on multiple sclerosis (MS)organizes and receives honoraria for grand rounds and neu-rology review courses and is local primary investigator fora clinical trial with MedDay Pharmaceuticals for which hereceives no personal compensation A Rabinstein reports nodisclosures relevant to the manuscript B Cree has receivedcompensation for consulting from AbbVie Biogen EMDSerono GeNeuro GenzymeSanofi Aventis Novartis andShire has given expert testimony and prepared an affidavit formedical malpractice cases (1 or 2 per year) within his area ofexpertise and has acted as consultant in a legal proceeding forAcorda and Biogen G Gronseth serves as associate editor(level of evidence review) for Neurologyreg serves on the edi-torial advisory board for Neurology Now and is compensatedby the American Academy of Neurology (AAN) for meth-odologic activities G Day holds stock in ANI PharmaceuticalsM Haboubi has received travel reimbursement and honorariafor grand rounds presentations in Madisonville KY J Halperand J Hosey report no disclosures relevant to the manuscriptD Jones has received personal compensation for consultingfrom Biogen and Genzyme has received honoraria fromthe Consortium of Multiple Sclerosis Centers (CMSC) theMultiple Sclerosis Association of America (MSAA) and thePharmacy Quality Alliance has received institutional researchsupport from Biogen and the National MS Society (NMSS)has received salary support from the CMSC and has receivedtravel reimbursement from Biogen and Genzyme and fromthe AAN Can Do MS the CMSC and the MSAA R Lisakserved as the President of the CMSC and serves as a memberof the Board of the DMC Foundation has served on scientificadvisory boards for Mallinckrodt Syntimmune Celegeneand Alexion serves as chair of the adjudication committee ofa clinical trial (PAREXEL) has received funding for travelfrom the CMSC the GBSCIDP Foundation Internationalthe NMSS and Syntimmune for travel to consultants meet-ings has served as a journal editor for Clinical and Experi-mental Neuroimmunology andClinical Neuropharmacology hasreceived publishing royalties from Willey for InternationalNeurology A Clinical Approach has received honoraria fromMallinckrodt Syntimmune and Teva Pharmaceuticals andfrom the consulting agencies AlphaSights ClearViewHealthcare Partners GLC and Insights Consulting hasserved on a speakers bureau for Teva Pharmaceuticals for talks
unrelated to pharmaceuticals has received research supportfrom Mallinckrodt for investigator-initiated wet bench stud-ies and from Acorda Avanir Biogen Chugai GenentechMedImmune Novartis and Teva Pharmaceuticals for servingas a site investigator in multicenter trials has given experttestimony prepared an affidavit and acted as witness for TevaPharmaceuticals and has acted as an expert on a patent casefor Acorda Wayne State University has received financialcompensation from the NMSS for his salary as principle in-vestigator for a research grant RA Marrie receives researchgrants from nonprofit organizations including CanadianInstitutes of Health Research (CIHR) the CMSC Crohnrsquosand Colitis Canada the NMSS the Multiple Sclerosis Societyof Canada the Multiple Sclerosis Scientific Research Foun-dation and Research Manitoba and serves on the editorialboard of Neurology D Pelletier has served on scientific ad-visory boards for Biogen EMD Serono GenzymeSanofiAventis Hoffman LaRoche and Novartis has received re-search support for Biogen Genzyme Hoffman LaRoche andthe National Institute of Neurologic Disorders and Stroke ofthe NIH and has received honoraria for providing consultingservices at scientific advisory board meetings from BiogenEMD Serono GenzymeSanofi Aventis Hoffman LaRocheand Novartis S Potrebic received an honorarium from CDIQuality Institute PLE for participation in a headacheappropriate-use criteria panel for imaging and receives travelreimbursement from the AAN for attending AAN ResidencyIn-Service Training Examination Work Group meetingsAAN Axon Registry Committee meetings AAN GuidelineDevelopment Dissemination and Implementation Sub-committee meetings and the Guidelines International Net-work North America Evidence-based Guidelines AffectingPolicy Practice and Stakeholders (E-GAPPS) conference RSommers C Sitcov and J Stachowiak report no disclosuresrelevant to the manuscript T Getchius is a former AANemployee and reports no relevant disclosures S Merillatreports no disclosures relevant to the manuscript T Prings-heim has received research support from the CIHR and ShireCanada Inc Go to NeurologyorgN for full disclosures
DisclaimerClinical practice guidelines practice advisories systematicreviews and other guidance published by the AmericanAcademy of Neurology and its affiliates are assessments ofcurrent scientific and clinical information provided as an ed-ucational service The information (1) should not be con-sidered inclusive of all proper treatments methods of care oras a statement of the standard of care (2) is not continuallyupdated and may not reflect the most recent evidence (newevidence may emerge between the time information is de-veloped and when it is published or read) (3) addresses onlythe question(s) specifically identified (4) does not mandateany particular course of medical care and (5) is not intendedto substitute for the independent professional judgment of thetreating provider as the information does not account forindividual variation among people with MS In all cases theselected course of action should be considered by the treating
798 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
provider in the context of treating the individual patientUse of the information is voluntary AAN provides thisinformation on an ldquoas isrdquo basis and makes no warrantyexpressed or implied regarding the information AANspecifically disclaims any warranties of merchantability orfitness for a particular use or purpose AAN assumes noresponsibility for any injury or damage to persons or propertyarising out of or related to any use of this information or forany errors or omissions
Conflict of interest statementThe American Academy of Neurology (AAN) is committedto producing independent critical and truthful clinical prac-tice guidelines (CPGs) Significant efforts are made to mini-mize the potential for conflicts of interest to influence therecommendations of this CPG To the extent possiblethe AAN keeps separate those who have a financial stake inthe success or failure of the products appraised in the CPGsand the developers of the guidelines Conflict of interest formswere obtained from all authors and reviewed by an oversightcommittee prior to project initiation AAN limits the partic-ipation of authors with substantial conflicts of interest TheAAN forbids commercial participation in or funding ofguideline projects Drafts of the guideline have been reviewedby at least 3 AAN committees a network of neurologistsNeurologyreg peer reviewers and representatives from relatedfields The AAN Guideline Author Conflict of Interest Policycan be viewed at aancom For complete information on thisprocess access the 2011 AAN process manual as amended4
Received July 12 2017 Accepted in final form February 15 2018
References1 Rae-Grant A Day GS Marrie RA et al for the Guideline Development Dissemi-
nation and Implementation Subcommittee of the American Academy of NeurologyPractice guideline recommendations summary disease-modifying therapies for adultswith multiple sclerosis report of the Guideline Development Dissemination andImplementation Subcommittee of the American Academy of Neurology Neurology201890777ndash788
2 Goodin DS Frohman EM Garmany GP et al on behalf of the American Academy ofNeurology and the MS Council for Clinical Practice Guidelines Disease-modifyingtherapies in multiple sclerosis subcommittee of the American Academy of Neurologyand the MS Council for Clinical Practice Guidelines report of the Therapeutics andTechnology Assessment Subcommittee of the American Academy of Neurology andthe MS Council for Clinical Practice Guidelines Neurology 200258169ndash178
3 Browne P Chandraratna D Angood C et al Atlas of Multiple Sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
4 American Academy of Neurology Clinical Practice Guideline Process Manual 2011ed [online] St Paul The American Academy of Neurology 2011 Available at aancompolicy-and-guidelinesguidelinesabout-guidelines2 Accessed March 122016
5 Institute of Medicine Eden J Levit L Berg A Morton S editors Committee onStandards for Systematic Reviews of Comparative Effectiveness ResearchWashington DC National Academies Press 2011
6 Institute of Medicine Committee on Standards for Developing Trustworthy ClinicalPractice Guidelines Clinical Practice Guidelines We Can Trust Washington DCNational Academies Press 2011
7 Shea BJ Grimshaw JM Wells GA et al Development of AMSTAR a measurementtool to assess the methodological quality of systematic reviews BMC Med ResMethodol 2007710
8 Guyatt GH Oxman AD Schunemann HJ Tugwell P Knottnerus A GRADEguidelines a new series of articles in the Journal of Clinical Epidemiology J ClinEpidemiol 201164380ndash382
8a Biogen and AbbVie announce the voluntary worldwide withdrawal of marketingauthorizations for ZINBRYTAreg (daclizumab) for relapsing multiple sclerosis [press
release] Available at httpmediabiogencompress-releaseautoimmune-diseasesbiogenC2A0and-abbvie-announceC2A0-voluntaryC2A0worldwide-withdrawal-marketi Issued March 2 2018 Accessed March 5 2018
9 Kappos L Radue EW OrsquoConnor P et al A placebo-controlled trial of oral fingolimodin relapsing multiple sclerosis N Engl J Med 2010362387ndash401
10 Calabresi P Radue EW Goodin D et al Safety and efficacy of fingolimod in patientswith relapsing-remitting multiple sclerosis (FREEDOMS II) a double-blind rando-mised placebo-controlled phase 3 trial Lancet Neurol 201413545ndash556
11 PRISMS (Prevention of Relapses and Disability by Interferon Beta-la Subcutaneouslyin Multiple Sclerosis) Study Group Randomised double-blind placebo-controlledstudy of interferon beta-1a in relapsingremitting multiple sclerosis Lancet 19983521498ndash1504
12 Polman C OrsquoConnor PW Havdrova E et al A randomized placebo-controlled trialof natalizumab for relapsing multiple sclerosis N Engl J Med 2006354899ndash910
13 Hauser SL Bar-Or A Comi G et al for the OPERA I and OPERA II ClinicalInvestigators Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosisN Engl J Med 2017376221ndash234
14 Giovannoni G Comi G Cook S et al on behalf of the CLARITY Study Group Aplacebo-controlled trial of oral cladribine for relapsing multiple sclerosis N Engl JMed 2010362416ndash426
15 Cohen J Coles AJ Arnold DL et al CARE-MS I Investigators Alemtuzumab versusinterferon beta 1a as first-line treatment for patients with relapsing-remitting multiplesclerosis a randomised controlled phase 3 trial Lancet 20123801819ndash1828
16 Cohen J Barkhof F Comi G et al on behalf of the TRANSFORMS Study GroupOral fingolimod or intramuscular interferon for relapsing multiple sclerosis N Engl JMed 2010362402ndash415
17 Panitch H Goodin DS Francis G et al or the University of British Columbia MSMRI Research Group Randomized comparative study of interferon beta-1a treat-ment regimens in MS the EVIDENCE Trial Neurology 2002591496ndash1506
18 Fox R Miller DH Phillips JT et al on behalf of the CONFIRM Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 or glatiramer in multiple sclerosisN Engl J Med 20123671087ndash1097
19 Massacesi L Tramacere I Amoroso S et al Azathioprine versus beta interferons forrelapsing-remitting multiple sclerosis a multicentre randomized non-inferiority trialPLoS One 20149e113371
20 Gold R Giovannoni G Selmaj K et al on behalf of the SELECT Study Inves-tigators Daclizumab high-yield process in relapsing-remitting multiple sclerosis(SELECT) a randomised double-blind placebo-controlled trial Lancet 20133812167ndash2175
21 Gold R Kappos L Arnold DL et al on behalf of the DEFINE Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 for relapsing multiple sclerosisN Engl J Med 20123671098ndash1107
22 Vollmer T Sorensen PS Selmaj K et al on behalf of the BRAVO Study Group Arandomized placebo-controlled phase III trial of oral laquinimod for multiple scle-rosis J Neurol 2014261773ndash783
23 Millefiorini E Gasperini C Pozzilli C et al Randomized placebo-controlled trial ofmitoxantrone in relapsing-remitting multiple sclerosis 24-month clinical and MRIoutcome J Neurol 1997244153ndash159
24 Calabresi P Kieseier BC Arnold DL et al for the ADVANCE Study InvestigatorsPegylated interferon beta-1a for relapsing-remitting multiple sclerosis (ADVANCE)a randomised phase 3 double-blind study Lancet Neurol 201413657ndash665
25 Hauser SL Waubant E Arnold DL et al for the HERMES Trial Group B-celldepletion with rituximab in relapsing-remitting multiple sclerosis N Engl J Med 2008358676ndash688
26 OrsquoConnor P Wolinsky JS Confavreux C et al for the TEMSO Trial Group Ran-domized trial of oral teriflunomide for relapsing multiple sclerosis N Engl J Med20113651293ndash1303
27 Kappos L Wiendl H Selmaj K et al Daclizumab HYP versus interferon beta-1a inrelapsing multiple sclerosis N Engl J Med 20153731418ndash1428
28 Frohman EM Cutter G Remington G et al A randomized blinded parallel-grouppilot trial of mycophenolate mofetil (CellCept) compared with interferon beta-1a(Avonex) in patients with relapsing-remitting multiple sclerosis Ther Adv NeurolDisord 2010315ndash28
29 Coles A TwymanCL Arnold DL et al the CARE-MS II Investigators Alemtuzumab forpatients with relapsing multiple sclerosis after disease-modifying therapy a randomisedcontrolled phase 3 trial Lancet 2012801829ndash1839
30 Zivadinov R Rudick RA De Masi R et al Effects of IV methylprednisolone on brainatrophy in relapsing-remitting MS Neurology 2001571239ndash1247
31 Remington GM Treadaway K Frohman T et al A one-year prospective ran-domized placebo-controlled quadruple-blinded phase II safety pilot trial ofcombination therapy with interferon beta-1a and mycophenolate mofetil in earlyrelapsing-remitting multiple sclerosis (TIME MS) Ther Adv Neurol Disord 201033ndash13
32 Jacobs L Cookfair DL Rudick RA et al Intramuscular interferon beta-1a for diseaseprogression in relapsing multiple sclerosis Ann Neurol 199639285ndash294
33 Confavreux C OrsquoConnor P Comi G et al for the TOWER Trial Group Oralteriflunomide for patients with relapsing multiple sclerosis (TOWER) a randomiseddouble-blind placebo-controlled phase 3 trial Lancet Neurol 201413247ndash256
34 Johnson KP Brooks BR Cohen JA et al Copolymer 1 reduces relapse rate andimproves disability in relapsing-remitting multiple sclerosis results of a phase IIImulticenter double-blind placebo-controlled trial Copolymer 1 Multiple SclerosisStudy Group Neurology 1995451268ndash1276
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 799
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
35 Bornstein MB Miller A Slagle S et al A pilot trial of COP 1 in exacerbating-remittingmultiple sclerosis N Engl J Med 1987317408ndash414
36 Ravnborg M Sorensen PS Andersson M et al Methylprednisolone in combinationwith interferon beta-1a for relapsing-remitting multiple sclerosis (MECOMBINstudy) a multicentre double-blind randomized placebo-controlled parallel-groupstudy Lancet Neurol 20109672ndash680
37 Lublin FD Cofield SS Cutter GR et al on behalf of the CombiRx InvestigatorsRandomized study combining interferon and glatiramer acetate in multiple sclerosisAnn Neurol 201373327ndash340
38 Ellison G Myers LW Mickey MR et al A placebo-controlled randomized double-masked variable dosage clinical trial of azathioprine with and without methylpred-nisolone in multiple sclerosis Neurology 1989391018ndash1026
39 Fazekas F Deisenhammer F Stasser-Fuchs S Nahler G Mamoli B Randomisedplacebo-controlled trial of monthly intravenous immunoglobulin therapy in relapsing-remitting multiple sclerosis Austrian Immunoglobulin in Multiple Sclerosis StudyGroup Lancet 1997349598ndash593
40 Achiron A Gabbay U Gilad R et al Intravenous immunoglobulin treatment inmultiple sclerosis effect on relapses Neurology 199850398ndash402
Neurologyreg Online CME Program
Earn CME while reading Neurology This program is available only to online Neurology subscribers Read the articles markedCME go to Neurologyorg and click on CME This will provide all of the information necessary to get started TheAmerican Academy of Neurology (AAN) is accredited by the Accreditation Council for Continuing Medical Education(ACCME) to sponsor continuing medical education for physicians Neurology is planned and produced in accordance withthe ACCME Essentials For more information contact AAN Member Services at 800-879-1960
NeurologyorgN Offers Important Information to Patients and Their Families
The Neurologyreg Patient Page providesbull A critical review of ground-breaking discoveries in neurologic research that are written especially for patients and their familiesbull Up-to-date patient information about many neurologic diseasesbull Links to additional information resources for neurologic patients
All Neurology Patient Page articles can be easily downloaded and printed and may be reproduced to distribute for educational purposesClick on the lsquoPatientsrsquo link on the home page (NeurologyorgN) for a complete index of Patient Pages
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Audio summaries of current issues Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
800 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000005345201890789-800 Neurology
Alexander Rae-Grant Gregory S Day Ruth Ann Marrie et al Implementation Subcommittee of the American Academy of Neurology
with multiple sclerosis Report of the Guideline Development Dissemination and Comprehensive systematic review summary Disease-modifying therapies for adults
This information is current as of April 23 2018
ServicesUpdated Information amp
httpnneurologyorgcontent9017789fullincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl201804239017789DC1
Supplementary material can be found at
References httpnneurologyorgcontent9017789fullref-list-1
This article cites 37 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9017789fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2018 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

(vs IFN-β-1a subcutaneous 3 times per week)15 and dacli-zumab (vs IFN-β-1a IM once weekly)27 See safety note onpage 7918a
There is insufficient evidence to determine the efficacy ofmycophenolate mofetil vs IFN-β-1a once weekly for reducingthe volume or number of MRI-detected T2 lesions (very lowconfidence)28
There is insufficient evidence to determine the efficacy of pulsedcorticosteroids29 relative to placebo for reducing the volume ornumber of MRI-detected T2 lesions (very low confidence)
Reducing loss of parenchymal volumeOcrelizumab13 is more effective than IFN-β-1a 44 μg sub-cutaneous 3 times weekly in reducing loss of parenchymalvolume (high confidence)
Alemtuzumab is probably more effective than IFN-β-1a 44 μgsubcutaneous 3 times weekly29 in reducing loss of paren-chymal volume (moderate confidence)
Pulsed corticosteroids30 are probably more effective thanplacebo in reducing loss of parenchymal volume (moderateconfidence)
There is insufficient evidence to determine the efficacy of thefollowing DMTs relative to placebo in reducing loss of pa-renchymal volume (very low confidence) IFN-β-1a 30 μg IMweekly22 andmycophenolate mofetil added to IFN-β-1a 30 μgIM weekly31
3 In people with RRMS are DMTs superior toplacebo or other DMTs in preventing diseaseprogression as measured by in-study diseaseprogression measuresThe most consistently reported measure for in-studydisability progression was the proportion of people withMS with disability progression Disability progression wasdefined by an increase in the Expanded DisabilityStatus Scale (EDSS) of 1 point in those with a baselineEDSS score of 50 or lower or an increase of 05 point inthose with a baseline EDSS score of 55 or higher sustainedfor 3 or 6 months and detected over a 2-year study period(figure 3)
The following DMTs are more effective than placebo in re-ducing the risk of disability progression in people with RRMS(high confidence) daclizumab HYP20 dimethylfumarate1821 fingolimod910 IFN-β-1a 30 μg IM weekly2232
IFN-β-1a 44 μg subcutaneous 3 times weekly11 mitoxan-trone23 natalizumab12 pegylated IFN24 andteriflunomide2633 See safety note on page 7918a
The following DMTs are more effective than other DMTs inreducing the risk of disability progression in people withRRMS (high confidence) alemtuzumab (vs IFN-β-1a 44 μgsubcutaneous 3 times weekly) 1529 and ocrelizumab (vs IFN-β-1a 44 μg subcutaneous 3 times weekly)13
Cladribine14 is probably more effective than placebo in re-ducing the risk of disability progression in people with RRMS(moderate confidence)
Table Efficacy of disease-modifying therapies (DMTs) for reducing the annualized relapse rate (ARR) and risk of relapse at2 years (continued)
Confidencestrength
Reduction of the ARR Reduction of risk of relapse at 2 y
Compared withplacebo
Compared with otherDMTs Compared with placebo Compared with other DMTs
mdash mdash mdash IFN-β-1b subcutaneous alternate daye46e47
possibly no more effective than glatirameracetate (Copaxone)
Very low Azathioprine insufficientto support or refutee40
mdash Azathioprine insufficient tosupport or refutee40
mdash
Immunoglobulinsinsufficient to support orrefute3940e48e49
mdash Cyclophosphamideinsufficient to support orrefute (outcome measured at12 mo)e42
mdash
Pulsed corticosteroidsinsufficient to support orrefute30
mdash Methotrexate insufficient tosupport or refutee2
mdash
Rituximab insufficient tosupport or refute25
mdash Pulsed corticosteroidsinsufficient to support orrefute30
mdash
Abbreviations HYP = high-yield process IFN-β = interferon-β IM = intramusculara See safety note on page 7918ab Glatiramer acetate included as a reference comparator in a dimethyl fumarate study and not powered for study of noninferiority or superiority required byregulatory agency
794 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Daclizumab is probably more effective than IFN-β-1a 30 μgIM27 in reducing the risk of disability progression in people withRRMS (moderate confidence) See safety note on page 7918a
Pulsed corticosteroids30 are possibly more effective thanplacebo in reducing the risk of disability progression in peoplewith RRMS (low confidence)
The following DMTs are possibly no more effective thanplacebo in reducing the risk of disability progression in peoplewith RRMS (low confidence) glatiramer acetate183435 andpulsed corticosteroids added to IFN-β-1a IM once weekly36
Fingolimod is possibly no more effective than IFN-β-1a IMweekly in reducing the risk of disability progression over1 year (low confidence)16 See safety note on page 7918a
IFN-β-1a is possibly no more effective than glatiramer acetatein reducing the risk of disability progression over 3 years (lowconfidence)37
There is insufficient evidence to determine the efficacy of thefollowing DMTs compared with placebo in reducing the riskof disability progression in people with RRMS (very lowconfidence) azathioprine38 immunoglobulins3940 IFN-β-1bsubcutaneous alternate daye1 and methotrexatee2
IFN-β-1b alternate day is probably less effective than glatir-amer acetate in reducing the risk of disability progression over2 years (moderate confidence)e1
4 In peoplewith RRMSwho experience diseaseactivity while on a DMT is changing toa different DMT superior to continuing thepresent DMT in terms of relapse rate and MRI-detected T2 or gadolinium-enhancedlesion activityFor individuals with RRMS who experienced a relapse onIFN-β or glatiramer acetate alemtuzumab is more effectivethan IFN-β-1a 44 μg subcutaneous 3 times per week in re-ducing the ARR the relapse risk disability progression andrisk of new or enlarging T2 lesions over 2 years (highconfidence)15
In individuals with RRMS who experience 1 or more relapsesin the preceding 12 months on IFN-β adding natalizumab ismore effective than adding placebo in decreasing the risk ofrelapse over 2 years the ARR the risk of disability progressionover 2 years and the risk of new or enlarging T2 lesions at1 year (high confidence)e3
In individuals with RRMS who experienced one ormore relapses in the preceding 12 months on glatiramer ac-etate there is insufficient evidence to determine the efficacy ofnatalizumab added to glatiramer acetate compared with pla-cebo added to glatiramer acetate in decreasing the risk ofrelapse at 6 months (very low confidence)e4
Natalizumab added to glatiramer acetate is probably moreeffective than placebo added to glatiramer acetate in
Figure 3 Outcome Relative risk (RR) of in-study disability progression at 2 years relapsing-remitting multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aOutcome measured at 1 year bVersus interferon-β-1a cOutcomemeasured at 3 years dSee safety note on page 7918a
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 795
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
decreasing the cumulative number of new or enlarging T2lesions at 6 months (moderate confidence)e4
Note that natalizumab is not presently approvedrecommended as an add-on therapy to other DMTs owingto potential safety concerns associated with combined use ofthis medication
5 In people with progressive MS are DMTssuperior to placeboor otherDMTsasmeasuredby relapse rate or in-studydisease progression
Risk of relapseFigure 4 presents these data regarding risk of relapse IFN-β-1b subcutaneous alternate day (SPMS) is more effectivethan placebo in reducing the risk of relapse in people withprogressive MS (high confidence)e5e6
The following DMTs are probably more effective than placeboin reducing the risk of relapse in people with progressive MS(moderate confidence) IFN-β-1a 60 μg IM weekly (SPMS)e7
and mitoxantrone (worsening RRMS and SPMS)e8
There is insufficient evidence to determine the efficacy of thefollowing DMTs compared with placebo in reducing the riskof relapse in people with progressive MS (very low confi-dence) azathioprine38 immunoglobulinse9e10 and metho-trexate (chronic progressive MS older terminology that isundefined but included present PPMS and SPMS diseasetypes)e11 There is insufficient evidence to determine theefficacy of high-dose corticosteroids compared with low-dosecorticosteroidse12 in reducing the risk of relapse in peoplewith SPMS (very low confidence)
Disability progressionThe following DMTs are probably more effective than pla-cebo in reducing the risk of in-study disability progression inpeople with progressive MS (RRMS or SPMS moderateconfidence) mitoxantrone (worsening RRMS and SPMS)e13
and ocrelizumab (PPMS)e14
The following DMTs are possibly no more effective thanplacebo in reducing the risk of in-study disability progressionin people with progressive MS (low confidence) cladribine(SPMS)e15 fingolimod (PPMS)e16 glatiramer acetate(progressive forms of MSe17 and PPMSe18) IFN-β-1a 30 μgIM weekly (SPMSe7 and PPMSe19) IFN-β-1a subcutaneous 3times per week (SPMS)e20 IFN-β-1b subcutaneous alternateday (SPMSe5e6 and PPMSe21) and rituximab (PPMS)e22
There is insufficient evidence to determine the efficacy of thefollowing DMTs relative to placebo in reducing the risk of in-study disability progression in people with progressive MS(very low confidence) azathioprine38 corticosteroids addedto mitoxantronee23 cyclophosphamidee24e25 immunoglobu-linse9e10 and methotrexate (CPMS [PPMS])e11
There is insufficient evidence to determine the efficacy ofhigh-dose corticosteroids relative to low-dose cortico-steroidse26 in reducing the risk of in-study disability pro-gression in people with progressive MS (very lowconfidence)
6 What are the AEs of DMTs in people with MScompared with placebo (AE-relateddiscontinuation and serious or life-threatening AEs)A comprehensive review of adverse effects associated withDMTs is included in the full-text document (data supplementto the companion recommendations article linkslwwcomWNLA429) and table
7 In people with CIS are DMTs superior toplacebo in decreasing the risk of conversionto MSFigure 5 presents the data regarding risk of conversion to MSin people with CIS For individuals with CIS the followingDMTs are more effective than placebo in reducing the pro-portion of individuals converting to MS (high confidence)glatiramer acetatee27 and IFN-β-1a subcutaneous 3 timesweeklye28
Figure 4 Outcome Relative risk (RR) of relapse at 2 years secondary progressive multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aHigh-dose corticosteroids vs low-dose corticosteroids bOutcomemeasured at 3 years
796 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
For individuals with CIS the following DMTs are probablymore effective than placebo in reducing the proportion ofindividuals converting to MS (moderate confidence)cladribinee29 immunoglobulinse30 IFN-β-1a 30 μg IMweeklye31 IFN-β-1b subcutaneous alternate daye32 andteriflunomidee33
DiscussionMultiple DMTs are now approved for use in CIS or MSallowing people with MS and clinicians to consider DMTmechanism of action efficacy and AE profile in the decision-making process This systematic review was used to developa practice guideline for the use of DMT for MS acknowl-edging the limits of current evidence Measures of efficacysuch as long-term disability patient satisfaction quality of lifeand effects on MS symptoms may be important to thedecision-making process but ultimately remain inadequatelystudied Similarly there is a dearth of high-quality evidencepertaining to the comparative efficacy of specific DMTs orvarious treatment strategies (eg high-efficacy treatment vsstepped-care treatment protocols) Future studies addressingthese and other questions are needed to further informtreatment recommendations particularly those pertaining towhen to switch or stop DMTs
Author contributionsDr Rae-Grant study concept and design acquisition of dataanalysis or interpretation of data draftingrevising the man-uscript critical revision of the manuscript for important in-tellectual content study supervision Dr Day study conceptand design analysis or interpretation of data draftingrevisingthe manuscript critical revision of the manuscript for im-portant intellectual content Dr Marrie study concept anddesign acquisition of data analysis or interpretation of datadraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Rabinsteinanalysis or interpretation of data draftingrevising the man-uscript Dr Cree study concept and design draftingrevising
the manuscript critical revision of the manuscript forimportant intellectual content Dr Gronseth analysis orinterpretation of data critical revision of the manuscript forimportant intellectual content study supervisionDr Haboubi study concept and design analysis or in-terpretation of data draftingrevising the manuscriptJ Halper study concept and design draftingrevising themanuscript critical revision of the manuscript for importantintellectual content Dr Hosey critical revision of the man-uscript for important intellectual content Dr Jones studyconcept and design draftingrevising the manuscript criticalrevision of the manuscript for important intellectual contentDr Lisak study concept and design draftingrevising themanuscript critical revision of the manuscript for importantintellectual content Dr Pelletier study concept and designdraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Potrebicstudy concept and design acquisition of data analysis or in-terpretation of data draftingrevising the manuscript criticalrevision of the manuscript for important intellectual contentstudy supervision C Sitcov study concept and designdraftingrevising the manuscript critical revision of themanuscript for important intellectual content R Sommersdraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Stacho-wiak study concept and design draftingrevising the manu-script critical revision of the manuscript for importantintellectual content TSD Getchius study supervisionSA Merillat draftingrevising the manuscript study super-vision Dr Pringsheim study concept and design acquisitionof data analysis or interpretation of data draftingrevising themanuscript critical revision of the manuscript for importantintellectual content study supervision
AcknowledgmentThe authors thank the North American Research CommitteeonMultiple Sclerosis (NARCOMS) Registry for its assistancein administering an outcomes survey the results of whichwere included in this practice guideline NARCOMS issupported in part by the Consortium of Multiple SclerosisCenters (CMSC) and the Foundation of the CMSC
Figure 5 Outcome Relative risk (RR) of conversion to multiple sclerosis over 2 years
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aOutcome measured at 1 year bOutcome measured at 3 years
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 797
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study fundingThis practice guideline was developed with financial supportfrom the American Academy of Neurology (AAN) Authorswho serve as AAN subcommittee members or as method-ologists (AR-G GSD AR GSG MH SP TP) orwho are or were AAN staffmembers (TSDG SAM) werereimbursed by the AAN for expenses related to travel tosubcommittee meetings where drafts of manuscripts werereviewed All authors on the panel were reimbursed by theAAN for expenses related to travel to 2 in-person meetings
DisclosureA Rae-Grant receives royalties from 2 textbooks he haspublished 1 on neurology and 1 on multiple sclerosis (MS)organizes and receives honoraria for grand rounds and neu-rology review courses and is local primary investigator fora clinical trial with MedDay Pharmaceuticals for which hereceives no personal compensation A Rabinstein reports nodisclosures relevant to the manuscript B Cree has receivedcompensation for consulting from AbbVie Biogen EMDSerono GeNeuro GenzymeSanofi Aventis Novartis andShire has given expert testimony and prepared an affidavit formedical malpractice cases (1 or 2 per year) within his area ofexpertise and has acted as consultant in a legal proceeding forAcorda and Biogen G Gronseth serves as associate editor(level of evidence review) for Neurologyreg serves on the edi-torial advisory board for Neurology Now and is compensatedby the American Academy of Neurology (AAN) for meth-odologic activities G Day holds stock in ANI PharmaceuticalsM Haboubi has received travel reimbursement and honorariafor grand rounds presentations in Madisonville KY J Halperand J Hosey report no disclosures relevant to the manuscriptD Jones has received personal compensation for consultingfrom Biogen and Genzyme has received honoraria fromthe Consortium of Multiple Sclerosis Centers (CMSC) theMultiple Sclerosis Association of America (MSAA) and thePharmacy Quality Alliance has received institutional researchsupport from Biogen and the National MS Society (NMSS)has received salary support from the CMSC and has receivedtravel reimbursement from Biogen and Genzyme and fromthe AAN Can Do MS the CMSC and the MSAA R Lisakserved as the President of the CMSC and serves as a memberof the Board of the DMC Foundation has served on scientificadvisory boards for Mallinckrodt Syntimmune Celegeneand Alexion serves as chair of the adjudication committee ofa clinical trial (PAREXEL) has received funding for travelfrom the CMSC the GBSCIDP Foundation Internationalthe NMSS and Syntimmune for travel to consultants meet-ings has served as a journal editor for Clinical and Experi-mental Neuroimmunology andClinical Neuropharmacology hasreceived publishing royalties from Willey for InternationalNeurology A Clinical Approach has received honoraria fromMallinckrodt Syntimmune and Teva Pharmaceuticals andfrom the consulting agencies AlphaSights ClearViewHealthcare Partners GLC and Insights Consulting hasserved on a speakers bureau for Teva Pharmaceuticals for talks
unrelated to pharmaceuticals has received research supportfrom Mallinckrodt for investigator-initiated wet bench stud-ies and from Acorda Avanir Biogen Chugai GenentechMedImmune Novartis and Teva Pharmaceuticals for servingas a site investigator in multicenter trials has given experttestimony prepared an affidavit and acted as witness for TevaPharmaceuticals and has acted as an expert on a patent casefor Acorda Wayne State University has received financialcompensation from the NMSS for his salary as principle in-vestigator for a research grant RA Marrie receives researchgrants from nonprofit organizations including CanadianInstitutes of Health Research (CIHR) the CMSC Crohnrsquosand Colitis Canada the NMSS the Multiple Sclerosis Societyof Canada the Multiple Sclerosis Scientific Research Foun-dation and Research Manitoba and serves on the editorialboard of Neurology D Pelletier has served on scientific ad-visory boards for Biogen EMD Serono GenzymeSanofiAventis Hoffman LaRoche and Novartis has received re-search support for Biogen Genzyme Hoffman LaRoche andthe National Institute of Neurologic Disorders and Stroke ofthe NIH and has received honoraria for providing consultingservices at scientific advisory board meetings from BiogenEMD Serono GenzymeSanofi Aventis Hoffman LaRocheand Novartis S Potrebic received an honorarium from CDIQuality Institute PLE for participation in a headacheappropriate-use criteria panel for imaging and receives travelreimbursement from the AAN for attending AAN ResidencyIn-Service Training Examination Work Group meetingsAAN Axon Registry Committee meetings AAN GuidelineDevelopment Dissemination and Implementation Sub-committee meetings and the Guidelines International Net-work North America Evidence-based Guidelines AffectingPolicy Practice and Stakeholders (E-GAPPS) conference RSommers C Sitcov and J Stachowiak report no disclosuresrelevant to the manuscript T Getchius is a former AANemployee and reports no relevant disclosures S Merillatreports no disclosures relevant to the manuscript T Prings-heim has received research support from the CIHR and ShireCanada Inc Go to NeurologyorgN for full disclosures
DisclaimerClinical practice guidelines practice advisories systematicreviews and other guidance published by the AmericanAcademy of Neurology and its affiliates are assessments ofcurrent scientific and clinical information provided as an ed-ucational service The information (1) should not be con-sidered inclusive of all proper treatments methods of care oras a statement of the standard of care (2) is not continuallyupdated and may not reflect the most recent evidence (newevidence may emerge between the time information is de-veloped and when it is published or read) (3) addresses onlythe question(s) specifically identified (4) does not mandateany particular course of medical care and (5) is not intendedto substitute for the independent professional judgment of thetreating provider as the information does not account forindividual variation among people with MS In all cases theselected course of action should be considered by the treating
798 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
provider in the context of treating the individual patientUse of the information is voluntary AAN provides thisinformation on an ldquoas isrdquo basis and makes no warrantyexpressed or implied regarding the information AANspecifically disclaims any warranties of merchantability orfitness for a particular use or purpose AAN assumes noresponsibility for any injury or damage to persons or propertyarising out of or related to any use of this information or forany errors or omissions
Conflict of interest statementThe American Academy of Neurology (AAN) is committedto producing independent critical and truthful clinical prac-tice guidelines (CPGs) Significant efforts are made to mini-mize the potential for conflicts of interest to influence therecommendations of this CPG To the extent possiblethe AAN keeps separate those who have a financial stake inthe success or failure of the products appraised in the CPGsand the developers of the guidelines Conflict of interest formswere obtained from all authors and reviewed by an oversightcommittee prior to project initiation AAN limits the partic-ipation of authors with substantial conflicts of interest TheAAN forbids commercial participation in or funding ofguideline projects Drafts of the guideline have been reviewedby at least 3 AAN committees a network of neurologistsNeurologyreg peer reviewers and representatives from relatedfields The AAN Guideline Author Conflict of Interest Policycan be viewed at aancom For complete information on thisprocess access the 2011 AAN process manual as amended4
Received July 12 2017 Accepted in final form February 15 2018
References1 Rae-Grant A Day GS Marrie RA et al for the Guideline Development Dissemi-
nation and Implementation Subcommittee of the American Academy of NeurologyPractice guideline recommendations summary disease-modifying therapies for adultswith multiple sclerosis report of the Guideline Development Dissemination andImplementation Subcommittee of the American Academy of Neurology Neurology201890777ndash788
2 Goodin DS Frohman EM Garmany GP et al on behalf of the American Academy ofNeurology and the MS Council for Clinical Practice Guidelines Disease-modifyingtherapies in multiple sclerosis subcommittee of the American Academy of Neurologyand the MS Council for Clinical Practice Guidelines report of the Therapeutics andTechnology Assessment Subcommittee of the American Academy of Neurology andthe MS Council for Clinical Practice Guidelines Neurology 200258169ndash178
3 Browne P Chandraratna D Angood C et al Atlas of Multiple Sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
4 American Academy of Neurology Clinical Practice Guideline Process Manual 2011ed [online] St Paul The American Academy of Neurology 2011 Available at aancompolicy-and-guidelinesguidelinesabout-guidelines2 Accessed March 122016
5 Institute of Medicine Eden J Levit L Berg A Morton S editors Committee onStandards for Systematic Reviews of Comparative Effectiveness ResearchWashington DC National Academies Press 2011
6 Institute of Medicine Committee on Standards for Developing Trustworthy ClinicalPractice Guidelines Clinical Practice Guidelines We Can Trust Washington DCNational Academies Press 2011
7 Shea BJ Grimshaw JM Wells GA et al Development of AMSTAR a measurementtool to assess the methodological quality of systematic reviews BMC Med ResMethodol 2007710
8 Guyatt GH Oxman AD Schunemann HJ Tugwell P Knottnerus A GRADEguidelines a new series of articles in the Journal of Clinical Epidemiology J ClinEpidemiol 201164380ndash382
8a Biogen and AbbVie announce the voluntary worldwide withdrawal of marketingauthorizations for ZINBRYTAreg (daclizumab) for relapsing multiple sclerosis [press
release] Available at httpmediabiogencompress-releaseautoimmune-diseasesbiogenC2A0and-abbvie-announceC2A0-voluntaryC2A0worldwide-withdrawal-marketi Issued March 2 2018 Accessed March 5 2018
9 Kappos L Radue EW OrsquoConnor P et al A placebo-controlled trial of oral fingolimodin relapsing multiple sclerosis N Engl J Med 2010362387ndash401
10 Calabresi P Radue EW Goodin D et al Safety and efficacy of fingolimod in patientswith relapsing-remitting multiple sclerosis (FREEDOMS II) a double-blind rando-mised placebo-controlled phase 3 trial Lancet Neurol 201413545ndash556
11 PRISMS (Prevention of Relapses and Disability by Interferon Beta-la Subcutaneouslyin Multiple Sclerosis) Study Group Randomised double-blind placebo-controlledstudy of interferon beta-1a in relapsingremitting multiple sclerosis Lancet 19983521498ndash1504
12 Polman C OrsquoConnor PW Havdrova E et al A randomized placebo-controlled trialof natalizumab for relapsing multiple sclerosis N Engl J Med 2006354899ndash910
13 Hauser SL Bar-Or A Comi G et al for the OPERA I and OPERA II ClinicalInvestigators Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosisN Engl J Med 2017376221ndash234
14 Giovannoni G Comi G Cook S et al on behalf of the CLARITY Study Group Aplacebo-controlled trial of oral cladribine for relapsing multiple sclerosis N Engl JMed 2010362416ndash426
15 Cohen J Coles AJ Arnold DL et al CARE-MS I Investigators Alemtuzumab versusinterferon beta 1a as first-line treatment for patients with relapsing-remitting multiplesclerosis a randomised controlled phase 3 trial Lancet 20123801819ndash1828
16 Cohen J Barkhof F Comi G et al on behalf of the TRANSFORMS Study GroupOral fingolimod or intramuscular interferon for relapsing multiple sclerosis N Engl JMed 2010362402ndash415
17 Panitch H Goodin DS Francis G et al or the University of British Columbia MSMRI Research Group Randomized comparative study of interferon beta-1a treat-ment regimens in MS the EVIDENCE Trial Neurology 2002591496ndash1506
18 Fox R Miller DH Phillips JT et al on behalf of the CONFIRM Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 or glatiramer in multiple sclerosisN Engl J Med 20123671087ndash1097
19 Massacesi L Tramacere I Amoroso S et al Azathioprine versus beta interferons forrelapsing-remitting multiple sclerosis a multicentre randomized non-inferiority trialPLoS One 20149e113371
20 Gold R Giovannoni G Selmaj K et al on behalf of the SELECT Study Inves-tigators Daclizumab high-yield process in relapsing-remitting multiple sclerosis(SELECT) a randomised double-blind placebo-controlled trial Lancet 20133812167ndash2175
21 Gold R Kappos L Arnold DL et al on behalf of the DEFINE Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 for relapsing multiple sclerosisN Engl J Med 20123671098ndash1107
22 Vollmer T Sorensen PS Selmaj K et al on behalf of the BRAVO Study Group Arandomized placebo-controlled phase III trial of oral laquinimod for multiple scle-rosis J Neurol 2014261773ndash783
23 Millefiorini E Gasperini C Pozzilli C et al Randomized placebo-controlled trial ofmitoxantrone in relapsing-remitting multiple sclerosis 24-month clinical and MRIoutcome J Neurol 1997244153ndash159
24 Calabresi P Kieseier BC Arnold DL et al for the ADVANCE Study InvestigatorsPegylated interferon beta-1a for relapsing-remitting multiple sclerosis (ADVANCE)a randomised phase 3 double-blind study Lancet Neurol 201413657ndash665
25 Hauser SL Waubant E Arnold DL et al for the HERMES Trial Group B-celldepletion with rituximab in relapsing-remitting multiple sclerosis N Engl J Med 2008358676ndash688
26 OrsquoConnor P Wolinsky JS Confavreux C et al for the TEMSO Trial Group Ran-domized trial of oral teriflunomide for relapsing multiple sclerosis N Engl J Med20113651293ndash1303
27 Kappos L Wiendl H Selmaj K et al Daclizumab HYP versus interferon beta-1a inrelapsing multiple sclerosis N Engl J Med 20153731418ndash1428
28 Frohman EM Cutter G Remington G et al A randomized blinded parallel-grouppilot trial of mycophenolate mofetil (CellCept) compared with interferon beta-1a(Avonex) in patients with relapsing-remitting multiple sclerosis Ther Adv NeurolDisord 2010315ndash28
29 Coles A TwymanCL Arnold DL et al the CARE-MS II Investigators Alemtuzumab forpatients with relapsing multiple sclerosis after disease-modifying therapy a randomisedcontrolled phase 3 trial Lancet 2012801829ndash1839
30 Zivadinov R Rudick RA De Masi R et al Effects of IV methylprednisolone on brainatrophy in relapsing-remitting MS Neurology 2001571239ndash1247
31 Remington GM Treadaway K Frohman T et al A one-year prospective ran-domized placebo-controlled quadruple-blinded phase II safety pilot trial ofcombination therapy with interferon beta-1a and mycophenolate mofetil in earlyrelapsing-remitting multiple sclerosis (TIME MS) Ther Adv Neurol Disord 201033ndash13
32 Jacobs L Cookfair DL Rudick RA et al Intramuscular interferon beta-1a for diseaseprogression in relapsing multiple sclerosis Ann Neurol 199639285ndash294
33 Confavreux C OrsquoConnor P Comi G et al for the TOWER Trial Group Oralteriflunomide for patients with relapsing multiple sclerosis (TOWER) a randomiseddouble-blind placebo-controlled phase 3 trial Lancet Neurol 201413247ndash256
34 Johnson KP Brooks BR Cohen JA et al Copolymer 1 reduces relapse rate andimproves disability in relapsing-remitting multiple sclerosis results of a phase IIImulticenter double-blind placebo-controlled trial Copolymer 1 Multiple SclerosisStudy Group Neurology 1995451268ndash1276
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 799
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
35 Bornstein MB Miller A Slagle S et al A pilot trial of COP 1 in exacerbating-remittingmultiple sclerosis N Engl J Med 1987317408ndash414
36 Ravnborg M Sorensen PS Andersson M et al Methylprednisolone in combinationwith interferon beta-1a for relapsing-remitting multiple sclerosis (MECOMBINstudy) a multicentre double-blind randomized placebo-controlled parallel-groupstudy Lancet Neurol 20109672ndash680
37 Lublin FD Cofield SS Cutter GR et al on behalf of the CombiRx InvestigatorsRandomized study combining interferon and glatiramer acetate in multiple sclerosisAnn Neurol 201373327ndash340
38 Ellison G Myers LW Mickey MR et al A placebo-controlled randomized double-masked variable dosage clinical trial of azathioprine with and without methylpred-nisolone in multiple sclerosis Neurology 1989391018ndash1026
39 Fazekas F Deisenhammer F Stasser-Fuchs S Nahler G Mamoli B Randomisedplacebo-controlled trial of monthly intravenous immunoglobulin therapy in relapsing-remitting multiple sclerosis Austrian Immunoglobulin in Multiple Sclerosis StudyGroup Lancet 1997349598ndash593
40 Achiron A Gabbay U Gilad R et al Intravenous immunoglobulin treatment inmultiple sclerosis effect on relapses Neurology 199850398ndash402
Neurologyreg Online CME Program
Earn CME while reading Neurology This program is available only to online Neurology subscribers Read the articles markedCME go to Neurologyorg and click on CME This will provide all of the information necessary to get started TheAmerican Academy of Neurology (AAN) is accredited by the Accreditation Council for Continuing Medical Education(ACCME) to sponsor continuing medical education for physicians Neurology is planned and produced in accordance withthe ACCME Essentials For more information contact AAN Member Services at 800-879-1960
NeurologyorgN Offers Important Information to Patients and Their Families
The Neurologyreg Patient Page providesbull A critical review of ground-breaking discoveries in neurologic research that are written especially for patients and their familiesbull Up-to-date patient information about many neurologic diseasesbull Links to additional information resources for neurologic patients
All Neurology Patient Page articles can be easily downloaded and printed and may be reproduced to distribute for educational purposesClick on the lsquoPatientsrsquo link on the home page (NeurologyorgN) for a complete index of Patient Pages
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Audio summaries of current issues Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
800 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000005345201890789-800 Neurology
Alexander Rae-Grant Gregory S Day Ruth Ann Marrie et al Implementation Subcommittee of the American Academy of Neurology
with multiple sclerosis Report of the Guideline Development Dissemination and Comprehensive systematic review summary Disease-modifying therapies for adults
This information is current as of April 23 2018
ServicesUpdated Information amp
httpnneurologyorgcontent9017789fullincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl201804239017789DC1
Supplementary material can be found at
References httpnneurologyorgcontent9017789fullref-list-1
This article cites 37 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9017789fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2018 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

Daclizumab is probably more effective than IFN-β-1a 30 μgIM27 in reducing the risk of disability progression in people withRRMS (moderate confidence) See safety note on page 7918a
Pulsed corticosteroids30 are possibly more effective thanplacebo in reducing the risk of disability progression in peoplewith RRMS (low confidence)
The following DMTs are possibly no more effective thanplacebo in reducing the risk of disability progression in peoplewith RRMS (low confidence) glatiramer acetate183435 andpulsed corticosteroids added to IFN-β-1a IM once weekly36
Fingolimod is possibly no more effective than IFN-β-1a IMweekly in reducing the risk of disability progression over1 year (low confidence)16 See safety note on page 7918a
IFN-β-1a is possibly no more effective than glatiramer acetatein reducing the risk of disability progression over 3 years (lowconfidence)37
There is insufficient evidence to determine the efficacy of thefollowing DMTs compared with placebo in reducing the riskof disability progression in people with RRMS (very lowconfidence) azathioprine38 immunoglobulins3940 IFN-β-1bsubcutaneous alternate daye1 and methotrexatee2
IFN-β-1b alternate day is probably less effective than glatir-amer acetate in reducing the risk of disability progression over2 years (moderate confidence)e1
4 In peoplewith RRMSwho experience diseaseactivity while on a DMT is changing toa different DMT superior to continuing thepresent DMT in terms of relapse rate and MRI-detected T2 or gadolinium-enhancedlesion activityFor individuals with RRMS who experienced a relapse onIFN-β or glatiramer acetate alemtuzumab is more effectivethan IFN-β-1a 44 μg subcutaneous 3 times per week in re-ducing the ARR the relapse risk disability progression andrisk of new or enlarging T2 lesions over 2 years (highconfidence)15
In individuals with RRMS who experience 1 or more relapsesin the preceding 12 months on IFN-β adding natalizumab ismore effective than adding placebo in decreasing the risk ofrelapse over 2 years the ARR the risk of disability progressionover 2 years and the risk of new or enlarging T2 lesions at1 year (high confidence)e3
In individuals with RRMS who experienced one ormore relapses in the preceding 12 months on glatiramer ac-etate there is insufficient evidence to determine the efficacy ofnatalizumab added to glatiramer acetate compared with pla-cebo added to glatiramer acetate in decreasing the risk ofrelapse at 6 months (very low confidence)e4
Natalizumab added to glatiramer acetate is probably moreeffective than placebo added to glatiramer acetate in
Figure 3 Outcome Relative risk (RR) of in-study disability progression at 2 years relapsing-remitting multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aOutcome measured at 1 year bVersus interferon-β-1a cOutcomemeasured at 3 years dSee safety note on page 7918a
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 795
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
decreasing the cumulative number of new or enlarging T2lesions at 6 months (moderate confidence)e4
Note that natalizumab is not presently approvedrecommended as an add-on therapy to other DMTs owingto potential safety concerns associated with combined use ofthis medication
5 In people with progressive MS are DMTssuperior to placeboor otherDMTsasmeasuredby relapse rate or in-studydisease progression
Risk of relapseFigure 4 presents these data regarding risk of relapse IFN-β-1b subcutaneous alternate day (SPMS) is more effectivethan placebo in reducing the risk of relapse in people withprogressive MS (high confidence)e5e6
The following DMTs are probably more effective than placeboin reducing the risk of relapse in people with progressive MS(moderate confidence) IFN-β-1a 60 μg IM weekly (SPMS)e7
and mitoxantrone (worsening RRMS and SPMS)e8
There is insufficient evidence to determine the efficacy of thefollowing DMTs compared with placebo in reducing the riskof relapse in people with progressive MS (very low confi-dence) azathioprine38 immunoglobulinse9e10 and metho-trexate (chronic progressive MS older terminology that isundefined but included present PPMS and SPMS diseasetypes)e11 There is insufficient evidence to determine theefficacy of high-dose corticosteroids compared with low-dosecorticosteroidse12 in reducing the risk of relapse in peoplewith SPMS (very low confidence)
Disability progressionThe following DMTs are probably more effective than pla-cebo in reducing the risk of in-study disability progression inpeople with progressive MS (RRMS or SPMS moderateconfidence) mitoxantrone (worsening RRMS and SPMS)e13
and ocrelizumab (PPMS)e14
The following DMTs are possibly no more effective thanplacebo in reducing the risk of in-study disability progressionin people with progressive MS (low confidence) cladribine(SPMS)e15 fingolimod (PPMS)e16 glatiramer acetate(progressive forms of MSe17 and PPMSe18) IFN-β-1a 30 μgIM weekly (SPMSe7 and PPMSe19) IFN-β-1a subcutaneous 3times per week (SPMS)e20 IFN-β-1b subcutaneous alternateday (SPMSe5e6 and PPMSe21) and rituximab (PPMS)e22
There is insufficient evidence to determine the efficacy of thefollowing DMTs relative to placebo in reducing the risk of in-study disability progression in people with progressive MS(very low confidence) azathioprine38 corticosteroids addedto mitoxantronee23 cyclophosphamidee24e25 immunoglobu-linse9e10 and methotrexate (CPMS [PPMS])e11
There is insufficient evidence to determine the efficacy ofhigh-dose corticosteroids relative to low-dose cortico-steroidse26 in reducing the risk of in-study disability pro-gression in people with progressive MS (very lowconfidence)
6 What are the AEs of DMTs in people with MScompared with placebo (AE-relateddiscontinuation and serious or life-threatening AEs)A comprehensive review of adverse effects associated withDMTs is included in the full-text document (data supplementto the companion recommendations article linkslwwcomWNLA429) and table
7 In people with CIS are DMTs superior toplacebo in decreasing the risk of conversionto MSFigure 5 presents the data regarding risk of conversion to MSin people with CIS For individuals with CIS the followingDMTs are more effective than placebo in reducing the pro-portion of individuals converting to MS (high confidence)glatiramer acetatee27 and IFN-β-1a subcutaneous 3 timesweeklye28
Figure 4 Outcome Relative risk (RR) of relapse at 2 years secondary progressive multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aHigh-dose corticosteroids vs low-dose corticosteroids bOutcomemeasured at 3 years
796 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
For individuals with CIS the following DMTs are probablymore effective than placebo in reducing the proportion ofindividuals converting to MS (moderate confidence)cladribinee29 immunoglobulinse30 IFN-β-1a 30 μg IMweeklye31 IFN-β-1b subcutaneous alternate daye32 andteriflunomidee33
DiscussionMultiple DMTs are now approved for use in CIS or MSallowing people with MS and clinicians to consider DMTmechanism of action efficacy and AE profile in the decision-making process This systematic review was used to developa practice guideline for the use of DMT for MS acknowl-edging the limits of current evidence Measures of efficacysuch as long-term disability patient satisfaction quality of lifeand effects on MS symptoms may be important to thedecision-making process but ultimately remain inadequatelystudied Similarly there is a dearth of high-quality evidencepertaining to the comparative efficacy of specific DMTs orvarious treatment strategies (eg high-efficacy treatment vsstepped-care treatment protocols) Future studies addressingthese and other questions are needed to further informtreatment recommendations particularly those pertaining towhen to switch or stop DMTs
Author contributionsDr Rae-Grant study concept and design acquisition of dataanalysis or interpretation of data draftingrevising the man-uscript critical revision of the manuscript for important in-tellectual content study supervision Dr Day study conceptand design analysis or interpretation of data draftingrevisingthe manuscript critical revision of the manuscript for im-portant intellectual content Dr Marrie study concept anddesign acquisition of data analysis or interpretation of datadraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Rabinsteinanalysis or interpretation of data draftingrevising the man-uscript Dr Cree study concept and design draftingrevising
the manuscript critical revision of the manuscript forimportant intellectual content Dr Gronseth analysis orinterpretation of data critical revision of the manuscript forimportant intellectual content study supervisionDr Haboubi study concept and design analysis or in-terpretation of data draftingrevising the manuscriptJ Halper study concept and design draftingrevising themanuscript critical revision of the manuscript for importantintellectual content Dr Hosey critical revision of the man-uscript for important intellectual content Dr Jones studyconcept and design draftingrevising the manuscript criticalrevision of the manuscript for important intellectual contentDr Lisak study concept and design draftingrevising themanuscript critical revision of the manuscript for importantintellectual content Dr Pelletier study concept and designdraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Potrebicstudy concept and design acquisition of data analysis or in-terpretation of data draftingrevising the manuscript criticalrevision of the manuscript for important intellectual contentstudy supervision C Sitcov study concept and designdraftingrevising the manuscript critical revision of themanuscript for important intellectual content R Sommersdraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Stacho-wiak study concept and design draftingrevising the manu-script critical revision of the manuscript for importantintellectual content TSD Getchius study supervisionSA Merillat draftingrevising the manuscript study super-vision Dr Pringsheim study concept and design acquisitionof data analysis or interpretation of data draftingrevising themanuscript critical revision of the manuscript for importantintellectual content study supervision
AcknowledgmentThe authors thank the North American Research CommitteeonMultiple Sclerosis (NARCOMS) Registry for its assistancein administering an outcomes survey the results of whichwere included in this practice guideline NARCOMS issupported in part by the Consortium of Multiple SclerosisCenters (CMSC) and the Foundation of the CMSC
Figure 5 Outcome Relative risk (RR) of conversion to multiple sclerosis over 2 years
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aOutcome measured at 1 year bOutcome measured at 3 years
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 797
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study fundingThis practice guideline was developed with financial supportfrom the American Academy of Neurology (AAN) Authorswho serve as AAN subcommittee members or as method-ologists (AR-G GSD AR GSG MH SP TP) orwho are or were AAN staffmembers (TSDG SAM) werereimbursed by the AAN for expenses related to travel tosubcommittee meetings where drafts of manuscripts werereviewed All authors on the panel were reimbursed by theAAN for expenses related to travel to 2 in-person meetings
DisclosureA Rae-Grant receives royalties from 2 textbooks he haspublished 1 on neurology and 1 on multiple sclerosis (MS)organizes and receives honoraria for grand rounds and neu-rology review courses and is local primary investigator fora clinical trial with MedDay Pharmaceuticals for which hereceives no personal compensation A Rabinstein reports nodisclosures relevant to the manuscript B Cree has receivedcompensation for consulting from AbbVie Biogen EMDSerono GeNeuro GenzymeSanofi Aventis Novartis andShire has given expert testimony and prepared an affidavit formedical malpractice cases (1 or 2 per year) within his area ofexpertise and has acted as consultant in a legal proceeding forAcorda and Biogen G Gronseth serves as associate editor(level of evidence review) for Neurologyreg serves on the edi-torial advisory board for Neurology Now and is compensatedby the American Academy of Neurology (AAN) for meth-odologic activities G Day holds stock in ANI PharmaceuticalsM Haboubi has received travel reimbursement and honorariafor grand rounds presentations in Madisonville KY J Halperand J Hosey report no disclosures relevant to the manuscriptD Jones has received personal compensation for consultingfrom Biogen and Genzyme has received honoraria fromthe Consortium of Multiple Sclerosis Centers (CMSC) theMultiple Sclerosis Association of America (MSAA) and thePharmacy Quality Alliance has received institutional researchsupport from Biogen and the National MS Society (NMSS)has received salary support from the CMSC and has receivedtravel reimbursement from Biogen and Genzyme and fromthe AAN Can Do MS the CMSC and the MSAA R Lisakserved as the President of the CMSC and serves as a memberof the Board of the DMC Foundation has served on scientificadvisory boards for Mallinckrodt Syntimmune Celegeneand Alexion serves as chair of the adjudication committee ofa clinical trial (PAREXEL) has received funding for travelfrom the CMSC the GBSCIDP Foundation Internationalthe NMSS and Syntimmune for travel to consultants meet-ings has served as a journal editor for Clinical and Experi-mental Neuroimmunology andClinical Neuropharmacology hasreceived publishing royalties from Willey for InternationalNeurology A Clinical Approach has received honoraria fromMallinckrodt Syntimmune and Teva Pharmaceuticals andfrom the consulting agencies AlphaSights ClearViewHealthcare Partners GLC and Insights Consulting hasserved on a speakers bureau for Teva Pharmaceuticals for talks
unrelated to pharmaceuticals has received research supportfrom Mallinckrodt for investigator-initiated wet bench stud-ies and from Acorda Avanir Biogen Chugai GenentechMedImmune Novartis and Teva Pharmaceuticals for servingas a site investigator in multicenter trials has given experttestimony prepared an affidavit and acted as witness for TevaPharmaceuticals and has acted as an expert on a patent casefor Acorda Wayne State University has received financialcompensation from the NMSS for his salary as principle in-vestigator for a research grant RA Marrie receives researchgrants from nonprofit organizations including CanadianInstitutes of Health Research (CIHR) the CMSC Crohnrsquosand Colitis Canada the NMSS the Multiple Sclerosis Societyof Canada the Multiple Sclerosis Scientific Research Foun-dation and Research Manitoba and serves on the editorialboard of Neurology D Pelletier has served on scientific ad-visory boards for Biogen EMD Serono GenzymeSanofiAventis Hoffman LaRoche and Novartis has received re-search support for Biogen Genzyme Hoffman LaRoche andthe National Institute of Neurologic Disorders and Stroke ofthe NIH and has received honoraria for providing consultingservices at scientific advisory board meetings from BiogenEMD Serono GenzymeSanofi Aventis Hoffman LaRocheand Novartis S Potrebic received an honorarium from CDIQuality Institute PLE for participation in a headacheappropriate-use criteria panel for imaging and receives travelreimbursement from the AAN for attending AAN ResidencyIn-Service Training Examination Work Group meetingsAAN Axon Registry Committee meetings AAN GuidelineDevelopment Dissemination and Implementation Sub-committee meetings and the Guidelines International Net-work North America Evidence-based Guidelines AffectingPolicy Practice and Stakeholders (E-GAPPS) conference RSommers C Sitcov and J Stachowiak report no disclosuresrelevant to the manuscript T Getchius is a former AANemployee and reports no relevant disclosures S Merillatreports no disclosures relevant to the manuscript T Prings-heim has received research support from the CIHR and ShireCanada Inc Go to NeurologyorgN for full disclosures
DisclaimerClinical practice guidelines practice advisories systematicreviews and other guidance published by the AmericanAcademy of Neurology and its affiliates are assessments ofcurrent scientific and clinical information provided as an ed-ucational service The information (1) should not be con-sidered inclusive of all proper treatments methods of care oras a statement of the standard of care (2) is not continuallyupdated and may not reflect the most recent evidence (newevidence may emerge between the time information is de-veloped and when it is published or read) (3) addresses onlythe question(s) specifically identified (4) does not mandateany particular course of medical care and (5) is not intendedto substitute for the independent professional judgment of thetreating provider as the information does not account forindividual variation among people with MS In all cases theselected course of action should be considered by the treating
798 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
provider in the context of treating the individual patientUse of the information is voluntary AAN provides thisinformation on an ldquoas isrdquo basis and makes no warrantyexpressed or implied regarding the information AANspecifically disclaims any warranties of merchantability orfitness for a particular use or purpose AAN assumes noresponsibility for any injury or damage to persons or propertyarising out of or related to any use of this information or forany errors or omissions
Conflict of interest statementThe American Academy of Neurology (AAN) is committedto producing independent critical and truthful clinical prac-tice guidelines (CPGs) Significant efforts are made to mini-mize the potential for conflicts of interest to influence therecommendations of this CPG To the extent possiblethe AAN keeps separate those who have a financial stake inthe success or failure of the products appraised in the CPGsand the developers of the guidelines Conflict of interest formswere obtained from all authors and reviewed by an oversightcommittee prior to project initiation AAN limits the partic-ipation of authors with substantial conflicts of interest TheAAN forbids commercial participation in or funding ofguideline projects Drafts of the guideline have been reviewedby at least 3 AAN committees a network of neurologistsNeurologyreg peer reviewers and representatives from relatedfields The AAN Guideline Author Conflict of Interest Policycan be viewed at aancom For complete information on thisprocess access the 2011 AAN process manual as amended4
Received July 12 2017 Accepted in final form February 15 2018
References1 Rae-Grant A Day GS Marrie RA et al for the Guideline Development Dissemi-
nation and Implementation Subcommittee of the American Academy of NeurologyPractice guideline recommendations summary disease-modifying therapies for adultswith multiple sclerosis report of the Guideline Development Dissemination andImplementation Subcommittee of the American Academy of Neurology Neurology201890777ndash788
2 Goodin DS Frohman EM Garmany GP et al on behalf of the American Academy ofNeurology and the MS Council for Clinical Practice Guidelines Disease-modifyingtherapies in multiple sclerosis subcommittee of the American Academy of Neurologyand the MS Council for Clinical Practice Guidelines report of the Therapeutics andTechnology Assessment Subcommittee of the American Academy of Neurology andthe MS Council for Clinical Practice Guidelines Neurology 200258169ndash178
3 Browne P Chandraratna D Angood C et al Atlas of Multiple Sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
4 American Academy of Neurology Clinical Practice Guideline Process Manual 2011ed [online] St Paul The American Academy of Neurology 2011 Available at aancompolicy-and-guidelinesguidelinesabout-guidelines2 Accessed March 122016
5 Institute of Medicine Eden J Levit L Berg A Morton S editors Committee onStandards for Systematic Reviews of Comparative Effectiveness ResearchWashington DC National Academies Press 2011
6 Institute of Medicine Committee on Standards for Developing Trustworthy ClinicalPractice Guidelines Clinical Practice Guidelines We Can Trust Washington DCNational Academies Press 2011
7 Shea BJ Grimshaw JM Wells GA et al Development of AMSTAR a measurementtool to assess the methodological quality of systematic reviews BMC Med ResMethodol 2007710
8 Guyatt GH Oxman AD Schunemann HJ Tugwell P Knottnerus A GRADEguidelines a new series of articles in the Journal of Clinical Epidemiology J ClinEpidemiol 201164380ndash382
8a Biogen and AbbVie announce the voluntary worldwide withdrawal of marketingauthorizations for ZINBRYTAreg (daclizumab) for relapsing multiple sclerosis [press
release] Available at httpmediabiogencompress-releaseautoimmune-diseasesbiogenC2A0and-abbvie-announceC2A0-voluntaryC2A0worldwide-withdrawal-marketi Issued March 2 2018 Accessed March 5 2018
9 Kappos L Radue EW OrsquoConnor P et al A placebo-controlled trial of oral fingolimodin relapsing multiple sclerosis N Engl J Med 2010362387ndash401
10 Calabresi P Radue EW Goodin D et al Safety and efficacy of fingolimod in patientswith relapsing-remitting multiple sclerosis (FREEDOMS II) a double-blind rando-mised placebo-controlled phase 3 trial Lancet Neurol 201413545ndash556
11 PRISMS (Prevention of Relapses and Disability by Interferon Beta-la Subcutaneouslyin Multiple Sclerosis) Study Group Randomised double-blind placebo-controlledstudy of interferon beta-1a in relapsingremitting multiple sclerosis Lancet 19983521498ndash1504
12 Polman C OrsquoConnor PW Havdrova E et al A randomized placebo-controlled trialof natalizumab for relapsing multiple sclerosis N Engl J Med 2006354899ndash910
13 Hauser SL Bar-Or A Comi G et al for the OPERA I and OPERA II ClinicalInvestigators Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosisN Engl J Med 2017376221ndash234
14 Giovannoni G Comi G Cook S et al on behalf of the CLARITY Study Group Aplacebo-controlled trial of oral cladribine for relapsing multiple sclerosis N Engl JMed 2010362416ndash426
15 Cohen J Coles AJ Arnold DL et al CARE-MS I Investigators Alemtuzumab versusinterferon beta 1a as first-line treatment for patients with relapsing-remitting multiplesclerosis a randomised controlled phase 3 trial Lancet 20123801819ndash1828
16 Cohen J Barkhof F Comi G et al on behalf of the TRANSFORMS Study GroupOral fingolimod or intramuscular interferon for relapsing multiple sclerosis N Engl JMed 2010362402ndash415
17 Panitch H Goodin DS Francis G et al or the University of British Columbia MSMRI Research Group Randomized comparative study of interferon beta-1a treat-ment regimens in MS the EVIDENCE Trial Neurology 2002591496ndash1506
18 Fox R Miller DH Phillips JT et al on behalf of the CONFIRM Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 or glatiramer in multiple sclerosisN Engl J Med 20123671087ndash1097
19 Massacesi L Tramacere I Amoroso S et al Azathioprine versus beta interferons forrelapsing-remitting multiple sclerosis a multicentre randomized non-inferiority trialPLoS One 20149e113371
20 Gold R Giovannoni G Selmaj K et al on behalf of the SELECT Study Inves-tigators Daclizumab high-yield process in relapsing-remitting multiple sclerosis(SELECT) a randomised double-blind placebo-controlled trial Lancet 20133812167ndash2175
21 Gold R Kappos L Arnold DL et al on behalf of the DEFINE Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 for relapsing multiple sclerosisN Engl J Med 20123671098ndash1107
22 Vollmer T Sorensen PS Selmaj K et al on behalf of the BRAVO Study Group Arandomized placebo-controlled phase III trial of oral laquinimod for multiple scle-rosis J Neurol 2014261773ndash783
23 Millefiorini E Gasperini C Pozzilli C et al Randomized placebo-controlled trial ofmitoxantrone in relapsing-remitting multiple sclerosis 24-month clinical and MRIoutcome J Neurol 1997244153ndash159
24 Calabresi P Kieseier BC Arnold DL et al for the ADVANCE Study InvestigatorsPegylated interferon beta-1a for relapsing-remitting multiple sclerosis (ADVANCE)a randomised phase 3 double-blind study Lancet Neurol 201413657ndash665
25 Hauser SL Waubant E Arnold DL et al for the HERMES Trial Group B-celldepletion with rituximab in relapsing-remitting multiple sclerosis N Engl J Med 2008358676ndash688
26 OrsquoConnor P Wolinsky JS Confavreux C et al for the TEMSO Trial Group Ran-domized trial of oral teriflunomide for relapsing multiple sclerosis N Engl J Med20113651293ndash1303
27 Kappos L Wiendl H Selmaj K et al Daclizumab HYP versus interferon beta-1a inrelapsing multiple sclerosis N Engl J Med 20153731418ndash1428
28 Frohman EM Cutter G Remington G et al A randomized blinded parallel-grouppilot trial of mycophenolate mofetil (CellCept) compared with interferon beta-1a(Avonex) in patients with relapsing-remitting multiple sclerosis Ther Adv NeurolDisord 2010315ndash28
29 Coles A TwymanCL Arnold DL et al the CARE-MS II Investigators Alemtuzumab forpatients with relapsing multiple sclerosis after disease-modifying therapy a randomisedcontrolled phase 3 trial Lancet 2012801829ndash1839
30 Zivadinov R Rudick RA De Masi R et al Effects of IV methylprednisolone on brainatrophy in relapsing-remitting MS Neurology 2001571239ndash1247
31 Remington GM Treadaway K Frohman T et al A one-year prospective ran-domized placebo-controlled quadruple-blinded phase II safety pilot trial ofcombination therapy with interferon beta-1a and mycophenolate mofetil in earlyrelapsing-remitting multiple sclerosis (TIME MS) Ther Adv Neurol Disord 201033ndash13
32 Jacobs L Cookfair DL Rudick RA et al Intramuscular interferon beta-1a for diseaseprogression in relapsing multiple sclerosis Ann Neurol 199639285ndash294
33 Confavreux C OrsquoConnor P Comi G et al for the TOWER Trial Group Oralteriflunomide for patients with relapsing multiple sclerosis (TOWER) a randomiseddouble-blind placebo-controlled phase 3 trial Lancet Neurol 201413247ndash256
34 Johnson KP Brooks BR Cohen JA et al Copolymer 1 reduces relapse rate andimproves disability in relapsing-remitting multiple sclerosis results of a phase IIImulticenter double-blind placebo-controlled trial Copolymer 1 Multiple SclerosisStudy Group Neurology 1995451268ndash1276
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 799
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
35 Bornstein MB Miller A Slagle S et al A pilot trial of COP 1 in exacerbating-remittingmultiple sclerosis N Engl J Med 1987317408ndash414
36 Ravnborg M Sorensen PS Andersson M et al Methylprednisolone in combinationwith interferon beta-1a for relapsing-remitting multiple sclerosis (MECOMBINstudy) a multicentre double-blind randomized placebo-controlled parallel-groupstudy Lancet Neurol 20109672ndash680
37 Lublin FD Cofield SS Cutter GR et al on behalf of the CombiRx InvestigatorsRandomized study combining interferon and glatiramer acetate in multiple sclerosisAnn Neurol 201373327ndash340
38 Ellison G Myers LW Mickey MR et al A placebo-controlled randomized double-masked variable dosage clinical trial of azathioprine with and without methylpred-nisolone in multiple sclerosis Neurology 1989391018ndash1026
39 Fazekas F Deisenhammer F Stasser-Fuchs S Nahler G Mamoli B Randomisedplacebo-controlled trial of monthly intravenous immunoglobulin therapy in relapsing-remitting multiple sclerosis Austrian Immunoglobulin in Multiple Sclerosis StudyGroup Lancet 1997349598ndash593
40 Achiron A Gabbay U Gilad R et al Intravenous immunoglobulin treatment inmultiple sclerosis effect on relapses Neurology 199850398ndash402
Neurologyreg Online CME Program
Earn CME while reading Neurology This program is available only to online Neurology subscribers Read the articles markedCME go to Neurologyorg and click on CME This will provide all of the information necessary to get started TheAmerican Academy of Neurology (AAN) is accredited by the Accreditation Council for Continuing Medical Education(ACCME) to sponsor continuing medical education for physicians Neurology is planned and produced in accordance withthe ACCME Essentials For more information contact AAN Member Services at 800-879-1960
NeurologyorgN Offers Important Information to Patients and Their Families
The Neurologyreg Patient Page providesbull A critical review of ground-breaking discoveries in neurologic research that are written especially for patients and their familiesbull Up-to-date patient information about many neurologic diseasesbull Links to additional information resources for neurologic patients
All Neurology Patient Page articles can be easily downloaded and printed and may be reproduced to distribute for educational purposesClick on the lsquoPatientsrsquo link on the home page (NeurologyorgN) for a complete index of Patient Pages
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Audio summaries of current issues Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
800 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000005345201890789-800 Neurology
Alexander Rae-Grant Gregory S Day Ruth Ann Marrie et al Implementation Subcommittee of the American Academy of Neurology
with multiple sclerosis Report of the Guideline Development Dissemination and Comprehensive systematic review summary Disease-modifying therapies for adults
This information is current as of April 23 2018
ServicesUpdated Information amp
httpnneurologyorgcontent9017789fullincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl201804239017789DC1
Supplementary material can be found at
References httpnneurologyorgcontent9017789fullref-list-1
This article cites 37 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9017789fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2018 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

decreasing the cumulative number of new or enlarging T2lesions at 6 months (moderate confidence)e4
Note that natalizumab is not presently approvedrecommended as an add-on therapy to other DMTs owingto potential safety concerns associated with combined use ofthis medication
5 In people with progressive MS are DMTssuperior to placeboor otherDMTsasmeasuredby relapse rate or in-studydisease progression
Risk of relapseFigure 4 presents these data regarding risk of relapse IFN-β-1b subcutaneous alternate day (SPMS) is more effectivethan placebo in reducing the risk of relapse in people withprogressive MS (high confidence)e5e6
The following DMTs are probably more effective than placeboin reducing the risk of relapse in people with progressive MS(moderate confidence) IFN-β-1a 60 μg IM weekly (SPMS)e7
and mitoxantrone (worsening RRMS and SPMS)e8
There is insufficient evidence to determine the efficacy of thefollowing DMTs compared with placebo in reducing the riskof relapse in people with progressive MS (very low confi-dence) azathioprine38 immunoglobulinse9e10 and metho-trexate (chronic progressive MS older terminology that isundefined but included present PPMS and SPMS diseasetypes)e11 There is insufficient evidence to determine theefficacy of high-dose corticosteroids compared with low-dosecorticosteroidse12 in reducing the risk of relapse in peoplewith SPMS (very low confidence)
Disability progressionThe following DMTs are probably more effective than pla-cebo in reducing the risk of in-study disability progression inpeople with progressive MS (RRMS or SPMS moderateconfidence) mitoxantrone (worsening RRMS and SPMS)e13
and ocrelizumab (PPMS)e14
The following DMTs are possibly no more effective thanplacebo in reducing the risk of in-study disability progressionin people with progressive MS (low confidence) cladribine(SPMS)e15 fingolimod (PPMS)e16 glatiramer acetate(progressive forms of MSe17 and PPMSe18) IFN-β-1a 30 μgIM weekly (SPMSe7 and PPMSe19) IFN-β-1a subcutaneous 3times per week (SPMS)e20 IFN-β-1b subcutaneous alternateday (SPMSe5e6 and PPMSe21) and rituximab (PPMS)e22
There is insufficient evidence to determine the efficacy of thefollowing DMTs relative to placebo in reducing the risk of in-study disability progression in people with progressive MS(very low confidence) azathioprine38 corticosteroids addedto mitoxantronee23 cyclophosphamidee24e25 immunoglobu-linse9e10 and methotrexate (CPMS [PPMS])e11
There is insufficient evidence to determine the efficacy ofhigh-dose corticosteroids relative to low-dose cortico-steroidse26 in reducing the risk of in-study disability pro-gression in people with progressive MS (very lowconfidence)
6 What are the AEs of DMTs in people with MScompared with placebo (AE-relateddiscontinuation and serious or life-threatening AEs)A comprehensive review of adverse effects associated withDMTs is included in the full-text document (data supplementto the companion recommendations article linkslwwcomWNLA429) and table
7 In people with CIS are DMTs superior toplacebo in decreasing the risk of conversionto MSFigure 5 presents the data regarding risk of conversion to MSin people with CIS For individuals with CIS the followingDMTs are more effective than placebo in reducing the pro-portion of individuals converting to MS (high confidence)glatiramer acetatee27 and IFN-β-1a subcutaneous 3 timesweeklye28
Figure 4 Outcome Relative risk (RR) of relapse at 2 years secondary progressive multiple sclerosis
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aHigh-dose corticosteroids vs low-dose corticosteroids bOutcomemeasured at 3 years
796 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
For individuals with CIS the following DMTs are probablymore effective than placebo in reducing the proportion ofindividuals converting to MS (moderate confidence)cladribinee29 immunoglobulinse30 IFN-β-1a 30 μg IMweeklye31 IFN-β-1b subcutaneous alternate daye32 andteriflunomidee33
DiscussionMultiple DMTs are now approved for use in CIS or MSallowing people with MS and clinicians to consider DMTmechanism of action efficacy and AE profile in the decision-making process This systematic review was used to developa practice guideline for the use of DMT for MS acknowl-edging the limits of current evidence Measures of efficacysuch as long-term disability patient satisfaction quality of lifeand effects on MS symptoms may be important to thedecision-making process but ultimately remain inadequatelystudied Similarly there is a dearth of high-quality evidencepertaining to the comparative efficacy of specific DMTs orvarious treatment strategies (eg high-efficacy treatment vsstepped-care treatment protocols) Future studies addressingthese and other questions are needed to further informtreatment recommendations particularly those pertaining towhen to switch or stop DMTs
Author contributionsDr Rae-Grant study concept and design acquisition of dataanalysis or interpretation of data draftingrevising the man-uscript critical revision of the manuscript for important in-tellectual content study supervision Dr Day study conceptand design analysis or interpretation of data draftingrevisingthe manuscript critical revision of the manuscript for im-portant intellectual content Dr Marrie study concept anddesign acquisition of data analysis or interpretation of datadraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Rabinsteinanalysis or interpretation of data draftingrevising the man-uscript Dr Cree study concept and design draftingrevising
the manuscript critical revision of the manuscript forimportant intellectual content Dr Gronseth analysis orinterpretation of data critical revision of the manuscript forimportant intellectual content study supervisionDr Haboubi study concept and design analysis or in-terpretation of data draftingrevising the manuscriptJ Halper study concept and design draftingrevising themanuscript critical revision of the manuscript for importantintellectual content Dr Hosey critical revision of the man-uscript for important intellectual content Dr Jones studyconcept and design draftingrevising the manuscript criticalrevision of the manuscript for important intellectual contentDr Lisak study concept and design draftingrevising themanuscript critical revision of the manuscript for importantintellectual content Dr Pelletier study concept and designdraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Potrebicstudy concept and design acquisition of data analysis or in-terpretation of data draftingrevising the manuscript criticalrevision of the manuscript for important intellectual contentstudy supervision C Sitcov study concept and designdraftingrevising the manuscript critical revision of themanuscript for important intellectual content R Sommersdraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Stacho-wiak study concept and design draftingrevising the manu-script critical revision of the manuscript for importantintellectual content TSD Getchius study supervisionSA Merillat draftingrevising the manuscript study super-vision Dr Pringsheim study concept and design acquisitionof data analysis or interpretation of data draftingrevising themanuscript critical revision of the manuscript for importantintellectual content study supervision
AcknowledgmentThe authors thank the North American Research CommitteeonMultiple Sclerosis (NARCOMS) Registry for its assistancein administering an outcomes survey the results of whichwere included in this practice guideline NARCOMS issupported in part by the Consortium of Multiple SclerosisCenters (CMSC) and the Foundation of the CMSC
Figure 5 Outcome Relative risk (RR) of conversion to multiple sclerosis over 2 years
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aOutcome measured at 1 year bOutcome measured at 3 years
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 797
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study fundingThis practice guideline was developed with financial supportfrom the American Academy of Neurology (AAN) Authorswho serve as AAN subcommittee members or as method-ologists (AR-G GSD AR GSG MH SP TP) orwho are or were AAN staffmembers (TSDG SAM) werereimbursed by the AAN for expenses related to travel tosubcommittee meetings where drafts of manuscripts werereviewed All authors on the panel were reimbursed by theAAN for expenses related to travel to 2 in-person meetings
DisclosureA Rae-Grant receives royalties from 2 textbooks he haspublished 1 on neurology and 1 on multiple sclerosis (MS)organizes and receives honoraria for grand rounds and neu-rology review courses and is local primary investigator fora clinical trial with MedDay Pharmaceuticals for which hereceives no personal compensation A Rabinstein reports nodisclosures relevant to the manuscript B Cree has receivedcompensation for consulting from AbbVie Biogen EMDSerono GeNeuro GenzymeSanofi Aventis Novartis andShire has given expert testimony and prepared an affidavit formedical malpractice cases (1 or 2 per year) within his area ofexpertise and has acted as consultant in a legal proceeding forAcorda and Biogen G Gronseth serves as associate editor(level of evidence review) for Neurologyreg serves on the edi-torial advisory board for Neurology Now and is compensatedby the American Academy of Neurology (AAN) for meth-odologic activities G Day holds stock in ANI PharmaceuticalsM Haboubi has received travel reimbursement and honorariafor grand rounds presentations in Madisonville KY J Halperand J Hosey report no disclosures relevant to the manuscriptD Jones has received personal compensation for consultingfrom Biogen and Genzyme has received honoraria fromthe Consortium of Multiple Sclerosis Centers (CMSC) theMultiple Sclerosis Association of America (MSAA) and thePharmacy Quality Alliance has received institutional researchsupport from Biogen and the National MS Society (NMSS)has received salary support from the CMSC and has receivedtravel reimbursement from Biogen and Genzyme and fromthe AAN Can Do MS the CMSC and the MSAA R Lisakserved as the President of the CMSC and serves as a memberof the Board of the DMC Foundation has served on scientificadvisory boards for Mallinckrodt Syntimmune Celegeneand Alexion serves as chair of the adjudication committee ofa clinical trial (PAREXEL) has received funding for travelfrom the CMSC the GBSCIDP Foundation Internationalthe NMSS and Syntimmune for travel to consultants meet-ings has served as a journal editor for Clinical and Experi-mental Neuroimmunology andClinical Neuropharmacology hasreceived publishing royalties from Willey for InternationalNeurology A Clinical Approach has received honoraria fromMallinckrodt Syntimmune and Teva Pharmaceuticals andfrom the consulting agencies AlphaSights ClearViewHealthcare Partners GLC and Insights Consulting hasserved on a speakers bureau for Teva Pharmaceuticals for talks
unrelated to pharmaceuticals has received research supportfrom Mallinckrodt for investigator-initiated wet bench stud-ies and from Acorda Avanir Biogen Chugai GenentechMedImmune Novartis and Teva Pharmaceuticals for servingas a site investigator in multicenter trials has given experttestimony prepared an affidavit and acted as witness for TevaPharmaceuticals and has acted as an expert on a patent casefor Acorda Wayne State University has received financialcompensation from the NMSS for his salary as principle in-vestigator for a research grant RA Marrie receives researchgrants from nonprofit organizations including CanadianInstitutes of Health Research (CIHR) the CMSC Crohnrsquosand Colitis Canada the NMSS the Multiple Sclerosis Societyof Canada the Multiple Sclerosis Scientific Research Foun-dation and Research Manitoba and serves on the editorialboard of Neurology D Pelletier has served on scientific ad-visory boards for Biogen EMD Serono GenzymeSanofiAventis Hoffman LaRoche and Novartis has received re-search support for Biogen Genzyme Hoffman LaRoche andthe National Institute of Neurologic Disorders and Stroke ofthe NIH and has received honoraria for providing consultingservices at scientific advisory board meetings from BiogenEMD Serono GenzymeSanofi Aventis Hoffman LaRocheand Novartis S Potrebic received an honorarium from CDIQuality Institute PLE for participation in a headacheappropriate-use criteria panel for imaging and receives travelreimbursement from the AAN for attending AAN ResidencyIn-Service Training Examination Work Group meetingsAAN Axon Registry Committee meetings AAN GuidelineDevelopment Dissemination and Implementation Sub-committee meetings and the Guidelines International Net-work North America Evidence-based Guidelines AffectingPolicy Practice and Stakeholders (E-GAPPS) conference RSommers C Sitcov and J Stachowiak report no disclosuresrelevant to the manuscript T Getchius is a former AANemployee and reports no relevant disclosures S Merillatreports no disclosures relevant to the manuscript T Prings-heim has received research support from the CIHR and ShireCanada Inc Go to NeurologyorgN for full disclosures
DisclaimerClinical practice guidelines practice advisories systematicreviews and other guidance published by the AmericanAcademy of Neurology and its affiliates are assessments ofcurrent scientific and clinical information provided as an ed-ucational service The information (1) should not be con-sidered inclusive of all proper treatments methods of care oras a statement of the standard of care (2) is not continuallyupdated and may not reflect the most recent evidence (newevidence may emerge between the time information is de-veloped and when it is published or read) (3) addresses onlythe question(s) specifically identified (4) does not mandateany particular course of medical care and (5) is not intendedto substitute for the independent professional judgment of thetreating provider as the information does not account forindividual variation among people with MS In all cases theselected course of action should be considered by the treating
798 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
provider in the context of treating the individual patientUse of the information is voluntary AAN provides thisinformation on an ldquoas isrdquo basis and makes no warrantyexpressed or implied regarding the information AANspecifically disclaims any warranties of merchantability orfitness for a particular use or purpose AAN assumes noresponsibility for any injury or damage to persons or propertyarising out of or related to any use of this information or forany errors or omissions
Conflict of interest statementThe American Academy of Neurology (AAN) is committedto producing independent critical and truthful clinical prac-tice guidelines (CPGs) Significant efforts are made to mini-mize the potential for conflicts of interest to influence therecommendations of this CPG To the extent possiblethe AAN keeps separate those who have a financial stake inthe success or failure of the products appraised in the CPGsand the developers of the guidelines Conflict of interest formswere obtained from all authors and reviewed by an oversightcommittee prior to project initiation AAN limits the partic-ipation of authors with substantial conflicts of interest TheAAN forbids commercial participation in or funding ofguideline projects Drafts of the guideline have been reviewedby at least 3 AAN committees a network of neurologistsNeurologyreg peer reviewers and representatives from relatedfields The AAN Guideline Author Conflict of Interest Policycan be viewed at aancom For complete information on thisprocess access the 2011 AAN process manual as amended4
Received July 12 2017 Accepted in final form February 15 2018
References1 Rae-Grant A Day GS Marrie RA et al for the Guideline Development Dissemi-
nation and Implementation Subcommittee of the American Academy of NeurologyPractice guideline recommendations summary disease-modifying therapies for adultswith multiple sclerosis report of the Guideline Development Dissemination andImplementation Subcommittee of the American Academy of Neurology Neurology201890777ndash788
2 Goodin DS Frohman EM Garmany GP et al on behalf of the American Academy ofNeurology and the MS Council for Clinical Practice Guidelines Disease-modifyingtherapies in multiple sclerosis subcommittee of the American Academy of Neurologyand the MS Council for Clinical Practice Guidelines report of the Therapeutics andTechnology Assessment Subcommittee of the American Academy of Neurology andthe MS Council for Clinical Practice Guidelines Neurology 200258169ndash178
3 Browne P Chandraratna D Angood C et al Atlas of Multiple Sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
4 American Academy of Neurology Clinical Practice Guideline Process Manual 2011ed [online] St Paul The American Academy of Neurology 2011 Available at aancompolicy-and-guidelinesguidelinesabout-guidelines2 Accessed March 122016
5 Institute of Medicine Eden J Levit L Berg A Morton S editors Committee onStandards for Systematic Reviews of Comparative Effectiveness ResearchWashington DC National Academies Press 2011
6 Institute of Medicine Committee on Standards for Developing Trustworthy ClinicalPractice Guidelines Clinical Practice Guidelines We Can Trust Washington DCNational Academies Press 2011
7 Shea BJ Grimshaw JM Wells GA et al Development of AMSTAR a measurementtool to assess the methodological quality of systematic reviews BMC Med ResMethodol 2007710
8 Guyatt GH Oxman AD Schunemann HJ Tugwell P Knottnerus A GRADEguidelines a new series of articles in the Journal of Clinical Epidemiology J ClinEpidemiol 201164380ndash382
8a Biogen and AbbVie announce the voluntary worldwide withdrawal of marketingauthorizations for ZINBRYTAreg (daclizumab) for relapsing multiple sclerosis [press
release] Available at httpmediabiogencompress-releaseautoimmune-diseasesbiogenC2A0and-abbvie-announceC2A0-voluntaryC2A0worldwide-withdrawal-marketi Issued March 2 2018 Accessed March 5 2018
9 Kappos L Radue EW OrsquoConnor P et al A placebo-controlled trial of oral fingolimodin relapsing multiple sclerosis N Engl J Med 2010362387ndash401
10 Calabresi P Radue EW Goodin D et al Safety and efficacy of fingolimod in patientswith relapsing-remitting multiple sclerosis (FREEDOMS II) a double-blind rando-mised placebo-controlled phase 3 trial Lancet Neurol 201413545ndash556
11 PRISMS (Prevention of Relapses and Disability by Interferon Beta-la Subcutaneouslyin Multiple Sclerosis) Study Group Randomised double-blind placebo-controlledstudy of interferon beta-1a in relapsingremitting multiple sclerosis Lancet 19983521498ndash1504
12 Polman C OrsquoConnor PW Havdrova E et al A randomized placebo-controlled trialof natalizumab for relapsing multiple sclerosis N Engl J Med 2006354899ndash910
13 Hauser SL Bar-Or A Comi G et al for the OPERA I and OPERA II ClinicalInvestigators Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosisN Engl J Med 2017376221ndash234
14 Giovannoni G Comi G Cook S et al on behalf of the CLARITY Study Group Aplacebo-controlled trial of oral cladribine for relapsing multiple sclerosis N Engl JMed 2010362416ndash426
15 Cohen J Coles AJ Arnold DL et al CARE-MS I Investigators Alemtuzumab versusinterferon beta 1a as first-line treatment for patients with relapsing-remitting multiplesclerosis a randomised controlled phase 3 trial Lancet 20123801819ndash1828
16 Cohen J Barkhof F Comi G et al on behalf of the TRANSFORMS Study GroupOral fingolimod or intramuscular interferon for relapsing multiple sclerosis N Engl JMed 2010362402ndash415
17 Panitch H Goodin DS Francis G et al or the University of British Columbia MSMRI Research Group Randomized comparative study of interferon beta-1a treat-ment regimens in MS the EVIDENCE Trial Neurology 2002591496ndash1506
18 Fox R Miller DH Phillips JT et al on behalf of the CONFIRM Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 or glatiramer in multiple sclerosisN Engl J Med 20123671087ndash1097
19 Massacesi L Tramacere I Amoroso S et al Azathioprine versus beta interferons forrelapsing-remitting multiple sclerosis a multicentre randomized non-inferiority trialPLoS One 20149e113371
20 Gold R Giovannoni G Selmaj K et al on behalf of the SELECT Study Inves-tigators Daclizumab high-yield process in relapsing-remitting multiple sclerosis(SELECT) a randomised double-blind placebo-controlled trial Lancet 20133812167ndash2175
21 Gold R Kappos L Arnold DL et al on behalf of the DEFINE Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 for relapsing multiple sclerosisN Engl J Med 20123671098ndash1107
22 Vollmer T Sorensen PS Selmaj K et al on behalf of the BRAVO Study Group Arandomized placebo-controlled phase III trial of oral laquinimod for multiple scle-rosis J Neurol 2014261773ndash783
23 Millefiorini E Gasperini C Pozzilli C et al Randomized placebo-controlled trial ofmitoxantrone in relapsing-remitting multiple sclerosis 24-month clinical and MRIoutcome J Neurol 1997244153ndash159
24 Calabresi P Kieseier BC Arnold DL et al for the ADVANCE Study InvestigatorsPegylated interferon beta-1a for relapsing-remitting multiple sclerosis (ADVANCE)a randomised phase 3 double-blind study Lancet Neurol 201413657ndash665
25 Hauser SL Waubant E Arnold DL et al for the HERMES Trial Group B-celldepletion with rituximab in relapsing-remitting multiple sclerosis N Engl J Med 2008358676ndash688
26 OrsquoConnor P Wolinsky JS Confavreux C et al for the TEMSO Trial Group Ran-domized trial of oral teriflunomide for relapsing multiple sclerosis N Engl J Med20113651293ndash1303
27 Kappos L Wiendl H Selmaj K et al Daclizumab HYP versus interferon beta-1a inrelapsing multiple sclerosis N Engl J Med 20153731418ndash1428
28 Frohman EM Cutter G Remington G et al A randomized blinded parallel-grouppilot trial of mycophenolate mofetil (CellCept) compared with interferon beta-1a(Avonex) in patients with relapsing-remitting multiple sclerosis Ther Adv NeurolDisord 2010315ndash28
29 Coles A TwymanCL Arnold DL et al the CARE-MS II Investigators Alemtuzumab forpatients with relapsing multiple sclerosis after disease-modifying therapy a randomisedcontrolled phase 3 trial Lancet 2012801829ndash1839
30 Zivadinov R Rudick RA De Masi R et al Effects of IV methylprednisolone on brainatrophy in relapsing-remitting MS Neurology 2001571239ndash1247
31 Remington GM Treadaway K Frohman T et al A one-year prospective ran-domized placebo-controlled quadruple-blinded phase II safety pilot trial ofcombination therapy with interferon beta-1a and mycophenolate mofetil in earlyrelapsing-remitting multiple sclerosis (TIME MS) Ther Adv Neurol Disord 201033ndash13
32 Jacobs L Cookfair DL Rudick RA et al Intramuscular interferon beta-1a for diseaseprogression in relapsing multiple sclerosis Ann Neurol 199639285ndash294
33 Confavreux C OrsquoConnor P Comi G et al for the TOWER Trial Group Oralteriflunomide for patients with relapsing multiple sclerosis (TOWER) a randomiseddouble-blind placebo-controlled phase 3 trial Lancet Neurol 201413247ndash256
34 Johnson KP Brooks BR Cohen JA et al Copolymer 1 reduces relapse rate andimproves disability in relapsing-remitting multiple sclerosis results of a phase IIImulticenter double-blind placebo-controlled trial Copolymer 1 Multiple SclerosisStudy Group Neurology 1995451268ndash1276
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 799
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
35 Bornstein MB Miller A Slagle S et al A pilot trial of COP 1 in exacerbating-remittingmultiple sclerosis N Engl J Med 1987317408ndash414
36 Ravnborg M Sorensen PS Andersson M et al Methylprednisolone in combinationwith interferon beta-1a for relapsing-remitting multiple sclerosis (MECOMBINstudy) a multicentre double-blind randomized placebo-controlled parallel-groupstudy Lancet Neurol 20109672ndash680
37 Lublin FD Cofield SS Cutter GR et al on behalf of the CombiRx InvestigatorsRandomized study combining interferon and glatiramer acetate in multiple sclerosisAnn Neurol 201373327ndash340
38 Ellison G Myers LW Mickey MR et al A placebo-controlled randomized double-masked variable dosage clinical trial of azathioprine with and without methylpred-nisolone in multiple sclerosis Neurology 1989391018ndash1026
39 Fazekas F Deisenhammer F Stasser-Fuchs S Nahler G Mamoli B Randomisedplacebo-controlled trial of monthly intravenous immunoglobulin therapy in relapsing-remitting multiple sclerosis Austrian Immunoglobulin in Multiple Sclerosis StudyGroup Lancet 1997349598ndash593
40 Achiron A Gabbay U Gilad R et al Intravenous immunoglobulin treatment inmultiple sclerosis effect on relapses Neurology 199850398ndash402
Neurologyreg Online CME Program
Earn CME while reading Neurology This program is available only to online Neurology subscribers Read the articles markedCME go to Neurologyorg and click on CME This will provide all of the information necessary to get started TheAmerican Academy of Neurology (AAN) is accredited by the Accreditation Council for Continuing Medical Education(ACCME) to sponsor continuing medical education for physicians Neurology is planned and produced in accordance withthe ACCME Essentials For more information contact AAN Member Services at 800-879-1960
NeurologyorgN Offers Important Information to Patients and Their Families
The Neurologyreg Patient Page providesbull A critical review of ground-breaking discoveries in neurologic research that are written especially for patients and their familiesbull Up-to-date patient information about many neurologic diseasesbull Links to additional information resources for neurologic patients
All Neurology Patient Page articles can be easily downloaded and printed and may be reproduced to distribute for educational purposesClick on the lsquoPatientsrsquo link on the home page (NeurologyorgN) for a complete index of Patient Pages
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Audio summaries of current issues Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
800 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000005345201890789-800 Neurology
Alexander Rae-Grant Gregory S Day Ruth Ann Marrie et al Implementation Subcommittee of the American Academy of Neurology
with multiple sclerosis Report of the Guideline Development Dissemination and Comprehensive systematic review summary Disease-modifying therapies for adults
This information is current as of April 23 2018
ServicesUpdated Information amp
httpnneurologyorgcontent9017789fullincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl201804239017789DC1
Supplementary material can be found at
References httpnneurologyorgcontent9017789fullref-list-1
This article cites 37 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9017789fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2018 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

For individuals with CIS the following DMTs are probablymore effective than placebo in reducing the proportion ofindividuals converting to MS (moderate confidence)cladribinee29 immunoglobulinse30 IFN-β-1a 30 μg IMweeklye31 IFN-β-1b subcutaneous alternate daye32 andteriflunomidee33
DiscussionMultiple DMTs are now approved for use in CIS or MSallowing people with MS and clinicians to consider DMTmechanism of action efficacy and AE profile in the decision-making process This systematic review was used to developa practice guideline for the use of DMT for MS acknowl-edging the limits of current evidence Measures of efficacysuch as long-term disability patient satisfaction quality of lifeand effects on MS symptoms may be important to thedecision-making process but ultimately remain inadequatelystudied Similarly there is a dearth of high-quality evidencepertaining to the comparative efficacy of specific DMTs orvarious treatment strategies (eg high-efficacy treatment vsstepped-care treatment protocols) Future studies addressingthese and other questions are needed to further informtreatment recommendations particularly those pertaining towhen to switch or stop DMTs
Author contributionsDr Rae-Grant study concept and design acquisition of dataanalysis or interpretation of data draftingrevising the man-uscript critical revision of the manuscript for important in-tellectual content study supervision Dr Day study conceptand design analysis or interpretation of data draftingrevisingthe manuscript critical revision of the manuscript for im-portant intellectual content Dr Marrie study concept anddesign acquisition of data analysis or interpretation of datadraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Rabinsteinanalysis or interpretation of data draftingrevising the man-uscript Dr Cree study concept and design draftingrevising
the manuscript critical revision of the manuscript forimportant intellectual content Dr Gronseth analysis orinterpretation of data critical revision of the manuscript forimportant intellectual content study supervisionDr Haboubi study concept and design analysis or in-terpretation of data draftingrevising the manuscriptJ Halper study concept and design draftingrevising themanuscript critical revision of the manuscript for importantintellectual content Dr Hosey critical revision of the man-uscript for important intellectual content Dr Jones studyconcept and design draftingrevising the manuscript criticalrevision of the manuscript for important intellectual contentDr Lisak study concept and design draftingrevising themanuscript critical revision of the manuscript for importantintellectual content Dr Pelletier study concept and designdraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Potrebicstudy concept and design acquisition of data analysis or in-terpretation of data draftingrevising the manuscript criticalrevision of the manuscript for important intellectual contentstudy supervision C Sitcov study concept and designdraftingrevising the manuscript critical revision of themanuscript for important intellectual content R Sommersdraftingrevising the manuscript critical revision of themanuscript for important intellectual content Dr Stacho-wiak study concept and design draftingrevising the manu-script critical revision of the manuscript for importantintellectual content TSD Getchius study supervisionSA Merillat draftingrevising the manuscript study super-vision Dr Pringsheim study concept and design acquisitionof data analysis or interpretation of data draftingrevising themanuscript critical revision of the manuscript for importantintellectual content study supervision
AcknowledgmentThe authors thank the North American Research CommitteeonMultiple Sclerosis (NARCOMS) Registry for its assistancein administering an outcomes survey the results of whichwere included in this practice guideline NARCOMS issupported in part by the Consortium of Multiple SclerosisCenters (CMSC) and the Foundation of the CMSC
Figure 5 Outcome Relative risk (RR) of conversion to multiple sclerosis over 2 years
IVIg = IV immunoglobulin LCL = lower confidence limit UCL = upper confidence limit aOutcome measured at 1 year bOutcome measured at 3 years
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 797
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study fundingThis practice guideline was developed with financial supportfrom the American Academy of Neurology (AAN) Authorswho serve as AAN subcommittee members or as method-ologists (AR-G GSD AR GSG MH SP TP) orwho are or were AAN staffmembers (TSDG SAM) werereimbursed by the AAN for expenses related to travel tosubcommittee meetings where drafts of manuscripts werereviewed All authors on the panel were reimbursed by theAAN for expenses related to travel to 2 in-person meetings
DisclosureA Rae-Grant receives royalties from 2 textbooks he haspublished 1 on neurology and 1 on multiple sclerosis (MS)organizes and receives honoraria for grand rounds and neu-rology review courses and is local primary investigator fora clinical trial with MedDay Pharmaceuticals for which hereceives no personal compensation A Rabinstein reports nodisclosures relevant to the manuscript B Cree has receivedcompensation for consulting from AbbVie Biogen EMDSerono GeNeuro GenzymeSanofi Aventis Novartis andShire has given expert testimony and prepared an affidavit formedical malpractice cases (1 or 2 per year) within his area ofexpertise and has acted as consultant in a legal proceeding forAcorda and Biogen G Gronseth serves as associate editor(level of evidence review) for Neurologyreg serves on the edi-torial advisory board for Neurology Now and is compensatedby the American Academy of Neurology (AAN) for meth-odologic activities G Day holds stock in ANI PharmaceuticalsM Haboubi has received travel reimbursement and honorariafor grand rounds presentations in Madisonville KY J Halperand J Hosey report no disclosures relevant to the manuscriptD Jones has received personal compensation for consultingfrom Biogen and Genzyme has received honoraria fromthe Consortium of Multiple Sclerosis Centers (CMSC) theMultiple Sclerosis Association of America (MSAA) and thePharmacy Quality Alliance has received institutional researchsupport from Biogen and the National MS Society (NMSS)has received salary support from the CMSC and has receivedtravel reimbursement from Biogen and Genzyme and fromthe AAN Can Do MS the CMSC and the MSAA R Lisakserved as the President of the CMSC and serves as a memberof the Board of the DMC Foundation has served on scientificadvisory boards for Mallinckrodt Syntimmune Celegeneand Alexion serves as chair of the adjudication committee ofa clinical trial (PAREXEL) has received funding for travelfrom the CMSC the GBSCIDP Foundation Internationalthe NMSS and Syntimmune for travel to consultants meet-ings has served as a journal editor for Clinical and Experi-mental Neuroimmunology andClinical Neuropharmacology hasreceived publishing royalties from Willey for InternationalNeurology A Clinical Approach has received honoraria fromMallinckrodt Syntimmune and Teva Pharmaceuticals andfrom the consulting agencies AlphaSights ClearViewHealthcare Partners GLC and Insights Consulting hasserved on a speakers bureau for Teva Pharmaceuticals for talks
unrelated to pharmaceuticals has received research supportfrom Mallinckrodt for investigator-initiated wet bench stud-ies and from Acorda Avanir Biogen Chugai GenentechMedImmune Novartis and Teva Pharmaceuticals for servingas a site investigator in multicenter trials has given experttestimony prepared an affidavit and acted as witness for TevaPharmaceuticals and has acted as an expert on a patent casefor Acorda Wayne State University has received financialcompensation from the NMSS for his salary as principle in-vestigator for a research grant RA Marrie receives researchgrants from nonprofit organizations including CanadianInstitutes of Health Research (CIHR) the CMSC Crohnrsquosand Colitis Canada the NMSS the Multiple Sclerosis Societyof Canada the Multiple Sclerosis Scientific Research Foun-dation and Research Manitoba and serves on the editorialboard of Neurology D Pelletier has served on scientific ad-visory boards for Biogen EMD Serono GenzymeSanofiAventis Hoffman LaRoche and Novartis has received re-search support for Biogen Genzyme Hoffman LaRoche andthe National Institute of Neurologic Disorders and Stroke ofthe NIH and has received honoraria for providing consultingservices at scientific advisory board meetings from BiogenEMD Serono GenzymeSanofi Aventis Hoffman LaRocheand Novartis S Potrebic received an honorarium from CDIQuality Institute PLE for participation in a headacheappropriate-use criteria panel for imaging and receives travelreimbursement from the AAN for attending AAN ResidencyIn-Service Training Examination Work Group meetingsAAN Axon Registry Committee meetings AAN GuidelineDevelopment Dissemination and Implementation Sub-committee meetings and the Guidelines International Net-work North America Evidence-based Guidelines AffectingPolicy Practice and Stakeholders (E-GAPPS) conference RSommers C Sitcov and J Stachowiak report no disclosuresrelevant to the manuscript T Getchius is a former AANemployee and reports no relevant disclosures S Merillatreports no disclosures relevant to the manuscript T Prings-heim has received research support from the CIHR and ShireCanada Inc Go to NeurologyorgN for full disclosures
DisclaimerClinical practice guidelines practice advisories systematicreviews and other guidance published by the AmericanAcademy of Neurology and its affiliates are assessments ofcurrent scientific and clinical information provided as an ed-ucational service The information (1) should not be con-sidered inclusive of all proper treatments methods of care oras a statement of the standard of care (2) is not continuallyupdated and may not reflect the most recent evidence (newevidence may emerge between the time information is de-veloped and when it is published or read) (3) addresses onlythe question(s) specifically identified (4) does not mandateany particular course of medical care and (5) is not intendedto substitute for the independent professional judgment of thetreating provider as the information does not account forindividual variation among people with MS In all cases theselected course of action should be considered by the treating
798 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
provider in the context of treating the individual patientUse of the information is voluntary AAN provides thisinformation on an ldquoas isrdquo basis and makes no warrantyexpressed or implied regarding the information AANspecifically disclaims any warranties of merchantability orfitness for a particular use or purpose AAN assumes noresponsibility for any injury or damage to persons or propertyarising out of or related to any use of this information or forany errors or omissions
Conflict of interest statementThe American Academy of Neurology (AAN) is committedto producing independent critical and truthful clinical prac-tice guidelines (CPGs) Significant efforts are made to mini-mize the potential for conflicts of interest to influence therecommendations of this CPG To the extent possiblethe AAN keeps separate those who have a financial stake inthe success or failure of the products appraised in the CPGsand the developers of the guidelines Conflict of interest formswere obtained from all authors and reviewed by an oversightcommittee prior to project initiation AAN limits the partic-ipation of authors with substantial conflicts of interest TheAAN forbids commercial participation in or funding ofguideline projects Drafts of the guideline have been reviewedby at least 3 AAN committees a network of neurologistsNeurologyreg peer reviewers and representatives from relatedfields The AAN Guideline Author Conflict of Interest Policycan be viewed at aancom For complete information on thisprocess access the 2011 AAN process manual as amended4
Received July 12 2017 Accepted in final form February 15 2018
References1 Rae-Grant A Day GS Marrie RA et al for the Guideline Development Dissemi-
nation and Implementation Subcommittee of the American Academy of NeurologyPractice guideline recommendations summary disease-modifying therapies for adultswith multiple sclerosis report of the Guideline Development Dissemination andImplementation Subcommittee of the American Academy of Neurology Neurology201890777ndash788
2 Goodin DS Frohman EM Garmany GP et al on behalf of the American Academy ofNeurology and the MS Council for Clinical Practice Guidelines Disease-modifyingtherapies in multiple sclerosis subcommittee of the American Academy of Neurologyand the MS Council for Clinical Practice Guidelines report of the Therapeutics andTechnology Assessment Subcommittee of the American Academy of Neurology andthe MS Council for Clinical Practice Guidelines Neurology 200258169ndash178
3 Browne P Chandraratna D Angood C et al Atlas of Multiple Sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
4 American Academy of Neurology Clinical Practice Guideline Process Manual 2011ed [online] St Paul The American Academy of Neurology 2011 Available at aancompolicy-and-guidelinesguidelinesabout-guidelines2 Accessed March 122016
5 Institute of Medicine Eden J Levit L Berg A Morton S editors Committee onStandards for Systematic Reviews of Comparative Effectiveness ResearchWashington DC National Academies Press 2011
6 Institute of Medicine Committee on Standards for Developing Trustworthy ClinicalPractice Guidelines Clinical Practice Guidelines We Can Trust Washington DCNational Academies Press 2011
7 Shea BJ Grimshaw JM Wells GA et al Development of AMSTAR a measurementtool to assess the methodological quality of systematic reviews BMC Med ResMethodol 2007710
8 Guyatt GH Oxman AD Schunemann HJ Tugwell P Knottnerus A GRADEguidelines a new series of articles in the Journal of Clinical Epidemiology J ClinEpidemiol 201164380ndash382
8a Biogen and AbbVie announce the voluntary worldwide withdrawal of marketingauthorizations for ZINBRYTAreg (daclizumab) for relapsing multiple sclerosis [press
release] Available at httpmediabiogencompress-releaseautoimmune-diseasesbiogenC2A0and-abbvie-announceC2A0-voluntaryC2A0worldwide-withdrawal-marketi Issued March 2 2018 Accessed March 5 2018
9 Kappos L Radue EW OrsquoConnor P et al A placebo-controlled trial of oral fingolimodin relapsing multiple sclerosis N Engl J Med 2010362387ndash401
10 Calabresi P Radue EW Goodin D et al Safety and efficacy of fingolimod in patientswith relapsing-remitting multiple sclerosis (FREEDOMS II) a double-blind rando-mised placebo-controlled phase 3 trial Lancet Neurol 201413545ndash556
11 PRISMS (Prevention of Relapses and Disability by Interferon Beta-la Subcutaneouslyin Multiple Sclerosis) Study Group Randomised double-blind placebo-controlledstudy of interferon beta-1a in relapsingremitting multiple sclerosis Lancet 19983521498ndash1504
12 Polman C OrsquoConnor PW Havdrova E et al A randomized placebo-controlled trialof natalizumab for relapsing multiple sclerosis N Engl J Med 2006354899ndash910
13 Hauser SL Bar-Or A Comi G et al for the OPERA I and OPERA II ClinicalInvestigators Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosisN Engl J Med 2017376221ndash234
14 Giovannoni G Comi G Cook S et al on behalf of the CLARITY Study Group Aplacebo-controlled trial of oral cladribine for relapsing multiple sclerosis N Engl JMed 2010362416ndash426
15 Cohen J Coles AJ Arnold DL et al CARE-MS I Investigators Alemtuzumab versusinterferon beta 1a as first-line treatment for patients with relapsing-remitting multiplesclerosis a randomised controlled phase 3 trial Lancet 20123801819ndash1828
16 Cohen J Barkhof F Comi G et al on behalf of the TRANSFORMS Study GroupOral fingolimod or intramuscular interferon for relapsing multiple sclerosis N Engl JMed 2010362402ndash415
17 Panitch H Goodin DS Francis G et al or the University of British Columbia MSMRI Research Group Randomized comparative study of interferon beta-1a treat-ment regimens in MS the EVIDENCE Trial Neurology 2002591496ndash1506
18 Fox R Miller DH Phillips JT et al on behalf of the CONFIRM Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 or glatiramer in multiple sclerosisN Engl J Med 20123671087ndash1097
19 Massacesi L Tramacere I Amoroso S et al Azathioprine versus beta interferons forrelapsing-remitting multiple sclerosis a multicentre randomized non-inferiority trialPLoS One 20149e113371
20 Gold R Giovannoni G Selmaj K et al on behalf of the SELECT Study Inves-tigators Daclizumab high-yield process in relapsing-remitting multiple sclerosis(SELECT) a randomised double-blind placebo-controlled trial Lancet 20133812167ndash2175
21 Gold R Kappos L Arnold DL et al on behalf of the DEFINE Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 for relapsing multiple sclerosisN Engl J Med 20123671098ndash1107
22 Vollmer T Sorensen PS Selmaj K et al on behalf of the BRAVO Study Group Arandomized placebo-controlled phase III trial of oral laquinimod for multiple scle-rosis J Neurol 2014261773ndash783
23 Millefiorini E Gasperini C Pozzilli C et al Randomized placebo-controlled trial ofmitoxantrone in relapsing-remitting multiple sclerosis 24-month clinical and MRIoutcome J Neurol 1997244153ndash159
24 Calabresi P Kieseier BC Arnold DL et al for the ADVANCE Study InvestigatorsPegylated interferon beta-1a for relapsing-remitting multiple sclerosis (ADVANCE)a randomised phase 3 double-blind study Lancet Neurol 201413657ndash665
25 Hauser SL Waubant E Arnold DL et al for the HERMES Trial Group B-celldepletion with rituximab in relapsing-remitting multiple sclerosis N Engl J Med 2008358676ndash688
26 OrsquoConnor P Wolinsky JS Confavreux C et al for the TEMSO Trial Group Ran-domized trial of oral teriflunomide for relapsing multiple sclerosis N Engl J Med20113651293ndash1303
27 Kappos L Wiendl H Selmaj K et al Daclizumab HYP versus interferon beta-1a inrelapsing multiple sclerosis N Engl J Med 20153731418ndash1428
28 Frohman EM Cutter G Remington G et al A randomized blinded parallel-grouppilot trial of mycophenolate mofetil (CellCept) compared with interferon beta-1a(Avonex) in patients with relapsing-remitting multiple sclerosis Ther Adv NeurolDisord 2010315ndash28
29 Coles A TwymanCL Arnold DL et al the CARE-MS II Investigators Alemtuzumab forpatients with relapsing multiple sclerosis after disease-modifying therapy a randomisedcontrolled phase 3 trial Lancet 2012801829ndash1839
30 Zivadinov R Rudick RA De Masi R et al Effects of IV methylprednisolone on brainatrophy in relapsing-remitting MS Neurology 2001571239ndash1247
31 Remington GM Treadaway K Frohman T et al A one-year prospective ran-domized placebo-controlled quadruple-blinded phase II safety pilot trial ofcombination therapy with interferon beta-1a and mycophenolate mofetil in earlyrelapsing-remitting multiple sclerosis (TIME MS) Ther Adv Neurol Disord 201033ndash13
32 Jacobs L Cookfair DL Rudick RA et al Intramuscular interferon beta-1a for diseaseprogression in relapsing multiple sclerosis Ann Neurol 199639285ndash294
33 Confavreux C OrsquoConnor P Comi G et al for the TOWER Trial Group Oralteriflunomide for patients with relapsing multiple sclerosis (TOWER) a randomiseddouble-blind placebo-controlled phase 3 trial Lancet Neurol 201413247ndash256
34 Johnson KP Brooks BR Cohen JA et al Copolymer 1 reduces relapse rate andimproves disability in relapsing-remitting multiple sclerosis results of a phase IIImulticenter double-blind placebo-controlled trial Copolymer 1 Multiple SclerosisStudy Group Neurology 1995451268ndash1276
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 799
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
35 Bornstein MB Miller A Slagle S et al A pilot trial of COP 1 in exacerbating-remittingmultiple sclerosis N Engl J Med 1987317408ndash414
36 Ravnborg M Sorensen PS Andersson M et al Methylprednisolone in combinationwith interferon beta-1a for relapsing-remitting multiple sclerosis (MECOMBINstudy) a multicentre double-blind randomized placebo-controlled parallel-groupstudy Lancet Neurol 20109672ndash680
37 Lublin FD Cofield SS Cutter GR et al on behalf of the CombiRx InvestigatorsRandomized study combining interferon and glatiramer acetate in multiple sclerosisAnn Neurol 201373327ndash340
38 Ellison G Myers LW Mickey MR et al A placebo-controlled randomized double-masked variable dosage clinical trial of azathioprine with and without methylpred-nisolone in multiple sclerosis Neurology 1989391018ndash1026
39 Fazekas F Deisenhammer F Stasser-Fuchs S Nahler G Mamoli B Randomisedplacebo-controlled trial of monthly intravenous immunoglobulin therapy in relapsing-remitting multiple sclerosis Austrian Immunoglobulin in Multiple Sclerosis StudyGroup Lancet 1997349598ndash593
40 Achiron A Gabbay U Gilad R et al Intravenous immunoglobulin treatment inmultiple sclerosis effect on relapses Neurology 199850398ndash402
Neurologyreg Online CME Program
Earn CME while reading Neurology This program is available only to online Neurology subscribers Read the articles markedCME go to Neurologyorg and click on CME This will provide all of the information necessary to get started TheAmerican Academy of Neurology (AAN) is accredited by the Accreditation Council for Continuing Medical Education(ACCME) to sponsor continuing medical education for physicians Neurology is planned and produced in accordance withthe ACCME Essentials For more information contact AAN Member Services at 800-879-1960
NeurologyorgN Offers Important Information to Patients and Their Families
The Neurologyreg Patient Page providesbull A critical review of ground-breaking discoveries in neurologic research that are written especially for patients and their familiesbull Up-to-date patient information about many neurologic diseasesbull Links to additional information resources for neurologic patients
All Neurology Patient Page articles can be easily downloaded and printed and may be reproduced to distribute for educational purposesClick on the lsquoPatientsrsquo link on the home page (NeurologyorgN) for a complete index of Patient Pages
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Audio summaries of current issues Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
800 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000005345201890789-800 Neurology
Alexander Rae-Grant Gregory S Day Ruth Ann Marrie et al Implementation Subcommittee of the American Academy of Neurology
with multiple sclerosis Report of the Guideline Development Dissemination and Comprehensive systematic review summary Disease-modifying therapies for adults
This information is current as of April 23 2018
ServicesUpdated Information amp
httpnneurologyorgcontent9017789fullincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl201804239017789DC1
Supplementary material can be found at
References httpnneurologyorgcontent9017789fullref-list-1
This article cites 37 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9017789fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2018 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

Study fundingThis practice guideline was developed with financial supportfrom the American Academy of Neurology (AAN) Authorswho serve as AAN subcommittee members or as method-ologists (AR-G GSD AR GSG MH SP TP) orwho are or were AAN staffmembers (TSDG SAM) werereimbursed by the AAN for expenses related to travel tosubcommittee meetings where drafts of manuscripts werereviewed All authors on the panel were reimbursed by theAAN for expenses related to travel to 2 in-person meetings
DisclosureA Rae-Grant receives royalties from 2 textbooks he haspublished 1 on neurology and 1 on multiple sclerosis (MS)organizes and receives honoraria for grand rounds and neu-rology review courses and is local primary investigator fora clinical trial with MedDay Pharmaceuticals for which hereceives no personal compensation A Rabinstein reports nodisclosures relevant to the manuscript B Cree has receivedcompensation for consulting from AbbVie Biogen EMDSerono GeNeuro GenzymeSanofi Aventis Novartis andShire has given expert testimony and prepared an affidavit formedical malpractice cases (1 or 2 per year) within his area ofexpertise and has acted as consultant in a legal proceeding forAcorda and Biogen G Gronseth serves as associate editor(level of evidence review) for Neurologyreg serves on the edi-torial advisory board for Neurology Now and is compensatedby the American Academy of Neurology (AAN) for meth-odologic activities G Day holds stock in ANI PharmaceuticalsM Haboubi has received travel reimbursement and honorariafor grand rounds presentations in Madisonville KY J Halperand J Hosey report no disclosures relevant to the manuscriptD Jones has received personal compensation for consultingfrom Biogen and Genzyme has received honoraria fromthe Consortium of Multiple Sclerosis Centers (CMSC) theMultiple Sclerosis Association of America (MSAA) and thePharmacy Quality Alliance has received institutional researchsupport from Biogen and the National MS Society (NMSS)has received salary support from the CMSC and has receivedtravel reimbursement from Biogen and Genzyme and fromthe AAN Can Do MS the CMSC and the MSAA R Lisakserved as the President of the CMSC and serves as a memberof the Board of the DMC Foundation has served on scientificadvisory boards for Mallinckrodt Syntimmune Celegeneand Alexion serves as chair of the adjudication committee ofa clinical trial (PAREXEL) has received funding for travelfrom the CMSC the GBSCIDP Foundation Internationalthe NMSS and Syntimmune for travel to consultants meet-ings has served as a journal editor for Clinical and Experi-mental Neuroimmunology andClinical Neuropharmacology hasreceived publishing royalties from Willey for InternationalNeurology A Clinical Approach has received honoraria fromMallinckrodt Syntimmune and Teva Pharmaceuticals andfrom the consulting agencies AlphaSights ClearViewHealthcare Partners GLC and Insights Consulting hasserved on a speakers bureau for Teva Pharmaceuticals for talks
unrelated to pharmaceuticals has received research supportfrom Mallinckrodt for investigator-initiated wet bench stud-ies and from Acorda Avanir Biogen Chugai GenentechMedImmune Novartis and Teva Pharmaceuticals for servingas a site investigator in multicenter trials has given experttestimony prepared an affidavit and acted as witness for TevaPharmaceuticals and has acted as an expert on a patent casefor Acorda Wayne State University has received financialcompensation from the NMSS for his salary as principle in-vestigator for a research grant RA Marrie receives researchgrants from nonprofit organizations including CanadianInstitutes of Health Research (CIHR) the CMSC Crohnrsquosand Colitis Canada the NMSS the Multiple Sclerosis Societyof Canada the Multiple Sclerosis Scientific Research Foun-dation and Research Manitoba and serves on the editorialboard of Neurology D Pelletier has served on scientific ad-visory boards for Biogen EMD Serono GenzymeSanofiAventis Hoffman LaRoche and Novartis has received re-search support for Biogen Genzyme Hoffman LaRoche andthe National Institute of Neurologic Disorders and Stroke ofthe NIH and has received honoraria for providing consultingservices at scientific advisory board meetings from BiogenEMD Serono GenzymeSanofi Aventis Hoffman LaRocheand Novartis S Potrebic received an honorarium from CDIQuality Institute PLE for participation in a headacheappropriate-use criteria panel for imaging and receives travelreimbursement from the AAN for attending AAN ResidencyIn-Service Training Examination Work Group meetingsAAN Axon Registry Committee meetings AAN GuidelineDevelopment Dissemination and Implementation Sub-committee meetings and the Guidelines International Net-work North America Evidence-based Guidelines AffectingPolicy Practice and Stakeholders (E-GAPPS) conference RSommers C Sitcov and J Stachowiak report no disclosuresrelevant to the manuscript T Getchius is a former AANemployee and reports no relevant disclosures S Merillatreports no disclosures relevant to the manuscript T Prings-heim has received research support from the CIHR and ShireCanada Inc Go to NeurologyorgN for full disclosures
DisclaimerClinical practice guidelines practice advisories systematicreviews and other guidance published by the AmericanAcademy of Neurology and its affiliates are assessments ofcurrent scientific and clinical information provided as an ed-ucational service The information (1) should not be con-sidered inclusive of all proper treatments methods of care oras a statement of the standard of care (2) is not continuallyupdated and may not reflect the most recent evidence (newevidence may emerge between the time information is de-veloped and when it is published or read) (3) addresses onlythe question(s) specifically identified (4) does not mandateany particular course of medical care and (5) is not intendedto substitute for the independent professional judgment of thetreating provider as the information does not account forindividual variation among people with MS In all cases theselected course of action should be considered by the treating
798 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
provider in the context of treating the individual patientUse of the information is voluntary AAN provides thisinformation on an ldquoas isrdquo basis and makes no warrantyexpressed or implied regarding the information AANspecifically disclaims any warranties of merchantability orfitness for a particular use or purpose AAN assumes noresponsibility for any injury or damage to persons or propertyarising out of or related to any use of this information or forany errors or omissions
Conflict of interest statementThe American Academy of Neurology (AAN) is committedto producing independent critical and truthful clinical prac-tice guidelines (CPGs) Significant efforts are made to mini-mize the potential for conflicts of interest to influence therecommendations of this CPG To the extent possiblethe AAN keeps separate those who have a financial stake inthe success or failure of the products appraised in the CPGsand the developers of the guidelines Conflict of interest formswere obtained from all authors and reviewed by an oversightcommittee prior to project initiation AAN limits the partic-ipation of authors with substantial conflicts of interest TheAAN forbids commercial participation in or funding ofguideline projects Drafts of the guideline have been reviewedby at least 3 AAN committees a network of neurologistsNeurologyreg peer reviewers and representatives from relatedfields The AAN Guideline Author Conflict of Interest Policycan be viewed at aancom For complete information on thisprocess access the 2011 AAN process manual as amended4
Received July 12 2017 Accepted in final form February 15 2018
References1 Rae-Grant A Day GS Marrie RA et al for the Guideline Development Dissemi-
nation and Implementation Subcommittee of the American Academy of NeurologyPractice guideline recommendations summary disease-modifying therapies for adultswith multiple sclerosis report of the Guideline Development Dissemination andImplementation Subcommittee of the American Academy of Neurology Neurology201890777ndash788
2 Goodin DS Frohman EM Garmany GP et al on behalf of the American Academy ofNeurology and the MS Council for Clinical Practice Guidelines Disease-modifyingtherapies in multiple sclerosis subcommittee of the American Academy of Neurologyand the MS Council for Clinical Practice Guidelines report of the Therapeutics andTechnology Assessment Subcommittee of the American Academy of Neurology andthe MS Council for Clinical Practice Guidelines Neurology 200258169ndash178
3 Browne P Chandraratna D Angood C et al Atlas of Multiple Sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
4 American Academy of Neurology Clinical Practice Guideline Process Manual 2011ed [online] St Paul The American Academy of Neurology 2011 Available at aancompolicy-and-guidelinesguidelinesabout-guidelines2 Accessed March 122016
5 Institute of Medicine Eden J Levit L Berg A Morton S editors Committee onStandards for Systematic Reviews of Comparative Effectiveness ResearchWashington DC National Academies Press 2011
6 Institute of Medicine Committee on Standards for Developing Trustworthy ClinicalPractice Guidelines Clinical Practice Guidelines We Can Trust Washington DCNational Academies Press 2011
7 Shea BJ Grimshaw JM Wells GA et al Development of AMSTAR a measurementtool to assess the methodological quality of systematic reviews BMC Med ResMethodol 2007710
8 Guyatt GH Oxman AD Schunemann HJ Tugwell P Knottnerus A GRADEguidelines a new series of articles in the Journal of Clinical Epidemiology J ClinEpidemiol 201164380ndash382
8a Biogen and AbbVie announce the voluntary worldwide withdrawal of marketingauthorizations for ZINBRYTAreg (daclizumab) for relapsing multiple sclerosis [press
release] Available at httpmediabiogencompress-releaseautoimmune-diseasesbiogenC2A0and-abbvie-announceC2A0-voluntaryC2A0worldwide-withdrawal-marketi Issued March 2 2018 Accessed March 5 2018
9 Kappos L Radue EW OrsquoConnor P et al A placebo-controlled trial of oral fingolimodin relapsing multiple sclerosis N Engl J Med 2010362387ndash401
10 Calabresi P Radue EW Goodin D et al Safety and efficacy of fingolimod in patientswith relapsing-remitting multiple sclerosis (FREEDOMS II) a double-blind rando-mised placebo-controlled phase 3 trial Lancet Neurol 201413545ndash556
11 PRISMS (Prevention of Relapses and Disability by Interferon Beta-la Subcutaneouslyin Multiple Sclerosis) Study Group Randomised double-blind placebo-controlledstudy of interferon beta-1a in relapsingremitting multiple sclerosis Lancet 19983521498ndash1504
12 Polman C OrsquoConnor PW Havdrova E et al A randomized placebo-controlled trialof natalizumab for relapsing multiple sclerosis N Engl J Med 2006354899ndash910
13 Hauser SL Bar-Or A Comi G et al for the OPERA I and OPERA II ClinicalInvestigators Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosisN Engl J Med 2017376221ndash234
14 Giovannoni G Comi G Cook S et al on behalf of the CLARITY Study Group Aplacebo-controlled trial of oral cladribine for relapsing multiple sclerosis N Engl JMed 2010362416ndash426
15 Cohen J Coles AJ Arnold DL et al CARE-MS I Investigators Alemtuzumab versusinterferon beta 1a as first-line treatment for patients with relapsing-remitting multiplesclerosis a randomised controlled phase 3 trial Lancet 20123801819ndash1828
16 Cohen J Barkhof F Comi G et al on behalf of the TRANSFORMS Study GroupOral fingolimod or intramuscular interferon for relapsing multiple sclerosis N Engl JMed 2010362402ndash415
17 Panitch H Goodin DS Francis G et al or the University of British Columbia MSMRI Research Group Randomized comparative study of interferon beta-1a treat-ment regimens in MS the EVIDENCE Trial Neurology 2002591496ndash1506
18 Fox R Miller DH Phillips JT et al on behalf of the CONFIRM Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 or glatiramer in multiple sclerosisN Engl J Med 20123671087ndash1097
19 Massacesi L Tramacere I Amoroso S et al Azathioprine versus beta interferons forrelapsing-remitting multiple sclerosis a multicentre randomized non-inferiority trialPLoS One 20149e113371
20 Gold R Giovannoni G Selmaj K et al on behalf of the SELECT Study Inves-tigators Daclizumab high-yield process in relapsing-remitting multiple sclerosis(SELECT) a randomised double-blind placebo-controlled trial Lancet 20133812167ndash2175
21 Gold R Kappos L Arnold DL et al on behalf of the DEFINE Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 for relapsing multiple sclerosisN Engl J Med 20123671098ndash1107
22 Vollmer T Sorensen PS Selmaj K et al on behalf of the BRAVO Study Group Arandomized placebo-controlled phase III trial of oral laquinimod for multiple scle-rosis J Neurol 2014261773ndash783
23 Millefiorini E Gasperini C Pozzilli C et al Randomized placebo-controlled trial ofmitoxantrone in relapsing-remitting multiple sclerosis 24-month clinical and MRIoutcome J Neurol 1997244153ndash159
24 Calabresi P Kieseier BC Arnold DL et al for the ADVANCE Study InvestigatorsPegylated interferon beta-1a for relapsing-remitting multiple sclerosis (ADVANCE)a randomised phase 3 double-blind study Lancet Neurol 201413657ndash665
25 Hauser SL Waubant E Arnold DL et al for the HERMES Trial Group B-celldepletion with rituximab in relapsing-remitting multiple sclerosis N Engl J Med 2008358676ndash688
26 OrsquoConnor P Wolinsky JS Confavreux C et al for the TEMSO Trial Group Ran-domized trial of oral teriflunomide for relapsing multiple sclerosis N Engl J Med20113651293ndash1303
27 Kappos L Wiendl H Selmaj K et al Daclizumab HYP versus interferon beta-1a inrelapsing multiple sclerosis N Engl J Med 20153731418ndash1428
28 Frohman EM Cutter G Remington G et al A randomized blinded parallel-grouppilot trial of mycophenolate mofetil (CellCept) compared with interferon beta-1a(Avonex) in patients with relapsing-remitting multiple sclerosis Ther Adv NeurolDisord 2010315ndash28
29 Coles A TwymanCL Arnold DL et al the CARE-MS II Investigators Alemtuzumab forpatients with relapsing multiple sclerosis after disease-modifying therapy a randomisedcontrolled phase 3 trial Lancet 2012801829ndash1839
30 Zivadinov R Rudick RA De Masi R et al Effects of IV methylprednisolone on brainatrophy in relapsing-remitting MS Neurology 2001571239ndash1247
31 Remington GM Treadaway K Frohman T et al A one-year prospective ran-domized placebo-controlled quadruple-blinded phase II safety pilot trial ofcombination therapy with interferon beta-1a and mycophenolate mofetil in earlyrelapsing-remitting multiple sclerosis (TIME MS) Ther Adv Neurol Disord 201033ndash13
32 Jacobs L Cookfair DL Rudick RA et al Intramuscular interferon beta-1a for diseaseprogression in relapsing multiple sclerosis Ann Neurol 199639285ndash294
33 Confavreux C OrsquoConnor P Comi G et al for the TOWER Trial Group Oralteriflunomide for patients with relapsing multiple sclerosis (TOWER) a randomiseddouble-blind placebo-controlled phase 3 trial Lancet Neurol 201413247ndash256
34 Johnson KP Brooks BR Cohen JA et al Copolymer 1 reduces relapse rate andimproves disability in relapsing-remitting multiple sclerosis results of a phase IIImulticenter double-blind placebo-controlled trial Copolymer 1 Multiple SclerosisStudy Group Neurology 1995451268ndash1276
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 799
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
35 Bornstein MB Miller A Slagle S et al A pilot trial of COP 1 in exacerbating-remittingmultiple sclerosis N Engl J Med 1987317408ndash414
36 Ravnborg M Sorensen PS Andersson M et al Methylprednisolone in combinationwith interferon beta-1a for relapsing-remitting multiple sclerosis (MECOMBINstudy) a multicentre double-blind randomized placebo-controlled parallel-groupstudy Lancet Neurol 20109672ndash680
37 Lublin FD Cofield SS Cutter GR et al on behalf of the CombiRx InvestigatorsRandomized study combining interferon and glatiramer acetate in multiple sclerosisAnn Neurol 201373327ndash340
38 Ellison G Myers LW Mickey MR et al A placebo-controlled randomized double-masked variable dosage clinical trial of azathioprine with and without methylpred-nisolone in multiple sclerosis Neurology 1989391018ndash1026
39 Fazekas F Deisenhammer F Stasser-Fuchs S Nahler G Mamoli B Randomisedplacebo-controlled trial of monthly intravenous immunoglobulin therapy in relapsing-remitting multiple sclerosis Austrian Immunoglobulin in Multiple Sclerosis StudyGroup Lancet 1997349598ndash593
40 Achiron A Gabbay U Gilad R et al Intravenous immunoglobulin treatment inmultiple sclerosis effect on relapses Neurology 199850398ndash402
Neurologyreg Online CME Program
Earn CME while reading Neurology This program is available only to online Neurology subscribers Read the articles markedCME go to Neurologyorg and click on CME This will provide all of the information necessary to get started TheAmerican Academy of Neurology (AAN) is accredited by the Accreditation Council for Continuing Medical Education(ACCME) to sponsor continuing medical education for physicians Neurology is planned and produced in accordance withthe ACCME Essentials For more information contact AAN Member Services at 800-879-1960
NeurologyorgN Offers Important Information to Patients and Their Families
The Neurologyreg Patient Page providesbull A critical review of ground-breaking discoveries in neurologic research that are written especially for patients and their familiesbull Up-to-date patient information about many neurologic diseasesbull Links to additional information resources for neurologic patients
All Neurology Patient Page articles can be easily downloaded and printed and may be reproduced to distribute for educational purposesClick on the lsquoPatientsrsquo link on the home page (NeurologyorgN) for a complete index of Patient Pages
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Audio summaries of current issues Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
800 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000005345201890789-800 Neurology
Alexander Rae-Grant Gregory S Day Ruth Ann Marrie et al Implementation Subcommittee of the American Academy of Neurology
with multiple sclerosis Report of the Guideline Development Dissemination and Comprehensive systematic review summary Disease-modifying therapies for adults
This information is current as of April 23 2018
ServicesUpdated Information amp
httpnneurologyorgcontent9017789fullincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl201804239017789DC1
Supplementary material can be found at
References httpnneurologyorgcontent9017789fullref-list-1
This article cites 37 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9017789fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2018 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

provider in the context of treating the individual patientUse of the information is voluntary AAN provides thisinformation on an ldquoas isrdquo basis and makes no warrantyexpressed or implied regarding the information AANspecifically disclaims any warranties of merchantability orfitness for a particular use or purpose AAN assumes noresponsibility for any injury or damage to persons or propertyarising out of or related to any use of this information or forany errors or omissions
Conflict of interest statementThe American Academy of Neurology (AAN) is committedto producing independent critical and truthful clinical prac-tice guidelines (CPGs) Significant efforts are made to mini-mize the potential for conflicts of interest to influence therecommendations of this CPG To the extent possiblethe AAN keeps separate those who have a financial stake inthe success or failure of the products appraised in the CPGsand the developers of the guidelines Conflict of interest formswere obtained from all authors and reviewed by an oversightcommittee prior to project initiation AAN limits the partic-ipation of authors with substantial conflicts of interest TheAAN forbids commercial participation in or funding ofguideline projects Drafts of the guideline have been reviewedby at least 3 AAN committees a network of neurologistsNeurologyreg peer reviewers and representatives from relatedfields The AAN Guideline Author Conflict of Interest Policycan be viewed at aancom For complete information on thisprocess access the 2011 AAN process manual as amended4
Received July 12 2017 Accepted in final form February 15 2018
References1 Rae-Grant A Day GS Marrie RA et al for the Guideline Development Dissemi-
nation and Implementation Subcommittee of the American Academy of NeurologyPractice guideline recommendations summary disease-modifying therapies for adultswith multiple sclerosis report of the Guideline Development Dissemination andImplementation Subcommittee of the American Academy of Neurology Neurology201890777ndash788
2 Goodin DS Frohman EM Garmany GP et al on behalf of the American Academy ofNeurology and the MS Council for Clinical Practice Guidelines Disease-modifyingtherapies in multiple sclerosis subcommittee of the American Academy of Neurologyand the MS Council for Clinical Practice Guidelines report of the Therapeutics andTechnology Assessment Subcommittee of the American Academy of Neurology andthe MS Council for Clinical Practice Guidelines Neurology 200258169ndash178
3 Browne P Chandraratna D Angood C et al Atlas of Multiple Sclerosis 2013a growing global problem with widespread inequity Neurology 2014831022ndash1024
4 American Academy of Neurology Clinical Practice Guideline Process Manual 2011ed [online] St Paul The American Academy of Neurology 2011 Available at aancompolicy-and-guidelinesguidelinesabout-guidelines2 Accessed March 122016
5 Institute of Medicine Eden J Levit L Berg A Morton S editors Committee onStandards for Systematic Reviews of Comparative Effectiveness ResearchWashington DC National Academies Press 2011
6 Institute of Medicine Committee on Standards for Developing Trustworthy ClinicalPractice Guidelines Clinical Practice Guidelines We Can Trust Washington DCNational Academies Press 2011
7 Shea BJ Grimshaw JM Wells GA et al Development of AMSTAR a measurementtool to assess the methodological quality of systematic reviews BMC Med ResMethodol 2007710
8 Guyatt GH Oxman AD Schunemann HJ Tugwell P Knottnerus A GRADEguidelines a new series of articles in the Journal of Clinical Epidemiology J ClinEpidemiol 201164380ndash382
8a Biogen and AbbVie announce the voluntary worldwide withdrawal of marketingauthorizations for ZINBRYTAreg (daclizumab) for relapsing multiple sclerosis [press
release] Available at httpmediabiogencompress-releaseautoimmune-diseasesbiogenC2A0and-abbvie-announceC2A0-voluntaryC2A0worldwide-withdrawal-marketi Issued March 2 2018 Accessed March 5 2018
9 Kappos L Radue EW OrsquoConnor P et al A placebo-controlled trial of oral fingolimodin relapsing multiple sclerosis N Engl J Med 2010362387ndash401
10 Calabresi P Radue EW Goodin D et al Safety and efficacy of fingolimod in patientswith relapsing-remitting multiple sclerosis (FREEDOMS II) a double-blind rando-mised placebo-controlled phase 3 trial Lancet Neurol 201413545ndash556
11 PRISMS (Prevention of Relapses and Disability by Interferon Beta-la Subcutaneouslyin Multiple Sclerosis) Study Group Randomised double-blind placebo-controlledstudy of interferon beta-1a in relapsingremitting multiple sclerosis Lancet 19983521498ndash1504
12 Polman C OrsquoConnor PW Havdrova E et al A randomized placebo-controlled trialof natalizumab for relapsing multiple sclerosis N Engl J Med 2006354899ndash910
13 Hauser SL Bar-Or A Comi G et al for the OPERA I and OPERA II ClinicalInvestigators Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosisN Engl J Med 2017376221ndash234
14 Giovannoni G Comi G Cook S et al on behalf of the CLARITY Study Group Aplacebo-controlled trial of oral cladribine for relapsing multiple sclerosis N Engl JMed 2010362416ndash426
15 Cohen J Coles AJ Arnold DL et al CARE-MS I Investigators Alemtuzumab versusinterferon beta 1a as first-line treatment for patients with relapsing-remitting multiplesclerosis a randomised controlled phase 3 trial Lancet 20123801819ndash1828
16 Cohen J Barkhof F Comi G et al on behalf of the TRANSFORMS Study GroupOral fingolimod or intramuscular interferon for relapsing multiple sclerosis N Engl JMed 2010362402ndash415
17 Panitch H Goodin DS Francis G et al or the University of British Columbia MSMRI Research Group Randomized comparative study of interferon beta-1a treat-ment regimens in MS the EVIDENCE Trial Neurology 2002591496ndash1506
18 Fox R Miller DH Phillips JT et al on behalf of the CONFIRM Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 or glatiramer in multiple sclerosisN Engl J Med 20123671087ndash1097
19 Massacesi L Tramacere I Amoroso S et al Azathioprine versus beta interferons forrelapsing-remitting multiple sclerosis a multicentre randomized non-inferiority trialPLoS One 20149e113371
20 Gold R Giovannoni G Selmaj K et al on behalf of the SELECT Study Inves-tigators Daclizumab high-yield process in relapsing-remitting multiple sclerosis(SELECT) a randomised double-blind placebo-controlled trial Lancet 20133812167ndash2175
21 Gold R Kappos L Arnold DL et al on behalf of the DEFINE Study InvestigatorsPlacebo-controlled phase 3 study of oral BG-12 for relapsing multiple sclerosisN Engl J Med 20123671098ndash1107
22 Vollmer T Sorensen PS Selmaj K et al on behalf of the BRAVO Study Group Arandomized placebo-controlled phase III trial of oral laquinimod for multiple scle-rosis J Neurol 2014261773ndash783
23 Millefiorini E Gasperini C Pozzilli C et al Randomized placebo-controlled trial ofmitoxantrone in relapsing-remitting multiple sclerosis 24-month clinical and MRIoutcome J Neurol 1997244153ndash159
24 Calabresi P Kieseier BC Arnold DL et al for the ADVANCE Study InvestigatorsPegylated interferon beta-1a for relapsing-remitting multiple sclerosis (ADVANCE)a randomised phase 3 double-blind study Lancet Neurol 201413657ndash665
25 Hauser SL Waubant E Arnold DL et al for the HERMES Trial Group B-celldepletion with rituximab in relapsing-remitting multiple sclerosis N Engl J Med 2008358676ndash688
26 OrsquoConnor P Wolinsky JS Confavreux C et al for the TEMSO Trial Group Ran-domized trial of oral teriflunomide for relapsing multiple sclerosis N Engl J Med20113651293ndash1303
27 Kappos L Wiendl H Selmaj K et al Daclizumab HYP versus interferon beta-1a inrelapsing multiple sclerosis N Engl J Med 20153731418ndash1428
28 Frohman EM Cutter G Remington G et al A randomized blinded parallel-grouppilot trial of mycophenolate mofetil (CellCept) compared with interferon beta-1a(Avonex) in patients with relapsing-remitting multiple sclerosis Ther Adv NeurolDisord 2010315ndash28
29 Coles A TwymanCL Arnold DL et al the CARE-MS II Investigators Alemtuzumab forpatients with relapsing multiple sclerosis after disease-modifying therapy a randomisedcontrolled phase 3 trial Lancet 2012801829ndash1839
30 Zivadinov R Rudick RA De Masi R et al Effects of IV methylprednisolone on brainatrophy in relapsing-remitting MS Neurology 2001571239ndash1247
31 Remington GM Treadaway K Frohman T et al A one-year prospective ran-domized placebo-controlled quadruple-blinded phase II safety pilot trial ofcombination therapy with interferon beta-1a and mycophenolate mofetil in earlyrelapsing-remitting multiple sclerosis (TIME MS) Ther Adv Neurol Disord 201033ndash13
32 Jacobs L Cookfair DL Rudick RA et al Intramuscular interferon beta-1a for diseaseprogression in relapsing multiple sclerosis Ann Neurol 199639285ndash294
33 Confavreux C OrsquoConnor P Comi G et al for the TOWER Trial Group Oralteriflunomide for patients with relapsing multiple sclerosis (TOWER) a randomiseddouble-blind placebo-controlled phase 3 trial Lancet Neurol 201413247ndash256
34 Johnson KP Brooks BR Cohen JA et al Copolymer 1 reduces relapse rate andimproves disability in relapsing-remitting multiple sclerosis results of a phase IIImulticenter double-blind placebo-controlled trial Copolymer 1 Multiple SclerosisStudy Group Neurology 1995451268ndash1276
NeurologyorgN Neurology | Volume 90 Number 17 | April 24 2018 799
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
35 Bornstein MB Miller A Slagle S et al A pilot trial of COP 1 in exacerbating-remittingmultiple sclerosis N Engl J Med 1987317408ndash414
36 Ravnborg M Sorensen PS Andersson M et al Methylprednisolone in combinationwith interferon beta-1a for relapsing-remitting multiple sclerosis (MECOMBINstudy) a multicentre double-blind randomized placebo-controlled parallel-groupstudy Lancet Neurol 20109672ndash680
37 Lublin FD Cofield SS Cutter GR et al on behalf of the CombiRx InvestigatorsRandomized study combining interferon and glatiramer acetate in multiple sclerosisAnn Neurol 201373327ndash340
38 Ellison G Myers LW Mickey MR et al A placebo-controlled randomized double-masked variable dosage clinical trial of azathioprine with and without methylpred-nisolone in multiple sclerosis Neurology 1989391018ndash1026
39 Fazekas F Deisenhammer F Stasser-Fuchs S Nahler G Mamoli B Randomisedplacebo-controlled trial of monthly intravenous immunoglobulin therapy in relapsing-remitting multiple sclerosis Austrian Immunoglobulin in Multiple Sclerosis StudyGroup Lancet 1997349598ndash593
40 Achiron A Gabbay U Gilad R et al Intravenous immunoglobulin treatment inmultiple sclerosis effect on relapses Neurology 199850398ndash402
Neurologyreg Online CME Program
Earn CME while reading Neurology This program is available only to online Neurology subscribers Read the articles markedCME go to Neurologyorg and click on CME This will provide all of the information necessary to get started TheAmerican Academy of Neurology (AAN) is accredited by the Accreditation Council for Continuing Medical Education(ACCME) to sponsor continuing medical education for physicians Neurology is planned and produced in accordance withthe ACCME Essentials For more information contact AAN Member Services at 800-879-1960
NeurologyorgN Offers Important Information to Patients and Their Families
The Neurologyreg Patient Page providesbull A critical review of ground-breaking discoveries in neurologic research that are written especially for patients and their familiesbull Up-to-date patient information about many neurologic diseasesbull Links to additional information resources for neurologic patients
All Neurology Patient Page articles can be easily downloaded and printed and may be reproduced to distribute for educational purposesClick on the lsquoPatientsrsquo link on the home page (NeurologyorgN) for a complete index of Patient Pages
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Audio summaries of current issues Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
800 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000005345201890789-800 Neurology
Alexander Rae-Grant Gregory S Day Ruth Ann Marrie et al Implementation Subcommittee of the American Academy of Neurology
with multiple sclerosis Report of the Guideline Development Dissemination and Comprehensive systematic review summary Disease-modifying therapies for adults
This information is current as of April 23 2018
ServicesUpdated Information amp
httpnneurologyorgcontent9017789fullincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl201804239017789DC1
Supplementary material can be found at
References httpnneurologyorgcontent9017789fullref-list-1
This article cites 37 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9017789fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2018 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

35 Bornstein MB Miller A Slagle S et al A pilot trial of COP 1 in exacerbating-remittingmultiple sclerosis N Engl J Med 1987317408ndash414
36 Ravnborg M Sorensen PS Andersson M et al Methylprednisolone in combinationwith interferon beta-1a for relapsing-remitting multiple sclerosis (MECOMBINstudy) a multicentre double-blind randomized placebo-controlled parallel-groupstudy Lancet Neurol 20109672ndash680
37 Lublin FD Cofield SS Cutter GR et al on behalf of the CombiRx InvestigatorsRandomized study combining interferon and glatiramer acetate in multiple sclerosisAnn Neurol 201373327ndash340
38 Ellison G Myers LW Mickey MR et al A placebo-controlled randomized double-masked variable dosage clinical trial of azathioprine with and without methylpred-nisolone in multiple sclerosis Neurology 1989391018ndash1026
39 Fazekas F Deisenhammer F Stasser-Fuchs S Nahler G Mamoli B Randomisedplacebo-controlled trial of monthly intravenous immunoglobulin therapy in relapsing-remitting multiple sclerosis Austrian Immunoglobulin in Multiple Sclerosis StudyGroup Lancet 1997349598ndash593
40 Achiron A Gabbay U Gilad R et al Intravenous immunoglobulin treatment inmultiple sclerosis effect on relapses Neurology 199850398ndash402
Neurologyreg Online CME Program
Earn CME while reading Neurology This program is available only to online Neurology subscribers Read the articles markedCME go to Neurologyorg and click on CME This will provide all of the information necessary to get started TheAmerican Academy of Neurology (AAN) is accredited by the Accreditation Council for Continuing Medical Education(ACCME) to sponsor continuing medical education for physicians Neurology is planned and produced in accordance withthe ACCME Essentials For more information contact AAN Member Services at 800-879-1960
NeurologyorgN Offers Important Information to Patients and Their Families
The Neurologyreg Patient Page providesbull A critical review of ground-breaking discoveries in neurologic research that are written especially for patients and their familiesbull Up-to-date patient information about many neurologic diseasesbull Links to additional information resources for neurologic patients
All Neurology Patient Page articles can be easily downloaded and printed and may be reproduced to distribute for educational purposesClick on the lsquoPatientsrsquo link on the home page (NeurologyorgN) for a complete index of Patient Pages
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Audio summaries of current issues Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
800 Neurology | Volume 90 Number 17 | April 24 2018 NeurologyorgN
Copyright ordf 2018 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000005345201890789-800 Neurology
Alexander Rae-Grant Gregory S Day Ruth Ann Marrie et al Implementation Subcommittee of the American Academy of Neurology
with multiple sclerosis Report of the Guideline Development Dissemination and Comprehensive systematic review summary Disease-modifying therapies for adults
This information is current as of April 23 2018
ServicesUpdated Information amp
httpnneurologyorgcontent9017789fullincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl201804239017789DC1
Supplementary material can be found at
References httpnneurologyorgcontent9017789fullref-list-1
This article cites 37 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9017789fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2018 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

DOI 101212WNL0000000000005345201890789-800 Neurology
Alexander Rae-Grant Gregory S Day Ruth Ann Marrie et al Implementation Subcommittee of the American Academy of Neurology
with multiple sclerosis Report of the Guideline Development Dissemination and Comprehensive systematic review summary Disease-modifying therapies for adults
This information is current as of April 23 2018
ServicesUpdated Information amp
httpnneurologyorgcontent9017789fullincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl201804239017789DC1
Supplementary material can be found at
References httpnneurologyorgcontent9017789fullref-list-1
This article cites 37 articles 8 of which you can access for free at
Citations httpnneurologyorgcontent9017789fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2018 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology


















