Complete recovery following sudden sensorineural hearing ... · SNHL is a multitfactorial process...
3
case report Hematol Oncol Stem Cell Ther 4(2) Second Quarter 2011 hemoncstem.edmgr.com 97 S ickle cell disease (SCD) is a hemolytic anemia quite prevalent in Oman, with the most recent epidemiological data suggesting a sickle cell gene carrier rate of about 6% and SCD prevalence of 0.2%. 1,2 e disease is characterized by a change in the shape of red cells to the classical sickled shape leading to a process of vessel occlusion involving the smallt and met diumtsized vessels in almost all parts of the body. e process of vasotocclusion is made worse by episodes of infections, dehydration or deoxygenation. 3 It is also known that patients with SCD are at an increased risk of thrombosis and this process is considt ered to contribute to several clinical features of the dist ease including leg ulcers, priapism, avascular necrosis of bone, pulmonary hypertension, acute chest syndrome, stroke, and apparently any random infarctive lesions that can occur anywhere in the body. e cochlea, the organ of hearing, is not immune from this process and audiometric assessment is a sensitive indicator of any sensorineural (perceptive) hearing loss resulting from any occlusive vascular involvement. 4 e prevalence of involvement of the ears in SCD pat tients is variable but it is reported to occur between 11% to 41% in black patients with this disease and can lead to sensorineural hearing loss (SNHL). 5,6 e pattern of involvement is also variable and it can be either unilatt eral, bilateral, temporary or permanent. 7,8 We report on Complete recovery following sudden sensorineural hearing loss in a patient with sickle cell disease Salam Alkindi, Najwa Arafa, M Al Okbi, Anil Pathare from the Department of haematology, College of medicine and health sciences, sultan Qaboos university hospital, muscat, oman Correspondence: Prof. salam alkindi · Department of haematology, College of medicine and health sciences, sultan Qaboos university hospital, Po Box 35, PC 123, al Khod, muscat, 000123 oman · t: +96899353188 f: +96824144887 · [email protected] · accepted: June 2011 hematol oncol stem Cell ther 2011; 4(2): 97-99 Doi: 10.5144/1658-3876.2011.97 a sickle cell disease (sCD) patient with vaso-occlusive crisis (VoC) developed sudden senserinural hear- ing loss (snhL), which responded well to a rapid course of corticosteroids along with exchange trans- fusions. the otolaryngologist should be aware of the otologic manifestations of sCD such as snhL. a good response to steroids, which averted a permanent hearing loss, warrants further studies to define the augmentive benefits of such therapy along with exchange transfusions in patients with sCD in VoC who develop sudden snhL. a young female with a complicated history of SCD who presented with a sudden onset of sensorineural hearing loss (SNHL) that completely resolved following antet cedent medical therapy. We wish to highlight here the need for appropriate and rapid audiometric evaluation and followtup treatment so that a reversible and treatt able cause for rapid hearing loss in patients with SCD with VOC such as ours can be quickly achieved. CASE A 26tyeartold Omani female with SCD (Hb S/S genot type) was admitted in January 2010 with acute painful crisis involving the chest, legs and back. Her medical history was significant and included a stroke in childt hood with complete neurological recovery, protein C deficiency, acute chest syndrome, and iron overload due to repeated blood transfusions/exchange. She was taking hydroxyurea, desferoxamine, penicillin V, folic acid, cotcodamol, aspirin and enoxaparin. On admist sion, she had stable vital signs with pallor and icterus. She was treated with hydration, pain management with morphine infusion and nontsteroidal antitinflammat tory drugs. Two days after admission, the patient awoke with acute complete hearing loss in the left ear. ere was no history of imbalance or vertigo and she was otherwise well, apart from her ongoing painful crisis. Her hearing had previously been considered normal.
Transcript of Complete recovery following sudden sensorineural hearing ... · SNHL is a multitfactorial process...

case report
Hematol Oncol Stem Cell Ther 4(2) Second Quarter 2011 hemoncstem.edmgr.com 97
Sickle cell disease (SCD) is a hemolytic anemia quite prevalent in Oman, with the most recent epidemiological data suggesting a sickle cell gene
carrier rate of about 6% and SCD prevalence of 0.2%.1,2 The disease is characterized by a change in the shape of red cells to the classical sickled shape leading to a process of vessel occlusion involving the smallt and mettdiumtsized vessels in almost all parts of the body. The process of vasotocclusion is made worse by episodes of infections, dehydration or deoxygenation.3
It is also known that patients with SCD are at an increased risk of thrombosis and this process is considttered to contribute to several clinical features of the disttease including leg ulcers, priapism, avascular necrosis of bone, pulmonary hypertension, acute chest syndrome, stroke, and apparently any random infarctive lesions that can occur anywhere in the body. The cochlea, the organ of hearing, is not immune from this process and audiometric assessment is a sensitive indicator of any sensorineural (perceptive) hearing loss resulting from any occlusive vascular involvement.4
The prevalence of involvement of the ears in SCD patttients is variable but it is reported to occur between 11% to 41% in black patients with this disease and can lead to sensorineural hearing loss (SNHL).5,6 The pattern of involvement is also variable and it can be either unilattteral, bilateral, temporary or permanent.7,8 We report on
Complete recovery following sudden sensorineural hearing loss in a patient with sickle cell diseaseSalam Alkindi, Najwa Arafa, M Al Okbi, Anil Pathare
from the Department of haematology, College of medicine and health sciences, sultan Qaboos university hospital, muscat, oman
Correspondence: Prof. salam alkindi · Department of haematology, College of medicine and health sciences, sultan Qaboos university hospital, Po Box 35, PC 123, al Khod, muscat, 000123 oman · t: +96899353188 f: +96824144887 · [email protected] · accepted: June 2011
hematol oncol stem Cell ther 2011; 4(2): 97-99
Doi: 10.5144/1658-3876.2011.97
a sickle cell disease (sCD) patient with vaso-occlusive crisis (VoC) developed sudden senserinural hear--ing loss (snhL), which responded well to a rapid course of corticosteroids along with exchange trans--fusions. the otolaryngologist should be aware of the otologic manifestations of sCD such as snhL. a good response to steroids, which averted a permanent hearing loss, warrants further studies to define the augmentive benefits of such therapy along with exchange transfusions in patients with sCD in VoC who develop sudden snhL.
a young female with a complicated history of SCD who presented with a sudden onset of sensorineural hearing loss (SNHL) that completely resolved following antettcedent medical therapy. We wish to highlight here the need for appropriate and rapid audiometric evaluation and followtup treatment so that a reversible and treatttable cause for rapid hearing loss in patients with SCD with VOC such as ours can be quickly achieved.
CASEA 26tyeartold Omani female with SCD (Hb S/S genotttype) was admitted in January 2010 with acute painful crisis involving the chest, legs and back. Her medical history was significant and included a stroke in childtthood with complete neurological recovery, protein C deficiency, acute chest syndrome, and iron overload due to repeated blood transfusions/exchange. She was taking hydroxyurea, desferoxamine, penicillin V, folic acid, cotcodamol, aspirin and enoxaparin. On admisttsion, she had stable vital signs with pallor and icterus. She was treated with hydration, pain management with morphine infusion and nontsteroidal antitinflammatttory drugs. Two days after admission, the patient awoke with acute complete hearing loss in the left ear. There was no history of imbalance or vertigo and she was otherwise well, apart from her ongoing painful crisis. Her hearing had previously been considered normal.

case report HEARING LOSS IN SICKLE CELL DISEASE
Hematol Oncol Stem Cell Ther 4(2) Second Quarter 2011 hemoncstem.edmgr.com98
Furthermore, clinical examination found no neurologittcal deficit. Investigations showed hemoglobin 7.5 g/dL, white blood cells 12.1×109/L, platelets 344×109/L, reticulocytes 538×109/L (25%), hemoglobin S 70.8%, hemoglobin F 1.0%, hemoglobin A 24.6% (transfused blood), hemoglobin A2 3.4%, lactate dehydrogenase 640 μ/L (normal range, 135t214), haptoglobin <0.06 g/L, total bilirubin 88 μmol/L, with otherwise normal renal and liver functions.
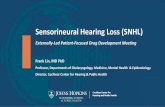
She was evaluated in the ENT department, and auttdiometry, middle ear compliance, acoustic reflex, and tone decay were ordered. Audiometry studies showed a profound hearing loss in the left ear and mild hearing loss in the right (Figure 1 top). Radiological evaluation showed a normal chest xtray, ultrasound of the abdottmen showed gallstones, magnetic resonance imaging with angiogram of the brain did not reveal any new neuttrological lesions except for a large frontal cystic encephttalomalacia due to an old infarction. She had extensive
investigations to look for an underlying pathology, inttcluding autoimmune work such as antinuclear antibodtties, autoantibody screen and antineutrophilic antibodtties and they were all negative. Polymerase chain reactttion (PCR) for CMV, hepatitis B, C and HIV were all negative, and rapid plasma reagin as well as Treponema pallidum hemagglutination were also negative. She was treated with exchange transfusions and started on oral steroids (prednisone 60 mg daily for a week), which was gradually reduced over two weeks. Additionally she rettceived beta histadine 16 mg three times daily, as well as exchange transfusions. Audiometry was done every three days and the patient discharged with normal heartting in both ears in 2 weeks (Figure 1 bottom).
DISCUSSIONNormal erythrocytes are compressible, disctshaped cells that flow easily through the smallest blood vesttsels, navigating blood vessels that are 1/3 of their diamtteter; these cells live about 120 days. In stark contrast, in SCD patients the abnormally sickletshaped red cells are rigid, and get stuck in small blood vessels, leading to the most frequent manifestations of this disease, namely vasocclusion. Moreover these red cells live for only 20 or fewer days, perpetuating the vicious cycle of increased red cell production followed by increased red cell destruction. The sickle cells interrupt blood flow by blocking small blood vessels especially in the capilttlarytvenous bed, where the partial pressure of oxygen is reduced, promoting and accelerating the sickle shape change. This morphological change, and its associated physiological change, drastically reduces the ability of red blood cell to navigate and deliver oxygen throughttout the body.9
SNHL is a multitfactorial process with idiopathic sudden SNHL being the most common diagnosis. The cochlea is highly sensitive to disruption of blood flow, and occlusion of labyrinthine vessels were shown in an animal model by Perlman to induce irreversible hearing loss.10 Ischemia of the stria vascularis, increased blood viscosity by crystallization of red blood cells, with dettvelopment of stasis, ischemia or hypoxia appears to be the outstanding pathophysiological phenomenon durtting crisis.11 Given its size, this tiny organ receives a disttproportionate percentage of the body’s blood and the extensive cochlear vascular anatomy, the high metabolic activity required to maintain both ionic and electrical characteristics of endolymph, and the highly dependent nature of evoked responses from the inner ear on brief episodes of anoxia, suggest that a secure and extensive cochlea blood flow is critical.12
Our patient presented with crisis due to SCD and
Figure 1. Pure tone audiogram before (top) and after (bottom) treatment.

case reportHEARING LOSS IN SICKLE CELL DISEASE
Hematol Oncol Stem Cell Ther 4(2) Second Quarter 2011 hemoncstem.edmgr.com 99
1. Al-Riyami AA, Suleiman AJ, Afifi M, Al-Lamki ZM, Daar S. A community–based study of common hereditary blood disorders in Oman. East Mediterr health J. 2001; 7(6): 1004-11.2. Alkindi S, Al Zadjali S, Al Madhani A, Daar S, Al Haddabi H, Al Abri Q, Gravell D, Berbar T, Pravin S, Pathare A, Krishnamoorthy R. Fore--casting hemoglobinopathy burden t h r o u g h neonatal screening in omani neonates. Hemoglo--bin. 2010;34(2):135-44.4. Todd GB, Serjeant GR, Larson MR. Sensori-neu--ral hearing loss in Jamaicans with SS disease. Acta Otolaryngol. 1973;76(4):268-725. Schiliro G, Samperi P, Testa R, Gupta RB, Gu
LH, Huisman TH. Clinical, hematological, and mo--lecular features in Sicilians with Hb S-beta- thalassemia. Am J Hematol. 1992;41(4):264-9.6. Piltcher O, Cigana L, Friedriech J, Ribeiro FA, da Costa SS. Sensorineural hearing loss among sickle cell disease patients from southern Brazil. Am J Otolaryngol. 2000;21(2):75-9.7. Schreibstein JM, Macdonald B, Cox C, Mcma--hon L, Bloom D, sudden hearing loss in sickle cell disease: a case report. Otolaryngol. Head neck Surg. 1997; 116(4): 541-4.8. O’Keeffe L, Sudden sensorineural hearing loss in sickle cell disease. J Laryngol Otol. 1993; 107(12): 1195.
9. Burch-Sims GP, Matlock VR. Hearing loss and auditory function in sickle cell disease. J Commun Disord. 2005;38(4):321-9.10. Perlman HB, Kimura R, experimental obstruc--tion of venous drainage and arterial supply of the inner ear. Ann Otol Rhinol Laryngol 1957; 66: 537-46.11. Diggs LW. The crisis in sickle cell anemia. American Journal of Clinical Pathology. 1956; 26: 1109–1118.12. Russell IJ, Cowley EM, the influence of tran--sient asphyxia on receptor potentials in inner hair cells of the guinea pig cochlea. Hearing research 1983, 11:373-384.
developed sudden hearing loss in all the frequencies of more than 30 dB of the left ear, strengthening the evidence that this process was related to SCD and she was treated with rapid exchange transfusions and stettroids. Interestingly, she presented with a number of confounding factors. She had a history of stroke, and although she had a normal hearing following the stroke, with no neurological deficit, it is conceivable that she was at a high risk of developing a vascular CNS event. Furthermore, she was intermittently on desferoxamine, an agent that is linked with auditory complications, alttthough usually this is only thought to occur at a lower ferritin level, and her current ferritin level was 2930 ng/mL (reference range, 20t300 ng/mL). This patient also had a complicated clinical course and presented with painful crisis, had a low hemoglobin level, with a
very high reticulocyte count (known for their adhesive properties) and high hemoglobin S level, all features supportive of aggravating a vasotocclusive process due to SCD. However, we had simultaneously investigattted her extensively to exclude other causes of sudden SNHL such as infection with negative viral studies, or no serological evidence of syphilis, and no evidence of autoimmune disease as documented by negative autottimmune markers. Furthermore this patient responded extremely well to steroids with rapid resolution of her symptoms and the hence the rare possibility of an autttoimmune process cannot be completely ruled out. A rapid short course of steroid can be recommended in such cases, unless there is an absolute contraindication to their use, as the consequences of permanent hearing loss are profound.
REFERENCES