Compartment Syndrome - ISPANispan.org/convention/files/2017/Presentations/Sunday/0500-Vaz.pdf ·...
34
Compartment Syndrome The Sneaky Emergency Maegan Vaz October 8, 2017
Transcript of Compartment Syndrome - ISPANispan.org/convention/files/2017/Presentations/Sunday/0500-Vaz.pdf ·...

Compartment
Syndrome
The Sneaky Emergency
Maegan Vaz
October 8, 2017

Case Study
• 36 yr old male
• Obese
• POD 1 s/p L
mandibulectomy, L neck
dissection with R fibula
reconstruction
• 10 hour long supine position
• Intubated in PACU overnight
(12 hours)
• PCA for pain
• Complaints
• Extreme R buttock pain –
exquisitely tender to
touch
• Erythema localized to
right buttock
• Swollen R buttock

What is compartment
syndrome?
A condition in which
increased compartment
pressure within a
confined space,
compromises the
circulation and viability
of the tissues within that
space
https://syndromespedia.com/wp-content/uploads/2012/06/Anterior-Compartment-Syndrome.jpg

First Documentation
The first medical reference
was in 1881, when German
doctor Richard von
Volkmann described a
permanent contracture of
the forearm related to
ischemia within muscle
compartments of the arm
https://en.wikipedia.org/wiki/Volkmann%27s_contracture

Anatomy Review
• Compartments –
grouping of muscles,
nerves and blood
vessels in the
extremities
• Inelastic fascia encases
the compartments,
protects the tissues, and
maintains tissue shape
Colton, C. (2012). Compartment Syndrome. [Digital Image]
Retrieved from : https://www2.aofoundation.org

Lower Extremity
Compartments - Calf
Figure 1. Cross-section Medial Calf. Adapted from “Grey’s Anatomy,”
2009. Retrieved from : https://radiopaedia.org/images/24012
• Anterior
• MOST likely to be affected
• Tibialis anterior, extensor muscles of toes, anterior tibial artery, and deep peroneal nerve
• Lateral
• Peroneus longus and peroneus brevis, superficial peroneal artery
• Deep Posterior
• Tibialis posterior, flexor digitorum longus, and flexor hallus longus
•Superficial Posterior• Gastrocnemius and soleus muscle.
Sural nerve• Lithotomy positions

Calf Cross - Section
Von Keudall, Arvind G et al. (September, 2015). Diagnosis and Treatment of
Acute Extremity Compartment Syndrome. The Lancet, Volume 386, Issue 100000,
pg 1299-1320. dio: http://dx.doi.org/10.1016/S0140-6736(15) 00277-9

Lower Extremity
Compartments – Thigh • Anterior
• Vastus lateralis, vastus intermedius, srtorius, and recutus femoris
• Femoral nerve/artery
• Medial
• Pectineus, external obturator, gracilis muscles
• Adductors
• Obturator nerve
• Posterior
• Semimembranous, semitendinosis, and biceps femoris
• Sciatic nerve Figure 2. Cross-section Medial Calf. Adapted from
“Grey’s Anatomy,” 2009. Retrieved from :
https://radiopaedia.org/images/24012
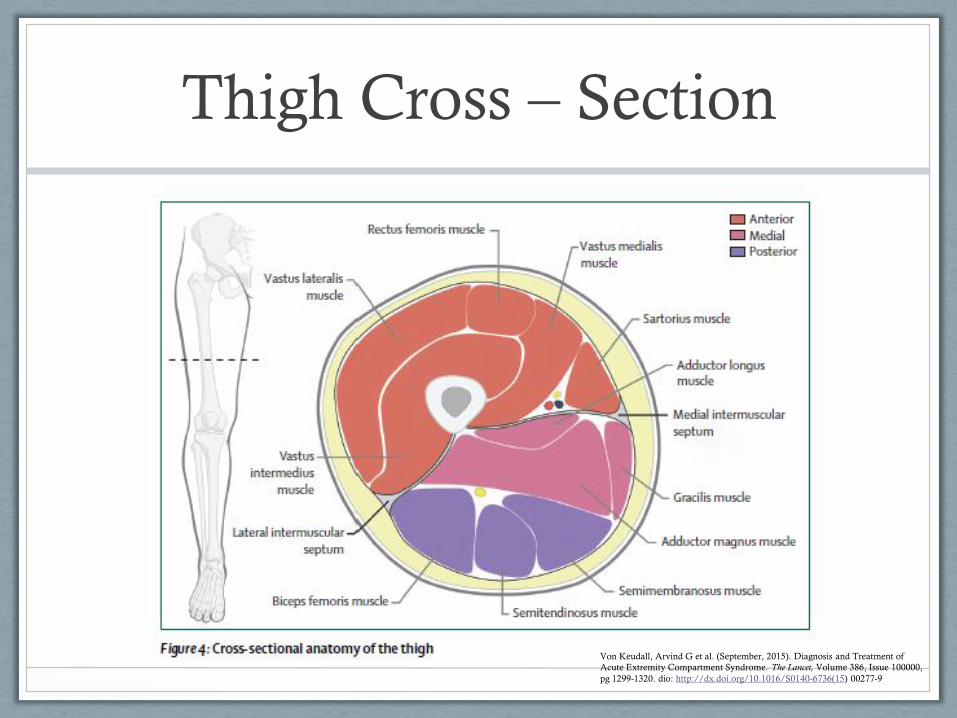
Thigh Cross – Section
Von Keudall, Arvind G et al. (September, 2015). Diagnosis and Treatment of
Acute Extremity Compartment Syndrome. The Lancet, Volume 386, Issue 100000,
pg 1299-1320. dio: http://dx.doi.org/10.1016/S0140-6736(15) 00277-9

Physical Assessment
• Lower Extremity - Calf
• Deep Peroneal Nerve (most commonly affected) - anterior compartment.
• Sensory territory is confined to webspace between 1st and 2nd toes and activates dorsiflexion
• Superficial Peroneal Nerve runs along lateral compartment and supplies dorsum of the foot (except 1st webspace)
• Posterior Tibial Nerve is within deep posterior compartment and provides sensation to plantar surface of the foot – motor function is flexion of the toes
McKnight, J. & Adcock, B. (December 1997). Paresthesias: A Diagnostic
Approach. American Family Physician. Volume 56, Issue 9, pg 2253-2260.

Physical Assessment
• Lower Extremity - Thigh
• Femoral Nerve
• Anterior Compartment
• Most commonly affected
• Obturator Nerve
• Medial Compartment of
thigh
• Sciatic Nerve
• Posterior Compartment of
thigh
McKnight, J. & Adcock, B. (December 1997). Paresthesias: A Diagnostic
Approach. American Family Physician. Volume 56, Issue 9, pg 2253-2260.
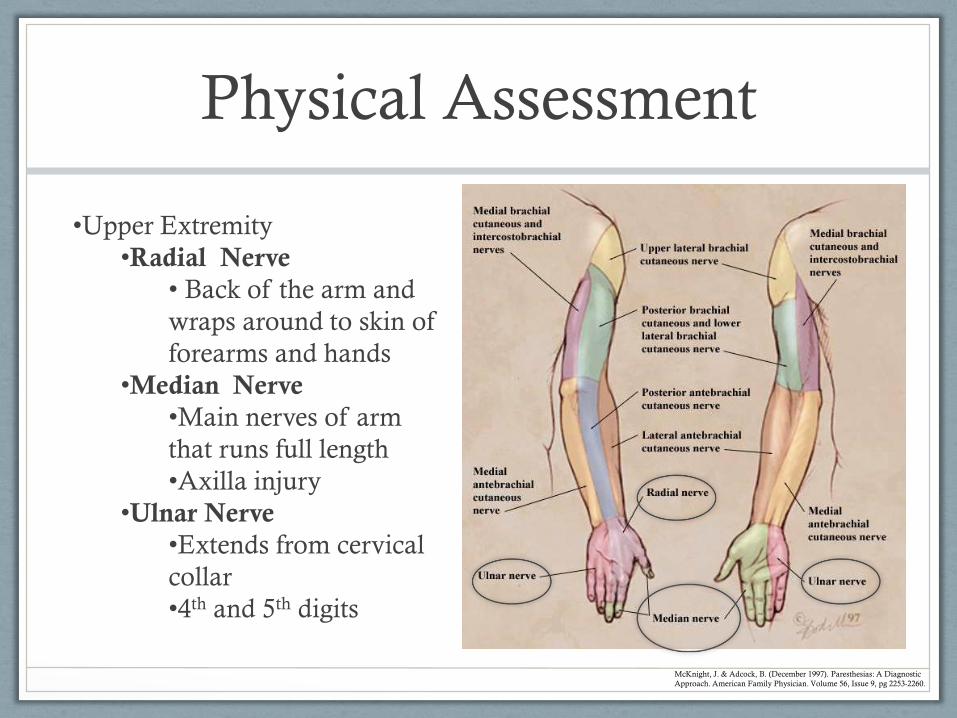
Physical Assessment
•Upper Extremity
•Radial Nerve
• Back of the arm and
wraps around to skin of
forearms and hands
•Median Nerve
•Main nerves of arm
that runs full length
•Axilla injury
•Ulnar Nerve
•Extends from cervical
collar
•4th and 5th digits
McKnight, J. & Adcock, B. (December 1997). Paresthesias: A Diagnostic
Approach. American Family Physician. Volume 56, Issue 9, pg 2253-2260.
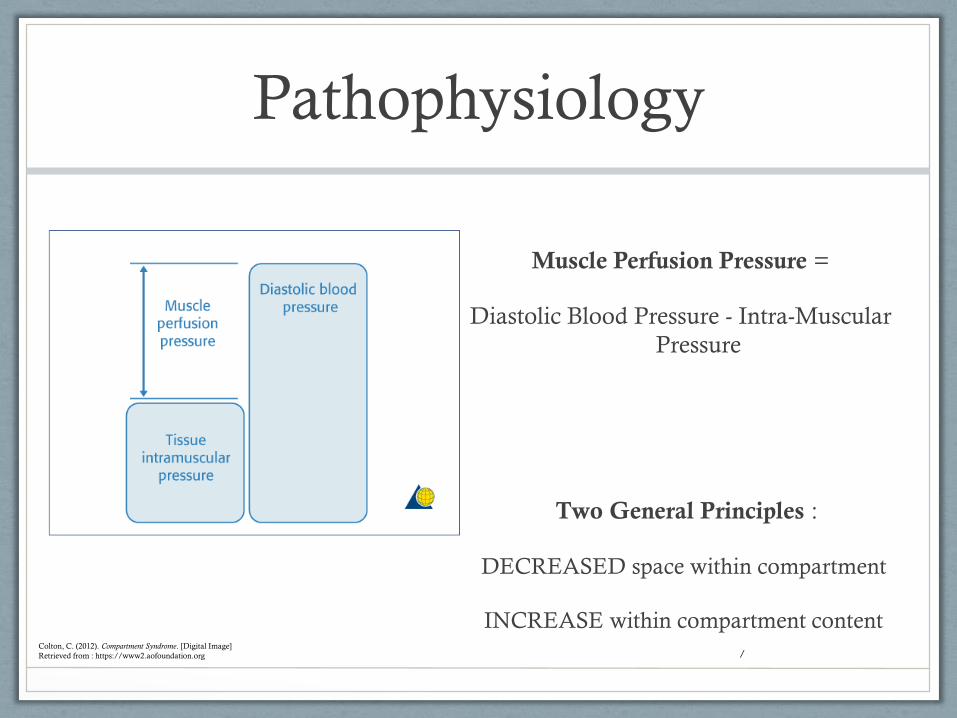
Pathophysiology
/
Muscle Perfusion Pressure =
Diastolic Blood Pressure - Intra-Muscular
Pressure
Two General Principles :
DECREASED space within compartment
INCREASE within compartment contentColton, C. (2012). Compartment Syndrome. [Digital Image]
Retrieved from : https://www2.aofoundation.org


Venous Outflow Obstruction
Pathophysiology
Decreased Arterial Perfusion
Multiple pathways leading to final
common pathway: cellular anoxia
death of the muscle within compartment.
Compartment Pressure
Increased Capillary
Permeability
Increased Intracompartmental
Pressure
ISCHEMIA

Causes of ACS
• Bone fracture (trauma or intentional) ~70%
• Crush Injury
• Hemorrhage (anticoagulation, intramuscular injury)
• Less common causes… r/t fluid retention –rhabdomyolysis, muscle hypertrophy, DVT
• Tight casts/splints/circumferential dressings/tourniquet
• Burns
• Injection injury/Extravasation
• Intra-osseous infusions
• Infection
• Surgical positioning
Any event (external or internal) that increases the
pressure within a compartment by decreasing the
capacity or increasing the volume

Clinical Presentation
Pain
6 P’s
Pallor
Pressure
Paresthesia Paralysis
Pulselessness

PAIN
• Pain that is out of proportion
to the injury
• Pain with passive stretch of
muscle
• Persistent deep ache or
burning
FIRST presenting symptom

PRESSURE
• Often not utilized – proper equipment required
and user errors are common
• >30-40 mmHg considered diagnostic

PARESTHESIA
• A condition in which you feel sensation of numbness or prickling
• Pins & Needles
• Early contained to one compartment
• Late globally within limb

PALLOR
• Rarely present
• Often times, redness
progresses to pallor
• Sign of vascular
injury and quickly
leads to ischemia
• LATE stage –
emergent
intervention require

PULSELESSNESS
• The existence of distal
pulses DO NOT exclude
compartment syndrome
• Check above and below
area of concern
• Late stage – indicates
progression
https://upload.wikimedia.org/wikipedia/commons/thumb/
d/d1/Pulse_sites-en.svg/220px-Pulse_sites-en.svg.png

PARALYSIS
• Complete loss of muscle function for one or more
muscle groups
• Very late finding indicating nerve damage
http://drawingbooks.org/lutz1/source/images/000088.png

Who is at risk?
Increased
Muscle Mass
Bone Fracture (2/3 of
patients)
Tibia/radius most
commonly seen
Trauma
Cast/Splint on
broken bone
OR - same
position for >
8 hrs
Lithotomy
Men in their
30’s

Diagnosis
Difficult to DEFINATIVELY diagnose early on
Late stage:
• Hyperkalemia from
muscle breakdown
• Acute renal failure or
myoglobinuria
Early Stage:
• Extreme, unrelenting
pain
• Elevated
intracompartmental
pressure

Diagnosis
Stryker Manometer is most commonly used
• Normal at rest 0 - 10 mmHg
• Pressures > 30-40mmHg require surgical decompression, combined with supporting clinical picture
https://www.slideshare.net/drrohitvikas/compartment-syndrome-14077010

Support Your Case
• What are the precipitating factors?
• Is this a high risk patient?
• Imaging
• MRI/CT scan can show swelling of the gluteal muscles
• Can use measure the pressure within the compartment?• Is it >30 – 40
mmHg?
• Additional helpful objective information • Elevated creatinine
phosphokinase (CPK) indicates muscle damage or ischemia

Treatment
• Surgical
decompression with a
fasciotomy is the
definitive treatment
• 8 hour ischemia time
can cause irreversible
damage to muscles
Nucleus Medical Media Inc / Alamy Stock Photo

Case Study – Review the Facts
• Age – young males at high risk
• Obese – muscular patients are often at higher risk,
but could weight and gravity play a factor?
• Time – OR for 10 hours, supine and intubated for at
least another 12 hours – unable to communicate
pain.
• Pain – Very tender. Exquisitely tender to touch. Is
there pain when flexing the hip?

Case Study #2
• 26 y/o athletic male with no prior medical history
• Playing soccer on day prior to admission was kicked in R thigh sustaining a hairline femur fracture
• Admitted for observation
• Ambulated w/pain into urgent care
• Denied numbness/tingling
• Labs on admission :
CPK 971 (22-198) K 5WBC 12.8 H&H 12.5/35.5 PLTs 213
Compartment pressure 45mmHg.

Fasciotomy
Incision prior
to fasciotomy
Fasciotomy in progress –
muscle is still beefy red
and viable

Prognosis
• Overall complication rate is about 50-60% if
treatment is delayed >12
• About 50% lower limbs require amputation when
treatment is delayed, 92% will develop neuropathy
• Mortality is related to renal failure or sepsis

Things to Remember
• Don’t dismiss pain – look
into the reason for the pain
• Don’t over medicate
• Perform a COMPLETE
exam
• Don’t elevate – need to
maintain perfusion
• TRUST YOUR GUT

References
Colton, C. (2012). Compartment Syndrome. [Digital Image] Retrieved from : https://www2.aofoundation.org
Donaldson, J., Haddad, B., & Khan, W. (June 27, 2014). The Pathophysiology, Diagnosis and Current Management of Acute
Compartment Syndrome. The Open Orthapaedics Journal. Volume 8, pg 185-193. doi: 10.2174/187432500140801085
Kam, J.L., Hu, M., Peiler, L.L., & Yamamoto, L.G. (July, 2003). Acute Compartment Syndrome Signs and Symptoms Described in
Medical Textbooks. Hawaii Medical Journal. Retrieved from http://evols.library.manoa.hawaii.edu/bitstream/10524/53621/1/2003-
07p142-144.pdf
Kostler, W., Strohm, P.C., & Sudkamp, N.P. (August, 2005) Acute Compartment Syndrome of the Limb. Injury. Volume 36 Issue 8,
pg 992-998. Retrieved from http://doi.org/10.1016/j.injury.2005.01.007
McKnight, J. & Adcock, B. (December 1997). Paresthesias: A Diagnostic Approach. American Family Physician. Volume 56, Issue
9, pg 2253-2260.
Stracciolini, A., & Hammerberg, M. (May 13, 2016). Acute Compartment Syndrome of the Extremities. UpToDate. Retrieved
from https://www.uptodate.com/contents/acute-compartment-syndrome-of-the-extremities
Ulmer, Todd. (September 2002). The Clinica Diagnosis of Compartment Syndrome of the Lower Leg: Are Clinical Findings
Predictive of the Disorder? Journal of Orthopaedic Trauma. Volume 16, Issue 7 & pp 572-577. Retrieved from
http://journals.lww.com/jorthotrauma/Abstract/2002/09000/The_Clinical_Diagnosis_of_Compartment_Syndrome_of.6.aspx
Von Keudall, Arvind G et al. (September, 2015). Diagnosis and Treatment of Acute Extremity Compartment Syndrome. The Lancet,
Volume 386, Issue 100000, pg 1299-1320. dio: http://dx.doi.org/10.1016/S0140-6736(15) 00277-9