Compartment syndrome
43
DR REMYA R KRISHNAN RESIDENT INTERN AZEEZIA MEDICAL COLLEGE
-
Upload
remya-radhakrishnan -
Category
Health & Medicine
-
view
36 -
download
1
Transcript of Compartment syndrome

DR REMYA R KRISHNAN RESIDENT INTERN AZEEZIA MEDICAL COLLEGE

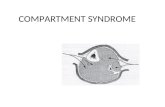
DefinitionAn elevation of the intercompartment
pressure to a level & duration without decompression will results in tissue ischemia and necrosis.
Occurs in closed osteofascial compartment Causes microvascular compromise

Types of compartment syndromeAcute compartment syndrome (ACS)
medical emergencycaused by a severe injurycan lead to permanent muscle damage.
Chronic compartment syndrome (CCS) known as exertional compartment syndrome not a medical emergencymost often caused by athletic exertion.

Pathophysiology

Pathophysiology The vicious cycle of Volkmann's
ischemia Increased intracompartmental Pressure increases local venous Pressure narrowed AV perfusion gradient compartment tamponadedecrease capillary blood flow O2 deprivation local tissue necrosis nerve injury and muscle ischemia

TheoriesCritical closing pressure theoryArteriovenous gradient theoryMacrovascular occlusion thoery

Etiology of ACSDECREASED COMPARTMENT SIZEINCREASED COMPARTMENT PRESSURE
7

Etiology of ACS Decrease compartment size Tight dressings/closure of fascial
defect External pressures : casts, splints ,
burn eschar, lying on limb for long period, lithotomy position

Etiology Increased compartment contentsSNAKE BITEIATROGENIC CAUSESFractures : the most common are
Tibial diaphysealDistal radial and forearm diaphyseal

Etiology Increased compartment contents• Hemorrhage -- vascular injury, coagulopathy• Muscle edema -- severe exercise , crush injury• Increase capillary permeability–
burn,orthopaedic surgeries• Soft tissue injury• Metabolic diseases– diabetes, hypertension

Increased compartment contents

Clinical features
Swelling/ Tightness of compartmentInappropiate and uncontrolled painStretch pain & rest painPallorPulselessnessParesthesiaParalysis (full recovery is rare)

In children :3 AANXIETYAGITATIONINCREASED REQUIREMENT OF
ANALGESICS
13

Whiteside' Theory:The development of a compartment syndrome also depends on
MPP = DBP(Diastolic BP) – CP(Intracompartment P)
Muscle perfusion pressure(MPP) < 30 mmHg
Tissue hypoxia
Measurement of Compartment pressures


Devices
Stryker hand-held system Stryker slit catheter
Newer devices

ManagementRemove cast/bandagePositioning of the limb at the level of the
heart - Do not elevate the affected limb decreases arterial pressure IV hydrationOxygen supplement


TreatmentOperative
Emergency fasciotomyPositive clinical presentation pressure = 30-45 mm Hg
Contraindications : Missed compartment syndrome (Various stage of muscle
infarction)

TypesForearm Syndromes
Deep forearm SyndromeCompresion ischemia
Anterior tibial SyndromeDeep posterior tibial SyndromePeroneal Compartment SyndromeSuperficial posttibial compartment Syndrome

Types by location2 compartments of arm4compatments of forearm10 compartments of hand3 compartments of thigh4 compartments of leg9compartments of foot

2 Compartments of arm1.Anterior
1. Biceps,Bracialis
2.Musculocutaneous n.
3.Brachial a.2.Posterior
1. Triceps2. Radial n.

4 Compartments of forearm1. Mobile wad : Brachioradialis, Radial n
2,3. Dorsal superficial&deep :Posterior intero-seous n & a
4. Volar superficial&deep :Median and Ulnar n. Radial a., Ulnar a., ant. interosseous a.
-most commonly affect volar
Dorsal incision

10 Compartments of hand

3 Compartments of thighAnterior
femoral nquadriceps sartorious
Posterior sciatic nhamstrings
Medialobturator nadductors


4 Compartments of leg1. Anterior : Tibialis anterior, EDL,EHLPeroneus2. Posterior-Superficial : Gastrocnemius, soleus, plantaris3. Posterior-Deep: FDL, FHL,Popliteus,Tibialis posterior, Tibial a,v,n.4. Lateral: Peroneus longus and brevis,peroneal n



9 Compartments of foot

Dorsal dual incision
Medial incision

ComplicationsMyonecrosis : after an ischemic insult of > 8 hrs.Treatment
fasciotomy + debridement of the muscles + neurolysis Volkmann ischemic contracture : myonecrosis
replaced with fibrous tissue myotendinous adhesion formation.
TreatmentNon-surgical (physiotherapy & bracing involve the
joints)Surgical
contracture release, nerve compression release,

Reperfusion syndrome : group of complications following reestablished blood flow to ischemic tissues
Occur after fasciotomy & restoration of blood flow
Evaluation : Fluid loss, Shock Acidosis Hyperkalemia Myoglobinuria, Renal failure
Management : Preoperative hydration Mannitol Bicarbonate
Complications

Complications Neurovascular injuryInfection

Chronic Compartment Syndrome
Known as exertional CS, recurrent CS or subacute CS
Typical patient is young (20-30s) athlete (long distance runner)or military recruits
Occur mainly in the lower limb

Pathophysiology
Not yet fully understoodProbably from increased muscle relaxation
pressure during exercise decreased muscle blood flow ischemic pain and impaired muscle
function

Recurrent pain Temporary paraesthesia & numbnessLimitation of movementsTenderness over the compartmentMuscle hernias seenBilateral involvement is common
Clinical features

PeriostitisEntrapment of the superficial peroneal
nerveTendinitis of the posterior tibial tendonStress fracture of tibiaIntermittent claudication
Differential diagnosis

Plain x-rays : show stress fractureTinel test : may be positive in superficial
peroneal nerve entrapmentNerve Conduction StudyMRI
Investigations

Treatment
Non-operative : NSAIDs Muscle relaxantsCessation or significant reduction of athletic
activities

Treatment Operative treatment
Single incision fasciotomy Double incision fasciotomy
After surgery :Physiotherapy is a must

Compartment syndrome is a serious syndrome, Which needs to be diagnosed early.Palpable pulse doesn’t exclude compartment syndromeIf diagnosis and fasciotomy were done within 24 hrs, the prognosis is good.If delayed, complications will develop.
The earlier you diagnose, the safer you are

THANK YOU