Compartment Syndrome
44
COMPARTMENT SYNDROME By; Sridevi Rajeeve Intern 2008 Batch 06/26/2022 1 sridevirajeeve_august2014_ortho
-
Upload
sridevi-rajeeve -
Category
Health & Medicine
-
view
435 -
download
3
description
Compartment Syndrome presented in a compact and easy manner with pictorial accompaniments.
Transcript of Compartment Syndrome

04/12/2023 sridevirajeeve_august2014_ortho 1
COMPARTMENT SYNDROME
By;
Sridevi RajeeveIntern
2008 Batch

04/12/2023 sridevirajeeve_august2014_ortho 2
DEFINITION Compartment syndrome is defined as the
elevated interstitial tissue pressure within a confined space in the body (an osseo-fascial compartment) leading to inadequate tissue perfusion and eventually leading to tissue necrosis within the compartment
True Orthopaedic Emergency!

04/12/2023 sridevirajeeve_august2014_ortho 3
ANATOMIC CONSIDERATIONS May occur in varied locations where closed
compartments exist in the bodyLeg (most common)Forearm (classic)ArmThighFootHandButtockAbdomen

04/12/2023 sridevirajeeve_august2014_ortho 4
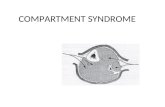
Classic location - Flexor compartment of the Forearm This location has several unique anatomic features that predispose CS
Strong fascial roof and at its entrance lie two potential obstructions○ First and lying most superficialis the lacertous fibrous fascia, which
fans medially from the biceps tendon as the latter inserts on the proximal radius.
○ The second is the bulky pronator teres muscle, which arises from the medial epicondyle and passes obliquely beneath the inelastic lacertous fibrosus to create a V-shaped sphincter beneath which the brachial artery and the median nerve must pass to enter the flexor compartment.
○ Collateral vessels serving the flexor compartment are minimal Oedema, haematoma or intramuscular haemorrhage in this crucial region
may cause sufficient compression of these neurovascular structures to precipitate the ischaemia–oedema vicious cycle.

04/12/2023 sridevirajeeve_august2014_ortho 5

04/12/2023 sridevirajeeve_august2014_ortho 6

04/12/2023 sridevirajeeve_august2014_ortho 7
AETIOLOGY1. ACUTE COMPARTMENT SYNDROME
(1) Increased Compartment Volume Fracture
○ Supracondylar humerus○ Forearm bones○ Distal radius○ Tibia
Soft-tissue injury○ Crush syndrome○ Severe contusion○ Muscle tear○ Gunshot wounds
Iatrogenic ○ Postoperative inflammation ○ Fracture fixation with oversize implants
Exertion (intensive muscle use)

04/12/2023 sridevirajeeve_august2014_ortho 8
• Tetany• Eclampsia• Seizures• Bleeding• Bleeding or coagulation disorder (e.g. haemophilia)• Anticoagulant therapy• Postoperative vascular injury• Traumatic rupture of vascular malformation• Fluid extravasations into soft tissues• Ruptured cysts/ganglia• During arthroscopy with fluid extravasation• Infection (acute haematogenous osteomyelitis)• Increased capillary permeability or pressure• Venous obstruction/ligation• After prolonged ischaemia/tourniquet• Arterial bypass grafting• Ergotamine ingestion• Thermal injury• Electrical injury• Frostbite• Snakebite• Intra-arterial drug injection
Most common – FRACTURE!Tibial Diaphyseal >Radial Shaft >Supracondylar

04/12/2023 sridevirajeeve_august2014_ortho 9
(2) Decreased Compartmental Volume
Tight casts/splints Prolonged limb pressure
Lengthy surgeries Anaesthesia Comatose patient
Excessive traction on fractured limb

04/12/2023 sridevirajeeve_august2014_ortho 10
PATHOPHYSIOLOGY Classical aetiopathogenesis: increased ICP in the
interstitium over itscapillary perfusion pressure, due to the accumulation of necrotic debris and/or haemorrhage, contents within the closed compartment of the deep fascia swell, raising the ICP to such a high level that blood cannot circulate in this closed compartment
Contents undergo varied degrees of necrosis and eventually fibrosis

04/12/2023 sridevirajeeve_august2014_ortho 11
THE VICIOUS CYCLE – OF DOOM?!

04/12/2023 sridevirajeeve_august2014_ortho 12

04/12/2023 sridevirajeeve_august2014_ortho 13
Normal resting intramuscular pressure is usually less than 6 mmHg
In compartment syndrome, the intramuscular pressure can increase to more than 100 mmHg The initial insult causes haemorrhage, oedema or
both in the closed fascial compartments of the extremities.
Rising compartment pressure ultimately leads to compartmental tamponade, microcirculatory impairment and sustained ischaemia

04/12/2023 sridevirajeeve_august2014_ortho 14
Compartmental pressures more than 30 mmHg maintained for more than 8 hours can cause irreversible muscle damage
Type 1 aerobic fibres (red/slow-twitch fibres), are more vulnerable to ischaemia than type 2 anaerobic fibres (white/fast-twitch fibres). That explains why some muscle groups are more vulnerable to ischaemic damage than others
Reduces the healing capacity of long bones, by possibly reducing the extra-osseous blood supply and Non-union can be a possible complication

04/12/2023 sridevirajeeve_august2014_ortho 15

04/12/2023 sridevirajeeve_august2014_ortho 16
DIAGNOSIS Medical/Orthopaedic emergency Any delay in its diagnosis is the single most
important cause of morbidity with potential to cause disastrous consequences including Amputation and even Death
Diagnosis of acute compartment syndrome is made clinically
Confirmed by actual measurement of compartmental tissue fluid pressure
A high index of suspicion is important to make a diagnosis!

04/12/2023 sridevirajeeve_august2014_ortho 17
CLINICAL DIAGNOSIS Classically, there are 6 "Ps" associated with
compartment syndromePain (out of proportion to what is expected based on
the physical exam findings)Paraesthesia Pallor Paresis/Paralysis Pulselessness Poikilothermia
The first signs of compartment syndrome are numbness, tingling and paresthesia

04/12/2023 sridevirajeeve_august2014_ortho 18
Reliability? Pain itself is an unreliable and variable indicator Pain if used as a diagnostic indicator of acute
compartment syndrome has a high proportion of missed or false negative cases
It cannot be elicited in unconscious patients and is an unreliable indicator in small children
Pain on passively stretching the muscles of the affected compartment (e.g. passively extending the fingers in acute compartment syndrome affecting the volar compartment of the forearm) is a recognized symptom

04/12/2023 sridevirajeeve_august2014_ortho 19
Palpable tenseness of the swollen affected compartment is often the earliest sign and palpating reproduces the patient’s pain
The compartment may feel very hard depending on the ICP and the overlying skin often appears shiny
Peripheral pulses are almost always present in acute compartment syndrome, unless the injury involves damage to vessels
Thus, if pulses are present, it does not exclude the diagnosis of compartment syndrome!

04/12/2023 sridevirajeeve_august2014_ortho 20
INTRACOMPARTMENTAL PRESSURE MEASUREMENT AND MONITORING CS is confirmed by measuring the ICP Most important investigation in ACS Several methods are available to measure the ICP:
1. Needle Manometer Method2. Wick Or Slit Catheter Technique3. Continuous Monitoring Infusion Technique4. Hand-held Transducers (Stryker Intra-compartmental
Pressure System)5. Near-infrared spectroscopy (NIRS)6. Pressure transducer modules (with a simple intravenous
catheter and needle) that are attached to most modern anaesthetic machines

04/12/2023 sridevirajeeve_august2014_ortho 21
ADJUNCT DIAGNOSTICS Radiographs
These are required to investigate for possible underlying fractures and fracture dislocation, their reduction and possible radio-opaque foreign bodies
Doppler flowmetry and arteriographyDoppler flowmetry and arteriography are valuable
in verifying a suspected arterial injury, but not for diagnosis of acute compartment syndrome. These investigations should not delay fasciotomy.

04/12/2023 sridevirajeeve_august2014_ortho 22

04/12/2023 sridevirajeeve_august2014_ortho 23
DELAYED DIAGNOSIS! Patients prone to delay in diagnosis of
compartment syndromeHead injuryCerebrovascular accidentSpinal cord injuryPeripheral nerve injuryAnaesthetized patients (general/local)Alcoholic/drug-overdosed patientsMentally disabled patientsBurn patientsInfants/young patients

04/12/2023 sridevirajeeve_august2014_ortho 24
MANAGEMENT
Goals for the management of acute compartment syndrome are to restore tissue perfusion to the affected
muscles and nerves of the compartment affected, to prevent or minimize the injury
to avoid any residual loss of function Treatment may be Non-operative for
Impending Compartment Syndrome Surgical for Established Compartment
Syndrome

04/12/2023 sridevirajeeve_august2014_ortho 25
NON-OPERATIVE MANAGEMENT Ensure patient is normotensive, as hypotension
reduces prefusion pressure and facilitates further tissue injury
Remove cicumferential bandages and cast. Alternative methods of immobilization or fixation should be chosen if necessary to maintain fracture reduction
Maintain the limb at level of the heart as elevation reduces the arterial inflow and the arterio-venous pressure gradient on which perfusion depends
Supplemental oxygen administration

04/12/2023 sridevirajeeve_august2014_ortho 26
Borderline symptomatic patients may be monitored with an indwelling catheter
Persistently borderline or doubtful patients should preferably have a fasciotomy rather than delay treatment
Fasciotomy: Prophylactic release of pressure before permanent damage occurs. Will not reverse injury from trauma

04/12/2023 sridevirajeeve_august2014_ortho 27
OPERATIVE MANAGEMENT
GOLD STANDARD: FASCIOTOMY! Open and extensive fasciotomies of all the
compartments within the part of the limb affected by CS

04/12/2023 sridevirajeeve_august2014_ortho 28
FASCIOTOMY INDICATIONS
Unequivocal clinical findingsPressure within 15-20 mmHg of DBPRising tissue pressureSignificant tissue injury or high risk pt > 6 hours of
total limb ischemiaInjury known for high risk of compartment syndromeAbsolute: >30-35mmHg with positive clinical
correlation CONTRA-INDICATION
Missed compartment syndrome (>24-48 hrs)

04/12/2023 sridevirajeeve_august2014_ortho 29
FASCIOTOMY
PrinciplesMake early diagnosisLong extensile incisionsRelease all fascial compartmentsPreserve neurovascular structuresDebride necrotic tissuesCoverage within 7-10 days

04/12/2023 sridevirajeeve_august2014_ortho 30
FASCIOTOMY
Fasciotomy not only relieves compartmental pressure, but also helps in re-establishing tissue perfusion if done timely enough and if there is no arterial injury or compromise

04/12/2023 sridevirajeeve_august2014_ortho 31
Legall four compartments must be decompressed, usually
via two long, longitudinal incisions. It will be necessary to debride necrotic tissue,
sometimes several times. Forearm
The three compartments (the mobile wad of three, the volar and extensor) can be released via two incisions (one curvilinear volar incision across the elbow and straight to the wrist to include releasing the carpal tunnel and one straight incision along the extensor ulna border)
HandHas 10 compartments(requiring five incisions) Similarly, the foot

04/12/2023 sridevirajeeve_august2014_ortho 32

04/12/2023 sridevirajeeve_august2014_ortho 33

04/12/2023 sridevirajeeve_august2014_ortho 34

04/12/2023 sridevirajeeve_august2014_ortho 35
POST-FASCIOTOMY CARE Wound Management after Fasciotomy
a bulky compression dressing and a splint are applied.
VAC (Vacuum Assisted Closure) can be usedFoot should be placed in neutral to prevent
equinus contractureWound is not closed at initial surgeryIncision for the fasciotomy usually can be closed
after 3 - 5 days

04/12/2023 sridevirajeeve_august2014_ortho 36
COMPLICATIONS RELATED TO FASCIOTOMIES Altered sensation within the margins of the wound
(77%) Dry, scaly skin (40%) Pruritus (33%) Discolored wounds (30%) Swollen limbs (25%) Tethered scars (26%) Recurrent ulceration (13%) Muscle herniation (13%) Pain related to the wound (10%) Tethered tendons (7%)

04/12/2023 sridevirajeeve_august2014_ortho 37
COMPLICATIONS OF COMPARTMENT SYNDROME
Volkmann’s contracture Weak dorsiflexors Claw toes Sensory loss Chronic pain Amputation Rhabdomyolysis Renal failure

04/12/2023 sridevirajeeve_august2014_ortho 38
CHRONIC COMPARTMENT SYNDROME
Chronic Compartment Syndrome usually occurs in young active patients afterintense muscular activity
Usually detected in the anterior compartment (anterior or posterior deep compartment)
Main symptoms involve pain, parasthesia of the musclewithin the affected compartment, after intense and continuing (over than 20-30 min) streching of musclegroups.
The symptoms recess progressively by interrupting any kind of exercise (15-20min)
Differential diagnosis include stress fracture, superficialfibular nerve entrapment syndrome, posterior tibialmuscle tendonitis.

04/12/2023 sridevirajeeve_august2014_ortho 39

04/12/2023 sridevirajeeve_august2014_ortho 40
Conservative treatment includes rest, anti-inflammatories, and manual decompression
Ideally, the affected limb should be positioned at the level of the heart
Patient adviced to decrease the level of activity
No relief forthcoming – Surgical Decompression

04/12/2023 sridevirajeeve_august2014_ortho 41
VOLKMANN’S ISCHEMIC CONTRACTURE Severe manifestation of Compartment
syndrome of Forearm Permanent flexion-contracture deformity of
hand at wrist and fingers Most affected muscles: Flexor digitorum
profundus and Flexor pollicis longus Classical claw-hand deformity

04/12/2023 sridevirajeeve_august2014_ortho 42
Volkmann’s Sign: in established VIC Extension of wrist produces exaggeration
of flexion deformity while on flexion, the deformities are less marked
Extensive scarring of forearm + Thin and fibrotic forearm Joint and soft tissue contractures Neurological deficits Gangrene (rare)

04/12/2023 sridevirajeeve_august2014_ortho 43
Treatment plan Moderate VIC
MAX-PAGE’S MUSCLE SLIDING OPERATION: releasing common flexor origin from medial epicondyle and passivele stretching fingers
CICATRIX EXCISION NEUROLYSIS TENDON TRANSFERS
Severe VIC CICATRIX EXCISION SEDDON’S CARPECTOMY: excising proximal row of carpal bones
to shorten forearm to overcome the effects of contacted muscles ARTHRODESIS of wrist in functional position AMPUTATION

04/12/2023 sridevirajeeve_august2014_ortho 44
THANK YOU!