Comparison of results of percutaneous transluminal coronary angioplasty with and without selective...
5
Comparison of Results of Percutaneous Transluminal Coronary Angioplasty With and Without Selective Requirement of Surgical Standby Andrbs Ihguez, MD, Carlos Macaya, MD, Rosana Hernandez, MD, Fernando Alfonso, MD, Javier Goicolea, MD, Jorge Casado, MD, and Pedro Zarco, MD To determine the outcome of percutaneous trans- luminal coronary angioplasty (PTCA) with the use of 2 different strategies of surgical coverage, the resutts of 1,283 consecutive PTCAs were ana- lyzed. In 269 procedures (21%) (patients consid- ered at high risk should acute vessel closure oc- cur - standby group) the operating room and the surgical team were ready for an immediate inter- vention. In the remaining 1,014 procedures (79%) (backup group), although the surgical team was “in house,” they were not necessarily ready for an immediate intervention. Mean age of the popula- tion was 56 f 10 years and 64% of patients were men. Coronary risk factors, medical treatment, clinical indication for PTCA, previous coronary surgery and left ventricular ejection fraction were similar in both groups. Dilatation was more fre- quently multiple (23 VI 16%, p <O&5), or per- formed in the left anterior descending coronary artery (71 vs 46%, p <O.OOl), in bypass grafts (4 vs 2%, p <0.02), in proximal coronary segments (72 VI 57%, p <O.OOl) or in lesions at bifurcation (35 vs 28%, p ~0.02) in the standby than in the backup group, respectively. PTCAs were less fre- quently performed during the same diagnostic procedure (15 vs 34%, p <O.OOl) in the standby group. Angiographic success was obtained in 91 and 92% of the attempted lesions and PTCA suc- cess in 89 and 66% of the procedures in the standby and backup groups, respectively. The in- cidence of death (1 vs 0.7%), acute myocardial in- farction (2.9 vs 2.7%) and emergency surgery (0.7 vs 0.1%) was also similar in both groups. Our results suggest that (1) PTCA is a safe procedure with a relatively low incidence of complications, in- dependent of the surgical coverage usedt (2) a rig- orous surgical standby is not necessary during all PTCA procedures; and (3) criteria for a better se- lection of high-risk patients who will require a rig- orous surgical coverage are still urgently needed. (Am J Cardiol 1992;69:1161-1165) From the Cardiopulmonar Department, Hospital Universitario “San Carlos,” Madrid, Spain. Manuscript received September 20, 1991; revised manuscript received and accepted December 19,199 I. Address for reprints: Carlos Macaya, MD, Hospital Universitario “San Carlos,” Serv. Expl. Cardiopulmonar, C/F’rof. Martin Lagos S/N, 28040 Madrid, Spain. T here are specific emergency situations during percutaneoustransluminal coronary angioplasty (PICA) in which surgery provides an expedi- tious method to solve complications. For this reason an experienced cardiovascular surgical team should always be available for emergencysurgery when PTCA proce- dures are being performed.* However, the precise ar- rangement for surgical standby varies from institution to institution. After PTCA, an incidence of 2 to 11% of acute coronary vessel closure has been reported.2-6 Acute coronary vesselclosure does not always imply a new myocardial infarction. Patients with acute closure during PTCA usually are considered candidates for emergency surgical revascularization in order to prevent acute myocardial ischemia and ongoing myocardial in- farction. Nevertheless, previous studies reported that 33 to 71% of patients who underwent emergency surgery developeda new myocardial infarction and 3 to 6% of them died during the perioperative period.3,7,8 In addi- tion, a repeat dilatation of the acutely closedvessel may be attempted as a conservative alternative to emergency bypass surgery.4-6For this reason and becauseof the suboptimal results obtained with emergency coronary surgery after PICA-related complications, we designed the present study to evaluate the impact of 2 strategies of surgical coverage, namely a “rigorous surgical stand- by” and a “surgical backup” (“in house” surgical team, but not necessarily ready to operate immediately), in the short-term results of PTCA. METHODS Between January 1986 and December 1990, a total of 1,283 consecutive PTCAs were performed at our in- stitution. In 269 PTCAs (21%) (334 lesions, 229 pa- tients) a rigorous standby surgery was organized (stand- by group). In the remaining 1,014PTCAs (79%) (1,204 lesions,841 patients) (backup group) such type of surgi- cal coverage was not required, although cardiac surgery was still available “on site.” PTCAs were performed us- ing steerable guidewire coronary angioplasty systems with a conventional coaxial or monorail technique. Dur- ing the last 287 proceduresof this series,the Palmaz- Schatz coronary stent was available and coronary stent- ing was considered in patients with suboptimal result, large subocclusive dissectionor acute vessel closure dur- ing PICA. Deffnitions: Angina was considered unstable if at rest, recent onset (<l month), after infarction or pro- STANDBY SURGERY DURING CORONARY ANGIOPIASTY 1161
-
Upload
andres-iniguez -
Category
Documents
-
view
212 -
download
0
Transcript of Comparison of results of percutaneous transluminal coronary angioplasty with and without selective...

Comparison of Results of Percutaneous Transluminal Coronary Angioplasty With and
Without Selective Requirement of Surgical Standby
Andrbs Ihguez, MD, Carlos Macaya, MD, Rosana Hernandez, MD, Fernando Alfonso, MD, Javier Goicolea, MD, Jorge Casado, MD, and Pedro Zarco, MD
To determine the outcome of percutaneous trans- luminal coronary angioplasty (PTCA) with the use of 2 different strategies of surgical coverage, the resutts of 1,283 consecutive PTCAs were ana- lyzed. In 269 procedures (21%) (patients consid- ered at high risk should acute vessel closure oc- cur - standby group) the operating room and the surgical team were ready for an immediate inter- vention. In the remaining 1,014 procedures (79%) (backup group), although the surgical team was “in house,” they were not necessarily ready for an immediate intervention. Mean age of the popula- tion was 56 f 10 years and 64% of patients were men. Coronary risk factors, medical treatment, clinical indication for PTCA, previous coronary surgery and left ventricular ejection fraction were similar in both groups. Dilatation was more fre- quently multiple (23 VI 16%, p <O&5), or per- formed in the left anterior descending coronary artery (71 vs 46%, p <O.OOl), in bypass grafts (4 vs 2%, p <0.02), in proximal coronary segments (72 VI 57%, p <O.OOl) or in lesions at bifurcation (35 vs 28%, p ~0.02) in the standby than in the backup group, respectively. PTCAs were less fre- quently performed during the same diagnostic procedure (15 vs 34%, p <O.OOl) in the standby group. Angiographic success was obtained in 91 and 92% of the attempted lesions and PTCA suc- cess in 89 and 66% of the procedures in the standby and backup groups, respectively. The in- cidence of death (1 vs 0.7%), acute myocardial in- farction (2.9 vs 2.7%) and emergency surgery (0.7 vs 0.1%) was also similar in both groups. Our results suggest that (1) PTCA is a safe procedure with a relatively low incidence of complications, in- dependent of the surgical coverage usedt (2) a rig- orous surgical standby is not necessary during all PTCA procedures; and (3) criteria for a better se- lection of high-risk patients who will require a rig- orous surgical coverage are still urgently needed.
(Am J Cardiol 1992;69:1161-1165)
From the Cardiopulmonar Department, Hospital Universitario “San Carlos,” Madrid, Spain. Manuscript received September 20, 1991; revised manuscript received and accepted December 19,199 I.
Address for reprints: Carlos Macaya, MD, Hospital Universitario “San Carlos,” Serv. Expl. Cardiopulmonar, C/F’rof. Martin Lagos S/N, 28040 Madrid, Spain.
T here are specific emergency situations during percutaneous transluminal coronary angioplasty (PICA) in which surgery provides an expedi-
tious method to solve complications. For this reason an experienced cardiovascular surgical team should always be available for emergency surgery when PTCA proce- dures are being performed.* However, the precise ar- rangement for surgical standby varies from institution to institution. After PTCA, an incidence of 2 to 11% of acute coronary vessel closure has been reported.2-6 Acute coronary vessel closure does not always imply a new myocardial infarction. Patients with acute closure during PTCA usually are considered candidates for emergency surgical revascularization in order to prevent acute myocardial ischemia and ongoing myocardial in- farction. Nevertheless, previous studies reported that 33 to 71% of patients who underwent emergency surgery developed a new myocardial infarction and 3 to 6% of them died during the perioperative period.3,7,8 In addi- tion, a repeat dilatation of the acutely closed vessel may be attempted as a conservative alternative to emergency bypass surgery.4-6 For this reason and because of the suboptimal results obtained with emergency coronary surgery after PICA-related complications, we designed the present study to evaluate the impact of 2 strategies of surgical coverage, namely a “rigorous surgical stand- by” and a “surgical backup” (“in house” surgical team, but not necessarily ready to operate immediately), in the short-term results of PTCA.
METHODS Between January 1986 and December 1990, a total
of 1,283 consecutive PTCAs were performed at our in- stitution. In 269 PTCAs (21%) (334 lesions, 229 pa- tients) a rigorous standby surgery was organized (stand- by group). In the remaining 1,014 PTCAs (79%) (1,204 lesions, 841 patients) (backup group) such type of surgi- cal coverage was not required, although cardiac surgery was still available “on site.” PTCAs were performed us- ing steerable guidewire coronary angioplasty systems with a conventional coaxial or monorail technique. Dur- ing the last 287 procedures of this series, the Palmaz- Schatz coronary stent was available and coronary stent- ing was considered in patients with suboptimal result, large subocclusive dissection or acute vessel closure dur- ing PICA.
Deffnitions: Angina was considered unstable if at rest, recent onset (<l month), after infarction or pro-
STANDBY SURGERY DURING CORONARY ANGIOPIASTY 1161

I
TABLE I Demographic Data
Groups
Standby
No. of procedureslpts. 2691229 Age (yr) 57 2 9 Men/women 169/60 Coronary risk factors
Hypertension 119 (44%) Diabetes 58 (22%) Hypercholesterolemia 95 (35%) Smokers 186 (69%) Family history 63 (23%)
Prior myocardial infarction 112 (42%) Prior coronary surgery 2 1(8%) Prior cardiac failure 15 (6%) Treatment before PTCA
Nitrates 213 (79%) p blockers 108 (40%) Calcium antagonists 221 (82%) Aspirin 191(71%) Heparin 34 (13%)
PTCA = percutaneous translummal coronary angiaplasty.
Backup
1,014/841 59L 11 699/ 142
453 (45%) 173 (17%) 415 (41%) 698 (69%) 222 (22%) 454 (45%)
63 (6%) 30 (3%)
848 (84%) 395 (39%) 795 (79%) 729 (72%) 127 (12%)
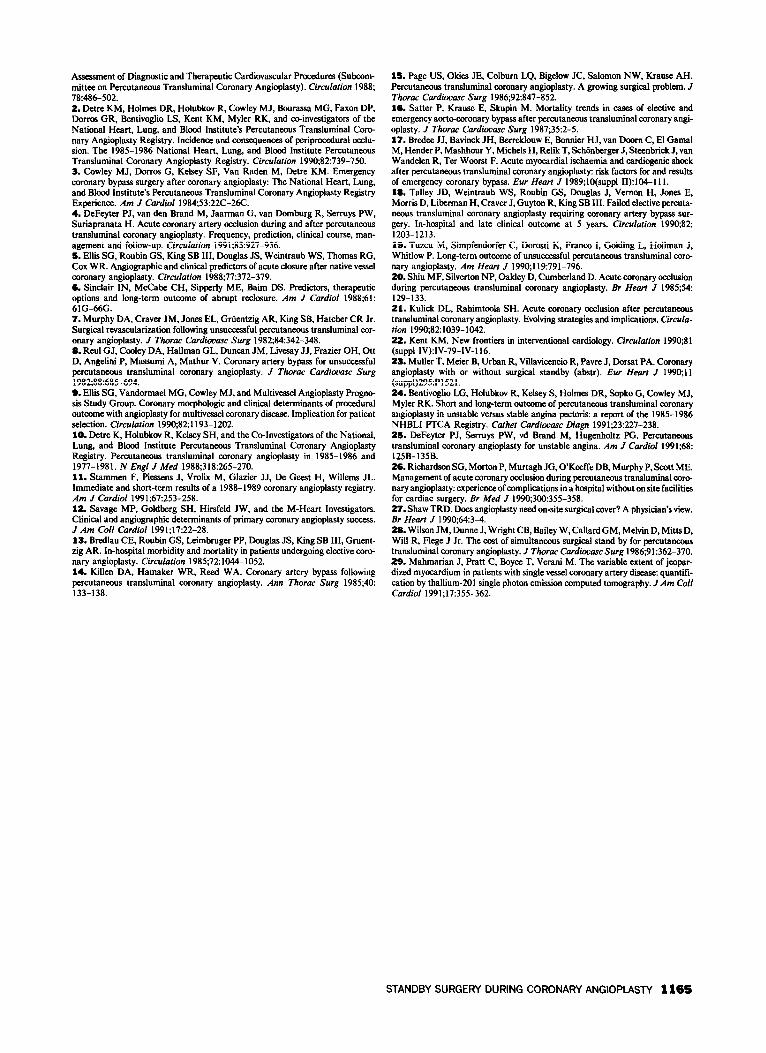
gressive despite adequate medical treatment. Coronary artery disease was considered multivessel if stenosis >50%, by visual assessment, was present in 12 major coronary arteries. Only severe stenosis (275%) was con- sidered for dilatation. Angiographic success was defined if luminal narrowing was reduced >20% and residual stenosis <50%.’ PICA procedures were considered suc- cessful when (1) angiographic success was achieved; (2) no major complication (death, acute myocardial infarc- tion, cardiac surgery) occurred during hospitalization; and (3) there was no evidence of vessel closure during hospitalization. In patients undergoing multivessel dila- tation, the FTCA procedure was considered successful if, at least the “culprit” lesion was successfully dilated and there was absence of major complications.9 Acute vessel occlusion was considered as “early closure” when
1
LESION MORPHOLOGY 1 %
100
ao- 61 *
60-
Ecc Irr Cal Bend Thr Bif Long
l pco.1 l * pqo.02
1162 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 69 MAY 1. 1992
it occurred during the procedure, before the patient had left the catheterization room, and as “late closure” when a vessel, initially dilated with success, had acute occlusion after the patient had left the catheterization room, but during hospitalization.
Surgical coverage was considered as standby if the surgical team and the operating room were ready for an emergency intervention to be started immediately. Standby surgery was required for patients who were po- tential surgical candidates and in whom the eventual closure of the attempted vessel was considered to be life- threatening. In the remaining patients, urgent surgery was still possible because the surgical team was in- house, but not necessarily ready to operate immediately (surgical backup group). General guidelines to exclude patients for rigorous surgical coverage were: patients not willing to be operated on, coronary anatomy not considered suitable for surgical revascularization, a con- comitant severe noncardiac disease, a prior myocardial infarction in the myocardium supplied by the vessel to be dilated, or dilatation of vessels with chronic total oc- clusions. Nevertheless, the decision of the kind of surgi- cal coverage required during FTCA was eventually made, on an individual basis, by the cardiologist per- forming the procedure, taking clinical and angiographic factors into consideration.
Data management and analysis: Data were pro spectively entered into a database specially designed for PTCA (Angiosystem-Cormedica”) installed on an IBM computer. Discontinuous variables were analyzed as percentages and continuous variables as mean f standard deviation, and compared by the chi-square and Student’s t test, respectively. Differences were consid- ered statistically significant at p <0.05. A logistic re- gression analysis was performed using computer soft- ware (SPSS/PC + Advanced Statistics”“, V2.0) to de termine independent correlates of acute vessel closure.
RESULTS Age, sex, coronary risk factors and patient’s medica-
tion were similar in both groups (Table I). Indication for PTCA was also similar in both groups: unstable an- gina in 188 (70%) versus 681 (67%) (p = not significant [NS]), stable angina in 54 (20%) versus 205 (20%) (p = NS), acute myocardial infarction in 6 (2%) versus 40 (4%), and silent &hernia in 21 (8%) versus 88 (9%) in the standby and backup groups, respectively. Baseline lesion morphologic features are shown in Figure 1. Ta- ble II summarizes the angiographic findings. A previous inferior myocardial infarction was present in 221 pa- tients (34 in the standby and 187 in the backup groups). The attempted lesion was located in the left anterior descending coronary artery in 13 of these patients (38%) with a previous inferior myocardial infarction in the standby group and in 30 patients (16%) in the back- up group (p <O.Ol).
Procedural data: Standby group patients underwent multiple dilatation more frequently (>l lesion or >l vessel, or both) and PTCA during the same angiograph- ic diagnostic procedure less frequently than in the back- up group patients. Angiographic and PTCA success rates were similar in both groups (Table III). In cases of

TABLE II Angiographic Findings
Groups
Standby Backup
No. of arteries narrowed Native coronary artery Grafts Native lesion location
Left anterior descending artery Circumflex artery Right coronary artery
Segment location Proximal Middle/distal
Stenosis before PTCA Stenosis after PTCA l-vessel disease Totally occluded vessels Collateral circulation LVEF LVEF < 50%
334 32 1 (96%)
13 (4%)
227 (71%) 42 (13%) 52 (16%)
240 (72%) 94 (28%)
87 + 8% 28 f 23% 150 (56%)
20 (6%) 68 (20%)
65+ 11 23 (12%)
1,204 1,179 (98%)
25 (2%) NS
<0.02
539 (46%) 266 (22%) 374 (32%)
687 (57%) 517 (43%)
88 + 26% 26 2 22% 592 (58%)
97 (8%) 218 (18%)
64 2 13 121 (16%)
<O.OOl <O.Ol <O.OOl
10.001 <O.OOl
NS NS NS NS NS NS NS
LVEF = leftventrtcular ejection fraction: NS = not significant; PTCA = percutaneous translumlnal coronary angw3plasiy.
multiple dilatation, a mean of 2.3 f 0.6 versus 2.3 f 0.7 lesions, per procedure, were attempted in the standby and backup groups, respectively. Dilatation was not suc- cessful in 9% of lesions (30 of 334) in the standby group versus 8% (100 of 1,204) in the backup group.
hmpkdhs-eadyandleteacutevesselcb sure: A total of 68 major complications occurred (5.3% of total PTCA or 6.3% of patients), with no differences between the standby and backup groups: acute myocar- dial infarction (8 cases [2.9%] vs 28 [2.7%]), emergency surgery (2 cases [0.7%] vs 1 [O.l%]), elective surgery (6 cases [2.2%] vs 12 [1.2%]) or death (3 cases [l%] vs 8 [0.7%]).
Of the 8 patients who died in the backup group, 3 were elderly patients (>75 years) who refused surgical revascularization before PTCA, 1 patient, with a metal- lic prosthesis (aortic position), died during an unsuc- cessful rescue PT.CA for a left main emboli that caused an acute myocardial infarction complicated with cardio- genie shock; 1 patient died of a gastrointestinal hemor- rhage 36 hours after PTCA, 1 patient died of an undi- agnosed subacute pericardial tamponade 6 hours after PTCA, 1 additional patient died suddenly 8 days after PTCA, and the last patient died during an emergency coronary angiography performed because of an acute ischemic event 16 hours after PTCA, with demonstra- tion of occlusion of the left circumflex artery (dilated artery) and a subocclusive thrombus in the left anterior descending coronary artery (previously normal) without time to be transferred to the operating room. Two pa- tients died during cardiac surgery, 1 from the standby group (emergency surgery for right coronary artery dis- section, despite an ischemic time <90 minutes) and 1 from the backup group (elective surgery for left anterior descending coronary artery dissection complicated with non-Q-wave myocardial infarction).
A total of 41 lesions (2.7%) had in-hospital acute occlusion (13 [32%] early closure and 28 [68%] late clo- sure). Of the 13 lesions with early closure, 6 (1.8%)
TABLE Ill Procedural Data
Groups
Standby Backup
No. of procedures/narrowings 269/334 1,014/1,204 Multiple dilatation 61 (23%) 163 (16%) p 10.02 PTCA during diagnosis 40 (15%) 343 (34%) p < 0.001 Angiographic success 304 (91%) 1,104 (92%) NS PTCA success 240 (89%) 895 (88%) NS
NS = not significant; PTCA = percutaneous transluminal coronary ang~oplasty.
were from the standby group and 7 (0.6%) from the backup group (p <O.l). By univariate analysis, none of the several clinical and angiographic baseline character- istics correlated with early closure during PTCA. Of the 28 lesions that had late closure, 5 were from the stand- by group and 23 from the backup group (p = NS). This represents 1.6 versus 2% of the lesions initially dilated with success in both groups. The in-hospital course of the 41 lesions (41 patients) with acute vessel closure is represented in Figure 2. Of the 41 lesions with acute occlusion, 26 were treated with a repeat PTCA and an- giographic success was achieved in 13 (50%). However, 4 of these patients eventually developed an acute myo- cardial infarction. Thus, PTCA success was achieved in 9 of 26 patients (35%). Seven of the 41 patients (17%) who experienced acute vessel closure (early or late) died during hospitalization (2 patients during surgery, 1 af- ter thrombolytic therapy, 2 elderly patients treated con- ventionally who refused surgery, 1 from a stroke 36 hours after a PTCA with stent deployment and 1 pa- tient of refractory ventricular fibrillation while he was waiting for elective surgery).
PTCA performed in the first 24 hours of an acute myocardial infarction (3 of 46 lesions [7%] vs 25 of 1,492 lesions [1.6%] [p <0.05]) and dilatation of totally occluded lesions (5 of 107 lesions [5%] vs 23 of 1,43 1 lesions [ 1.6%] [p <0.02]) were associated with late acute closure on univariate analysis, but that association disappeared on multivariate analysis.
Vessel patency (after suboptimal result, or large or subocclusive dissection) was achieved with a successful Palmaz-Schatz stent deployment in 22 lesions (3 from the standby and 19 from the backup groups).
‘WI -PJ I
Conventional 2 treatment 7
Thrombolytic 1 treatment 1
Emergency 2 Surgery
I3 ,
Elective Surgery 2
6 Repeat PTCA 20
4 Successful 7 2 Failed 3
FIGURE 2. InhspRd uwseofthe41lezsiam(41~) wRhacutewsseldosw~PTCA=pem&momtranrkmhd ewonvy~.
STANDBY SURGERY DURING CORONARY ANGlOPlASlY 1163

DISCUSSION The presence of a rigorous surgical coverage was
considered mandatory during the initial stages of PTCA technique.*,* The reason for this policy was an incidence of acute myocardial infarction of 4.9% and requirement of emergency coronary surgery in 5.8% of patients dur- ing PTCA.2,3,7v8 At present, even with more complex le- sions attempted, the PTCA success rate is 90% and the incidence of emergency surgery has decreased to 3.5%i” and to 1.6 to 2.7% in recent series.*iJ* Several reasons have contributed to this fact: (1) Emergency revascular- ization surgery is not always the best approach to the problem of acute closure during or after PTCA. The results reported in the largest series of emergency sur- gery after complicated PTCA demonstrated a peri- operative acute myocardial infarction rate from 21 to 71%, and an in-hospital incidence of death of 1 to 12%.3,7,8J3-19 (2) Nowadays, many periprocedural coro- nary occlusions can be successfully managed with re- peat balloon dilatation, with a mortality rate ranging from 0 to 20%,2~4-6~20 comparable to the mortality rate of emergency surgery. (3) In addition, other alternative therapeutic techniques (autoperfusion catheters, laser, stems, atherectomy devices)21~22 may improve patients’ tolerance to ischemia or to PTCA results, or both, and may be eventually used to treat PTCA complications in an attempt to reduce the need for emergency surgery. (4) The dramatic increase in the number of PTCAs in the last few years has made the need for a procedural risk stratification mandatory; therefore, different kinds of surgical coverage might be required. Only 1 prelimi- nary study by Muller et al*’ has been reported on this issue. In this study, high-risk patients (according to the size of the infarction expected in the event of acute ves- sel closure) on whom surgical coverage was required were characterized by better ejection fraction, more fre- quent left anterior descending coronary artery dilata- tion, less collateralized vessels and a lower incidence of prior infarction. No patient died in this high-risk group versus 7 patients (1.2%) in the low-risk group (surgical coverage not required in advance), 8% of patients had a new myocardial infarction versus 5%, and 3.5% required emergency surgery versus 0.3% in both groups, respec- tively.*) In our study, patients who underwent dilatation of the proximal segment of the left anterior descending coronary artery (in particular those with a previous in- ferior myocardial infarction), dilatation of lesions at a bifurcation point, those undergoing multiple dilatation, or patients on whom dilatation of lesions in bypass grafts was planned, were preferably considered to be high risk. They may probably require a rigorous stand- by surgery. Despite this, and in agreement with oth- ers 11,** major complication rate (death, acute myocar- dial infarction, cardiac surgery) was relatively low in our series (5.3% of total PTCAs) and was not signifi- cantly different in the groups considered high- or low- risk (7 vs 5%, respectively). With such unpredictable and low complication rates, very large series would be required to demonstrate the usefulness of any interven- tional approach (e.g., full standby surgery). Neverthe- less, patients with unstable angina (according to rather restrictive definition)2324,25 and unfavorable morphologic
characteristics of the lesion (type B2 or C, eccentric) have been associated with a higher risk of complica- tions.‘V,9.1*
The report of Richardson et a126 and Shaw27 demon- strated that with careful selection of patients (l-vessel disease and normal left ventricular function), PTCA might even be safely performed in a hospital with “off site” cardiac surgery.
In our experience, the low rate of patients who were referred for emergency surgery could be related to (1) the deployment of coronary stents in cases of periproce- dural dissection or acute occlusion, and (2) our policy of managing PTCA-related complications in a conserva- tive way, with preference of repeat PTCA and elective rather than emergency surgery. This approach may be the treatment of choice in most patients with acute an- gioplasty complications for several reasons: (1) The mortality rate was similar in the backup group com- pared with the standby group. (2) There were no deaths in the backup group, which might be attributed to the delay in surgical revascularization. (3) In our series, up to 35% of vessels attempted after acute closure were successfully reopened by repeat PTCA. (4) Only 4 of the 4 1 patients (10%) with evidence of acute vessel clo- sure who were managed by repeat PTCA, thrombolytic therapy or conventional methods died of cardiac causes during hospitalization. This death incidence is similar to that reported after emergency surgery. Finally, as a so- cioeconomic consideration, the cost of a rigorous stand- by surgical team has been estimated at $630.00 per pro- cedure and the number of hours a complete surgical team should spend in a “non-productive” activity, at 38 hours/month.28 Moreover, as Richardson et a126 sug- gested, a rigorous surgical standby team may also in- crease the already long waiting list for surgery that ex- ists in many countries with National Public Health Ser- vices. For these reasons, we believe that a full surgical standby team should be reserved for a limited number of high-risk patients.
Study limitations The major limitation of this study is that it is nonrandomized. Nevertheless, randomiza- tion of patients considered to be at high risk presents serious ethical limitations. The few end point events ob- served for the entire study group may justify that statis- tical analysis could not detect any differences that may exist (type 2 error). A strict prospective study rather than a retrospective analysis of prospectively collected data would have been preferable. Patients were assigned to the standby or backup groups according to the previ- ously defined criteria, but the cardiologist performing the procedure always made the final decision. Accord- ingly, the decision was performed on an individual basis, and some degree of subjectivity usually involved the se- lection of the kind of surgical coverage used. However, marked heterogenicity in the extent of jeopardized myo- cardium implies that stratification of risk cannot be per- formed from angiographic information alone.29
REFERENCES 1. Guidelines for Percutaneous Transluminal Coronary Angioplasty. A Report of the American College of Cardiology/American Heart Association Task Force on
1164 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 69 MAY 1, 1992
Assessment of Diagnostic and Therapeutic Cardiovascular Procedures (Suhcom- mittw on Percutaneous Transluminal Coronary Angioplasty). Circulation 1988; 78:486-502. 2. Detre KM, Holmes DR, Holubkov R, Cowley MJ, Bourassa MG, Faxon DP, Dorms GR, Bentivoglio LS, Kent KM, Myler RK, and coinvestigators of the National Heart, Lung, and Blood Institute’s Percutaneous Transluminal Core nary Angioplasty Registry. Incidence and consequences of periprocedural occlu- sion. The 19851986 National Heart, Lung, and Blood Institute Percutaneous Transluminal Coronary Angioplasty Registry. Circulation 1990,82:739-750. 3. Cowley MJ, Dorms G, Kelsey SF, Van Raden M, Detre KM. Emergency coronary bypass surgery after coronary angioplasty: The National Heart, Lung, and Blood Institute’s Percutaneous Transluminal Coronary Angioplasty Registry Experience. Am J Cardiol 1984;53:22C-26C. 4. DeFeyter PJ, van den Brand M, Jaarman G, van Domburg R, Serruys PW, Suriapranata H. Acute coronary artery occlusion during and after percutaneous transluminal coronary angioplasty. Frequency, prediction, clinical course, mart- agement and follow-up. Circulation 1991;83:927-936. 5. Ellis SG, Roubin GS, King SB III, Douglas JS, Weintraub WS, Thomas RG, COY. WR. Angiographic and clinical predictors of acute closure after native vessel coronary angioplasty. Circulation 198%77x372-379. 6. Sinclair IN, McCabe CH, Sipperly ME, Bairn DS. Predictors, therapeutic options and long-term outcome of abrupt reclosure. Am J Cardiol 1988;61: 61G-66G. 7. Murphy DA. Craver JM, Jones EL, Grtiemzig AR, King SB, Hatcher CR Jr. Surgical revascularimtion following unsuccessful percutaneous transluminal cor- onary angioplasty. J Thorac Cardiovasc Surg 1982;84:342-348. 8. Reul GJ, Cooley DA, Hallman GL, Duncan JM, Livesay JJ. Frazier OH, Ott D, Angelini P, Massumi A, Mathur V. Coronary artery bypass for unsuccessful percutaneous transluminal coronary angioplasty. J Thorac Cardiouasc Surg 1982;88:685-694. 9. Ellis SG, Vandormael MG, Cowley MJ, and Multivessel Angioplasty Progno sis Study Group. Coronary morphologic and clinical determinants of procedural outcome with angioplasty for multivessel coronary disease. Implication for patient selection. Circulation 1990;82: 1193- 1202. 10. Detre K, Holubkov R, Kelsey SH, and the Co-Investigators of the National, Lung, and Blood Institute Percutaneous Transluminal Coronary Angioplasty Registry. Percutaneous transluminal coronary angioplasty in 1985-1986 and 1977-1981. N Engl J Med 1988;318:265-270. 11. Stammen F, Piemens J, Vrolix M, Glazier JJ, De Gee& H, Willems JL. Immediate and short-term results of a 1988-1989 coronary angioplasty registry. Am J Cardiol 1991;67:253-258. 12. Savage MP, Goldberg SH, Hirsfeld JW, and the M-Heart Investigators. Clinical and angiographic determinants of primary coronary angioplasty success. J Am Co11 Cardiol 1991;17:22-28. 13. Bredlau CE, Roubin GS, Leimbruger PP, Douglas JS, King SB III, Gruent- zig AR. In-hospital morbidity and mortality in patients undergoing elective core nary angioplasty. Circulation 1985;72:1044-1052. 14. Killen DA, Hamaker WR, Reed WA. Coronary artery bypass following percutaneous transluminal coronary angioplasty. Ann Thorac Surg 1985;40: 133-138.
15. Page US, Okies JE, Colbum LQ, Biielow JC, Salomon NW, Krause AH. Percutaneous transhuninal coronary angioplasty. A growing surgical problem. J Thorac Cardibvaw Surg 1986;92:847-852. 16. Satter P, Krause E, Skupin M. Mortality trends in cases of elective and emergency aortworonary bypass after percutaneous transluminal coronary angi- oplasty. J Thorac Cardiovasc Surg 1987;35:2-5. 17. Bredee JJ, Bavinck JH, Berreklouw E, Bonnier HJ, van Doom C, El Gamal M, Hender P, Mashhour Y, Michels H, Relik T, Sch6nlxrger J, Steenbrick J, van Wandelen R, Ter Woorst F. Acute myccardial ischaemia and cardiogenic shock after percutaneous transluminal coronary angioplasty: risk factors for and results of emergency coronary bypass. Eur Heart J 1989;lO(suppl 11):104-111. 18. Talley JD, Weintrauh WS, Roubin GS, Douglas J, Vernon H, Jones E. Morris D, Liberman H, Craver J, Guyton R, King SB III. Failed elective percuta- neous transluminal coronary angioplasty requiring coronary artery bypass sur- gery. In-hospital and late clinical outcome at 5 years. Circulation 1990;82: 1203-1213. IS. Tuzcu M, Simpfendorfer C, Dorosti K, France I, Gelding L, Holhnan J, Whitlow P. Long-term outcome of unsuccessful percutaneous transluminal core nary angioplasty. Am Heart J 1990;119:791-796. 20. Shiu MF, Silverton NP, Oakley D, Cumberland D. Acute coronary occlusion during percutaneous transluminal coronary angioplasty. Er Heart J 1985;54: 129-133. 21. Kulick DL, Rahimtoola SH. Acute coronary occlusion after percutaneous transluminal coronary angioplasty. Evolving strategies and implications. Circula- tion 1990;82:1039-1042. 22. Kent KM. New frontiers in interventional cardiology. Circulation 199O;Sl (suppl IV):IV-79-IV-116. 23. Muller T, Meier B, Urban R, Villavicencio R, Pavre J, Dorsat PA. Coronary angioplasty with or without surgical standby (abstr). Fur Hearr J 199o;ll (suppl)295:Pl521. 24. Bentivoglio LG, Holubkov R, Kelsey S, Holmes DR, Sopko G, Cowley MJ, Myler RK. Short and long-term outcome of percutaneous transluminal coronary angioplasty in unstable versus stable angina pectoris: a report of the 1985-1986 NHBLI PTCA Registry. Cafhet Cardiovasc Diagn 1991;23:227-238. 25. DeFeyter PJ, Serruys PW, vd Brand M, Hugenholtz PG. Percutaneous transluminal coronary angioplasty for unstable angina. Am J Cardiol 1991;68: 125B-135B. 26. Richardson SG, Morton P, Murtagh JG, O’Keeffe DB, Murphy P, Scott ME. Management of acute coronary occlusion during percutaneous transluminal core nary angioplasty: experience of complications in a hospital without on site facilities for cardiac surgery. Br Med J 1990;300:355-358. 27. Shaw TRD. Does angioplasty need on-site surgical cover? A physician’s view. Br Heart J 1990;64:3-4. 28. Wilson JM, Dunne J, Wright CB, Bailey W, Callard GM, Melvin D, Mitts D, Will R, Flege J Jr. The cost of simultaneous surgical stand by for Percutaneous transluminal coronary angioplasty. J Thorac Cardiouasc Surg 1986;91:362-370. 29. Mahmarian J, Pratt C, Boyce T, Verani M. The variable extent of jeopar- dized myocardium in patients with single vessel coronary artery disease: quantift- cation by thallium-201 single photon emission computed tomography. J Am Co11 Cardiol 1991;17:355-362.
STANDBY SURGERY DURING CORONARY ANGIOPIASW 116s