ECHOCARDIOGRAPHY/ANGIOGRAPHY DEEPAK NANDAN ECHOCARDIOGRAPHY/ANGIOGRAPHY DEEPAK NANDAN.

Clin. Cardiol. 23,417420 (2000)
Comparison of Echocardiography and Electron Beam Tomography in Differentiating the Etiology of Heart Failure
THUY LE, M.D., JOHN Y. KO, B.s., H. TINA KIM, M.D., PAMELA AKINWALE, B.s., MATIMEW J. BUDOFF, M.D.
The Department of Medicine, Division of Cardiology, Harbor-UCLA Research and Education Institute, Torrance, California, USA
Summary
Background: The clinical manifestations in patients with ischemic cardiomyopathy are often indistinguishable from those in patients with primary dilated cardiomyopathy (DCM). Clinicians often base work-up of patients with heart failure on echocardiographic wall motion abnormalities; however misclassification can lead to unnecessary coronary angiography.
Hypothesis: The study was undertaken to evaluate the diag- nostic ability of echocardiography and electron beam tomog- raphy (EBT) to differentiate between ischemic and nonis- chemic cardiomyopathy.
Methods: The accuracy of EBT and echocardiography was compared in 11 1 patients undergoing coronary angiography for the evaluation of heart failure. The presence of coronary calcification (CC) by EBT or segmental wall motion abnor- malities by echocardiography was used as evidence of coro- nary-induced cardiomyopathy.
Results: Of 63 patients, 61 (97%) with obstructive coro- nary artery disease had CC by EBT. This sensitivity was sig- nificantly higher compared with 43 of 63 patients (68%) with segmental wall motion abnormalities by echocardiography (p < 0.00 1 ). Of 48 patients without obstructive coronary artery disease by angiography, 39 (8 1 %) had no CC by EBT and 35 (73%) had no segmental wall motion (global hypolunesis) by echocardiography (p = 0.33). The overall accuracy of EBT to differentiate ischemic from nonischemic cardiomyopathy was 90%, significantly higher than echocardiography (70%,
Conclusion: This double-blind study demonstrates that the presence of CC by EBT is superior to that of segmental wall motion abnormalities by echocardiography to distinguish is- chemic from nonischemic cardiomyopathy. This modality may prove to be an important diagnostic tool when the etiolo- gy of the cardiomyopathy is not clinically evident.
p<O.Ool).
Address for reprints:
Matthew J . Budoff, M.D., F.A.C.C. Saint John's Cardiovascular Research Center 1124 West Carson Street, RB-2 Torrance, CA 90502, USA
Received: May 24, 1999 Accepted with revision: August 12, 1999
Key words: electron beam tomography, echocardiography, cardiomyopathy, heart failure, etiology
Introduction
The clinical manifestations in patients with ischemic car- diomyopathy are often indistinguishable from those in pa- tients with primary dilated cardiomyopathy (DCM). Some pa- tients with severe left ventricular dysfunction from coronary artery disease (CAD) have no history of angina or myocardial infarction. Heart failure may be the primary manifestation of CAD in these patients, whereas in some patients with primary DCM cardiomyopathy angina may be the dominant clinical feature.I4 The detection of CAD in patients with cardiomy- opathy has important prognostic implication^.^ Patients with ischemic cardiomyopathy have improved survival with revas- cularization.c10
Early attempts to distinguish ischemic from nonischemic cardiomyopathy using echocardiography have been report- ed."-I3 Echocardiographic evidence of regional wall motion abnormalities, usually suggestive of CAD, have been ob- served in patients with DCM.14 Conversely, the presence of global hypokinesis and right ventricular dilatation, usually seen in patients with primary DCM, have been reported in is- chemic cardiomyopathy. l 3 These limitations of echocar- diography often preclude definitive clinical decisions in many individual cases. The study of left ventricular wall motion by echocardiography often necessitated coronary angiography, with its attendant risks, to establish a definitive diagnosis. l 6
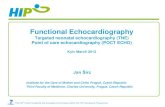
Electron beam tomography (EBT) has the ability to detect the presence of atherosclerotic calcification accurately'7-*0 (Fig. 1). Budoff et al.I7 have demonstrated its usefulness for the reliable distinction between cardiomyopathy due to CAD and nonischemic DCM. The present study provides a detailed assessment of patients with heart failure of unknown etiology who underwent echocardiography, EBT, and angiography. This study was done to compare the accuracy of EBT with that of two-dimensional (2-D) echocardiography in distinguishing ischemic cardiomyopathy from primary DCM.
Methods
Patient Population
The study group consisted of 1 1 1 patients with cardiomy- opathy of unknown etiology with a left ventricular ejection fraction of < 40%. All patients underwent the following tests:

418 Clin. Cardiol. Vol. 23, June 2000
FIG. 1 Electron beam computed tomography coronary scan of a 52-year-old man with ischemic cardiomyopathy, with severe dou- ble-vessel obstructive coronary artery disease on catheterization. Extensive calcifications of the left main, left anterior descending, and circumflex artery are seen.
(1 ) coronary catheterization for evaluation of the etiology of heart failure, (2) EBT coronary scanning to evaluate for cor- onary calcifications within 3 months of angiography, and (3) echocardiography within 2 weeks of angiography. All pa- tients were in New York Heart Association functional class II to IV at the time of angiography. Patients whose electrocar- diograms (ECGs) showed changes indicative of a Q-wave myocardial infarction were excluded. Electrocardiograms were evaluated by a cardiologist blinded to the other studies. Patients with significant valvular disease, shown by echocar- diography or angiography, were excluded. All subjects signed a written consent form approved by the Institutional Review Board at Harbor-UCLA Medical Center.
Echocardiographic Protocol
All participating patients received a standard transthoracic echocardiogram. Standard parasternal long- and short-axis and apical two-chamber and four-chamber views were ac- quired. An experienced reader interpreted echocardiograms in blinded fashion. Patients were considered to have coronary-in- duced cardiomyopathy if there was presence of segmental wall motion abnormalities. Conversely, patients with no seg- mental wall motion abnormalities (global hypokinesis) were considered to have DCM.
Electron Beam Computed Tomography Coronary scanprotocol
The EBT studies were performed with the Imatron C- 150XL Ultrafast computed tomographic scanner (Imatron, San Francisco, Calif.) in the high-resolution volume mode us- ing a 100 ms exposure time. Electrocardiographic triggering was employed, so that each image was obtained at the same point in diastole, corresponding to 80% of the R-R interval.
Proximal coronary artery visualization was obtained without contrast medium injection, and at least 20 consecutive images were obtained at 3 mm intervals beginning 1 cm below the ca- rina and progressing caudally to include the proximal coro- nary arteries. Total radiation exposure using this technique was c 1 Rad per patient.
The lesion score was calculated by multiplying the lesion area by a density factor derived from the maximal Hounsfield unit within this area, as previously described.l8 The density factor was assigned in the following manner: 1 for lesions whose maximal density were 130-199 Hu, 2 for lesions 200- 299 Hu, 3 for lesions 300-399 Hu, and 4 for lesions > 400 Hu. A total calcium score was determined by summing individual lesion scores from each of four anatomic sites (left main, left anterior descending, circumflex, and right coronary arteries).
Angiographic Protocol
The coronary angiograms were analyzed by an experienced reader blinded to the results of the echocardiogram and EBT studies. The left main, left anterior descending, circumflex, and right coronary arteries were assessed in multiple projec- tions. Visual estimates of the percentage of luminal stenosis for each lesion were recorded. The maximum stenosis per ves- sel was placed in one of five categories: none, luminal irregu- larities (< 50% stenosis), 50-74%, 75-99%, or 100% occlu- sion. A 50% luminal diameter stenosis by angiography was considered significant in any vessel.
Classification of Cardiomyopathy
Classification of the etiology of left ventricular dysfunction was based entirely on arteriographic findings. Patients were considered to have cardiomyopathy secondary to CAD if a significant stenosis (2 50% luminal artery stenosis) was pre- sent in one or more major coronary arteries with a wall motion abnormality in the dependent myocardial territory. Converse- ly, patients were considered to have DCM if coronary angiog- raphy failed to reveal significant CAD.
Statistical Analysis
All values are reported as mean f standard deviation. Data were analyzed using a two-tailed unpaired t-test for comparing categorical variables. All tests of significance were two tailed, and significance was defined at the 10.05 level. McNemars analysis was used to compare differences of qualitative sam- ples. Standard estimates of sensitivity, specificity, and predic- tive values were obtained by use of two-by-two contingency tables. Accuracy was defined as true positives plus true nega- tives divided by all patients.
ReSUltS
We examined 11 1 patients (mean age 55 k 11 years) with cardiomyopathy of unknown etiology. All patients underwent cardiac catheterization for diagnosis. By coronary angio-

T. Le et al.: Echocardiography and EBT for discerning etiology of heart failure 419
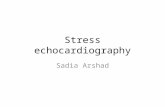
FIG. 2 Overall sensitivities, specificities, and accuracies of electron beam tomography (EBT) coronary calcification and echocardiogra- phy (by segmental wall motion abnormalities) for obstructive coro- nary artery disease (>50% occlusion by angiography). The sensitiv- ity and accuracy of EBT to differentiate ischemic from nonischemic cardiomyopathy were significantly higher than two-dimensional echocardiography (p ~0.001 for both). = EBCT coronary calci- um, H = echocardiography.
graphic criteria, 63 patients had ischemic and 48 had nonis- chemic cardiomyopathy. There were no significant differences between the two groups with regard to age, gender, ethnicity, or prevalence of individual risk factors. Of the 63 patients with obstructive CAD, 10 had single-vessel, 24 had double-vessel, and 29 had triple-vessel disease. Of these 63 patients, EBT identified coronary calchcation (CC) in 61 patients (scote > 0, sensitivity 97%). In contrast, echocardiography only demon- strated segmented wall motion abnormalities in 43 of the 63 patients with obstructive CAD (sensitivity 68%). The sensitiv- ity of EBT to diagnose cardiomyopathy from CAD is signifi- cantly higher than that of echocardiography (p < 0.001). Of the 48 patients without CAD by angiography, 39 had no CC by EBT (specificity 8 1 %), whereas 35 of the 48 patients without CAD had no segmental wall motion (only global hypokinesis) by echocardiography (specificity 73%, p = 0.33). The overall accuracy of EBT (90%) to differentiate between ischemic and nonischemic cardiomyopathy was significantly higher than 2-D echocardiography (70%, p<O.001). (Fig. 2). Figure 3 demonstrates the EBT score and the presence of angiographi- cally significant disease by angiography.
RG. 3 Electron beam tomography (EBT) scores (using the Agat- ston method) displayed by etiology of heart failure (ischemic or di- lated cardiomyopathy).
both groups of patients (those with and without CAD) as con- firmed in our study. Our echocardiographic results, demon- strating 68% sensitivity and 73% specificity for identification of ischemic etiology, are similar to other studies. Diaz et al. l 2
demonstrated regional wall motion abnormalities in 65% of patients with ischemic cardiornyopathy and in 44% of patients with DCM (specificity of 56%). Medina etal. l 3 demonstrated regional wall motion abnormalities by echocardiography in 44 patients, and 38 (86%) of these had significant CAD, usually double- or triple-vessel obstruction; of the 16 patients with DCM and diffuse left ventricular hypokinesis, 8 (specificity = 50%) had evidence of CAD. Unfortunately, definitive diagno- sis is often elusive without concomitant cardiac catheteriza- tion, with the attendant risks and costs.
Our data indicate that EBT can accurately distinguish be- tween the clinical entities of DCM and coronary-induced car- diomyopathy. The results are similar to those of Shemesh et al.,23 who demonstrated that the detection of CC yielded a 100% sensitivity and 92% specificity in the diagnosis of is- chemic cardiomyopathy. The sensitivity, specificity, and pre- dictive value established by this technique are more accurate than when echocardiography is used. Numerous studies have shown that CC assessment using EBT has been compared with angiography, with sensitivities ranging 88 to 100% for signifi- cant angiographic stenoses.20. 24,25 This could prevent the need for high-risk invasive coronary angiography in patients in whom the etiology of cardiomyopathy is indeterminate.
Study Limitations Discussion
It is not uncommon to encounter a clinical situation in which the etiology of the presenting cardiomyopathy is not readily apparent. In patients with cardiomyopathy secondary to CAD, broader treatment options may lead to prolonged sur- vival.”’O It is of clinical importance to have a reliable nonin- vasive study to differentiate between DCM and coronary-in- duced cardiomyopathy. Conflicting results have been reported with echocardiography.21. 22 Echocardiographic evidence of segmental left ventricular wall motion abnormalities support- ing a diagnosis of CAD is not a very sensitive marker. Diffuse left ventricular hypokinesis and right ventricular dilatation suggestive of primary dilated cardiomyopathy can be seen in
This study has several limitations and could be considered to have a selection bias. Some patients were referred to an- giography because of the presence of cardiomyopathy and an echocardiogram with segmental wall motion abnormalities. Similarly, some patients conceivably with DCM and echocar- diograms with global hypokinesis might not be referred for angiography and thus are not included in the study.26 This post-test referral bias could lead to a higher sensitivity (more true positives) and lower specificity (fewer true negatives). Electron beam tomography was performed after the angio- gram, therefore no post-test referral bias occurred for this modality. Another potential limitation is that analysis of wall motion was limited to qualitative techniques. The lower sensi-

420 Clin. Cardiol. Vol. 23, June 2000
tivity seen by echocardiography might be partially explained by the exclusion of patients with Q-wave infarctions which might produce more segmental wall motion abnormalities. However, it was the intent of this study to evaluate the diag- nostic potential of these modalities in cases where there was no obvious infarction. The diagnostic ability of the EBT scan is not influenced by the presence or absence of Q waves. Finally, coronary angiography cannot differentiate precisely between ischemic and nonischemic cardiomyopathy since the two conditions may coexist.
Conclusions
In this study, electron beam tomography proved superior to echocardiography as a noninvasive means to distinguish accu- rately between ischemic from nonischemic cardiomyopathy. The presence of regional wall motion abnormalities estab- lished by echocardiographic technique is an indicator for the presence of CAD. This is true for patients with normal left ventricular dimension^.'^ In patients with DCM, the presence of regional wall motion abnormalities is neither sensitive nor specific for detection of 1 3 9 27, 28 Many patients with DCM with echocardiographic evidence of segmental wall mo- tion abnormahties undergo cardiac catheterization to establish a definitive diagnosis. Use of EE3T may eliminate the need for indiscriminate use of cardiac catheterization in this population.
References
I .
2.
3.
4.
5.
6.
7.
8.
9.
10.
Kannel WB, Abbott RD: Incidence and prognosis of unrecognized myocardial infarction: An update of the Framingham Study. N Engl JMed l98~3l1:1144-1147 Raferty EB, Banks DC, Oram S: Occlusive disease of the coronary arteries presenting as primary congestive cardiomyopathy. Lancet
Greenberg JM, Murphy JH, Okada RD, Pohost GM, Strauss HW, Boucher CA: Value and limitations of radionuclide angiography in determining the cause of reduced left ventricular ejection fraction: Comparison of idiopathic dilated cardiomyopathy and coronary artery disease. Am J Curdiol1985;55:541-544 Gau GT, Goodwin JF, Oakley CM, Olsen EG, Rahimtoola SH, Raphael MJ, Steiner RE: Q-waves and coronary arteriography in cardiomyopathy. BrHeurt J 1972;341034-1041 Franciosa JA, Wilen MW, Ziesche S, Cohn J: Survival in man with severe chronic left ventricular failure due to coronary heart disease or idiopathic dilated cardiomyopathy. Am J Cardiol 1983;5 1:
Passamani E, Davis KB, Gdespie MJ, Killip T A randomized trial of coronary artery bypass surgery. Survival of patients with a low ejection fraction. NEngl JMed 1985;312:1665-1672 Pigott JD, Kouchoukos NT, Oberman A, Cutter GR: Late results of surgical and medical therapy for patients with coronary artery dis- ease and depressed left ventricular function. J Am Coll Curdiol
Alderman EL, Fisher LD, Litwin P, Kaiser GC, Myers WO, May- nard C, Levine F, Schloss M: Results of coronary artery surgery in patients with poor left ventricular function (CASS). Circulation
Zubiate P, Kay JH, Mendez AM: Myocardial revascularization for the patient with drastic impairment of function of the left ventricle. J Thoruc Cutdiovusc S u e 1977;73:8&86 Freeman Ap, Walsh WF, Giles RW, Choy D, Newman DC, Horton DA, Wright JS, Murray Ip: Early and long-term results of coronary
1969;2:1147-1150
83 1-837
19855: 1035-1045
1983;68:785-795
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
artery bypass grafting with severely depressed left ventricular per- formance. Am J Curdiol1984;54749-754 Chen Y, Shemd W, Dwyer EM Jr: Value of two-dimensional echocardiography in evaluating coronary artery disease: A ran- domized blinded analysis. JAm Coll CurdiolI985;5:911-917 Diaz RA, Nihoyannopoulos P, Athanassopoulos G, Oakley CM: Usefulness of echocardiography to differentiate dilated cardiomy- opathy from coronary induced heart failure. Am J Cardiol 1991; 68: 1224-1227 Medina R, Panidis IP, Morganroth J, Kotler MN, Mintz GS: The value of echocardiographic regional wall motion abnormalities in detecting coronary artery disease in patients with or without a dilat- ed left ventricle.Am HeurtJ 1985;109:799-803 Wallis DE, O’Connel JB, Henkin RE, Costanso-Nordin MR, Scan- Ion PJ: Segmental wall motion abnormalities in dilated cardiomy- opathy. A common finding and good prognostic sign. J Am Coll Curdiol1984;4:674-679 Davis K, Kennedy JW, Kemp HG, Judkins MP, Gosselin AJ, Kilip T Complications of coronary arteriography from the Collaborative Study of Coronary Artery Surgery (CASS). Circulation 1979;59:
Wyman RM, Safian RD, Portway V, Skillman JJ, McKay RG, Baim DS: Current complications of diagnostic and therapeutic catheterization. JAm Coll Cutdiol1988; 12: 14W1406 Budoff MJ, Shavelle DM, Lamont DH, Kim HT, Akinwale P, Kennedy JM, Brundage BH: Usefulness of electron beam comput- ed tomography scanning for distinguishing ischemic from nonis- chemic cardiomyopathy. JAm Coll Curdiol1998;32: 1173-1 178 Rumberger JA, Schwartz RS, Simons B, Sheedy PF, Edwards WD, Fitzpatrick L A Relation of coronary calcium determined by elec- tron beam computed tomography and lumen narrowing determined by autopsy. Am J Curdiol1994;74: 1 169-1 173 Janowitz WR, Agatston AS, Viamonte M: Comparison of serial quantitative evaluation of calcified coronary artery plaque by ultra- fast computed tomography in persons with and without obstructive coronary artery disease. Am J Curdiol199 1 ;68: 14 Budoff MJ, Georgiou D, Brody A, Agatston AS, Kennedy J, Wolflciel C, Stanford W, Shields P, Lewis RJ, Janowitz WR, Rich S, Brundage BH: Ultrafast computed tomography as a diagnostic modality in the detection of coronary artery disease: A multicenter study. Circulation 1996;93:898-904 Rumberger JA, Sheedy PF, Breen FJ, Schwartz RS: Electron beam CT coronary calcium score cutpoints and severity of associated an- giography luminal stenosis. J A m Coll Curdiol1997;29: 1542-1548 Shors CM, Kozul VJ, Henderson F The differential diagnosis of congestive cardiomyopathy by echocardiography. Angiology 1975;
Shemesh J, Tenenbaum A, Fisman EZ, Har-Zahav Y, Rath S, Apter S, Itzchak Y, Motro M: Coronary calcium as a reliable tool for dif- ferentiating ischemic from nonischemic cardiomyopathy. Am J Curdiol1996;77: 19 1-1 94 Simons DB, Schwartz RS, Sheedy PF, Breen JF, Edwards WD, Rumberger JA: Coronary artery calcification by ultrafast CT pre- dicts stenosis size: A necropsy study. Circulation 1990;82:62-63 Hamby RI, Tabrah F, Wisoff BG, Hartstein ML: Coronary artery calcification: Clinical implications and angiographic correlates. Am Heart J 1974;87:565-570 Corya BC, Feigenbaum H, Rasmussen S, Black MJ: Echocardio- graphic features of congestive cardiomyopathy compared with nor- mal subjects and patients with coronary artery disease. Circulution
Iskandrian AS, Helfield H, Lemlek J, Lee J, Iskandrian B, Heo J: Differentiation between primary dilated cardiomyopathy and is- chemic cardiomyopathy based on right ventricular performance. Am HeurtJ 1992;123:768-773 Sharp SM, Sawada SG, Segar DS, Ryan T, Kovacs R, Fineberg NS, Feigenbaum H: Dobutamine stress echocardiography: Detection of coronary artery disease in patients with dilated cardiomyopathy. JAm Coll Curdiol1994;24934-939
1105-1 11 1
26:723-733
1974;49:1153-1162