Comparison of 99m Tc-N-DBODC5 and 99m Tc-MIBI of Myocardial Perfusion...
11
Hindawi Publishing Corporation BioMed Research International Volume 2013, Article ID 145427, 10 pages http://dx.doi.org/10.1155/2013/145427 Clinical Study Comparison of 99m Tc-N-DBODC5 and 99m Tc-MIBI of Myocardial Perfusion Imaging for Diagnosis of Coronary Artery Disease Haiyan Ma, Sijin Li, Zhifang Wu, Jianzhong Liu, Haiyan Liu, and Xiaoshan Guo Department of Nuclear Medicine, First Affiliated Hospital of Shanxi Medical University, 85 Jiefang South Road, Taiyuan, Shanxi 030001, China Correspondence should be addressed to Sijin Li; [email protected] Received 20 April 2013; Accepted 20 May 2013 Academic Editor: Hong Zhang Copyright © 2013 Haiyan Ma et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Despite recent advances in therapeutic and diagnostic approaches, coronary artery disease (CAD) and its related car- diac disorders represent the most common cause of death in the United States. Nuclear myocardial perfusion imaging (MPI) technologies play a pivotal role in the diagnosis and treatment design for CAD. Recently, in order to develop improved MPI agents for diagnosis of CAD, 99m Tc-[bis(dimethoxypropylphosphinoethyl)-ethoxyethyl-amine(PNP5)]-[bis(N- ethoxyethyl)dithiocarbamato(DBODC)]nitride(N-DBODC5)( 99m Tc-N-DBODC5) with a faster liver clearance than conventional single-photon emission computed tomography (SPECT) imaging agents (technetium 99m sestamibi ( 99m Tc-MIBI) or technetium 99m tetrofosmin) has been introduced. In preclinical and phase I studies, 99m Tc-N-DBODC5 has shown characteristics of an essentially ideal MPI tracer. Importantly, however, there is no data to support the use of 99m Tc-N-DBODC5 to evaluate myocardial ischemia in patients with suspected CAD. e present study was designed to assess the clinical value of this agent; the findings of stress and rest MPI aſter the administration of this agent were compared to those of stress and rest 99m Tc-MIBI, as well as those of coronary angiography, with respect to the detection of CAD. Our findings indicated the usefulness of 99m Tc-N-DBODC5 as a promising MPI agent. 1. Introduction Coronary artery disease (CAD) remains the single greatest cause of death in men and women in the USA, despite a declining total death rate. Using 2005 data, over 445,000 (or 1 in every 5) deaths in the USA were due to CAD, and it ranked highest among all disease categories in hospital discharges [1]. CAD also remains the third leading cause of death of the Chinese population, creating a significant socioeconomic burden [2]. erefore, the reduction of the morbidity and mortality due to CAD is of primary importance to physicians and patients. Nuclear cardiology, cardiovascular magnetic resonance, cardiac computed tomography, position emission computed tomography, and coronary angiography (CA) are imaging modalities that have been used to measure myocardial perfusion, leſt ventricular function, and coronary anatomy for clinical management and research [3]. Based on current guidelines, invasive CA is a suitable diagnostic procedure for patients with a high pretest likelihood of significant coronary artery disease either with or without troublesome symptoms or clinical findings [4, 5]. In this population, the reported diagnostic yield of invasive CA is 44–48% [6–8]. However, in reality, invasive CA has an even lower diagnostic yield of obstructive CAD of approximately 38% [9]. Noninvasive testing could be of value to defer from invasive diagnostic procedures. Stress myocardial perfusion imaging (MPI) has emerged as an important noninvasive mean of evaluating patients with suspected CAD, with over 8.5 million evaluations performed annually in the USA [10]. e most commonly used imaging modality for this purpose is single-photon emission computed tomography (SPECT) [11]. e advantages of nuclear MPI for the detec- tion of CAD are as follows: first, it enables the simple, safe, and noninvasive assessment of myocardial ischemia and reduction of coronary flow reserve using exercise or pharmacological stress. In addition, it provides leſt ven- tricular functional information on coronary arteries, which
Transcript of Comparison of 99m Tc-N-DBODC5 and 99m Tc-MIBI of Myocardial Perfusion...

Hindawi Publishing CorporationBioMed Research InternationalVolume 2013 Article ID 145427 10 pageshttpdxdoiorg1011552013145427
Clinical StudyComparison of 99mTc-N-DBODC5 and 99mTc-MIBI of MyocardialPerfusion Imaging for Diagnosis of Coronary Artery Disease
Haiyan Ma Sijin Li Zhifang Wu Jianzhong Liu Haiyan Liu and Xiaoshan Guo
Department of Nuclear Medicine First Affiliated Hospital of Shanxi Medical University 85 Jiefang South RoadTaiyuan Shanxi 030001 China
Correspondence should be addressed to Sijin Li lisj-nmhotmailcom
Received 20 April 2013 Accepted 20 May 2013
Academic Editor Hong Zhang
Copyright copy 2013 Haiyan Ma et al This is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Despite recent advances in therapeutic and diagnostic approaches coronary artery disease (CAD) and its related car-diac disorders represent the most common cause of death in the United States Nuclear myocardial perfusion imaging(MPI) technologies play a pivotal role in the diagnosis and treatment design for CAD Recently in order to developimproved MPI agents for diagnosis of CAD 99mTc-[bis(dimethoxypropylphosphinoethyl)-ethoxyethyl-amine(PNP5)]-[bis(N-ethoxyethyl)dithiocarbamato(DBODC)]nitride(N-DBODC5)(99mTc-N-DBODC5) with a faster liver clearance than conventionalsingle-photon emission computed tomography (SPECT) imaging agents (technetium 99m sestamibi (99mTc-MIBI) or technetium99m tetrofosmin) has been introduced In preclinical and phase I studies 99mTc-N-DBODC5 has shown characteristics of anessentially ideal MPI tracer Importantly however there is no data to support the use of 99mTc-N-DBODC5 to evaluate myocardialischemia in patients with suspected CAD The present study was designed to assess the clinical value of this agent the findings ofstress and rest MPI after the administration of this agent were compared to those of stress and rest 99mTc-MIBI as well as thoseof coronary angiography with respect to the detection of CAD Our findings indicated the usefulness of 99mTc-N-DBODC5 as apromising MPI agent
1 Introduction
Coronary artery disease (CAD) remains the single greatestcause of death in men and women in the USA despite adeclining total death rate Using 2005 data over 445000 (or 1in every 5) deaths in the USAwere due to CAD and it rankedhighest among all disease categories in hospital discharges[1] CAD also remains the third leading cause of death ofthe Chinese population creating a significant socioeconomicburden [2] Therefore the reduction of the morbidity andmortality due to CAD is of primary importance to physiciansand patients
Nuclear cardiology cardiovascular magnetic resonancecardiac computed tomography position emission computedtomography and coronary angiography (CA) are imagingmodalities that have been used to measure myocardialperfusion left ventricular function and coronary anatomyfor clinical management and research [3] Based on currentguidelines invasive CA is a suitable diagnostic procedure
for patients with a high pretest likelihood of significantcoronary artery disease either with or without troublesomesymptoms or clinical findings [4 5] In this populationthe reported diagnostic yield of invasive CA is 44ndash48[6ndash8] However in reality invasive CA has an even lowerdiagnostic yield of obstructive CAD of approximately 38[9] Noninvasive testing could be of value to defer frominvasive diagnostic procedures Stress myocardial perfusionimaging (MPI) has emerged as an important noninvasivemean of evaluating patients with suspected CAD with over85 million evaluations performed annually in the USA [10]
The most commonly used imaging modality for thispurpose is single-photon emission computed tomography(SPECT) [11] The advantages of nuclear MPI for the detec-tion of CAD are as follows first it enables the simplesafe and noninvasive assessment of myocardial ischemiaand reduction of coronary flow reserve using exercise orpharmacological stress In addition it provides left ven-tricular functional information on coronary arteries which
2 BioMed Research International
is different from the morphological information providedby CA [12] Furthermore CA is the standard techniquefor assessing epicardial coronary anatomy and MPI is thestandard technique for assessing myocardial perfusion andis appropriate for the quantitative evaluation of myocardialperfusion conditions [13]
Thallium-201 (201Tl) technetium 99m sestamibi (99mTc-MIBI) and technetium99m tetrofosmin (99mTc-tetrofosmin)are three traditional routinely used MPI tracers and areclinical-validated tracers for evaluation of SPECT MPI [14ndash16] Because 201Tl is a cyclotron-produced isotope it isexpensive and it is not easily available for routine clinicaluse inmany developing countriesTherefore from a practicalstandpoint 99mTc-MIBI or 99mTc-tetrofosmin is the preferredagent for a gated SPECT study However tracer activitybelow the diaphragm is commonly seen with 99mTc-MIBIand 99mTc-tetrofosmin and this can reduce accuracy in somestudies [17 18]
Recently 99mTc-N-DBODC5 with a faster liver clearancethan conventional SPECT imaging agents has been intro-duced It is a new lipophilic monocationic 99mTc-labeledcompound that is currently under clinical investigation asa MPI agent [19ndash24] Basic research and phase I studieshave shown the safety excellent biodistribution and highimage quality of this radiopharmaceutical [22 25 26] Like99mTc-MIBI and 99mTc-tetrofosmin 99mTc-N-DBODC5 alsoa monocationic lipophilic complex is possibly localized inthe mitochondrial fraction Marmion et al [27] and Bolzatiet al [28] reported that the lipophilic characteristics andelectronic charge of the tracer were thought to be importantImportantly however the clinical value of diagnosis of CADhas not been fully explored
In order to evaluate the clinical value of this agent thefindings of stress and restMPI after the administration of thisagent were compared to those of stress and rest 99mTc-MIBIMPI as well as those of CA with respect to the detection ofCAD
2 Methods
21 Patient Population Of 120 patients admitted to thehospital because of chest pain fromMarch 2010 to December2011 46 (31 males mean age 6008plusmn858 years (Table 1)) whounderwent stress-rest 99mTc-N-DBODC5 SPECT 99mTc-MIBI SPECT and coronary arteriography were included inthis study If the creatine kinase concentration was morethan twice the upper normal limit or there was positivetroponin T or if there was evidence of previous myocardialinfarction coronary angioplasty or a coronary artery bypassgraft surgery the patients were excluded
22 Preparation of 99119898Tc-N-DBODC5 99mTc-N-DBODC5was prepared using a lyophilized kit formulation purchasedfrom Beijing Shihong Pharmaceutical Center The salinesolution of sodium pertechnetate (10mL 1110MBq) wasadded to an SDH vial (Vail A 50mg of succinate dehydro-genase 50mg of 12-diaminopropane-NNN1015840N1015840-tetraaceticacid and 005mg of SnCl
2sdot2H2O) Then the solution was
Table 1 Study group
Parameter Value119899 46MF 3115Age (yr) 6008 plusmn 858 (39ndash74)Hypertension 31Hyperlipidemia 19Diabetes mellitus 14Smoking 26Trigger of chest pain
Effort 22Rest 13Not specific 11
ECG abnormality 11ST-T elevation 3ST-T depression 8ge50 of luminal narrowing 29One-vessel disease 14Two-vessel disease 11Three-vessel disease 4Data are presented as mean plusmn SD or number () as appropriate
kept at room temperature for 15min to form a [99mTcN]2+intermediate The other two lyophilized vials (Vail B 20mgof PNP5 Vail C 20mg of DBODC) were dissolved with10mL of saline solution respectively And then the salinesolutions ofVails B andCwere added to the vial of [99mTcN]2+intermediate (Vail A) The resulting solution was heated at100∘C for 15min Before injection the solution was filtratedthrough a 022-120583mmembraneThe 99mTc-MIBI was obtainedusing a lyophilized kit formulation (Beijing Shihong Phar-maceutical Center) in the First Affiliated Hospital of ShanxiMedical University
Radiochemical purity (RCP) was determined by thin-layer chromatography (TLC) TLC was conducted onpolyamide film as the station phase and salineacetone (v v= 6 1) as the mobile phase Retention factor (Rf) for 99mTc-N-DBODC5 is 03ndash06 The RCP was more than 95 in eachexperimental study and the purity was still greater than 95at least 6 h
23 Exercise Protocol Figure 1 shows that a two-day proto-col was used for both 99mTc-MIBI and 99mTc-N-DBODC5MPI Image acquisition procedures conformed to the ASNCimaging guidelines [29 30] and the aged-adjusted max-imal heart rate was the endpoint on an ergometer butother endpoints included physical exhaustion uncommonarrhythmia severe angina or significant hypotension At theendpoint of the symptom-limited bicycle ergometer exer-cise 740MBq of 99mTc-N-DBODC5 (mean injected activity7408 plusmn 111MBq) was injected exercise was continued fora further 2min
Each patient underwent an exercise 99mTc-MIBI studywithin 7 days of the 99mTc-N-DBODC5 study For the 99mTc-MIBI (7415 plusmn 123MBq) SPECT study the exercise protocol
BioMed Research International 3
Imaging protocols 2-day exercise stressrest
Stress (day 1)
Inject 20ndash25 mCi 1-2 minsprior to peak
Exercise Gated imaging
0 30(mins)
Rest (day 2)Inject
20ndash25 mCiGated imaging
0 60(mins)
Figure 1 99mTc-N-DBODC5 and 99mTc-MIBI imaging protocolstwo-day exercise stressrest
of patients was identical to that for the 99mTc-N-DBODC5study 99mTc-N-DBODC5 and 99mTc-MIBI were used asmyocardial perfusion agents in a random sequence
24 Gated SPECT Acquisition and Image Reconstruction Pa-tients were imaged in the supine position with their armsraised SPECT images were acquired with a fixed 90∘ two-headed gamma camera (Infinia VC Hawkeye General Elec-tric USA) using a low-energy high-resolution parallel-holecollimator from the 45∘ right anterior oblique to the 45∘ leftposterior position Acquisition parameters were as followsdetectors at 90∘ 180∘ rotation at 3∘ steps with automaticbody contouring 35 s acquisition per step 64 times 64 matrixzoom times128 and energy window 140 keV plusmn 10 The totalacquisition time was approximately 20min The same filterswere used for both tracers The raw projection datasetswere filtered with a Butterworth filter (cut off frequency050 cyclespixel and power 60 for rest images cut offfrequency 050 cyclespixel and power 50 for stress images)No scatter or attenuation correction was performed
25 Heart-to-Organ Analysis 99mTc-N-DBODC5 and 99mTc-MIBI heart-to-organ count ratios were calculated from theanterior projection of each tomographic acquisition Regionsof interests (ROIs) were drawn around the entire left ventric-ular myocardium over the hepatic margin adjacent to theinferoapical wall of the left ventricle excluding the biliarytree and over the inferior left ventricular wall adjacent largeintestine activityThemean counts per pixel in the three ROIswere normalized to the injected tracer activity after decaycorrection and to a standard acquisition time of 1min Heart-to-liver and heart-to-intestine ratios were then computed[31]
26 Image Quality Assessing For MPI analyses at firsttwo experienced observers judged which image sets from99mTc-MIBI and 99mTc-N-DBODC5 were superior in imagequality on the basis of patient motion statistical noise traceractivity below the diaphragm heart-to-organ count ratio andsharpness without knowledge of the radiopharmaceutical orpatient identity [32]
27 MPI Image Interpretation Both overall qualitative diag-nosis and semiquantitative 17 segment with 5-point [33] (0= normal 4 = absent tracer uptake) scorings were employedin the independent blinded read by two expert readerswho were experienced in SPECT MPI interpretation In thismodel the left anterior descending artery (LAD) distributionterritory comprises seven segments (segments 1-2 7-8 13-14 and 17) the left circumflex artery (LCX) comprises fivesegments (segments 3-4 9-10 and 15) and the right coronaryartery (RCA) comprises five segments (segments 5-6 11-12and 16) SPECT stressrest studies were classified for eachmyocardial region in the following manner normal if all thesegments were normal after stress ischemic if at least onesegments improved at rest and scar if no segments improvedat rest In addition the summed stress (SSS) summed rest(SRS) and summed difference scores (SDSs) were calculatedand ischemia was defined as SDS ge 2 [34] The 99mTc-MIBIand 99mTc-N-DBODC5 images were separately interpretedwithout knowing the clinical histories results of coronaryangiography or other radionuclide findings
28 Coronary Angiography Interpretation All coronary angi-ograms were interpreted with quantitative CA in a coronaryangiography core laboratory blinded to the clinical or imag-ing results A coronary stenosis was considered present whenthere was a stenosis ge 50 in diameter in any epicardialcoronary artery The presence of one or more coronarystenoses defined the presence of significant CAD
29 Statistical Analysis All statistical analyses were per-formed using the statistical package SPSS 160 (Chicago ILUSA) The results were expressed as the mean value plusmn SDThe difference in left ventricular function parameters andperfusion scores were compared using a paired Studentrsquost-test Comparison of the proportion was made with theMcNemar test CA results were used as the ldquogold standardrdquoAgreements between CA and SPECT results were defined asthe kappa (120581) value 119875 lt 005 was considered significant
3 Results
31 Coronary Angiography Of the 46 patients studied 29had ge50 luminal diameter stenosis in at least one majorcoronary vessel Fourteen had single-vessel disease 11 hadtwo-vessel disease and four had three-vessel disease 15patients showed significant stenosis in the RCA 19 in theLAD and 14 in the LCX The remaining 17 patients hadnormal or nonsignificantly stenosed coronary arteries
4 BioMed Research International
(a) (b)
(c) (d)
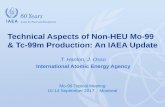
Figure 2 Comparison of liver clearance of the two tracers in anterior tomographic planar images of a patient (as shown in the black arrowH heart Lv liver) (a) Exercise stress 99mTc-N-DBODC5 (b) Exercise stress 99mTc-MIBI (c) rest 99mTc-N-DBODC5 and (d) rest 99mTc-MIBI
00
02
04
06
08
10
12
Hea
rt-to
-live
r rat
io
Stress 30 min Rest 60 minTime after injection
99m Tc-N-DBODC599m Tc-MIBI
lowast
P lt 005 versus 99mTc-MIBIlowast
lowast
(a)
Stress 30 min Rest 60 minTime after injection
99m Tc-N-DBODC599m Tc-MIBI
00
05
10
15
20
25
Hea
rt-to
-inte
stine
ratio
lowast
lowast
lowast
P lt 005 versus 99mTc-MIBI
(b)
Figure 3 Heart-to-liver ratio and heart-to-intestine ratiomeasured with an anterior projection images at stress for 30min and rest for 60minfor 99mTc-N-DBODC5 and 99mTc-MIBI in 46 patients
32 Heart-to-Organ Count Ratio Qualitative analyses ofimages acquired of 99mTc-N-DBODC5 both at rest andduring stress revealed no significant overlap between traceraccumulation in the inferior wall of the ventricle and in thesubdiaphragmatic region (Figure 2)
Figure 3 depicts the heart-to-liver count ratios (a) andheart-to-intestine count ratios (b) of 99mTc-N-DBODC5 and
99mTc-MIBI in 46 patientsThemyocardium-to-liver ratios of99mTc-N-DBODC5 and 99mTc-MIBI studies were 097 plusmn 007and 051 plusmn 002 respectively at stress The myocardium-to-liver ratios of 99mTc-N-DBODC5 and 99mTc-MIBI MPI were078 plusmn 004 and 062 plusmn 001 respectively at rest On theother hand the mean heart-to-intestine ratios of 99mTc-N-DBODC5 were 212 plusmn 001 and 136 plusmn 002 for stress and
BioMed Research International 5
(a) (b)
(c)
Figure 4 Abnormal MPI in the vertical long-axis slices of a representative patient Both 99mTc-N-DBODC5 (a) and 99mTc-MIBI (b) imagesdemonstrate an inferoposterior defect (white arrows) The defect is well visualized on two tracer images corresponding to the CA resultThis coronary angiography (c) detected a stenosis of 90 in the RCA The concordance for diagnosis of myocardial ischemia was seen on99mTc-N-DBODC5 and 99mTc-MIBI studies
rest images respectivelyThe average heart-to-intestine ratiosof 99mTc-MIBI were 162 plusmn 001 and 091 plusmn 000 for stressand rest images respectively 99mTc-N-DBODC5 studies hada significantly higher heart-to-organ count ratio comparedwith 99mTc-MIBI studies (119875 lt 005)
33 Image Quality In the stress perfusion imaging 99mTc-N-DBODC5MPI was superior in quality to 99mTc-MIBIMPI in37 of the 46 patients studied In the remaining nine patientsthe MPI was judged to be of equal quality In the restingperfusion imaging 99mTc-N-DBODC5 images were superiorin all the patients studied In general the 99mTc-N-DBODC5MPI had more counts with less statistical noise less traceractivity below the diaphragm and desirable heart-to-organcount ratio compared with 99mTc-MIBI MPI
34 Gated SPECT Findings Table 2 shows the results ofscan segments between the 99mTc-N-DBODC5 and 99mTc-MIBI MPI Of the 782 segments that could be interpretedby both techniques 302 were concordantly normal 119 wereconcordantly reversible and 136 were concordantly nonre-versible 99mTc-N-DBODC5SPECTdetectedmore reversibledefects than did 99mTc-MIBI SPECT (240 versus 140 119875 lt005 McNemar test) 99mTc-MIBI SPECT identified more
nonreversible defects than did 99mTc-N-DBODC5 SPECT(312 versus 152 119875 lt 0001 McNemar test) Seventy-onesegments interpreted as normal on 99mTc-N-DBODC5 cor-responded to nonreversible defects on 99mTc-MIBI SPECTimages In contrast 12 normal 99mTc-MIBI segments cor-responded to nonreversible defects on 99mTc-N-DBODC5images When the patterns of uptake (normal reversibledefect and nonreversible defect) of 99mTc-N-DBODC5 and99mTc-MIBI were compared there was concordance in 71(557782) of segments
Table 3 shows the results of left ventricular functionparameters in the two techniques used In this study theend-diastolic volume (EDV) end-systolic volume (ESV) leftventricular ejection fraction (LVEF) and transient ventric-ular dysfunction (TID) were assessed by MPI using twotracers No statistically significant differences in MPI param-eters were observed between the 99mTc-MIBI and 99mTc-N-DBODC5 studies However the scores of myocardialperfusion defects for the detection of CAD were higher with99mTc-MIBI than with 99mTc-N-DBODC5 (119875 = 0012 forSSS 119875 = 0020 for SDS resp)
35 Detection of CAD Table 4 shows the sensitivity andspecificity of two tracers in diagnosing CAD Based on CA
6 BioMed Research International
Table 2 The comparison of myocardial perfusion in a total of 782 segments with 99mTc-N-DBODC5 and 99mTc-MIBI SPECT exerciseimaging
99mTc-N-DBODC599mTc-MIBI Total
Normal Reversible defect Nonreversible defectlowast
Normal 302 (39) 17 (2) 71 (9) 390Reversible defectlowast 16 (2) 119 (15) 105 (13) 240Nonreversible defect 12 (2) 4 (1) 136 (17) 152Total 330 140 312 782Data are presented as number lowast119875 lt 0001 99mTc-MIBI versus 99mTc-N-DBODC5 for nonreversible defect segments lowast119875 lt 005 99mTc-N-DBODC5 versus99mTc-MIBI for reversible defect segments McNemar test was used
Table 3 MPI findings of two tracers on left ventricular functionparameters and ischemia scores in 46 patients
Parameter 99mTc-MIBI 99mTc-N-DBODC5LVEF ()
Exercise 542 plusmn 113 567 plusmn 92Rest 631 plusmn 85 648 plusmn 79
EDV (mL)Exercise 815 plusmn 186 832 plusmn 163Rest 973 plusmn 164 991 plusmn 137
ESV (mL)Exercise 432 plusmn 97 414 plusmn 123Rest 594 plusmn 136 602 plusmn 98
SSS 121 plusmn 14995333 96 plusmn 16SRS 72 plusmn 08 79 plusmn 09SDS 42 plusmn 05995333 36 plusmn 04TID 096 plusmn 006 094 plusmn 002Data are presented asmeanplusmn SD or number () as appropriate995333statisticallysignificant 99mTc-MIBI versus 99mTc-N-DBODC5 (119875 lt 005) pairedStudentrsquos 119905-test was used LVEF left ventricular ejection fraction EDVend-diastolic volume ESV end-systolic volume SSS summed stress scoresSRS summed rest scores SDS summed difference scores TID transientventricular dysfunction
overall figures for sensitivity and specificity in identificationof CAD were 86 (2529) and 65 (1117) for 99mTc-MIBI imaging On the other hand the overall sensitivityand specificity for the detection of CAD were 86 (2529)and 88 (1517) for 99mTc-N-DBODC5 SPECT studies Theconcordance of ischemia diagnosis sensitivity of a represen-tative patient for the two tracers is shown in Figure 4 Theaccuracy was 078 for 99mTc-MIBI and 087 for 99mTc-N-DBODC5 Angiography agreement was very good for 99mTc-N-DBODC5 (120581 = 073) and moderate for 99mTc-MIBI (120581 =052) Specificity and accuracy were not significantly differentbut better for the 99mTc-N-DBODC5 group when comparedto 99mTc-MIBI SPECT (specificity 88-65 accuracy 87-78)
36 Detection of Disease in Individual Coronary VesselsTable 4 also shows the sensitivity and specificity of the twotracers in detecting individual-stenosed vessels Of a total of138 arteries in 46 patients 48 arteries had significant stenosesand 90 had insignificant lesions or were normal Overall
figures for sensitivity and specificity in identifying individual-stenosed vessels were 67 (3248) and 86 (7790) for 99mTc-MIBI imaging overall sensitivity and specificity to diagnoseindividual significantly stenosed vessels were 69 (3348)and 92 (8390) for 99mTc-N-DBODC5 SPECT studies
On the other hand sensitivity and specificity for RCAstenosis vessel lesion detection using 99mTc-MIBI MPI were87 and 68 compared to 87 and 87 for 99mTc-N-DBODC5 MPI LAD stenosis (53 sensitivity and 96specificity for 99mTc-MIBI 63 sensitivity and 96 speci-ficity for 99mTc-N-DBODC5 resp) and left circumflex(LCX) (64 sensitivity and 94 specificity for 99mTc-MIBI57 sensitivity and 94 specificity for 99mTc-N-DBODC5resp) Angiography agreement was very good for 99mTc-N-DBODC5 (120581 = 063 for LAD 120581 = 071 for RCA resp) andmoderate for 99mTc-MIBI (120581 = 052 for LAD 120581 = 048 forRCA resp) In contrast the angiography agreement was verygood for 99mTc-MIBI (120581 = 062 for LCX) and moderate for99mTc-N-DBODC5 (120581 = 055 for LCX) (Table 4) Overall thespecificity of 99mTc-N-DBODC5 SPECT to detect individualRCA stenosis was better (2731 87) than that of 99mTc-MIBISPECT (2131 68) despite having no statistical significance
4 Discussion
These preliminary results demonstrate that stress-restmyocardial perfusion SPECT with 99mTc-N-DBODC5 isa sensitive method for detecting CAD and identifyingstenosed coronary arteries For the detection of CADmore importantly 99mTc-N-DBODC5 MPI reached goodagreement compared with CA (120581 = 073)
41 Advantages of 99119898Tc-N-DBODC5 99mTc-N-DBODC5 isa new lipophilic monocationic and nitride 99mTc-labeledtracer that is rapidly cleared from the liver after intravenousinjection It possesses good stability under physiological con-ditions Importantly 99mTc-N-DBODC5 exhibits more rapidliver washout than either 99mTc-MIBI or 99mTc-tetrofosminFor example at 60min after injection in rats the heartliverratio of 99mTc-N-DBODC5 is approximately ten times higherthan that of 99mTc-MIBI or 99mTc-tetrofosmin Preclinicalstudies have shown that 99mTc-N-DBODC5 SPECT canidentify previous ischemia as areas of reduced tracer uptake[25 26] Furthermore the rapid liver clearance and highuptake in the myocardium of 99mTc-N-DBODC5 will allow
BioMed Research International 7
Table 4 Sensitivity specificity and diagnostic accuracy of scintigraphic perfusion studies and agreement with coronary angiography
Overall LAD LCX RCAMIBI DBODC MIBI DBODC MIBI DBODC MIBI DBODC
No of disease 25 25 10 12 9 8 13 13Sensitivity () 86 86 53 63 64 57 87 87Specificity () 65 88 96 96 94 94 68 87Accuracy () 78 87 78 83 85 83 74 87998771Kappa (120581) 053 073 052 063 062 055 048 071Data are presented as number () MIBI = 99mTc-MIBI DBODC = 99mTc-N-DBODC5 LAD left anterior descending coronary artery LCX left circumflexcoronary artery RCA right coronary artery 998771CA was used as the ldquogold standardrdquo for the calculation of the 120581 which is determine between SPECT MPI andCA If there is no agreement 120581 = 020ndash039 moderate agreement 120581 = 040ndash059 very good agreement 120581 = 060ndash079 excellent agreement 120581 = 080ndash100
SPECT images of the left ventricle to be acquired earlyand with excellent quality [22] The ratios of heart-to-liverwere consistent with the previous report study [22] Thesecharacteristics are suitable particularly for patients withsuspected acute coronary syndromes and without diagnosticelectrocardiogram because early diagnosis is needed in suchpatients for timely therapeutic decisionmaking 99mTc-MIBIon the other hand may require a wait time of up to 1 h forimaging
In the present study the heart-to-organ count ratio of99mTc-N-DBODC5 MPI was superior to that of 99mTc-MIBIin 46 patients Compared with 99mTc-MIBI MPI 99mTc-N-DBODC5 MPI had better image quality in most patientsFurthermore in this study exercise stress myocardial imageswere performed 30min after 99mTc-N-DBODC5 injectionand excellent MPI with high contrast was possible
42 Clinical Value of 99119898Tc-N-DBODC5 for the Detection ofCAD This clinical trial assesses the diagnostic value of thisagent to detect CAD comparing it with stress 99mTc-MIBIMPI and CA
In this study compared with 99mTc-MIBI MPI 99mTc-N-DBODC5MPI indicates the same sensitivity and better speci-ficity and accuracy to detect coronary disease in patientsalthough none of the differences were significant On theother hand more importantly angiography agreement wasvery good for 99mTc-N-DBODC5 (120581 = 073) and moderatefor 99mTc-MIBI (120581 = 052) thus compared with 99mTc-MIBI MPI it provides a high degree of concordance for theevaluation of CAD specifically in excluding perfusion abnor-malities in patients with suspected CAD Possible reasons forthis difference may be fast liver clearance favorable heart-to-organ ratio and high image quality 99mTc-N-DBODC5with rapid liver clearancemay significantly reduce the photonscatter from the liver into the inferoposterior walls Thisreduces the artifactual decreased myocardial perfusion andimproves the diagnostic accuracy for the detection of CADcompared with other 99mTc-labeled perfusion agents [24]
Unsurprisingly Braat et al [35] and Germano et al [36]noted that technetium-labeled MPI agents with a fast liverclearance can significantly reduce the photon scatter fromthe liver into the inferior walls but the radioactivity may betransferred to the gastrointestinal area and increased bowel
and gastric activity were seen as a problem associated withhigh liver uptake in the visual and quantitative interpretationof the inferoposterior myocardial walls In this study boweluptakewas frequently seen on the 99mTc-N-DBODC5 imagesbut did not result in any nondiagnostic scans
For the detection of coronary disease in patients 99mTc-MIBI produced abnormal results for MPI in four patientswho had no angiographically detected stenosis Some of thesefalse-positive results may be due in part to the liver-to-heart artifacts In this study we could classify fixed perfusiondefects as soft-tissue attenuation artifacts or infarcts by usinggated SPECT Because an artifactual defect would shownormal contraction (wall motion or thickening) on a gatedimage artifacts can be differentiated from a true infarct [37]
For the detection of individual vessel stenosis on theother hand angiography agreement was very good for 99mTc-N-DBODC5 (120581=071 for RCA) andmoderate for 99mTc-MIBI(120581 = 048 for RCA) For LAD and LCX arteries stenosis thediagnosis of myocardial ischemia on 99mTc-N-DBODC5 and99mTc-MIBI study had the same specificity and it was similarto that of two tracer to diagnose sensitivity and accuracy ofmyocardial ischemia Abnormal results of myocardial imagesin individual RCA vessel stenosis (six arteries-stenosed ves-sels for RCA) were obtained in the 99mTc-MIBI studieswhile CA and 99mTc-N-DBODC5 studies showed normalfindings in the same individual RCA vessel territories Someof these false-positive results may be due to photon scatterfrom the liver and intestine into the inferoposterior walls99mTc-MIBI concentration located below the left diaphragm(ie liver and bowel) may cause an artifactual perfusiondefect in the adjacent myocardial a phenomenon knownas the ldquoliver-heart artifactrdquo [36 38] Moreover the inferiorand inferoposterior regions were dominated mainly by RCAterritories corresponding to the myocardial short axis andvertical long axis while arteries regions which LAD and LCXdominated were less interfered from ldquoliver-heart artifactrdquoFinally for clinical applications 99mTc-N-DBODC5 offersbetter determination of detects particularly in the infero-posterior wall on myocardial images A typical example of afalse-positive perfusion defect in the inferior wall is shown inFigure 5
On a segment-to-segment basis complete agreementbetween the two imaging agents occurred in 71 of segments
8 BioMed Research International
(a) (b) (c)
Figure 5 Serial short-axis and vertical long-axis slices of stress-rest 99mTc-N-DBODC5 images (b) and stress-rest 99mTc-MIBI images (c) ofa representative patient with normal CA (a) Because of intense uptake of technetium 99mTc-MIBI in the liver high liver background activitycan be observed Furthermore a false-positive myocardial perfusion defect was also seen in the inferoposterior wall segments supplied bythe RCA territory (white arrows) Importantly however at stress and rest the inferoposterior wall segments of 99mTc-N-DBODC5 imagesare clearly separated from the subdiaphragmatic activity
However more myocardial segments were nonreversible on99mTc-MIBI images than on 99mTc-N-DBODC5 images Onthe contrary 99mTc-N-DBODC5MPI had a higher reversibledefect than that of 99mTc-MIBI A possible reason for thisdifference may be due in part to the ldquoliver-heart artifactrdquoThe presence of high liver activity adjacent to the inferior wallresults fromoversubtraction of activity from the inferior wallTherefore the more ldquoliver-heart artifactrdquo in the inferoposte-rior wall on myocardial images the more false nonreversibledefects in the inferoposterior wall on myocardial perfusionsegmental analysis In other words the less reversible defectsin the inferoposterior wall were deduced on 99mTc-MIBIMPIsegmental analysis
More importantly however the main advantage andclinical value of 99mTc-N-DBODC5 can improve diagnosticspecificity and reduce the false-positive diagnosis of patientsand associated treatment fees
5 Limitations
In this study we did not attempt to assess the absolute diag-nostic accuracy of 99mTc-N-DBODC5 because definitive
conclusions in this regard can only be drawn by study-ing larger patient cohort In addition although 99mTc-N-DBODC5 did not track flow as well as 201Tl the magni-tudes of the pharmacologic stress-induced perfusion defectswere comparable to those previously reported for 99mTc-tetrofosmin Thus direct comparison between 99mTc-N-DBODC5 and 99mTc-tetrofosmin should be further provedin the same patient population Overall 99mTc-N-DBODC5MPI will become an important diagnostic tool in the evalua-tion of myocardial perfusion
6 Conclusion
This preliminary clinical study showed that 99mTc-N-DBODC5 and 99mTc-MIBI MPI provide comparable diag-nostic information for patients undergoing exercise rest fordetection of CAD In addition 99mTc-N-DBODC5 doesnot exhibit the disadvantages of 99mTc-MIBI in this studyBy contrast because of its high heart-organ count ratioin comparison to 99mTc-MIBI it improves high degree ofdiagnostic concordance in defining or excluding perfusionabnormalities in patients with CADTherefore it can become
BioMed Research International 9
the agent of choice for the evaluation ofmyocardial perfusionand ventricular function in patients with CAD
Abbreviations
CAD Coronary artery diseaseMPI Myocardial perfusion imagingCA Coronary angiographySPECT Single-photon emission computed
tomographyPET Positron emission computed
tomography99mTc-MIBI Technetium 99m sestamibi99mTc-N-DBODC5 99mTc(N)(DBODC)(PNP5)201Tl Thallium-20199mTc-tetrofosmin Technetium-99m-tetrofosminROI Regions of interestLAD Left anterior descending arteryLCX Left circumflex arteryRCA Right coronary arterySSS Summed stress scoreSRS Summed rest scoreSDS Summed difference scoreEDV End-diastolic volumeESV End-systolic volumeLVEF Left ventricular ejection fraction
Ethics Statement
This study was conducted in accordance with the HelsinkiDeclaration All subjects provided written informed consentbefore MPI acknowledging that they understood their rightsand obligations This study was approved by the ResearchEthics Committee of Shanxi Medical University
Conflict of Interests
The authors declare that they have no conflict of interest
Acknowledgments
This research is partly supported by Grants from the YouthScience and Technology Research Foundation of ShanxiProvince (no 2009021043-3) The authors acknowledge themembers of the participating staff for their contribution tothis clinical study
References
[1] National Hospital Discharge Survey National Health StatisticsReport no 5 2006
[2] J He D Gu X Wu et al ldquoMajor causes of death among menand women in Chinardquo The New England Journal of Medicinevol 353 no 11 pp 1124ndash1134 2005
[3] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardized myocardial sementation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare pro-fessionals from the Cardiac Imaging Committee of the Council
on Clinical Cardiology of the American Heart AssociationrdquoCirculation vol 105 no 4 pp 539ndash542 2002
[4] R J Gibbons J Abrams K Chatterjee et al ldquoACCAHA 2002guideline update for the management of patients with chronicstable anginamdashsummary article a report of the AmericanCollege of CardiologyAmerican Heart Association Task Forceon Practice Guidelines (Committee on the Management ofPatients With Chronic Stable Angina)rdquo Journal of the AmericanCollege of Cardiology vol 41 no 1 pp 159ndash168 2003
[5] WWijns P Kolh N Danchin et al ldquoGuidelines on myocardialrevascularizationrdquo European Heart Journal vol 31 pp 2501ndash2555 2010
[6] J M Jensen K A Oslashvrehus L H Nielsen J K Jensen HM Larsen and B L Noslashrgaard ldquoParadigm of pretest riskstratification before coronary computed tomographyrdquo Journalof Cardiovascular Computed Tomography vol 3 no 6 pp 386ndash391 2009
[7] N RMollet F Cademartiri C VanMieghem et al ldquoAdjunctivevalue of CT coronary angiography in the diagnostic work-up ofpatients with typical angina pectorisrdquo European Heart Journalvol 28 no 15 pp 1872ndash1878 2007
[8] R G E J Groutars J F Verzijlbergen M M C Tiel-Van Buulet al ldquoThe accuracy of 1-day dual-isotopemyocardial SPECT ina population with high prevalence of coronary artery diseaserdquoInternational Journal of Cardiovascular Imaging vol 19 no 3pp 229ndash238 2003
[9] M R Patel E D Peterson D Dai et al ldquoLow diagnostic yieldof elective coronary angiographyrdquo The New England Journal ofMedicine vol 362 no 10 pp 886ndash895 2010
[10] ldquoPharmacologic stress testingrdquo in Nuclear Cardiac ImagingPriniciples and Applications A E Iskandrian and E V GarciaEds pp 293ndash315 OxfordUniversity Press NewYork NY USA4th edition 2008
[11] R R Russell III and B L Zaret ldquoNuclear cardiology presentand futurerdquo Current Problems in Cardiology vol 31 no 9 pp557ndash629 2006
[12] G Germano H Kiat P B Kavanagh et al ldquoAutomatic quan-tification of ejection fraction from gated myocardial perfusionSPECTrdquo Journal of Nuclear Medicine vol 36 no 11 pp 2138ndash2147 1995
[13] S R Underwood C Anagnostopoulos M Cerqueira et alldquoMyocardial perfusion scintigraphy the evidencerdquo EuropeanJournal of Nuclear Medicine and Molecular Imaging vol 31 pp261ndash291 2004
[14] J Heo and A S Iskandrian ldquoTechnetium-labeled myocardialperfusion agentsrdquo Cardiology Clinics vol 12 no 2 pp 187ndash1981994
[15] B L Zaret P Rigo F J T Wackers et al ldquoMyocardial perfusionimaging with 99mTc tetrofosmin comparison to 201Tl imagingand coronary angiography in a phase III multicenter trialrdquoCirculation vol 91 no 2 pp 313ndash319 1995
[16] J J Mahmarian and M S Verani ldquoExercise thallium-201perfusion scintigraphy in the assessment of coronary arterydiseaserdquoAmerican Journal of Cardiology vol 67 no 14 pp 2Dndash11D 1991
[17] D D Miller L T Younis B R Chaitman and H StratmannldquoDiagnostic accuracy of dipyridamole technetium 99m-labeledsestamibi myocardial tomography for detection of coronaryartery diseaserdquo Journal of Nuclear Cardiology vol 4 no 1 pp18ndash24 1997
10 BioMed Research International
[18] Z He A S Iskandrian N C Gupta and M S Verani ldquoAssess-ing coronary artery disease with dipyridamole technetium-99m-tetrofosmin SPECT amulticenter trialrdquo Journal of NuclearMedicine vol 38 no 1 pp 44ndash48 1997
[19] A Boschi C Bolzati L Uccelli et al ldquoA class of asymmetricalnitrido 99mTc heterocomplexes as heart imaging agents withimproved biological propertiesrdquoNuclearMedicine Communica-tions vol 23 no 7 pp 689ndash693 2002
[20] A Boschi L Uccelli C Bolzati et al ldquoSynthesis and biologicevaluation of monocationic asymmetric 99mTc-nitride hetero-complexes showing high heart uptake and improved imagingpropertiesrdquo Journal of Nuclear Medicine vol 44 no 5 pp 806ndash814 2003
[21] C Bolzati M Cavazza-Ceccato S Agostini S TokunagaD Casara and G Bandoli ldquoSubcellular distribution andmetabolism studies of the potential myocardial imaging agent[99mTc(N)(DBODC)(PNP5)]+rdquo Journal of Nuclear Medicinevol 49 no 8 pp 1336ndash1344 2008
[22] C Cittanti L Uccelli M Pasquali et al ldquoWhole-body biodis-tribution and radiation dosimetry of the new cardiac tracer99mTc-N-DBODCrdquo Journal of Nuclear Medicine vol 49 no 8pp 1299ndash1304 2008
[23] K Hatada L M Riou M Ruiz et al ldquo99mTc-N-DBODC5a new myocardial perfusion imaging agent with rapid liverclearance comparison with 99mTc-sestamibi and 99mTc-tetrofosmin in ratsrdquo Journal of Nuclear Medicine vol 45 no 12pp 2095ndash2101 2004
[24] T Takeda J Wu and T T Lwin ldquo99mTc-N-DBODC5 a novelmyocardial perfusion imaging agent for diagnosis of coronaryartery disease a reviewrdquo Recent Patents on Cardiovascular DrugDiscovery vol 1 no 2 pp 161ndash166 2006
[25] K Hatada M Ruiz L M Riou et al ldquoOrgan biodistributionand myocardial uptake washout and redistribution kinetics ofTc-99m N-DBODC5 when injected during vasodilator stressin canine models of coronary stenosesrdquo Journal of NuclearCardiology vol 13 no 6 pp 779ndash790 2006
[26] W Zhang W Fang B Li X Wang and Z He ldquoExperimentalstudy of [99mTc(PNP5) (DBODC)]+ as a new myocardialperfusion imaging agentrdquo Cardiology vol 112 no 2 pp 89ndash972009
[27] M E Marmion S R Woulfe W L Neumann D L Nosco andE Deutsch ldquoPreparation and characterization of technetiumcomplexes with Schiff base and phosphine coordination 1Complexes of technetium-99g and -99m with substitutedacac2en and trialkyl phosphines (where acac2en = NN1015840-ethylenebis[acetylacetone iminato])rdquo Nuclear Medicine andBiology vol 26 no 7 pp 755ndash770 1999
[28] C Bolzati L Uccelli A Boschi et al ldquoSynthesis of a novel classof nitrido Tc-99m radiopharmaceuticals with phosphino-thiolligands showing transient heart uptakerdquo Journal of InorganicBiochemistry vol 78 no 3 pp 369ndash374 2000
[29] M J Henzlova M D Cerqueira J J Mahmarian and S YaoldquoStress protocols and tracersrdquo Journal of Nuclear Cardiology vol13 no 6 pp e80ndashe90 2006
[30] C L Hansen R A Goldstein D S Berman et al ldquoMyocardialperfusion and function single photon emission computedtomographyrdquo Journal of Nuclear Cardiology vol 13 no 6 ppe97ndashe120 2006
[31] P Flamen A Bossuyt and P R Franken ldquoTechnetium-99m-tetrofosmin in dipyridamole-stressmyocardial SPECT imagingintraindividual comparison with technetium-99m-sestamibirdquoJournal of Nuclear Medicine vol 36 no 11 pp 2009ndash2015 1995
[32] N Tamaki N Takahashi M Kawamoto et al ldquoMyocardialtomography using technetium-99m-tetrofosmin to evaluatecoronary artery diseaserdquo Journal of Nuclear Medicine vol 35no 4 pp 594ndash600 1994
[33] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardizedmyocardial segmentation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare profes-sionals from the Cardiac Imaging Committee of the Councilon Clinical Cardiology of the American Heart AssociationrdquoJournal of Nuclear Cardiology vol 9 no 2 pp 240ndash245 2002
[34] T Sharir G Germano X Kang et al ldquoPrediction of myocardialinfarction versus cardiac death by gated myocardial perfusionSPECT risk stratification by the amount of stress-inducedischemia and the poststress ejection fractionrdquo Journal of NuclearMedicine vol 42 no 6 pp 831ndash837 2001
[35] S H Braat B Leclercq R Itti A Lahiri B Sridhara and PRigo ldquoMyocardial imaging with technetium-99m-tetrofosmincomparison of one-day and two-day protocolsrdquo Journal ofNuclear Medicine vol 35 no 10 pp 1581ndash1585 1994
[36] G Germano T Chua H Kiat J S Areeda andD S Berman ldquoAquantitative phantom analysis of artifacts due to hepatic activ-ity in technetium-99m myocardial perfusion SPECT studiesrdquoJournal of Nuclear Medicine vol 35 no 2 pp 356ndash359 1994
[37] A K Paul andH A Nabi ldquoGatedmyocardial perfusion SPECTbasic principles technical aspects and clinical applicationsrdquoJournal of Nuclear Medicine Technology vol 32 no 4 pp 179ndash187 2004
[38] J Nuyts P Dupont V Van den Maegdenbergh S Vleugels PSuetens and L Mortelmans ldquoA study of the liver-heart artifactin emission tomographyrdquo Journal of Nuclear Medicine vol 36no 1 pp 133ndash139 1995
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 BioMed Research International
is different from the morphological information providedby CA [12] Furthermore CA is the standard techniquefor assessing epicardial coronary anatomy and MPI is thestandard technique for assessing myocardial perfusion andis appropriate for the quantitative evaluation of myocardialperfusion conditions [13]
Thallium-201 (201Tl) technetium 99m sestamibi (99mTc-MIBI) and technetium99m tetrofosmin (99mTc-tetrofosmin)are three traditional routinely used MPI tracers and areclinical-validated tracers for evaluation of SPECT MPI [14ndash16] Because 201Tl is a cyclotron-produced isotope it isexpensive and it is not easily available for routine clinicaluse inmany developing countriesTherefore from a practicalstandpoint 99mTc-MIBI or 99mTc-tetrofosmin is the preferredagent for a gated SPECT study However tracer activitybelow the diaphragm is commonly seen with 99mTc-MIBIand 99mTc-tetrofosmin and this can reduce accuracy in somestudies [17 18]
Recently 99mTc-N-DBODC5 with a faster liver clearancethan conventional SPECT imaging agents has been intro-duced It is a new lipophilic monocationic 99mTc-labeledcompound that is currently under clinical investigation asa MPI agent [19ndash24] Basic research and phase I studieshave shown the safety excellent biodistribution and highimage quality of this radiopharmaceutical [22 25 26] Like99mTc-MIBI and 99mTc-tetrofosmin 99mTc-N-DBODC5 alsoa monocationic lipophilic complex is possibly localized inthe mitochondrial fraction Marmion et al [27] and Bolzatiet al [28] reported that the lipophilic characteristics andelectronic charge of the tracer were thought to be importantImportantly however the clinical value of diagnosis of CADhas not been fully explored
In order to evaluate the clinical value of this agent thefindings of stress and restMPI after the administration of thisagent were compared to those of stress and rest 99mTc-MIBIMPI as well as those of CA with respect to the detection ofCAD
2 Methods
21 Patient Population Of 120 patients admitted to thehospital because of chest pain fromMarch 2010 to December2011 46 (31 males mean age 6008plusmn858 years (Table 1)) whounderwent stress-rest 99mTc-N-DBODC5 SPECT 99mTc-MIBI SPECT and coronary arteriography were included inthis study If the creatine kinase concentration was morethan twice the upper normal limit or there was positivetroponin T or if there was evidence of previous myocardialinfarction coronary angioplasty or a coronary artery bypassgraft surgery the patients were excluded
22 Preparation of 99119898Tc-N-DBODC5 99mTc-N-DBODC5was prepared using a lyophilized kit formulation purchasedfrom Beijing Shihong Pharmaceutical Center The salinesolution of sodium pertechnetate (10mL 1110MBq) wasadded to an SDH vial (Vail A 50mg of succinate dehydro-genase 50mg of 12-diaminopropane-NNN1015840N1015840-tetraaceticacid and 005mg of SnCl
2sdot2H2O) Then the solution was
Table 1 Study group
Parameter Value119899 46MF 3115Age (yr) 6008 plusmn 858 (39ndash74)Hypertension 31Hyperlipidemia 19Diabetes mellitus 14Smoking 26Trigger of chest pain
Effort 22Rest 13Not specific 11
ECG abnormality 11ST-T elevation 3ST-T depression 8ge50 of luminal narrowing 29One-vessel disease 14Two-vessel disease 11Three-vessel disease 4Data are presented as mean plusmn SD or number () as appropriate
kept at room temperature for 15min to form a [99mTcN]2+intermediate The other two lyophilized vials (Vail B 20mgof PNP5 Vail C 20mg of DBODC) were dissolved with10mL of saline solution respectively And then the salinesolutions ofVails B andCwere added to the vial of [99mTcN]2+intermediate (Vail A) The resulting solution was heated at100∘C for 15min Before injection the solution was filtratedthrough a 022-120583mmembraneThe 99mTc-MIBI was obtainedusing a lyophilized kit formulation (Beijing Shihong Phar-maceutical Center) in the First Affiliated Hospital of ShanxiMedical University
Radiochemical purity (RCP) was determined by thin-layer chromatography (TLC) TLC was conducted onpolyamide film as the station phase and salineacetone (v v= 6 1) as the mobile phase Retention factor (Rf) for 99mTc-N-DBODC5 is 03ndash06 The RCP was more than 95 in eachexperimental study and the purity was still greater than 95at least 6 h
23 Exercise Protocol Figure 1 shows that a two-day proto-col was used for both 99mTc-MIBI and 99mTc-N-DBODC5MPI Image acquisition procedures conformed to the ASNCimaging guidelines [29 30] and the aged-adjusted max-imal heart rate was the endpoint on an ergometer butother endpoints included physical exhaustion uncommonarrhythmia severe angina or significant hypotension At theendpoint of the symptom-limited bicycle ergometer exer-cise 740MBq of 99mTc-N-DBODC5 (mean injected activity7408 plusmn 111MBq) was injected exercise was continued fora further 2min
Each patient underwent an exercise 99mTc-MIBI studywithin 7 days of the 99mTc-N-DBODC5 study For the 99mTc-MIBI (7415 plusmn 123MBq) SPECT study the exercise protocol
BioMed Research International 3
Imaging protocols 2-day exercise stressrest
Stress (day 1)
Inject 20ndash25 mCi 1-2 minsprior to peak
Exercise Gated imaging
0 30(mins)
Rest (day 2)Inject
20ndash25 mCiGated imaging
0 60(mins)
Figure 1 99mTc-N-DBODC5 and 99mTc-MIBI imaging protocolstwo-day exercise stressrest
of patients was identical to that for the 99mTc-N-DBODC5study 99mTc-N-DBODC5 and 99mTc-MIBI were used asmyocardial perfusion agents in a random sequence
24 Gated SPECT Acquisition and Image Reconstruction Pa-tients were imaged in the supine position with their armsraised SPECT images were acquired with a fixed 90∘ two-headed gamma camera (Infinia VC Hawkeye General Elec-tric USA) using a low-energy high-resolution parallel-holecollimator from the 45∘ right anterior oblique to the 45∘ leftposterior position Acquisition parameters were as followsdetectors at 90∘ 180∘ rotation at 3∘ steps with automaticbody contouring 35 s acquisition per step 64 times 64 matrixzoom times128 and energy window 140 keV plusmn 10 The totalacquisition time was approximately 20min The same filterswere used for both tracers The raw projection datasetswere filtered with a Butterworth filter (cut off frequency050 cyclespixel and power 60 for rest images cut offfrequency 050 cyclespixel and power 50 for stress images)No scatter or attenuation correction was performed
25 Heart-to-Organ Analysis 99mTc-N-DBODC5 and 99mTc-MIBI heart-to-organ count ratios were calculated from theanterior projection of each tomographic acquisition Regionsof interests (ROIs) were drawn around the entire left ventric-ular myocardium over the hepatic margin adjacent to theinferoapical wall of the left ventricle excluding the biliarytree and over the inferior left ventricular wall adjacent largeintestine activityThemean counts per pixel in the three ROIswere normalized to the injected tracer activity after decaycorrection and to a standard acquisition time of 1min Heart-to-liver and heart-to-intestine ratios were then computed[31]
26 Image Quality Assessing For MPI analyses at firsttwo experienced observers judged which image sets from99mTc-MIBI and 99mTc-N-DBODC5 were superior in imagequality on the basis of patient motion statistical noise traceractivity below the diaphragm heart-to-organ count ratio andsharpness without knowledge of the radiopharmaceutical orpatient identity [32]
27 MPI Image Interpretation Both overall qualitative diag-nosis and semiquantitative 17 segment with 5-point [33] (0= normal 4 = absent tracer uptake) scorings were employedin the independent blinded read by two expert readerswho were experienced in SPECT MPI interpretation In thismodel the left anterior descending artery (LAD) distributionterritory comprises seven segments (segments 1-2 7-8 13-14 and 17) the left circumflex artery (LCX) comprises fivesegments (segments 3-4 9-10 and 15) and the right coronaryartery (RCA) comprises five segments (segments 5-6 11-12and 16) SPECT stressrest studies were classified for eachmyocardial region in the following manner normal if all thesegments were normal after stress ischemic if at least onesegments improved at rest and scar if no segments improvedat rest In addition the summed stress (SSS) summed rest(SRS) and summed difference scores (SDSs) were calculatedand ischemia was defined as SDS ge 2 [34] The 99mTc-MIBIand 99mTc-N-DBODC5 images were separately interpretedwithout knowing the clinical histories results of coronaryangiography or other radionuclide findings
28 Coronary Angiography Interpretation All coronary angi-ograms were interpreted with quantitative CA in a coronaryangiography core laboratory blinded to the clinical or imag-ing results A coronary stenosis was considered present whenthere was a stenosis ge 50 in diameter in any epicardialcoronary artery The presence of one or more coronarystenoses defined the presence of significant CAD
29 Statistical Analysis All statistical analyses were per-formed using the statistical package SPSS 160 (Chicago ILUSA) The results were expressed as the mean value plusmn SDThe difference in left ventricular function parameters andperfusion scores were compared using a paired Studentrsquost-test Comparison of the proportion was made with theMcNemar test CA results were used as the ldquogold standardrdquoAgreements between CA and SPECT results were defined asthe kappa (120581) value 119875 lt 005 was considered significant
3 Results
31 Coronary Angiography Of the 46 patients studied 29had ge50 luminal diameter stenosis in at least one majorcoronary vessel Fourteen had single-vessel disease 11 hadtwo-vessel disease and four had three-vessel disease 15patients showed significant stenosis in the RCA 19 in theLAD and 14 in the LCX The remaining 17 patients hadnormal or nonsignificantly stenosed coronary arteries
4 BioMed Research International
(a) (b)
(c) (d)
Figure 2 Comparison of liver clearance of the two tracers in anterior tomographic planar images of a patient (as shown in the black arrowH heart Lv liver) (a) Exercise stress 99mTc-N-DBODC5 (b) Exercise stress 99mTc-MIBI (c) rest 99mTc-N-DBODC5 and (d) rest 99mTc-MIBI
00
02
04
06
08
10
12
Hea
rt-to
-live
r rat
io
Stress 30 min Rest 60 minTime after injection
99m Tc-N-DBODC599m Tc-MIBI
lowast
P lt 005 versus 99mTc-MIBIlowast
lowast
(a)
Stress 30 min Rest 60 minTime after injection
99m Tc-N-DBODC599m Tc-MIBI
00
05
10
15
20
25
Hea
rt-to
-inte
stine
ratio
lowast
lowast
lowast
P lt 005 versus 99mTc-MIBI
(b)
Figure 3 Heart-to-liver ratio and heart-to-intestine ratiomeasured with an anterior projection images at stress for 30min and rest for 60minfor 99mTc-N-DBODC5 and 99mTc-MIBI in 46 patients
32 Heart-to-Organ Count Ratio Qualitative analyses ofimages acquired of 99mTc-N-DBODC5 both at rest andduring stress revealed no significant overlap between traceraccumulation in the inferior wall of the ventricle and in thesubdiaphragmatic region (Figure 2)
Figure 3 depicts the heart-to-liver count ratios (a) andheart-to-intestine count ratios (b) of 99mTc-N-DBODC5 and
99mTc-MIBI in 46 patientsThemyocardium-to-liver ratios of99mTc-N-DBODC5 and 99mTc-MIBI studies were 097 plusmn 007and 051 plusmn 002 respectively at stress The myocardium-to-liver ratios of 99mTc-N-DBODC5 and 99mTc-MIBI MPI were078 plusmn 004 and 062 plusmn 001 respectively at rest On theother hand the mean heart-to-intestine ratios of 99mTc-N-DBODC5 were 212 plusmn 001 and 136 plusmn 002 for stress and
BioMed Research International 5
(a) (b)
(c)
Figure 4 Abnormal MPI in the vertical long-axis slices of a representative patient Both 99mTc-N-DBODC5 (a) and 99mTc-MIBI (b) imagesdemonstrate an inferoposterior defect (white arrows) The defect is well visualized on two tracer images corresponding to the CA resultThis coronary angiography (c) detected a stenosis of 90 in the RCA The concordance for diagnosis of myocardial ischemia was seen on99mTc-N-DBODC5 and 99mTc-MIBI studies
rest images respectivelyThe average heart-to-intestine ratiosof 99mTc-MIBI were 162 plusmn 001 and 091 plusmn 000 for stressand rest images respectively 99mTc-N-DBODC5 studies hada significantly higher heart-to-organ count ratio comparedwith 99mTc-MIBI studies (119875 lt 005)
33 Image Quality In the stress perfusion imaging 99mTc-N-DBODC5MPI was superior in quality to 99mTc-MIBIMPI in37 of the 46 patients studied In the remaining nine patientsthe MPI was judged to be of equal quality In the restingperfusion imaging 99mTc-N-DBODC5 images were superiorin all the patients studied In general the 99mTc-N-DBODC5MPI had more counts with less statistical noise less traceractivity below the diaphragm and desirable heart-to-organcount ratio compared with 99mTc-MIBI MPI
34 Gated SPECT Findings Table 2 shows the results ofscan segments between the 99mTc-N-DBODC5 and 99mTc-MIBI MPI Of the 782 segments that could be interpretedby both techniques 302 were concordantly normal 119 wereconcordantly reversible and 136 were concordantly nonre-versible 99mTc-N-DBODC5SPECTdetectedmore reversibledefects than did 99mTc-MIBI SPECT (240 versus 140 119875 lt005 McNemar test) 99mTc-MIBI SPECT identified more
nonreversible defects than did 99mTc-N-DBODC5 SPECT(312 versus 152 119875 lt 0001 McNemar test) Seventy-onesegments interpreted as normal on 99mTc-N-DBODC5 cor-responded to nonreversible defects on 99mTc-MIBI SPECTimages In contrast 12 normal 99mTc-MIBI segments cor-responded to nonreversible defects on 99mTc-N-DBODC5images When the patterns of uptake (normal reversibledefect and nonreversible defect) of 99mTc-N-DBODC5 and99mTc-MIBI were compared there was concordance in 71(557782) of segments
Table 3 shows the results of left ventricular functionparameters in the two techniques used In this study theend-diastolic volume (EDV) end-systolic volume (ESV) leftventricular ejection fraction (LVEF) and transient ventric-ular dysfunction (TID) were assessed by MPI using twotracers No statistically significant differences in MPI param-eters were observed between the 99mTc-MIBI and 99mTc-N-DBODC5 studies However the scores of myocardialperfusion defects for the detection of CAD were higher with99mTc-MIBI than with 99mTc-N-DBODC5 (119875 = 0012 forSSS 119875 = 0020 for SDS resp)
35 Detection of CAD Table 4 shows the sensitivity andspecificity of two tracers in diagnosing CAD Based on CA
6 BioMed Research International
Table 2 The comparison of myocardial perfusion in a total of 782 segments with 99mTc-N-DBODC5 and 99mTc-MIBI SPECT exerciseimaging
99mTc-N-DBODC599mTc-MIBI Total
Normal Reversible defect Nonreversible defectlowast
Normal 302 (39) 17 (2) 71 (9) 390Reversible defectlowast 16 (2) 119 (15) 105 (13) 240Nonreversible defect 12 (2) 4 (1) 136 (17) 152Total 330 140 312 782Data are presented as number lowast119875 lt 0001 99mTc-MIBI versus 99mTc-N-DBODC5 for nonreversible defect segments lowast119875 lt 005 99mTc-N-DBODC5 versus99mTc-MIBI for reversible defect segments McNemar test was used
Table 3 MPI findings of two tracers on left ventricular functionparameters and ischemia scores in 46 patients
Parameter 99mTc-MIBI 99mTc-N-DBODC5LVEF ()
Exercise 542 plusmn 113 567 plusmn 92Rest 631 plusmn 85 648 plusmn 79
EDV (mL)Exercise 815 plusmn 186 832 plusmn 163Rest 973 plusmn 164 991 plusmn 137
ESV (mL)Exercise 432 plusmn 97 414 plusmn 123Rest 594 plusmn 136 602 plusmn 98
SSS 121 plusmn 14995333 96 plusmn 16SRS 72 plusmn 08 79 plusmn 09SDS 42 plusmn 05995333 36 plusmn 04TID 096 plusmn 006 094 plusmn 002Data are presented asmeanplusmn SD or number () as appropriate995333statisticallysignificant 99mTc-MIBI versus 99mTc-N-DBODC5 (119875 lt 005) pairedStudentrsquos 119905-test was used LVEF left ventricular ejection fraction EDVend-diastolic volume ESV end-systolic volume SSS summed stress scoresSRS summed rest scores SDS summed difference scores TID transientventricular dysfunction
overall figures for sensitivity and specificity in identificationof CAD were 86 (2529) and 65 (1117) for 99mTc-MIBI imaging On the other hand the overall sensitivityand specificity for the detection of CAD were 86 (2529)and 88 (1517) for 99mTc-N-DBODC5 SPECT studies Theconcordance of ischemia diagnosis sensitivity of a represen-tative patient for the two tracers is shown in Figure 4 Theaccuracy was 078 for 99mTc-MIBI and 087 for 99mTc-N-DBODC5 Angiography agreement was very good for 99mTc-N-DBODC5 (120581 = 073) and moderate for 99mTc-MIBI (120581 =052) Specificity and accuracy were not significantly differentbut better for the 99mTc-N-DBODC5 group when comparedto 99mTc-MIBI SPECT (specificity 88-65 accuracy 87-78)
36 Detection of Disease in Individual Coronary VesselsTable 4 also shows the sensitivity and specificity of the twotracers in detecting individual-stenosed vessels Of a total of138 arteries in 46 patients 48 arteries had significant stenosesand 90 had insignificant lesions or were normal Overall
figures for sensitivity and specificity in identifying individual-stenosed vessels were 67 (3248) and 86 (7790) for 99mTc-MIBI imaging overall sensitivity and specificity to diagnoseindividual significantly stenosed vessels were 69 (3348)and 92 (8390) for 99mTc-N-DBODC5 SPECT studies
On the other hand sensitivity and specificity for RCAstenosis vessel lesion detection using 99mTc-MIBI MPI were87 and 68 compared to 87 and 87 for 99mTc-N-DBODC5 MPI LAD stenosis (53 sensitivity and 96specificity for 99mTc-MIBI 63 sensitivity and 96 speci-ficity for 99mTc-N-DBODC5 resp) and left circumflex(LCX) (64 sensitivity and 94 specificity for 99mTc-MIBI57 sensitivity and 94 specificity for 99mTc-N-DBODC5resp) Angiography agreement was very good for 99mTc-N-DBODC5 (120581 = 063 for LAD 120581 = 071 for RCA resp) andmoderate for 99mTc-MIBI (120581 = 052 for LAD 120581 = 048 forRCA resp) In contrast the angiography agreement was verygood for 99mTc-MIBI (120581 = 062 for LCX) and moderate for99mTc-N-DBODC5 (120581 = 055 for LCX) (Table 4) Overall thespecificity of 99mTc-N-DBODC5 SPECT to detect individualRCA stenosis was better (2731 87) than that of 99mTc-MIBISPECT (2131 68) despite having no statistical significance
4 Discussion
These preliminary results demonstrate that stress-restmyocardial perfusion SPECT with 99mTc-N-DBODC5 isa sensitive method for detecting CAD and identifyingstenosed coronary arteries For the detection of CADmore importantly 99mTc-N-DBODC5 MPI reached goodagreement compared with CA (120581 = 073)
41 Advantages of 99119898Tc-N-DBODC5 99mTc-N-DBODC5 isa new lipophilic monocationic and nitride 99mTc-labeledtracer that is rapidly cleared from the liver after intravenousinjection It possesses good stability under physiological con-ditions Importantly 99mTc-N-DBODC5 exhibits more rapidliver washout than either 99mTc-MIBI or 99mTc-tetrofosminFor example at 60min after injection in rats the heartliverratio of 99mTc-N-DBODC5 is approximately ten times higherthan that of 99mTc-MIBI or 99mTc-tetrofosmin Preclinicalstudies have shown that 99mTc-N-DBODC5 SPECT canidentify previous ischemia as areas of reduced tracer uptake[25 26] Furthermore the rapid liver clearance and highuptake in the myocardium of 99mTc-N-DBODC5 will allow
BioMed Research International 7
Table 4 Sensitivity specificity and diagnostic accuracy of scintigraphic perfusion studies and agreement with coronary angiography
Overall LAD LCX RCAMIBI DBODC MIBI DBODC MIBI DBODC MIBI DBODC
No of disease 25 25 10 12 9 8 13 13Sensitivity () 86 86 53 63 64 57 87 87Specificity () 65 88 96 96 94 94 68 87Accuracy () 78 87 78 83 85 83 74 87998771Kappa (120581) 053 073 052 063 062 055 048 071Data are presented as number () MIBI = 99mTc-MIBI DBODC = 99mTc-N-DBODC5 LAD left anterior descending coronary artery LCX left circumflexcoronary artery RCA right coronary artery 998771CA was used as the ldquogold standardrdquo for the calculation of the 120581 which is determine between SPECT MPI andCA If there is no agreement 120581 = 020ndash039 moderate agreement 120581 = 040ndash059 very good agreement 120581 = 060ndash079 excellent agreement 120581 = 080ndash100
SPECT images of the left ventricle to be acquired earlyand with excellent quality [22] The ratios of heart-to-liverwere consistent with the previous report study [22] Thesecharacteristics are suitable particularly for patients withsuspected acute coronary syndromes and without diagnosticelectrocardiogram because early diagnosis is needed in suchpatients for timely therapeutic decisionmaking 99mTc-MIBIon the other hand may require a wait time of up to 1 h forimaging
In the present study the heart-to-organ count ratio of99mTc-N-DBODC5 MPI was superior to that of 99mTc-MIBIin 46 patients Compared with 99mTc-MIBI MPI 99mTc-N-DBODC5 MPI had better image quality in most patientsFurthermore in this study exercise stress myocardial imageswere performed 30min after 99mTc-N-DBODC5 injectionand excellent MPI with high contrast was possible
42 Clinical Value of 99119898Tc-N-DBODC5 for the Detection ofCAD This clinical trial assesses the diagnostic value of thisagent to detect CAD comparing it with stress 99mTc-MIBIMPI and CA
In this study compared with 99mTc-MIBI MPI 99mTc-N-DBODC5MPI indicates the same sensitivity and better speci-ficity and accuracy to detect coronary disease in patientsalthough none of the differences were significant On theother hand more importantly angiography agreement wasvery good for 99mTc-N-DBODC5 (120581 = 073) and moderatefor 99mTc-MIBI (120581 = 052) thus compared with 99mTc-MIBI MPI it provides a high degree of concordance for theevaluation of CAD specifically in excluding perfusion abnor-malities in patients with suspected CAD Possible reasons forthis difference may be fast liver clearance favorable heart-to-organ ratio and high image quality 99mTc-N-DBODC5with rapid liver clearancemay significantly reduce the photonscatter from the liver into the inferoposterior walls Thisreduces the artifactual decreased myocardial perfusion andimproves the diagnostic accuracy for the detection of CADcompared with other 99mTc-labeled perfusion agents [24]
Unsurprisingly Braat et al [35] and Germano et al [36]noted that technetium-labeled MPI agents with a fast liverclearance can significantly reduce the photon scatter fromthe liver into the inferior walls but the radioactivity may betransferred to the gastrointestinal area and increased bowel
and gastric activity were seen as a problem associated withhigh liver uptake in the visual and quantitative interpretationof the inferoposterior myocardial walls In this study boweluptakewas frequently seen on the 99mTc-N-DBODC5 imagesbut did not result in any nondiagnostic scans
For the detection of coronary disease in patients 99mTc-MIBI produced abnormal results for MPI in four patientswho had no angiographically detected stenosis Some of thesefalse-positive results may be due in part to the liver-to-heart artifacts In this study we could classify fixed perfusiondefects as soft-tissue attenuation artifacts or infarcts by usinggated SPECT Because an artifactual defect would shownormal contraction (wall motion or thickening) on a gatedimage artifacts can be differentiated from a true infarct [37]
For the detection of individual vessel stenosis on theother hand angiography agreement was very good for 99mTc-N-DBODC5 (120581=071 for RCA) andmoderate for 99mTc-MIBI(120581 = 048 for RCA) For LAD and LCX arteries stenosis thediagnosis of myocardial ischemia on 99mTc-N-DBODC5 and99mTc-MIBI study had the same specificity and it was similarto that of two tracer to diagnose sensitivity and accuracy ofmyocardial ischemia Abnormal results of myocardial imagesin individual RCA vessel stenosis (six arteries-stenosed ves-sels for RCA) were obtained in the 99mTc-MIBI studieswhile CA and 99mTc-N-DBODC5 studies showed normalfindings in the same individual RCA vessel territories Someof these false-positive results may be due to photon scatterfrom the liver and intestine into the inferoposterior walls99mTc-MIBI concentration located below the left diaphragm(ie liver and bowel) may cause an artifactual perfusiondefect in the adjacent myocardial a phenomenon knownas the ldquoliver-heart artifactrdquo [36 38] Moreover the inferiorand inferoposterior regions were dominated mainly by RCAterritories corresponding to the myocardial short axis andvertical long axis while arteries regions which LAD and LCXdominated were less interfered from ldquoliver-heart artifactrdquoFinally for clinical applications 99mTc-N-DBODC5 offersbetter determination of detects particularly in the infero-posterior wall on myocardial images A typical example of afalse-positive perfusion defect in the inferior wall is shown inFigure 5
On a segment-to-segment basis complete agreementbetween the two imaging agents occurred in 71 of segments
8 BioMed Research International
(a) (b) (c)
Figure 5 Serial short-axis and vertical long-axis slices of stress-rest 99mTc-N-DBODC5 images (b) and stress-rest 99mTc-MIBI images (c) ofa representative patient with normal CA (a) Because of intense uptake of technetium 99mTc-MIBI in the liver high liver background activitycan be observed Furthermore a false-positive myocardial perfusion defect was also seen in the inferoposterior wall segments supplied bythe RCA territory (white arrows) Importantly however at stress and rest the inferoposterior wall segments of 99mTc-N-DBODC5 imagesare clearly separated from the subdiaphragmatic activity
However more myocardial segments were nonreversible on99mTc-MIBI images than on 99mTc-N-DBODC5 images Onthe contrary 99mTc-N-DBODC5MPI had a higher reversibledefect than that of 99mTc-MIBI A possible reason for thisdifference may be due in part to the ldquoliver-heart artifactrdquoThe presence of high liver activity adjacent to the inferior wallresults fromoversubtraction of activity from the inferior wallTherefore the more ldquoliver-heart artifactrdquo in the inferoposte-rior wall on myocardial images the more false nonreversibledefects in the inferoposterior wall on myocardial perfusionsegmental analysis In other words the less reversible defectsin the inferoposterior wall were deduced on 99mTc-MIBIMPIsegmental analysis
More importantly however the main advantage andclinical value of 99mTc-N-DBODC5 can improve diagnosticspecificity and reduce the false-positive diagnosis of patientsand associated treatment fees
5 Limitations
In this study we did not attempt to assess the absolute diag-nostic accuracy of 99mTc-N-DBODC5 because definitive
conclusions in this regard can only be drawn by study-ing larger patient cohort In addition although 99mTc-N-DBODC5 did not track flow as well as 201Tl the magni-tudes of the pharmacologic stress-induced perfusion defectswere comparable to those previously reported for 99mTc-tetrofosmin Thus direct comparison between 99mTc-N-DBODC5 and 99mTc-tetrofosmin should be further provedin the same patient population Overall 99mTc-N-DBODC5MPI will become an important diagnostic tool in the evalua-tion of myocardial perfusion
6 Conclusion
This preliminary clinical study showed that 99mTc-N-DBODC5 and 99mTc-MIBI MPI provide comparable diag-nostic information for patients undergoing exercise rest fordetection of CAD In addition 99mTc-N-DBODC5 doesnot exhibit the disadvantages of 99mTc-MIBI in this studyBy contrast because of its high heart-organ count ratioin comparison to 99mTc-MIBI it improves high degree ofdiagnostic concordance in defining or excluding perfusionabnormalities in patients with CADTherefore it can become
BioMed Research International 9
the agent of choice for the evaluation ofmyocardial perfusionand ventricular function in patients with CAD
Abbreviations
CAD Coronary artery diseaseMPI Myocardial perfusion imagingCA Coronary angiographySPECT Single-photon emission computed
tomographyPET Positron emission computed
tomography99mTc-MIBI Technetium 99m sestamibi99mTc-N-DBODC5 99mTc(N)(DBODC)(PNP5)201Tl Thallium-20199mTc-tetrofosmin Technetium-99m-tetrofosminROI Regions of interestLAD Left anterior descending arteryLCX Left circumflex arteryRCA Right coronary arterySSS Summed stress scoreSRS Summed rest scoreSDS Summed difference scoreEDV End-diastolic volumeESV End-systolic volumeLVEF Left ventricular ejection fraction
Ethics Statement
This study was conducted in accordance with the HelsinkiDeclaration All subjects provided written informed consentbefore MPI acknowledging that they understood their rightsand obligations This study was approved by the ResearchEthics Committee of Shanxi Medical University
Conflict of Interests
The authors declare that they have no conflict of interest
Acknowledgments
This research is partly supported by Grants from the YouthScience and Technology Research Foundation of ShanxiProvince (no 2009021043-3) The authors acknowledge themembers of the participating staff for their contribution tothis clinical study
References
[1] National Hospital Discharge Survey National Health StatisticsReport no 5 2006
[2] J He D Gu X Wu et al ldquoMajor causes of death among menand women in Chinardquo The New England Journal of Medicinevol 353 no 11 pp 1124ndash1134 2005
[3] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardized myocardial sementation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare pro-fessionals from the Cardiac Imaging Committee of the Council
on Clinical Cardiology of the American Heart AssociationrdquoCirculation vol 105 no 4 pp 539ndash542 2002
[4] R J Gibbons J Abrams K Chatterjee et al ldquoACCAHA 2002guideline update for the management of patients with chronicstable anginamdashsummary article a report of the AmericanCollege of CardiologyAmerican Heart Association Task Forceon Practice Guidelines (Committee on the Management ofPatients With Chronic Stable Angina)rdquo Journal of the AmericanCollege of Cardiology vol 41 no 1 pp 159ndash168 2003
[5] WWijns P Kolh N Danchin et al ldquoGuidelines on myocardialrevascularizationrdquo European Heart Journal vol 31 pp 2501ndash2555 2010
[6] J M Jensen K A Oslashvrehus L H Nielsen J K Jensen HM Larsen and B L Noslashrgaard ldquoParadigm of pretest riskstratification before coronary computed tomographyrdquo Journalof Cardiovascular Computed Tomography vol 3 no 6 pp 386ndash391 2009
[7] N RMollet F Cademartiri C VanMieghem et al ldquoAdjunctivevalue of CT coronary angiography in the diagnostic work-up ofpatients with typical angina pectorisrdquo European Heart Journalvol 28 no 15 pp 1872ndash1878 2007
[8] R G E J Groutars J F Verzijlbergen M M C Tiel-Van Buulet al ldquoThe accuracy of 1-day dual-isotopemyocardial SPECT ina population with high prevalence of coronary artery diseaserdquoInternational Journal of Cardiovascular Imaging vol 19 no 3pp 229ndash238 2003
[9] M R Patel E D Peterson D Dai et al ldquoLow diagnostic yieldof elective coronary angiographyrdquo The New England Journal ofMedicine vol 362 no 10 pp 886ndash895 2010
[10] ldquoPharmacologic stress testingrdquo in Nuclear Cardiac ImagingPriniciples and Applications A E Iskandrian and E V GarciaEds pp 293ndash315 OxfordUniversity Press NewYork NY USA4th edition 2008
[11] R R Russell III and B L Zaret ldquoNuclear cardiology presentand futurerdquo Current Problems in Cardiology vol 31 no 9 pp557ndash629 2006
[12] G Germano H Kiat P B Kavanagh et al ldquoAutomatic quan-tification of ejection fraction from gated myocardial perfusionSPECTrdquo Journal of Nuclear Medicine vol 36 no 11 pp 2138ndash2147 1995
[13] S R Underwood C Anagnostopoulos M Cerqueira et alldquoMyocardial perfusion scintigraphy the evidencerdquo EuropeanJournal of Nuclear Medicine and Molecular Imaging vol 31 pp261ndash291 2004
[14] J Heo and A S Iskandrian ldquoTechnetium-labeled myocardialperfusion agentsrdquo Cardiology Clinics vol 12 no 2 pp 187ndash1981994
[15] B L Zaret P Rigo F J T Wackers et al ldquoMyocardial perfusionimaging with 99mTc tetrofosmin comparison to 201Tl imagingand coronary angiography in a phase III multicenter trialrdquoCirculation vol 91 no 2 pp 313ndash319 1995
[16] J J Mahmarian and M S Verani ldquoExercise thallium-201perfusion scintigraphy in the assessment of coronary arterydiseaserdquoAmerican Journal of Cardiology vol 67 no 14 pp 2Dndash11D 1991
[17] D D Miller L T Younis B R Chaitman and H StratmannldquoDiagnostic accuracy of dipyridamole technetium 99m-labeledsestamibi myocardial tomography for detection of coronaryartery diseaserdquo Journal of Nuclear Cardiology vol 4 no 1 pp18ndash24 1997
10 BioMed Research International
[18] Z He A S Iskandrian N C Gupta and M S Verani ldquoAssess-ing coronary artery disease with dipyridamole technetium-99m-tetrofosmin SPECT amulticenter trialrdquo Journal of NuclearMedicine vol 38 no 1 pp 44ndash48 1997
[19] A Boschi C Bolzati L Uccelli et al ldquoA class of asymmetricalnitrido 99mTc heterocomplexes as heart imaging agents withimproved biological propertiesrdquoNuclearMedicine Communica-tions vol 23 no 7 pp 689ndash693 2002
[20] A Boschi L Uccelli C Bolzati et al ldquoSynthesis and biologicevaluation of monocationic asymmetric 99mTc-nitride hetero-complexes showing high heart uptake and improved imagingpropertiesrdquo Journal of Nuclear Medicine vol 44 no 5 pp 806ndash814 2003
[21] C Bolzati M Cavazza-Ceccato S Agostini S TokunagaD Casara and G Bandoli ldquoSubcellular distribution andmetabolism studies of the potential myocardial imaging agent[99mTc(N)(DBODC)(PNP5)]+rdquo Journal of Nuclear Medicinevol 49 no 8 pp 1336ndash1344 2008
[22] C Cittanti L Uccelli M Pasquali et al ldquoWhole-body biodis-tribution and radiation dosimetry of the new cardiac tracer99mTc-N-DBODCrdquo Journal of Nuclear Medicine vol 49 no 8pp 1299ndash1304 2008
[23] K Hatada L M Riou M Ruiz et al ldquo99mTc-N-DBODC5a new myocardial perfusion imaging agent with rapid liverclearance comparison with 99mTc-sestamibi and 99mTc-tetrofosmin in ratsrdquo Journal of Nuclear Medicine vol 45 no 12pp 2095ndash2101 2004
[24] T Takeda J Wu and T T Lwin ldquo99mTc-N-DBODC5 a novelmyocardial perfusion imaging agent for diagnosis of coronaryartery disease a reviewrdquo Recent Patents on Cardiovascular DrugDiscovery vol 1 no 2 pp 161ndash166 2006
[25] K Hatada M Ruiz L M Riou et al ldquoOrgan biodistributionand myocardial uptake washout and redistribution kinetics ofTc-99m N-DBODC5 when injected during vasodilator stressin canine models of coronary stenosesrdquo Journal of NuclearCardiology vol 13 no 6 pp 779ndash790 2006
[26] W Zhang W Fang B Li X Wang and Z He ldquoExperimentalstudy of [99mTc(PNP5) (DBODC)]+ as a new myocardialperfusion imaging agentrdquo Cardiology vol 112 no 2 pp 89ndash972009
[27] M E Marmion S R Woulfe W L Neumann D L Nosco andE Deutsch ldquoPreparation and characterization of technetiumcomplexes with Schiff base and phosphine coordination 1Complexes of technetium-99g and -99m with substitutedacac2en and trialkyl phosphines (where acac2en = NN1015840-ethylenebis[acetylacetone iminato])rdquo Nuclear Medicine andBiology vol 26 no 7 pp 755ndash770 1999
[28] C Bolzati L Uccelli A Boschi et al ldquoSynthesis of a novel classof nitrido Tc-99m radiopharmaceuticals with phosphino-thiolligands showing transient heart uptakerdquo Journal of InorganicBiochemistry vol 78 no 3 pp 369ndash374 2000
[29] M J Henzlova M D Cerqueira J J Mahmarian and S YaoldquoStress protocols and tracersrdquo Journal of Nuclear Cardiology vol13 no 6 pp e80ndashe90 2006
[30] C L Hansen R A Goldstein D S Berman et al ldquoMyocardialperfusion and function single photon emission computedtomographyrdquo Journal of Nuclear Cardiology vol 13 no 6 ppe97ndashe120 2006
[31] P Flamen A Bossuyt and P R Franken ldquoTechnetium-99m-tetrofosmin in dipyridamole-stressmyocardial SPECT imagingintraindividual comparison with technetium-99m-sestamibirdquoJournal of Nuclear Medicine vol 36 no 11 pp 2009ndash2015 1995
[32] N Tamaki N Takahashi M Kawamoto et al ldquoMyocardialtomography using technetium-99m-tetrofosmin to evaluatecoronary artery diseaserdquo Journal of Nuclear Medicine vol 35no 4 pp 594ndash600 1994
[33] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardizedmyocardial segmentation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare profes-sionals from the Cardiac Imaging Committee of the Councilon Clinical Cardiology of the American Heart AssociationrdquoJournal of Nuclear Cardiology vol 9 no 2 pp 240ndash245 2002
[34] T Sharir G Germano X Kang et al ldquoPrediction of myocardialinfarction versus cardiac death by gated myocardial perfusionSPECT risk stratification by the amount of stress-inducedischemia and the poststress ejection fractionrdquo Journal of NuclearMedicine vol 42 no 6 pp 831ndash837 2001
[35] S H Braat B Leclercq R Itti A Lahiri B Sridhara and PRigo ldquoMyocardial imaging with technetium-99m-tetrofosmincomparison of one-day and two-day protocolsrdquo Journal ofNuclear Medicine vol 35 no 10 pp 1581ndash1585 1994
[36] G Germano T Chua H Kiat J S Areeda andD S Berman ldquoAquantitative phantom analysis of artifacts due to hepatic activ-ity in technetium-99m myocardial perfusion SPECT studiesrdquoJournal of Nuclear Medicine vol 35 no 2 pp 356ndash359 1994
[37] A K Paul andH A Nabi ldquoGatedmyocardial perfusion SPECTbasic principles technical aspects and clinical applicationsrdquoJournal of Nuclear Medicine Technology vol 32 no 4 pp 179ndash187 2004
[38] J Nuyts P Dupont V Van den Maegdenbergh S Vleugels PSuetens and L Mortelmans ldquoA study of the liver-heart artifactin emission tomographyrdquo Journal of Nuclear Medicine vol 36no 1 pp 133ndash139 1995
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 3
Imaging protocols 2-day exercise stressrest
Stress (day 1)
Inject 20ndash25 mCi 1-2 minsprior to peak
Exercise Gated imaging
0 30(mins)
Rest (day 2)Inject
20ndash25 mCiGated imaging
0 60(mins)
Figure 1 99mTc-N-DBODC5 and 99mTc-MIBI imaging protocolstwo-day exercise stressrest
of patients was identical to that for the 99mTc-N-DBODC5study 99mTc-N-DBODC5 and 99mTc-MIBI were used asmyocardial perfusion agents in a random sequence
24 Gated SPECT Acquisition and Image Reconstruction Pa-tients were imaged in the supine position with their armsraised SPECT images were acquired with a fixed 90∘ two-headed gamma camera (Infinia VC Hawkeye General Elec-tric USA) using a low-energy high-resolution parallel-holecollimator from the 45∘ right anterior oblique to the 45∘ leftposterior position Acquisition parameters were as followsdetectors at 90∘ 180∘ rotation at 3∘ steps with automaticbody contouring 35 s acquisition per step 64 times 64 matrixzoom times128 and energy window 140 keV plusmn 10 The totalacquisition time was approximately 20min The same filterswere used for both tracers The raw projection datasetswere filtered with a Butterworth filter (cut off frequency050 cyclespixel and power 60 for rest images cut offfrequency 050 cyclespixel and power 50 for stress images)No scatter or attenuation correction was performed
25 Heart-to-Organ Analysis 99mTc-N-DBODC5 and 99mTc-MIBI heart-to-organ count ratios were calculated from theanterior projection of each tomographic acquisition Regionsof interests (ROIs) were drawn around the entire left ventric-ular myocardium over the hepatic margin adjacent to theinferoapical wall of the left ventricle excluding the biliarytree and over the inferior left ventricular wall adjacent largeintestine activityThemean counts per pixel in the three ROIswere normalized to the injected tracer activity after decaycorrection and to a standard acquisition time of 1min Heart-to-liver and heart-to-intestine ratios were then computed[31]
26 Image Quality Assessing For MPI analyses at firsttwo experienced observers judged which image sets from99mTc-MIBI and 99mTc-N-DBODC5 were superior in imagequality on the basis of patient motion statistical noise traceractivity below the diaphragm heart-to-organ count ratio andsharpness without knowledge of the radiopharmaceutical orpatient identity [32]
27 MPI Image Interpretation Both overall qualitative diag-nosis and semiquantitative 17 segment with 5-point [33] (0= normal 4 = absent tracer uptake) scorings were employedin the independent blinded read by two expert readerswho were experienced in SPECT MPI interpretation In thismodel the left anterior descending artery (LAD) distributionterritory comprises seven segments (segments 1-2 7-8 13-14 and 17) the left circumflex artery (LCX) comprises fivesegments (segments 3-4 9-10 and 15) and the right coronaryartery (RCA) comprises five segments (segments 5-6 11-12and 16) SPECT stressrest studies were classified for eachmyocardial region in the following manner normal if all thesegments were normal after stress ischemic if at least onesegments improved at rest and scar if no segments improvedat rest In addition the summed stress (SSS) summed rest(SRS) and summed difference scores (SDSs) were calculatedand ischemia was defined as SDS ge 2 [34] The 99mTc-MIBIand 99mTc-N-DBODC5 images were separately interpretedwithout knowing the clinical histories results of coronaryangiography or other radionuclide findings
28 Coronary Angiography Interpretation All coronary angi-ograms were interpreted with quantitative CA in a coronaryangiography core laboratory blinded to the clinical or imag-ing results A coronary stenosis was considered present whenthere was a stenosis ge 50 in diameter in any epicardialcoronary artery The presence of one or more coronarystenoses defined the presence of significant CAD
29 Statistical Analysis All statistical analyses were per-formed using the statistical package SPSS 160 (Chicago ILUSA) The results were expressed as the mean value plusmn SDThe difference in left ventricular function parameters andperfusion scores were compared using a paired Studentrsquost-test Comparison of the proportion was made with theMcNemar test CA results were used as the ldquogold standardrdquoAgreements between CA and SPECT results were defined asthe kappa (120581) value 119875 lt 005 was considered significant
3 Results
31 Coronary Angiography Of the 46 patients studied 29had ge50 luminal diameter stenosis in at least one majorcoronary vessel Fourteen had single-vessel disease 11 hadtwo-vessel disease and four had three-vessel disease 15patients showed significant stenosis in the RCA 19 in theLAD and 14 in the LCX The remaining 17 patients hadnormal or nonsignificantly stenosed coronary arteries
4 BioMed Research International
(a) (b)
(c) (d)
Figure 2 Comparison of liver clearance of the two tracers in anterior tomographic planar images of a patient (as shown in the black arrowH heart Lv liver) (a) Exercise stress 99mTc-N-DBODC5 (b) Exercise stress 99mTc-MIBI (c) rest 99mTc-N-DBODC5 and (d) rest 99mTc-MIBI
00
02
04
06
08
10
12
Hea
rt-to
-live
r rat
io
Stress 30 min Rest 60 minTime after injection
99m Tc-N-DBODC599m Tc-MIBI
lowast
P lt 005 versus 99mTc-MIBIlowast
lowast
(a)
Stress 30 min Rest 60 minTime after injection
99m Tc-N-DBODC599m Tc-MIBI
00
05
10
15
20
25
Hea
rt-to
-inte
stine
ratio
lowast
lowast
lowast
P lt 005 versus 99mTc-MIBI
(b)
Figure 3 Heart-to-liver ratio and heart-to-intestine ratiomeasured with an anterior projection images at stress for 30min and rest for 60minfor 99mTc-N-DBODC5 and 99mTc-MIBI in 46 patients
32 Heart-to-Organ Count Ratio Qualitative analyses ofimages acquired of 99mTc-N-DBODC5 both at rest andduring stress revealed no significant overlap between traceraccumulation in the inferior wall of the ventricle and in thesubdiaphragmatic region (Figure 2)
Figure 3 depicts the heart-to-liver count ratios (a) andheart-to-intestine count ratios (b) of 99mTc-N-DBODC5 and
99mTc-MIBI in 46 patientsThemyocardium-to-liver ratios of99mTc-N-DBODC5 and 99mTc-MIBI studies were 097 plusmn 007and 051 plusmn 002 respectively at stress The myocardium-to-liver ratios of 99mTc-N-DBODC5 and 99mTc-MIBI MPI were078 plusmn 004 and 062 plusmn 001 respectively at rest On theother hand the mean heart-to-intestine ratios of 99mTc-N-DBODC5 were 212 plusmn 001 and 136 plusmn 002 for stress and
BioMed Research International 5
(a) (b)
(c)
Figure 4 Abnormal MPI in the vertical long-axis slices of a representative patient Both 99mTc-N-DBODC5 (a) and 99mTc-MIBI (b) imagesdemonstrate an inferoposterior defect (white arrows) The defect is well visualized on two tracer images corresponding to the CA resultThis coronary angiography (c) detected a stenosis of 90 in the RCA The concordance for diagnosis of myocardial ischemia was seen on99mTc-N-DBODC5 and 99mTc-MIBI studies
rest images respectivelyThe average heart-to-intestine ratiosof 99mTc-MIBI were 162 plusmn 001 and 091 plusmn 000 for stressand rest images respectively 99mTc-N-DBODC5 studies hada significantly higher heart-to-organ count ratio comparedwith 99mTc-MIBI studies (119875 lt 005)
33 Image Quality In the stress perfusion imaging 99mTc-N-DBODC5MPI was superior in quality to 99mTc-MIBIMPI in37 of the 46 patients studied In the remaining nine patientsthe MPI was judged to be of equal quality In the restingperfusion imaging 99mTc-N-DBODC5 images were superiorin all the patients studied In general the 99mTc-N-DBODC5MPI had more counts with less statistical noise less traceractivity below the diaphragm and desirable heart-to-organcount ratio compared with 99mTc-MIBI MPI
34 Gated SPECT Findings Table 2 shows the results ofscan segments between the 99mTc-N-DBODC5 and 99mTc-MIBI MPI Of the 782 segments that could be interpretedby both techniques 302 were concordantly normal 119 wereconcordantly reversible and 136 were concordantly nonre-versible 99mTc-N-DBODC5SPECTdetectedmore reversibledefects than did 99mTc-MIBI SPECT (240 versus 140 119875 lt005 McNemar test) 99mTc-MIBI SPECT identified more
nonreversible defects than did 99mTc-N-DBODC5 SPECT(312 versus 152 119875 lt 0001 McNemar test) Seventy-onesegments interpreted as normal on 99mTc-N-DBODC5 cor-responded to nonreversible defects on 99mTc-MIBI SPECTimages In contrast 12 normal 99mTc-MIBI segments cor-responded to nonreversible defects on 99mTc-N-DBODC5images When the patterns of uptake (normal reversibledefect and nonreversible defect) of 99mTc-N-DBODC5 and99mTc-MIBI were compared there was concordance in 71(557782) of segments
Table 3 shows the results of left ventricular functionparameters in the two techniques used In this study theend-diastolic volume (EDV) end-systolic volume (ESV) leftventricular ejection fraction (LVEF) and transient ventric-ular dysfunction (TID) were assessed by MPI using twotracers No statistically significant differences in MPI param-eters were observed between the 99mTc-MIBI and 99mTc-N-DBODC5 studies However the scores of myocardialperfusion defects for the detection of CAD were higher with99mTc-MIBI than with 99mTc-N-DBODC5 (119875 = 0012 forSSS 119875 = 0020 for SDS resp)
35 Detection of CAD Table 4 shows the sensitivity andspecificity of two tracers in diagnosing CAD Based on CA
6 BioMed Research International
Table 2 The comparison of myocardial perfusion in a total of 782 segments with 99mTc-N-DBODC5 and 99mTc-MIBI SPECT exerciseimaging
99mTc-N-DBODC599mTc-MIBI Total
Normal Reversible defect Nonreversible defectlowast
Normal 302 (39) 17 (2) 71 (9) 390Reversible defectlowast 16 (2) 119 (15) 105 (13) 240Nonreversible defect 12 (2) 4 (1) 136 (17) 152Total 330 140 312 782Data are presented as number lowast119875 lt 0001 99mTc-MIBI versus 99mTc-N-DBODC5 for nonreversible defect segments lowast119875 lt 005 99mTc-N-DBODC5 versus99mTc-MIBI for reversible defect segments McNemar test was used
Table 3 MPI findings of two tracers on left ventricular functionparameters and ischemia scores in 46 patients
Parameter 99mTc-MIBI 99mTc-N-DBODC5LVEF ()
Exercise 542 plusmn 113 567 plusmn 92Rest 631 plusmn 85 648 plusmn 79
EDV (mL)Exercise 815 plusmn 186 832 plusmn 163Rest 973 plusmn 164 991 plusmn 137
ESV (mL)Exercise 432 plusmn 97 414 plusmn 123Rest 594 plusmn 136 602 plusmn 98
SSS 121 plusmn 14995333 96 plusmn 16SRS 72 plusmn 08 79 plusmn 09SDS 42 plusmn 05995333 36 plusmn 04TID 096 plusmn 006 094 plusmn 002Data are presented asmeanplusmn SD or number () as appropriate995333statisticallysignificant 99mTc-MIBI versus 99mTc-N-DBODC5 (119875 lt 005) pairedStudentrsquos 119905-test was used LVEF left ventricular ejection fraction EDVend-diastolic volume ESV end-systolic volume SSS summed stress scoresSRS summed rest scores SDS summed difference scores TID transientventricular dysfunction
overall figures for sensitivity and specificity in identificationof CAD were 86 (2529) and 65 (1117) for 99mTc-MIBI imaging On the other hand the overall sensitivityand specificity for the detection of CAD were 86 (2529)and 88 (1517) for 99mTc-N-DBODC5 SPECT studies Theconcordance of ischemia diagnosis sensitivity of a represen-tative patient for the two tracers is shown in Figure 4 Theaccuracy was 078 for 99mTc-MIBI and 087 for 99mTc-N-DBODC5 Angiography agreement was very good for 99mTc-N-DBODC5 (120581 = 073) and moderate for 99mTc-MIBI (120581 =052) Specificity and accuracy were not significantly differentbut better for the 99mTc-N-DBODC5 group when comparedto 99mTc-MIBI SPECT (specificity 88-65 accuracy 87-78)
36 Detection of Disease in Individual Coronary VesselsTable 4 also shows the sensitivity and specificity of the twotracers in detecting individual-stenosed vessels Of a total of138 arteries in 46 patients 48 arteries had significant stenosesand 90 had insignificant lesions or were normal Overall
figures for sensitivity and specificity in identifying individual-stenosed vessels were 67 (3248) and 86 (7790) for 99mTc-MIBI imaging overall sensitivity and specificity to diagnoseindividual significantly stenosed vessels were 69 (3348)and 92 (8390) for 99mTc-N-DBODC5 SPECT studies
On the other hand sensitivity and specificity for RCAstenosis vessel lesion detection using 99mTc-MIBI MPI were87 and 68 compared to 87 and 87 for 99mTc-N-DBODC5 MPI LAD stenosis (53 sensitivity and 96specificity for 99mTc-MIBI 63 sensitivity and 96 speci-ficity for 99mTc-N-DBODC5 resp) and left circumflex(LCX) (64 sensitivity and 94 specificity for 99mTc-MIBI57 sensitivity and 94 specificity for 99mTc-N-DBODC5resp) Angiography agreement was very good for 99mTc-N-DBODC5 (120581 = 063 for LAD 120581 = 071 for RCA resp) andmoderate for 99mTc-MIBI (120581 = 052 for LAD 120581 = 048 forRCA resp) In contrast the angiography agreement was verygood for 99mTc-MIBI (120581 = 062 for LCX) and moderate for99mTc-N-DBODC5 (120581 = 055 for LCX) (Table 4) Overall thespecificity of 99mTc-N-DBODC5 SPECT to detect individualRCA stenosis was better (2731 87) than that of 99mTc-MIBISPECT (2131 68) despite having no statistical significance
4 Discussion
These preliminary results demonstrate that stress-restmyocardial perfusion SPECT with 99mTc-N-DBODC5 isa sensitive method for detecting CAD and identifyingstenosed coronary arteries For the detection of CADmore importantly 99mTc-N-DBODC5 MPI reached goodagreement compared with CA (120581 = 073)
41 Advantages of 99119898Tc-N-DBODC5 99mTc-N-DBODC5 isa new lipophilic monocationic and nitride 99mTc-labeledtracer that is rapidly cleared from the liver after intravenousinjection It possesses good stability under physiological con-ditions Importantly 99mTc-N-DBODC5 exhibits more rapidliver washout than either 99mTc-MIBI or 99mTc-tetrofosminFor example at 60min after injection in rats the heartliverratio of 99mTc-N-DBODC5 is approximately ten times higherthan that of 99mTc-MIBI or 99mTc-tetrofosmin Preclinicalstudies have shown that 99mTc-N-DBODC5 SPECT canidentify previous ischemia as areas of reduced tracer uptake[25 26] Furthermore the rapid liver clearance and highuptake in the myocardium of 99mTc-N-DBODC5 will allow
BioMed Research International 7
Table 4 Sensitivity specificity and diagnostic accuracy of scintigraphic perfusion studies and agreement with coronary angiography
Overall LAD LCX RCAMIBI DBODC MIBI DBODC MIBI DBODC MIBI DBODC
No of disease 25 25 10 12 9 8 13 13Sensitivity () 86 86 53 63 64 57 87 87Specificity () 65 88 96 96 94 94 68 87Accuracy () 78 87 78 83 85 83 74 87998771Kappa (120581) 053 073 052 063 062 055 048 071Data are presented as number () MIBI = 99mTc-MIBI DBODC = 99mTc-N-DBODC5 LAD left anterior descending coronary artery LCX left circumflexcoronary artery RCA right coronary artery 998771CA was used as the ldquogold standardrdquo for the calculation of the 120581 which is determine between SPECT MPI andCA If there is no agreement 120581 = 020ndash039 moderate agreement 120581 = 040ndash059 very good agreement 120581 = 060ndash079 excellent agreement 120581 = 080ndash100
SPECT images of the left ventricle to be acquired earlyand with excellent quality [22] The ratios of heart-to-liverwere consistent with the previous report study [22] Thesecharacteristics are suitable particularly for patients withsuspected acute coronary syndromes and without diagnosticelectrocardiogram because early diagnosis is needed in suchpatients for timely therapeutic decisionmaking 99mTc-MIBIon the other hand may require a wait time of up to 1 h forimaging
In the present study the heart-to-organ count ratio of99mTc-N-DBODC5 MPI was superior to that of 99mTc-MIBIin 46 patients Compared with 99mTc-MIBI MPI 99mTc-N-DBODC5 MPI had better image quality in most patientsFurthermore in this study exercise stress myocardial imageswere performed 30min after 99mTc-N-DBODC5 injectionand excellent MPI with high contrast was possible
42 Clinical Value of 99119898Tc-N-DBODC5 for the Detection ofCAD This clinical trial assesses the diagnostic value of thisagent to detect CAD comparing it with stress 99mTc-MIBIMPI and CA
In this study compared with 99mTc-MIBI MPI 99mTc-N-DBODC5MPI indicates the same sensitivity and better speci-ficity and accuracy to detect coronary disease in patientsalthough none of the differences were significant On theother hand more importantly angiography agreement wasvery good for 99mTc-N-DBODC5 (120581 = 073) and moderatefor 99mTc-MIBI (120581 = 052) thus compared with 99mTc-MIBI MPI it provides a high degree of concordance for theevaluation of CAD specifically in excluding perfusion abnor-malities in patients with suspected CAD Possible reasons forthis difference may be fast liver clearance favorable heart-to-organ ratio and high image quality 99mTc-N-DBODC5with rapid liver clearancemay significantly reduce the photonscatter from the liver into the inferoposterior walls Thisreduces the artifactual decreased myocardial perfusion andimproves the diagnostic accuracy for the detection of CADcompared with other 99mTc-labeled perfusion agents [24]
Unsurprisingly Braat et al [35] and Germano et al [36]noted that technetium-labeled MPI agents with a fast liverclearance can significantly reduce the photon scatter fromthe liver into the inferior walls but the radioactivity may betransferred to the gastrointestinal area and increased bowel
and gastric activity were seen as a problem associated withhigh liver uptake in the visual and quantitative interpretationof the inferoposterior myocardial walls In this study boweluptakewas frequently seen on the 99mTc-N-DBODC5 imagesbut did not result in any nondiagnostic scans
For the detection of coronary disease in patients 99mTc-MIBI produced abnormal results for MPI in four patientswho had no angiographically detected stenosis Some of thesefalse-positive results may be due in part to the liver-to-heart artifacts In this study we could classify fixed perfusiondefects as soft-tissue attenuation artifacts or infarcts by usinggated SPECT Because an artifactual defect would shownormal contraction (wall motion or thickening) on a gatedimage artifacts can be differentiated from a true infarct [37]
For the detection of individual vessel stenosis on theother hand angiography agreement was very good for 99mTc-N-DBODC5 (120581=071 for RCA) andmoderate for 99mTc-MIBI(120581 = 048 for RCA) For LAD and LCX arteries stenosis thediagnosis of myocardial ischemia on 99mTc-N-DBODC5 and99mTc-MIBI study had the same specificity and it was similarto that of two tracer to diagnose sensitivity and accuracy ofmyocardial ischemia Abnormal results of myocardial imagesin individual RCA vessel stenosis (six arteries-stenosed ves-sels for RCA) were obtained in the 99mTc-MIBI studieswhile CA and 99mTc-N-DBODC5 studies showed normalfindings in the same individual RCA vessel territories Someof these false-positive results may be due to photon scatterfrom the liver and intestine into the inferoposterior walls99mTc-MIBI concentration located below the left diaphragm(ie liver and bowel) may cause an artifactual perfusiondefect in the adjacent myocardial a phenomenon knownas the ldquoliver-heart artifactrdquo [36 38] Moreover the inferiorand inferoposterior regions were dominated mainly by RCAterritories corresponding to the myocardial short axis andvertical long axis while arteries regions which LAD and LCXdominated were less interfered from ldquoliver-heart artifactrdquoFinally for clinical applications 99mTc-N-DBODC5 offersbetter determination of detects particularly in the infero-posterior wall on myocardial images A typical example of afalse-positive perfusion defect in the inferior wall is shown inFigure 5
On a segment-to-segment basis complete agreementbetween the two imaging agents occurred in 71 of segments
8 BioMed Research International
(a) (b) (c)
Figure 5 Serial short-axis and vertical long-axis slices of stress-rest 99mTc-N-DBODC5 images (b) and stress-rest 99mTc-MIBI images (c) ofa representative patient with normal CA (a) Because of intense uptake of technetium 99mTc-MIBI in the liver high liver background activitycan be observed Furthermore a false-positive myocardial perfusion defect was also seen in the inferoposterior wall segments supplied bythe RCA territory (white arrows) Importantly however at stress and rest the inferoposterior wall segments of 99mTc-N-DBODC5 imagesare clearly separated from the subdiaphragmatic activity
However more myocardial segments were nonreversible on99mTc-MIBI images than on 99mTc-N-DBODC5 images Onthe contrary 99mTc-N-DBODC5MPI had a higher reversibledefect than that of 99mTc-MIBI A possible reason for thisdifference may be due in part to the ldquoliver-heart artifactrdquoThe presence of high liver activity adjacent to the inferior wallresults fromoversubtraction of activity from the inferior wallTherefore the more ldquoliver-heart artifactrdquo in the inferoposte-rior wall on myocardial images the more false nonreversibledefects in the inferoposterior wall on myocardial perfusionsegmental analysis In other words the less reversible defectsin the inferoposterior wall were deduced on 99mTc-MIBIMPIsegmental analysis
More importantly however the main advantage andclinical value of 99mTc-N-DBODC5 can improve diagnosticspecificity and reduce the false-positive diagnosis of patientsand associated treatment fees
5 Limitations
In this study we did not attempt to assess the absolute diag-nostic accuracy of 99mTc-N-DBODC5 because definitive
conclusions in this regard can only be drawn by study-ing larger patient cohort In addition although 99mTc-N-DBODC5 did not track flow as well as 201Tl the magni-tudes of the pharmacologic stress-induced perfusion defectswere comparable to those previously reported for 99mTc-tetrofosmin Thus direct comparison between 99mTc-N-DBODC5 and 99mTc-tetrofosmin should be further provedin the same patient population Overall 99mTc-N-DBODC5MPI will become an important diagnostic tool in the evalua-tion of myocardial perfusion
6 Conclusion
This preliminary clinical study showed that 99mTc-N-DBODC5 and 99mTc-MIBI MPI provide comparable diag-nostic information for patients undergoing exercise rest fordetection of CAD In addition 99mTc-N-DBODC5 doesnot exhibit the disadvantages of 99mTc-MIBI in this studyBy contrast because of its high heart-organ count ratioin comparison to 99mTc-MIBI it improves high degree ofdiagnostic concordance in defining or excluding perfusionabnormalities in patients with CADTherefore it can become
BioMed Research International 9
the agent of choice for the evaluation ofmyocardial perfusionand ventricular function in patients with CAD
Abbreviations
CAD Coronary artery diseaseMPI Myocardial perfusion imagingCA Coronary angiographySPECT Single-photon emission computed
tomographyPET Positron emission computed
tomography99mTc-MIBI Technetium 99m sestamibi99mTc-N-DBODC5 99mTc(N)(DBODC)(PNP5)201Tl Thallium-20199mTc-tetrofosmin Technetium-99m-tetrofosminROI Regions of interestLAD Left anterior descending arteryLCX Left circumflex arteryRCA Right coronary arterySSS Summed stress scoreSRS Summed rest scoreSDS Summed difference scoreEDV End-diastolic volumeESV End-systolic volumeLVEF Left ventricular ejection fraction
Ethics Statement
This study was conducted in accordance with the HelsinkiDeclaration All subjects provided written informed consentbefore MPI acknowledging that they understood their rightsand obligations This study was approved by the ResearchEthics Committee of Shanxi Medical University
Conflict of Interests
The authors declare that they have no conflict of interest
Acknowledgments
This research is partly supported by Grants from the YouthScience and Technology Research Foundation of ShanxiProvince (no 2009021043-3) The authors acknowledge themembers of the participating staff for their contribution tothis clinical study
References
[1] National Hospital Discharge Survey National Health StatisticsReport no 5 2006
[2] J He D Gu X Wu et al ldquoMajor causes of death among menand women in Chinardquo The New England Journal of Medicinevol 353 no 11 pp 1124ndash1134 2005
[3] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardized myocardial sementation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare pro-fessionals from the Cardiac Imaging Committee of the Council
on Clinical Cardiology of the American Heart AssociationrdquoCirculation vol 105 no 4 pp 539ndash542 2002
[4] R J Gibbons J Abrams K Chatterjee et al ldquoACCAHA 2002guideline update for the management of patients with chronicstable anginamdashsummary article a report of the AmericanCollege of CardiologyAmerican Heart Association Task Forceon Practice Guidelines (Committee on the Management ofPatients With Chronic Stable Angina)rdquo Journal of the AmericanCollege of Cardiology vol 41 no 1 pp 159ndash168 2003
[5] WWijns P Kolh N Danchin et al ldquoGuidelines on myocardialrevascularizationrdquo European Heart Journal vol 31 pp 2501ndash2555 2010
[6] J M Jensen K A Oslashvrehus L H Nielsen J K Jensen HM Larsen and B L Noslashrgaard ldquoParadigm of pretest riskstratification before coronary computed tomographyrdquo Journalof Cardiovascular Computed Tomography vol 3 no 6 pp 386ndash391 2009
[7] N RMollet F Cademartiri C VanMieghem et al ldquoAdjunctivevalue of CT coronary angiography in the diagnostic work-up ofpatients with typical angina pectorisrdquo European Heart Journalvol 28 no 15 pp 1872ndash1878 2007
[8] R G E J Groutars J F Verzijlbergen M M C Tiel-Van Buulet al ldquoThe accuracy of 1-day dual-isotopemyocardial SPECT ina population with high prevalence of coronary artery diseaserdquoInternational Journal of Cardiovascular Imaging vol 19 no 3pp 229ndash238 2003
[9] M R Patel E D Peterson D Dai et al ldquoLow diagnostic yieldof elective coronary angiographyrdquo The New England Journal ofMedicine vol 362 no 10 pp 886ndash895 2010
[10] ldquoPharmacologic stress testingrdquo in Nuclear Cardiac ImagingPriniciples and Applications A E Iskandrian and E V GarciaEds pp 293ndash315 OxfordUniversity Press NewYork NY USA4th edition 2008
[11] R R Russell III and B L Zaret ldquoNuclear cardiology presentand futurerdquo Current Problems in Cardiology vol 31 no 9 pp557ndash629 2006
[12] G Germano H Kiat P B Kavanagh et al ldquoAutomatic quan-tification of ejection fraction from gated myocardial perfusionSPECTrdquo Journal of Nuclear Medicine vol 36 no 11 pp 2138ndash2147 1995
[13] S R Underwood C Anagnostopoulos M Cerqueira et alldquoMyocardial perfusion scintigraphy the evidencerdquo EuropeanJournal of Nuclear Medicine and Molecular Imaging vol 31 pp261ndash291 2004
[14] J Heo and A S Iskandrian ldquoTechnetium-labeled myocardialperfusion agentsrdquo Cardiology Clinics vol 12 no 2 pp 187ndash1981994
[15] B L Zaret P Rigo F J T Wackers et al ldquoMyocardial perfusionimaging with 99mTc tetrofosmin comparison to 201Tl imagingand coronary angiography in a phase III multicenter trialrdquoCirculation vol 91 no 2 pp 313ndash319 1995
[16] J J Mahmarian and M S Verani ldquoExercise thallium-201perfusion scintigraphy in the assessment of coronary arterydiseaserdquoAmerican Journal of Cardiology vol 67 no 14 pp 2Dndash11D 1991
[17] D D Miller L T Younis B R Chaitman and H StratmannldquoDiagnostic accuracy of dipyridamole technetium 99m-labeledsestamibi myocardial tomography for detection of coronaryartery diseaserdquo Journal of Nuclear Cardiology vol 4 no 1 pp18ndash24 1997
10 BioMed Research International
[18] Z He A S Iskandrian N C Gupta and M S Verani ldquoAssess-ing coronary artery disease with dipyridamole technetium-99m-tetrofosmin SPECT amulticenter trialrdquo Journal of NuclearMedicine vol 38 no 1 pp 44ndash48 1997
[19] A Boschi C Bolzati L Uccelli et al ldquoA class of asymmetricalnitrido 99mTc heterocomplexes as heart imaging agents withimproved biological propertiesrdquoNuclearMedicine Communica-tions vol 23 no 7 pp 689ndash693 2002
[20] A Boschi L Uccelli C Bolzati et al ldquoSynthesis and biologicevaluation of monocationic asymmetric 99mTc-nitride hetero-complexes showing high heart uptake and improved imagingpropertiesrdquo Journal of Nuclear Medicine vol 44 no 5 pp 806ndash814 2003
[21] C Bolzati M Cavazza-Ceccato S Agostini S TokunagaD Casara and G Bandoli ldquoSubcellular distribution andmetabolism studies of the potential myocardial imaging agent[99mTc(N)(DBODC)(PNP5)]+rdquo Journal of Nuclear Medicinevol 49 no 8 pp 1336ndash1344 2008
[22] C Cittanti L Uccelli M Pasquali et al ldquoWhole-body biodis-tribution and radiation dosimetry of the new cardiac tracer99mTc-N-DBODCrdquo Journal of Nuclear Medicine vol 49 no 8pp 1299ndash1304 2008
[23] K Hatada L M Riou M Ruiz et al ldquo99mTc-N-DBODC5a new myocardial perfusion imaging agent with rapid liverclearance comparison with 99mTc-sestamibi and 99mTc-tetrofosmin in ratsrdquo Journal of Nuclear Medicine vol 45 no 12pp 2095ndash2101 2004
[24] T Takeda J Wu and T T Lwin ldquo99mTc-N-DBODC5 a novelmyocardial perfusion imaging agent for diagnosis of coronaryartery disease a reviewrdquo Recent Patents on Cardiovascular DrugDiscovery vol 1 no 2 pp 161ndash166 2006
[25] K Hatada M Ruiz L M Riou et al ldquoOrgan biodistributionand myocardial uptake washout and redistribution kinetics ofTc-99m N-DBODC5 when injected during vasodilator stressin canine models of coronary stenosesrdquo Journal of NuclearCardiology vol 13 no 6 pp 779ndash790 2006
[26] W Zhang W Fang B Li X Wang and Z He ldquoExperimentalstudy of [99mTc(PNP5) (DBODC)]+ as a new myocardialperfusion imaging agentrdquo Cardiology vol 112 no 2 pp 89ndash972009
[27] M E Marmion S R Woulfe W L Neumann D L Nosco andE Deutsch ldquoPreparation and characterization of technetiumcomplexes with Schiff base and phosphine coordination 1Complexes of technetium-99g and -99m with substitutedacac2en and trialkyl phosphines (where acac2en = NN1015840-ethylenebis[acetylacetone iminato])rdquo Nuclear Medicine andBiology vol 26 no 7 pp 755ndash770 1999
[28] C Bolzati L Uccelli A Boschi et al ldquoSynthesis of a novel classof nitrido Tc-99m radiopharmaceuticals with phosphino-thiolligands showing transient heart uptakerdquo Journal of InorganicBiochemistry vol 78 no 3 pp 369ndash374 2000
[29] M J Henzlova M D Cerqueira J J Mahmarian and S YaoldquoStress protocols and tracersrdquo Journal of Nuclear Cardiology vol13 no 6 pp e80ndashe90 2006
[30] C L Hansen R A Goldstein D S Berman et al ldquoMyocardialperfusion and function single photon emission computedtomographyrdquo Journal of Nuclear Cardiology vol 13 no 6 ppe97ndashe120 2006
[31] P Flamen A Bossuyt and P R Franken ldquoTechnetium-99m-tetrofosmin in dipyridamole-stressmyocardial SPECT imagingintraindividual comparison with technetium-99m-sestamibirdquoJournal of Nuclear Medicine vol 36 no 11 pp 2009ndash2015 1995
[32] N Tamaki N Takahashi M Kawamoto et al ldquoMyocardialtomography using technetium-99m-tetrofosmin to evaluatecoronary artery diseaserdquo Journal of Nuclear Medicine vol 35no 4 pp 594ndash600 1994
[33] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardizedmyocardial segmentation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare profes-sionals from the Cardiac Imaging Committee of the Councilon Clinical Cardiology of the American Heart AssociationrdquoJournal of Nuclear Cardiology vol 9 no 2 pp 240ndash245 2002
[34] T Sharir G Germano X Kang et al ldquoPrediction of myocardialinfarction versus cardiac death by gated myocardial perfusionSPECT risk stratification by the amount of stress-inducedischemia and the poststress ejection fractionrdquo Journal of NuclearMedicine vol 42 no 6 pp 831ndash837 2001
[35] S H Braat B Leclercq R Itti A Lahiri B Sridhara and PRigo ldquoMyocardial imaging with technetium-99m-tetrofosmincomparison of one-day and two-day protocolsrdquo Journal ofNuclear Medicine vol 35 no 10 pp 1581ndash1585 1994
[36] G Germano T Chua H Kiat J S Areeda andD S Berman ldquoAquantitative phantom analysis of artifacts due to hepatic activ-ity in technetium-99m myocardial perfusion SPECT studiesrdquoJournal of Nuclear Medicine vol 35 no 2 pp 356ndash359 1994
[37] A K Paul andH A Nabi ldquoGatedmyocardial perfusion SPECTbasic principles technical aspects and clinical applicationsrdquoJournal of Nuclear Medicine Technology vol 32 no 4 pp 179ndash187 2004
[38] J Nuyts P Dupont V Van den Maegdenbergh S Vleugels PSuetens and L Mortelmans ldquoA study of the liver-heart artifactin emission tomographyrdquo Journal of Nuclear Medicine vol 36no 1 pp 133ndash139 1995
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 BioMed Research International
(a) (b)
(c) (d)
Figure 2 Comparison of liver clearance of the two tracers in anterior tomographic planar images of a patient (as shown in the black arrowH heart Lv liver) (a) Exercise stress 99mTc-N-DBODC5 (b) Exercise stress 99mTc-MIBI (c) rest 99mTc-N-DBODC5 and (d) rest 99mTc-MIBI
00
02
04
06
08
10
12
Hea
rt-to
-live
r rat
io
Stress 30 min Rest 60 minTime after injection
99m Tc-N-DBODC599m Tc-MIBI
lowast
P lt 005 versus 99mTc-MIBIlowast
lowast
(a)
Stress 30 min Rest 60 minTime after injection
99m Tc-N-DBODC599m Tc-MIBI
00
05
10
15
20
25
Hea
rt-to
-inte
stine
ratio
lowast
lowast
lowast
P lt 005 versus 99mTc-MIBI
(b)
Figure 3 Heart-to-liver ratio and heart-to-intestine ratiomeasured with an anterior projection images at stress for 30min and rest for 60minfor 99mTc-N-DBODC5 and 99mTc-MIBI in 46 patients
32 Heart-to-Organ Count Ratio Qualitative analyses ofimages acquired of 99mTc-N-DBODC5 both at rest andduring stress revealed no significant overlap between traceraccumulation in the inferior wall of the ventricle and in thesubdiaphragmatic region (Figure 2)
Figure 3 depicts the heart-to-liver count ratios (a) andheart-to-intestine count ratios (b) of 99mTc-N-DBODC5 and
99mTc-MIBI in 46 patientsThemyocardium-to-liver ratios of99mTc-N-DBODC5 and 99mTc-MIBI studies were 097 plusmn 007and 051 plusmn 002 respectively at stress The myocardium-to-liver ratios of 99mTc-N-DBODC5 and 99mTc-MIBI MPI were078 plusmn 004 and 062 plusmn 001 respectively at rest On theother hand the mean heart-to-intestine ratios of 99mTc-N-DBODC5 were 212 plusmn 001 and 136 plusmn 002 for stress and
BioMed Research International 5
(a) (b)
(c)
Figure 4 Abnormal MPI in the vertical long-axis slices of a representative patient Both 99mTc-N-DBODC5 (a) and 99mTc-MIBI (b) imagesdemonstrate an inferoposterior defect (white arrows) The defect is well visualized on two tracer images corresponding to the CA resultThis coronary angiography (c) detected a stenosis of 90 in the RCA The concordance for diagnosis of myocardial ischemia was seen on99mTc-N-DBODC5 and 99mTc-MIBI studies
rest images respectivelyThe average heart-to-intestine ratiosof 99mTc-MIBI were 162 plusmn 001 and 091 plusmn 000 for stressand rest images respectively 99mTc-N-DBODC5 studies hada significantly higher heart-to-organ count ratio comparedwith 99mTc-MIBI studies (119875 lt 005)
33 Image Quality In the stress perfusion imaging 99mTc-N-DBODC5MPI was superior in quality to 99mTc-MIBIMPI in37 of the 46 patients studied In the remaining nine patientsthe MPI was judged to be of equal quality In the restingperfusion imaging 99mTc-N-DBODC5 images were superiorin all the patients studied In general the 99mTc-N-DBODC5MPI had more counts with less statistical noise less traceractivity below the diaphragm and desirable heart-to-organcount ratio compared with 99mTc-MIBI MPI
34 Gated SPECT Findings Table 2 shows the results ofscan segments between the 99mTc-N-DBODC5 and 99mTc-MIBI MPI Of the 782 segments that could be interpretedby both techniques 302 were concordantly normal 119 wereconcordantly reversible and 136 were concordantly nonre-versible 99mTc-N-DBODC5SPECTdetectedmore reversibledefects than did 99mTc-MIBI SPECT (240 versus 140 119875 lt005 McNemar test) 99mTc-MIBI SPECT identified more
nonreversible defects than did 99mTc-N-DBODC5 SPECT(312 versus 152 119875 lt 0001 McNemar test) Seventy-onesegments interpreted as normal on 99mTc-N-DBODC5 cor-responded to nonreversible defects on 99mTc-MIBI SPECTimages In contrast 12 normal 99mTc-MIBI segments cor-responded to nonreversible defects on 99mTc-N-DBODC5images When the patterns of uptake (normal reversibledefect and nonreversible defect) of 99mTc-N-DBODC5 and99mTc-MIBI were compared there was concordance in 71(557782) of segments
Table 3 shows the results of left ventricular functionparameters in the two techniques used In this study theend-diastolic volume (EDV) end-systolic volume (ESV) leftventricular ejection fraction (LVEF) and transient ventric-ular dysfunction (TID) were assessed by MPI using twotracers No statistically significant differences in MPI param-eters were observed between the 99mTc-MIBI and 99mTc-N-DBODC5 studies However the scores of myocardialperfusion defects for the detection of CAD were higher with99mTc-MIBI than with 99mTc-N-DBODC5 (119875 = 0012 forSSS 119875 = 0020 for SDS resp)
35 Detection of CAD Table 4 shows the sensitivity andspecificity of two tracers in diagnosing CAD Based on CA
6 BioMed Research International
Table 2 The comparison of myocardial perfusion in a total of 782 segments with 99mTc-N-DBODC5 and 99mTc-MIBI SPECT exerciseimaging
99mTc-N-DBODC599mTc-MIBI Total
Normal Reversible defect Nonreversible defectlowast
Normal 302 (39) 17 (2) 71 (9) 390Reversible defectlowast 16 (2) 119 (15) 105 (13) 240Nonreversible defect 12 (2) 4 (1) 136 (17) 152Total 330 140 312 782Data are presented as number lowast119875 lt 0001 99mTc-MIBI versus 99mTc-N-DBODC5 for nonreversible defect segments lowast119875 lt 005 99mTc-N-DBODC5 versus99mTc-MIBI for reversible defect segments McNemar test was used
Table 3 MPI findings of two tracers on left ventricular functionparameters and ischemia scores in 46 patients
Parameter 99mTc-MIBI 99mTc-N-DBODC5LVEF ()
Exercise 542 plusmn 113 567 plusmn 92Rest 631 plusmn 85 648 plusmn 79
EDV (mL)Exercise 815 plusmn 186 832 plusmn 163Rest 973 plusmn 164 991 plusmn 137
ESV (mL)Exercise 432 plusmn 97 414 plusmn 123Rest 594 plusmn 136 602 plusmn 98
SSS 121 plusmn 14995333 96 plusmn 16SRS 72 plusmn 08 79 plusmn 09SDS 42 plusmn 05995333 36 plusmn 04TID 096 plusmn 006 094 plusmn 002Data are presented asmeanplusmn SD or number () as appropriate995333statisticallysignificant 99mTc-MIBI versus 99mTc-N-DBODC5 (119875 lt 005) pairedStudentrsquos 119905-test was used LVEF left ventricular ejection fraction EDVend-diastolic volume ESV end-systolic volume SSS summed stress scoresSRS summed rest scores SDS summed difference scores TID transientventricular dysfunction
overall figures for sensitivity and specificity in identificationof CAD were 86 (2529) and 65 (1117) for 99mTc-MIBI imaging On the other hand the overall sensitivityand specificity for the detection of CAD were 86 (2529)and 88 (1517) for 99mTc-N-DBODC5 SPECT studies Theconcordance of ischemia diagnosis sensitivity of a represen-tative patient for the two tracers is shown in Figure 4 Theaccuracy was 078 for 99mTc-MIBI and 087 for 99mTc-N-DBODC5 Angiography agreement was very good for 99mTc-N-DBODC5 (120581 = 073) and moderate for 99mTc-MIBI (120581 =052) Specificity and accuracy were not significantly differentbut better for the 99mTc-N-DBODC5 group when comparedto 99mTc-MIBI SPECT (specificity 88-65 accuracy 87-78)
36 Detection of Disease in Individual Coronary VesselsTable 4 also shows the sensitivity and specificity of the twotracers in detecting individual-stenosed vessels Of a total of138 arteries in 46 patients 48 arteries had significant stenosesand 90 had insignificant lesions or were normal Overall
figures for sensitivity and specificity in identifying individual-stenosed vessels were 67 (3248) and 86 (7790) for 99mTc-MIBI imaging overall sensitivity and specificity to diagnoseindividual significantly stenosed vessels were 69 (3348)and 92 (8390) for 99mTc-N-DBODC5 SPECT studies
On the other hand sensitivity and specificity for RCAstenosis vessel lesion detection using 99mTc-MIBI MPI were87 and 68 compared to 87 and 87 for 99mTc-N-DBODC5 MPI LAD stenosis (53 sensitivity and 96specificity for 99mTc-MIBI 63 sensitivity and 96 speci-ficity for 99mTc-N-DBODC5 resp) and left circumflex(LCX) (64 sensitivity and 94 specificity for 99mTc-MIBI57 sensitivity and 94 specificity for 99mTc-N-DBODC5resp) Angiography agreement was very good for 99mTc-N-DBODC5 (120581 = 063 for LAD 120581 = 071 for RCA resp) andmoderate for 99mTc-MIBI (120581 = 052 for LAD 120581 = 048 forRCA resp) In contrast the angiography agreement was verygood for 99mTc-MIBI (120581 = 062 for LCX) and moderate for99mTc-N-DBODC5 (120581 = 055 for LCX) (Table 4) Overall thespecificity of 99mTc-N-DBODC5 SPECT to detect individualRCA stenosis was better (2731 87) than that of 99mTc-MIBISPECT (2131 68) despite having no statistical significance
4 Discussion
These preliminary results demonstrate that stress-restmyocardial perfusion SPECT with 99mTc-N-DBODC5 isa sensitive method for detecting CAD and identifyingstenosed coronary arteries For the detection of CADmore importantly 99mTc-N-DBODC5 MPI reached goodagreement compared with CA (120581 = 073)
41 Advantages of 99119898Tc-N-DBODC5 99mTc-N-DBODC5 isa new lipophilic monocationic and nitride 99mTc-labeledtracer that is rapidly cleared from the liver after intravenousinjection It possesses good stability under physiological con-ditions Importantly 99mTc-N-DBODC5 exhibits more rapidliver washout than either 99mTc-MIBI or 99mTc-tetrofosminFor example at 60min after injection in rats the heartliverratio of 99mTc-N-DBODC5 is approximately ten times higherthan that of 99mTc-MIBI or 99mTc-tetrofosmin Preclinicalstudies have shown that 99mTc-N-DBODC5 SPECT canidentify previous ischemia as areas of reduced tracer uptake[25 26] Furthermore the rapid liver clearance and highuptake in the myocardium of 99mTc-N-DBODC5 will allow
BioMed Research International 7
Table 4 Sensitivity specificity and diagnostic accuracy of scintigraphic perfusion studies and agreement with coronary angiography
Overall LAD LCX RCAMIBI DBODC MIBI DBODC MIBI DBODC MIBI DBODC
No of disease 25 25 10 12 9 8 13 13Sensitivity () 86 86 53 63 64 57 87 87Specificity () 65 88 96 96 94 94 68 87Accuracy () 78 87 78 83 85 83 74 87998771Kappa (120581) 053 073 052 063 062 055 048 071Data are presented as number () MIBI = 99mTc-MIBI DBODC = 99mTc-N-DBODC5 LAD left anterior descending coronary artery LCX left circumflexcoronary artery RCA right coronary artery 998771CA was used as the ldquogold standardrdquo for the calculation of the 120581 which is determine between SPECT MPI andCA If there is no agreement 120581 = 020ndash039 moderate agreement 120581 = 040ndash059 very good agreement 120581 = 060ndash079 excellent agreement 120581 = 080ndash100
SPECT images of the left ventricle to be acquired earlyand with excellent quality [22] The ratios of heart-to-liverwere consistent with the previous report study [22] Thesecharacteristics are suitable particularly for patients withsuspected acute coronary syndromes and without diagnosticelectrocardiogram because early diagnosis is needed in suchpatients for timely therapeutic decisionmaking 99mTc-MIBIon the other hand may require a wait time of up to 1 h forimaging
In the present study the heart-to-organ count ratio of99mTc-N-DBODC5 MPI was superior to that of 99mTc-MIBIin 46 patients Compared with 99mTc-MIBI MPI 99mTc-N-DBODC5 MPI had better image quality in most patientsFurthermore in this study exercise stress myocardial imageswere performed 30min after 99mTc-N-DBODC5 injectionand excellent MPI with high contrast was possible
42 Clinical Value of 99119898Tc-N-DBODC5 for the Detection ofCAD This clinical trial assesses the diagnostic value of thisagent to detect CAD comparing it with stress 99mTc-MIBIMPI and CA
In this study compared with 99mTc-MIBI MPI 99mTc-N-DBODC5MPI indicates the same sensitivity and better speci-ficity and accuracy to detect coronary disease in patientsalthough none of the differences were significant On theother hand more importantly angiography agreement wasvery good for 99mTc-N-DBODC5 (120581 = 073) and moderatefor 99mTc-MIBI (120581 = 052) thus compared with 99mTc-MIBI MPI it provides a high degree of concordance for theevaluation of CAD specifically in excluding perfusion abnor-malities in patients with suspected CAD Possible reasons forthis difference may be fast liver clearance favorable heart-to-organ ratio and high image quality 99mTc-N-DBODC5with rapid liver clearancemay significantly reduce the photonscatter from the liver into the inferoposterior walls Thisreduces the artifactual decreased myocardial perfusion andimproves the diagnostic accuracy for the detection of CADcompared with other 99mTc-labeled perfusion agents [24]
Unsurprisingly Braat et al [35] and Germano et al [36]noted that technetium-labeled MPI agents with a fast liverclearance can significantly reduce the photon scatter fromthe liver into the inferior walls but the radioactivity may betransferred to the gastrointestinal area and increased bowel
and gastric activity were seen as a problem associated withhigh liver uptake in the visual and quantitative interpretationof the inferoposterior myocardial walls In this study boweluptakewas frequently seen on the 99mTc-N-DBODC5 imagesbut did not result in any nondiagnostic scans
For the detection of coronary disease in patients 99mTc-MIBI produced abnormal results for MPI in four patientswho had no angiographically detected stenosis Some of thesefalse-positive results may be due in part to the liver-to-heart artifacts In this study we could classify fixed perfusiondefects as soft-tissue attenuation artifacts or infarcts by usinggated SPECT Because an artifactual defect would shownormal contraction (wall motion or thickening) on a gatedimage artifacts can be differentiated from a true infarct [37]
For the detection of individual vessel stenosis on theother hand angiography agreement was very good for 99mTc-N-DBODC5 (120581=071 for RCA) andmoderate for 99mTc-MIBI(120581 = 048 for RCA) For LAD and LCX arteries stenosis thediagnosis of myocardial ischemia on 99mTc-N-DBODC5 and99mTc-MIBI study had the same specificity and it was similarto that of two tracer to diagnose sensitivity and accuracy ofmyocardial ischemia Abnormal results of myocardial imagesin individual RCA vessel stenosis (six arteries-stenosed ves-sels for RCA) were obtained in the 99mTc-MIBI studieswhile CA and 99mTc-N-DBODC5 studies showed normalfindings in the same individual RCA vessel territories Someof these false-positive results may be due to photon scatterfrom the liver and intestine into the inferoposterior walls99mTc-MIBI concentration located below the left diaphragm(ie liver and bowel) may cause an artifactual perfusiondefect in the adjacent myocardial a phenomenon knownas the ldquoliver-heart artifactrdquo [36 38] Moreover the inferiorand inferoposterior regions were dominated mainly by RCAterritories corresponding to the myocardial short axis andvertical long axis while arteries regions which LAD and LCXdominated were less interfered from ldquoliver-heart artifactrdquoFinally for clinical applications 99mTc-N-DBODC5 offersbetter determination of detects particularly in the infero-posterior wall on myocardial images A typical example of afalse-positive perfusion defect in the inferior wall is shown inFigure 5
On a segment-to-segment basis complete agreementbetween the two imaging agents occurred in 71 of segments
8 BioMed Research International
(a) (b) (c)
Figure 5 Serial short-axis and vertical long-axis slices of stress-rest 99mTc-N-DBODC5 images (b) and stress-rest 99mTc-MIBI images (c) ofa representative patient with normal CA (a) Because of intense uptake of technetium 99mTc-MIBI in the liver high liver background activitycan be observed Furthermore a false-positive myocardial perfusion defect was also seen in the inferoposterior wall segments supplied bythe RCA territory (white arrows) Importantly however at stress and rest the inferoposterior wall segments of 99mTc-N-DBODC5 imagesare clearly separated from the subdiaphragmatic activity
However more myocardial segments were nonreversible on99mTc-MIBI images than on 99mTc-N-DBODC5 images Onthe contrary 99mTc-N-DBODC5MPI had a higher reversibledefect than that of 99mTc-MIBI A possible reason for thisdifference may be due in part to the ldquoliver-heart artifactrdquoThe presence of high liver activity adjacent to the inferior wallresults fromoversubtraction of activity from the inferior wallTherefore the more ldquoliver-heart artifactrdquo in the inferoposte-rior wall on myocardial images the more false nonreversibledefects in the inferoposterior wall on myocardial perfusionsegmental analysis In other words the less reversible defectsin the inferoposterior wall were deduced on 99mTc-MIBIMPIsegmental analysis
More importantly however the main advantage andclinical value of 99mTc-N-DBODC5 can improve diagnosticspecificity and reduce the false-positive diagnosis of patientsand associated treatment fees
5 Limitations
In this study we did not attempt to assess the absolute diag-nostic accuracy of 99mTc-N-DBODC5 because definitive
conclusions in this regard can only be drawn by study-ing larger patient cohort In addition although 99mTc-N-DBODC5 did not track flow as well as 201Tl the magni-tudes of the pharmacologic stress-induced perfusion defectswere comparable to those previously reported for 99mTc-tetrofosmin Thus direct comparison between 99mTc-N-DBODC5 and 99mTc-tetrofosmin should be further provedin the same patient population Overall 99mTc-N-DBODC5MPI will become an important diagnostic tool in the evalua-tion of myocardial perfusion
6 Conclusion
This preliminary clinical study showed that 99mTc-N-DBODC5 and 99mTc-MIBI MPI provide comparable diag-nostic information for patients undergoing exercise rest fordetection of CAD In addition 99mTc-N-DBODC5 doesnot exhibit the disadvantages of 99mTc-MIBI in this studyBy contrast because of its high heart-organ count ratioin comparison to 99mTc-MIBI it improves high degree ofdiagnostic concordance in defining or excluding perfusionabnormalities in patients with CADTherefore it can become
BioMed Research International 9
the agent of choice for the evaluation ofmyocardial perfusionand ventricular function in patients with CAD
Abbreviations
CAD Coronary artery diseaseMPI Myocardial perfusion imagingCA Coronary angiographySPECT Single-photon emission computed
tomographyPET Positron emission computed
tomography99mTc-MIBI Technetium 99m sestamibi99mTc-N-DBODC5 99mTc(N)(DBODC)(PNP5)201Tl Thallium-20199mTc-tetrofosmin Technetium-99m-tetrofosminROI Regions of interestLAD Left anterior descending arteryLCX Left circumflex arteryRCA Right coronary arterySSS Summed stress scoreSRS Summed rest scoreSDS Summed difference scoreEDV End-diastolic volumeESV End-systolic volumeLVEF Left ventricular ejection fraction
Ethics Statement
This study was conducted in accordance with the HelsinkiDeclaration All subjects provided written informed consentbefore MPI acknowledging that they understood their rightsand obligations This study was approved by the ResearchEthics Committee of Shanxi Medical University
Conflict of Interests
The authors declare that they have no conflict of interest
Acknowledgments
This research is partly supported by Grants from the YouthScience and Technology Research Foundation of ShanxiProvince (no 2009021043-3) The authors acknowledge themembers of the participating staff for their contribution tothis clinical study
References
[1] National Hospital Discharge Survey National Health StatisticsReport no 5 2006
[2] J He D Gu X Wu et al ldquoMajor causes of death among menand women in Chinardquo The New England Journal of Medicinevol 353 no 11 pp 1124ndash1134 2005
[3] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardized myocardial sementation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare pro-fessionals from the Cardiac Imaging Committee of the Council
on Clinical Cardiology of the American Heart AssociationrdquoCirculation vol 105 no 4 pp 539ndash542 2002
[4] R J Gibbons J Abrams K Chatterjee et al ldquoACCAHA 2002guideline update for the management of patients with chronicstable anginamdashsummary article a report of the AmericanCollege of CardiologyAmerican Heart Association Task Forceon Practice Guidelines (Committee on the Management ofPatients With Chronic Stable Angina)rdquo Journal of the AmericanCollege of Cardiology vol 41 no 1 pp 159ndash168 2003
[5] WWijns P Kolh N Danchin et al ldquoGuidelines on myocardialrevascularizationrdquo European Heart Journal vol 31 pp 2501ndash2555 2010
[6] J M Jensen K A Oslashvrehus L H Nielsen J K Jensen HM Larsen and B L Noslashrgaard ldquoParadigm of pretest riskstratification before coronary computed tomographyrdquo Journalof Cardiovascular Computed Tomography vol 3 no 6 pp 386ndash391 2009
[7] N RMollet F Cademartiri C VanMieghem et al ldquoAdjunctivevalue of CT coronary angiography in the diagnostic work-up ofpatients with typical angina pectorisrdquo European Heart Journalvol 28 no 15 pp 1872ndash1878 2007
[8] R G E J Groutars J F Verzijlbergen M M C Tiel-Van Buulet al ldquoThe accuracy of 1-day dual-isotopemyocardial SPECT ina population with high prevalence of coronary artery diseaserdquoInternational Journal of Cardiovascular Imaging vol 19 no 3pp 229ndash238 2003
[9] M R Patel E D Peterson D Dai et al ldquoLow diagnostic yieldof elective coronary angiographyrdquo The New England Journal ofMedicine vol 362 no 10 pp 886ndash895 2010
[10] ldquoPharmacologic stress testingrdquo in Nuclear Cardiac ImagingPriniciples and Applications A E Iskandrian and E V GarciaEds pp 293ndash315 OxfordUniversity Press NewYork NY USA4th edition 2008
[11] R R Russell III and B L Zaret ldquoNuclear cardiology presentand futurerdquo Current Problems in Cardiology vol 31 no 9 pp557ndash629 2006
[12] G Germano H Kiat P B Kavanagh et al ldquoAutomatic quan-tification of ejection fraction from gated myocardial perfusionSPECTrdquo Journal of Nuclear Medicine vol 36 no 11 pp 2138ndash2147 1995
[13] S R Underwood C Anagnostopoulos M Cerqueira et alldquoMyocardial perfusion scintigraphy the evidencerdquo EuropeanJournal of Nuclear Medicine and Molecular Imaging vol 31 pp261ndash291 2004
[14] J Heo and A S Iskandrian ldquoTechnetium-labeled myocardialperfusion agentsrdquo Cardiology Clinics vol 12 no 2 pp 187ndash1981994
[15] B L Zaret P Rigo F J T Wackers et al ldquoMyocardial perfusionimaging with 99mTc tetrofosmin comparison to 201Tl imagingand coronary angiography in a phase III multicenter trialrdquoCirculation vol 91 no 2 pp 313ndash319 1995
[16] J J Mahmarian and M S Verani ldquoExercise thallium-201perfusion scintigraphy in the assessment of coronary arterydiseaserdquoAmerican Journal of Cardiology vol 67 no 14 pp 2Dndash11D 1991
[17] D D Miller L T Younis B R Chaitman and H StratmannldquoDiagnostic accuracy of dipyridamole technetium 99m-labeledsestamibi myocardial tomography for detection of coronaryartery diseaserdquo Journal of Nuclear Cardiology vol 4 no 1 pp18ndash24 1997
10 BioMed Research International
[18] Z He A S Iskandrian N C Gupta and M S Verani ldquoAssess-ing coronary artery disease with dipyridamole technetium-99m-tetrofosmin SPECT amulticenter trialrdquo Journal of NuclearMedicine vol 38 no 1 pp 44ndash48 1997
[19] A Boschi C Bolzati L Uccelli et al ldquoA class of asymmetricalnitrido 99mTc heterocomplexes as heart imaging agents withimproved biological propertiesrdquoNuclearMedicine Communica-tions vol 23 no 7 pp 689ndash693 2002
[20] A Boschi L Uccelli C Bolzati et al ldquoSynthesis and biologicevaluation of monocationic asymmetric 99mTc-nitride hetero-complexes showing high heart uptake and improved imagingpropertiesrdquo Journal of Nuclear Medicine vol 44 no 5 pp 806ndash814 2003
[21] C Bolzati M Cavazza-Ceccato S Agostini S TokunagaD Casara and G Bandoli ldquoSubcellular distribution andmetabolism studies of the potential myocardial imaging agent[99mTc(N)(DBODC)(PNP5)]+rdquo Journal of Nuclear Medicinevol 49 no 8 pp 1336ndash1344 2008
[22] C Cittanti L Uccelli M Pasquali et al ldquoWhole-body biodis-tribution and radiation dosimetry of the new cardiac tracer99mTc-N-DBODCrdquo Journal of Nuclear Medicine vol 49 no 8pp 1299ndash1304 2008
[23] K Hatada L M Riou M Ruiz et al ldquo99mTc-N-DBODC5a new myocardial perfusion imaging agent with rapid liverclearance comparison with 99mTc-sestamibi and 99mTc-tetrofosmin in ratsrdquo Journal of Nuclear Medicine vol 45 no 12pp 2095ndash2101 2004
[24] T Takeda J Wu and T T Lwin ldquo99mTc-N-DBODC5 a novelmyocardial perfusion imaging agent for diagnosis of coronaryartery disease a reviewrdquo Recent Patents on Cardiovascular DrugDiscovery vol 1 no 2 pp 161ndash166 2006
[25] K Hatada M Ruiz L M Riou et al ldquoOrgan biodistributionand myocardial uptake washout and redistribution kinetics ofTc-99m N-DBODC5 when injected during vasodilator stressin canine models of coronary stenosesrdquo Journal of NuclearCardiology vol 13 no 6 pp 779ndash790 2006
[26] W Zhang W Fang B Li X Wang and Z He ldquoExperimentalstudy of [99mTc(PNP5) (DBODC)]+ as a new myocardialperfusion imaging agentrdquo Cardiology vol 112 no 2 pp 89ndash972009
[27] M E Marmion S R Woulfe W L Neumann D L Nosco andE Deutsch ldquoPreparation and characterization of technetiumcomplexes with Schiff base and phosphine coordination 1Complexes of technetium-99g and -99m with substitutedacac2en and trialkyl phosphines (where acac2en = NN1015840-ethylenebis[acetylacetone iminato])rdquo Nuclear Medicine andBiology vol 26 no 7 pp 755ndash770 1999
[28] C Bolzati L Uccelli A Boschi et al ldquoSynthesis of a novel classof nitrido Tc-99m radiopharmaceuticals with phosphino-thiolligands showing transient heart uptakerdquo Journal of InorganicBiochemistry vol 78 no 3 pp 369ndash374 2000
[29] M J Henzlova M D Cerqueira J J Mahmarian and S YaoldquoStress protocols and tracersrdquo Journal of Nuclear Cardiology vol13 no 6 pp e80ndashe90 2006
[30] C L Hansen R A Goldstein D S Berman et al ldquoMyocardialperfusion and function single photon emission computedtomographyrdquo Journal of Nuclear Cardiology vol 13 no 6 ppe97ndashe120 2006
[31] P Flamen A Bossuyt and P R Franken ldquoTechnetium-99m-tetrofosmin in dipyridamole-stressmyocardial SPECT imagingintraindividual comparison with technetium-99m-sestamibirdquoJournal of Nuclear Medicine vol 36 no 11 pp 2009ndash2015 1995
[32] N Tamaki N Takahashi M Kawamoto et al ldquoMyocardialtomography using technetium-99m-tetrofosmin to evaluatecoronary artery diseaserdquo Journal of Nuclear Medicine vol 35no 4 pp 594ndash600 1994
[33] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardizedmyocardial segmentation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare profes-sionals from the Cardiac Imaging Committee of the Councilon Clinical Cardiology of the American Heart AssociationrdquoJournal of Nuclear Cardiology vol 9 no 2 pp 240ndash245 2002
[34] T Sharir G Germano X Kang et al ldquoPrediction of myocardialinfarction versus cardiac death by gated myocardial perfusionSPECT risk stratification by the amount of stress-inducedischemia and the poststress ejection fractionrdquo Journal of NuclearMedicine vol 42 no 6 pp 831ndash837 2001
[35] S H Braat B Leclercq R Itti A Lahiri B Sridhara and PRigo ldquoMyocardial imaging with technetium-99m-tetrofosmincomparison of one-day and two-day protocolsrdquo Journal ofNuclear Medicine vol 35 no 10 pp 1581ndash1585 1994
[36] G Germano T Chua H Kiat J S Areeda andD S Berman ldquoAquantitative phantom analysis of artifacts due to hepatic activ-ity in technetium-99m myocardial perfusion SPECT studiesrdquoJournal of Nuclear Medicine vol 35 no 2 pp 356ndash359 1994
[37] A K Paul andH A Nabi ldquoGatedmyocardial perfusion SPECTbasic principles technical aspects and clinical applicationsrdquoJournal of Nuclear Medicine Technology vol 32 no 4 pp 179ndash187 2004
[38] J Nuyts P Dupont V Van den Maegdenbergh S Vleugels PSuetens and L Mortelmans ldquoA study of the liver-heart artifactin emission tomographyrdquo Journal of Nuclear Medicine vol 36no 1 pp 133ndash139 1995
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 5
(a) (b)
(c)
Figure 4 Abnormal MPI in the vertical long-axis slices of a representative patient Both 99mTc-N-DBODC5 (a) and 99mTc-MIBI (b) imagesdemonstrate an inferoposterior defect (white arrows) The defect is well visualized on two tracer images corresponding to the CA resultThis coronary angiography (c) detected a stenosis of 90 in the RCA The concordance for diagnosis of myocardial ischemia was seen on99mTc-N-DBODC5 and 99mTc-MIBI studies
rest images respectivelyThe average heart-to-intestine ratiosof 99mTc-MIBI were 162 plusmn 001 and 091 plusmn 000 for stressand rest images respectively 99mTc-N-DBODC5 studies hada significantly higher heart-to-organ count ratio comparedwith 99mTc-MIBI studies (119875 lt 005)
33 Image Quality In the stress perfusion imaging 99mTc-N-DBODC5MPI was superior in quality to 99mTc-MIBIMPI in37 of the 46 patients studied In the remaining nine patientsthe MPI was judged to be of equal quality In the restingperfusion imaging 99mTc-N-DBODC5 images were superiorin all the patients studied In general the 99mTc-N-DBODC5MPI had more counts with less statistical noise less traceractivity below the diaphragm and desirable heart-to-organcount ratio compared with 99mTc-MIBI MPI
34 Gated SPECT Findings Table 2 shows the results ofscan segments between the 99mTc-N-DBODC5 and 99mTc-MIBI MPI Of the 782 segments that could be interpretedby both techniques 302 were concordantly normal 119 wereconcordantly reversible and 136 were concordantly nonre-versible 99mTc-N-DBODC5SPECTdetectedmore reversibledefects than did 99mTc-MIBI SPECT (240 versus 140 119875 lt005 McNemar test) 99mTc-MIBI SPECT identified more
nonreversible defects than did 99mTc-N-DBODC5 SPECT(312 versus 152 119875 lt 0001 McNemar test) Seventy-onesegments interpreted as normal on 99mTc-N-DBODC5 cor-responded to nonreversible defects on 99mTc-MIBI SPECTimages In contrast 12 normal 99mTc-MIBI segments cor-responded to nonreversible defects on 99mTc-N-DBODC5images When the patterns of uptake (normal reversibledefect and nonreversible defect) of 99mTc-N-DBODC5 and99mTc-MIBI were compared there was concordance in 71(557782) of segments
Table 3 shows the results of left ventricular functionparameters in the two techniques used In this study theend-diastolic volume (EDV) end-systolic volume (ESV) leftventricular ejection fraction (LVEF) and transient ventric-ular dysfunction (TID) were assessed by MPI using twotracers No statistically significant differences in MPI param-eters were observed between the 99mTc-MIBI and 99mTc-N-DBODC5 studies However the scores of myocardialperfusion defects for the detection of CAD were higher with99mTc-MIBI than with 99mTc-N-DBODC5 (119875 = 0012 forSSS 119875 = 0020 for SDS resp)
35 Detection of CAD Table 4 shows the sensitivity andspecificity of two tracers in diagnosing CAD Based on CA
6 BioMed Research International
Table 2 The comparison of myocardial perfusion in a total of 782 segments with 99mTc-N-DBODC5 and 99mTc-MIBI SPECT exerciseimaging
99mTc-N-DBODC599mTc-MIBI Total
Normal Reversible defect Nonreversible defectlowast
Normal 302 (39) 17 (2) 71 (9) 390Reversible defectlowast 16 (2) 119 (15) 105 (13) 240Nonreversible defect 12 (2) 4 (1) 136 (17) 152Total 330 140 312 782Data are presented as number lowast119875 lt 0001 99mTc-MIBI versus 99mTc-N-DBODC5 for nonreversible defect segments lowast119875 lt 005 99mTc-N-DBODC5 versus99mTc-MIBI for reversible defect segments McNemar test was used
Table 3 MPI findings of two tracers on left ventricular functionparameters and ischemia scores in 46 patients
Parameter 99mTc-MIBI 99mTc-N-DBODC5LVEF ()
Exercise 542 plusmn 113 567 plusmn 92Rest 631 plusmn 85 648 plusmn 79
EDV (mL)Exercise 815 plusmn 186 832 plusmn 163Rest 973 plusmn 164 991 plusmn 137
ESV (mL)Exercise 432 plusmn 97 414 plusmn 123Rest 594 plusmn 136 602 plusmn 98
SSS 121 plusmn 14995333 96 plusmn 16SRS 72 plusmn 08 79 plusmn 09SDS 42 plusmn 05995333 36 plusmn 04TID 096 plusmn 006 094 plusmn 002Data are presented asmeanplusmn SD or number () as appropriate995333statisticallysignificant 99mTc-MIBI versus 99mTc-N-DBODC5 (119875 lt 005) pairedStudentrsquos 119905-test was used LVEF left ventricular ejection fraction EDVend-diastolic volume ESV end-systolic volume SSS summed stress scoresSRS summed rest scores SDS summed difference scores TID transientventricular dysfunction
overall figures for sensitivity and specificity in identificationof CAD were 86 (2529) and 65 (1117) for 99mTc-MIBI imaging On the other hand the overall sensitivityand specificity for the detection of CAD were 86 (2529)and 88 (1517) for 99mTc-N-DBODC5 SPECT studies Theconcordance of ischemia diagnosis sensitivity of a represen-tative patient for the two tracers is shown in Figure 4 Theaccuracy was 078 for 99mTc-MIBI and 087 for 99mTc-N-DBODC5 Angiography agreement was very good for 99mTc-N-DBODC5 (120581 = 073) and moderate for 99mTc-MIBI (120581 =052) Specificity and accuracy were not significantly differentbut better for the 99mTc-N-DBODC5 group when comparedto 99mTc-MIBI SPECT (specificity 88-65 accuracy 87-78)
36 Detection of Disease in Individual Coronary VesselsTable 4 also shows the sensitivity and specificity of the twotracers in detecting individual-stenosed vessels Of a total of138 arteries in 46 patients 48 arteries had significant stenosesand 90 had insignificant lesions or were normal Overall
figures for sensitivity and specificity in identifying individual-stenosed vessels were 67 (3248) and 86 (7790) for 99mTc-MIBI imaging overall sensitivity and specificity to diagnoseindividual significantly stenosed vessels were 69 (3348)and 92 (8390) for 99mTc-N-DBODC5 SPECT studies
On the other hand sensitivity and specificity for RCAstenosis vessel lesion detection using 99mTc-MIBI MPI were87 and 68 compared to 87 and 87 for 99mTc-N-DBODC5 MPI LAD stenosis (53 sensitivity and 96specificity for 99mTc-MIBI 63 sensitivity and 96 speci-ficity for 99mTc-N-DBODC5 resp) and left circumflex(LCX) (64 sensitivity and 94 specificity for 99mTc-MIBI57 sensitivity and 94 specificity for 99mTc-N-DBODC5resp) Angiography agreement was very good for 99mTc-N-DBODC5 (120581 = 063 for LAD 120581 = 071 for RCA resp) andmoderate for 99mTc-MIBI (120581 = 052 for LAD 120581 = 048 forRCA resp) In contrast the angiography agreement was verygood for 99mTc-MIBI (120581 = 062 for LCX) and moderate for99mTc-N-DBODC5 (120581 = 055 for LCX) (Table 4) Overall thespecificity of 99mTc-N-DBODC5 SPECT to detect individualRCA stenosis was better (2731 87) than that of 99mTc-MIBISPECT (2131 68) despite having no statistical significance
4 Discussion
These preliminary results demonstrate that stress-restmyocardial perfusion SPECT with 99mTc-N-DBODC5 isa sensitive method for detecting CAD and identifyingstenosed coronary arteries For the detection of CADmore importantly 99mTc-N-DBODC5 MPI reached goodagreement compared with CA (120581 = 073)
41 Advantages of 99119898Tc-N-DBODC5 99mTc-N-DBODC5 isa new lipophilic monocationic and nitride 99mTc-labeledtracer that is rapidly cleared from the liver after intravenousinjection It possesses good stability under physiological con-ditions Importantly 99mTc-N-DBODC5 exhibits more rapidliver washout than either 99mTc-MIBI or 99mTc-tetrofosminFor example at 60min after injection in rats the heartliverratio of 99mTc-N-DBODC5 is approximately ten times higherthan that of 99mTc-MIBI or 99mTc-tetrofosmin Preclinicalstudies have shown that 99mTc-N-DBODC5 SPECT canidentify previous ischemia as areas of reduced tracer uptake[25 26] Furthermore the rapid liver clearance and highuptake in the myocardium of 99mTc-N-DBODC5 will allow
BioMed Research International 7
Table 4 Sensitivity specificity and diagnostic accuracy of scintigraphic perfusion studies and agreement with coronary angiography
Overall LAD LCX RCAMIBI DBODC MIBI DBODC MIBI DBODC MIBI DBODC
No of disease 25 25 10 12 9 8 13 13Sensitivity () 86 86 53 63 64 57 87 87Specificity () 65 88 96 96 94 94 68 87Accuracy () 78 87 78 83 85 83 74 87998771Kappa (120581) 053 073 052 063 062 055 048 071Data are presented as number () MIBI = 99mTc-MIBI DBODC = 99mTc-N-DBODC5 LAD left anterior descending coronary artery LCX left circumflexcoronary artery RCA right coronary artery 998771CA was used as the ldquogold standardrdquo for the calculation of the 120581 which is determine between SPECT MPI andCA If there is no agreement 120581 = 020ndash039 moderate agreement 120581 = 040ndash059 very good agreement 120581 = 060ndash079 excellent agreement 120581 = 080ndash100
SPECT images of the left ventricle to be acquired earlyand with excellent quality [22] The ratios of heart-to-liverwere consistent with the previous report study [22] Thesecharacteristics are suitable particularly for patients withsuspected acute coronary syndromes and without diagnosticelectrocardiogram because early diagnosis is needed in suchpatients for timely therapeutic decisionmaking 99mTc-MIBIon the other hand may require a wait time of up to 1 h forimaging
In the present study the heart-to-organ count ratio of99mTc-N-DBODC5 MPI was superior to that of 99mTc-MIBIin 46 patients Compared with 99mTc-MIBI MPI 99mTc-N-DBODC5 MPI had better image quality in most patientsFurthermore in this study exercise stress myocardial imageswere performed 30min after 99mTc-N-DBODC5 injectionand excellent MPI with high contrast was possible
42 Clinical Value of 99119898Tc-N-DBODC5 for the Detection ofCAD This clinical trial assesses the diagnostic value of thisagent to detect CAD comparing it with stress 99mTc-MIBIMPI and CA
In this study compared with 99mTc-MIBI MPI 99mTc-N-DBODC5MPI indicates the same sensitivity and better speci-ficity and accuracy to detect coronary disease in patientsalthough none of the differences were significant On theother hand more importantly angiography agreement wasvery good for 99mTc-N-DBODC5 (120581 = 073) and moderatefor 99mTc-MIBI (120581 = 052) thus compared with 99mTc-MIBI MPI it provides a high degree of concordance for theevaluation of CAD specifically in excluding perfusion abnor-malities in patients with suspected CAD Possible reasons forthis difference may be fast liver clearance favorable heart-to-organ ratio and high image quality 99mTc-N-DBODC5with rapid liver clearancemay significantly reduce the photonscatter from the liver into the inferoposterior walls Thisreduces the artifactual decreased myocardial perfusion andimproves the diagnostic accuracy for the detection of CADcompared with other 99mTc-labeled perfusion agents [24]
Unsurprisingly Braat et al [35] and Germano et al [36]noted that technetium-labeled MPI agents with a fast liverclearance can significantly reduce the photon scatter fromthe liver into the inferior walls but the radioactivity may betransferred to the gastrointestinal area and increased bowel
and gastric activity were seen as a problem associated withhigh liver uptake in the visual and quantitative interpretationof the inferoposterior myocardial walls In this study boweluptakewas frequently seen on the 99mTc-N-DBODC5 imagesbut did not result in any nondiagnostic scans
For the detection of coronary disease in patients 99mTc-MIBI produced abnormal results for MPI in four patientswho had no angiographically detected stenosis Some of thesefalse-positive results may be due in part to the liver-to-heart artifacts In this study we could classify fixed perfusiondefects as soft-tissue attenuation artifacts or infarcts by usinggated SPECT Because an artifactual defect would shownormal contraction (wall motion or thickening) on a gatedimage artifacts can be differentiated from a true infarct [37]
For the detection of individual vessel stenosis on theother hand angiography agreement was very good for 99mTc-N-DBODC5 (120581=071 for RCA) andmoderate for 99mTc-MIBI(120581 = 048 for RCA) For LAD and LCX arteries stenosis thediagnosis of myocardial ischemia on 99mTc-N-DBODC5 and99mTc-MIBI study had the same specificity and it was similarto that of two tracer to diagnose sensitivity and accuracy ofmyocardial ischemia Abnormal results of myocardial imagesin individual RCA vessel stenosis (six arteries-stenosed ves-sels for RCA) were obtained in the 99mTc-MIBI studieswhile CA and 99mTc-N-DBODC5 studies showed normalfindings in the same individual RCA vessel territories Someof these false-positive results may be due to photon scatterfrom the liver and intestine into the inferoposterior walls99mTc-MIBI concentration located below the left diaphragm(ie liver and bowel) may cause an artifactual perfusiondefect in the adjacent myocardial a phenomenon knownas the ldquoliver-heart artifactrdquo [36 38] Moreover the inferiorand inferoposterior regions were dominated mainly by RCAterritories corresponding to the myocardial short axis andvertical long axis while arteries regions which LAD and LCXdominated were less interfered from ldquoliver-heart artifactrdquoFinally for clinical applications 99mTc-N-DBODC5 offersbetter determination of detects particularly in the infero-posterior wall on myocardial images A typical example of afalse-positive perfusion defect in the inferior wall is shown inFigure 5
On a segment-to-segment basis complete agreementbetween the two imaging agents occurred in 71 of segments
8 BioMed Research International
(a) (b) (c)
Figure 5 Serial short-axis and vertical long-axis slices of stress-rest 99mTc-N-DBODC5 images (b) and stress-rest 99mTc-MIBI images (c) ofa representative patient with normal CA (a) Because of intense uptake of technetium 99mTc-MIBI in the liver high liver background activitycan be observed Furthermore a false-positive myocardial perfusion defect was also seen in the inferoposterior wall segments supplied bythe RCA territory (white arrows) Importantly however at stress and rest the inferoposterior wall segments of 99mTc-N-DBODC5 imagesare clearly separated from the subdiaphragmatic activity
However more myocardial segments were nonreversible on99mTc-MIBI images than on 99mTc-N-DBODC5 images Onthe contrary 99mTc-N-DBODC5MPI had a higher reversibledefect than that of 99mTc-MIBI A possible reason for thisdifference may be due in part to the ldquoliver-heart artifactrdquoThe presence of high liver activity adjacent to the inferior wallresults fromoversubtraction of activity from the inferior wallTherefore the more ldquoliver-heart artifactrdquo in the inferoposte-rior wall on myocardial images the more false nonreversibledefects in the inferoposterior wall on myocardial perfusionsegmental analysis In other words the less reversible defectsin the inferoposterior wall were deduced on 99mTc-MIBIMPIsegmental analysis
More importantly however the main advantage andclinical value of 99mTc-N-DBODC5 can improve diagnosticspecificity and reduce the false-positive diagnosis of patientsand associated treatment fees
5 Limitations
In this study we did not attempt to assess the absolute diag-nostic accuracy of 99mTc-N-DBODC5 because definitive
conclusions in this regard can only be drawn by study-ing larger patient cohort In addition although 99mTc-N-DBODC5 did not track flow as well as 201Tl the magni-tudes of the pharmacologic stress-induced perfusion defectswere comparable to those previously reported for 99mTc-tetrofosmin Thus direct comparison between 99mTc-N-DBODC5 and 99mTc-tetrofosmin should be further provedin the same patient population Overall 99mTc-N-DBODC5MPI will become an important diagnostic tool in the evalua-tion of myocardial perfusion
6 Conclusion
This preliminary clinical study showed that 99mTc-N-DBODC5 and 99mTc-MIBI MPI provide comparable diag-nostic information for patients undergoing exercise rest fordetection of CAD In addition 99mTc-N-DBODC5 doesnot exhibit the disadvantages of 99mTc-MIBI in this studyBy contrast because of its high heart-organ count ratioin comparison to 99mTc-MIBI it improves high degree ofdiagnostic concordance in defining or excluding perfusionabnormalities in patients with CADTherefore it can become
BioMed Research International 9
the agent of choice for the evaluation ofmyocardial perfusionand ventricular function in patients with CAD
Abbreviations
CAD Coronary artery diseaseMPI Myocardial perfusion imagingCA Coronary angiographySPECT Single-photon emission computed
tomographyPET Positron emission computed
tomography99mTc-MIBI Technetium 99m sestamibi99mTc-N-DBODC5 99mTc(N)(DBODC)(PNP5)201Tl Thallium-20199mTc-tetrofosmin Technetium-99m-tetrofosminROI Regions of interestLAD Left anterior descending arteryLCX Left circumflex arteryRCA Right coronary arterySSS Summed stress scoreSRS Summed rest scoreSDS Summed difference scoreEDV End-diastolic volumeESV End-systolic volumeLVEF Left ventricular ejection fraction
Ethics Statement
This study was conducted in accordance with the HelsinkiDeclaration All subjects provided written informed consentbefore MPI acknowledging that they understood their rightsand obligations This study was approved by the ResearchEthics Committee of Shanxi Medical University
Conflict of Interests
The authors declare that they have no conflict of interest
Acknowledgments
This research is partly supported by Grants from the YouthScience and Technology Research Foundation of ShanxiProvince (no 2009021043-3) The authors acknowledge themembers of the participating staff for their contribution tothis clinical study
References
[1] National Hospital Discharge Survey National Health StatisticsReport no 5 2006
[2] J He D Gu X Wu et al ldquoMajor causes of death among menand women in Chinardquo The New England Journal of Medicinevol 353 no 11 pp 1124ndash1134 2005
[3] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardized myocardial sementation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare pro-fessionals from the Cardiac Imaging Committee of the Council
on Clinical Cardiology of the American Heart AssociationrdquoCirculation vol 105 no 4 pp 539ndash542 2002
[4] R J Gibbons J Abrams K Chatterjee et al ldquoACCAHA 2002guideline update for the management of patients with chronicstable anginamdashsummary article a report of the AmericanCollege of CardiologyAmerican Heart Association Task Forceon Practice Guidelines (Committee on the Management ofPatients With Chronic Stable Angina)rdquo Journal of the AmericanCollege of Cardiology vol 41 no 1 pp 159ndash168 2003
[5] WWijns P Kolh N Danchin et al ldquoGuidelines on myocardialrevascularizationrdquo European Heart Journal vol 31 pp 2501ndash2555 2010
[6] J M Jensen K A Oslashvrehus L H Nielsen J K Jensen HM Larsen and B L Noslashrgaard ldquoParadigm of pretest riskstratification before coronary computed tomographyrdquo Journalof Cardiovascular Computed Tomography vol 3 no 6 pp 386ndash391 2009
[7] N RMollet F Cademartiri C VanMieghem et al ldquoAdjunctivevalue of CT coronary angiography in the diagnostic work-up ofpatients with typical angina pectorisrdquo European Heart Journalvol 28 no 15 pp 1872ndash1878 2007
[8] R G E J Groutars J F Verzijlbergen M M C Tiel-Van Buulet al ldquoThe accuracy of 1-day dual-isotopemyocardial SPECT ina population with high prevalence of coronary artery diseaserdquoInternational Journal of Cardiovascular Imaging vol 19 no 3pp 229ndash238 2003
[9] M R Patel E D Peterson D Dai et al ldquoLow diagnostic yieldof elective coronary angiographyrdquo The New England Journal ofMedicine vol 362 no 10 pp 886ndash895 2010
[10] ldquoPharmacologic stress testingrdquo in Nuclear Cardiac ImagingPriniciples and Applications A E Iskandrian and E V GarciaEds pp 293ndash315 OxfordUniversity Press NewYork NY USA4th edition 2008
[11] R R Russell III and B L Zaret ldquoNuclear cardiology presentand futurerdquo Current Problems in Cardiology vol 31 no 9 pp557ndash629 2006
[12] G Germano H Kiat P B Kavanagh et al ldquoAutomatic quan-tification of ejection fraction from gated myocardial perfusionSPECTrdquo Journal of Nuclear Medicine vol 36 no 11 pp 2138ndash2147 1995
[13] S R Underwood C Anagnostopoulos M Cerqueira et alldquoMyocardial perfusion scintigraphy the evidencerdquo EuropeanJournal of Nuclear Medicine and Molecular Imaging vol 31 pp261ndash291 2004
[14] J Heo and A S Iskandrian ldquoTechnetium-labeled myocardialperfusion agentsrdquo Cardiology Clinics vol 12 no 2 pp 187ndash1981994
[15] B L Zaret P Rigo F J T Wackers et al ldquoMyocardial perfusionimaging with 99mTc tetrofosmin comparison to 201Tl imagingand coronary angiography in a phase III multicenter trialrdquoCirculation vol 91 no 2 pp 313ndash319 1995
[16] J J Mahmarian and M S Verani ldquoExercise thallium-201perfusion scintigraphy in the assessment of coronary arterydiseaserdquoAmerican Journal of Cardiology vol 67 no 14 pp 2Dndash11D 1991
[17] D D Miller L T Younis B R Chaitman and H StratmannldquoDiagnostic accuracy of dipyridamole technetium 99m-labeledsestamibi myocardial tomography for detection of coronaryartery diseaserdquo Journal of Nuclear Cardiology vol 4 no 1 pp18ndash24 1997
10 BioMed Research International
[18] Z He A S Iskandrian N C Gupta and M S Verani ldquoAssess-ing coronary artery disease with dipyridamole technetium-99m-tetrofosmin SPECT amulticenter trialrdquo Journal of NuclearMedicine vol 38 no 1 pp 44ndash48 1997
[19] A Boschi C Bolzati L Uccelli et al ldquoA class of asymmetricalnitrido 99mTc heterocomplexes as heart imaging agents withimproved biological propertiesrdquoNuclearMedicine Communica-tions vol 23 no 7 pp 689ndash693 2002
[20] A Boschi L Uccelli C Bolzati et al ldquoSynthesis and biologicevaluation of monocationic asymmetric 99mTc-nitride hetero-complexes showing high heart uptake and improved imagingpropertiesrdquo Journal of Nuclear Medicine vol 44 no 5 pp 806ndash814 2003
[21] C Bolzati M Cavazza-Ceccato S Agostini S TokunagaD Casara and G Bandoli ldquoSubcellular distribution andmetabolism studies of the potential myocardial imaging agent[99mTc(N)(DBODC)(PNP5)]+rdquo Journal of Nuclear Medicinevol 49 no 8 pp 1336ndash1344 2008
[22] C Cittanti L Uccelli M Pasquali et al ldquoWhole-body biodis-tribution and radiation dosimetry of the new cardiac tracer99mTc-N-DBODCrdquo Journal of Nuclear Medicine vol 49 no 8pp 1299ndash1304 2008
[23] K Hatada L M Riou M Ruiz et al ldquo99mTc-N-DBODC5a new myocardial perfusion imaging agent with rapid liverclearance comparison with 99mTc-sestamibi and 99mTc-tetrofosmin in ratsrdquo Journal of Nuclear Medicine vol 45 no 12pp 2095ndash2101 2004
[24] T Takeda J Wu and T T Lwin ldquo99mTc-N-DBODC5 a novelmyocardial perfusion imaging agent for diagnosis of coronaryartery disease a reviewrdquo Recent Patents on Cardiovascular DrugDiscovery vol 1 no 2 pp 161ndash166 2006
[25] K Hatada M Ruiz L M Riou et al ldquoOrgan biodistributionand myocardial uptake washout and redistribution kinetics ofTc-99m N-DBODC5 when injected during vasodilator stressin canine models of coronary stenosesrdquo Journal of NuclearCardiology vol 13 no 6 pp 779ndash790 2006
[26] W Zhang W Fang B Li X Wang and Z He ldquoExperimentalstudy of [99mTc(PNP5) (DBODC)]+ as a new myocardialperfusion imaging agentrdquo Cardiology vol 112 no 2 pp 89ndash972009
[27] M E Marmion S R Woulfe W L Neumann D L Nosco andE Deutsch ldquoPreparation and characterization of technetiumcomplexes with Schiff base and phosphine coordination 1Complexes of technetium-99g and -99m with substitutedacac2en and trialkyl phosphines (where acac2en = NN1015840-ethylenebis[acetylacetone iminato])rdquo Nuclear Medicine andBiology vol 26 no 7 pp 755ndash770 1999
[28] C Bolzati L Uccelli A Boschi et al ldquoSynthesis of a novel classof nitrido Tc-99m radiopharmaceuticals with phosphino-thiolligands showing transient heart uptakerdquo Journal of InorganicBiochemistry vol 78 no 3 pp 369ndash374 2000
[29] M J Henzlova M D Cerqueira J J Mahmarian and S YaoldquoStress protocols and tracersrdquo Journal of Nuclear Cardiology vol13 no 6 pp e80ndashe90 2006
[30] C L Hansen R A Goldstein D S Berman et al ldquoMyocardialperfusion and function single photon emission computedtomographyrdquo Journal of Nuclear Cardiology vol 13 no 6 ppe97ndashe120 2006
[31] P Flamen A Bossuyt and P R Franken ldquoTechnetium-99m-tetrofosmin in dipyridamole-stressmyocardial SPECT imagingintraindividual comparison with technetium-99m-sestamibirdquoJournal of Nuclear Medicine vol 36 no 11 pp 2009ndash2015 1995
[32] N Tamaki N Takahashi M Kawamoto et al ldquoMyocardialtomography using technetium-99m-tetrofosmin to evaluatecoronary artery diseaserdquo Journal of Nuclear Medicine vol 35no 4 pp 594ndash600 1994
[33] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardizedmyocardial segmentation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare profes-sionals from the Cardiac Imaging Committee of the Councilon Clinical Cardiology of the American Heart AssociationrdquoJournal of Nuclear Cardiology vol 9 no 2 pp 240ndash245 2002
[34] T Sharir G Germano X Kang et al ldquoPrediction of myocardialinfarction versus cardiac death by gated myocardial perfusionSPECT risk stratification by the amount of stress-inducedischemia and the poststress ejection fractionrdquo Journal of NuclearMedicine vol 42 no 6 pp 831ndash837 2001
[35] S H Braat B Leclercq R Itti A Lahiri B Sridhara and PRigo ldquoMyocardial imaging with technetium-99m-tetrofosmincomparison of one-day and two-day protocolsrdquo Journal ofNuclear Medicine vol 35 no 10 pp 1581ndash1585 1994
[36] G Germano T Chua H Kiat J S Areeda andD S Berman ldquoAquantitative phantom analysis of artifacts due to hepatic activ-ity in technetium-99m myocardial perfusion SPECT studiesrdquoJournal of Nuclear Medicine vol 35 no 2 pp 356ndash359 1994
[37] A K Paul andH A Nabi ldquoGatedmyocardial perfusion SPECTbasic principles technical aspects and clinical applicationsrdquoJournal of Nuclear Medicine Technology vol 32 no 4 pp 179ndash187 2004
[38] J Nuyts P Dupont V Van den Maegdenbergh S Vleugels PSuetens and L Mortelmans ldquoA study of the liver-heart artifactin emission tomographyrdquo Journal of Nuclear Medicine vol 36no 1 pp 133ndash139 1995
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 BioMed Research International
Table 2 The comparison of myocardial perfusion in a total of 782 segments with 99mTc-N-DBODC5 and 99mTc-MIBI SPECT exerciseimaging
99mTc-N-DBODC599mTc-MIBI Total
Normal Reversible defect Nonreversible defectlowast
Normal 302 (39) 17 (2) 71 (9) 390Reversible defectlowast 16 (2) 119 (15) 105 (13) 240Nonreversible defect 12 (2) 4 (1) 136 (17) 152Total 330 140 312 782Data are presented as number lowast119875 lt 0001 99mTc-MIBI versus 99mTc-N-DBODC5 for nonreversible defect segments lowast119875 lt 005 99mTc-N-DBODC5 versus99mTc-MIBI for reversible defect segments McNemar test was used
Table 3 MPI findings of two tracers on left ventricular functionparameters and ischemia scores in 46 patients
Parameter 99mTc-MIBI 99mTc-N-DBODC5LVEF ()
Exercise 542 plusmn 113 567 plusmn 92Rest 631 plusmn 85 648 plusmn 79
EDV (mL)Exercise 815 plusmn 186 832 plusmn 163Rest 973 plusmn 164 991 plusmn 137
ESV (mL)Exercise 432 plusmn 97 414 plusmn 123Rest 594 plusmn 136 602 plusmn 98
SSS 121 plusmn 14995333 96 plusmn 16SRS 72 plusmn 08 79 plusmn 09SDS 42 plusmn 05995333 36 plusmn 04TID 096 plusmn 006 094 plusmn 002Data are presented asmeanplusmn SD or number () as appropriate995333statisticallysignificant 99mTc-MIBI versus 99mTc-N-DBODC5 (119875 lt 005) pairedStudentrsquos 119905-test was used LVEF left ventricular ejection fraction EDVend-diastolic volume ESV end-systolic volume SSS summed stress scoresSRS summed rest scores SDS summed difference scores TID transientventricular dysfunction
overall figures for sensitivity and specificity in identificationof CAD were 86 (2529) and 65 (1117) for 99mTc-MIBI imaging On the other hand the overall sensitivityand specificity for the detection of CAD were 86 (2529)and 88 (1517) for 99mTc-N-DBODC5 SPECT studies Theconcordance of ischemia diagnosis sensitivity of a represen-tative patient for the two tracers is shown in Figure 4 Theaccuracy was 078 for 99mTc-MIBI and 087 for 99mTc-N-DBODC5 Angiography agreement was very good for 99mTc-N-DBODC5 (120581 = 073) and moderate for 99mTc-MIBI (120581 =052) Specificity and accuracy were not significantly differentbut better for the 99mTc-N-DBODC5 group when comparedto 99mTc-MIBI SPECT (specificity 88-65 accuracy 87-78)
36 Detection of Disease in Individual Coronary VesselsTable 4 also shows the sensitivity and specificity of the twotracers in detecting individual-stenosed vessels Of a total of138 arteries in 46 patients 48 arteries had significant stenosesand 90 had insignificant lesions or were normal Overall
figures for sensitivity and specificity in identifying individual-stenosed vessels were 67 (3248) and 86 (7790) for 99mTc-MIBI imaging overall sensitivity and specificity to diagnoseindividual significantly stenosed vessels were 69 (3348)and 92 (8390) for 99mTc-N-DBODC5 SPECT studies
On the other hand sensitivity and specificity for RCAstenosis vessel lesion detection using 99mTc-MIBI MPI were87 and 68 compared to 87 and 87 for 99mTc-N-DBODC5 MPI LAD stenosis (53 sensitivity and 96specificity for 99mTc-MIBI 63 sensitivity and 96 speci-ficity for 99mTc-N-DBODC5 resp) and left circumflex(LCX) (64 sensitivity and 94 specificity for 99mTc-MIBI57 sensitivity and 94 specificity for 99mTc-N-DBODC5resp) Angiography agreement was very good for 99mTc-N-DBODC5 (120581 = 063 for LAD 120581 = 071 for RCA resp) andmoderate for 99mTc-MIBI (120581 = 052 for LAD 120581 = 048 forRCA resp) In contrast the angiography agreement was verygood for 99mTc-MIBI (120581 = 062 for LCX) and moderate for99mTc-N-DBODC5 (120581 = 055 for LCX) (Table 4) Overall thespecificity of 99mTc-N-DBODC5 SPECT to detect individualRCA stenosis was better (2731 87) than that of 99mTc-MIBISPECT (2131 68) despite having no statistical significance
4 Discussion
These preliminary results demonstrate that stress-restmyocardial perfusion SPECT with 99mTc-N-DBODC5 isa sensitive method for detecting CAD and identifyingstenosed coronary arteries For the detection of CADmore importantly 99mTc-N-DBODC5 MPI reached goodagreement compared with CA (120581 = 073)
41 Advantages of 99119898Tc-N-DBODC5 99mTc-N-DBODC5 isa new lipophilic monocationic and nitride 99mTc-labeledtracer that is rapidly cleared from the liver after intravenousinjection It possesses good stability under physiological con-ditions Importantly 99mTc-N-DBODC5 exhibits more rapidliver washout than either 99mTc-MIBI or 99mTc-tetrofosminFor example at 60min after injection in rats the heartliverratio of 99mTc-N-DBODC5 is approximately ten times higherthan that of 99mTc-MIBI or 99mTc-tetrofosmin Preclinicalstudies have shown that 99mTc-N-DBODC5 SPECT canidentify previous ischemia as areas of reduced tracer uptake[25 26] Furthermore the rapid liver clearance and highuptake in the myocardium of 99mTc-N-DBODC5 will allow
BioMed Research International 7
Table 4 Sensitivity specificity and diagnostic accuracy of scintigraphic perfusion studies and agreement with coronary angiography
Overall LAD LCX RCAMIBI DBODC MIBI DBODC MIBI DBODC MIBI DBODC
No of disease 25 25 10 12 9 8 13 13Sensitivity () 86 86 53 63 64 57 87 87Specificity () 65 88 96 96 94 94 68 87Accuracy () 78 87 78 83 85 83 74 87998771Kappa (120581) 053 073 052 063 062 055 048 071Data are presented as number () MIBI = 99mTc-MIBI DBODC = 99mTc-N-DBODC5 LAD left anterior descending coronary artery LCX left circumflexcoronary artery RCA right coronary artery 998771CA was used as the ldquogold standardrdquo for the calculation of the 120581 which is determine between SPECT MPI andCA If there is no agreement 120581 = 020ndash039 moderate agreement 120581 = 040ndash059 very good agreement 120581 = 060ndash079 excellent agreement 120581 = 080ndash100
SPECT images of the left ventricle to be acquired earlyand with excellent quality [22] The ratios of heart-to-liverwere consistent with the previous report study [22] Thesecharacteristics are suitable particularly for patients withsuspected acute coronary syndromes and without diagnosticelectrocardiogram because early diagnosis is needed in suchpatients for timely therapeutic decisionmaking 99mTc-MIBIon the other hand may require a wait time of up to 1 h forimaging
In the present study the heart-to-organ count ratio of99mTc-N-DBODC5 MPI was superior to that of 99mTc-MIBIin 46 patients Compared with 99mTc-MIBI MPI 99mTc-N-DBODC5 MPI had better image quality in most patientsFurthermore in this study exercise stress myocardial imageswere performed 30min after 99mTc-N-DBODC5 injectionand excellent MPI with high contrast was possible
42 Clinical Value of 99119898Tc-N-DBODC5 for the Detection ofCAD This clinical trial assesses the diagnostic value of thisagent to detect CAD comparing it with stress 99mTc-MIBIMPI and CA
In this study compared with 99mTc-MIBI MPI 99mTc-N-DBODC5MPI indicates the same sensitivity and better speci-ficity and accuracy to detect coronary disease in patientsalthough none of the differences were significant On theother hand more importantly angiography agreement wasvery good for 99mTc-N-DBODC5 (120581 = 073) and moderatefor 99mTc-MIBI (120581 = 052) thus compared with 99mTc-MIBI MPI it provides a high degree of concordance for theevaluation of CAD specifically in excluding perfusion abnor-malities in patients with suspected CAD Possible reasons forthis difference may be fast liver clearance favorable heart-to-organ ratio and high image quality 99mTc-N-DBODC5with rapid liver clearancemay significantly reduce the photonscatter from the liver into the inferoposterior walls Thisreduces the artifactual decreased myocardial perfusion andimproves the diagnostic accuracy for the detection of CADcompared with other 99mTc-labeled perfusion agents [24]
Unsurprisingly Braat et al [35] and Germano et al [36]noted that technetium-labeled MPI agents with a fast liverclearance can significantly reduce the photon scatter fromthe liver into the inferior walls but the radioactivity may betransferred to the gastrointestinal area and increased bowel
and gastric activity were seen as a problem associated withhigh liver uptake in the visual and quantitative interpretationof the inferoposterior myocardial walls In this study boweluptakewas frequently seen on the 99mTc-N-DBODC5 imagesbut did not result in any nondiagnostic scans
For the detection of coronary disease in patients 99mTc-MIBI produced abnormal results for MPI in four patientswho had no angiographically detected stenosis Some of thesefalse-positive results may be due in part to the liver-to-heart artifacts In this study we could classify fixed perfusiondefects as soft-tissue attenuation artifacts or infarcts by usinggated SPECT Because an artifactual defect would shownormal contraction (wall motion or thickening) on a gatedimage artifacts can be differentiated from a true infarct [37]
For the detection of individual vessel stenosis on theother hand angiography agreement was very good for 99mTc-N-DBODC5 (120581=071 for RCA) andmoderate for 99mTc-MIBI(120581 = 048 for RCA) For LAD and LCX arteries stenosis thediagnosis of myocardial ischemia on 99mTc-N-DBODC5 and99mTc-MIBI study had the same specificity and it was similarto that of two tracer to diagnose sensitivity and accuracy ofmyocardial ischemia Abnormal results of myocardial imagesin individual RCA vessel stenosis (six arteries-stenosed ves-sels for RCA) were obtained in the 99mTc-MIBI studieswhile CA and 99mTc-N-DBODC5 studies showed normalfindings in the same individual RCA vessel territories Someof these false-positive results may be due to photon scatterfrom the liver and intestine into the inferoposterior walls99mTc-MIBI concentration located below the left diaphragm(ie liver and bowel) may cause an artifactual perfusiondefect in the adjacent myocardial a phenomenon knownas the ldquoliver-heart artifactrdquo [36 38] Moreover the inferiorand inferoposterior regions were dominated mainly by RCAterritories corresponding to the myocardial short axis andvertical long axis while arteries regions which LAD and LCXdominated were less interfered from ldquoliver-heart artifactrdquoFinally for clinical applications 99mTc-N-DBODC5 offersbetter determination of detects particularly in the infero-posterior wall on myocardial images A typical example of afalse-positive perfusion defect in the inferior wall is shown inFigure 5
On a segment-to-segment basis complete agreementbetween the two imaging agents occurred in 71 of segments
8 BioMed Research International
(a) (b) (c)
Figure 5 Serial short-axis and vertical long-axis slices of stress-rest 99mTc-N-DBODC5 images (b) and stress-rest 99mTc-MIBI images (c) ofa representative patient with normal CA (a) Because of intense uptake of technetium 99mTc-MIBI in the liver high liver background activitycan be observed Furthermore a false-positive myocardial perfusion defect was also seen in the inferoposterior wall segments supplied bythe RCA territory (white arrows) Importantly however at stress and rest the inferoposterior wall segments of 99mTc-N-DBODC5 imagesare clearly separated from the subdiaphragmatic activity
However more myocardial segments were nonreversible on99mTc-MIBI images than on 99mTc-N-DBODC5 images Onthe contrary 99mTc-N-DBODC5MPI had a higher reversibledefect than that of 99mTc-MIBI A possible reason for thisdifference may be due in part to the ldquoliver-heart artifactrdquoThe presence of high liver activity adjacent to the inferior wallresults fromoversubtraction of activity from the inferior wallTherefore the more ldquoliver-heart artifactrdquo in the inferoposte-rior wall on myocardial images the more false nonreversibledefects in the inferoposterior wall on myocardial perfusionsegmental analysis In other words the less reversible defectsin the inferoposterior wall were deduced on 99mTc-MIBIMPIsegmental analysis
More importantly however the main advantage andclinical value of 99mTc-N-DBODC5 can improve diagnosticspecificity and reduce the false-positive diagnosis of patientsand associated treatment fees
5 Limitations
In this study we did not attempt to assess the absolute diag-nostic accuracy of 99mTc-N-DBODC5 because definitive
conclusions in this regard can only be drawn by study-ing larger patient cohort In addition although 99mTc-N-DBODC5 did not track flow as well as 201Tl the magni-tudes of the pharmacologic stress-induced perfusion defectswere comparable to those previously reported for 99mTc-tetrofosmin Thus direct comparison between 99mTc-N-DBODC5 and 99mTc-tetrofosmin should be further provedin the same patient population Overall 99mTc-N-DBODC5MPI will become an important diagnostic tool in the evalua-tion of myocardial perfusion
6 Conclusion
This preliminary clinical study showed that 99mTc-N-DBODC5 and 99mTc-MIBI MPI provide comparable diag-nostic information for patients undergoing exercise rest fordetection of CAD In addition 99mTc-N-DBODC5 doesnot exhibit the disadvantages of 99mTc-MIBI in this studyBy contrast because of its high heart-organ count ratioin comparison to 99mTc-MIBI it improves high degree ofdiagnostic concordance in defining or excluding perfusionabnormalities in patients with CADTherefore it can become
BioMed Research International 9
the agent of choice for the evaluation ofmyocardial perfusionand ventricular function in patients with CAD
Abbreviations
CAD Coronary artery diseaseMPI Myocardial perfusion imagingCA Coronary angiographySPECT Single-photon emission computed
tomographyPET Positron emission computed
tomography99mTc-MIBI Technetium 99m sestamibi99mTc-N-DBODC5 99mTc(N)(DBODC)(PNP5)201Tl Thallium-20199mTc-tetrofosmin Technetium-99m-tetrofosminROI Regions of interestLAD Left anterior descending arteryLCX Left circumflex arteryRCA Right coronary arterySSS Summed stress scoreSRS Summed rest scoreSDS Summed difference scoreEDV End-diastolic volumeESV End-systolic volumeLVEF Left ventricular ejection fraction
Ethics Statement
This study was conducted in accordance with the HelsinkiDeclaration All subjects provided written informed consentbefore MPI acknowledging that they understood their rightsand obligations This study was approved by the ResearchEthics Committee of Shanxi Medical University
Conflict of Interests
The authors declare that they have no conflict of interest
Acknowledgments
This research is partly supported by Grants from the YouthScience and Technology Research Foundation of ShanxiProvince (no 2009021043-3) The authors acknowledge themembers of the participating staff for their contribution tothis clinical study
References
[1] National Hospital Discharge Survey National Health StatisticsReport no 5 2006
[2] J He D Gu X Wu et al ldquoMajor causes of death among menand women in Chinardquo The New England Journal of Medicinevol 353 no 11 pp 1124ndash1134 2005
[3] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardized myocardial sementation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare pro-fessionals from the Cardiac Imaging Committee of the Council
on Clinical Cardiology of the American Heart AssociationrdquoCirculation vol 105 no 4 pp 539ndash542 2002
[4] R J Gibbons J Abrams K Chatterjee et al ldquoACCAHA 2002guideline update for the management of patients with chronicstable anginamdashsummary article a report of the AmericanCollege of CardiologyAmerican Heart Association Task Forceon Practice Guidelines (Committee on the Management ofPatients With Chronic Stable Angina)rdquo Journal of the AmericanCollege of Cardiology vol 41 no 1 pp 159ndash168 2003
[5] WWijns P Kolh N Danchin et al ldquoGuidelines on myocardialrevascularizationrdquo European Heart Journal vol 31 pp 2501ndash2555 2010
[6] J M Jensen K A Oslashvrehus L H Nielsen J K Jensen HM Larsen and B L Noslashrgaard ldquoParadigm of pretest riskstratification before coronary computed tomographyrdquo Journalof Cardiovascular Computed Tomography vol 3 no 6 pp 386ndash391 2009
[7] N RMollet F Cademartiri C VanMieghem et al ldquoAdjunctivevalue of CT coronary angiography in the diagnostic work-up ofpatients with typical angina pectorisrdquo European Heart Journalvol 28 no 15 pp 1872ndash1878 2007
[8] R G E J Groutars J F Verzijlbergen M M C Tiel-Van Buulet al ldquoThe accuracy of 1-day dual-isotopemyocardial SPECT ina population with high prevalence of coronary artery diseaserdquoInternational Journal of Cardiovascular Imaging vol 19 no 3pp 229ndash238 2003
[9] M R Patel E D Peterson D Dai et al ldquoLow diagnostic yieldof elective coronary angiographyrdquo The New England Journal ofMedicine vol 362 no 10 pp 886ndash895 2010
[10] ldquoPharmacologic stress testingrdquo in Nuclear Cardiac ImagingPriniciples and Applications A E Iskandrian and E V GarciaEds pp 293ndash315 OxfordUniversity Press NewYork NY USA4th edition 2008
[11] R R Russell III and B L Zaret ldquoNuclear cardiology presentand futurerdquo Current Problems in Cardiology vol 31 no 9 pp557ndash629 2006
[12] G Germano H Kiat P B Kavanagh et al ldquoAutomatic quan-tification of ejection fraction from gated myocardial perfusionSPECTrdquo Journal of Nuclear Medicine vol 36 no 11 pp 2138ndash2147 1995
[13] S R Underwood C Anagnostopoulos M Cerqueira et alldquoMyocardial perfusion scintigraphy the evidencerdquo EuropeanJournal of Nuclear Medicine and Molecular Imaging vol 31 pp261ndash291 2004
[14] J Heo and A S Iskandrian ldquoTechnetium-labeled myocardialperfusion agentsrdquo Cardiology Clinics vol 12 no 2 pp 187ndash1981994
[15] B L Zaret P Rigo F J T Wackers et al ldquoMyocardial perfusionimaging with 99mTc tetrofosmin comparison to 201Tl imagingand coronary angiography in a phase III multicenter trialrdquoCirculation vol 91 no 2 pp 313ndash319 1995
[16] J J Mahmarian and M S Verani ldquoExercise thallium-201perfusion scintigraphy in the assessment of coronary arterydiseaserdquoAmerican Journal of Cardiology vol 67 no 14 pp 2Dndash11D 1991
[17] D D Miller L T Younis B R Chaitman and H StratmannldquoDiagnostic accuracy of dipyridamole technetium 99m-labeledsestamibi myocardial tomography for detection of coronaryartery diseaserdquo Journal of Nuclear Cardiology vol 4 no 1 pp18ndash24 1997
10 BioMed Research International
[18] Z He A S Iskandrian N C Gupta and M S Verani ldquoAssess-ing coronary artery disease with dipyridamole technetium-99m-tetrofosmin SPECT amulticenter trialrdquo Journal of NuclearMedicine vol 38 no 1 pp 44ndash48 1997
[19] A Boschi C Bolzati L Uccelli et al ldquoA class of asymmetricalnitrido 99mTc heterocomplexes as heart imaging agents withimproved biological propertiesrdquoNuclearMedicine Communica-tions vol 23 no 7 pp 689ndash693 2002
[20] A Boschi L Uccelli C Bolzati et al ldquoSynthesis and biologicevaluation of monocationic asymmetric 99mTc-nitride hetero-complexes showing high heart uptake and improved imagingpropertiesrdquo Journal of Nuclear Medicine vol 44 no 5 pp 806ndash814 2003
[21] C Bolzati M Cavazza-Ceccato S Agostini S TokunagaD Casara and G Bandoli ldquoSubcellular distribution andmetabolism studies of the potential myocardial imaging agent[99mTc(N)(DBODC)(PNP5)]+rdquo Journal of Nuclear Medicinevol 49 no 8 pp 1336ndash1344 2008
[22] C Cittanti L Uccelli M Pasquali et al ldquoWhole-body biodis-tribution and radiation dosimetry of the new cardiac tracer99mTc-N-DBODCrdquo Journal of Nuclear Medicine vol 49 no 8pp 1299ndash1304 2008
[23] K Hatada L M Riou M Ruiz et al ldquo99mTc-N-DBODC5a new myocardial perfusion imaging agent with rapid liverclearance comparison with 99mTc-sestamibi and 99mTc-tetrofosmin in ratsrdquo Journal of Nuclear Medicine vol 45 no 12pp 2095ndash2101 2004
[24] T Takeda J Wu and T T Lwin ldquo99mTc-N-DBODC5 a novelmyocardial perfusion imaging agent for diagnosis of coronaryartery disease a reviewrdquo Recent Patents on Cardiovascular DrugDiscovery vol 1 no 2 pp 161ndash166 2006
[25] K Hatada M Ruiz L M Riou et al ldquoOrgan biodistributionand myocardial uptake washout and redistribution kinetics ofTc-99m N-DBODC5 when injected during vasodilator stressin canine models of coronary stenosesrdquo Journal of NuclearCardiology vol 13 no 6 pp 779ndash790 2006
[26] W Zhang W Fang B Li X Wang and Z He ldquoExperimentalstudy of [99mTc(PNP5) (DBODC)]+ as a new myocardialperfusion imaging agentrdquo Cardiology vol 112 no 2 pp 89ndash972009
[27] M E Marmion S R Woulfe W L Neumann D L Nosco andE Deutsch ldquoPreparation and characterization of technetiumcomplexes with Schiff base and phosphine coordination 1Complexes of technetium-99g and -99m with substitutedacac2en and trialkyl phosphines (where acac2en = NN1015840-ethylenebis[acetylacetone iminato])rdquo Nuclear Medicine andBiology vol 26 no 7 pp 755ndash770 1999
[28] C Bolzati L Uccelli A Boschi et al ldquoSynthesis of a novel classof nitrido Tc-99m radiopharmaceuticals with phosphino-thiolligands showing transient heart uptakerdquo Journal of InorganicBiochemistry vol 78 no 3 pp 369ndash374 2000
[29] M J Henzlova M D Cerqueira J J Mahmarian and S YaoldquoStress protocols and tracersrdquo Journal of Nuclear Cardiology vol13 no 6 pp e80ndashe90 2006
[30] C L Hansen R A Goldstein D S Berman et al ldquoMyocardialperfusion and function single photon emission computedtomographyrdquo Journal of Nuclear Cardiology vol 13 no 6 ppe97ndashe120 2006
[31] P Flamen A Bossuyt and P R Franken ldquoTechnetium-99m-tetrofosmin in dipyridamole-stressmyocardial SPECT imagingintraindividual comparison with technetium-99m-sestamibirdquoJournal of Nuclear Medicine vol 36 no 11 pp 2009ndash2015 1995
[32] N Tamaki N Takahashi M Kawamoto et al ldquoMyocardialtomography using technetium-99m-tetrofosmin to evaluatecoronary artery diseaserdquo Journal of Nuclear Medicine vol 35no 4 pp 594ndash600 1994
[33] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardizedmyocardial segmentation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare profes-sionals from the Cardiac Imaging Committee of the Councilon Clinical Cardiology of the American Heart AssociationrdquoJournal of Nuclear Cardiology vol 9 no 2 pp 240ndash245 2002
[34] T Sharir G Germano X Kang et al ldquoPrediction of myocardialinfarction versus cardiac death by gated myocardial perfusionSPECT risk stratification by the amount of stress-inducedischemia and the poststress ejection fractionrdquo Journal of NuclearMedicine vol 42 no 6 pp 831ndash837 2001
[35] S H Braat B Leclercq R Itti A Lahiri B Sridhara and PRigo ldquoMyocardial imaging with technetium-99m-tetrofosmincomparison of one-day and two-day protocolsrdquo Journal ofNuclear Medicine vol 35 no 10 pp 1581ndash1585 1994
[36] G Germano T Chua H Kiat J S Areeda andD S Berman ldquoAquantitative phantom analysis of artifacts due to hepatic activ-ity in technetium-99m myocardial perfusion SPECT studiesrdquoJournal of Nuclear Medicine vol 35 no 2 pp 356ndash359 1994
[37] A K Paul andH A Nabi ldquoGatedmyocardial perfusion SPECTbasic principles technical aspects and clinical applicationsrdquoJournal of Nuclear Medicine Technology vol 32 no 4 pp 179ndash187 2004
[38] J Nuyts P Dupont V Van den Maegdenbergh S Vleugels PSuetens and L Mortelmans ldquoA study of the liver-heart artifactin emission tomographyrdquo Journal of Nuclear Medicine vol 36no 1 pp 133ndash139 1995
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 7
Table 4 Sensitivity specificity and diagnostic accuracy of scintigraphic perfusion studies and agreement with coronary angiography
Overall LAD LCX RCAMIBI DBODC MIBI DBODC MIBI DBODC MIBI DBODC
No of disease 25 25 10 12 9 8 13 13Sensitivity () 86 86 53 63 64 57 87 87Specificity () 65 88 96 96 94 94 68 87Accuracy () 78 87 78 83 85 83 74 87998771Kappa (120581) 053 073 052 063 062 055 048 071Data are presented as number () MIBI = 99mTc-MIBI DBODC = 99mTc-N-DBODC5 LAD left anterior descending coronary artery LCX left circumflexcoronary artery RCA right coronary artery 998771CA was used as the ldquogold standardrdquo for the calculation of the 120581 which is determine between SPECT MPI andCA If there is no agreement 120581 = 020ndash039 moderate agreement 120581 = 040ndash059 very good agreement 120581 = 060ndash079 excellent agreement 120581 = 080ndash100
SPECT images of the left ventricle to be acquired earlyand with excellent quality [22] The ratios of heart-to-liverwere consistent with the previous report study [22] Thesecharacteristics are suitable particularly for patients withsuspected acute coronary syndromes and without diagnosticelectrocardiogram because early diagnosis is needed in suchpatients for timely therapeutic decisionmaking 99mTc-MIBIon the other hand may require a wait time of up to 1 h forimaging
In the present study the heart-to-organ count ratio of99mTc-N-DBODC5 MPI was superior to that of 99mTc-MIBIin 46 patients Compared with 99mTc-MIBI MPI 99mTc-N-DBODC5 MPI had better image quality in most patientsFurthermore in this study exercise stress myocardial imageswere performed 30min after 99mTc-N-DBODC5 injectionand excellent MPI with high contrast was possible
42 Clinical Value of 99119898Tc-N-DBODC5 for the Detection ofCAD This clinical trial assesses the diagnostic value of thisagent to detect CAD comparing it with stress 99mTc-MIBIMPI and CA
In this study compared with 99mTc-MIBI MPI 99mTc-N-DBODC5MPI indicates the same sensitivity and better speci-ficity and accuracy to detect coronary disease in patientsalthough none of the differences were significant On theother hand more importantly angiography agreement wasvery good for 99mTc-N-DBODC5 (120581 = 073) and moderatefor 99mTc-MIBI (120581 = 052) thus compared with 99mTc-MIBI MPI it provides a high degree of concordance for theevaluation of CAD specifically in excluding perfusion abnor-malities in patients with suspected CAD Possible reasons forthis difference may be fast liver clearance favorable heart-to-organ ratio and high image quality 99mTc-N-DBODC5with rapid liver clearancemay significantly reduce the photonscatter from the liver into the inferoposterior walls Thisreduces the artifactual decreased myocardial perfusion andimproves the diagnostic accuracy for the detection of CADcompared with other 99mTc-labeled perfusion agents [24]
Unsurprisingly Braat et al [35] and Germano et al [36]noted that technetium-labeled MPI agents with a fast liverclearance can significantly reduce the photon scatter fromthe liver into the inferior walls but the radioactivity may betransferred to the gastrointestinal area and increased bowel
and gastric activity were seen as a problem associated withhigh liver uptake in the visual and quantitative interpretationof the inferoposterior myocardial walls In this study boweluptakewas frequently seen on the 99mTc-N-DBODC5 imagesbut did not result in any nondiagnostic scans
For the detection of coronary disease in patients 99mTc-MIBI produced abnormal results for MPI in four patientswho had no angiographically detected stenosis Some of thesefalse-positive results may be due in part to the liver-to-heart artifacts In this study we could classify fixed perfusiondefects as soft-tissue attenuation artifacts or infarcts by usinggated SPECT Because an artifactual defect would shownormal contraction (wall motion or thickening) on a gatedimage artifacts can be differentiated from a true infarct [37]
For the detection of individual vessel stenosis on theother hand angiography agreement was very good for 99mTc-N-DBODC5 (120581=071 for RCA) andmoderate for 99mTc-MIBI(120581 = 048 for RCA) For LAD and LCX arteries stenosis thediagnosis of myocardial ischemia on 99mTc-N-DBODC5 and99mTc-MIBI study had the same specificity and it was similarto that of two tracer to diagnose sensitivity and accuracy ofmyocardial ischemia Abnormal results of myocardial imagesin individual RCA vessel stenosis (six arteries-stenosed ves-sels for RCA) were obtained in the 99mTc-MIBI studieswhile CA and 99mTc-N-DBODC5 studies showed normalfindings in the same individual RCA vessel territories Someof these false-positive results may be due to photon scatterfrom the liver and intestine into the inferoposterior walls99mTc-MIBI concentration located below the left diaphragm(ie liver and bowel) may cause an artifactual perfusiondefect in the adjacent myocardial a phenomenon knownas the ldquoliver-heart artifactrdquo [36 38] Moreover the inferiorand inferoposterior regions were dominated mainly by RCAterritories corresponding to the myocardial short axis andvertical long axis while arteries regions which LAD and LCXdominated were less interfered from ldquoliver-heart artifactrdquoFinally for clinical applications 99mTc-N-DBODC5 offersbetter determination of detects particularly in the infero-posterior wall on myocardial images A typical example of afalse-positive perfusion defect in the inferior wall is shown inFigure 5
On a segment-to-segment basis complete agreementbetween the two imaging agents occurred in 71 of segments
8 BioMed Research International
(a) (b) (c)
Figure 5 Serial short-axis and vertical long-axis slices of stress-rest 99mTc-N-DBODC5 images (b) and stress-rest 99mTc-MIBI images (c) ofa representative patient with normal CA (a) Because of intense uptake of technetium 99mTc-MIBI in the liver high liver background activitycan be observed Furthermore a false-positive myocardial perfusion defect was also seen in the inferoposterior wall segments supplied bythe RCA territory (white arrows) Importantly however at stress and rest the inferoposterior wall segments of 99mTc-N-DBODC5 imagesare clearly separated from the subdiaphragmatic activity
However more myocardial segments were nonreversible on99mTc-MIBI images than on 99mTc-N-DBODC5 images Onthe contrary 99mTc-N-DBODC5MPI had a higher reversibledefect than that of 99mTc-MIBI A possible reason for thisdifference may be due in part to the ldquoliver-heart artifactrdquoThe presence of high liver activity adjacent to the inferior wallresults fromoversubtraction of activity from the inferior wallTherefore the more ldquoliver-heart artifactrdquo in the inferoposte-rior wall on myocardial images the more false nonreversibledefects in the inferoposterior wall on myocardial perfusionsegmental analysis In other words the less reversible defectsin the inferoposterior wall were deduced on 99mTc-MIBIMPIsegmental analysis
More importantly however the main advantage andclinical value of 99mTc-N-DBODC5 can improve diagnosticspecificity and reduce the false-positive diagnosis of patientsand associated treatment fees
5 Limitations
In this study we did not attempt to assess the absolute diag-nostic accuracy of 99mTc-N-DBODC5 because definitive
conclusions in this regard can only be drawn by study-ing larger patient cohort In addition although 99mTc-N-DBODC5 did not track flow as well as 201Tl the magni-tudes of the pharmacologic stress-induced perfusion defectswere comparable to those previously reported for 99mTc-tetrofosmin Thus direct comparison between 99mTc-N-DBODC5 and 99mTc-tetrofosmin should be further provedin the same patient population Overall 99mTc-N-DBODC5MPI will become an important diagnostic tool in the evalua-tion of myocardial perfusion
6 Conclusion
This preliminary clinical study showed that 99mTc-N-DBODC5 and 99mTc-MIBI MPI provide comparable diag-nostic information for patients undergoing exercise rest fordetection of CAD In addition 99mTc-N-DBODC5 doesnot exhibit the disadvantages of 99mTc-MIBI in this studyBy contrast because of its high heart-organ count ratioin comparison to 99mTc-MIBI it improves high degree ofdiagnostic concordance in defining or excluding perfusionabnormalities in patients with CADTherefore it can become
BioMed Research International 9
the agent of choice for the evaluation ofmyocardial perfusionand ventricular function in patients with CAD
Abbreviations
CAD Coronary artery diseaseMPI Myocardial perfusion imagingCA Coronary angiographySPECT Single-photon emission computed
tomographyPET Positron emission computed
tomography99mTc-MIBI Technetium 99m sestamibi99mTc-N-DBODC5 99mTc(N)(DBODC)(PNP5)201Tl Thallium-20199mTc-tetrofosmin Technetium-99m-tetrofosminROI Regions of interestLAD Left anterior descending arteryLCX Left circumflex arteryRCA Right coronary arterySSS Summed stress scoreSRS Summed rest scoreSDS Summed difference scoreEDV End-diastolic volumeESV End-systolic volumeLVEF Left ventricular ejection fraction
Ethics Statement
This study was conducted in accordance with the HelsinkiDeclaration All subjects provided written informed consentbefore MPI acknowledging that they understood their rightsand obligations This study was approved by the ResearchEthics Committee of Shanxi Medical University
Conflict of Interests
The authors declare that they have no conflict of interest
Acknowledgments
This research is partly supported by Grants from the YouthScience and Technology Research Foundation of ShanxiProvince (no 2009021043-3) The authors acknowledge themembers of the participating staff for their contribution tothis clinical study
References
[1] National Hospital Discharge Survey National Health StatisticsReport no 5 2006
[2] J He D Gu X Wu et al ldquoMajor causes of death among menand women in Chinardquo The New England Journal of Medicinevol 353 no 11 pp 1124ndash1134 2005
[3] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardized myocardial sementation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare pro-fessionals from the Cardiac Imaging Committee of the Council
on Clinical Cardiology of the American Heart AssociationrdquoCirculation vol 105 no 4 pp 539ndash542 2002
[4] R J Gibbons J Abrams K Chatterjee et al ldquoACCAHA 2002guideline update for the management of patients with chronicstable anginamdashsummary article a report of the AmericanCollege of CardiologyAmerican Heart Association Task Forceon Practice Guidelines (Committee on the Management ofPatients With Chronic Stable Angina)rdquo Journal of the AmericanCollege of Cardiology vol 41 no 1 pp 159ndash168 2003
[5] WWijns P Kolh N Danchin et al ldquoGuidelines on myocardialrevascularizationrdquo European Heart Journal vol 31 pp 2501ndash2555 2010
[6] J M Jensen K A Oslashvrehus L H Nielsen J K Jensen HM Larsen and B L Noslashrgaard ldquoParadigm of pretest riskstratification before coronary computed tomographyrdquo Journalof Cardiovascular Computed Tomography vol 3 no 6 pp 386ndash391 2009
[7] N RMollet F Cademartiri C VanMieghem et al ldquoAdjunctivevalue of CT coronary angiography in the diagnostic work-up ofpatients with typical angina pectorisrdquo European Heart Journalvol 28 no 15 pp 1872ndash1878 2007
[8] R G E J Groutars J F Verzijlbergen M M C Tiel-Van Buulet al ldquoThe accuracy of 1-day dual-isotopemyocardial SPECT ina population with high prevalence of coronary artery diseaserdquoInternational Journal of Cardiovascular Imaging vol 19 no 3pp 229ndash238 2003
[9] M R Patel E D Peterson D Dai et al ldquoLow diagnostic yieldof elective coronary angiographyrdquo The New England Journal ofMedicine vol 362 no 10 pp 886ndash895 2010
[10] ldquoPharmacologic stress testingrdquo in Nuclear Cardiac ImagingPriniciples and Applications A E Iskandrian and E V GarciaEds pp 293ndash315 OxfordUniversity Press NewYork NY USA4th edition 2008
[11] R R Russell III and B L Zaret ldquoNuclear cardiology presentand futurerdquo Current Problems in Cardiology vol 31 no 9 pp557ndash629 2006
[12] G Germano H Kiat P B Kavanagh et al ldquoAutomatic quan-tification of ejection fraction from gated myocardial perfusionSPECTrdquo Journal of Nuclear Medicine vol 36 no 11 pp 2138ndash2147 1995
[13] S R Underwood C Anagnostopoulos M Cerqueira et alldquoMyocardial perfusion scintigraphy the evidencerdquo EuropeanJournal of Nuclear Medicine and Molecular Imaging vol 31 pp261ndash291 2004
[14] J Heo and A S Iskandrian ldquoTechnetium-labeled myocardialperfusion agentsrdquo Cardiology Clinics vol 12 no 2 pp 187ndash1981994
[15] B L Zaret P Rigo F J T Wackers et al ldquoMyocardial perfusionimaging with 99mTc tetrofosmin comparison to 201Tl imagingand coronary angiography in a phase III multicenter trialrdquoCirculation vol 91 no 2 pp 313ndash319 1995
[16] J J Mahmarian and M S Verani ldquoExercise thallium-201perfusion scintigraphy in the assessment of coronary arterydiseaserdquoAmerican Journal of Cardiology vol 67 no 14 pp 2Dndash11D 1991
[17] D D Miller L T Younis B R Chaitman and H StratmannldquoDiagnostic accuracy of dipyridamole technetium 99m-labeledsestamibi myocardial tomography for detection of coronaryartery diseaserdquo Journal of Nuclear Cardiology vol 4 no 1 pp18ndash24 1997
10 BioMed Research International
[18] Z He A S Iskandrian N C Gupta and M S Verani ldquoAssess-ing coronary artery disease with dipyridamole technetium-99m-tetrofosmin SPECT amulticenter trialrdquo Journal of NuclearMedicine vol 38 no 1 pp 44ndash48 1997
[19] A Boschi C Bolzati L Uccelli et al ldquoA class of asymmetricalnitrido 99mTc heterocomplexes as heart imaging agents withimproved biological propertiesrdquoNuclearMedicine Communica-tions vol 23 no 7 pp 689ndash693 2002
[20] A Boschi L Uccelli C Bolzati et al ldquoSynthesis and biologicevaluation of monocationic asymmetric 99mTc-nitride hetero-complexes showing high heart uptake and improved imagingpropertiesrdquo Journal of Nuclear Medicine vol 44 no 5 pp 806ndash814 2003
[21] C Bolzati M Cavazza-Ceccato S Agostini S TokunagaD Casara and G Bandoli ldquoSubcellular distribution andmetabolism studies of the potential myocardial imaging agent[99mTc(N)(DBODC)(PNP5)]+rdquo Journal of Nuclear Medicinevol 49 no 8 pp 1336ndash1344 2008
[22] C Cittanti L Uccelli M Pasquali et al ldquoWhole-body biodis-tribution and radiation dosimetry of the new cardiac tracer99mTc-N-DBODCrdquo Journal of Nuclear Medicine vol 49 no 8pp 1299ndash1304 2008
[23] K Hatada L M Riou M Ruiz et al ldquo99mTc-N-DBODC5a new myocardial perfusion imaging agent with rapid liverclearance comparison with 99mTc-sestamibi and 99mTc-tetrofosmin in ratsrdquo Journal of Nuclear Medicine vol 45 no 12pp 2095ndash2101 2004
[24] T Takeda J Wu and T T Lwin ldquo99mTc-N-DBODC5 a novelmyocardial perfusion imaging agent for diagnosis of coronaryartery disease a reviewrdquo Recent Patents on Cardiovascular DrugDiscovery vol 1 no 2 pp 161ndash166 2006
[25] K Hatada M Ruiz L M Riou et al ldquoOrgan biodistributionand myocardial uptake washout and redistribution kinetics ofTc-99m N-DBODC5 when injected during vasodilator stressin canine models of coronary stenosesrdquo Journal of NuclearCardiology vol 13 no 6 pp 779ndash790 2006
[26] W Zhang W Fang B Li X Wang and Z He ldquoExperimentalstudy of [99mTc(PNP5) (DBODC)]+ as a new myocardialperfusion imaging agentrdquo Cardiology vol 112 no 2 pp 89ndash972009
[27] M E Marmion S R Woulfe W L Neumann D L Nosco andE Deutsch ldquoPreparation and characterization of technetiumcomplexes with Schiff base and phosphine coordination 1Complexes of technetium-99g and -99m with substitutedacac2en and trialkyl phosphines (where acac2en = NN1015840-ethylenebis[acetylacetone iminato])rdquo Nuclear Medicine andBiology vol 26 no 7 pp 755ndash770 1999
[28] C Bolzati L Uccelli A Boschi et al ldquoSynthesis of a novel classof nitrido Tc-99m radiopharmaceuticals with phosphino-thiolligands showing transient heart uptakerdquo Journal of InorganicBiochemistry vol 78 no 3 pp 369ndash374 2000
[29] M J Henzlova M D Cerqueira J J Mahmarian and S YaoldquoStress protocols and tracersrdquo Journal of Nuclear Cardiology vol13 no 6 pp e80ndashe90 2006
[30] C L Hansen R A Goldstein D S Berman et al ldquoMyocardialperfusion and function single photon emission computedtomographyrdquo Journal of Nuclear Cardiology vol 13 no 6 ppe97ndashe120 2006
[31] P Flamen A Bossuyt and P R Franken ldquoTechnetium-99m-tetrofosmin in dipyridamole-stressmyocardial SPECT imagingintraindividual comparison with technetium-99m-sestamibirdquoJournal of Nuclear Medicine vol 36 no 11 pp 2009ndash2015 1995
[32] N Tamaki N Takahashi M Kawamoto et al ldquoMyocardialtomography using technetium-99m-tetrofosmin to evaluatecoronary artery diseaserdquo Journal of Nuclear Medicine vol 35no 4 pp 594ndash600 1994
[33] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardizedmyocardial segmentation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare profes-sionals from the Cardiac Imaging Committee of the Councilon Clinical Cardiology of the American Heart AssociationrdquoJournal of Nuclear Cardiology vol 9 no 2 pp 240ndash245 2002
[34] T Sharir G Germano X Kang et al ldquoPrediction of myocardialinfarction versus cardiac death by gated myocardial perfusionSPECT risk stratification by the amount of stress-inducedischemia and the poststress ejection fractionrdquo Journal of NuclearMedicine vol 42 no 6 pp 831ndash837 2001
[35] S H Braat B Leclercq R Itti A Lahiri B Sridhara and PRigo ldquoMyocardial imaging with technetium-99m-tetrofosmincomparison of one-day and two-day protocolsrdquo Journal ofNuclear Medicine vol 35 no 10 pp 1581ndash1585 1994
[36] G Germano T Chua H Kiat J S Areeda andD S Berman ldquoAquantitative phantom analysis of artifacts due to hepatic activ-ity in technetium-99m myocardial perfusion SPECT studiesrdquoJournal of Nuclear Medicine vol 35 no 2 pp 356ndash359 1994
[37] A K Paul andH A Nabi ldquoGatedmyocardial perfusion SPECTbasic principles technical aspects and clinical applicationsrdquoJournal of Nuclear Medicine Technology vol 32 no 4 pp 179ndash187 2004
[38] J Nuyts P Dupont V Van den Maegdenbergh S Vleugels PSuetens and L Mortelmans ldquoA study of the liver-heart artifactin emission tomographyrdquo Journal of Nuclear Medicine vol 36no 1 pp 133ndash139 1995
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

8 BioMed Research International
(a) (b) (c)
Figure 5 Serial short-axis and vertical long-axis slices of stress-rest 99mTc-N-DBODC5 images (b) and stress-rest 99mTc-MIBI images (c) ofa representative patient with normal CA (a) Because of intense uptake of technetium 99mTc-MIBI in the liver high liver background activitycan be observed Furthermore a false-positive myocardial perfusion defect was also seen in the inferoposterior wall segments supplied bythe RCA territory (white arrows) Importantly however at stress and rest the inferoposterior wall segments of 99mTc-N-DBODC5 imagesare clearly separated from the subdiaphragmatic activity
However more myocardial segments were nonreversible on99mTc-MIBI images than on 99mTc-N-DBODC5 images Onthe contrary 99mTc-N-DBODC5MPI had a higher reversibledefect than that of 99mTc-MIBI A possible reason for thisdifference may be due in part to the ldquoliver-heart artifactrdquoThe presence of high liver activity adjacent to the inferior wallresults fromoversubtraction of activity from the inferior wallTherefore the more ldquoliver-heart artifactrdquo in the inferoposte-rior wall on myocardial images the more false nonreversibledefects in the inferoposterior wall on myocardial perfusionsegmental analysis In other words the less reversible defectsin the inferoposterior wall were deduced on 99mTc-MIBIMPIsegmental analysis
More importantly however the main advantage andclinical value of 99mTc-N-DBODC5 can improve diagnosticspecificity and reduce the false-positive diagnosis of patientsand associated treatment fees
5 Limitations
In this study we did not attempt to assess the absolute diag-nostic accuracy of 99mTc-N-DBODC5 because definitive
conclusions in this regard can only be drawn by study-ing larger patient cohort In addition although 99mTc-N-DBODC5 did not track flow as well as 201Tl the magni-tudes of the pharmacologic stress-induced perfusion defectswere comparable to those previously reported for 99mTc-tetrofosmin Thus direct comparison between 99mTc-N-DBODC5 and 99mTc-tetrofosmin should be further provedin the same patient population Overall 99mTc-N-DBODC5MPI will become an important diagnostic tool in the evalua-tion of myocardial perfusion
6 Conclusion
This preliminary clinical study showed that 99mTc-N-DBODC5 and 99mTc-MIBI MPI provide comparable diag-nostic information for patients undergoing exercise rest fordetection of CAD In addition 99mTc-N-DBODC5 doesnot exhibit the disadvantages of 99mTc-MIBI in this studyBy contrast because of its high heart-organ count ratioin comparison to 99mTc-MIBI it improves high degree ofdiagnostic concordance in defining or excluding perfusionabnormalities in patients with CADTherefore it can become
BioMed Research International 9
the agent of choice for the evaluation ofmyocardial perfusionand ventricular function in patients with CAD
Abbreviations
CAD Coronary artery diseaseMPI Myocardial perfusion imagingCA Coronary angiographySPECT Single-photon emission computed
tomographyPET Positron emission computed
tomography99mTc-MIBI Technetium 99m sestamibi99mTc-N-DBODC5 99mTc(N)(DBODC)(PNP5)201Tl Thallium-20199mTc-tetrofosmin Technetium-99m-tetrofosminROI Regions of interestLAD Left anterior descending arteryLCX Left circumflex arteryRCA Right coronary arterySSS Summed stress scoreSRS Summed rest scoreSDS Summed difference scoreEDV End-diastolic volumeESV End-systolic volumeLVEF Left ventricular ejection fraction
Ethics Statement
This study was conducted in accordance with the HelsinkiDeclaration All subjects provided written informed consentbefore MPI acknowledging that they understood their rightsand obligations This study was approved by the ResearchEthics Committee of Shanxi Medical University
Conflict of Interests
The authors declare that they have no conflict of interest
Acknowledgments
This research is partly supported by Grants from the YouthScience and Technology Research Foundation of ShanxiProvince (no 2009021043-3) The authors acknowledge themembers of the participating staff for their contribution tothis clinical study
References
[1] National Hospital Discharge Survey National Health StatisticsReport no 5 2006
[2] J He D Gu X Wu et al ldquoMajor causes of death among menand women in Chinardquo The New England Journal of Medicinevol 353 no 11 pp 1124ndash1134 2005
[3] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardized myocardial sementation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare pro-fessionals from the Cardiac Imaging Committee of the Council
on Clinical Cardiology of the American Heart AssociationrdquoCirculation vol 105 no 4 pp 539ndash542 2002
[4] R J Gibbons J Abrams K Chatterjee et al ldquoACCAHA 2002guideline update for the management of patients with chronicstable anginamdashsummary article a report of the AmericanCollege of CardiologyAmerican Heart Association Task Forceon Practice Guidelines (Committee on the Management ofPatients With Chronic Stable Angina)rdquo Journal of the AmericanCollege of Cardiology vol 41 no 1 pp 159ndash168 2003
[5] WWijns P Kolh N Danchin et al ldquoGuidelines on myocardialrevascularizationrdquo European Heart Journal vol 31 pp 2501ndash2555 2010
[6] J M Jensen K A Oslashvrehus L H Nielsen J K Jensen HM Larsen and B L Noslashrgaard ldquoParadigm of pretest riskstratification before coronary computed tomographyrdquo Journalof Cardiovascular Computed Tomography vol 3 no 6 pp 386ndash391 2009
[7] N RMollet F Cademartiri C VanMieghem et al ldquoAdjunctivevalue of CT coronary angiography in the diagnostic work-up ofpatients with typical angina pectorisrdquo European Heart Journalvol 28 no 15 pp 1872ndash1878 2007
[8] R G E J Groutars J F Verzijlbergen M M C Tiel-Van Buulet al ldquoThe accuracy of 1-day dual-isotopemyocardial SPECT ina population with high prevalence of coronary artery diseaserdquoInternational Journal of Cardiovascular Imaging vol 19 no 3pp 229ndash238 2003
[9] M R Patel E D Peterson D Dai et al ldquoLow diagnostic yieldof elective coronary angiographyrdquo The New England Journal ofMedicine vol 362 no 10 pp 886ndash895 2010
[10] ldquoPharmacologic stress testingrdquo in Nuclear Cardiac ImagingPriniciples and Applications A E Iskandrian and E V GarciaEds pp 293ndash315 OxfordUniversity Press NewYork NY USA4th edition 2008
[11] R R Russell III and B L Zaret ldquoNuclear cardiology presentand futurerdquo Current Problems in Cardiology vol 31 no 9 pp557ndash629 2006
[12] G Germano H Kiat P B Kavanagh et al ldquoAutomatic quan-tification of ejection fraction from gated myocardial perfusionSPECTrdquo Journal of Nuclear Medicine vol 36 no 11 pp 2138ndash2147 1995
[13] S R Underwood C Anagnostopoulos M Cerqueira et alldquoMyocardial perfusion scintigraphy the evidencerdquo EuropeanJournal of Nuclear Medicine and Molecular Imaging vol 31 pp261ndash291 2004
[14] J Heo and A S Iskandrian ldquoTechnetium-labeled myocardialperfusion agentsrdquo Cardiology Clinics vol 12 no 2 pp 187ndash1981994
[15] B L Zaret P Rigo F J T Wackers et al ldquoMyocardial perfusionimaging with 99mTc tetrofosmin comparison to 201Tl imagingand coronary angiography in a phase III multicenter trialrdquoCirculation vol 91 no 2 pp 313ndash319 1995
[16] J J Mahmarian and M S Verani ldquoExercise thallium-201perfusion scintigraphy in the assessment of coronary arterydiseaserdquoAmerican Journal of Cardiology vol 67 no 14 pp 2Dndash11D 1991
[17] D D Miller L T Younis B R Chaitman and H StratmannldquoDiagnostic accuracy of dipyridamole technetium 99m-labeledsestamibi myocardial tomography for detection of coronaryartery diseaserdquo Journal of Nuclear Cardiology vol 4 no 1 pp18ndash24 1997
10 BioMed Research International
[18] Z He A S Iskandrian N C Gupta and M S Verani ldquoAssess-ing coronary artery disease with dipyridamole technetium-99m-tetrofosmin SPECT amulticenter trialrdquo Journal of NuclearMedicine vol 38 no 1 pp 44ndash48 1997
[19] A Boschi C Bolzati L Uccelli et al ldquoA class of asymmetricalnitrido 99mTc heterocomplexes as heart imaging agents withimproved biological propertiesrdquoNuclearMedicine Communica-tions vol 23 no 7 pp 689ndash693 2002
[20] A Boschi L Uccelli C Bolzati et al ldquoSynthesis and biologicevaluation of monocationic asymmetric 99mTc-nitride hetero-complexes showing high heart uptake and improved imagingpropertiesrdquo Journal of Nuclear Medicine vol 44 no 5 pp 806ndash814 2003
[21] C Bolzati M Cavazza-Ceccato S Agostini S TokunagaD Casara and G Bandoli ldquoSubcellular distribution andmetabolism studies of the potential myocardial imaging agent[99mTc(N)(DBODC)(PNP5)]+rdquo Journal of Nuclear Medicinevol 49 no 8 pp 1336ndash1344 2008
[22] C Cittanti L Uccelli M Pasquali et al ldquoWhole-body biodis-tribution and radiation dosimetry of the new cardiac tracer99mTc-N-DBODCrdquo Journal of Nuclear Medicine vol 49 no 8pp 1299ndash1304 2008
[23] K Hatada L M Riou M Ruiz et al ldquo99mTc-N-DBODC5a new myocardial perfusion imaging agent with rapid liverclearance comparison with 99mTc-sestamibi and 99mTc-tetrofosmin in ratsrdquo Journal of Nuclear Medicine vol 45 no 12pp 2095ndash2101 2004
[24] T Takeda J Wu and T T Lwin ldquo99mTc-N-DBODC5 a novelmyocardial perfusion imaging agent for diagnosis of coronaryartery disease a reviewrdquo Recent Patents on Cardiovascular DrugDiscovery vol 1 no 2 pp 161ndash166 2006
[25] K Hatada M Ruiz L M Riou et al ldquoOrgan biodistributionand myocardial uptake washout and redistribution kinetics ofTc-99m N-DBODC5 when injected during vasodilator stressin canine models of coronary stenosesrdquo Journal of NuclearCardiology vol 13 no 6 pp 779ndash790 2006
[26] W Zhang W Fang B Li X Wang and Z He ldquoExperimentalstudy of [99mTc(PNP5) (DBODC)]+ as a new myocardialperfusion imaging agentrdquo Cardiology vol 112 no 2 pp 89ndash972009
[27] M E Marmion S R Woulfe W L Neumann D L Nosco andE Deutsch ldquoPreparation and characterization of technetiumcomplexes with Schiff base and phosphine coordination 1Complexes of technetium-99g and -99m with substitutedacac2en and trialkyl phosphines (where acac2en = NN1015840-ethylenebis[acetylacetone iminato])rdquo Nuclear Medicine andBiology vol 26 no 7 pp 755ndash770 1999
[28] C Bolzati L Uccelli A Boschi et al ldquoSynthesis of a novel classof nitrido Tc-99m radiopharmaceuticals with phosphino-thiolligands showing transient heart uptakerdquo Journal of InorganicBiochemistry vol 78 no 3 pp 369ndash374 2000
[29] M J Henzlova M D Cerqueira J J Mahmarian and S YaoldquoStress protocols and tracersrdquo Journal of Nuclear Cardiology vol13 no 6 pp e80ndashe90 2006
[30] C L Hansen R A Goldstein D S Berman et al ldquoMyocardialperfusion and function single photon emission computedtomographyrdquo Journal of Nuclear Cardiology vol 13 no 6 ppe97ndashe120 2006
[31] P Flamen A Bossuyt and P R Franken ldquoTechnetium-99m-tetrofosmin in dipyridamole-stressmyocardial SPECT imagingintraindividual comparison with technetium-99m-sestamibirdquoJournal of Nuclear Medicine vol 36 no 11 pp 2009ndash2015 1995
[32] N Tamaki N Takahashi M Kawamoto et al ldquoMyocardialtomography using technetium-99m-tetrofosmin to evaluatecoronary artery diseaserdquo Journal of Nuclear Medicine vol 35no 4 pp 594ndash600 1994
[33] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardizedmyocardial segmentation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare profes-sionals from the Cardiac Imaging Committee of the Councilon Clinical Cardiology of the American Heart AssociationrdquoJournal of Nuclear Cardiology vol 9 no 2 pp 240ndash245 2002
[34] T Sharir G Germano X Kang et al ldquoPrediction of myocardialinfarction versus cardiac death by gated myocardial perfusionSPECT risk stratification by the amount of stress-inducedischemia and the poststress ejection fractionrdquo Journal of NuclearMedicine vol 42 no 6 pp 831ndash837 2001
[35] S H Braat B Leclercq R Itti A Lahiri B Sridhara and PRigo ldquoMyocardial imaging with technetium-99m-tetrofosmincomparison of one-day and two-day protocolsrdquo Journal ofNuclear Medicine vol 35 no 10 pp 1581ndash1585 1994
[36] G Germano T Chua H Kiat J S Areeda andD S Berman ldquoAquantitative phantom analysis of artifacts due to hepatic activ-ity in technetium-99m myocardial perfusion SPECT studiesrdquoJournal of Nuclear Medicine vol 35 no 2 pp 356ndash359 1994
[37] A K Paul andH A Nabi ldquoGatedmyocardial perfusion SPECTbasic principles technical aspects and clinical applicationsrdquoJournal of Nuclear Medicine Technology vol 32 no 4 pp 179ndash187 2004
[38] J Nuyts P Dupont V Van den Maegdenbergh S Vleugels PSuetens and L Mortelmans ldquoA study of the liver-heart artifactin emission tomographyrdquo Journal of Nuclear Medicine vol 36no 1 pp 133ndash139 1995
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 9
the agent of choice for the evaluation ofmyocardial perfusionand ventricular function in patients with CAD
Abbreviations
CAD Coronary artery diseaseMPI Myocardial perfusion imagingCA Coronary angiographySPECT Single-photon emission computed
tomographyPET Positron emission computed
tomography99mTc-MIBI Technetium 99m sestamibi99mTc-N-DBODC5 99mTc(N)(DBODC)(PNP5)201Tl Thallium-20199mTc-tetrofosmin Technetium-99m-tetrofosminROI Regions of interestLAD Left anterior descending arteryLCX Left circumflex arteryRCA Right coronary arterySSS Summed stress scoreSRS Summed rest scoreSDS Summed difference scoreEDV End-diastolic volumeESV End-systolic volumeLVEF Left ventricular ejection fraction
Ethics Statement
This study was conducted in accordance with the HelsinkiDeclaration All subjects provided written informed consentbefore MPI acknowledging that they understood their rightsand obligations This study was approved by the ResearchEthics Committee of Shanxi Medical University
Conflict of Interests
The authors declare that they have no conflict of interest
Acknowledgments
This research is partly supported by Grants from the YouthScience and Technology Research Foundation of ShanxiProvince (no 2009021043-3) The authors acknowledge themembers of the participating staff for their contribution tothis clinical study
References
[1] National Hospital Discharge Survey National Health StatisticsReport no 5 2006
[2] J He D Gu X Wu et al ldquoMajor causes of death among menand women in Chinardquo The New England Journal of Medicinevol 353 no 11 pp 1124ndash1134 2005
[3] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardized myocardial sementation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare pro-fessionals from the Cardiac Imaging Committee of the Council
on Clinical Cardiology of the American Heart AssociationrdquoCirculation vol 105 no 4 pp 539ndash542 2002
[4] R J Gibbons J Abrams K Chatterjee et al ldquoACCAHA 2002guideline update for the management of patients with chronicstable anginamdashsummary article a report of the AmericanCollege of CardiologyAmerican Heart Association Task Forceon Practice Guidelines (Committee on the Management ofPatients With Chronic Stable Angina)rdquo Journal of the AmericanCollege of Cardiology vol 41 no 1 pp 159ndash168 2003
[5] WWijns P Kolh N Danchin et al ldquoGuidelines on myocardialrevascularizationrdquo European Heart Journal vol 31 pp 2501ndash2555 2010
[6] J M Jensen K A Oslashvrehus L H Nielsen J K Jensen HM Larsen and B L Noslashrgaard ldquoParadigm of pretest riskstratification before coronary computed tomographyrdquo Journalof Cardiovascular Computed Tomography vol 3 no 6 pp 386ndash391 2009
[7] N RMollet F Cademartiri C VanMieghem et al ldquoAdjunctivevalue of CT coronary angiography in the diagnostic work-up ofpatients with typical angina pectorisrdquo European Heart Journalvol 28 no 15 pp 1872ndash1878 2007
[8] R G E J Groutars J F Verzijlbergen M M C Tiel-Van Buulet al ldquoThe accuracy of 1-day dual-isotopemyocardial SPECT ina population with high prevalence of coronary artery diseaserdquoInternational Journal of Cardiovascular Imaging vol 19 no 3pp 229ndash238 2003
[9] M R Patel E D Peterson D Dai et al ldquoLow diagnostic yieldof elective coronary angiographyrdquo The New England Journal ofMedicine vol 362 no 10 pp 886ndash895 2010
[10] ldquoPharmacologic stress testingrdquo in Nuclear Cardiac ImagingPriniciples and Applications A E Iskandrian and E V GarciaEds pp 293ndash315 OxfordUniversity Press NewYork NY USA4th edition 2008
[11] R R Russell III and B L Zaret ldquoNuclear cardiology presentand futurerdquo Current Problems in Cardiology vol 31 no 9 pp557ndash629 2006
[12] G Germano H Kiat P B Kavanagh et al ldquoAutomatic quan-tification of ejection fraction from gated myocardial perfusionSPECTrdquo Journal of Nuclear Medicine vol 36 no 11 pp 2138ndash2147 1995
[13] S R Underwood C Anagnostopoulos M Cerqueira et alldquoMyocardial perfusion scintigraphy the evidencerdquo EuropeanJournal of Nuclear Medicine and Molecular Imaging vol 31 pp261ndash291 2004
[14] J Heo and A S Iskandrian ldquoTechnetium-labeled myocardialperfusion agentsrdquo Cardiology Clinics vol 12 no 2 pp 187ndash1981994
[15] B L Zaret P Rigo F J T Wackers et al ldquoMyocardial perfusionimaging with 99mTc tetrofosmin comparison to 201Tl imagingand coronary angiography in a phase III multicenter trialrdquoCirculation vol 91 no 2 pp 313ndash319 1995
[16] J J Mahmarian and M S Verani ldquoExercise thallium-201perfusion scintigraphy in the assessment of coronary arterydiseaserdquoAmerican Journal of Cardiology vol 67 no 14 pp 2Dndash11D 1991
[17] D D Miller L T Younis B R Chaitman and H StratmannldquoDiagnostic accuracy of dipyridamole technetium 99m-labeledsestamibi myocardial tomography for detection of coronaryartery diseaserdquo Journal of Nuclear Cardiology vol 4 no 1 pp18ndash24 1997
10 BioMed Research International
[18] Z He A S Iskandrian N C Gupta and M S Verani ldquoAssess-ing coronary artery disease with dipyridamole technetium-99m-tetrofosmin SPECT amulticenter trialrdquo Journal of NuclearMedicine vol 38 no 1 pp 44ndash48 1997
[19] A Boschi C Bolzati L Uccelli et al ldquoA class of asymmetricalnitrido 99mTc heterocomplexes as heart imaging agents withimproved biological propertiesrdquoNuclearMedicine Communica-tions vol 23 no 7 pp 689ndash693 2002
[20] A Boschi L Uccelli C Bolzati et al ldquoSynthesis and biologicevaluation of monocationic asymmetric 99mTc-nitride hetero-complexes showing high heart uptake and improved imagingpropertiesrdquo Journal of Nuclear Medicine vol 44 no 5 pp 806ndash814 2003
[21] C Bolzati M Cavazza-Ceccato S Agostini S TokunagaD Casara and G Bandoli ldquoSubcellular distribution andmetabolism studies of the potential myocardial imaging agent[99mTc(N)(DBODC)(PNP5)]+rdquo Journal of Nuclear Medicinevol 49 no 8 pp 1336ndash1344 2008
[22] C Cittanti L Uccelli M Pasquali et al ldquoWhole-body biodis-tribution and radiation dosimetry of the new cardiac tracer99mTc-N-DBODCrdquo Journal of Nuclear Medicine vol 49 no 8pp 1299ndash1304 2008
[23] K Hatada L M Riou M Ruiz et al ldquo99mTc-N-DBODC5a new myocardial perfusion imaging agent with rapid liverclearance comparison with 99mTc-sestamibi and 99mTc-tetrofosmin in ratsrdquo Journal of Nuclear Medicine vol 45 no 12pp 2095ndash2101 2004
[24] T Takeda J Wu and T T Lwin ldquo99mTc-N-DBODC5 a novelmyocardial perfusion imaging agent for diagnosis of coronaryartery disease a reviewrdquo Recent Patents on Cardiovascular DrugDiscovery vol 1 no 2 pp 161ndash166 2006
[25] K Hatada M Ruiz L M Riou et al ldquoOrgan biodistributionand myocardial uptake washout and redistribution kinetics ofTc-99m N-DBODC5 when injected during vasodilator stressin canine models of coronary stenosesrdquo Journal of NuclearCardiology vol 13 no 6 pp 779ndash790 2006
[26] W Zhang W Fang B Li X Wang and Z He ldquoExperimentalstudy of [99mTc(PNP5) (DBODC)]+ as a new myocardialperfusion imaging agentrdquo Cardiology vol 112 no 2 pp 89ndash972009
[27] M E Marmion S R Woulfe W L Neumann D L Nosco andE Deutsch ldquoPreparation and characterization of technetiumcomplexes with Schiff base and phosphine coordination 1Complexes of technetium-99g and -99m with substitutedacac2en and trialkyl phosphines (where acac2en = NN1015840-ethylenebis[acetylacetone iminato])rdquo Nuclear Medicine andBiology vol 26 no 7 pp 755ndash770 1999
[28] C Bolzati L Uccelli A Boschi et al ldquoSynthesis of a novel classof nitrido Tc-99m radiopharmaceuticals with phosphino-thiolligands showing transient heart uptakerdquo Journal of InorganicBiochemistry vol 78 no 3 pp 369ndash374 2000
[29] M J Henzlova M D Cerqueira J J Mahmarian and S YaoldquoStress protocols and tracersrdquo Journal of Nuclear Cardiology vol13 no 6 pp e80ndashe90 2006
[30] C L Hansen R A Goldstein D S Berman et al ldquoMyocardialperfusion and function single photon emission computedtomographyrdquo Journal of Nuclear Cardiology vol 13 no 6 ppe97ndashe120 2006
[31] P Flamen A Bossuyt and P R Franken ldquoTechnetium-99m-tetrofosmin in dipyridamole-stressmyocardial SPECT imagingintraindividual comparison with technetium-99m-sestamibirdquoJournal of Nuclear Medicine vol 36 no 11 pp 2009ndash2015 1995
[32] N Tamaki N Takahashi M Kawamoto et al ldquoMyocardialtomography using technetium-99m-tetrofosmin to evaluatecoronary artery diseaserdquo Journal of Nuclear Medicine vol 35no 4 pp 594ndash600 1994
[33] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardizedmyocardial segmentation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare profes-sionals from the Cardiac Imaging Committee of the Councilon Clinical Cardiology of the American Heart AssociationrdquoJournal of Nuclear Cardiology vol 9 no 2 pp 240ndash245 2002
[34] T Sharir G Germano X Kang et al ldquoPrediction of myocardialinfarction versus cardiac death by gated myocardial perfusionSPECT risk stratification by the amount of stress-inducedischemia and the poststress ejection fractionrdquo Journal of NuclearMedicine vol 42 no 6 pp 831ndash837 2001
[35] S H Braat B Leclercq R Itti A Lahiri B Sridhara and PRigo ldquoMyocardial imaging with technetium-99m-tetrofosmincomparison of one-day and two-day protocolsrdquo Journal ofNuclear Medicine vol 35 no 10 pp 1581ndash1585 1994
[36] G Germano T Chua H Kiat J S Areeda andD S Berman ldquoAquantitative phantom analysis of artifacts due to hepatic activ-ity in technetium-99m myocardial perfusion SPECT studiesrdquoJournal of Nuclear Medicine vol 35 no 2 pp 356ndash359 1994
[37] A K Paul andH A Nabi ldquoGatedmyocardial perfusion SPECTbasic principles technical aspects and clinical applicationsrdquoJournal of Nuclear Medicine Technology vol 32 no 4 pp 179ndash187 2004
[38] J Nuyts P Dupont V Van den Maegdenbergh S Vleugels PSuetens and L Mortelmans ldquoA study of the liver-heart artifactin emission tomographyrdquo Journal of Nuclear Medicine vol 36no 1 pp 133ndash139 1995
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

10 BioMed Research International
[18] Z He A S Iskandrian N C Gupta and M S Verani ldquoAssess-ing coronary artery disease with dipyridamole technetium-99m-tetrofosmin SPECT amulticenter trialrdquo Journal of NuclearMedicine vol 38 no 1 pp 44ndash48 1997
[19] A Boschi C Bolzati L Uccelli et al ldquoA class of asymmetricalnitrido 99mTc heterocomplexes as heart imaging agents withimproved biological propertiesrdquoNuclearMedicine Communica-tions vol 23 no 7 pp 689ndash693 2002
[20] A Boschi L Uccelli C Bolzati et al ldquoSynthesis and biologicevaluation of monocationic asymmetric 99mTc-nitride hetero-complexes showing high heart uptake and improved imagingpropertiesrdquo Journal of Nuclear Medicine vol 44 no 5 pp 806ndash814 2003
[21] C Bolzati M Cavazza-Ceccato S Agostini S TokunagaD Casara and G Bandoli ldquoSubcellular distribution andmetabolism studies of the potential myocardial imaging agent[99mTc(N)(DBODC)(PNP5)]+rdquo Journal of Nuclear Medicinevol 49 no 8 pp 1336ndash1344 2008
[22] C Cittanti L Uccelli M Pasquali et al ldquoWhole-body biodis-tribution and radiation dosimetry of the new cardiac tracer99mTc-N-DBODCrdquo Journal of Nuclear Medicine vol 49 no 8pp 1299ndash1304 2008
[23] K Hatada L M Riou M Ruiz et al ldquo99mTc-N-DBODC5a new myocardial perfusion imaging agent with rapid liverclearance comparison with 99mTc-sestamibi and 99mTc-tetrofosmin in ratsrdquo Journal of Nuclear Medicine vol 45 no 12pp 2095ndash2101 2004
[24] T Takeda J Wu and T T Lwin ldquo99mTc-N-DBODC5 a novelmyocardial perfusion imaging agent for diagnosis of coronaryartery disease a reviewrdquo Recent Patents on Cardiovascular DrugDiscovery vol 1 no 2 pp 161ndash166 2006
[25] K Hatada M Ruiz L M Riou et al ldquoOrgan biodistributionand myocardial uptake washout and redistribution kinetics ofTc-99m N-DBODC5 when injected during vasodilator stressin canine models of coronary stenosesrdquo Journal of NuclearCardiology vol 13 no 6 pp 779ndash790 2006
[26] W Zhang W Fang B Li X Wang and Z He ldquoExperimentalstudy of [99mTc(PNP5) (DBODC)]+ as a new myocardialperfusion imaging agentrdquo Cardiology vol 112 no 2 pp 89ndash972009
[27] M E Marmion S R Woulfe W L Neumann D L Nosco andE Deutsch ldquoPreparation and characterization of technetiumcomplexes with Schiff base and phosphine coordination 1Complexes of technetium-99g and -99m with substitutedacac2en and trialkyl phosphines (where acac2en = NN1015840-ethylenebis[acetylacetone iminato])rdquo Nuclear Medicine andBiology vol 26 no 7 pp 755ndash770 1999
[28] C Bolzati L Uccelli A Boschi et al ldquoSynthesis of a novel classof nitrido Tc-99m radiopharmaceuticals with phosphino-thiolligands showing transient heart uptakerdquo Journal of InorganicBiochemistry vol 78 no 3 pp 369ndash374 2000
[29] M J Henzlova M D Cerqueira J J Mahmarian and S YaoldquoStress protocols and tracersrdquo Journal of Nuclear Cardiology vol13 no 6 pp e80ndashe90 2006
[30] C L Hansen R A Goldstein D S Berman et al ldquoMyocardialperfusion and function single photon emission computedtomographyrdquo Journal of Nuclear Cardiology vol 13 no 6 ppe97ndashe120 2006
[31] P Flamen A Bossuyt and P R Franken ldquoTechnetium-99m-tetrofosmin in dipyridamole-stressmyocardial SPECT imagingintraindividual comparison with technetium-99m-sestamibirdquoJournal of Nuclear Medicine vol 36 no 11 pp 2009ndash2015 1995
[32] N Tamaki N Takahashi M Kawamoto et al ldquoMyocardialtomography using technetium-99m-tetrofosmin to evaluatecoronary artery diseaserdquo Journal of Nuclear Medicine vol 35no 4 pp 594ndash600 1994
[33] M D Cerqueira N J Weissman V Dilsizian et al ldquoStan-dardizedmyocardial segmentation and nomenclature for tomo-graphic imaging of the heart a statement for healthcare profes-sionals from the Cardiac Imaging Committee of the Councilon Clinical Cardiology of the American Heart AssociationrdquoJournal of Nuclear Cardiology vol 9 no 2 pp 240ndash245 2002
[34] T Sharir G Germano X Kang et al ldquoPrediction of myocardialinfarction versus cardiac death by gated myocardial perfusionSPECT risk stratification by the amount of stress-inducedischemia and the poststress ejection fractionrdquo Journal of NuclearMedicine vol 42 no 6 pp 831ndash837 2001
[35] S H Braat B Leclercq R Itti A Lahiri B Sridhara and PRigo ldquoMyocardial imaging with technetium-99m-tetrofosmincomparison of one-day and two-day protocolsrdquo Journal ofNuclear Medicine vol 35 no 10 pp 1581ndash1585 1994
[36] G Germano T Chua H Kiat J S Areeda andD S Berman ldquoAquantitative phantom analysis of artifacts due to hepatic activ-ity in technetium-99m myocardial perfusion SPECT studiesrdquoJournal of Nuclear Medicine vol 35 no 2 pp 356ndash359 1994
[37] A K Paul andH A Nabi ldquoGatedmyocardial perfusion SPECTbasic principles technical aspects and clinical applicationsrdquoJournal of Nuclear Medicine Technology vol 32 no 4 pp 179ndash187 2004
[38] J Nuyts P Dupont V Van den Maegdenbergh S Vleugels PSuetens and L Mortelmans ldquoA study of the liver-heart artifactin emission tomographyrdquo Journal of Nuclear Medicine vol 36no 1 pp 133ndash139 1995
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom