ComparativePharmacokineticsandAlkylatingActivityofFraction...
6
(CANCER RESEARCH 49, 753-757. February 1, 1989) Comparative Pharmacokinetics and Alkylating Activity of Fractionated Intravenous and Oral Ifosfamide in Patients with Bronchogenic Carcinoma M. J. Lind,1 J. M. Margison, T. Cerny, N. Thatcher, and P. M. Wilkinson CRC Department of Medical Oncology [M. J. L., T. C.. N. T.], Department of Clinical Pharmacology ¡J. M. M., P. M. W.], Christie Hospital and Holt Radium Institute, Manchester, M20 9BX, United Kingdom ABSTRACT 20 patients with advanced non-small cell lung cancer were treated with ifosfamide and mesna 1.5 jj/nr daily for 5 days; 10 received the drug by mouth and 10 i.v. Both schedules resulted in a reduction in the elimination half-life with an increased total and nonrenal clearance of ifosfamide over the 5-day period. Oral administration resulted in an unacceptably high incidence of encephalopathy(5/10) which was not seen in the i.v. group. In two patients this encephalopathy manifested itself as coma which lasted for 24 to 48 h but was fully reversible and in the other three cases as somnolence occurring for more than 50% of the patients' waking hours. Nadir blood counts and response rates were similar in both arms. The encephalopathy suggests that there are metabolic differences be tween the i.v. and oral routes and that a metabolite rather than the parent drug is responsible for this syndrome. In addition it was shown that the total and nonrenal clearance of the drug was significantly less when the drug was administered orally. None of the pharmacokinetic parameters either singly or in combina tion predicted for ifosfamide toxicity. No correlation between the creati- nine clearance and ifosfamide renal clearance was demonstrated suggest ing tubular reabsorption of the drug. In conclusion, ifosfamide cannot be given orally at the conventionally employed i.v. doses. INTRODUCTION Ifosfamide (I) (3-(2-chlorethyl)-2-(2-chlorethylamino)tetra- hydro-2H-1,2,3 oxazaphosphorine oxidej (Mitoxana) is a struc tural isomer of the oxazaphosphorine cyclophosphamide, a widely used alkylating agent. It is a "prodrug" that requires biotransformation in order to become cytotoxic. This occurs mainly in the liver (1) by the action of a mixed function oxidase producing the active metabolites 4-hydroxyifosfamide (2) and isophosphoramide mustard (3). Ifosfamide is less myelosup- pressive than cyclophosphamide (4) but is more urotoxic than the latter drug (5). However, with the introduction of the uroprotector mesna (uromitexan) in 1982 (6), this toxicity is now largely avoidable. This has resulted in réévaluation of ifosfamide in many malignancies (7-15). In the majority of these studies Ifosfamide has been administered intravenously with mesna either as a 24-h infusion or fractionated over 3-5 days. Cerny et al. (16) and Wagner et al. (17) have both shown the bioavailability of orally administered ifosfamide to be close to 100%. However both authors found an unacceptably high level of central nervous system toxicity at conventionally em ployed doses. A study of patients with non-small cell lung cancer comparing fractionated doses of ifosfamide given either orally or i.v. over 5 days was planned to determine whether encepha lopathy could be avoided by dividing the oral dose over several days. In addition a pharmacokinetic study was undertaken to ascertain if any pharmacokinetic parameter correlated with drug toxicity and to determine any differences in pharmacoki netic handling between the two routes of administration. Received 4/20/88; revised 10/3/88; accepted 10/26/88. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1To whom requests for reprints should be addressed, at Department of Medical Oncology, University of Manchester, Christie Hospital, Wilmslow Road, M20 9BX, England. PATIENTS, MATERIALS, AND METHODS Patients 20 patients with advanced histologically proven non-small cell lung cancer were treated with ifosfamide. Their median age was 59.5 years (range, 44-71 years) and all had pretreatment Karnofsky scores >50 and creatinine clearances of >50 ml/min. The two regimens employed were as follows: (a) 10 patients received i.v. ifosfamide (Boehringer Ingelheim, Mitoxana) at a dose of 1.5 g/ m2/day for 5 days. The dose was rounded down to the nearest 500 mg. Ifosfamide was given as a 30-min infusion in 250 ml normal saline. The uroprotector 2-mercaptoethane sodium (mesna) was given at a dose of 1.5 g/m2/day in 2 liters of normal saline as a 24-h infusion for 5 days. (¿>) 10 patients received oral ifosfamide (only available as 500- mg capsules) at a dose of 1.5 g/m2/day for 5 days 30-60 min before breakfast. The dosage was rounded up or down as outlined in a. Mesna was administered in a similar manner as outlined in a with a further 500 mg of oral mesna given every 6 h for four doses after the last i.v. mesna dose on Day 5. Serial blood samples were collected at 0, 0.25, 0.5, 1, 1.5, 2, 2.5, 3, 6, 9, and 24 h postifosfamide administration on each of the 5 days in addition to 24-h urine samples. Blood samples were centrifuged im mediately; the serum was separated off and stored at —¿ 20'C. Urine samples were also stored at —¿ 20°C. Analytical Methods Plasma, Urinary Ifosfamide and Urinary 4Keto Ifosfamide Assay. These were determined using the high-performance liquid Chromato graphie method of Margison et al. (18). Metabolite Alkylating Activity. Total alkylating activity was meas ured using a modification of the method of Friedman and Boger (19) in which the color developed by reaction with nitro-benzyl-pyridine was extracted into ether containing 5% triethylamine. Bischloroethylamine was used as a standard and values extrapolated from the standard curve were converted to Mg/ml equivalents of nor nitrogen mustard. As ifosfamide reacts weakly with nitro-benzyl-pyridine a second standard curve was constructed containing ifosfamide at concentrations in the range found in serum. The contribution of ifosfamide to the total alkylating activity of the sample could therefore be determined and a value for the alkylating activity of ifosfamide metabolites could thus be assessed. Kinetic Analysis. For patients receiving i.v. drug the serum concen tration profile was fitted to a two compartment model using the noniterative computer programme MODFIT as described by Mclntosh (20). The intercept and rate constants were used to calculate the half- lives (Iv,), area under the curve (AUG.) and volumes of distribution Total body clearance was determined by the formula, C/,0i = D/ AUG., where D is the dose administered. By measuring the 24-h urinary excretion of ifosfamide the renal clearance of the drug can be calculated from the formula, Cl, = .Y./AUG», where Cl, is the renal clearance and Xu is the amount excreted in the urine over 24 h. From Cl, the nonrenal clearance of the drug could be derived from the formula, CI,0, = Cl, + Cl„„ where Cl,, is the nonrenal clearance. For the oral data a linear regression analysis of the terminal phase was used to determine the half-life and rate constant. The area under the curve was calculated by the trapezoidal rule and extrapolated to infinity using the Nelson Wagner correction factor, i.e., AUG. = AUCi4 + Cu/K,r,m, where AUC34 is the area under the curve for the first 24 h, 753 on April 23, 2018. © 1989 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
-
Upload
truongkhue -
Category
Documents
-
view
214 -
download
1
Transcript of ComparativePharmacokineticsandAlkylatingActivityofFraction...

(CANCER RESEARCH 49, 753-757. February 1, 1989)
Comparative Pharmacokinetics and Alkylating Activity of Fractionated Intravenous
and Oral Ifosfamide in Patients with Bronchogenic CarcinomaM. J. Lind,1 J. M. Margison, T. Cerny, N. Thatcher, and P. M. Wilkinson
CRC Department of Medical Oncology [M. J. L., T. C.. N. T.], Department of Clinical Pharmacology ¡J.M. M., P. M. W.], Christie Hospital and Holt Radium Institute,Manchester, M20 9BX, United Kingdom
ABSTRACT
20 patients with advanced non-small cell lung cancer were treated withifosfamide and mesna 1.5 jj/nr daily for 5 days; 10 received the drug bymouth and 10 i.v. Both schedules resulted in a reduction in the eliminationhalf-life with an increased total and nonrenal clearance of ifosfamide overthe 5-day period. Oral administration resulted in an unacceptably highincidence of encephalopathy(5/10) which was not seen in the i.v. group.In two patients this encephalopathy manifested itself as coma whichlasted for 24 to 48 h but was fully reversible and in the other three casesas somnolence occurring for more than 50% of the patients' waking
hours. Nadir blood counts and response rates were similar in both arms.The encephalopathy suggests that there are metabolic differences between the i.v. and oral routes and that a metabolite rather than the parentdrug is responsible for this syndrome. In addition it was shown that thetotal and nonrenal clearance of the drug was significantly less when thedrug was administered orally.
None of the pharmacokinetic parameters either singly or in combination predicted for ifosfamide toxicity. No correlation between the creati-nine clearance and ifosfamide renal clearance was demonstrated suggesting tubular reabsorption of the drug. In conclusion, ifosfamide cannot begiven orally at the conventionally employed i.v. doses.
INTRODUCTION
Ifosfamide (I) (3-(2-chlorethyl)-2-(2-chlorethylamino)tetra-hydro-2H-1,2,3 oxazaphosphorine oxidej (Mitoxana) is a structural isomer of the oxazaphosphorine cyclophosphamide, awidely used alkylating agent. It is a "prodrug" that requires
biotransformation in order to become cytotoxic. This occursmainly in the liver (1) by the action of a mixed function oxidaseproducing the active metabolites 4-hydroxyifosfamide (2) andisophosphoramide mustard (3). Ifosfamide is less myelosup-pressive than cyclophosphamide (4) but is more urotoxic thanthe latter drug (5). However, with the introduction of theuroprotector mesna (uromitexan) in 1982 (6), this toxicity isnow largely avoidable. This has resulted in réévaluationofifosfamide in many malignancies (7-15). In the majority ofthese studies Ifosfamide has been administered intravenouslywith mesna either as a 24-h infusion or fractionated over 3-5days. Cerny et al. (16) and Wagner et al. (17) have both shownthe bioavailability of orally administered ifosfamide to be closeto 100%. However both authors found an unacceptably highlevel of central nervous system toxicity at conventionally employed doses. A study of patients with non-small cell lung cancercomparing fractionated doses of ifosfamide given either orallyor i.v. over 5 days was planned to determine whether encephalopathy could be avoided by dividing the oral dose over severaldays. In addition a pharmacokinetic study was undertaken toascertain if any pharmacokinetic parameter correlated withdrug toxicity and to determine any differences in pharmacokinetic handling between the two routes of administration.
Received 4/20/88; revised 10/3/88; accepted 10/26/88.The costs of publication of this article were defrayed in part by the payment
of page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
1To whom requests for reprints should be addressed, at Department of MedicalOncology, University of Manchester, Christie Hospital, Wilmslow Road, M209BX, England.
PATIENTS, MATERIALS, AND METHODS
Patients
20 patients with advanced histologically proven non-small cell lungcancer were treated with ifosfamide. Their median age was 59.5 years(range, 44-71 years) and all had pretreatment Karnofsky scores >50and creatinine clearances of >50 ml/min.
The two regimens employed were as follows: (a) 10 patients receivedi.v. ifosfamide (Boehringer Ingelheim, Mitoxana) at a dose of 1.5 g/m2/day for 5 days. The dose was rounded down to the nearest 500 mg.Ifosfamide was given as a 30-min infusion in 250 ml normal saline.The uroprotector 2-mercaptoethane sodium (mesna) was given at adose of 1.5 g/m2/day in 2 liters of normal saline as a 24-h infusion for5 days. (¿>)10 patients received oral ifosfamide (only available as 500-mg capsules) at a dose of 1.5 g/m2/day for 5 days 30-60 min before
breakfast. The dosage was rounded up or down as outlined in a. Mesnawas administered in a similar manner as outlined in a with a further500 mg of oral mesna given every 6 h for four doses after the last i.v.mesna dose on Day 5.
Serial blood samples were collected at 0, 0.25, 0.5, 1, 1.5, 2, 2.5, 3,6, 9, and 24 h postifosfamide administration on each of the 5 days inaddition to 24-h urine samples. Blood samples were centrifuged immediately; the serum was separated off and stored at —¿�20'C. Urinesamples were also stored at —¿�20°C.
Analytical Methods
Plasma, Urinary Ifosfamide and Urinary 4Keto Ifosfamide Assay.These were determined using the high-performance liquid Chromatographie method of Margison et al. (18).
Metabolite Alkylating Activity. Total alkylating activity was measured using a modification of the method of Friedman and Boger (19)in which the color developed by reaction with nitro-benzyl-pyridine wasextracted into ether containing 5% triethylamine. Bischloroethylaminewas used as a standard and values extrapolated from the standard curvewere converted to Mg/ml equivalents of nor nitrogen mustard. Asifosfamide reacts weakly with nitro-benzyl-pyridine a second standardcurve was constructed containing ifosfamide at concentrations in therange found in serum. The contribution of ifosfamide to the totalalkylating activity of the sample could therefore be determined and avalue for the alkylating activity of ifosfamide metabolites could thus beassessed.
Kinetic Analysis. For patients receiving i.v. drug the serum concentration profile was fitted to a two compartment model using thenoniterative computer programme MODFIT as described by Mclntosh(20). The intercept and rate constants were used to calculate the half-lives (Iv,), area under the curve (AUG.) and volumes of distribution
Total body clearance was determined by the formula, C/,0i = D/AUG., where D is the dose administered. By measuring the 24-h urinaryexcretion of ifosfamide the renal clearance of the drug can be calculatedfrom the formula, Cl, = .Y./AUG»,where Cl, is the renal clearance andXu is the amount excreted in the urine over 24 h. From Cl, the nonrenalclearance of the drug could be derived from the formula, CI,0, = Cl, +Cl„„where Cl,, is the nonrenal clearance.
For the oral data a linear regression analysis of the terminal phasewas used to determine the half-life and rate constant. The area underthe curve was calculated by the trapezoidal rule and extrapolated toinfinity using the Nelson Wagner correction factor, i.e., AUG. = AUCi4+ Cu/K,r,m, where AUC34 is the area under the curve for the first 24 h,
753
on April 23, 2018. © 1989 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

FRACTIONATED i.V. AND ORAL IFOSFAMIDE
CM is the concentration of drug at 24 h, and AVi,,,,is the eliminationrate constant.
The volume of distribution was calculated from the formula, Vipa=X/Co, where Vdfois the volume of distribution, X is the dose and Co isthe concentration at time 0 when the terminal phase is extrapolatedback to zero. Total body clearance, renal clearance and nonrenalclearance were calculated as described for the i.v. data.
Statistical Methods. To determine any change with time of pharma-cokinetic parameters, a Friedman two-way analysis of variance wasused. To compare parameters between the i.v. and oral groups a Mann-Whitney test was used. To examine any correlations between pharma-cokinetic parameters and toxicity Kendall correlation tests were used.
RESULTS
Ifosfamide Pharmacokinetics
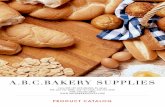
The pharmacokinetic parameters for the i.v. group are summarized in Table 1 and shown graphically in Fig. 1. The valuesare expressed as medians and ranges. The terminal eliminationhalf-life declined from a median of 6.163 (range, 3.894-8.154)hours on Day 1 to 3.762 (range, 2.655-4.780) hours on Day 5(P = 0.018 Friedman). The total clearance of parent drugincreased from a median of 69.185 (range, 60.877-80.500) ml/min on Day 1 to 123.185 (range, 102.15-181.69) ml/min onDay 5 (P = 0.0001 Friedman) and was associated with anincrease in the nonrenal clearance from 60.082 (range, 47.027-65.134) to 104.285 (range, 100.470-167.815) ml/min (P =0.002 Friedman) Table 1. However there was no significantincrease in the renal clearance of ifosfamide or the percentageurinary excretion of drug per 24-h period over the 5 days. Inaddition the area under the serum concentration time curve fellfrom 574.8 (range, 284.000-821.400) to 346.33 (range,200.425-407.800) Mg/ml. (P = 0.0001 Friedman).
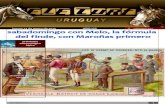
Following oral administration of the drug, peak ifosfamidelevels were reached between 1 and 2 h postadministration (seeFig. 2). The median elimination half-life declined from 5.775(range, 4.620-6.93) h on Day 1 to 3.46 (range, 2.230-4.330) hon Day 5 (P = 0.031 Friedman). The total clearance increasedfrom 51.334 (range, 39.000-69.600) ml/min on Day 1 to85.833 (range, 69.166-109.833 mls/min on Day 5 (P= 0.024).This was associated with an increase in the nonrenal clearancefrom 46.554 (range, 34.959-53.308) ml/min on Day 1 to67.881 (range, 57.520-79.323) ml/min on Day 5 (P = 0.02Friedman). However there was no significant increase in therenal clearance of ifosfamide or the percentage urinary excre
tion of drug from Day 1 to 5. In addition the area under theserum concentration time curve fell from 680.651 (range,529.147-1105.535) Mgh/ml on Day 1 to 382.620 (range,323.885-471.871) Mgh/ml on Day 5 (P = 0.008 Friedman).
Comparing the pharmacokinetic parameters between i.v. andoral administration in Tables 1 and 2 there was no significantdifference on any one day between elimination half-life, areaunder the curve, and renal clearance, with respect to route ofadministration. However the total clearance and nonrenal clearance were significantly less on any one day when the drug wasadministered orally (P< 0.05 Mann-Whitney). In addition Vd(p0)was significantly less than Vdw (P < 0.05 Mann-Whitney) onany one day.
Despite the wide variability in pharmacokinetic parametersthere was no correlation between any such parameter and thedevelopment of hematological (measured as the nadir absolutewhite blood count or percentage change in white blood cellcount) or CNS toxicity.
Metabolite Alkylating Levels and Excretion of 4-Ketoifosfamide
These results are summarized in Tables 3 and 4 and graphically in Figs. 3 and 4.
i.v.. In those patients receiving the drug i.v. there was anincrease in the area under the metabolite alkylating curve onsuccessive days of administration but this did not reach statistical significance. However, the peak metabolite alkylating activity rose from 7.96 (range, 5.600-17.700) (/ig equivalents ofnornitrogen mustard/ml) on Day 1 to 14.05 (range, 7.880-24.660) on Day 5 (P = 0.005 Friedman). In addition there wasa significant increase in the 24-h urinary excretion of 4-keto-ifosfamide from 0.064 (range, 0-0.32) (percentage of parentdrug administered) on Day 1 to 0.32 (range, 0.15-0.72) on Day5 (/>= 0.001 Friedman).
Oral. In patients receiving the drug orally the peak metabolitealkylating levels and area under the metabolite alkylating curveincreased over the 5 days. However the difference was notstatistically significant. Likewise urinary levels of 4-ketoifos-famide increased over this period of time but was not statistically significantly.
Oral Versus i.v.. There was no statistical significant differencein metabolite alkylating levels between oral and i.v. administration.
Wide variability in the serum concentration of alkylatingmetabolites was seen; some patients produced virtually no suchmetabolites in the serum on certain days and others very high
Table 1 Pharmacokinetic parameters in 10 patients with non-small cell lung cancer receiving 1.5 g/m1 of i.v. ifosfamide per day, Days 1-5
Values are medians and ranges.
ParameterTvß(h)°C/,,,,
(ml/min)*CI,
(ml/min)fCl„
(ml/min)''AUC_G<gri/ml)'Va
(liters/16.163(3.894-8.154)69.185(64.600-112.300)11.101(4.218-17.973)60.082(47.027-65.134)574.800(284.000-821.400)40.330(28.700-51.900)24.620(3.640-7.790)82.139(85.300-143.999)12.823(3.439-20.727)72.309(54.358-93.995)488.251(334.082-724.899)40.350(28.500-61.810)Day34.330(2.390-4.950)94.003(81.8300-147.900)15.070(7.042-20.365)81.443(69.733-126.000)385.668(238.250-555.203)34.800(19.730-61.810)44.318(3.300-4.620)112.820(102.150-181.690)17.159(9.680-29.947)93.020(71.143-123.360)346.330(227.082-468.600)41.540(28.870-51.390)53.762(2.655-4.780)123.185(60.870-80.500)14.836(5.369-29.988)104.285(100.470-167.815)284.036(200.425-407.800)39.920(31.260-34.640)P0.0180.00010.1440.0020.00010.970"
T*ß,terminal eliminationhalf-life.*C/10„total bodyclearance.'CI,, renalclearance.dCl„,nonrenalclearance.'AUG., area under thecurve.fVa, volume of distribution.
754
on April 23, 2018. © 1989 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

FRACTIONATED i.v. AND ORAL IFOSFAMIDE
TIME/hrs0 10 20 30
Fig. 1. Mean ifosfamide levels in patients receiving i.v. ifosfamide (l.S g/m2)Days 1-5.
10°
DAY 1
DAY 2
DAY 3DAY 4
DAY 5
20
Fig. 2. Mean ifosfamide levels in patients receiving oral ifosfamide (l.S g/m2)Days 1-5.
levels. However there was no correlation between metabolitealkylating activity and hematological or neurological toxicity.
Clinical Data
Toxicity. The median nadir WBC (measured at 10 days afterthe start of chemotherapy) experienced in the i.v. group was3.8 x lO'/Hter and that in the oral group 5.45 x 109/lher (/>>0.05 Student's t test).
Five of the patients in the oral arm experienced CNS toxicity> WHO Grade III (20) requiring early termination of theirtreatment course as opposed to none of the patients in the i.v.arm (0.01 < P < 0.02, eh i-squared). Two of these patients inthe oral arm became comatosed for 24-48 h but recoveredcompletely without any neurological sequelae. Mild degrees ofencephalopathy, consisting mainly of somnolence (<50% ofwaking hours), were seen in the i.v. arm of the study. Nauseaand vomiting were mild and identical in both arms.
Tumor Response. A total of eight partial responses were seen;four occurring in each arm.
DISCUSSION
Our initial values for the terminal half-life, clearance, andvolume of distribution in the i.v. group compare well with thoseof other investigators (21-23). The results presented here indicate that fractionation of either an i.v. or orally administereddose of ifosfamide over 5 days results in increased nonrenal andtotal clearance of the parent drug. This was associated with adecrease in the elimination half-life, and an increase in the peak
metabolite alkylating activity, the AUC of the metabolite alkylating activity time curve, and production of 4-ketoifosfamide.
One possible explanation is that fractionation of the ifosfamide dosage leads to induction of those enzymes responsible formetabolism of the drug. Similar results have been obtained withfractionating cyclophosphamide administration (24). Furtherevidence for auto induction of cyclophosphamide metabolismcomes from D'Incaici et al. (25) who compared the pharmaco-
kinetics of the first and last courses of patients receiving cyclophosphamide continuously for 1 year and found the half-life tobe shorter after continual exposure to the drug. In support ofthis theory Tchekmedyian et al. (26) have shown that the areaunder the alkylating activity time curve following a 5-day continuous infusion of cyclophosphamide was three times thatexpected when the same dose was given as a bolus.
More recently it has been shown that fractionating the doseof cyclophosphamide over 2 days leads to increased peak levelsof the 4-hydroxy metabolite (27). Wagner (28) has also pub
lished data on the pharmacokinetic of i.v. ifosfamide dosagefractionated over a 2-day period and has shown a decrease inelimination half-life from 6.4 ±2.4 h on Day 1 to 5.3 ±2.8 hon Day 2. A reduction in ifosfamide half-life from 8.3 h to 6.3h over a 3-day period has also been demonstrated (29). Ourdata show that a further reduction in the elimination half-life
occurs with more prolonged administration of the drug.This phenomenon of auto induction of metabolism may also
explain why fractionation of ifosfamide dosage is associatedwith an improved therapeutic index (30, 31). Of particularinterest was the high incidence and severity of CNS side-effects
in patients receiving the drug by the oral route. A metaboliterather than the parent compound is likely to be responsible forthis toxicity and imply with a first-pass effect is producing more
active metabolites with the oral route. However, the near 100%
Table 2 Pharmacokinetic parameters in 10 patients with non-small cell lung cancer receiving 1.5 g/m2 of oral ifosfamide per day, Days 1-5
Values are medians and ranges.
ParameterT*(h)cC/,,»
(ml/min)"Cl,
(ml/min)'Cl„
(ml/min/AUC.
Gigh/ml)"K^,
(liters)*15.775(4.620-6.930)51.334(39.000-69.660)7.829(0.058-16.358)46.554(34.959-53.308)680.651(529.147-1105.535)24.035(16.730-36.410)23.745(3.300-5.330)63.167(39.833-88.333)6.610(3.480-16.348)60.860(51.823-76.727)525.321(422.230-732.915)21.865(11.970-33.170)Day3"3.850(3.300-5.330)66.666(37.166-121.500)12.153(3.480-27.659)57.420(29.553-93.841)464.482(269.830-563.522)22.930(10.650-39.220)4»3.460(3.150-5.770)70.833(54.000-127.333)12.500(0.000-34.184)70.138(44.166-93.1490)441.016(291.270-552.000)23.605(16.200-39.600)5»3.460(2.230-4.330)85.833(69.166-109.833)16.705(0.000-21.930)67.881(57.520-79.323)382.620(323.885-471.875)25.960(16.590-32.900)P0.0310.0240.1500.0200.0080.910
" Median of nine patients.'' Median of six patients.' /.:. terminal elimination half-life.a C/ioi, total body clearance.' <'/,. renal clearance.1CI,,, nonrenal clearance.* AUG., area under the curve.* KI/»,volume of distribution.
755
on April 23, 2018. © 1989 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

FRACTIONATED i.v. AND ORAL IFOSFAMIDE
Table 3 Metabolic parameters in 10 patients with non-small cell lung cancer receiving 1.5 g/m2 of i.v. ifosfamide per day, Days 1-5
Values are medians and ranges.
ParameterMetabolite"AUC (Mgh/ml
equivalents of nornitrogenmustard)Peak
metabolite alkylating activity (*igh/ml equivalents ofnornitrogenmustard)4-Keto
I (%)*1132.595
(34.570-182.595)7.960
(5.360-17.700)0.064
(0.000-0.320)2135.845
(71.170-212.010)10.800
(4.390-14.360)0.222
(0.028-0.340)Day3130.570
(86.510-312.750)8.845
(7.900-20.400)0.217
(0.100-0.376)4120.790
(69.800-226.720)9.590
(5.120-15.400)0.233
(0.115-0.430)5166.555
(70.080-238.720)14.050(7.880-24.660)0.320
(0.150-0.720)P0.0950.0050.0006
°Metabolite AUC, area under the metabolite alkylating activity time curve.* 4-Keto I, the percentage of the administered dose excreted as 4-ketoifosfamide.
Table 4 Metabolic parameters in 10 patients with non-small cell lung cancer receiving 1.5 g/m2 of oral ifosfamide per day, Days 1-5
Values are medians and ranges.
ParameterMetabolite'AUC (jigh/ml
equivalents of nornitrogenmustard)Peak
metabolite alkylating activity Gjgh/ml equivalents ofnornitrogenmustard)4-Keto
I (%f183.735
(0.689-211.170)6.015
(1.990-11.380)0.158
(0.004-0.450)290.085
(6.886-291.170)7.120
(2.750-16.310)0.165
(0.098-0.340)Day3"124.315
(61.458-247.275)7.580
(4.720-16.080)0.240
(0.020-0.590)4*188.207
(87.900-248.390)10.035
(5.810-20.740)0.280
(0.070-0.370)5*90.489
(56.301-202.669)8.380
(5.350-19.590)0.250
(0.000-0.610)P0.2750.1340.355
" Median of nine patients.* Median of six patients.c Metabolite AUC, area under the metabolite alkylating activity time curve.d 4-Keto I, percentage of the administered dose excreted as 4-ketoifosfamide.
10-
g8
Fig. 3. Mean metabolite alkylating levels in patients receiving i.v. ifosfamide(1.5 g/m2) Days 1-5.
I 8
I
DAYlDAYS
Fig. 4. Mean metabolite alkylating levels in patients receiving oral ifosfamide(1.5 g/m2) Days 1-5.
bioavailability demonstrated by other investigators fails to demonstrate any significant first-pass effect.
One explanation may be that rather than quantitative differences, there may be qualitative differences in the metabolismbetween the two routes of administration. Oral administrationof cyclophosphamide results in a greater production of alkylating metabolites than i.v. administration supporting this theory.
Juma et al. (32) speculated that a different profile of metabolites was produced by oral administration. Others however
have failed to show any significant difference in the levels of 4-hydroxy cyclophosphamide and phosphoramide mustard between oral and i.v. routes of administration (33). It is howeverimportant to realize that the metabolism of ifosfamide is notidentical to that of cyclophosphamide. Dechloroethylation canaccount for up to 25% of the metabolism of ifosfamide (34),while this pathway is a very minor one for cyclophosphamidemetabolism. In this context, dechloroethylation of ifosfamideresulting in the production of chloracetaldehyde has been suggested by Goren et al. (35) as a possible cause of the CNStoxicity and it may be that this pathway predominates in oraladministration.
When the area under the metabolite alkylating activity timecurve and the peak alkylating metabolite level attained on eachday of ifosfamide administration in the two patient groups inTables 3 and 4 are compared, there was at no time a significantdifference between i.v. and oral routes of administration. It ishowever important to realize the limitations of the NBP reaction. Certain metabolites of cyclophosphamide and ifosfamideare nonreactive or only weakly positive in this test e.g., acroleindoes not alkylate. It is therefore possible to envision a situationwhere two patients have identical alkylating activity in theserum but quite different profiles of metabolites. For this reasona simple method of assaying all the metabolites individuallywould be useful. Oral administration could result in a differentprofile of metabolites which is not reflected in the NBP test.
In our study none of the pharmacokinetic parameters measured correlated with either CNS toxicity or levels of leucopenia.Furthermore there was no correlation between the AUC for theplasma metabolite alkylating activity and the nadir white bloodcell count or percentage change in white blood count. Our datais in contrast to the data of Mourisden et al. (36). This is againprobably a reflection of the lack of specificity of the NBP
756
on April 23, 2018. © 1989 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

FRACTIONATED i.V. AND ORAL 1FOSFAMIDE
reaction and the complexity of the metabolic pathway of ifos-famide.
The values obtained for the renal clearance of ifosfamidewere very much lower than the creatinine clearance and therewas no correlation between the creatinine clearance and renalclearance of the drug unlike the results of Nelson (29). For adrug as water soluble as ifosfamide this data suggests somedegree of tubular reabsorption.
With regard to the comparative pharmacokinetics betweenoral and i.v. administration, the total body clearance, nonrenalclearance, and volumes of distribution were statistically significantly less with oral administration. Our value for V^p,agreesclosely with that obtained by Allen (21) and approximatesclosely to the total body water. This suggests that when administered i.v. ifosfamide is distributed throughout the total bodywater with little tissue binding. The lower value of Va^ isdifficult to explain, but Vd(mand Vd(p0)are not strictly comparable as both parameters are model dependent. There is noclear explanation of this discrepancy but it suggests that ifosfamide is distributed differently with oral administration. Weconclude that ifosfamide fractionated over 5 days leads toautoinduction of its metabolism. The clearance of the drug islower by the oral route and may be related to the higherincidence of CNS side-effects.
REFERENCES
1. Brock, N., and Hohrst, H-J. ÃœberDie Aktiverung von Cyclophosphamid inVivo und IB Vitro. Arzneim. Forsch., 13:1021-1031, 1963.
2. Connors, T. A., Cox, P. J., Farmer, P. B., Foster, A. B., and Jarman, M.Some studies of the active intermediates formed in the microsomal metabolism of cyclophosphamide and isophosphamide. Biochem. Pharmacol., 23:115-129, 1974.
3. Brock, N. The oxazaphosphorines. Cancer Treat. Rev., /»(Suppl.A): 3-15,1983.
4. Brade, W., Seeber, S., and Herdirch, K. Comparative activity of cyclophosphamide and ifosfamide. Cancer Chemother. Pharmacol., M'fSuppL 2): 1-9,
1986.5. Teufel, G., and Pfleiderer, A. Ifosfamid im Vergleich zu Endoxan bei fort
geschrittenem Ovarialkarzinomen. Geburtshilfe Frauenheilkd., 36: 274,1986.
6. Bryant, B. M., Jarman, M., Ford, H. T., and Smith, I. E. Prevention ofisophosphamide-induced urothelial toxicity with 2 mercaptoethane sulphon-ate sodium (mesnum) in patients with advanced carcinoma. Lancet., 22:657-659, 1980.
7. Hoefer, H., Scheef, W., Titscher, R., and Kokron, O. Treatment of broncho-genie cancer and lung métastasesof solid tumours with ifosfamid (Author'stransÃ).Osterr-Kneip-Mag., /: 3-7, 1974.
8. Costanzi, J. J., Cagliano, R., Loukas, D., Panettiere, F. J., and Hokanson,J. A. Ifosfamide in thà treatment of recurrent or disseminated lung cancer.A phase II study of two dose schedules. Cancer (Phila.), 41: 1715-1719,1978.
9. Klein, H. O., Wickramanayake, P. D., Coerper, Cl., Christian, E., Pohl, J.,and Brock, N. High dose ifosfamide and mesna as continuous infusion overfive days-a phase I/II trial. Cancer Treat. Rev., 70(Suppl. A): 167-173,1983.
10. Marti, C., Kroner, T., and Cserhati, M. Iphosphamide in the treatment ofmetastatic osteosarcoma (Abstract). UICC Congress, Lausanne, 41:05-0041,1981.
11. Coleman, R. E., Harper, P. G., Gallagher, C, Osborne, R. Rankin, E. M.,Silverstone, A. C., Slevin, M. L., Souhami, R. L., Tobias, J. S., and Trask,C. W. A phase II study of ifosfamide in advanced and relapsed carcinoma ofthe cervix. Cancer Chemother. Pharmacol., /*(3): 280-283, 1986.
12. Blackledge, G., Meanwell, C., Mould, J., Lawton, F., Stuart, N., Kavanagh,N., Spooner, J.. Latief, D., and Chetiyawardana, A. Studies of Ifosfamide incervical carcinoma (Abstract 17). J. Cancer Res. Clin. Oncol., J(Suppl. S32):1986.
13. De la Garza, J., and Cardenas, J. Ifosfamide (Holaxan IFA) in the treatmentof advanced ovarian carcinoma (Abstract 428). Proceedings of the 13th
International Cancer Congress, Seattle, p. 76, 1982.14. Wandl, U., Kath, R., Schumacher, G., Niederle, N., Hoffken, K., and
Schmidt, C. G. Treatment of high risk non seminomatous germ cell tumours(Abstract 702). 4th European Conference on Clinical Oncology and CancerNursing, 1987.
15. Schvartzman, E., Scopinaro, M., and Angueyra, N. Phase II study of Ifosfamide as a single drug for relapsed patients (Abstract 611). 4th EuropeanConference on Clinical Oncology and Cancer Nursing, 1987.
16. Cerny, T., Margison, J. M., Thatcher, N., and Wilkinson, P. M. Bioavail-ability of ifosfamide in patients with bronchial carcinoma. Cancer Chemother. Pharmacol., 18: 261-264, 1986.
17. Wagner, T., and Drings, P. Pharmacokinetics and Bioavailability of OralIfosfamide in tumour therapy. In: W. P. Brade, G. A. Nagel, S. Seeber (eds.),Ifosfamide in Tumour Therapy. Contributions to Oncology, Vol. 26, pp. 53-59. Basel: Karger, 1987.
18. Margison, J. M., Cerny, T., Thatcher, N., and Wilkinson, P. M. A simplequantitative HPLC assay for ifosfamide in biological fluids. Biomed. Chro-matogr., 7(3): 101-103, 1986.
19. Friedman, O. M., and Boger, E. Colorimetrie estimation of the nitrogenmustards in aqueous media. Anal. Chem., 33: 906-910, 1961.
20. Mcintosh, J. E. A., and Mcintosh, R. P. Mathematical Modeling and Computing in Endocrinology. Berlin: Springer-Verlag, 1980.
21. Allen, L. M., Creaven, P. J., and Nelson, R. L. Studies on the humanpharmacokinetics of ifosfamide (NSC-109724). Cancer Treat. Rep., 60:451 -458, 1976.
22. Wagner, T., Heydrich, D., Jork, T., Voelecker, G., and Hohorst, H. J.Comparative study on human pharmacokinetics of activated ifosfamide andcyclophosphamide by a modified fluorometric test. J. Cancer Res. Clin.Oncol., /00.-95-104, 1984.
23. Schmoll, H. J., Diehl, V., Hartlapp, J., Illiger, H. J., Mitrou, P. S. Hoffman,L., Schmilz, D., Bombik, B. M., Beyer, J. H., Queisser, W., Haselberger, H.,Sterry., Douwes, F. W., and Schnait, U. Vorlaufige Ergebnisse der Phase HIStudie Bleomycin/Vinblastin/Cisplaytin/Ifosfamid bei disseminierten Hodentumoren. In: H. H. Illiger, H. Sack, S. Seeber, and L. Weissbach (eds.),Nicht-Seminomatose Hodentumoren Contributions to Oncology, Vol. 8,209-216. Basel: Karger, 1982. Contrib. Oncol., 8: 209-216, 1982.
24. Graham, M. I., Shaw, I. C, Souhami, R. L., Sidau, B., Harper, P. G., andMaclean, A. E. Decreased plasma half life of cyclophosphamide duringrepeated high dose administration. Cancer Chemother. Pharmacol., 10:192-193, 1983.
25. D'Incaici, M., Bolis, G., Facchinetti, T., Mangioni, C., Morase, L., Moraz-
zoni, P., and Salmona, M. Decreased half life of Cyclophosphamide inpatients under continual treatment. Eur. J. Cancer, 15: 7-10, 1979.
26. Simon Tchekmedyian, N., Egorin, M. J., Cohen, B. E., Kaplan, R. S., Poplin,E., and Aisner, J. Phase I clinical and pharmacokinetic study of cyclophosphamide administered by five day continuous intravenous infusion. CancerChemother. Pharmacol., 18: 33-38, 1986.
27. Schuler, U., Ehninger, G., and Wagner, T. Repeated high dose cyclophosphamide administration in bone marrow transplantation: exposure to activated metabolites. Cancer Chemother. Pharmacol., 20: 248-252, 1987.
28. Wagner, T., and Ehninger, G. Self induction of cyclophosphamide andifosfamide metabolism by repeated high dose treatment. Ifosfamide in tumourtherapy. In: W. P. Brade, G. A. Nagel, S. Seeber (eds.), Contribution toOncology, Vol. 26, pp. 53-59. Basel: Karger, 1987.
29. Nelson, R. L., Allen, L. M., and Creaven, P. J. Pharmacokinetics of divideddose ifosfamide. Clin. Pharmacol. Ther., 19: 365-370, 1976.
30. Klein, O. H., Wickramanyake, P. D., Christian, E., and Coerper, C. Therapeutic effects of single push or fractionated injections or continous infusionof oxazophosphorines (Cyclophosphamide, Ifosfamide, Asta Z 7557). Cancer(Phila.), 54(Suppl. 6): 1193-1203, 1984.
31. Morgan, L. R., Harrison, E. F., Hawke, J. E., Hunter, H. L., Costanzi, J. J.,Plotkin, D., Tucker, W. G., and Worall, P. M. Toxicity of single vs Frac-tionated-Dose ifosfamide in Non Small Cell lung Cancer: A multicenterstudy. Semin. Oncol. 5>(Suppl. 1): 66-70, 1982.
32. Juma, F. D., Rogers, H. J., and Trounce, J. R. Pharmacokinetics of cyclophosphamide and alkylating activity in man after intravenous and oraladministration. Br. J. Clin. Pharmacol., «(3):209-17, 1979.
33. Struck, R. F., Alberts, D. S., Home, K., Phillips, J. G., Peng, Y-M., andRoe, D. J., Plasma pharmacokinetics of cyclophosphamide and its cytotoxicmetabolites after intravenous versus oral administration in a randomizedcrossover trial. Cancer Res., 47: 2723-2726, 1987.
34. Norpoth, K. Studies on the metabolism of isophospnamide (NSC-109724)in man. Cancer Treat. Rep., 60:437-443, 1976.
35. Goren, M. P., Wright, R. K., Pratt, C. B., and Pell, F. E. Dechlorethylationof ifosfamide and neurotoxicity. Lancet, 2: 1219-1220, 1986.
36. Mouridsen, H. T., Witten, J., Frederickson, P. L., and Hulsback, I. Studieson the correlation between rate of biotransformation and haematologicaltoxicity of cyclophosphamide (Letter). Acta Pharmacol. Toxicol. (Copenh.),43(4): 328-330, 1978.
757
on April 23, 2018. © 1989 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1989;49:753-757. Cancer Res M. J. Lind, J. M. Margison, T. Cerny, et al. Bronchogenic CarcinomaFractionated Intravenous and Oral Ifosfamide in Patients with Comparative Pharmacokinetics and Alkylating Activity of
Updated version
http://cancerres.aacrjournals.org/content/49/3/753
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/49/3/753To request permission to re-use all or part of this article, use this link
on April 23, 2018. © 1989 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from