Comparative Effectiveness Research in the United States: a ...Secure Site · ulcer disease and...
1
For more information touch the symbol. An interactive version of this poster is being presented at the ISMPP meeting. Background • Comparative effectiveness research (CER) is designed to inform health care decisions by providing evidence on the effectiveness, benefits, and harms of treatment options from research studies that compare drugs, medical devices, tests, surgeries, or ways to deliver health care. 1 • Government-sponsored CER is currently established in European countries such as England, Denmark, Germany, and France, and is used to inform choices between treatment options and to make reimbursement decisions. • In the United States, CER has been gaining prominence as a result of $1.1 billion allocated to CER research under the American Recovery and Reinvestment Act of 2009. Several government agencies conduct CER, notably The Agency for Healthcare Research and Quality (AHRQ). 2 • The AHRQ’s CER research is encompassed in the general Effective Health Care Program, which was initiated in 2005. 3 Objectives • To describe the process of CER generation in terms of public access to developmental stages and final outputs. • To quantify CER reports by general descriptive therapeutic areas and by AHRQ described areas of interest. • To qualitatively analyze the information provided in the reports for specific recommendations about drug choice with regard to efficacy or cost. Research Design and Methods • A search was conducted using the AHRQ search engine for all CER documents generated from 2005 to January 12, 2011. The following parameters were used to search: — All conditions — All research reviews and reports — All stages of development (In Progress, Draft, Final) • Reports specifically titled “comparative effectiveness” were assessed and classified into broad therapeutic areas. These areas were then reorganized to match the 14 AHRQ priority conditions. • CER report executive summaries from the most common therapy area were qualitatively analyzed to determine: — General sources of information — Types of analyses — Specific drug/treatment recommendations with cost implications Results Generation of Research Review Reports (Figure 1) Quantitative Analysis of Research Review Reports • Of 115 total proposals, drafts, and reports, 67 specifically contained the term “Comparative Effectiveness” in the title. The distribution of documents according to stage of development is presented in Figure 2. • For broad classification, the areas were subdivided, and the most common therapy areas were determined to be CVD (14 CER documents, including protocols, drafts, and reports), hematology/ oncology (8), psychiatry (8), rheumatology (6), and metabolics (5). • The reports were additionally classified by AHRQ priority conditions (Figure 3). Qualitative Analysis of Cardiovascular Research Review Reports • Of the 14 cardiovascular documents, 7 were reports (Table 1). • Data used to generate reports were obtained from a variety of sources, including Medline, Cochrane Central Register of Controlled Trials, and scientific information packets submitted by the pharmaceutical manufacturers. • While specific cost was not mentioned in the reports, efficacy summaries presented results with cost implications such as: — Evidence against the add-on use of a medical device 3 • “Studies that compared stent placement to no stent placement found no difference in outcomes” – Report number 5 — Similar efficacy of 2 drug classes where one drug class has more generic options 4 • “ACEIs and ARBs appear to have similar long-term effects on blood pressure among individuals with essential hypertension” – Report number 10 • The process of CER review generation allows for the input of various stakeholders. • Of the top 14 priority conditions identified by the AHRQ, cardiovascular disease is the area that is most commonly researched and reported. • CER executive summaries and full reports present a descriptive summary of the current literature landscape (including potential data gaps) and comprehensive data summaries for many interventions and therapeutic classes. • CER reports present arguments regarding efficacy and safety that could support reimbursement decisions that are adverse to the interests of branded pharmaceuticals. • The current number of protocols and drafts in progress suggests that the CER landscape will change dramatically in the coming years. Survey 1. Do you feel that the increasing role of CER will impact the way you plan publications? 2. Has CER already changed the way you design and report studies? 3. If CER has impacted your publication planning, have you employed the following strategies: a. Earlier timing of head-to-head studies? b. Reactively addressed this by defensive publications? 4. Have you been involved in formulating a response during formal comment periods? References 1. http://effectivehealthcare.ahrq.gov. Accessed January 12, 2010. 2. Sox HC. Ann Intern Med. 2010;153:469-472. 3. Balk E, et al. Comparative Effectiveness of Management Strategies for Renal Artery Stenosis. Comparative Effectiveness Review No. 5. (Prepared by Tufts-New England Medical Center Evidence-based Practice Center under Contract No. 290-02-0022.) Rockville, MD: Agency for Healthcare Research and Quality. October 2006. 4. Matchar DB, et al. Comparative Effectiveness of Angiotensin-Converting Enzyme Inhibitors (ACEIs) and Angiotensin II Receptor Antagonists (ARBs) for Treating Essential Hypertension. Comparative Effectiveness Review No. 10. (Prepared by Duke Evidence-based Practice Center under Contract No. 290-02-0025.) Rockville, MD: Agency for Healthcare Research and Quality. November 2007. William Watkins, a Alexandra Silveira, a Christopher Bailey, a and Sheelah Smith b a PPSI Inc., a PAREXEL company, Stamford, CT, USA b PPSI Inc., a PAREXEL company, Worthing, UK OBJECTIVE: Government-sponsored comparative effectiveness research (CER) is established in Europe and is gaining prominence in the United States, raising concern that CER might be used to restrict access to branded products. We analyzed CER summaries from the US Agency for Healthcare Research and Quality (AHRQ) to determine therapy areas of interest and implications for publication planning. METHODS: CER summaries in the AHRQ database were categorized by therapeutic area. Summaries in the most frequent category were qualitatively analyzed. RESULTS: 67 CER documents, including reports, protocols, and drafts, were available. The most common therapy areas were cardiovascular disease (CVD) (14 CERs, including drafts/protocols), hematology/oncology (8), psychiatry (8), rheumatology (6), and metabolics (5). The reports utilized publicly available data, emphasizing primary literature obtained through PubMed. Where available, data were meta-analyzed. The 7 final CVD reports were analyzed qualitatively. An illustrative example compared ACEIs (an antihypertensive class with many generic options) with ARBs (an antihypertensive class with many branded members), concluding no difference in efficacy. A difference in adverse events of cough in favor of ARBs was acknowledged; relative cost was not explicitly mentioned. CONCLUSIONS: AHRQ reports include comprehensive data summaries for many interventions and therapeutic classes. Although subtly conveyed, CER reports include arguments that support restricted access to newer or branded products. Publication planners should be aware of CERs in development and consider strategies to clarify data and provide context. ABSTRACT Comparative Effectiveness Research in the United States: Implications for Publication Planners CONCLUSIONS Figure 1: Developmental stages of the AHRQ CER reviews Research topic suggestions are open to the public. The program prioritizes recommended research questions based on a pre-established set of criteria. Depending on the available evidence, the topic focus is developed into either a research review or new research. The research is conducted by an Evidence-based Practice Center (EPC). During development, the public can comment at various stages to give input. Additionally, industry stakeholders and others can submit scientific information packets with detailed study-specific information. The final research report is available online and summarized into various guides for different audiences. Adapted from AHRQ Web site. 1 Figure 2: Distribution of CER documents by developmental stage The majority of documents were in the protocol/draft stages. Drafts 28% Reports 30% Protocols 42% Figure 3: Distribution of CER documents by therapy area The top 5 areas are depicted in the graph. The 14 AHRQ priority conditions are diabetes mellitus; arthritis and nontraumatic joint disorders; cancer; depression and other mental health disorders; cardiovascular disease, including stroke and hypertension; dementia, including Alzheimer’s disease; developmental delays, attention deficit hyperactivity disorder and autism; functional limitations and disabilities; infectious diseases, including HIV/AIDS; obesity; peptic ulcer disease and dyspepsia; pregnancy, including preterm birth; pulmonary disease/asthma; and substance abuse. 1 Depression and other mental health disorders 12% Arthritis and nontraumatic joint disorders 15% Cancer 12% Diabetes mellitus 6% Other 34% Cardiovascular disease 21% NO NO NO NO NO YES YES YES YES YES Research Question Submission New Research or Research Review Research Review Draft Report (posted online) Research Abstract or Key Questions (posted online) Final Report Suggestions open to public Available for public comment Available for public comment Summary Guides of Research Review Are Generated for Various Audiences Available for SIP submission PAREXEL International +1 781 487 9900 www.PAREXEL.com Report Title Comparative Effectiveness of Management Strategies for Renal Artery Stenosis Comparative Effectiveness of Management Strategies for Renal Artery Stenosis: 2007 Update Comparative Effectiveness of Percutaneous Coronary Interventions and Coronary Artery Bypass Grafting for Coronary Artery Disease Comparative Effectiveness of Angiotensin- Converting Enzyme Inhibitors (ACEIs) and Angiotensin II Receptor Antagonists (ARBs) for Treating Essential Hypertension Comparative Effectiveness of Radiofrequency Catheter Ablation for Atrial Fibrillation Comparative Effectiveness of Lipid-Modifying Agents Comparative Effectiveness of Angiotensin Converting Enzyme Inhibitors or Angiotensin II Receptor Blockers Added to Standard Medical Therapy for Treating Stable Ischemic Heart Disease Report Number 5 5-Update 9 10 15 16 18 Table 1: Cardiovascular executive summaries available for analysis
Transcript of Comparative Effectiveness Research in the United States: a ...Secure Site · ulcer disease and...

For more information touch the symbol.
An interactive version of this poster is being presented at the ISMPP meeting.
Background
• Comparative effectiveness research (CER) is designed to inform health care decisions by providing evidence on the effectiveness, benefits, and harms of treatment options from research studies that compare drugs, medical devices, tests, surgeries, or ways to deliver health care.1
• Government-sponsored CER is currently established in European countries such as England, Denmark, Germany, and France, and is used to inform choices between treatment options and to make reimbursement decisions.
• In the United States, CER has been gaining prominence as a result of $1.1 billion allocated to CER research under the American Recovery and Reinvestment Act of 2009. Several government agencies conduct CER, notably The Agency for Healthcare Research and Quality (AHRQ).2
• The AHRQ’s CER research is encompassed in the general Effective Health Care Program, which was initiated in 2005.3
Objectives
• To describe the process of CER generation in terms of public access to developmental stages and final outputs.
• To quantify CER reports by general descriptive therapeutic areas and by AHRQ described areas of interest.
• To qualitatively analyze the information provided in the reports for specific recommendations about drug choice with regard to efficacy or cost.
Research Design and Methods
• A search was conducted using the AHRQ search engine for all CER documents generated from 2005 to January 12, 2011. The following parameters were used to search:
— All conditions
— All research reviews and reports
— All stages of development (In Progress, Draft, Final)
• Reports specifically titled “comparative effectiveness” were assessed and classified into broad therapeutic areas. These areas were then reorganized to match the 14 AHRQ priority conditions.
• CER report executive summaries from the most common therapy area were qualitatively analyzed to determine:
— General sources of information
— Types of analyses
— Specific drug/treatment recommendations with cost implications
Results
Generation of Research Review Reports (Figure 1)
Quantitative Analysis of Research Review Reports
• Of 115 total proposals, drafts, and reports, 67 specifically contained the term “Comparative Effectiveness” in the title. The distribution of documents according to stage of development is presented in Figure 2.
• For broad classification, the areas were subdivided, and the most common therapy areas were determined to be CVD (14 CER documents, including protocols, drafts, and reports), hematology/oncology (8), psychiatry (8), rheumatology (6), and metabolics (5).
• The reports were additionally classified by AHRQ priority conditions (Figure 3).
Qualitative Analysis of Cardiovascular Research Review Reports
• Of the 14 cardiovascular documents, 7 were reports (Table 1).
• Data used to generate reports were obtained from a variety of sources, including Medline, Cochrane Central Register of Controlled Trials, and scientific information packets submitted by the pharmaceutical manufacturers.
• While specific cost was not mentioned in the reports, efficacy summaries presented results with cost implications such as:
— Evidence against the add-on use of a medical device3
• “Studies that compared stent placement to no stent placement found no difference in outcomes” – Report number 5
— Similar efficacy of 2 drug classes where one drug class has more generic options4
• “ACEIs and ARBs appear to have similar long-term effects on blood pressure among individuals with essential hypertension” – Report number 10
• The process of CER review generation allows for the input of various stakeholders.
• Of the top 14 priority conditions identified by the AHRQ, cardiovascular disease is the area that is most commonly researched and reported.
• CER executive summaries and full reports present a descriptive summary of the current literature landscape (including potential data gaps) and comprehensive data summaries for many interventions and therapeutic classes.
• CER reports present arguments regarding efficacy and safety that could support reimbursement decisions that are adverse to the interests of branded pharmaceuticals.
• The current number of protocols and drafts in progress suggests that the CER landscape will change dramatically in the coming years.
Survey
1. Do you feel that the increasing role of CER will impact the way you plan publications?
2. Has CER already changed the way you design and report studies?
3. If CER has impacted your publication planning, have you employed the following strategies:
a. Earlier timing of head-to-head studies?
b. Reactively addressed this by defensive publications?
4. Have you been involved in formulating a response during formal comment periods?
References
1. http://effectivehealthcare.ahrq.gov. Accessed January 12, 2010.
2. Sox HC. Ann Intern Med. 2010;153:469-472.
3. Balk E, et al. Comparative Effectiveness of Management Strategies for Renal Artery Stenosis. Comparative Effectiveness Review No. 5. (Prepared by Tufts-New England Medical Center Evidence-based Practice Center under Contract No. 290-02-0022.) Rockville, MD: Agency for Healthcare Research and Quality. October 2006.
4. Matchar DB, et al. Comparative Effectiveness of Angiotensin-Converting Enzyme Inhibitors (ACEIs) and Angiotensin II Receptor Antagonists (ARBs) for Treating Essential Hypertension. Comparative Effectiveness Review No. 10. (Prepared by Duke Evidence-based Practice Center under Contract No. 290-02-0025.) Rockville, MD: Agency for Healthcare Research and Quality. November 2007.
William Watkins,a Alexandra Silveira,a Christopher Bailey,a and Sheelah Smithb
aPPSI Inc., a PAREXEL company, Stamford, CT, USAbPPSI Inc., a PAREXEL company, Worthing, UK
OBjective: Government-sponsored comparative effectiveness research (CER) is established in Europe and is gaining prominence in the United States, raising concern that CER might be used to restrict access to branded products. We analyzed CER summaries from the US Agency for Healthcare Research and Quality (AHRQ) to determine therapy areas of interest and implications for publication planning. MethODS: CER summaries in the AHRQ database were categorized by therapeutic area. Summaries in the most frequent category were qualitatively analyzed. ReSultS: 67 CER documents, including reports, protocols, and drafts, were available. The most common therapy areas were cardiovascular disease (CVD) (14 CERs, including drafts/protocols), hematology/oncology (8), psychiatry (8), rheumatology (6), and metabolics (5). The reports utilized publicly available data, emphasizing primary literature obtained through PubMed. Where available, data were meta-analyzed. The 7 final CVD reports were analyzed qualitatively. An illustrative example compared ACEIs (an antihypertensive class with many generic options) with ARBs (an antihypertensive class with many branded members), concluding no difference in efficacy. A difference in adverse events of cough in favor of ARBs was acknowledged; relative cost was not explicitly mentioned. cOncluSiOnS: AHRQ reports include comprehensive data summaries for many interventions and therapeutic classes. Although subtly conveyed, CER reports include arguments that support restricted access to newer or branded products. Publication planners should be aware of CERs in development and consider strategies to clarify data and provide context.
AB
StR
Ac
t
Comparative Effectiveness Research in the United States: Implications for Publication Planners
cO
nc
luS
iOn
S
Figure 1: Developmental stages of the AHRQ CER reviews Research topic suggestions are open to the public. The program prioritizes recommended research questions based on a pre-established set of criteria. Depending on the available evidence, the topic focus is developed into either a research review or new research. The research is conducted by an Evidence-based Practice Center (EPC). During development, the public can comment at various stages to give input. Additionally, industry stakeholders and others can submit scientific information packets with detailed study-specific information. The final research report is available online and summarized into various guides for different audiences. Adapted from AHRQ Web site.1
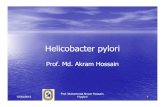
Figure 2: Distribution of CER documents by developmental stage The majority of documents were in the protocol/draft stages.
Drafts28%
Reports30%
Protocols42%
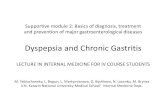
Figure 3: Distribution of CER documents by therapy area The top 5 areas are depicted in the graph. The 14 AHRQ priority conditions are diabetes mellitus; arthritis and nontraumatic joint disorders; cancer; depression and other mental health disorders; cardiovascular disease, including stroke and hypertension; dementia, including Alzheimer’s disease; developmental delays, attention deficit hyperactivity disorder and autism; functional limitations and disabilities; infectious diseases, including HIV/AIDS; obesity; peptic ulcer disease and dyspepsia; pregnancy, including preterm birth; pulmonary disease/asthma; and substance abuse.1
Depression and othermental health disorders
12%
Arthritis and nontraumaticjoint disorders
15%
Cancer12%
Diabetes mellitus6%
Other34%
Cardiovasculardisease
21%
NO
NO
NO
NO
NO
YES
YES
YES
YES
YES
ResearchQuestion
Submission
New Researchor Research
Review
ResearchReview Draft
Report(posted online)
ResearchAbstractor Key
Questions(posted online)
Final Report
Suggestionsopen to public
Available forpublic comment
Available forpublic comment
SummaryGuides ofResearchReview AreGenerated forVariousAudiences
Available for SIP submission
PAReXel international+1 781 487 9900
www.PAREXEL.com
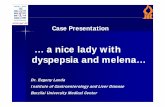
Report Title
Comparative Effectiveness of Management Strategies for Renal Artery Stenosis
Comparative Effectiveness of Management Strategies for Renal Artery Stenosis: 2007 Update
Comparative Effectiveness of Percutaneous Coronary Interventions and Coronary Artery Bypass Grafting for Coronary Artery Disease
Comparative Effectiveness of Angiotensin- Converting Enzyme Inhibitors (ACEIs) and Angiotensin II Receptor Antagonists (ARBs) for Treating Essential Hypertension
Comparative Effectiveness of Radiofrequency Catheter Ablation for Atrial Fibrillation
Comparative Effectiveness of Lipid-Modifying Agents
Comparative Effectiveness of Angiotensin Converting Enzyme Inhibitors or Angiotensin II Receptor Blockers Added to Standard Medical Therapy for Treating Stable Ischemic Heart Disease
Report Number
5
5-Update
9
10
15
16
18
Table 1: Cardiovascular executive summaries available for analysis