Comparative analysis of different transection techniques ... · Original research Comparative...
49
MINUTES SAT-Rdmp, Common Vision Workshop, Brussels 28 Sept 2011 Minutes-CVPanelDiscussion-Brussels-28Sept2011-V1-111227-clean.doc 1 / 49 MINUTES Small Air Transport – Roadmap (SAT-Rdmp), CSA-SA, FP7 Project, What: MINUTES of the Panel Discussion “Three Pivotal Questions” held on workshop “Common Vision for Small Aircraft Transport Mode”, organized in the framework of SAT-Rdmp Project Who: Moderator: Krzysztof PIWEK (ILOT) Panelists: Adriaan de GRAAFF (Ad Cuenta) Stefaan GHIJS (Aeolus) Tony HENLEY (THL) Marcello AMATO (CIRA) Jaroslav RŮŽIČKA (Evektor, EGAMA) Zbigniew MĄCZKA (Polish Civil Aviation Office) Jozsef ROHACS (BUTE) Pablo PEREZ-ILLANA (EC) When: 28 Sept 2011 Where: Regione Campania – Brussels Office, Avenue De Cortenbergh 60, Why: Discuss with representatives of the SAT Community, EC, Regulators, Manufactures, Operators about the elements of the SAT Vision in order to build up a “Common” shared view of the future Small Aircraft Transport System as a component of the European Integrated Transport.
Transcript of Comparative analysis of different transection techniques ... · Original research Comparative...

lable at ScienceDirect
International Journal of Surgery 11 (2013) 826e833
ORIGINAL RESEARCH
Contents lists avai
International Journal of Surgery
journal homepage: www.journal-surgery.net
Original research
Comparative analysis of different transection techniques in minorand major hepatic resections: A prospective cohort study
Carina Riediger a,*,d, Michael W. Mueller a,b,d, Florian Geismann a, Andreas Lehmann c,Tibor Schuster c, Christoph W. Michalski a, Klaus Kuhn c, Helmut Friess a
aDepartment of Surgery, Technische Universität München, Ismaninger Str. 22, 81675 Munich, GermanybDepartment of Surgery, Klinikum Bad Canstatt, Prießnitzweg 24, 70374 Stuttgart, Germanyc Institute of Medical Statistics and Epidemiology, Technische Universität München, Ismaninger Str. 22, 81675 Munich, Germany
a r t i c l e i n f o
Article history:Received 30 June 2013Received in revised form1 August 2013Accepted 20 August 2013Available online 28 August 2013
Keywords:Liver transection techniquesStaplerWater-jetElectrocauteryHepatectomy
* Corresponding author. Current address: DepartmVascular Surgery, University Hospital Carl Gustav CDresden, Fetscherstrasse 74, 01307 Dresden, Germafax: þ49 351 4587240.
E-mail address: Carina.Riediger@uniklinikum-dresd These authors contributed equally.
1743-9191/$ e see front matter � 2013 Surgical Assohttp://dx.doi.org/10.1016/j.ijsu.2013.08.010
a b s t r a c t
Background: In liver surgery different transection techniques are available without clear evidenceregarding indication and advantage for each technique.The aim of this study was to identify the most superior liver transection technique between the differenttechniques (stapler, water-jet and electrocautery). Comparative analyses were performed for minor andmajor hepatectomies.Methods: In a single-center study, all liver resections performed between July 2007 and July 2012 wereprospectively recorded and analysed.Results: 366 liver resections were included according to predefined eligibility criteria.No clear benefit for one particular technique in minor or major hepatectomy could be shown. Cost-effectiveness analysis revealed disadvantages for stapler-hepatectomies. However, minor hepatec-tomies were performed with significantly lower morbidity (p < 0.001), lower operating time (p ¼ 0.001),fewer need of transfusion (p < 0.0001) and shorter ICU stay (p ¼ 0.001) than major hepatectomies.Conclusions: If possible, minor hepatectomies should be chosen. Competing techniques, selected ac-cording to surgeon’s preference, revealed no significant differences in primary outcome measures.
� 2013 Surgical Associates Ltd. Published by Elsevier Ltd. All rights reserved.
1. Introduction
Liver surgery is still associated with considerable morbidity.Prior to the introduction of modern transection techniques, mor-tality rates, mostly as a result of bleeding following liver resections,were high and frequent.1 The reduction of intraoperative blood-losshas not only been shown to influence short term outcomes, but alsolong-term results.2 It has been reported that disease-free survivalafter liver resection for malignancies is associated with the numberof perioperative blood transfusions.3 Biliary complications are thesecond most common cause of morbidity, with a 5e15% rate ofbiliary leakage4 and are, interestingly, related to the number ofblood transfusions.3 To reduce the risk of complications, surgicaltechniques for liver transection were improved.5 While liver
ent of General, Thoracic andarus, Technische Universitätny. Tel.: þ49 351 45818353;
den.de (C. Riediger).
ciates Ltd. Published by Elsevier Lt
transection had formerly been carried out with a scalpel or byfinger fracture technique, more advanced methods are currentlyavailable.6e8
Themost important surgical techniques generally used today forliver resection are the finger fracture or crush/clamp technique, thecavitron ultrasonic surgical aspirator (CUSA, Cavitron, Inc. Stanford,Conn., USA), the water-jet, the stapler and monopolar or bipolarelectrocautery. Another sophisticated method, not yet routinelyused, is radiofrequency-assisted liver resection (HABIB, Unomed,Switzerland).9e18 Recently, different sealing devices such as ultra-sound scissors and harmonic scalpels (Ultracision, Ethicon, Nor-derstedt, Germany), as well as the electrothermal bipolar vesselsealing system (EBVS) (LigaSure, Covidien, Germany) have gainedmore importance in liver surgery.19e23
Due to improvements in technology, morbidity and mortalityrates in liver resection have decreased dramatically over the lasttwo decades.24 Perioperative mortality rates are reported with lessthan 5% and morbidity rates vary between 20 and 40%.25e27
Even though there are many different techniques available, theoptimal transection technique is still missing. A number of studieshave compared various methods, with differing results. However,
d. All rights reserved.

C. Riediger et al. / International Journal of Surgery 11 (2013) 826e833 827
ORIGINAL RESEARCH
evidence on which transection technique is in favour in regard tominor or major liver resection is not available.28e30
In this study, a comprehensive comparative single-center anal-ysis of 366 liver resections was performed to identify the superiorliver transection technique for minor and major hepatectomies.Comparative analyses between stapler, water-jet and electrocau-tery for minor hepatectomies and between stapler and water-jetdissection in major hepatectomies were performed.
2. Methods
2.1. Patients
In this single-center study, all patients’ data of patients receiving a liver resec-tion were prospectively recorded between July 2007 and July 2012 in an electronicdatabase and analysed. Patient characteristics, pre- and postoperative treatment,laboratory values, operative procedures, intra- and perioperative data, complica-tions, hospital stay, etc. were prospectively recorded in the database. Analysis ofsurgical procedures included anatomical segmentectomies, non-anatomical
Cohort 1 (n=111)
Major Liver resections
Included (Ju
July 2012
Analyzed (
- Descriptive st- Mortality, mor
Excluded for Analysis
(n=4)
- CUSA (n=2)
- HABIB (n=1)
- Others (n=1)
Cohort 1 (n=107)
Major liver resections
Stapler n=81
vs
Waterjet n=26
Analyzed (
- Electrocau
- Stapler (n=
- Waterjet (n
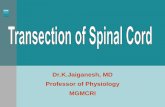
Fig. 1. Overview showing the formation of groups for further an
segmentectomies, right and extended right hemihepatectomies, as well as left andextended left hemihepatectomies.
For preoperative imaging and surgical planning, at least one computed scanwasperformed. Patients who received liver resections during another operation such ascolorectal resection, gastrectomy, esophagectomy or pancreatectomy, wereexcluded from the analysis. Smallest atypical liver resections in terms of resectionalbiopsies during laparotomy or diagnostic laparoscopy were mostly classified as bi-opsies and were also excluded.
In a first assessment the whole cohort was analysed in regard to major andminor liver resection. In a second evaluation the surgical techniques usedmost werethen compared for minor and major liver resections. A detailed overview is given inFig. 1.
2.2. Liver transection techniques/surgeons
Transection techniques included in this analysis were stapler transection (GIA�Autosuture� Universal stapler, Covidien, Germany), water-jet (Hydro-Jet�, Erbe,Tuebingen, Germany) and electrocautery for minor liver resections. For major liverresections stapler transection technique (GIA� Autosuture� Universal stapler,Covidien, Germany) and water-jet (Hydro-Jet�, Erbe, Tuebingen, Germany) were
ly 2007-
) and
n= 366)
atistics;bidity
Cohort 2 (n=255)
Minor liver resections
Excluded for Analysis
(n=82)
- CUSA (n=1)- HABIB (n=15)- Others/combined
methods (n=66)
Cohort 2 (n=165)
Minor liver
resections
Electrocautery n=58
vs
Stapler n=72
vs
Waterjet n=35
n=272)
tery (n=58)
153)
=61)
n=8 patients excluded due to missing technical information
alyses out of 366 liver resections included in this analysis.

Table 1Patients’ characteristics of n ¼ 366 patients as well as for minor and major liverresections.
Whole cohortn ¼ 366
Major hepaticresectionsn ¼ 111
Minor hepaticresections n ¼ 255
MedianAge (years) 64 (range 17e87) 64 (range 17e87) 65 (range 20e86)
GenderMale 210 (57.4%) 65 (58.6%) 145 (56.9%)Female 156 (42.6%) 46 (41.4%) 110 (43.1%)
ASA ASA I: 30 (8.2%) ASA I: 8 (7.2%) ASA I: 22 (8.6%)ASA II: 213 (58.2%) ASA II: 70 (63.1%) ASA II: 143 (56.1%)ASA III: 116 (31.7%) ASA III: 33 (29.7%) ASA III: 83 (32.5%)ASA IV: 6 (1.6%) ASA IV: 0 ASA IV: 6 (2.4%)ASA V: 1 (0.3%) ASA V: 0 ASAV: 1 (0.4%)
Hepatitis B 11 (3%) 5 (4.5%) 6 (2.4%)Hepatitis C 17 (4.6%) 3 (2.7%) 14 (5.5%)Liver cirrhosis 54 (14.8%) 13 (11.7%) 41 (16.2%)MELD score Median 7
(range 6e23)Median 7(range 6e8)
Median 7(range 6e23)
Pre-treatment 124 (33.9%) 47 (42.3%) 77 (30.4%)CTX 97 (26.5%) 34 (30.6%) 63 (24.9%)RFA 8 (2.2%) 2 (1.8%) 6 (2.4%)TACE 25 (6.8%) 17 (15.3%) 8 (3.2%)Radiation 15 (4.1%) 4 (3.6%) 11 (4.3%)Preliminary
liverresection
76 (20.8%) 16 (14.4%) 59 (23.3%)
ASA ¼ American Society of Anesthesiologists; MELD ¼ model of endstage liverdisease; CTX ¼ chemotherapy; RFA ¼ radiofrequency ablation; TACE ¼ transarterialchemoembolization.
Table 2Indication for liver resections of n¼ 366 patients as well as for minor andmajor liverresections.
Whole cohortn ¼ 366
Major hepaticresectionsn ¼ 111
Minor hepaticresectionsn ¼ 255
Malignancies 287 (78.4%) 96 (86.5%) 191 (74.9%)HCC 67 (18.3%) 23 (20.7%) 44 (17.3%)CCC (incl. GBC) 43 (11.7%) 24 (21.6%) 19 (7.5%)Metastases 167 (45.6%) 43 (38.7%) 124 (48.6%)Others 10 (2.7%) 6 (5.4%) 4 (1.6%)
Benign tumors 57 (15.6%) 12 (10.8%) 45 (17.6%)Cysts 25 (6.8%) 1 (0.9%) 24 (9.4%)FNH 8 (2.2%) 0 8 (3.1%)Adenoma 7 (1.9%) 3 (2.7%) 4 (1.6%)Haemangioma 5 (1.4%) 1 (0.9%) 4 (1.6%)Others 12 (3.3%) 7 (6.3%) 5 (2%)
Liver injury 22 (6%) 3 (2.7%) 19 (7.5%)
HCC ¼ hepatocellular carcinoma; CCC ¼ cholangiocarcinoma; GBC ¼ gallbladdercarcinoma; FNH ¼ focal nodular hyperplasia.
C. Riediger et al. / International Journal of Surgery 11 (2013) 826e833828
ORIGINAL RESEARCH
included. The transection technique was chosen along surgeon’s preference. Alloperations included in this analysis were performed by one of 6 experienced liversurgeons. Analyses of the six surgeons regarding outcome parameters revealed nosignificant differences (data not shown). Therefore, surgeons could be excluded asfactor affecting the outcome of liver transections in this study.
2.3. Cost calculation
Material costs for the stapler used in our hospital for stapler hepatectomies werecalculated with 108 Euros/stapler (GIA� Autosuture� Universal stapler, Covidien,Germany) and 150 Euros/roticulator (Universal load unit, 60 mm/2.5 mm, Covidien,Germany). Material costs for the water-jet (Hydro-Jet�, Erbe, Tuebingen, Germany)in our hospital were calculated with 100 Euros/operation. Electrocautery did notinduce additional costs.
The total cost for one minute of operation time in our hospital was calculated at13 Euros/minute.
2.4. Statistical analyses
Statistical analysis was performed using IBM SPSS Statistics software, version 20(SPSS Inc., Chicago, IL, USA). Data are described by means � standard deviation or,where appropriate, by median values and interquartile range [IQR]. Explorativegroup comparisons were conducted using non-parametric approaches i.e. theKruskaleWallis test and ManneWhitney U test, as indicated by the number ofgroups to be compared. All statistical tests were conducted two-sided, and a p-value<0.05 was considered to indicate statistical power. In order to sustain maximumstatistical power, no correction of p-values in the course of multiple testing wasperformed. However, results of all formal comparisons are thoroughly reported sothat an informal adjustment of p-values may be performed.
3. Results
Following the exclusion process, n ¼ 366 liver resections per-formed between July 2007 and July 2012 were included in ouranalysis.
3.1. Overall cohort and comparison major vs. minor liver resections
1. Patient characteristics
Patients’ general condition and co-morbidities were reflected inthe ASA (American Society of Anesthesiologists) score: most pa-tients were classified as ASA II (56.8%) or ASA III (30.9%). Patientspresenting with liver cirrhosis n ¼ 54 (14.8%) showed a medianMELD (model of endstage liver disease) score of 7, ranging from 6 to23. Detailed patient characteristics are shown in Table 1.
2. Definition of the extent of liver resection
Major hepatic resections were defined as liver resection of atleast �3 anatomical segments, minor resections as resection of lessthan3 anatomical segments and all atypical resections. In the cohortanalysed, we recorded n¼ 111major resections (30.3%) and n¼ 255minor resections (69.7%). In more detail: n ¼ 77 right or extendedright hemihepatectomies (21%) and n ¼ 27 left or extended lefthemihepatectomies (7.4%) were performed. An anatomical seg-mentectomy was performed in 89 cases (24.4%) whereas non-anatomical resections were performed in 173 cases (47%).
3. Indications for liver resections
287 (78.4%) patients were operated for malignant and n ¼ 57patients (15.6%) for benign diseases and 22 patients (6%) requiredliver surgery for liver trauma (Table 2).
Separate analysis revealed no significantly higher need of intra-or postoperative transfusion in patients receiving liver transectionfor trauma. Noteworthy, that only patients who received primaryliver resection were included in this analysis. Patients treated byliver packing for acute, severe bleeding without resection of pa-renchyma were not included in this analysis.
4. Surgical techniques
Liver transectionwas performed by the use of a vascular stapler,monopolar/bipolar electrocautery, water-jet, CUSA andradiofrequency-assisted liver resections (HABIB). An argon beamcoagulator was available for each operation and used additionallyin most operations (n ¼ 326/366; 89%). Major liver resections werealmost exclusively performed using a stapler or water-jet. In n ¼ 67cases (‘Others’), liver resections were performed by the use of atleast two combined methods (stapler þwater-jet, etc.); those werenot included in the analysis (Fig. 1/Table 3).
5. Intraoperative management
The median operating time of the overall cohort was 200 min,with a range of 24e800 min. The median operating time for majorliver resections was significantly higher than that of minor re-sections (p ¼ 0.001) (Table 4).

Table 3Different liver transection techniques used in major and minor hepatic resections.
Whole cohortn ¼ 366
Major hepaticresectionsn ¼ 111
Minor hepaticresectionsn ¼ 255
Transection techniqueStapler 153 (41.8%) 81 (73%) 72 (28.2%)Water-jet 61 (16.7%) 26 (23.4%) 35 (13.7%)Electrocautery 58 (15.8%) 0 58 (22.8%)HABIB 16 (4.4%) 1 (0.9%) 15 (5.9%)CUSA 3 (0.8%) 2 (1.8%) 1 (0.4%)Other 75 (20.5%) 1 (0.9%) 74 (29%)
HABIB ¼ radiofrequency-assisted liver resections; CUSA ¼ cavitron ultrasonic sur-gical aspirator.
C. Riediger et al. / International Journal of Surgery 11 (2013) 826e833 829
ORIGINAL RESEARCH
6. Postoperative management and complications.
Postoperative data is shown in Table 4. Significant differencesbetween minor and major hepatic resections were recordedregarding the intensive-care unit (ICU) stay, re-operation, mortality(between day 1 and 42) and the intra-/post-operative need fortransfusion of red blood cells (RBC) and fresh frozen plasma (FFP).Postoperative complications occurred in 120 cases, resulting in anoverall morbidity of 33%. Surgical complications were recorded in79 cases (21.6%), whereas medical complications occurred in 74cases (20.2%). The total rate of morbidity, as well as the frequency ofsurgical complications, showed a statistically significant contrastbetween minor and major hepatectomies, whereas the medicalcomplications did not reveal any significant difference betweenboth groups. In the overall cohort, the most common surgicalcomplications were wound infection (7.1%), liver or intra-abdominal abscess (6.9%) and biliary complications such as fistulaor bilioma (6.9%), whereas non-surgical complications were mainlypulmonary complications (8.5%), cholangitis (2.7%), renal (2.7%)and cardiac complications (2.7%).
3.2. Comparison of different transection techniques
Major liver resections were predominantly performed by theuse of stapler and water-jet techniques, whereas minor resectionswere largely carried out using monopolar/bipolar electrocautery,stapler and water-jet. Comparative analyses of the different tran-section techniques were performed for stapler vs. water-jet vs.electrocautery for minor resections (n ¼ 165) (Table 5), and for
Table 4Intra- and postoperative parameters for the whole cohort and comparison between miPPSB ¼ prothrombin complex concentrate; IE ¼ international units.
Whole cohort n ¼ 366 Major hepa
Operating time (minutes) Median 200 (range 24e800) Median 27Pringle manoeuvre 67 (18.3%) 34 (30.6%)Intensive care unit (days) Median 1 (range 0e60) Median 2 (Mechanical ventilation (days) Median 0 (range 0e29) Median 0 (Morbidity 120 (33%) 55 (49.5%)Surgical complications 79 (21.6%) 36 (32.4%)Medical complications 74 (20.2%) 30 (27.0%)Re-operation 27 (7.4%) 12 (10.8%)In-hospital mortality 15 (4.1%) 8 (7.2%)IntraoperativeRBC Median 0 (range 0e69) Median 1 (FFP Median 0 (range 0e98) Median 4 (PPSB Median 0 (range 0-18600IE) Median 0 (
PostoperativeRBC Median 0 (range 0e14) Median 0 (FFP Median 0 (range 0e56) Median 0 (PPSB Median 0 (range 0e5000 IE) Median 0 (
stapler vs. water-jet for major hepatic resections (n¼ 107) (Table 6).Liver resections using CUSA (n ¼ 3), and HABIB (n ¼ 16) wereexcluded from this comparative analysis due to the small number ofcases (Fig. 1).
1. Minor liver resections- electrocautery vs. stapler vs. water-jet
Statistical analyses of our data revealed no significant difference,other than the use of intraoperative Pringle manoeuvre, betweenthe different resection groups. However, some tendencies wereseen: the electrocautery group included more patients sufferingfrom liver cirrhosis (20.7%) compared to the stapler (12.5%) andwater-jet groups (14.3%) (Table 5a). Intra- and postoperative data(Table 5b) showed longer operating times for the water-jet group(median 219 min), than in the electrocautery (median 180 min) orstapler group (median 162.5 min). The mortality rate was lower inthe electrocautery group (0) than in the stapler 2/72 (2.8%) orwater-jet groups 1/35 (2.9%), whereas re-operation was more oftennecessary in the stapler group (6.9%) than in electrocautery (3.4%)and water-jet groups (2.9%), respectively. Those observations werenot statistically significant. Though without statistical significance,more complications were observed in the water-jet group. Notably,pulmonary complications (11.4%) including pulmonary embolism,pleural effusion and pneumonia were highest in this group as werethe rate of bilioma and biliary fistula (5.7%). In contrast, cholangitiswas highest in the stapler group (2.8%) as were bleeding compli-cations (4.2%). The highest rate of surgical site infections wasobserved in the electrocautery group (8.6%).
2. Major liver resections- comparison stapler vs. water-jet
Comparative analysis of the stapler (n ¼ 81) and water-jet(n ¼ 26) techniques was performed in n ¼ 107 major liver re-sections. No significant differences were observed between bothresection groups in regard to intra- and postoperative data. As withthe minor resection comparison, some trends were seen (Table 6b).
Patients in the water-jet group showed a higher median age (67years) and a greater percentage of liver cirrhosis (23.1%) comparedto the stapler group (63 years; liver cirrhosis 7.4%), whereas pa-tients in the stapler group showed higher rates of pre-treatment(including chemotherapy, transarterial chemoembolization(TACE), radiation or previous liver surgery) (43.2% vs. 30.8%),respectively (Table 6a). The median operating time was longer inthe water-jet group (298 min) than in the stapler group (median
nor and major liver resections. RBC ¼ red blood cells; FFP ¼ fresh frozen plasma:
tic resections n ¼ 111 Minor hepatic resections n ¼ 255 p-Value
8.5 (range 32e750) Median 188 (range 24e800) 0.00133 (13%) 0.005
range 0e40) Median 1 (range 0e60) 0.001range 0e25) Median 0 (range 0e29) 0.283
65 (25.7%) <0.00143 (17%) 0.00244 (17.3%) 0.07215 (5.9%) 0.1597 (2.8%) 0.099
range 0e12) Median 0 (range 0e69) <0.001range 0e36) Median 0 (range 0e98) <0.001range 0e1200 IE) Median 0 (range 0-18600IE) 0.485
range 0e11) Median 0 (range 0e14) 0.016range 0e56) Median 0 (range 0e18) <0.001range 0e5000 IE) Median 0 (range 0e4200 IE) 0.094

Table 5(a): Patients’ characteristics of the comparative analysis between electrocautery vs. stapler vs. water-jet in n ¼ 165 minor liver resections. (b): Comparative analysis betweenelectrocautery vs. stapler vs. water-jet in n ¼ 165 minor liver resections. Intra- and postoperative parameters.
Electrocautery n ¼ 58 Stapler n ¼ 72 Water-jet n ¼ 35
MedianAge (years) 65 66 65ASA score ASA I:5 (8.6%) ASA I: 8(11.1%) ASA I: 1 (2.9%)
ASA II: 34 (58.7%) ASA II: 42 (58.3%) ASA II: 21 (60%)ASA III: 18 (31%) ASA III: 21 (29.2%) ASA III: 12 (34.2%)ASA IV: 1 (1.7%) ASA IV: 1 (1.4%) ASA IV: 1 (2.9%)
Hepatitis B 2 (3.4%) 2 (2.8%) 1 (2.9%)Hepatitis C 3 (5.2%) 4 (5.6%) 1 (2.9%)Liver cirrhosis 12 (20.7%) 9 (12.5%) 5 (14.3%)MELD score Median 7 (range 7e8) Median 8 (range 6e9) Median 8.5 (range 7e18)Pre-treatment 23 (39.7%) 25 (34.7%) 11 (31.4%)CTX 19 (32.8%) 23 (31.9%) 27 (33.3%)RFA 4 (6.9%) 1 (1.4%) 0TACE 1 (1.7%) 2 (2.8%) 1 (2.9%)Radiation 4 (6.9%) 6 (8.3%) 0Preliminary liver resection 19 (32.8%) 15 (20.8%) 10 (28.6%)
Electrocautery n ¼ 58 Stapler n ¼ 72 Water-jet n ¼ 35 p-Value
Operating time (minutes) Median 180 min (range 24e435) Median 162.50 (range 59e559) Median 219 min (range 95e407) 0.053Pringle manoeuvre 9 (15.5%) 13 (18.1%) 7 (20%) 0.042Intensive care unit (days) Median 1 (range 0e14) Median 0.5 (range 0e31) Median 1 (range 0e16) 0.124Mechanical ventilation (days) Median 0 (range 0e2) Median 0 (range 0e18) Median 0 (range 0e16) 0.198Morbidity 14 (24%) 16 (22%) 7 (20%) 0.897Surgical complications 8 (13.8%) 10 (13.9%) 6 (17.1%) 0.894Non-surgical complications 9 (15.5%) 10 (13.9%) 7 (20%) 0.719Re-operation 2 (3.4%) 5 (6.9%) 1 (2.9%) 0.549In-hospital mortality 0 2 (2.8%) 1 (2.9%) 0.443IntraoperativeRBC Median 0 (range 0e4) Median 0 (range 0e26) Median 0 (range 0e5) 0.729FFP Median 0 (range 0e6) Median 0 (range 0e40) Median 0 (range 0e12) 0.599PPSB Median 0 Median 0 (range 0e5400 IE) Median 0 0.143
PostoperativeRBC Median 0 (range 0e2) Median 0 (range 0e8) Median 0 (range 0e7) 0.747FFP Median 0 (range 0e8) Median 0 (range 0e18) Median 0 (range 0e10) 0.185PPSB Median 0 Median 0 (range 0e1800 IE) Median 0 (range 0e1800 IE) 0.613
ASA ¼ American Society of Anesthesiologists; MELD ¼ model of endstage liver disease; CTX ¼ chemotherapy; RFA ¼ radiofrequency ablation; TACE ¼ transarterial che-moembolization.RBC ¼ red blood cells; FFP ¼ fresh frozen plasma: PPSB ¼ prothrombin complex concentrate; IE ¼ international units.
C. Riediger et al. / International Journal of Surgery 11 (2013) 826e833830
ORIGINAL RESEARCH
267min), however, more transfusions of PPSB and FFPwere neededduring stapler resection and a slightly longer ICU stay was neces-sary. The re-operation rate was slightly higher in the water-jetgroup (7.7% vs. 6.2%), as well as the rate of morbidity (47% vs.54%). In comparison, the mortality rate was higher in the staplergroup (11.1% vs. 7.7%) (Table 6b).
In more detail, the rate of bilioma and biliary fistula was higherin the water-jet group (23%) whereas cholangitis occurred moreoften after stapler hepatectomy (6.2%). While stapler hepatectomywas associated with more intraabdominal abscess (13.6%) andsepsis (2.5%), water-jet liver dissection showed more pulmonary(19.1%), renal complications (7.6%) and was associated with higherrate of temporary liver insufficiency (11%).
3.3. Resection margins
Histopathological analysis of the resection margins of the wholecohort revealed R0 resection rate in 77%, R1 in 12 %, R2 in 5% and Rxin 6%.
Comparing major and minor liver resections we registered anoverall rate of R0 in 78%, R1 in 12 %, R2 in 3 % and Rx in 7% in majorresections. In detail comparing different resection techniques formajor hepatectomies we noted 81% R0, 4% R1, 4% R2 and 11 % Rxresection rates in the stapler group whereas R0 resection rate waschronicled in 100% in the water jet group.
In minor hepatectomies, 77% showed R0,12% R1, 7% R2 and 4% Rxresection rates. Comparing the different resection techniques in mi-nor hepatectomies we found 69% R0 and 31% R1 in the elctrocautery
group,whereas 71%R0,14%R1and4%R2 and 11%Rxwere seen in thestapler group. The water- jet group showed 75% R0, 25% R1.
3.4. Cost-effectiveness calculation
Amedian number of 6 roticulators (range from 1e21) were usedper stapler hepatectomy. In greater detail: a median number of 10roticulators were necessary for major stapler hepatectomies,whereas a median of 6 roticulators were necessary in minor staplerhepatectomies.
Thus, the additional material costs for stapler hepatectomyvaried between 258 and 3158 Euros (median 1008 Euros); (a me-dian of 1608 Euros for major hepatectomies and a median of1008 Euros for minor hepatectomies, respectively). For water-jethepatectomies, additional costs of median 100 Euros/operationwere calculated for minor, as well as for major hepatectomies. Theusage of electrocautery did not lead to additional material costs.The median cost of operating time (calculated with 13 Euros/min-ute) for major hepatectomies was 3471 Euros for stapler hepatec-tomies and 3874 Euros for water-jet hepatectomies. For minorhepatectomies, the median cost of operating time was 2340 Eurosfor electrocautery, 2113 Euros for the stapler and 2847 Euros forwater-jet dissection (Table 7).
4. Discussion
Various liver transection techniques are compared in severalstudies in the literature.

Table 6a): Patients’ characteristics of the comparative analysis between stapler vs. water-jet in n ¼ 107 major liver resections. (b): Comparative analysis between stapler vs. water-jetin n ¼ 107 major liver resections. Intra- and postoperative results.
Stapler n ¼ 81 Water-jet n ¼ 26
ASA ASA I: 6 (7.4%) ASA I: 2 (7.7%)ASA II: 51 (63%) ASA II: 16 (61.5%)ASA III: 24 (29.6%) ASA III: 8 (30.8%)
Hepatitis B 3 (3.7%) 2 (7.7%)Hepatitis C 3 (3.7%) 0Liver cirrhosis 6 (7.4%) 6 (23.1%)MELD score Median 6 (range 6e8) Median 6 (range 6e8)Pre-treatment 35 (43.2%) 8 (30.8%)CTX 27 (33.3%) 4 (15.4%)RFA 2 (2.5%) 0TACE 9 (11.1%) 6 (23.1%)Radiation 3 (3.7%) 1 (3.8%)Preliminary liver resection 11 (13.6%) 4 (15.4%)
Stapler n ¼ 81 Water-jet n ¼ 26 p-Value
Age (years) Median 63 Median 67 0.139Operating time (minutes) Median 267 (range 71e750) Median 298 (range 136e553) 0.492Pringle manoeuvre 26 (32.1%) 7 (26.9%) <0.001Intensive care unit (days) Median 2(range 0e40) Median 2 (range 0e10) 0.563Mechanical ventilation (days) Median 0 (range 0e29) Median 0 (range 0e5) 0.107Morbidity 38 (47%) 14 (54%) 0.697Surgical complications 25 (30.9%) 9 (34.6%) 0.908Medical complications 19 (23.5%) 7 (26.9%) 0.949Re-operation 5 (6.2%) 2 (7.7%) 0.898In-hospital mortality 9 (11.1%) 2 (7.7%) 0.855IntraoperativeRBC Median 1 (range 0e12) Median 1 (range 0e10) 0.95FFP Median 4 (range 0e36) Median 1 (range 0e24) 0.383PPSB Median 0 (range 0e1200 IE) Median 0 0.577
PostoperativeRBC Median 0 (range 0e11) Median 0 (range 0e4) 0.45FFP Median 0 (range 0e56) Median 0 (range 0e18) 0.342PPSB Median 0 (range 0e1500 IE) Median 0 (range 0e5000 IE) 0.463
ASA ¼ American Society of Anesthesiologists; MELD ¼ model of endstage liver disease; CTX ¼ chemotherapy; RFA ¼ radiofrequency ablation; TACE ¼ transarterial che-moembolization.RBC ¼ red blood cells; FFP ¼ fresh frozen plasma: PPSB ¼ prothrombin complex concentrate; IE ¼ international units.
C. Riediger et al. / International Journal of Surgery 11 (2013) 826e833 831
ORIGINAL RESEARCH
In a comparative analysis of clamp crushing, water-jet, CUSAand dissecting sealer, Lesurtel et al. described the advantages of theclamp crushing technique (shorter operating times and reducedblood loss) over the CUSA and water-jet techniques, in a random-ized controlled trial.24 By comparison, Fan and other authors reportadvantages of the CUSA technique over the clamp crushing tech-nique in a retrospective analysis.31 Other comparative analysesrevealed no differences between clamp crushing and CUSA; espe-cially in operation time.29,30 Another group compared the crushclamping technique, the stapler and the dissecting sealer. No sig-nificant differences with regard to the need for transfusion, or ICUand hospital stay were reported, whereas some variation inconnection with biliary leakage (without statistical significance)was seen.28 Delis et al. compared the crush clamping technique andthe radiofrequencyeassisted liver resection technique (Habib).Even though the crush clamping technique showed shorter oper-ating time with the same amount of blood loss, the authors
Table 7Cost-effectiveness calculation for the different liver transection techniques.
Minor hepatectomy
Transection technique Electrocautery StaplerMedian operating time 180 min 162.5 minMedian price for operating time 2340 Euro 2113 EuroMedian additional material costs / 108 Euro þ
900 EuroMedian summary of additional
material costs and operatingtime costs
2340 Euro 3121 Euro
conclude that the radiofrequency-assisted liver resection techniqueis reliable in cirrhotic patients.32 However, no clear advantage ofone particular method is proven.
In comparison with other centers, monopolar or bipolar elec-trocautery, vascular stapler and the water-jet technique weremainly used for liver transections in our center. CUSA or tissue linkdissecting sealer was rarely used. The radiofrequency-assisted livertransection technique was used exceptionally in a small number ofpatients and was therefore not included into the comparativeanalysis.
In this study, we were able to show clear differences betweenmajor hepatic resections (�3 liver segments resected) and minorhepatic resections (<3 liver segments resected). This result is notsurprising and is in accordance with the literature.33,34 Operationtime was significantly longer in major hepatic resections. Further-more, the total rate of morbidity and surgical morbidity wassignificantly higher in major hepatic resections. However, there
Major hepatectomy
Water-Jet Stapler Water-Jet219 min 267 min 298 min2847 Euro 3471 Euro 3874 Euro100 Euro 108 Euro þ 1500 Euro 100 Euro
2947 Euro 5079 Euro 3974 Euro

C. Riediger et al. / International Journal of Surgery 11 (2013) 826e833832
ORIGINAL RESEARCH
was no significant difference in medical complications betweenmajor and minor hepatic resections. The need for intra- and post-operative transfusion of red blood cells and fresh frozen plasmawassignificantly higher in major resections. Therefore, minor hepaticresections should, if possible, always be given priority. Especially inpatients with colorectal metastases, minor hepatic resectionsshould be favoured if technically feasible. Major liver resectionswere mostly performed by stapler and water-jet, whereas minorresections were mostly conducted using the stapler, water-jet orelectrocautery. Statistically significant variation was shown be-tween minor and major resections, regardless of the transectiondevice. There were no significant differences found between thevarious transection techniques analysed for minor and major re-sections. However, some trends were seen. Similar to other studies,stapler hepatectomy resulted in the fastest operating time for mi-nor and major liver resections, whereas the water-jet required thelongest operative period in both groups.16 In both minor and majorresections, the need for intraoperative blood transfusion washighest in the stapler group. In minor resections, liver dissectionsusing electrocautery required the lowest blood transfusion.
In contrast to other studies, the highest morbidity rate was seenin the water-jet dissection group for minor and major liver re-sections. Particularly, pulmonary complications occurred mostfrequently after water-jet hepatectomies. This could be procedure-related. Due to the jet of water, material may be flushed into theblood circulation, causing pulmonary problems. There is only onecase report in the literature, describing a pulmonary embolism in ayoung patient during a liver resectionwith the water-jet.35 In otherstudies, there was no evidence for an increased risk of pulmonarycomplications after water-jet dissection.36 In contrast, Koo et al.describe a higher incidence of venous air embolisms in liver dis-sections performed with CUSA.30 Furthermore, biliary complica-tions seem to be higher after water-jet dissection. These resultspartially contradict the literature. Most authors do not report ahigher incidence of biliary complications and there is only onegroup who has reported a higher incidence of biliary abscesses.37
Some authors in favour of the vascular stapler argue that shorteroperation times justify higher material costs, others argue thatstapler hepatectomies tend to showmore biliary complications.16,38
In our data, stapler hepatectomies resulted in shorter operatingtimes in both minor and major liver resections, even though nostatistically significant advantage over the other methods analysedwas seen. Our internal cost-effectiveness analysis of the differenttechniques revealed a clear disadvantage for stapler hepatectomy:the median time saved during stapler hepatectomies in major re-sections was 52 min � 13 Euros (or 403 Euros), as compared to thewater-jet. In minor hepatectomies, stapler hepatectomy couldreduce the operating time by a median of 17 min (or 227 Euros),compared to electrocautery, or 56 min (or 734 Euros) compared towater-jet dissection. The median additional material costs wereapproximately 1500 Euros compared to the water-jet technique formajor hepatectomies, app. 1000 Euros compared to the electro-cautery and app. 900 Euros compared to the water-jet for minorhepatectomies. Thus, there is no economic benefit, neither forminor nor for major liver resections, conferred by reduced oper-ating time in stapler hepatectomies.
In summary, in this single-centre analysis, a significant advan-tage for minor hepatic resection, in comparison with major liverresection could be shown. The various liver transection techniquesdid not produce any statistically significant advantage for any oneparticular method used inminor or major hepatectomies. However,minorhepatic resections can be performed safely,withoutmortalityand with low morbidity, by using electrocautery. The water-jettechnique can be considered as a reliable liver transection tech-nique formajor andminor liver resections. Economic disadvantages
were shown in our cost-effectiveness analysis for stapler hepatec-tomies. Careful consideration of the additional costs, and if theyjustify the use of stapler devices in liver surgery, is recommended.However, the choice of transection technique is strongly dependenton the surgeon and his/her preference.
Ethical approvalPatients signed informed consent for retrospective data analysis.
FundingNo specific sources of funding.
Author contributionCarina Riediger- study design, data collections, data analysis,
writingMichael W. Mueller- study design, data collections, data anal-
ysis, writingFlorian Geismanne study design, data collections, data analysis,
writing.Andreas Lehmann e study design, data collections, data anal-
ysis, writing.Tibor Schuster e study design, data collections, data analysis,
writing.Christoph W. Michalski e study design, data collections, data
analysis, writingKlaus Kuhn e study design, data collections, data analysis,
writingHelmut Friess e study design, data collections, data analysis,
writing
Conflict of interestNo conflicts of interest.
References
1. Foster JH, Berman MM. Solid liver tumors. Major Probl Clin Surg 1977;22:1e342.
2. Gozzetti G, Mazziotti A, Grazi GL, et al. Liver resection without blood trans-fusion. Br J Surg 1995;82(8):1105e10.
3. Kooby DA, Stockman J, Ben-Porat L, et al. Influence of transfusions on periop-erative and long-term outcome in patients following hepatic resection forcolorectal metastases. Ann Surg 2003;237(6):860e9 [discussion 869e870].
4. Nagano Y, Togo S, Tanaka K, et al. Risk factors and management of bile leakageafter hepatic resection. World J Surg 2003;27(6):695e8.
5. Aragon RJ, Solomon NL. Techniques of hepatic resection. J Gastrointest Oncol2012;3(1):28e40.
6. Pachter HL, Spencer FC, Hofstetter SR, Coppa GF. Experience with the fingerfracture technique to achieve intra-hepatic hemostasis in 75 patients withsevere injuries of the liver. Ann Surg 1983;197(6):771e8.
7. Burdio F, Grande L, Berjano E, et al. A new single-instrument technique forparenchyma division and hemostasis in liver resection: a clinical feasibilitystudy. Am J Surg 2010;200(6):e75e80.
8. Horgan PG. A novel technique for parenchymal division during hepatectomy.Am J Surg 2001;181(3):236e7.
9. Lin TY. A simplified technique for hepatic resection: the crush method. AnnSurg 1974;180(3):285e90.
10. Poon RT, Fan ST, Lo CM, et al. Improving perioperative outcome expands therole of hepatectomy in management of benign and malignant hepatobiliarydiseases: analysis of 1222 consecutive patients from a prospective database.Ann Surg 2004;240(4):698e708 [discussion 708e610].
11. Sun HC, Qin LX, Lu L, et al. Randomized clinical trial of the effects of abdominaldrainage after elective hepatectomy using the crushing clamp method. Br J Surg2006;93(4):422e6.
12. Fasulo F, Giori A, Fissi S, Bozzetti F, Doci R, Gennari L. Cavitron ultrasonicsurgical aspirator (CUSA) in liver resection. Int Surg 1992;77(1):64e6.
13. Nagano Y, Matsuo K, Kunisaki C, et al. Practical usefulness of ultrasonic surgicalaspirator with argon beam coagulation for hepatic parenchymal transection.World J Surg 2005;29(7):899e902.
14. Rau HG, Duessel AP, Wurzbacher S. The use of water-jet dissection in open andlaparoscopic liver resection. HPB (Oxford) 2008;10(4):275e80.
15. Papachristou DN, Barters R. Resection of the liver with a water jet. Br J Surg1982;69(2):93e4.
16. Schemmer P, Friess H, Hinz U, et al. Stapler hepatectomy is a safe dissectiontechnique: analysis of 300 patients. World J Surg 2006;30(3):419e30.

C. Riediger et al. / International Journal of Surgery 11 (2013) 826e833 833
ORIGINAL RESEARCH
17. Weber JC, Navarra G, Jiao LR, Nicholls JP, Jensen SL, Habib NA. New techniquefor liver resection using heat coagulative necrosis. Ann Surg 2002;236(5):560e3.
18. Stella M, Percivale A, Pasqualini M, et al. Radiofrequency-assisted liver resec-tion. J Gastrointest Surg 2003;7(6):797e801.
19. Schmidbauer S, Hallfeldt KK, Sitzmann G, Kantelhardt T, Trupka A. Experiencewith ultrasound scissors and blades (UltraCision) in open and laparoscopicliver resection. Annals of Surgery 2002;235(1):27e30.
20. Sugo H, Mikami Y, Matsumoto F, et al. Hepatic resection using the harmonicscalpel. Surg Today 2000;30(10):959e62.
21. Strasberg SM, Drebin JA, Linehan D. Use of a bipolar vessel-sealing device forparenchymal transection during liver surgery. J Gastrointest Surg 2002;6(4):569e74.
22. Romano F, Franciosi C, Caprotti R, Uggeri F, Uggeri F. Hepatic surgery using theLigasure vessel sealing system. World J Surg 2005;29(1):110e2.
23. Campagnacci R, De Sanctis A, Baldarelli M, et al. Hepatic resections by means ofelectrothermal bipolar vessel device (EBVS) LigaSure V: early experience. SurgEndosc 2007;21(12):2280e4.
24. Lesurtel M, Selzner M, Petrowsky H, McCormack L, Clavien PA. How shouldtransection of the liver be performed?: a prospective randomized study in 100consecutive patients: comparing four different transection strategies. Ann Surg2005;242(6):814e22 [discussion 822e813].
25. Fong Y, Fortner J, Sun RL, Brennan MF, Blumgart LH. Clinical score for pre-dicting recurrence after hepatic resection for metastatic colorectal cancer:analysis of 1001 consecutive cases. Ann Surg 1999;230(3):309e18 [discussion318e321].
26. Nordlinger B, Guiguet M, Vaillant JC, et al. Surgical resection of colorectalcarcinoma metastases to the liver. A prognostic scoring system to improve caseselection, based on 1568 patients. Association Francaise de Chirurgie. Cancer1996;77(7):1254e62.
27. Minagawa M, Makuuchi M, Torzilli G, et al. Extension of the frontiers of surgicalindications in the treatment of liver metastases from colorectal cancer: long-term results. Ann Surg 2000;231(4):487e99.
28. Castaldo ET, Earl TM, Chari RS, et al. A clinical comparative analysis of crush/clamp, stapler, and dissecting sealer hepatic transection methods. HPB (Oxford)2008;10(5):321e6.
29. Takayama T, Makuuchi M, Kubota K, et al. Randomized comparison of ultra-sonic vs clamp transection of the liver. Arch Surg 2001;136(8):922e8.
30. Koo BN, Kil HK, Choi JS, Kim JY, Chun DH, Hong YW. Hepatic resection by thecavitron ultrasonic surgical aspirator increases the incidence and severity ofvenous air embolism. Anesth Analg 2005;101(4):966e70 [table of contents].
31. Fan ST. Technique of hepatectomy. Br J Surg 1996;83(11):1490e1.32. Delis S, Bakoyiannis A, Tassopoulos N, et al. Clamp-crush technique vs.
radiofrequency-assisted liver resection for primary and metastatic liver neo-plasms. HPB (Oxford) 2009;11(4):339e44.
33. Billingsley KG, Jarnagin WR, Fong Y, Blumgart LH. Segment-oriented hepaticresection in the management of malignant neoplasms of the liver. J Am CollSurg 1998;187(5):471e81.
34. Andreou A, Vauthey JN, Cherqui D, et al. Improved long-term survival aftermajor resection for hepatocellular carcinoma: a multicenter analysis based ona new definition of major hepatectomy. J Gastrointest Surg 2013;17(1):66e77.
35. Smith JA. Possible venous air embolism with a new water jet dissector. Br JAnaesth 1993;70(4):466e7.
36. Vollmer CM, Dixon E, Sahajpal A, et al. Water-jet dissection for parenchymaldivision during hepatectomy. HPB (Oxford) 2006;8(5):377e85.
37. Baer HU, Gilg M, Maddern GJ, Blumgart LH. High velocity water jet dissection inliver surgery. Helv Chir Acta 1992;59(2):437e42.
38. Smith DL, Arens JF, Barnett Jr CC, Izzo F, Curley SA. A prospective evaluation ofultrasound-directed transparenchymal vascular control with linear cuttingstaplers in major hepatic resections. Am J Surg 2005;190(1):23e9.