
Companion October2012
36
The essential publication for BSAVA members companion OCTOBER 2012 Exotic pet and wildlife nursing Puppy Contracts Exploring welfare initiatives P6 Clinical Conundrum German Shepherd with respiratory signs P10 How To… Perform pericardiocentesis P14
description
bsava revista
Transcript of Companion October2012

The essential publication for BSAVA membersThe essential publication for BSAVA members
companionOCTOBER 2012
Exotic pet and wildlife nursing
Puppy ContractsExploring welfare initiativesP6
Clinical ConundrumGerman Shepherd with respiratory signsP10
How To…Perform pericardiocentesisP14

2 | companion
EJCAP ONLINE
Don’t forget that as a BSAVA member you are enti tled to free online access to EJCAP – register at www.fecava.org/EJCAP to access the latest issue.
PETSAVERS FUNDED STUDYCalcium and phosphate homeostasis in hyperthyroid catsThis PetSavers-funded study found that changes in plasma parathyroid hormone and fi broblast growth factor-23 concentrati ons which occur in hyperthyroid cats are not mediators of progression of chronic kidney disease; however, fi broblast growth factor-23 would appear to have some prognosti c signifi cance in hyperthyroidism.
Screening of ragdoll cats for kidney diseaseIn this study, ultrasonographic fi ndings compati ble with chronic kidney disease were observed in almost 10% of cats, and polycysti c kidney disease occurred at a low prevalence.
Rectal lymphoma in 11 dogsThis retrospecti ve study found that canine lymphoma of the rectum is associated with a favourable prognosis.
Scatt er radiati on dose levels in small animal radiographyThe authors conclude that while the doses recorded were small in terms of associated risk, they are nonetheless cumulati ve, which
companion is published monthly by the British Small Animal Veterinary Association, Woodrow House, 1 Telford Way, Waterwells Business Park, Quedgeley, Gloucester GL2 2AB. This magazine is a member-only benefi t. Veterinary schools interested in receiving companion should email [email protected]. We welcome all comments and ideas for future articles.
Tel: 01452 726700Email: [email protected]
Web: www.bsava.com
ISSN: 2041-2487
Editorial BoardEditor – Mark Goodfellow MA VetMB CertVR DSAM DipECVIM-CA MRCVSCPD Editor – Simon Tappin MA VetMB CertSAM DipECVIM-CA MRCVSPast President – Andrew Ash BVetMed CertSAM MBA MRCVS
■ CPD Editorial TeamPatricia Ibarrola DVM DSAM DipECVIM-CA MRCVSTony Ryan MVB CertSAS DipECVS MRCVSLucy McMahon BVetMed (Hons) DipACVIM MRCVSDan Batchelor BVSc PhD DSAM DipECVIM-CA MRCVSEleanor Raffan BVM&S CertSAM DipECVIM-CA MRCVS
■ Features Editorial TeamAndrew Fullerton BVSc (Hons) MRCVSMathew Hennessey BVSc MRCVS
■ Design and ProductionBSAVA Headquarters, Woodrow House
No part of this publication may be reproduced in any form without written permission of the publisher. Views expressed within this publication do not necessarily represent those of the Editor or the British Small Animal Veterinary Association.
For future issues, unsolicited features, particularly Clinical Conundrums, are welcomed and guidelines for authors are available on request; while the publishers will take every care of material received no responsibility can be accepted for any loss or damage incurred.
BSAVA is committed to reducing the environmental impact of its publications wherever possible and companion is printed on paper made from sustainable resources and can be recycled. When you have finished with this edition please recycle it in your kerbside collection or local recycling point. Members can access the online archive of companion at www.bsava.com .
3 BSAVA NewsLatest from your Association
4–5 ConsultationsUpdates & have your say on nurse anaesthesia
6–9 Puppy ContractsExploring welfare initiatives
10–13 Clinical ConundrumA German Shepherd with respiratory signs
14–18 How To…Perform pericardiocentesis
20 CongressRichard Dawkins announced as special speaker
21–22 Congress ManagementMaking the most of your PR
23–25 PublicationsExotic pet and wildlife nursing
26–27 PetSaversLatest fundraising and funding news
28–29 WSAVA NewsThe World Small Animal Veterinary Association
30–31 The companion InterviewBeverley Cuddy
33 Focus On…North West Region
34–35 CPD DiaryWhat’s on in your area
Additional stock photography Dreamstime.com© Britishbeef; © Katrina Brown; © Liumangtiger; © Michael Pettigrew; © Mikael Damkier; © Nullornotset; © Okeanas
What’s in JSAP this month?
Here are just a few of the topics that will feature in your October issue:
can result in a more signifi cant dose. Therefore manual restraint should be avoided and other forms of immobilisati on should be used.
The suscepti bility of Pseudomonas spp. isolated from dogs with oti ti s to topical ear cleanersTopical treatment with ear cleaners is considered to be a valuable adjunct in the treatment of canine oti ti s that involves multi anti microbial-resistant organisms such as Pseudomonas spp. The use of these preparati ons as a sole form of therapy may be eff ecti ve in some cases.
Pedicle ligati on in ovariohysterectomyThe results of this study suggest that uti lising a knot design that has more inherent resistance to slippage of the fi rst throw may be preferable over square and surgeon’s knots when tying a ligature on a bulky vascular pedicle like the ovarian stump in a large bitch.
Log on to www.bsava.com to access the JSAP archive online. ■

companion | 3
BSAVA Scottish Congress committee celebrated their most successful Congress to date with over 200 delegates and almost 50 different commercial exhibitors joining them in Edinburgh last month. With main lecture streams covering Ophthalmology and Orthopaedics for vets
and Nutrition/Nutraceuticals and Neonatology for nurses alongside a series of afternoon seminars, there was plenty to entice a wide range of delegates from Scotland, England, Isle of Man, Canada, Germany, Finland and the USA, making Scottish Congress 2012 a truly international affair.
Delegates and exhibitors were kept entertained with a pub quiz on the Friday, and on the Saturday the Gala Dinner and Ceilidh dancing carried on into the early hours of Sunday morning, giving a real Scottish feel to the event.
Plans are already underway for 2013 with the event to be held once again at the Edinburgh Conference Centre, Heriot-Watt – from 30 August to 1 September. Topics will include Cardiology and Neurology for vets and Clinical Pathology/Laboratory Skills and Wound Management for nurses. ■
In the coming weeks you will have news about membership renewal for 2013 – asking you to update your details and consider Direct Debit. We are making more efforts to make it easier for you to renew and
ensure you don’t miss out on your current benefits, or the loyalty bonus due to you.
Congress registrationBecause you can register now for 2013 Congress it is possible to register in an incorrect category. For instance, you might be a 3rd Year Qualified Member in 2012, but will become a Full Member in 2013, when the event takes place. So please make sure you renew promptly and that you select the appropriate Congress registration for your status in 2013. If you have any questions about Congress or for more information about benefits and renewal visit the website or email [email protected] or call 01452 726700. ■
Important renewal information
WSAVA were delighted to have received a record donation of £10,000 from BSAVA to support their education programmes in Sub-Saharan Africa.
In many ways, this region is the ‘final frontier’ for small animal medicine. WSAVA says that the lack of even basic equipment, such as microscopes, is an issue of great concern. BSAVA’s donation is being combined with funding to the tune of 4000 Euros received annually by the WSAVA from the Netherlands Association for Companion Animal Medicine (NACAM). ■
BSAVA funding CPD in Sub-Saharan Africa
An international fl avour at Scottish Congress 2012

4 | companion
Speak louderHave your say on consultations
The role of the vet in animal welfareRespondents did consider that the five welfare needs were a helpful way of considering animal welfare, and the most commonly mentioned welfare problems were:
■ Obesity ■ Behaviour problems
– Stress in cats (especially in multi-cat households)
– Boredom/lack of exercise (dogs/rabbits) ■ Husbandry problems (especially in exotic pets) ■ Chronic pain/disease (especially in geriatrics) ■ Problems of inbreeding – breathing problems and
atopic dermatitis mentioned.
Most of the responses concentrated on the need to educate owners, especially before/in the early stages of ownership. There was general agreement that vets and nurses could be doing more to promote animal welfare and that there may be a role for BSAVA in providing support materials for this.
Compulsory microchip scanningHalf of respondents reported that they routinely scan new pets registered at their practice, and all bar one favour this procedure in theory. However only 2/16 routinely check these details against the appropriate database, with respondents mentioning how time-consuming it is to ring several numbers to get the right database and out of date information as the main problems. Individual respondents also mentioned the possibility that stolen animals might not be presented at a practice and may miss out on needed treatment, as well as problems that could arise if veterinary surgeons became involved in ownership disputes.
Overall, vets responding to this survey are willing to scan but there is a long way to go in getting the database provision to a point where it is practical.
Speak louderHave your say on Speak louderHave your say on Speak louder
While these responses are helpful to BSAVA, we would prefer to have much larger numbers of responses on which to base our decisions and responses. So please take a few minutes to read and respond to the following consultation.
If you have any comments on any of the consultations mentioned in this article or ideas on how to increase member response please contact Sally Everitt (Scientific Policy Officer) – email [email protected] . ■
BSAVA is frequently asked to comment on matters of policy or interest to government or other organisations. In responding to consultations we aim to represent the
views and interests of veterinary surgeons in small animal practice – but to do this we need your help. At other times we need information to plan future activity within BSAVA. Please keep your eye on notices in companion – and where we are given short notice, we will email you asking you to take part. This way we can be truly representative in our responses and when formulating policy.
Two recent consultations (featured in June companion) asked about the role of the vet in animal welfare and attitudes to compulsory microchip scanning. While the responses we received were very interesting and valuable, the number of responses was small (7 and 16 respectively). Here is a brief summary of the responses, followed by our latest consultation on the role of the veterinary nurse in monitoring and maintaining anaesthesia.

companion | 5
A recent motion in the Scottish Parliament proposed that “like humans, animals should only receive care from extensively-trained staff, and calls on veterinary surgeries to only
use registered veterinary nurses to monitor anaesthetised animals” (John Finnie, August 9th).
Current guidance from the RCVS states that “Monitoring a patient during anaesthesia and the recovery period is the responsibility of the veterinary surgeon, but may be carried out on his or her behalf by a suitably trained person” and that “Veterinary nurses and student veterinary nurses may be directed to assist veterinary surgeons with the maintenance of anaesthesia and the monitoring of patients under anaesthesia”. Following discussion at VN Council, the RCVS is reviewing the position of VNs and lay individuals in relation to anaesthesia.
Although many people support the idea of Registered Veterinary Nurses (RVNs) being available to monitor all anaesthetics, concern has arisen that at the present time there are insufficient RVNs to make this practicable. In response to this, SPVS and The College of Animal Welfare have developed a Level 2 certificate in “assisting veterinary surgeons with anaesthesia and sedation and monitoring animal patients”, which will be awarded by City and Guilds.
In order to represent your views when discussing these developments with outside bodies, BSAVA need you to take a few minutes to complete the following questionnaire. You can either post your completed questionnaire to us, or preferably complete the online questionnaire at www.bsava.com/consultations – it should only take a few moments. Thank you. ■
Monitoring and maintaining anaesthesia: the role of the veterinary nurse
NURSES MONITORING AND MAINTAINING ANAESTHESIA QUESTIONNAIRE
1. Please describe your positi on in practi ce (vet, nurse, employer, employee)
6. Should qualifi ed veterinary nurses be allowed to alter vaporiser setti ngs without authorisati on from the veterinary surgeon?
[ ] Yes [ ] No Comment:
8. Would you encourage lay staff to take the certi fi cate in assisti ng veterinary surgeons with anaesthesia and sedati on and monitoring animal pati ents?
[ ] Yes [ ] No Comment:
9. Would you encourage qualifi ed veterinary nurses to undertake further training in anaesthesia?
[ ] Yes [ ] No Comment:
10. Any other comments on the role of nurses in anaesthesia
7. Should qualifi ed veterinary nurses be allowed to induce anaesthesia? [ ] Yes [ ] No Comment:
3. Proporti on of small animal work carried out in your practi ce (approximate percentage)
4. Is the practi ce registered with the RCVS Practi ce standards scheme?
[ ] No [ ] Core standards (Tier1) [ ] GP Practi ce (Tier 2) [ ] Hospital (Tier 3) [ ] Emergency Service Clinic [ ] Veterinary Nurse Training Practi ce
5. Who assists the veterinary surgeon in monitoring anaestheti cs in your practi ce?
Always Usually Someti mes Never Registered veterinary nurses [ ] [ ] [ ] [ ] Listed veterinary nurses [ ] [ ] [ ] [ ] Student veterinary nurses [ ] [ ] [ ] [ ] Lay staff involved in nursing duti es [ ] [ ] [ ] [ ] Lay staff not normally involved in [ ] [ ] [ ] [ ] nursing duti es
2. How many staff are employed in your practi ce? [ ] Veterinary surgeons [ ] Registered veterinary nurses [ ] Listed veterinary nurses [ ] Student veterinary nurses [ ] Lay staff involved in nursing duti es [ ] Lay staff not normally involved in nursing duti es

6 | companion
Puppy contractsIt is four years since the BBC documentary Pedigree Dogs Exposed highlighted the dangers of inherited diseases in dogs emerging from an artificially shallow gene pool. Since then, veterinary and animal welfare organisations have launched a number of initiatives aimed at improving the physical and mental health of puppies. John Bonner looks at progress so far

companion | 7
How does a pet owner avoid being sold a poorly pup? In most cases, if you find that you have bought faulty goods, the answer is simple – you take them back. But if the object
purchased is a living, breathing canine infant then the situation is a little more complicated.
If the puppy has an inherited condition, this may not become obvious until the animal is weeks or years old. Yet, even it is detected earlier, when the puppy has only been with its new family for a few days, they are already likely to have established strong emotional bonds which make it impossible for them to send it back to the breeder.
The best guarantee for the new owners that their puppy is healthy is for it to have been examined by a veterinary surgeon before any money changes hands. Many practices already provide their dog-breeding clients with a document that they can give to the buyer, stating that the animal has been seen and appears to be in good shape. With that in mind – this autumn the Advisory Council on the Welfare Issues of Dog Breeding (ACWIDB) will be conducting a pilot study for a scheme involving a standardised veterinary health check form.
This is a three-month trial involving around 50 breeders and their usual veterinary practice. If successful, it will then be launched nationwide in early 2013, according to Chris Laurence, an ACWIDB Council member and former chief veterinary officer with the Dogs Trust.
Aims of the CouncilThe form is the latest in a series of steps that have been taken by the council to try and reduce the number of pet owners who experience the emotional and financial distress which may arise if their pet is found to have a serious genetic or conformation-related disorder. When the Council was established in February 2010, in the wake of the controversy surrounding Jemima Harrison’s film, it reasoned that the most important safeguard for a new puppy owner is good quality information on what to look for in a new puppy.
So its first task was to set up a website offering advice on the issues to be considered when thinking of buying a pedigree puppy – or indeed any dog, irrespective of age and breed. The ACWIDB also
recognised that understanding of the science underlying many of the health and welfare problems encountered in dogs was inadequate, and drew up a programme for future research in this area.
The ‘puppy contract’ projectsAs a multidisciplinary group of experts supported by each of the main dog welfare charities, the ACWIDB is leading the development of a strategy for improved canine health. But it is not the only influential group working in this area.
In its July 2012 report on ‘A healthier future for pedigree dogs’, the Associate Parliamentary Group for Animal Welfare set out the agenda for political action to facilitate change. This included backing the concept of a puppy contract to be signed and kept by the new owner and the breeder, pet shop or other business supplying their animal.
8 | companion
Puppy contracts
The RSPCA and the BVA Animal Welfare Foundation decided to develop this idea, with the April launch of their puppy information pack. This contains both a formal, legally binding contract to be signed by both parties and a document containing information about the pup’s parentage and any screening tests carried out to identify inherited disease. The information pack is intended to be an evolving project and its contents will be reviewed after a year, said Lisa Richards, a scientific officer in the RSPCA companion animals department.
In a separate initiative, the Dogs Trust and Kennel Club have come together to create a puppy plan to try to ensure that a new pet is sound in mind as well as body. The plan sets out steps to ensure that the pup is properly socialised and with early life experiences that may prevent the development of the sort of behavioural problems that are the main cause of dogs being rehomed as adults.
With this profusion of different initiatives, there is certainly a risk that prospective pet owners could feel overwhelmed by the amount of advice being offered, acknowledges Paula Boyden, the Dogs Trust’s current CVO. However, she points out that initiatives like the puppy information pack and the puppy plan address different issues and are apparently intended to be complementary. The only area where there is any redundancy is in the issue of puppy contracts where the RSPCA/BVA AWF initiative covers much the same ground as the Kennel Club contracts. The main
difference is that the latter only really attracts the attention of pedigree dog breeeders. Paula points out that it is still early days and there is potential for bringing the two schemes together to reduce the risk of confusing potential owners.
To what end?Unlike any previous documents provided by the breeder for those buying their puppies, the RSPCA/AWF contract is intended to have legal standing, and could form the basis for a claim for redress in the civil courts if the information provided were false or incomplete, explains James Yeates, RSPCA’s CVO. Plus, it can benefit both sides in the transaction, he asserts. “It empowers the good, responsible and loving breeder to showcase their stock and show that their puppies are the best and healthiest available.”
In contrast, the health check form is not intended to be a guarantee of the puppy’s suitability for sale, says Harvey Locke, senior vice-president of the BVA, whose organisation strongly supports the scheme. “It is not meant to have any legal standing. It is a low-cost, precursory check that is intended to encourage breeders to have the whole litter examined by a vet before it goes off for sale.”
Harvey Locke points out that the health check is intended to identify only those physical signs of inherited defects that be would detected during any routine pre-vaccination check by a general practitioner, without specialist knowledge or equipment. Veterinary surgeons are asked to look at 24 parameters that would be a normal part of the physical examination of a new patient. The examination may help to identify defects which had not been noticed by the breeder, such as a cleft palate or an irregular heart sound.
The role of the vetThe wording on the certificate also makes clear that the examination is a snapshot of the puppy’s health status on that particular date, and cannot be expected to predict any subsequent changes. “The check will not detect some inherited defects that may manifest themselves later in life or may be affected by the environment in which the puppy is reared. It is therefore not a guarantee that the puppy is without any faults,” it warns.
Yet, despite these caveats, the Veterinary Defence

companion | 9
…we always advise vets to exercise caution when signing any
form of certification. These forms will be treated as certificates and
the vet will be responsible for what is said at the time…
Society has serious concerns about the principle behind the vendor certificate. Clinical signs of conditions such as a heart murmur may not be detectable if the puppy is examined at 6 weeks old but become very obvious a few months later, says Fred McKeating, technical services director for the society.
“We get a couple of calls every month concerning cases where the purchaser has been presented with a certificate produced by the breeder saying that the animals have been checked by a vet. When something goes wrong, it is the vet who gets the blame.”
Similar pre-purchase checks carried out by equine practitioners are a regular source of problems for the VDS. “So, as an insurance company, we can only indemnify vets who produce these certificates for their clients when the examinations are carried out under very controlled circumstances.” He warned practitioners to avoid being presented with a box of almost identical black Labrador puppies and being expected to make a rapid examination of each at a cost that does not erode the breeder’s commercial margin.
“We always advise vets to exercise caution when signing any form of certification. These forms will be treated as certificates and the vet will be responsible for what is said at the time. So the more extensive and well defined the examination is, the better protected the vet will be.”
Caroline Bower, a director of a large veterinary hospital in Plymouth, believes that the certificates can make a positive contribution to raising health standards in puppies, provided that breeders and buyers understand the limitations of a physical examination
carried out without specialist equipment or laboratory tests. “They will show that the breeder is taking their responsibilities seriously and reduce the likelihood that a buyer will face the dilemma of whether or not to take the puppy back when it is found to be unhealthy but only after it has become part of the family.”
Caroline is confident that colleagues would appreciate the importance of carrying out a thorough physical examination before signing their name to a certificate. It was also vital that all the puppies in a litter are individually identifiable with a microchip, and that they are examined one at a time with the rest of the litter kept outside the consulting room until needed. She also feels that practitioners should be given guidance on some aspects of the examination, particularly the time that it is expected to take, so that they can charge realistically for the service.
Stephanie Writer-Davies, a Hertfordshire-based practitioner and member of council of the Society of Practising Veterinary Surgeons agreed that clear advice would be necessary to help those practitioners asked to complete the certificates. But she believed that the scheme is a positive step and would want to see the documents given to all new dog owners.
“SPVS would like to see them used for all puppy purchases, including those from pet shops for example, since not all puppies are sold directly from breeders. In theory, this should help to improve dog health and welfare and encourage owners to engage with a veterinary practice from the beginning with all the benefits of the advice and the services provided that help keep their puppy happy and healthy,” she said. ■

10 | companion
Clinical conundrum
Elisabeth Henderson, intern at the University of Bristol, invites companion readers to consider a German Shepherd bitch with respiratory signs
Case presentationA 9-year-old neutered German Shepherd bitch was referred with a one-week history of lethargy, reluctance to lie down, an unproductive cough, dyspnoea, retching and one episode of vomiting.
The dog was fed a complete dog food, but wasn’t up to date on routine vaccinations, flea treatment or worming. There was no history of travel outside the United Kingdom or exposure to toxins. The owners reported a mild improvement in the frequency of coughing with amoxicillin/clavulanate and meloxicam.
Routine haematology and biochemistry blood testing (results unremarkable) and radiographs of the thoracic cavity under general anaesthesia (Figure 1) had been carried out via the referring veterinary surgeon on the day of presentation.
List the differential diagnoses for pleural effusionDifferential diagnoses for pleural effusion are listed in Table 1. In this case, no analysis was performed on the fluid at the referring vets; however, the macroscopic appearance was of a serosanguineous fluid, which is most frequently consistent with a modified transudate.
Figure 1: Right lateral (A) and dorsoventral (B) thoracic radiographs
A
B
What is your interpretation of the thoracic radiographs?The radiographs reveal a marked pleural effusion, causing the lungs to have a ‘scalloped’ appearance in both radiographs. It is impossible to assess the cardiac silhouette, due to the overlying opacity. There is also marked deviation of the caudal trachea dorsally and to the right side. Tracheal deviation laterally would suggest that there is a soft tissue lesion within the thoracic cavity, e.g. mediastinal or heart-based mass. The lung pattern appears normal; however this is difficult to interpret due to the overlying opacity.
Following radiography, bilateral therapeutic thoracocentesis was performed to stabilise the patient prior to transportation. Approximately one litre of pleural fluid was removed, mainly from the right side of the thoracic cavity.

companion | 11
Clinical examinationClinical examination on arrival revealed:
■ A normal body condition (body condition score 5/9) ■ Tachypnoea at rest (RR>100 breaths/min) with
increased inspiratory effort ■ Hypersalivation ■ Pale pink and moist mucous membranes with a
capillary refill time of <2 seconds ■ Tachycardia (180 beats/min) and muffled
cardiopulmonary sounds ventrally, and ■ A tense abdomen.
What would be the next diagnostic step?It was deemed that further drainage of the pleural space was required, due to the presence of dyspnoea/tachypnoea; further imaging of the thoracic cavity was also indicated. The dog was administered flow-by oxygen, and general anaesthesia was induced for the placement of a thoracic drain. Small-bore chest drains can be placed in most patients using local anaesthesia, with possible sedation, but this patient was anaesthetised to allow further imaging after drainage.
During anaesthesia, ventilation was required to maintain oxygen saturation above 95%, especially when the dog was positioned in lateral recumbency. Bilateral small-bore chest drains were placed using a Seldinger technique† and a further 900 ml of
serosanguineous fluid was removed from the pleural space. After this, the dog was able to maintain adequate oxygen saturation >97% without ventilation assistance. Respiratory rate decreased and ETCO2 was 50–58 mmHg. Further thoracic imaging following drainage of the pleural effusion was performed to see whether an underlying cause could be identified.
What is your interpretation of the CT images?The post-contrast longitudinal section (Figure 2A) reveals a large heterogeneous soft tissue-attenuating mass lesion within the
Transudate Hypoalbuminaemia (hepati c failure, protein-losing nephropathy, protein-losing enteropathy, third-space loss)
Modifi ed transudate
Neoplasia, ruptured diaphragm with organ entrapment, right-sided congesti ve heart failure (pericardial eff usion or restricti on, tricuspid regurgitati on, cardiomyopathy, pulmonary hypertension), lung lobe torsion, long-standing transudate, vasculiti s, pulmonary thromboembolism, pyometra, secondary to abdominal surgery
Exudate Neoplasia: mediasti nal (lymphoma, thymoma), mesothelioma, rib chrondrosarcoma, osteosarcomaPyothorax: migrati ng foreign body, penetrati ng wound, parapneumonic eff usion, ruptured oesophagus, abscessed neoplasia, haematogenousSterile infl ammati on: dirofi lariasis, lung lobe torsion, pulmonic eosinophilic infi ltrate, ruptured diaphragm with organ entrapment, pancreati ti s
Chylothorax Idiopathic, traumati c thoracic duct rupture, congenital, dirofi lariasis, jugular vein thrombosis, neoplasia, right-sided congesti ve heart failure
Haemothorax Coagulopathy, neoplasia, trauma, lung lobe torsion
Table 1: Differential diagnoses for pleural effusion
† See How To in the August 2012 issue of companion
12 | companion
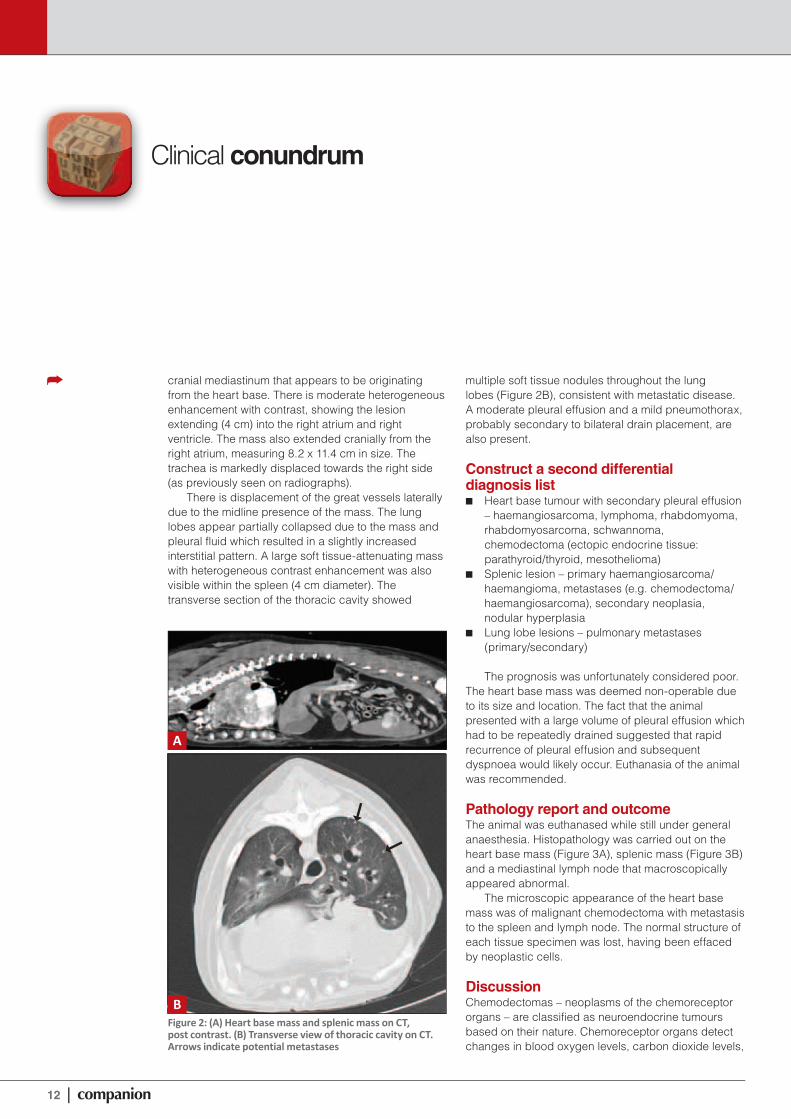
Figure 2: (A) Heart base mass and splenic mass on CT, post contrast. (B) Transverse view of thoracic cavity on CT. Arrows indicate potential metastases
A
B
Clinical conundrum
cranial mediastinum that appears to be originating from the heart base. There is moderate heterogeneous enhancement with contrast, showing the lesion extending (4 cm) into the right atrium and right ventricle. The mass also extended cranially from the right atrium, measuring 8.2 x 11.4 cm in size. The trachea is markedly displaced towards the right side (as previously seen on radiographs).
There is displacement of the great vessels laterally due to the midline presence of the mass. The lung lobes appear partially collapsed due to the mass and pleural fluid which resulted in a slightly increased interstitial pattern. A large soft tissue-attenuating mass with heterogeneous contrast enhancement was also visible within the spleen (4 cm diameter). The transverse section of the thoracic cavity showed
multiple soft tissue nodules throughout the lung lobes (Figure 2B), consistent with metastatic disease. A moderate pleural effusion and a mild pneumothorax, probably secondary to bilateral drain placement, are also present.
Construct a second differential diagnosis list
■ Heart base tumour with secondary pleural effusion – haemangiosarcoma, lymphoma, rhabdomyoma, rhabdomyosarcoma, schwannoma, chemodectoma (ectopic endocrine tissue: parathyroid/thyroid, mesothelioma)
■ Splenic lesion – primary haemangiosarcoma/haemangioma, metastases (e.g. chemodectoma/haemangiosarcoma), secondary neoplasia, nodular hyperplasia
■ Lung lobe lesions – pulmonary metastases (primary/secondary)
The prognosis was unfortunately considered poor. The heart base mass was deemed non-operable due to its size and location. The fact that the animal presented with a large volume of pleural effusion which had to be repeatedly drained suggested that rapid recurrence of pleural effusion and subsequent dyspnoea would likely occur. Euthanasia of the animal was recommended.
Pathology report and outcomeThe animal was euthanased while still under general anaesthesia. Histopathology was carried out on the heart base mass (Figure 3A), splenic mass (Figure 3B) and a mediastinal lymph node that macroscopically appeared abnormal.
The microscopic appearance of the heart base mass was of malignant chemodectoma with metastasis to the spleen and lymph node. The normal structure of each tissue specimen was lost, having been effaced by neoplastic cells.
DiscussionChemodectomas – neoplasms of the chemoreceptor organs – are classified as neuroendocrine tumours based on their nature. Chemoreceptor organs detect changes in blood oxygen levels, carbon dioxide levels,

companion | 13
CONTRIBUTE A CLINICAL CONUNDRUM
If you have an unusual or interesti ng case that you would like to share with your colleagues, please submit photographs and brief history, with relevant questi ons and a short but comprehensive explanati on, in no more than 1500 words to [email protected] submissions will be peer-reviewed.
pH and blood temperature. They act via the parasympathetic nervous system to elicit appropriate changes in cardiorespiratory function.
Chemodectomas arising from the aortic body are the most commonly reported chemoreceptor tumour in the dog. The aortic body is located within the pericardium at the base of the heart, typically between the aortic arch and the pulmonary artery.
These neoplasms are non-functional, are often locally invasive, and rarely metastasize. In one study of 357 cases of chemoreceptor tumours in dogs, only 12% of aortic body tumours had distant metastases, most frequently to the liver and lungs. In this case there was metastatic spread to the spleen and mediastinal lymph node.
Studies have indicated that brachycephalic breeds of dogs (e.g. Boston Terrier and Boxer), are more commonly affected, based upon the theory that the chronic hypoxia associated with these breeds leads to hyperplasia of the chemoreceptor organs. Some studies indicate that male dogs have a higher incidence of pathology than females.
Unless these tumours are of sufficient size to cause impairment of the heart and large vessels, they often go unnoticed and frequently they are found incidental to other disease processes. Partial resection of these tumours may be possible, but in this case the tumour infiltrated both the right atrium and ventricle and was sadly non-resectable. ■
Figure 3: (A) Longitudinal section of heart base mass. (B) Transverse section of splenic massA B
AVAILABLE FROM BSAVA
BSAVA Manual of Canine and Feline Oncology3rd editi onEdited by: Jane Dobson and Duncan Lascelles
Building on the success of previous editi ons, this fully updated Manual encompasses the important advances made over recent years, while keeping the text practi cal and user-friendly. A wealth of new photographs has been included to illustrate the clinical, diagnosti c and therapeuti c aspects of a range of tumours. The growing importance of ethical considerati ons and palliati ve care are also recognized, and exciti ng developments and treatment possibiliti es explored.
“...an excellent publicati on…suffi ciently rewritt en and updated to make it a worthwhile purchase, even for those veterinarians already in possession of the second editi on. The content is ‘state of the art’ as much as possible… remains very easy to read…a very att racti ve purchase for practi ti oners and students…” JOURNAL OF SMALL ANIMAL PRACTICE
Member price: £55.00Non-member price: £85.00

14 | companion
How to perform pericardiocentesis
Pericardial effusion (PE) is the accumulation of fluid within the pericardial sac (Figure 1). Investigation as to the cause of the
PE, as well as its drainage, are essential to allow specific treatment and accurate assessment of prognosis. Most commonly, the fluid appears serosanguineous, although in some cases it may be a clear transudate, whole blood, chyle, or a septic exudate. In dogs, PE is primarily caused by neoplastic disease, with right atrial haemangiosarcoma (Figure 2) representing the most common tumour.
Other neoplastic causes of PE in dogs are heart base tumours (chemodectomas), mesothelioma and lymphoma. Left atrial tears, infections, haemorrhage, trauma and foreign bodies are other less common causes of PE. When a primary cause cannot be identified, the effusion is termed ‘idiopathic’. In cats, PE is less commonly observed and is usually the result of congestive heart failure or feline infectious peritonitis, although other more rare aetiologies have also been reported.
When to perform pericardiocentesisAs fluid collects in the pericardial sac, it markedly impedes the filling ability of the heart (diastolic dysfunction). Since the right side of the heart tends to “suffer” most because of its thinner wall, PE normally results in signs of right-sided congestive heart failure, with pleural
effusion, jugular pulsation–distension, liver congestion and ascites. Pericardial effusion causing these clinical signs is also referred to as cardiac tamponade.
The fluid accumulated in the pericardial sac needs to be removed (pericardiocentesis) as soon as possible, using one of the several techniques available. Many dogs and cats tolerate pericardiocentesis unsedated, although mild sedation may be necessary in some cases. The withdrawal of even a small amount of pericardial fluid may dramatically and rapidly improve the patient’s haemodynamic status.
How to prepare the patient for the procedureMost clinicians prefer to restrain the animal in left lateral recumbency in order to approach the pericardium from the right side of the chest, therefore avoiding the risk of puncturing the branches of the left coronary artery. However, other clinicians prefer a right-sided approach with the patient in sternal recumbency. The cranioventral part of the right hemithorax (see Figure 3) should be
Luca and Heidi Ferasin of Specialist Veterinary Cardiology Consultancy Ltd take us step by step through the procedure
Figure 1: Thoracic radiograph, right-lateral view, of a 10-year-old female neutered Labrador with idiopathic pericardial effusion (PE). Cardiomegaly with a globular shape and very sharp outline of the heart are typical radiographic features of PE. Mild to moderate ascites and pleural effusion are also visible
CFigure 2: Echocardiographic images obtained from an 8-year-old female neutered Boxer (right parasternal long axis view) showing a moderate pericardial effusion (PE). Arrows in (A) indicate the diastolic collapse of the right atrial wall due to the pressure exerted by the pericardial fluid. Arrows in (B) highlight the presence of a rounded right atrial mass consistent with cardiac haemangiosarcoma. (C) shows a very small amount of PE following successful palliative pericardiocentesis
A
B

companion | 15
surgically prepared and a surgical drape placed on the chest to avoid any hair contamination. The operator should wear surgical gloves and maintain the sterility of the operational area and instruments throughout the procedure.
Electrocardiographic (ECG) monitoring allows identification of rhythm abnormalities during pericardiocentesis; these are usually represented by ventricular ectopics that may occur when the needle or the catheter touches the epicardial surface of the heart. The amplitude of the ECG complexes tends to increase as soon as the pericardial fluid drainage is started, reaching a normal amplitude after successful completion of the procedure. Some clinicians prefer to perform the procedure under ultrasound guidance, in order to visualise the penetration of the needle in the pericardial sac and assess the amount of residual fluid during drainage. However, ultrasonographic guidance is not crucial for pericardiocentesis and it requires additional precautions to maintain the sterility of the surgically prepared area and operator’s hands.
Anecdotal recommendations advocate a rapid intravenuous infusion of an isotonic crystalloid solution prior to pericardiocentesis in an attempt to restore the systemic blood pressure. However, it is unclear whether this intervention is really beneficial, since most of the infused fluid may be retained within the venous bed due
to the reduced venous return caused by cardiac tamponade.
A clotting profile should be considered prior to pericardiocentesis in all cases when rodenticide poisoning cannot be completely ruled out in the patient’s history.
Where and how to insert the needleSeveral different pericardiocentesis techniques are possible depending on personal preference and the equipment available. The general principles behind them are similar and are discussed below, with three specific techniques described later in more detail.
■■ Regardless of the chosen pericardiocentesis technique, the needle needs to be inserted at the level of the 5th or 6th right ventral intercostal space (Figure 3).
■■ Before inserting the needle, local anaesthetic (e.g. lidocaine) is infiltrated under the skin at the insertion point.
■■ After approximately one minute, an equal volume of local anaesthetic is injected deeper, at the level of the intercostal muscles and parietal pleura (Figure 4A).
■■ A small stab incision is made through the skin with a No. 11 scalpel blade (Figure 4B).
■■ The needle is then inserted through the
Table 1: Pericardiocentesis equipment checklistPlain tube A: for monitoring signs of clotting; plain tube B: for laboratory biochemistry; plain tube C: for bacterial culture; EDTA tube: for cytological evaluation; (*) injectable lidocaine; (**) as shown in Figure 8
Technique 1(Intravenous catheter)
Technique 2(urinary catheter)
Technique 3(Seldinger wire)
Surgical gloves
Surgical drape
Scrubbing set
Scalpel blade (No. 11)
14 or 16G 5” intravenous catheter
2 ml syringe with 23G needle
Injectable local anaesthetic (*)
20 or 30 ml Luer lock syringe
3-way stopcock
IV fluid extension line
Kidney dish
Graduated collecting vessel
Plain tube A
Plain tube B
Plain tube C
EDTA tube
Self-adhesive plaster
Urinary catheter
Pericardiocentesis set (**)
Figure 3: The ideal point of needle insertion for pericardiocentesis in dogs and cats is indicated with an asterisk (*). The needle is inserted at the 5th or 6th right ventral intercostal space (costochondral junction) and advanced through the pleural triangle (often called the cardiac notch) where there is no lung tissue between the needle tip and the heart
small stab incision, perpendicular to the chest wall, and subsequently slowly advanced medially and slightly dorsally (Figure 4C). The needle should advance smoothly without finding any significant resistance until the pericardium, the perforation of which is felt as a small “popping” sensation, like perforating a paper sheet; the fingers may sense a distinct “give” when the needle penetrates the pericardial sac.
■■ Pericardial perforation is usually followed by a slow flow of bloody fluid through the hub of the needle. If the tip of the needle touches the epicardium, the needle hub will move rhythmically with the heart beat and usually causes ventricular ectopics visible on the ECG trace.
■■ A small sample of fluid can be placed into a plain tube to monitor for signs of clotting. To perform this test, it is sufficient to turn the tube upside down every 30 seconds for 2–3 minutes. Blood that has been present in the pericardial space for even a short time should be defibrinated and should not clot. Clotting blood suggests that the needle has either inadvertently entered a cardiac chamber or has caused epicardial injury; therefore the needle should be withdrawn slightly.
■■ Another simple technique for differentiating bloody pericardial fluid from blood is to measure the fluid PCV and compare it with venous blood PCV. Blood PCV will be significantly higher than pericardial fluid PCV.
■■ Samples for biochemical and cytological analysis should also be collected at this stage.

16 | companion
How to perform pericardiocentesis
Technique 1 (over-the-needle intravenous catheter)■■ The equipment needed is listed in
Table 1.■■ Additional side holes can be made in
the intravenous catheter with the scalpel blade prior to its insertion, to increase the suction capacity and fluid flow (Figure 5).
■■ After needle insertion into the pericardial sac, fluid (usually bloody) starts flowing through the needle hub (Figure 6A, B & C). Fluid samples are collected for monitoring clotting and other laboratory tests.
■■ A kidney dish should be positioned underneath to collect the initial flow of fluid. In some cases, the pressure of the pericardial fluid is not sufficient to cause a spontaneous flow and gentle suction with a 2 ml syringe might be necessary to verify the presence of the needle in the pericardial sac.
■■ At this point, the stylet is held firmly with two fingers while, using the opposite hand, the catheter is slid gently a few centimetres over the stylet into the pericardial sac.
■■ The stylet is then removed and an extension set attached to the catheter (Figure 6D & E).
■■ A three-way stopcock is subsequently attached to the other end of the tube (Figure 6F).
■■ The second port will be connected to the syringe and the third port will be positioned above the collecting vessel. The port connected to the syringe will be open at all times. The port connected to the patient will be open during suction. Once the syringe is filled with fluid, the patient port is closed and the plunger of the syringe is pushed to empty the fluid into the graduated collecting vessel.
■■ The cyclic suctions should continue until there is no more fluid flowing in the syringe. At this point, gentle small advancements and withdrawals of the catheter may allow removal of residual fluid pockets.
■■ At the end of the procedure, the catheter is slowly withdrawn with gentle rotatory movements.
■■ The amount of fluid that can be drained depends on several factors, including the size of the patient and the severity and duration of the underlying condition. This can vary from 10–20 ml in a cat to more than one litre in a large breed dog (Figure 6G).
■■ After the procedure, an ultrasonographic assessment can reveal if the pericardiocentesis has been successful or whether there is significant residual PE that may warrant a second intervention.
BA CFigure 4: (A) A small amount of local anaesthetic is infiltrated under the skin and deeper, at the level of the intercostal muscles and parietal pleura, at the insertion point. (B) A small stab incision is made through the skin with a No. 11 scalpel blade. (C) The catheter is inserted through the incision, perpendicular to the chest wall, and directed medially and slightly dorsally
B
A
CFigure 5: How to create side holes in an intravenous catheter. (A) A 14G 5.25” intravenous catheter; (B) and (C) 2–3 side holes are created with a No. 11 scalpel blade. This will increase the suction capacity and fluid flow

companion | 17
■■ Marked abdominal effusions can also be drained following pericardiocentesis. However, ascites normally resolves spontaneously in a day or two following the normalisation of the cardiac preload.
■■ There is no need to suture the skin at the level of the stab lesion; however, a small adhesive dressing can be placed to avoid further bleeding and reduce the risk of post-procedure infections.
Technique 2 (urinary catheter)This technique can be considered for large breed dogs where the catheter may not be long enough to remain in situ as the pericardial sac shrinks as a result of fluid drainage. It helps to increase the rigidity of the catheter, which may otherwise be compressed by the intercostal muscles. The technique can be easily performed by inserting a sterile urinary catheter through an intravenous catheter (or needle) inserted as described above.
■■ The equipment needed is listed in Table 1.
A
C
E
B
D
F GFigure 6: Over-the-needle intravenous catheter technique. (A) Skin incision. (B) Catheter and stylet are introduced through the skin incision. (C) Pericardial fluid flowing through the stylet hub. (D) The stylet is withdrawn, leaving only the catheter in the pericardial space. (E) An intravenous giving set extension tube is connected to the catheter. (F) Pericardial fluid is pumped into a collecting jar using a 3-way stopcock attached to a 20 ml Luer lock syringe. (G) Pericardial fluid collected after successful pericardiocentesis in an 8-year-old male neutered German Shepherd Dog
■■ It is good practice, before starting the procedure, to verify that the urinary catheter is thin enough to pass freely through the catheter/needle.
■■ Once the urinary catheter is in the pericardial sac, the needle can be removed and the catheter can be connected to the three-way stopcock (Figure 7).
■■ The procedure is then continued as described for the IV catheter technique.
The major advantage of using a urinary catheter is that it will stay in the pericardial sac even after its reduction in size following drainage. Furthermore, the catheter tip is very smooth and rarely causes damages to the epicardium even after several ‘to-and-fro’ movements.
Technique 3 (Seldinger wire)There are several commercial pericardiocentesis kits available based on the Seldinger technique. One of these kits is shown in Figure 8.
■■ The needle is placed as described above. Once it has penetrated the
A
B
CFigure 7: Urinary catheter technique. (A) A sterile urinary catheter is inserted through an intravenous catheter (or a long needle) and advanced in the pericardial space. (B) Pericardial fluid starts flowing into the catheter; (C) The catheter is connected to a 20 ml syringe through a 3-way stopcock
Figure 8: Pericardiocentesis set based on Seldinger wire technique. (A) Skin scrubbing pads; (B) scalpel blade; (C) needle; (D) dilator; (E) catheter; (F) guide wire; (G) Luer lock syringes; (H) three-way stopcock; (I) collecting bag; (J) suture material

18 | companion
How to perform pericardiocentesis
pericardial sac (Figure 9A), the flexible tip of the guide wire is advanced through the needle into the pericardial space (Figure 9B).
■■ The needle is then withdrawn (Figure 9C) and replaced with a soft, multi-side hole catheter (Figure 9D) which is advanced over the guide wire with a gentle rotatory movement through the skin and into the pericardial space (Figure 9E).
■■ An instrument called a ‘dilator’ is available in these kits to dilate the needle track, although this operation is often unnecessary due to the previous stab incision with the scalpel blade and the rigid tapered nature of the catheter.
■■ Once the catheter is in position, the guide wire is removed (Figure 9F) and fluid is aspirated as described for the other techniques above (Figure G, H & I).
Potential complicationsComplications are uncommon but may include laceration of a coronary artery, perforation of the right atrium or right ventricle, and pneumothorax secondary to lung lesions. Ventricular arrhythmias and atrial fibrillation are occasionally observed but they are usually self-limiting and spontaneously reversible. Dissemination of tumorous cells in the chest cavity and rapid relapse of fluid accumulation, even within minutes or hours, is expected in cases of malignant PE, especially when caused by cardiac haemangiosarcomas.
Pericardiocentesis is an essential therapeutic technique for the small animal practitioner, as removal of even a small volume of pericardial fluid can alleviate cardiac tamponade dramatically, improving right-sided cardiac function. Ultimately the success of the procedure depends on the cause of the PE, which determines the long-term prognosis. ■
Figure 9: Seldinger wire pericardiocentesis technique. (A) Needle insertion. (B) A guide wire is fed through the hub of the needle. (C) The needle is withdrawn, leaving the guide wire in the pericardial space. (D) Multi-side hole catheter. (E) The side hole catheter is advanced over the guide wire into the pericardial space. (F) Once the side-hole catheter is in position, the guide wire is removed. (G) Fluid is flowing through the hub of the catheter. (H) The hub of the catheter is connected to an IV extension tube. (I) The other end of the tube is connect to 20 ml Luer lock syringe via a 3-way stopcock for suction
A B
C D
E F
G H
I

For more information or to book your course
www.bsava.com
Learn@Lunch webinarsThese regular monthly lunchtime (1–2pm) webinars are FREE to BSAVA members – just book your place through the website in order to attend. The topics will be clinically relevant, and particularly aimed at vets and nurses in first opinion practice. There will be separate webinar programmes for vets and for nurses. This is a great MEMBER BENEFIT.
Coming soon … ■ Triage of the emergency case – webinar for nurses,
17 October ■ Lameness in young dogs – webinar for vets,
7 November ■ What to say to a grieving owner
– webinar for nurses, 14 November
All prices are inclusive of VAT. Stock photography: Dreamstime.com. © Alptraum; © Alterfalter; © Lena Andersson
Surgery of the pelvis4 DecemberDesigned for general practitioners, offering a clinically relevant approach to the diagnosis and decision making
SPEAKER
Kevin Parsons
VENUE
Woodrow House, Gloucester
FEES
BSAVA Member: £227.00Non BSAVA Member: £340.00
Crusty canines and festering felines6 NovemberEnjoy greater confidence with diagnosis and treatment of dermatology cases. Includes a practical cytology workshop
SPEAKER
Natalie Barnard
VENUE
Crabwell Manor, Chester
FEES
BSAVA Member: £227.00Non BSAVA Member: £340.00
Infectious diseases of the rabbit20 NovemberA cutting-edge day course for veterinary surgeons treating rabbits in practice
SPEAKER
Emma Keeble
VENUE
Woodrow House, Gloucester
FEES
BSAVA Nurse Member: £227.00Non Member: £340.00

“By all means let’s be open-minded, but not so open-minded that our brains drop out.”
Richard Dawkins
Congress · 4–7 APRIL 2013
20 | companion
Lord Robert Winston provided the BSAVA Special Lecture this year. So how do we top a Lord? Well, how about with a ‘god’? For this is how The Telegraph newspaper described
author and evolutionary biologist Richard Dawkins – “the god of atheism”.
Although Dawkins is a prolific writer who first came to prominence with his 1976 book The Selfish Gene, it is his strident manifesto for secularism, The God Delusion, that now finds him so frequently called upon for comment – and often causing controversy.
Taking up the baton passed by the likes of Lord Winston, Susan Greenfield and Phil Hammond – Dawkins is in prestigious scientific company as our special speaker for the BSAVA lecture, sponsored in 2013 by Anistel. This takes place on the Thursday afternoon of Congress in Hall 1, with a capacity for a 1500 audience (the exhibition stays open during the lecture). The lecture is open to anyone with a Congress badge. The event generates a huge amount of publicity and showcases Congress as an important
venue for scientific excellence.Along with Stephen Hawkins, Dawkins is
one of the few scientists that members of the public can easily name, in part due to his willingness to engage in academic and media debates. Dawkins was born in Nairobi in 1941 where his father worked for the British colonial service. He returned to Britain after the War to grow up on the family’s estate
farm. He studied zoology at Balliol College, Oxford, where he was tutored by Nobel
Prize-winning ethologist Nikolaas Tinbergen, graduating in 1962. He received his MA and DPhil degrees by 1966, and remained a research assistant for another year, when his research concerned models of animal decision-making.
DAWKINS’ ACHIEVEMENTS
In additi on to the Internati onal Cosmos Prize, Professor Dawkins’ awards have included the Silver Medal of the Zoological Society of London (1989), the Royal Society’s Michael Faraday Award (1990), the Nakayama Prize for Achievement in Human Science (1990), the Kistler Prize (2001), the Shakespeare Prize (2005), the Lewis Thomas Prize (2007), Galaxy Award 2007 for Best Author and Audible Download Book of the Year (for The God Delusion) and the Karlheinz Deschner Award (2007), the same year he was honoured by Time Life as one of the 100 most infl uenti al people. He has honorary doctorates in both literature and science, and is a Fellow of the Royal Society of Literature as well as a Fellow of the Royal Society.
He has since been an assistant professor of zoology at the University of California, Berkeley, and a lecturer and reader in zoology at the University of Oxford. In 1995 he was appointed Simonyi Professor for the Public Understanding of Science, a position that had been endowed by Charles Simonyi with the express intention that the holder “be expected to make important contributions to the public understanding of some scientific field”, and that its first holder should be Richard Dawkins.
Since 1970 he has been a fellow of New College. He has delivered a number of inaugural and other lectures – and it is a going to be a treat for delegates to hear him speak at Congress in April 2013. Afterwards, delegates attending the talk are encouraged back over to the NIA for drinks at the Welcome Reception.
The BSAVA lecture is one of the many additional social events taking place next year – Party Night is always a huge draw, and makes Congress a great place to meet and make friends, as well as access the very best veterinary science. ■
The Special Lecture at BSAVA Congress 2013 is being presented by one of the foremost names in British science
Talking Dawkins

companion | 21
Congress · 4–7 APRIL 2013Congress · 4–7 APRIL 2013Congress · 4–7 APRIL 2013Congress
television crew from the programme “It’s me or the dog” arrived for a ‘recce’ at the practice where he was working as the night vet. None of his colleagues was particularly keen to appear before the camera, so the 1995 Edinburgh graduate volunteered to give it a try. Although the sequence filmed that day wasn’t used, the director had noted how comfortable he looked in the new role and asked him to appear in a later programme in the series.
That led to regular invitations to pass on his knowledge on the BBC Breakfast programme, the Paul O’Grady show and a range of television shows both in the UK and, on occasions, in the United States. He is also in demand as a speaker on local and national radio and as a correspondent for a number of pet magazines, and has had two books published.
Lest anyone thinks this is a path to riches, Marc points out that most of his appearances in the media have been poorly paid, or entirely unpaid, and taking time off from his clinical duties meant that he was often losing money. Yet the work is rewarding in other ways. “I got the bug after that first encounter with the television crew. I realised what a fantastic
Getting chased off the premises by a group of heavies while on a covert mission filming the welfare conditions at a Ukrainian
zoo – now that wouldn’t be a typical day’s work for most veterinary surgeons.
This was hardly a routine task for Marc Abraham, either. These days he can normally be found practising his surgical skills on the cat and dog population at Grove Lodge Vets’ Southwick clinic. But he has also carved out a career as one of the country’s most prominent media vets and that incident was just one of his adventures since discovering that he has a talent for communicating with pet owners through their television screens.
Marc will be sharing his thoughts on how to get the right messages across to clients during a management session at BSAVA Congress in Birmingham next April.
He will tell colleagues that they don’t need to have natural flair or extensive training to raise the public profile of their practice.
“I will be talking about public relations, which is something that the profession has traditionally tried to steer clear of. If they try at all, then it is often something that often they don’t do particularly well.”
Being a good communicator does help but having passion for your vocation is what matters most, he says. “If, as vets and VNs, we genuinely care about animals and the way that they are looked after, then we just get on with it – and try to put those messages across.”
Surprising secondary careerMarc was already writing a regular weekly column on pet care issues for the local newspaper when he got his break in broadcasting. In 2006, a Channel 4
Professions needs to get proud about PR
As part of the comprehensive and compelling management programme at Congress, Marc Abraham will be talking about how everyone can contribute to the practice’s communications strategy

22 | companion
Congress · 4–7 APRIL 2013
Professions needs to get proud about PR
opportunity this gives to connect with a huge number of people all at once and try to put over simple but important points about animal welfare.”
Reluctant heroesMarc believes that many practitioners miss the opportunity to reach out to the public through the media because they don’t really understand what qualifies as news or how to go about publicising a news story. “But we are very lucky; much of what we do is news as far as a local newspaper audience is concerned. If you remove an unusual foreign body from a dog’s gut, rescue a kitten that has got itself stuck somewhere or take in an orphaned fox cub, then those are terrific picture stories for a local newspaper.”
He will pass on a few tips on how to go about preparing a press release or to use the work of the practice as material for a regular column. The local newspaper can also be encouraged to carry stories about the practice based on its marketing activities.
Marc believes that many practitioners are reluctant to consider marketing activities that they fear will be expensive and provide intangible results. This is not necessarily the case, he says, indicating that his practice’s modest investment in sponsoring a local boys’ football team has produced a lot of positive media coverage and generated considerable goodwill in the area. He points out that the younger generation is a key audience for the welfare messages that all practices are trying to convey and so they should seize upon any opportunity to give talks in schools.
Marc was recently awarded the CEVA award for his contribution to animal welfare for his media work, as a patron of several welfare charities and for his efforts in support of the campaign against puppy farming and other forms of animal welfare abuse.
This is in itself superb PR – Mark says
THREE DAYS OF ESSENTIAL MANAGEMENT
After the success of the two days of management lectures at Congress 2012, delegates asked for a couple of changes – lose the management marquee and relocate somewhere else in the NIA, and add in even more lectures of the same quality. We listened – so in 2013 there will be three days of management talks in the comfort of the Olympian Suite (downstairs in the NIA). Being in the NIA means you can easily get to the exhibition as well as the lectures, and you still have the Sunday free to do a proper tour and see all that’s on offer.
Here is a taste of what you can expect from the expanded Management Programme. For details and to register visit www.bsava.com or email [email protected] if you have any questions.
Thursday■■ Brian Faulkner – Understanding and managing values, beliefs and opinions as the basis of
leadership■■ Brian Faulkner – What is emotional intelligence and how can we use it to deliver customer
satisfaction?■■ Brian Faulkner – Pyschology of confidence, achievement and success in veterinary practice■■ Rosie Allister – Wellbeing in the vet profession: what do we know and why does it matter?■■ Rosie Allister – New graduates: approaches to reducing attrition and improving performance
through understanding wellbeing■■ Rosie Allister – Mentoring in practice
Friday■■ Peter Heathcote – Our cultural journey from zero to hero■■ Mark Abraham – PR the clever way■■ David Hinton – Using your PMS data to improve your practice performance■■ David Hinton – Have a better business with what you have now■■ Richard Holmes – The Specsavers corporate view of marketing messages■■ Richard Holmes – The corporate view: consumer-centred communication■■ Richard Holmes – The corporate view: making your brand LIVE■■ Darren Mackintosh – Fit for practice: how running an award-winning health club helps me run
our veterinary practice
Saturday■■ Alex German – Setting up an obesity clinic■■ Monica Augusto – Setting up a diabetes clinic■■ Neil Burton – Setting up an arthritis clinic■■ Brian Sharp – Setting up a physiotherapy clinic■■ Tobias Grave – setting up an emergency clinic■■ Luke Gamble – Setting up a travel clinic■■ Martha Cannon – Setting up a cat-friendly clinic■■ Laura Blackwood – Setting up an oncology clinic
that there are plenty of other awards schemes at a local level which a PR-savvy practice should consider entering as a low-cost and potentially high-reward method for promoting its work.
So, adopting a professional approach to PR will help to safeguard the health of the business, as well as raising the welfare standards for the neighbourhood pet population. But it will also serve to counter the one recurring bad news story which all
practitioners will have read about – the claim that veterinary services are expensive. “If you are seen to be engaging with the people in your area, I think that becomes much less of an issue. Clients do not mind spending money because they know about the work that you do, not just during that particular consultation but throughout the year. It is all about becoming the veterinary voice of your community.” ■

companion | 23
Nursing requirements for exotic pets
Within the last 10 years, the variety of animals seen in general practice has increased alongside owner expectations. Molly Varga and Rachel Lumbis, co-editors of the new BSAVA Manual of Exotic Pet and Wildlife Nursing with Lucy Gott, describe some of the specialist nursing requirements of the more exotic pets
The increase in the number of exotic pets seen in practice places a responsibility on both veterinary surgeons and nurses to apply their skills and knowledge effectively to the
management of less familiar species. Even popular exotic pets, such as rabbits, have significantly different nursing requirements to those of dogs and cats.
On the face of it, these three cases studies present very similar veterinary and nursing challenges. The goal for each case is the same – to support the animal through its illness and restore it to health. However, the manner in which this goal is achieved is different for each species.
CASE STUDY 1 – MILO
Milo is a 14-year-old cat. She has chronic renal failure and requires both fluid therapy and assisted feeding.
■■ Current bodyweight is 3 kg■■ Fluid requirements – Milo is 10% dehydrated. She
requires 300 ml [10(%) x 3(kg) x 10] over 48 hours to replace the fluid deficit. Her maintenance fluid requirement is 150 ml [50(ml) x 3(kg)] per day. Total fluid requirement is 300 ml per day (12.5 ml/hour) plus 4 ml/kg per episode of vomiting (ongoing losses)
■■ Resting energy requirement is 160 kcal/day [(30 x 3(kg)) + 70]
CASE STUDY 2 – HERBIE
Herbie is a 4-year-old rabbit. He is in gut stasis.
■■ Current bodyweight is 3 kg■■ Fluid requirements – Herbie is apparently 5%
dehydrated; however, his gut contents appear very doughy, suggesting that the dehydration is probably 10%. He requires 300 ml [10(%) x 3(kg) x 10] over 48 hours to replace the fluid deficit. His maintenance fluid requirement is 210 ml [70(ml) x 3(kg)] per day. Total fluid requirement is 360 ml per day (15 ml/hour) plus 4 ml/kg for ongoing losses
■■ Basal energy requirement is 158 kcal/day [70 x (3(kg))0.75] multiplied by an illness factor of 1.25. He requires 197 kcal/day
CASE STUDY 3 – FRED
Fred is an African Grey parrot. He presented with vomiting and his condition is deteriorating. He has hypocalcaemia. Fred requires appropriate supportive therapy.
■■ Current bodyweight is 300 g■■ Fluid requirements – Fred is approximately
5% dehydrated. He requires 15 ml [5(%) x 0.3(kg) x 10] over 48 hours to replace the fluid deficit. His maintenance fluid requirement is 100 ml/kg/day. Total fluid requirement is 37.5 ml per day (1.5 ml/hour) plus 4 ml/kg for ongoing losses
■■ Basal energy requirement is 17.55 kcal/day [78 x (0.3(kg))0.75] multiplied by an illness factor of 1.25. He requires 22 kcal/day

24 | companion
Nursing requirements for exotic pets
CatsIt has long since been recognised that cats thrive better in an environment without dogs. As a result it is now commonplace in the UK to have a dedicated cat ward within the hospital and even separate waiting rooms and treatment areas for dogs and cats. Provision of litter trays, a place to hide (e.g. can be as basic as a towel draped across the front of the cage) and familiar foods are all key to encouraging normal feeding and toileting behaviour in hospital. Cats are tolerant (to an extent!) of intravenous fluid provision and repeat injections or oral medications. Many cats will also accept supportive feeding when required. Nasogastric tubes present more of a challenge, but this can be easily overcome with the use of an Elizabethan collar.
RabbitsAs a profession, we are becoming better at recognising that rabbits (the third most popular pet in the UK) have different requirements from those of cats. These differences mainly stem from the fact that rabbits are a prey species, which is a very different concept when considering hospitalization, since the most commonly seen species in practice (i.e. dogs and cats) are predators.
Ideally, rabbits should be housed separately from predator species and preferably out of sight, sound and smell contact. However, this is often difficult to achieve without compromising the ability of veterinary staff to adequately observe inpatients. As for cats, rabbits should be provided with a place to hide within the hospital cage (a cardboard box or pieces of large plastic drainpipe are suitable) and many rabbits are trained to use a litter tray (Figure 1).
As a prey species, rabbits appear more tolerant of injections and the administration of medications; however, the effects of the stress caused by these interventions should not be ignored. Rabbits that are severely stressed have been shown to become oliguric, and this can adversely affect the provision of fluid therapy. In addition, rabbits in a hospital situation often take several hours to days to settle enough to eat normally, an activity that is crucial for the health of their gut. Veterinary staff need to be aware of these potential complications, as behavioural cues indicating
an adverse event (such as biting or vocalisation) are often not seen.
BirdsThe nursing requirements of birds differ again from those of cats and rabbits. Parrots, in particular, often bond with their owners and fare better in hospital if they can form a bond with a member of staff. Parrots are also neophobic and often suspicious of novel food items, making any dietary changes difficult.
Handling parrots is often stressful for both the animal and the member of staff. Unfortunately, due to their high metabolic rate, frequent handling is required to administer fluids and provide supportive feeding. When they are ill, birds benefit from peace and quiet; however, when they are starting to recover, they seem to enjoy the hustle and bustle of busier areas (Figure 2).
Figure 1: An indoor rabbit set-up. A hide area, tunnels for bolt holes, a hay rack and a litter tray have been provided. As large an area as possible should be provided, to allow the rabbit to exercise fully
Figure 2: A ward for avian and reptilian patients

companion | 25
From a safety perspective, parrots present several challenges. They can inflict a severe bite and their claws can inflict painful wounds. Veterinary staff need to be taught how to handle these animals safely. Birds can also spread the zoonotic infection psittacosis (caused by Chlamydophila psittaci), and the dust and down they shed can exacerbate asthma, eventually causing significant lung pathology in humans.
Comparative fluid requirementsMany principles of fluid therapy as a supportive treatment for cats can also be applied to exotic pet patients. However, it should be noted that small mammals have a significantly higher fluid requirement than cats. This is due to: higher metabolic rate; increased glomerular filtration rate; and relatively larger lung surface area, resulting in greater fluid loss via respiration. Birds also have a higher metabolic rate, and subsequently a greater fluid requirement, than cats. However, as with reptiles, birds excrete protein waste products in the form of uric acid rather than urea, which requires less water for excretion.
The anatomical and physiological differences, as well as the risk of fluid overload, in small mammals, birds and reptiles compared with dogs and cats, means that initially a more conservative infusion rate is required and that less traditional routes of fluid administration should be considered. Regardless of the species, voluntary water intake can be encouraged through the provision of an appropriate container. Advice should always be sought from the owner regarding the supply of water bottles, bowls or other alternative receptacles in the home environment.
Comparative energy requirementsWhen formulating a nutritional plan for hospitalised patients, it is important to communicate with the owner and consider the patient’s normal dietary habits at home. This is particularly important for cats, as they often favour a specific texture, flavour and consistency of food; they may also have preferences regarding the timing of meals and the position and design of food bowls.
Energy requirements in cats are calculated using the resting energy requirement. This is the amount of energy (measured in kilocalories) required for
maintaining homeostasis whilst a patient rests quietly in a stress-free, non-fasted, thermoneutral environment. Traditionally, the resting energy requirement was multiplied by an illness factor of between 1.0 and 2.0 to account for the increase in metabolism associated with different conditions and injuries. The subjective nature of such factors, combined with the potential for overfeeding, has led to the discontinuation of this practice. Current recommendations involve the use of the resting energy requirement as a baseline and modifying food intake according to changes in bodyweight and body condition score.
Small mammals, birds and reptiles have a greater surface area related to bodyweight and a higher energy expenditure than cats. In these species, the basal energy requirement (rather than the resting energy requirement) multiplied by a disease factor is anticipated to prevent weight loss and is therefore advocated. The higher metabolic rate in these animals dictates a more ad libitum feeding schedule and prolonged periods of fasting should be avoided. As with dogs and cats, it is essential to obtain a thorough dietary history and establish any preferences in relation to diet and feeding bowl. ■
NOW AVAILABLE
The BSAVA Manual of Exoti c Pet and Wildlife Nursing is the latest additi on to the series of nursing ti tles. It covers commonly kept species and takes the reader through a logical sequence: from the initi al phone call (including initi al contact advice), through to consultati on, admitt ance, hospitalisati on and interventi on. The Manual is designed to be practi cal and user-friendly, so that readers experienced in the care of dogs and cats can fi nd relevant informati on easily and apply it directly to exoti c pet and wildlife species.
Additi onal content, including client handouts, is available online to readers
Member price: £45.00Non-member price: £68.00
To purchase your copy, visit the BSAVA website at www.bsava.com or call our Membership and Customer Service Team on 01452 726700.

26 | companion
Picture perfect pets
The annual PetSavers photography competition is ready to invite your entry, so now is the time to visit www.petsavers.org.uk for full details on how to enter.
The digital photography competition organised by PetSavers has had some really creative entries in recent years, and it attracts veterinary professionals
and pet owners alike.The theme for
this year’s competition is ‘Priceless Moments’.
PetSavers is calling on vets, VNs and their pet-owning clients to snap and share those priceless moments we have with our animals
The judges will be looking for qualities such as humour and personality in the photos, as well as general photographic skill.
See what has caught the judges’ eye in the past by taking a look at last year’s winning entries (pictured), or viewing all of our previous winners by visiting our website. Many of the winning images have been made into PetSavers cards, so who knows – you might even find Rex or Felix being sent out on thousands of Christmas greetings in the future.
How to enterThe competition is in two categories; Adult (16 and over) and Junior (under 16). First prize in each category is £200 in photography vouchers, second prize is £100 in photography vouchers and third prize is £50 in photography vouchers.
The closing date is Thursday 31 January 2013. Entry to the competition could not be easier; simply email your photographs to [email protected]. An entry form, which can be downloaded from the website, must also be submitted; this can be emailed with your photograph or alternatively you can print and fax the form to us at 01452 726701.
Get the practice involvedYou can help us promote our photography competition by displaying posters and telling your clients about it. It is also a great way to introduce them to the vital work that PetSavers does to improve the quality of life and welfare of companion animals. If you would like more information about PetSavers or this competition, including terms and conditions, then email us or visit the website. n
Top: (L–R) Timmy Kettyle, 2nd prize winner in Junior Category of PetSavers Photography Competition 2012; Philip Lhermette, PetSavers Chair; Adam Philips, 1st prize winner in Adult Category of PetSavers Photography Competition 2012.Bottom: (left) Timmy Kettyle’s entry: Where did you say it went?; (right) Adam Philips’ entry: Wash behind the ears!
1st prize winner in Junior Category of PetSavers Photography Competition 2012
Other finalists in PetSavers Photography Competition 2012. Clockwise from top
left: 2nd prize winner in Adult Category; 3rd prize winner in
Adult Category; 3rd prize winner in Junior Category

companion | 27
Committed giving allows you to make a regular donation towards the work of PetSavers: donations can be made monthly, quarterly
or on an annual basis. A regular gift to PetSavers enables us to plan for the future, and in addition it is very important for any charity to have a secure fund-base.
Who are our committed givers?Many different people donate on a regular basis, including those in the veterinary profession who have received funding for training or research, and pet owners who
Immune-mediated haemolytic anaemia (IMHA) is a common cause of anaemia in dogs. The disease involves destruction of red blood cells by the dog’s own immune system. Despite increasing availability
of blood transfusions, many dogs still die from IMHA, a major cause of death being thromboembolic disease (blood clots).
Drugs to reduce blood clot formation improve survival in dogs with IMHA. One such group of drugs are the anti-platelet drugs, including aspirin and clopidogrel. These are commonly used in dogs with IMHA as they have been shown to improve survival and can be administered as once-daily tablets. The doses used are based on studies in healthy dogs and such studies have shown that individual dogs respond differently to the same dose of these drugs.
The purpose of this trial is to look at the effects of aspirin and clopidogrel, used at standard doses, in dogs with IMHA. This will mainly involve looking at the
Committed givingwant to do what they can to support PetSavers’ work to improve treatment and diagnosis for the illnesses and conditions that affect pets. Some people give in memory of beloved pets sadly lost to them.
Becoming a committed giverIf you would like to support PetSavers and become a committed giver you will need to arrange a standing order with your bank. A downloadable form is available on our website – www.petsavers.org.uk, or call Gemma White on 01452 726723 for details.
Gift AidIf you become a PetSavers committed giver we may be able to make your donations go even further. If you sign the gift aid declaration, PetSavers can claim 28p back in tax for every £1 that you have donated. This is valid for any donations made in the last six years prior to signing the declaration and for all future donations.
To be eligible to sign a gift aid declaration you must pay enough UK income tax and/or capital gains tax to cover the amount of tax the charity will reclaim. There is a gift aid declaration on the committed giving form which can be downloaded from our website, or we can arrange to send one to you. Thank you for considering this excellent way of funding our work – you can make all the difference. n
platelets of treated dogs using a technique known as impedance aggregometry. We will compare the platelets of dogs with IMHA before and after treatment and look to see how this relates to the dose of anti-platelet drug used and the survival of the dog.
This study will benefit future dogs with IMHA by enhancing our understanding of what anti-platelet drugs do in this disease and how best to monitor and adjust them. We hope this and future studies will help to reduce the mortality rate in dogs with IMHA. n
Effects of anti-platelet drugs in IMHA dogsLindsay Kellett-Gregory of the Royal Veterinary College outlines her PetSavers-funded study to assess the efficacy of currently prescribed anti-platelet drugs in reducing clot formation in IMHA
Continue reading about projects PetSavers has funded this year by reading next month’s issue of companion magazine. To find out more about applying for funding or fundraising for PetSavers, email [email protected] or call Gemma White on 01452 726723.

28 | companion
Ellen van Nierop is a Dutch vet living and working in Ecuador. She completed her studies at the Rijksuniversiteit, Ghent, Belgium. She then volunteered at wildlife centres around the world
before settling and starting work in Ecuador eleven years ago. She later met her husband, also a vet, and they set up their own small animal clinic together.
Ellen has been the Ecuadorian representative of the WSAVA for the Asociación de Médicos Veterinarios Especialistas en Pequeñas Especies (AMVEPE) since 2009 and, during that time, she’s been heavily involved in making the WSAVA relevant to vets in Ecuador. In addition to her work as a vet, Ellen has sought additional training in finance and administration and is currently a year from completing a five-year Engineer
WSAVA welcomes new board memberThe WSAVA is growing fast and expanding its activities into more and more areas. Ellen van Nierop has been appointed to strengthen the Executive Board and help it to deliver our goals
in Accounting and Auditing qualification.Commenting on her role on the WSAVA’s
Executive Board, she says: “I come eager to help and to learn and am very excited to be a part of a large international organisation that is making a difference in communication and continuous education for veterinarians. I hope to represent first line veterinarians who have political, economical, or linguistic difficulties in getting full access to continuous education in the small animal field. I wish to put my knowledge of developing countries, languages and communication skills, as well as my acquired knowledge in the administrative and financial field, to work with a group of like-minded international veterinarians who have already shown that it is possible to go beyond the limits of nationalities and circumstances towards our common ultimate goal – the wellbeing of our small animal friends.”
Welcoming Ellen, WSAVA President Peter Ihrke comments: “Ellen has been an outstanding country representative for Ecuador and shares our passion for driving the WSAVA’s work forward. We are absolutely delighted that she has agreed to join the Executive Board. Her skills as a veterinarian and linguist are matched by her understanding of finance and administration. She will be a great asset to the team.” Ellen’s appointment is subject to assembly ratification in March 2013. n
WSAVA/FASAVA 2013
We are delighted to invite all veterinarians and veterinary nurses to join your kiwi colleagues, from 6–9 March 2013 at the Sky City Conventi on Centre, Auckland. This is a once in a lifeti me opportunity to come to New Zealand and experience a world-class small animal veterinary conference at the same ti me. Registrati ons are now available – get in early to obtain the early bird specials. See you there!Pieter VerhoekChairman, Local Organising Committ eeWSAVA/FASAVA Congress 2013 Pieter Verhoek
companion | 29
At last a quiet moment to talk to WSAVA members everywhere – greetings to you all! It has been another
busy few months for the WSAVA. I’m pleased to say that we’ve been continuing our focus on the fight against rabies, with Professor Michael Day representing us at the OIE meeting in May. We gave a joint lecture on the eradication of rabies in Africa and Asia. It was well attended, showing the high level of interest in this topic. We firmly believe that the eradication of rabies is achievable and that vets must play an essential role in vaccinating at-risk dogs. Recent research from Professor Cleaveland in the UK confirms that most cases of rabies can be prevented by vaccinating 70% of free-roaming and captive dogs.
We’re also delighted to introduce our newest Board member Dr Ellen van Nierop. She’s a great addition to the team and her background in finance will be particularly valuable. Welcome Ellen!
We have developed a new look e-bulletin. Siraya Chunekamrai, our honorary secretary and PR chairperson, welcomes your feedback and stories for future issues, to be sent to [email protected].
People often ask me why we work so hard for the WSAVA. My answer is: ‘Because I love it!’ The WSAVA is a great cause and we are a wonderful family. By working together, we are changing the world and making it a better place for man and its companion animals. n
WSAVA President Peter Ihrke is recuperating from recent back surgery and sends his best wishes, so Past President Jolle Kirpensteijn shares some highlights of recent WSAVA activity
Update from the Past President
WSAVA President Dr Peter Ihrke and WSAVA Past President Professor Jolle Kirpensteijn
WSAVA/FASAVA World Congress 2013 will feature a stream on veterinary dermatology, covering a range of topics from the smelly dog to the itchy cat, led by Mike Shipstone
from Australia and Paul Bloom from the USA. This will also include an update on the surgical treatment of ear disease by Alex Walker from New Zealand.
For those with an interest in veterinary dentistry, we have Brook Niemiec from the US and Tony Caiafa from Australia. These outstanding veterinary dentists will cover periodontics, endodontics and feline dental disease.
Those interested in exotic and wildlife medicine haven’t been forgotten–David Vella from Australia will provide the essentials on managing the small mammal and reptile population, while Laurel Degernes from the USA will present some detailed topics in avian medicine.
Whatever your area of interest, we have something to please everyone. Eight consecutive streams over four days will give you ample opportunity to mix and match whatever takes your fancy. In addition there will be six State-of-the-Art lectures where experts in their fields will present the very latest research. Do not miss this opportunity to attend the greatest veterinary event to be presented in New Zealand.
Full programme available at www.wsava2013.org/programme. n
World Congress 2013 – more to look forward toRichard Jerram, Chair, Scientific Programme, continues his preview of the science that will be available in Auckland

30 | companion
Beverley Cuddy is Publisher, Editor and majority shareholder of Dogs Today magazine, after pursuing a management buy-out 20 years ago to save the magazine from closure. She had a column in the Mail on Sunday for eight years and writes for the Guardian, Times and Telegraph. She is chairman of the Tailwaggers Club Trust, a charity that helps pet owners in distress, and is a trustee with Hounds for Heroes, which aims to provide specially trained assistance dogs to injured and disabled people of both the UK armed forces and civilian emergency services. She is married to Graham Smith, MD of Loudhouse Communications, and they have three sons. They live with their dogs, Oscar a Bearded Collie, and Tess, a Dogs Trust graduate who is a working Springer Spaniel
Beverley Cuddy
the companion interview
Didn’t you even manage to shoe-horn your hobby into your history degree and design business?Somehow, I got a degree in history, but by then I was a championship show judge and had already started my first design business. At its height we produced over 100 different Bearded Collie-related lines. Yes – even my dissertation had been a bit doggy – I chose the concept of animal cruelty in Victorian Britain, pretty much the history of the RSPCA. The research had meant spending some time looking at the archives at ancient weekly show dog paper Our Dogs and they asked me to write for them, so I stumbled into journalism. A year
QTell us about your passion for dogs and how that developed into competing at Crufts.
AMy teachers despaired. I had been a promising student until I got my first Bearded Collie at age 11. I’d
met a very wonderful Beardie called Percy. I picked out Chi-Chi from one of Percy’s litters and stumbled into showing dogs quite by accident. Even handicapped by a young novice handler, Chi-Chi quickly became a champion. Her son and daughter did, too. School seemed very boring in comparison and I even played truant from two mock ‘O’ levels to compete at Cruft’s.
later I was head-hunted by their rival Dog World and I had to leave my eight Beardies with my long-suffering parents when I headed down south.
With so many dogs you must have had your fair share of visits to the vets?Just before I left home, my latest show prospect, Sally, contracted parvovirus. It was that terrible era when lots of dogs died. A very young vet, Miss Morton, had joined our local practice in St Helens. I didn’t know she was destined to be a future BVA President, but I’d have even voted for her to be Prime Minister after she helped us to save Sally’s life. We had to hydrate Sally at

companion | 31
…more recently we launched the Don’t Cook Your Dog campaign…
all charities and organisations stood shoulder to shoulder… I think this was
possibly one of our finest hours…
home by mouth. Those seven days and nights changed me forever.
How did your career progress in the pet press?A year subbing boring show reports was followed by a few more as Kennel Club’s Information Officer. I moved sideways on to the KC’s own magazine and putting a magazine together was the most fun I’d had in years. However I was coming home to an empty flat and I wanted a job where I could afford to live with my dogs. A role in corporate relations at British Telecom tripled my salary, but within a year I was bored. An advert in the Guardian for a new dog magazine changed all that. And when I discovered that the person in charge was Viscount Rothermere, the proprietor of the Daily Mail, I was excited but slightly daunted.
Tell us about your relationship with the newspaper magnetOur first meeting was interesting. I was just a young girl from Liverpool; my experience of what to say to titled media moguls was very patchy. We had a good chat about dogs and he said something I knew was wrong and I corrected him. It seemed key and after that we got along very well. He encouraged me to campaign to make life better for our best friends. Sadly, while he and I believed in what we were doing, the hundreds of people in between us in the management structure thought we were both barking mad!
I was only the editor and somehow we lost £350,000 after some very expensive TV advertising. The shareholders started to get grumpy and the decision was taken to close the magazine. It’s a long story, but I bought the magazine for £1 and Lord Rothermere decided to become a shareholder in my new company. He told me his financial advisor had told him to do it. He showed me a photo of his advisor – it was Ryu-Ma, his Akita!
Campaigning has been central to the publication; what have been the key campaigns?In the last two decades we’ve certainly kept going with the campaigns: health reforms, tailwaggers against cosmetic tail docking, introduction of pet passports, DDA reform, positive training methods, anti-battery farming puppies, pro-rescue… there’s a lot more to come. More recently we launched the Don’t Cook Your Dog campaign to press for zero tolerance of dogs being left in hot cars. The campaign quickly went global. All charities and organisations stood shoulder to shoulder. I think this was possibly one of our finest hours.
How did you get involved in Hounds for Heroes?Over the years I have heard so many amazing stories of how the love of a good dog had changed someone’s life. But none compare with Endal. In 1999 I heard a rumour that there was an assistance dog that had started using a cash machine to help his owner. Allen Parton had survived a massive head injury that wiped most of his memory. He came home in a wheelchair barely able to speak. After a couple of attempts at killing himself a Labrador called Endal had somehow made a connection and pulled Allen out of the darkest of places and restored his hope.
Endal’s practical and emotional support meant that this very special dog did a lot more than just open washing machine doors. Allen started to talk, to go to the pub, to start to enjoy the life he had, rather than mourn the one he couldn’t remember. He had no idea who his wife and children were when he came home. He looked much the same, but he was an entirely different man. Thanks to Endal, Allen regained his self-esteem. Allen and Sandra fell in love all over again and remarried. Thanks to Endal, Allen had
become the articulate and inspirational man he is today.
Allen really wanted other returning troops and injured emergency personnel to be given the chance of their own Endal effect, so he decided to start his own charity, Hounds for Heroes. I am delighted to be a trustee and to have watched Allen’s remarkable progress these last 12 years. He’s written a column in the magazine for many years, so the readers feel they’ve been with him at every turn too. If you haven’t read Allen and Sandra’s best selling book Endal, you really should! It’s quite a story. Hounds for Heroes is only three years old but it is probably the fastest-growing charity in Britain today. Two squadrons of pups are already in training.
What other dog charities are close to your heart?I’m also Chairman of an ancient charity called Tailwaggers Club Trust. They discovered me after our anti-tail docking campaign of the same name inadvertently infringed their copyright. It’s a tiny charity that really could do with more funds. It’s unique in that each case is taken on its own merits and people are at least able to tell someone about their pet-related crisis. Most often it’s people struggling to pay an unexpected vet bill after a dramatic life-changing episode. Some of the stories are heart-breaking and people have already remortgaged or sold their possessions but they still face life or death decisions. Other cases need more practical help, like the older lady who became suddenly homeless and was sleeping in her car because the local council wouldn’t let her keep her dogs while she waited for emergency housing. ■
FURTHER INFORMATION
You can fi nd out more about Beverley’s chariti es at:
■ www.houndsforheroes.com ■ www.tailwaggersclubtrust.com
For more information or to orderwww.bsava.comBSAVA reserves the right to alter prices where necessary without prior notice.
companion offer of the monthExclusive offer for companion readers – call BSAVA on 01452 726700 and quote ‘companion offer – Raptors’.
Missed this recent Manual?BSAVA Manual of Canine and Feline
Surgical PrinciplesA Foundation ManualProvides a solid grounding for the basic principles of veterinary surgery. Covers:
■ Surgical facilities and equipment ■ Preoperative and postoperative considerations ■ Surgical biology and techniques
WHAT THEY SAY“…well-craft ed, well-balanced, well-organized… a very useful additi on to any library…” JOURNAL OF SMALL ANIMAL PRACTICE (in press)
On offer while stocks lastBSAVA Manual of
Rabbit Medicine and Surgery2nd editionThis popular Manual reflects the increased understanding of rabbit health and disease. This edition includes:
■ Nursing care ■ Cardiovascular disorders
Got this in your practice library?BSAVA Manual of Canine and Feline
Advanced Veterinary Nursing2nd editionVeterinary nursing has progressed rapidly and this Manual provides practical information for those nursing at an advanced level. Includes:
■ Physiotherapy ■ Dentistry ■ Advanced imaging, including endoscopy ■ Nursing-led clinics
WHAT THEY SAY“…an excepti onally well-presented manual, which is enjoyable to read and very easy to follow...” VETERINARY RECORD
BSAVA PublicationsCOMMUNICATING VETERINARY KNOWLEDGE
BSAVA Manual of
Raptors, Pigeons and Passerine Birds
■ Commonly kept species ■ Problems seen in clinical practice ■ Husbandry, medicine and surgery ■ Formulary and laboratory reference ranges included
Offer is available to BSAVA members only. Ends 31 October 2012. Free P&P on telephone orders for UK and Eire delivery, online rates of P&P apply for overseas orders.
WHAT THEY SAY“...should fi nd its way to the library of every Veterinary Surgeon working with birds…” FALCO
BSAVA Member Price: £49.00Price to non-members: £75.00
BSAVA Member Price: £49.00 £35.00Price to non-members: £75.00 £55.00
companion offer: £54.00 £34.00Price to non-members: £85.00
BSAVA Member Price: £49.00Price to non-members: £70.00
Note: BSAVA Manual of Rabbit Imaging, Surgery and Dentistry due 2013; BSAVA Manual of Rabbit Medicine due 2014
WHAT THEY SAY“...provides a large amount of informati on you will require on a daily basis...” JOURNAL OF SMALL ANIMAL PRACTICE
■ Dentistry ■ Diagnostic imaging

companion | 33
CPD coming soon…
Wednesday 7 November 2012 (Evening meeting)Pain
■ Speaker: Matt Gurney ■ Holiday Inn, Haydock ■ Full BSAVA Members: FREE
Non BSAVA Members: £24 inc. VATSunday 9 December 2012 (Day meeting)Collapse!
■ Speaker: Rebecca Litt ler ■ Swallow Hotel, Preston ■ Full BSAVA Members: £180 inc. VAT
Non BSAVA Members: £300 inc. VATTuesday 19 February 2013 (Evening meeting)Immunology
■ Speaker: Nat Whitley ■ Holiday Inn, Chester ■ Full BSAVA Members: FREE
Non BSAVA Members: £24 inc. VATWednesday 6 March 2013 (Evening meeting)Avoiding an RCVS complaint
■ Speaker: John Hird ■ Holiday Inn, Haydock ■ Full BSAVA Members: FREE
Non BSAVA Members: £24 inc. VATThursday 19 September 2013 (Evening meeting)Avian emergencies
■ Speaker: Molly Varga ■ Brockholes Nature Reserve, Preston ■ Full BSAVA Members: FREE
Non BSAVA Members: £24 inc. VATTuesday 12 November 2013 (Evening meeting)Spinal surgery
■ Speaker: Turlough O’Neil ■ Holiday Inn, Haydock ■ Full BSAVA Members: FREE
Non BSAVA Members: £24 inc. VATWednesday 4 December 2013 (Day meeting)Cardiac disease including practical ultrasound
■ Speaker: Simon Swift ■ David Lloyd Club, Chorley ■ Full BSAVA Members: £180 inc. VAT
Non BSAVA Members: £300 inc. VAT
WHO’S WHO ON NORTH WEST COMMITTEE
■ Chair: Rebecca Litt ler ■ Treasurer: Neale Roach ■ PetSavers: Ruth McElroy ■ Committ ee Member: Simone der Weduwen
Focus on...BSAVA North West Region
MEMBERS: don’t forget to bring a valid BSAVA membership card to the meeting!
Please visit www.bsava.com for further information on prices and course content. ■
The team in BSAVA’s North West region is always keen to hear what local colleagues want in terms of CPD – so please email your ideas to [email protected] with
your suggestions on topics and speakers – and to find out about getting involved and helping to design the delivery of CPD in your area.
Regional committees help to provide local and regional day and evening courses aimed at the practitioner looking to update their current knowledge and techniques, and provide opportunities to meet neighbouring colleagues. We are always looking for fresh faces to assume positions within regional committees. Committee members generate ideas, including how and where courses are delivered and which speakers are invited.
Getting involved gives you the capability to shape regional CPD and meet new people. There are a range of benefits available to committee members such as complimentary BSAVA Congress registration, the opportunity to attend other regions’ CPD throughout the country and the knowledge that you are helping to shape the future of your profession.
So far in 2012 North West has had a truly mixed bag of meetings. The two evening meetings – Rebecca Littler on diabetes and Victoria Roberts on chicken medicine – were fantastically successful and extremely well attended. Sadly, this was not continued into the spring day-long meeting in Haydock where Turlough O’Neill was to speak on fracture repairs. Due to lack of pre-registrations we had to postpone that event, but we plan to hold the course in 2013, as it promises to be an excellent meeting.
As regards the venues that we select – these are chosen with the thought in mind that we are shaped like a tall box as our region runs from Cumbria down to Staffordshire; so we try to use three venues, as this allows all of our BSAVA members the opportunity to get to at least two meetings without a significant journey. However, please let us know if we are missing out on a good venue or location, so that we can continue to serve our members as best we can. ■
CPD coming soon…
Wednesday 7 November 2012 (Evening meeting)
Speaker: Matt GurneyHoliday Inn, Haydock

34 | companion
CPD diary
EVENING WEBINAR
Wednesday 3 October 20:00–21:00Advanced reptile medicineSpeaker: Joanna HedleyOnlineDetails from [email protected]
EVENING WEBINAR
Thursday 18 October 20:00–21:00Coughing dogs and catsSpeaker: Mike MartinOnlineDetails from [email protected]
DAY MEETING FOR NURSES
Tuesday 2 OctoberNursing reptiles: keeping everything to scaleSpeaker: Matthew RendleBlackpool Zoo, FY3 8PPDetails from [email protected]
EVENING MEETING – NORTH WEST REGION
Thursday 4 OctoberUse of steroids in otitisSpeaker: Sue PatersonHoliday Inn Chester South, Wrexham Road, Chester CH4 9DLDetails from [email protected]
EVENING MEETING – NORTHERN IRELAND REGION
Thursday 4 OctoberCanine pancreatitis: an update on causes, diagnosis and treatmentSpeaker: Penny WatsonStormont Hotel, Upper Newtownards Road, Belfast BT4 3LPDetails from [email protected]
DAY MEETING – METROPOLITAN REGION
Tuesday 23 OctoberNeurology back to basicsSpeaker: Laurent GarosiThe Kennel Club, 1–5 Clarges Street, Piccadilly, London W1J 8ABDetails from [email protected]
EVENING MEETING – SOUTH WALES REGION
Tuesday 23 OctoberTortoises: tips and tricks to become an expertSpeaker: Mike JessopCarmarthen Veterinary Centre SA31 3SADetails from [email protected]
DAY MEETING
Thursday 25 OctoberOld bugs and new bugs: what do I need to know about infectious disease in cats?Speaker: Samantha TaylorBSAVA Headquarters, Woodrow House, Gloucester GL2 2ABDetails from [email protected]
EVENING MEETING – MIDLAND REGION
Tuesday 16 OctoberPitfalls in interpretation of in‑house laboratory resultsSpeaker: Joy ArcherYew Lodge Hotel, 33 Packington Hill, Kegworth, Derby DE74 2DFDetails from [email protected]
EVENING MEETING – KENT REGION
Thursday 18 OctoberOrthopaedic diseases of the carpusSpeaker: Christopher StorkBest Western Russell Hotel, 136 Boxley Road, Maidstone ME14 2AEDetails from [email protected]
EVENING MEETING – SOUTH WEST REGION
Tuesday 9 OctoberPassport perils: update on PETS scheme, leishmaniasis and other imported diseasesSpeaker: Séverine TaskerAztec Hotel and Spa, Aztec West Business Park, Almondsbury, Bristol BS32 4TSDetails from [email protected]
EVENING MEETING – SOUTH WALES REGION
Wednesday 10 OctoberQuiz night with the BSAVA PresidentThe Unicorn Inn, Church Road, Llanedeyrn, Cardiff CF3 9YADetails from [email protected]
DAY MEETING – SURREY AND SUSSEX REGION
Thursday 11 OctoberAn update on feline endocrinologySpeaker: Martha CannonHoliday Inn, Povey Cross Road, Gatwick RH6 0BADetails from [email protected]
October 2012
EVENING MEETING – SOUTH WEST REGION
Tuesday 16 OctoberFilm readingSpeakers: Esther Barrett and Chris Warren-SmithKingsley Village, A30, Penhale, Fraddon, Cornwall TR9 6NADetails from [email protected]
EVENING MEETING – SOUTH WEST REGION
Thursday 18 OctoberFilm readingSpeakers: Nic Hayward and Kate BradleyCommunal Building, School of Veterinary Science, University of Bristol, Langford, North Somerset BS40 5DUDetails from [email protected]
DAY MEETING
Thursday 4 OctoberCoughing in the dog and catSpeaker: Mike MartinUplands House, High WycombeDetails from [email protected]
DAY MEETING
Tuesday 9 OctoberCanine developmental elbow diseaseSpeaker: Noel FitzpatrickBSAVA Headquarters, Woodrow House, Gloucester GL2 2ABDetails from [email protected]
DAY MEETING – SOUTH WEST REGION
Friday 5 and Saturday 6 OctoberImaging the emergency and critical care patientSpeakers: Nicolette Hayward, Ross Doust, Federica Corletto, Esther Barrett, Andrew ParryClifton Pavilion, Bristol Zoo Gardens, Clifton, Bristol BS8 3HADetails from [email protected]
EVENING WEBINAR
Monday 8 OctoberCanine infectious diseasesSpeaker: Patricia IbarrolaOnlineDetails from [email protected]

companion | 35
EVENING WEBINAR
Tuesday 12 NovemberOld bugs and new bugs: what do I need to know about infectious disease in cats?Speaker: Samantha TaylorOnlineDetails from [email protected]
EVENING WEBINAR
Tuesday 20 NovemberCrusty canine and festering felineSpeaker: Natalie BarnardOnlineDetails from [email protected]
November 2012
DAY MEETING – SCOTTISH REGION
Sunday 28 OctoberDiagnostic imaging: interactive and case‑based abdominal and thoracic imaging, primarily radiographySpeaker: Gawain HammondDunkeld Hilton Hotel, Perthshire PH8 0HXDetails from [email protected]
EVENING MEETING – SOUTH WEST REGION
Wednesday 14 NovemberClinical pathologySpeaker: Kathleen TennantCanalside, Huntworth, Bridgwater, Somerset TA7 0AJDetails from [email protected]
OTHER UPCOMING BSAVA CPD COURSESSee www.bsava.com for further details
■■ BSAVA Education Tuesday 4 December Decision making for the hips and pelvis
■■ Midland Region Wednesday 5 December Evidence-based management of renal failure
■■ South Wales Region Wednesday 6 December Liver disease
■■ Kent Region Thursday 6 December Christmas Referrals Fair. Not just skin deep: cutaneous manifestations of systemic disease
EXCLUSIVE FOR MEMBERSExtra 10% discount on all BSAVA
publications for members attending any BSAVA CPD event.
All dates were correct at time of going to print; however, we would suggest that you contact the organisers for confirmation.
DAY MEETING – SOUTHERN REGION
Thursday 25 OctoberA practical guide to in‑house cytology including urinalysisSpeaker: Balazs SzladovitsPotters Heron Hotel, Ampfield, Romsey, Hampshire SO51 9ZFDetails from [email protected]
DAY MEETING
Tuesday 6 NovemberCrusty canines and festering felinesSpeaker: Natalie BarnardCrabwall Manor, ChesterDetails from [email protected]
EVENING MEETING – NORTHERN IRELAND REGION
Thursday 1 NovemberWound managementSpeaker: Georgie HollisVSSCo, Lisburn BT28 2SADetails from [email protected]
EVENING MEETING – KENT REGION
Wednesday 7 NovemberDentistry in rabbits and rodentsSpeaker: Cedric TuttBest Western Russell Hotel, 136 Boxley Road, Maidstone ME14 2AEDetails from [email protected]
EVENING MEETING – SOUTH WALES REGION
Wednesday 7 NovemberNasal diseaseSpeakers: Nic Hayward and Kit SturgessThe International Legacy Hotel, Cardiff CF15 7LDDetails from [email protected]
EVENING MEETING – MIDLAND REGION
Thursday 8 NovemberInterpretation of abdominal ultrasound imagesSpeaker: Andrew ParryWolverhampton Medical Institute, New Cross Hospital, Wolverhampton, West Midlands WV10 0QPDetails from [email protected]
EVENING MEETING – SOUTHERN REGION
Thursday 22 NovemberChronic vomiting and diarrhoea in cats: a practical approach to investigation and treatmentSpeaker: Martha CannonBeechdown, Beechdown Park, Winchester Road, Basingstoke RG22 4ESDetails from [email protected]
EVENING MEETING – SCOTTISH REGION
Thursday 22 NovemberKeep calm and carry on: seizure management in dogsSpeaker: Annette WessmanGlasgow University Vet SchoolDetails from [email protected]
DAY MEETING – SOUTH WEST REGION
Thursday 22 NovemberMedical and surgical management of canine lower urinary tract diseaseSpeakers: Ian Battersby and Ronan DoyleAlveston House Hotel, Alveston, Thornbury, Bristol BS35 2LADetails from [email protected]
DAY MEETING – SOUTH WEST REGION
Friday 23 NovemberMedical and surgical management of canine lower urinary tract diseaseSpeakers: Ian Battersby and Ronan DoyleKingsley Village, A30, Penhale, Fraddon, Cornwall TR9 6NADetails from [email protected]
DAY MEETING – EAST ANGLIA REGION
Sunday 11 NovemberWhat’s new in oncology?Speaker: Gerry PoltonThe Cambridge Belfry, Cambourne, Cambridge CB23 6BWDetails from [email protected]
DAY MEETING
Tuesday 20 NovemberCommon and emerging infectious diseases in the pet rabbit: an up to date reviewSpeaker: Emma KeebleBSAVA Headquarters, Woodrow House, Gloucester GL2 2ABDetails from [email protected]
EVENING MEETING – NORTH EAST REGION
Wednesday 7 NovemberInappetent catsSpeaker: Roger WilkinsonIDEXX Laboratories Wetherby, Grange House, Sandbeck Way, Wetherby, West Yorkshire LS22 7DNDetails from [email protected]
EVENING MEETING – NORTH WEST REGION
Wednesday 7 NovemberPainSpeaker: Matt GurneyHoliday Inn, HaydockDetails from [email protected]

With a fresh approach, BSAVA Congress 2013 offers something for everyone; vets, nurses, practice managers, new graduates, experienced principals, specialists, general practitioners, and everyone ‘in between’. With such a diverse programme and creative delivery, no other veterinary conference offers so much for the whole of your team.
Reasons to attend■■ More than 300 lectures■■ A ‘lifecycle’ approach to the lectures – relevant to your career stage■■ Be challenged and encouraged in interactive and small-group sessions■■ “State of the Art” lectures■■ Plenty in the programme to stretch even the most experienced GP■■ A creative approach to practical, hands-on sessions■■ Management programme expanded to three days – great for vets,
VNs and managers■■ Clinical Research Abstracts and poster displays nurturing new science■■ Largest small animal commercial exhibition in Europe with over
250 exhibitors■■ Great networking opportunities at social events
The ICC / NIA
Birmingham – UK
www.bsava.com/congress
Register online now
4–7 April 2013
The Congress for the whole team


















