Common ENT Problems: HldhHow to evaluate and … ENT...Common ENT Problems: HldhHow to evaluate and...
49
Common ENT Problems: Common ENT Problems: H l d h H l d h How to evaluate and when How to evaluate and when to refer to refer to refer to refer Maria C Veling M D Maria C. Veling M.D. Pediatric Otolaryngology University of Kentucky April 2009 1 April 2009
Transcript of Common ENT Problems: HldhHow to evaluate and … ENT...Common ENT Problems: HldhHow to evaluate and...
Common ENT Problems: Common ENT Problems: H l d hH l d hHow to evaluate and when How to evaluate and when
to referto referto referto refer
Maria C Veling M DMaria C. Veling M.D.Pediatric OtolaryngologyUniversity of Kentucky
April 20091
April 2009

ObjectivesObjectives
• Identify symptoms and findings of clinically significant adenotonsillar hypertrophy
• Describe the current guidelines for tonsillectomy and adenoidectomyadenoidectomy
• Describe the current treatment guidelines for otitis media
• Define indications for surgery in pediatric sinusitis• Describe other emergent ENT outpatient scenarios
Clinical Indicators for T&AClinical Indicators for T&A• Patient with 3 or more infections of tonsils and/or adenoids per
year despite adequate medical therapy.year despite adequate medical therapy.• Peritonsillar abscess unresponsive to medical management.• Chronic or recurrent tonsillitis associated with the streptococcal
carrier state and not responding to beta-lactamase-resistant antibioticsantibiotics.
• Persistent foul taste or breath due to chronic tonsillitis not responsive to medical therapy.
• Hypertrophy causing dental malocclusion or adversely affecting f i l th d t d b th d ti torofacial growth documented by orthodontist.
• Hypertrophy causing upper airway obstruction, severe dysphagia, sleep disorders, or cardiopulmonary complications.
• Unilateral tonsil hypertrophy presumed neoplastic. yp p y p p
http://www.entnet.org/Practice/indicators/tonsillectomy.html

OBSTRUCTIONOBSTRUCTION
4
Ad ill H hAd ill H hAdenotonsillar HypertrophyAdenotonsillar Hypertrophy• Symptoms
• Snoringg• Mouth breather• Restless Sleep• Apnea• Difficulty swallowing solids
M ffl d i• Muffled voice• Hypo nasal speech

T ill SiT ill SiTonsillar SizeTonsillar Size
• 0 in Fossa• +1 <25%• +2 25-50%• +2 25-50%• +3 50-75%• +4 >75%
Obstructive indicators forObstructive indicators forObstructive indicators for Obstructive indicators for T&A T&A
• Upper airway obstructionSl di d• Sleep disorders
• Cardiopulmonary complicationsp y p• Dental malocclusion or facial
growth abnormalitiesgrowth abnormalities• Severe dysphagia

OSA in ChildrenOSA in Children> 400 000 T&A’s are performed• > 400,000 T&A s are performed per year in children mostly for OSA
• Most tonsillectomies are performed in children for mild OSA
• OSA is associated with behavioral problems and is known to significantly affect quality-of-life
• < 10% of Otolaryngologists request PSG prior to T&A for OSA

Pediatric OSA and BehaviorPediatric OSA and Behavior
• Several large studies have shown that children with SDB have behavioral problems
• Attention• Hyperactivity• AggressionAggression• Irritability• Emotional and peer problems• Somatic complaints
N. Goldstein, et al Arch Otolaryngol Head Neck Surg. 128 (2002) 770N. Goldstein, et al Arch Otolaryngol Head Neck Surg. 128 (2002) 770--775. 775. Mitchell RB Kelly J LongMitchell RB Kelly J Long Term Changes in the Behavior of Children after Adenotonsillectomy for Obstructive Sleep ApneaTerm Changes in the Behavior of Children after Adenotonsillectomy for Obstructive Sleep ApneaMitchell RB, Kelly J. LongMitchell RB, Kelly J. Long--Term Changes in the Behavior of Children after Adenotonsillectomy for Obstructive Sleep Apnea. Term Changes in the Behavior of Children after Adenotonsillectomy for Obstructive Sleep Apnea. Otolaryngol Head Neck Surg. 2006 Mar;134(3):374Otolaryngol Head Neck Surg. 2006 Mar;134(3):374--8.8.

Pediatric OSAPediatric OSA-- Outcome StudiesOutcome Studies
• PSG normalizes in 70-80% of “normal” children after T&Achildren after T&A
• QOL of life improves dramatically. Over 95% of caregivers report improvementof caregivers report improvement
• Behavior improves in 50% of children• Correlation between improvements in PSG• Correlation between improvements in PSG,
QOL and behavior is poor
Mitchell RB. Adenotonsillectomy for obstructive sleep apnea in children: outcome evaluated by pre- and postoperative polysomnography. (TRIO THESIS) L 200 O 11 (10) 1844 4Laryngoscope. 2007 Oct;117(10):1844-54.

INFECTIONINFECTION
11

Infectious indications forInfectious indications forInfectious indications for Infectious indications for TonsillectomyTonsillectomy
• 6-8 Episodes in one yearp y• 4-5 Episodes per year for 2
yearsyears• 3 Episodes per year for 3 years

P i ill bP i ill bPeritonsillar abscessPeritonsillar abscess• Oropharyngeal
asymmetryy y• Trismus• “Hot Potato” voice• Hot Potato voice• CT scan hardly
ever necessary• 20% will recur

Goals of adenotonsillectomyGoals of adenotonsillectomyGoals of adenotonsillectomyGoals of adenotonsillectomy
• Adenotonsillectomy for sleep disordered breathing (SDB) in children is associated with improvements in sleep quality of life andimprovements in sleep, quality-of-life and behavioral problems
• Approximately 20% of normal weight childrenApproximately 20% of normal weight children and 70% of obese children have persistent SDB after adenotonsillectomy
• Diminished rate of infection after adenotonsillectomy

OTITIS MEDIAOTITIS MEDIA
15

Otitis MediaOtitis MediaOtitis MediaOtitis Media
• Otitis media is generally defined by the presence of effusion within the middle ear without reference to its cause or pathogenesis
• Acute otitis media (AOM) is usually associated with the rapid onset of symptoms and signs of acute infection in the middle ear space, including fever, otalgia, p g ginflammation or bulging of the tympanic membrane, and purulent middle ear effusion
• Otitis media with effusion (OME) is the presence of• Otitis media with effusion (OME) is the presence of serous, mucoid, or mucopurulent fluid in the middle ear without acute symptoms.
Otitis Media Otitis Media Natural history
• After an episode of untreated AOM spontaneous• After an episode of untreated AOM, spontaneous clearance of OME may be expected in approximately 75% of children within 3 months;
ith t t t f th t i d l t 3with treatment of the acute episode, clearance at 3 months may be as high as 90%.
• Patients with effusions with duration of at least 3• Patients with effusions with duration of at least 3 months at the time of diagnosis have the poorest prognosis, with only 27% clearance at 6 months and 32% at 1 year.
Rosenfeld RM: Natural history of untreated otitis media. In Evidence-Based Otitis Media. Edited by Rosenfeld RM, Bluestone CD. Hamilton,Based Otitis Media. Edited by Rosenfeld RM, Bluestone CD. Hamilton, Ontario: BC Decker; 1999:157–177

O i i M diO i i M diOtitis MediaOtitis Media
The pathogenesis is multifactorial
• infection
impaired Eustachian tube function• impaired Eustachian tube function
• immature immune status
• allergy

Surgical treatment of Otitis MediaSurgical treatment of Otitis MediaSurgical treatment of Otitis MediaSurgical treatment of Otitis Media
Acute Otitis Media• Most studies of myringotomy with or without
antibiotic therapy for AOM suggest no significant advantage over antibiotic therapy alone.
• The primary value of myringotomy or tympanocentesis is for culture to guide antibiotic therapy.
Rosenfeld RM: What to expect from surgical therapy. In Evidence Based Otitis Media. Edited by Rosenfeld RM, Bluestone CD. Hamilton, Ontario: BC Decker; 1999:207–221Decker; 1999:207–221.

Surgical treatment of Otitis MediaSurgical treatment of Otitis MediaSurgical treatment of Otitis MediaSurgical treatment of Otitis Media
Recurrent Acute Otitis Media (rAOM)Recurrent Acute Otitis Media (rAOM)• Studies of rAOM suggest a trend toward improvement with
conservative management
• As a result, for children with rAOM whose episodes are nonsevere or have occurred only for a limited period, watchful waiting is often indicatedwatchful waiting is often indicated.
• surgery for rAOM should be recommended only for patients with severe symptoms and a history of at least three or four episodes in a 6-month period, anticipating at best a modest reduction in the frequency of infection

Otitis Media with EffusionOtitis Media with EffusionOtitis Media with EffusionOtitis Media with Effusion
Management is initiated with two goals in mind
• Restoration of normal hearing-g
• Associated with conductive hearing loss causing an average threshold elevation of 25 to 30 dB
• Avoidance of middle ear sequelae-
• Result from chronic or intermittent negative pressure i t i b t ti Thicausing tympanic membrane retraction. This process
may result in flaccidity and atelectasis in the posterosuperior tympanic membrane and the pars flaccida, culminating in ossicular discontinuity or h l t tcholesteatoma.

Surgical treatment of Otitis MediaSurgical treatment of Otitis Media
Otitis Media with Effussion (OME)( )• Tympanostomy tubes are a reasonable consideration in
patients with at least 3 months of bilateral or 6 months of unilateral effusion or in patients in whom a majority of theunilateral effusion, or in patients in whom a majority of the previous year was spent with middle ear disease
• Patients with effusions for less time but who also have severe symptoms severe hearing loss or development ofsevere symptoms, severe hearing loss, or development of atelectasis or retraction pockets should also be considered
• Adenoidectomy may be reserved for the second set of tubes, y ybut should be considered primarily in patients with a history of chronic nasal obstruction or adenoiditis

AdenoidectomyAdenoidectomyAdenoidectomyAdenoidectomy
• Many trials now demonstrate that adenoidectomy is y yefficacious when performed as an adjunctive procedure to tubes.
Rosenfeld RM: What to expect from surgical therapy. In Evidence-Based Otiti M di Edit d b R f ld RM Bl t CD H ilt O t i BCOtitis Media. Edited by Rosenfeld RM, Bluestone CD. Hamilton, Ontario: BC Decker; 1999:207–221.
• Children with adenoidectomy tend to have fewer episodes of OME and seem to require fewer repeat tube insertionsof OME and seem to require fewer repeat tube insertions.
Coyte PC, Croxford R, McIsaac W, et al.: The role of adjuvant adenoidectomy and tonsillectomy in the outcome of the insertion of tympanostomy tubes. New Engl J Med 2001, 344:1188–1195. Bibliographic Li k [C t t Li k]Links [Context Link]
Boston M, McCook J, Burke B, et al.: Incidence of and risk factors for additional tympanostomy tube insertion in children. Arch Otolaryngol Head Neck Surg 2003, 129:293–296.

Surgical indications for middle Surgical indications for middle ggear dysfunctionear dysfunction
• Prolonged middle ear effusions Hearing loss• Hearing loss
• To obtain material for culture to guide antibiotic therapyantibiotic therapy
• In patients with severe symptoms and a history of at least three or four episodes inhistory of at least three or four episodes in a 6-month period
PEDIATRIC CHRONICPEDIATRIC CHRONIC SINUSITISSINUSITIS
25

Pediatric Chronic SinusitisPediatric Chronic SinusitisPediatric Chronic Sinusitis Pediatric Chronic Sinusitis • The precise diagnosis of sinusitis in children is often
diffi lt t k b f th l fdifficult to make because of the overlap of symptomatology with more common conditions such as viral upper respiratory infections and adenoid infection or hypertrophyinfection or hypertrophy.
• Acute rhinosinusitis often presents as a URI with worsening of symptoms (most notably nasal discharge, cough, and halitosis) 7 to 10 days after onset
• Chronic rhinosinusitis (CRS) is defined as a low-Chronic rhinosinusitis (CRS) is defined as a lowgrade infectious process lasting more than 3 months

Pediatric Chronic Sinusitis Pediatric Chronic Sinusitis Diagnosis
• Symptoms lasting more then 3 monthsN l b t ti• Nasal obstruction
• Nasal discharge• Cough• Halitosis• Headache• Recurrent acute rhinosinusitis (ARS)( )
• Six or more episodes of ARS per year, each lasting at least 10 days, with persistent changes on CT at least 4 weeks after medical management and with healthy intervals between episodesp
Pediatric Chronic Sinusitis Pediatric Chronic Sinusitis
Comorbid risk factors- Anything that leads toComorbid risk factors Anything that leads toinflammation and obstruction of the sinus ostia
• Viral infection• Allergic rhinitis• Secondary exposure to tobacco smoke• Daycare attendance• Daycare attendance• Bacterial load of the adenoidal pad• Gastro esophageal reflux disease• Cystic Fibrosis• Primary Ciliary Dyskinesia• Immune deficiency

Pediatric Chronic SinusitisPediatric Chronic SinusitisPediatric Chronic Sinusitis Pediatric Chronic Sinusitis (CS)(CS)
Sobol, Steven E. MD, MSc; Samadi, Daniel S. MD; Kazahaya, Ken MD; Tom, Lawrence W. C. MD Trends in the Management of Pediatric Chronic Sinusitis: Survey
f th A i S i t f P di t i Ot l l L 115(1) 78 80of the American Society of Pediatric Otolaryngology. Laryngoscope. 115(1):78-80, January 2005.

Pediatric Chronic SinusitisPediatric Chronic SinusitisPediatric Chronic Sinusitis Pediatric Chronic Sinusitis

P di i Ch i Si i iP di i Ch i Si i iPediatric Chronic Sinusitis Pediatric Chronic Sinusitis • Treatment- Medical Management
• Amoxicillin/clavulanate, high-dose amoxicillin, cefpodoxime, or cefuroximeor cefuroxime
• Recommended duration of therapy is a total of 10 to 21 days• If initial therapy is ineffective, it is switched to a broader
spectrum antibiotic or combination therapy should bespectrum antibiotic, or combination therapy should be considered.
• Culture-directed therapyf f• Identify and treat any underlying factors that may contribute
to sinus disease

Pediatric Chronic SinusitisPediatric Chronic SinusitisPediatric Chronic Sinusitis Pediatric Chronic Sinusitis
Treatment- Surgical ManagementTreatment Surgical Management• Surgery in children with CS is usually indicated only when
there is failure of maximal medical management.
• First-line surgical management usually consists of adenoidectomy to remove the adenoid pad as a bacterial reservoir for the sinusesreservoir for the sinuses.
• Children whose symptoms persist after adenoidectomy should be referred for immune function and allergy testing
Cand sinus CT
Clary R: Is there a future for pediatric sinus surgery? An American perspective. Int J Pediatr Otorhinolaryngol 2003; 67:S213-S215. The author reviews the recent history of FESS in the pediatric population and examines current t d i th i l t f h i hi i ititrends in the surgical management of chronic rhinosinusitis.

Functional Endoscopic Sinus Functional Endoscopic Sinus Surgery (FESS)Surgery (FESS)Surgery (FESS)Surgery (FESS)
• Failure of maximal medical therapy adenoidectomy andFailure of maximal medical therapy, adenoidectomy, and culture-directed systemic antibiotics
• Anatomic abnormalities identified which predispose to chronic hi i iti b b t ti l i l d irhinosinusitis by obstructing normal sinonasal drainage
pathways
• In sinonasal polyposis, to facilitate application of topical steroidsIn sinonasal polyposis, to facilitate application of topical steroids or as an adjunct to desensitization in aspirin-sensitive patients
• With orbital or intracranial complications of sinonasal disease
• In cystic fibrosis, to improve quality of life and facilitate application of topical antibiotics with activity against PseudomonasPseudomonas

Management of PediatricManagement of PediatricManagement of Pediatric Management of Pediatric Chronic SinusitisChronic Sinusitis
Medical treatment• Antibiotics• Nasal steroids• Saline irrigations
Id tif d t t d l i f t th t• Identify and treat any underlying factors that may contribute to sinus disease
Surgical treatment• Adenoidectomy
FESS• FESS

POTPOURRIPOTPOURRI
35

Acute otitis media complicated byAcute otitis media complicated byAcute otitis media complicated by Acute otitis media complicated by facial nerve paralysisfacial nerve paralysis
• Treatment includes CSF penetrating antibiotics and consultation ASAP for widefor wide myringotomy with possiblepossible mastoidectomy
36

O i i EO i i EOtitis ExternaOtitis Externa
Signs and Symptoms• Severe external auditory canal• Severe external auditory canal
swellingDrainage/debris in canal• Drainage/debris in canal
• Registers high on the pain scale• Periauricular adenopathy,
inflammation
37

O i i EO i i EOtitis ExternaOtitis Externa
38

N l FN l FNasal FracturesNasal Fractures
• Most common facial fracture• Rule out CSF rhinorrhea• Rule out CSF rhinorrhea• Rule out septal hematoma• Patient should be seen by surgeon
within the first 3-5 days of injurywithin the first 3 5 days of injury
39

N l FN l FNasal FractureNasal Fracture
40

Septal HematomaSeptal Hematoma• Blood accumulation which separates the
cartilage from the perichondriumcartilage from the perichondrium• Diagnosis
• Usually bilateral reddish septal swellingy p g• Severe nasal obstruction• Usually painful
• Treatment• Fluid removal and packing or plicating suture• Rx should be instituted within 24 hours
• Sequelae can include infection, cartilage i fib i ddl d f itnecrosis, fibrosis, saddle nose deformity
41

S l HS l HSeptal HematomaSeptal Hematoma
42

A i l HA i l HAuricular HematomaAuricular Hematoma

Traumatic Tympanic MembraneTraumatic Tympanic MembraneTraumatic Tympanic Membrane Traumatic Tympanic Membrane PerforationPerforation
• Usually involves the posterior quadrant
• Usually heals within a fewUsually heals within a few days
• Evaluation should include hearing testhearing test
• Immediate referral for complaints of hearing loss, vertigo or facial nerve e t go o ac a e edysfunction

Foreign BodiesForeign BodiesForeign BodiesForeign Bodies
• Most foreign bodies of the nose or ear are not an emergency
• Exception would be a causticException would be a caustic substance which should be removed immediately
• When the foreign body is aWhen the foreign body is a battery drops are contraindicated because the electrical charge will produce electrolysis of any electrolyte-rich fluid
• This produces hydroxides which will cause a severe alkaline burn
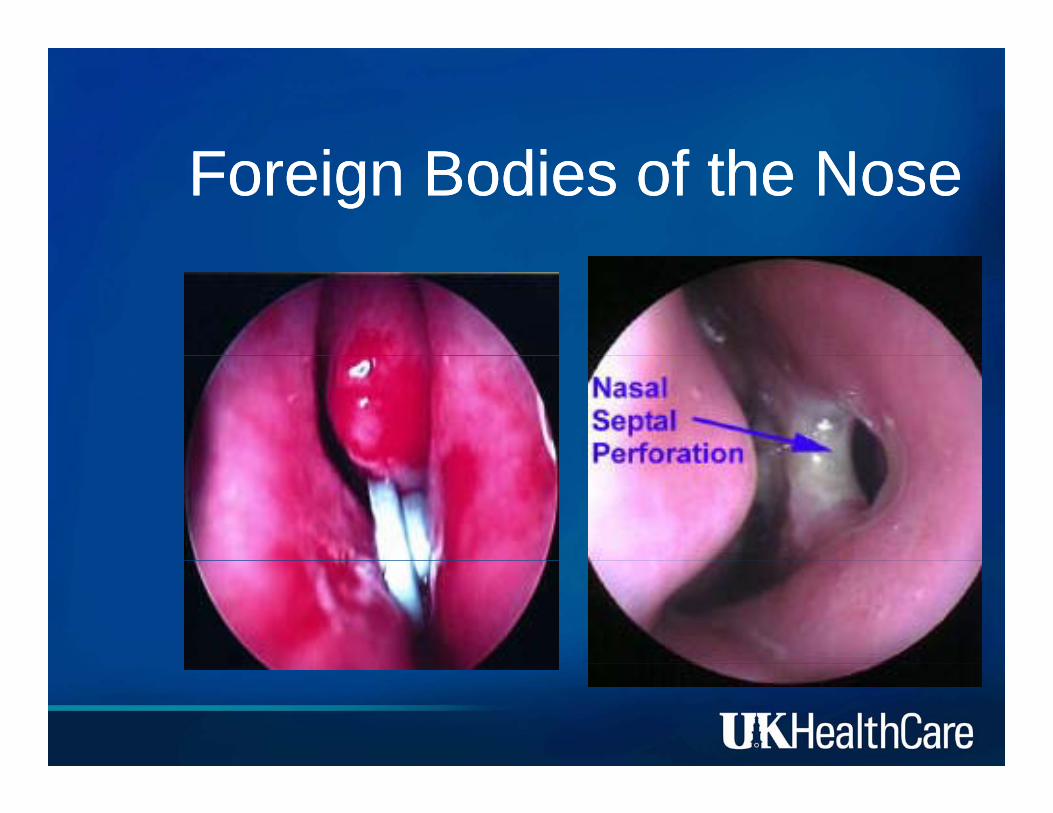
F i B di f h NF i B di f h NForeign Bodies of the NoseForeign Bodies of the Nose

F i b di f hF i b di f hForeign bodies of the noseForeign bodies of the nose
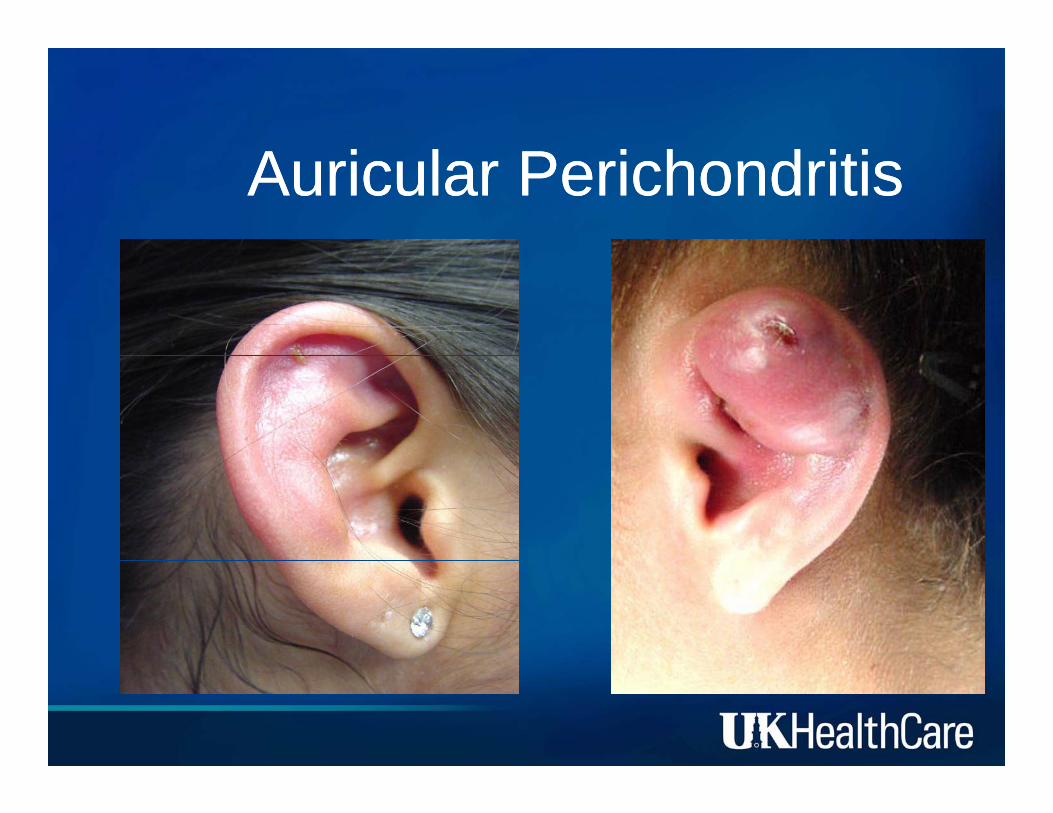
A i l P i h d i iA i l P i h d i iAuricular PerichondritisAuricular Perichondritis

THANK-YOU!!
PLEASE DON’T HESITATE TO PLEASE DON’T HESITATE TO CALL (UKCALL (UK--MD)MD)CALL (UKCALL (UK--MD)MD)
MARIA VELING M.D.MARIA VELING M.D.S O SS O SABBAS YOUNES M.D.ABBAS YOUNES M.D.
![Antenna Pattern Builder Simulation Communicator · [ Tgt Emi tter On & Intermi ent - TDOA/FDOA - Predator North - 446.1 MHz ] Proposal Enhancement Features • Evaluate Product Claims](https://static.fdocuments.net/doc/165x107/5d07073288c9939a7f8bb005/antenna-pattern-builder-simulation-communicator-tgt-emi-tter-on-intermi.jpg)