
Committees Term of Reference - QQMDqqmd.org/content/images/productpreview/QQMD-CS-0001.pdf ·...
22
Committees Term of Reference 1. CME and Patient Education Committee (Terms of Reference) 2. Code Blue Committee (Terms of Reference) 3. Governance Board (Terms Of Reference) 4. Infection Control Committee (Terms of Reference) 5. IT - Health Information Management Committee (Terms of Reference) 6. Medical Records Review Committee (Terms of Reference) 7. Mortality & Morbidity Committee (Terms Of Reference) 8. Nursing Leaders Committee (Terms Of Reference) 9. OR Committee_(Terms Of Reference) 10. Performance and Blood Utilization Review Committee (Terms Of Reference) 11. PURCHASING, STOCK CONTROL & PHYSICAL COUNT COMMITTEE (Terms Of reference) 12. QUALITY COUNCIL (Terms of Reference) 13. Safety & Risk Management Committee (Terms of Reference) 14. SENIOR MANAGEMENT COMMITTEE & Big SMC (Terms of Reference) 15. Antibiotic Committee-Pharmacy Therapeutics Committee (term of Reference) 16. Pharmacy & Therapeutics Committee (term of Reference) 17. Human Resources & Staff affairs Committee (TERMS OF REFERENCE) 18. Learning & Development Committee 19. Ethics Committee (Terms of Reference) 20. Renal Transplantation committee 21. Clinical Team Committee (Terms Of Reference) 22. Clinical Team Committee consolidated report 23. JCI reaccreditation preparation steering committee (Terms of reference)
Transcript of Committees Term of Reference - QQMDqqmd.org/content/images/productpreview/QQMD-CS-0001.pdf ·...
Committees Term of Reference
1. CME and Patient Education Committee (Terms of Reference)
2. Code Blue Committee (Terms of Reference)
3. Governance Board (Terms Of Reference)
4. Infection Control Committee (Terms of Reference)
5. IT - Health Information Management Committee (Terms of Reference)
6. Medical Records Review Committee (Terms of Reference)
7. Mortality & Morbidity Committee (Terms Of Reference)
8. Nursing Leaders Committee (Terms Of Reference)
9. OR Committee_(Terms Of Reference)
10. Performance and Blood Utilization Review Committee (Terms Of Reference)
11. PURCHASING, STOCK CONTROL & PHYSICAL COUNT COMMITTEE (Terms Of reference)
12. QUALITY COUNCIL (Terms of Reference)
13. Safety & Risk Management Committee (Terms of Reference)
14. SENIOR MANAGEMENT COMMITTEE & Big SMC (Terms of Reference)
15. Antibiotic Committee-Pharmacy Therapeutics Committee (term of Reference)
16. Pharmacy & Therapeutics Committee (term of Reference)
17. Human Resources & Staff affairs Committee (TERMS OF REFERENCE)
18. Learning & Development Committee
19. Ethics Committee (Terms of Reference)
20. Renal Transplantation committee
21. Clinical Team Committee (Terms Of Reference)
22. Clinical Team Committee consolidated report
23. JCI reaccreditation preparation steering committee (Terms of reference)

QQMD (CME & PATIENT EDUCATION COMMITTEE)
(TERM OF REFRENCES)
Document #: QQMD/CME & PATIENT EDUCATION COMMITTEE/TOR
Page 1 of 2
QQMD/CME & PATIENT EDUCATION COMMITTEE/TOR
Report to: MEDICAL BOARD COMMITTEE
CHAIR: ………………
MEMBERS: Voting:
MEMBERS: Voting:
Medical Staff Representative
Nursing Staff Representative
Quality management Representative
Pharmacy services Representative
Physiotherapy Representative
Clinical Nutrition Representative
Others as appointed by Chair
QUORUM:
50% of members excluding the Chair
MEETINGS: The Patient/Family Education Task Force Committee shall meet monthly but no
less than ten times a year. Special meetings to handle urgent decisions will be called at the
discretion of chair.
Minutes shall be maintained for all meetings. The minute format shall be reporting by exception
with responsibility and recommended action documented.
The minutes shall be forwarded to MEDICAL BOARD COMMITTEE for action and or
approval.
The agenda shall be sent to all members at least one week prior to the meeting unless the meeting
is for urgent matters.
Additional Information:
PURPOSE:
The Patient/Family Education Committee is a multi-disciplinary team acting on behalf of the
Medical Staff to examine the hospital system for patient/family learning and for building and
maintaining an effective patient/family education system.
The purpose of the Patient/Family Education Task Force Committee is to set standard and goals
aimed at developing the staff performance and services directly related to the patients’ education
to increase patient/family awareness and participation in health maintenance and improvement.
TERMS OF REFERENCE:
1. Establish a hospital-wide patient/family education system
2. Standardise patient/family education processes
3. Prepare patient/Family Education Materials
4. Approve all patient /family education materials used in the Hospital

QQMD (CODE BLUE COMMITTEE)
(TERM OF REFRENCES)
Document #: QQMD/CODE BLUE COMMITTEE/TOR
Page 1 of 2
QQMD/CODE BLUE COMMITTEE/TOR
Pag
e1
Reports to: MEDICAL BOARD Committee
CHAIR: MEDICAL DIRECTORS OF ICUs.
MEMBERS: Voting:
Medical Director.
ER Manager.
NNICU Manager.
Director of Nursing Department.
Quality Manager
Specialists Physicians Manager
Others as appointed by Chair
QUORUM:
50% of members excluding the Chair
MEETINGS:
The Code Blue Committee shall meet monthly but no less than ten times a year. Special meetings to
handle urgent decisions will be called at the discretion of chair.
Minutes shall be maintained for all meetings.
The minute format shall be reporting by exception with responsibility and recommended action
documented.
The minutes shall be forwarded to the MEDICAL Board Committee for action and or approval.
The agenda shall be sent to all members at least one week prior to the meeting unless the meeting is for
urgent matters.
Additional Information:
PURPOSE:
The CODE BLUE Committee is a multi-disciplinary advisory body acting on behalf of the Medical
Staff to formulate policies on the administration of artificial heart and lung action in the event of cardiac
and/or respiratory arrest; and closed-chest cardiac massage.
The purpose of the CODE BLUE Committee is to promote high standards of patient care through
monitoring and evaluating of the quality and appropriateness of all major components of cardio-
pulmonary resuscitation functions.
TERMS OF REFERENCE:
1. Review CPR policies and procedures.
2. Develop standards and indicators for monitoring effectiveness of CPR.
3. Develop a system to record and evaluate every resuscitation incident.
4. Plan and support training courses by certified trainers for medical and nursing staff.
5. Developing a planned training program by certified trainers for the related staff.
QQMD (GOVERNANCE BOARD COMMITTEE)
(TERM OF REFRENCES)
Document #: QQMD/MEDICAL BOARDCOMMITTEE/TOR
Page 3 of 3
QQMD/MEDICAL BOARDCOMMITTEE/TOR
17. Is responsible for identifying and planning for the types of clinical services required to meet the
goals of the patients served.
18. Provide oversight of contracts for clinical or management services.
19. Ensure that there are uniform programs for recruitment, retention, development and continuing
education of all staff.
20. Assure that one or more qualified individuals provide direction for each department or service in
the organization and that the direction includes identifying in writing the services to be provided,
that the services are coordinated and integrated within the department or service with other
departments or services, recommend space, equipment, staffing and other resources needed by the
department or service, recommend criteria for selecting the department or service’s professional
staff and choose or recommend individuals who meet those criteria, provide orientation and
training to all staff of the department or service appropriate to their responsibilities, monitor the
department’s or service’s performance as well as staff performance.
21. Establish a framework for ethical management that ensures that patient care is provided within
business, financial, ethical, and legal norms and that protects patients and their rights which
includes marketing, admissions, transfer and discharge, and disclosure of ownership and any
business and professional conflicts that may not be in the patient’s best interests. These
framework’s goals are to support ethical decision making in clinical care.
BASELINE AGENDA REQUIREMENTS:
I. Call to order
II. Approval/Revision of previous minutes
1. Guest Relation Feedback- GRM- 30 minutes
2. Feedback from Nursing and Operations- DON/Nursing Rep; GMO- 15 minutes
3. Night Shift Feedback-NDM- 30 minutes
4. Quality Report- QM – 30 minutes
5. Sales Report - SM- 30 minutes
6. Cash Patient analysis- OFA -30 minutes
7. Revenue Report- ACFO – 30 minutes
8. Accounts Receivables status & Collection Forecast-MOM-30 minutes
9. P&L statement and Cash Flow Report- ACFO- 30 minutes
III. Other Business : Any of the HODs called as per top management request
IV. Adjournment
QQMD (INFECTION CONTROL COMMITTEE)
(TERM OF REFRENCES)
Document #: QQMD/IC COMMITTEE/TOR
Page 2 of 3
QQMD/IC COMMITTEE/TOR
4. Review hospital infection related statistics prepared on a monthly basis and recommend specific
actions to be taken by the infection control team, various departments and wards, and specific
staff.
5. Educate through lectures, symposia, workshops and seminars medical, nursing and ancillary staff,
patients and their attendants regarding infection control issues.
6. Ensure that notifiable diseases are adequately reported and communicated to the appropriate
authorities.
7. Recommend regular supply of appropriate equipment, consumables and drugs required to prevent
and manage nosocomial infections.
8. Ensure that the various hospital contractors (e.g.: cleaning, catering, pest control, laundry, etc.)
abide by the terms of their contracts in aspects related to control of infections, use of detergents
and disinfectants, and general hygiene of the hospital.
9. Review all environmental contracts affecting the management of infection control prior to their
approval.
BASELINE AGENDA REQUIREMENTS: Suggest
I. Call to Order
a. Review of Minutes of Previous Meeting
b. Revisions/Approval of Minutes
II. Committee Reports
a. Statistical Reports (TRENDED) Based on per 1000 patient days.
i. Infection Rate (# total infections/patient days X 1000)
ii. Nosocomial Rate (#nosocomial infections/patient days X 1000)
1. broken down by unit/location
2. broken down by
a. urinary tract catheter/non catheter
b. respiratory
c. decubitus ulcer
d. surgical site
e. other
iii. Community Acquired Infection Rate (#community Acquired/patient days X
1000)
iv. Multi-drug Resistant Infection (MDRI) Rate (# MDRI’s /patient days X 1000)
1. broken down by type
a. TB
b. MRSA
c. MDRI, non MRSA
v. Nosocomial Sepsis Rate (#Nosocomial Sepsis/patient days X 1000)
vi. Death from Nosocomial Infection Rate(# of deaths determined to be secondary to
nosocomial infections/patient days X 1000)
vii. Employee Health Report
1. Food Poisoning
2. Diarrhea

QQMD (INFECTION CONTROL COMMITTEE)
(TERM OF REFRENCES)
Document #: QQMD/IC COMMITTEE/TOR
Page 3 of 3
QQMD/IC COMMITTEE/TOR
viii. Needle sticks
III. Policy and Procedure Review
a. Annual policy review. (bring 1/12th to each meeting)
b. New Policy review
IV. Reports of In service Education(Database % staff educated, reporting issues)
a. In services (Target groups, plan, etc.)
b. Education boards/brochures
c. Special seminars
V. Other Business
a. National and International Infection Concerns
b. Risk Reporting, i.e. SARS, Ebola, etc.
c. Review of cleaning chemicals—Annually and as proposing changes
i. Does Chemical Meet Infection Control needs
ii. Plans for educating cleaning staff on proper use
iii. Environmental impact

QQMD (Information Technology COMMITTEE)
(TERM OF REFRENCES)
Document #: QQMD/IT COMMITTEE/TOR
Page 1 of 2
QQMD/IT COMMITTEE/TOR
Reports to: Senior Management Committee
CHAIR: IT Department Manager
MEMBERS: Voting:
GMO
Ward Secretary Manager
Purchasing department Representative
Admission & Billing Manager
Pharmacy Representative
Finance Department Representative
Others as appointed by Chair
QUORUM:
50% of members excluding the Chair
MEETINGS: The Health Information Management Committee shall meet monthly but no less than ten
times a year. Special meetings to handle urgent decisions will be called at the discretion of chair.
Minutes shall be maintained for all meetings. The minute format shall be reporting by exception with
responsibility and recommended action documented.
The minutes shall be forwarded to the Hospital Senior Management Committee for action and / or
approval.
The agenda shall be sent to all members at least one week prior to the meeting unless the meeting is for
urgent matters.
Additional Information:
PURPOSE:
The Health Information Management Committee is a multi-disciplinary advisory body acting on behalf of
the SM Committee to oversight the acquisition, implementation, and use of information technology and
management services regarding improving the overall quality of patient care at the hospital.
The purpose of the Health Information Management Committee is to identify important health
information management and technology issues and develop plans and actions to address these concerns.
TERMS OF REFERENCE:
1. Developing and updating the Hospital Information Management Plan.
2. Evaluating the process of computerizing health information at the hospital.
3. Ensuring that the hospital implements information security policies and control procedures.
4. Developing a planned training program by certified trainers for the related staff.
QQMD (SENIOR MANAGEMENT COMMITTEE)
(TERM OF REFRENCES)
Document #: QQMD/SMC COMMITTEE/TOR
Page 3 of 3
QQMD/SMC COMMITTEE/TOR
BASELINE AGENDA REQUIREMENTS:
I. Call to order
II. Approval/Revision of previous minutes
Departments called for meeting set in the approved order for SMC meeting
Regular SMC meeting:
Departments shall report:
a- KPIs results: measures that appear in department dashboard
b- Department statistics: measures of core services that are not included in the
dashboard
c- Complaints / Incident Reports: that are raised from the department stating the
action needed and departments which are requested for cooperation to solve
d- Inquiries From Other Departments : inquiries Requested from other department
“stated” to follow up during coming week and reported in the coming sector
e- Follow up of Pending Issues/Complaints: Follow up of issues raised against the
department in Previous SMC
f- Improvement Projects / Business Process Improvement: either an existing project
or any OFI “an Opportunity for Improvement” shall be reported for follow up
g- Others: for other valuable information, the coming updates on the system will
depend on the frequency of new information reported in this sector
All pending issues shall be documented by relevant HOD and action taken for all pending issues
reported in the next SMC except for strategic decisions, which will be followed up on monthly
basis “Big SMC” meeting
Big SMC meeting
a- Deteriorated KPIs follow-up: compared to previous month with primitive data
collection on probable causes and recommended actions
b- Follow-up of still Pending Issues/Complaints: to take action for each.
c- Committees & meetings attended by the department and follow up of actions taken.
d- Improvement Projects / Business Process Improvement still hunting any OFI.
III. Other Business
IV. Adjournment

Committees Master
Decisions Follow up Sheet

Committee Date Decisions Sent date Received date Status
Nursing leadership 00/00/20Nursing Director asked IT Manager that all
items to be bar coded and stickers asap.00/00/20 00/00/20 ongoing
Nursing leadership 00/00/20Rule and responsibility of
the Head Nurse should be activated 00/00/20 00/00/20 Done
Nursing leadership 00/00/20
Part time only will be 3 months and will
pay full insurance but the cancellation will
be discussed with HR.
00/00/20 00/00/20 Done
Nursing leadership 00/00/20
Charge Supplies,Nursing Director
asked from Head Nurses to not stop
the charge supply training for all the
staff nurses.
00/00/20 00/00/20 Done
Nursing leadership 00/00/20Instrument collection/Humidifier
check.00/00/20 00/00/20 Done
Nursing leadership 00/00/20 Pharmacy instructions “discussion” 00/00/20 00/00/20 Done
Nursing leadership 00/00/20 Standardize of auditing 00/00/20 00/00/20 Done
Nursing leadership 00/00/20 Teaching Program 00/00/20 00/00/20 ongoing
Nursing leadership 00/00/20customer feedback To be
reduce it as much as possible 00/00/20 00/00/20 Done
Nursing leadership 00/00/20 decrease Medication Error 00/00/20 00/00/20 Pending
Nursing leadership 00/00/20 decrease Customer feedback 00/00/20 00/00/20 Pending
Decisions taken in Committees from (Month) 20-- to (Month) 20--Decision Follow up Cycle

Minutes Demonstrations

Page 1 of 3 QQMD-QMD-FRM-021
Issue No.: 0 Issue Date: 0/0/20
Revision No.:0
Meeting Title: Code Blue Committee
MINUTES
[MEETING DATE] 30/ 07 /2011
[MEETING TIME] 14:00 PM- 15:30 PM
[MEETING LOCATION] TRAINING ROOM
MEETING CALLED BY Dr. Mohamed Khalil
TYPE OF MEETING Monthly
FACILITATOR Mr. ……………………….
NOTE TAKER Mr. ……………………….
TIMEKEEPER Dr ………………………….
ATTENDEES
Dr. ………………….; Dr. ………………….; Dr. ………………….; Dr. …………………., Ms. …………………., Ms. …………………., Mr. …………………. , Ms. …………………., Ms. …………………., Ms…………………..
Agenda topics This Meeting represent July
[TIME ALLOTTED] ONE HOUR
Matters arising from minutes of previous meeting
DISCUSSION
Briefing of the previous code blue committee minutes was done by Dr. Mohamed Khalil. The list of ACLS trained and certified physicians were sent to Dr. Adel Omran. The code blue events for the current month were revised and the documentation was satisfactory with minimal comments on the medications. The AHA dolls are in the purchase and every thing was done from our clinical side, it needs a financial approval and support. Two cricothyroidotomy set are requested by Dr. Mohamed Ali to be available in the E.R Crash Cart, it will be followed up by the E.R manager. Portable suction not resolved and bending, Mr.fathy needs E-Mail to fasten the process.
Page 3 of 3 QQMD-QMD-FRM-021
Issue No.: 0 Issue Date: 0/0/20
Revision No.:0
Code Blue cases during July
Thank You
No Name & MRN Age Consultant Date& area of
code event
Outcome of code
1
Abdel Hamid Ali Elsaid
MRN 210739
71
years
Dr. Hussam
Salah
26/07/2011
ER Unsuccessful
2 3 4 5

Page 1 of 3 QQMD-QMD-FRM-021
Issue No.: 0 Issue Date: 0/0/20
Revision No.:0
Quality council committee
DATE: 22/11/2012 TIME: 10:00 AM LOCATION: TRAINING ROOM
MEETING CALLED BY Quality Department
TYPE OF MEETING Quality council committee
FACILITATOR Dr. Mohamed ameen
NOTE TAKER Dr. …………………
INVITED MEMBERS HODs
TOPIC NAME: BLS & ACLS
DISCUSSION BLS & ACLS
Dr. Mohamed ameen explained the demonstration of new electronic recertification of BLS for the consultants. The site starts with video explains the BLS to the consultants. After reviewing the video the consultant will answer MCQ questions and. Pass score will be 8/10.the certificate will be submitted to HR Dr. Mohamed ameen requested Medical director to provide valid BLS exam and its model answer.
CONCLUSIONS
Demonstration of new electronic recertification of BLS for the consultants had been explained
A slip containing the link, password and the name will be sent to the consultant to register in the website. A clip will be opened explaining the BLS. Then an application will be opened containing 10questions.
The result will be sent to HR data base including the consultant code, result and the expire date
training department will be responsible to archive the certificates and the names
Code blue committee will be responsible to provide the baseline or current status of the BLS, the plan and to provide the quality department weekly with the ratio of BLS certified number.
ACTION ITEMS PERSON RESPONSIBLE DEADLINE
Provide the approved BLS Video, questions and its model answer Code blue committee
Certificates archiving training department
To provide the following:
Baseline of BLS (current status) Certification and recertification plan of BLS
Weekly report of the BLS ratio (KPI)
Official approval of the “RESUSCITATION TECHNIQUE TRAINING “policy which modified by quality department
Code blue committee
TOPIC NAME: PRIVILAGE AND CREDENTIAL
DISCUSSION
Dr. Mohamed ameen repeated the what had been discussed that Nurses have to know how to access to the doctors privilege
The attending physician is the responsible person to check the privilege according to the patient’s plan of care. If there is any problem regarding the privilege. She/he has to report to the specialist physician manager
The specialist physician manger is responsible to monitor the process
The specialist physician manger and the medical director are responsible to update the privilege of consultants and specialist physicians.
Page 1 of 3 QQMD-QMD-FRM-021
Issue No.: 0 Issue Date: 0/0/20
Revision No.:0
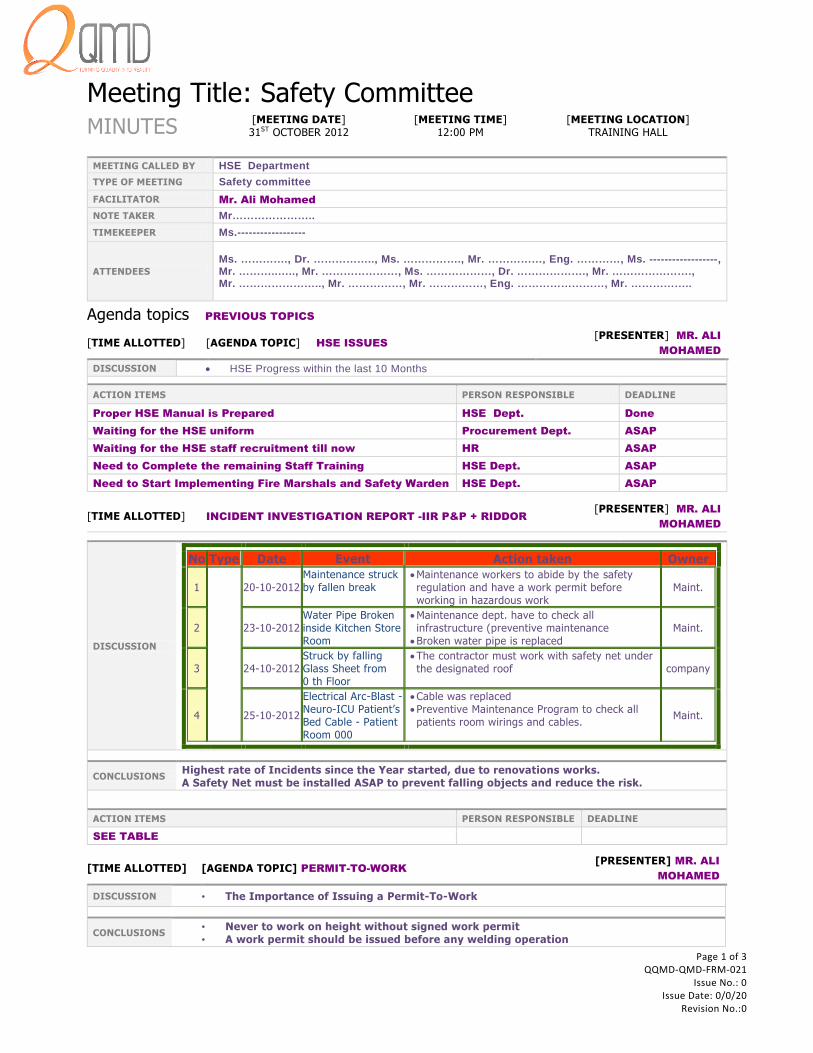
Meeting Title: Safety Committee MINUTES
[MEETING DATE] 31ST OCTOBER 2012
[MEETING TIME] 12:00 PM
[MEETING LOCATION] TRAINING HALL
MEETING CALLED BY HSE Department
TYPE OF MEETING Safety committee
FACILITATOR Mr. Ali Mohamed
NOTE TAKER Mr…………………..
TIMEKEEPER Ms.------------------
ATTENDEES
Ms. …………., Dr. …………….., Ms. ……………., Mr. ……………, Eng. …………, Ms. ------------------, Mr. ………..….., Mr. …………………, Ms. ………………, Dr. ………………., Mr. …………………., Mr. ………………….., Mr. ……………, Mr. ……………, Eng. ……………………, Mr. ……………..
Agenda topics PREVIOUS TOPICS
[TIME ALLOTTED] [AGENDA TOPIC] HSE ISSUES [PRESENTER] MR. ALI
MOHAMED
DISCUSSION HSE Progress within the last 10 Months
ACTION ITEMS PERSON RESPONSIBLE DEADLINE
Proper HSE Manual is Prepared HSE Dept. Done
Waiting for the HSE uniform Procurement Dept. ASAP
Waiting for the HSE staff recruitment till now HR ASAP
Need to Complete the remaining Staff Training HSE Dept. ASAP
Need to Start Implementing Fire Marshals and Safety Warden HSE Dept. ASAP
[TIME ALLOTTED] INCIDENT INVESTIGATION REPORT -IIR P&P + RIDDOR
[PRESENTER] MR. ALI
MOHAMED
DISCUSSION
No Type Date Event Action taken Owner
1
20-10-2012
Maintenance struck by fallen break
Maintenance workers to abide by the safety regulation and have a work permit before working in hazardous work
Maint.
2 23-10-2012 Water Pipe Broken inside Kitchen Store Room
Maintenance dept. have to check all infrastructure (preventive maintenance
Broken water pipe is replaced
Maint.
3 24-10-2012 Struck by falling Glass Sheet from 0 th Floor
The contractor must work with safety net under the designated roof company
4 25-10-2012
Electrical Arc-Blast - Neuro-ICU Patient’s Bed Cable - Patient Room 000
Cable was replaced Preventive Maintenance Program to check all patients room wirings and cables.
Maint.
CONCLUSIONS Highest rate of Incidents since the Year started, due to renovations works. A Safety Net must be installed ASAP to prevent falling objects and reduce the risk.
ACTION ITEMS PERSON RESPONSIBLE DEADLINE
SEE TABLE
[TIME ALLOTTED] [AGENDA TOPIC] PERMIT-TO-WORK [PRESENTER] MR. ALI
MOHAMED
DISCUSSION • The Importance of Issuing a Permit-To-Work
CONCLUSIONS • Never to work on height without signed work permit • A work permit should be issued before any welding operation

Committees Templates

TITLE OF MEETING
Subject: Date: 00/00/20
Facilitator: Location :
Page 1 of 1 QQMD-QMD-FRM-026
Issue No.: 0 Issue Date: 0/0/20
Revision No.:0
SR
Invitee Signature Designation Department Sign in
Time
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19

LEAN COMMITTEES QQMD

Lean Committees
2 | P a g e
INTRODUCTION
Committees follow up shows that there is a lot of defects & waste in QQMD committees, that’s why Quality
Management Department (QMD) chosen the lean approach to improve committee
function in QQMD.
The project was done following the lean thinking 5 principles:
Principle 1 - Specify value
Principle 2 - Identify and visualize value stream
Principle 3 - Making the value steps flow through identifying waste
Principle 4 - Pulling committee cycle instead of pushing
Principle 5 - Perfection
PRINCIPLE 1 - SPECIFY VALUE
The first step in lean committees is to identify Committee stakeholder & their value perspectives, this was done through:
1. Observations of QQMD committees.
2. Reviewing QQMD committees meeting minutes.
3. Conducting Focus group with HODs.
4. Conducting HODs “Committees questionnaire”.
We reached the following conclusions from collecting stakeholder voices & views regarding QQMD committees’
function, which helps to identify demand from committees.
Customers Voice of the customer
HODs - Participation in decision making - Too much time spent in committee
Top management - Decision making - HOD commitment to Attendance
Quality Management Department (QMD)
- Updated TORs - Committees follow TORs - Follow up of decisions - Follow schedule/ no overlap - Covers JCI requirements
PRINCIPLE 2 - IDENTIFY AND VISUALIZE VALUE STREAM
The second stage is drawing, understanding & analyzing committee consequences & events, which to enable committee
stakeholder:
1. To visualize the current committee meetings practices and activities.
2. Highlight the non-value added steps & waiting time (delay) in committee process.
3. To Identify QQMD committees waste.
This was done by:
1. DRAWING A DETAILED FLOW CHART : SEE FIGURE 1

Lean Committees
3 | P a g e
FIGURE 1: COMMITTEES VALUE STREAM MAP SHOWING VALUE ADDED, NON-VALUE ADDED & WAITING TIME

Lean Committees
4 | P a g e
From the value stream map (the above figure), we can classify committee process steps to:
1. Process steps that definitely create value: Discussion
New decisions
Members execute decisions 2. Process steps that create no value but are
necessary, due to current state of the system:
Review approve TORs
members preparing reports
Writing & sending meeting minutes
QMD decisions follow up cycle
archiving meeting minutes 3. Process steps that create no value and
can be eliminated: sending notification, invitations & agenda
meeting room reservation
meeting room coordination with QMD
reporting in a committee
2. DRAWING COMMITTEE TIMELINE; SEE FIGURE 2
FIGURE 2: COMMITTEES TIMELINE SHOWING TIME SPENT IN EACH COMMITTEE
Committee’s timeline shows that:
Only 30 minutes of a 120 minutes spend in a single committee is value added time, which is the
time of members discussing a topic & reaching a final decision after going through pros & cons of
every possible suggestion for a decision, which is the ultimate goal of a committee.

Lean Committees
10 | P a g e
PRINCIPLE 5 - PERFECTION
Committee item Changes after lean
Schedule All committees to be held on Thursdays from 12:00 PM to 2:00 PM
Duration 45 minutes
frequency Committee Frequency
SMC, CTC, Infection control, safety, code blue, morbidity & mortality, Pharmacy , medical records
Monthly committee
QC, Team A meeting weekly committees
Governance board Biannual
* HR, Nursing, blood utilization, purchase, IT committees can be departmental committees, organized coordinated & controlled by the related department & committee chairmen. *Kidney, liver transplantations, Ethics, patient education, credentials & privilege, continuous medical education committees can be organized coordinated & controlled by clinical team leaders.
Session
2 committees shall be held in the same session as follows:
1st week Big SMC
2nd week Infection Control - Safety
3rd week Code Blue - Morbidity & Mortality
4h week Pharmacy – medical records
Logistics Annual Training room reservation to be done according to committees’ schedule
Purpose/Content Minimize time spent in reporting & displaying results, statistics or KPIs, discussions should be directed to decision making.
Major changes in TORs
Committee Major changes
Governance board
To be held biannual
1st half of the year, the purpose of GB is to review annual budget, financial plan for the next year, departmental objectives.
By the end of the year, a second GB is held for the final approvals of policies & procedures, hospital plans, organization chart.
Quality circle Incident reporting review, corrective action is to be added to QC quarterly.
SMC Weekly SMC is cancelled as its mainly reporting, yet


















