Commissioning Guide Diabetes and Kidney Care Services
30
Diabetes and Kidney Care Commissioning Diabetes and Kidney Care Services June 2011 Supporting, Improving, Caring
Transcript of Commissioning Guide Diabetes and Kidney Care Services

Diabetes and Kidney Care
CommissioningDiabetes and
Kidney Care Services
June 2011
Supporting, Improving, Caring
NHS Diabetes information Reader Box
Review Date 2013
Commissioning Diabetes and Kidney Care
NHS Diabetes and NHS Kidney Care would like to thank the following for their advice and contribution tothe development of this commissioning guide:
Hugh Rayner Consultant in Renal Medicine, Heart of England NHS Trust
Charlie Tomson Consultant in Renal Medicine, North Bristol NHS Trust
Hugh Cairns Consultant in Renal Medicine, King’s College Hospital NHS Foundation Trust
Niru Goenka Consultant in Diabetes and Endocrinology, Countess of Chester NHS FoundationTrust
And to Thoreya Swage who wrote this publication.

3
Page
Commissioning for Diabetes and Kidney Care 5
Features of Diabetes and Kidney Care Services 6
Diabetes and Kidney Care Services Intervention Map 8
Contracting Framework for Diabetes and Kidney Care Services 11
Standard Service Specification Template for Diabetes and Kidney Care 25
Contents


5
Commissioning for Diabetes andKidney Care The NHS Diabetes commissioning approach helps to deliver high quality integrated care through a three-stepprocess that ensures key elements needed to build an excellent diabetes service are in place. The approach issupported by a wide range of proven tools, resources and examples of shared learning.
Step 1 – involves understanding the local diabetespopulation health needs by developing a local HealthNeeds Assessment and setting up a steering groupwith key stakeholder involvement including a leadclinician, lead commissioner, lead diabetes nurse andlead service user
Step 2 – involves the development of a servicespecification to describe the model of care to becommissioned. This becomes the document onwhich tenders may be issued.
Step 3 – involves monitoring the delivery of theservice specification by the provider and evaluatingthe performance of the service. Input from thesteering group with service user representation willbe an important mechanism for monitoring theservice as well as patient surveys.
This commissioning guide has been developed byNHS Diabetes and NHS Kidney Care with keystakeholders including clinical and social servicesprofessionals and patient groups represented byDiabetes UK.
It is not designed to replace the Standard NHSContracts as many of the legal and contractualrequirements have already been identified in this setof documents. Rather, it is intended to form the basisof a discussion or development of diabetes andkidney care services between commissioners andproviders from which a contract for services can thenbe agreed.
This commissioning guide consists of:
• A description of the key features of good diabetesand kidney care
• A high level intervention map. This interventionmap describes the key high level actions orinterventions (both clinical and administrative)diabetes and kidney care services shouldundertake in order to provide the most efficientand effective care, from admission to discharge (ordeath) from the service.
It is not intended to be a care pathway or clinicalprotocol, rather it describes how a true ‘diabeteswithout walls’1 service should operate going acrossthe current sectors of health care.
The intervention map may describe current servicemodels or it may describe what should ideally beprovided by diabetes and kidney care services.
• A diabetes and kidney care contracting frameworkthat brings together all the key standards of qualityand policy relating to diabetes and kidney care
• A template service specification for diabetes andkidney care services that forms part of schedule 2part 1 ,or section 1 (module B) of the StandardNHS Contract covering the key headings requiredof a specification. It is recommended that thecommissioner checks which mandatory headingsare required for each type of care as specified bythe Standard NHS Contracts.
For further detail on how to approach thecommissioning of diabetes services please seehttp://www.diabetes.nhs.uk/commissioning_resource
Step 2
Step 3
• Understanding your diabetes population health needs
• Implementing improved services and evaluation
• Understanding what you need to commission for an integrated service
Step 1
1 Commissioning Diabetes Without Walls , 2011, http://www.diabetes.nhs.uk/commissioning_resource/
6
High quality diabetes and kidney care servicesshould ensure:
• that people with diabetes have a regularassessment and review of renal function(including management of anaemia and boneconditions) as part of their diabetes assessmentand care planning process
• that patients with chronic kidney disease anddiabetes who require specialist care are seen injoint nephrology and diabetes services
• there is access to vascular services for vascularaccess for haemodialysis
• there is access to transplantation services whichprovide combined kidney and pancreatictransplantation as appropriate
• that there is regular training and development inbasic diabetes competences for hospital staffcaring for people who have renal conditions anddiabetes
• that there is regular training and developmentfor all health care professionals who providediabetes care on the management of kidneyconditions
• that there are monitored protocols for hospitalstaff on when to access diabetes specialistadvice and intervention for people with diabeteswho have renal conditions
• that there are monitored protocols in place toensure that patients can continue to managetheir diabetes themselves while in hospital (foodand medication)
• that data items included in the National RenalDataset are reported accurately and completelyon all patients on Renal Replacement Therapy
In addition, the service should:
• be developed in a co-ordinated way, taking fullaccount of the responsibilities of other agenciesin providing comprehensive care and placingusers at the centre of decisions about their careand support - "no decision about me withoutme" (Equity and Excellence: Liberating theNHSi).
• be commissioned jointly by health and socialcare based on a joint health needs assessmentwhich meets the specific needs of the localpopulation, using a holistic approach asdescribed by the generic model for themanagement of long term conditionsii
• provide effective and safe care to people withdiabetes in a range of settings including thepatient’s home, in accordance with the NICEQuality Standards for Diabetesiii
• deliver the outcomes for diabetes as determinedby the NHS Outcomes Frameworkiv
• take into account the emotional, psychologicaland mental wellbeing of the patientv
• take into account all diverse and personal needswith respect to access to care
• ensure that services are responsive andaccessible to people with Learning Disabilitiesvi
• ensure that the family/carers of people withdiabetes have access to psychological support
Features of Diabetes and KidneyCare Services
i Available on the DH website athttp://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_117353
ii Available on the DH website at http://www.dh.gov.uk/en/Healthcare/Longtermconditions/DH_120915
iii Quality Standards: Diabetes in adults, http://www.nice.org.uk/guidance/qualitystandards/qualitystandards.jsp
iv Available on the DH website athttp://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_122944
v Emotional and Psychological Support and Care in Diabetes, Joint Diabetes UK and NHS Diabetes Emotional and PsychologicalSupport Working Group, 2010 http://www.diabetes.nhs.uk/our_work_areas/emotional_and_psychological/
vi http://www.diabetes.nhs.uk/commissioning_resource

7
• have effective clinical networks with clear clinicalleadership across the boundaries of care whichclearly identify the role and responsibilities ofeach member of the diabetes healthcare team
• ensure that there are a wide range of optionsavailable to people with diabetes to support selfmanagement and individual preferences
• take into account services provided by socialcare and the voluntary sector
• provide patient/carer/family education ondiabetes not only at diagnosis but also duringcontinuing management at every stage of care
• provide education on diabetes management toother staff and organisations that supportpeople with diabetes
• have a capable and effective workforce that hasthe appropriate training and updating andwhere the staff have the skills and competenciesin the management of people with diabetes
• provide multidisciplinary care that manages thetransition between children and adult servicesand adult and older peoples’ services
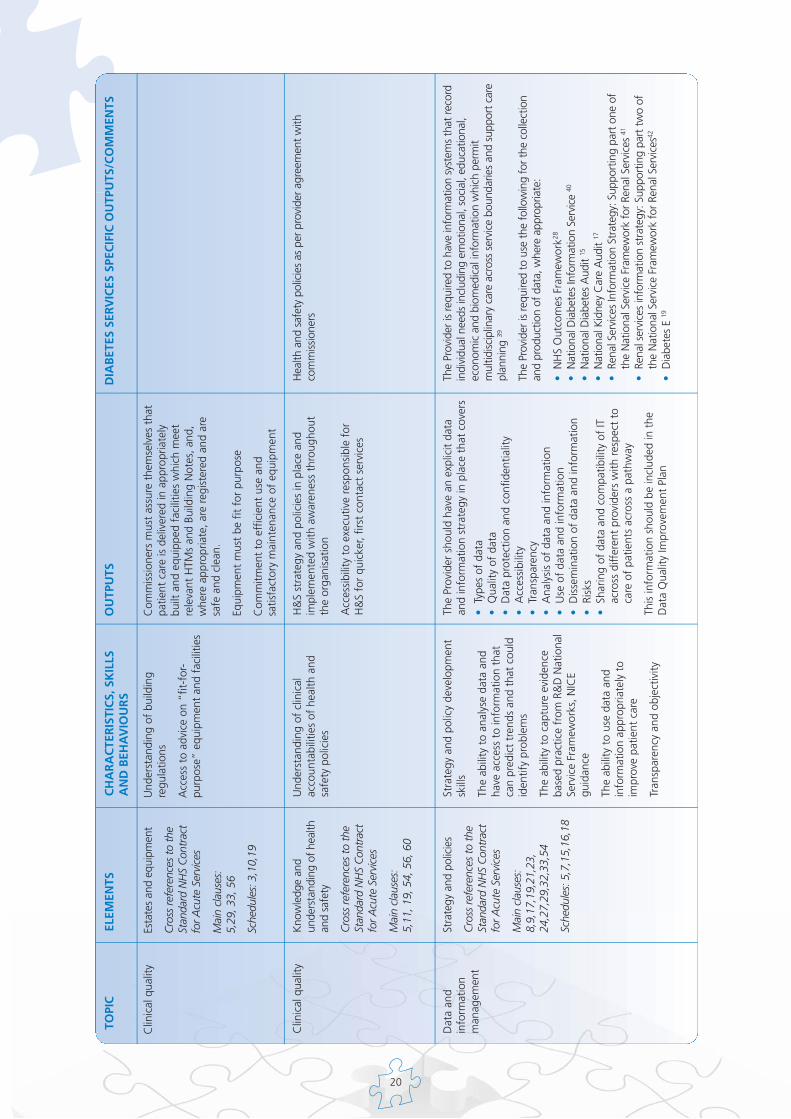
• have integrated information systems that recordindividual needs including emotional, social,
educational, economic and biomedicalinformation which permit multidisciplinary careacross service boundaries and support careplanningvii
• produce information on the outcomes ofdiabetes care including contributing to nationaldata collections and audits
• have adequate governance arrangements, e.g.local mortality and morbidity meetings ondiabetes care to learn from errors and improvepatient safety
• take account of patient experience, includingPatient Reported Outcomes Measures, in thedevelopment and monitoring of servicedeliveryviii
• deliver the separate modules of care accordingto the best practice quality markers
• actively monitor the uptake of services,responding to non-attenders and monitoringcomplaints and untoward incidents
vii http://www.diabetes.nhs.uk/year_of_care/it/
viii http://www.ic.nhs.uk/proms

8
NH
S D
iab
etes
Dia
bet
es a
nd
kid
ney
car
e C
hro
nic
kid
ney
dis
ease
ris
k as
sess
men
t
Hea
lth
Nee
ds
Ass
essm
ent
Dia
gn
osi
s o
fd
iab
etes
See
com
mis
sion
ing
gu
ides
for
CY
P,
diag
nosi
s an
d co
ntin
uing
car
e an
d ol
der
peop
le
Ass
essm
ent
for
oth
er
po
ssib
le
com
plic
atio
ns
of
dia
bet
es
See
com
mis
sion
ing
gu
ides
for
CY
P,
diag
nosi
s an
d co
ntin
uing
car
e an
d ol
der
peop
le
Ass
essm
ent
of
ren
al f
un
ctio
n
E.g.
-Bl
ood
pres
sure
-al
bum
in/
crea
tinin
e ra
tio
-eG
FR
- se
rum
cre
atin
ine
-as
sess
men
t of
gl
ycae
mic
con
trol
-di
et
-sm
okin
g st
atus
-ch
eck
for
anae
mia
- ch
eck
for
bone
co
nditi
ons
Ad
vice
on
lif
esty
le
E.g.
- sm
okin
g-
diet
(sal
t in
take
et
c)
Trea
t h
yper
ten
sio
n,
if p
rese
nt,
ac
cord
ing
to
ag
reed
p
roto
cols
Rev
iew
of
resu
lts
of
ren
al
fun
ctio
n t
ests
Evid
ence
o
f ch
ron
ic
kid
ney
dis
ease
?
Yes
Stag
ing
of
chro
nic
ki
dn
ey
dis
ease
Ren
al f
un
ctio
n
det
erio
rati
ng
?
No
Yes
Ref
erra
l to
sp
ecia
list
care
re
qu
ired
?
Yes
No
Go
to
p
age
9
Rev
iew
dat
e ag
reed
-U
pdat
e ca
re p
lan
-U
pdat
e ca
re p
lan
No
-fr
eque
ncy
of
revi
ew a
ccor
ding
to
agr
eed
prot
ocol
s
-up
date
car
e pl
an
-se
e N
ICE
guid
ance
on
chro
nic
kidn
ey
dise
ase
Man
agem
ent
of
chro
nic
kid
ney
d
isea
se in
clu
din
g
anae
mia
an
d b
on
e co
nd
itio
ns
Diabetes and Kidney Care ServicesIntervention Map

9
NH
S D
iab
etes
Dia
bet
es a
nd
kid
ney
car
e Sp
ecia
list
kid
ney
car
e
Fro
m
pag
e 8
Nep
hro
log
y as
sess
men
t at
jo
int
ren
al/
dia
bet
esse
rvic
e
chec
k:
-re
nal f
unct
ion
- bl
ood
pres
sure
-ca
rdio
vasc
ular
ris
k
- an
aem
ia
- bo
ne c
ondi
tions
-gl
ycae
mic
con
trol
-ch
eck
feet
Ren
al
Rep
lace
men
tTh
erap
y p
lan
nin
g
req
uir
ed?
Yes No
Ad
vice
on
lif
esty
le
Ad
vice
on
o
ther
ris
k fa
cto
rs f
or
chro
nic
kid
ney
d
isea
se
Rev
iew
dat
e ag
reed
-up
date
car
e pl
an-
e.g.
Chr
onic
N
SAID
use
etc
E.g.
Sm
okin
g-
Exer
cise
-di
etGo
to
p
age
10
Ap
pro
pri
ate
med
icat
ion
Man
agem
ent
of
com
plic
atio
ns
of
kid
ney
d
isea
se

10
NH
S D
iab
etes
Dia
bet
es a
nd
kid
ney
car
e Sp
ecia
list
kid
ney
car
e
Fro
m
pag
e 9
Ren
al
Rep
lace
men
t Th
erap
y p
lan
nin
g
init
iate
d
Ren
al
Rep
lace
men
tTh
erap
y tr
eatm
ent
op
tio
ns
dis
cuss
ed
Ren
alR
epla
cem
ent
Ther
apy
inap
pro
pri
ate?
Yes No
See
com
mis
sio
nin
g
gu
ide
for
End
of
Life
C
are
Ren
al
Rep
lace
men
t Th
erap
y o
pti
on
ag
reed
an
d
imp
lem
ente
d
-di
alys
is
-tr
ansp
lant
-co
nsid
er r
efer
ral
for
sim
ulta
neou
s pa
ncre
as a
nd
kidn
ey
tran
spla
ntat
ion
acco
rdin
g to
ag
reed
pro
toco
ls
Co
nti
nu
ed
man
agem
ent
of
dia
bet
es in
clu
din
g
com
plic
atio
ns
of
dia
bet
es
Man
agem
ent
of
cho
sen
Ren
al
Rep
lace
men
tTh
erap
y o
pti
on
ac
cord
ing
to
ag
reed
pro
toco
ls
-up
date
car
e pl
an
Rev
iew
of
cho
sen
R
enal
R
epla
cem
ent
Ther
apy
op
tio
n
acco
rdin
g t
o
agre
ed p
roto
cols
-ar
rang
emen
ts f
or
vasc
ular
acc
ess,
if
requ
ired
-pa
tient
edu
catio
n-
dial
ysis
Ass
essm
ent
of
card
iova
scu
lar
risk
Co
nti
nu
ing
man
agem
ent
of
com
plic
atio
ns
of
kid
ney
dis
ease
11
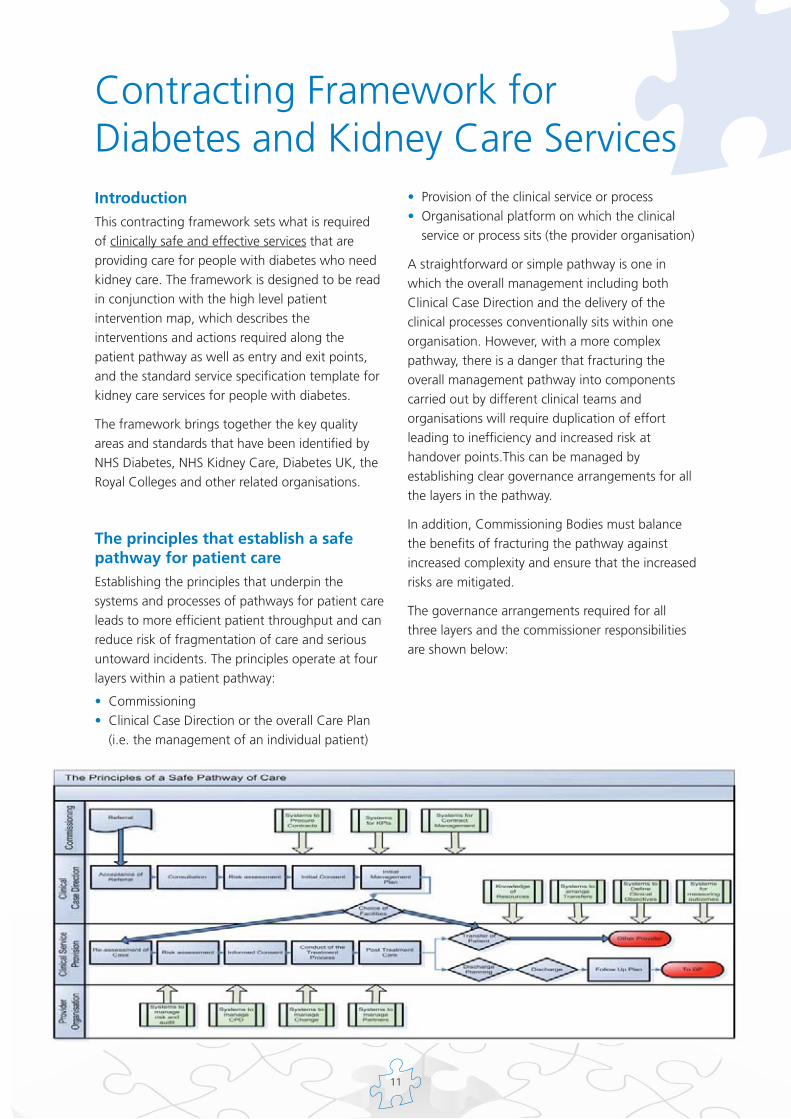
IntroductionThis contracting framework sets what is requiredof clinically safe and effective services that areproviding care for people with diabetes who needkidney care. The framework is designed to be readin conjunction with the high level patientintervention map, which describes theinterventions and actions required along thepatient pathway as well as entry and exit points,and the standard service specification template forkidney care services for people with diabetes.
The framework brings together the key qualityareas and standards that have been identified byNHS Diabetes, NHS Kidney Care, Diabetes UK, theRoyal Colleges and other related organisations.
The principles that establish a safepathway for patient care Establishing the principles that underpin thesystems and processes of pathways for patient careleads to more efficient patient throughput and canreduce risk of fragmentation of care and seriousuntoward incidents. The principles operate at fourlayers within a patient pathway:
• Commissioning• Clinical Case Direction or the overall Care Plan
(i.e. the management of an individual patient)
• Provision of the clinical service or process• Organisational platform on which the clinical
service or process sits (the provider organisation)
A straightforward or simple pathway is one inwhich the overall management including bothClinical Case Direction and the delivery of theclinical processes conventionally sits within oneorganisation. However, with a more complexpathway, there is a danger that fracturing theoverall management pathway into componentscarried out by different clinical teams andorganisations will require duplication of effortleading to inefficiency and increased risk athandover points.This can be managed byestablishing clear governance arrangements for allthe layers in the pathway.
In addition, Commissioning Bodies must balancethe benefits of fracturing the pathway againstincreased complexity and ensure that the increasedrisks are mitigated.
The governance arrangements required for allthree layers and the commissioner responsibilitiesare shown below:
Contracting Framework forDiabetes and Kidney Care Services

12
In essence, at each level, there are governancearrangements to ensure sound and safe systems ofdelivery of patient care with clear lines ofaccountability between each level.
Diabetes and Kidney Care ServicesThe key principles of good diabetes and kidneycare services is to provide a high quality servicethat is reliable in terms of delivery and timelyaccess for patients requiring that care.
Care of people with diabetes who have renalcomplications is provided by a number of differentteams in the primary, community and acutesetting. It is essential that there is co-ordination ofcare of patients through the care planning processand that the nephrologist/diabetes physiciansretain joint responsibility for overall patient careacross the whole pathway and retain overallresponsibility for the management of side effectsand further complications.
The initial management and continuing care ofindividuals with diabetes should include anassessment of their emotional and psychologicalwell-being, together with timely access toappropriate psychological and biological/psychiatricinterventions. Mental health disorders can posesignificant barriers to diabetes care and thereforemental health stability is vital for good self care1.
The services themselves will also have clinicaloversight and accountability for governancepurposes.
This contracting framework focuses on peoplewith diabetes, including children and young peopleand older people, who require care for the renalcomplications of diabetes. This contractingframework should also be read in conjunction withthe diabetes commissioning guides for childrenand young people, prevention and risk assessment,
diagnosis and continuing care, older people, Endof Life Care and follow the principles for theeffective commissioning of services for people withLearning Disabilities2.
Ensuring qualityCommissioning Bodies should ensure that thediabetes and kidney care services commissionedare of the highest quality. There may, in addition,be some organisations that wish to offer theirservices, but do not have a history of providingsuch care.
i) For provider organisations already involved inthe delivery of diabetes and kidney careservices, there should be retrospective evidenceof systems being in place, implemented andworking.
ii) For organisations new to the arena, thecommissioner should reassure itself that theprovider has the organisational attributes,governance arrangements, systems andprocesses set up to provide the platform forsafe and effective delivery of diabetes andkidney care services to be provided.
This framework describes what theCommissioning Body needs to ensure ispresent or addressed in its discussions withthe provider organisation.
Under the ‘elements’ column there are crossreferences to the Standard NHS Contract for AcuteServices– bilateral (main clauses and schedules)3.(The cross references also apply to the clauses andschedules in the Standard NHS Contract forCommunity Services).This is to assist commissionersand providers in having an overview of how theelements link to the Standard NHS Contract. Someof the areas are open to interpretation andconsequently the references are not exhaustive.

13
TOPI
CEL
EMEN
TSC
HA
RA
CTE
RIS
TIC
S, S
KIL
LSA
ND
BEH
AV
IOU
RS
OU
TPU
TSD
IAB
ETES
SER
VIC
ES S
PEC
IFIC
OU
TPU
TS/C
OM
MEN
TS
Gov
erna
nce
Lead
ersh
ip
Cro
ss re
fere
nces
to th
eSt
anda
rd N
HS
Con
trac
tfo
r Acu
te S
ervi
ces
Mai
n cl
ause
s:11
,16,
19,3
3,48
,49,
51,5
3, 6
0
Sche
dule
s: 1
0
Cla
rity
of t
he o
rgan
isat
ion’
spu
rpos
e w
ith e
xplic
itco
mm
itmen
t to
pro
vidi
ng h
igh
qual
ity s
ervi
ces
A c
ultu
re t
hat
dem
onst
rate
s an
open
lear
ning
eth
os
An
orga
nisa
tion
that
is le
gal a
ndet
hica
l in
all i
ts a
ctiv
ities
Prov
ider
mus
t ha
ve o
rgan
isat
iona
l str
uctu
reth
at p
rovi
des
lead
ersh
ip f
or a
ll pr
ofes
sion
san
d di
scip
lines
In p
artic
ular
, the
re m
ust
be a
cor
pora
tecl
inic
al d
irect
or w
ith t
he r
espo
nsib
ility
and
acco
unta
bilit
y fo
r th
e cl
inic
al s
ervi
ce
Ther
e m
ust
be a
lear
ning
fra
mew
ork
in t
heor
gani
satio
n
Ther
e sh
ould
be
a de
signa
ted
clin
ical
dire
ctor
with
resp
onsib
ility
and
acco
unta
bilit
y fo
r dia
bete
s an
d ki
dney
car
e se
rvic
es
Gov
erna
nce
Inte
grat
ed G
over
nanc
e
Cro
ss re
fere
nces
to th
eSt
anda
rd N
HS
Con
trac
tfo
r Acu
te S
ervi
ces
Mai
n cl
ause
s:11
,19,
27,4
8,49
,51,
53,5
4,56
, 60
Sche
dule
s:
10
An
orga
nisa
tion
that
is g
uide
d by
the
prin
cipl
es o
f go
odgo
vern
ance
:
- cl
arity
of
purp
ose
- pa
rtic
ipat
ion
and
enga
gem
ent
- ru
le o
f la
w-
tran
spar
ency
- re
spon
sive
ness
- eq
uity
and
incl
usiv
enes
s-
effe
ctiv
enes
s an
d ef
ficie
ncy
- ac
coun
tabi
lity
An
orga
nisa
tion
that
acc
epts
resp
onsi
bilit
y an
d ac
coun
tabi
lity
for
all i
ts a
ctio
ns
Cle
ar o
rgan
isat
iona
l and
int
egra
ted
gove
rnan
ce s
yste
ms
and
stru
ctur
es in
pla
cew
ith c
lear
line
s of
acc
ount
abili
ty a
ndre
spon
sibi
litie
s fo
r al
l fun
ctio
ns. T
his
incl
udes
inte
rfac
es a
nd t
rans
ition
s be
twee
nse
rvic
es
Qua
lity
Gov
erna
nce
in th
e N
HS.
A g
uide
for p
rovi
der b
oard
s4
Gov
erna
nce
Clin
ical
Gov
erna
nce
Cro
ss re
fere
nces
to th
eSt
anda
rd N
HS
Con
trac
tfo
r Acu
te S
ervi
ces
Mai
n cl
ause
s:4,
4A,6
,9,1
0,12
,14,
15,1
6,17
,19,
21,
27,2
9,31
,32,
33,
48,4
9,51
,53,
54
Sche
dule
s:
3 (p
arts
1,2,
4,4A
,4B,
4C,5
,6),
7,10
,12,
18,2
0
Expl
icit
com
mitm
ent
to q
ualit
yan
d pa
tient
saf
ety
Patie
nt f
ocus
ed w
ith r
espe
ct f
orth
e pe
rson
al w
ishe
s of
pat
ient
s in
all a
spec
ts o
f th
eir
care
A c
omm
itmen
t to
inno
vatio
n an
dco
ntin
uous
impr
ovem
ent
Clin
ical
Gov
erna
nce
syst
ems
and
polic
ies
shou
ld b
e in
pla
ce a
nd in
tegr
ated
into
orga
nisa
tiona
l gov
erna
nce
with
cle
ar li
nes
of a
ccou
ntab
ility
and
res
pons
ibili
ty f
or a
llcl
inic
al g
over
nanc
e fu
nctio
ns
e.g.
•C
linic
al A
udit
•C
linic
al R
isk
Man
agem
ent
•U
ntow
ard
Inci
dent
Rep
ortin
g•
Infe
ctio
n C
ontr
ol•
Med
icin
es M
anag
emen
t•
Info
rmed
Con
sent
•Ra
isin
g C
once
rns
All
sub-
cont
ract
ors
mus
t mee
t gov
erna
nce
and
lead
ersh
ipar
rang
emen
ts o
f the
mai
n pr
ovid
er o
rgan
isatio
n
Com
miss
ione
r, pr
ovid
er a
nd N
HS
Litig
atio
n A
utho
rity
mus
tre
view
the
Clin
ical
Neg
ligen
ce S
chem
e fo
r Tru
sts
arra
ngem
ents
/or o
ther
org
anisa
tiona
l / p
rofe
ssio
nal i
ndem
nity
arr
ange
men
ts
The
serv
ice
shou
ld h
ave
in p
lace
writ
ten
prot
ocol
s an
dpr
oced
ures
def
inin
g cl
ear l
ines
of a
ccou
ntab
ility
and
resp
onsib
ility
.
The
serv
ice
is re
quire
d to
com
ply
with
gui
delin
es, p
ublic
hea
lthgu
idan
ce a
nd a
ppra
isals
publ
ished
by
the
Nat
iona
l Ins
titut
e fo
rH
ealth
and
Clin
ical
Exc
elle
nce
that
are
rele
vant
to th
e ca
repr
ovid
ed b
y th
e se
rvic
e 5

14
TOPI
CEL
EMEN
TSC
HA
RA
CTE
RIS
TIC
S, S
KIL
LSA
ND
BEH
AV
IOU
RS
OU
TPU
TSD
IAB
ETES
SER
VIC
ES S
PEC
IFIC
OU
TPU
TS/C
OM
MEN
TS
Gov
erna
nce
Clin
ical
Gov
erna
nce
•St
aff
Dev
elop
men
t•
Com
plai
nts
Man
agem
ent
•Pa
tient
and
Pub
lic In
volv
emen
t•
Patie
nt d
igni
ty a
nd r
espe
ct
•Eq
ualit
y an
d di
vers
ity•
Intr
oduc
ing
new
tec
hnol
ogie
s an
dtr
eatm
ents
•A
n ex
tern
ally
acc
redi
ted
Qua
lity
Ass
uran
ce s
yste
m a
nd in
tern
al e
rror
repo
rtin
g in
volv
ing
all s
taff
gro
ups.
CG
sys
tem
s sh
ould
hav
e cl
ear
and
dem
onst
rabl
e lin
ks t
o ot
her
NH
S sy
stem
sw
ith c
olla
bora
tive
CG
act
iviti
es a
nd s
harin
gof
exp
erie
nce
and
lear
ning
Prov
ider
sho
uld
prod
uce
annu
al C
linic
alG
over
nanc
e re
port
s as
par
t of
NH
S C
Gre
port
ing
syst
em
Prov
ider
s ar
e re
quire
d to
agr
eeC
omm
issi
onin
g fo
r Q
ualit
y an
d In
nova
tion
sche
mes
(CQ
UIN
) for
dia
bete
s ca
re, e
.g.
mod
el C
QU
IN s
chem
e pr
opos
ed b
y th
e N
HS
Inst
itute
for
Inno
vatio
n an
d Im
prov
emen
t 13
In a
dditi
on, t
he s
ervi
ce is
requ
ired
to c
ompl
y w
ith th
e fo
llow
ing:
i. G
uida
nce
publ
ishe
d by
NIC
E
•Ea
rly id
entif
icat
ion
and
man
agem
ent o
f chr
onic
kid
ney
dise
ase
in a
dults
in p
rimar
y an
d se
cond
ary
care
6
•A
naem
ia m
anag
emen
t in
peop
le w
ith c
hron
ic k
idne
y di
seas
e 7
•Th
e cl
inic
al e
ffec
tiven
ess
and
cost
eff
ectiv
enes
s of
pat
ient
educ
atio
n m
odel
s fo
r dia
bete
s 8
•M
edic
ines
adh
eren
ce: i
nvol
ving
pat
ient
s in
dec
ision
s ab
out
pres
crib
ed m
edic
ines
and
sup
port
ing
adhe
renc
e 9
The
serv
ice
is al
so re
quire
d to
com
ply
with
:
•cl
inic
al g
uide
lines
for T
ype
2 D
iabe
tes
Mel
litus
pro
duce
d by
the
Euro
pean
Dia
bete
s W
orki
ng P
arty
for O
lder
Peo
ple
10
•Re
nal S
peci
fic M
anag
emen
t of M
edic
ines
11
•G
uide
lines
for L
CP
Dru
g Pr
escr
ibin
g in
Adv
ance
d C
hron
icK
idne
y D
isea
se 12
Clin
ical
qua
lity
Qua
lity
assu
ranc
e
Cro
ss re
fere
nces
to th
eSt
anda
rd N
HS
Con
trac
tfo
r Acu
te S
ervi
ces
Mai
n cl
ause
s:4,
4A,1
2,16
,17,
18,
19,2
0,21
, 31,
32,
33, 5
4
Sche
dule
s:
2,3
(par
ts 4
, 4A
,4B,
4C,5
,6)
7, 1
0,12
, 18,
20
Und
erst
andi
ng t
he c
once
pt o
fcl
inic
al q
ualit
y
Has
con
cern
for
qua
lity
whi
lew
orki
ng e
ffic
ient
ly
An
unde
rsta
ndin
g of
the
use
of
audi
t, p
atie
nt a
nd s
taff
fee
dbac
kto
impr
ove
qual
ity
An
orga
nisa
tion
that
pro
vide
scl
arity
of
obje
ctiv
es a
nd p
rom
otes
refle
ctiv
e pr
actic
e to
impr
ove
qual
ity o
f pa
tient
car
e
Qua
lity
assu
ranc
e sy
stem
s m
ust
be in
pla
cean
d ap
prov
ed b
y co
mm
issi
onin
g bo
dy w
ithre
gula
r re
port
ing
of o
utco
mes
Prov
ider
s ar
e re
quire
d to
pub
lish
qual
ityac
coun
ts f
or t
he p
ublic
rep
ortin
g of
qua
lity
incl
udin
g sa
fety
, exp
erie
nce
and
outc
omes
Prov
ider
s sh
ould
par
ticip
ate
in n
atio
nal
audi
t pr
ogra
mm
es
Dia
bete
s an
d K
idne
y C
are
serv
ices
mus
t com
ply
with
the
perf
orm
ance
mea
sure
s re
quire
d of
NH
S se
rvic
es, i
.e m
eetin
g: 14
•Re
ferr
al to
Tre
atm
ent w
aits
(95t
h pe
rcen
tile
mea
sure
s)
•A
&E
Qua
lity
Indi
cato
rs•
Am
bula
nce
resp
onse
tim
es
The
serv
ices
are
requ
ired
to p
artic
ipat
e in
the
follo
win
gac
tiviti
es/p
rogr
amm
es:
•N
atio
nal D
iabe
tes
Aud
it 15
•N
atio
nal D
iabe
tes
Inpa
tient
Aud
it of
Acu
te T
rust
s 16
(NB
Prov
ider
s m
ay w
ish to
con
duct
add
ition
al a
udits
in th
e ar
eas
iden
tifie
d in
this
docu
men
t)•
Nat
iona
l Kid
ney
Car
e A
udit
17
•Pa
tient
Exp
erie
nce
Surv
eys
18
•D
iabe
tes
E 19
•Pa
tient
Rep
orte
d O
utco
mes
Mea
sure
s 20

15
TOPI
CEL
EMEN
TSC
HA
RA
CTE
RIS
TIC
S, S
KIL
LSA
ND
BEH
AV
IOU
RS
OU
TPU
TSD
IAB
ETES
SER
VIC
ES S
PEC
IFIC
OU
TPU
TS/C
OM
MEN
TS
Clin
ical
qua
lity
Wor
kfor
ce/ s
taff
Clin
ical
sta
ff a
ttrib
utes
criti
cal t
o sa
fety
and
qual
ity o
f int
erve
ntio
ns
Cro
ss re
fere
nces
to th
eSt
anda
rd N
HS
Con
trac
tfo
r Acu
te S
ervi
ces
Mai
n cl
ause
s:11
,16,
26,3
3, 4
8 ,5
6
The
prov
ider
org
anis
atio
n ha
ssy
stem
s an
d pr
oced
ures
in p
lace
to a
ssur
e th
e co
mm
issi
oner
tha
tth
eir
clin
ical
tea
m h
as t
hene
cess
ary
qual
ifica
tions
, ski
lls,
know
ledg
e an
d ex
perie
nce
tode
liver
the
ser
vice
Staf
f ar
e co
mpe
tent
and
fit
for
purp
ose
Prov
ider
to
satis
fy c
omm
issi
oner
tha
t al
lst
aff
have
cur
rent
app
rais
al, c
lear
ance
s an
dre
gist
ratio
n ch
ecks
and
hav
e de
mon
stra
ted
com
pete
nce
in a
ll pr
oced
ures
rel
evan
t to
path
way
.
Prov
ider
to s
atisf
y co
mm
issio
ner t
hat t
hey
can
recr
uit (
orpr
ocur
e) a
nd re
tain
a c
ompe
tent
clin
ical
team
to d
eliv
er th
ese
rvic
e
Spec
ific
qual
ifica
tions
requ
ired
of h
ealth
pro
fess
iona
ls pr
ovid
ing
the
serv
ice
are:
•Fo
r med
ical
pra
ctiti
oner
s:
o D
iabe
tes:
regi
stra
tion
with
the
GM
C a
nd e
vide
nce
offu
rthe
r qua
lific
atio
n in
dia
bete
s ca
re o
r exp
erie
nce
with
indi
abet
es c
linic
o N
ephr
olog
y: re
gist
ratio
n w
ith th
e G
MC
and
evi
denc
e of
furt
her q
ualif
icat
ion
in re
nal m
edic
ine
•N
urse
s:
o D
iabe
tes
: reg
istra
tion
with
the
NM
C, f
urth
er e
vide
nce
ofqu
alifi
catio
n in
dia
bete
s ca
re o
r exp
erie
nce
with
in d
iabe
tes
clin
ic a
nd a
n in
tere
st in
nep
hrop
athy
21
o N
ephr
olog
y: re
gist
ratio
n w
ith th
e N
MC
and
furt
her
evid
ence
of q
ualif
icat
ion
in re
nal m
edic
ine
or e
xper
ienc
ew
ithin
nep
hrol
ogy
clin
ic•
Die
titia
ns 21
:o
Dia
bete
s: re
gist
ratio
n w
ith th
e H
PC a
nd fu
rthe
r evi
denc
eof
qua
lific
atio
n in
dia
bete
s ca
re o
r exp
erie
nce
with
indi
abet
es c
linic
o N
ephr
olog
y: re
gist
ratio
n w
ith th
e H
PC a
nd fu
rthe
rev
iden
ce o
f qua
lific
atio
n in
die
tetic
s an
d re
nal m
edic
ine
orex
perie
nce
with
in n
ephr
olog
y cl
inic
•Po
diat
rists
:o
Dia
bete
s: re
gist
ratio
n w
ith th
e H
PC a
nd fu
rthe
r evi
denc
eof
qua
lific
atio
n in
dia
bete
s ca
re o
r exp
erie
nce
with
indi
abet
es c
linic
Hea
lthca
re p
rofe
ssio
nals
invo
lved
in d
eliv
erin
g ca
re fo
r peo
ple
with
dia
bete
s w
ho h
ave
rena
l com
plic
atio
ns a
re re
quire
d to
hav
eth
e re
leva
nt c
ompe
tenc
ies
in th
e m
anag
emen
t of22
:
•di
abet
es
•C
hron
ic K
idne
y D
isea
se

16
TOPI
CEL
EMEN
TSC
HA
RA
CTE
RIS
TIC
S, S
KIL
LSA
ND
BEH
AV
IOU
RS
OU
TPU
TSD
IAB
ETES
SER
VIC
ES S
PEC
IFIC
OU
TPU
TS/C
OM
MEN
TS
Clin
ical
qua
lity
Wor
kfor
ce/ s
taff
Clin
ical
sta
ffco
mpe
tenc
ies
in u
se o
feq
uipm
ent
Cro
ss re
fere
nces
to th
eSt
anda
rd N
HS
Con
trac
tfo
r Acu
te S
ervi
ces
Mai
n cl
ause
s:11
, 16,
17,
21,
26,
33
The
prov
ider
org
anis
atio
n ha
ssy
stem
s in
pla
ce t
o as
sure
the
com
mis
sion
er t
hat
thei
r cl
inic
alte
am a
re c
ompe
tent
to
use
all
equi
pmen
t ne
eded
to
deliv
er t
hese
rvic
e
Prov
ider
to
satis
fy t
he c
omm
issi
oner
tha
t al
lst
aff
have
had
doc
umen
ted
com
pete
nce
asse
ssm
ent
rela
tive
to a
ll eq
uipm
ent
used
inco
ntra
ct.
All
heal
thca
re p
rofe
ssio
nals
invo
lved
in d
eliv
erin
g ca
re fo
r peo
ple
with
dia
bete
s w
ho h
ave
card
iova
scul
ar c
ompl
icat
ions
are
requ
ired
to h
ave
the
rele
vant
com
pete
ncie
s in
usin
g ap
prop
riate
equi
pmen
t e.g
. blo
od g
luco
se a
nd k
eton
e m
onito
rs, i
nsul
inde
liver
y de
vice
s in
clud
ing
insu
lin p
umps
etc
Clin
ical
qua
lity
Wor
kfor
ce /
staf
f
Dev
elop
men
t
Cro
ss re
fere
nces
to th
eSt
anda
rd N
HS
Con
trac
tfo
r Acu
te S
ervi
ces
Mai
n cl
ause
s:11
,16,
19,3
0, 4
8
The
prov
ider
org
anis
atio
n ha
ssy
stem
s in
pla
ce t
o as
sure
the
com
mis
sion
er t
hat
thei
r cl
inic
alte
am is
for
mal
ly in
duct
ed a
ndre
ceiv
es o
ngoi
ng a
ssis
tanc
e to
deve
lop
thei
r sk
ills,
kno
wle
dge
and
expe
rienc
e t
o en
sure
tha
tth
ey a
re a
lway
s fu
lly u
pdat
ed
Prov
ider
to
satis
fy c
omm
issi
oner
of
thei
rco
mm
itmen
t to
indu
ctio
n an
d C
PD r
elev
ant
to r
oles
Prov
ider
to
satis
fy t
he c
omm
issi
oner
of
thei
rco
mm
itmen
t to
tra
in s
taff
to
mee
t fu
ture
serv
ice
need
s
All
Hea
lth C
are
prof
essi
onal
s sh
ould
hav
e su
ffic
ient
stu
dy le
ave
allo
catio
n (t
ime
and
finan
ce) t
o en
able
them
to d
evel
op s
kills
appr
opria
tely
Clin
ical
qua
lity
Regi
stra
tion
and
licen
sing
Cro
ss re
fere
nces
to th
eSt
anda
rd N
HS
Con
trac
tfo
r Acu
te S
ervi
ces
Mai
n cl
ause
s:4,
4A,5
,9,1
0,11
,12,
14,1
5,16
17,1
8,19
,21,
26,
27,2
9,33
,34,
35,
3643
,48,
49,5
253
,54,
56,6
0
Sche
dule
: 2,
3,4,
5,6,
8,10
,12
,13,
15,1
7,
19, 2
0
The
Prov
ider
is r
equi
red
to b
ere
gist
ered
with
the
Car
e Q
ualit
yC
omm
issi
on t
o de
mon
stra
te t
hat
is m
eets
the
ess
entia
l sta
ndar
dsof
qua
lity
and
safe
ty f
or t
here
gula
ted
activ
ities
del
iver
ed.
The
Prov
ider
is r
equi
red
to b
elic
ense
d w
ith t
he N
HS
Econ
omic
Regu
lato
r (M
onito
r) in
ord
er t
opr
ovid
e N
HS
care
.
Com
plia
nce
with
the
Car
e Q
ualit
yC
omm
issi
on a
nd M
onito
r re
quire
men
tsC
ompl
ianc
e w
ith th
e fo
llow
ing
Nat
iona
l Ser
vice
Fra
mew
orks
,w
here
app
licab
le:
•Re
nal N
SF 23
•O
lder
Peo
ple’
s N
SF 24
•N
SF fo
r Chi
ldre
n, Y
oung
Peo
ple
and
Mat
erni
ty S
ervi
ces
25
•Th
e M
enta
l Hea
lth S
trat
egy26
•Lo
ng T
erm
Con
ditio
ns N
SF 27
Com
plia
nce
with
Car
e Q
ualit
y C
omm
issi
on R
evie
ws

17
TOPI
CEL
EMEN
TSC
HA
RA
CTE
RIS
TIC
S, S
KIL
LSA
ND
BEH
AV
IOU
RS
OU
TPU
TSD
IAB
ETES
SER
VIC
ES S
PEC
IFIC
OU
TPU
TS/C
OM
MEN
TS
Clin
ical
qua
lity
Patie
nt p
athw
ay
Cro
ss re
fere
nces
to th
eSt
anda
rd N
HS
Con
trac
tfo
r Acu
te S
ervi
ces
Mai
n cl
ause
s:4,
4A,9
,10,
12,1
4,15
,16,
17,
18,
19,2
0,21
,27,
29,
32 ,3
3, 3
4,35
,36,
54
Sche
dule
s:
3 (p
arts
1 a
nd 2
)
Resp
onsi
vene
ss a
nd p
artic
ipat
ive
appr
oach
to
incl
udin
g pa
tient
s’vi
ews
abou
t th
eir
care
in t
hede
sign
of
care
pat
hway
s
Col
labo
ratio
n w
ith o
ther
orga
nisa
tions
invo
lved
in t
hepa
tient
pat
hway
to
prov
ide
ase
amle
ss p
athw
ay o
f ca
re
All
poss
ible
ent
ry a
nd e
xit
poin
ts m
ust
bede
fined
with
com
preh
ensi
ve p
atie
ntpa
thw
ays
that
fac
ilita
te s
moo
th p
assa
gean
d ef
fect
ive,
eff
icie
nt c
are
for
patie
nts
All
inte
rfac
es in
the
pat
hway
mus
t be
defin
ed s
o th
at c
ontin
uity
of
clin
ical
car
e is
ensu
red
with
no
frac
turin
g of
the
pat
hway
Ther
e m
ust
be s
peci
ficat
ion
of c
lear
timel
ines
and
ale
rt m
echa
nism
s fo
rpo
tent
ial b
reac
hes
Ther
e sh
ould
be
audi
t of
pat
hway
to
ensu
reth
at s
tand
ards
are
met
Ther
e m
ust
be e
xplic
it sp
ecifi
catio
n of
prov
ider
and
com
mis
sion
er r
espo
nsib
ilitie
sfo
r th
e w
hole
pat
ient
epi
sode
fro
mre
gist
ratio
n to
fin
al d
isch
arge
Acc
ount
abili
ties
shou
ld b
e ag
reed
and
docu
men
ted
by a
ll st
akeh
olde
rs
Ther
e ar
e a
num
ber
of s
ervi
ces
supp
ortin
gpa
tient
s w
ith d
iabe
tes
and
ther
e m
ust
becl
ear
sub
cont
ract
s st
atin
g th
e re
ferr
alcr
iteria
and
acc
ess
to t
hese
sup
port
ing
serv
ices
.
The
path
way
sho
uld
follo
w th
e pr
inci
ples
set
out
by
the
Gen
eric
Long
Ter
m C
ondi
tions
mod
el 30
. Thi
s in
clud
es:
•St
ratif
ying
the
leve
ls of
nee
d an
d ris
k •
Cas
e m
anag
emen
t•
Pers
onal
ised
car
e pl
anni
ng•
Supp
ortin
g pe
ople
to s
elf c
are
•A
ssis
tive
tech
nolo
gy
The
key
elem
ents
of d
iabe
tes
and
kidn
ey c
are
serv
ices
sho
uld
incl
ude
•C
hron
ic k
idne
y di
seas
e ris
k as
sess
men
t and
initi
al m
anag
emen
t •
The
early
iden
tific
atio
n an
d m
anag
emen
t of c
ardi
ovas
cula
rco
mpl
icat
ions
of d
iabe
tes
31
(see
als
o th
e C
omm
issi
onin
g G
uide
for c
ardi
ovas
cula
r ser
vice
s fo
rpe
ople
with
dia
bete
s) 2
•Sp
ecia
list k
idne
y ca
re
1. C
hron
ic k
idne
y di
seas
e ris
k as
sess
men
t and
initi
al m
anag
emen
t
•Th
ere
shou
ld b
e ag
reed
pro
toco
ls fo
r ass
essin
g th
e ris
k of
: o
diab
etes
o th
e ef
fect
s of
sm
okin
g o
chro
nic
kidn
ey d
isea
seo
hype
rten
sion
(e.g
. NH
S H
ealth
Che
cks
for 4
0 -7
4 ye
ar o
lds32
).•
Ther
e sh
ould
be
agre
ed p
roto
cols
for:
o th
e m
anag
emen
t of c
hron
ic k
idne
y di
seas
e o
man
agem
ent o
f ana
emia
o m
anag
emen
t of b
one
cond
ition
s
Clin
ical
qua
lity
Out
com
es
Cro
ss re
fere
nces
to th
eSt
anda
rd N
HS
Con
trac
tfo
r Acu
te S
ervi
ces
Mai
n cl
ause
s:4,
4A,1
0,14
,15,
16,2
1
Sche
dule
:3
(par
t 5),
5 (p
arts
1,2
,3),
12
Com
preh
ensi
ve u
nder
stan
ding
and
com
mitm
ent
to d
eliv
erin
gan
d im
prov
ing
outc
omes
of
care
Com
plia
nce
with
the
NH
S O
utco
mes
Fram
ewor
k28C
ompl
ianc
e w
ith th
e Q
ualit
y St
anda
rds
for D
iabe
tes,
spe
cific
ally
29

18
TOPI
CEL
EMEN
TSC
HA
RA
CTE
RIS
TIC
S, S
KIL
LSA
ND
BEH
AV
IOU
RS
OU
TPU
TSD
IAB
ETES
SER
VIC
ES S
PEC
IFIC
OU
TPU
TS/C
OM
MEN
TS
Clin
ical
qua
lity
Patie
nt p
athw
ayA
t en
try
to p
athw
ay:
The
Com
mis
sion
er s
houl
d as
sure
them
selv
es t
hat
the
prov
ider
has
sys
tem
san
d pr
oces
ses
in p
lace
to
i) re
gist
er p
atie
nts
ii) c
olle
ct r
elev
ant
clin
ical
and
adm
inis
trat
ive
data
iii) m
anag
e th
e ap
poin
tmen
t pr
oces
s,(r
eapp
oint
men
t an
d D
NA
pro
cess
, if
appr
opria
te)
iv) p
rovi
de in
form
atio
n to
pat
ient
sv)
und
erta
ke in
itial
ass
essm
ent
in t
heap
prop
riate
loca
tion
At
poin
t of
inte
rven
tion:
The
Com
mis
sion
er s
houl
d as
sure
them
selv
es t
hat
the
prov
ider
has
sys
tem
san
d pr
oces
ses
in p
lace
to
ensu
re t
hat:
i) th
e in
terv
entio
n is
con
duct
ed s
afel
yan
d in
acc
orda
nce
with
acc
epte
dqu
ality
sta
ndar
ds a
nd g
ood
clin
ical
prac
tice.
ii) t
he p
atie
nt r
ecei
ves
appr
opria
te c
are
durin
g th
e in
terv
entio
n(s)
, inc
ludi
ng o
ntr
eatm
ent
revi
ew a
nd s
uppo
rt, i
nac
cord
ance
with
bes
t cl
inic
al p
ract
ice
iii) w
here
clin
ical
em
erge
ncie
s or
com
plic
atio
ns d
o oc
cur
they
are
man
aged
in a
ccor
danc
e w
ith b
est
clin
ical
pra
ctic
eiv
) the
inte
rven
tion
is c
arrie
d ou
t in
afa
cilit
y w
hich
pro
vide
s a
safe
envi
ronm
ent
of c
are
and
min
imis
esris
k to
pat
ient
s, s
taff
and
vis
itors
v) t
he in
terv
entio
n is
und
erta
ken
by s
taff
with
the
nec
essa
ry q
ualif
icat
ions
, ski
lls,
expe
rienc
e an
d co
mpe
tenc
e vi
) The
re a
re a
rran
gem
ents
for
the
man
agem
ent
of o
ut o
f ho
urs
care
acco
rdin
g to
bes
t cl
inic
al p
ract
ice
o m
anag
emen
t of h
yper
tens
ion
o w
hen
to re
fer f
or s
peci
alist
rena
l/dia
bete
s ca
re•
Ever
y pa
tient
with
chr
onic
kid
ney
dise
ase
shou
ld h
ave
aki
dney
car
e pl
an 33
2. T
he e
arly
iden
tific
atio
n an
d m
anag
emen
t of c
ardi
ovas
cula
rco
mpl
icat
ions
of d
iabe
tes
•th
ere
shou
ld b
e pr
otoc
ols
in p
lace
to id
entif
y an
d m
anag
e th
eca
rdio
vasc
ular
com
plic
atio
ns o
f dia
bete
s as
car
diac
co-
mor
bidi
ty h
as a
sig
nific
ant i
mpa
ct o
n re
nal c
ompl
icat
ions
31
3. S
peci
alis
t kid
ney
care
•pe
ople
with
dia
bete
s w
ho n
eed
spec
ialis
t kid
ney
care
sho
uld
be s
een
by jo
int n
ephr
olog
y an
d di
abet
es s
ervi
ces
•th
ere
shou
ld b
e pr
otoc
ols
in p
lace
to s
cree
n, p
reve
nt a
ndm
anag
e ot
her c
ompl
icat
ions
of d
iabe
tes,
e.g
. foo
t car
e,ca
rdio
vasc
ular
car
e an
d ey
es•
the
man
agem
ent o
f a
pers
on w
ith d
iabe
tes
who
is a
dmitt
edfo
r man
agem
ent o
f the
ir re
nal c
ondi
tion
shou
ld fo
llow
the
prin
cipl
es s
et o
ut in
the
emer
genc
y an
d in
patie
ntco
mm
issio
ning
gui
de, i
.e.2
o ha
ve a
cces
s to
the
mul
tidis
cipl
inar
y sp
ecia
list d
iabe
tes
team
o ha
ve a
dmis
sion
and
dis
char
ge c
are
plan
so
have
clo
se li
aiso
n w
ith th
eir c
are
co-o
rdin
ator
o th
ere
shou
ld b
e pr
otoc
ols
in p
lace
to a
llow
pat
ient
s, w
hoar
e ab
le to
do
so, t
o se
lf m
anag
e th
eir d
iabe
tes
med
icat
ion.
Patie
nts
may
nee
d to
be
refe
rred
to th
e fo
llow
ing
serv
ices
as
part
of t
heir
kidn
ey c
are:
•Va
scul
ar s
ervi
ces
(for
vas
cula
r acc
ess)
•D
ialy
sis
34,3
5
•Tr
ansp
lant
atio
n se
rvic
es –
incl
udin
g ac
cess
to c
ombi
ned
kidn
ey a
nd p
ancr
eatic
tran
spla
ntat
ion
serv
ices
, as
appr
opria
te•
Rena
l Wel
fare
Off
icer
36
•En
d of
Life
Car
e 37
( see
also
Com
miss
ioni
ng G
uide
for
Dia
bete
s an
d En
d of
Life
Car
e 2 )

19
TOPI
CEL
EMEN
TSC
HA
RA
CTE
RIS
TIC
S, S
KIL
LSA
ND
BEH
AV
IOU
RS
OU
TPU
TSD
IAB
ETES
SER
VIC
ES S
PEC
IFIC
OU
TPU
TS/C
OM
MEN
TS
Clin
ical
qua
lity
Patie
nt p
athw
ayA
t ex
it fr
om p
athw
ay:
The
Com
mis
sion
er s
houl
d as
sure
them
selv
es t
hat
prov
ider
has
sys
tem
s an
dpr
oces
ses,
whi
ch a
re a
gree
d w
ith a
ll pa
rtie
san
d ne
twor
ks, i
n pl
ace
to:
i) un
dert
ake
tele
phon
e tr
iage
ii) m
ake
urge
nt o
nwar
d re
ferr
als
whe
relif
e-th
reat
enin
g co
nditi
ons
or s
erio
usun
expe
cted
pat
holo
gies
are
dis
cove
red
durin
g an
inte
rven
tion/
asse
ssm
ent
iii) e
nsur
e th
at p
atie
nts
rece
ive
disc
harg
ein
form
atio
n re
leva
nt t
o th
eir
inte
rven
tion
incl
udin
g ar
rang
emen
tsfo
r co
ntac
ting
the
prov
ider
and
fol
low
up if
req
uire
div
) pro
vide
tim
ely
feed
back
to
the
refe
rrer
re in
terv
entio
n, c
ompl
icat
ions
and
prop
osed
fol
low
up
v) e
nsur
e th
at t
he p
atie
nt r
ecei
ves
requ
ired
drug
s/dr
essi
ngs/
aids
vi) e
nsur
e th
at s
uppo
rt is
in p
lace
with
othe
r ca
re a
genc
ies
as a
ppro
pria
te
Prov
ider
s sh
ould
ens
ure
acce
ss to
tran
spor
t fac
ilitie
s to
ena
ble
atte
ndan
ce fo
r spe
cial
ist tr
eatm
ent,
as re
quire
d
Prov
ider
s ar
e re
quire
d to
take
not
e of
the
resu
lts o
f the
Nat
iona
lSu
rvey
of P
eopl
e w
ith D
iabe
tes
38
Clin
ical
qua
lity
Clin
ical
em
erge
ncy
situa
tions
Cro
ss re
fere
nces
to th
eSt
anda
rd N
HS
Con
trac
tfo
r Acu
te S
ervi
ces
Mai
n cl
ause
s:6,
11,1
2,13
,14,
15,1
8,32
,33,
42,
54
Sche
dule
s:
2, 3
(par
t 1 a
nd 3
), 12
Abi
lity
to n
egot
iate
and
agr
eear
rang
emen
ts w
ith a
ppro
pria
tepe
rson
nel a
nd o
rgan
isat
ions
to
prov
ide
effe
ctiv
ely
for
emer
genc
ysi
tuat
ions
The
Com
mis
sion
ers
shou
ld s
atis
fyth
emse
lves
tha
t pr
ovid
er h
as s
yste
ms,
proc
esse
s an
d co
mpe
tent
per
sonn
el a
re in
plac
e an
d im
plem
ente
d to
ens
ure
that
all
clin
ical
em
erge
ncie
s an
d co
mpl
icat
ions
are
hand
led
in a
ccor
danc
e w
ith b
est
prac
tice
Ther
e sh
ould
be
prot
ocol
s in
pla
ce to
ens
ure
the
avai
labi
lity
ofad
vice
and
/or s
uppo
rt o
f spe
cial
ist d
iabe
tes
clin
ical
sta
ff to
man
age
diab
etes
clin
ical
em
erge
ncy
situa
tions
, e.g
. dur
ing
asu
rgic
al p
roce
dure
or o
ther
clin
ical
inte
rven
tion
for t
hem
anag
emen
t of t
he re
nal c
ondi
tion
20
TOPI
CEL
EMEN
TSC
HA
RA
CTE
RIS
TIC
S, S
KIL
LSA
ND
BEH
AV
IOU
RS
OU
TPU
TSD
IAB
ETES
SER
VIC
ES S
PEC
IFIC
OU
TPU
TS/C
OM
MEN
TS
Clin
ical
qua
lity
Kno
wle
dge
and
unde
rsta
ndin
g of
hea
lthan
d sa
fety
Cro
ss re
fere
nces
to th
eSt
anda
rd N
HS
Con
trac
tfo
r Acu
te S
ervi
ces
Mai
n cl
ause
s:5,
11, 1
9, 5
4, 5
6, 6
0
Und
erst
andi
ng o
f cl
inic
alac
coun
tabi
litie
s of
hea
lth a
ndsa
fety
pol
icie
s
H&
S st
rate
gy a
nd p
olic
ies
in p
lace
and
impl
emen
ted
with
aw
aren
ess
thro
ugho
utth
e or
gani
satio
n
Acc
essi
bilit
y to
exe
cutiv
e re
spon
sibl
e fo
rH
&S
for
quic
ker,
first
con
tact
ser
vice
s
Hea
lth a
nd s
afet
y po
licie
s as
per
pro
vide
r agr
eem
ent w
ithco
mm
issio
ners
Dat
a an
din
form
atio
nm
anag
emen
t
Stra
tegy
and
pol
icie
s
Cro
ss re
fere
nces
to th
eSt
anda
rd N
HS
Con
trac
tfo
r Acu
te S
ervi
ces
Mai
n cl
ause
s:8,
9,17
,19,
21,2
3,24
,27,
29,3
2,33
,54
Sche
dule
s: 5
,7,1
5,16
,18
Stra
tegy
and
pol
icy
deve
lopm
ent
skill
s
The
abili
ty t
o an
alys
e da
ta a
ndha
ve a
cces
s to
info
rmat
ion
that
can
pred
ict
tren
ds a
nd t
hat
coul
did
entif
y pr
oble
ms
The
abili
ty t
o ca
ptur
e ev
iden
ceba
sed
prac
tice
from
R&
D N
atio
nal
Serv
ice
Fram
ewor
ks, N
ICE
guid
ance
The
abili
ty t
o us
e da
ta a
ndin
form
atio
n ap
prop
riate
ly t
oim
prov
e pa
tient
car
e
Tran
spar
ency
and
obj
ectiv
ity
The
Prov
ider
sho
uld
have
an
expl
icit
data
and
info
rmat
ion
stra
tegy
in p
lace
tha
t co
vers
•Ty
pes
of d
ata
•Q
ualit
y of
dat
a•
Dat
a pr
otec
tion
and
conf
iden
tialit
y•
Acc
essi
bilit
y•
Tran
spar
ency
•A
naly
sis
of d
ata
and
info
rmat
ion
•U
se o
f da
ta a
nd in
form
atio
n•
Dis
sem
inat
ion
of d
ata
and
info
rmat
ion
•Ri
sks
•Sh
arin
g of
dat
a an
d co
mpa
tibili
ty o
f IT
acro
ss d
iffer
ent
prov
ider
s w
ith r
espe
ct t
oca
re o
f pa
tient
s ac
ross
a p
athw
ay
This
info
rmat
ion
shou
ld b
e in
clud
ed in
the
Dat
a Q
ualit
y Im
prov
emen
t Pl
an
The
Prov
ider
is re
quire
d to
hav
e in
form
atio
n sy
stem
s th
at re
cord
indi
vidu
al n
eeds
incl
udin
g em
otio
nal,
soci
al, e
duca
tiona
l,ec
onom
ic a
nd b
iom
edic
al in
form
atio
n w
hich
per
mit
mul
tidisc
iplin
ary
care
acr
oss
serv
ice
boun
darie
s an
d su
ppor
t car
epl
anni
ng 39
The
Prov
ider
is re
quire
d to
use
the
follo
win
g fo
r the
col
lect
ion
and
prod
uctio
n of
dat
a, w
here
app
ropr
iate
:
•N
HS
Out
com
es F
ram
ewor
k28
•N
atio
nal D
iabe
tes
Info
rmat
ion
Serv
ice
40
•N
atio
nal D
iabe
tes
Aud
it 15
•N
atio
nal K
idne
y C
are
Aud
it 17
•Re
nal S
ervi
ces
Info
rmat
ion
Stra
tegy
: Sup
port
ing
part
one
of
the
Nat
iona
l Ser
vice
Fra
mew
ork
for R
enal
Ser
vice
s 41
•Re
nal s
ervi
ces
info
rmat
ion
stra
tegy
: Sup
port
ing
part
two
ofth
e N
atio
nal S
ervi
ce F
ram
ewor
k fo
r Ren
al S
ervi
ces42
•D
iabe
tes
E 19
Clin
ical
qua
lity
Esta
tes
and
equi
pmen
t
Cro
ss re
fere
nces
to th
eSt
anda
rd N
HS
Con
trac
tfo
r Acu
te S
ervi
ces
Mai
n cl
ause
s:5,
29, 3
3, 5
6
Sche
dule
s: 3
,10,
19
Und
erst
andi
ng o
f bu
ildin
gre
gula
tions
Acc
ess
to a
dvic
e on
“fit
-for
-pu
rpos
e” e
quip
men
t an
d fa
cilit
ies
Com
mis
sion
ers
mus
t as
sure
the
mse
lves
tha
tpa
tient
car
e is
del
iver
ed in
app
ropr
iate
lybu
ilt a
nd e
quip
ped
faci
litie
s w
hich
mee
tre
leva
nt H
TMs
and
Build
ing
Not
es, a
nd,
whe
re a
ppro
pria
te, a
re r
egis
tere
d an
d ar
esa
fe a
nd c
lean
.
Equi
pmen
t m
ust
be f
it fo
r pu
rpos
e
Com
mitm
ent
to e
ffic
ient
use
and
satis
fact
ory
mai
nten
ance
of
equi
pmen
t

21
TOPI
CEL
EMEN
TSC
HA
RA
CTE
RIS
TIC
S, S
KIL
LSA
ND
BEH
AV
IOU
RS
OU
TPU
TSD
IAB
ETES
SER
VIC
ES S
PEC
IFIC
OU
TPU
TS/C
OM
MEN
TS
Dat
a an
din
form
atio
nm
anag
emen
t
Stra
tegy
and
pol
icie
sTh
ere
shou
ld b
e po
licie
s in
pla
ce t
hat
incl
ude:
•C
onfid
entia
lity
Cod
e of
Pra
ctic
e•
Dat
a Pr
otec
tion
•Fr
eedo
m o
f In
form
atio
n•
Hea
lth R
ecor
ds•
Info
rmat
ion
Gov
erna
nce
Man
agem
ent
•In
form
atio
n Q
ualit
y A
ssur
ance
•In
form
atio
n Se
curit
y
Ther
e m
ust
be a
nam
ed in
divi
dual
who
isth
e C
aldi
cott
Gua
rdia
n
•Q
ualit
y an
d O
utco
mes
Fra
mew
ork43
•H
ospi
tal E
piso
de S
tatis
tics44
•U
K R
enal
Reg
istr
y 45
•Pa
tient
Exp
erie
nce
18,3
8
•Pa
tient
Sat
isfa
ctio
n 38
•Pa
tient
Rep
orte
d O
utco
mes
Mea
sure
s 20
•N
atio
nal D
iabe
tes
Con
tinui
ng C
are
Dat
aset
46
•N
atio
nal R
enal
Dat
aset
47
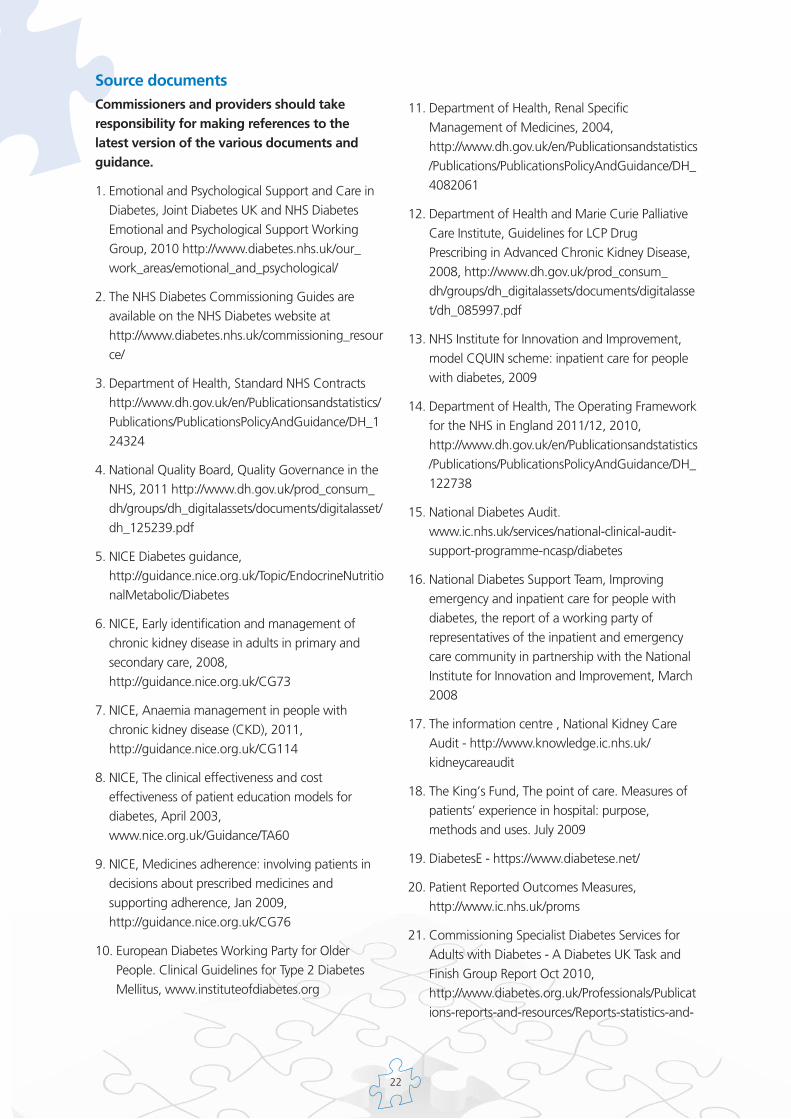
22
Source documentsCommissioners and providers should takeresponsibility for making references to thelatest version of the various documents andguidance.
1. Emotional and Psychological Support and Care inDiabetes, Joint Diabetes UK and NHS DiabetesEmotional and Psychological Support WorkingGroup, 2010 http://www.diabetes.nhs.uk/our_work_areas/emotional_and_psychological/
2. The NHS Diabetes Commissioning Guides areavailable on the NHS Diabetes website athttp://www.diabetes.nhs.uk/commissioning_resource/
3. Department of Health, Standard NHS Contractshttp://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_124324
4. National Quality Board, Quality Governance in theNHS, 2011 http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_125239.pdf
5. NICE Diabetes guidance,http://guidance.nice.org.uk/Topic/EndocrineNutritionalMetabolic/Diabetes
6. NICE, Early identification and management ofchronic kidney disease in adults in primary andsecondary care, 2008,http://guidance.nice.org.uk/CG73
7. NICE, Anaemia management in people withchronic kidney disease (CKD), 2011,http://guidance.nice.org.uk/CG114
8. NICE, The clinical effectiveness and costeffectiveness of patient education models fordiabetes, April 2003,www.nice.org.uk/Guidance/TA60
9. NICE, Medicines adherence: involving patients indecisions about prescribed medicines andsupporting adherence, Jan 2009,http://guidance.nice.org.uk/CG76
10. European Diabetes Working Party for OlderPeople. Clinical Guidelines for Type 2 DiabetesMellitus, www.instituteofdiabetes.org
11. Department of Health, Renal SpecificManagement of Medicines, 2004,http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4082061
12. Department of Health and Marie Curie PalliativeCare Institute, Guidelines for LCP DrugPrescribing in Advanced Chronic Kidney Disease,2008, http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_085997.pdf
13. NHS Institute for Innovation and Improvement,model CQUIN scheme: inpatient care for peoplewith diabetes, 2009
14. Department of Health, The Operating Frameworkfor the NHS in England 2011/12, 2010,http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_122738
15. National Diabetes Audit.www.ic.nhs.uk/services/national-clinical-audit-support-programme-ncasp/diabetes
16. National Diabetes Support Team, Improvingemergency and inpatient care for people withdiabetes, the report of a working party ofrepresentatives of the inpatient and emergencycare community in partnership with the NationalInstitute for Innovation and Improvement, March2008
17. The information centre , National Kidney CareAudit - http://www.knowledge.ic.nhs.uk/kidneycareaudit
18. The King’s Fund, The point of care. Measures ofpatients’ experience in hospital: purpose,methods and uses. July 2009
19. DiabetesE - https://www.diabetese.net/
20. Patient Reported Outcomes Measures,http://www.ic.nhs.uk/proms
21. Commissioning Specialist Diabetes Services forAdults with Diabetes - A Diabetes UK Task andFinish Group Report Oct 2010,http://www.diabetes.org.uk/Professionals/Publications-reports-and-resources/Reports-statistics-and-

23
case-studies/Reports/Commissioning-Specialist-Diabetes-Services-for-Adults-with-Diabetes---Defining-A-Specialist-Diabetes-UK-Task-and-Finish-Group-Report-October-2010/
22. Skills for Health, Diabetes CompetencyFramework and Renal Competences,https://tools.skillsforhealth.org.uk/
23. Department of Health, The National ServiceFramework for Renal Services, January 2004http://www.dh.gov.uk/en/Healthcare/Renal/DH_4102636
24. Department of Health, National ServiceFramework for Older People, May 2001,http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4003066
25. National Service Framework for Children, YoungPeople and Maternity Services, 2004http://www.dh.gov.uk/en/Healthcare/Children/DH_4089111
26. Department of Health, No health without mentalhealth: a cross-government mental healthoutcomes strategy for people of all ages,February 2011,http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_123766
27. Department of Health, The National ServiceFramework for Long Term Conditions, March2005 http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4105361
28. Department of Health, The NHS OutcomesFramework 2011/12, December 2010http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_122944
29. NICE, Quality Standards: Diabetes in adults,March 2011, http://www.nice.org.uk/guidance/qualitystandards/qualitystandards.jsp
30. Generic Long-term conditions modelhttp://www.dh.gov.uk/en/Healthcare/Longtermconditions/DH_120915
31. Renal Specialised Commissioners, The National
Service Framework for Renal Services Part OneDialysis and Transplantation ImplementationToolkit For Commissioners Based on Best Practice,2004 http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_4097253.pdf
32. Putting Prevention First, NHS Health Check,Vascular risk assessment and management , Bestpractice guidance, 2009,www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_097489
33. NHS Kidney Care, My Kidney Care Planhttp://www.kidneycare.nhs.uk/_Resourcestodownload-MyKidneyCarePlan.aspx
34. NHS Kidney Care, Specification for theCommissioning of Peritoneal Dialysis Pathway ,2009 http://www.kidneycare.nhs.uk/_Resourcestodownload-Specifications.aspx
35. NHS Kidney Care, Achieving Autonomy forKidney Services Seven Steps Toolkithttp://www.kidneycare.nhs.uk/Library/Achieving_Autonomy_for_Kidney_Services_FINAL.pdf
36. NHS Kidney Care, The Role of the Renal WelfareOfficer, Kidney Care Matters online, Case study,August 2009,http://www.kidneycare.nhs.uk/_Whatworks-Casestudies-Theroleoftherenalwelfareofficer.aspx
37. End of Life Care for Advanced Kidney Disease, Aframework for implementation, 2009,http://www.kidneycare.nhs.uk/Library/EndofLifeCareFINAL.pdf
38. Healthcare Commission, National Survey ofPeople with Diabetes, 2006,www.cqc.org.uk/usingcareservices/healthcare/patientsurveys/servicesforpeoplewithdiabetes.cfm
39. York and Humber integrated IT system,http://www.diabetes.nhs.uk/
40. National Diabetes Information Service,www.diabetes-ndis.org
41. Department of Health, Renal Services InformationStrategy, 2004,http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/

24
dh_4070588.pdf
42. Department of Health, Renal services informationstrategy: Supporting part two of the NationalService Framework for Renal Services, 2005http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4113496
43. Quality and Outcomes Framework,http://www.nice.org.uk/aboutnice/qof/qof.jsp
44. Hospital Episode Statistics,www.ic.nhs.uk/statistics-and-data-collections/hospital-care/hospital-activity-hospital-episode-statistics--hes
45. UK Renal Registry,http://www.renalreg.com/About-Us/about.html
46. National Diabetes Continuing Care Dataset,www.ic.nhs.uk/webfiles/Services/Datasets/Diabetes/dccrdataset.pdf
47. National Renal Dataset,http://www.ic.nhs.uk/services/datasets/document-
downloads/renal

25
This specification forms Schedule 2, Part 1 orsection 1 (module B), ‘The Services - ServiceSpecifications’ of the Standard NHSContractsa
Service specifications are developed in partnershipbetween commissioners and provider agenciesand are based on agreed evidence-based care andtreatment models. Diabetes and Renal Networkshave an important role to play in developing thespecifications. Specifications should be open toscrutiny and available to all service users/carers asa statement of standards that the user/carer canexpect to receive.
The following documentation, developed bythe Diabetes Commissioning Advisory Groupin conjunction with NHS Kidney Careprovides further detail/guidance to supportthe development of this specification:
• The intervention map for diabetes and kidneycare services
• The contracting framework for diabetes andkidney care services
This specification template assumes that theservices are compliant with the contractingframework for diabetes and kidney care services.
This template also provides examples of whatcommissioners may wish to consider whendeveloping their own service specifications.
Description of diabetes and kidneycare services:Diabetes and kidney care services includes anassessment of risk of chronic kidney disease aspart of the initial and continuing management ofpeople with diabetes, management of renalfunction and associated conditions such ashypertension and metabolic bone disorders,management of all the stages of renal failure withspecialist input with access to transplantation anddialysis services.
The final specification should take into account:
• national, network and local guidance andstandards for diabetes and kidney careservices.
• local needs.
• cross references to the Specification for theCommissioning of Peritoneal DialysisPathwayb and the autonomous kidneyservices toolkitc
This specification is supported by other relatedwork in diabetes commissioning such as:
• the web-based Diabetes Community HealthProfiles (Yorkshire and Humber Public HealthObservatory)
• the web-based Health Needs Assessment Tool(National Diabetes Information Service).
These provide comprehensive information forneeds assessment, planning and monitoring ofdiabetes services
Standard Service SpecificationTemplate for Diabetes and Kidney Care
a Standard NHS Contracts http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_124324
b NHS Kidney Care, Specification for the Commissioning of Peritoneal Dialysis Pathway , 2009http://www.kidneycare.nhs.uk/i/assets/Commissioning_of_PD_Pathway_Nov09_FINAL.pdf
c NHS Kidney Care, Achieving Autonomy for Kidney Services Seven Steps Toolkithttp://www.kidneycare.nhs.uk/i/assets/Achieving_Autonomy_for_Kidney_Services_FINAL.pdf

26
Introduction• A general overview of the services identifying
why the services are needed, includingbackground to the services and why they arebeing developed or in place.
• A statement on how the services relate to eachother within the whole system should beincluded describing the keystakeholders/relationships which influence theservices, e.g. multi-disciplinary diabetes teamand renal team, etc
• Any relevant diabetes and renal clinicalnetworks and screening/risk assessmentprogrammes applicable to the services, e.g.NHS Health Check
• Details of all interdependencies or sub-contractors for any part of the service and anoutline of the purpose of the contract shouldbe stated, including arrangements for clinicalaccountability and responsibility, as appropriate
Purpose, Role and Clientele1. A clear statement on the primary purpose of
the services and details of what will beprovided and for whom:
• Who the services are for (e.g. children,young people, adults and older people withdiabetes who require kidney care for therenal complications of diabetes)
• What the services aim to achieve within agiven timeframe
• The objectives of the services
• The desired outcomes and how these aremonitored and measured
Scope of the Services2. What does the service do? This section will
focus on the types of high level therapeuticinterventions that are required for the types ofneed the services will respond to.
• How the services responds to age, culture,disability, and gender sensitive issues
• Assessment – details of what it is and co-morbidity assessment and referrals to allrelevant specialties
• Service planning – High level view of whatthe services are and how they are used;how patients enter the pathway/journey;what are the stages undertaken andcontinuing management up to end of lifecare. The aims of service planning are to:
o Develop, manage and reviewinterventions along the patient journey
o Ensure access to other specialities /care,as appropriate
o Ensure that care planning is undertakenby the diabetes multi-disciplinary team(as defined locally) with a clear care co-ordination function
o Ensure that transition from childrens’ toadults’ services or adults’ to olderpeoples’ services is negotiated andexplicitly planned around the assessedneeds of each individual person
• Holistic review of patients in themanagement of their diabetes using theprinciples of an integrated care model forpeople with long term conditions that ispatient-centred, including self care and selfmanagement, clinical treatment, facilitatingindependence, psychological support andother social care issues
• Risk assessment procedures
• Detail of evidence base of the service –i.e.the contracting framework for diabetesand kidney care, guidance produced byRoyal College of Physicians, Diabetes UK etc.
Service Delivery3. Patient Journey/intervention map
Flow diagram of the patient pathway showingaccess and exit/transfer points – see the patientintervention map for diabetes and kidney careservices as a starting point
4. Treatment protocols/interventionsInclude all individual treatment protocols inplace within the services or planned to be used
5. This will include a breakdown of how thepatient will receive the services and fromwhom. It should be a clear statement of staffqualifications/experience and/or training (if

27
appropriate) and clinical or managerialsupervision arrangements. It should specify, asappropriate:
• Geographical coverage/boundaries – i.e.the services should be available for childrenand young people, adult and older peoplewho live in the clinical commissioninggroup area
• Hours of operation including, week-end,bank holiday and on-call arrangements
• Minimum level of experience andqualifications of staff (i.e. doctors –diabetologists, nephrologists and GPs,Nursing staff – diabetes nurse specialists,renal care nurses etc, other allied healthprofessionals, e.g. dietitians, pharmacistsetc and other support and administrativestaff)
• Confirmation of the arrangements toidentify the Care Co-ordinator for eachpatient with diabetes (i.e. who holds theresponsibility and role).
• Staff induction and developmental training
6. Equipment• Upgrade and maintenance of relevant
equipment and facilities
• Technical specifications (if any)
Identification, Referral andAcceptance criteria7. This should make clear how patients will be
identified, assessed, and accepted to theservices. Acceptance should be based on typesof need and/or patient.
8. How should patients be referred?
• Who is acceptable for referral and fromwhere
• Details of evaluation process - Are thereclear exclusion criteria or set alternatives tothe service? How might a patient betransferred?
• Response time detail and how are patientsprioritised
Discharge/Service Complete/PatientTransfer/Transition criteria9. The intention of this section is to make clear
when a patient should be transferred from oneaspect of the diabetes service to another is andwhen this would be reached.
• How is a treatment pathway reviewed?
• How does the service decide that a patientis ready for discharge
• How are goals and outcomes assessed andreviewed?
• What procedure is followed on discharge,including arrangements for follow-up
Quality Standards10. The service is required to deliver care
according to the standards for clinical practiceset by the National Institute for Health andClinical Excellenced,e
11. As a minimum, the Provider is required toagree a local Commissioning for Quality andInnovation scheme for services for peoplewith diabetes. (Insert details of the CQUINScheme agreed)
12. The service is required to deliver the outcomesfor diabetes as determined by the NHSOutcomes Frameworkf
Activity and PerformanceManagement13. This must include performance indicators,
thresholds, methods of measurement andconsequences of breach of contract. Thesewill be set and agreed prior to the signing ofthe overall agreement.
14. Activity plans – Where appropriate, identifythe anticipated level of activity the servicemay deliver; provide details of any activitymeasures and their description /method ofcollection, targets, thresholds andconsequences of variances above or belowtarget.
d http://www.nice.org.uk/guidance/qualitystandards/qualitystandards.jsp
e http://www.nice.org.uk/guidance/qualitystandards/chronickidneydisease/ckdqualitystandard.jsp
f http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_122944

28
Continual Service Improvement15. As part of the monitoring and evaluation
procedures, the service will identify a methodof agreeing measurements for continuousimprovement of the service being offeredand work to ensure unmet need is bothidentified and brought to the attention of thecommissioner.
16. ReviewThis section should set out a review date anda mechanism for review.
The review should include both thespecifications for continuing fitness forpurpose and the providers’ delivery againstthe specification.
This should set out the process by which thisreview will be conducted.
This should also identify how complianceagainst the specification will be monitored inyear.
17. Agreed byThis should set out who agrees/accepts thespecification on behalf of all parties.
This should include the diabetes and kidneycare providers, commissioner and network.


Further copies of this publication can be ordered from Prontaprint, by emailing [email protected] or tel: 0116 275 3333, quoting DIABETES 120
www.diabetes.nhs.uk