Coming Soon - david potach - Knee Biomechanics during a ......patellar tendon-bone or four-stranded...
10
Knee Biomechanics during a Jump-Cut Maneuver: Effects of Sex and ACL Surgery DANIEL L. MIRANDA 1,2 , PAUL D. FADALE 1 , MICHAEL J. HULSTYN 1 , ROBERT M. SHALVOY 1 , JASON T. MACHAN 1,3,4 , and BRADEN C. FLEMING 1,2,5 1 Department of Orthopaedics, The Warren Alpert Medical School, Brown University and Rhode Island Hospital, Providence, RI; 2 Center for Biomedical Engineering, Brown University, Providence, RI; 3 Department of Surgery, The Warren Alpert Medical School, Brown University, Providence, RI; 4 Biostatistics, Rhode Island Hospital, Providence, RI; and 5 School of Engineering, Brown University, Providence, RI ABSTRACT MIRANDA, D. L., P. D. FADALE, M. J. HULSTYN, R. M. SHALVOY, J. T. MACHAN, and B. C. FLEMING. Knee Biomechanics during a Jump-Cut Maneuver: Effects of Sex and ACL Surgery. Med. Sci. Sports Exerc., Vol. 45, No. 5, pp. 942–951, 2013. Purpose: The purpose of this study was to compare kinetic and knee kinematic measurements from male and female anterior cruciate ligament (ACL)–intact (ACL INT ) and ACL-reconstructed (ACL REC ) subjects during a jump-cut maneuver using biplanar videoradiography. Methods: Twenty subjects were recruited; 10 ACL INT (5 men and 5 women) and 10 ACL REC (4 men and 6 women, 5 yr postsurgery). Each subject performed a jump-cut maneuver by landing on a single leg and performing a 45- side-step cut. Ground reaction force (GRF) was measured by a force plate and expressed relative to body weight. Six-degree-of-freedom knee kinematics were determined from a biplanar videoradiography system and an optical motion capture system. Results: ACL INT female subjects landed with a larger peak vertical GRF (P G 0.001) compared with ACL INT male subjects. ACL INT subjects landed with a larger peak vertical GRF (P e 0.036) compared with ACL REC subjects. Regardless of ACL reconstruction status, female subjects underwent less knee flexion angle excursion (P = 0.002) and had an increased average rate of anterior tibial translation (0.05%Ims j1 T 0.01%Ims j1 , P = 0.037) after contact compared with male subjects. Furthermore, ACL REC subjects had a lower rate of anterior tibial translation compared with ACL INT subjects (0.05%Ims j1 T 0.01%Ims j1 , P = 0.035). Finally, no striking differences were observed in other knee motion parameters. Conclusion: Women permit a smaller amount of knee flexion angle excursion during a jump-cut maneuver, resulting in a larger peak vertical GRF and increased rate of anterior tibial translation. Notably, ACL REC subjects also perform the jump cut maneuver with lower GRF than ACL INT subjects 5 yr postsurgery. This study proposes a causal sequence whereby increased landing stiffness (larger peak vertical GRF combined with less knee flexion angle excursion) leads to an increased rate of anterior tibial translation while performing a jump-cut maneuver. Key Words: KINEMATICS, KINETICS, LANDING STIFFNESS, GROUND REACTION FORCE, ANTERIOR TIBIAL TRANSLATION, BIPLANAR VIDEORADIOGRAPHY I njuries to the anterior cruciate ligament (ACL) are com- monly associated with sport maneuvers involving jump- ing, landing, and cutting (16). These maneuvers result in a sudden loading of the ACL due to the deceleration of the tibia that occurs after landing but just before a rapid direction change (17). Approximately 70% of ACL injuries occur during deceleration maneuvers without contact from another athlete (23). Although men experience noncontact decelera- tion injury, women are reported to be up to 10 times more prone when participating in the same high-risk activities (19). Although many theories exist, the ACL failure mechanism and the associated sex bias remain unclear. During normal function, the ACL restrains excessive an- terior tibial translation and stabilizes secondary knee rotations (i.e., internal/external (IN/EX) and abduction/adduction) (22). ACL reconstruction has become the gold standard of treat- ment for athletes with an ACL tear in an attempt to restore joint stability and to return patients to a high functional level (13). Unfortunately, of the 400,000 patients that undergo ACL reconstruction in the United States each year, up to 5% are at risk for reinjury (40), 45% fail to return to their preinjury sport level (5), and 80% to 90% will develop radio- graphic evidence of osteoarthritis even as early as 7 yr postsurgery (20). Given the unexplained greater risk of noncontact deceler- ation ACL injury in female subjects, any differences between sex and ACL reconstruction status in the kinematic and kinetic factors during associated sport activities may point to root causes for injury, reinjury, and avenues for prevention and rehabilitation. Unfortunately, the biomechanics of male and female ACL-intact (ACL INT ) and ACL-reconstructed Address for correspondence: Braden C. Fleming, Ph.D., Warren Alpert Medical School of Brown University, 1 Hoppin Street, Coro West, Suite 404, Provi- dence, RI 02903; E-mail: [email protected]. Submitted for publication July 2012. Accepted for publication October 2012. Supplemental digital content is available for this article. Direct URL cita- tions appear in the printed text and are provided in the HTML and PDF versions of this article on the journal_s Web site (www.acsm-msse.org). 0195-9131/13/4505-0942/0 MEDICINE & SCIENCE IN SPORTS & EXERCISE Ò Copyright Ó 2013 by the American College of Sports Medicine DOI: 10.1249/MSS.0b013e31827bf0e4 942 APPLIED SCIENCES Copyright © 2013 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
Transcript of Coming Soon - david potach - Knee Biomechanics during a ......patellar tendon-bone or four-stranded...

Knee Biomechanics during a Jump-CutManeuver: Effects of Sex and ACL Surgery
DANIEL L.MIRANDA1,2, PAULD. FADALE1, MICHAEL J. HULSTYN1, ROBERTM. SHALVOY1, JASON T. MACHAN1,3,4,and BRADEN C. FLEMING1,2,5
1Department of Orthopaedics, The Warren Alpert Medical School, Brown University and Rhode Island Hospital, Providence,RI; 2Center for Biomedical Engineering, Brown University, Providence, RI; 3Department of Surgery, The Warren AlpertMedical School, Brown University, Providence, RI; 4Biostatistics, Rhode Island Hospital, Providence, RI; and 5School ofEngineering, Brown University, Providence, RI
ABSTRACT
MIRANDA, D. L., P. D. FADALE, M. J. HULSTYN, R. M. SHALVOY, J. T. MACHAN, and B. C. FLEMING. Knee Biomechanics
during a Jump-Cut Maneuver: Effects of Sex and ACL Surgery. Med. Sci. Sports Exerc., Vol. 45, No. 5, pp. 942–951, 2013. Purpose:
The purpose of this study was to compare kinetic and knee kinematic measurements from male and female anterior cruciate ligament
(ACL)–intact (ACLINT) and ACL-reconstructed (ACLREC) subjects during a jump-cut maneuver using biplanar videoradiography.Methods:
Twenty subjects were recruited; 10 ACLINT (5 men and 5 women) and 10 ACLREC (4 men and 6 women, 5 yr postsurgery). Each subject
performed a jump-cut maneuver by landing on a single leg and performing a 45- side-step cut. Ground reaction force (GRF) was
measured by a force plate and expressed relative to body weight. Six-degree-of-freedom knee kinematics were determined from a biplanar
videoradiography system and an optical motion capture system. Results: ACLINT female subjects landed with a larger peak vertical GRF
(P G 0.001) comparedwithACLINT male subjects. ACLINT subjects landed with a larger peak vertical GRF (P e 0.036) compared with ACLRECsubjects. Regardless of ACL reconstruction status, female subjects underwent less knee flexion angle excursion (P = 0.002) and had an increased
average rate of anterior tibial translation (0.05%Imsj1 T 0.01%Imsj1, P = 0.037) after contact compared with male subjects. Furthermore,
ACLREC subjects had a lower rate of anterior tibial translation compared with ACLINT subjects (0.05%Imsj1 T 0.01%Imsj1, P = 0.035). Finally,
no striking differences were observed in other knee motion parameters. Conclusion: Women permit a smaller amount of knee flexion angle
excursion during a jump-cut maneuver, resulting in a larger peak vertical GRF and increased rate of anterior tibial translation. Notably, ACLRECsubjects also perform the jump cut maneuver with lower GRF than ACLINT subjects 5 yr postsurgery. This study proposes a causal sequence
whereby increased landing stiffness (larger peak vertical GRF combined with less knee flexion angle excursion) leads to an increased rate of
anterior tibial translation while performing a jump-cut maneuver. Key Words: KINEMATICS, KINETICS, LANDING STIFFNESS,
GROUND REACTION FORCE, ANTERIOR TIBIAL TRANSLATION, BIPLANAR VIDEORADIOGRAPHY
Injuries to the anterior cruciate ligament (ACL) are com-monly associated with sport maneuvers involving jump-ing, landing, and cutting (16). These maneuvers result in
a sudden loading of the ACL due to the deceleration of thetibia that occurs after landing but just before a rapid directionchange (17). Approximately 70% of ACL injuries occurduring deceleration maneuvers without contact from anotherathlete (23). Although men experience noncontact decelera-tion injury, women are reported to be up to 10 times more
prone when participating in the same high-risk activities (19).Although many theories exist, the ACL failure mechanismand the associated sex bias remain unclear.
During normal function, the ACL restrains excessive an-terior tibial translation and stabilizes secondary knee rotations(i.e., internal/external (IN/EX) and abduction/adduction) (22).ACL reconstruction has become the gold standard of treat-ment for athletes with an ACL tear in an attempt to restorejoint stability and to return patients to a high functional level(13). Unfortunately, of the 400,000 patients that undergoACL reconstruction in the United States each year, up to5% are at risk for reinjury (40), 45% fail to return to theirpreinjury sport level (5), and 80% to 90% will develop radio-graphic evidence of osteoarthritis even as early as 7 yrpostsurgery (20).
Given the unexplained greater risk of noncontact deceler-ation ACL injury in female subjects, any differences betweensex and ACL reconstruction status in the kinematic andkinetic factors during associated sport activities may point toroot causes for injury, reinjury, and avenues for preventionand rehabilitation. Unfortunately, the biomechanics of maleand female ACL-intact (ACLINT) and ACL-reconstructed
Address for correspondence: Braden C. Fleming, Ph.D., Warren Alpert MedicalSchool of Brown University, 1 Hoppin Street, Coro West, Suite 404, Provi-dence, RI 02903; E-mail: [email protected] for publication July 2012.Accepted for publication October 2012.Supplemental digital content is available for this article. Direct URL cita-tions appear in the printed text and are provided in the HTML and PDFversions of this article on the journal_s Web site (www.acsm-msse.org).
0195-9131/13/4505-0942/0MEDICINE & SCIENCE IN SPORTS & EXERCISE�Copyright � 2013 by the American College of Sports Medicine
DOI: 10.1249/MSS.0b013e31827bf0e4
942
APP
LIED
SCIENCES
Copyright © 2013 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

(ACLREC) knees during high-risk noncontact decelerationactivities, such as a jump-cut maneuver, are not well under-stood. These data have previously been difficult to obtain, inpart, because noninvasive measurement of kinematics hasbeen limited to optical motion capture (OMC), which dependon surface markers that are prone to artifact from soft tissueoscillation immediately after landing (24).
Biplanar videoradiography, however, allows for direct mea-surement of in vivo bone motion, circumventing the effectof soft tissue artifact (14,28,29,33,34,36,37). Biplanarvideoradiography has recently been used to study dynamicACLINT and ACLREC knee motion during running (33,34),two-legged drop landings (28,29,36,37), and single-leg hop-ping (14). Although these studies have made significant con-tributions to our understanding of both ACLINT and ACLRECknee function during running, drop landing, and hopping, thecombined jump-cut maneuver, which is more commonly as-sociated with noncontact deceleration ACL injury, has notbeen investigated (15,17). In addition, the biomechanics ofACLREC subjects during these other dynamic tasks were in-vestigated between 4 and 12 months after surgery (14,33,34).Although these time points are crucial for quantifying the im-mediate effects of ACL reconstruction, understanding thebiomechanics of the knee more than 5 yr after surgery mayprovide further insight into the long-term recovery process.
The purpose of this study was to compare force plate kineticdata and knee kinematic measurements from male and femaleACLINT and ACLREC recreational athletes during a jump-cutmaneuver in hopes that the differences would point to plausiblerisk factors for injury. Knee kinematic measurements wereprimarily obtained from biplanar videoradiography; however,knee flexion/extension (FL/EX) outside the field of view(FOV) of the biplanar videoradiography system was obtainedfrom traditional OMC. The specific aims were to determinedifferences due to both sex and ACL reconstruction statusbetween ACLREC patients, who were at least 5 yr postsurgery,and ACLINT control subjects. More specifically, it was antici-pated that ACLINT women would tend to perform the jump-cut maneuver more upright with more landing stiffness thanACLINT men. This would be evident as decreased knee flexi-on angle excursion and increased peak ground reaction force(GRF), relative to their body weight, resulting in greater
tibial translation (particularly anterior). In contrast, it wasnot known whether or not ACLREC females and males 5 yrpostreconstruction would follow a similar pattern or iftheir injury and subsequent repair and rehabilitation wouldhave resulted in altered kinetic and kinematic parameters(tested as an interaction between sex and ACL reconstruc-tion status).
METHODS
Subjects. All experimental procedures were approved bythe institutional review board. Twenty recreational athleteswere enrolled in this study. Of these subjects, 10 wereACLINT (5 males and 5 females) and 10 were ACLREC (4 malesand 6 females; seven bone-patellar tendon-bone autograftsand three hamstring tendon autografts). Age, weight, andheight for all subjects are displayed in Table 1. The inclusioncriteria for the ACLINT subjects were as follows: 1) no historyof lower extremity injury, 2) no neurological disease(s), 3) nopregnancy, and 4) a Tegner activity score of 5 or greater (35).It should be noted that the ACLINT subjects were part of aseparate study investigating the effects of soft tissue artifacton kinematic outcomes during a combined jump-cut maneu-ver (24). The inclusion criteria for the ACLREC patients wereas follows: 1) unilateral ACL reconstruction using bone-patellar tendon-bone or four-stranded hamstring tendon auto-graft (looped semitendinosus and gracilis), 2) at least 5 yr ofpost-ACL reconstruction, 3) no systemic infection, 4) no neu-rological disease(s), 5) no pregnancy, and 6) a Tegner activityscore of 5 or greater. The ACL reconstruction surgery type wasconfirmed from patient records. After granting their informedconsent, each subject was outfitted with 23 retroreflective sur-face markers on a single leg to permit measurement of foot,shank, and thigh motion using OMC (10). The outfitted legwas chosen at random for the ACLINT subjects (6L and 4R).For the ACLREC subjects, the ACL reconstructed leg wasoutfitted (7L and 3R).
Jump-cut maneuver. Each subject performed a jump-cut maneuver that was adapted from the study of Ford et al.(15) and previously described in detail (24). Briefly, threetargets were placed on the floor within the testing environment(Fig. 1A). The first target was in the center of a force plate
TABLE 1. ACLINT and ACLREC male and female age, mass, and height demographics.
Parameter ACL Status Mean SEM P Sex Mean SEM P Interaction Mean SEM P
Age (yr) ACLINT 25.20 1.64 0.464 M 27.53 1.74 0.235 INT � M 25.80 2.32 0.481INT � F 24.60 2.32
ACLREC 26.96 1.67 F 24.63 1.57 REC � M 29.25 2.59REC � F 24.67 2.12
Mass (kg) ACLINT 73.16 2.93 0.242 M 84.88 3.11 G0.001 INT � M 81.53 4.15 0.617INT � F 65.07 4.15
ACLREC 78.26 2.99 F 66.55 2.81 REC � M 88.49 4.64REC � F 68.03 3.79
Height (cm) ACLINT 172.85 2.09 0.736 M 178.70 2.21 0.003 INT � M 177.40 2.95 0.605INT � F 168.30 2.95
ACLREC 173.88 2.13 F 168.03 2.00 REC � M 180.00 3.30REC � F 167.75 2.70
A two-way ANOVA was performed on each set of demographics data, and no statistically significant differences (P e 0.05) were found between sex and condition. Statistically significantdifferences (P e 0.05) are in boldface.
KNEE BIOMECHANICS DURING A JUMP-CUT MANEUVER Medicine & Science in Sports & Exercised 943
APPLIED
SCIEN
CES
Copyright © 2013 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

(Kistler model 9281B, Amherst, NY). The other two targetswere placed toward the left and right of the landing target atan angle of 45-. Before beginning the maneuver, the subjectwas asked to stand approximately 1 m from the force platewith their knees bent approximately 45-. Upon hearing averbal ‘‘GO’’ prompt, the subject jumped upward and for-ward toward the first landing target. At the same time as theverbal ‘‘GO’’ prompt, a visual directional prompt, left (L) orright (R), cued the subject as to which direction to cut afterlanding on the target with one leg. Upon landing, the subjectperformed a sidestep cut and then jogged past the respec-tive angled targets. For example, if a subject was promptedto cut to the left, they would land, cut, and push off withtheir right leg. A trial was excluded if the subject incorrectly
performed the jump-cut maneuver (landing outside the tar-get area, incorrect cut direction, crossover cut, etc.). A total of10 correctly executed trials were performed, and the subjectwas unaware of the directional prompt before a given trial.
Data collection and processing. The jump-cut man-euvers were carried out, and kinetic and kinematic data weregathered in the W.M. Keck Foundation XROMM Facility atBrown University (Providence, RI; http://www.xromm.org).A four-camera OMC system (Qualisys Oqus 5, Gothenburg,Sweden) was used to track the retroreflective surface markers(10-mm diameter) on each subject’s outfitted leg during theentire jump-cut maneuver at a capture rate of 250 Hz. A forceplate (Kistler model 9281B) was used to measure the GRF at5000 Hz. The biplanar videoradiography system was engagedfor a maximum of six trials and measured motion at 250 Hzwithin a restricted FOV above the force plate (26). This wasdone to reduce radiation exposure and maximize the likeli-hood that the jump-cut maneuver occurred within the FOV ofthe biplanar videoradiography system. All devices were timesynchronized. Image dedistortion and 3-D space calibrationfollowed established protocols using custom MATLAB software(XrayProject, Brown University; http://www.xromm.org) (9).
In addition, a single static clinical computed tomography(CT) scan was collected for each subject’s outfitted knee.Image volumes were captured in the axial plane at 80 kVpwhile using GE’s SMART mA and Bone Plus reconstructionalgorithms. The voxel resolution (slice thickness and in-planeresolution) for each scan was less than 0.625 � 0.465 �0.465 mm3. The voxels corresponding to the femur and tibiawere isolated from each CT volume using previously de-scribed methods (25) implemented in commercially availableimage segmentation software (Mimics v14; Materialise, AnnArbor, MI).
Custom markerless tracking software (Autoscoper, BrownUniversity; http://www.xromm.org) was used to process thebiplanar videoradiography data (26). Briefly, isolated CTvolumes for the femur and tibia were input into a virtual 3-Denvironment containing the biplanar videoradiography sequen-ces and their calibration information. Digitally reconstructedradiographs (DRR) were generated from the CT volumes,and the kinematic transforms from CT space to each radio-graph frame were determined after optimally matching theDRR with the two views from the biplanar videoradiographysystem (Fig. 1B). It has previously been shown that in vivobone motion can be determined within 0.25 mm and 0.25-using these methods (7,26). Furthermore, the rotational andtranslational tracking precision for this study was estimatedat 0.08- and 0.45 mm, respectively.
The retroreflective marker data from the OMC systemwere filtered using a digital low-pass Butterworth filterwith a cutoff frequency of 25 Hz. The kinematic transformsof the femur and tibia obtained from the biplanar video-radiography system were converted into quaternions. Aquaternion is represented by four parameters that can befiltered (12). A digital Butterworth filter with a 25-Hz cutofffrequency was applied to the three kinematic translation
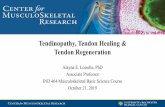
FIGURE 1—A, Illustration depicting the experimental setup used tocapture both biplanar videoradiography and OMC data during ajump-cut maneuver. A screen directly in front of the subject promptedthem with the directional arrow. The subject would land and cut in thedirection they were prompted using the opposite leg. For example, ifprompted with the left arrow, the subject would land and cut to the leftusing their right leg. The four OMC cameras are not displayed in thisfigure; however, they were positioned to capture the retroreflectivemarkers shown on the subject’s right leg. B, Example frame from theAutoscoper markerless tracking software. Each view represents oneframe from each of the two videoradiographs generated from the twoimage intensifiers (A). The blue and black portions of the images rep-resent the actual radiographs. The orange femur represents the DRR.Both the DRR and videoradiographs have been enhanced with a Sobeledge detection filter and a contact filter. This was done to create astrong visual match between the DRR and actual radiograph. Thetranslational manipulator is shown. This manipulator allowed the userto translate the DRR within the 3-D environment. A rotational ma-nipulator was also available to the user. The DRR is shown here afterperforming markerless registration. The knee shown in this image isfrom one of the ACLREC subjects. Both interference screws are visiblein the femur and tibia.
http://www.acsm-msse.org944 Official Journal of the American College of Sports Medicine
APP
LIED
SCIENCES
Copyright © 2013 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

parameters and the four quaternion parameters. The filteredquaternion parameters were converted back to rotation matri-ces and recombined with the filtered kinematic translations.The GRF data was filtered using a digital Butterworth filterwith a 100-Hz cutoff frequency.
Data analysis. For comparison between subjects, thevertical GRF was normalized by body weight. A character-istic peak (Fig. 2A) was observed in the vertical GRF withinthe first 25 ms. This peak vertical GRF was quantified by itstime after contact (peak vertical GRF time) and its magni-tude (peak vertical GRF magnitude).
The kinematics of the tibia with respect to the femur weredescribed for both OMC and biplanar videoradiography datasets using two independent anatomical coordinate systems(ACS). These ACSs were determined from the 3-D CT modelsof the femur and tibia using previously described methods(25). To use the same ACS for both OMC and biplanar vid-eoradiography, their global coordinate spaces were coregis-tered using a rigid lattice containing spherical markers thatwere radioopaque and retroreflective (24). The mean and SDfor the root mean square fit error of the coregistration trans-forms was 0.31 T 0.09 mm.
Knee joint rotations in FL/EX, adduction/abduction (AD/AB), and IN/EX rotations of the tibia relative to the femurwere interpreted using the method described by Grood andSuntay (18). Joint translations in medial/lateral (ME/LA)and anterior/posterior (AN/PO) displacements of the tibia
relative to the femur were determined by a vector originatingat the origin of femoral ACS and terminating at the origin ofthe tibial ACS (14). The ME/LA and AN/PO translationswere normalized for each subject according to the ME/LAor AN/PO width of their tibial plateau, similar to the methodreported by Tanifuji et al. (32). These translations are inter-preted as percentage ME/LA or AN/PO tibial plateau width.Normalization was performed to make kinematic evalua-tions on individuals of different sizes.
Because of the limited FOV of the biplanar videoradio-graphy system, the joint rotations and translations were timenormalized from 16 ms before contact to 60 ms after contact.This window was selected because it was common to all sub-jects for at least one trial. For comparison, all joint rotationsand translations were zeroed at contact and interpreted as ex-cursion. The average rate and maximum rate of AN/PO ex-cursion was determined for each subject. Average rate wascalculated as the total range divided by the change in time, andthe maximum rate was calculated as the maximum time de-rivative. In addition, the area under the curve (AUC), whichsimplifies time-series curve comparisons, was calculated foreach time-series kinematic excursion trace by integrating thesignal with respect to time.
The FOV of the OMC system is significantly larger thanthat of the biplanar videoradiography system, permittingthe measurement of knee FL/EX angle outside the periodcontaining the biplanar videoradiography data. Despite the
FIGURE 2—A, ACLINT vertical GRF. B, ACLREC vertical GRF. Each subject’s GRF was normalized by their respective weight. Thus, vertical GRFunits are in body weights. Notice the highlighted peak in the ACLINT vertical GRF graph. All curves are displayed as mean T 1 SD. The vertical line oneach graph represents the time at contact. C, ACLINT AN/PO translational excursion. D, ACLREC AN/PO translational excursion. Anterior is positiveand posterior is negative. All AN/PO translations were normalized for each subject by their respective tibial plateau width. Thus, translational unitsare defined as a percentage of the total tibial width in the anterior–posterior direction. It should be noted that the AN/PO translational excursion datawere obtained from the biplanar videoradiography system.
KNEE BIOMECHANICS DURING A JUMP-CUT MANEUVER Medicine & Science in Sports & Exercised 945
APPLIED
SCIEN
CES
Copyright © 2013 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

soft tissue artifact observed in secondary rotations (AD/ABand IN/EX rotation) and translations (ME/LA and AN/PO)obtained from OMC, FL/EX remains relatively unaffected(24). Using the OMC data, the minimum flexion angle aftercontact was determined. In addition, the change from mini-mum flexion angle to maximum flexion angle after contactwas calculated and interpreted as excursion. The OMC datawere presented for only knee joint FL/EX. The biplanarvideoradiography data are presented for all other kine-matic parameters (AD/AB and IN/EX rotations, ME/LAand AN/PO translations).
The described kinematic and GRF outcomes were deter-mined for each applicable subject trial, and then all trialswere ensemble averaged for each subject. Comparisons be-tween sex (M and F) and ACL reconstruction status (ACLINTand ACLREC) were made for all kinematic and kinetic vari-ables using two-way ANOVA. These tests were performedwith a significance level (alpha) of 0.05. Pairwise multiplecomparisons were made using the Holm–Sidak method whena significant sex and ACL reconstruction status interactionwas determined. The Holm–Sidak method maintains alphaat 0.05 across a set of hypothesis tests and adjusts P valuesdifferently depending on their values ranked against eachother. This is effective at maintaining alpha and avoidingbeta inflation.
RESULTS
A statistically significant interaction (P = 0.003) betweensex and ACL reconstruction status was observed for thepeak vertical GRF (Fig. 2). Within the ACLINT subjects, thefemales had a peak vertical GRF that was 1.45 body weightslarger than the male subjects (P G 0.001). In contrast, theACLREC male and female subjects had nearly equal peakvertical GRF. The ACLREC male subjects’ peak verticalGRF was 0.22 body weights larger than the female ACLREC
subjects but was not statistically significant (P = 0.522).When comparing within ACL reconstruction status, both themale and female ACLINT subjects had a larger peak verticalGRF than the male and female ACLREC subjects, respec-tively. The male ACLINT subjects’ peak vertical GRF were0.80 body weights larger than the male ACLREC subjects(P = 0.036), and the female ACLINT subjects’ peak verti-cal GRF were 2.46 body weights larger than the femaleACLREC subjects (P G 0.001).
The peak vertical GRF for the female subjects occurred6.24 ms earlier than the male subjects (P = 0.021). Theinteraction between sex and ACL reconstruction status ap-proached but was not statistically significant (P = 0.117);the peak vertical GRF for the female ACLREC subjects oc-curred only 2.21 ms before the male ACLREC subjects.Conversely, the peak vertical GRF for the female ACLINT
subjects occurred 10.27 ms before the male ACLINT subjects.Moreover, the peak vertical GRF appears to occur earlier inACLINT subjects than ACLREC subjects (4.80 ms, P = 0.066).
The average rate of AN/PO translational excursion (Fig. 2)was 0.05%Imsj1 larger for ACLINT subjects compared withACLREC subjects (P = 0.035) and 0.05%Imsj1 larger forfemale subjects compared with male subjects (P = 0.037).The maximum rate of AN/PO translational excursion was0.13%Imsj1 larger in female ACLINT subjects as comparedwith male ACLINT subjects; however, the difference betweensexes in ACLREC subjects was only 0.01%Imsj1. Pairwisemultiple comparisons revealed that maximum AN/PO trans-lational excursion rate differences were significant for malesversus females within ACLINT subjects (P = 0.027) and forACLINT versus ACLREC within female (P = 0.007). In addi-tion, the AUC of the AN/PO translational excursion wasobserved to be 55%Ims larger for ACLINT subjects thanACLREC subjects (P = 0.180). The AUC for the female sub-jects was also larger than the AUC for the male subjects(64%Ims, P = 0.122). No significant interaction between sexand ACL reconstruction status was observed (P = 0.961).However, the AUC of the AN/PO translational excursionwas observed to be 66%Ims larger for female ACLINT sub-jects than for male ACLINT subjects, and the AUC for thefemale ACLREC subjects was also larger than the AUC for themale ACLREC subjects (62.1%Ims). These AN/PO trans-lational kinematic data were determined from the biplanarvideoradiography system.
The AD/AB rotational excursion (Fig. 3) was relativelyconstant after contact, changing less than 2- for both maleand female ACLREC and ACLINT subjects. Despite theminimal rotational change after contact, the female subjectswere abducting (valgus) slightly after contact, whereas themale subjects were adducting (varus) slightly after contact(the average female abduction excursion was equal to 1.02-and the average male adduction excursion was equal to1.07-, P = 0.033). The IN/EX rotational excursion (Fig. 3)for all subjects followed a consistent pattern. Specifically,the male and female ACLINT and ACLREC subjects all beganinternally rotating after contact. Although no statisticallysignificant differences were observed in any group, theACLINT male and female subjects had a 76-Ims larger AUCthan the ACLREC male and female subjects (P = 0.171).These AD/AB and IN/EX rotational kinematic data weredetermined from the biplanar videoradiography system.
The minimum flexion angle occurred at or immediatelyafter ground contact. After this, all of the subjects absorbedthe landing and continued the cut by flexing through stancephase to a maximum flexion angle. Using the OMC data toquantify the minimum flexion angle, maximum flexion angle,and the flexion angle excursion (change from minimum tomaximum flexion angle), we observed that females tended tobe more flexed at contact (P = 0.054), but their total excursionwas significantly less (P = 0.002) (Fig. 4). These FL/EX ki-nematic data were determined from the OMC system.
We have included the following data as supplementaldigital content to provide contextual reference for the aboveresults: 1) the knee angles (in degrees) at contact and peakvertical GRF for knee FL/EX, AD/AB, and IN/EX obtained
http://www.acsm-msse.org946 Official Journal of the American College of Sports Medicine
APP
LIED
SCIENCES
Copyright © 2013 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

from OMC and biplanar videoradiography (see Table A, Sup-plemental Digital Content 1, http://links.lww.com/MSS/A242);2) the peak AN/PO and ME/LA knee translations in millimetersand their respective time points in milliseconds (see Table B,Supplemental Digital Content 2, http://links.lww.com/MSS/A243);and 3) the AN/PO and ME/LA knee translation excursionsin millimeters (see Table C, Supplemental Digital Content 3,http://links.lww.com/MSS/A244).
DISCUSSION
We have compared knee kinematic and kinetic measure-ments from male and female ACLINT and ACLREC recrea-tional athletes during a jump-cut maneuver associated withnoncontact deceleration ACL injury. Two major findingswere observed in our study. First, female subjects who havenever had an ACL reconstruction appeared to perform thejump-cut maneuver with greater landing stiffness (smalleramount of knee flexion angle excursion combined with largerpeak vertical GRF [28]) than males with or without a historyof ACL reconstruction and other females with a history ofACL reconstruction. This was evidenced by the differencesobserved in the knee flexion angle excursion, which trans-lated to qualitatively comparable differences in peak verticalGRF. Second, the male and female ACLREC subjects appearto perform the jump-cut maneuver with less energy than theACLINT subjects, resulting in a lower peak vertical GRF even5 yr or more after their reconstruction. This may be a result of
differences in strength, confidence, habit, and/or training aftertheir injury.
These kinetic differences likely influence the differencesobserved in the rate of anterior tibial translation after contact,which is a common instigator of ACL injury. Specifically, weobserved that anterior tibial translation increased at a faster
FIGURE 3—A, ACLINT AD/AB rotational excursion. B, ACLREC AD/AB rotational excursion. Adduction is positive and abduction is negative. C,ACLINT IN/EX rotational excursion. D, ACLREC IN/EX rotational excursion. All rotational excursion units are in degrees. All curves are displayed asmean T 1 SD. The vertical line on each graph represents the time at contact. It should be noted that these data were obtained from the biplanarvideoradiography system.
FIGURE 4—Left y-axis, minimum knee flexion angle for ACLINT andACLREC male and female subjects. Minimum flexion occurred at orimmediately after ground contact. No statistically significant differ-ences between sex and condition were observed for minimum kneeflexion angle values; however, the asterisk (*) represents a P value of0.054, denoting an apparent sex difference. Right y-axis, knee flexionangle excursion for ACLINT and ACLREC male and female subjects.Knee flexion angle excursion was defined as the change in knee flexionangle from minimum flexion to maximum flexion. A statistically sig-nificant difference was observed between male and female subjects.This is highlighted by the double asterisk (**), which represents aP value of 0.002. The minimum knee flexion angle and knee flexion angleexcursion units are in degrees. It should be noted that these data wereobtained from the OMC system.
KNEE BIOMECHANICS DURING A JUMP-CUT MANEUVER Medicine & Science in Sports & Exercised 947
APPLIED
SCIEN
CES
Copyright © 2013 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

rate in female ACLINT subjects compared with their maleACLINT counterparts (Fig. 2). Notably, peak anterior tibialtranslation for the ACLINT female subjects occurred within60 ms. A similar peak was not observed in the male ACLINT
subjects or the male and female ACLREC subjects. Interest-ingly, the time-to-peak vertical GRF was significantly less infemale subjects as compared with male subjects. Also, thetime-to-peak vertical GRF appears to be smaller in ACLINT
subjects as compared with ACLREC subjects. The increasedrate of anterior tibial translation observed in female ACLINT
subjects is likely a result of the larger and more rapid peakvertical GRF observed immediately after ground contact.This rapid and large peak vertical GRF appears to produce a‘‘snapping’’ motion that differs from the more gradual in-crease in peak vertical GRF and anterior tibial translationobserved in male ACLINT subjects and male and femaleACLREC subjects. It may be that there is a reliable tendencyfor females to absorb less energy upon landing, which,through greater peak vertical GRF, resultant forces, and/orabnormal kinematics, may increase the risk for ACL injury.
Previous research has suggested that increased landingstiffness, as characterized by a smaller amount of kneeflexion angle excursion combined with a high vertical GRFduring landing and cutting activities, place individuals atincreased risk of ACL injury (6,8,11). Attempts have beenmade to correlate increased landing stiffness with increasedanterior tibial translation with the goal of developing kneeinjury prevention training and rehabilitation programs (28).During the jump-cut maneuver in our study, the femalesubjects landed and cut with less knee flexion angle excur-sion after contact. This result, when interpreted in the con-text of the faster and larger peak vertical GRF, confirms thatthe females are performing the jump-cut maneuver withmore landing stiffness. This finding is in contrast to theobservations made for the male subjects, who appear to beabsorbing the energy they are applying at ground contact byflexing through the landing and subsequent cut. Moreover,the AN/PO translation never reached a maximum (within60 ms after contact) and increased at a lower rate aftercontact for the male ACLINT and male and female ACLREC
subjects. This combination of increased knee flexion angleexcursion and/or reduced peak vertical GRF (decreasedlanding stiffness) may contribute to the slower time-to-peakanterior tibial translation after contact for these subjects.
In a similar study investigating the knee kinematics ofACLINT females during four functional tasks, Myers et al.(29) observed that anterior tibial translation was increased inactivities of increasing external loading. Specifically, theyobserved a 2.4-mm increase in anterior tibial translation dur-ing landing maneuvers as compared with walking. Moreover,their results show the same characteristic peak vertical GRFimmediately after ground contact during the landing tasks.This peak is absent in the vertical GRF walking trace. Con-versely, another study by Myers et al. (28) showed no dif-ferences in anterior tibial translation between soft and stiffdrop landings. The authors attributed these findings to the
ability of the ligaments and musculature about the knee tokeep joint translations within a safe envelope of motionduring controlled activities where external loading con-ditions are anticipated. Although no excessive rotational ortranslation motion was observed in our study, the increasedrate of anterior translation in female ACLINT subjects sug-gests that stiffer landings under more unanticipated cuttingactivities may affect kinematic translations more thancontrolled, anticipated activities. Furthermore, the lowerrate of anterior tibial translation seen in the ACLREC sub-jects immediately after contact may be influenced by thelower peak vertical GRF.
This low peak vertical GRF observed in both male andfemale ACLREC subjects matches results from Paterno et al.(30,31) and Vairo et al. (38). In two separate studies, Paternoet al. showed ACLREC male and female subjects decreasedpeak vertical GRF when performing landing activities 2 yrafter reconstruction. Vairo et al. reported decreased verticalpeak GRF upon landing from a vertical drop among ACLRECsubjects approximately 2 yr postsurgery. These results areconsistent with those reported in our study for ACLREC menand women who are at least 5 yr postreconstruction. In addi-tion, no sex differences were observed in the peak GRF withinACLREC subjects. Even after 5 yr of strengthening activities,including formal rehabilitation, functional exercise, and returnto sports, the ACLREC subjects performed the jump-cut ma-neuver with less energy compared with the ACLINT subjects.Although the exact mechanisms for this are unknown, it ispossible that both behavioral and neuromechanical deficien-cies are present in the ACLREC subjects when performingjump-cut maneuvers on their previously injured limb. Alter-natively, it is possible that the altered mechanics are a resultof protective habits obtained during the ACLREC subjects’rehabilitation. Additional research investigating neuromus-cular activity and contralateral biomechanics may provideadditional insight into the reduced vertical GRF observed inboth male and female ACLREC subjects.
In addition to the larger peak vertical GRF and rate ofanterior tibial translation, the female subjects were generallyabducting after contact (Figs. 3A–B). This is an interestingfinding because videographic studies have suggested that avalgus (abduction) collapse is involved in the noncontactdeceleration ACL injury mechanism (21). Furthermore, theresults presented herein are consistent with previous reportssuggesting that females land with more knee abductioncompared with males (15). Although the female subjects inour study were abducting after contact compared with themale subjects, the total amount of abduction (G2-) does notseem to correspond to a valgus collapse position. This maybe a result of the subjects’ ability to safely perform the jump-cut maneuver, which was implemented in our study tochallenge the ACL. A valgus collapse position was not ob-served, neither were any adverse events (injury).
No significant differences were observed between sexand ACL reconstruction status for both IN/EX rotation orME/LA translation after contact (Table 2). In general, all
http://www.acsm-msse.org948 Official Journal of the American College of Sports Medicine
APP
LIED
SCIENCES
Copyright © 2013 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

subjects began internally rotating after contact and remainedstable in the ME/LA direction. With exception to the sexdifference observed in AD/AB angle, the similar kinematicoutcomes observed between sex and ACL reconstructionstatus after contact do not support our hypothesis. Denewethet al. (14) showed that, as compared with the ACLINT con-tralateral knees, ACLREC knees were more externally rotatedand less laterally translated during a single-leg hopped land-ing. Unfortunately, obtaining contralateral limb kinematicswas not feasible for our study. This makes direct comparisonsdifficult; however, Deneweth et al. does report total IN/EXexcursion to be approximately 5- and total ME/LA translationto be less than 1 mm for both reconstructed and contralateral
knees. These excursion values align with the results presentedin our study.
Despite the kinematic similarities, additional research in-vestigating surface interactions between the medial and lateralcompartments of the knee may provide more specific insightinto subtle kinematic differences between both sex andACL reconstruction status. Specifically, methods have beendeveloped to identify distance-weighted proximity centroids,regions of closest proximity (1), and point-based surfacevelocities (2,3). These techniques take advantage of the ac-curacy associated with biplanar videoradiography to makeinferences about biomechanical changes at the articulat-ing surfaces of the femur and tibia with the hope of better
TABLE 2. ACLINT and ACLREC male and female kinematic AUC, rate, and peak vertical GRF results.
Outcome ACL Status Mean SEM P Sex Mean SEM P Interaction Mean SEM P
AD\AB excursionAUC (-Ims)
ACLINT j5.18 13.74 0.406 M 26.03 14.58 0.033 INT � M 25.88 19.43 0.415INT � F j36.24 19.43
ACLREC 11.57 14.03 F j19.65 13.16 REC � M 26.19 21.73REC � F j3.05 17.74
IN\EX excursionAUC (-Ims)
ACLINT 76.59 32.91 0.171 M 38.06 34.21 0.815 INT � M 86.81 45.61 0.505INT � F 66.37 45.61
ACLREC 10.59 32.25 F 49.04 30.88 REC � M j10.63 50.99REC � F 31.71 41.63
ME\LA excursionAUC (%Ims(mmIms))
ACLINT 6.56(4.06)
12.65(9.31)
0.153 M j17.35(j14.25)
13.41(9.87)
0.269 INT � M j6.85(j5.72)
17.89(13.16)
0.739
INT � F 19.97(13.83)
17.89(13.16)
ACLREC j20.57(j15.92)
12.91(9.50)
F 3.34(2.319)
12.11(8.91)
REC � M j27.84(22.79)
20.00(14.72)
REC � F j13.292(j9.20)
16.33(12.02)
AN\PO excursionAUC (%Ims(mmImsj1))
ACLINT 303.85(162.80)
27.417(15.08)
0.180 M 244.38(139.89)
29.08(15.99)
0.122 INT � M 270.85(150.74)
38.77(21.33)
0.961
INT � F 336.84(174.85)
38.77(21.33)
ACLREC 248.96(138.56)
27.98(15.39)
F 308.42(161.47)
26.25(14.44)
REC � M 217.91(129.04)
43.35(23.84)
REC � F 280.01(148.08)
35.40(19.47)
AN\PO averagerate (%Imsj1
(mmImsj1))
ACLINT 0.22(0.12)
0.02(0.01)
0.035 M 0.17(0.10)
0.02(0.01)
0.037 INT � M 0.18(0.10)
0.02(0.01)
0.213
INT � F 0.26(0.13)
0.02(0.01)
ACLREC 0.17(0.10)
0.02(0.01)
F 0.22(0.12)
0.01(0.01)
REC � M 0.16(0.10)
0.02(0.01)
REC � F 0.18(0.10)
0.02(0.01)
AN\PO maximumrate (%Imsj1*(mmImsj1))
ACLINT 0.39(0.21)
0.03(0.01)
0.035 M 0.31(0.18)
0.03(0.02)
0.135 INT � M 0.32(0.18)
0.04(0.02)
0.087
INT � F 0.45(0.23)
0.04(0.02)
ACLREC 0.30(0.17)
0.03(0.02)
F 0.37(0.19)
0.03(0.01)
REC � M 0.30(0.18)
0.04(0.02)
REC � F 0.29(0.16)
0.03(0.02)
Peak vertical GRFmagnitude bodyweight**
ACLINT 1.53 0.17 NA M 2.04 0.17 NA INT � M 2.44 0.23 0.003INT � F 3.88 0.23
ACLREC 3.16 0.16 F 2.65 0.16 REC � M 1.64 0.26REC � F 1.42 0.21
PEAK vertical GRFtime (ms)
ACLINT 16.73 1.70 0.066 M 22.25 1.80 0.021 INT � M 21.87 2.40 0.117INT � F 11.60 2.40
ACLREC 21.53 1.74 F 16.01 1.63 REC � M 22.63 2.69REC � F 20.42 2.19
A two-way ANOVA was performed on each set of data. Statistically significant differences (P e 0.05) are in boldface Roman. Near statistical significance (P e 0.10) is in boldface italics.Pairwise comparisons were made using the Holm–Sidak method when a significant (or near significant) sex and ACL reconstruction status interaction was determined. These results,denoted by the * or **, are given as footnotes. The data presented in the parentheses (ME/LA and AN/PO AUC, AN/PO rates) are the raw translational values in millimeters. Finally, itshould be noted that the kinematic data presented in this table were obtained from the biplanar videoradiography system.*MvF in I: P = 0.027; MvF in R: P = 0.863; IvR in M: P = 0.751; IvR in F: P = 0.007.**MvF in I: P G 0.001; MvF in R: P = 0.522; IvR in M: P = 0.036; IvR in F: P G 0.001
KNEE BIOMECHANICS DURING A JUMP-CUT MANEUVER Medicine & Science in Sports & Exercised 949
APPLIED
SCIEN
CES
Copyright © 2013 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

understanding the initiation and progression of osteoarthritisin ACLREC individuals (4).
As investigators, we are limited to studying potential injurymechanisms in a laboratory testing environment withoutmany of the situations presented in a sporting environment.Our study investigated male and female ACLINT and ACLREC
subjects while they performed an activity in a controlledlaboratory setting that has been associated with noncontactdeceleration ACL injury. The incorporation of the ‘‘unantic-ipated’’ element to the jump-cut maneuver mimicked the de-celeration and cutting action associated with many sportingevents. Despite the design, studies that use biplanar video-radiography will be hindered by the inability to capture sub-jects performing sports activities in their native environments.
We acknowledge the small sample size for investigatingkinematic and kinetic interactions between sex and ACLreconstruction status. Although we did ensure that all sub-jects were recreational athletes, we were not able to controlfor surgeon or rehabilitation protocol for the ACLREC sub-jects. In addition, we recognize the limitation of using twodifferent graft types in our study. Based on biomechanicalstudies (34,39) and randomized clinical trials (27), we assumedthat both bone-patellar tendon-bone and four-stranded ham-string tendon grafts would respond similarly during the jump-cut maneuver studied herein but recognized this as a studylimitation.
Limitations associated with biplanar videoradiographyshould be noted. Specifically, the FOV restricted our abilityto capture kinematic data for all subjects from 16 ms beforecontact to 60 ms after contact. Previous research has shownthat peak anterior tibial translation occurs between 40 and50 ms after contact (37), within the temporal range studied.Finally, each subject received up to 22 mrem of radiationexposure as a result of the biplanar videoradiography systemand CT scan. Although this falls well below the guidelinesinstituted by the National Institutes of Health RadiationSafety Committee for acceptable radiation exposure to
research subjects within a year (5 rem), it does limit thenumber of data collection trials. All subjects were awareof and gave informed consent to radiation exposure.
In conclusion, the results presented in our study supportour hypothesis that kinematic and kinetic differences wouldbe observed between both sex and ACL reconstructionstatus during a jump-cut maneuver. Specifically, we foundthat female ACLINT subjects landed and cut with a smalleramount of knee flexion angle excursion and larger peakvertical GRF than the male ACLINT subjects. Furthermore,we observed that the ACLREC subjects had a significantlylower peak vertical GRF just after impact as compared withthe ACLINT subjects. We also noted that female ACLINT
subjects appear to have an increased rate of anterior tibialtranslation just after contact. Our study associates the in-creased rate of anterior tibial translation to increased landingstiffness (larger peak vertical GRF combined with smallerknee flexion angle excursion) while performing the jump-cut maneuver. With respect to AD/AB, IN/EX rotation, andME/LA translation, differences were only observed AD/ABangle. The female subjects in our study were abducting aftercontact compared with the male subjects; however, theamount of abduction does not appear to correspond to avalgus collapse position. Finally, no significant interactionswere found between sex and ACL reconstruction status forIN/EX rotation or ME/LA translation after contact.
The authors greatly acknowledge the efforts of AlisonM. Biercevicz,Michelle M. Gosselin, Joel B. Schwartz, and JamesC. Tarrent for theirassistance in data collection and subject preparation. Funding forthis project was received from the W.M. Keck Foundation, NIH 2R01-AR047910, NIH COBRE 2P20-GM104937, and the Lucy LippittEndowment.
The authors declare no conflict of interest.Its contents are solely the responsibility of the authors and do not
necessarily represent the official views of the W.M. Keck Foundation,NIAMS, National Institutes of Health, or the American College ofSports Medicine.
REFERENCES
1. Anderst WJ, Tashman S. A method to estimate in vivo dynamicarticular surface interaction. J Biomech. 2003;36(9):1291–9.
2. Anderst WJ, Tashman S. The association between velocity of thecenter of closest proximity on subchondral bones and osteoarthritisprogression. J Orthop Res. 2009;27(1):71–7.
3. Anderst WJ, Tashman S. Using relative velocity vectors to revealaxial rotation about the medial and lateral compartment of theknee. J Biomech. 2010;43(5):994–7.
4. Andriacchi TP, Mundermann A, Smith RL, Alexander EJ, DyrbyCO, Koo S. A framework for the in vivo pathomechanics of os-teoarthritis at the knee. Ann Biomed Eng. 2004;32(3):447–57.
5. Ardern CL, Taylor NF, Feller JA, Webster KE. Return-to-sportoutcomes at 2 to 7 years after anterior cruciate ligament recon-struction surgery. Am J Sports Med. 2012;40(1):41–8.
6. Beutler A, de la Motte S, Marshall S, Padua D, Boden B. Musclestrength and qualitative jump–landing differences in male and femalemilitary cadets: the jump-ACL study. J Sports Sci Med. 2009;8:663–71.
7. Bey MJ, Zauel R, Brock SK, Tashman S. Validation of a newmodel-based tracking technique for measuring three-dimensional,in vivo glenohumeral joint kinematics. J Biomech Eng. 2006;128(4):604–9.
8. Boden BP, Dean GS, Feagin JA, Garrett WE. Mechanisms of an-terior cruciate ligament injury. Orthopedics. 2000;23(6):573–8.
9. Brainerd EL, Baier DB, Gatesy SM, et al. X-ray reconstruction ofmoving morphology (XROMM): precision, accuracy and appli-cations in comparative biomechanics research. J Exp Zool A EcolGenet Physiol. 2010;313(5):262–79.
10. Buczek FL, Rainbow MJ, Cooney KM, Walker MR, Sanders JO.Implications of using hierarchical and six degree-of-freedom modelsfor normal gait analyses. Gait Posture. 2010;31(1):57–63.
11. Chappell JD, Creighton RA, Giuliani C, Yu B, Garrett WE.Kinematics and electromyography of landing preparation in verti-cal stop-jump: risks for noncontact anterior cruciate ligament in-jury. Am J Sports Med. 2007;35(2):235–41.
http://www.acsm-msse.org950 Official Journal of the American College of Sports Medicine
APP
LIED
SCIENCES
Copyright © 2013 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

12. Coburn J, Crisco JJ. Interpolating three-dimensional kinematicdata using quaternion splines and hermite curves. J Biomech Eng.2005;127(2):311–7.
13. Dargel J, Gotter M, Mader K, Pennig D, Koebke J, Schmidt-Wiethoff R. Biomechanics of the anterior cruciate ligament andimplications for surgical reconstruction. Strategies Trauma LimbReconstr. 2007;2(1):1–12.
14. Deneweth JM, Bey MJ, McLean SG, Lock TR, Kolowich PA,Tashman S. Tibiofemoral joint kinematics of the anterior cruciateligament-reconstructed knee during a single-legged hop landing.Am J Sports Med. 2010;38(9):1820–8.
15. Ford KR, Myer GD, Toms HE, Hewett TE. Gender differences inthe kinematics of unanticipated cutting in young athletes. Med SciSports Exerc. 2005;37(1):124–9.
16. Gianotti SM, Marshall SW, Hume PA, Bunt L. Incidence of an-terior cruciate ligament injury and other knee ligament injuries: anational population-based study. J Sci Med Sport. 2009;12(6):622–7.
17. Griffin LY, Albohm MJ, Arendt EA, et al. Understanding andpreventing noncontact anterior cruciate ligament injuries: a reviewof the Hunt Valley II meeting, January 2005. Am J Sports Med.2006;34(9):1512–32.
18. Grood ES, Suntay WJ. A joint coordinate system for the clinicaldescription of three-dimensional motions: application to the knee.J Biomech Eng. 1983;105(2):136–44.
19. Gwinn DE, Wilckens JH, McDevitt ER, Ross G, Kao TC. Therelative incidence of anterior cruciate ligament injury in men andwomen at the United States Naval Academy. Am J Sports Med.2000;28(1):98–102.
20. Junkin DM, Johnson DJ, Fu FH, et al. Knee ligament injuries.Orthopaedic Knowledge Update: Sports Medicine 4. 4th ed.American Academy of Orthopaedic Surgeons; Rosemont, IL: 2009.pp. 135–53.
21. Krosshaug T, Nakamae A, Boden BP, et al. Mechanisms of ante-rior cruciate ligament injury in basketball: video analysis of 39cases. Am J Sports Med. 2007;35(3):359–67.
22. Markolf KL, Kochan A, Amstutz HC. Measurement of kneestiffness and laxity in patients with documented absence of theanterior cruciate ligament. J Bone Joint Surg Am. 1984;66(2):242–52.
23. McNair PJ, Marshall RN, Matheson JA. Important features asso-ciated with acute anterior cruciate ligament injury. N Z Med J.1990;103(901):537–9.
24. Miranda DL, Rainbow MJ, Crisco JJ, Fleming BC. Kinematicdifferences between optical motion capture and biplanar video-radiography during a jump-cut maneuver. J Biomech. 2013;46(3):567–73.
25. Miranda DL, Rainbow MJ, Leventhal EL, Crisco JJ, Fleming BC.Automatic determination of anatomical coordinate systems forthree-dimensional bone models of the isolated human knee. JBiomech. 2010;43(8):1623–6.
26. Miranda DL, Schwartz JB, Loomis AC, Brainerd EL, Fleming BC,Crisco JJ. Static and dynamic error of a biplanar videoradiography
system using marker-based and markerless tracking techniques. JBiomech Eng. 2011;133(12):121002.
27. Mohtadi NG, Chan DS, Dainty KN, Whelan DB. Patellar tendonversus hamstring tendon autograft for anterior cruciate ligamentrupture in adults. Cochrane Database Syst Rev. 2011;(9):CD005960.
28. Myers CA, Torry MR, Peterson DS, et al. Measurements oftibiofemoral kinematics during soft and stiff drop landings usingbiplane fluoroscopy. Am J Sports Med. 2011;39(8):1714–22.
29. Myers CA, Torry MR, Shelburne KB, et al. In vivo tibiofemoralkinematics during 4 functional tasks of increasing demand usingbiplane fluoroscopy. Am J Sports Med. 2012;40(1):170–8.
30. Paterno MV, Ford KR, Myer GD, Heyl R, Hewett TE. Limbasymmetries in landing and jumping 2 years following anteriorcruciate ligament reconstruction. Clin J Sport Med. 2007;17(4):258–62.
31. Paterno MV, Schmitt LC, Ford KR, Rauh MJ, Myer GD, HewettTE. Effects of sex on compensatory landing strategies upon returnto sport after anterior cruciate ligament reconstruction. J OrthopSports Phys Ther. 2011;41(8):553–9.
32. Tanifuji O, Sato T, Kobayashi K, et al. Three-dimensional in vivomotion analysis of normal knees using single-plane fluoroscopy.J Orthop Sci. 2011;16(6):710–8.
33. Tashman S, Collon D, Anderson K, Kolowich P, Anderst W.Abnormal rotational knee motion during running after anterior cru-ciate ligament reconstruction. Am J Sports Med. 2004;32(4):975–83.
34. Tashman S, Kolowich P, Collon D, Anderson K, Anderst W.Dynamic function of the ACL-reconstructed knee during running.Clin Orthop Relat Res. 2007;454:66–73.
35. Tegner Y, Lysholm J. Rating systems in the evaluation of kneeligament injuries. Clin Orthop Relat Res. 1985;(198):43–9.
36. Torry MR, Myers C, Shelburne KB, et al. Relationship of kneeshear force and extensor moment on knee translations in femalesperforming drop landings: a biplane fluoroscopy study. ClinBiomech (Bristol, Avon). 2011;26(10):1019–24.
37. Torry MR, Shelburne KB, Peterson DS, et al. Knee kinematicprofiles during drop landings: a biplane fluoroscopy study. MedSci Sports Exerc. 2011;43(3):533–41.
38. Vairo GL, Myers JB, Sell TC, Fu FH, Harner CD, Lephart SM.Neuromuscular and biomechanical landing performance subse-quent to ipsilateral semitendinosus and gracilis autograft anteriorcruciate ligament reconstruction. Knee Surg Sports TraumatolArthrosc. 2008;16(1):2–14.
39. Wilson TW, Zafuta MP, Zobitz M. A biomechanical analysis ofmatched bone-patellar tendon-bone and double-looped semiten-dinosus and gracilis tendon grafts. Am J Sports Med. 1999;27(2):202–7.
40. Wright RW, Dunn WR, Amendola A, et al. Risk of tearing theintact anterior cruciate ligament in the contralateral knee and rup-turing the anterior cruciate ligament graft during the first 2 yearsafter anterior cruciate ligament reconstruction: a prospectiveMOON cohort study. Am J Sports Med. 2007;35(7):1131–4.
KNEE BIOMECHANICS DURING A JUMP-CUT MANEUVER Medicine & Science in Sports & Exercised 951
APPLIED
SCIEN
CES
Copyright © 2013 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.