ComET Peer Input Meeting Context & Objectives Nov. 8th, 2004 B ette Meek, Health Canada .
38
ComET Peer Input Meeting ComET Peer Input Meeting Context & Objectives Context & Objectives Nov. 8th, 2004 Nov. 8th, 2004 B B ette Meek, Health Canada ette Meek, Health Canada www.hc-sc.gc.ca/exsd-dse www.hc-sc.gc.ca/exsd-dse
-
Upload
emerson-jacox -
Category
Documents
-
view
216 -
download
0
Transcript of ComET Peer Input Meeting Context & Objectives Nov. 8th, 2004 B ette Meek, Health Canada .

ComET Peer Input Meeting ComET Peer Input Meeting Context & ObjectivesContext & Objectives
Nov. 8th, 2004Nov. 8th, 2004
BBette Meek, Health Canadaette Meek, Health Canadawww.hc-sc.gc.ca/exsd-dsewww.hc-sc.gc.ca/exsd-dse

2ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Who Are We?
• Existing Substances Division of the Healthy Environments & Consumer Safety Branch of Health Canada (HECS/HC)
• Address HC responsibilities for Existing Industrial Chemicals under the Canadian Environmental Protection Act (CEPA)
• Partnership with Environment Canada – Administrators of CEPA
– What does this mean…………………..????

3ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
The Canadian Environmental Protection Act (CEPA)
• To protect the environment, human life and health from risks associated with pollution
• Primary authority to assess and manage the risks posed by toxic substances (not covered under other legislation) to protect health and the environment– Risk assessment the scientific underpinning
• Progressive, encompassing with broad range of powers for (e.g.):– information gathering & reporting/research – assessment and management/control– Enforcement/Emergency planning
• Administered by Environment Canada and Health Canada– Introduced in 1988 and renewed in 1999 – Provision for renewal every 5 years

4ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
What is “CEPA toxic”? Outcome of Risk Assessment
• A substance is “CEPA toxic” when it enters or may enter the environment in a quantity or under conditions that:– “have or may have an immediate or long-term
harmful effect on the environment or its biological diversity” – subsection 64(a)
– “constitute or may constitute a danger to the environment on which life depends” – subsection 64(b)
– “constitute or may constitute a danger in Canada to human life or health” – subsection 64(c)

5ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Mandated Timeframes in CEPA
Risk Assessment
Risk ManagementResearch & Surveillance
Public CEPA Registry
Program Management
Drivers
Mandated CEPA time-frames

ComET Peer Input meeting, Cincinnati, Nov. 8th/04
2
Existing Substances under CEPA
• Approximately 23,000 substances (e.g., industrial chemicals) on the Domestic Substances List (DSL)
• The DSL was created for the purpose of defining a “new substance” under CEPA– If “notified” at time of compilation, not considered
“new”• Includes substances “grandfathered” under the legislation
– i.e., those used for commercial manufacturing or manufactured or imported in Canada at • >100 kg/year between January 1, 1984 and December 31,
1986 • Organics (50%), inorganics, polymers and substances of
unknown or variable composition, complex reaction products & biological materials (UVCBs)

7ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Assessment of CEPA Existing Substances – Health Canada Mandate
• Address both exposure and effect to set priorities for risk management– Consumer & Environmental Exposure– All age groups– Multimedia
• Identifying most important media/sources of human exposure
• Source characterizations to inform risk management– Information Gathering/Industrial Surveys
• Publicly accountable – transparent process, peer review, documented outcome
• Information gathering, reverse onus provisions, but responsibility of Government considerable

8ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
CEPA – Why Consumer Exposure?
• CEPA is progressive, requiring systematic consideration of multimedia exposure to existing chemicals
• Broad range of powers under CEPA for risk management of substances
• HECS has responsibility for both the Hazardous Products Act & CEPA – health aspects

9ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Assessment of CEPA Existing Substances • Under CEPA ’88, assessments focussed on limited
numbers of Priority Substances (5 yr mandated timeframe)– N= 44 on Priority Substance List 1 (completed
1994)– N= 25 on Priority Substance List 2 (completed
2000)• CEPA ’99 extended our mandate to all Existing
Substances in Canada (n=23,000)– “Categorization” by 2006 to set priorities for
“screening” & full (Priority Substances) assessment
• Mandate is leading, internationally

10ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
CATEGORIZATION of the Domestic Substances List (DSL) (First Phase) (n=23,000)
Decisions of Other
Jurisdictions
Public Nominations
No further action under this program
CEPA-Toxic
No further action under this program
CEPA-Toxic
IN-DEPTH ASSESSMENT - Priority Substances List (Third Phase)
Risk Management
Risk Management
Greatest Potentialfor Human Exposure
Substances that are Persistent or Bioaccumulative
“Inherently Toxic”to Humans
“Inherently Toxic” tonon-Human Organisms
SCREENING ASSESSMENT (Second Phase)
STAGE 1
STAGE 2
STAGE N-1
STAGE N
STAGE 3
CEPA Existing Substances Program

11ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
“Categorization” (Priority Setting) for Existing Substances
• Short Term Objective:– To systematically set priorities for data generation
and assessment for both human health and ecological effects of all Existing Substances, without bias
• Long Term Objective:– Greater consistency in consideration of New
versus Existing Substances• Why is this Important?
– Many, if not most Existing Substances pose greater risk than New Substances
– Widespread use, often higher toxicity– Not systematically considered

12ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Principles of “Categorization” of Existing Substances (Cont’d)
• Requires significant technical capacity to “develop”/ “force” the science for precedent setting mandate– Expanding previous work on exposure/predictive
hazard tools– Drawing upon relevant resources internationally
• E.g., collaboration with European Commission/European industry
• Cut for “categorization” to be determined by the deadline (2006) & informed by:– public debate – iterative stages of “sorting” to identify priorities
• Simple and complex tools

13ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Principles/Objectives of “Categorization” of Existing Substances (Cont’d)
• First stages must be simple/pragmatic to address all substances, based on limited information for each
• Simple tools– Subsequent stages must be discriminating to set
true priorities for further work• Complex tools
• Protective– Conservative choices in the absence of data
• Challenge of the legislative construct– Relevance of persistence (P) or bioaccumulation
(B) to human health

14ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Products of “Categorization” under CEPA & Similar Programs (e.g., European Union)
• Information gathering/global repositories for Existing Chemicals– More data/information on existing
chemicals in the public domain• Development/refinement of predictive tools
• Exposure (modelling)• Effect [(Quantitative) structure activity
relationships (Q)SARs]
• Predictive tools will help additionally focus testing and research

15ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Process – Meeting the Mandate
• Key: Development of robust proposals for review in public forum, including:– Public peer input on complex components– External peer review of various components by
experts internationally • including those from stakeholder groups selected by
independent party
– Workshops of stakeholders to solicit input on specialized aspects
• Interpreting use codes
• Formal response to public comment

16ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Process – Meeting the Mandate (Cont’d)• Interface internationally to access forward looking
peer reviewed methodology addressing critical areas (in particular predictive tools) – Where industrial stakeholders could contribute
most• Continuing updates to all stakeholders
– industry, environmental groups, others• Communications pieces prepared & distributed as
soon as various components conceptualized in period leading up to full proposals – http://www.hc-sc.gc.ca/exsd-dse

17ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Efficiently Identifying Highest Priorities from a Human Health Perspective - Approach• Initial application of simple, discriminating tool on exposure
to address all 23,000 substances to prioritize - “greatest potential for exposure” (GPE), “intermediate potential for exposure” (IPE) & “lowest potential for exposure” (LPE)– Draws on information submitted in compilation of the
Domestic Substances List• Application of simple, discriminating tool to address hazard
for all 23,000 substances– Draws on work completed internationally
• Priority-based application of more complex tools to additionally refine list & order priorities – Exposure, dose-response– Priority setting takes into account where P or B has
potential to meaningfully contribute to human exposure

18ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
DOMESTIC SUBSTANCES LIST
Substances that are Persistent and/or Bioaccumulative According to the Regulations
Substances that are Persistent and/or
Bioaccumulative and Not “Inherently Toxic” to Non-
human OrganismsSubstances that are Persistent
and/or Bioaccumulative and “Inherently Toxic” to Non-
human Organisms
ENVIRONMENT CANADA
EC Substances Identified forScreening Assessment
Risk ranked list of Health Canada substances for screening
PROPOSED FRAMEWORK FOR DSL CATEGORIZATION
LowHigh
Highest
Lowest
HEALTH CANADA
DSL Substances Identified as Hazardous to Human
Health
DSL Substances Ranked According to Potential For Exposure

19ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Health Priorities for Screening Assessment Prioritized on the Basis of Potential Risk to Human Health (Exposure & Toxicity) – ca. 1000
PROPOSED APPROACH FOR HEALTH-RELATED COMPONENTS
OF DSL CATEGORIZATION
Low
High
Application of More Complex Tools to Refine Exposure Prioritization,
Identify Hazardous Substances and Evaluate Exposure-Response
Application of Simple Tools to
Prioritize According to Potential for
Exposure & Hazard for Entire DSL
DOMESTIC SUBSTANCES LIST
DSL Substances Ranked According to Potential For Exposure
LPE
DSL Substances Identified
as Hazardous to Human
Health
DSL Substances Identified
as Hazardous to Human
Health
GPE
IPE +
LPE
GPE
IPE

20ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
DSL TOOLS - HEALTH
Exposure
• SimET (Relative ranking of all DSL substances based on submitters (S),quantity (Q) and expert ranked use (ERU))
• ComET (Quantitative upper bound exposure estimate based upon use scenario, phys/chem properties & bioavailability)
Exposure-Response Tool
• ERT (measures of exposure-response developed [where possible] on the basis of measured or predicted carcinogenic potency, reference values or effect levels)
Hazard [High (H) or Low (L)]
• SimHaz (identification of high or low hazard compounds by various agencies based on weight of evidence)
• ComHaz (Hierarchical approach for multiple endpoints & data sources [e.g., (Q)SAR] including weight of evidence)

21ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Simple & Complex Exposure & Hazard Tools – What’s the Difference?
• Complexity of the exposure tools relates simply to level of information– Simple exposure tool is based on limited
information available for all substances– Complex exposure tool requires more information
to be discriminating• Simple hazard tools bias to selection of data-rich
compounds– i.e., all compounds are not treated the same way
• Complex hazard tools address all compounds in the same manner, thereby identifying those which are priorities for both data generation and assessment

22ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Simple Exposure Tool (SimET): Relative Ranking for all DSL substances
10%8.4
4.3
3
2
0
102
2
1
13227
189
94.5
58.4
0
≥105 kg/yrQ
Q
S
S
U
UInitial GPE list of 849 substancesIPE list of additional 1779
Quantity(Log)
Number of Submitters
Σ Use Code Indices
QuantityNumber of Submitters
Σ Use Code Indices
10%

23ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Criteria for Greatest, Intermediate and Lowest Potential for Exposure (GPE, IPE &
LPE)
Quantity (kg/year)
Number of Submitters
Sum of the Expert Ranked Use Code Indices
GPE > 100 000 Top 10% Top 10%
IPE > 10 000 n.a. Top 30%
LPE All All All

24ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
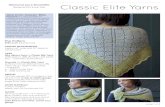
Complex Exposure Tool (ComET)
INHALATION
CROP ANDANIMAL PRODUCT
INGESTION
AQUEOUSEXPOSURE(ingestion,
dermal,inhalation)
IndustrialEffluents
Uptake byorganisms
Uptake byvegetation
IndustrialReleases to Soil
Drinking Water Bathing, Showering
IndustrialAtmospheric
Releases
SOILEXPOSURE(ingestion,
dermal)
Cosmetics
AdhesivesPaints
SprayCleaners
CONSUMERPRODUCTS(ingestion,
dermal,inhalation)
ComET - Near-fieldexposuresComET - Exposure to man from the environment

25ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Objectives of ComET – Existing Substances
• Upper bound quantitative estimate of combined consumer & multimedia environmental exposure, taking into account accessible information on:– Use categories, sentinel product scenarios – Physical/chemical properties– Bioavailability– Emissions
• Relevant to priority setting for both categorization and screening

26ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Another Exposure Model – Why??????
• Need to develop a much larger number of exposure scenarios than currently exist
• Need to integrate age specific exposure patterns particularly for products
• Need to extend existing fugacity models to address media of human exposure
• Provides the basis for additional refinement for higher level assessment by Health Canada and initiatives of other jurisdictions to systematically consider Existing Substances– Moving beyond the “data rich” focus of Existing
Substances

27ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
SimHaz – the Simple Discriminating Hazard ToolWeight of Evidence for Specified Endpoints• High Hazard Lists
– Cancer (IARC, EU, HC, US EPA etc.)– Genotoxicity (EU)– Developmental Toxicity (EU)– Reproductive Toxicity (EU)– Respiratory Sensitization (EU)
• Low Hazard Lists– PMRA Pesticide Formulants 4A List– OECD Low Concern List– “Grandfathered” lists DON’T COUNT!!

28ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
ComHaz – Setting Aside Non Priorities
• First stage: – Conservative hierarchical consideration of
multiple health endpoints • Specific criteria for a range of endpoints selected on
basis of potential public health impact and likelihood of available information
• Conservative “first hit” for data (most recent considered initially) or QSAR for range of endpoints
– Range of endpoints for genotoxicity – Low hazard compounds (e.g., those with potency
less than criteria) set aside from further consideration
• Focussing attention on higher priorities– Compounds not set aside go on to second stage
of priority setting

29ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
ComHaz - Weight of Evidence to Define Priorities
• Second stage:– Crude weight of evidence for data/(Q)SAR (latter
restricted to cancer/genotoxicity)• Observation in numbers of species/sexes, route
of administration• For genotoxicity, predictive strength of various
assays (i.e., in vivo vs. in vitro) mutagenicity/clastogenicity assays > DNA damage > Indicator tests)
– Consistency of repeated results– Robustness of (Q)SAR models

30ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Applying the Tools - Health Priorities for Categorization – the “Maximal” List
• Based on application of the “tools” to date, a maximum of 1904 substances (i.e., the draft “maximal” list) identified for further consideration in categorization for health– High (n=576), medium (n=989) and low
likelihood (n=331) of remaining on list in 2006• List released to focus the submission of solicited
information on the identity, use and/or toxicity on any substance prioritized for further consideration– Reducing the list prior to 2006– Focus on subset of high and the medium
likelihood group where tools still being applied

31ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
How Will ComET contribute to refinement of the maximal list/risk ranking?
Maximal List• For those in high likelihood and mid likelihood groups,
could lead to compounds being set aside on the basis of exposure, alone
Risk Ranking• Lower relative risk based on comparison with effect
level or potency estimate leading to lower priorityRemember: Priority setting is not risk assessment
– but allows non priorities to be set aside, &– identifies priorities for further consideration

32ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
CATEGORIZATION of the Domestic Substances List (DSL) (First Phase) (n=23,000)
Decisions of Other
Jurisdictions
Public Nominations
No further action under this program
CEPA-Toxic
No further action under this program
CEPA-Toxic
IN-DEPTH ASSESSMENT - Priority Substances List (Third Phase)
Risk Management
Risk Management
Greatest Potentialfor Human Exposure
Substances that are Persistent or Bioaccumulative
“Inherently Toxic”to Humans
“Inherently Toxic” tonon-Human Organisms
SCREENING ASSESSMENT (Second Phase)
STAGE 1
STAGE 2
STAGE N-1
STAGE N
STAGE 3
CEPA Existing Substances Program

33ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Screening Assessments for Health Priorities – Gaining Efficiencies in Assessment• Draws on work completed in other jurisdictions• Consideration of weight of evidence of hazard and
“margins of exposure” which compare upper bounding estimates of exposure to lowest effect levels– High hazard, proposed “toxic”– Margin wide, “set aside”– Margin small, additional assessment
• Decision making on the basis of adequacy of the margins, with clear delineation of confidence/uncertainties– draws on considerable collective experience
within HC (simplified process)• Concise model, focussing on critical information

34ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Framework for Screening – Health Priorities
Phase 3: Screening Health Assessment
• Screening health assessment of the nature of PFOS/PBDEs
Phase 1: Determination of Health-Related Priorities
• Application of “tools” to identify health-priorities for screening assessment.
• If substance is low health hazard/low exposure, not a health priority, no further work required (not 64c “CEPA-toxic”).
Phase 2: Issue Identification for Health-Related Priorities
• For substances still prioritized once both simple and complex exposure and hazard tools applied, issue identification to highlight likely critical areas of focus based on input from relevant sources and parties

35ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
History of Development of ComET
• Work initiated in January/04• First discussion on conceptual aspects
between Lifeline and Health Canada – March/04
• Presentations to stakeholders – May/04– CEPA Industry Coordinating Group, other
industry groups and environmental interest groups
• Engagement of Trent University – June/04• Peer Input meeting – November/04

36ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Objectives of this Peer Input Meeting on ComET
• Increased understanding of how the “tool” will contribute not only to the CEPA program but for other Governments/industry
• Solicit input/information/comment on the architecture/data to populate for decision making on the program
• Encourage collaboration to avoid duplication and maximize use of resources to contribute to development of increasingly more refined models– more scenarios– increased complexity

37ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
Keep in Mind
• Development of this “tool” (ComET) is a work in progress– Default values provided principally as examples,
for illustration, currently– Not encompassing at this stage
• Continuing suggestions are welcome, but this is NOT peer review– Deadline will determine form of peer review
pre 2006• It is the “tool” (ComET) which is the focus of this
meeting, not the substances– Substances for illustrative purposes, only
• “Tool” currently a spreadsheet but form will change

38ComET Peer Input meeting,
Cincinnati, Nov. 8th/04
More Information?
• Health Canada Existing Substances Division Website – http://www.hc-sc.gc.ca/exsd-dse
• Health Canada Existing Substances Mailing List – http://www.hc-sc.gc.ca/hecs-sesc/exsd/listserv.htm
• CEPA Registry – (http:// www.ec.ca/CEPARegistry)