Combined Surgical Treatment of Thoracic Outlet

of 12
-
Upload
triptykhanna -
Category
Documents
-
view
44 -
download
0
description
treatment for thoracic outlet
Transcript of Combined Surgical Treatment of Thoracic Outlet
-
7/15/2019 Combined Surgical Treatment of Thoracic Outlet
1/12
Combined surgical treatment of thoracic outlet
syndrome: transaxillary first rib resection and
transcervical scalenectomy
Erdog an Atasoy, MDDepartment of Surgery, University of Louisville School of Medicine, Louisville, KY
Kleinert, Kutz and Associates Hand Care Center, PLLC, Suite 700, 225 Abraham Flexner Way,
Louisville, KY 40202, USA
Surgical procedures performed to relieve tho-
racic outlet syndrome (TOS) have changed
dramatically since 1861 when cervical rib resection
was introduced [1]. Table 1 describes the evolution
of these procedures.
Presently, transaxillary first rib resection and
transcervical anterior and middle scalenectomy
are the most popular and standard procedures forthe surgical treatment of TOS. First rib resection
is recommended for lower-level TOS (involving
the C8T1 roots). Scalenectomy usually is the
preferred treatment for upper-level TOS (involv-
ing the C5, C6, and C7 roots), or following
whiplash injury and recurrent TOS after a pre-
viously performed first rib resection. Markedly
obese and big or excessively muscular patients
also are considered candidates for scalenectomy,
because complete resection of the first rib can be
difficult and carries a higher risk for these
patients.
In the early 1980s, some surgeons believed that
combining these two procedures was the answer
to complete TOS relief. They performed the
scalenectomy first and then followed with a trans-
axillary first rib resection [2,3]. Since 1989 the
author has combined these two surgeries but has
performed the transaxillary first rib resection first
and then followed immediately with a transcervical
anterior and medial scalenectomy [4]. By perform-
ing these two procedures in this order the author
has accomplished total decompression of the
thoracic outlet area.
Following a complete first rib resection, the
anterior and middle scalenectomy can be per-
formed easily, because all of the distal insertions of
these muscles have been released from the first rib.
During anterior scalenectomy, the distal in-sertion of the anterior scalene muscle (which was
cut at the time of the first rib resection) and the
subclavian artery are clearly visible when the
intact sheath of the scalene muscle is exposed and
pierced with a scissor. The integrity of the artery is
protected easily. During middle scalenectomy the
previously divided distal end of the middle scalene
muscle and the long thoracic nerve can be exposed
easily once the sheath of the middle scalene muscle
is cut.
Nearly 80% of the anterior scalene muscle and
40%50% of the middle scalene muscle can be
removed during the scalenectomy while ensuring
the complete integrity of the phrenic and long
thoracic nerves. During the scalenectomy, the
surgeon can see the intact sheaths of both scalene
muscles and remaining muscle fibers of the
anterior scalene muscle (which may appear
attached to the subclavian artery). If these muscle
sheaths and fibers are left intact, they may cause
the scalene muscles to become attached to the bed
of the resected first rib. Therefore, they must be
cut during the scalenectomy to decrease the risk ofrecurrent symptoms.E-mail address: [email protected]
0749-0712/04/$ - see front matter 2004 Elsevier Inc. All rights reserved.
doi:10.1016/S0749-0712(03)00077-5
Hand Clin 20 (2004) 7182
mailto:[email protected]:[email protected]:[email protected] -
7/15/2019 Combined Surgical Treatment of Thoracic Outlet
2/12
The technique of transaxillary first rib resection
Although several approaches have been de-
scribed in the literature (ie, supraclavicular, ante-
rior, infraclavicular, and posterior), the author has
found the transaxillary approach to be the most
effective.
With the patient under general anesthesia,
a Foley catheter is inserted into the patients
bladder and the patient is positioned in the lateral
position. The patients chest is turned approxi-mately 4550 posteriorly. A towel-covered 4-
inch thick foam roll is placed under the opposite
axilla. One pillow is placed on the table under the
patients leg that is touching the table, and
another pillow is placed between the patients
semiflexed legs. A padded chest brace is applied to
the edge of the table to support the patients chest,
and a rolled 3- to 4-foot wide sheath is placed
between the patients back, buttock, and the chest
brace. A wide tape is applied on the hip to help
stabilize the patient, and an extra strap is placed
on the mid thigh for further support.Surgical preparation and draping are done on
the entire upper extremity, the shoulder, the axilla,
and the anterior and posterior chest walls on the
surgical side. Two-layer stockinet is applied over
the full length of the extremity up to the axilla.
This enables full mobility of the upper extremity,
which is important.
Under the instruction and direction of the
operating surgeon, the surgical assistant applies
intermittent controlled traction on the patients
arm. This is an important part of the surgerybecause controlled arm traction and proper
wound edge retraction enable the surgeon to see
the deep part of the operative field, the full length
of the first rib, and all vital structures. The
assistant places his forearm under the forearm of
the patient on the same side. He grips the patients
wrist with his opposite hand and then grips his
own wrist with his other hand (Fig. 1A). Roos [5]
described this as the wristlock holding technique.
This method enables the assistant to hold the
patients arm without putting any pressure on
the patients forearm nerves. It also decreases
the effort required by the surgical assistant andminimizes his discomfort. Mechanical arm hold-
ing devices are not satisfactory for this purpose,
because controlled, intermittent, precise arm
traction that allows for an instantaneous change
of direction and degree is important during the
surgery, and only a human assistant can achieve
this.
With the patients arm fully abducted by the
surgical assistant, a 5- to 6-in long smile-shaped
incision is marked slightly below the axillary
hairline where the axilla and chest wall meet. Thismarking is located near the level of the third rib
(Fig. 1B). The incision is performed along the
marked line, deepened through subcutaneous
tissue, and then continued through the axillary
fascia. During the incision, a few arterial and
venous branches from the lateral axillary vessels
and sometimes one or two smaller nerve branches
(branches of the third intercostobrachial cutane-
ous nerve) can be seen. If possible these vessels are
preserved, and during wound edge retraction they
help to protect the nerve branches. Retraction
of the skin flaps with small rake-like retractorsis helpful. After further deepening the dissec-
tion through the axillary fascia, which can be
Table 1
Evolution of thoracic outlet syndrome surgery
Name of operation
Year first
performed
Surgeon who
introduced it
Cervical rib resection 1861 Coote [1]
First rib resection 1908 Murphy [6]
Scalenotomy 1927 Adson and Coffey [7]
First rib resection - posterior approach 1961 Clagett [10]
First rib resection - supra and infra clavicular approach 1960s Various surgeons
First rib resection - transaxillary approach 1966 Roos [11]
Scalenectomy 1938 Adson
Refined scalenectomy 1979 Sanders [12]
Combined approach (transaxillary
first rib resection followed
immediately by transcervical
anterior and medial scalenectomy)
1989 Atasoy [4]
72 E. Atasoy/ Hand Clin 20 (2004) 7182
-
7/15/2019 Combined Surgical Treatment of Thoracic Outlet
3/12
distinctive in some patients, the axillary fat pad is
exposed. The axillary fatty tissue has a different
appearance than the subcutaneous fat. The
dissection is deepened directly down to the chest
wall until the areolar tissue on the chest cage
becomes visible. It is important to go straightdown to the chest wall without disturbing the
axillary lymph nodes that are present in the
axillary fat pad, otherwise the axillary fat pad
may be cut, the lymph nodes, and lymphatic
drainage may be disturbed, and the surgeon may
get lost in the operative field.
During this stage the longer ends of the
Richardson retractor are used to perform wound
retraction. The branches of the second and
sometimes the smaller third intercostobrachial
cutaneous nerves can be seen at the mid to lateralside of the operative field, and they should be
protected. These nerves innervate the posterior
portion of the axilla and medial posterior upper
arm skin.
When the ceiling of the axilla is reached, the
subclavian vein may become visible. The thin
membrane that covers the top of the first rib, the
subclavian vessels, and the lower trunk is pushed
gently upward with a sponge stick. This action
exposes the subclavian vein, the insertion of
the anterior scalene muscle to the first rib, the
subclavian artery, and the lower trunk of thebrachial plexus (see Fig. 1B). Using the curved or
sharp ends of the Overholt rib stripper (Fig. 1C)
to continue the anterior dissection, the subclavius
tendon and the costocoracoid ligament and their
insertions are exposed. The dissection continues
posteriorly to expose the middle scalene muscle
and its wide insertion to the first rib, and finally
the T1 root of the lower trunk posteriorly. If the
highest thoracic artery that is present in 30%
40% of cases is encountered, it is ligated, divided,
or cauterized, depending on its size.Sometimes the first two digitations of the
serratus anterior muscle to the first and second
rib are prominent and prevent good visualization
of the posterior part of the first rib. Dividing or
stripping these digitations from the first and
second ribs can resolve this problem.
Evaluating the tautness of the T1 and lower
trunk when the wide end of the long finger forceps
touches them can determine the tension caused by
the surgical assistant holding the patients arm in
traction. If the surgeon notices any excessive
tautness when touching the T1 and lower trunk,the assistant is asked to relax the arm. Intermit-
tent traction and relaxation prevents ischemic and
traction injury to the brachial plexus and gives the
surgical assistant a chance to rest his arms.
When the first rib is exposed anteriorly from
the costochondral junction posteriorly to its neck,
the important structures that are visible include the
costocoracoid ligament, subclavius tendon, sub-clavian vein, lower portion and insertion of the
anterior scalene muscle to the first rib, subclavian
artery, scalene minimus (if present), the T1 root
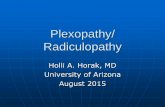
Fig. 1. Right transaxillary first rib resection. (A)
Marking of the incision and holding of the arm in the
wristlock position. (B ) (i) Location of skin incision. (ii)
Exposure of first rib, scalene muscles, subclavian artery
and vein. The dotted lines show the intended cut on thescalene muscles. (C) Complete assortment of instru-
ments used during a first rib resection. Overholt rib
strippers (elevators) are in top center of photograph, and
to their right are Cameron Haight strippers (elevators).
Rib cutters are in top left, Sauerbach first rib rongeurs
are in lower center, and large and small Richardson
retractors are in upper right. (D) Schematic axillary view
of right thoracic outlet anatomy with right arm fully
abducted. (E) Subperiosteal dissection of first rib with
a Cameron Haight elevator, and levering of first rib with
the handle of long finger pick-up. (F) Cutting of first rib
in the dissected area. (G ) Removal of the anterior por-
tion of the first rib. (H) Removal of the posterior
portion of the first rib. (I) View following a 90%95%
resection of the first rib.
73E. Atasoy/ Hand Clin 20 (2004) 7182
-
7/15/2019 Combined Surgical Treatment of Thoracic Outlet
4/12
Fig. 1 (continued)
74 E. Atasoy/ Hand Clin 20 (2004) 7182
-
7/15/2019 Combined Surgical Treatment of Thoracic Outlet
5/12
Fig. 1 (continued)
75E. Atasoy/ Hand Clin 20 (2004) 7182
-
7/15/2019 Combined Surgical Treatment of Thoracic Outlet
6/12
(which emerges from under the very back portion
of the first rib and extends and joins to the C8 to
form the lower trunk), and finally, the wide
insertion of the middle scalene muscle to the first
rib (Fig. 1D). If the scalenus minimus muscle is
present, which occurs in 30%50% of TOS cases[6,7], it usually inserts on the first rib between the
subclavian artery and T1 root of the lower trunk.
Generally the dissection and mobilization of
the first rib is performed from the anterior to
posterior direction. The most anterior structures,
the costocoracoid ligament and the subclavius
tendon insertion on the first rib, are divided either
by the sharp curved end of the Overholt stripper or
by a long-handled knife, using extreme caution
around the subclavian vein. Next the anterior
scalene muscle is dissected carefully from thesubclavian artery and vein using the blunt wide
end of a long finger forceps, the unopened tip of
a long dissection scissor, or even a fingertip, if the
area can be reached easily. The next step is to
divide the anterior scalene muscle, which can be
done either by gently passing a right-angle clamp
behind a portion of the muscle, pulling anteriorly,
and then making a few attempts to cut it near its
insertion or cutting it with a smaller bite with
a long scissor. The remaining few intact fibers are
close to the subclavian vein and artery and they
can be left alone and divided later during theremoval of the first rib. After dividing the anterior
scalene muscle, attention is focused on the middle
scalene muscle. Using the wide end of the long
finger forceps, the subclavian artery and T1 branch
of the plexus are pushed gently, achieving full
exposure of the portion of the middle scalene
muscle near its insertion to the first rib. The
middle scalene muscle insertion to the first rib is
cut either with a long scissor or by gently inserting
a right-angle clamp under a portion of the muscle
and gently pulling it off and tearing it from the firstrib. The remaining undivided, high-positioned
muscle fibers are pushed away from the first rib
with an Overholt or a long rib stripper.
If the scalenus minimus muscle and any
recognizable bands are present, they are cut at
their insertion to the first rib and a portion of
them is removed.
Next, the first rib is freed from the intercostal
muscles along the inferior border with the sharp,
flat-notched end of the Overholt rib stripper. The
middle part of the first rib is dissected approxi-
mately 2 inches along the posterior surface. Usingeither the flat end of the Overholt stripper or
preferably the wide flat end of the long finger
pick-up, the first rib is leveraged on the second rib.
Then, using the flat, thinner end of the Cameron
Haight rib elevator, subperiosteal dissection of the
first rib is performed (Fig. 1E). The curved end of
the Overholt stripper is used to continue the
periosteal stripping.Next, the curved end of the most suitable
Overholt stripper is passed gently under the
dissected portion of the first rib between the
periosteum and the first rib. To separate the first
rib from the soft tissue, the tip of the stripper is
pushed gently upward, carefully staying close to
the first rib at the concave border. When the tip of
the stripper is visible at the upper border of the
first rib, the area is scraped gently, both anteriorly
and posteriorly, to make enough room to pass the
rib cutter through the space. The wide end of thelong finger pick-up can be used to push the lower
plexus and subclavian artery gently upward.
Then, using a straight rib cutter, the first rib is
divided (Fig. 1F). The anterior portion of the rib
is grasped with a Kocher clamp, lifted up gently,
pulled outward and dissected from the posterior
periosteum. The few remaining fibers of the
anterior scalene muscle attached to the upper
border of the first rib are divided carefully.
Dissection of the anterior portion of the first rib
is continued at least 1 cm beyond the costochon-
dral junction. The subclavian vein is close to theupper edge of this portion of the rib and it should
be protected. The costochondral junction is
scored with an Overholt strippers longer, curved
end. Then an attempt is made to avulse the
anterior portion of the first rib at the costochon-
dral junction. If dissection has not been extended
beyond the costochondral junction, the avulsion
can tear the pleura, causing pneumothorax. If
avulsion does not occur, the anterior portion of
the first rib is cut and removed (Fig. 1G). Then
the sharp tips are rongeured up to the costochon-dral junction.
Next, using a Kocher clamp or a long finger
pick-up interchangeably, the posterior portion of
the first rib is lifted up, pulled outward, and dis-
sected from the posterior periosteum and from the
soft tissues along the upper and lower borders up
to the transverse process of T1 vertebra. Maximum
care should be given to avoid injury to the sub-
clavian vessels and the lower portion of the
brachial plexus, especially T1, which has a close
relationship with the posterior portion of the
first rib.This portion of the first rib is cut with Roos
right-angle rib cutter or a straight rub cutter as far
76 E. Atasoy/ Hand Clin 20 (2004) 7182
-
7/15/2019 Combined Surgical Treatment of Thoracic Outlet
7/12
back as possible (Fig. 1H). A large Sauerbruchs
first rib rongeur and then a smaller size of the
same rongeur are used to remove the remaining
posterior portion of the rib up to the transverse
process, if possible. If the transverse process of T1
cannot be reached because of the difficulty inperforming the dissection, no more than 1 cm of
the first rib can be left in this area.
After removing the first rib, the loose ends of
both scalene muscles are trimmed as high as safety
permits (Fig. 1I).
Occasionally arterial bleeding may occur in the
middle scalene muscle from the deep transverse
cervical artery (dorsal scapular artery) or from
one of its branches. Smaller bleeding can be
controlled easily by applying pressure with
a sponge stick or using a silver vascular clip.If the bleeding is excessive and not accessible
through the axilla, an immediate scalenectomy is
necessary. The bleeding can be located easily at
the middle scalenectomy site and controlled
quickly.
If major bleeding from the subclavian vein or
artery occurs during the first rib resection,
immediate action must be taken. Usually a tear
in the subclavian vein is small, and because of low
venous pressure, bleeding is not severe. Finger
pressure, suctioning the operative field, and
suturing the tear with an interrupted or a contin-uous 6-0 Prolene vessel suture can control such
bleeding. The size of the tear determines the
severity of subclavian artery bleeding. To control
bleeding in the subclavian artery, immediate
pressure must be applied and then the operative
field must be suctioned, vascular clamps applied,
and the tear must be stitched with 5-0 or 6-
0 Prolene vessel sutures. During TOS surgery the
rate of major vessel injury is 1% or less.
After meticulous hemostasis is achieved, the
wound is irrigated first with lactated Ringerssolution and then bacitracin solution (50,000 U in
1000 mL Ringers solution). Then a 1-in Penrose
drain is inserted through a small stab wound just
below the posterior end of the incision, and the
end of the drain is placed in the high point in the
axillary space just behind the T1 nerve. The drain
is sutured to the skin with 5-0 nylon. Then the
axillary fascia is closed with an interrupted
5-0 polyglactin suture. Skin closure is performed
in two layers: several interrupted 5-0 polyglactin
sutures are placed in the deep layer of the dermis
including a little bit of fatty tissue below thedermis, and 5-0 polyglactin continuous sutures are
placed in the dermis. Then steri-strips are applied
to the skin. The dressing should include a 4 4
pad on the incision, three to four open layers of
ABD pads on the drain site, and long taping.
Dressing changes should be performed at least
daily and sometimes twice a day. The drain
usually is removed in 48 hours.The pneumothorax incidence is less than 10%
in the authors cases; if pneumothorax occurs,
a small chest tube (size 28) can be inserted through
the fourth or fifth intercostal space at the mid-
axillary line and connected to pleura-vactype
drainage. If the pleural tear is large enough it can
be sutured and at least partially closed. The chest
tube usually is removed the next day.
If a cervical rib is present, is 2 in or longer, and
is not articulated with the first rib, resection of
only the cervical rib is usually sufficient and firstrib resection is not needed. If the cervical rib is
articulated with the first rib, usually the cervical
and first rib are removed; generally, the fusion site
is removed, then the cervical rib is removed,
followed by the first rib. A cervical rib less than
1 cm does not need to be resected as long as the soft
tissue attachments to the cervical rib are dissected
and removed. Then a full first rib resection is
performed.
If the first rib is wide or the fusion between the
first and second ribs is wide, it may not be possible
to cut this wide area completely with the bite ofthe straight rib cutter. In such cases a wedge
resection is performed first in the wide area. Once
the area is narrowed, complete cutting can be
performed easily with a straight rib cutter.
In a muscular person who also may have
hyperabduction syndrome (especially a male),
pectoralis minor division near the coracoid should
be performed as a supplement to first rib re-
section, either before or after first rib resection
(preferably before). Through the same incision,
the pectoralis minor is dissected from the pector-alis major, keeping its nerve supply intact and
divided just below the coracoid process by using
electrocautery.
The most common complaint after transaxil-
lary first rib resection is decreased sensation
associated with some paresthesias along the upper
medial and posterior aspect of the upper arm.
This usually is caused by traction placed on the
second and third intercostobrachial cutaneous
nerves during the surgery, and most of the time
it is temporary. Permanent injury to the brachial
plexus (usually T1 and C8) has been reportedrarely. Permanent major nerve injury occurs in
less than 0.5% of cases as a result of TOS surgery.
77E. Atasoy/ Hand Clin 20 (2004) 7182
-
7/15/2019 Combined Surgical Treatment of Thoracic Outlet
8/12
With long thoracic nerve injury, the patient
may have a mild to marked winging of the
scapula. If the winging of the scapula is severe
enough to disable the patients shoulder girdle
motions and does not show any improvement for
at least 1 year, then a scapulothoracic stabilizationprocedure is considered [8].
Sympathetic overactivity causing severe cold-
ness and Raynaud phenomenon-like symptoms
has been observed in some cases of TOS. In these
patients, a transaxillary first rib resection followed
with a transthoracic upper extremity sympathec-
tomy is most likely necessary (through the same
incision and third intercostal space). The T4, T3,
T2, and only the lower third of the stellate
ganglion are removed by clipping and cutting
their rami. For further details see Management ofPeripheral Nerve Problems, Second Edition, 1998,
Chapter Eighteen [9].
The technique of scalenectomy
With the patient under general anesthesia, the
chest and head are elevated approximately 40. A
long piece of 3- to 4-inch thick foam is placed
across and under the shoulders to moderately
hyperextend the neck, which is turned to the side
opposite the surgical area. One or two pillows areplaced under the knees to keep them moderately
flexed. Skin markings are made at the edges of the
suprasternal notch, the clavicle, the AC joint, and
the sternocleidomastoid and trapezium muscles.
The external jugular vein, cervical plexus, and
spinal accessory nerves also are marked (Fig. 2A).
The skin incision is nearly 8 cm long along
the skin crease and approximately 1.52 cm above
the clavicle, starting at the medial border of the
sternocleidomastoid muscle and extending to
the anterior border of the trapezius muscle. Theincision is made through the skin, subcutaneous
tissue, and platysma. First, the proximal skin flap,
which includes the skin, subcutaneous tissue, and
platysma, is developed from the sternocleidomas-
toid fascia, omohyoid fascia, and prescalene fat
tissue. The external jugular vein is preserved and
dissection is continued upward until the lower
branch of the cervical plexus is visualized or until
the dissection is close to it (at the middle of the
lateral border of the sternocleidomastoid muscle).
During the proximal dissection, the transverse
cervical branches of the cervical plexus thatextend over the sternocleidomastoid fascia that
are encountered are elevated with the flap and
preserved. Next the distal flap is mobilized on the
omohyoid and sternocleidomastoid fascia down
to its insertion to the clavicle. The distal flap
should include the skin, platysma, and the full
thickness fatty tissue under the platysma and over
the sternocleidomastoid muscle. Using this dis-section technique protects the supraclavicular
branches of the cervical plexus and helps them
remain in the fatty tissue of the distal flap.
Then the omohyoid muscle and fascia are
divided with a cutting Bovie and most of the
clavicular insertion of the sternocleidomastoid
muscle is divided along the top of the clavicle
for better exposure of the prescalene fat and
internal jugular vein (Fig. 2B).
The lateral border of the sternocleidomastoid
muscle is freed from the prescalene fat until theinternal jugular vein becomes visible. Next the
exposed prescalene fat is incised and mobilized
with a dissecting scissor along the internal jugular
vein, staying approximately 1 cm away from the
vein on the right side and nearly 1.5 cm away on
the left side, because the left side has more
lymphatic tissue than the right side. This part of
the dissection is a little more bloody than usual
because of the abundant vascularity of the
prescalene fat. All bleeding points are cauterized
as the surgery progresses. The superficial (trans-
verse) cervical artery and accompanying vein,which generally can be visualized at the lower part
of the wound, are ligated and divided (Fig. 2C).
During the prescalene fatty tissue mobilization,
the phrenic nerve can be visualized and protected.
It usually crosses the anterior scalene muscle from
the lateral to medial direction, starting at the C5
root of the brachial plexus. If the phrenic nerve is
located more medial than usual, the prescalene fat
pad is mobilized medially first to provide better
exposure of the phrenic nerve, the ascending
cervical artery, and the accompanying vein. Thenthe fat pad is mobilized laterally over the brachial
plexus until the lateral border of the middle
scalene muscle becomes visible. Next the phrenic
nerve (sometimes one or two accessory phrenic
nerves can be present) is mobilized gently, leaving
some fatty tissue and possibly the ascending
cervical artery along the nerve to maintain an
abundant blood supply to the nerve. The nerve is
retracted gently with a wide silastic vascular loop
by the assistant surgeon.
After adequate mobilization of the prescalene
fat pad, the full length of the anterior scalenemuscle and the lower end of the scalene sheath are
well exposed. If the first rib resection has been
78 E. Atasoy/ Hand Clin 20 (2004) 7182
-
7/15/2019 Combined Surgical Treatment of Thoracic Outlet
9/12
performed just before the scalenectomy, the
surgeon can see some bloody fluid inside the
sheath of the anterior scalene muscle at its lower
end. The fascia is opened carefully to expose the
freshly cut and proximally retracted end of the
anterior scalene muscle. The subclavian artery is
visibile under the previously divided anterior
scalene muscle. To get full exposure of the
subclavian artery, the remaining intact muscle
fibers are divided carefully. Some of the fibers may
seem to be attached to the subclavian artery. The
anterior scalene muscle is mobilized medially andlaterally along the ascending cervical artery and
brachial plexus respectively (C5C6 roots) and is
mobilized posteriorly upward on the fibro-fatty
tissue covering the C7 and C8 roots. Then it is
divided at the C5 level just below the phrenic
nerve takeoff and is removed. Sometimes it is
easier to first divide the anterior scalene muscle
proximally using traction on the muscle with
a heavy pick-up below the phrenic nerve takeoff
from the C5. Then with the combined proximally
and distally oriented dissection, the anterior
scalene muscle can be removed.
Next the posterior fibro-fatty sheath of the
anterior scalene muscle is dissected. While goingthrough this structure and removing a portion of
it, one can see (if present) the deep transverse
Fig. 2. Right scalenectomy. (A) Incision and superficial anatomy for a right scalenectomy. (B) Elevation of the skin flaps
and the exposure of the sternocleidomastoid muscle and prescalene fat. (C) Mobilization of the prescalene fat along the
internal jugular vein as a laterally based flap; ligation, division of the superficial cervical artery and exposure of the
phrenic nerve, and division of most of the clavicular head of the sternocleidomastoid muscle. (D) Exposure of the divided
lower end of the middle scalene muscle (which was divided during the previously performed first rib resection) and
exposure of the long thoracic nerve. (E) Suturing prescalene fat along the internal jugular vein and covering the brachial
plexus.
79E. Atasoy/ Hand Clin 20 (2004) 7182
-
7/15/2019 Combined Surgical Treatment of Thoracic Outlet
10/12
cervical artery (dorsal scapular artery) that lies
between the C6 and C7 and sometimes between
the C7 and C8. If this artery is in the way, it can
be divided and ligated to provide better exposure
of the C7, C8, and T1 roots. The scalenus
minimus, if present, usually lies near the C8 root,and it is removed. Following this, all branches of
the brachial plexus are dissected carefully, freed,
and exposed. Usually approximately 80% of the
anterior scalene muscle is removed.
If the scalenectomy is the only procedure to be
performed, the phrenic nerve is mobilized first, as
explained previously. Then the anterior scalene
muscle is divided slowly, carefully, and completelyat the middle part, keeping in mind that the sub-
clavian artery may pass through the muscle
Fig. 2 (continued)
80 E. Atasoy/ Hand Clin 20 (2004) 7182
-
7/15/2019 Combined Surgical Treatment of Thoracic Outlet
11/12
substance. Next the distal portion of the anterior
scalene muscle is dissected carefully from the
brachial plexus, which is just lateral and posterior,
the subclavian artery, which is deep and posterior,
and ascending cervical artery, which is medial. The
subclavian vein usually is not exposed; it isanterior to the muscle. The distal portion of the
anterior scalene muscle is removed at or near its
insertion to the first rib. Then the proximal portion
of the muscle is dissected and removed as
described previously.
Following the anterior scalenectomy, attention
is directed to the middle scalene muscle. First the
long thoracic nerve is exposed carefully and
preserved. Its usual location is at the lateral border
of the middle scalene muscle, and it exits this muscle
at the junction of the middle and lower third (Fig.2D). Sometimes an unusual location of the nerve is
observed; it may exit the muscle more anteriorly
through the substance of the lower part. On some
occasions more than one branch of the nerve is
observed, and these branches join further distally
beyond the exposed area. For this reason the sur-
geon must be careful during the dissection, before
and while dividing the middle scalene muscle.
If first rib resection has been performed just
before the scalenectomy, the intact middle scalene
muscle sheath is opened at its distal portion and
divided lower end of the middle scalene muscleexposed (see Fig. 2D), the remaining muscle fibers
are cut, and usually 40%50% of the muscle is
removed. During the dissection and removal of the
middle scalene muscle, again full attention should
be directed to the integrity of the long thoracic
nerve whose branches originate from C5, C6, and
C7, runthrough the middle scalene muscle, andjoin
together either inside or outside the muscle.
If the deep transverse cervical artery (dorsal
scapular artery) is present and is inthe way,it can be
re-ligated and divided in the middle scalene area forbetter exposure of the depth of the operative field.
At the deeper area of the middle scalene space, one
can see the tip of the previously inserted axillary
drain. If necessary, any remaining sharp end of the
first rib that can be palpated through the middle
scalene space can be exposed easily and removed
with a rongeur. If the first rib resection was not
done before the scalenectomy, after exposing and
protecting the long thoracic nerve, the middle
scalene muscle is divided carefully at or near its
insertion to the first rib, and at least the distal one
third to one half of it is removed.Following meticulous hemostasis, the wound
irrigation is performed first with a few hundred ml
of lactated Ringers solution and then bacitracin
solution (50,000 U in 1000 mL lactated Ringers
solution). Two small (0.25 in) drains are inserted
from the lateral corner of the incision, through the
prescalene fat pad, down to the middle and
anterior scalene spaces. The prescalene fat pad isapproximated with interrupted 5-0 polyglactin
910 (Vicryl) sutures by overlapping the medial
portion onto the lateral portion to give good fatty
tissue coverage to the brachial plexus (Fig. 2E).
Next the platysma and deep portion of the dermis
are approximated with interrupted 5-0 Vicryl
sutures and the skin is closed with running dermal
absorbable 5-0 Vicryl sutures. Then steri-strips are
placed on the skin and a mild compression
dressing is applied to the neck. Daily or twice
a day dressing changes can be performed, and thedrain sites can be cleaned with alcohol or
hydrogen peroxide solution. The neck drains are
removed in 24 hours, the axillary drain, which is
inserted right after the first rib resection, is
removed in 48 hours, and the patient is discharged
with postoperative instruction for wound care
and active neck and shoulder range-of-motion
exercises.
Complications following scalenectomy may
include neck hematoma, chylous drainage (mostly
from the left side), occasionally long-lasting
dyspnea (caused by phrenic nerve irritation ordisturbed blood supply to the nerve), and rarely
mild Horner syndrome. Hematoma may require
surgical intervention if it is extensive. Chylous
drainage may require repeated aspiration, and if it
persists, surgical exploration and ligation of the
lymph vessel may be necessary. Dyspnea and mild
Horner syndrome require observation, although
they usually improve spontaneously.
From late 1989 through the end of 2002, 532
surgeries were performed in the authors institu-
tion using the combined surgical procedure forTOS. The patients on whom these surgeries were
performed included 44 males and 396 females. The
most common age range was 2540 years and the
mean age was 38 years. The youngest patient was
10 years and the oldest was 63 years of age.
Results of combined surgical procedure for TOS
A simple grading system has been set up based
on the patients opinions of their percentage of
improvement following combined primary sur-
gery for TOS. The rate of symptom improvementafter combined primary surgery was graded
empirically (Table 2).
81E. Atasoy/ Hand Clin 20 (2004) 7182
-
7/15/2019 Combined Surgical Treatment of Thoracic Outlet
12/12
One hundred two patients returned a mailed
questionnaire regarding the outcome of their
surgery. Ninety-five percent of the patients re-
ported improvement of their symptoms after the
combined procedure. Only three patients who had
surgery using the combined procedure techniquedeveloped symptomatic recurrent symptoms.
These patients were operated on a second time.
One of these patients had good improvement after
the secondary surgery, another experienced a
30%50% improvement in symptoms, and the
third had an initial improvement and 6 months
later developed recurrent symptoms again.
Although the author has had only three
patients who have required secondary surgery
for recurrent symptoms, our overall no improve-
ment or recurrence rate after the combined
procedure is 5%10%. Several patients (approx-imately 40%50%) [4] were diagnosed with
associated peripheral nerve compression in the
involved extremity and had additional surgery for
their peripheral nerve compressions before or
after the combined procedure.
The authors complications with the combined
procedure are as follows: less than 10% had
pneumothorax, several patients had temporary
phrenic nerve palsy caused by surgical manipula-
tion and traction, and 1012 patients (approxi-
mately 2%) experienced neck seroma thatrequired aspiration only. No major vessel injuries
occurred, except a small tear (less than 0.5 in) in
the subclavian vein in two patients, which were
repaired without incident. In addition, no major
wound infections, neck hematomas, or chylous
drainages were observed.
References
[1] Coote H. Pressure on the axillary vessels and nerve
by an exostosis from cervical rib: interference with
the circulation of the arm, removal of the rib and
exostosis; recovery. Med Times Gazette 1861;2:108.
[2] Qvarfordt PG, Ehrenfeld WK, Stoney RJ. Supra-
clavicular radical scalenectomy and transaxillary
first rib resection for the thoracic outlet syndrome.
Am J Surg 1984;148:1116.
[3] Wiley E. Discussion in Roos D.B. The place for
scalenectomy and first rib resection in TOC.
Surgery 1982;92:1084.
[4] Atasoy E. Thoracic outlet compression syndrome.
Ortho Clin N Am 1996;27(2):265303.
[5] Roos DB. Experience with first rib resection for
thoracic outlet syndrome. Ann Surg 1971;173:
42942.
[6] Murphy T. Brachial neuritis caused by pressure of
first rib. Aus Med J 1910;15:5825.
[7] Adson AW, Coffey JR. Cervical rib: a method of
anterior approach for relief of symptoms by division
of the scalenus anticus. Ann Surg 1927;85:83957.
[8] Atasoy E, Majd M. Scapulothoracic stabilization
for winging of the scapula using strips of autoge-
nous fascia lata. J Bone Joint Surg [Br] 2000;82(6):8137.
[9] Atasoy E, Kleinert HE. Surgical sympathectomy
sympathetic blocksupper and lower extremity,
local plexus level. In: Omer GE, Van Beek AL,
editors. Management of peripheral nerve problems.
2nd edition. Philadelphia: WB Saunders; 1998.
p. 15771.
[10] Clagett OT. Presidential address: research and pro-
search. J Thorac Cardiovasc Surg 1962;44:15366.
[11] Roos DB. Transaxillary approach to first rib
resection to relieve thoracic outlet treatment. Ann
Surg 1966;163:354.
[12] Sanders RJ, Monsour JW, Gerber WF, et al.Scalenectomy versus first rib resection for treatment
of the thoracic outlet syndrome. Surgery 1979;
85:10921.
Table 2
Results of combined first rib resection and scalenectomy
Percent improvement Description No of patients
70%100% Excellent 36
50%70% Good 24
30%50% Better 26
10%30% Fair 9
Less than 10% Very poor 5
Results based on 102 respondents to a questionnaire,
out of 532 surgeries.
82 E. Atasoy/ Hand Clin 20 (2004) 7182