Combined approaches of skull base 360°
34
Combined approaches of skull base 360° 26-6-2016 6.55 pm
-
Upload
murali-chand-nallamothu -
Category
Education
-
view
4.117 -
download
4
Transcript of Combined approaches of skull base 360°

Combined approaches of skull base 360°
26-6-20166.55 pm

Great teachers – All this is their work . I am just the reader of their books .
Prof. Paolo castelnuovo
Prof. Aldo Stamm Prof. Mario Sanna
Prof. Magnan

For Other powerpoint presentatioins of “ Skull base 360° ”
I will update continuosly with date tag at the end as I am getting more & more information
click
www.skullbase360.in - you have to login to slideshare.net with Facebook account after clicking www.skullbase360.in

Anterior skull base is combined with Lateral skull base [ neurosurgical skull base or trans-temporal
skull base approaches ]

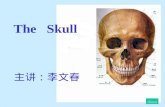
Anterior skull base & Neurosurgical skull base can be combined like in this ossifying fibroma video https://www.youtube.com/watch?v=3nr5f8Wbsk4 . See the microscope used by neurosurgeon & endoscope by the ENT
surgeon in the below photo at the same time . - case done by Dr .Satish jain [ https://www.facebook.com/satish.jain.75 ] [ http://www.jainenthospital.org/ ]

Case done by Dr .Satish jain [ https://www.facebook.com/satish.jain.75 ]
[ http://www.jainenthospital.org/ ]
Another case of ossifying fibroma without combined approach – going from nose to pterion – click https://www.youtube.com/watch?v=tp1vYADb5xc

JNA surgery by 4 corridors approach - by Dr. James K. Liu - I feel this 4 corridor is safest surgery for intracavernous & intracranial extension JNAs rather than removing only by nose. Orbitozygomatic transcavernous gives proximal & distal control of ICA . Endoscopic Caldwell-Luc ( Tranasmaxillary ) preserves Nose anatomy – see video https://www.youtube.com/watch?v=ekwOfEmHGWg&feature=youtu.be

JNA selection of approach discussion
https://www.facebook.com/groups/347913135290330/permalink/575333442548297
/

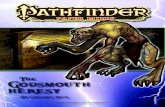
360-degree skull base surgery for giant pituitary adenoma. A. Coronal T1 with contrast MRI.B. Sagittal T1 with contrast MRI.

The patient is a 43-year-old female who presentedwith worsening vision changes. An MRI revealed a
giant pituitary tumor with severe suprasellar extensionand clival invasion (Figs 21–6A and 21–6B). Prolactin
levels were normal. Also, multiple flow voidsare noted surrounding the tumor and “pinching”the tumor margins. These are the anterior (ACAs)
and middle cerebral (MCAs) arteries. This case illustratesthe importance of having a knowledge and
understanding of ALL skull base surgical options.This tumor should be examined with a 360-degree
approach. An endonasal approach should be used for the clival and sellar portions and
could likelyeven decompress the midportion of the suprasellarportion for optic chiasm decompression. Howeveran anterior-lateral (orbito-zygomatic-craniotomy)
approach would be best for clearance of the tumoraway from the ACAs and MCAs and the intraventricular
portion of the tumor. Endoscopic assistancevia the craniotomy could be used in conjunction
with the microscope to get angled views.

Pterional & anterior skull base are combined .

Prof . Mario sanna says combined approaches in lateral skull base into two
1. Retrolabyrinthine Subtemporal Transapical [ = transpetrous ] and Retrolabyrinthine transtentorial approaches
2. Combined Transpetrous approaches + FTOZ

Retrolabyrinthine Subtemporal Transapical [ = transpetrous ] and Retrolabyrinthine transtentorial approaches

1. Retrolabyrinthine Transpetrous ( = Transapical )Subtemporal Approach
2. Retrolabyrinthine Transpetrous ( = Transapical )Subtemporal Transtentorial Approach
Retrolabyrinthine Subtemporal Transapical Approach
Retrolabyrinthine Subtemporal Transtentorial Approach

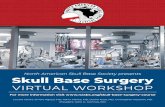
Retrolabyrinthine Subtemporal Transapical (Transpetrous Apex) Approach
Schematic drawing showing the incision to be performed.
A retrolabyrinthine approach is performed.

The dura of the middle fossa is detached from the superior surface of the temporal bone from posterior to anterior.
With further detachment of the dura, the middle meningeal (MMA) artery is clearly identified.

The middle meningeal artery (MMA) and the three branches(V1, V2, V3) of the trigeminal nerve are identified.
View after cutting the middle meningeal artery (MMA) andthe mandibular branch of the trigeminal nerve (V).

The internal auditory canal (IAC) is identified.
A large diamond burr is used to drill the petrous apex.

The petrous apex has been drilled. The internal carotid artery(ICA) is identified.
At higher magnification, the abducent nerve (VI) is identifiedat the level of the tip of the petrous apex (PA).

Panoramic view showing the structures after opening of theposterior fossa dura.
At higher magnification, the anterior inferior cerebellar artery (AICA)is seen stemming from the basilar artery (BA) at the prepontine cistern. The artery is crossed by the abducent nerve (VI). Note the good control of the prepontine cistern through this approach.

Tilting the microscope downward, the lower cranial nervesare well seen.

Retrolabyrinthine Subtemporal Transtentorial Approach
The retrolabyrinthine craniotomy has been performed. The petrous apex has been partially drilled.
The middle fossa dura (*) is incised.

The tentorium (*) is cut, taking care not to injure thetrochlear nerve.
The tentorium is further cut until the tentorial notch isreached. With retraction of the temporal lobe the optic (II), oculomotor(III) and contralateral oculomotor (IIIc) nerves are seen.

Branches of the trigeminal nerve (V1, V2, V3) at the level ofthe lateral wall of the cavernous sinus.

A view of the cerebellopontine angle through the retrolabyrinthine approach Note the narrow field and limited control.
Posterior fossa dura (PFD) structures exposed through the standard retrolabyrinthine approach.
A view of the posterior fossa dura through the combined retrolabyrinthine subtemporal transapical approach.

The middle fossa dura has been cut. The oculomotor nerve (III) is clearly seen.
With more retraction of the temporal lobe and the tentorium(*), the optic nerve (II) is seen.

Combined Transpetrous approaches + FTOZ
1. Transpetrous approaches – to prevent brain retraction & get control of posterior fossa
2. FTOZ – to get control of middle cranial fossa

Advantages of the Combined Transpetrous + FTOZ approaches
1. Complete and single-stage removal of large tumors extending to both the posterior and middle fossae. The FTOZ approach offers excellent control of the middle and infratemporal fossa components but has poor control of the posterior fossa. On the other hand, the transpetrous approaches afford excellent exposure of the posterior fossa with minimal middle fossa control. The combination of both approaches provides excellent visibility of both fossae, particularly at the area of Meckel’s cave where the tumor components usually interconnect.
2. The extensive bone removal allows maximal exposure while minimizing the amount of brain retraction needed.

Upper incision for FTOZ , lower incision for transpetrous approaches

Transpetrous approaches are – for better understanding click PPT http://www.slideshare.net/muralichandnallamothu/petrous-apex-360-48222034
1. Retrolabyrinthine Transpetrous ( = Transapical ) &2. Translabyrinthine Transpetrous ( = Transapical ) &
3. Transcochlear Transpetrous ( = Transapical )

Combined Transpetrous approaches + FTOZ
1. Retrolabyrinthine Transpetrous ( = Transapical ) + FTOZ
2. Translabyrinthine Transpetrous ( = Transapical ) + FTOZ &
3. Transcochlear Transpetrous ( = Transapical ) + FTOZ
4. Infratemporal fossa approach type B + Transzygomatic

Neurosurgeons are doing FTOZ + kawase approach to get control of middle cranial fossa & posterior cranial
fossa respectively
For FTOZ + Kawase approach click 1. https://www.youtube.com/watch?v=qgItZDwRYjk 2. https://www.youtube.com/watch?v=M89uijtuzQA3. https://www.youtube.com/watch?v=es-U3QitxdY4. https://www.youtube.com/watch?v=vDGO4kVy0Gc5. http://www.aiimsnets.org/skull_base_tumors.asp6. http://aiimsnets.org/AnteriorTranspetrosalapproach.asp#
others https://www.youtube.com/results?search_query=frontotemporal+orbitozygomatic+approach
https://www.youtube.com/results?search_query=kawase+approach

FTOZ + kawase approch cadaver albums
• https://www.facebook.com/groups/383508355070291/permalink/896897763731345/
• https://www.facebook.com/groups/383508355070291/permalink/897122833708838/

For Other powerpoint presentatioins of “ Skull base 360° ”
I will update continuosly with date tag at the end as I am getting more & more information
click
www.skullbase360.in - you have to login to slideshare.net with Facebook account after clicking www.skullbase360.in