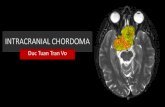

Colors / styles to use in ppt - ALATRO - Asociación Ibero ... · (Ocular, Pediatrics, Base of...
84
Protect, Enhance and Save Lives The Best in Proton Therapy, Today and Tomorrow Protones/Fotones Dra. Berta Roth
Transcript of Colors / styles to use in ppt - ALATRO - Asociación Ibero ... · (Ocular, Pediatrics, Base of...

Protect, E
nhance and Save Lives
The Best in P
roton Therapy, Today and Tomorrow
Protones/Fotones
Dra. Berta Roth
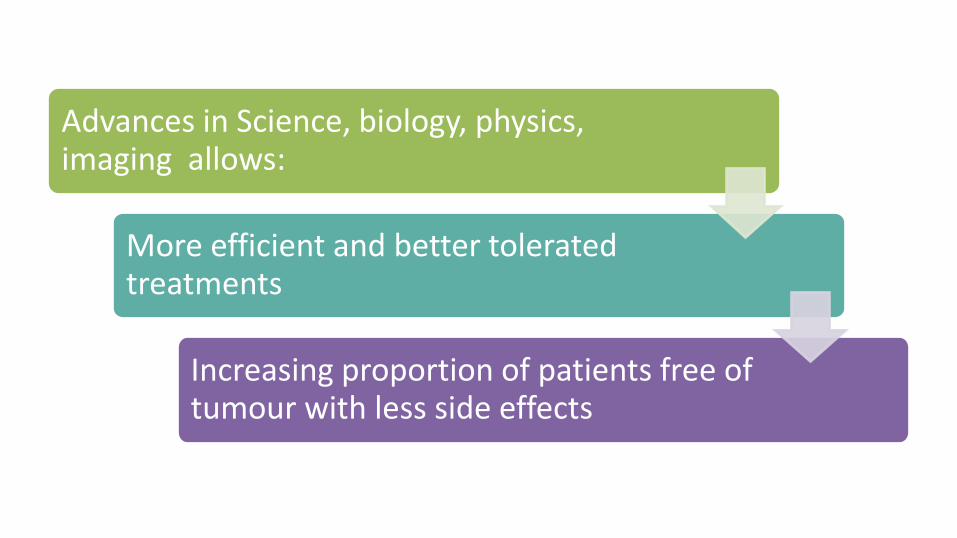
Advances in Science, biology, physics, imaging allows:
More efficient and better tolerated treatments
Increasing proportion of patients free of tumour with less side effects

Radiotherapy in 2016
Precision
Individualization
Organ Preservation
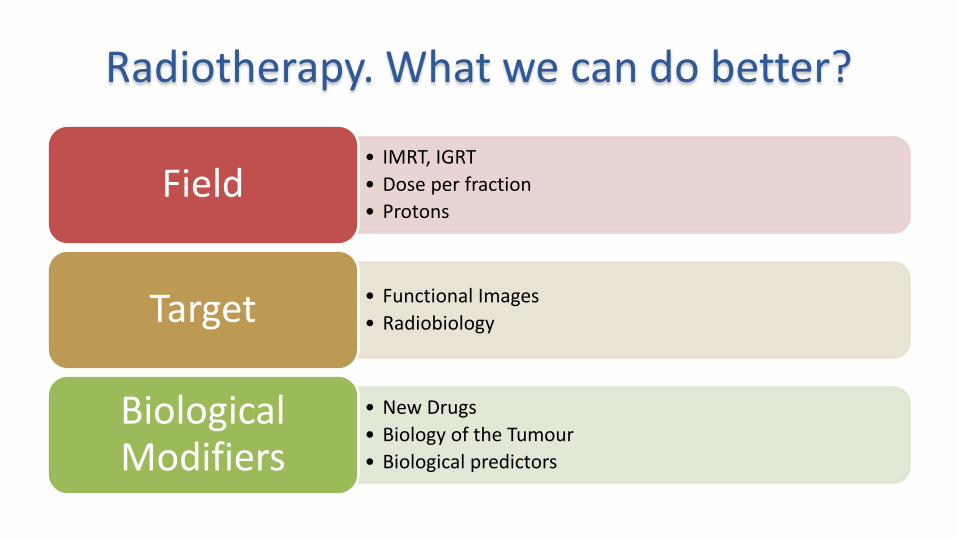
Radiotherapy. What we can do better?
• IMRT, IGRT • Dose per fraction • Protons
Field
• Functional Images • Radiobiology Target
• New Drugs • Biology of the Tumour • Biological predictors
Biological Modifiers

cost / sophistication
precision
2D RT
IMRT (XR Intensity modulation)
IGRT Image guided
3D RT, conformal
stereotactic radiotherapy
cyberknife
tomotherapy
Carbon ions
protons
photons « hadrons »
>80% radiotherapy
Optimal Therapeutic Ratio: cure/toxicity
Precision !!!
To adapt the machine to the patient
and not the patient to the machine
Individualized versus “one fits all” !!!!
IGRT / IMRT / SBRT / SRS/ PROTON.........
Why heavier hadron beams? • Precision therapy conformed to tumor • Sparing of normal tissues • Increased DNA damage in tumor • Increased effect on hypoxic tumors • Less repair of sublethal anf potentially lethal damage in cell
cycle • Short overall treatment course • Use of radioactive beam component for treatment
verification
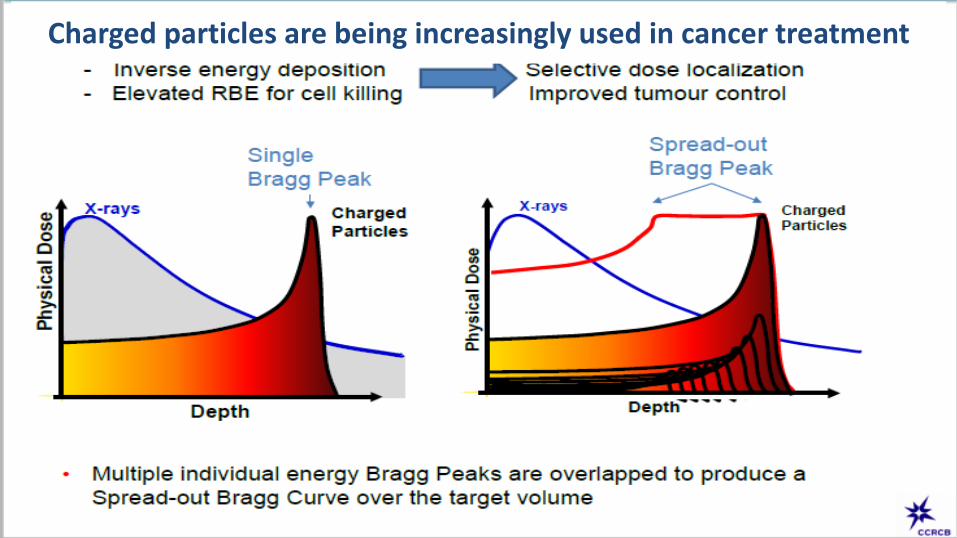
Charged particles are being increasingly used in cancer treatment

Highest Dose is near the point of beam entry.
Tumor Dose is less than the entry dose.
Dose is also delivered beyond the tumor target. Photons
(X-Rays)
Protons

Protect, E
nhance and Save Lives
The Best in P
roton Therapy, Today and Tomorrow
Ballistic advantages No radiation beyond the Bragg Peak tumor;
Homogeneous dose along the defined modulation
Distal & Proximal Conformality to tumor shape
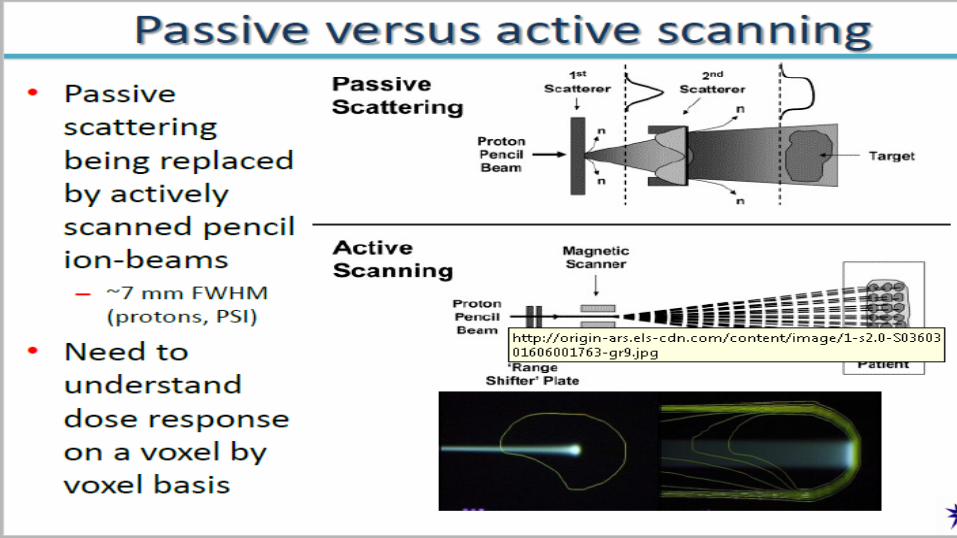
(PBS)
Example: Single Field Uniform Dose using in Pencil Beam Scanning
11
Why Proton Therapy? The dose deposition / Bragg peak

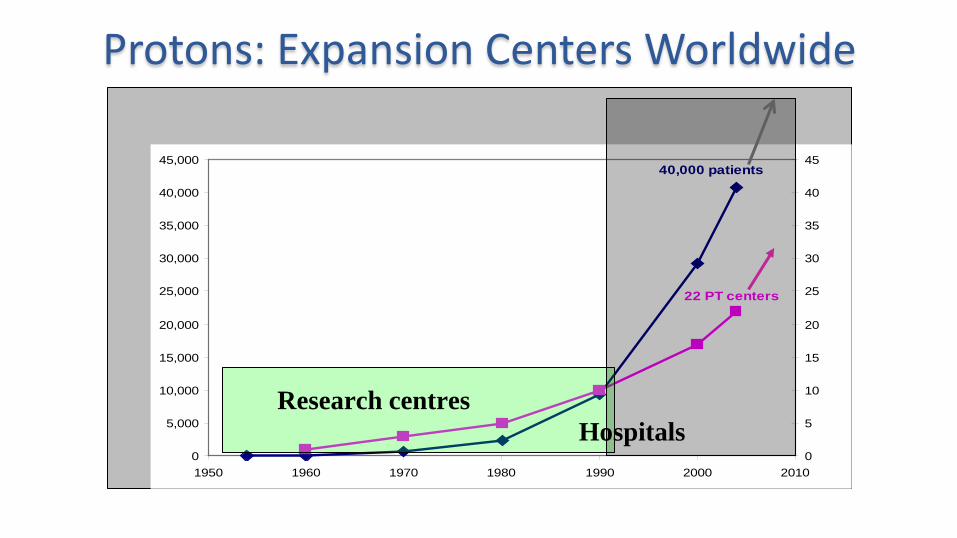
42 centres with protons (USA 14, Europe 12, Japan 8, …..) 6 centres with carbon ions (Japan 3, Europe 2, China 1) 3 dual centres (p+ C-12) 27 new centres planned 107,792 treated patients (93,452 with p+, 10753 with C-12) + 46,000 in the past 5 years ( ≈ 10,000 patients per year )
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
45,000
1950 1960 1970 1980 1990 2000 20100
5
10
15
20
25
30
35
40
4540,000 patients
22 PT centers
Research centres Hospitals
Protons: Expansion Centers Worldwide
Protect, E
nhance and Save Lives
The Best in P
roton Therapy, Today and Tomorrow
15
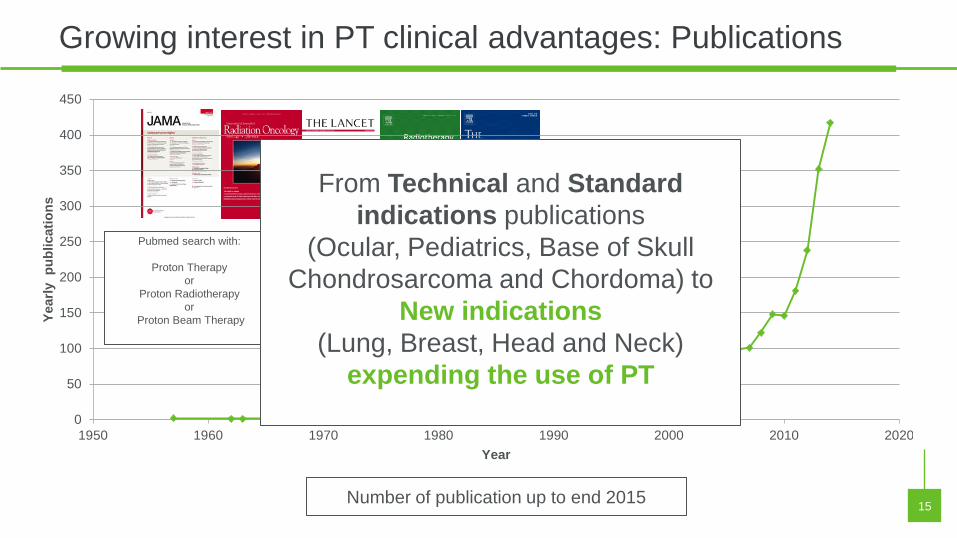
Growing interest in PT clinical advantages: Publications
Number of publication up to end 2015
…
0
50
100
150
200
250
300
350
400
450
1950 1960 1970 1980 1990 2000 2010 2020
Year
ly p
ublic
atio
ns
Year
Pubmed search with:
Proton Therapy or
Proton Radiotherapy or
Proton Beam Therapy
From Technical and Standard indications publications
(Ocular, Pediatrics, Base of Skull Chondrosarcoma and Chordoma) to
New indications (Lung, Breast, Head and Neck)
expending the use of PT

Protect, E
nhance and Save Lives
The Best in P
roton Therapy, Today and Tomorrow
PT Advantages: From Beam properties to Clinical benefits
16
Tumor control Toxicity PR
OBA
BILI
TY
DOSE OF RADIATION
Photons Protons Widening of the
Therapeutic Ratio

Protect, E
nhance and Save Lives
The Best in P
roton Therapy, Today and Tomorrow
PT Advantages: From Beam properties to Clinical benefits
17
0
10
20
30
40
50
60
70
80
90
100
Current standard (IMRTphotons)
Protons
Prob
abilit
y (%
)
Complications Local tumour control
Improvement of local
tumor control Prevention of complications
Photons
Protons
Courtesy of Prof Lagendijk
Pro
babi
lity
Improve Local Control Reduce Normal
Tissues Complications Decrease
integral dose (secondary cancer) PT is the
treatment of choice for retreatment
Tumor control Toxicity


Protect, E
nhance and Save Lives
The Best in P
roton Therapy, Today and Tomorrow
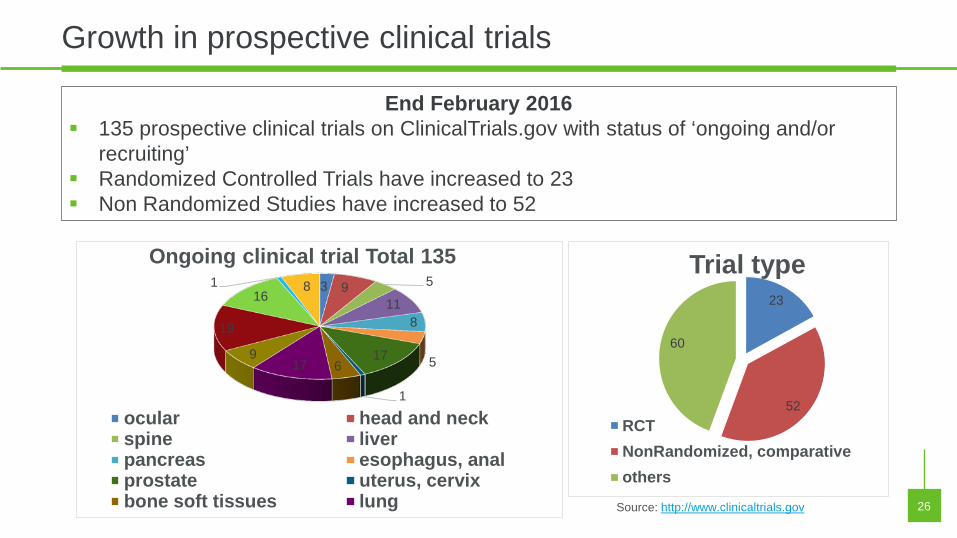
23
52
60
Trial type
RCTNonRandomized, comparativeothers
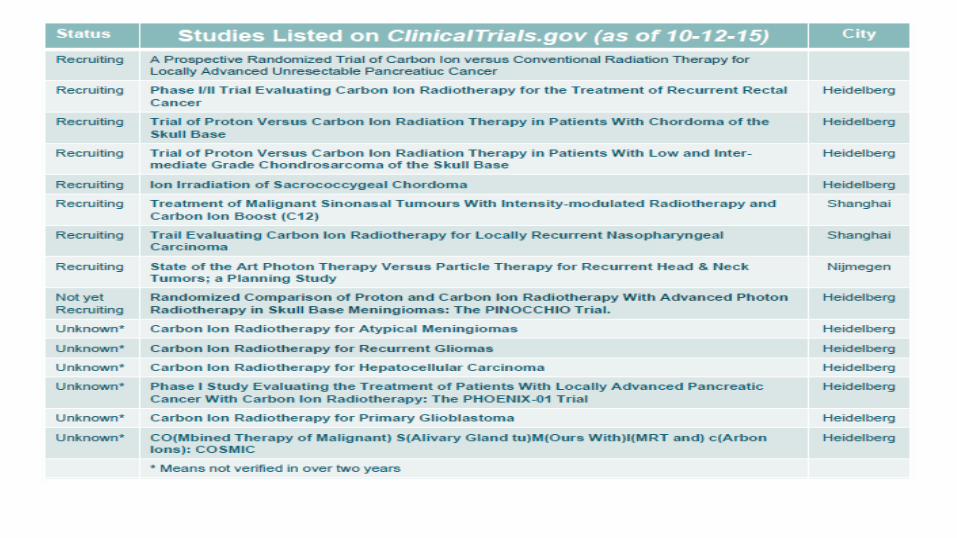
26 Source: http://www.clinicaltrials.gov
End February 2016 135 prospective clinical trials on ClinicalTrials.gov with status of ‘ongoing and/or
recruiting’ Randomized Controlled Trials have increased to 23 Non Randomized Studies have increased to 52
3 9 5
11 8
5 17
1
6 17 9
19
16 1 8
Ongoing clinical trial Total 135
ocular head and neckspine liverpancreas esophagus, analprostate uterus, cervixbone soft tissues lung
Growth in prospective clinical trials

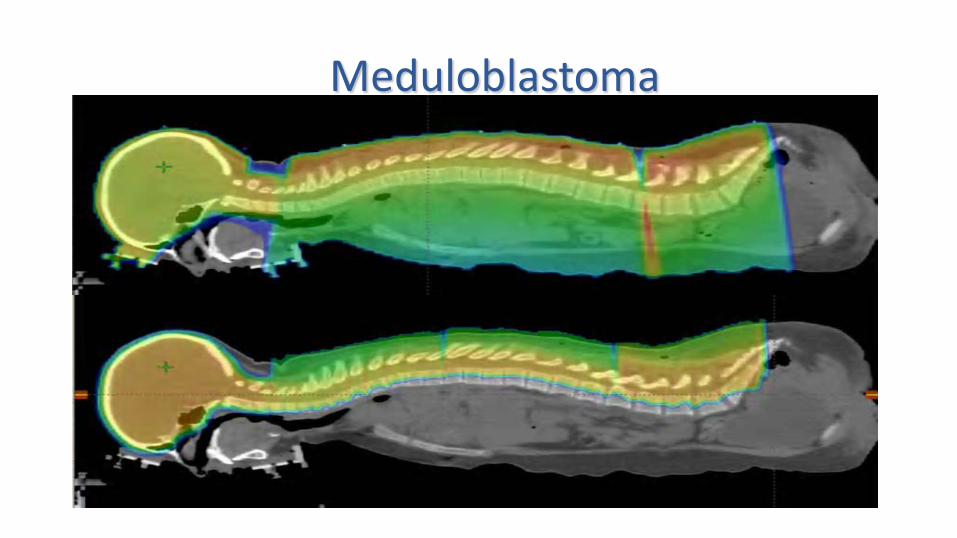
Meduloblastoma
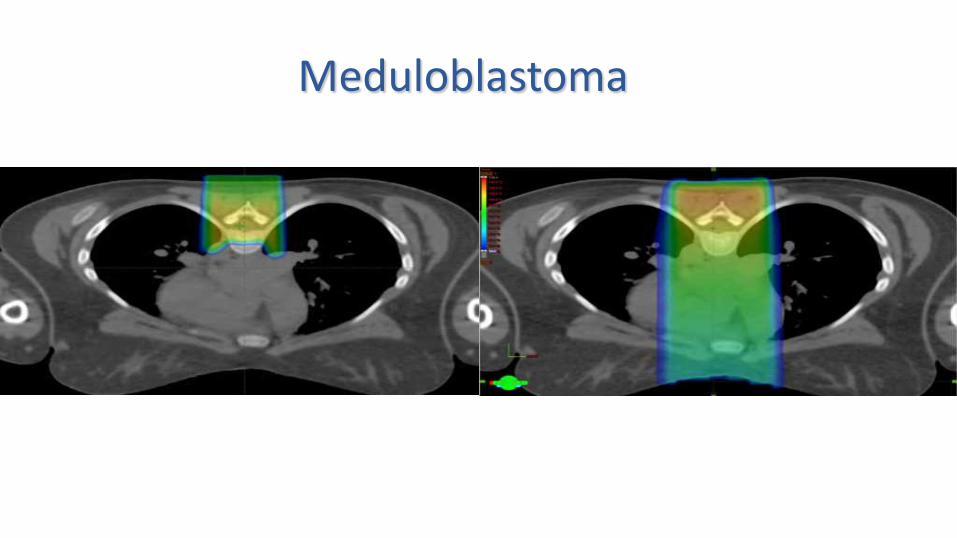
Meduloblastoma
Protect, E
nhance and Save Lives
The Best in P
roton Therapy, Today and Tomorrow
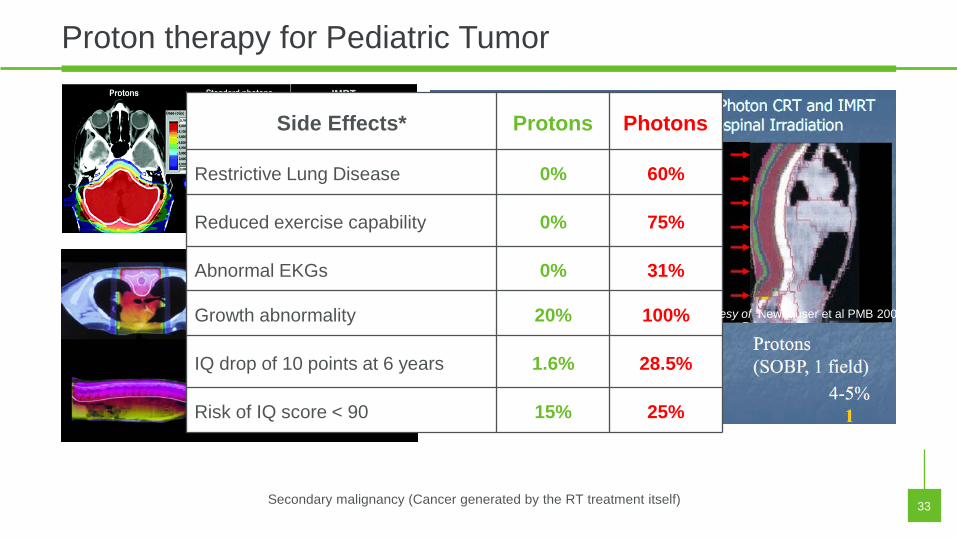
Proton therapy for Pediatric Tumor
33
Side Effects* Protons Photons
Restrictive Lung Disease 0% 60%
Reduced exercise capability 0% 75%
Abnormal EKGs 0% 31%
Growth abnormality 20% 100%
IQ drop of 10 points at 6 years 1.6% 28.5%
Risk of IQ score < 90 15% 25%
Courtesy of Newhauser et al PMB 2009
Secondary malignancy (Cancer generated by the RT treatment itself)
Decreased risk of 2nd cancer with protons
• 503 proton patients, 1974-2001 • Matched with 1,591 photon pts, by site, year, pathology • Mean F-Up 7.7 vs 6.1 y. • Risk : 6.4% (protons) vs 12.8% (photons) adjusted: 2.73 (p < .0001)
Chung CS et al, ASTRO, 2008, abstr 17


Protect, E
nhance and Save Lives
The Best in P
roton Therapy, Today and Tomorrow
Proton Therapy for Head and Neck
44
Protect, E
nhance and Save Lives
The Best in P
roton Therapy, Today and Tomorrow
Vol
ume
(%)
Vol
ume
(%)
Dose (Gy) Dose (Gy)
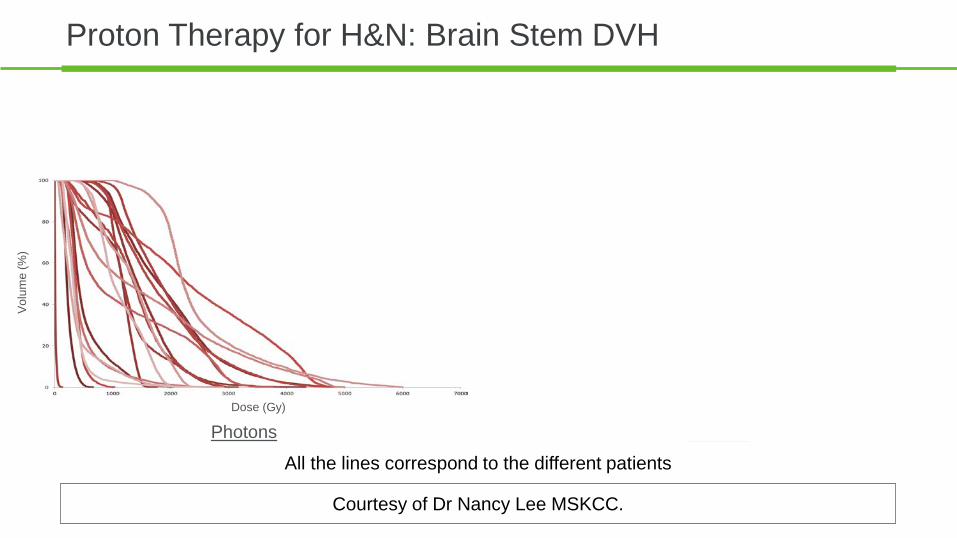
Proton Therapy for H&N: Brain Stem DVH
Courtesy of Dr Nancy Lee MSKCC.
All the lines correspond to the different patients
Photons Protons

Protect, E
nhance and Save Lives
The Best in P
roton Therapy, Today and Tomorrow
Vol
ume
(%)
Vol
ume
(%)
Dose (Gy) Dose (Gy)
Proton Therapy for H&N: Spinal Cord DVH
Courtesy of Dr Nancy Lee MSKCC.
All the lines correspond to the different patients
Photons Protons

Protect, E
nhance and Save Lives
The Best in P
roton Therapy, Today and Tomorrow
Photons Protons
Vol
ume
(%)
Vol
ume
(%)
Dose (Gy) Dose (Gy)
Proton Therapy for H&N: Oral Cavity DVH
Courtesy of Dr Nancy Lee MSKCC.
All the lines correspond to the different patients
Protect, E
nhance and Save Lives
The Best in P
roton Therapy, Today and Tomorrow
Photons Protons
Vol
ume
(%)
Vol
ume
(%)
Dose (Gy) Dose (Gy)
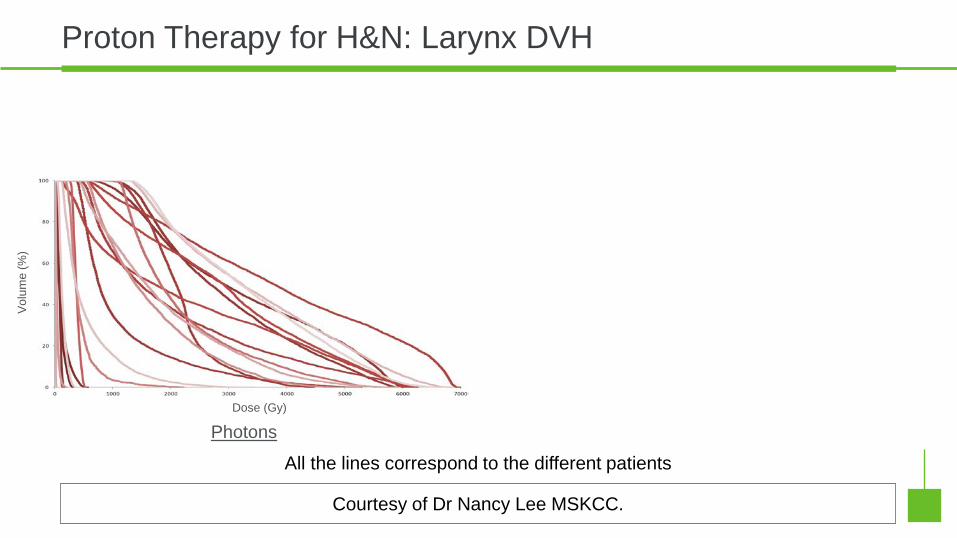
Proton Therapy for H&N: Larynx DVH
Courtesy of Dr Nancy Lee MSKCC.
All the lines correspond to the different patients
Protect, E
nhance and Save Lives
The Best in P
roton Therapy, Today and Tomorrow
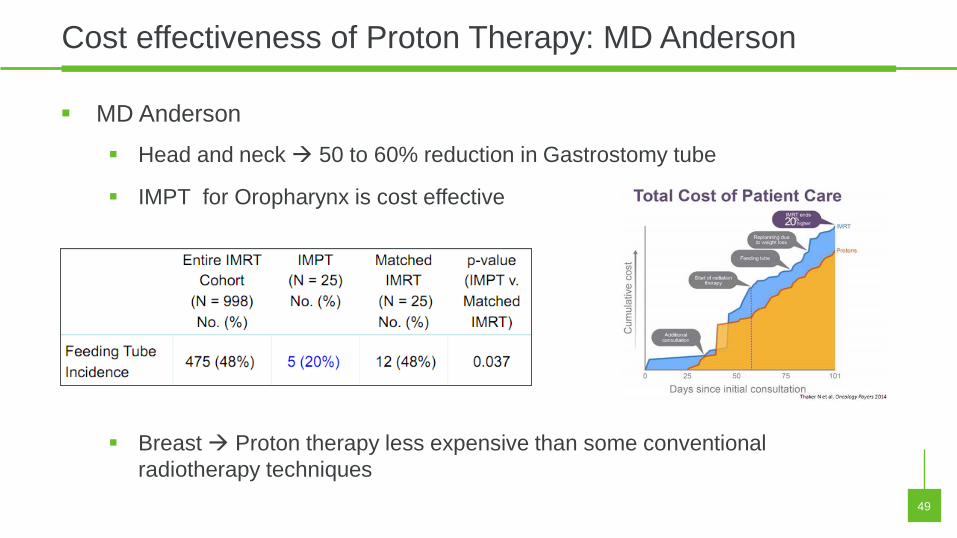
Cost effectiveness of Proton Therapy: MD Anderson
49
MD Anderson
Head and neck 50 to 60% reduction in Gastrostomy tube
IMPT for Oropharynx is cost effective
Breast Proton therapy less expensive than some conventional radiotherapy techniques
Protect, E
nhance and Save Lives
The Best in P
roton Therapy, Today and Tomorrow
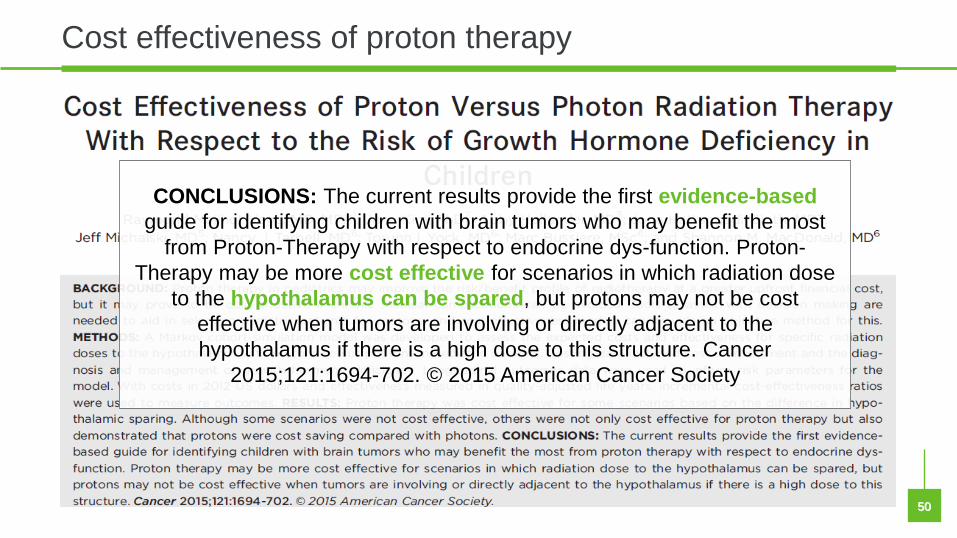
Cost effectiveness of proton therapy
50 50
CONCLUSIONS: The current results provide the first evidence-based guide for identifying children with brain tumors who may benefit the most
from Proton-Therapy with respect to endocrine dys-function. Proton-Therapy may be more cost effective for scenarios in which radiation dose
to the hypothalamus can be spared, but protons may not be cost effective when tumors are involving or directly adjacent to the hypothalamus if there is a high dose to this structure. Cancer
2015;121:1694-702. © 2015 American Cancer Society
Protect, E
nhance and Save Lives
The Best in P
roton Therapy, Today and Tomorrow
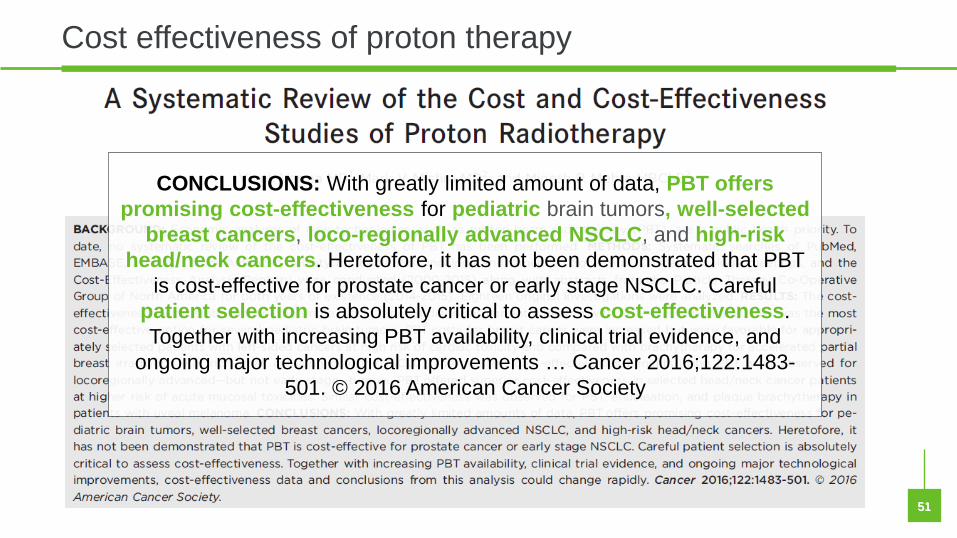
Cost effectiveness of proton therapy
51 51
CONCLUSIONS: With greatly limited amount of data, PBT offers promising cost-effectiveness for pediatric brain tumors, well-selected
breast cancers, loco-regionally advanced NSCLC, and high-risk head/neck cancers. Heretofore, it has not been demonstrated that PBT
is cost-effective for prostate cancer or early stage NSCLC. Careful patient selection is absolutely critical to assess cost-effectiveness. Together with increasing PBT availability, clinical trial evidence, and
ongoing major technological improvements … Cancer 2016;122:1483-501. © 2016 American Cancer Society

RACIONAL DE LOS PROTONES EN CÁNCER DE MAMA
• EL CANCER DE MAMA ES UNA ENFERMEDAD ALTAMENTE CURABLE Y POR LO CUAL LAS PACIENTES SON LARGAS SOBREVIVIENTES POR LO QUE PUEDEN EXPERIMENTAR MAS TOXICIDADES TARDIAS.
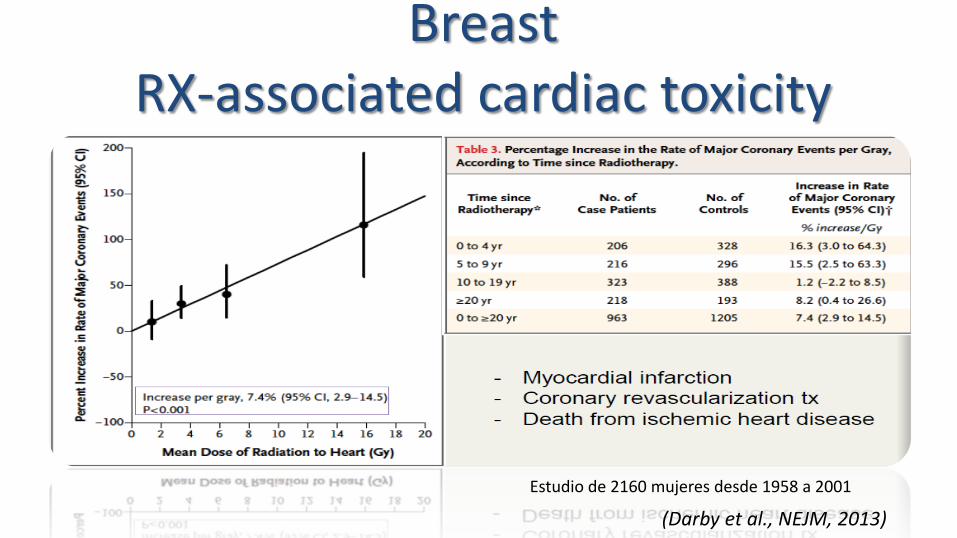
Breast RX-associated cardiac toxicity
(Darby et al., NEJM, 2013) Estudio de 2160 mujeres desde 1958 a 2001

ANATOMIA: ARTERIAS CORONARIAS (Nilsson, JCO, 2011)
1+2+3 = Right CA 5+6 = Left main 7+8+9+10 = Left Anterior descending
Lt Tangential fields = Lt breast/chest Wall
( Rt Int Mam = Rt breast = Electrons++)

SPARING HIGH DOSE RT • For tangent
field to cover IMN left, LAD & portion RV & LV would receive full dose.
• For a tangent field to cover IMN right, RCA would receive
Protect, E
nhance and Save Lives
The Best in P
roton Therapy, Today and Tomorrow
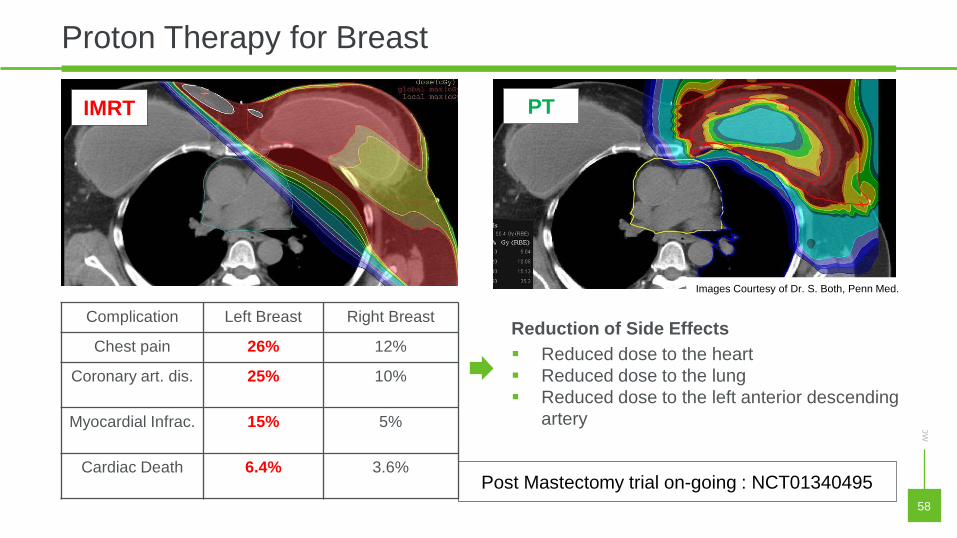
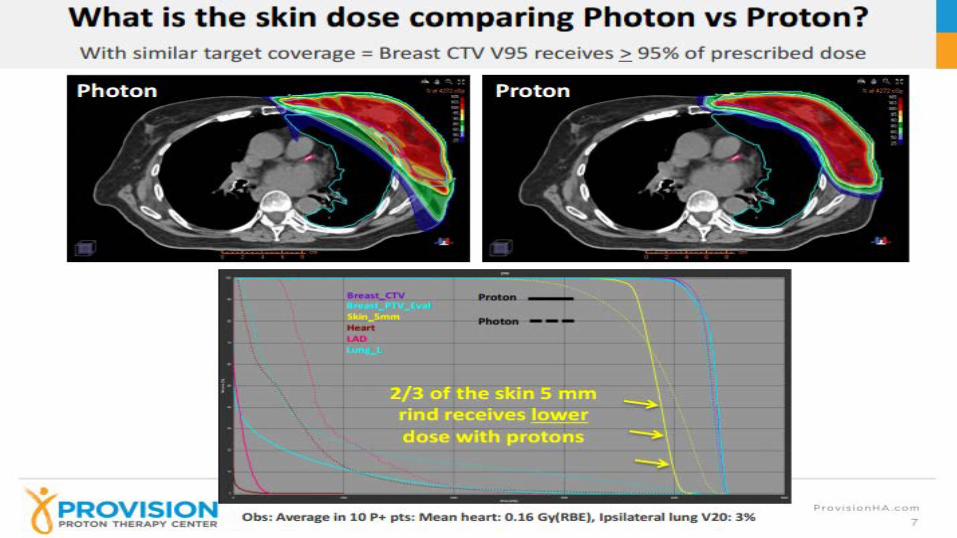
Proton Therapy for Breast
58
58
IMRT PT
Reduction of Side Effects Reduced dose to the heart Reduced dose to the lung Reduced dose to the left anterior descending
artery
Images Courtesy of Dr. S. Both, Penn Med.
Post Mastectomy trial on-going : NCT01340495
Complication Left Breast Right Breast
Chest pain 26% 12%
Coronary art. dis. 25% 10%
Myocardial Infrac. 15% 5%
Cardiac Death 6.4% 3.6%

• Protons allow for an external beam plan with non- target breast tisuue sparing more comparable to brachytherapy
• Modest reduction lung and heart (most patients)
El-Ghamry IJROBP 2002
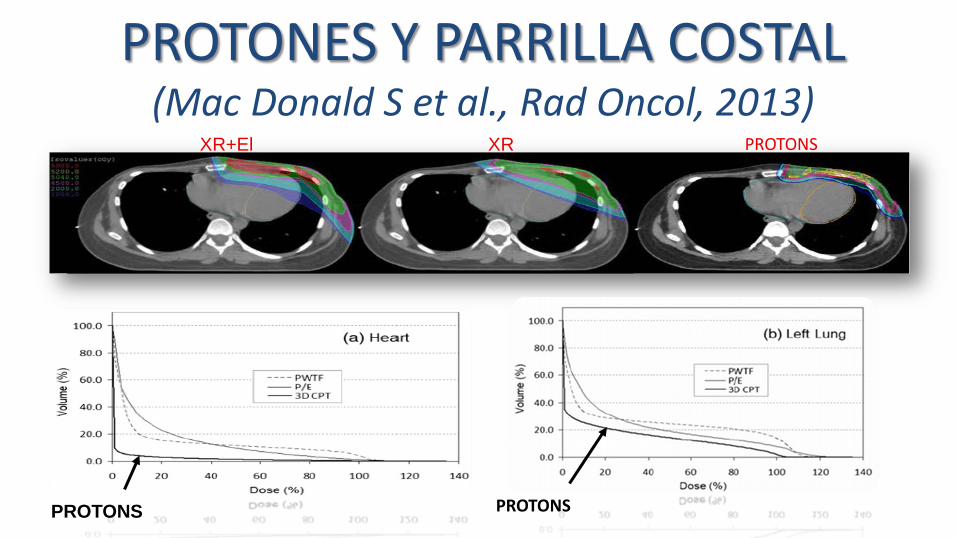
PROTONES Y PARRILLA COSTAL (Mac Donald S et al., Rad Oncol, 2013)
PROTONS PROTONS
PROTONS XR+El XR
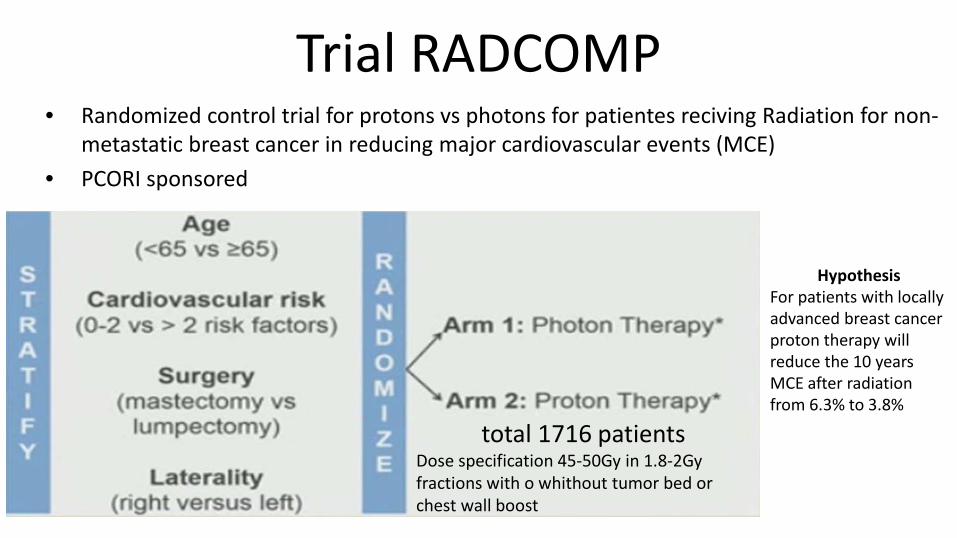
Trial RADCOMP • Randomized control trial for protons vs photons for patientes reciving Radiation for non-
metastatic breast cancer in reducing major cardiovascular events (MCE) • PCORI sponsored
total 1716 patients Dose specification 45-50Gy in 1.8-2Gy fractions with o whithout tumor bed or chest wall boost
Hypothesis For patients with locally advanced breast cancer proton therapy will reduce the 10 years MCE after radiation from 6.3% to 3.8%

Pancreatic Cancer Facts...
• 43,140 Annual Cases – Perhaps 50% present with localized disease
• Perhaps 50% of these are “resectable” or “curable”
–And yet the “cure” rate is only about 20% for these “curable” patients.
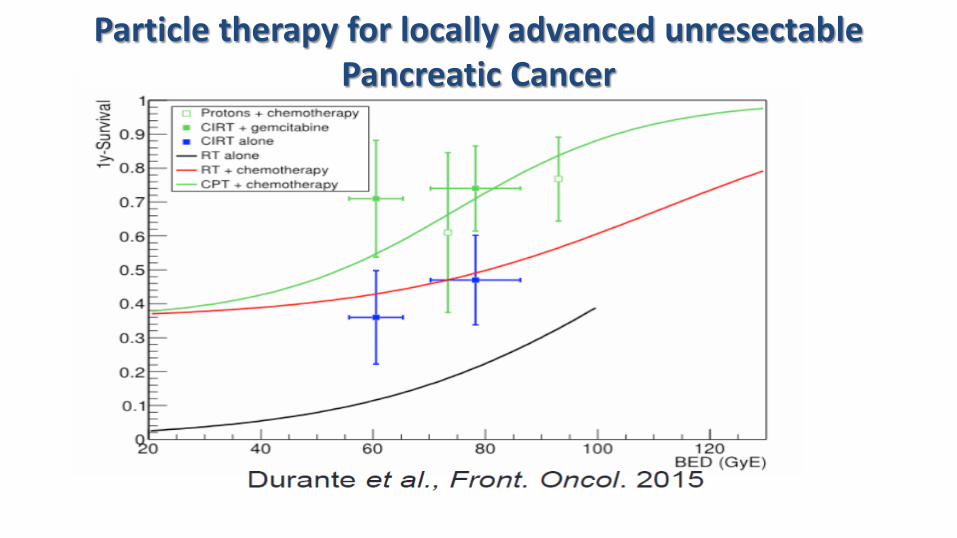
Particle therapy for locally advanced unresectable Pancreatic Cancer
More Facts
• Local control is a necessary condition for cure. • Surgery is a necessary condition for local control. • Surgery is not a sufficient condition for local control.
The problem with the Pancreaticoduodenectomy...
…is that even with negative nodes and negative surgical margins, 50% to 80% of patients will suffer a local failure if they do not receive postoperative radiotherapy.
Are you ready for the bad news?
• Hopkins data: – Pawlik TM, Surgery, 2007
• 905 Whipples from 1995 to 2005 –Node positivity was…79.3% –Margin positivity was …41.1%
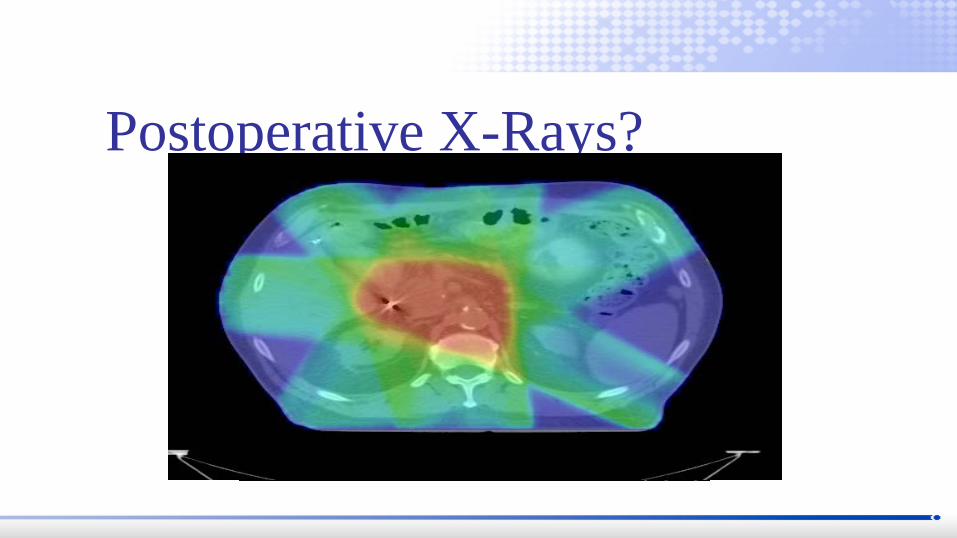
Postoperative X-Rays?

Problems with postoperative radiotherapy…
MGH data shows a 36% local/regional failure rate at 3 years after postoperative chemoradiation.
RTOG 97-04 shows a 23% to 28% local failure rate.
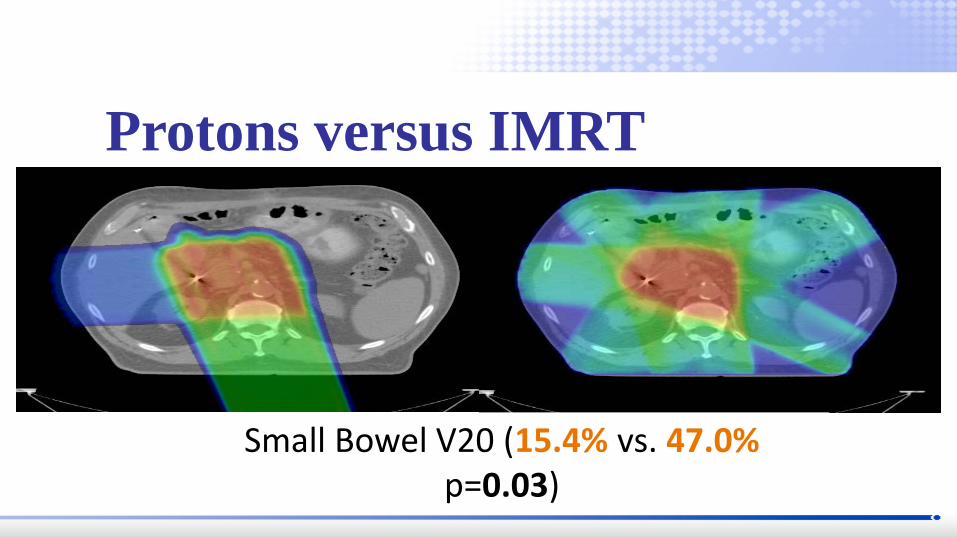
Protons versus IMRT
Small Bowel V20 (15.4% vs. 47.0% p=0.03)
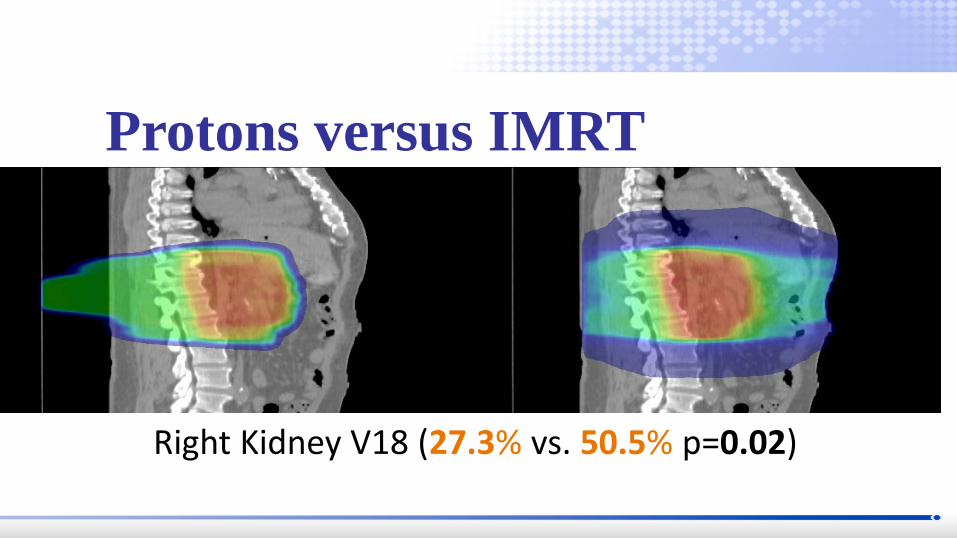
Protons versus IMRT
Right Kidney V18 (27.3% vs. 50.5% p=0.02)

What about efficacy?

PC01 Protocol (continued)
Median Survival 18.4 months
2 Year Local Control 69% 2 Year Overall
Survival 31%
Summary #1 • Surgical outcome data demonstrates
a high rate of local failure which is only marginally improved with postoperative radiotherapy.
Summary #2 • Our experience suggests that these fears
are unjustified with proton therapy: – Dosimetry – Lack of acute or late radiotherapy toxicity – Surgical experience showing no increase in complications for unresectable
patients receiving high dose radiotherapy before surgery.
UFPTI protocols: – PC01 … Unresectable disease … 59.40CGE with concomitant
Capecitabine (closed) – PC02 ... Resectable and marginally resectable disease … 50.40CGE
with concomitant Capecitabine. – PC03 … Postoperative adjuvant with weekly Gemcitabine
• 50.40CGE for R0 resections • 54.00CGE for R1 resections • 59.40CGE for R2 resections

UFPTI protocols:
– PC04 ( in development) … “initally unresectable” disease…63CGE in 28 fractions (mimics NRG 1201) with concomitant capecitabine.
• +/- equivalent of 70CGE at 2CGE per fraction
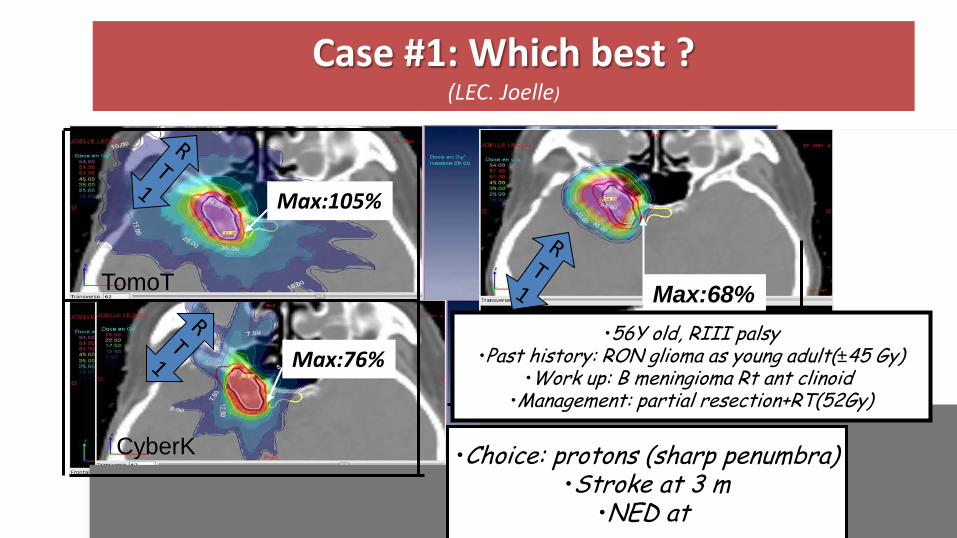
Case #1: Which best ? (LEC. Joelle)
Max:68%
Max:105%
Max:76%
TomoT
CyberK
Pr
•Choice: protons (sharp penumbra) •Stroke at 3 m
•NED at
•56Y old, RIII palsy •Past history: RON glioma as young adult(±45 Gy)
•Work up: B meningioma Rt ant clinoid •Management: partial resection+RT(52Gy)

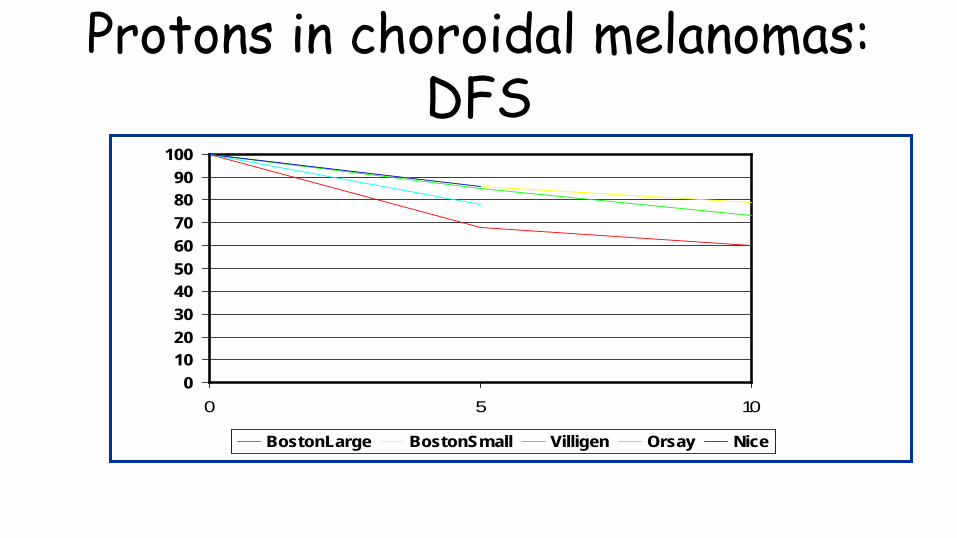
Protons in choroidal melanomas: DFS
0102030405060708090
100
0 5 10
BostonLarge BostonSmall Villigen Orsay Nice
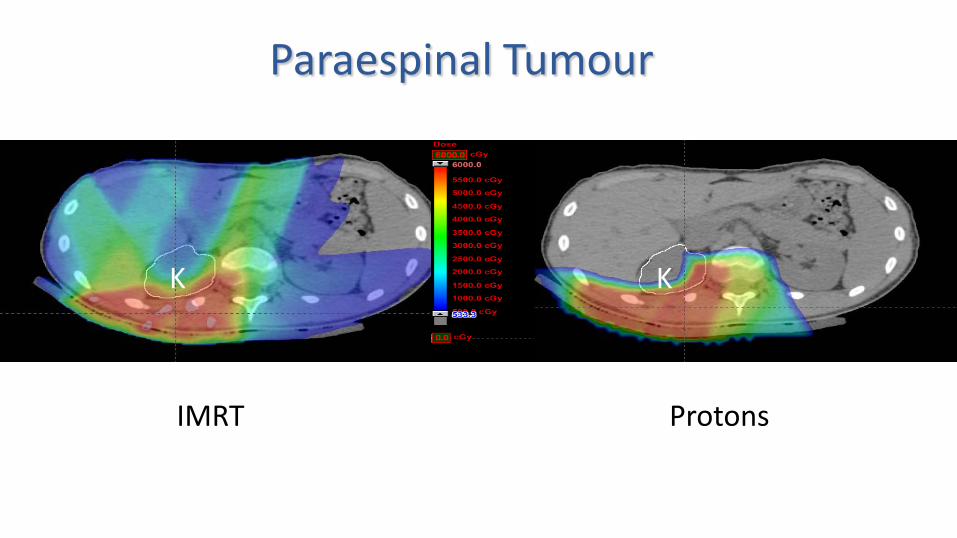
K K
Protons IMRT
Paraespinal Tumour
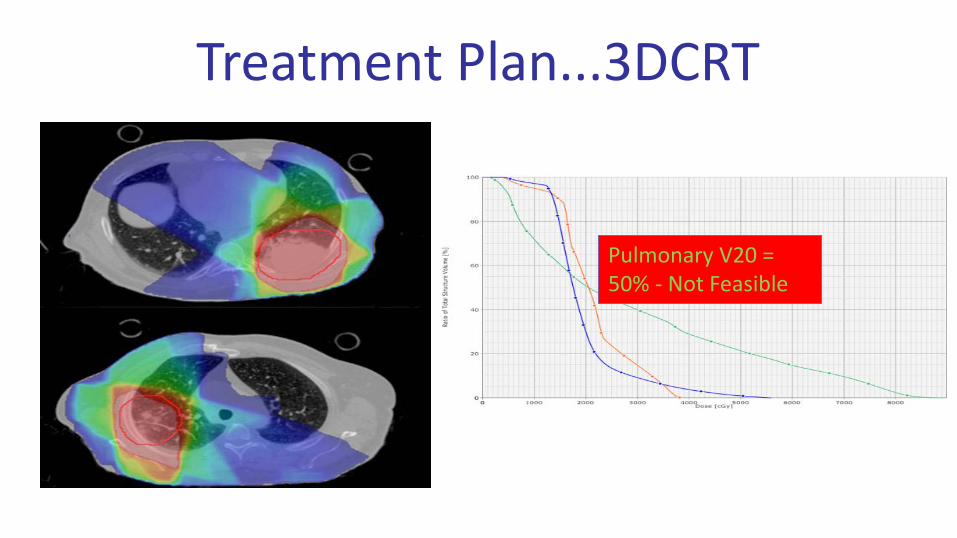
Treatment Plan...3DCRT
Pulmonary V20 = 50% - Not Feasible
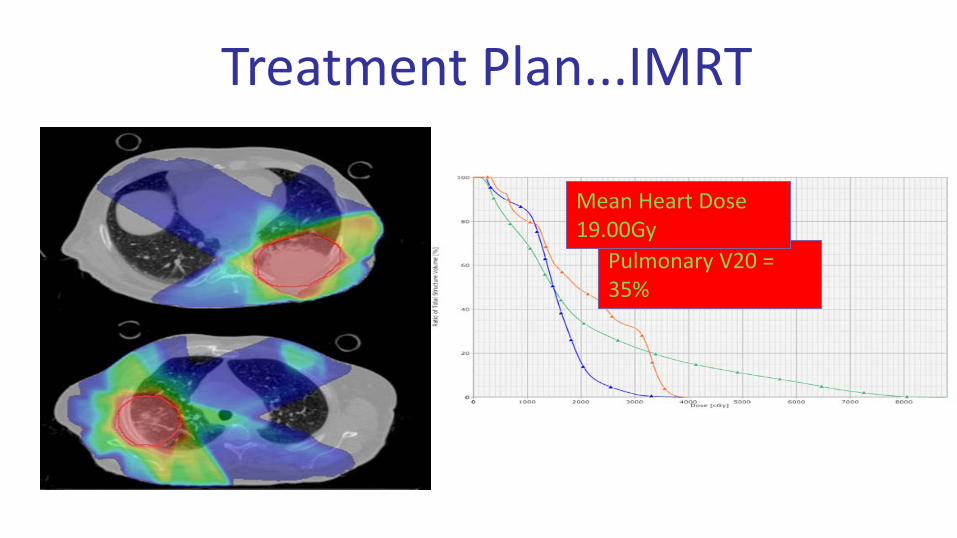
Treatment Plan...IMRT
Pulmonary V20 = 35%
Mean Heart Dose 19.00Gy
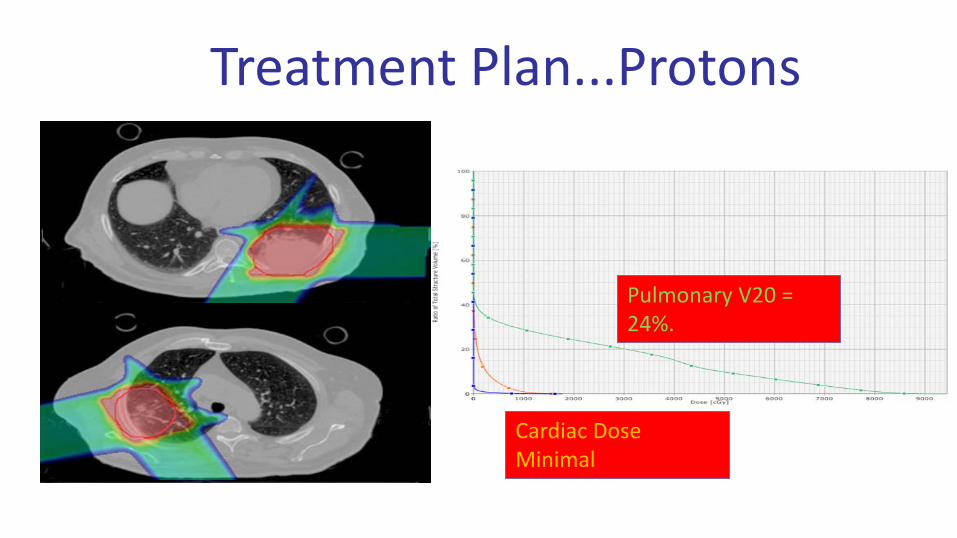
Treatment Plan...Protons
Pulmonary V20 = 24%.
Cardiac Dose Minimal
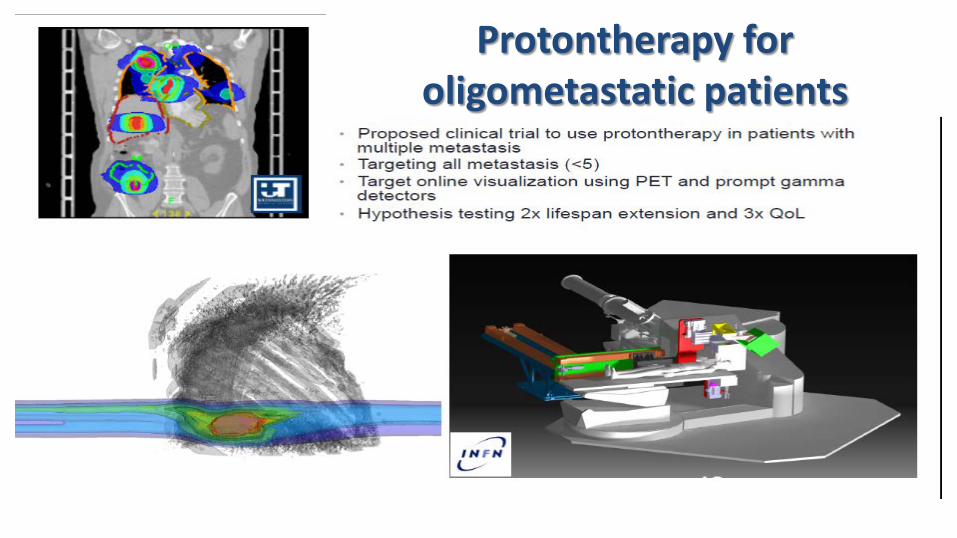
Protontherapy for oligometastatic patients
Potential Number of Patients in Argentina
( Population: 40 M)
• RT Conventional: 20.000 pt/year every 10 M Hab = 80.000 patients Protontherapy: 10-15 % pt RT = 8.000-12.000 pt/year

Proton Therapy and Advanced Radiotherapy Center
Instituto Roffo FCDN
Protonterapia

Which future for Hadrons ?
Today...
Tomorrow…
CARBON ? Others ?
PROTONS
PHOTONS PROTONS