Colo-rectal Carcinoma at a glance !!!
95
SUMAN RAJ BARAL COMS, BHARATPUR Colorectal Carcinoma
-
Upload
suman-baral -
Category
Health & Medicine
-
view
565 -
download
0
Transcript of Colo-rectal Carcinoma at a glance !!!
SUMAN RAJ BARALCOMS, BHARATPUR
Colorectal Carcinoma
Third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast and lung or bronchus cancer) in the United States.
The lifetime risk in the United States is 5.51% (1 in 18) for men and 5.10% (1 in 20) for women.
The risk for developing invasive colorectal cancer increases with age, with more than 90% of new cases being diagnosed in patients older than 50 years.
There has been a significant increase in 5-year survival rates over the last 30 years
1. GENETC FACTORS
2. ENVIRONMENTAL FACTORS
Factors Associated
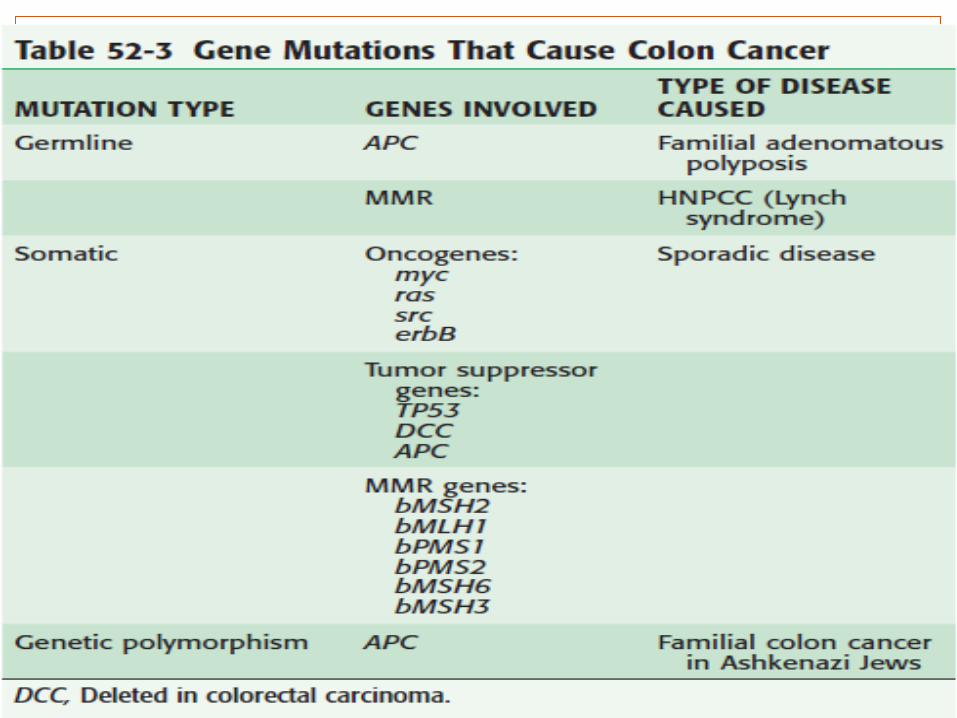
1. Genetic factors
Hereditary, sporadic, or familial form.
Hereditary forms : characterized by Family history, young age at onset, and the presence of other specific tumors and
defects. Familial adenomatous polyposis (FAP) and hereditary nonpolyposis colorectal cancer
(HNPCC). the specific mutation is present in all cells of the affected individual
Sporadic colorectal cancer Absence of family history Generally affects an older population (60 to 80 years of age) Presents as an isolated colon or rectal lesion. mutations associated with the cancer are limited to the tumor itself
Genetics of colorectal cancer initiation and progression proceed along similar pathways in the hereditary and sporadic forms of the disease.
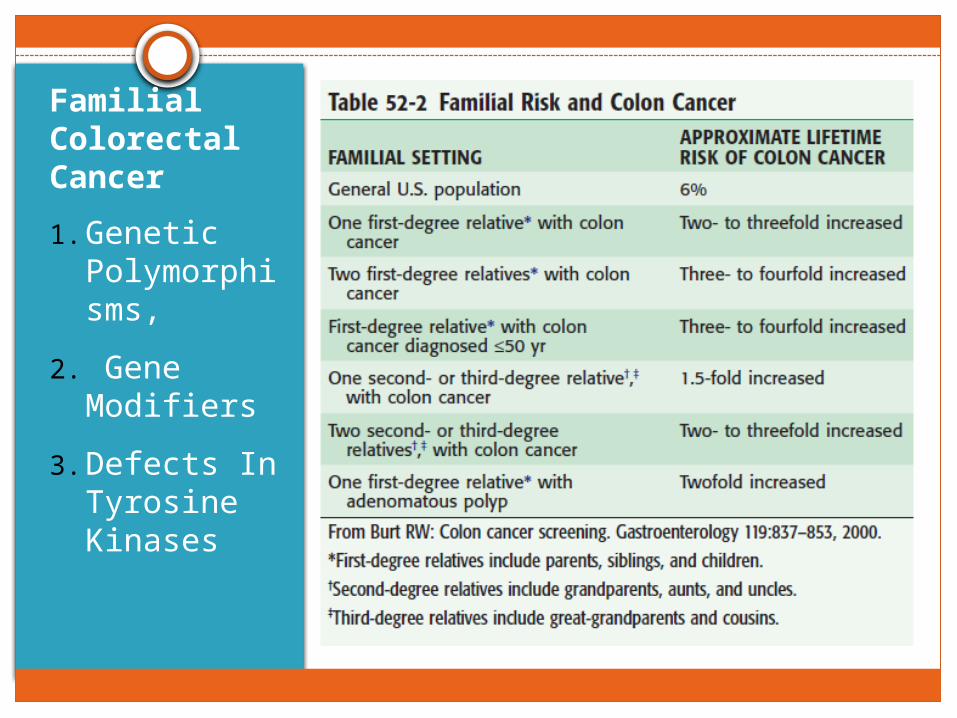
Familial Colorectal Cancer1. Genetic
Polymorphisms,
2. Gene Modifiers
3. Defects In Tyrosine Kinases
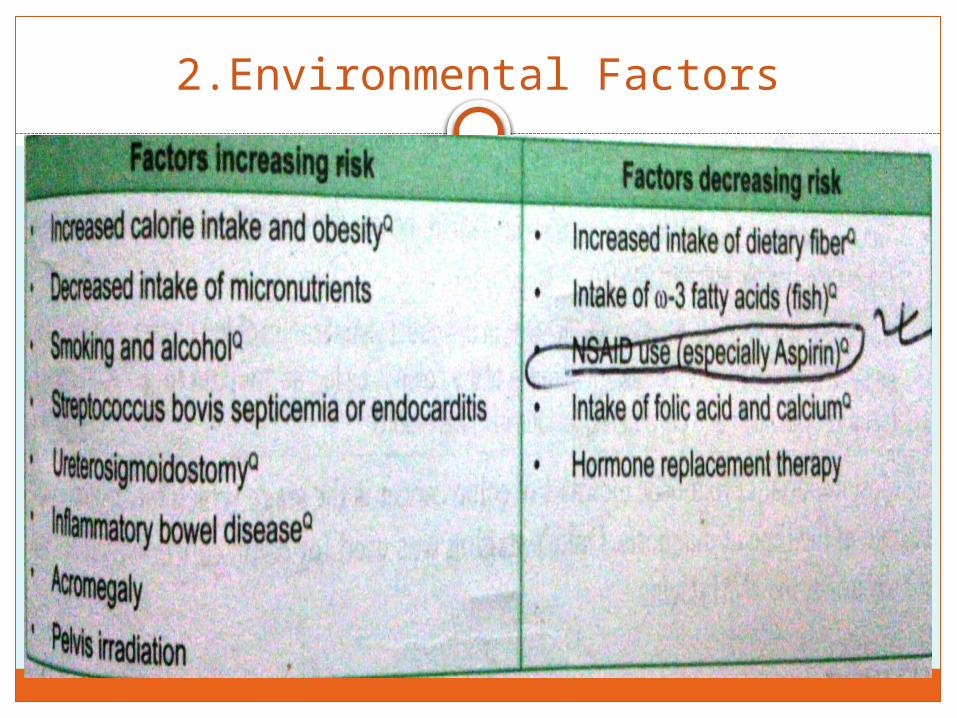
2.Environmental Factors
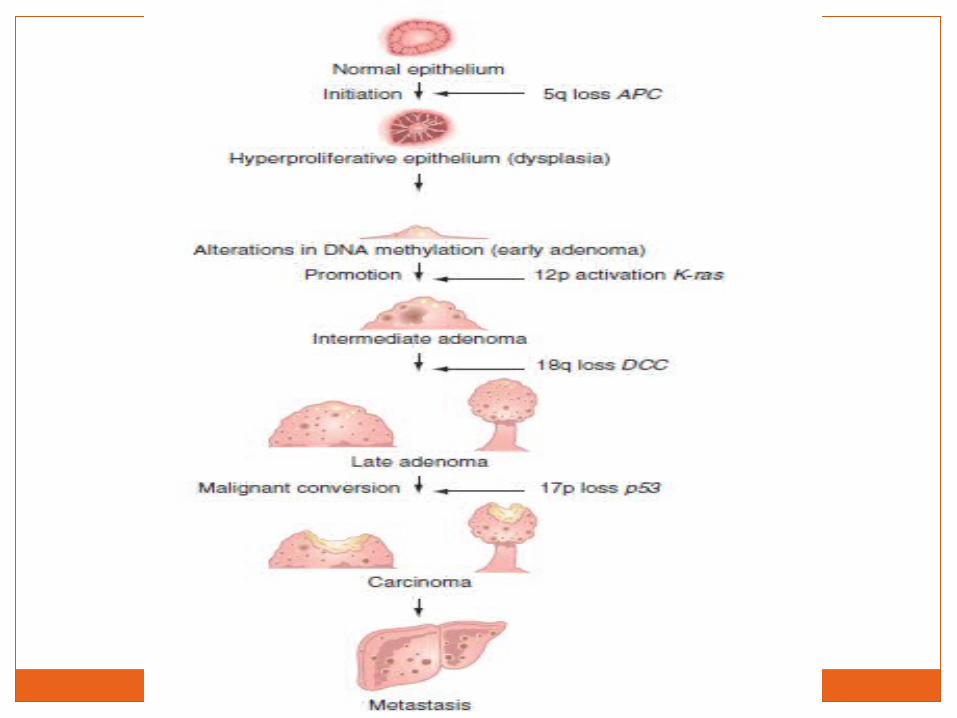
Pathogenesis
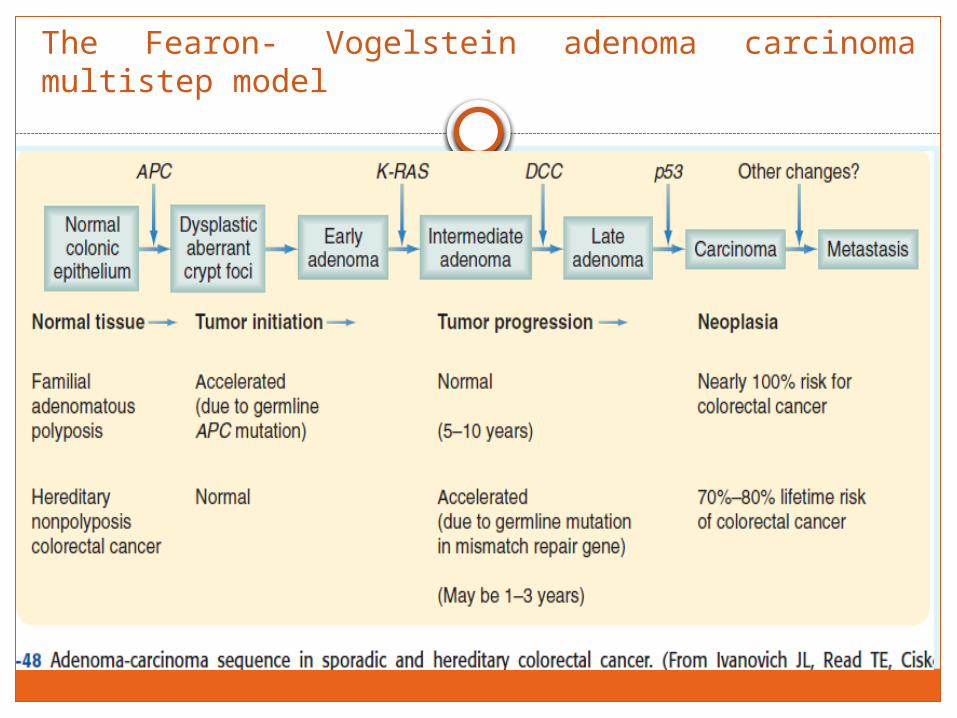
The Fearon- Vogelstein adenoma carcinoma multistep model
Adenoma-Carcinoma Sequence
Hypothesis
Colorectal carcinomas evolve through a progression of benign polyps to invasive carcinoma
Tiny colonic cancers arising de novo from normal mucosa : are rare
Adenoma-carcinoma sequence: now accepted
COLORECTAL POLYPAny mass projecting into the lumen of
the bowel above the surface of the intestinal epithelium.
Classification
Grossly : 1. Pedunculated(with a stalk)2. Sessile (flat, without a stalk).
Histologic appearance :1. Tubular adenoma (with branched tubular glands) :
1. 65% to 80% 2. often pedunculated3. less atypia in tubular adenomas 4. less than a 5% incidence of carcinoma in an adenomatous polyp smaller than 1 cm
in diameter2. Villous adenoma (with long finger-like projections of the surface epithelium :
1. 5 to 10 %2. commonly sessile severe 3. atypia or dysplasia (precancerous cellular change)4. 50% chance that a villous adenoma larger than 2 cm in diameter will contain a
cancer3. Tubulovillous adenoma (with elements of both cellular patterns). 10 to 25 %
The treatment of an adenomatous or villous polyp is removal, usually by colonoscopy.
The presence of any polypoid lesion is an indication for a complete colonoscopy and polypectomy, if feasible.
Polyps On a stalk are often removed by a snare passed through the colonoscope
Sessile (flat) polyps : technical problems because of the danger of perforation associated with the
snare technique. Elevate the sessile polyp from the underlying muscularis with saline injection,
permitting subsequent endoscopic excision, Often require segmental colectomy for complete removal
Polyps should be considered precursors of cancer and, when cancer arises in a polyp, careful consideration needs to be given to ensure the adequacy of treatment.
Invasive carcinoma describes the situation in which malignant cells have extended through the muscularis mucosae of the polyp, whether it is a lesion on a stalk or a sessile lesion.
Carcinoma confined to the muscularis mucosae does not metastasize and the cellular abnormalities should be described as atypia.Complete excision of this type of polyp is adequate treatment.
If invasive carcinoma penetrates the muscularis mucosae, consideration of the risk for lymph node metastasis and local recurrence is required to determine whether a more extensive resection is required.
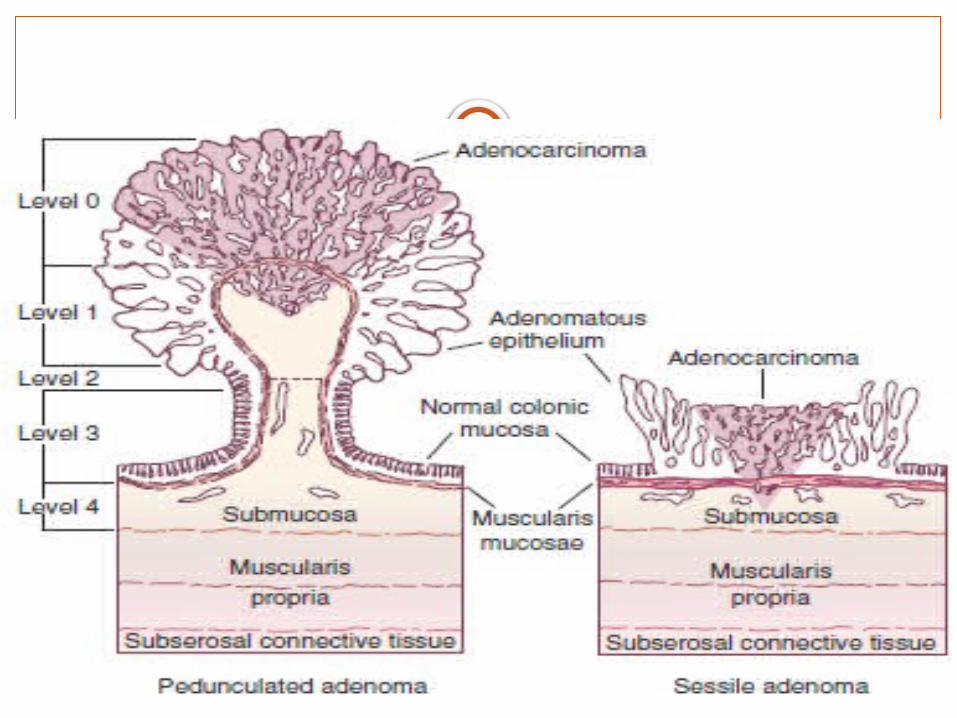
Haggitt and colleagues : Classification
Polyps containing cancer according to the depth of invasion as follows :
I. Level 0: Carcinoma does not invade the muscularis mucosae (carcinoma-in-situ or intramucosal carcinoma).
II. Level 1: Carcinoma invades through the muscularis mucosae into the submucosa but is limited to the head of the polyp.
III. Level 2: Carcinoma invades the level of the neck of the polyp (junction between the head and stalk).
IV. Level 3: Carcinoma invades any part of the stalk.V. Level 4: Carcinoma invades into the submucosa of the bowel wall
below the stalk of the polyp but above the muscularis propria.
By definition, all sessile polyps with invasive carcinoma are level 4 by Haggitt’s criteria.
If a polyp contains a histologically poorly differentiated invasive carcinoma, or if there are cancer cells observed in the lymphovascular spaces, there is a more than a 10% chance of metastases and these lesions should be treated aggressively.
A pedunculated polyp with invasion to levels 1, 2, and 3 has a low risk for lymph node metastasis or local recurrence and complete excision of the polyp is adequate if the poor prognostic factors mentioned earlier are absent.
A sessile polyp containing invasive cancer has at least a 10% chance of metastasis to regional lymphnodes, but if the lesion is well or moderately differentiated, there is no lymphovascular invasion noted, and the lesion can be completely excised, the depth of invasion by the cancer may provide useful prognostic information. There is a high risk for lymph node and distant metastases associated with sessile cancers in the rectum, and these lesions should be treated aggressively.
Hyperplastic polyps are the most common colonic polyps but are usually small and composed of cells showing dysmaturation and hyperplasia. The small diminutive polyps have been regarded as benign in nature, with no neoplastic potential.
The histologic appearance of these polyps is serrated (saw-toothed; Figs. 2-58 and 52-59). Of these polyps, 90% are smaller than 3 mm in diameter, and these diminutive lesions are generally considered to have no malignant potential. However, adenomatous changes can be found in hyperplastic polyps, and therefore the polyps should be excised for histologic examination. Theseserrated adenomas have been observed to be associated with the development of cancers that predominate in the right side of the colon, more frequently in older women and smokers. They appear to be associated with the microsatellite instability characteristic of defects in DNA repair mechanisms.
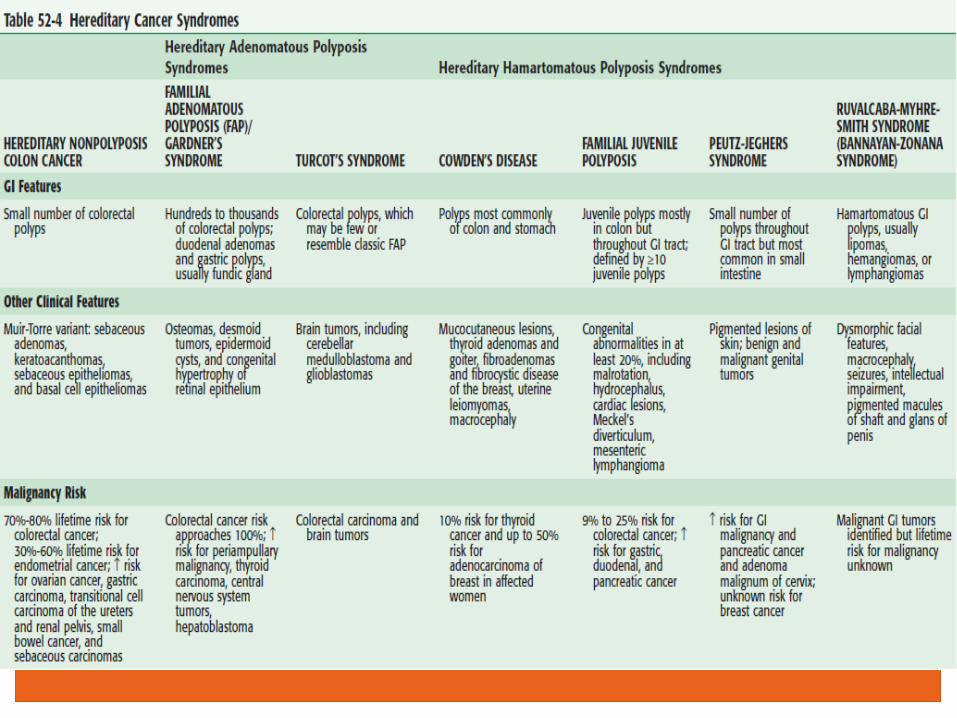
1. HEREDITAR Y NONPOLYPOSIS COLON CANCER2. FAMILIAL ADENOMAT OUS POLYPOSIS (FAP)/
3. GARDNER ’S SYNDROME 4. TURCOT’S SYNDROME
5. COWDEN’S DISEASE6. FAMILIAL JUVENILE POLYPOSIS
7. PE UTZ-JEGHER S SYNDROME8. RUVALCABA-MYHRE -SMITH SYNDROME
(BANNAYAN-ZONANA SYNDROME)
Hereditary Cancer Syndromes
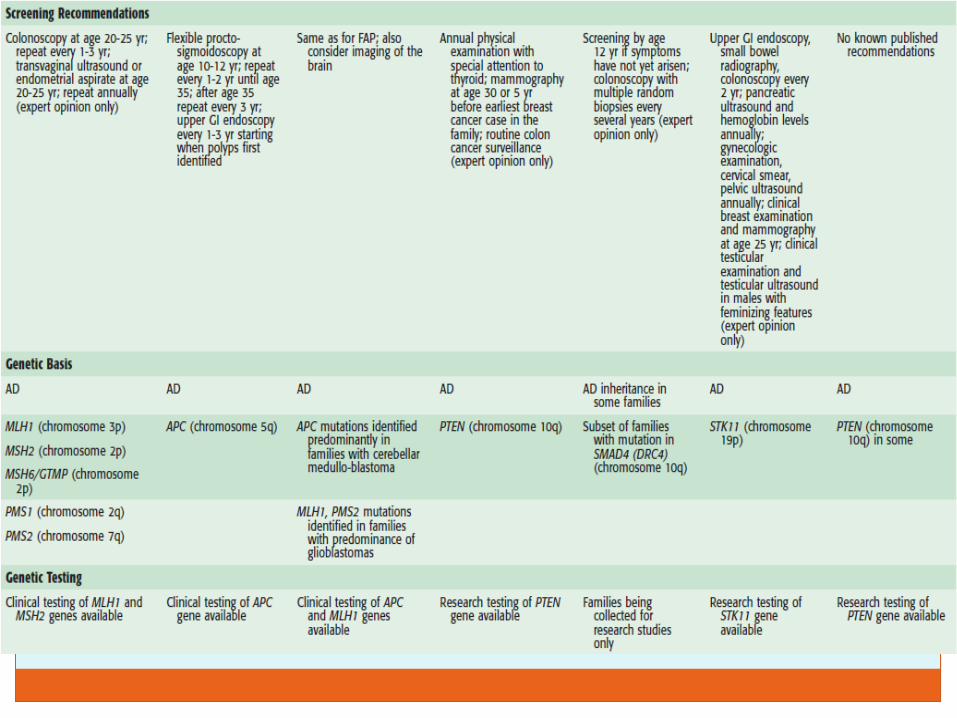
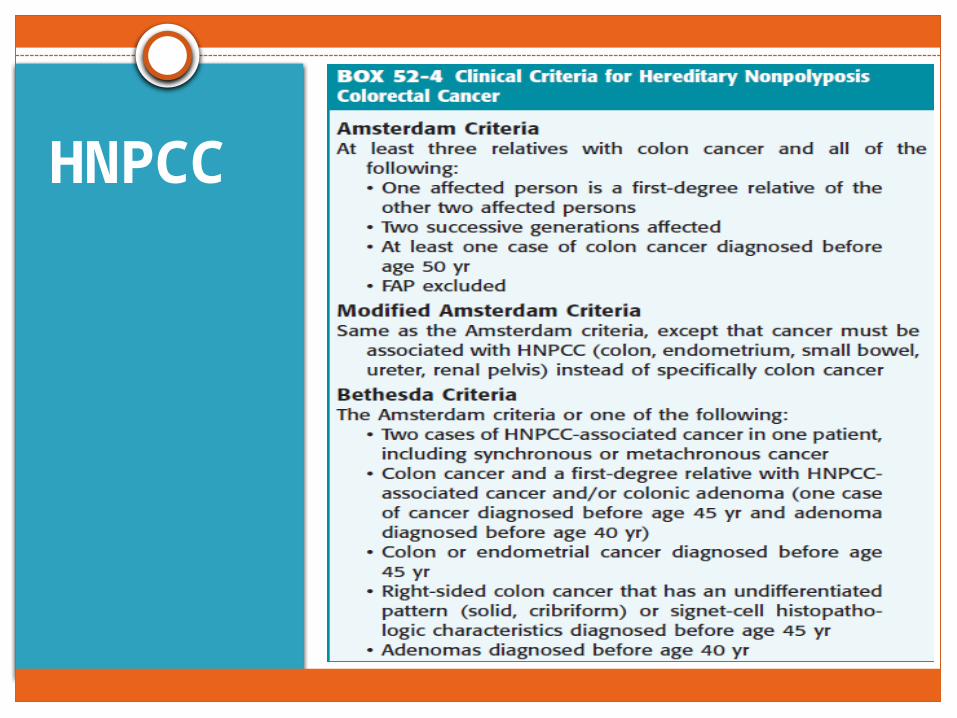
HNPCC
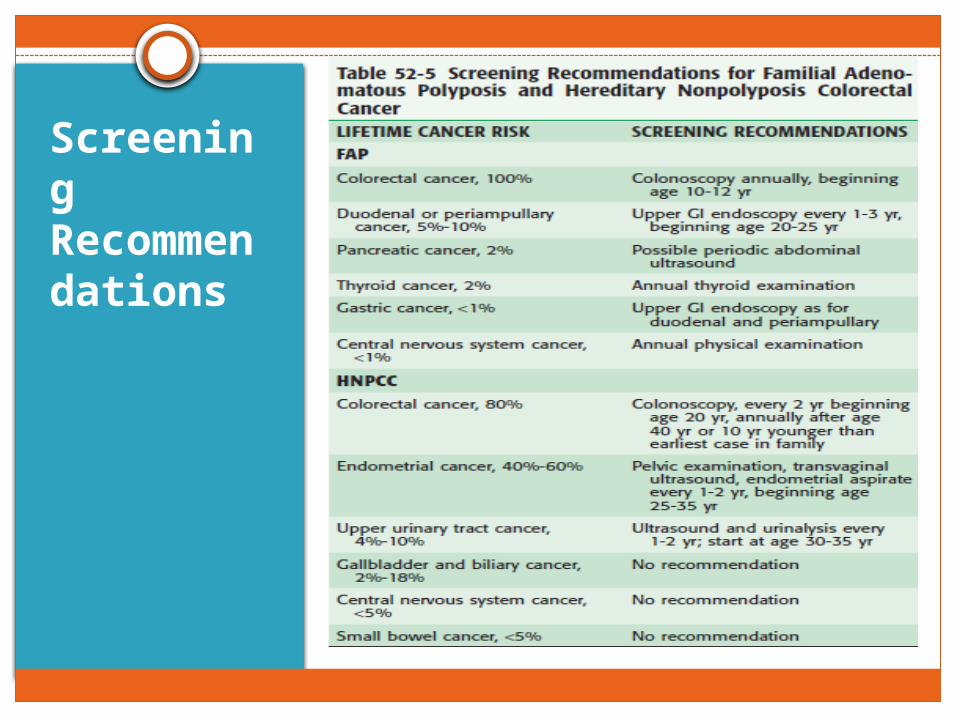
Screening Recommendations
Clinical Features
Signs and symptoms
Varied, nonspecificDependent
on the location of the tumor in colon The extent of constriction of the lumen caused by the
cancer.
Usually above 55 yearsEarly symptoms : insignificant that the patient
does not seek advice for six months or more Diagnosis is often delayed in younger patients as
these symptoms are attributed to benign causes.
Bleeding
Right-sided colon Cancer Bleeding can produce dark tarry stools (melena). Bleeding is asymptomatic and detected only by anemia discovered by a routine hemoglobin
determination. Iron deficiency anemia in any male or nonmenstruating female should lead to a search for a
source of bleeding from the GI tract.
Bleeding is often associated with colon cancer but, in approximately one third of patients with a proven colon cancer, the hemoglobin level is normal and the stool test results are negative for occult blood.
Rectal Ca Earliest and most common symptom. Nothing characteristic about the time at which it occurs, nor is the colour or the amount of
blood distinctive Occurs at the end of defaecation Stains underclothing May simulate internal haemorrhoids every respect Haemorrhoids and carcinoma can coexist
Left Colon Cancer often constrictive in nature. change in bowel habit, most often reported as increasing
constipation. Sigmoid cancers
Mimic diverticulitis, presenting with pain, fever, and obstructive symptoms.
At least 20% of patients with sigmoid cancer also have diverticular disease, making the correct diagnosis difficult at times.
Can also cause colovesical or colovaginal fistulas. Such fistulas are more commonly caused by diverticulitis, but it is imperative that the correct diagnosis be established because the treatment of colon cancer is substantially different than treatment of diverticulitis.
Tenesmus : CA Rectum Sense of incomplete defaecation a distressing straining to empty the bowels without
resultant evacuation The patient’s bowels open, but there is the sensation that
there are more faeces to be passed Very important early symptom and is present in tumours of
the lower half of the rectum.
Spurious diarrhoea : CA Rectum The patient may endeavour to empty the rectum several
times a day often with the passage of flatus and a little bloodstained mucus (‘bloody slime’).
Alteration in bowel habit The patient may find it necessary to start taking an aperient or to
supplement the usual dose. A patient who has to get up early in order to defaecate, or one who
passes blood and mucus in addition to faeces (‘early-morning bloody diarrhoea’), is usually found to be suffering from carcinoma of the rectum.
Annular carcinoma at the rectosigmoid junction : suffers with increasing constipation
Growth in the ampulla of the rectum :Early morning diarrhoea Pain
Pain is a late symptom, but pain of a colicky character may accompany advanced tumours of the rectosigmoid, and is caused by some degree of intestinal obstruction.
When a deep carcinomatous ulcer of the rectum erodes the prostate or bladder, there may be severe pain.
Pain in the back, or sciatica, occurs when the cancer invades the sacral plexus.
Weight loss metastases Weight loss is suggestive of hepatic metastases.
Advanced colorectal cancer can cause a change in bowel habits and intestinal obstruction
Diagnosis

Abdominal examination
Normal in early cases.
Advanced annular tumour at the rectosigmoid junction, signs of obstruction of the large intestine are present.
By the time the patient seeks advice, metastases in the liver may be palpable.
When the peritoneum has become studded with secondary deposits, ascites usually results.
Rectal examination
Neoplasm can be felt digitally: in early cases as a nodule with an indurated base. When the centre ulcerates, a shallow depression will be found, the edges of which are raised and everted.
On bimanual examination The lower extremity of a carcinoma situated in the rectosigmoid junction.
Finger smeared with blood or mucopurulent material tinged with blood.
When situated in the lower third of the rectum, involved lymph nodes can sometimes be felt as one or more hard, oval swellings in the mesorectum posteriorly or posterolaterally above the tumour.
In females, a vaginal examination should be performed and, when the neoplasm is situated on the anterior wall of the rectum, with one finger in the vagina and another in the rectum, very accurate palpation can be carried out.
Proctosigmoidoscopy
Will always show a carcinoma, if present, provided that the rectum is emptied of faeces beforehand.
Biopsy
Using biopsy forceps via a sigmoidoscope, a portion of the edge of the tumour can be removed.
If possible, another specimen from the more central part of the growth should also be obtained.
Colonoscopy
Gold standard for establishing the diagnosis
Required if possible in all patients to exclude a synchronous tumour, be it an adenoma or a carcinoma.
If a proximal adenoma is found, it can be conveniently snared and removed via the colonoscope.
If a synchronous carcinoma is present, the operative strategy will need changing.
If a full colonoscopy is not possible, a CT colonography or barium enema can be performed.
Colonoscopy
When a stenosing carcinoma is present, it may not be possible to do colonoscopy, to visualise the proximal colon.
Due to high incidence of synchronous tumours(3%) it is imperative that a colonoscopy is always performed either before or within a few months of surgical resection.
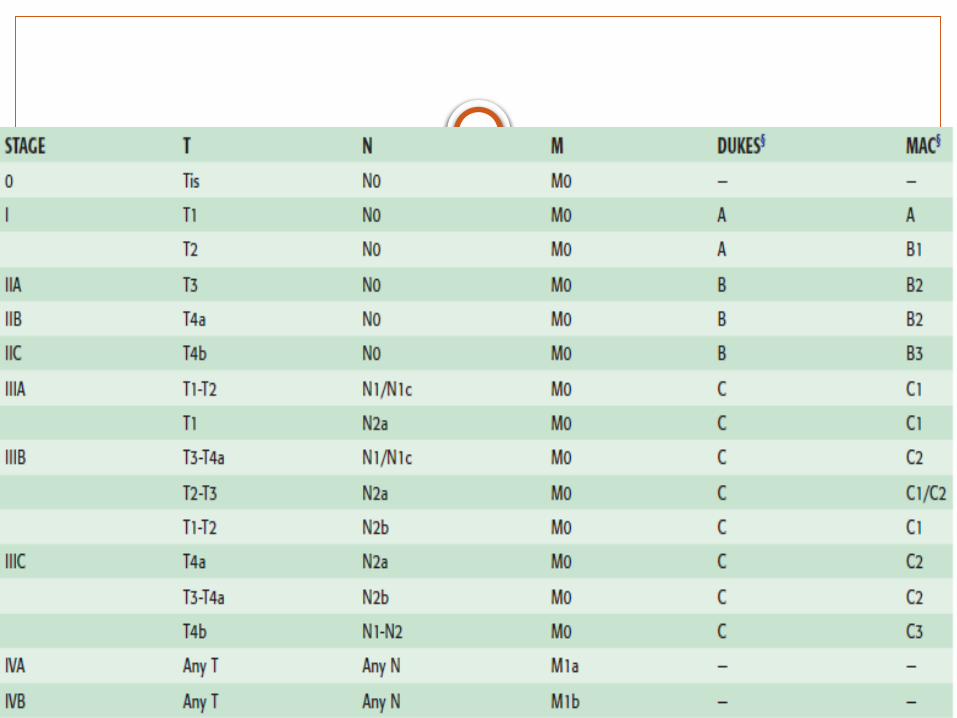
1. DUKES STAGING2. MODIFIED DUKES
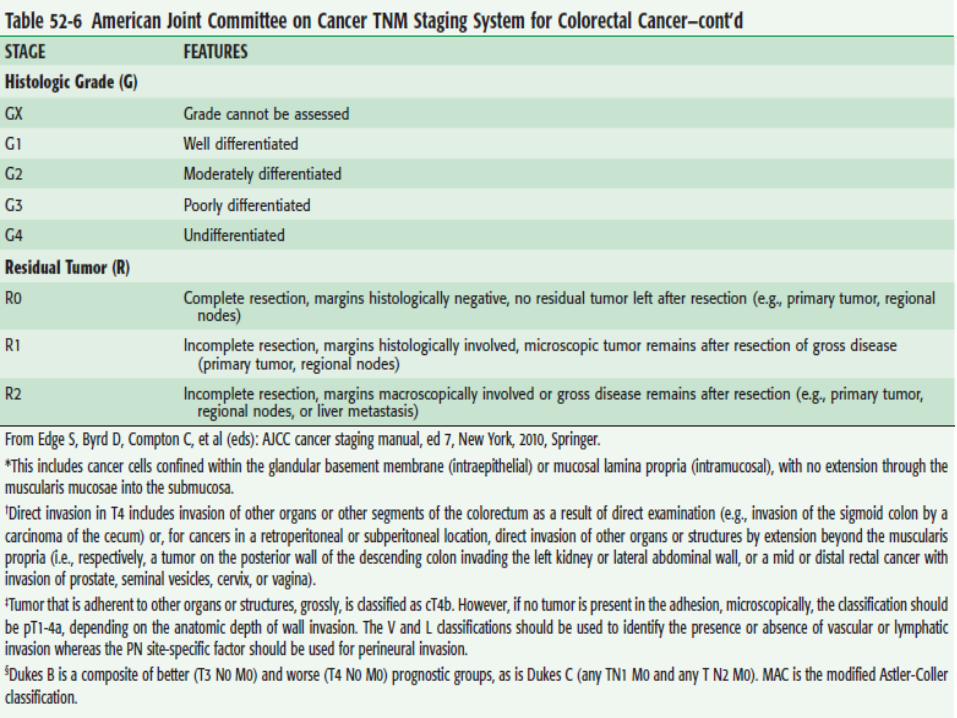
3. TNM STAGING
Staging
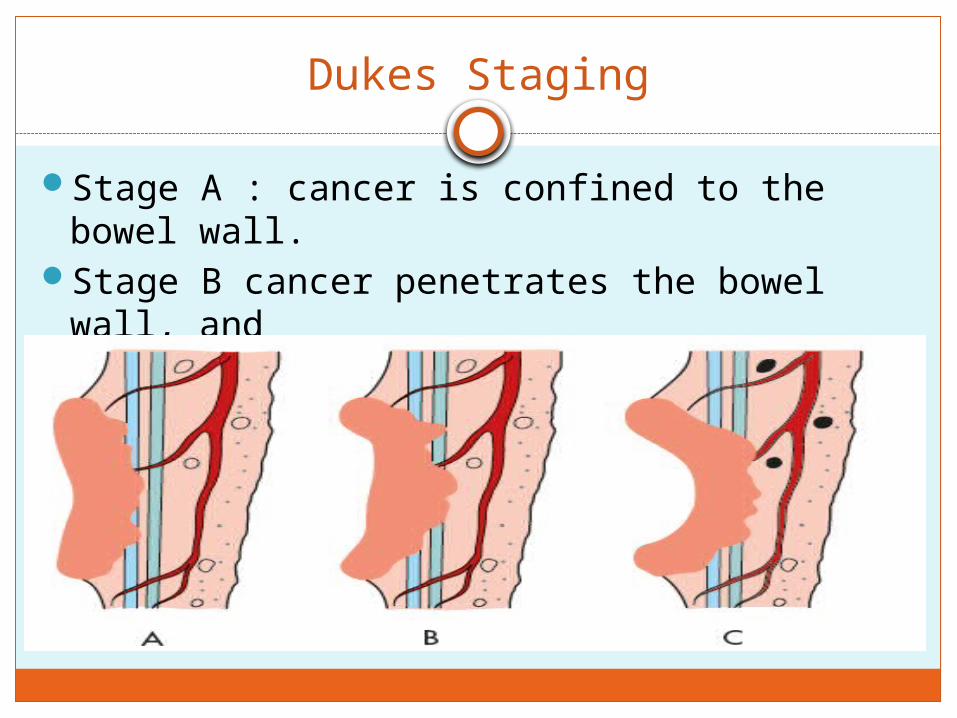
Dukes Staging
Stage A : cancer is confined to the bowel wall.
Stage B cancer penetrates the bowel wall, and
stage C cancer indicates lymph node metastases
Modified Dukes Staging
B1 :tumors that partially penetrated the muscularis propria
B2 :tumors that fully penetrated this layer
C1: The tumors that had invaded lymph nodes but did not penetrate the entire bowel wall
C2 :tumors that invaded lymph nodes and did penetrate the entire wall
Stage D for tumors with distant metastasis
Clinical Staging- cTNM
Based on medical history, physical examination, and endoscopy.
Examinations designed to detect metastatic disease (M) include chest x-rays, CT (including pelvis, abdomen, chest), MRI, and positron emission tomography (PET) or fused PET-CT scans.
Clinical staging : determines whether preoperative adjuvant treatment is indicated.
Preoperative stage determined by :endo-rectal ultrasound (EUS), pelvic CT, and pelvic MRI, with or without an endo-rectal coil.
Pathological staging pTNM
Provides a basis for prognosis and consideration of the need for further (adjuvant) treatment.
Patients who were given a clinical stage (cTNM) prior to the initiation of preoperative adjuvant treatment, usually combined radiation and chemotherapy, will have a modified pathologic stage assessed after examination of the surgically resected specimen; that stage is indicated by the “y” prescript (ypTNM).
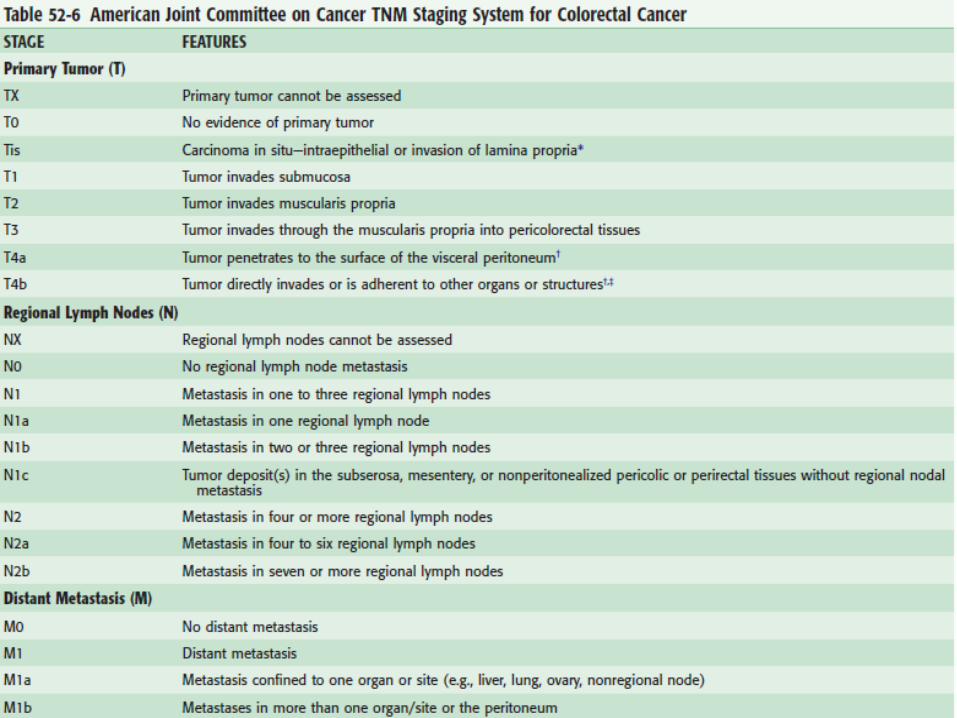
Cancer cells confined within the glandular basement membrane (intraepithelial) or lamina propria (intramucosal) with no extension through the muscularis mucosae are not associated with a risk of metastasis and are defined as in situ carcinoma −pTis.
T4 cancers that penetrate to the surface of the visceral peritoneum (pT4a) have a better prognosis than tumors that directly invade or adhere to other organs (pT4b)
Increasing numbers of involved lymph nodes are associated with a worsening prognosis, and the most recent classification system takes this into account.
Prognostic factors
These include the following: Tumor deposits—TDs The number of satellite tumor deposits discontinuous from the
edge of the cancer that are not associated with a residual lymph node
Tumor regression grade that permits the pathologic response to neoadjuvant therapy to be graded
The circumferential resection margin—CRM The distance from the edge of tumor to the nearest dissected
margin of the surgical resection Microsatellite instability (MSI) Perineural invasion—PN histologic cancerous invasion of the regional nerves KRAS mutation status
The KRAS mutation has been shown to be associated with lack of response to treatment with monoclonal antibodies directed against the epidermal growth factor receptor (EGFR) in patients with metastatic colorectal cancer.
Treatment and Follow-Up
Objective of surgery
Removal of the primary cancer with adequate margins, regional lymphadenectomy, and restoration of the continuity of the GI tract by anastomosis.
Extent of resection is determined by the location of the cancer, its blood supply and draining lymphatic system, and presence or absence of direct extension into adjacent organs.
Important to resect the lymphatics, which parallel the arterial supply, to the greatest extent possible in an attempt to render the abdomen free of lymphatic metastases.
If hepatic metastases are subsequently detected, they may still be resected for cure in some cases if the abdominal disease has been completely eradicated.
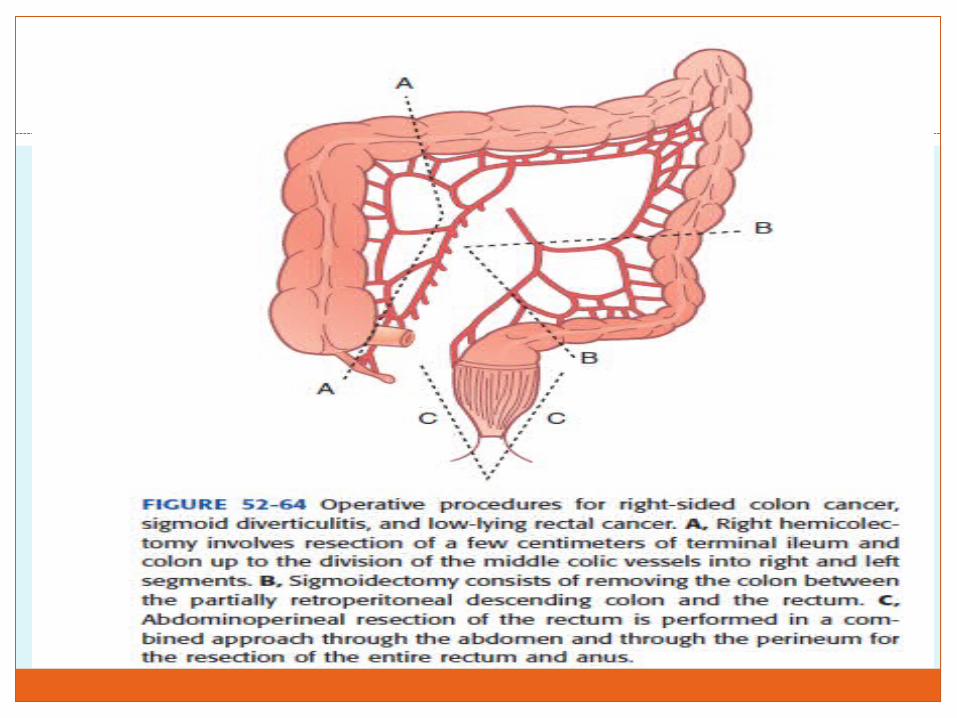
Right hemicolectomy : Involving the cecum, ascending colon, and hepatic flexure removal of the bowel from 4 to 6 cm proximal to the ileocecal
valve to the portion of the transverse colon supplied by the right branch of the middle colic artery.
An anastomosis is fashioned between the terminal ileum and transverse colon.
Extended right hemicolectomy : transverse colon lesions Division of the right and middle colic arteries at their origin, with
removal of the right and transverse colon supplied by these vessels.
The anastomosis is fashioned between the terminal ileum and proximal left colon.
Left hemicolectomy : tumors of the descending colon resection from the splenic flexure to the rectosigmoid junction
Sigmoidectomy : tumors of the sigmoid colon.
It is important that both segments of the intestine used for the anastomosis have an excellent blood supply and that there be no tension on the anastomosis.
Avoid incorporating the proximal sigmoid colon into an anastomosis because of the often tenuous blood supply from the IMA and frequent involvement of the sigmoid colon with diverticular disease.
Abdominal colectomy (sometimes called subtotal colectomy or total colectomy) removal of the entire colon from the ileum to the rectum,
with continuity restored by an ileorectal anastomosis. Because of loss of the absorptive and storage capacity of
the colon, this procedure causes an increase in stool frequency.
Patients younger than 60 years generally tolerate this well, with gradual adaptation of the small bowel mucosa, increased water absorption, and an acceptable stool frequency of one to three movements daily.
In older individuals, however, abdominal colectomy may result in significant chronic diarrhea.
Abdominal colectomy is indicated for patients with multiple primary tumors, for individuals with HNPCC, and occasionally for those with completely obstructing sigmoid cancers.
Tumors causing complete obstruction
Diagnosis is best established by resection of the tumor without the benefit of preoperative colonoscopy.
First approach : Hartmann’s operation Resection of the segment of colon containing the
obstructing cancer, suture closure of the distal sigmoid or rectum, and constructing a colostomy .
Intestinal continuity could be reestablished later, after the colon had been cleansed with purgatives, by taking down the colostomy and fashioning a colorectal anastomosis.
Tumors causing complete obstruction
Second approach Resect the segment of left colon containing the cancer Cleanse the remaining colon with saline lavage by
inserting a catheter through the appendix or ileum into the cecum and irrigating the contents from the colon.
A primary anastomosis between the prepared colon and rectum can then be fashioned without the need for a temporary colostomy.
Third approach For obstructing cancers of the sigmoid colon Resect the tumor and the entire colon proximal to the
tumor and fashion an anastomosis between the ileum and distal sigmoid colon (subtotal colectomy and ileo-sigmoid anastomosis).
Advantage of avoiding a temporary colostomy and eliminating the need to search for synchronous lesions in the colon proximal to the cancer. However, patients treated by this approach may have more frequent bowel movements.
Endoscopic techniques
Permit the placement of a stent introduced with the aid of a colonoscope that traverses the obstructed tumor and expands, re-creating a lumen, relieving the obstruction, and permitting a bowel preparation and elective operation with primary colorectal Anastomosis.
The approaches discussed concern obstruction of the left colon.
Complete obstruction of the right colon or cecum by cancer occurs less frequently.
Patients present with signs and symptoms of a small bowel obstruction. If an obstruction of the proximal colon is suspected, a water-soluble contrast study is useful to verify the diagnosis and evaluate the distal colon for the presence of a synchronous lesion.
Obstructing cancer of the proximal colon is treated by right hemicolectomy, with primary anastomosis between the ileum and transverse colon.
Patients with tumors that are not obstructing should undergo a thorough evaluation for metastatic disease.
Includes a thorough physical examination, chest x-ray, liver function tests, and measurement of the carcinoembryonic antigen (CEA) level.
Most surgeons now perform CT or MRI to inspect the liver more thoroughly for metastases and search for other intra-abdominal pathology
The presence of hepatic metastatic disease does not preclude surgical excision of the primary tumor.
Unless the hepatic metastatic disease is extensive, excising the primary cancer can provide excellent palliation.
Bleeding and obstruction caused by the tumor can be avoided and, if the metastatic disease in the liver is resectable, the patient may yet be cured.
5-year survival rate
Stage I colon cancer - 90%.Stage II colon cancer 75%. Stage III patients, with lymph node metastasis, is
50% Stage IV disease (distant metastases) less than 5%.
Further treatment and follow-up of patients treated by segmental colectomy for colon cancer is directed by the stage of the disease.
Approximately 85% of recurrences are detected within 2 years of the time of resection, so follow-up strategy should be especially intensive during that period.
Stage I Colon Cancer
Colonoscopic examination 1 year after the operation to inspect the anastomosis
To detect any new or missed polyps. Should be repeated annually if any polyps are detected and
removed, until an examination reveals the absence of polyps.
Then,every 5 years unless a strong family history or other genetic risk factor is present
CEA level : Every 3 months during the first 2 years, even if the
preoperative CEA level was normal. A rising CEA level requires further tests to search for
metastatic disease, including a CT scan (or MRI) of the abdomen and chest, and possibly a PET scan.
The goal : detect early recurrence that is amenable to treatment. Isolated hepatic or pulmonary metastases are amenable to
resection, with a 5-year survival rate of 20%.
Multiple or unresectable metastases may respond to current chemotherapeutic agents.
Stage II colon cancer
Postoperative treatment is somewhat controversial.
ASCO suggests a course of 5-flurouracil (5-FU)–based adjuvant chemotherapy for stage II patients with at least one poor prognostic indicator including insufficient lymph node sampling (<12 nodes resected
with the specimen) T4 lesions Poorly differentiated histology Bowel perforation.
Current practice in most areas appears to favor the addition of oxaliplatin in early-stage disease to 5-FU– leucovorin
Further follow-up of stage II patients includes a CEA level every 3 months for 2 years, every 6 months for a total of 5 years, and annual CT scans of the abdomen and chest for at least the first 3 years.
Stage III Colon Cancers
Benefit from adjuvant chemotherapy.
The addition of oxaliplatin to the 5-FU–leucovorin regimen (FOLFOX) has resulted in an improvement of disease-free survival rates at 3 years to 78% (compared with 73% with 5-FU–leucovorin alone).
Irinotecan (Camptosar) not demonstrated efficacy in the adjuvant setting and is not currently used for the treatment of stage III patients.
Stage IV Colon Cancer
Depends on the location and extent of the metastases.
Isolated hepatic or pulmonary lesions may be amenable to resection.
Chemotherapy is indicated, with new agents complementing the 5-FU regimens that remain the keystone of therapy. Effective for metastatic disease are the monoclonal
antibodies bevacizumab (Avastin), cetuximab (Erbitux), and panitumumab(Vectibix).
Cetuximab, a chimeric (mouse-human) and panitumumab a fully human monoclonal antibody bind to and inhibit the EGFR, which is overexpressed in 60% to
80% of colorectal cancers Effective only on tumors that do not have a mutation of the KRAS
gene. Genetic testing to confirm the absence of KRAS mutations
(indicating the presence of the KRAS wild-type gene) before recommending the use of these EGFR inhibitors.
Shown clinical efficacy in patients with metastatic colorectal cancer, both as monotherapy and in combination with irinotecan and FOLFOX.
Bevacizumab, a VEGFR inhibitor, has also improved survival when added to regimens that include irinotecan, 5-FU–leucovorin, or oxaliplatin.
Rectal Cancer
Controversy concerning the precise role of surgery, radiation therapy, and chemotherapy and the ideal timing of each modality with relation to the others.
Multimodality treatment of rectal cancer, the criteria for patient selection remains controversial.
Biologic properties of the rectum, combined with its anatomic distance from the small intestine afforded by its retroperitoneal pelvic location, provides an opportunity for treatment by radiation therapy that is not feasible for colon tumors
Radiation therapy
preoperative radiation is superior to postoperative radiation.
Preoperative radiation (combined with chemotherapy) was generally reserved for locally advanced distal rectal cancers (within 10 cm of the anal verge, stage II or higher),
short-term preoperative radiation (25 Gy over 5 days) results in a significant reduction in the local recurrence rate and improved disease-free survival for all stages of rectal cancer.
Chemotherapy
The combination of neoadjuvant (preoperative) radiation (usually, 4500 to 5040 cGy) with infusional 5-FU–leucovorin (and, more recently, with the addition of oxaliplatin) often results in dramatic reduction in tumor size (downstaging), and may result in apparently complete eradication of the tumor in up to 25% of cases.
Increase the ability to preserve continence by down-staging the cancer
Shrinking tumor size permit an anastomosis in the anal canal
Neoadjuvant treatment
In Europe, the short course of radiation (25 Gy), followed by extirpative surgery (low anterior resection or abdominal perineal resection), is the most common approach.
In the United States, stage II or higher rectal cancers are more commonly treated with preoperative chemoradiation consisting of 4500 to 5040 cGy of radiation in conjunction with infusional 5-FU–based chemotherapy.
The radiation is delivered over a period of 5 to 6 weeks, and surgery (low anterior resection or abdominal perineal resection) is done 6 to 10 weeks after completion of the radiation therapy.
A diverting stoma (ileostomy or transverse colostomy) is usually fashioned (with irradiated rectum) to protect the anastomosis and the stoma is then closed 10 weeks later, when studies show satisfactory healing of the anastomosis.
Local excision
Transanal approach, and usually involves excision of the full thickness of the rectal wall underlying the tumor.
Local excisions do not allow complete removal of lymph nodes in the mesorectum, so operative staging is limited.
three- to five fold higher recurrence rate compared with similar stage cancers treated by radical surgical resection.
The operation is indicated for mobile tumors smaller than 4 cm in diameter, that
involve less than 40% of the rectal wall circumference, and that are located within 6 cm of the anal verge.
Tumors should be stage T1 (limited to the submucosa) or T2 (limited to the muscularis propria), well or moderately differentiated histologically, and with no vascular or lymphatic invasion. There should be no evidence of nodal disease on preoperative ultrasound or MRI.
palliation of more advanced cancer in patients with severe comorbid disease
Require complete excision of the cancer, with adequate margins of normal tissue.
Suturing the rectal defect closed after the local excision, this is not mandatory because the operative site is below the peritoneal reflection.
Close follow-up is mandatory, in that approx 8% of T1 lesions recur and the recurrence rate for T2 lesions has been shown in some series to exceed 20%.
Transanal Endoscopic Microsurgery
An approach for the local excision of favorable rectal tumors (T1 cancers and sessile polyps) through a device designed to provide access to the mid and proximal rectum.
Advantages : excellent exposure to tumors in a difficult area of access
Technique is somewhat difficult to perform, the equipment is expensive, and the number of lesions amenable to this approach is relatively small.
Complications bleeding, urinary retention, perforation into the peritoneal cavity, and fecal
soilage. The dilation of the anal sphincters by the large endoscope may be associated
with subsequent fecal incontinence(transient)
Fulguration
Eradicates the cancer by using an electrocautery device that destroys the tumor by creating a full-thickness eschar at the tumor site, requires extension of the eschar into the perirectal fat, thus destroying both the tumor and rectal wall.
Can be used only for lesions below the peritoneal reflection.
Complications postoperative fever and significant bleeding, which can occur
as late as 10 days after the operation.
Technique cannot provide a specimen to assess the pathologic stage because the tumor and margins are disintegrated by fulguration.
The procedure is reserved for patients with a prohibitive operative risk and limited life expectancy; it has largely been replaced by transanal excision
Abdominal Perineal Resection( Miles procedure)
Complete excision of the rectum and anus, by concomitant dissection through the abdomen and perineum, with suture closure of the perineum and creation of a permanent colostomy
The rectum and sigmoid colon are mobilized through an abdominal incision.
The pelvic dissection is carried to the level of the levator ani muscles to excise the anus, anal sphincters, and distal rectum.
Positioning the patient in the prone position for the perineal excision permits a more cylindrical specimen (wider margins of normal tissue) to be obtained, with a reduction in positive circumferential margins, which should reduce the incidence of local recurrence.
Indicated tumor involves the anal sphincters or is too close to
the sphincters to obtain adequate margins, or in patients in whom sphincter-preserving surgery is not possible because of unfavorable body habitus or poor preoperative sphincter control.
A well-fashioned colostomy will often provide a superior quality of life to colo-anal anastomosis in an older patient or in a patient whose sphincter has been compromised by childbirth, radiation, or previous ano-rectal operations.
Low Anterior Resection
Resection of the rectum through an abdominal approach removing the portion of bowel containing the cancer and the mesorectum completely, which contains the lymphatic channels that drain the tumor bed.
The term anterior resection (an abbreviation for the more correct term, anterior proctosigmoidectomy with colorectal anastomosis) indicates resection of the proximal rectum or rectosigmoid above the peritoneal reflection
For cancers involving the lower half of the rectum, the entire mesorectum, which contains the lymph channels draining the tumor bed, should be excised in continuity with the rectum.
Total mesorectal excision, produces the complete resection of an intact package of the rectum and its adjacent mesorectum, enveloped within the visceral pelvic fascia with uninvolved circumferential margins.
The use of the technique of total mesorectal excision has resulted in a significant increase in 5-year survival rates (50% to 75%), a decrease in local recurrence rates (30% to 5%), and a decrease in the incidence of impotence and bladder dysfunction (85% to <15%).
Intestinal continuity is reestablished by fashioning an anastomosis between the descending colon and rectum, by the introduction of the circular stapling device or hand sewn.
If there is concern about the integrity of the anastomosis, or if the patient has received high-dose preoperative chemoradiation, a temporary proximal colostomy or ileostomy should be made to permit complete healing of the Anastomosis.
The stoma can be closed in approximately 10 weeks if proctoscopy and contrast studies verify the integrity of the anastomosis.
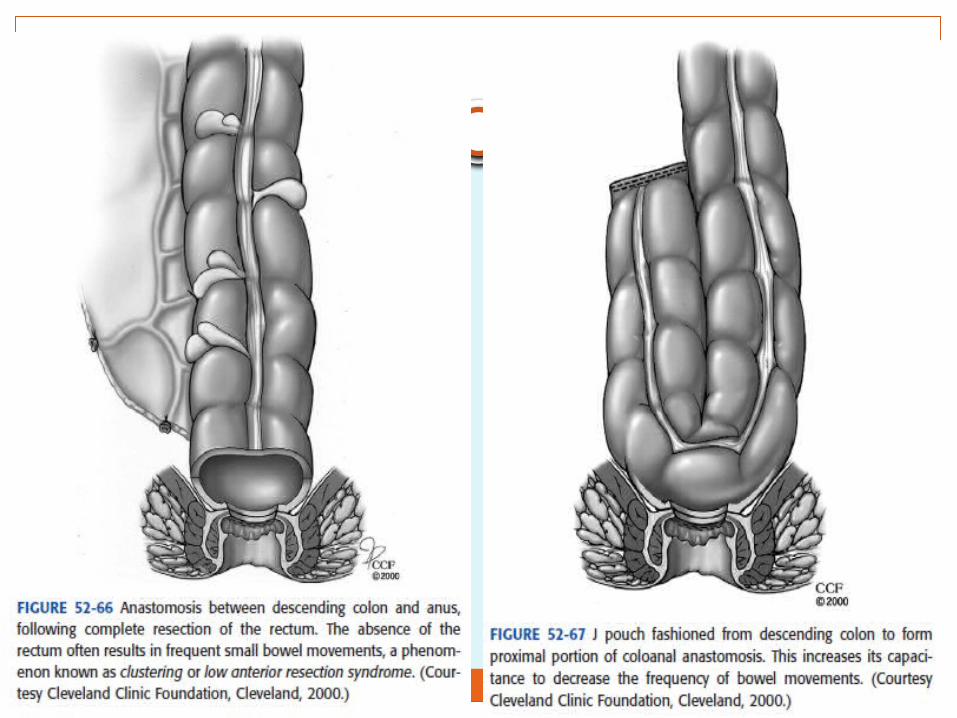
Result in significant alteration of bowel habits attributed to the loss of the normal rectal capacity
Patients treated with this operation often experience frequent small bowel movements (low anterior resection syndrome or clustering). This problem can be addressed by fashioning a colonic J pouch as the proximal component of the anastomosis
Sphincter-Sparing Abdominal Perineal Resection
With Coloanal Anastomosis
Cancer in the distal rectum cannot be resected with adequate margins while preserving the anal sphincter.
Use of preoperative radiation and chemotherapy to shrink the tumor to an extent that acceptable margins can be achieved.
If the anal sphincters do not need to be sacrificed to achieve adequate margins based on oncologic principles, a permanent stoma may be avoided with a sphincter sparing abdominal perineal resection, with an anastomosis between the colon and anal canal.
For young patients with rectal tumors who have a favorable body habitus and good preoperative sphincter function.

THANKS