Collaborative Action to Improve the Oral Health of ... · Collaborative Action to Improve the Oral...
45
Collaborative Action to Improve the Oral Health of Patients with Dementia in the West Midlands Mark Dermont BDS MPH MFGDP(UK) DDPH DPDS Specialty Registrar in Dental Public Health Dr Sol MBBS BSc MRCPsych Acting Consultant in Old Age Psychiatry M
Transcript of Collaborative Action to Improve the Oral Health of ... · Collaborative Action to Improve the Oral...
Collaborative Action to Improve the
Oral Health of Patients with Dementia in the West Midlands
Mark Dermont BDS MPH MFGDP(UK) DDPH DPDS Specialty Registrar in Dental Public Health
Dr Sol MBBS BSc MRCPsych
Acting Consultant in Old Age Psychiatry M
Scope
• How did the project come about?
• Why focus on early intervention?
• The project so far
• Shared learning
M
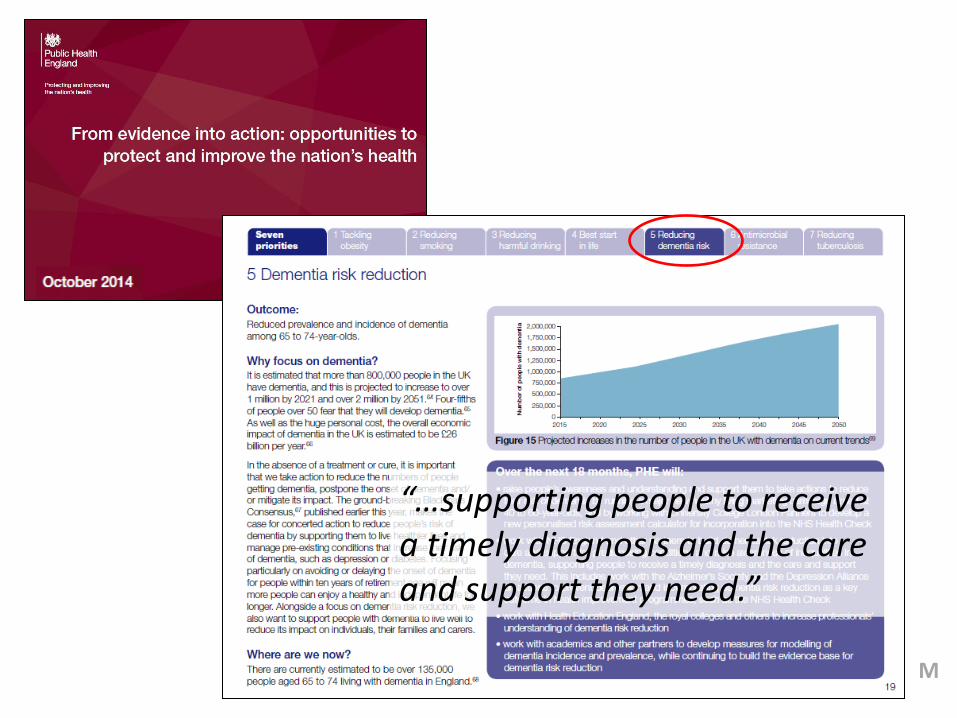
“…supporting people to receive a timely diagnosis and the care and support they need.”
M
From Evidence to Action
1. Evidence - Is there a problem?
- Does a solution exist?
2. Opportunity - To highlight issues
- Gain support for project
3. Action - Collaborative approach
M
Dementia cases nationally and in
Birmingham1 • Dementia estimated to be present in:
– 20% of those aged 80+ – 40% of those aged 90+
• Approx 17,000 pts. in the ‘younger’ category (30s,40s) • More cases likely to be undiagnosed (GP incentives)
• Birmingham and Solihull
– 16,000 dementia sufferers – Expected > 20,000 by 2021
1. Birmingham and Solihull dementia strategy 2013-16. Birmingham City Council. 2013. S
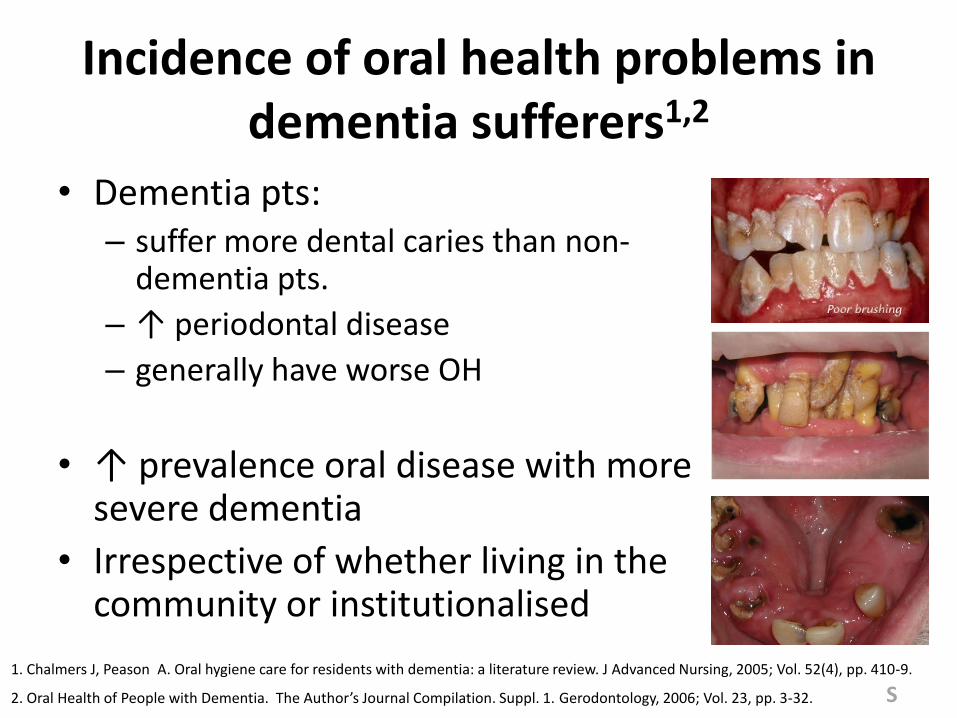
Incidence of oral health problems in
dementia sufferers1,2 • Dementia pts:
– suffer more dental caries than non-dementia pts.
– ↑ periodontal disease
– generally have worse OH
• ↑ prevalence oral disease with more severe dementia
• Irrespective of whether living in the community or institutionalised
1. Chalmers J, Peason A. Oral hygiene care for residents with dementia: a literature review. J Advanced Nursing, 2005; Vol. 52(4), pp. 410-9.
2. Oral Health of People with Dementia. The Author’s Journal Compilation. Suppl. 1. Gerodontology, 2006; Vol. 23, pp. 3-32. S
Incidence of oral health problems in dementia sufferers
• Many suffer oral disease before they enter residential care
• Once in care continue to progress….
• Dementia patients: – > dental treatment need than non-dementia pts, but…
– decreased utilisation of dental services1
• Alzheimer’s Society: – >50% reported dental problems2
– 8% of respondents had attended for dental care in past year
1. Alheimer's Society. Food for thought. 2000. Alzheimer's Society. 2. Chalmer sJ, Pearson A. Oral hygiene care for residents with dementia: a literature review. J Advanced Nursing, 2005; Vol. 52, pp. 410-419.
S
WHY?
• Increasingly cariogenic diet & altered feeding patterns
– Frequency of intake key
• Declining self-care (brushing / toothpaste use)
• Dentures not cleaned
• Sugar-containing medicines
• Decreased access to professional care to address problems
…dental diseases are largely preventable
S

The impact of poor oral health
• Caries and sequelae
• Perio Dx / mobile teeth
• Candidal infections
• Loose dentures
• Failing restorations
• Fractured teeth
• Pain • Swelling • Discomfort • Difficulty eating / swallowing • Xerostomia/ sore mouth • Spreading infections • Difficulty speaking
• Dehydration • Malnutrition • Mood & Depression • Irritability • Social withdrawal • Aspiration pneumonia • morbidity/mortality
S •
•
•
In later dementia….
• Undiagnosed dental pathology can trigger
Behavioural and Psychological Symptoms of Dementia (BPSD)
• Reduced ability to communicate BPSD
• In turn↑ likelihood of pt. being started on drugs to treat the symptoms rather than addressing underlying physical cause
S
In later dementia….
• Pharmacological agents prescribed can ↓general and oral health……
• potentiating further pain/discomfort….
• Antipsychotics
– ↑Stroke risk + overall mortality rates when used in dementia cases
– Threefold increase observed in RCTs
S
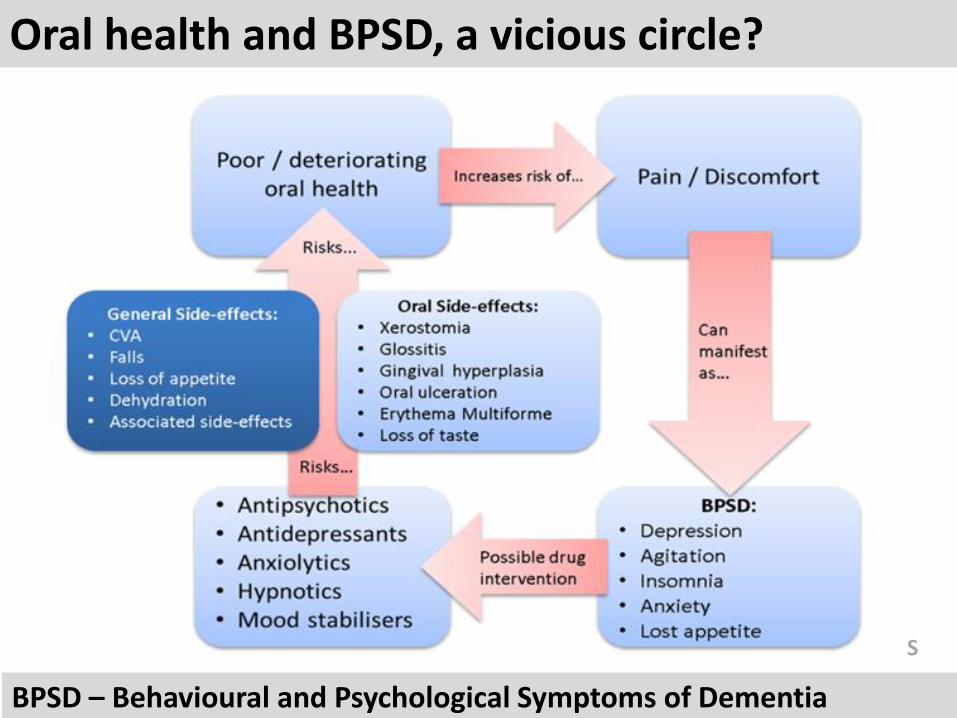
Oral health and BPSD, a vicious circle?
BPSD – Behavioural and Psychological Symptoms of Dementia
S
Barriers to maintaining good oral
health in dementia There are many, including:
• Cariogenic diet Vs. need to feed
• ↓ Ability to self-care / receive care
• OH knowledge of patient/carer
• Capacity consent in later disease
• Complex cases & polypharmacy
• Finding a dentist
• Care homes and domiciliary care…
Downstream Difficult
S
From Evidence to Action
1. Evidence - Is there a problem?
- Does a solution exist?
2. Opportunity - To highlight issues
- Gain support for project
3. Action - Collaborative approach
S
Early Intervention for Dementia
• Aim: To help those with dementia live well now and into the future
• Help individual adapt to dx and to work with families to build confidence, resilience and skills to face the future
• Making the diagnosis is one small part
S
Early Intervention for Dementia
• Society’s view of dementia is changing
• Large proportion of people experiencing early signs wish to know
• Previously prevailing view in society was to refrain from discussing dementia
• 2 common beliefs led to illusion that doing nothing is best
S
Early Intervention for Dementia
1. People developing dementia are unaware of their impairments and are happy in their ignorance not true
2. There is nothing that can be done if a diagnosis is made early, as dementia is an incurable condition not true
S
The Memory Clinic
• As demand for Dx started to grow memory clinic
• Many models……same focus (Dx + medication)
• Received Dx… pts. felt unsupported
“after a diagnosis people need to be shown a path, not shown the door”
S
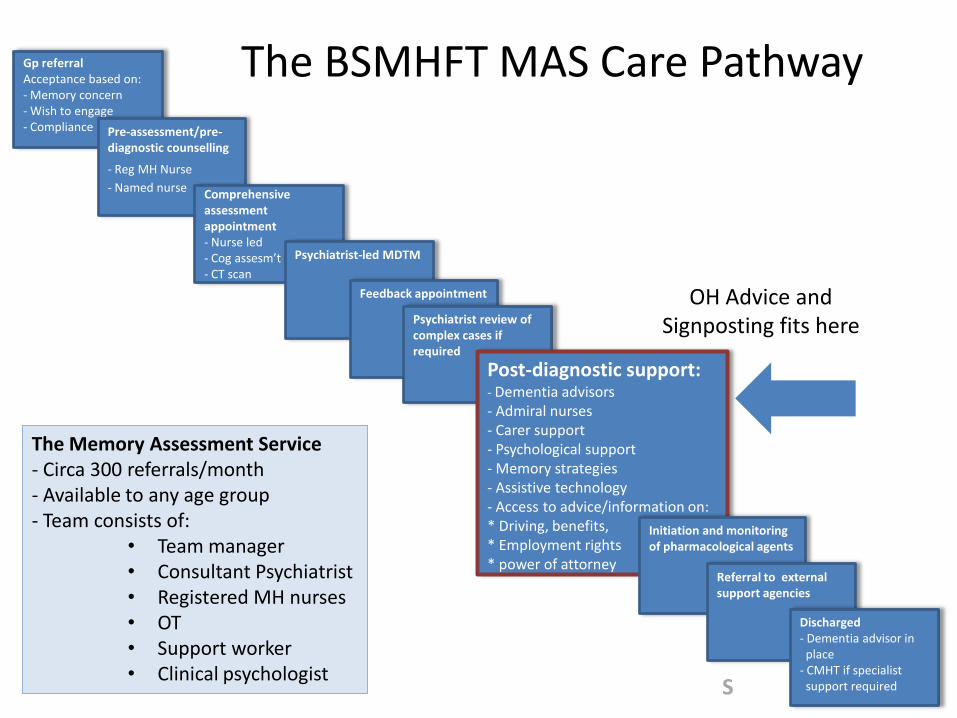
Gp referral Acceptance based on: - Memory concern - Wish to engage - Compliance
Pre-assessment/pre-diagnostic counselling
- Reg MH Nurse
- Named nurse
The Memory Assessment Service - Circa 300 referrals/month - Available to any age group - Team consists of:
• Team manager • Consultant Psychiatrist • Registered MH nurses • OT • Support worker • Clinical psychologist
Comprehensive assessment appointment - Nurse led - Cog assesm’t - CT scan
Psychiatrist-led MDTM
Feedback appointment
Psychiatrist review of complex cases if required Post-diagnostic support:
- Dementia advisors - Admiral nurses - Carer support - Psychological support - Memory strategies - Assistive technology - Access to advice/information on: * Driving, benefits, * Employment rights * power of attorney
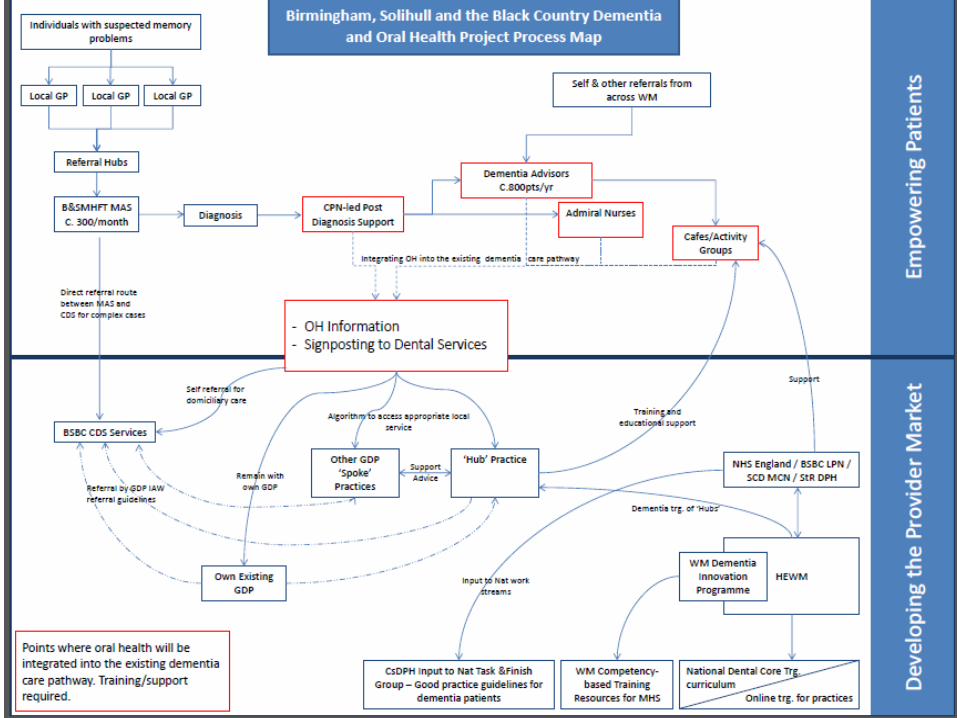
The BSMHFT MAS Care Pathway
OH Advice and Signposting fits here
Initiation and monitoring of pharmacological agents
Referral to external support agencies
Discharged - Dementia advisor in place - CMHT if specialist support required
S
Examples of support following Dx
• Dementia advisors – Work closely during post diagnostic intervention – Main point of contact following D/C. offer signposting,
advice etc.
• Admiral nurses
– Support family and carers of people with dementia
• Dementia café
– Forum to meet
S
Potential benefits of early oral health intervention in dementia patients
• Follows model of existing early intervention services (MAS)
• Pts. more physically and mentally capable in early disease (0-4 yrs)
• Most aspects of oral care should be possible:
– Treatment planning and prevention with patient
– Discussion around patient’s wishes re. teeth of concern
• Later in the disease: – Pt. may be unable to consent – uncooperative /immobile – treatment options become limited
• Dental professionals may be able to pick up early stage dementia
S
M
What is needed?
• Patients & carers need to know there are options
• Dental teams need to be aware of particular needs in this (early dementia) group
• Patients need to be signposted early to appropriate services
• Mental Health Services need to know what to do
M
Purpose of Project
Integrate key oral health messages into the existing Mental Health Services dementia care pathway
Develop signposting to dementia friendly dental services to improve access to appropriate oral health care.
M
Purpose of Project
Integrate key oral health messages into the existing Mental Health Services dementia care pathway
S
Develop signposting to dementia friendly dental services to improve access to appropriate oral health care.
Signposting:
Continue to see own dental team or,
Assist patient in finding a local dentist or,
If appropriate, signpost to Specialist in SCD
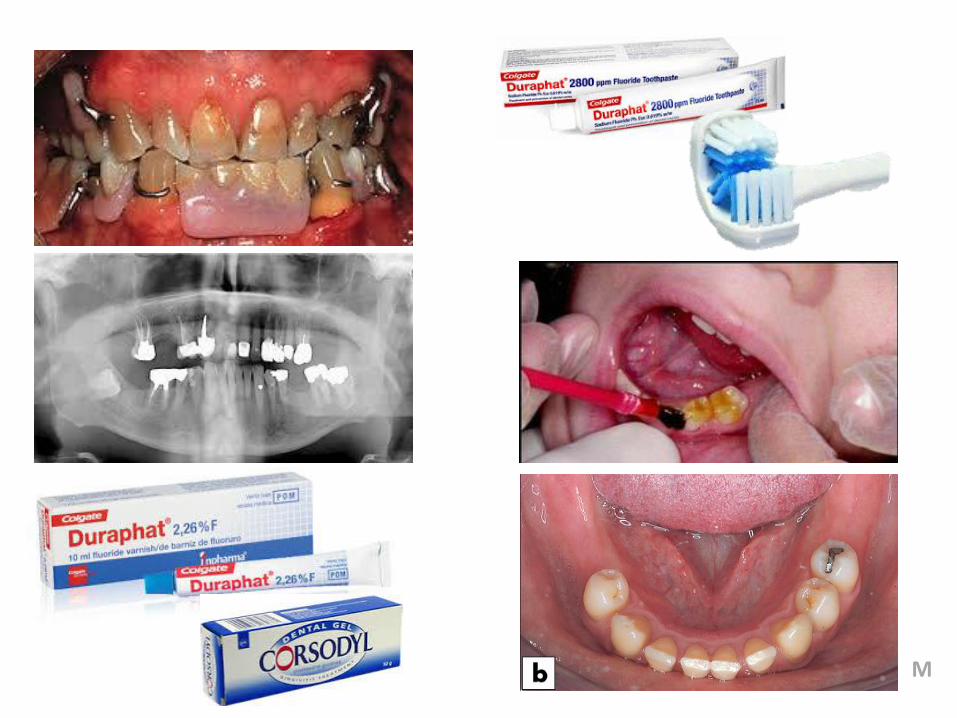
Messages:
• Visit dentist and discuss dementia
• Discuss prevention of future dental problems
• Twice daily brushing with a strong fluoride toothpaste
• Spit don’t rinse after brushing
• Reduce sugary foods & drink intake each day
• Highlighting the availability of sugar-free medicines
M
From Evidence to Action
1. Evidence - Is there a problem?
- Does a solution exist?
2. Opportunity - To highlight issues
- Gain support for project
3. Action - Collaborative approach
M
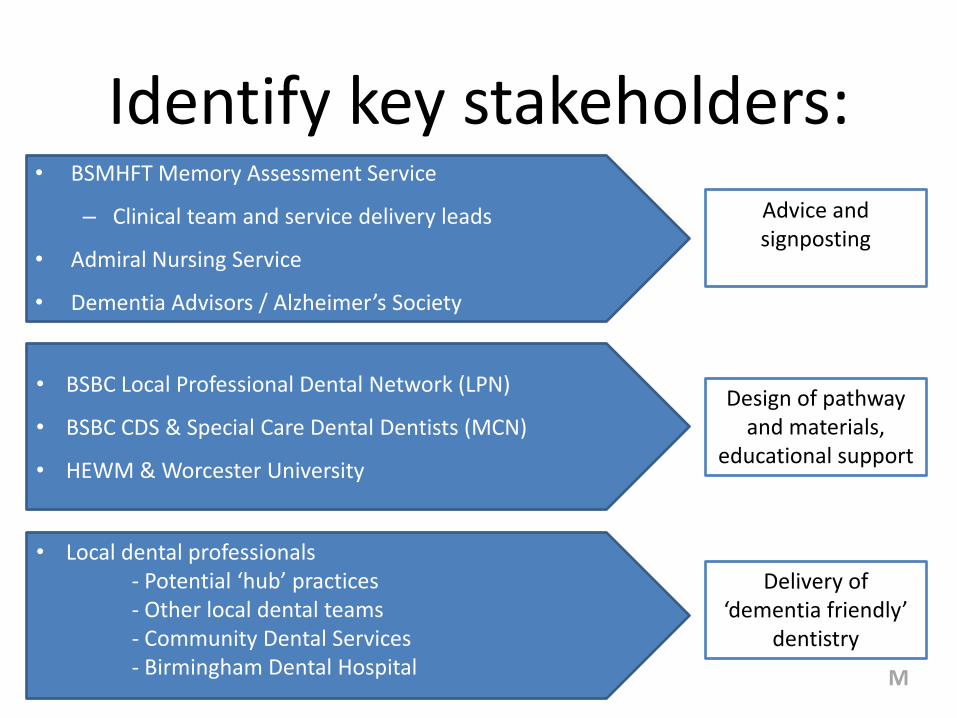
Identify key stakeholders:
• BSMHFT Memory Assessment Service
– Clinical team and service delivery leads
• Admiral Nursing Service
• Dementia Advisors / Alzheimer’s Society
M
• BSBC Local Professional Dental Network (LPN)
• BSBC CDS & Special Care Dental Dentists (MCN)
• HEWM & Worcester University
• Local dental professionals - Potential ‘hub’ practices - Other local dental teams - Community Dental Services - Birmingham Dental Hospital
Design of pathway and materials,
educational support
Advice and signposting
Delivery of ‘dementia friendly’
dentistry
Project Steps
1. Understand Patient/Carer Needs
Focus groups with service users and BMAS staff
2. Engagement with project stakeholders
- Mental Health Services (BMAS)
- Dental profession and commissioners (NHS England, SCD MCN, LPN, LDC etc.)
3. Develop work plan and supporting materials
- Supported by special care managed clinical network
M
Results from focus groups – Service Users
“…I’m afraid of going, I don’t know what will happen” [Patient]
“I wouldn’t tell the dentist about my dementia. I don’t trust him” [Patient ]
M
“…Oh it was great stress yes and he still isn’t speaking to any dentist…I’m not going to take him back again unless there is another emergency” [Carer]
…and lots of positive comments!
Results from focus groups - carers
“I think there is a need that a couple of dentists within even the Birmingham area that come with a real trusted recommendation… …and that they really understand the needs of the family and the needs of the carers.” [Carer]
“There’s perhaps a need for a dentist within the dementia service…not just our dementia but within the dementia service, that is trusted and that you know and understand” [Carer ]
Key Themes:
• Fear from uncertainty
• Not disclosing their illness
• Seeking ‘trust’
• Asking for advice
• Being unsure what support is available
M
Learning from Focus Groups
• Qualitative evidence of local need
• knowledge gap re. oral health and services
• Helped identify;
– User requirements for dementia friendly dentistry
– Valued existing resources (e.g. Dementia Cafes)
• Highlighted need to encourage dementia discussion between patients and dental team
M
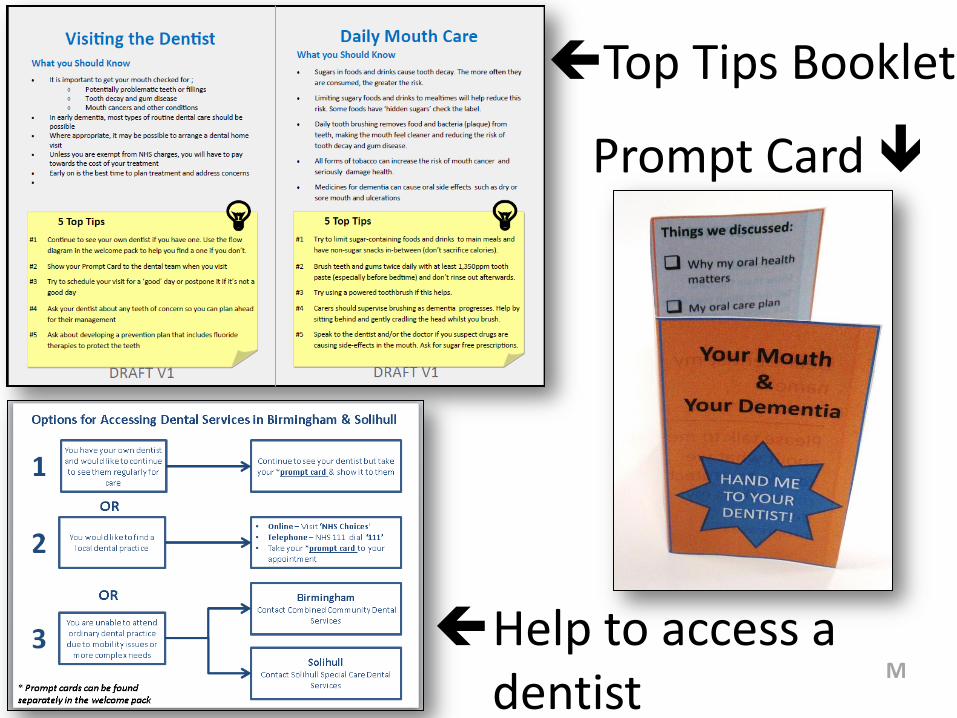
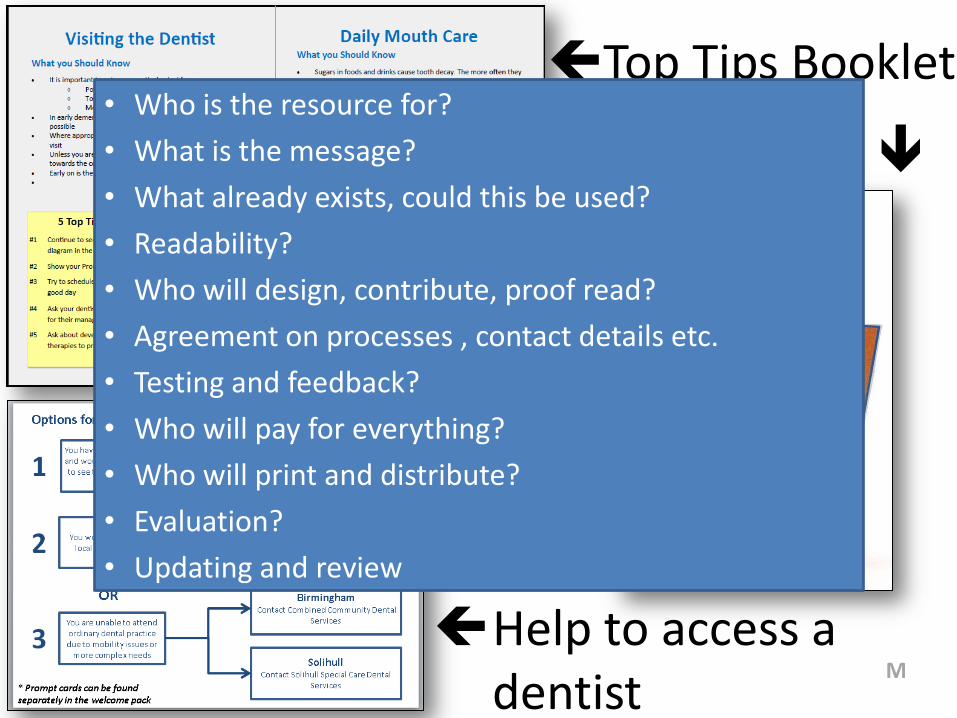
Top Tips Booklet
Prompt Card
Help to access a dentist
M
Top Tips Booklet
Prompt Card
Help to access a dentist
• Who is the resource for?
• What is the message?
• What already exists, could this be used?
• Readability?
• Who will design, contribute, proof read?
• Agreement on processes , contact details etc.
• Testing and feedback?
• Who will pay for everything?
• Who will print and distribute?
• Evaluation?
• Updating and review
M
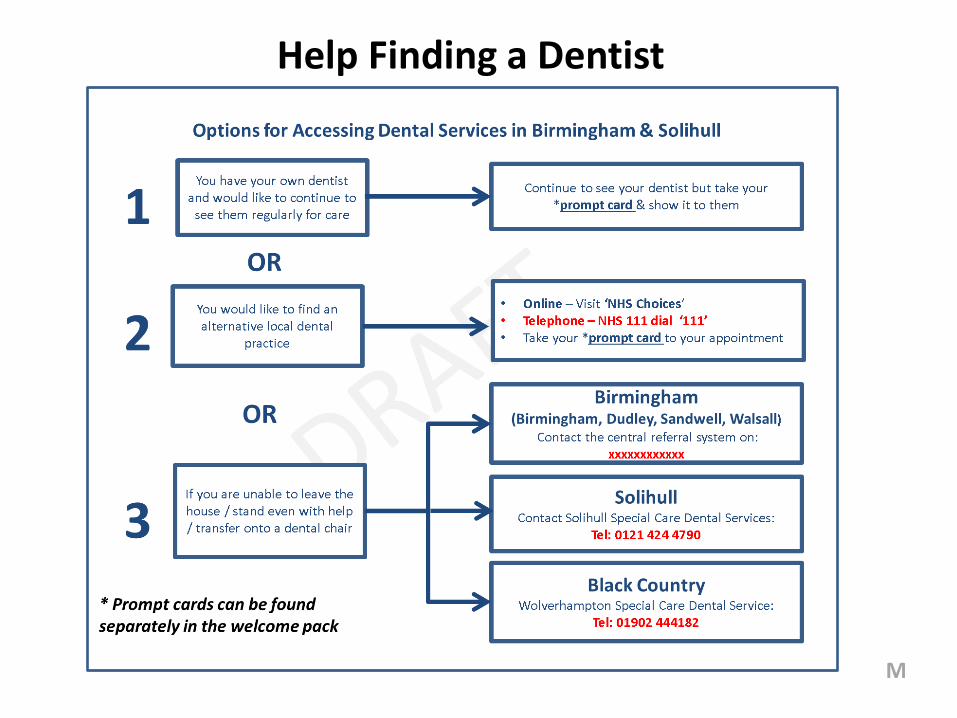
Help Finding a Dentist
M
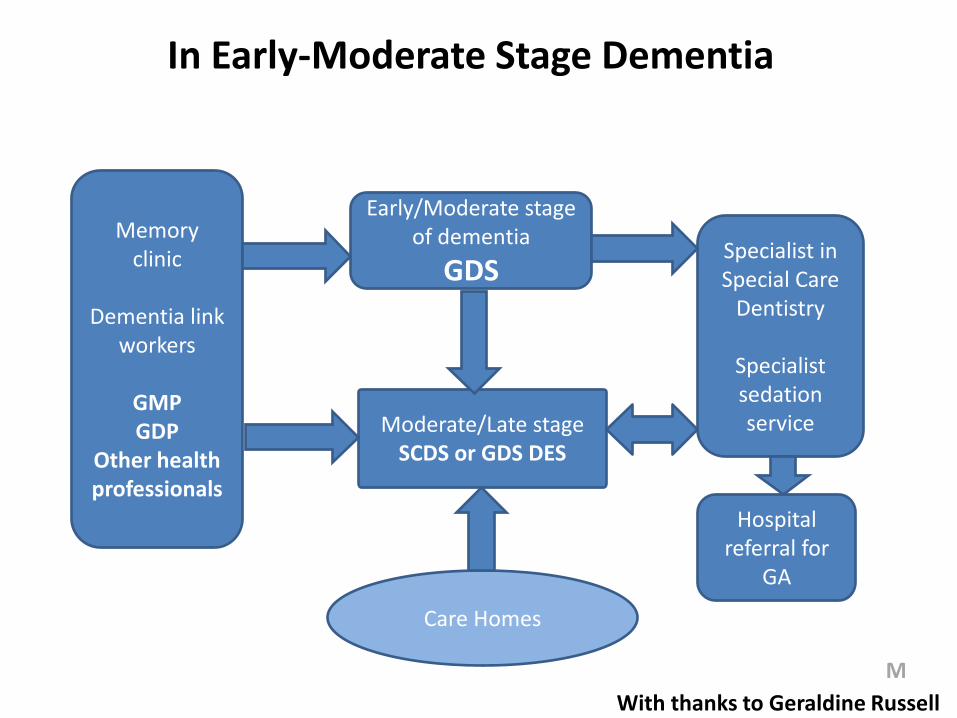
Memory clinic
Dementia link
workers
GMP GDP
Other health professionals
Early/Moderate stage of dementia
GDS
Moderate/Late stage SCDS or GDS DES
Hospital referral for
GA
Specialist in Special Care
Dentistry
Specialist sedation service
Care Homes
With thanks to Geraldine Russell
In Early-Moderate Stage Dementia
M

Evaluating the Patient Materials
Dementia Cafe
Activity Group
M

Progress to-date
• Link between Mental Health Services and Special Care Dentists
• Developed patient resources
• Input to HEWM and National Dementia Working Group
• Developed a training Pack - delivered at Dementia Cafes
• BMAS audit to ensure OH advice part of routine care plan
M
But: How to link the pathway to dementia friendly practices?
• Involvement of NHS England Dental LPN
• Funding for 3yrs to support: – Training 6 local practices to become ‘Dementia Friendly Hubs’
– Link directly into MAS pathway
– Accept signposted pts. / Local dementia ‘champions’ / Input at D.Cafes
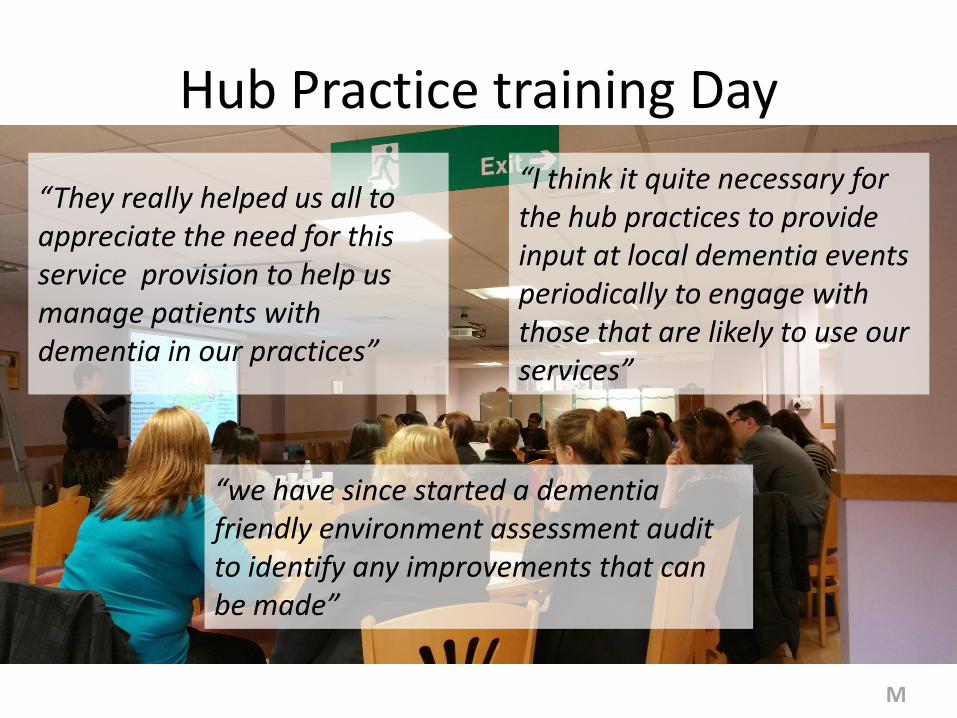
Hub Practice training Day
“They really helped us all to appreciate the need for this service provision to help us manage patients with dementia in our practices”
“we have since started a dementia friendly environment assessment audit to identify any improvements that can be made”
“I think it quite necessary for the hub practices to provide input at local dementia events periodically to engage with those that are likely to use our services”
M
M
Raising Awareness
…and managing expectations!
Challenges
• Mental Health Services – How will we know the pathway is working?
• Patients – How will benefits be demonstrated?
• Hub Practices – What will a successful pilot look like?
– What are the on-going training requirements?
M
Learning Points
• No ‘one-size fits all’ solution
• Dental LPNs and MCNs integral to planning/delivery
(Timely opportunities?) • Different commissioning models
• Utilise existing systems where
possible
• Consider national situation (NHS England, guides for commissioning)
M
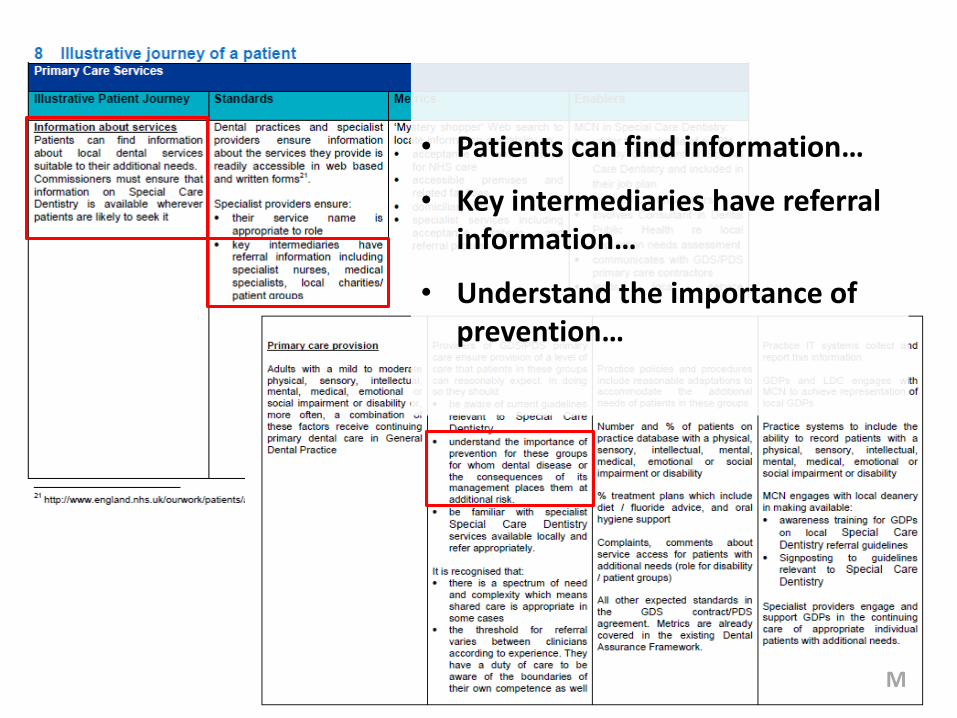
• Patients can find information…
• Key intermediaries have referral information…
• Understand the importance of prevention…
M
Conclusion
• Work in progress
• Similar work around UK
• Shared learning with Worcestershire SCD/MAS
Contact:
THANKS FOR LISTENING