Cold injuries to the lower extremity Matthew Spiva.
39
Cold injuries to the lower extremity Matthew Spiva
-
Upload
hillary-lee -
Category
Documents
-
view
220 -
download
1
Transcript of Cold injuries to the lower extremity Matthew Spiva.

Cold injuries to the lower extremity
Matthew Spiva
Introduction
The purpose of this discussion is to review the signs, symptoms, and treatment of cold injuries of the lower extremity.

Assessing cold injuries
Assess for systemic hypothermia
Neurovascular assessment
HPI: temperature + wind velocity = Wind chill, duration of exposure, and time ellapsed since exposure.
PMH: Tetanus status, antibiotic allergy, alcoholism, drug use, mental status, PVD, smoker.

Discussion
Hypothermia
Raynauds
Trenchfoot/Immersion foot
Chilblains/Pernio
Frost bite
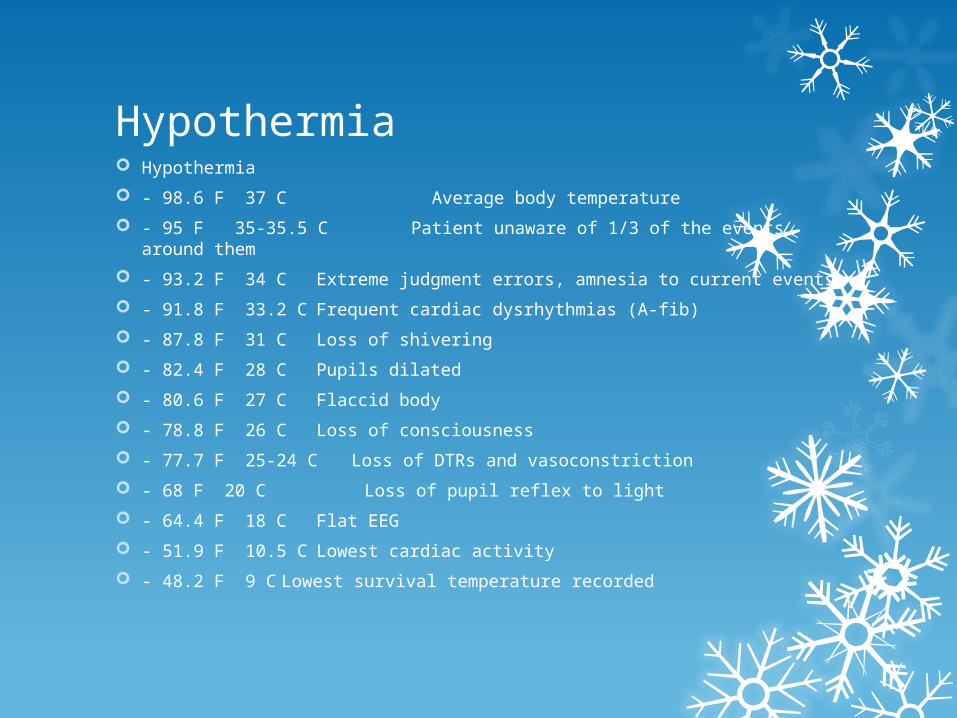
Hypothermia Hypothermia
- 98.6 F 37 C Average body temperature
- 95 F 35-35.5 C Patient unaware of 1/3 of the events around them
- 93.2 F 34 C Extreme judgment errors, amnesia to current events
- 91.8 F 33.2 C Frequent cardiac dysrhythmias (A-fib)
- 87.8 F 31 C Loss of shivering
- 82.4 F 28 C Pupils dilated
- 80.6 F 27 C Flaccid body
- 78.8 F 26 C Loss of consciousness
- 77.7 F 25-24 C Loss of DTRs and vasoconstriction
- 68 F 20 C Loss of pupil reflex to light
- 64.4 F 18 C Flat EEG
- 51.9 F 10.5 C Lowest cardiac activity
- 48.2 F 9 C Lowest survival temperature recorded

Hypothermia
A patient that presents with frostbite may also have hypothermia and it must be considered prior to the treatment of frostbite
The patient with hypothermia may present with: Mild cases
Shivering
Slow mentation
Poor coordination
Moderate to severe
Violent shivering
Muscle rigidity
Stupor
Hypotension
Lowered respiration

http://www.firstaidforeveryone.ie/wp-content/uploads/2011/07/hypothermia-first-aid3.jpg

Hypothermia
Treatment: Slow rewarming performed by colonic irrigation, warmed IV,
Dialysis, and inhalation re-warming
Monitor vital signs and labs for worsening condition

Raynaud’s
http:/
/www.northcoastfootcareblog.com/wp-content/uploads/2008/01/raynauds-2.jpg
Raynaud’s phenomenon
An exaggeration of vasomotor responses to cold or emotional stress
Hyperactivation of the sympathetic nervous system causing extreme vasoconstriction of the peripheral blood vessels, leading to tissue hypoxia
Chronic, recurrent cases of Raynaud’s phenomenon can result in atrophy of the skin, subcutaneous tissues, and muscle. In rare cases it can cause ulceration and even ischemic gangrene
Smoking, hormonal influence, and caffeine all worsen and increase the intensity of the attacks.

http://sammyantha.hubpages.com/hub/Aromatherapy-Blends-Raynauds-phenomenon#
Raynauds Treatment Control cold exposure
Special heated gloves
Meds:
Calcium channel blockers: relax and open up small peripheral blood vessels
nifedipine (Adalat CC, Afeditab CR, Procardia), amlodipine (Norvasc) and felodipine (Plendil)
Alpha blockers: counteract the actions of norepinephrine
prazosin (Minipress) and doxazosin (Cardura)
Vasoldilators:
nitroglycerin cream
losartan (Cozaar), the erectile dysfunction medication sildenafil (Viagra, Revatio), fluoxetine (Prozac, Sarafem)
Avoid: Beta blockers, birth control pills, and vasoconstrictors such as pseudoephedrine
Surgery/procedures:
Sympathetic nerve resection/ablation
Nerve blocks
Amputation

Trenchfoot: Cold + wet prolonged vasoconstriction tissue necrosis
Most commonly found in military personnel, hunters, and fishermen. The foot has been exposed to wet and cold conditions for an extended period of at least 10 hours. In some instances, the area may appear similar to severe frostbite. The affected limb becomes edematous and appears white, waxy, cyanotic, and mottled
Symptoms initially include numbness, tingling, and hypereshtesia
Blistering, swelling, erythema, ecchymosis, and ulceration may occur

http://www.madisonpodiatrist.com/blog/post/war-horse-film-star-got-trench-foot.html

http://trialx.com/g/Trench_Foot-4.jpg
http://trialx.com/g/Trench_Foot-3.jpeg
http://homeinthehills.co.nz
/health.html
http://www.accessmedicine.ca/search/searchAMResultImg.aspx?rootterm=trench+foot&rootID=35918&searchType=1

Trenchfoot
Prevention: Wear dry mixed fiber socks
Treat hyperhidrosis
Keep feet dry
Treatment: Elevate the extremity and gently rewarm the limb resulting
in hyperemia followed by erythema, intense burning and tingling
A post hypothermic phase occurs at 2-6 weeks resulting in cyanosis of the limb
Permanent cold sensitivity can be a sequela of trench foot

Chilblains/Pernio
http://healthndine.com/wp-content/uploads/chilblains.jpg

Chilblains/Pernio
Chilblains are the mildest form of cold injury. Usually, they are found in female patients on the dorsum of the hands and feet and on the face where the skin has been exposed to cold, wet, and windy conditions.
Pruritus and erythematous, dry, rough, and swollen skin are evident. Papules that may later ulcerate may also be present.
Chilblains usually will last the duration of cold weather, with symptoms ceasing on the return of warm weather. Patients have to be reminded to protect any exposed areas and to apply lotion to eliminate the pruritus and rough skin.
Chilblains/Pernio
May be secondary to underlying medical condtions:
-CML
-Anorexia nervosa
-Dysproteinemias
-Macroglobulinemia
-Cryoglobulinemia, cryofibringonemia, cold agglutinins
-Anitphospholipid Ab syndrome
- Raynauds
- SLE

http://www.funscrape.com/Image/31833/Chilblains.html
http://www.funscrape.com/Image/31838/Chilblains.html
http://www.funscrape.com/Image/31834/Chilblains.html
Chilblains/Pernio
Treatment: Warming
Exercise (promotes blood flow)
Nifedipine
Ca+ channel blocker
Relaxes smooth muscle and creates vasodilation
10 to 20 mg PO tid
Wound care if necessary
Avoid nicotine, cold, EtOH

Frostbite
http://carlosdaman.wordpress.com/2009/03/15/pictures-pictures-more-pictures/frostbite-72542211/
Frostbite
Water conducts heat 25 times faster than air, thus a person who has cold and wet feet is more susceptible to frostbite.
Predisposing factors are the African-American population, poor nutritional status, the amount of tissue exposed, tight shoe gear or clothing restricting blood flow, lack of activity, concurrent injury, previous cold injury
Underlying diseases such as diabetes, peripheral vascular disease, and renal failure also predispose one to frostbite.
The pathophysiology of frostbite is thought to occur in the following ways:
1. Slow freezing leads to ice crystal formation in the extra-cellular fluid. (Most cases)
2. Rapid freezing causes ice crystal formation intra-cellularly. Touching the skin to freezing metal can result in this type of freezing.
3. Vasomotor responses to freezing yield vasoconstriction and stasis resulting in increased blood viscosity and coagulation. Perfusion is inadequate.
This + slow freezing = frostbitten tissue

More on Frostbite
Frostbite is a disease of morbidity not mortality
Affects mostly mountaineers, cold weather enthusiasts, soldiers, those who work in the cold, the homeless, and individuals stranded in the cold
Frostnip no permenant tissue damage
Frostbite is 2/2 both immediate cold induced cell death and a more gradual inflammatory process and tissue ischemia.
Fluid and electrolyte fluxes cause lysis of the cell membranes and cell death resulting in inflammation with the release of thromboxane A2, PG F2-alpha, bradykinins, and histamine the end result of which is ischemia and necrosis.
This process is made worse with thawing and refreezing

Frostbite
Symptoms: Firm/hard and cool to the touch
Affected area appears waxy, white, or blotchy blue-gray
Pain, burning, pruritis, but may not be apparent until the body part is warmed
Clumsiness due to joint and muscle stiffness
Profound edema, hemorrhagic and/or serous blisters, necrosis and gangrene may occur
Frostbite Classifications
Like bums, frostbite is classified according to the depth of destruction. Currently, two classifications exist. The first depicts the extent of injury by degrees:
First degree:
Hyperemia and edema are evident. Hard white plaques form after rewarming. The patient experiences pruritus or burning.
This stage is characterized by the absence of blister formation.
Second degree:
Hyperemia with vesicle formation occurs. The skin is red and feels hot and dry after treatment. Swelling occurs, along with desquamation of the blebs after re-warming.
Third degree:
Necrosis of the skin and underlying tissue occurs. Blebs are hemorrhagic. Rewarming leads to severe edema at the 6-day mark.
Anesthesia ensues, followed by aching and throbbing. The necrotic tissue forms an eschar that forms an ulcer after undergoing desquamation.
Fourth degree:
Complete necrosis and loss of tissue occur. Bone can be destroyed. Rewarming causes a mottled or deep red appearance. No edema occurs in the injured area. Gangrene and mummification are evident quickly. Demarcation may take up to 90 days.

Frostbite Classifications
The second classification system, which appears to be gaining widespread support, is described as follows:
Superficial frostbite: This affects the epidermis and dermis. The area is white, but the tissues are resilient when palpated.
Deep frostbite: Not only are the epidermis and dermis affected, but extension to tendons and bone occurs. When the tissue is palpated, there is a lack of resilience. The frostbitten area is stiff. Often, it resembles a piece of frozen meat .

http://www.greatnorthernprepper.com/wp-content/uploads/2012/10/frostbite-feet.jpg

http://www.project-himalaya.com/gallery-everest-frostbite.html

http://doctorrennie.files.wordpress.com/2012/05/frostbite-feet-may-19.jpg

Frostbite Treatment
Usually requires analgesics during thawing
Superficial frostbite (frostnip) can be rewarmed by applying constant warmth with gentle pressure from a warm hand (w/o rubbing) or by placing the affected body part against another part of the body that is warm

Frostbite treatment
Full thickness frostbite is usually treated best by rapid thawing at temperatures slightly above body temperature
Immerse body part in warm water 40-42 C (104 – 107.6 F) until it has returned to normal temperature (approx.. 30 minutes) (i.e. whirlpool)
Keep affected area elevated at room temperature uncovered or with a loose sterile dressing
When one is in the field and a part becomes frostbitten, there should be no rewarming if a chance of refreezing exists. It is better to arrive at a hospital in a frozen state than to refreeze and increase tissue destruction and hypoxia.

Frostbite
Deep frost-bite, which is analogous to a deep burn, may require surgery after 2 or 3 weeks.
Radiographs are obtained to rule out the presence of gas. Technetium bone scans can depict cold spots in the deep frostbitten part that correlate with a poor prognosis for healing.
One should remember this important admonition when treating frostbite: January's frostbite is July's amputation
Amputation or debridement should not be performed until a line of demarcation between viable and dead tissue is established at approximately 3-5 weeks
Blisters and blebs are left intact if they are hemorrhagic.
Clear blisters are débrided and are covered with a non-adherent sterile dressing.
Débridement of necrotic tissue is not performed acutely.
Cloudy blisters are degloved and are treated with local wound care.
Eschars can form, and they may be incised, especially in areas of movement
Medications/Interventions:
Due to vascular thrombosis in addition to regular treatment one may administer heparin and/or tPA as this has been shown to increase favorable outcomes U of U conducted a study from 2001-2006 using tPA and conventional
treatment and compared them to patients who just received conventional therapy. The result was those who received tPA had only a 10% amputation rate compared to 41% in the conventional only group.
Tetanus prohylaxis
NSAIDs good for preventing inflammation
Opiods are necessary for pain control
Hyperbarics were thought not to work previously but recent studies show that there has been some benefit
Pentoxifylline has shown good outcomes when used in animals with frostbite. (Often used in claudication)

Summary of key points Assess for hypothermia and treat accordingly
Raynaud’s – avoid cold climates, keep hands and feet warm, avoid nicotine, EtOH, caffeine, beta blockers, birth control pills, and any vasoconstrictors Treat with warming affected area, heated gloves, Calcium channel
blockers (nifedipine), Alpha blockers (Prazosin), Vasodilators (Nitro cream), nerve blocks, nerve ablation, amputation.
Trenchfoot – Avoid prolonged LE exposure to wet/cold, change socks, treat hyperhydrosis (botox?), elevate and gently rewarm, and wound care as necessary.
Pernio – live somewhere warm, keep exposed areas covered, warm the injured tissue, nifedipine, local wound care if necessary.
Frostbite – Do not thaw if refreezing may occur, requires analgesics while thawing, superficial - apply heat, full thickness - immerse in whirlpool, leave bloody bullae alone, drain clear bullae, deroof cloudy bullae, local wound care, obtain x-rays, heparin, tPA, NSAIDs, opiates, tetanus, hyperbarics, Pentoxifylline. January’s frostbite is July’s amputation

References Kupper T, Steffgen J, Jansing P. Cold exposure during helicopter rescue operations in the Western Alps. Ann
Occup Hyg 2003; 47:7.
http://healthcare.utah.edu/publicaffairs/publications/HSR/PDF/Fall_07/Clinical%20Firsts.pdf
Eric stamps lecture on cold injuries (SMU)
Crawford MC, frostbite, eMedicine, July 18th 2007
Up to date subject search keywords “Cold injuries”
Kroeger K, Janssen S, Niebel W. Frostbite in a mountaineer. Vasa 2004; 33:173.
Atenstaedt RL. Trench foot: the medical response in the first World War 1914-18. Wilderness Environ Med 2006; 17:282.
Twomey JA, Peltier GL, Zera RT. An open-label study to evaluate the safety and efficacy of tissue plasminogen activator in treatment of severe frostbite. J Trauma 2005; 59:1350.
Bruen KJ, Ballard JR, Morris SE, et al. Reduction of the incidence of amputation in frostbite injury with thrombolytic therapy. Arch Surg 2007; 142:546.
Hayes DW Jr, Mandracchia VJ, Considine C, Webb GE. Pentoxifylline. Adjunctive therapy in the treatment of pedal frostbite. Clin Podiatr Med Surg 2000; 17:715.
http://www.mayoclinic.com/health/raynauds-disease/DS00433/DSECTION=treatments-and-drugs
Pocket Podiatrics by Leon Watkins, DPM
http://www.epodiatry.com/chilblains.htm
Reamy BV. Frostbite: review and current concepts. J Am Board Fam Pract 1998; 11:34.
Cauchy E, Marsigny B, Allamel G, et al. The value of technetium 99 scintigraphy in the prognosis of amputation in severe frostbite injuries of the extremities: A retrospective study of 92 severe frostbite injuries. J Hand Surg Am 2000; 25:969.
Twomey JA, Peltier GL, Zera RT. An open-label study to evaluate the safety and efficacy of tissue plasminogen activator in treatment of severe frostbite. J Trauma 2005; 59:1350.
Bruen KJ, Ballard JR, Morris SE, et al. Reduction of the incidence of amputation in frostbite injury with thrombolytic therapy. Arch Surg 2007; 142:546.
Finderle Z, Cankar K. Delayed treatment of frostbite injury with hyperbaric oxygen therapy: a case report. Aviat Space Environ Med 2002; 73:392.
Hayes DW Jr, Mandracchia VJ, Considine C, Webb GE. Pentoxifylline. Adjunctive therapy in the treatment of pedal frostbite. Clin Podiatr Med Surg 2000; 17:715.

Thank You