Cognitive dysfunction: an under-recognized symptom of ... · Significativa influenza sulla storia...
45
ADHD dell’adulto tra bipolarità e ossessività Giuseppe Maina S.C.D.U Psichiatria - A.O.U. San Luigi Gonzaga Università degli Studi di Torino
Transcript of Cognitive dysfunction: an under-recognized symptom of ... · Significativa influenza sulla storia...

ADHD dell’adulto
tra bipolarità e ossessività
Giuseppe Maina
S.C.D.U Psichiatria - A.O.U. San Luigi Gonzaga Università degli Studi di Torino

Adult ADHD and Bipolar Disorder

Adult ADHD and Bipolar Disorder
1. DIAGNOSTIC OVERLAP

Adult ADHD and Bipolar Disorder
1. DIAGNOSTIC OVERLAP
2. COMORBIDITIES
+

1. DIAGNOSTIC OVERLAP

Babcock and Ornstein. Postgraduate Medicine, 2009
European Network Adult ADHD Conference, 2011
ImpatienceImpatience
Mood instabilityMood instability
ForgetfulnessForgetfulness
DistractibilityDistractibility
Initial insomniaInitial insomnia
Inner restlessnessInner restlessness
Low self-esteemLow self-esteem
Over-activityOver-activity
Emotionally unstableEmotionally unstable
InattentionInattention
ImpulsivenessImpulsiveness
Ipo/maniaDepression

Kooij et al, J Att Dis 2012
Mood and anxiety symptoms and ADHD

Neurobiological overlap between ADHD and BD
Rommel et al, Brain Topogr 2016

Reimherr et al, Journal of Clinical Psychiatry 2007
Emotional dysregulation co-varies with ADHD symptoms during treatment response
0
10
20
30
40
50
60
70
80
90
100 p <.001 p <.001p<.001
p=.002
Ch
oe
n's
d
Outcomes for adhd clinical scale as a function of treatment (methylphenidate or placebo)

ADHD and Bipolar Disorder:main differences
Clinical course:
stable Vs recurrent
Onset:
early Vs variable

Adult ADHD and Bipolar Disorder
2. COMORBIDITIES
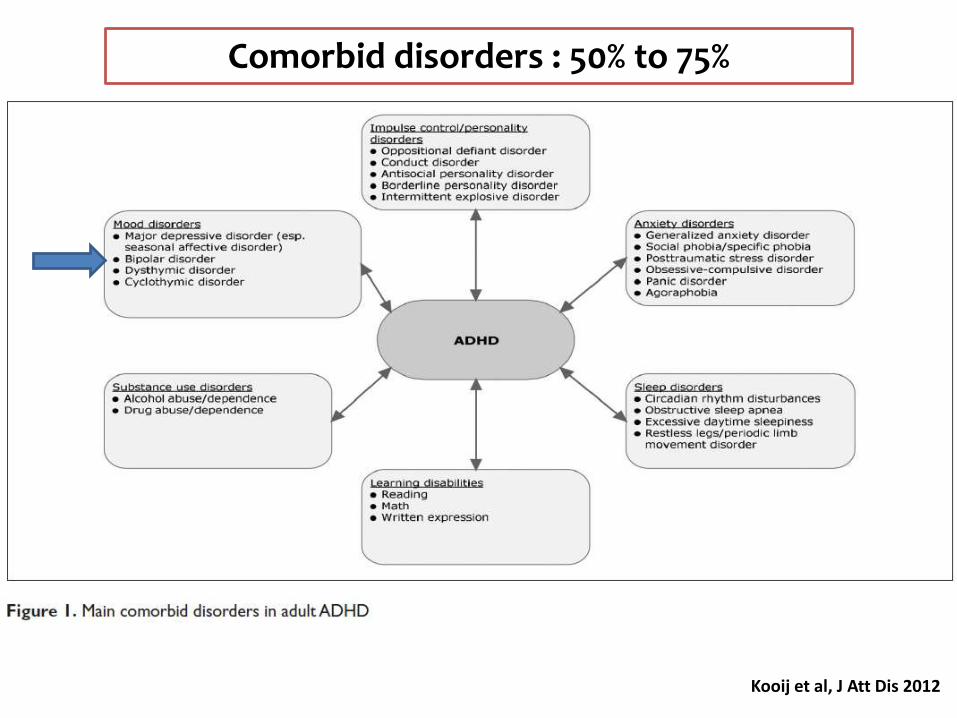
Kooij et al, J Att Dis 2012
Comorbid disorders : 50% to 75%

ADHD
Patients with Bipolar Disorder

Comorbidity of ADHD with other DSM-IV disorders
Kessler et al, Am J Psychiatry 2006

ADHD comorbidity in Bipolar adults
Nieremberg et al, Biol Psychiatry 2005
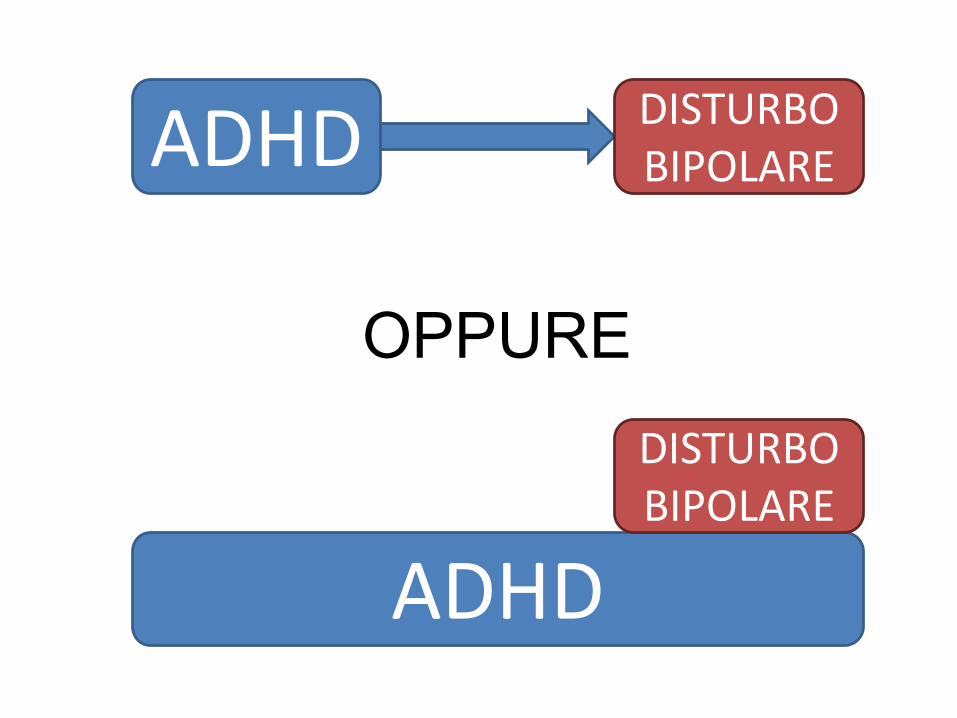
ADHD DISTURBO BIPOLARE
ADHD
DISTURBO BIPOLARE
OPPURE

ADHD comorbidity in Bipolar adults
Nieremberg et al, Biol Psychiatry 2005
0,00%
10,00%
20,00%
30,00%
40,00%
50,00%
60,00%
70,00%
80,00%
90,00%
Bipolar I Bipolar II
Bipolar I vs. Bipolar II
ADHD no ADHD
p= .04
p= .013
N = 1000

Patients with ADHD

X
BIPOLAR
DISORDER
Patients with ADHD
X
X
X X

Hesson and Fowler, Journal of Attention Disorder 2015

0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
Abuso disostanze
Depressionemaggiore
SpettroBipolare
Disturbi diPersonalità
DOC Disturbi diansia
ADHD senzacomorbidità
ADHD dell’adulto (n= 128): comorbidità
Oliva et al, data on file

0%
10%
20%
30%
40%
50%
60%
70%
80%
ANTIDEPRESSIVI BDZ AC VALPROICO SALI DI LITIO ALTRI STAB
ADHD dell’adulto (n= 128): trattamenti in corso
(prima valutazione)
Oliva et al, data on file

Wang et al, Journal of Psychiatric Research 2016
n= 144920

Wang et al, Journal of Psychiatric Research, 2016
La terapia con metilfenidatolong-term (>365 gg)
protegge dallo sviluppo di DB

Etain et al, Australian & New Zealand Journal of Psychiatry, 2016n= 276
ABUSO DI SOSTANZE

Etain et al, Australian & New Zealand Journal of Psychiatry, 2016
NUMERO DI TAC
n= 276

n= 413
Yen et al, Acta Psychiatrica Scandinavica, 2016

Wen-Hsuan Lan et al Journal of Attention Disorders, 2015
ADHD was an independent risk factor for suicide
attempts in BD
n= 500 pts (15 to 24 years old)

Psychosomatics 2013; 54: 437-442
5,20%
5,40%
5,60%
5,80%
6,00%
6,20%
6,40%
6,60%
6,80%
7,00%
current lifetime
ADHD comorbidity in bipolar disorders (n=309)
6.8%
5.8%

Psychosomatics 2013; 54: 437-442
0%
5%
10%
15%
20%
25%
with ADHD without ADHD
At least one suicide attempt
Suicide attempts in bipolar patients with and without ADHD (n=309)
20.6%
14.2%

Psychosomatics 2013; 54: 437-442
Suicide attempts in bipolar patients with and without ADHD (n=309)
0
0,5
1
1,5
2
2,5
with ADHD without ADHD
Number of suicide attempts

Response to mood stabilizer in bipolar adolescents with ADHD
State et al, J Clinical Psychiatry, 2004
lithium vs.
divalproex=
no differences

Viktorin et al, The American Journal of Psychiatry, 2016
n= 2037

Adult ADHD and OCD

Kooij et al, J Att Dis, 2012
Comorbid disorders : 50% to 75%

ADHD comorbidity (definite or probable) in a large sampleof patients with Obsessive-Compulsive Disorder (n=405)
Maina et al, data on file
8
n
1.97Total OCD patients (n=405)
%Lifetime ADHD comorbidity

Çelebi et al, Journal of Attention Disorders, 2016
The Features of comorbidity of childhoodADHD in patients with
Obsessive Compulsive Disorder

Çelebi et al, Journal of Attention Disorders, 2016
The Features of comorbidity of childhoodADHD in patients with
Obsessive Compulsive Disorder

ADHD comorbidity (definite or probable) in a large sampleof pazients with Obsessive-Compulsive Disorder (n=405)
Maina et al, data on file
3
8
n
16.6OCD with tics (n=18)
1.97Total OCD patients (n=405)
%Lifetime ADHD comorbidity

Sheppard et al, Depression and anxiety, 2010
0,00%
5,00%
10,00%
15,00%
20,00%
25,00%
30,00%
35,00%
40,00%
45,00%
Probable or definite hoarding Definite Hoarding
ADHD vs. no ADHD in OCD patients
ADHD no ADHD
p= .01
p= .09

Sheppard et al, Depression and anxiety, 2010

ADHD comorbidity (definite or probable) in a large sampleof pazients with Obsessive-Compulsive Disorder (n=405)
Maina et al, data on file
7
3
8
n
14.6OCD with prominent hoarding (n=48)
16.6OCD with tics (n=18)
1.97Total OCD patients (n=405)
%Lifetime ADHD comorbidity

ADHD nell’adulto e disturbo bipolare
CONCLUSIONI:
1. Ampia sovrapposizione diagnostica
2. Frequente comorbidità lifetime ADHD espone al rischio di disturbo bipolare
3. Significativa influenza sulla storia clinica del
disturbo bipolare
decorso sfavorevole
risposta ai trattamenti

ADHD nell’adulto e DOC
CONCLUSIONI:
1. Associazione significativa con
Disturbo da accumulo
Disturbo da tic
1. Non dati su trattamenti specifici

AMBULATORIO ADHD DELL’ADULTO
SCDU PSICHIATRIA AOU SAN LUIGI GONZAGA
DIRETTORE: PROF. GIUSEPPE MAINA
RESPONSABILE: DOTT. FRANCESCO OLIVA
COLLABORATORI:DOTT. STEFANO BRAMANTEDOTT. CLAUDIO CAREZANA
DOTT. GABRIELE NIBBIODOTT. ALBERTO PORTIGLIATTI POMERI









![Accumulo Summit 2015: Building Aggregation Systems on Accumulo [Leveraging Accumulo]](https://static.fdocuments.net/doc/165x107/55a5e46f1a28ab2d368b47d4/accumulo-summit-2015-building-aggregation-systems-on-accumulo-leveraging-accumulo.jpg)