
cobas b 123 POC system Focus on what matters€¦ · e.g.: cobas b 123 POC, cobas b 221 and cobas b...
12
cobas b 123 POC system Focus on what matters 06265901001 COBAS, COBAS B, COBAS H, COBAS BGE LINK, COBAS INTEGRA, LIGHTCYCLER, SEPTIFAST, URISYS, ACCU-CHEK, COAGUCHEK, and LIFE NEEDS ANSWERS are trademarks of Roche. ©2010 Roche Roche Diagnostics Ltd. CH-6343 Rotkreuz Switzerland www.cobas.com
Transcript of cobas b 123 POC system Focus on what matters€¦ · e.g.: cobas b 123 POC, cobas b 221 and cobas b...
cobas b 123 POC systemFocus on what matters
0626
5901
001
COBAS, COBAS B, COBAS H, COBAS BGE LINK, COBAS INTEGRA, LIGHTCYCLER, SEPTIFAST, URISYS, ACCU-CHEK, COAGUCHEK, and LIFE NEEDS ANSWERS are trademarks of Roche.
©2010 Roche
Roche Diagnostics Ltd.CH-6343 RotkreuzSwitzerlandwww.cobas.com
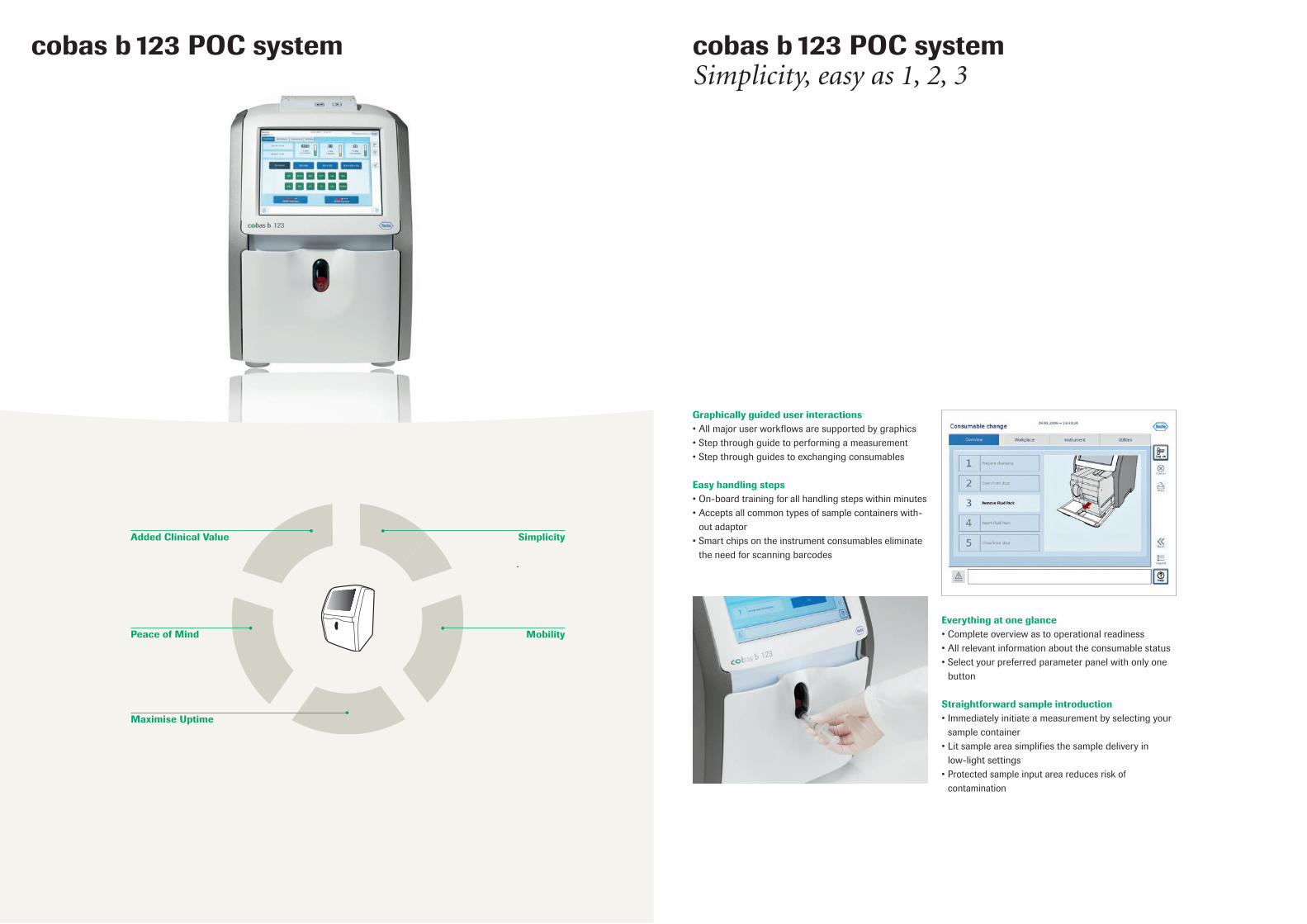
cobas b 123 POC systemSimplicity, easy as 1, 2, 3
Everything at one glance•Completeoverviewastooperationalreadiness•Allrelevantinformationabouttheconsumablestatus•Selectyourpreferredparameterpanelwithonlyone button
Straightforward sample introduction•Immediatelyinitiateameasurementbyselectingyour samplecontainer•Litsampleareasimplifiesthesampledeliveryin low-light settings•Protectedsampleinputareareducesriskof contamination
Graphically guided user interactions•Allmajoruserworkflowsaresupportedbygraphics•Stepthroughguidetoperformingameasurement•Stepthroughguidestoexchangingconsumables
Easy handling steps•On-boardtrainingforallhandlingstepswithinminutes•Acceptsallcommontypesofsamplecontainerswith- outadaptor•Smartchipsontheinstrumentconsumableseliminate the need for scanning barcodes
cobas b 123 POC system
Added Clinical Value
Peace of Mind
Simplicity
Mobility
Maximise Uptime
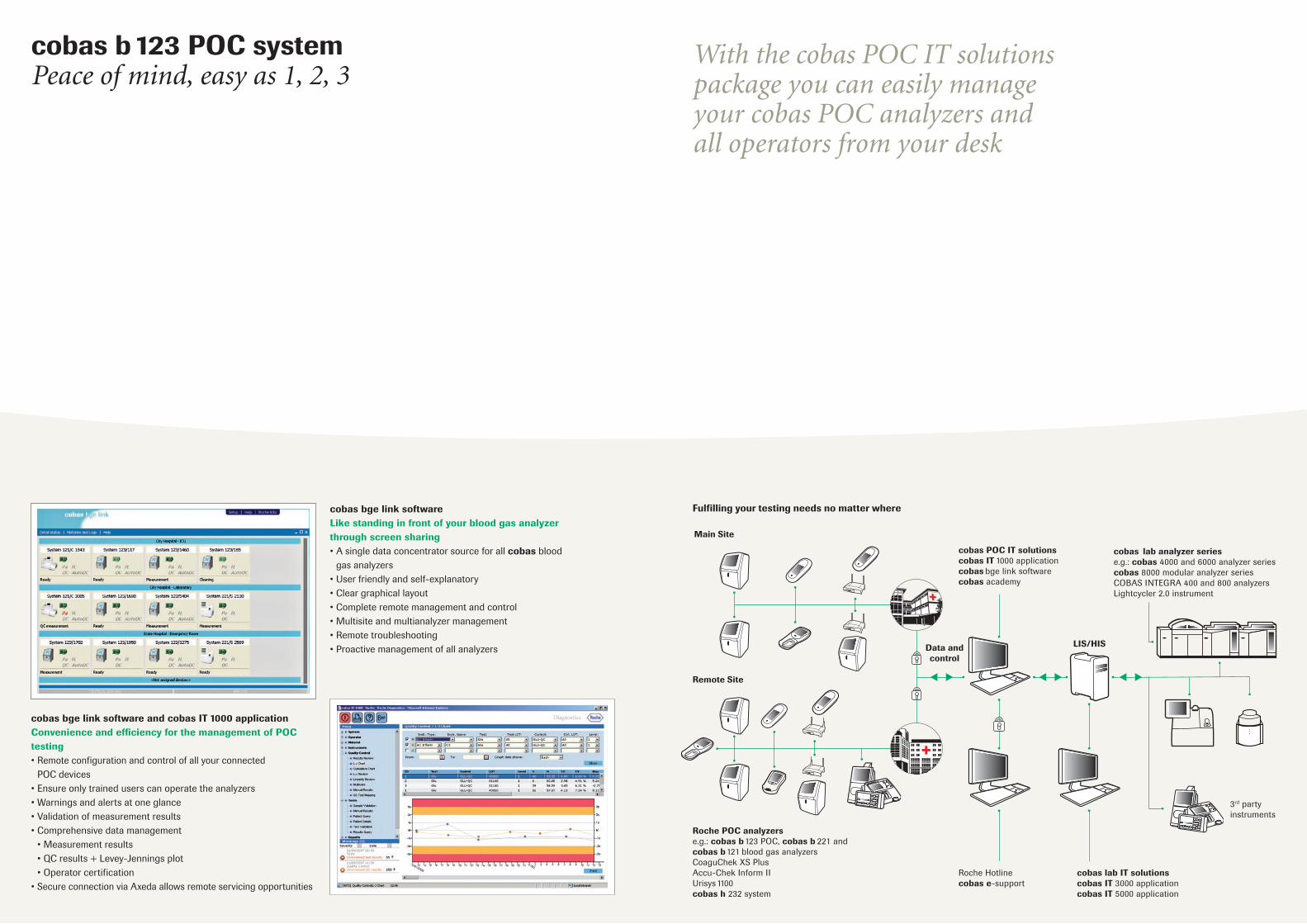
cobas b 123 POC systemPeace of mind, easy as 1, 2, 3
cobas bge link softwareLike standing in front of your blood gas analyzer through screen sharing•Asingledataconcentratorsourceforallcobas blood gasanalyzers•Userfriendlyandself-explanatory•Cleargraphicallayout•Completeremotemanagementandcontrol•Multisiteandmultianalyzermanagement•Remotetroubleshooting•Proactivemanagementofallanalyzers
cobas bge link software and cobas IT 1000 applicationConvenience and efficiency for the management of POC testing•Remoteconfigurationandcontrolofallyourconnected POCdevices•Ensureonlytraineduserscanoperatetheanalyzers•Warningsandalertsatoneglance•Validationofmeasurementresults•Comprehensivedatamanagement •Measurementresults •QCresults+Levey-Jenningsplot •Operatorcertification•SecureconnectionviaAxedaallowsremoteservicingopportunities
Remote Site
Main Site
cobas POC IT solutionscobas IT1000applicationcobas bge link softwarecobasacademy
Data and control
Roche Hotline cobas e-support
LIS/HIS
cobas lab analyzer seriese.g.: cobas4000and6000analyzerseriescobas8000modularanalyzerseriesCOBASINTEGRA400and800analyzersLightcycler2.0instrument
Roche POC analyzerse.g.: cobas b 123 POC, cobas b 221 and cobas b121bloodgasanalyzersCoaguChek XS PlusAccu-Chek Inform IIUrisys1100cobas h232system
3rdpartyinstruments
cobas lab IT solutionscobas IT3000applicationcobas IT5000application
Fulfilling your testing needs no matter where
With the cobas POC IT solutions package you can easily manage your cobas POC analyzers and all operators from your desk

3
1
2
cobas b 123 POC systemMobility, easy as 1, 2, 3
Adapting to your needs•Withflexibleconfigurationsandathroughputofupto30samples
perhourthecobas b123POCsystemcanbeeasilycustomizedtotheclinicalneedsintheICU,ER,NICU,OR,dialysisunitsand ofthelaboratorysetting
•Thefullcobas b123POCparameterpanelincludespH,pCO2, pO2, Na+, K+, Ca2+, Cl-, Hct, Glu, Lac, tHb, SO2, O2Hb, HHb, COHb, MetHb,andbilirubin(tBilirubin).Plusanextensiverangeofcalculatedparameters
•FlexibilityandscalabilityallowsclinicallyrelevantandcostefficientPoint-of-Caretesting
•Allconsumablescanbeinterchangedbetweencobas b 123 POC systemsuptoamaximumoftentimes.
•Optionalmobilecart,UPS(uninteruptablepowersource)backupandwirelessconnectivityenableoperationwhereeverneeded
1 BG=pH,pCO2,pO22 Electrolytes=Na+, K+, Ca2+, Cl -
3 AutoQC=automaticqualitycontrolsystem
Four sensor configurations:•BG1+Hct•BG+Hct+Electrolytes2 •BG+Hct+Electrolytes+Glu•BG+Hct+Electrolytes+Glu+Lac
Four instrument configurations:•withoutAutoQCandCOOX•withAutoQC•withCOOX•withAutoQCandCOOX
Sixpackconfigurations:•WithoutCOOX:200,400,or700samples•WithCOOX:200,400,or700samples
1
2
3
Increase your flexibility
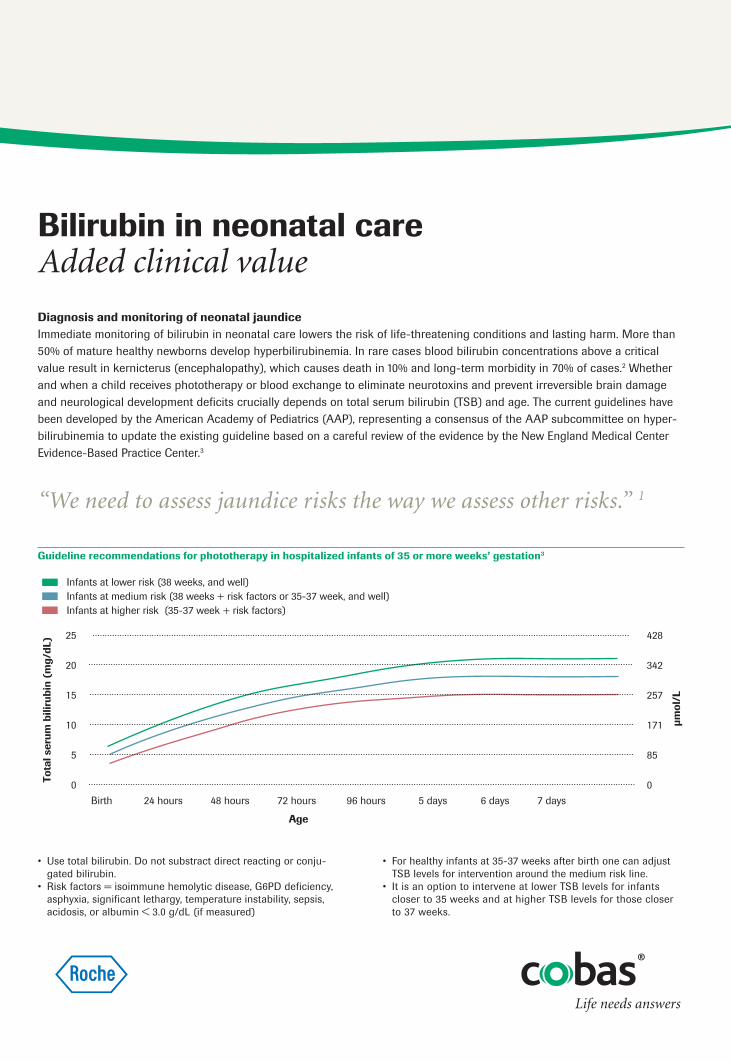
Diagnosis and monitoring of neonatal jaundiceImmediate monitoring of bilirubin in neonatal care lowers the risk of life-threatening conditions and lasting harm. More than 50% of mature healthy newborns develop hyperbilirubinemia. In rare cases blood bilirubin concentrations above a critical value result in kernicterus (encephalopathy), which causes death in 10% and long-term morbidity in 70% of cases.2 Whether and when a child receives phototherapy or blood exchange to eliminate neurotoxins and prevent irreversible brain damage and neurological development deficits crucially depends on total serum bilirubin (TSB) and age. The current guidelines have been developed by the American Academy of Pediatrics (AAP), representing a consensus of the AAP subcommittee on hyper-bilirubinemia to update the existing guideline based on a careful review of the evidence by the New England Medical Center Evidence-Based Practice Center.3
Bilirubin in neonatal care Added clinical value
• Usetotalbilirubin.Donotsubstractdirectreactingorconju-gated bilirubin.
• Riskfactors=isoimmunehemolyticdisease,G6PDdeficiency,asphyxia, significant lethargy, temperature instability, sepsis, acidosis, or albumin < 3.0 g/dL (if measured)
Guideline recommendations for phototherapy in hospitalized infants of 35 or more weeks’ gestation3
“We need to assess jaundice risks the way we assess other risks.” 1
25
20
15
10
5
0
428
342
257
171
85
0
Birth 24 hours 48 hours 72 hours 96 hours 5 days 6 days 7 days
Infants at lower risk (38 weeks, and well)Infants at medium risk (38 weeks + risk factors or 35-37 week, and well)Infants at higher risk (35-37 week + risk factors)
Age
µmol
/L
Tota
l ser
um b
iliru
bin
(mg/
dL)
• Forhealthyinfantsat35-37weeksafterbirthonecanadjustTSB levels for inter vention around the medium risk line.
• ItisanoptiontointerveneatlowerTSBlevelsforinfantscloser to 35 weeks and at higher TSB levels for those closer to 37 weeks.

Bilirubin on cobas b 123 POC systemHuge benefit out of a small sample Bilirubin testing on a blood gas analyzer at the POC is a fast, valid and effective method in implementing the guideline rec-ommendations. 40-70 µL (micro mode*) of whole blood is all the cobas b 123 POC analyzer needs to deliver reliable results within 2 minutes. This small sample volume means signifi-cantly less harm to the newborn. The method is also suitable for monitoring borderline elevated bilirubin levels and treatment response in severe hyperbilirubinemia.
* in development
“Give physicians the tools to implement the guidelines: Risk assess-ment tool at bedside.” 1
COBAS,COBASBandLIFENEEDSANSWERSaretrademarksofRoche.
©2010Roche
RocheDiagnosticsLtd.CH-6343RotkreuzSwitzerlandwww.cobas.com
0626
5901
001
The authors of an AAP technical report conclude high TSB levels exceeding 20 mg/dL to cause kernicterus with an increasing probability when TSB levels are ≥ 30 mg/dL.2,4Unknownisthevariablesusceptibilityofinfants.5 According to the guidelines of the AAP, infants with a TSB level of 25 mg/dL or higher at any time should be admitted immediately and directly to a hos-pital pediatric service for intensive phototherapy.3 To identify and treat endangered children promptly, all neonates need to be monitored. The AAP also recommends a systematic approach to the prevention of severe hyperbilirubinemia and kernicterus, andadvocatestheestablishmentofstandingprotocolsfornursingassessmentofjaundicewhichencompassTSBtesting.3
References 1 AAP 2008. www.aap.org/qualityimprovement/quiin/shb/hyperbili.pdf,
accessedMarch2009.2 Ip,S.,Chung,M.,Kulig,J.,O’Brien,R.,Sege,R.etal.(2004).American
AcademyofPediatrics,TechnicalReport,AnEvidence-BasedReviewofImportant Issues Concerning Neonatal Hyperbilirubinemia. Pediatrics. 114, e130-e153.
3 Maisels,M.J.,Baltz,R.D.,Bhutani,V.K.,Newman,T.B.,Palmer,H.etal.(2004).AmericanAcademyofPediatrics,ClinicalPracticeGuideline,Management of Hyperbilirubinemia in the Newborn Infant 35 or More WeeksofGestation.Pediatrics 114(1),297-316.
4 Newman,T.B.,Liljestrand,P.,Jeremy,R.J.,Ferriero,D.M.,Wu,Y.W.etal.(2006).OutcomesamongNewbornswithTotalSerumBilirubinLevelsof25mgperDeciliterorMore.N Engl J Med. 354,1889-1900.
5 CanadianPaediatricSociety.(2007).Guidelinesfordetection,manage-ment and prevention of hyperbili rubinemia in term and late preterm newborn infants (35 or more weeks’ gestation). Paediatr Child Health. 12 (suppl. B), 1B-12B.
“The best available method for predicting severe hyperbilirubin emia appears to be the use of a timed TSB measurement analyzed in the context of the in fant’s gestational age.” 5

PoC lactate monitoring ensures rapid detection of life-threatening conditions for the right decisions on timeHigh lactate is a marker of severe physiological stress and risk of death. It represents the metabolic changes accompany-ing severe tissue stress and hypoperfusion. Contrary to long-standing belief, lactate is not only a marker of hypoxia but also serves as a metabolic signal.2 The lactate level represents a balance between generation and elimination and so should not be interpreted in isolation from oxygen status and blood pH.3 Measurement of blood lactate concentrations is therefore a vital addition to the blood gas analysis process. Rapid and reliable assay results are essential in ensuring that clinicians detect life-threatening conditions on time and make the right treatment decisions without delay. Repeated measurement of blood lactate concentrations at short intervals enable an evaluation of disease progression, prognosis, and response to treatment.
Vital and versatile: Impact of lactate-testing in critical care and emergenciesSepsis & septic shock: According to the international guidelines for management of severe sepsis and septic shock, 2008, sepsis-induced shock is defined as tissue hypoperfusion (hypotension persisting after initial fluid challenge or blood lactate con-centration > 4 mmol/L).4 Blood lactate concentration is an initial parameter for protocolized resuscitation of patients within the first six hours.4 All patients with a lactate level > 4 mmol/L, whatever their blood pressure is, are entered in the early goal-direct-ed therapy portion of the severe sepsis resuscitation bundle.5 It has been shown that blood lactate levels have a greater prognos-tic value than oxygen-derived variables and that serial lactate levels improve the prognostic value and help guide therapy.6,7
Lactate in critical care and emergenciesAdded clinical value
Lactate as a key parameter: prognosis in sepsis7
“Lactate measurement has evolved as a routine clinical monitor in criti-cally ill patients. It has been suggested that measurement of blood lactate should be routinely available in critical care settings.” 1
1.0
0.8
0.6
0.4
0.2
0.0
0 10 20 30 40 50 60
Lactate clearance ≥10%Lactate clearance <10%
Days
Pro
babi
lity
of s
urvi
val

References 1 Mizok, B.A. (2002). Point-of-Care Testing of Blood Lactate. J Lab Med. 26(1/2), 77-81.2 Levy, B., Gibot, S., Franck, P., Cravoisy, A., Bollaert, P.E. (2005). Relation between
muscle Na+K+ ATPase activity and raised lactate concentrations in septic shock: a prospective study. Lancet. 365 (9462), 871-875.
3 Handy, J. (2006). Lactate – The bad boy of metabolism, or simply misunderstood? Current Anaesthesia & Critical Care. 17, 71-76.
4 Dellinger R.P., Levy, M.M., Carlet, J.M., Bion, J., Parker, M.M. et al. (2008). Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med. 36(1), 296-327.
5 Surviving Sepsis Campaign. www.survivingsepsis.org/bundles/individual_chang-es/serum_lactate, accessed March 2009.
6 Bakker, J., Coffernils, M., Leon, M., Gris, P., Vincent, J.L. (1991). Blood lactate levels are superior to oxygen derived variables in predicting outcome in human septic shock. Chest. 99, 956-962.
7 Nguyen, H.B., Rivers, E.P., Knoblich, B.P., Jacobsen, G., Muzzin, A. et al. (2004). Early lactate clearance is associated with improved outcome in severe sepsis and septic shock. Crit Care Med. 32(8), 1637-1642.
8 Mavric, Z., Zaputović, L., Zagar, D., Matana, A., Smokvina, D. (1991). Usefulness of blood lactate as a predictor of shock development in acute myocardial infarction. Am J Card. 67, 565–568.
Cardiac diseases: Elevated lactate levels predict the development of shock in patients with acute myocardial infarction.8 In patients surviving the first 48 hours after cardiac arrest, serial lactate measurements have a high prognostic value for mortal-ity and neurologic outcome.9 Goal-directed therapy (GDT) based on sequential point of care blood lactate measurements 24 hours after congenital heart surgery sig nificantly reduced the mortality in neonates and especially those infants undergoing higher-risk surgeries.10
Circulatory shock: Lactate levels and clearance have been established as a diagnostic, therapeutic and prognostic marker of tissue hypoxia in circulatory shock.11
Trauma: Lactate values correlate with Injury Severity Score and Glasgow Coma Score for trauma patients entering the ED. Admission lactate improves triage assessment in severely injured patients.12,13
Burn injuries: The inability to clear lactate in the first 48 hours of burn resuscitation differs signi ficantly between survivors and non-survivors of burn injuries. According to study data, mortality in burn patients can be reduced by better control of fluid loading in burn resuscitation.14
Lactate on cobas b 123 POC system: Rapid results within 2 minutesLactate testing on a blood gas analyzer at the point of care is a fast, valid and effective method in implementing the recom-mended rapid turnaround times. PoC blood lactate testing with cobas b 123 analyzer is technology for the titration of therapy. Reliable results are available within 2 minutes to the clinician at the bedside, enabling timely alterations in therapy.
9 Kliegel, A., Losert, H., Sterz, F., Holzer, M., Zeiner, A. et al. (2004). Serial lactate de-terminations for prediction of outcome after cardiac arrest. Medicine (Baltimore). 83(5), 274-279.
10 Rossi, A.F., Khan, D. (2004). Point of care testing: improving pediatric outcomes. Clin Biochem. 37(6), 456-461.
11 Matejovic, M., Radermacher, P., Fontaine, E. (2007). Lactate in shock: a high-octane fuel for the heart? Intensive Care Med. 33, 406-408.
12 Coats, T.J., Smith, J.E., Lockey, D., Russel, M. (2002). Early Increases in Blood Lactate Following Injury. J. R. Army Med Corps. 148, 140–143.
13 Cerovic, O., Golubovi, V., Spec-Marn, A., Kremzar, B., Vidmar, G. (2003). Relation-ship between injury severity and lactate levels in severely injured patients. Intensive Care Med. 29(8), 1300-1305.
14 Jeng, J.C., Lee, K., Jablonski, K. Jordan, M.H. (1997). Serum Lactate and Base Defi-cit Suggest Inadequate Resuscitation of Patients with Burn Injuries: Application of a Point-of-Care Laboratory Instrument. J Burn Care Rehabil. 18, 402–405.
15 Nichols, J.H. (2006). National Academy of Clinical Biochemistry laboratory medicine practice guidelines: evidence based practice for point of care testing. AACC Press.
COBAS, COBAS B and LIFE NEEDS ANSWERS are trademarks of Roche.
© 2010 Roche
Roche Diagnostics Ltd.CH-6343 RotkreuzSwitzerland www.cobas.com
“Overall, the guideline developers recommend that POCT of lactate results be considered as a way to improve outcomes in critical care patients.” 15
0626
5901
001
cobas b 123 POC systemProduct specifications
Measured parameters
Blood gases Specified rangepH 6.5-8.0 pCO2 10-150 mmHg (1.33-19.95 kPa)pO2 10-700 mmHg (1.33-93.10 kPa)ElectrolytesNa+ 100-200 mmol/LK+ 1-15 mmol/LCa2+ 0.1-2.5 mmol/L Cl- 70-150 mmol/LHct 10-75%MetabolitesLactate 1-20 mmol/LGlucose 1-30 mmol/LCO-Oximetry(1)
tHb 4-25 g/dL (2.5-15.5 mmol/L)SO2 30-100%O2Hb 30-100%COHb 0-70%MetHb 0-70%HHb 0-70%Bilirubin (total) 3-50 mg/dL (51.3-855 μmol/L)
Calculated parameters H+, cHCO3
-, ctCO2(P), FO2Hb, BE, BEecf, BB, SO2(1), P50, ctO2,
ctCO2(B), pHst, cHCO3-st, PAO2, AaDO2, a/AO2, avDO2, RI, Shunt,
nCa2+, AG, pHt, H+t, PCO2t, PO2
t, PAO2t, AaDO2
t, a/AO2t, RIt, Hct(c),
MCHC, BO2, BEact, Osmolality, OER, Heart minute volume (Qt),
P/F index
Sample volumeParameter VolumeBG(3) + Hct + Electrolytes(4) + Glu + Lac + COOX 123 μLBG + Hct + Electrolytes + Glu + Lac 102 μLMicro Mode(2) full menu 70 μLMicro Mode full menu without COOX (2) 40 μL
COBAS, COBAS B, LIFE NEEDS ANSWERS and AUTOQC are trademarks of Roche.
© 2010 Roche
Roche Diagnostics Ltd.CH-6343 RotkreuzSwitzerlandwww.cobas.com
0626
5901
001
Sample types Whole blood, aqueous and blood-based QC solutions, plural fluids* and dialysate*
Calibration Interval System calibration Every 24 hours 1 point-calibration Every 60 minutes (programmable 30 or 60 minutes*) 2 point-calibration Every 12 hours are programmable for 4, 8 or 12 hours Data processing Intel, Celeron M, 800 Hz Monitor Built-in color TFT-LCD 10.4 inch flat screen (touchscreen) Thermal printer Built-in, 111 mm width, graphical capability Supported protocols POCT1-A, ASTM Electrical requirements Power rating 100-240 V, 200 W, 50 / 60 Hz autoselecting Ambient temperature +15° to +32°C (59 to 89.6°F) Relative humidity, not condensed 15-85% Power cable A local supply required Options CO-Oximeter 512 nm wavelengths AutoQC Automatic QC system with room for 24 QC ampoules Barcode scanner Hand held or benchtop Mobile cart UPS (Uninterruptible power supply) APC BACK-UPs CS 350 VA USB/SERIAL 230 V Wireless capability W-Lan modem recommended Test certificate UL UL3101-1 CE conformity IVD-Directive 98/79/EC (IEC 1010-1 / EN 61010-1 / EN 61010-2-101) Dimension/weight instrument Width 33 cm Height 47 cm Depth 32 cm Weight (without solutions, without AutoQC) 18 kg
1optional / 2scheduled for development / 3BG = pH, pCO2, pO2 / 4Electrolytes = Na+, K+, Ca2+, CI- / * in development
cobas b 123 POC systemMaximizing uptime, easy as 1, 2, 3
All Roche support elements ensure maximum availability of your analyzer systemsRoche ensures a smooth installation process through thorough preparation• Conductdetailedsitesurvey• CollectITandconnectivityinformation• Coordinatedeliveryinformation• DeterminetrainingrequirementsThesepreparatoryactivitiesallowatimelyandefficientinstallationandimmediateoperatortraining.

COBAS,COBASBandLIFENEEDSANSWERSaretrademarksofRoche.
©2010Roche
RocheDiagnosticsLtd.CH-6343RotkreuzSwitzerlandwww.cobas.com
0626
5901
001
cobas e-support – immediate troubleshooting via remote accesscobas e-services• Improvedanalyzeruptimebyremotediagnosisresolving analyzerissues• Additionaloperatortrainingwithremotesessions
Depot service• Noon-sitevisitsfromservicespecialistsrequired• Immediateanalyzerswapwithnolossofdatabaseor configurationdata
On-site service• ARocheservicespecialistvisitsyouon-site
Hotline support• Trainedhotlinespecialistssupportyouintrouble-shooting andapplicationquestions
Remote expert screen sharing • Immediateanddirectsupportintervention
Remote software updates• Lessinterferencewithdepartmentsroutinebyelectronic softwareupdatesforcobas b123POCsystemsconnected toRoche.
Monitoring system status • Earlyerrordetectionandproactiveserviceintervention
Trouble shooting reports• Acertificatereportsthecobas b123POCsystemcondition
Please contact your local Roche service organization to receive information about local availability of these service elements.
Elements of support/ support options
cobas e-services Remote expert screen sharing
Remote software updates
Monitoring system status
Trouble shooting reports
On-site service
Depot service
Hotline support
✔✔✔
Maximizingavailability


















