Cobalt-chromium sirolimus eluting Sirolimus eluting coronary … · 2019. 11. 21. · BiOSS IM ®...
24
Sirolimus eluting coronary bifurcation stent DISTAL PROXIMAL Long-term effectiveness and safety of the sirolimus-eluting BiOSS LIM ® dedicated bifurcation stent in the treatment of distal left main stenosis: an international registry Robert J. Gil, MD, PhD; Jacek Bil, MD, PhD; Maik J. Grundeken, MD; Luis A. Iñigo Garcia, MD; Dobrin Vassilev, MD, PhD; Adam Kern, MD, PhD; Tomasz Pawłowski, MD, PhD; Joanna J. Wykrzykowska, MD, PhD; Patrick W. Serruys, MD, PhD REFERENCES: Official Journal of EuroPCR and the European Association of Percutaneous Cardiovascular Interventions (EAPCI), Volume 12-Number 10-November 2016; e1246-e1254 Regular drug-eluting stents versus the dedicated coronary bifurcation sirolimus-eluting BiOSS LIM ® stent: the randomised, multicentre, open-label, controlled POLBOS II trial Robert J. Gil, MD, PhD; Jacek Bil, MD, PhD; Maik J. Grundeken, MD; Adam Kern, MD, PhD; Luis A. Iñigo Garcia, MD; Dobrin Vassilev, MD, PhD; Tomasz Pawłowski, MD, PhD; Radoslaw Formuszewicz, MD; Sławomir Dobrzycki, MD, PhD; Joanna J. Wykrzykowska, MD, PhD; Patrick W. Serruys, MD, PhD REFERENCES: Official Journal of EuroPCR and the European Association of Percutaneous Cardiovascular Interventions (EAPCI), Volume 12-Number 11- December 2016; e1404-e1412
Transcript of Cobalt-chromium sirolimus eluting Sirolimus eluting coronary … · 2019. 11. 21. · BiOSS IM ®...

Sirolimus eluting coronary bifurcation stent
Cobalt-chromium sirolimus eluting coronary bifurcation stent
DIS
TAL
PRO
XIM
AL
Long-term effectiveness and safety of the sirolimus-eluting BiOSS LIM® dedicated bifurcation stent in the treatment of distal left main stenosis: an international registryRobert J. Gil, MD, PhD; Jacek Bil, MD, PhD; Maik J. Grundeken, MD; Luis A. Iñigo Garcia, MD; Dobrin Vassilev, MD, PhD; Adam Kern, MD, PhD; Tomasz Pawłowski, MD, PhD; Joanna J. Wykrzykowska, MD, PhD; Patrick W. Serruys, MD, PhD
REFERENCES: Official Journal of EuroPCR and the European Association of Percutaneous Cardiovascular Interventions (EAPCI), Volume 12-Number 10-November 2016; e1246-e1254
Regular drug-eluting stents versus the dedicated coronary bifurcation sirolimus-eluting BiOSS LIM® stent: the randomised, multicentre, open-label, controlled POLBOS II trialRobert J. Gil, MD, PhD; Jacek Bil, MD, PhD; Maik J. Grundeken, MD; Adam Kern, MD, PhD; Luis A. Iñigo Garcia, MD; Dobrin Vassilev, MD, PhD; Tomasz Pawłowski, MD, PhD; Radoslaw Formuszewicz, MD; Sławomir Dobrzycki, MD, PhD; Joanna J. Wykrzykowska, MD, PhD; Patrick W. Serruys, MD, PhD
REFERENCES: Official Journal of EuroPCR and the European Association of Percutaneous Cardiovascular Interventions (EAPCI), Volume 12-Number 11- December 2016; e1404-e1412


BiOSS LIM® in distal LM stenosis
1
C L I N I C A L R E S E A R C HCORONARY INTERVENT IONS
1246
EuroIntervention 2
016
;12
:1246
-125
4 published online ahead of print O
ctober 2
015
D
OI: 10
.42
44
/EIJY1
5M
10_0
5
© Europa Digital & Publishing 2016. All rights reserved.
*Corresponding author: Department of Invasive Cardiology, Central Clinical Hospital of the Ministry of Interior, 137 Woloska Street, 02-507 Warsaw, Poland. E-mail: [email protected]
Long-term effectiveness and safety of the sirolimus-eluting BiOSS LIM® dedicated bifurcation stent in the treatment of distal left main stenosis: an international registry
Robert J. Gil1,2*, MD, PhD; Jacek Bil1, MD, PhD; Maik J. Grundeken3, MD; Luis A. Iñigo Garcia4, MD; Dobrin Vassilev5, MD, PhD; Adam Kern6, MD, PhD; Tomasz Pawłowski1, MD, PhD; Joanna J. Wykrzykowska3, MD, PhD; Patrick W. Serruys7, MD, PhD
1. Department of Invasive Cardiology, Central Clinical Hospital of the Ministry of Interior, Warsaw, Poland; 2. Institute of Experimental and Clinical Medicine, Polish Academy of Science, Warsaw, Poland; 3. Heart Center, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands; 4. Costa del Sol Hospital, Marbella, Spain; 5. Alexandrovska University Hospital, Sofia, Bulgaria; 6. Faculty of Medical Sciences, University of Varmia and Masuria, Olsztyn, Poland; 7. International Centre for Circulatory Health, NHLI, Imperial College London, London, United Kingdom
GUEST EDITOR: Jens Flensted Lassen, MD, PhD; The Heart Centre, Rigshospitalet, University Hospital of Copenhagen, Copenhagen, Denmark
AbstractAims: The aim of this study was to assess prospectively the effectiveness and safety of a new version of the dedicated bifurcation BiOSS stent, the sirolimus-eluting BiOSS LIM, for the treatment of distal left main (LM) stenosis.
Methods and results: This was a prospective international registry which enrolled patients with NSTE-ACS or stable angina. Provisional T-stenting was the mandated strategy. The primary endpoint was the cumulative rate of cardiac death, myocardial infarction (MI) and target lesion revascularisation (TLR) at 12 months. Twelve-month quantitative coronary angiography endpoints included late lumen loss and per-cent diameter stenosis. A total of 74 patients with distal LM stenosis were enrolled. Seventy-three of the 74 patients (aged 67±9 years, 23% women, 20.3% NSTE-ACS, SYNTAX score 22.4±4.4) were success-fully treated with the BiOSS LIM stent, with additional side branch placement of regular DES in 11 patients (14.9%). Periprocedural MI occurred in one (1.4%) patient. The 12-month MACE rate was 9.5% without cardiac death or definite stent thrombosis. TLR and MI rates were 6.8% (n=5) and 2.7% (n=2), respectively.
Conclusions: The use of the BiOSS LIM dedicated bifurcation stent for the treatment of distal LM steno-sis was feasible and safe, with promising long-term clinical effectiveness.
KEYWORDS
• BiOSS LIM®
• dedicated bifurcation stent
• left main (LM) stenosis
• sirolimus-eluting stent
SUBMITTED ON 13/03/2015 - REVISION RECEIVED ON 04/05/2015 - ACCEPTED ON 19/05/2015
C L I N I C A L R E S E A R C HCORONARY INTERVENT IONS
1246
EuroIntervention 2
016
;12
:1246
-125
4 published online ahead of print O
ctober 2
015
D
OI: 10
.42
44
/EIJY1
5M
10_0
5
© Europa Digital & Publishing 2016. All rights reserved.
*Corresponding author: Department of Invasive Cardiology, Central Clinical Hospital of the Ministry of Interior, 137 Woloska Street, 02-507 Warsaw, Poland. E-mail: [email protected]
Long-term effectiveness and safety of the sirolimus-eluting BiOSS LIM® dedicated bifurcation stent in the treatment of distal left main stenosis: an international registry
Robert J. Gil1,2*, MD, PhD; Jacek Bil1, MD, PhD; Maik J. Grundeken3, MD; Luis A. Iñigo Garcia4, MD; Dobrin Vassilev5, MD, PhD; Adam Kern6, MD, PhD; Tomasz Pawłowski1, MD, PhD; Joanna J. Wykrzykowska3, MD, PhD; Patrick W. Serruys7, MD, PhD
1. Department of Invasive Cardiology, Central Clinical Hospital of the Ministry of Interior, Warsaw, Poland; 2. Institute of Experimental and Clinical Medicine, Polish Academy of Science, Warsaw, Poland; 3. Heart Center, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands; 4. Costa del Sol Hospital, Marbella, Spain; 5. Alexandrovska University Hospital, Sofia, Bulgaria; 6. Faculty of Medical Sciences, University of Varmia and Masuria, Olsztyn, Poland; 7. International Centre for Circulatory Health, NHLI, Imperial College London, London, United Kingdom
GUEST EDITOR: Jens Flensted Lassen, MD, PhD; The Heart Centre, Rigshospitalet, University Hospital of Copenhagen, Copenhagen, Denmark
AbstractAims: The aim of this study was to assess prospectively the effectiveness and safety of a new version of the dedicated bifurcation BiOSS stent, the sirolimus-eluting BiOSS LIM, for the treatment of distal left main (LM) stenosis.
Methods and results: This was a prospective international registry which enrolled patients with NSTE-ACS or stable angina. Provisional T-stenting was the mandated strategy. The primary endpoint was the cumulative rate of cardiac death, myocardial infarction (MI) and target lesion revascularisation (TLR) at 12 months. Twelve-month quantitative coronary angiography endpoints included late lumen loss and per-cent diameter stenosis. A total of 74 patients with distal LM stenosis were enrolled. Seventy-three of the 74 patients (aged 67±9 years, 23% women, 20.3% NSTE-ACS, SYNTAX score 22.4±4.4) were success-fully treated with the BiOSS LIM stent, with additional side branch placement of regular DES in 11 patients (14.9%). Periprocedural MI occurred in one (1.4%) patient. The 12-month MACE rate was 9.5% without cardiac death or definite stent thrombosis. TLR and MI rates were 6.8% (n=5) and 2.7% (n=2), respectively.
Conclusions: The use of the BiOSS LIM dedicated bifurcation stent for the treatment of distal LM steno-sis was feasible and safe, with promising long-term clinical effectiveness.
KEYWORDS
• BiOSS LIM®
• dedicated bifurcation stent
• left main (LM) stenosis
• sirolimus-eluting stent
SUBMITTED ON 13/03/2015 - REVISION RECEIVED ON 04/05/2015 - ACCEPTED ON 19/05/2015

BiOSS LIM® in distal LM stenosis
21247
EuroIntervention 2
016
;12
:1246
-125
4
BiOSS LIM® in distal LM stenosis
IntroductionLeft main (LM) coronary artery disease with >50% narrowing is found in 4-6% of all patients undergoing coronary angiogra-phy and is associated with multivessel disease in about 70% of cases1.
The introduction of newer-generation drug-eluting stents (DES) and lessons learned from intravascular ultrasound (IVUS) guidance have significantly improved the results of percutaneous coronary intervention (PCI) treatment of LM disease. Recently, two meta-analyses showed that the primary endpoint of one-year major adverse cardiovascular events (MACE) was non-sig-nificantly different in the PCI group compared to the coronary artery bypass graft (CABG) group (14.5% vs. 11.8%, respec-tively, p=0.11)2,3.
Previous studies have shown that PCI for ostial/mid-shaft lesions was associated with better clinical outcomes than for lesions located in the distal LM, mainly due to a lower need for repeat revascularisations4. However, in most cases atherosclero-sis develops in the distal part of the LM, including the bifur-cation or trifurcation5. Therefore, the optimal treatment is still the subject of debate. Dedicated bifurcation stents (DBS) are one of the proposed solutions. Devices such as the Tryton® (Tryton Medical Inc., Durham, NC, USA) and Axxess™ (Biosensors International Ltd, Singapore, Singapore) stents have already been used in LM treatment6,7.
Previously, we have published clinical data on the paclitaxel-eluting version of the BiOSS® dedicated bifurcation stent (BiOSS Expert®; Balton, Warsaw, Poland) for the treatment of distal LM disease8. The BiOSS stent was further developed and recently a new version eluting sirolimus became available: the BiOSS LIM® (Balton). The main aim of the present study was to assess prospectively the effectiveness and safety of the new sirolimus-eluting BiOSS LIM for the treatment of distal LM disease.
MethodsSTUDY POPULATION AND STUDY DESIGNBetween July and December 2013, patients with distal LM dis-ease who were considered suitable by the Heart Team to undergo PCI were eligible to be enrolled in this registry. Implantations were performed in four centres in Bulgaria, Poland and Spain. The inclusion criteria were: patients with stable coronary artery disease (CAD) or non-ST-segment elevation acute coronary syn-drome (NSTE-ACS), aged ≥18 years who had a de novo coronary distal LM stenosis. The main exclusion criteria were: ST-elevation myocardial infarction (STEMI), Medina 0,0,1 bifurcations, base-line eGFR <30 ml/min/1.73 m2, inability to take dual antiplatelet therapy for 12 months, or a left ventricular ejection fraction ≤30%. Written informed consent was obtained from all patients before cardiac catheterisation. The institutional review board of each par-ticipating centre approved the study protocol.
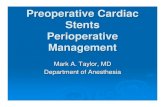
INTERVENTIONAL PROCEDURE, DEVICE DESCRIPTION AND CONCOMITANT MEDICATIONSThe BiOSS LIM is a coronary, balloon-expandable, dedicated bifurcation stent. The platform is made of 316L stainless steel (strut thickness 120 μm) and is coated with a biodegradable poly-mer that elutes sirolimus (drug concentration: 1.4 µg/mm2). The rapid exchange delivery system is compatible with 0.014” guide-wires and 5 Fr guiding catheters. The BiOSS LIM consists of a proximal and a distal part joined together with two connection struts at the middle zone (the length of the connection struts varies from 0.9 to 1.5 mm, depending on the stent size, when the stent is crimped on the balloon) (Figure 1).
The default strategy within this registry consisted of a single stent implantation in the main vessel (MV) - main branch (MB) crossing the side branch (SB). Bifurcation lesions were assessed according to the Medina classification (QCA assessment)9.
Figure 1. BiOSS LIM deployment. A) Distal left main stenosis – pre-procedure view. B) BiOSS LIM positioning with proper location of three markers. C) BiOSS LIM implantation. D) Post-procedure view.

BiOSS LIM® in distal LM stenosis
31248
EuroIntervention 2
016
;12
:1246
-125
4
There was no restriction regarding lesion length. MV predilatation and/or SB predilatation were performed according to the operator’s decision. The stent was then implanted in the MV-MB. Proximal optimisation technique (POT) was left to the operator’s decision. SB rewiring and SB post-dilatation/stent placement were at the discretion of the operator. A stent in the SB was implanted only if there was a proximal residual stenosis greater than 70% after balloon dilatation, a significant flow impairment after MV-MB stenting or a flow-limiting dissection (according to the provisional T-stenting strategy). Optionally, the procedure was finished with final kissing balloon (FKB) dilatation.
Procedures were performed in a standard way via radial or fem-oral access using 6 or 7 Fr guiding catheters. Pharmacological treatment was according to the most recent guidelines.
Troponin I (TnI), creatine kinase (CK) and creatine kinase-myo-cardial band (CK-MB) were measured pre-procedurally and after six and 24 hours post procedure in all patients. Periprocedural myocardial infarction (type 4a) was defined according to the third universal definition10.
FOLLOW-UPClinical follow-up was performed with office visits or by tele-phone at one and 12 months after the index procedure. Adverse events were monitored throughout the study period. Follow-up coronary angiography was performed at 12 months unless it was clinically indicated earlier.
ENDPOINTSThe primary endpoint was the cumulative rate of MACE, consist-ing of cardiac death, myocardial infarction (MI) and repeat revascu-larisation of the target lesion (TLR). Secondary endpoints included cardiac death, all-cause death, MI, TLR, target vessel revascularisa-tion (TVR), stent thrombosis (ST), late lumen loss (LLL), device success and angiographic success. Cardiac death included death resulting from an acute MI, sudden cardiac death, death due to heart failure and death due to cardiac procedures. All deaths were deemed cardiac unless proven otherwise. MI was defined according to the third universal definition10. TLR and TVR were defined according to the Academic Research Consortium definitions.
Device success was defined as successful deployment of the BiOSS LIM stent at the intended site of the target lesion. Angiographic success was defined as an end-procedural MV-MB diameter stenosis less than 20% and SB ostial stenosis less than 70% without significant dissection and flow impairment.
ANGIOGRAPHIC ANALYSISTwo orthogonal projections were chosen to visualise the treated bifurcation. All recordings were performed after intracoronary administration of nitroglycerine (200 μg). Quantitative coronary angiographic (QCA) analysis was performed using the dedi-cated bifurcation software CAAS 5.11 (Pie Medical Imaging BV, Maastricht, The Netherlands). Calibration was performed using the guiding catheter in all cases. The three bifurcation
segments (MV, MB, SB) were analysed separately according to the European Bifurcation Club (EBC) consensus11. The following parameters were reported: lesion length, reference vessel diameter (RVD), minimal lumen diameter (MLD). Percentage diameter ste-nosis (%DS), acute lumen gain (ALG) and LLL were calculated as described previously8. The point of bifurcation (POB, the mid-dle point at the carina level) was determined automatically by the software.
STATISTICAL ANALYSISContinuous variables were presented as mean±standard devia-tion. Categorical data were presented as numbers (%). Continuous variables were compared using an unpaired two-sided Student’s t-test, and categorical data using the χ2 test or Fisher’s exact test, where appropriate. If distribution was not normal (verified with the Shapiro-Wilk test), Wilcoxon signed-rank tests and Mann-Whitney U tests were used. P-values of <0.05 were considered statistically significant. Statistical analyses were performed using R 3.0.2 for OS (R Foundation, Vienna, Austria).
ResultsBASELINE CLINICAL CHARACTERISTICSBetween July and December 2013, 74 patients were enrolled. The baseline characteristics are presented in detail in Table 1. Mean age was 67±9 years. Multivessel disease was diagnosed in 61 patients (82.4%), and there were eight (10.8%) cases of protected LM (i.e., patent grafts on LAD/LCX). The study cohort included was a rela-tively diseased population with 26 (35.1%) patients being diabetic and 41 (55.4%) with a previous myocardial infarction. Fifty-nine patients (79.7%) underwent elective PCI for stable coronary artery disease, while 15 patients presented with unstable angina (n=10, 13.5%) or NSTEMI (n=5, 6.8%).
ANGIOGRAPHIC AND PROCEDURAL CHARACTERISTICSMean SYNTAX score was 22.4±4.4. Lesion characteristics are also presented in Table 1 and Medina classification (on QCA) is presented in Table 2. “True” bifurcation lesions (i.e., Medina 0,1,1; 1,0,1 or 1,1,1) accounted for 56.8% (n=42). The BiOSS LIM stent was implanted from the LM towards the LAD in the majority of cases (90.5%). The main procedural variables are pre-sented in Table 3. Device success rate was 98.6%. There was only one delivery failure in which the stent was deformed due to heavy calcification, but did not fall from the balloon. After safe retrieval of this stent and further predilatation, the patient was successfully treated with a new BiOSS LIM stent. The MV was predilated in half of the cases. In four patients (5.4%) it was necessary to implant a regular DES as second stent in the MB because of a dif-fuse lesion not completely covered by the BiOSS stent (n=1) or because of a distal dissection (n=3). Additional balloon dilatations of the SB were performed in one third of the cases while a conse-quent implantation of a regular DES in the SB was performed in 14.9% of cases (n=11). The rate of POT use was 24.3%, whereas the rate of FKB use was 47.3%.

BiOSS LIM® in distal LM stenosis
41249
EuroIntervention 2
016
;12
:1246
-125
4
BiOSS LIM® in distal LM stenosis
CLINICAL OUTCOMESThere was one (1.4%) periprocedural MI due to a transient SB occlusion. Additionally, five (6.7%) cases of in-hospital increase of TnI level (max 1.2 ng/ml) were registered. These were asymp-tomatic, without ECG changes and did not require a repeat coro-nary angiography (i.e., did not meet the criteria of the third universal definition).
Table 1. Baseline clinical characteristics.
Baseline clinical characteristics n=74 (%)
Age, years 67±9
Women, n (%) 17 (23)
Hypertension 65 (87.8)
Hypercholesterolaemia 63 (85.1)
Diabetes type 2 26 (35.1)
Prior MI 41 (55.4)
Prior PCI 40 (54.1)
CABG 15 (20.3)
Peripheral artery disease 4 (5.4)
Chronic kidney disease 11 (14.9)
EuroSCORE II 1.65±1.4%
Clinical indication for PCI
planned PCI 59 (79.7)
UA 10 (13.5)
NSTEMI 5 (6.8)
STEMI 0
Baseline angiographic characteristics n=74 (%)
SYNTAX score 22.42±4.38
Multivessel disease 61 (82.4)
Functional LIMA on LAD 8 (10.8)
Lesion type A 0
B1 26 (35.2)
B2 36 (48.5)
C 12 (16.3)
CABG: coronary artery bypass graft; LAD: left anterior descending artery; LIMA: left intramammary artery; MI: myocardial infarction; NSTEMI: non-ST-elevation myocardial infarction; PCI: percutaneous coronary intervention; STEMI: ST-elevation myocardial infarction; UA: unstable angina
Table 2. Medina classification changes.
Medina typeBaseline n=74 (%)
Post-procedure n=74 (%)
Follow-up n=63 (%)
1,1,1 19 (25.7) 0 0
1,0,1 12 (16.2) 0 0
0,1,1 11 (14.9) 0 1 (1.6)
1,0,0 15 (20.3) 0 0
1,1,0 10 (13.5) 0 0
0,1,0 7 (9.5) 0 2 (3.2)
0,0,1 0 9 (12.2) 10 (15.9)
0,0,0 0 65 (87.8) 50 (79.3)
Medina classification was based on QCA assessment.
Table 3. Procedural characteristics.
Parameter n=74 (%)Device success 73 (98.6)
MV predilatation 38 (51.4)
SB predilatation 14 (18.9)
Both branches predilatation 9 (12.2)
Nominal stent diameter in MV, mm 4.05±0.32
Nominal stent diameter in MB, mm 3.32±0.33
Nominal stent length, mm 17.57±2.81
SB post-dilatation 26 (35.1)
FKB 35 (47.3)
POT 18 (24.3)
Additional stent in SB* 11 (14.9)
Additional stent in MB* 4 (5.4)
Fluoroscopy time, min 16.7±8.7
Contrast volume, ml 152±56
Vascular access radial/femoral 45 (60.8)/29 (39.2)
Guiding catheter 6 Fr/7 Fr 59 (79.7)/15 (20.3)
*Additional classic drug-eluting stent. FKB: final kissing balloon; MB: main branch; MV: main vessel; POT: proximal optimisation technique; SB: side branch
Table 4. Clinical results.
Endpoints30 days
n=74 (%)12 mo
n=74 (%)
MACE 1 (1.4) 7 (9.5)
Death 0 0
Cardiac death 0 0
MI 1 (1.4) 2 (2.7)
Stroke 0 0
ST 0 0
TLR 0 5 (6.8)
TVR 0 9 (12.2)
PCI in another vessel 2 (2.7) 7 (9.5)
MACE: major adverse cardiovascular events; MI: myocardial infarction; PCI: percutaneous coronary intervention; ST: stent thrombosis; TLR: target lesion revascularisation; TVR: target vessel revascularisation
Clinical follow-up at 12 months was available in all patients (Table 4). The cumulative incidence of MACE was 9.5% (n=7). There were no (cardiac) deaths, no strokes and no stent thrombo-ses. One patient with diffuse in-stent restenosis experienced an MI (12-month MI rate: 2.7%). TLR was performed in five patients (6.8%), two of which were with POBA and three with another DES. Four (5.4%) of them were clinically driven.
QUANTITATIVE CORONARY ANGIOGRAPHY ANALYSISQCA data using bifurcation software are presented in Table 5. The immediate angiographic success rate was 100%. QCA analy-sis revealed that the BiOSS LIM implantation caused a significant increase of MLD and decrease of %DS in the MV as well as in the MB. Both the distal bifurcation angle (between MB and SB) and

BiOSS LIM® in distal LM stenosis
51250
EuroIntervention 2
016
;12
:1246
-125
4
the proximal MV to SB angle were not affected by the procedure. Acute lumen gain was 1.66±0.61 mm in the MV, 0.98±0.54 mm in the MB, and 0.15±0.61 mm in the SB.
Twelve-month follow-up angiography was available in 70 patients (94.6%). Follow-up QCA analysis could be performed in 63 (90%) cases. Seven cases had to be excluded due to inadequate view of the bifurcation, overlapping vessel segments, or presence of angiographic guidewires. LLL was 0.13±0.18 mm in the MV, 0.18±0.12 mm in the MB, and 0.08±0.06 mm in the SB (Table 5).
RESTENOSIS PATTERNIn one case the in-stent restenosis pattern was diffuse, while there was a focal restenosis in four of five (80%) cases. Restenosis was mainly located in the MB and in the SB. In four of five (80%) restenosis cases, a BiOSS LIM stent with a proximal diameter of 3.5 mm was implanted. Moreover, in four of five (80%) restenosis cases there was a second stent implanted in the SB, in which FKB was not performed except for one case. Moreover, POT was not performed in four (80%) restenosis cases (Table 6).
To verify whether the mid zone of the BiOSS LIM stent (at the position of the two joining struts) was a “weak” point prone to
Table 5. Quantitative coronary angiographic data analysis.
Pre-stenting Post-stenting FU
Main vessel
MV lesion length, mm 7.57±2.54
MV – RVD, mm 3.69±0.34 3.66±0.43 3.69±0.45
MV - %DS 56.4±16.4% 10.2±5.1%* 14.8±9%**
MLD, mm 1.62±0.65 3.28±0.41* 3.16±0.51
ALG, mm 1.66±0.61
LLL, mm 0.13±0.18
Main branch
MB lesion length, mm 9.10±5.45
MB – RVD, mm 2.74±0.31 2.82±0.34 2.88±0.33
MB - %DS 43.1±19.4% 10.5±5.2%* 18.3±15.9%**
MLD, mm 1.54±0.49 2.52±0.32* 2.35±0.51**
ALG, mm 0.98±0.54
LLL, mm 0.18±0.12
Side branch
SB lesion length, mm 3.47±3.17
SB – RVD, mm 2.34±0.42 2.22±0.51 2.27±0.53
SB - %DS 38.8±19.7% 28.7±18.2%* 33.9±19%
MLD, mm 1.44±0.56 1.59±0.58 1.51±0.60
ALG, mm 0.15±0.61
LLL, mm 0.08±0.06
Angle MV-SB, degrees 118±32 113±24 112±26
Angle MB-SB, degrees 96±34 91±29 91±31
Contour corrected 12±7.5% 8±5% 9±6%
* p<0.05 for pre vs. post. ** p<0.05 for post vs. FU. ALG: acute lumen gain; FU: follow-up; LLL: late lumen loss; MB: main branch; MLD: minimal lumen diameter; MV: main vessel; RVD: reference vessel diameter; SB: side branch; %DS: % diameter stenosis
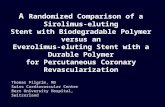
restenosis, we analysed the distance in each stent segment between the MLD and POB using QCA. The middle zone is located bilater-ally 1.2 mm from the POB to the MV-MB. Figure 2 shows a scat-ter plot with the distance from the POB on the horizontal axis and the %DS at the MLD site in each segment on the vertical axis, indicating that the middle zone is not prone to restenosis (i.e., >50% restenosis).
DiscussionThe use of the BiOSS LIM stent for treatment of distal LM steno-sis was associated with a high rate of device and angiographic suc-cess in a cohort with high-risk patients and lesions. At 12-month follow-up, the cumulative MACE rate was 9.5% without cardiac death or definite ST. The TLR rate was 6.8%, while the MI rate was 2.7%.
The vast majority of the included patients had concomitant comorbidities such as hypertension, diabetes, prior MI or prior CABG: these rates were at least comparable to studies with differ-ent DBS6,7 as well as to those in the paper by Bil et al analysing the performance of the BiOSS Expert stent in distal LM stenosis8.
It is worth mentioning that the implantation success rate of the BiOSS LIM stent in the current registry seems to be superior to other DBS in non-LM bifurcations7,12-17 as well as in LM bifurca-tions6. This suggests that the BiOSS stent is a user-friendly device. This might be explained by the lack of issues such as guidewire criss-crossing, improper device orientation or larger device pro-files. Moreover, there was a relatively lower rate of SB stent implantation (14.9% of cases) than in other studies (30-50%)6,12,15. This might have been caused by the fact that this stent may provoke less carina displacement, because of the specific design of the BiOSS stent (with differences in proximal and distal diam-eters), adapting to the natural bifurcation geometry. However,
Table 6. TLR cases.
No. 1. 2. 3. 4. 5.
Time to TLR, months 6 9 11 6 12
Type focal focal focal diffuse focal
BiOSS stent diameter, mm 3.5×3 3.5×2.75 3.5×3 3.5×2.75 4.25×3.75
BiOSS stent length, mm 18 18 15 18 18
FKB + – + – +
POT – – – + –
DES in SB + – + + +
Medina type at baseline 0,1,1 1,0,1 1,0,1 1,0,1 1,1,1
Medina type at FU 0,0,1 0,1,0 0,0,1 0,1,1 0,0,1
MLD-POB in MV at FU, mm – – – – –
MLD-POB in MB at FU, mm – 2.31 – 4.09 –
MLD-POB in SB at FU, mm 3.4 – 4.3 0.84 5.02
Treatment DES POBA DES DES POBA
DES: drug-eluting stent; FKB: final kissing balloon; FU: follow-up; MB: main branch; MLD-POB: distance between minimal lumen diameter and point of bifurcation in cases with %DS ≥50%; MV: main vessel; POBA: plain old balloon angioplasty; POT: proximal optimisation technique; SB: side branch

BiOSS LIM® in distal LM stenosis
61251
EuroIntervention 2
016
;12
:1246
-125
4
BiOSS LIM® in distal LM stenosis
the lower SB stenting rate might also be explained by the lower rate of side branch involvement, which was 56.8% on QCA in our study6,18-20. No apparent difficulties with rewiring of the SB were observed in our study, confirming the hypothesis that the BiOSS LIM stent is well-suited to the provisional T-stenting strategy20.
In the present paper, we found less periprocedural MI (1.4%) and increased levels of TnI (6.7%) compared to those we found in the BiOSS Expert LM registry (15.1% in-hospital increase of TnI, of which 9.4% met the criteria of periprocedural MI)8, which might be explained by the more aggressive protocol with higher rates of FKB used in the previous study.
The MACE rate in our current study was 9.5%, and the rate of TLR was 6.8%. In the first-in-man BiOSS LIM registry, these rates were 11.7% (MACE) and 8.3% (TLR)21; in the BiOSS Expert stent in LM study the rates were both 9.3%8. The somewhat higher rates of MACE and TLR in the FIM BiOSS LIM registry com-pared to the present paper might be explained by the difference in sirolimus concentration of the current BiOSS LIM stent. Initially, the concentration of sirolimus was 1 µg/mm2, while the concen-tration of the current version is 1.4 µg/mm2. This hypothesis is supported by the late lumen loss values obtained in the currently presented population. The LLL values we found in the current reg-istry (MV: 0.13 mm, MB: 0.18 mm, SB: 0.08 mm) were smaller than those obtained in the BiOSS LIM registry in non-LM lesions (MV: 0.35 mm, MB: 0.34 mm, SB: 0.18 mm)21 as well as in the paclitaxel-eluting BiOSS Expert in LM study (MV: 0.20 mm,
MB: 0.26 mm, SB 0.13 mm)8. These data might also suggest that the change of the drug (from paclitaxel to sirolimus) is associated with lower LLL and that the potential benefit of BiOSS over con-ventional DES might be greater in the LM (with more significant differences in diameters between the MV and the MB) than in non-LM bifurcation lesions22.
The TLR rate was comparable to other studies with values within the range of 6.6%-12%6,7,14-16. However, in other studies there were higher rates of predilatation and post-dilatation, as well as FKB7,12-16. Worth mentioning is the fact that the complexity of the coronary anatomy (SYNTAX score 22.4±4.4) was higher in our study compared to other trials6. Moreover, in the original paper of Serruys et al, the 12-month cumulative rate of MACE in a pop-ulation of patients with low SYNTAX score (0-22) was 14.7% and with intermediate SYNTAX score (23-32) was 16.7%1. A recent study by Moynagh et al showed that the endpoint rate, defined as target vessel failure (cardiac death, target vessel MI, and clinically driven TLR), in LM with PES stenting was 16.3% and with EES stenting 7.6%23. Compared to these historical cohorts, the results of the BiOSS LIM we found seem to be favourable, although ran-domised data are needed to prove that.
Worth stressing is the fact that our LM study population was of intermediate to high complexity. To summarise the criteria for complex LM bifurcation lesions, we can use criteria proposed by Chen et al in the DEFINITION trial, which are as follows: Medina 1,1,1/0,1,1 with side branch diameter minimally 2.5 mm, side
Figure 2. Restenosis pattern. A) Bifurcation scheme showing the mean distance between POB and MLD location at follow-up. B) Scatter plot showing no binary restenosis cases in the middle zone of the stent. MB: main branch; MLD: minimal lumen diameter; MV: main vessel; POB: point of bifurcation; SB: side branch

BiOSS LIM® in distal LM stenosis
71252
EuroIntervention 2
016
;12
:1246
-125
4
branch %DS ≥70% as well as SB lesion length ≥10 mm. Although the rate of true bifurcation was higher in the TRYTON LM reg-istry (84% vs. 57%), in our study the SYNTAX score was higher (20 vs. 23 points)24.
Importantly, the pattern of restenosis did not reveal the middle zone (with only the two connection struts) to be the “weak point” of the BiOSS LIM stent. The MLD sites were located significantly fur-ther away from the POB at follow-up than pre-procedure (Figure 2). The restenosis cases were more frequently observed in stents with smaller nominal parameters (>50% restenosis in stents with proxi-mal diameter ≤3.75 mm vs. >3.75 mm was 16.7% vs. 5.6%, respec-tively). Apart from the smaller nominal stent diameter, restenosis was associated with double stenting and the low rate of FKB and POT. Interestingly, the same pattern of restenosis was observed in the BiOSS Expert stent in LM registry8. These results were in agreement with the results of the NORDIC 3 study, in which FKB reduced angiographic side branch restenosis, especially in patients with true bifurcation lesions25 as well as with the results of the POLBOS I study, in which POT in the BiOSS group was associated with a lower rate of TLR26. The POT technique ensures better stent apposition in the MV, and improves the flow to the SB. This tech-nique is recommended by the EBC27. Moreover, Kim et al as well as others have shown that the one-stent technique is better than the two-stent technique in distal LM treatment28,29.
QCA analyses were performed with dedicated bifurcation soft-ware. Dedicated bifurcation 2D QCA software is recommended since it was proven to be superior to straight vessel QCA applied in bifurcations30. Furthermore, a recent study has shown excellent inter-observer variability when using this software, even in dis-tinct core labs31. Dedicated software enables integrated assessment of the reference function including the MV step-down, measure-ment of angulations between vessels and reporting in segmental models. Compared with the single-vessel analysis we performed in the BiOSS Expert stent in LM registry8, it enabled us to eval-uate the MLD site relative to the POB. Furthermore, it allowed a more detailed analysis of bifurcation segments and angles.
LimitationsThe present study has the limitations of a registry. These cases are selected and therefore may not reflect an “all-comer” LM bifur-cation lesion population. There was no control group to compare the use of this dedicated bifurcation stent and stenting with other devices and techniques. Moreover, the number of patients enrolled in the registry was relatively low, and more studies, including ran-domised trials, are needed to draw more definitive conclusions. QCA was not possible in 100% of the cohort for the reasons explained above. The use of intravascular imaging (IVUS) tech-niques was not available in the majority of cases and not system-atically analysed.
ConclusionsThe use of the BiOSS LIM stent for treatment of distal LM ste-nosis is feasible and results in good acute angiographic results.
The safety of the procedure and 12-month clinical outcome are acceptable in this high-risk PCI group. At 12-month follow-up, the cumulative MACE rate was 9.5% with no cardiac death or defi-nite stent thrombosis. The TLR rate was 6.8% (n=5) and the MI rate was 2.7% (n=2). The 12-month QCA results of the MB were excellent and comparable with LLL values of best-in-class DES in non-bifurcation lesions.
Impact on daily practiceThis report has shown that implantation of the dedicated bifur-cation BiOSS LIM stent in distal left main stenosis in patients with a moderate SYNTAX score is safe and effective. Also, these results suggest that the sirolimus-eluting BiOSS LIM stent has better results than the paclitaxel-eluting BiOSS Expert stent. This stent might pose an interesting option in coronary bifurcation treatment, especially when there is a large differ-ence in the diameter between the main vessel and the main branch.
Guest EditorThis paper was guest edited by Jens Flensted Lassen, MD, PhD, The Heart Centre, Rigshospitalet, University Hospital of Copenhagen, Copenhagen, Denmark.
Conflict of interest statementR.J. Gil was the medical consultant of the Balton Company. The other authors have no conflicts of interest to declare. The Guest Editor has no conflicts of interest to declare.
References 1. Serruys PW, Morice MC, Kappetein AP, Colombo A, Holmes DR, Mack MJ, Stahle E, Feldman TE, van den Brand M, Bass EJ, Van Dyck N, Leadley K, Dawkins KD, Mohr FW; SYNTAX Investigators. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360:961-72. 2. Capodanno D, Stone GW, Morice MC, Bass TA, Tamburino C. Percutaneous coronary intervention versus coronary artery bypass graft surgery in left main coronary artery disease: a meta-analysis of randomized clinical data. J Am Coll Cardiol. 2011;58:1426-32. 3. Ferrante G, Presbitero P, Valgimigli M, Morice MC, Pagnotta P, Belli G, Corrada E, Onuma Y, Barlis P, Locca D, Eeckhout E, Di Mario C, Serruys PW. Percutaneous coronary intervention versus bypass surgery for left main coronary artery disease: a meta-analysis of randomised trials. EuroIntervention. 2011;7:738-46. 4. Naganuma T, Chieffo A, Meliga E, Capodanno D, Park SJ, Onuma Y, Valgimigli M, Jegere S, Makkar RR, Palacios IF, Costopoulos C, Kim YH, Buszman PP, Chakravarty T, Sheiban I, Mehran R, Naber C, Margey R, Agnihotri A, Marra S, Capranzano P, Leon MB, Moses JW, Fajadet J, Lefevre T, Morice MC, Erglis A, Tamburino C, Alfieri O, Serruys PW, Colombo A. Long-term

BiOSS LIM® in distal LM stenosis
81253
EuroIntervention 2
016
;12
:1246
-125
4
BiOSS LIM® in distal LM stenosis
clinical outcomes after percutaneous coronary intervention for ostial/mid-shaft lesions versus distal bifurcation lesions in unpro-tected left main coronary artery: the DELTA Registry (drug-eluting stent for left main coronary artery disease): a multicenter registry evaluating percutaneous coronary intervention versus coronary artery bypass grafting for left main treatment. JACC Cardiovasc Interv. 2013;6:1242-9. 5. Morice MC, Serruys PW, Kappetein AP, Feldman TE, Stahle E, Colombo A, Mack MJ, Holmes DR, Torracca L, van Es GA, Leadley K, Dawkins KD, Mohr F. Outcomes in patients with de novo left main disease treated with either percutaneous coronary intervention using paclitaxel-eluting stents or coronary artery bypass graft treatment in the Synergy Between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery (SYNTAX) trial. Circulation. 2010;121:2645-53. 6. Magro M, Girasis C, Bartorelli AL, Tarantini G, Russo F, Trabattoni D, D’Amico G, Galli M, Gomez Juame A, de Sousa Almeida M, Simsek C, Foley D, Sonck J, Lesiak M, Kayaert P, Serruys PW, van Geuns RJ. Acute procedural and six-month clini-cal outcome in patients treated with a dedicated bifurcation stent for left main stem disease: the TRYTON LM multicentre registry. EuroIntervention. 2013;8:1259-69. 7. Hasegawa T, Ako J, Koo BK, Miyazawa A, Sakurai R, Chang H, Dens J, Verheye S, Grube E, Honda Y, Fitzgerald PJ. Analysis of left main coronary artery bifurcation lesions treated with biolimus-eluting DEVAX AXXESS plus nitinol self-expand-ing stent: intravascular ultrasound results of the AXXENT trial. Catheter Cardiovasc Interv. 2009;73:34-41. 8. Bil J, Gil RJ, Vassilev D, Rzezak J, Kulawik T, Pawlowski T. Dedicated bifurcation paclitaxel-eluting stent BiOSS Expert® in the treatment of distal left main stem stenosis. J Interv Cardiol. 2014;27:242-51. 9. Medina A, Suarez de Lezo J, Pan M. [A new classification of coronary bifurcation lesions]. [Article in Spanish] Rev Esp Cardiol. 2006;59:183. 10. Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD. Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction, Katus HA, Lindahl B, Morrow DA, Clemmensen PM, Johanson P, Hod H, Underwood R, Bax JJ, Bonow RO, Pinto F, Gibbons RJ, Fox KA, Atar D, Newby LK, Galvani M, Hamm CW, Uretsky BF, Steg PG, Wijns W, Bassand JP, Menasche P, Ravkilde J, Ohman EM, Antman EM, Wallentin LC, Armstrong PW, Simoons ML, Januzzi JL, Nieminen MS, Gheorghiade M, Filippatos G, Luepker RV, Fortmann SP, Rosamond WD, Levy D, Wood D, Smith SC, Hu D, Lopez-Sendon JL, Robertson RM, Weaver D, Tendera M, Bove AA, Parkhomenko AN, Vasilieva EJ, Mendis S. Third universal definition of myocardial infarction. Circulation. 2012;126:2020-35. 11. Louvard Y, Thomas M, Dzavik V, Hildick-Smith D, Galassi AR, Pan M, Burzotta F, Zelizko M, Dudek D, Ludman P, Sheiban I, Lassen JF, Darremont O, Kastrati A, Ludwig J, Iakovou I, Brunel P, Lansky A, Meerkin D, Legrand V, Medina A, Lefevre T.
Classification of coronary artery bifurcation lesions and treatments: time for a consensus! Catheter Cardiovasc Interv. 2008;71:175-83. 12. Costa RA, Abizaid A, Abizaid AS, Garcia del Blanco B, Berland J, Petrov I, Brenot P, van Guens RJ, Royer T, Rubino P, Lesiak M, Fajadet J; BIPAX Investigators. Procedural and early clinical outcomes of patients with de novo coronary bifurcation lesions treated with the novel Nile PAX dedicated bifurcation poly-mer-free paclitaxel coated stents: results from the prospective, mul-ticentre, non-randomised BIPAX clinical trial. EuroIntervention. 2012;7:1301-9. 13. Del Blanco BG, Marti G, Bellera N, Otaegui I, Serra V, Ferreira I, Domingo E, Angel J, Candell J, Garcia-Dorado D. Clinical and procedural evaluation of the Nile Croco® dedicated stent for bifurcations: a single centre experience with the first 151 consecutive non-selected patients. EuroIntervention. 2011;7:216-24. 14. Onuma Y, Muller R, Ramcharitar S, van Geuns RJ, Louvard Y, Morel MA, Morice MC, Davis R, Kaplan AV, Lefevre T, Grube E, Serruys PW. Tryton I, First-In-Man (FIM) study: six month clinical and angiographic outcome, analysis with new quantitative coronary angiography dedicated for bifurcation lesions. EuroIntervention. 2008;3:546-52. 15. Ormiston JA, Lefevre T, Grube E, Allocco DJ, Dawkins KD. First human use of the TAXUS Petal paclitaxel-eluting bifurcation stent. EuroIntervention. 2010;6:46-53. 16. Verheye S, Ramcharitar S, Grube E, Schofer JJ, Witzenbichler B, Kovac J, Hauptmann KE, Agostoni P, Wiemer M, Lefevre T, Spaargaren R, Serruys PW, Garcia-Garcia HM, van Geuns RJ. Six-month clinical and angiographic results of the STENTYS® self-apposing stent in bifurcation lesions. EuroIntervention. 2011;7:580-7. 17. Grundeken MJ, Asgedom S, Damman P, Lesiak M, Norell MS, Garcia E, Bethencourt A, Woudstra P, Koch KT, Vis MM, Henriques JP, Onuma Y, Foley DP, Bartorelli AL, Stella PR, Tijssen JG, de Winter RJ, Wykrzykowska JJ. Six-month and one-year clinical outcomes after placement of a dedicated coronary bifurcation stent: a patient-level pooled analysis of eight registry studies. EuroIntervention. 2013;9:195-203. 18. Vassilev D, Gil R, Milewski K. Bifurcation Optimisation Stent System (BiOSS Lim) with sirolimus elution: results from por-cine coronary artery model. EuroIntervention. 2011;7:614-20. 19. Gil RJ, Vassilev D, Michalek A, Kern A, Formuszewicz R, Dobrzycki S, Wojcik J, Lesiak M, Kardaszewicz P, Lekston A. Dedicated paclitaxel-eluting bifurcation stent BiOSS® (bifurcation optimisation stent system): 12-month results from a prospective registry of consecutive all-comers population. EuroIntervention. 2012;8:316-24. 20. Gil RJ, Bil J, Michalek A, Vassiliev D, Costa RA. Comparative analysis of lumen enlargement mechanisms achieved with the bifurcation dedicated BiOSS stent versus classical coronary stent implantations by means of provisional side branch stenting strat-egy: an intravascular ultrasound study. Int J Cardiovasc Imaging. 2013;29:1667-76.

BiOSS LIM® in distal LM stenosis
91254
EuroIntervention 2
016
;12
:1246
-125
4
21. Gil RJ, Bil J, Vassiliev D, Inigo Garcia LA. First-in-man study of dedicated bifurcation sirolimus-eluting stent: 12-month results of BiOSS LIM® Registry. J Interv Cardiol. 2015;28:51-60. 22. Vassilev D, Mateev H, Alexandrov A, Karamfiloff K, Gil RJ. Double bifurcation optimization stent system technique for left main stenosis. J Interv Cardiol. 2014;27:570-3. 23. Moynagh A, Salvatella N, Harb T, Darremont O, Boudou N, Dumonteil N, Lefevre T, Carrie D, Louvard Y, Leymarie JL, Chevalier B, Morice MC, Garot P. Two-year outcomes of everolimus vs. paclitaxel-eluting stent for the treatment of unprotected left main lesions: a propensity score matching comparison of patients included in the French Left Main Taxus (FLM Taxus) and the LEft MAin Xience (LEMAX) registries. EuroIntervention. 2013;9:452-62. 24. Chen SL, Sheiban I, Xu B, Jepson N, Paiboon C, Zhang JJ, Ye F, Sansoto T, Kwan TW, Lee M, Han YL, Lv SZ, Wen SY, Zhang Q, Wang HC, Jiang TM, Wang Y, Chen LL, Tian NL, Cao F, Qiu CG, Zhang YJ, Leon MB. Impact of the complexity of bifurca-tion lesions treated with drug-eluting stents: the DEFINITION study (Definitions and impact of complEx biFurcation lesIons on clinical outcomes after percutaNeous coronary IntervenTIOn using drug-eluting steNts). JACC Cardiovasc Interv. 2014;7:1266-76. 25. Niemela M, Kervinen K, Erglis A, Holm NR, Maeng M, Christiansen EH, Kumsars I, Jegere S, Dombrovskis A, Gunnes P, Stavnes S, Steigen TK, Trovik T, Eskola M, Vikman S, Romppanen H, Makikallio T, Hansen KN, Thayssen P, Aberge L, Jensen LO, Hervold A, Airaksinen J, Pietila M, Frobert O, Kellerth T, Ravkilde J, Aaroe J, Jensen JS, Helqvist S, Sjogren I, James S, Miettinen H, Lassen JF, Thuesen L; Nordic-Baltic PCI Study Group. Randomized comparison of final kissing balloon dil-atation versus no final kissing balloon dilatation in patients with coronary bifurcation lesions treated with main vessel stenting: the Nordic-Baltic Bifurcation Study III. Circulation. 2011;123:79-86.
26. Gil R, Bil J, Džavík V, Vassilev D, Kern A, Formuszewicz R, Zalewska-Adamiec M, Dobrzycki S. Regular Drug-Eluting Stent vs Dedicated Coronary Bifurcation BiOSS Expert Stent: Multicenter Open-Label Randomized Controlled POLBOS I Trial. Can J Cardiol. 2015;31:671-8. 27. Lassen JF, Holm NR, Stankovic G, Lefevre T, Chieffo A, Hildick-Smith D, Pan M, Darremont O, Albiero R, Ferenc M, Louvard Y. Percutaneous coronary intervention for coronary bifur-cation disease: consensus from the first 10 years of the European Bifurcation Club meetings. EuroIntervention. 2014;10:545-60. 28. Kim WJ, Kim YH, Park DW, Yun SC, Lee JY, Kang SJ, Lee SW, Lee CW, Park SW, Park SJ. Comparison of single- versus two-stent techniques in treatment of unprotected left main coronary bifurcation disease. Catheter Cardiovasc Interv. 2011;77:775-82. 29. Chen SL, Zhang Y, Xu B, Ye F, Zhang J, Tian N, Liu Z, Qian X, Ding S, Li F, Zhang A, Liu Y, Lin S. Five-year clinical follow-up of unprotected left main bifurcation lesion stenting: one-stent versus two-stent techniques versus double-kissing crush tech-nique. EuroIntervention. 2012;8:803-14. 30. Ishibashi Y, Grundeken MJ, Nakatani S, Iqbal J, Morel MA, Genereux P, Girasis C, Wentzel JJ, Garcia-Garcia HM, Onuma Y, Serruys PW. In vitro validation and comparison of different soft-ware packages or algorithms for coronary bifurcation analysis using calibrated phantoms: Implications for clinical practice and research of bifurcation stenting. Catheter Cardiovasc Interv. 2015;85:554-63. 31. Grundeken MJ, Ishibashi Y, Genereux P, LaSalle L, Iqbal J, Wykrzykowska JJ, Morel MA, Tijssen JG, de Winter RJ, Girasis C, Garcia-Garcia HM, Onuma Y, Leon MB, Serruys PW. Inter-core lab variability in analyzing quantitative coronary angiography for bifurcation lesions: a post-hoc analysis of a randomized trial. JACC Cardiovasc Interv. 2015;8:305-14.

POLBOS II clinical trial
10
C L I N I C A L R E S E A R C HCORONARY INTERVENT IONS
e1404
EuroIntervention 2016
;12
:e14
04
-e1412
published online ahead of print N
ovember 2
015
published online e
-edition Decem
ber 2
016
D
OI: 10
.42
44
/EIJY1
5M
11_11
© Europa Digital & Publishing 2016. All rights reserved.
*Corresponding author: Department of Invasive Cardiology, Central Clinical Hospital of the Ministry of Interior, 137 Woloska Street, 02-507 Warsaw, Poland. E-mail: [email protected]
Regular drug-eluting stents versus the dedicated coronary bifurcation sirolimus-eluting BiOSS LIM® stent: the randomised, multicentre, open-label, controlled POLBOS II trial
Robert J. Gil1,2*, MD, PhD; Jacek Bil1, MD, PhD; Maik J. Grundeken3, MD; Adam Kern4, MD, PhD; Luis A. Iñigo Garcia5, MD; Dobrin Vassilev6, MD, PhD; Tomasz Pawłowski1, MD, PhD; Radoslaw Formuszewicz7, MD; Sławomir Dobrzycki8, MD, PhD; Joanna J. Wykrzykowska3, MD, PhD; Patrick W. Serruys9, MD, PhD
1. Department of Invasive Cardiology, Central Clinical Hospital of the Ministry of Interior, Warsaw, Poland; 2. Institute of Experimental and Clinical Medicine, Polish Academy of Science, Warsaw, Poland; 3. Heart Center, Academic Medical Center - University of Amsterdam, Amsterdam, The Netherlands; 4. Faculty of Medical Sciences, University of Varmia and Masuria, Olsztyn, Poland; 5. Costa del Sol Hospital, Marbella, Spain; 6. Alexandrovska University Hospital, Sofia, Bulgaria; 7. 10th Clinical Military Hospital, Bydgoszcz, Poland; 8. Department of Invasive Cardiology, Medical University in Bialystok, Bialystok, Poland; 9. International Centre for Circulatory Health, NHLI, Imperial College London, London, United Kingdom
GUEST EDITOR: David Hildick-Smith, MD, FRCP, FSCAI; Sussex Cardiac Centre, Brighton and Sussex University Hospitals NHS Trust, Brighton, United Kingdom
AbstractAims: The aim of the POLBOS II randomised trial was to compare any regular drug-eluting stents (rDES) with the dedicated bifurcation sirolimus-eluting stent BiOSS LIM for the treatment of coronary bifurca-tion lesions. The secondary aim was to study the effect of final kissing balloon inflation (FKBI) on clinical outcomes.
Methods and results: Between December 2012 and December 2013, 202 patients with stable coronary artery disease or non-ST-segment elevation acute coronary syndrome were randomly assigned 1:1 to treat-ment of the coronary bifurcation lesions either with the BiOSS LIM stent (n=102) or with an rDES (n=100). Coronary re-angiography was performed at 12 months. The primary endpoint was the composite of cardiac death, myocardial infarction (MI), and target lesion revascularisation (TLR) at 12 months. The target ves-sel was located in the left main in one third of the cases (35.3% in BiOSS and 38% in rDES). Side branch treatment was required in 8.8% (rDES) and 7% (BiOSS). At 12 months, the cumulative MACE incidence was similar in both groups (11.8% [BiOSS] vs. 15% [rDES, p=0.08]), as was the TLR rate (9.8% vs. 9% [p=0.8]). The binary restenosis rates were significantly lower in the FKBI subgroup of the BiOSS group (5.9% vs. 11.8%, p<0.05).
Conclusions: MACE rates as well as TLR rates were comparable between the BiOSS LIM and rDES. At 12 months, cumulative MACE incidence was similar in both groups (11.8% vs. 15%), as was the TLR rate (9.8% vs. 9%). Significantly lower rates of restenosis were observed in the FKBI subgroup of the BiOSS group.
KEYWORDS
• BiOSS LIM®
• dedicated bifurcation stent
• sirolimus-eluting stent
SUBMITTED ON 19/04/2015 - REVISION RECEIVED ON 16/06/2015 - ACCEPTED ON 25/09/2015

POLBOS II clinical trial
11
EuroIntervention 2016
;12
:e14
04
-e1412
e1405
POLBOS II clinical trial
IntroductionDrug-eluting stents (DES) started being used in coronary bifur-cations in the early 2000s and clearly improved midterm angio-graphic and clinical outcomes compared with bare metal stents1. However, bifurcation lesions still pose a therapeutic challenge during percutaneous coronary interventions (PCI). Therefore, the use of dedicated bifurcation stents (DBS) is one of the proposed potential solutions to improve short-term as well as long-term out-comes. However, up to now only two randomised trials comparing DES with DBS have been published, one with the BiOSS Expert® stent (Balton, Warsaw, Poland), and one with the Tryton Side Branch Stent (Tryton Medical, Durham, NC, USA)2,3.
The aim of the POLBOS II (POLish Bifurcation Optimal Stenting) trial was to compare the use of any regular drug-eluting stent (rDES) with a dedicated bifurcation sirolimus-eluting stent BiOSS LIM® (Balton) for the treatment of coronary bifurcation lesions. The secondary aim was to study the effect of final kissing balloon inflation (FKBI) on clinical outcomes.
MethodsSTUDY POPULATION AND STUDY DESIGNThe POLBOS II trial was a randomised, open-label, controlled study conducted between December 2012 and December 2013 in four centres in Poland and in one centre in Spain. The inclu-sion criteria were: stable coronary artery disease (CAD) or non-ST-segment elevation acute coronary syndrome (NSTE-ACS), age ≥18 years, de novo coronary bifurcation lesion (including unpro-tected left main stem), main vessel (MV) diameter ≥2.5 mm and side branch (SB) diameter ≥2.0 mm on visual estimation. Main exclusion criteria were: ST-segment elevation myocardial infarc-tion (STEMI), Medina 0,0,1 bifurcations, baseline serum creatinine level ≥177 µmol/L (2.0 mg/dl), inability to take dual antiplatelet therapy for 12 months, left ventricular ejection fraction ≤30%, and the lack of informed consent. The institutional review board of each participating centre approved the study protocol (88/2010, ClinicalTrials.gov Identifier: NCT02198300).
INTERVENTIONAL PROCEDURE, DEVICE DESCRIPTION AND CONCOMITANT MEDICATIONAfter signing informed consent, patients were randomly assigned to one of two treatment strategies, BiOSS LIM stent implanta-tion or rDES implantation. Patients randomised to the rDES group underwent a second randomisation: completing the procedure with or without FKBI (Figure 1). Patients were randomised by telephone call to an external office, where the random allocation sequence was generated, and the participants were assigned using a sealed opaque envelope system (randomisation 1:1).
The BiOSS LIM is a coronary, dedicated balloon-expandable bifurcation stent. The platform is made of 316L stainless steel (strut thickness 120 μm) and is coated with a biodegradable poly-mer that elutes sirolimus (drug concentration: 1.4 µg/mm2). The rapid exchange delivery system is compatible with conventional 0.014” guidewires and 5 Fr guiding catheters. The BiOSS LIM
POLBOS IIStudy flow chartAssessed for eligibility
(n=266)
Excluded (n=64):– not meeting inclusion criteria (n=45)– refused to sign informed consent (n=19)
Randomised(n=202)
BiOSS LIM® groupn=102
Observation (n=102)
Lost to FU (n=1)1 non-cardiac death
Analysed ITT(n=102)
Regular rDES groupn=100
FKBI no FKBI n=49 n=51
Observation (n=100)
Lost to FU (n=3)3 sudden deaths of unknown reason
Analysed ITT(n=100)An
alys
isFo
llow-
upAl
locat
ionEn
rolm
ent
Figure 1. POLBOS II - study flow chart. FKBI: final kissing balloon inflation; FU: follow-up; ITT: intention-to-treat; rDES: regular drug-eluting stent
consists of two parts, proximal and distal, joined with two con-nection struts at the middle zone (length: 0.9-1.5 mm, depending on stent size)4,5.
In the rDES group, the use of any approved regular DES avail-able in the participating cathlabs was allowed at the discretion of the operator. The following stents were available: paclitaxel-eluting stents (PES) (Luc-Chopin2® [Balton], Coroflex® Please [B. Braun, Melsungen AG, Melsungen, Germany]), everolimus-eluting stents (EES) (XIENCE® [Abbott Vascular, Santa Clara, CA, USA], PROMUS [Boston Scientific Corp., Marlborough, MA, USA]), sirolimus-eluting stents (SES) (PROLIM® [Balton], Orsiro [Biotronik, Bülach, Switzerland], Cre8™ [CID, Saluggia, Italy]), Biolimus A9-eluting stents (BES) (BioMime™ [Meril, Vapi, Gujarat, India], BioMatrix™ [Biosensors, Singapore]), and zotarolimus-eluting stents (ZES) (Resolute Integrity [Medtronic, Minneapolis, MN, USA]).
The default strategy in both treatment groups consisted of the provisional strategy. A single stent was implanted in the MV-main branch (MB) across the SB in all patients. Bifurcation lesions were assessed according to the Medina classification (visual assess-ment)6. There was no restriction regarding lesion length. MV pre-dilatation and/or SB predilatation was performed according to the operator’s decision. The stent was then implanted in the MV-MB. Next, the proximal optimisation technique (POT) was recom-mended, utilising a short non-compliant balloon in the proximal part of the MV stent. The balloon for POT was positioned with the

POLBOS II clinical trial
12
EuroIntervention 2016
;12
:e14
04
-e1412
e1406
distal marker in front of the carina7. After rewiring, SB post-dila-tation/stent implantation was performed if indicated. A stent in the SB was implanted only if there was >70% residual stenosis in the SB and/or significant flow impairment (TIMI 0-1) after MV-MB stenting and/or a flow-limiting dissection.
The procedure was completed with FKBI dilatation. In the BiOSS group this step was left to the operator’s discretion, while in the rDES group it was performed according to the result of a second randomisation.
Procedures were performed according to local standards via radial or femoral access using 6 or 7 Fr guiding catheters. Pharmacological treatment was according to the most recent guidelines.
Troponin I (TnI), creatine kinase (CK) and creatine kinase-myo-cardial band (CK-MB) were measured pre-procedure and after six and 24 hours post procedure in all patients. Periprocedural myo-cardial infarction (type 4a) was defined according to the third uni-versal definition8.
FOLLOW-UPClinical follow-up was performed with office visits or by tel-ephone at one and 12 months after intervention. Adverse events were monitored throughout the study period. Follow-up coronary angiography was performed at 12 months, unless clinically indi-cated earlier.
ENDPOINTSThe primary endpoint was the cumulative rate of major adverse car-diovascular events (MACE) consisting of cardiac death, myocardial infarction (MI) and target lesion revascularisation (TLR). Secondary endpoints included cardiac death, all-cause death, MI, TLR, target vessel revascularisation (TVR), stent thrombosis (ST), late lumen loss (LLL) and device success. Cardiac death included death result-ing from an acute MI, sudden cardiac death, death due to heart fail-ure and death due to cardiac procedures. All deaths were deemed cardiac unless proven otherwise. MI was defined according to the third universal definition8. Clinically driven TLR was defined as reintervention of the target lesion due to presence of a symptomatic ≥50% diameter stenosis during follow-up. Angiographically driven TLR was defined as reintervention due to angiographic detection of significant restenosis (≥70%) in a patient who was clinically asymp-tomatic. TVR was defined as any revascularisation of any segment of the index coronary artery. LLL was calculated based on quanti-tative coronary angiographic (QCA) results and was defined as the post-procedural minimal luminal diameter minus the minimal lumi-nal diameter (in millimetres) at 12-month follow-up. Device success was defined as successful deployment of the intended stent in the target site without a system failure.
ANGIOGRAPHIC ANALYSISTwo orthogonal projections were chosen to visualise the treated bifurcation. All recordings were performed after intracoronary administration of nitroglycerine (200 μg). QCA analysis was per-formed using the dedicated bifurcation software CAAS 5.11 (Pie
Medical Imaging BV, Maastricht, The Netherlands). Calibration was performed using the guiding catheter in all cases. The three bifurcation segments (MV, MB, SB) were analysed separately according to the European Bifurcation Club (EBC) consen-sus document9. The following parameters were reported: lesion length, reference vessel diameter (RVD), minimal lumen diame-ter (MLD). Percentage diameter stenosis (%DS), acute lumen gain (ALG) and LLL were calculated as described previously10. The point of bifurcation (POB) was determined automatically by the software and defined as the mid-point of the largest circle that can be fitted in the bifurcation area, touching all three contours, as pre-viously described11.
STATISTICAL ANALYSISContinuous variables were presented as mean±SD. Categorical data were presented as numbers (%). Continuous variables were compared using an unpaired Student’s two-sided t-test, and cat-egorical data using the χ2 test or Fisher’s exact test, as appropri-ate. If distribution was not normal (verified with the Shapiro-Wilk test), Wilcoxon signed-rank tests and Mann-Whitney U tests were used. P-values of <0.05 were considered statistically significant. Statistical analyses were performed using R 3.0.2 for OS (R Foundation, Vienna, Austria).
ResultsBASELINE CLINICAL CHARACTERISTICSBetween December 2012 and December 2013, a total of 202 patients were enrolled and randomly assigned to either the BiOSS group (n=102) or the rDES group (n=100). Among patients from the rDES group, 49 were randomised to FKBI and 51 to no FKBI (Figure 1). The mean age was 67.2±8.8 years in the BiOSS group and 66.6±9.0 years in the rDES group (p=0.93). Baseline clini-cal characteristics were well matched between the two groups, although there were more patients with diabetes type 2 in the BiOSS group (44.1% vs. 32%, p=0.01), and more patients with peripheral artery disease in the rDES group (3.9% vs. 9%, p=0.03) (Table 1).
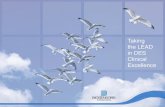
ANGIOGRAPHIC AND PROCEDURAL CHARACTERISTICSLesions were located in the left anterior descending artery (LAD) in almost half of the cases (BiOSS vs. rDES: 44.1% vs. 43%, p=0.9), and in the left main (LM) in about one third of the cases (BiOSS vs. rDES: 35.3% vs. 38%, p=0.84). The rest were located in either the left circumflex artery (LCx) (BiOSS vs. rDES: 15.7% vs. 15.0%, p=0.88) or the right coronary artery (RCA) (BiOSS vs. rDES: 4.9% vs. 4%, p=0.9). In the rDES group, EES (46%) were used most frequently, followed by SES (24%). More details are presented in Figure 2A-Figure 2C. No difference between the two groups was observed regarding the distribution of true (i.e., Medina 1,1,1, 1,0,1, 0,1,1) and non-true bifurcations (Table 2).
The main procedural variables are presented in Table 3. The device success rate was 99% in both groups. Mean BiOSS Expert nominal stent diameters were 3.74±0.45 mm (MV) and

POLBOS II clinical trial
13
EuroIntervention 2016
;12
:e14
04
-e1412
e1407
POLBOS II clinical trial
3.03±0.43 mm (MB). Mean stent length was 17.83±2.69 mm, while the mean maximal implantation pressure was 14.3±4.5 atm. In the rDES group nominal stent parameters were as follows: diameter 3.35±0.51 mm, length 19.94±6.32 mm and mean maxi-mal implantation pressure 17.2±3.7 atm. Procedural characteristics in the two groups were similar, except for rates of FKBI and POT, which were higher in the rDES group, 32.7% vs. 49% (p<0.01)
Table 1. Baseline population characteristics.
BiOSS group rDES group
Baseline clinical characteristics n=102 (%) n=100 (%)
Age, years 67.2±8.8 66.6±9.0
Women, n (%) 24 (23.1) 25 (25)
Hypertension 86 (84.3) 81 (81)
Hypercholesterolaemia 85 (83.3) 81 (81)
Diabetes type 2 45 (44.1) 32 (32)*
Prior MI 44 (43.1) 48 (48)
Prior PCI 53 (52) 57 (57)
CABG 13 (12.7) 16 (16)
Peripheral artery disease 4 (3.9) 9 (9)*
Chronic kidney disease 11 (10.8) 7 (7)
History of smoking 21 (20.6) 26 (26)
EuroSCORE II 1.35±1.1% 1.42±1.3%
Clinical indication for PCI
planned PCI 78 (76.9) 75 (75)
UA 9 (8.8) 11 (11)
NSTEMI 15 (14.3) 14 (14)
STEMI 0 0
Baseline angiographic characteristics n=102 (%) n=100 (%)
SYNTAX score 17.53±3.47 18.21±2.35
Multivessel disease 74 (72.6) 68 (68)
Lesion type A 3 (2.9) 2 (2)
B1 45 (44.1) 40 (40)
B2 28 (27.5) 39 (39)*
C 26 (25.5) 19 (19)
*p<0.05. CABG: coronary artery bypass graft; MI: myocardial infarction; NSTEMI: non-ST-elevation myocardial infarction; PCI: percutaneous coronary intervention; rDES: regular drug-eluting stent; STEMI: ST-elevation myocardial infarction; UA: unstable angina
Table 2. Medina classification according to QCA.
Medina typeBaseline Post-procedure Follow-up
BiOSS n=102 (%) rDES n=100 (%) BiOSS n=102 (%) rDES n=100 (%) BiOSS n=86 (%) rDES n=85 (%)
1,1,1 42 (41.2) 40 (40) 0 0 3 (3.5) 3 (3.5)
1,0,1 12 (11.8) 14 (14) 0 0 1 (1.2) 1 (1.2)
0,1,1 25 (24.5) 28 (28) 0 0 1 (1.2) 1 (1.2)
1,0,0 4 (3.9) 5 (5) 0 0 4 (4.7) 3 (3.5)
1,1,0 17 (16.8) 13 (15) 0 0 1 (1.2) 0
0,1,0 2 (1.9) 0 0 0 3 (3.5) 1 (1.2)
0,0,1 0 0 10 (9.8) 8 (8) 6 (7) 8 (9.4)
0,0,0 0 0 92 (90.2) 92 (92) 67 (78) 68 (80)
rDES: regular drug-eluting stent
Table 3. Procedural characteristics.
ParameterBiOSS group
n (%)rDES group
n (%)
Successful implantation 101 (99) 99 (99)
MV predilatation 57 (55.9) 77 (77)*
SB predilatation 40 (39.2) 29 (29)*
Both branches predilatation 24 (23.5) 27 (27)
Nominal stent diameter, mm – 3.35±0.51*
Nominal stent diameter in MV, mm 3.74±0.45 –
Nominal stent diameter in MB, mm 3.03±0.43 –
Nominal stent length, mm 17.83±2.69 19.94±6.32*
SB post-dilatation 50 (49.0) 54 (54.0)
POT 38 (37.3) 68 (68)*
FKBI 34 (32.7) 49 (49)*¶
Additional stent in SB 9 (8.8) 7 (7.0)
Dissection requiring an additional stent in MV-MB 5 (4.9) 6 (6.0)
Fluoroscopy time, min 12.6±10.7 12.7±5.7
Contrast volume, ml 131±45 134±37
Vascular access femoral/radial 36.3%/63.7% 19%/81%
Guiding catheter 6 Fr/7 Fr 95.1%/4.9% 100%/0%
*p<0.05. ¶FKBI was performed according to randomisation in the rDES group and according to the operator’s discretion in the BiOSS LIM group. FKBI: final kissing balloon inflation; MB: main branch; MV: main vessel; POT: proximal optimisation technique; rDES: regular drug-eluting stent; SB: side branch
and 37.3% vs. 68% (p<0.01), respectively. In both groups, the MV was predilated in more than half of the lesions (BiOSS 55.9% vs. rDES 77%, p=0.03), and the implantation of an additional rDES in the SB was required in nine cases (8.8%) in the BiOSS group and in seven cases (7%) in the rDES group (p=0.9).
CLINICAL OUTCOMESThere was one (1%) periprocedural MI in each group (due to tran-sient SB occlusion and/or atherosclerotic debris embolisation). Additionally, there were six (5.9%) patients in the BiOSS group and eight (8%) in the rDES group with in-hospital increased TnI levels (max 1.9 ng/ml). These were all asymptomatic, without

POLBOS II clinical trial
14
EuroIntervention 2016
;12
:e14
04
-e1412
e1408
ECG changes and did not require repeat coronary angiography (i.e., they did not meet the criteria of MI type 4a).
Clinical follow-up at 12 months was available in all patients who were alive (Table 4). The cumulative incidence of MACE was numerically lower in the BiOSS group although it did not reach statistical significance (11.8% in the BiOSS group vs. 15% in the rDES group, p=0.09). In the BiOSS group one non-cardiac death (secondary to a malignancy) occurred, whereas cardiac death occurred in three patients in the rDES group (all sudden deaths of unknown cause). One case of definite ST was observed in each group, both subacute. The TLR rate was comparable between both
groups (BiOSS group vs. rDES group: 9.8% vs. 9.0%, p=0.8). When considering only clinically driven TLR there were five (4.9%) cases in the BiOSS group and three (3.0%) cases in the rDES group (p=NS). Also, there was a trend towards a lower TLR rate in the LM subgroup in the BiOSS group (8.3% vs. 10.5%). Moreover, in the PES subgroup of the rDES group the TLR rate was 22.7%, whereas in the “olimus” subgroup it was only 5.1%. Detailed data concerning the type of restenosis with regard to DES type in the rDES group are presented in Appendix Table 1, Appendix Table 2. Figure 3 shows the position of the MLD sites, with their corresponding diameter stenosis values, relative to the
LM35%
LAD44%
LCx16%
RCA5% LM
38%
LAD43%
LCx15%
RCA4%
2%6% 22%
24%MV MB SB
A B
C D
Lesion location in BiOSS group Lesion location in rDES group
Types of drugs in rDES group Late lumen loss
0.16 0.14
0.280.23
0.320.26
46%
Figure 2. POLBOS II trial results. A) Lesion location in the BiOSS group. B) Lesion location in the rDES group. C) Types of drugs in regular DES group. D) Late lumen loss after 12 months.
Figure 3. MLD distribution in the BiOSS LIM stent after 12 months.

POLBOS II clinical trial
15
EuroIntervention 2016
;12
:e14
04
-e1412
e1409
POLBOS II clinical trial
POB for each bifurcation segment separately. It shows that the middle zone is not more susceptible to restenosis than the seg-ments more proximal to or distal from the POB.
QCA ANALYSISAngiographic follow-up at 12 months was performed in 182 patients (90.1%), of whom 92 (90.2%) were randomised to the BiOSS group and 90 (90%) to the rDES group. Follow-up QCA analysis was performed in 171 (84.7%) cases. Eleven cases had to be excluded due to an inadequate view at the bifurcation lesion, overlapping vessel segments, or the presence of angiographic guidewires. Angiographic data are presented in Table 5. The two groups were well matched in baseline QCA characteristics. Quantitative angiographic analysis revealed that the BiOSS LIM stent as well as rDES implantation caused a significant increase of MLD and decrease of %DS in the MV and MB. However, this procedure did not affect angle alpha between the MV and SB. When comparing LLL values, there were no significant differ-ences in the MV (BiOSS vs. rDES: 0.28 vs. 0.23 mm, p=NS), in the MB (0.32 vs. 0.26 mm, p=NS) as well as in the SB (0.16 vs. 0.14 mm, p=NS) (Figure 2D). Within the rDES group, the smallest LLL values were observed in the EES subgroup, and the largest in the PES subgroup (Appendix Table 3). LLL values were greater in non-LMS bifurcation lesions in all subgroups.
FKBI VS. NO FKBI – SUBGROUP ANALYSISSubgroup analysis regarding FKBI versus no FKBI revealed that in both groups (BiOSS group and rDES group) FKBI was related to a higher rate of SB stenting, longer fluoroscopy time and a greater likelihood of the treated lesions being located in the LM. However, in the FKBI subgroup there was a significantly lower rate of restenosis in the BiOSS group (5.9% vs. 11.8%, p<0.05). Such an association was not present in the rDES group (10.2% vs. 7.8%, p=NS). Moreover, the POT technique has a more pro-nounced effect on the TLR rate than the FKBI and in both groups was significantly associated with a lower rate of TLR (in the
Table 5. Angiographic data.
BiOSS group rDES group
Pre-intervention
MV - RVD, mm 3.59±0.23 3.48±0.29
MV - %DS 61±14 59±16
MV - MLD, mm 1.4±0.24 1.43±0.27
MB - RVD, mm 3.01±0.12 3.07±0.23
MB - %DS 48±16 49±16
MB - MLD, mm 1.56±0.18 1.57±0.19
SB - RVD, mm 2.45±0.39 2.34±0.34
SB - %DS 54±24 45±18
SB - MLD, mm 1.13±0.2 1.29±0.16
Angle MV-SB 76±21 69±23
Angle MB-SB 87±23 76±23
MV lesion length, mm 9.3±3.4 9.7±3.7
MB lesion length, mm 8.3±2.9 9.8±3.4
SB lesion length, mm 4.2±2.1 3.9±2.8
Post-intervention
MV - RVD, mm 3.68±0.19 3.53±0.25
MV - %DS 11±4 8±9
MV - MLD, mm 3.28±0.15 3.25±0.19
MV - ALG, mm 1.88±0.19 1.82±0.24
MB - RVD, mm 3.1±0.38 3.15±0.32
MB - %DS 14±12 13±8
MB - MLD, mm 2.67±0.27 2.74±0.21
MB - ALG, mm 1.11±0.16 1.17±0.18
SB - RVD, mm 2.41±0.14 2.39±0.22
SB - %DS 32±19 28±21
SB - MLD, mm 1.64±0.2 1.72±0.15
SB - ALG, mm 0.51±0.16 0.43±0.18
Angle MV-SB 79±21 79±23
Angle MB-SB 86±23 66±23
Follow-up
MV - RVD, mm 3.72±0.13 3.57±0.19
MV - %DS 19±6 15±10
MV - MLD, mm 3.0±0.17 3.02±0.21
MB - RVD, mm 3.12±0.28 3.18±0.23
MB - %DS 24±12 22±13
MB - MLD, mm 2.35±0.32 2.48±0.28
SB - RVD, mm 2.43±0.14 2.37±0.18
SB - %DS 39±19 33±17
SB - MLD, mm 1.48±0.2 1.58±0.18
Angle MV-SB 78±18 76±14
Angle MB-SB 84±19 69±19
ALG: acute lumen gain
Table 4. Clinical results.
BiOSS group n=102 (%) rDES group n=100 (%)
30 days 12 mo 30 days 12 mo
MACE 2 (1.9) 12 (11.8) 2 (2) 15 (15)
All-cause death 0 1 (1) 0 3 (3)
Cardiac death 0 0 0 3 (3)
MI 1 (1) 2 (1.9) 1 (1) 3 (3)
Definite ST 1 (1) 1 (1) 1 (1) 1 (1)
Cumulative TLR 1 (1) 10 (9.8) 1 (1) 9 (9)
Clinically driven TLR 1 (1) 5 (4.9) 1 (1) 3 (3)
TVR 1 (1) 14 (13.7) 1 (1) 12 (12)
PCI in another vessel 0 8 (7.8) 0 6 (6)
MACE: major adverse cardiovascular events; MI: myocardial infarction; PCI: percutaneous coronary intervention; rDES: regular drug-eluting stent; ST: stent thrombosis; TLR: target lesion revascularisation; TVR: target vessel revascularisation
BiOSS group: 5.3% vs. 12.5%, p<0.05 and in the rDES group: 2.9% vs. 25%, p<0.01). Additionally, there was a trend towards lower LLL in both the BiOSS group and the rDES group when FKBI and POT were applied (Appendix Table 1).

POLBOS II clinical trial
16
EuroIntervention 2016
;12
:e14
04
-e1412
e1410
DiscussionThe main findings of this study are as follows: 1) the 12-month cumulative MACE rates were comparable between the BiOSS LIM and the rDES treatment groups; 2) TLR rates were also com-parable between BiOSS LIM and rDES; 3) FKBI did not improve outcomes in rDES, although this was underpowered; 4) a sub-group of patients in whom POT with FKBI was performed showed better angiographic and clinical outcomes; 5) the BiOSS LIM pro-vides a single stent bifurcation treatment option with a very high rate of implantation success.
The BiOSS stent is a stainless steel construction based on the physiological concept of the coronary bifurcation anatomy and the coronary blood flow. Results of the BiOSS Expert Registry eval-uating the BiOSS paclitaxel-eluting stent were encouraging and, subsequently, the randomised POLBOS I trial comparing BiOSS Expert with rDES was conducted3,12. However, in the meantime many studies have shown paclitaxel-eluting stents to be inferior to “olimus”-eluting stents13. Therefore, a new version of the BiOSS stent, the BiOSS LIM, eluting sirolimus, was designed. After near completion of the POLBOS I trial, the POLBOS II trial was started, in which the sirolimus-eluting BiOSS LIM was compared with rDES.
The results of both POLBOS I and POLBOS II have shown that the BiOSS stent performs very well in distal LM stenosis14. There was no difference between sirolimus- and paclitaxel-eluting BiOSS stents. This suggests that the design of the BiOSS stent itself plays a crucial role. Also, lower LLL values in the LM subgroup suggest that this stent might be better suited for bifurcations with a greater difference in diameters between MV and MB, such as the LMS/LAD/LCX bifurcation (Appendix Table 3). These results were also initially observed in registries of the BiOSS stents in the LM10,15.
The stepped design of the BiOSS stent delivery balloon was created, theoretically, to ensure an FKBI- and POT-like effect, thus allowing operators frequently to omit this part of the procedure. During analysis of the current data we indeed found that the per-centages of FKBI and POT were relatively low. These data sug-gest that the operators also had the perception that the features of the BiOSS stent design might remove the need for POT and/or FKBI as procedural steps during PCI of bifurcation lesions. Unfortunately, in the subgroup of patients treated with BiOSS in whom FKBI and POT were not performed, we found worse clinical outcomes and a trend towards higher LLL values. This unfavourable outcome might be due to the fact that the semi-com-pliant delivery balloon is not as efficient in POT as the recom-mended non-compliant balloon catheter (according to the EBC). Also, in the distal part of the stent the semi-compliant delivery balloon might not keep its parameters (it might gain too much in diameter) and cause the plaque shift as well as the carina shift. Therefore, the use of FKBI might restore the correct anatomical conditions in the bifurcation and improve the outcome. The impact of FKBI on clinical outcomes found in both POLBOS trials was in agreement with NORDIC III study findings, in which FKBI reduced angiographic side branch restenosis, especially in patients
with true bifurcation lesions3,16. However, to the best of our knowl-edge, we show for the first time the importance of POT as the final part of coronary stent implantation in bifurcation lesions. It should be stressed that in our study POT had a more pronounced posi-tive effect on TLR rates (5.3% with POT vs. 12.5% without POT, p<0.05, in the BiOSS group; and 2.9% with POT vs. 25% without POT in the rDES group, p<0.01).
Importantly, the pattern of restenosis did not reveal the mid-dle zone (with only the two connection struts) as a “weak point” of the BiOSS LIM stent. The MLD sites were located signifi-cantly further away from the POB at follow-up than pre-procedure (Figure 3).
BiOSS stents are made of stainless steel and therefore have rel-atively thick struts (120 µm without polymer), which might pre-dispose to excessive neointimal proliferation. The ISAR-STEREO trial demonstrated that a thin-strut stent had a lower rate of reste-nosis than a thick-strut stent of similar design17. Similar results were found in several other trials18-20. During recent years the industry has applied platinum chromium and cobalt-chromium alloys to achieve stents with so-called thin struts (i.e., <90 µm)21.
Although the clinical results obtained with the BiOSS Expert are satisfactory, the BiOSS concept remains under development (Appendix Table 4). The next generation of the BiOSS stent, made of cobalt-chromium with a strut thickness of 70 µm, but with the same sirolimus concentration and biodegradable polymer, is cur-rently under development. The results obtained in the POLBOS I and II trials are very consistent. The results of the BiOSS LIM stent (even without optimisation) were comparable to rDES. It is assumed that only the thin-strut BiOSS version may achieve bet-ter results. Therefore, it was decided to prepare a new randomised, international study – POLBOS III, where the newest thin-strut BiOSS version will be compared with the most tested representa-tives of “olimus” stents (EES, ZES).
STUDY LIMITATIONSThe POLBOS II trial has several limitations that should be acknowledged. First of all, the sample size was relatively small. Furthermore, a 100% angiographic follow-up rate could not be achieved, although a follow-up rate of 90% is in line with similar studies. The use of multiple stent types and drugs in the control group is also a limitation, although this aspect of the design was intended to replicate real-world clinical practice. The predictable randomisation scheme may potentially have biased the decisions of investigators to randomise patients with certain angiographic characteristics. Finally, the differences in FKBI/POT strategies between the two study groups (randomisation in the rDES group and operator choice in the BiOSS group) may also have influenced the results.
ConclusionThe success rate of implantation of the BiOSS LIM stent is very high. The cumulative rate of MACE is comparable between BiOSS and rDES groups. The TLR rate achieved with the BiOSS

POLBOS II clinical trial
17
EuroIntervention 2016
;12
:e14
04
-e1412
e1411
POLBOS II clinical trial
LIM was comparable to that obtained with rDES. The POLBOS II trial sets an important benchmark for future studies with new generations of BiOSS stents eluting “olimus” drugs and utilising newer stent materials.
Impact on daily practiceThis trial has shown that implantation of the dedicated bifurca-tion BiOSS LIM stent is safe and effective. Also, the results for MACE and TLR rates were comparable between the BiOSS LIM and rDES groups. Therefore, this stent might be an alter-native in some cases of coronary bifurcation treatment, espe-cially when there is a large difference in diameter between the main vessel and the main branch.
Guest EditorThis paper was guest edited by David Hildick-Smith, MD, Sussex Cardiac Centre, Brighton and Sussex University Hospitals NHS Trust, Brighton, United Kingdom.
Conflict of interest statementR. Gil was the medical consultant of the Balton Company. The other authors have no conflicts of interest to declare. The guest editor is a proctor/adviser for Medtronic, Boston Scientific, Edwards Lifesciences, and St. Jude Medical.
References 1. Routledge HC, Lefevre T, Colombo A, Oldroyd KG, Hamm CW, Guagliumi G, von Scheidt W, Guetta V, Ruzyllo W, Wittebols K, Goedhart DM, Serruys PW. Three-year clinical out-come of percutaneous treatment of bifurcation lesions in multives-sel coronary artery disease with the sirolimus-eluting stent: insights from the Arterial Revascularisation Therapies Study, part II (ARTS II). EuroIntervention. 2009;5:190-6. 2. Genereux P, Kumsars I, Lesiak M, Kini A, Fontos G, Slagboom T, Ungi I, Metzger DC, Wykrzykowska JJ, Stella PR, Bartorelli AL, Fearon WF, Lefevre T, Feldman RL, LaSalle L, Francese DP, Onuma Y, Grundeken MJ, Garcia-Garcia HM, Laak LL, Cutlip DE, Kaplan AV, Serruys PW, Leon MB. A ran-domized trial of a dedicated bifurcation stent versus provisional stenting in the treatment of coronary bifurcation lesions. J Am Coll Cardiol. 2015;65:533-43. 3. Gil RJ, Bil J, Dzavik V, Vassilev D, Kern A, Formuszewicz R, Zalewska-Adamiec M, Dobrzycki S. Regular Drug-Eluting Stent vs Dedicated Coronary Bifurcation BiOSS Expert Stent: Multicenter Open-Label Randomized Controlled POLBOS I Trial. Can J Cardiol. 2015;31:671-8. 4. Gil RJ, Bil J, Vassiliev D, Inigo Garcia LA. First-in-man study of dedicated bifurcation sirolimus-eluting stent: 12-month results of BiOSS LIM® Registry. J Interv Cardiol. 2015;28:51-60. 5. Vassilev D, Gil R, Milewski K. Bifurcation Optimisation Stent System (BiOSS Lim) with sirolimus elution: results from por-cine coronary artery model. EuroIntervention. 2011;7:614-20.
6. Medina A, Suarez de Lezo J, Pan M. [A new classification of coronary bifurcation lesions]. Rev Esp Cardiol. 2006;59:183. 7. Lassen JF, Holm NR, Stankovic G, Lefevre T, Chieffo A, Hildick-Smith D, Pan M, Darremont O, Albiero R, Ferenc M, Louvard Y. Percutaneous coronary intervention for coronary bifur-cation disease: consensus from the first 10 years of the European Bifurcation Club meetings. EuroIntervention. 2014;10:545-60. 8. Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD, Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction. Katus HA, Lindahl B, Morrow DA, Clemmensen PM, Johanson P, Hod H, Underwood R, Bax JJ, Bonow RO, Pinto F, Gibbons RJ, Fox KA, Atar D, Newby LK, Galvani M, Hamm CW, Uretsky BF, Steg PG, Wijns W, Bassand JP, Menasche P, Ravkilde J, Ohman EM, Antman EM, Wallentin LC, Armstrong PW, Simoons ML, Januzzi JL, Nieminen MS, Gheorghiade M, Filippatos G, Luepker RV, Fortmann SP, Rosamond WD, Levy D, Wood D, Smith SC, Hu D, Lopez-Sendon JL, Robertson RM, Weaver D, Tendera M, Bove AA, Parkhomenko AN, Vasilieva EJ, Mendis S. Third universal definition of myocardial infarction. Circulation. 2012;126:2020-35. 9. Louvard Y, Thomas M, Dzavik V, Hildick-Smith D, Galassi AR, Pan M, Burzotta F, Zelizko M, Dudek D, Ludman P, Sheiban I, Lassen JF, Darremont O, Kastrati A, Ludwig J, Iakovou I, Brunel P, Lansky A, Meerkin D, Legrand V, Medina A, Lefevre T. Classification of coronary artery bifurcation lesions and treatments: time for a consensus! Catheter Cardiovasc Interv. 2008;71: 175-83. 10. Bil J, Gil RJ, Vassilev D, Rzezak J, Kulawik T, Pawlowski T. Dedicated bifurcation paclitaxel-eluting stent BiOSS Expert® in the treatment of distal left main stem stenosis. J Interv Cardiol. 2014;27:242-51. 11. Grundeken MJ, Ishibashi Y, Ramcharitar S, Tuinenburg JC, Reiber JH, Tu S, Aben JP, Girasis C, Wykrzykowska JJ, Onuma Y, Serruys PW. The need for dedicated bifurcation quantitative coro-nary angiography (QCA) software algorithms to evaluate bifurca-tion lesions. EuroIntervention. 2015;11 Suppl V:V44-9. 12. Gil RJ, Vassilev D, Michalek A, Kern A, Formuszewicz R, Dobrzycki S, Wojcik J, Lesiak M, Kardaszewicz P, Lekston A. Dedicated paclitaxel-eluting bifurcation stent BiOSS® (bifurcation optimisation stent system): 12-month results from a prospective registry of consecutive all-comers population. EuroIntervention. 2012;8:316-24. 13. Qian J, Chen Z, Ma J, Ge J. Sirolimus- versus paclitaxel-elut-ing stents for coronary bifurcations intervention: a meta-analysis of five clinical trials. Catheter Cardiovasc Interv. 2012;80:507-13. 14. Sibbald M, Chan W, Daly P, Horlick E, Ing D, Ivanov J, Mackie K, Osten MD, Overgaard CB, Dzavik V. Long-term out-come of unprotected left main stenting: a Canadian tertiary care experience. Can J Cardiol. 2014;30:1407-14. 15. Gil RJ, Bil J, Grundeken MJ, Iñigo Garcia LA, Vassilev D, Kern A, Pawłowski T, Wykrzykowska JJ, Serruys PW. Long-term effectiveness and safety of the sirolimus-eluting BiOSS LIM®

POLBOS II clinical trial
18
EuroIntervention 2016
;12
:e14
04
-e1412
e1412
dedicated bifurcation stent in the treatment of distal left main steno-sis: an international registry. EuroIntervention. 2016;12:1246-54. 16. Niemela M, Kervinen K, Erglis A, Holm NR, Maeng M, Christiansen EH, Kumsars I, Jegere S, Dombrovskis A, Gunnes P, Stavnes S, Steigen TK, Trovik T, Eskola M, Vikman S, Romppanen H, Makikallio T, Hansen KN, Thayssen P, Aberge L, Jensen LO, Hervold A, Airaksinen J, Pietila M, Frobert O, Kellerth T, Ravkilde J, Aaroe J, Jensen JS, Helqvist S, Sjogren I, James S, Miettinen H, Lassen JF, Thuesen L; Nordic-Baltic PCI Study Group. Randomized comparison of final kissing balloon dil-atation versus no final kissing balloon dilatation in patients with coronary bifurcation lesions treated with main vessel stenting: the Nordic-Baltic Bifurcation Study III. Circulation. 2011;123:79-86. 17. Kastrati A, Mehilli J, Dirschinger J, Dotzer F, Schuhlen H, Neumann FJ, Fleckenstein M, Pfafferott C, Seyfarth M, Schömig A. Intracoronary stenting and angiographic results: strut thickness effect on restenosis outcome (ISAR-STEREO) trial. Circulation. 2001;103:2816-21. 18. Pache J, Kastrati A, Mehilli J, Schuhlen H, Dotzer F, Hausleiter J, Fleckenstein M, Neumann FJ, Sattelberger U, Schmitt C, Muller M, Dirschinger J, Schömig A. Intracoronary
stenting and angiographic results: strut thickness effect on resteno-sis outcome (ISAR-STEREO-2) trial. J Am Coll Cardiol. 2003;41:1283-8. 19. Briguori C, Sarais C, Pagnotta P, Liistro F, Montorfano M, Chieffo A, Sgura F, Corvaja N, Albiero R, Stankovic G, Toutoutzas C, Bonizzoni E, Di Mario C, Colombo A. In-stent reste-nosis in small coronary arteries: impact of strut thickness. J Am Coll Cardiol. 2002;40:403-9. 20. Rittersma SZ, de Winter RJ, Koch KT, Bax M, Schotborgh CE, Mulder KJ, Tijssen JG, Piek JJ. Impact of strut thickness on late luminal loss after coronary artery stent placement. Am J Cardiol. 2004;93:477-80. 21. Menown IB, Noad R, Garcia EJ, Meredith I. The platinum chromium element stent platform: from alloy, to design, to clinical practice. Adv Ther. 2010;27:129-41.
Supplementary dataAppendix Table 1. Details of TLR cases.Appendix Table 2. Target lesion revascularisation.Appendix Table 3. Late lumen loss.Appendix Table 4. Clinical outcomes of BiOSS studies.

POLBOS II clinical trial
19
EuroIntervention 20
16
;12
1
POLBOS II clinical trial
Appendix Table 1. Details of TLR cases.
DES group
No. FU (mo) DES (type, size) Location Medina at FU FKBI POT SB DES Treat
1 11 SES, 3×18 mm LM 0,0,1 – – – POBA
2 11 PES, 4×15 mm LM 1,0,0 – + – DES
3 12 EES, 2.75×18 mm LCx 1,1,1 – – – DES
4 12 PES, 2.5×16 mm LCx 0,0,1 + – – DES
5 12 PES, 3.5×22 mm LAD 0,0,1 + – – DES
6 12 PES, 3.5×20 mm LM 1,1,1 + – – CABG
7 9 EES, 2.75×18 mm LAD 0,0,1 + – – DEB
8 1 ZES, 2.75×22 mm LAD 1,1,1 + – – POBA
9 12 PES, 3×15 mm LM 0,0,1 – + – DES
BiOSS group
No. FU (mo) BiOSS size Location Medina at FU FKBI POT SB DES Treat
1 12 3.5×2.75×18 mm LAD 1,0,1 – – – DES
2 7 3.75×3×23 mm LAD 1,1,0 – – – DES
3 12 4.25×3.5×18 mm LAD 0,1,1 + – – DES
4 12 4.25×3.5×18 mm LAD 1,0,0 – + – POBA
5 5 4.25×3.5×15 mm LM 1,1,1 – – – CABG
6 5 4.25×3.5×23 mm LM 1,1,1 – + – CABG
7 12 3.75×3×15 mm RCA 1,1,1 – – – DES
8 3 3.5×3×23 mm LAD 0,0,1 + – – DES
9 12 3.5×3×15 mm LAD 0,0,1 – – – POBA
10 5 3.5×2.75×18 mm LM 0,1,1 – – – DES
Appendix Table 2. Target lesion revascularisation.
Stent typeTotal population LM subgroup Non-LM subgroup
n % n % n %
BiOSS 10/102 9.8% 3/36 8.3% 7/66 10.6%
rDES 9/100 9% 4/38 10.5% 5/62 8%
Paclitaxel 5/22 22.7% 1/5 20% 4/17 23.5%
Everolimus 2/46 4.3% 1/16 6.25% 1/30 3.3%
Sirolimus 1/24 4.2% 1/11 9.1% 0/13 0%
Biolimus 0/6 0% 0/4 0% 0/2 0%
Zotarolimus 1/2 50% 1/2 50% 0/0 0%
“Olimus” 4/78 5.1% 3/38 7.9% 1/62 1.6%
LM: left main; rDES: regular drug-eluting stent
Supplementary data

POLBOS II clinical trial
20
EuroIntervention 20
16
;12
2
Appendix Table 3. Late lumen loss.
Stent type
Late lumen loss (mm)
Total population LM subgroup Non-LM subgroup
MV MB SB MV MB SB MV MB SB
BiOSS 0.28±0.12 0.32±0.16 0.16±0.1 0.15±0.14 0.2±0.1 0.12±0.1 0.36±0.14 0.38±0.12 0.18±0.07
rDES 0.23±0.14 0.26±0.15 0.14±0.06 0.17±0.13 0.21±0.14 0.13±0.07 0.26±0.16* 0.29±0.14* 0.14±0.08
Paclitaxel 0.39±0.2* 0.46±0.17* 0.14±0.05 0.32±0.17* 0.38±0.23* 0.09±0.04 0.42±0.21 0.48±0.15* 0.15±0.09
Everolimus 0.14±0.07* 0.15±0.08* 0.13±0.07 0.12±0.06 0.14±0.06 0.12±0.09 0.15±0.08* 0.16±0.09* 0.13±0.07
Sirolimus 0.26±0.14 0.29±0.18 0.16±0.1 0.18±0.15 0.24±0.11 0.17±0.06 0.32±0.13 0.34±0.21 0.15±0.09
Biolimus 0.15±0.13* 0.20±0.18* 0.13±0.08 0.13±0.11 0.18±0.12 0.12±0.09 0.20±0.14* 0.25±0.15* 0.16±0.08
Zotarolimus 0.29±0.11 0.32±0.15 0.18±0.04 0.29±0.11* 0.32±0.15* 0.18±0.04 – – –
*p<0.05 when compared to corresponding BiOSS LIM LLL value. LM: left main; MB: main branch; MV: main vessel; rDES: regular drug-eluting stent; SB: side branch
Appendix Table 4. Clinical outcomes of BiOSS studies.
POLBOS I POLBOS II FIM registry LMS registry
BiOSS Expert n=120 (%) BiOSS LIM n=102 (%) BiOSS LIM n=60 (%) BiOSS LIM n=74 (%)
MACE 16 (13.1) 12 (11.8) 6 (10) 7 (9.5)
All-cause death 2 (1.7) 1 (1) 1 (1.7) 0
Cardiac death 0 0 0 0
MI 2 (1.6) 2 (1.9) 1 (1.7) 2 (2.7)
Definite ST 1 (0.8) 1 (1) 0 0
Cumulative TLR 14 (11.5) 10 (9.8) 5 (8.3) 5 (6.8)
Clinically driven TLR 7 (5.8) 5 (4.9) 1 (1.7) 3 (4.1)
TVR 19 (15.8) 14 (13.7) 7 (11.7) 9 (12.2)
PCI in another vessel 9 (7.5) 8 (7.8) 8 (13.3) 7 (9.5)

Innovative Co-Cr sirolimus eluting coronary bifurcation stent system
Implant construction allows Bioss stent adjust to vessel curvature
Mid-markerof the delivery system
Distal
ProximalIMPORTANT:
proximal part of the mid marker shall be placed
in the line with carina tip
Before stenting
Stenting
Positioning against carina
Final effect
• Unique configuration of the delivery system ensuring safety and efficacy during the stent implantation procedure
• Delivery system minimizes the negative effects of procedure, protecting the carina tip from being crushed or damaged
• Large cell of the stent in place of side branch entrance gives possibility to enter the SB with any standard size conventional stent
• Precision of implantation procedure thanks to three radiopaque markers

294 Modlińska Str., 03-152 Warsaw, POLAND
ph.: (+48) 22 597 44 00, fax: (+48) 22 597 44 44
e-mail: [email protected], www.balton.pl
● Next-Generation Co-Cr sirolimus eluting bifurcation stent
● New sizes
● Strut thickness 0.07 mm
● Biodegradable polymer
New Generation
INterNatIoNal PateNt
Cobalt-chromium sirolimus eluting coronary bifurcation stent
DIS
TAL
PRO
XIM
AL