Coagulopathy in children
41
WELCOME TO ALL
-
Upload
mohammad-saiful-islam -
Category
Education
-
view
25 -
download
0
Transcript of Coagulopathy in children

WELCOME TO ALL

2
Coagulopathy in children
Dr. Mohammed Saiful IslamResident ( Phase:A),
Department of Paediatric Surgery, BSMMU.Bangladesh.
20/09/2016, Venue: Paediatric surgery class room.

Objectives• To define & understand the extent of
coagulopathy.• A review of coagulation pathways.• Discussions on Platelet disorders.• Key points discussions associated with
coagulation factor disorders.• Perioperative strategies to meet the
challenges of coagulopathy in case of children.

Definition:Group of medical
conditions resulting from deficiency of clotting factors, inhibition of coagulation process or excessive activity of the fibrinolytic system.
Reff: de Gruchy 5th

Bleeding disorders
Coagulopathy

Extent of Coagulopaty:
• VESSEL WALL ABNORMALITIES:
• PLATELETS DISORDER:
• COAGULATION DISORDER:

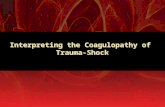
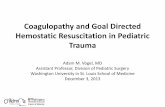
INTRINSIC EXTRINSIC
PROTHROMBIN(II) THROMBIN(III)
FIBRINOGEN
FIBRIN
(I)V
X
Tissue ThromboplastinCollagen
XIIXI
IXVIII
VII
PTPTT Vit.K, Liver
CLOTTING MECHANISM (Easy to keep in mind)

PLATELETS DISORDERS:
• QUANTITATIVE PLATELETS DISORDERs.
• QUALITATIVE PLATELET DYSFUNCTION.

QUANTITATIVE PLATELETS DISORDER (Thrombocytopenia)
Mechanisms:1. Failure of megakaryocytic
maturation.2. Excessive platelets consumption
after their release into circulation i.e ITP, DIC etc.
3. Platelets sequestration in enlarged spleen i.e HYPERSPLEENISM.

QUANTITATIVE PLATELETS DISORDER (Continued…)
S/S:• Petechial cutaneous bleeding,• Intracranial bleeding,• Oozing from mucus membrane &
skin surface. Lab: Decreased platelets count and prolong bleeding time.

(Thrombocytopenia) Causes:
Marrow Disorder• Aplastic anemia.• Haematological
malignancy.• Myelodysplastic
disorder.• B12 defficiency.
Non Marrow Disorder• Immune disorders.• ITP, Drug induced.• Sec: ALL, SLE.• Post transfusion.• DIC.• Human immunodeficiency syndrome. • Hyperspleenism.• Haemangiomas.• Sepsis.• Viral infection.

Thrombocytopenia (Continued…)
• Management:– Rx Underlying cause.– Platelet transfusion.

IDIOPATHIC THROMBOCYTOPENIC PURPURA(ITP)
• An autoimmune antibody IgG is formed against unknown antigen of platelets membrane/surface.
• Antipletelet antibody binds to complement, but platelets are not destroyed by direct lysis.
• Destruction takes place in spleen, where spleenic macrophages destroyes antibody coated platelets.

IDIOPATHIC THROMBOCYTOPENIC PURPURA. (Continued…)
Clinical Features: Often precipitated by viral infection
and usually self limiting. Asymptomatic, not febrile. Present with mucosal/skin bleeding,
mennorrhagia, purpura, petechiae. Females are more affected (2:1
male/female ratio).

IDIOPATHIC THROMBOCYTOPENIC PURPURA. (Continued…) Δ LAB:Platelets below 10,000 /ml.Bone marrow will appear normal.RxPREDNISONONE: 1-2 mg/kg/day. Immunoglobulin: 1g/kg/day 2-3 days.DANAZOLE: 600mg/day response rate is 50%IMMUNOSUPPERESSIVE DRUGS: i-e vincristine,
vinblastine, azathioprine, cyclosporin, cyclophosphomide.
SPLEENECTOMY.Prognosis:
Good, if disease is initially controlled with prednisolone, Spleenectomy is definite Rx.

QUALITATIVE PLATELET DISORDER
CONGENITAL:• Glanzmann’s
thrombasthenia.• Bernard souliar
syndrome.• Von Willibrand’s
disease.
ACQUIRED • Myeloproliferative disorder.• Uremia.• Drugs i-e NSAIDS Aspirin.• Autoantibody.• Fibrin degradation products.

QUALITATIVE PLATELET DISORDERGLANZMANN’s THROMBASTHENIA:Autosomal recessive disorder.Lack of receptors (glycoprotein Ib & IIIa)
for fibrinogen on platelets.Platelets fails to aggregate in respons to
ADP, collagen, thrombin.Clinical Features: Mucosal bleedingLAB:Platelets no’s and morphology are normal B.T is prolonged Rx:Platelet transfusion

QUALITATIVE PLATELET DISORDERBERNARD SOULIER SYNDROME:Autosomal recessive intrinsic platelets disorder.Due to lack of glycoprotein (Gp1b), receptor for
vonWillibrand’s factor.Clinical Features:Presents with mucosal bleeding and post
operative oozes.LAB:Thrombocytopenia may be present, and Platelets
are abnormally large in size.BT is prolonged Von Willibrand’s factor Normal .Rx:Platelet transfusion

QUALITATIVE PLATELET DISORDERVON-WILLIBRAND’S DISEASE:
• Autosomal dominant (gene for vWF is located on chromosome 12.)
• vWF is synthesized by endothelial cells and megakaryocytes.
• It acts as carrier protein for factor VIII by non-covalent bond.
• A defect therefore leads to decreased plasma factor VIII level.

VON-WILLIBRAND’S DISEASE (Continued….)
• It also forms bridges between platelets and sub endothelium.
• There fore defect of vWF leads to prolonged bleeding.

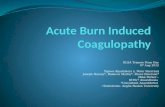
VON-WILLIBRAND’S DISEASE (Continued….)
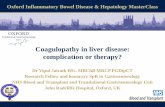
Figure: Structure and function of factor VIII-von Willebrand factor (vWF) complex.

VON-WILLIBRAND’S DISEASE (Continued….)
Clinical Features:• Mucosal bleeding (mild-massive)LAB:• Reduced level of vWF.• Secondary reduction in factor VIII.• Prolonged bleeding time (B.T).

VON-WILLIBRAND’S DISEASE (Continued….)
Rx:• MILD HAEMORRHAGES:
Desmopressin 0.3 μg/kg, after which vWF levels usually raise 3 units in 30-90 minutes.
• MASSIVE HAEMORRHAGES:Factor VIII transfusion.

COAGULATION DISORDER: Coagulation factor disorder can be either due to single factor def., i.e. a “congenital deficiency”, e.g factor VIII resulting in HAEMOPHILIA-A or due to multiple factor defficiency which is an ‘’acquired condition” e.g Sec: to liver disease or warfarin therapy.

• HEAMOPHILIA – A (CLASSIC / TRUE HAEMOPHILIA)
• HAEMOPHILLIA – B (CHRISTMAS DISEASE).
• Other specific factor deficiency (e.g. Factor І, ІІ, ІІІ etc. deficiency).
COAGULATION DISORDER:CONGENITAL BLEEDING DISORDER:

COAGULATION DISORDERACQUIRED BLEEDING DISORDER
• DIC• Liver disease • Renal disease• Vitamin K deficiency• Massive blood transfusion• Anticoagulant drugs.

HAEMOPHILIA• X-linked recessive disorder. • Due to deficiency of factor VIII (Haemophiia A)
or factor IX (Haemophiia B) .

HAEAMOPHILIA (Continued….)
C/F:• Bleeding occurs as bruising at the age of 6
months.• Trauma results in excessively bleeding.• Recurrent bleeding /hemorrhage in knee, elbow,
ankle, and hip. (Hemarthrosis).• Mucus membrane /internal bleeding of mouth,
lips, gums, brain and kidney also occur.• Muscle haematoma esp. calf and Psoas muscle .Rx• Cryoprecipitate or Factor VIII infusion ( in
Haemophiia A) & Factor IX infusion (in Haemophilia B)

HAEAMOPHILIA (Continued….)
LONG TERM COMPLICATIONsCOMPLICATION due to repeated
hemorrhage:– Arthropathy of large joints eg knee, elbow– Muscle atrophy due to haematoma– Mononeuropathy due to pressure of
haematoma.COMPLICATION due to therapy
– Antifactor VIII antibody develops.– Virus transmission Hepatitis B,C + HIV etc.

HAEAMOPHILIA (Continued….)
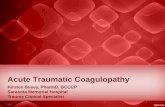
Figure: Haemarthrosis & Arthropathy.

SURGERY IN A CHILD WITH HAEMOPHILLIA:
• In minor Surgery:Factor VIII should be at least 50% of the normal predicted value.
• In Major Surgery: Factor VIII should be 100%. Half life of Factor VIII is 8 to 12 hours. Factor VIII should be substituted just
before surgery & 12 hours after the initial dose ( Target is to pass the time of reactionary haemorrhage).

Calculation of Factor VІІІ
% Desired Χ Wt in Kg
• Amount of Factor VІІІ = K
Here, value of K is 1.5 for Haemophilia A & 0.75 for Haemophilia B.

DISSAMINATED INTRAVASCULAR COAGULATION
Disseminated Intravascular Coagulation (DIC) is a thrombo-haemorrhagic disorder appearing as a secondary complication of several diseases, where there is consumption of platelets and clotting factors in the circulation as well as secondary activation of plasminogen fibrinolytic system.

DIC:CAUSES
A Infection: 1. Gram negative
septicaemia 2.
Meningococcaemia3.
Pneumococcaemia4.Malaria
B. Massive injury:
1. Massive trauma
2. Extensive burn (severe burn)
3. Extensive surgery (brain, lung, prostate, etc.)
C. Carcinoma: 1. Pancreas 2. Lungs 3. Stomach 4. Prostate, etc.
D. Others: 1. Transfusion
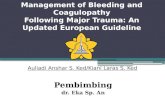
reaction 2. Fat embolism 3. Snake bite 4. Shock, etc.

Fig: Pathophysiology of disseminated intravascular coagulation.

DIC (Continued….)CLINICAL FEATURES:• Bleeding & thrombosis, bleeding is more
than thrombosis.• Features of complications.LAB:• Thrombocytopenia• Prolong PT• APTT may be normal/increased• Low fibrinogen• Increased level FDP/D-dimmer

Treatment of DICRx. Underlying cause.General Measures: Correction & prevention of :• Dehydration• Renal failure• Acidosis and • ShockReplacement:• Platelets transfusion if platelets counts below
10,000/ml• Cryoprecipitate to maintain plasma fibrinogen level
above 150 mg/dl • FFP• Heparin, if there is DVT, Pulmonary thrombosis.

WARCRAFT FOR SURGERY IN A CHILD HAVING
ANTICOAGULANT THERAPY
• If patient on oral anticoaguant:Dose adjustment for INR within 2.5 to 3.5.During surgery INR should be 1.5 or less.
• If patient on Parenteral anticoaguant:Per operative APTT should be within 1.5 to
2.5 times of normal range.

WARCRAFT FOR SURGERY (Continued….)
• During emergency surgery: Inj. Vitamin K should be administered.
FFP & Factor concentrate of ІІ, VІІ, ІX & X should be kept in hand.
Per operative & Post operative monitoring of PT, INR.

WARCRAFT FOR SURGERY (Continued….)
• During elective surgery:• Minor surgery:
» Oral anticoagulant should be stopped 2 to 3 days prior to surgery.
• Major surgery:» Oral anticoagulant should be stopped 4
to 5 days prior to surgery.» Then low molecular weight heparin
should be started.» Heparin should be stopped 4 hours prior
to surgery & restarted 12 hours after surgery.

THANK YOU