
CLOSTRIDIUM DIFFICILE INFECTION UPDATE - Critical … · CLOSTRIDIUM DIFFICILE INFECTION UPDATE ......
25
CLOSTRIDIUM DIFFICILE INFECTION UPDATE Richard Siebert Critical Care Fellow Steve Biko Academic Hospital
Transcript of CLOSTRIDIUM DIFFICILE INFECTION UPDATE - Critical … · CLOSTRIDIUM DIFFICILE INFECTION UPDATE ......

CLOSTRIDIUM DIFFICILE INFECTION
UPDATE
Richard Siebert
Critical Care Fellow
Steve Biko Academic Hospital

WHAT’S NEW ?
• Reseach and therapy based on the gut microbiota has grown substantially and
evidence for bacteriotherapy and more tailored bacteriotherapy is growing.
• PCR testing has become widely avalaible with one step and two step protocols making
diagnostic testing more realiabe and faster.
• Community aquired ( >12 weeks since being in a health care facility) has emerged

• 453000 cases in the US in 2011
• 29000 deaths !
• Considered a public health emergency in
US., Canada and Europe
• >¼ of infections are community acquired
• Cost to US $1.5 Billion 2011 , projected
cost to Europe 3.7 euros in 2013
• South african data limited
N Engl J Med
Volume 372(9):825-834February 26, 2015

SOUTH AFRICAN DATA
• Single centre prospective trial : GSH 651 patients
• N Rajabally, G Watermeyer SouthAfr Med J 2013;103(3):168-172.
• Stools screened for toxin A if + further PCR testing
• Patient’s younger - 41
• Antibiotic exposure
• Inflamatory bowel disease
• Very low rate of HA-CDI compared to US/European studies

CLOSTRDIUM DIFFICILE
• First isolated in 1935 in healthy infants
• Highly prevelant in infants as the microbiota matures Clos. Diff disappears !
• Antibodies deveoped to toxin A and B give
• Non invasive gram positive , spore forming toxin producing bacillus which colonizes the colon
• Spores are heat , acid , alcohol and antibiotic resistant
• Diarrhoea is caused by Toxin A and B and
• The binary toxin emerging as a virulent factor in NAPI/027/B1 strain
• tcdA , tcdB and tcdC genes control the production of toxin A and B
• Virulence of the infecting strain ( BI/NAP1/027) and host immune response determine the
clinical expression of the disease
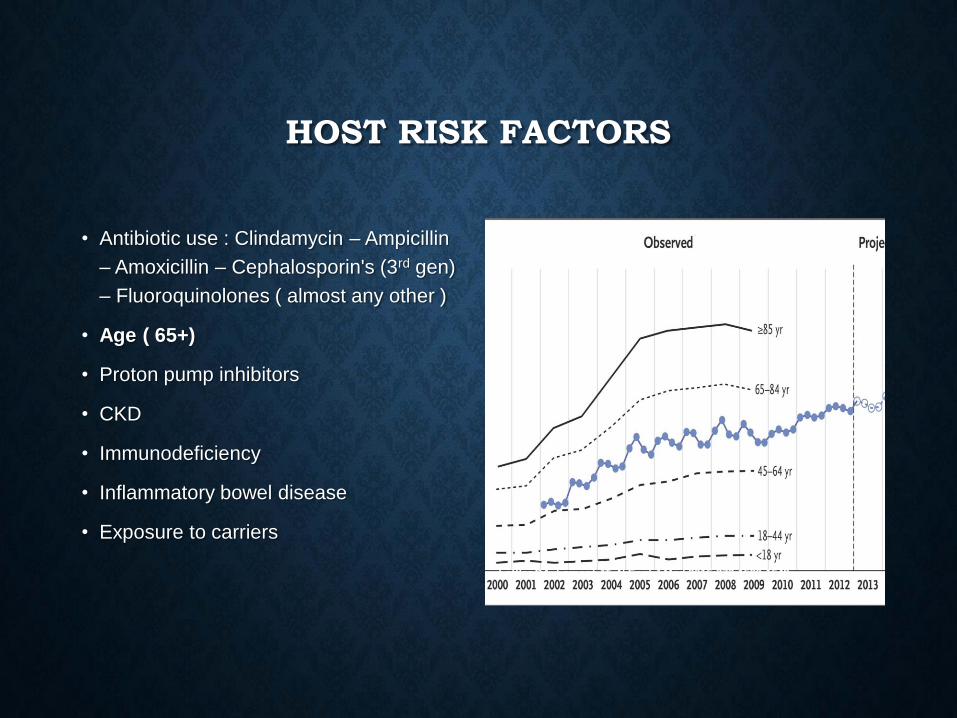
HOST RISK FACTORS
• Antibiotic use : Clindamycin – Ampicillin
– Amoxicillin – Cephalosporin's (3rd gen)
– Fluoroquinolones ( almost any other )
• Age ( 65+)
• Proton pump inhibitors
• CKD
• Immunodeficiency
• Inflammatory bowel disease
• Exposure to carriers
Leffler DA, Lamont JT. N Engl J Med 2015;372:1539-1548

GUT MICROBIOTA
• NIH human microbiome project and European Metgenomics of the human intestinal tract
consortium
• Healthy microbiota as certain features :
• Large number of micro-organisms
• Large number of species
• Increased number of certain bacterial phyla : ie Furmicutes and Bacteroidetes
• Decreased number of certain phyla : ie Proteobacteria
• A number of diseases' are associated with an abnormal microbiota including metabolic
disturbances i.e.#. obesity / IBD / Colon cancer
Robert et al : Gastroenterology, 2014-05-01, Volume 146, Issue

MICROBIOTA
Gastroenterology.
Shanahan, Fergus; Quigley, Eamonn M.M.. Published May 1, 2014. Volume
146, Issue 6. Pages 1554-1563.RUPNIK M. N ENGL J MED 2015;372:1566-1568.
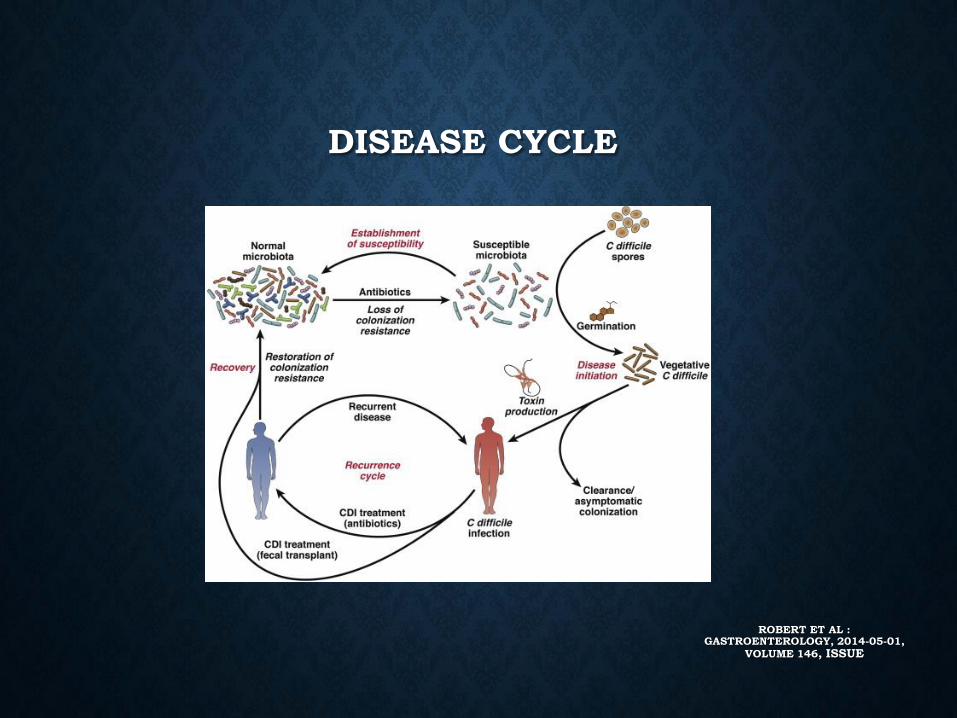
DISEASE CYCLE
ROBERT ET AL : GASTROENTEROLOGY, 2014-05-01,
VOLUME 146, ISSUE

DIAGNOSIS
• > 3 unformed stools> 24h or
• Radiological evidence of ileus or toxic megacolon and
• Positive stool test or endoscopic or histopathologic evidence of pseudomembraneous
colitis

STOOL TEST
• Gold standard test : Toxigenic culture + Cell cytotoxicity assay
• Rapid test
• EIA –GDH
• EIA – Toxin A+B
• NAAT – ( Nuclear acid amplification testing)
• LAMP - ( Loop-mediated isothermal amplification)

LABORATORY DIAGNOSIS
GDH and
EIA
Single stool
Specimen that
‘takes shape of
container’
Both
+ve
Both -veTest
Positive
Test negativeNo further testing
required
GDA
+ve
EIA -ve
PCR for Toxin
gene+ve -ve
Test negativeNo further testing
required
Test Positive
P. Marik Evidence based critical care 3rd Rd.

MARKERS OF DISEASE SEVERITY
• ( BI/NAP1/027) strain ;3 x increased mortality 1
• WBC > 15000/mm3
• > CREATINE > 1.5 BASELINE
• HYPOTENSION , ILEUS , MEGAOLON
1. Loo VG NEJM 2005 ; 353 2442-9
2. ISDA CDI guideline 2010
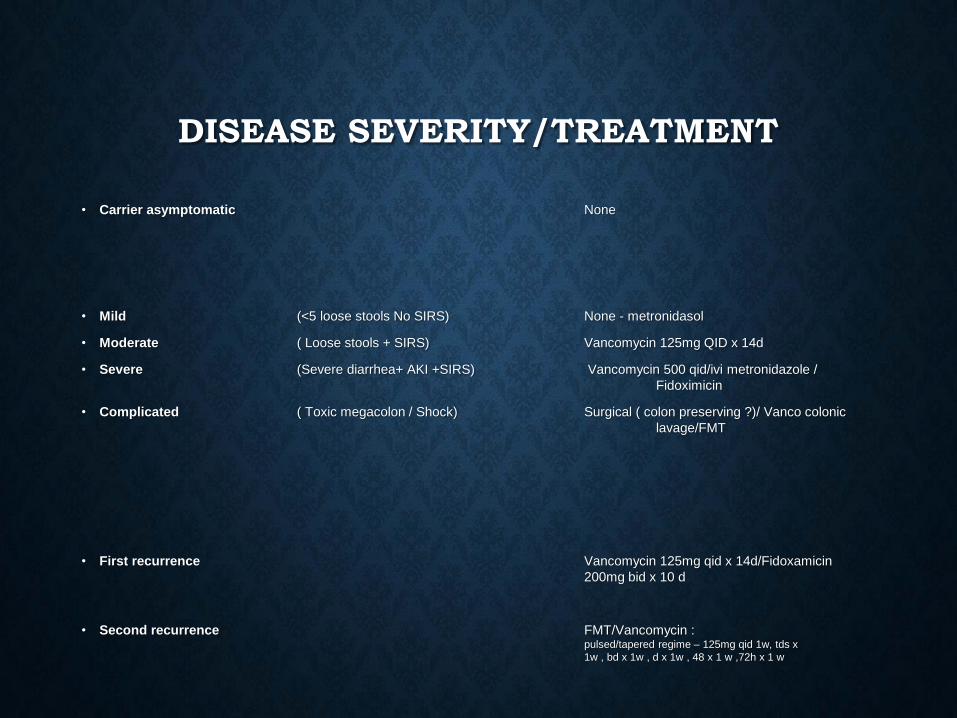
DISEASE SEVERITY/TREATMENT
• Carrier asymptomatic None
• Mild (<5 loose stools No SIRS) None - metronidasol
• Moderate ( Loose stools + SIRS) Vancomycin 125mg QID x 14d
• Severe (Severe diarrhea+ AKI +SIRS) Vancomycin 500 qid/ivi metronidazole /
Fidoximicin
• Complicated ( Toxic megacolon / Shock) Surgical ( colon preserving ?)/ Vanco colonic
lavage/FMT
• First recurrence Vancomycin 125mg qid x 14d/Fidoxamicin
200mg bid x 10 d
• Second recurrence FMT/Vancomycin :pulsed/tapered regime – 125mg qid 1w, tds x
1w , bd x 1w , d x 1w , 48 x 1 w ,72h x 1 w

OTHER TREATMENTS OPTIONS
• Teicoplanin
• Tigecycline
• Ramoplanin
• Rifaximin
• Nitazoxanide
• Toxin binders – televomer
• Probiotics ? Kefir
• Vaccines

PROBIOTICS ?
• Inconclusive ?
• Probiotic associated bacteraemia and fungemia in critical ill and immune deficient
patients a concern
• Recent case series using kefir ( fermented milk) with staggered and tapered doses of
vancomycin/metronidasole showed less recurrences 1.
1. Bakken et al Clinical Infect Disease 2014;59)

RELAPSES
• 25%-30% of cases
• Second and 3rd relapses are problematic
• Standard treatment is Vancomycin Pulse/ tapered regime but what to do when it doesn’t
work ?

TREATMENT FOR RECURRENCE
Fidaxomicin versus Vancomycin for Clostridium difficile Infection
Treatment with Monoclonal
Antibodies against Clostridium
difficile Toxins
N Engl J Med
Volume 364(5):422-431February 3, 2011
N Engl J Med
Volume 362(3):197-205
January 21, 2010

FECAL MICROBIOTA TRANSPLANT
• First described by Chinese 4th century to treat severe diarrhea
• Coprophagia occurs in the animal kingdom
• Used by vetenarians
• First case published of FMT for CDI was in 1983
• Currently FMT is being used more frequently ( 500 cases published for CDI)with
guidelines recently set up for indications and preparation of FMT

Duodenal Infusion of Donor Feces for Recurrent Clostridium difficile
Els van Nood, M.D., Anne Vrieze, M.D., Max Nieuwdorp, M.D., Ph.D., Susana Fuentes, Ph.D., Erwin G. Zoetendal,
Ph.D., Willem M. de Vos, Ph.D., Caroline E. Visser, M.D., Ph.D., Ed J. Kuijper, M.D., Ph.D., Joep F.W.M. Bartelsman, M.D., Jan G.P. Tijssen, Ph.D., Peter Speelman, M.D., Ph.D., Marcel G.W. Dijkgraaf, Ph.D., and
Josbert J. Keller, M.D., Ph.D.
N Engl J Med
Volume 368(5):407-415January 31, 2013

From Stool Transplants to Next-Generation Microbiota Therapeutics
Gastroenterology.
Petrof, Elaine O.; Khoruts, Alexander. Published May 1, 2014. Volume 146, Issue 6.
Pages 1573-1582.
Open bioma stool banks ?

Update on Fecal Microbiota
Transplantation 2015: Indications,
Methodologies, Mechanisms, and
Outlook
Gastroenterology, 2015-07-01, Volume 149, Issue 1, Pages 223-237
Contraindications
- AB in the last 3 months
- Metabolic syndrome
- GI illness / malignancy/surgery
- Autoimmune diseases
- Chronic pain syndroms
- Infectious diseases : numerous to be tested

Conclusions and Relevance Among patients with CDI
who clinically recovered following treatment with
metronidazole or vancomycin, oral administration of
spores of NTCD-M3 was well tolerated and appeared to
be safe. Nontoxigenic C difficile strain M3 colonized the
gastrointestinal tract and significantly reduced CDI
recurrence.
Administration of Spores of Nontoxigenic Clostridium difficile Strain M3 for Prevention of
Recurrent C difficile Infection: A Randomized Clinical Trial
JAMA. 2015;313(17):1719-1727.

PREVENTION
• Antibiotic use : antibiotic stewardship
• Decontamination and isolation
Vaccine development against toxoids of Tcd A and
TcD B



















