Close monitoring of serum HBV DNA levels and liver enzymes levels is most useful in the management...
2
Close monitoring of serum HBV DNA levels and liver enzymes levels is most useful in the management of patients with occult HBV infection To the Editor: We read with interest the study by Zacharakis et al. [1] regarding the role of serial measurement of HBV DNA levels in Greek patients with chronic HBeAg( ) hepatitis B infection. We agree that serial HBV DNA le- vel assessment may be crucial in the prediction of the natural history of HBeAg( ) patients, indeed, HBV car- riers who are negative for HBeAg may replicate HBV to low levels and reactivation of HBV may occur spontane- ously or as a result of immunosuppression. Similarly, HBsAg negative patients with occult HBV infections may reactivate in several contexts and such HBsAg neg- ative patients were also shown to be associated with high risk of severe liver disease including cirrhosis or hepato- cellularcarcinoma. We collected data concerning occult HBV infections studying a group of 26 patients (15 men, mean age 48) suffering from cryptogenetic hepati- tis. Patients remained negative at the time of diagnosis for HBsAg by three different immunoassays (AgHBs plus, Bio-rad, HBsAg Ultra, bioMerieux, HBsAg Enzy- How reproducible are rat steatosis models using high-fat diets? Reply I To the Editor: In their Letter to the Editor, Marsman et al. [1] raised the question of the reproducibility of Lieber–Decarli (LDC) high-fat diets for the induction of fatty liver in rats [2]. The data presented in the letter revealed a strik- ing difference in gains in body weight between the rats in Marsman’s study and those in Lieber’s study. The rats (Wistar, sex unknown, N = 5) reported by Marsman et al. had gained 98 g after 21 days of the LCD high- fat diet ad libitum, whereas in Lieber’s study, the rats (male Sprague–Dawley, N = 22) had gained 173 g. Thus daily body weight gain in Marsman’s study (4.2 g) was only half of that in Lieber’study. (8.2 ± 1.1 g), suggest- ing an improper methodology in liquid diet feeding, de- spite, as it was claimed, ‘‘following the authors’ exact methodology”. Furthermore, no caloric intake of the high-fat diet or the control standard diet were indicated in Marsman’s letter, while Lieber et al. reported a total caloric intake of 1767 ± 42 kcal in 3 weeks and 86 ± 1.7 kcal daily and a comparable intake of the stan- dard diet. Indeed, gains in body weight of rats (4.2 g/ day) in Marsman’s feeding protocol were nearly identi- cal to those of rats (4.7 ± 0.1 g, N = 12) fed a restricted high-fat diet (two-thirds of the amount spontaneously consumed by rats fed ad libitum) described by Lieber et al. Since dietary restricted rats developed only modest steatosis compared to panlobular steatosis in rats fed ad libitum, one may wonder whether the lack of fatty liver induction in Marsman’s feeding protocol is the result of a lower caloric intake caused by an insufficient con- sumption of the high-fat diet, reminiscent of the dietary restriction protocol in Lieber’s study. Furthermore, body weight gains in either ad libitum or dietary re- stricted feeding, and associated fatty changes were reproduced in a later study published in Journal of Hepatology [3]. It is imperative that Marsman et al. reassess the liquid diet feeding methodology to ensure that both caloric intake and gains in body weight are equivalent to those described by Lieber et al. [2,3]. Until then it is presumptuous to conclude that the Lieber– Decarli high-fat diet model is not reproducible for the pathogenesis of hepatosteatosis in rats. References [1] Marsman HA, Al-Saady RL, Heger M, van Gulik TM. How reproducible are rat steatosis models using high fat diets? J Hepatol 2009;51:822–823. [2] Lieber CS, Leo MA, Mak KM, Xu Y, Cao Q, Ren C, et al. Model of nonalcoholic steatohepatitis. Am J Clin Nutr 2004;79: 502–509. [3] Lieber CS, Decarli LM, Leo MA, Mak KM, Ponomarenko A, Ren C, et al. Beneficial effects versus toxicity of medium-chain triacyl- glycerols in rats with NASH. J Hepatol 2008;48:318–326. Ki M. Mak Mount Sinai School of Medicine, Medical Education/Anatomy & Functional Morphology, 1 Gustave Levy Place, New York, NY 10029, USA Tel.: +1 212 2417275; fax: +1 212 8601174. E-mail address: [email protected] Maria A. Leo James J. Peters VA Medical Center, Bronx, New York, NY, USA doi:10.1016/j.jhep.2009.05.019 q The authors are the developers of the Lieber–Decarli (LDC) high- fat diet for the induction of fatty liver in rats. 824 Letters to the Editor / Journal of Hepatology 51 (2009) 821–828
-
Upload
isabelle-chemin -
Category
Documents
-
view
214 -
download
0
Transcript of Close monitoring of serum HBV DNA levels and liver enzymes levels is most useful in the management...

How reproducible are rat steatosis models using high-fat diets? Reply I
Ki M. MakMount Sinai School of Medicine,
Medical Education/Anatomy & Functional Morphology,
1 Gustave Levy Place, New York, NY 10029, USA
Tel.: +1 212 2417275; fax: +1 212 8601174.
E-mail address: [email protected]
Maria A. LeoJames J. Peters VA Medical Center, Bronx, New York,
824 Letters to the Editor / Journal of Hepatology 51 (2009) 821–828
To the Editor:
In their Letter to the Editor, Marsman et al. [1] raisedthe question of the reproducibility of Lieber–Decarli(LDC) high-fat diets for the induction of fatty liver inrats [2]. The data presented in the letter revealed a strik-ing difference in gains in body weight between the rats inMarsman’s study and those in Lieber’s study. The rats(Wistar, sex unknown, N = 5) reported by Marsmanet al. had gained 98 g after 21 days of the LCD high-fat diet ad libitum, whereas in Lieber’s study, the rats(male Sprague–Dawley, N = 22) had gained 173 g. Thusdaily body weight gain in Marsman’s study (4.2 g) wasonly half of that in Lieber’study. (8.2 ± 1.1 g), suggest-ing an improper methodology in liquid diet feeding, de-spite, as it was claimed, ‘‘following the authors’ exactmethodology”. Furthermore, no caloric intake of thehigh-fat diet or the control standard diet were indicatedin Marsman’s letter, while Lieber et al. reported a totalcaloric intake of 1767 ± 42 kcal in 3 weeks and86 ± 1.7 kcal daily and a comparable intake of the stan-dard diet. Indeed, gains in body weight of rats (4.2 g/day) in Marsman’s feeding protocol were nearly identi-cal to those of rats (4.7 ± 0.1 g, N = 12) fed a restrictedhigh-fat diet (two-thirds of the amount spontaneouslyconsumed by rats fed ad libitum) described by Lieberet al. Since dietary restricted rats developed only modeststeatosis compared to panlobular steatosis in rats fed ad
libitum, one may wonder whether the lack of fatty liverinduction in Marsman’s feeding protocol is the result ofa lower caloric intake caused by an insufficient con-sumption of the high-fat diet, reminiscent of the dietaryrestriction protocol in Lieber’s study. Furthermore,
Close monitoring of serum HBV DNmost useful in the management of p
q The authors are the developers of the Lieber–Decarli (LDC) high-fat diet for the induction of fatty liver in rats.
body weight gains in either ad libitum or dietary re-stricted feeding, and associated fatty changes werereproduced in a later study published in Journal ofHepatology [3]. It is imperative that Marsman et al.reassess the liquid diet feeding methodology to ensurethat both caloric intake and gains in body weight areequivalent to those described by Lieber et al. [2,3]. Untilthen it is presumptuous to conclude that the Lieber–Decarli high-fat diet model is not reproducible for thepathogenesis of hepatosteatosis in rats.
References
[1] Marsman HA, Al-Saady RL, Heger M, van Gulik TM. Howreproducible are rat steatosis models using high fat diets? J Hepatol2009;51:822–823.
[2] Lieber CS, Leo MA, Mak KM, Xu Y, Cao Q, Ren C, et al.Model of nonalcoholic steatohepatitis. Am J Clin Nutr 2004;79:502–509.
[3] Lieber CS, Decarli LM, Leo MA, Mak KM, Ponomarenko A, RenC, et al. Beneficial effects versus toxicity of medium-chain triacyl-glycerols in rats with NASH. J Hepatol 2008;48:318–326.
A levels and liver enzymes levels isatients with occult HBV infection
NY, USA
doi:10.1016/j.jhep.2009.05.019
To the Editor:
We read with interest the study by Zacharakis et al.[1] regarding the role of serial measurement of HBVDNA levels in Greek patients with chronic HBeAg(�)hepatitis B infection. We agree that serial HBV DNA le-vel assessment may be crucial in the prediction of thenatural history of HBeAg(�) patients, indeed, HBV car-riers who are negative for HBeAg may replicate HBV tolow levels and reactivation of HBV may occur spontane-ously or as a result of immunosuppression. Similarly,
HBsAg negative patients with occult HBV infectionsmay reactivate in several contexts and such HBsAg neg-ative patients were also shown to be associated with highrisk of severe liver disease including cirrhosis or hepato-cellularcarcinoma. We collected data concerning occultHBV infections studying a group of 26 patients (15men, mean age 48) suffering from cryptogenetic hepati-tis. Patients remained negative at the time of diagnosisfor HBsAg by three different immunoassays (AgHBsplus, Bio-rad, HBsAg Ultra, bioMerieux, HBsAg Enzy-

Isabelle Chemin *
Olivier GuillaudINSERM – U871,
151 Cours A. Thomas, 69003 Lyon, France* Tel.: +33 4 37497417.
E-mail address: [email protected] (I. Chemin).
Philippe Chevallier QueyronLaboratoire de Virologie Nord,
Hospices Civils de Lyon, Lyon, France
Christian TrepoHotel-Dieu – Hepatogastroenterologie, Lyon, France
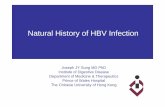
GGT N - ALAT NALAT N - GGT aNALAT aN - GGT aNALAT aN - GGT N
67 %
14%
11%7%
Fig. 1. HBV infection parameters overtime. (A) Liver enzyme levels for all patients and all dates (n = 274), GGT (gamma glutamyl transpeptidase),
ALAT (alanine amino transferase); N: normal, aN: abnormal. (B) Maximal viral load measured by quantitative PCR [2] during the follow-up of each
patient (n = 26). (C) Representation of the follow-up of one of the occult HBV patients considering ALAT level and HBV viral load.
Letters to the Editor / Journal of Hepatology 51 (2009) 821–828 825
gnost, Dade Behring). A total of 274 serum sampleswere tested showing elevation of ALT, GGT or bothin 80% of the cases (Fig. 1A). A high dynamic in viralloads was observed and may reach 106 or 107 HBV gen-ome per ml as detected by light cycler PCR as shown onFig. 1B and C [2].
Since molecular biology tools are improving it ap-pears that monitoring of HBV chronic infection mayinclude HBV DNA levels. It has recently become evi-dent that HBV may also persist in the form of serolog-ically silent infections, leading to the concept of occultinfection. Such infection may represent a non-negligiblepart of cryptogenetic hepatitis cases whose diagnosisand clinical spectrum remain unclear. In a recent state-ment, occult HBV infection has been defined as thepresence of viral DNA in the liver in the absence ofHBsAg but with low titer or even absence of HBVDNA in serum [3]. Our study as well as the study byZacharakis et al., underline the importance of sequen-tial testing of patients for HBV DNA level, which isa key for assessing liver disease activity and predictingthe risk of cirrhosis or hepatocellularcarcinoma. It isalso the clue to decide on the possibility of adaptedantiviral treatment in order to prevent HBV reactiva-tions or transmission of HBV in the transplantation
context.References
[1] Zacharakis G, Koskinas J, Kotsiou S, Tzara F, Vafeiadis N,Papoutselis M, et al. The role of serial measurement of serum HBVDNA levels in patients with chronic HBeAg(�) hepatitis Binfection: association with liver disease progression. A prospectivecohort study. J Hepatol 2008;49:884–891.
[2] Mrani S, Chemin I, Menouar K, Guillaud O, Pradat P, Borghi G,et al. Occult HBV infection may represent a major risk factor ofnon-response to antiviral therapy of chronic hepatitis C. J MedVirol 2007;79:1075–1081.
[3] Raimondo G, Allain JP, Brunetto MR, Buendia MA, Chen DS,Colombo M, et al. Statements from the Taormina expert meetingon occult hepatitis B virus infection. J Hepatol 2008;49:652–657.
doi:10.1016/j.jhep.2009.06.007