Clonal expansion of immunoglobulin M CD27 B cells in HCV
14
IMMUNOBIOLOGY Clonal expansion of immunoglobulin M CD27 B cells in HCV-associated mixed cryoglobulinemia Edgar D. Charles, 1,2 Rashidah M. Green, 1 Svetlana Marukian, 1 Andrew H. Talal, 2 Gerond V. Lake-Bakaar, 2 Ira M. Jacobson, 2 Charles M. Rice, 1 and Lynn B. Dustin 1 1 Center for the Study of Hepatitis C, Laboratory of Virology and Infectious Disease, Rockefeller University, New York, NY; and 2 Department of Medicine, Division of Gastroenterology and Hepatology, Weill Medical College of Cornell University, New York, NY Hepatitis C virus (HCV) is associated with B-cell lymphoproliferative disor- ders such as mixed cryoglobulinemia (MC) and B-cell non-Hodgkin lymphoma (B-NHL). The pathogenesis of these dis- orders remains unclear, and it has been proposed that HCV drives the pro- liferation of B cells. Here we demon- strate that certain HCV MC subjects have clonal expansions of immuno- globulin M (IgM) IgD low/ CD21 low CD27 B cells. Using RT-PCR to amplify Ig from these singly sorted cells, we show that these predominantly rheuma- toid factor-encoding V H 1-69/J H 4 and V 3-20 gene segment-restricted cells have low to moderate levels of somatic hypermutations. Ig sequence analysis suggests that antigen selection drives the generation of mutated clones. These findings lend further support to the no- tion that specific antigenic stimulation leads to B-cell proliferation in HCV MC and that chronic B-cell stimulation may set the stage for malignant transforma- tion and the development of B-NHL. The finding that these hypermutated, mar- ginal zone-like IgM CD27 B cells are clonally expanded in certain subjects with MC offers insight into mechanisms of HCV-associated MC and B-cell malig- nancy. This study was registered at www.clinicaltrials.gov as NCT00219999. (Blood. 2008;111:1344-1356) © 2008 by The American Society of Hematology Introduction Up to 170 million people worldwide are chronically infected with hepatitis C virus (HCV), which is the leading indication for liver transplantation in the United States and Europe. 1,2 Although hepatocytes are the primary target for HCV infection, mixed cryoglobulinemia (MC), considered a benign B-cell proliferative disorder, can affect up to 50% of HCV patients. 3,4 HCV MC is predominantly characterized by cold-precipitable complexes of monoclonal immunoglobulin (Ig) M kappa () rheumatoid factor (RF), polyreactive IgG, HCV RNA, and HCV structural pro- teins. 3,5,6 MC symptoms range from weakness, arthralgias, and palpable purpura to more severe manifestations, such as neuropa- thy and membranoproliferative glomerulonephritis. 7 HCV infec- tion is also associated with the development of B-cell non-Hodgkin lymphoma (B-NHL). 8-14 The mechanisms by which HCV causes B-cell proliferation (reviewed in Dustin and Rice 15 ) remain puzzling. Several studies have demonstrated the presence of abnormal clonal B-cell populations in the liver and blood of HCV–infected persons. 16-18 Patients with HCV MC and B-NHL frequently have clonal B cells that use Ig heavy chain variable (V H ) 1-69 and Ig V 3 gene segments, 19-22 which can encode RF of the WA idiotype. 23 Chronic antigenic stimulation by HCV may select a clonally expanded B-cell receptor (BCR) repertoire, which later progresses to B-NHL, 24 similar to Helicobacter pylori–induced mucosa-associated lymphoid tissue lymphomas. 25 Consistent with this idea, Ig cloned from an HCV B-NHL patient was shown to bind to the HCV structural protein, E2. However, this Ig does not cross-react with IgG. 26 It has also been suggested that HCV E2 directly activates polyclonal B cells by binding to CD81, a tetraspanin that forms part of the B-cell coreceptor. 27 Furthermore, it was reported that the memory B-cell compart- ment from HCV persons is polyclonally activated and that it contains decreased steady-state levels of CD27 memory cells, which rapidly differentiate independently of the BCR. 28 How- ever, these latter 2 studies fail to account for the clonal IgM restriction frequently seen in HCV MC and B-NHL. Others have proposed that direct HCV infection of B cells may cause oncogenic transformation, particularly through t(14;18) translo- cation. 29,30 Although t(14;18)-positive cells have been detected in HCV-infected patients, they are also present in up to 50% of healthy persons. 31 Moreover, it is controversial whether HCV can infect B cells (Lanford et al 32 and L.B.D., unpublished data, 2007), and this hypothesis also fails to explain the clonal B-cell expansions frequently seen in HCV infection. In support of the polyclonally activated B-cell model, it was recently reported that HCV patients have high levels of activated naive B cells in the blood and that levels of total B-cell activation do not significantly differ between MC and MC persons. 27 These findings contrasted with our earlier finding that most HCV patients had no evidence of circulating activated B cells. 33 This discrepancy led us to analyze peripheral B cells from HCV MC and HCV MC patients. We have found that, in most HCV patients, circulating B cells show no evidence of current or prior activation. However, certain HCV MC pa- Submitted July 17, 2007; accepted October 12, 2007. Prepublished online as Blood First Edition paper, October 17, 2007; DOI 10.1182/blood-2007-07- 101717. The online version of this article contains a data supplement. The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this article is hereby marked ‘‘advertisement’’ in accordance with 18 USC section 1734. © 2008 by The American Society of Hematology 1344 BLOOD, 1 FEBRUARY 2008 VOLUME 111, NUMBER 3 For personal use only. on December 6, 2018. by guest www.bloodjournal.org From
Transcript of Clonal expansion of immunoglobulin M CD27 B cells in HCV

IMMUNOBIOLOGY
Clonal expansion of immunoglobulin M�CD27� B cells in HCV-associatedmixed cryoglobulinemia
Edgar D. Charles,1,2 Rashidah M. Green,1 Svetlana Marukian,1 Andrew H. Talal,2 Gerond V. Lake-Bakaar,2 Ira M. Jacobson,2
Charles M. Rice,1 and Lynn B. Dustin1
1Center for the Study of Hepatitis C, Laboratory of Virology and Infectious Disease, Rockefeller University, New York, NY; and 2Department of Medicine, Divisionof Gastroenterology and Hepatology, Weill Medical College of Cornell University, New York, NY
Hepatitis C virus (HCV) is associatedwith B-cell lymphoproliferative disor-ders such as mixed cryoglobulinemia(MC) and B-cell non-Hodgkin lymphoma(B-NHL). The pathogenesis of these dis-orders remains unclear, and it has beenproposed that HCV drives the pro-liferation of B cells. Here we demon-strate that certain HCV�MC� subjectshave clonal expansions of immuno-globulin M (IgM)���IgDlow/�CD21low
CD27� B cells. Using RT-PCR to amplify
Ig from these singly sorted cells, weshow that these predominantly rheuma-toid factor-encoding VH1-69/JH4 andV�3-20 gene segment-restricted cellshave low to moderate levels of somatichypermutations. Ig sequence analysissuggests that antigen selection drivesthe generation of mutated clones. Thesefindings lend further support to the no-tion that specific antigenic stimulationleads to B-cell proliferation in HCV MCand that chronic B-cell stimulation may
set the stage for malignant transforma-tion and the development of B-NHL. Thefinding that these hypermutated, mar-ginal zone-like IgM�CD27� B cells areclonally expanded in certain subjectswith MC offers insight into mechanismsof HCV-associated MC and B-cell malig-nancy. This study was registered atwww.clinicaltrials.gov as NCT00219999.(Blood. 2008;111:1344-1356)
© 2008 by The American Society of Hematology
Introduction
Up to 170 million people worldwide are chronically infected withhepatitis C virus (HCV), which is the leading indication for livertransplantation in the United States and Europe.1,2 Althoughhepatocytes are the primary target for HCV infection, mixedcryoglobulinemia (MC), considered a benign B-cell proliferativedisorder, can affect up to 50% of HCV patients.3,4 HCV MC ispredominantly characterized by cold-precipitable complexes ofmonoclonal immunoglobulin (Ig) M kappa (�) rheumatoid factor(RF), polyreactive IgG, HCV RNA, and HCV structural pro-teins.3,5,6 MC symptoms range from weakness, arthralgias, andpalpable purpura to more severe manifestations, such as neuropa-thy and membranoproliferative glomerulonephritis.7 HCV infec-tion is also associated with the development of B-cell non-Hodgkinlymphoma (B-NHL).8-14
The mechanisms by which HCV causes B-cell proliferation(reviewed in Dustin and Rice15) remain puzzling. Severalstudies have demonstrated the presence of abnormal clonalB-cell populations in the liver and blood of HCV–infectedpersons.16-18 Patients with HCV MC and B-NHL frequently haveclonal B cells that use Ig heavy chain variable (VH) 1-69 and Ig�V�3 gene segments,19-22 which can encode RF of the WAidiotype.23 Chronic antigenic stimulation by HCV may select aclonally expanded B-cell receptor (BCR) repertoire, which laterprogresses to B-NHL,24 similar to Helicobacter pylori–inducedmucosa-associated lymphoid tissue lymphomas.25 Consistentwith this idea, Ig cloned from an HCV� B-NHL patient wasshown to bind to the HCV structural protein, E2. However, this
Ig does not cross-react with IgG.26 It has also been suggestedthat HCV E2 directly activates polyclonal B cells by binding toCD81, a tetraspanin that forms part of the B-cell coreceptor.27
Furthermore, it was reported that the memory B-cell compart-ment from HCV� persons is polyclonally activated and that itcontains decreased steady-state levels of CD27� memory cells,which rapidly differentiate independently of the BCR.28 How-ever, these latter 2 studies fail to account for the clonal IgM�restriction frequently seen in HCV MC and B-NHL. Others haveproposed that direct HCV infection of B cells may causeoncogenic transformation, particularly through t(14;18) translo-cation.29,30 Although t(14;18)-positive cells have been detectedin HCV-infected patients, they are also present in up to 50% ofhealthy persons.31 Moreover, it is controversial whether HCVcan infect B cells (Lanford et al32 and L.B.D., unpublished data,2007), and this hypothesis also fails to explain the clonal B-cellexpansions frequently seen in HCV infection.
In support of the polyclonally activated B-cell model, it wasrecently reported that HCV� patients have high levels ofactivated naive B cells in the blood and that levels of total B-cellactivation do not significantly differ between MC� and MC�
persons.27 These findings contrasted with our earlier finding thatmost HCV patients had no evidence of circulating activated Bcells.33 This discrepancy led us to analyze peripheral B cellsfrom HCV�MC� and HCV�MC� patients. We have found that,in most HCV patients, circulating B cells show no evidence ofcurrent or prior activation. However, certain HCV�MC� pa-
Submitted July 17, 2007; accepted October 12, 2007. Prepublished onlineas Blood First Edition paper, October 17, 2007; DOI 10.1182/blood-2007-07-101717.
The online version of this article contains a data supplement.
The publication costs of this article were defrayed in part by page chargepayment. Therefore, and solely to indicate this fact, this article is herebymarked ‘‘advertisement’’ in accordance with 18 USC section 1734.
© 2008 by The American Society of Hematology
1344 BLOOD, 1 FEBRUARY 2008 � VOLUME 111, NUMBER 3
For personal use only.on December 6, 2018. by guest www.bloodjournal.orgFrom

tients harbor a substantial population of clonally expandedIgM�Ig��IgDlow/�CD21lowCD27� B cells in the peripheralcirculation. Moreover, these B cells express RF-like Ig that is inmost cases hypermutated, indicating specific antigen-drivenmaturation. Furthermore, phylogenetic analysis suggests thatthis hypermutation is a result of antigen selection. An associa-tion of IgM� memory-like B cells with MC, which itself isassociated with B-NHL, is consistent with a model in whichchronic, specific antigenic stimulation of IgM� B cells predis-poses toward neoplastic transformation.
Methods
Patients
The studies were approved by the Institutional Review Boards at theRockefeller University and New York-Presbyterian Hospitals. Beforeenrollment, written informed consent was obtained from donors in accor-dance with the Declaration of Helsinki. We enrolled HCV Ab�, HCVRNA� subjects whose medical history or physical examination wasconsistent with arthralgias and/or palpable purpura. We additionallyscreened for sensorimotor neuropathy by neurologic examination. All HCVRNA� subjects were HIV Ab�. For controls, we enrolled HCV Ab�, HBV-immunized healthy volunteers at low risk for HIV. We also enrolled HCVRNA�, HCV Ab� patients who had undergone antiviral treatment withpegylated interferon and ribavirin and who subsequently had 2 separateconfirmations of HCV RNA less than 50 IU/mL at least 6 months aftercessation of treatment and were sustained virologic responders.
Blood collection and processing
A total of 50 mL of blood was collected into Vacutainer tubes containingacid-citrate-dextrose solution A (BD Biosciences, Franklin Lakes, NJ) and aserum separator tube (prewarmed to 37°C). We obtained serum by allowingblood to clot at 37°C followed by centrifugation at 800g. Plasma wasobtained by room-temperature centrifugation and was stored at �80°C. Toobtain peripheral blood mononuclear cells (PBMCs), cells were separatedon lymphocyte separation medium (ICN, Costa Mesa, CA) by centrifuga-tion at 800g. The mononuclear cell layer was washed 3 times inphosphate-buffered saline (PBS) supplemented with 1% N-2-hydroxyeth-ylpiperazine-N-2-ethanesulfonic acid (HEPES) and 2% fetal bovine serum.Cells were resuspended at a concentration of 107/mL in RPMI 1640supplemented with 0.5% HEPES, 20% fetal bovine serum, and 7.5%dimethylsulfoxide for cryopreservation. Cells were slowly frozen to �80°Cand maintained at �150°C. Viable cell recovery was typically more than90% as judged by incorporation of an amine-reactive violet dye (LIVE/DEAD Fixable Dead Cell Stain, Invitrogen, Carlsbad, CA).
Clinical tests
To test for MC, we incubated serum at 4°C for 1 week and examined it dailyfor the presence of a cryoprecipitate.34 To determine MC type, anestablished protocol was followed.35 Cryoprecipitate was spun in a 4°Cmicrocentrifuge at 650g for 15 minutes, the supernatant was removed, andthe pellet was vortexed 6 times with 5 mL of ice-cold PBS, each timespinning out the cryoprecipitate for 15 minutes at 650g. The sample wasthen resuspended in 100 �L of PBS and was redissolved by incubation at37°C for 1 hour. Immunofixation was performed for IgM, IgG, IgA, Ig�,and Ig� using an immunofixation kit (Binding Site, Birmingham, UnitedKingdom), following the manufacturer’s instructions. HCV RNA wasquantified by the Roche Amplicor assay (version 2.0, Roche Diagnostics,Branchberg, NJ). HCV genotypes were determined by sequencing of theHCV NS5B region. Liver biopsies were evaluated by pathologists accord-ing to the Scheuer system.36 These actions, in addition to serum alanineaminotransferase (ALT) measurements, were performed as part of HCVpatients’ medical care. We measured plasma IgM RF using ELISA (BethylLaboratories, Montgomery, TX).
Antibodies
The following mouse mAbs were used: anti-CD19, anti-CD20, anti-CD3,anti-IgM, anti-IgD, anti-CD27, anti-CD69, anti-CD5, anti-CD21, andanti-CD25. FITC, phycoerythrin (PE), PE-Cy7, peridinin chlorophyllprotein cyanin 5.5 (PerCP-Cy5.5), allophycocyanin, Alexa Fluor 700,Alexa Fluor 488, and allophycocyanin Cy7 were used as fluorophores.Conjugated mAbs were obtained from BD PharMingen (San Diego, CA).Goat polyclonal F(ab�)2 PE anti-� and biotin anti-� were from SouthernBiotech (Birmingham, AL), and LIVE/DEAD Fixable Dead Cell Stain wasfrom Invitrogen.
Flow cytometric analysis
Cells (7 � 106/sample) were stained with the indicated Abs at RT in PBSsupplemented with 2% (w/v) BSA (Fraction V; Fisher Biotech, Fair Lawn,NJ) and 0.02% NaN3. Cells were incubated with primary and secondaryAbs for 30 minutes each, and were washed thrice after each stain withincubation buffer. Cells were fixed in PBS/2% paraformaldehyde andanalyzed within 1 hour on an LSRII flow cytometer (BD ImmunocytometrySystems, San Jose, CA). Data were analyzed using FlowJo (Tree Star,Ashland, OR). Lymphocytes were identified by forward and side-anglelight scatter characteristics. Dead lymphocytes, identified by positiveLIVE/DEAD stain, were excluded from further analysis.
CDR3 PCR
DNA was recovered from 3 � 106 PBMCs using a QIAamp DNA BloodMini Kit (Qiagen, Valencia, CA). PCR amplification was performed onup to 0.5 �g of DNA with a seminested protocol of amplificationaccording to a well-established procedure.37 The upstream primer wascomplementary to the conserved third framework V region (FR3) of theIgH gene, and the downstream primer annealed to an outer conservedregion of the IgH joining (J) region in the first round of amplification andto an inner conserved sequence of the same J region in the secondround.38 All samples were tested in 2 separate PCR experiments, andclonal and polyclonal CDR3 DNA controls, as well as a wateronly control, were included. At the end of amplification, 15 �L of thereaction mixture was analyzed by 12% polyacrylamide gel electro-phoresis, stained with ethidium bromide, and optically analyzed byultraviolet transillumination. Gels were scanned using an Epson Expres-sion 1600 scanner (Epson America, Torrance, CA) and densitometricanalysis was performed with ImageJ software (National Institutes ofHealth [NIH], Bethesda, MD).39 Clonal expansion was determined bythe presence of one or more discrete, dominant bands within an 80- to120-bp size range, and a polyclonal population was indicated by thepresence of a smear with no specific dominant bands.
Single-cell sorting
For single-cell sorting, incubations and washes were performed as forimmunophenotyping, except incubations were performed on ice in theabsence of added 0.02% NaN3. Moreover, cells were not fixed inparaformaldehyde after staining. Either IgM���CD21lowCD27�,IgM���CD21lowCD27�, IgM���CD5�CD27�, IgM���CD5�CD27�, orIgM���CD27�, single cells were sorted using a MoFlo cell sorter (DakoCytomaton, Ft. Collins, CO), directly seeded into 96-well plates containing4 �L lysis solution (0.5� PBS containing 10 mM DTT, 2 U RNase Inhibitor(Invitrogen) and 3 U Prime RNase Inhibitor (Eppendorf)), and immediatelyfrozen on dry ice. Samples were stored at �80°C.
VH and V� RT-PCR
We followed an established protocol for cloning VH and V� from singleB cells.40 Briefly, RNA was reverse transcribed in 14 �L reactionscontaining random hexamer primers and 50 U Superscript II RT (Invitro-gen) for 55 minutes at 40°C. RT-PCR reactions, primer sequences, andcloning strategy were as previously described.40 For VH, we used a pool offamily-specific sense primers directed to the 5� conserved leader and Vregions, and a downstream antisense primer directed to the first constant
CLONAL EXPANSION OF IgM�CD27� B CELLS IN HCV MC 1345BLOOD, 1 FEBRUARY 2008 � VOLUME 111, NUMBER 3
For personal use only.on December 6, 2018. by guest www.bloodjournal.orgFrom

region of IgM (C�). Amplification was performed using Taq polymerase(Invitrogen). A second round of PCR was performed on this reactionproduct with VH- and JH-specific primers. For V�, we used pooledfamily-specific primers directed to the 5� conserved leader and V� regions,and a downstream antisense primer to the conserved C� region. Weamplified this PCR product with a 5� pan V� primer and a downstream 3� C�
primer. IgH and Ig� variable regions were sent for sequencing (BioticSolutions, New York, NY).
Analysis of somatic hypermutation and phylogeny
The International ImMunoGeneTics information system41 and NIHJoinsolver42 were used to identify the V, D, and J segments and somaticmutations of Ig genes.43 The ratio of replacement (R) and silent (S)
mutations was determined and analyzed according to a binomialdistribution model,44 using a web-based JAVA applet.45 Nucleotidesequences were aligned using Clustal W.46 Phylogenetic trees wereconstructed with MacVector (Accelrys, San Diego, CA), usingdistance-based neighbor-joining analysis performed on Tamura-Neineighbor estimates. Bootstrap analyses were conducted using1000 replicates.
Statistics
Values of clinical tests are reported as means (� SD). To test the nullhypothesis that clonal Ig was not more prevalent among HCV�MC�
subjects, Fisher exact test was used to compute a P value. All othercomparisons used the Kruskal-Wallis test, followed by the Dunn multiplecomparison test, as appropriate. We computed all statistics with Prism(GraphPad, San Diego, CA).
Accession numbers
GenBank accession numbers for the cloned Ig sequences are EF624068-EF624206, EF624208-EF624238, and EU146311-EU146395.47
Results
Characteristics of study subjects
Twenty-five patients with signs or symptoms suggestive ofcryoglobulinemic vasculitis, such as arthralgia, palpable pur-pura, peripheral neuropathy, and glomerulonephritis, were en-rolled. Subsequent tests revealed that 12 of these patients had
Table 1. Characteristics of subjects
CharacteristicHCV Ab�,
N � 16HCV�, Ab�,
N � 10HCV�,N � 25
Age, y
Mean (95% CI) 39.4 (33.8-45.0) 54.6 (47.0-62.3) 53.3 (49.7-56.7)
Median 37 54 54
Range 24-55 39-71 29-69
Males, no. (%) 7 (43.4) 3 (30.0) 9 (36.0)
Race or ethnic group, no. (%)
White 14 (87.5) 7 (70.0) 17 (68.0)
Black 1 (6.2) 0 (0.0) 3 (12.0)
Hispanic 1 (6.2) 2 (20.0) 5 (20.0)
Asian 0 (0.0) 1 (10.0) 0 (0.0)
MC positive, no. (%) 0 (0) 0 (0) 12 (48)
MC indicates mixed cryoglobulinemia.
Table 2. Characteristics of HCV� subjects
Subjectno. Sex Age, y
HCV riskfactor
HCVtreatment
statusALT,IU/mL HCV GT
HCV RNA,IU/mL � 106 Stage Extrahepatic conditions
Plasma [IgM RF],IU/mL
MCtype
HCV� MC�
108 M 57 IVDU Naive 38 1 0.3 ND Arthralgia 137.6 NA
159* M 59 Unknown NR 85 1a 10.1 3 Arthralgia 22.7 NA
162 M 51 IVDU NR 46 1b 0.29 0 Arthralgia 8.5 NA
1087 M 58 IVDU Naive 39 1 0.7 0 Arthralgia 13.6 NA
1148 F 48 Unknown Naive 41 1a 10 2 NHL (in remission), neuropathy 6.4 NA
1235 F 41 Unknown Naive 376 2b 3.9 ND Arthralgia 4.0 NA
1330 F 54 IVDU Naive 35 1a 10 2 Arthralgia, palpable purpura 8.3 NA
1339 M 58 IVDU Naive 60 1 4.25 4 Arthralgia 6.6 NA
1345 M 57 IVDU Naive 29 1a 0.3 ND Arthralgia 6.7 NA
1349 F 53 Transfusion Naive 27 2b 3.1 ND Arthralgia 7.5 NA
1373 F 49 INDU Relapser 29 1a 0.47 3 Palpable purpura 15.0 NA
1419 F 47 IVDU Naive 23 1a 0.83 3 Arthralgia, palpable purpura 6.5 NA
1446 F 67 Transfusion Naive 26 2b 0.6 0 Palpable purpura 60.9 NA
HCV� MC�
192 M 55 Unknown Naive 38 2b 0.66 1 Arthralgia, palpable purpura 10.0 III, IgM�
389* M 55 IVDU NR 52 1a 2 3 Arthralgia, palpable purpura, neuropathy 7.5 II, IgM�
734* M 53 Unknown Naive 117 1a 2.6 1 Arthralgia 32.6 ND
773* F 29 Unknown Naive 148 1b 0.38 4 Arthralgia, palpable purpura 68.8 II, IgM�
880* F 54 Unknown Naive 40 1b 3.08 ND Arthralgia, palpable purpura 46.2 II, IgM�
960* F 46 IVDU Relapser 33 1a 4.2 2 Arthralgia 93.3 II, IgM�
1073* F 46 Unknown NR 38 1a 1.34 2 Arthralgia, palpable purpura, neuropathy 37.0 II, IgM�
1308* F 54 IVDU Naive 95 1a 0.7 1 NHL 237.5 II, IgM�
1403* F 47 IVDU NR 13 1 1.34 4 Palpable purpura, GN, pulmonary hemorrhage 323.9 II, IgM�
1432* F 69 Transfusion Relapser 56 1a 0.03 4 Palpable purpura, hemolytic anemia 35.2 II, IgM�
11502 F 67 Transfusion Naive 41 1a 0.11 2 Arthralgia 21.4 ND
92200* F 57 Transfusion Naive ND 2b 3.1 2 Arthralgia, palpable purpura 5.3 III, IgM�
GT indicates genotype; IVDU, intravenous drug use; NA, not applicable; ND, not determined; NR, nonresponder; NHL, non-Hodgkin lymphoma; INDU, intranasal drug use;and GN, glomerulonephritis.
* Subjects with clonal Ig (as determined by PBMC DNA CDR3 PCR).
1346 CHARLES et al BLOOD, 1 FEBRUARY 2008 � VOLUME 111, NUMBER 3
For personal use only.on December 6, 2018. by guest www.bloodjournal.orgFrom

demonstrable cryoprecipitates. Characteristics of the groups arepresented in Table 1. The HCV Ab� group was completely freeof arthralgia, palpable purpura, and neuropathy. Two HCV�,Ab� subjects had arthralgias. Only HCV� subjects had labora-tory evidence of MC. HCV�, Ab� subjects had previously beeninfected with HCV genotype 1 (n 7), 2b (n 1), 3b (n 1),or HCV of unknown genotype (n 1).
Table 2 describes the characteristics of the HCV-infected group.One HCV�MC� subject (1308) had a triclonal paraproteinemia onserum immunofixation electrophoresis and underwent bone mar-row biopsy, which revealed monotypic B cells with a normalkaryotype, consistent with low-grade NHL. Another HCV�MC�
patient (1148) had NHL in remission after treatment with cyclophos-phamide, doxorubicin, vincristine, and prednisone 1 year beforeenrollment. Compared with MC� subjects, MC� subjects tended tohave more than one MC related symptom or disease. Consistentwith an earlier report,48 monosymptomatic arthralgia was nonspe-cific for MC. IgM RF was not significantly elevated in HCV�MC�
subjects compared with HCV�MC� subjects. In the 10 subjectsin whom MC was typed, the cryoprecipitate was IgM�, and 8 of10 subjects had type II MC.
HCV�MC� patients have clonal B-cell expansions
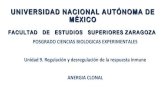
We performed Ig CDR3 PCR on DNA isolated from PBMCs toassess for clonality (Figure 1). HCV�, Ab� patient samplesyielded DNA smears indicating polyclonality. Similarly, allHCV Ab� volunteers had evidence of polyclonal CDR3 (data
not shown). Consistent with previous reports,16,17 clonalCDR3 was highly correlated with the presence of MC. Monoclo-nal or oligoclonal bands with sizes between 80 to 120 basepairs were found in 10 of 12 HCV�MC� subjects, and in 1 of13 HCV�MC� subjects (P .001, Fisher exact test). Theseresults suggest that the elevated IgM and RF frequently seen inHCV�MC� patients is the result of clonal B-cell proliferation.Because, in the absence of overt malignancy, B-cell clonalexpansion requires activation through a B cell’s unique BCR,these data are consistent with the hypothesis that there isan antigenic stimulus that causes MC disease in differentHCV-infected patients.
B cells from certain HCV�MC� subjects are biased toward arestricted IgM���IgDlow/�CD21lowCD27� phenotype
We used flow cytometry to identify the expanded B-cell clonalsubpopulation in this subset of HCV�MC� subjects. We testedwhether our cell freezing protocol altered the detectable B-cellimmunophenotype. We saw no difference in B-cell activationmarkers between fresh and frozen B-cell samples (Figure S1,available on the Blood website; see the Supplemental Materialslink at the top of the online article). We then determined whetherHCV� subjects with clonal Ig had increased percentages ofperipheral B cells (Table 3). After gating on lymphocytes, weexcluded dead cells, and we selected CD19�, CD20� B cells(Figure S2A). B-cell percentages (measured as the percentage oflymphocytes expressing CD19 and CD20) were slightly increased
Figure 1. Ig CDR3 PCR. DNA was isolated from PBMCs,amplified following an established protocol (see “CDR3PCR”) and run on a 12% polyacrylamide gel. PolyclonalCDR3s are indicated by the presence of DNA smearsbetween 80 and 120 bp, the expected size range ofCDR3. Monoclonal and oliglonal CDR3s are reflected bythe presence of solitary, or 2 to 3 bands, respectively, inthe expected size range (A). Densitometric analysis ofgel bands (B). *Patients with MC.
Table 3. B-cell subsets among subject groups
GroupCD19�,CD20�
cells,%
CD19�, CD20� cells, %
��, ��, % ��, CD27�,% IgM�,CD27�, % IgM�, IgDlow/�, % CD21low,CD27�, % % CD5�
HCV Ab�, n 16 14.74 � 5.82 47.42 � 11.30 17.23 � 9.78 13.43 � 7.59 8.21 � 6.20 3.41 � 2.29 22.18 � 5.82
HCV�, Ab�, n 10 13.75 � 6.02 52.07 � 4.98 17.33 � 6.47 10.12 � 4.66 5.61 � 4.41 3.47 � 3.41 13.75 � 6.02
HCV� clonal, n 11 18.55 � 6.73 65.23 � 20.84* 42.40 � 22.16† 35.90 � 25.53* 23.85 � 19.85 20.94 � 17.64* 18.55 � 6.73
HCV� polyclonal, n 14 20.14 � 8.17 51.72 � 6.53 19.22 � 15.33 15.61 � 13.03 9.73 � 9.92 4.86 � 2.80 20.14 � 8.17
Values are means (� SD).*P .05, Dunn multiple comparison test.†P .01, Dunn multiple comparison test.
CLONAL EXPANSION OF IgM�CD27� B CELLS IN HCV MC 1347BLOOD, 1 FEBRUARY 2008 � VOLUME 111, NUMBER 3
For personal use only.on December 6, 2018. by guest www.bloodjournal.orgFrom

in some HCV� patients compared with HCV Ab� volunteers andHCV�, Ab� patients. There were no differences in B-cell percent-ages between HCV�MC� and HCV�MC� groups. When wecalculated the absolute numbers of B cells by multiplying theB-cell percentages by the corresponding total lymphocyte counts,we found no differences among the groups (data not shown). Thesefindings confirmed our earlier study reporting normal B-cellfrequencies in most HCV� subjects.33 We did not detect signifi-cantly different percentages of the activation markers CD69 andCD25 among B cells from our patient groups (data not shown),suggesting that B cells are not polyclonally activated during HCVinfection.
Consistent with the fact that MC RF is IgM�, we found thatcertain HCV�MC� patients had B cells with a tremendous �light chain bias, exhibiting �/� ratios up to 90:10 (Figure S3A).This ratio was significantly increased among HCV� subjectswith clonal, as opposed to polyclonal, CDR3 (Table 3). Most ofthe �� and IgM� B cells in these patients expressed CD27(Figure S3B,C), which is a marker for memory B cells.49 HCV�
subjects with clonal, as opposed to polyclonal, CDR3 hadsignificantly increased percentages of ��CD27� and IgM�CD27�
B cells. Most of the expanded IgM� B cells wereIgDlow/� (Figure S3D). Interestingly, CD27� B cells from 5 of 11
HCV�MC� subjects, but from none of the HCV�MC� subjectsor controls, exhibited markedly diminished CD21 (Figure S3E).HCV� subjects with clonal, as opposed to polyclonal,CDR3 had significantly increased percentages of CD21lowCD27�
B cells. We thus identified a subset of HCV� patients with clonalIg that had an expansion of IgM���IgDlow/�CD21lowCD27�
B cells. We gated on ��CD27� and IgM�CD27� B-cell sub-sets in selected patients (Table 4; Figure S4). In selected HCV�
MC� patients, the expanded IgM���CD27� subset was pre-dominantly IgDlow/�.
Several groups have reported increased intrahepatic andperipheral CD5� B cells among HCV� subjects, and they havesuggested that this reflects increased “natural” Ab production inHCV infection.50,51 Although CD5� B-1a cells seem to beresponsible for the production of natural Abs in mice,52 theassociation between CD5� B cells and natural Abs in humans isnot as clear, and evidence suggests that CD5 expression isinducible.53 Despite these drawbacks, we measured CD5�
B cells by flow cytometry (Figure S2C). Consistent with anothergroup’s finding54 and our earlier report,33 the frequency of CD5�
B cells was not significantly increased among HCV� subjects,nor did frequencies significantly differ between HCV�MC� andHCV�MC� patients (Table 3). However, 2 HCV� patients(1446 and 960) had very high levels of CD5� B cells. Takentogether, these data confirm that the majority of HCV� patientsdo not have expansions of CD5� B cells.
HCV�MC� subjects’ expanded IgM� ��CD21lowCD27� B cellsbear restricted, clonal Ig
We sorted single IgM���CD21lowCD27� B cells from subjectsLDU 077, LDU 095, 389, 773, 1403, 1308, and 1432. We wereunable to singly sort IgM���CD21lowCD27� B cells from otherHCV�MC� patients either because of a lack of cryopreserved
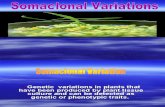
Figure 2. Phylogenetic analysis of VH (left) and V� (right) from subject 1432’s IgM��� CD27�CD21low B cells. Trees were constructed using neighbor-joining analysis ofTamura-Nei distances calculated from pairwise comparisons of Ig DNA sequences. Percentages of bootstrap support ( � 50%) from 1000 replicate samples (analyzed by theneighbor joining method) are indicated to the left of the support node. VH and V� from B cell A5 of patient 1403 serve as reference sequences.
Table 4. IgD� and CD5� subsets among selected subjects’ IgM�,CD27� B cells
SubjectIgM�, IgDlow/�
cells, %*� �, IgDlow/�
cells, %†CD5�, IgDlow/�
cells, %‡
HCV Ab� (LDU 095) 23.2 45.5 15.9
HCV� polyclonal (1419) 4.4 27.8 12.3
HCV� clonal (1308) 58.2 67.5 39.1
HCV� clonal (1403) 46.9 66.5 32.7
*Percentage of CD19�, CD20�, � �, CD27� cells.†Percentage of CD19�, CD20�, IgM�, CD27� cells.‡Percentage of CD19�, CD20�, IgM�, CD27� cells.
1348 CHARLES et al BLOOD, 1 FEBRUARY 2008 � VOLUME 111, NUMBER 3
For personal use only.on December 6, 2018. by guest www.bloodjournal.orgFrom

Table 5. IgH gene segment usages, nucleotide insertions, and CDR3 sequences in IgM���CD27� B cells
Subject no./status*/subset VH DH JH VD (P,N) DJ (P,N) IgH CDR3 sequence
LDU 077/HCV Ab� (CD21low)
Clones, no
1/8 3-74*01 3-16*02 4*02 0,13 1,2 CVRASWYYDRWGQG
1/8 1-46*01 3-16*02 4*02 1,6 1,3 CAREHGGGYDYWGQG
1/8 3-15*07 IR1*01R 2*01 0,30 1,0 CATGGRHSDYLLRGYFDLWGRG
1/8 3-30*03 6-06*01 6*02 0,0 0,11 CAKYSSTSNYYYGMDVWGQG
1/8 3-07*01 3-16*01 4*02 0,3 0,2 CASGLRYFDYWGQG
1/8 3-74*01 7-27*01 3*02 0,24 0,18 CARARGWAVETGSSEMIWAFDIWGQG
1/8 3-74*01 1-20*01 4*02 0,14 1,4 CVKDYNWNAGDYWGQG
1/8 4-04*02 4-17*01 4*02 0,3 0,0 CARGNGDYYFDYWGQG
LDU 095/HCV Ab� (CD21low)
Clones, no.
1/2 5-a 3-10*01 4*02 1,4 0,10 CARHGYGSGSYYDYWGQG
1/2 4-34*01 2-08*01R 6*02 0,34 0,0 CARVITRASPGTDGRTNMDVWGQG
389/HCV�MC� (CD21low)
Clones, no.
1/13 1-46*01 3-22*01 4*02 1,4 0,2 CARTSYYYDSSGYYPFDYWGQG
1/13 5-51*01 6-13*01 3*01 0,9 3,4 CARGQRAAAFDVWGQG
1/13 4-59*01 6-13*01 6*02 3,1 0,8 CARAPGIAAGNLPYYYYGMDVWGQG
1/13 3-21*01 3-22*01 4*02 1,5 0,1 CARYYYDSSGSYYFDYWGQG
1/13 4-34*01 3-22*01 2*01 1,10 1,8 CARGCGMHYDSSAGRYFDLWGRG
1/13 3-15*01 1-26*01 4*02 1,1 1,6 CTTAIVGAIHGDYWGQG
1/13 3-48*02 6-25*01 4*02 0,4 0,3 CARELGYSRPDYWGQG
1/13 3-49*03 4-23*01 4*02 0,6 0,2 CTSGRRWYLDYWGQG
1/13 3-21*01 4-17*01 6*02 1,8 0,5 CARDNQGTTGGYYYYGMDVWGQG
1/13 1-69*01 1-26*01 3*02 1,26 1,1 CAMAATREGSRKWELRAFDIWGQG
1/13 3-53*02 3-22*01 6*02 0,3 0,6 CARGITMNLHYYYGMDVWGQG
1/13 1-03*01 2-02*01 4*02 0,4 0,11 CARGYCSSTSCQYYSDYWGQG
1/13 3-23*01 1-07*01 6*02 1,24 0,15 CAKEGVPAAPRAYNWNSFFWSCMDVWGQG
773/HCV�MC� (CD21low)
Clones, no.
7/12† 1-69*01 6-13*01 4*02 0,0 0,8 CAREGIAAAVNPFDYWGQG
4/12† 1-69*06 2-15*01 4*02 1,4 1,14 CAREGRSGNVNPYDYWGQG
1/12 1-69*06 3-16*01 2*02 2,8 0,13 CAREGEAGGVGRNWAFDIWGQG
960/HCV�MC� (CD5�)
Clones, no.
1/7 1-69*01 3-22*01 4*02 1,5 1,16 CARDMGSSAYFFFYWGQG
1/7 3-66*01 IR*01R 4*02 0,0 1,25 CARGGPSKEPFDCWGQG
1/7 3-11*01 6-19*01 4*02 2,4 2,0 CARDQLWLAYWGQG
1/7 3-23*01 6-13*01 6*02 0,12 2,2 CAAPRLAAAGPYYYYYYGMDVWGQG
1/7 3-23*01 6-06*01 4*02 0,12 0,13 CAKEGGAGAARLGSFSYWGQG
1/7 3-21*01 1-01*01R 3*02 0,0 2,10 CARSFSGAGAFDIWGQG
1/7 3-23*01 3-22*01 4*02 3,6 0,0 CAKDRGRYDSFDYWGQG
1073/HCV�MC� (All)
Clones, no.
1/10 3-74*01 IR1*01R 4*02 3,1 2,7 CTRGLWDHDYWGQG
1/10 3-72*01 6-19*01 6*03 1,15 0,23 CAIGPGFNSGRYYYYYMAVWGKG
1/10 3-74*01 3-09*01 4*02 0,29 0,0 CARDRYTFGTTPLDWGPG
1/10 3-30*04 5-12*01 3*02 1,8 1,6 CARDRAGVATIIGADAFDIWGQG
1/10 4-39*02 6-19*01 4*02 2,14 1,0 CTRRARGSGWYYWGQG
1/10 3-23*01 4-17*01 6*02 0,9 0,10 CAKGPSSVTRIKSYYYYGMDVWGQG
1/10 4-39*06 5-12*01 5*02 2,4 0,30 CARSEVATVVFVVLASQLFDWGQG
1/10 5-51*03 6-13*01 5*02 0,10 0,6 CARLGRSAAGTDLFDPWGQG
1/10 7-04-1*02 3-16*01 6*03 0,3 0,9 CARRDYEGHLDVWGKG
1/10 5-51*01 5-05*01 1*01 0,23 0,8 CARGFGRGLGASYWGSEYFQHWGQG
1308/HCV�MC� (CD21low)
Clones, no.
15/15† 3-7*01 1-26*02 3*02 0,0 0,12 CARDGDLGSGSRSMGAFDIWGQG
1403/HCV�MC� (CD21low)
Clones, no.
9/18† 1-69*01 3-22*01R 4*02 1,5 0,19 CARAYGNNPTEVYWVYWGQG
5/18† 1-18*01 2-15*01 6*02 0,9 0,34 CARDGAVCSGSSCRGNYYYYGLDVWGQG
VD (P,N) and DJ (P,N) indicate the number of palindromic (P) and nontemplated (N) nucleotides inserted at the VD and DJ joins, respectively. The bold type in the IgHCDR3 sequence indicates aa residues between position 106 and the conserved tryptophan in all JH segments.
*IgM�� � CD27� B-cell subset.†in column 1 indicates clonal populations.
CLONAL EXPANSION OF IgM�CD27� B CELLS IN HCV MC 1349BLOOD, 1 FEBRUARY 2008 � VOLUME 111, NUMBER 3
For personal use only.on December 6, 2018. by guest www.bloodjournal.orgFrom

PBMCs (subjects 734, 880, and 92200), or because of the lowfrequency of these cell subsets. We were able to singly sortIgM���CD27� B cells from subject 1073. We cloned the entireexpressed Ig VH region (and for selected subjects, the entire IgV� region) from individual cells using a 2-stage, unbiased IgRT-PCR strategy.40 Results for VH and V� are summarized inTables 5, 6. In contrast to HCVAb� controls, IgM���CD21lowCD27�
B cells from the HCV�MC� patients exhibited marked VH, JH, and V�
gene segment usage restriction. Eleven of 12 IgM���CD21lowCD27�
B cells isolated from patient 773, 22 of 22 from subject 1432, and 10 of18 from patient 1403 used the RF-encoding gene segments VH1-69/JH4.There was a similar pattern of V�3-20 restriction in these subjects. AllIgM���CD21lowCD27� B cells isolated from patient 1308 used VH3-7/JH3 and V�3-15/J�1.
Earlier studies have shown that hepatic lymphoid aggregatesfrom HCV�MC� subjects consist predominantly of CD5�
B cells.55 As mentioned in “B cells from certain HCV�MC�
subjects are biased toward a restricted IgM���IgDlow/�CD27�
phenotype,” increased intrahepatic and peripheral CD5� B cellshave been reported among HCV� subjects,50,51 suggesting that
the B cells arising in the liver and stimulated by HCV antigensmay be CD5�. We therefore decided to clone Ig fromIgM���CD27�CD5� and IgM���CD27�CD5� B cells isolatedfrom subjects 1446 and 960 (who both had increased percent-ages of CD5� B cells) and from subject 1403 (to determinewhether unmutated clonal Ig was produced by CD5� cells). Wecould not recover any IgM���CD27�CD5� B cells from subject960. Of IgM���CD27�CD5� B cells, 1 of 7 clones from subject960, 2 of 6 from subject 1403, and 3 of 13 from the HCV�MC�
subject 1446 demonstrated VH1-69/JH4 gene segment usage,whereas no VH1-69/JH4 usage was seen among 10 clones fromsubject 1446’s IgM���CD27�CD5� B cells, suggesting thatthis gene segment restriction is not seen in CD5� cells. Of the2 VH1-69�/JH4� clones from 1403, one was unmutated and theother had only 2 mutations, suggesting that the unmutated clonalpopulation may arise from CD5� B cells.
Patients 1308 and 1432 had monoclonal IgM���CD21low
CD27� B cells, as indicated by the presence of identical CDR3 andpalindromic (P) and nontemplated (N) nucleotides at the VHDH,DHJH, and V�J� joins. We identified 2 clonal populations in subject
Table 5. IgH gene segment usages, nucleotide insertions, and CDR3 sequences in IgM���CD27� B cells (Continued)
Subject no./status*/subset VH DH JH VD (P,N) DJ (P,N) IgH CDR3 sequence
1/18 1-69*01 4-17*01 4*02 1,2 2,9 CAREGYGDYGRPYDYWGQG
1/18 3-20*01 1-26*01 6*02 2,1 0,0 CARAGGSYYYYYGMDVWGQG
1/18 3-21*01 3-22*01 4*02 3,11 1,6 CTRDGPYYDSSGFEYWGQG
1/18 3-23*01 2-15*01 6*02 1,13 1,8 CAKTLRSNVVVVATTHYYGMDVWGQG
1403/HCV�MC� (CD5�)
Clones, no.
2/6† 1-69*01 3-22*01R 4*02 1,5 0,19 CARAYGNNPTEVYWVYWGQG
1/6 3-23*01 3-10*01 4*02 0,12 0,4 CAKGGPRFTMVRGVKIYFDYWGQG
1/6 3-07*01 6-13*01 6*03 3,7 0,1 CARAQSFSWSMDVWGQG
1/6 1-18*01 2-15*01 6*02 0,9 0,34 CARDGAVCSGSSCRGNYYYYGLDVWGQG
1/6 3-23*01 3-10*01 2*01 0,3 1,23 CAGGSGSYSLLGPHWHIDLWGQG
1432/HCV�MC� (CD21low)
Clones, no.
22/22† 1-69*01 3-03*01 4*02 0,16 0,2 CARDYGERESGYYFYWGQG
1446/HCV�MC� (CD5�)
Clones, no.
1/10 1-03*01 2-21*02 4*02 2,7 2,1 CARGVIYCGGDCYSGDYWGQG
1/10 3-23*01 2-15*01 6*02 0,2 0,11 CAKGGYAEGAYYYYGMDVWGQG
1/10 3-15*01 1-07*01 4*02 4,5 2,2 CTTDLFLLELRCDYWGQG
1/10 3-30*03 3-22*01 4*02 0,30 0,1 CAKGGDTAMVLSNYYDSSGVDYWGQG
1/10 5-51*01 3-10*01 4*02 0,10 0,21 CARRKSDYYGSGRAGFSDYWGQG
1/10 4-34*01 3-10*01 4*02 1,5 0,5 CARAPSITMVRGVINEFDYWGQG
1/10 3-21*01 4-17*01 4*02 0,5 0,3 CARDRPTVTTVFDYWGQG
1/10 3-15*01 3-10*01 6*03 2,2 0,0 CTTDRYYGSGSYYYGMDVWGQG
1/10 1-03*01 6-25*01 6*03 3,1 0,2 CARASGHYYYYMDVWGKG
1/10 3-15*01 6-19*01 4*02 0,7 0,13 CTTVGVIAVAGGFRGDYWGQG
1446/HCV�MC� (CD5�)
Clones, no.
3/13† 1-69*01 4-17*01 4*02 1,7 2,5 CAREGRATVTNPFDYWGQG
3/13† 3-11*03 IR1*01 4*02 0,14 2,0 CARGARLEGPVDYWGQG
2/13 3-15*01 IR1*01 5*02 0,2 0,14 CATGRDFYRFDPWGQG
1/13 1-18*01 4-17*01 4*02 0,14 1,6 CATRGRDTGDYEGDWGQG
1/13 3-23*01 4-17*01 4*02 1,11 0,13 CAKGRTSITVQYDSWGQG
1/13 3-15*01 3-22*01 4*02 2,5 1,7 CTTDPGITMIVVVPQGFDYWGQG
1/13 3-48*02 6-19*01 4*02 0,10 1,16 CAREARRSSGWYFHEIDYWGQG
1/13 4-34*01 2-15*01 4*02 1,7 1,29 CARTPRYCSGATCNKIMGLDHWGQG
VD (P,N) and DJ (P,N) indicate the number of palindromic (P) and nontemplated (N) nucleotides inserted at the VD and DJ joins, respectively. The bold type in the IgHCDR3 sequence indicates aa residues between position 106 and the conserved tryptophan in all JH segments.
*IgM�� � CD27� B-cell subset.†in column 1 indicates clonal populations.
1350 CHARLES et al BLOOD, 1 FEBRUARY 2008 � VOLUME 111, NUMBER 3
For personal use only.on December 6, 2018. by guest www.bloodjournal.orgFrom

773. The largest, represented by 7 of 12 B cells, contained a CDR3exactly identical to that previously reported from a patient withsalivary gland mucosa–associated lymphoid tissue lymphoma.56
That identical CDR3 regions containing N nucleotides have beenidentified in 2 different patients strongly suggests a commonantigenic stimulus in the 2 patients, as it is extremely unlikely thatthese identical regions could arise by chance. The VH1-69/JH4clonal population in subject 1446’s IgM���CD27�CD5� B cellshad a CDR3 that differed by one amino acid from a CDR3previously recovered by another group from an unrelatedHCV�MC� subject’s expanded B cells.57 We identified 2 clonalpopulations among subject 1403’s IgM���CD21lowCD27� B cells.As mentioned, the predominant clonal VH1-69/JH4 population wasalso seen in 2 of 6 of 1403’s IgM���CD27�CD5� B cells. ClonalIg was not seen in subject 389’s IgM���CD21lowCD27� B cellsnor in subject 1073’s IgM���CD27� B cells. Because clonal Igwas seen in these subjects’ unfractionated PBMCs, this suggeststhat the clonally expanded B cells in these subjects were notCD21lowCD27�.
The expanded IgM���CD21lowCD27� B cells in certainHCV�MC� subjects contain somatically hypermutated Igs
The majority of expanded IgM���CD21lowCD27� B cellsexhibited low to moderate levels of somatic hypermutation(SHM; Table 7). An exception was subject 1403 whose clonalVH1-69/JH4 cells were unmutated. Within each clonalIgM���CD21lowCD27� B-cell population, the mutational fre-quency varied significantly among individual cells. Except forsubject 389, each HCV�MC� subject from whom Igswere cloned had several Igs with significantly scarce R muta-tions in their FR regions, (pR(FR) 0.05), indicative ofselection based on structural constraint for antigen-Ig binding.However, only 3 of these Igs had a significant excess ofR mutations in CDR, (pR(CDR) 0.05). Despite VH SHM,CDR3 sequences were strikingly conserved among clonalpopulations, suggestive of a positive selection. Most V� wereless hypermutated than their corresponding VH, reflective of thelower mutation rate of Ig� seen in the general population.49 Incontrast to VH, more V� had an excess of R(CDR) than they hada scarcity of R(FR).
Igs from HCV�MC� subjects demonstrate features of clonalevolution
We constructed phylogenetic trees for VH and V� from subject1432’s IgM���CD21lowCD27� B cells (Figure 2). When com-bined with the Ig mutation rates from Table 7, these treesdemonstrate that for both VH and V�, mutations are sharedamong different B cells. A pattern of clonal evolution isapparent, as the more hypermutated clones also contain muta-tions present in the less hypermutated clones. Interestingly,6 B cells (D2, D4, D6, D9, E3, and F6) that had highly evolvedIgH also had significant scarce R(FR), further indication that astructural constraint in FR provides selective pressure for thesecells. The VH and V� phylogenies correlate well with oneanother. Cells with relatively large VH mutational frequencieshave correspondingly large V� mutational frequencies. This fact,combined with similar patterns of shared VH and V� mutationsamong these cells, provides strong evidence that the observedmutations are not PCR artifacts. Similar results were obtainedon phylogenetic analysis of Ig clones from subjects 773, 1308,and 1403 (data not shown). Taken together, these data suggestthat the expanded IgM���CD21lowCD27� B cells in certainHCV�MC� subjects undergo successive rounds of SHM.However, the relatively low mutation rates and theoccasional presence of unmutated B-cell clonal expansionssuggest that affinity maturation is not an absolute requirementfor these cells.
Discussion
A major finding of our study is the identification of clonallyexpanded IgM���IgDlow/�CD21lowCD27� B cells expressinghypermutated RF-like Ig in a subgroup of HCV�MC� patients.In addition, we describe for the first time cloning of VH and V�
from single B cells obtained from HCV�MC� patients. Ourcloning strategy was unbiased in its amplification of Ig genesegments; the gene segment usage we observed in our healthyvolunteers corresponds to that previously reported in the general
Table 6. Ig� gene segment usages, nucleotides insertions, andCDR3 sequences in IgM���CD21lowCD27� B cells
Subject no./status V� J� VJ (P,N) Ig� CDR3 sequence
LDU 077/HCV Ab�
Clones, no.
1/8 4-1*01 2*01 0,20 CHQYYAFPHTFGO
1/8 2-28*01 4*01 1,2 CMQALQTPLTFGG
1/8 1-39*01 2*01 1,10 CQQSYSTPSHTFGQ
1/8 1-33*01 2*01 0,0 CQQYDNLPPYTFGQ
1/8 3-20*01 1*01 0,15 CQHYRSSLWTFGQ
1/8 2-29*01 1*01 1,17 CMQGLHLPPTFGQ
1/8 1-8*01 1*01 2,0 CQQYYSYPRTFGQ
LDU 095/HCV Ab�
Clones, no.
1/2 4-1*01 4*01 0,0 HQYYRTPLTFGG
1/2 1-39*01 2*01 0,0 CQQSYRTPHTFGQ
773/HCV�MC�
Clones, no.
7/12* 3-20*01 1*01 0,1 CQQYGSSPQTFGQ
4/12* 3-20*01 1*01 0,1 CQQYGSSPQTFGQ
1/12 3-20*01 1*01 1,1 CQQYGSSRTFGQ
1403/HCV�MC�
Clones, no.
9/18* 3-20*01 4*01 0,0 CQQYGSSPTFGG
5/18* 3-20*01 2*01 1,0 CQQYGSSRYTFGQ
1/18 3-20*01 2*01 1,0 CQQYGSSPYTFGQ
1/18 3-20*01 4*01 2,0 CQQYGSSSLTFGG
1/18 1-27*01 4*01 0,0 CQKYNSAPLTFGG
1/18 1-6*01 2*01 0,0 CLQDYNYPYTFGQ
1308/HCV�MC�
Clones, no.: 15/15* 3-15*01 1*01 0,0 CQQYNNWPPWTFGQ
1432/HCV�MC�
Clones, no.: 22/22* 3-20*01 2*02 1,1 CQQYGSSPRTFGQ
VJ (P,N) indicates the number of palindromic (P) and nontemplated (N)nucleotides inserted at the VJ join. The bold type in the Ig� CDR3 sequence indicatesaa residues between position 106 and the conserved phenylalanine in all J�
segments.* in column 1 indicates clonal populations.
CLONAL EXPANSION OF IgM�CD27� B CELLS IN HCV MC 1351BLOOD, 1 FEBRUARY 2008 � VOLUME 111, NUMBER 3
For personal use only.on December 6, 2018. by guest www.bloodjournal.orgFrom

population.58 It is also unlikely that we overestimated muta-tional frequencies because of potential Taq polymerase errors.We performed duplicate VH PCR reactions on reverse-transcribed cDNA from 10 different B cells, and we noted only2 discordant nucleotides (2 stage VH PCR error rate: 1 of 1860nucleotides). Moreover, we routinely did not detect mutations inCD27� cells, and mutational frequencies among subjects’ VH
and V� were highly correlated.The finding that a subset of HCV�MC� patients have
clonally expanded, hypermutated, Ig gene segment–restricted,memory-like B cells suggests that specific antigenic stimulationis responsible for the B-cell proliferation in HCV MC. Ourfindings contrast with an earlier claim that polyclonal activationof naive B cells occurs during chronic HCV infection.27 Of note,we did not detect any increased CD69 or CD25 expressionamong any subjects’ B cells. However, this latter result is notsurprising, given the role of CD69 in retaining activated B cellsin lymph nodes.59 It is possible that any recently activatedB cells may leave the blood and not be detected. Important, notall HCV�MC� patients have noticeably expanded B-cell subsets.The finding of clonal VH1-69/JH4 B cells in subject1446 (HCV�MC� and without a detectable clonal CDR3 band)suggests that these clonal expansions may be occurring subclini-cally in some patients. That we did not recover clonal Ig in theIgM���CD21lowCD27� B cells of patient 389 and in theIgM���CD27� B cells of patient 1073 (both of whomwere HCV�MC� with clonal CDR3, yet without detect-able B-cell expansion) suggests that either clonal Ig is present atlow frequencies or is present in different B-cell subsets inthese patients. Our results, which are consistent with2 prior studies, lend support to the hypothesis that chronic,specific antigenic stimulation of IgM� B cells predisposestoward neoplastic transformation. In one study, regression ofWA RF-bearing IgM���IgD�CD5� B cells occurred concomi-tantly with the decline of HCV RNA during interferon-�treatment.57 The CDR3 of the cells in the cited study57 is highlyhomologous to that of subject 1446’s clonal IgM���CD27�CD5�
B cells. In another study, splenic marginal zone lymphomaregressed in patients whose HCV was successfully treated withinterferon �-2b.60
IgM�CD27� cells are important in defending against bacte-rial pathogens in a T cell–independent manner, and it has beenproposed that such cells are the circulating form of splenicmarginal zone (MZ) B cells.61,62 MZ B cells are thought to bedistinct from GC or post-GC B cells,63 and SHM in these cellsdoes not require accessory molecules such as CD40L or CD40.64
In healthy humans, IgM� memory B cells have been demon-strated to comprise approximately 10% to 25% of peripheralB cells64,65 and to have lower SHM rates than class-switchedmemory B cells. We have found that IgM�CD27� cells com-prise up to 75% of circulating B cells in a subset of HCV�MC�
patients and that these cells have low levels of SHM. Moreover,these IgM� memory B cells are IgDlow/�, which distinguishesthem from previously reported hypermutated IgM�IgD�CD27�
B cells in healthy adults.49 Our findings are consistent with thefact that HCV is associated with both splenic66,67 and extras-plenic, nodal MZ lymphomas, the latter of which have beenfound to be made up of B cells frequently harboring mutatedVH1-69 gene segments.68
Our finding that in certain HCV�MC� subjects, IgM� memory-like B cells have reduced expression of CD21 contrasts with thecharacterization of MZ cells as being CD21high.62 Interestingly,
reduced CD21 expression was reported on B cells from patientswith systemic lupus erythematosis69 and HIV.70 We have previouslyobserved reduced CD21 expression on HCV� patients’ B cells.33
Down-regulation of CD21 may serve to dampen B-cell responsive-ness to BCR-mediated activation and proliferation. However, it isalso possible that reduced CD21 is a normal feature of B cells thathave been stimulated by antigen,71 or it may be emblematic ofapoptotic cells.72
Our analysis of CD5�IgM���CD27� and CD5�IgM���CD27�
B cells, although conducted on only 3 subjects and 1 subject,respectively, suggests that the clonal, VH1-69/JH4-restricted B cellsseen in some HCV�MC� patients are CD5�. This is consistent withprior reports of CD5� MZ-like B-cell lymphoproliferation in someHCV�MC� patients,57,60 and it suggests that CD5 expression is nota universal feature of the expanded B-cell subsets seen in HCVMC. We are currently in the process of sorting CD5�IgM���CD27�
and CD5�IgM���CD27� B cells from additional, newly identifiedHCV�MC� patients with clonal IgM���IgDlow/�CD21lowCD27�
B-cell expansions.An interesting finding is that, whereas 3 HCV�MC� subjects
had hypermutated clonal B cells, one patient’s clonal B cells wereof germ line sequence, despite being CD27�. Our studies areconsistent with the findings of Ivanovski et al,19 who foundrestricted, hypemutated VH and VL genes in PBMCs isolated fromHCV patients with immunocytomas. It is unclear if SHM correlateswith autoreactivity in HCV MC. We are currently defining theautoreactive profiles of Ig cloned from our HCV�MC� subjects.Whether autoreactivity is inversely correlated with the presence ofSHM is of extreme interest.
It is not known how these Ig-restricted memory-like B cellsare stimulated to expand in some HCV�MC� patients. Onepossibility is that the Ig on these B cells reacts with an HCVantigen and/or cross-reacts with a self-molecule, such as IgG,which may be bound to HCV. The finding that the clonal B-cellpopulation of one of our HCV�MC� patients expresses a CDR3that is exactly identical to the CDR3 from a patient with salivarygland lymphoma is intriguing in light of a report that a particularantigen selects Igs bearing identical CDR3 in different per-sons.73 Persistent inflammation is a common feature of HCVinfection, Sjogren syndrome, and H pylori infection. All of thesesyndromes are associated with B-NHL. In these diseases,antigen-containing immune complexes may bind to low-affinityautoreactive BCR. Concomitant stimulation of toll-like recep-tors (TLR), coupled with (or in lieu of) cognate T-cell help, maylead to B-cell activation and proliferation. It has been shown invitro that IgG-bound Borrelia burgdorferi is capable of breakingRF-expressing B cells’ state of immunologic tolerance bybinding to both BCR and TLR.74 Moreover, it has beenshown that chromatin-IgG complexes can lead to activation ofRF� B cells by engagement of IgM and TLR9.75 We arecurrently testing the hypothesis that immune complexedHCV induces expansion of RF� B cells by dual engagement ofBCR and TLR7.
In conclusion, we have characterized in detail a subset ofHCV�MC� patients with gene segment-restricted, clonallyexpanded IgM���IgDlow/�CD21lowCD27� B cells. We empha-size that our studies are of peripheral B cells. It is unclear howrepresentative these cells are of the B cells in the hepaticmicroenvironment. Importantly, clonal intrahepatic RF-produc-ing B cells have been shown in HCV�MC� patients.17 Theidentification of such highly restricted, potentially autoreactive,Igs in a subset of HCV�MC� patients gives us hope that
1352 CHARLES et al BLOOD, 1 FEBRUARY 2008 � VOLUME 111, NUMBER 3
For personal use only.on December 6, 2018. by guest www.bloodjournal.orgFrom

Table 7. Analysis of mutations in IgM���CD21lowCD27� B cells
Subject no., B cell
Heavy chain Light chain
VH mutations(%) aa �
R/S(FR)
R/S(CDR)
p(R)FR
p(R)CDR
V� mutations(%) aa �
R/S(FR)
R/S(CDR)
p(R)FR
p(R)CDR
LDU 077
F1 23 (8.32) 17 12/5 5/1 0.163 0.131 7 (2.81) 4 1/0 3/2 0.019 0.025
G1 0 (0.00) 0 0/0 0/0 — — 0 (0.00) 0 0/0 0/0 — —
G4 23 (8.32) 11 3/8 8/4 0.000 0.006 7 (2.85) 3 1/1 3/2 0.008 0.041
G5 7 (2.59) 4 4/2 0/1 0.388 0.817 6 (2.60) 4 3/0 2/1 0.292 0.131
G6 1 (0.37) 0 0/1 0/0 0.180 0.567 0 (0.00) 0 0/0 0/0 — —
H3 23 (8.32) 16 8/5 9/1 0.004 0.001 9 (3.85) 8 3/0 6/0 0.052 0.000
H6 16 (5.93) 8 4/3 7/2 0.002 0.002 12 (4.8) 9 8/3 1/0 0.820 0.700
H7 0 (0) 0 0/0 0/0 — — 0 (0.00) 0 0/0 0/0 — —
LDU 095
B3 5 (1.94) 4 3/1 1/0 0.450 0.324 2 (0.80) 2 1/0 1/0 — —
C4 8 (3.14) 4 4/3 0/1 0.246 0.841 4 (1.73) 3 0/1 3/0 0.338 0.083
LDU 389
A1 1 (0.37) 1 1/0 0/0 0.686 0.569 — — — — — —
A4 0 (0.00) 0 0/0 0/0 — — — — — — — —
B3 3 (1.12) 1 1/2 0/0 0.182 0.679 — — — — — —
B7 0 (0.00) 0 0/0 0/0 — — — — — — — —
C10 0 (0.00) 0 0/0 0/0 — — — — — — — —
C12 0 (0.00) 0 0/0 0/0 — — — — — — — —
D5 0 (0.00) 0 0/0 0/0 — — — — — — — —
D9 1 (0.36) 1 1/0 0/0 0.686 0.569 — — — — — —
E2 0 (0.00) 0 0/0 0/0 — — — — — — — —
E8 6 (2.22) 4 3/2 1/0 0.271 0.392 — — — — — —
2F1 3 (1.12) 2 2/1 0/0 0.533 0.679 — — — — — —
F2 6 (2.27) 5 2/1 3/0 0.086 0.021 — — — — — —
G9 2 (0.74) 0 0/0 0/2 0.069 0.628 — — — — — —
LDU 773
D7* 6 (2.22) 3 1/3 2/0 0.017 0.110 5 (2.14) 3 2/1 1/1 0.132 0.206
D10* 6 (2.22) 3 1/2 2/1 0.017 0.110 2 (0.85) 2 1/0 1/0 0.338 0.083
E3* 7 (2.59) 1 1/5 0/1 0.007 0.817 5 (2.14) 4 2/1 2/0 0.132 0.032
E5* 5 (1.85) 4 2/1 2/0 0.174 0.077 6 (2.56) 5 2/1 3/0 0.062 0.005
F5* 8 (2.96) 1 1/4 0/3 0.003 0.841 3 (1.28) 3 1/0 2/0 0.152 0.010
F10* 8 (2.96) 5 3/3 2/0 0.088 0.185 6 (2.56) 3 2/2 1/1 0.062 0.245
G1* 4 (1.48) 3 2/1 1/0 0.319 0.263 1 (0.43) 1 1/0 0/0 0.669 0.542
C10* 2 (0.74) 2 1/0 1/0 0.377 0.134 4 (1.71) 3 2/0 1/1 0.265 0.166
E7* 18 (6.67%) 6 5/10 1/2 0.002 0.819 6 (2.56) 3 1/2 2/1 0.010 0.046
F8* 3 (1.11) 2 2/1 0/0 0.538 0.675 4 (1.71) 3 2/1 1/0 0.265 0.166
G7* 14 (5.19) 9 7/4 2/1 0.179 0.431 4 (1.71) 2 2/2 0/0 0.265 0.647
C11 9 (3.33) 6 4/2 2/1 0.148 0.226 6 (2.56) 5 5/1 0/0 0.787 0.703
LDU 1403
A5* 0 (0.00) 0 0/0 0/0 — — 3 (1.28) 2 2/1 0/0 0.488 0.615
G3* 0 (0.00) 0 0/0 0/0 — — 3 (1.28) 2 2/1 0/0 0.488 0.615
C6* 0 (0.00) 0 0/0 0/0 — — 3 (1.28) 2 2/1 0/0 0.488 0.615
C7* 0 (0.00) 0 0/0 0/0 — — 3 (1.28) 2 2/1 0/0 0.488 0.615
D3* 0 (0.00) 0 0/0 0/0 — — 3 (1.28) 2 2/1 0/0 0.488 0.615
D9* 0 (0.00) 0 0/0 0/0 — — 5 (2.14) 4 4/1 0/0 0.711 0.676
D11* 0 (0.00) 0 0/0 0/0 — — 3 (1.28) 2 2/1 0/0 0.488 0.615
H9* 0 (0.00) 0 0/0 0/0 — — 4 (1.71) 3 3/1 0/0 0.612 0.647
B2* 0 (0.00) 0 0/0 0/0 — — 3 (1.28) 2 2/1 0/0 0.488 0.615
E1* 9 (3.33) 3 1/4 2/2 0.001 0.226 2 (0.85) 1 0/0 1/1 0.057 0.083
E3* 9 (3.33) 3 1/4 2/2 0.001 0.226 3 (1.28) 2 1/0 1/1 0.152 0.125
H1* 11 (4.07) 4 2/5 2/2 0.002 0.308 4 (1.71) 3 2/0 1/1 0.265 0.166
H4* 9 (3.33) 3 1/4 2/2 0.001 0.226 3 (1.28) 1 0/1 1/1 0.027 0.207
B1* 15 (5.56) 6 3/7 3/2 0.001 0.227 1 (0.43) 0 0/1 0/0 0.169 0.541
F2 14 (5.19) 12 8/2 4/0 0.344 0.068 5 (2.14) 3 2/2 1/0 0.132 0.206
E9 8 (2.96) 6 3/1 3/1 0.088 0.047 3 (1.28) 1 0/2 1/0 0.019 0.125
G6 17 (6.30) 9 7/8 2/0 0.042 0.543 5 (2.03) 5 4/0 1/0 0.711 0.206
H12 12 (4.44% 8 2/2 6/2 0.001 0.001 5 (2.03) 4 5/0 0/0 0.936 0.676
V mutations indicate number of mutations in V; aa , number of aa replacements in V; R/S (FR), ratio of replacement mutations to synonymous mutations in the V FR; R/S(CDR), ratio of replacement mutations to synonymous mutations in the V CDR1 and CDR2; p(R)FR, probability of significant scarcity of R mutations in FR; p(R)CDR, probabilityof significant excess of R mutations in CDR1 and CDR2.
— indicates that the value was not computed.*indicates clonal populations.
CLONAL EXPANSION OF IgM�CD27� B CELLS IN HCV MC 1353BLOOD, 1 FEBRUARY 2008 � VOLUME 111, NUMBER 3
For personal use only.on December 6, 2018. by guest www.bloodjournal.orgFrom

elucidation of the precise antigenic stimulus responsible for MCformation will reveal the mechanism of HCV-induced B-cellproliferative disorders.
Acknowledgments
We are grateful for the generosity of the patient volunteers. We thank theRockefeller University Hospital Department of Nursing and PatientCare Services, Gertrudis Soto and Queenie Brown for assistance inpatient enrollment and sample acquisition. Svetlana Mazel, manager ofRockefeller’s Flow Cytometry Research Center, and Peter Lopez,manager of Aaron Diamond AIDS Research Center’s Core Facilities,provided expert assistance with flow cytometry. We acknowledgeRaymond Peterson for database management and Knut Wittkowski forstatistical advice. We also thank Michel Nussenzweig and SergeyYurasov for helpful discussions.
This study was supported in part by the National Institutes ofHealth/National Institute of Allergy and Infectious Diseases grantR01AI60561 (L.B.D.), the Irma T. Hirschl/Monique Weill-Caulier Trust(L.B.D.), General Clinical Research Center grant M01-RR00102 (toRockefeller University Hospital), and Center for Translational ScienceAward grant 1UL1 RR024143-01 (to Rockefeller University Hospital)from the NIH National Center for Research Resources. E.D.C. issupported in part by the Clinical Scholar Program of RockefellerUniversity Hospital.
AuthorshipContribution: E.D.C., L.B.D., R.M.G., and S.M. devised andperformed experiments; E.D.C., G.V.L.-B., A.H.T., and I.M.J.provided patient referrals; E.D.C., L.B.D., C.M.R., S.M., G.V.L.-B., A.H.T., and I.M.J. interpreted results; and E.D.C. and L.B.D.designed the research and wrote the paper.
Table 7. Analysis of mutations in IgM���CD21lowCD27� B cells (Continued)
Subject no. B cell
Heavy chain Light chain
VH mutations(%) aa �
R/S(FR)
R/S(CDR)
p(R)FR
p(R)CDR
V� mutations(%) aa �
R/S(FR)
R/S(CDR)
p(R)FR
p(R)CDR
LDU 1308
B12* 9 (3.33) 4 1/3 3/2 0.001 0.065 2 (0.87) 2 2/0 0/0 0.781 0.580
C3* 3 (1.11) 2 2/0 0/1 0.538 0.675 5 (2.16) 3 2/1 1/1 0.132 0.206
C4* 8 (2.96) 4 2/2 2/2 0.021 0.185 3 (1.30) 1 0/2 1/0 0.019 0.125
C9* 5 (1.85) 1 1/4 0/0 0.039 0.756 1 (0.43) 1 0/0 1/0 0.169 0.042
C11* 4 (1.48) 2 1/2 1/0 0.087 0.263 2 (0.87) 2 0/0 2/0 0.057 0.003
D1* 0 (0.00) 0 0/0 0/0 — — 1 (0.43) 1 0/0 1/0 0.169 0.042
D4A* 8 (2.96) 5 4/2 1/1 0.246 0.487 5 (2.16) 2 1/3 1/0 0.026 0.206
D4B* 10 (3.70) 6 3/4 3/0 0.024 0.087 7 (3.03) 3 3/3 1/0 0.114 0.283
D5* 8 (2.96) 4 3/2 1/2 0.088 0.487 0 (0.00) 0 0/0 0/0 — —
D11* 6 (2.22) 5 3/1 2/0 0.278 0.110 6 (2.60) 4 3/2 1/0 0.217 0.245
E3* 6 (2.22) 5 4/0 1/1 0.568 0.381 6 (2.60) 4 3/1 2/0 0.217 0.046
H2* 6 (2.22) 4 4/1 0/1 0.568 0.789 4 (1.73) 3 3/1 0/0 0.612 0.647
H7* 5 (1.85) 2 2/2 1/0 0.174 0.324 2 (0.87) 1 0/1 1/0 0.057 0.083
I6* 2 (0.74) 2 1/0 1/0 0.377 0.134 2 (0.87) 1 0/1 1/0 0.057 0.083
LDU 1432
B2* 3 (1.11) 2 2/1 0/0 0.538 0.675 5 (2.14) 2 2/1 0/2 0.132 0.676
B4* 10 (3.47) 6 4/3 2/1 0.085 0.267 3 (1.28) 1 1/1 0/1 0.152 0.615
B5* 3 (1.04) 1 1/2 0/0 0.186 0.675 3 (1.28) 1 1/1 0/1 0.152 0.615
C2* 7 (2.59) 5 4/2 1/0 0.388 0.436 4 (1.71) 4 3/0 1/0 0.012 0.166
C3* 7 (2.59) 4 3/1 1/2 0.161 0.436 5 (2.14) 2 2/2 0/1 0.132 0.676
C4* 5 (1.85) 4 3/1 1/0 0.450 0.323 5 (2.14) 2 1/1 1/2 0.026 0.206
C8* 2 (0.74) 2 1/0 1/0 0.377 0.134 4 (1.71) 3 3/0 0/1 0.612 0.647
D1* 3 (1.11) 2 2/0 0/1 0.538 0.675 2 (0.85) 1 1/0 0/1 0.338 0.580
D2* 12 (4.44) 6 3/4 3/2 0.006 0.137 6 (2.56) 2 2/3 0/1 0.062 0.703
D4* 8 (2.96) 2 2/4 0/2 0.021 0.041 5 (2.14) 2 2/2 0/1 0.132 0.676
D5* 3 (1.11) 2 2/1 0/0 0.538 0.675 3 (1.28) 1 1/1 0/1 0.152 0.615
D6* 11 (4.07) 4 4/3 1/3 0.047 0.619 5 (2.14) 2 2/2 0/1 0.132 0.676
D8* 9 (3.33) 4 4/2 0/3 0.150 0.863 6 (2.56) 3 2/2 1/1 0.132 0.676
D9* 9 (3.33) 4 3/3 1/2 0.047 0.534 7 (2.99) 3 4/2 0/1 0.310 0.728
D11* 8 (2.96) 5 4/2 0/1 0.388 0.817 2 (0.85) 1 0/0 1/1 0.057 0.083
E2* 5 (1.85) 3 2/2 1/0 0.174 0.324 3 (1.28) 2 1/0 1/1 0.152 0.125
E3* 9 (3.33) 3 2/4 1/2 0.010 0.534 6 (2.56) 3 2/2 1/1 0.062 0.245
E5* 5 (1.85) 2 2/3 0/0 0.174 0.756 3 (1.28) 2 2/0 0/1 0.488 0.615
E11* 1 (0.37) 1 1/0 0/0 0.688 0.567 2 (0.85) 1 1/0 0/1 0.338 0.580
F1* 5 (1.85) 2 1/3 1/0 0.039 0.324 4 (1.71) 1 1/1 0/2 0.064 0.647
F3* 7 (2.59) 5 5/0 1/1 0.669 0.436 4 (1.71) 1 1/1 0/2 0.064 0.647
F6* 8 (2.96) 2 2/4 0/2 0.021 0.841 7 (2.99) 4 3/2 1/1 0.114 0.283
V mutations indicate number of mutations in V; aa , number of aa replacements in V; R/S (FR), ratio of replacement mutations to synonymous mutations in the V FR; R/S(CDR), ratio of replacement mutations to synonymous mutations in the V CDR1 and CDR2; p(R)FR, probability of significant scarcity of R mutations in FR; p(R)CDR, probabilityof significant excess of R mutations in CDR1 and CDR2.
— indicates that the value was not computed.*indicates clonal populations.
1354 CHARLES et al BLOOD, 1 FEBRUARY 2008 � VOLUME 111, NUMBER 3
For personal use only.on December 6, 2018. by guest www.bloodjournal.orgFrom

Conflict-of-interest disclosure: The authors declare no compet-ing financial interests.
Correspondence: Lynn B. Dustin, Center for the Study of
Hepatitis C, Laboratory of Virology and Infectious Disease,Rockefeller University, Box 64, 1230 York Ave, New York, NY10021; e-mail: [email protected].
References
1. Keeffe EB. Liver transplantation: current statusand novel approaches to liver replacement. Gas-troenterology. 2001;120:749-762.
2. Di Bisceglie AM, McHutchison J, Rice CM. Newtherapeutic strategies for hepatitis C. Hepatology.2002;35:224-231.
3. Agnello V, Chung RT, Kaplan LM. A role for hepa-titis C virus infection in type II cryoglobulinemia.N Engl J Med. 1992;327:1490-1495.
4. Mayo MJ. Extrahepatic manifestations of hepati-tis C infection. Am J Med Sci. 2003;325:135-148.
5. Perl A, Gorevic PD, Ryan DH, Condemi JJ, Rusz-kowski RJ, Abraham GN. Clonal B cell expan-sions in patients with essential mixed cryoglobuli-naemia. Clin Exp Immunol. 1989;76:54-60.
6. Sansonno D, Dammacco F. Hepatitis C virus,cryoglobulinaemia, and vasculitis: immune com-plex relations. Lancet Infect Dis. 2005;5:227-236.
7. Agnello V. The etiology and pathophysiology ofmixed cryoglobulinemia secondary to hepatitis Cvirus infection. Springer Semin Immunopathol.1997;19:111-129.
8. Ferri C, Caracciolo F, Zignego AL, et al. HepatitisC virus infection in patients with non-Hodgkin’slymphoma. Br J Haematol. 1994;88:392-394.
9. Matsuo K, Kusano A, Sugumar A, Nakamura S,Tajima K, Mueller NE. Effect of hepatitis C virusinfection on the risk of non-Hodgkin’s lymphoma:a meta-analysis of epidemiological studies. Can-cer Sci. 2004;95:745-752.
10. Weng WK, Levy S. Hepatitis C virus (HCV) andlymphomagenesis. Leuk Lymphoma. 2003;44:1113-1120.
11. La Civita L, Zignego AL, Monti M, LongombardoG, Pasero G, Ferri C. Mixed cryoglobulinemia asa possible preneoplastic disorder. ArthritisRheum. 1995;38:1859-1860.
12. Monti G, Pioltelli P, Saccardo F, et al. Incidenceand characteristics of non-Hodgkin lymphomas ina multicenter case file of patients with hepatitis Cvirus-related symptomatic mixed cryoglobuline-mias. Arch Intern Med. 2005;165:101-105.
13. De Re V, De Vita S, Marzotto A, et al. Pre-malig-nant and malignant lymphoproliferations in anHCV–infected type II mixed cryoglobulinemic pa-tient are sequential phases of an antigen-drivenpathological process. Int J Cancer. 2000;87:211-216.
14. Giordano TP, Henderson L, Landgren O, et al.Risk of non-Hodgkin lymphoma and lymphoprolif-erative precursor diseases in US veterans withhepatitis C virus. JAMA. 2007;297:2010-2017.
15. Dustin LB, Rice CM. Flying under the radar: theimmunobiology of hepatitis C. Annu Rev Immu-nol. 2007;25:71-99.
16. Franzin F, Efremov DG, Pozzato G, Tulissi P,Batista F, Burrone OR. Clonal B-cell expansionsin peripheral blood of HCV–infected patients. Br JHaematol. 1995;90:548-552.
17. Sansonno D, De Vita S, Iacobelli AR, Cornac-chiulo V, Boiocchi M, Dammacco F. Clonal analy-sis of intrahepatic B cells from HCV–infected pa-tients with and without mixed cryoglobulinemia.J Immunol. 1998;160:3594-3601.
18. Racanelli V, Sansonno D, Piccoli C, D’Amore FP,Tucci FA, Dammacco F. Molecular characteriza-tion of B cell clonal expansions in the liver ofchronically hepatitis C virus–infected patients.J Immunol. 2001;167:21-29.
19. Ivanovski M, Silvestri F, Pozzato G, et al. Somatichypermutation, clonal diversity, and preferentialexpression of the VH 51p1/VL kv325 immuno-globulin gene combination in hepatitis C virus–
associated immunocytomas. Blood. 1998;91:2433-2442.
20. De Re V, De Vita S, Marzotto A, et al. Sequenceanalysis of the immunoglobulin antigen receptorof hepatitis C virus–associated non-Hodgkin lym-phomas suggests that the malignant cells are de-rived from the rheumatoid factor-producing cellsthat occur mainly in type II cryoglobulinemia.Blood. 2000;96:3578-3584.
21. Gasparotto D, De Re V, Boiocchi M. Hepatitis Cvirus, B-cell proliferation and lymphomas. LeukLymphoma. 2002;43:747-751.
22. Carbonari M, Caprini E, Tedesco T, et al. HepatitisC virus drives the unconstrained monoclonal ex-pansion of VH1-69-expressing memory B cells intype II cryoglobulinemia: a model of infection-driven lymphomagenesis. J Immunol. 2005;174:6532-6539.
23. Knight GB, Agnello V, Bonagura V, Barnes JL,Panka DJ, Zhang QX. Human rheumatoid factorcross-idiotypes: IV. Studies on WA XId-positiveIgM without rheumatoid factor activity provide evi-dence that the WA XId is not unique to rheuma-toid factors and is distinct from the 17.109 and G6XIds. J Exp Med. 1993;178:1903-1911.
24. De Rosa FG, Pucillo LP, Casato M, Agnello V.Myths, misconceptions and mixed cryoglobuline-mia associated with HCV infection. Minerva Gas-troenterol Dietol. 2002;48:319-329.
25. Carlson SJ, Yokoo H, Vanagunas A. Progres-sion of gastritis to monoclonal B-cell lymphomawith resolution and recurrence following eradi-cation of Helicobacter pylori. JAMA. 1996;275:937-939.
26. Quinn ER, Chan CH, Hadlock KG, Foung SK,Flint M, Levy S. The B-cell receptor of a hepatitisC virus (HCV)–associated non-Hodgkin lym-phoma binds the viral E2 envelope protein, impli-cating HCV in lymphomagenesis. Blood. 2001;98:3745-3749.
27. Rosa D, Saletti G, De Gregorio E, et al. Activationof naive B lymphocytes via CD81, a pathogeneticmechanism for hepatitis C virus–associated Blymphocyte disorders. Proc Natl Acad Sci U S A.2005;102:18544-18549.
28. Racanelli V, Frassanito MA, Leone P, et al. Anti-body production and in vitro behavior of CD27-defined B-cell subsets: persistent hepatitis C vi-rus infection changes the rules. J Virol. 2006;80:3923-3934.
29. Zignego AL, Giannelli F, Marrocchi ME, et al.T(14;18) translocation in chronic hepatitis C virusinfection. Hepatology. 2000;31:474-479.
30. Zuckerman E, Zuckerman T, Sahar D, et al. Theeffect of antiviral therapy on t(14;18) translocationand immunoglobulin gene rearrangement in pa-tients with chronic hepatitis C virus infection.Blood. 2001;97:1555-1559.
31. Roulland S, Lebailly P, Lecluse Y, Heutte N,Nadel B, Gauduchon P. Long-term clonal persis-tence and evolution of t(14;18)-bearing B cells inhealthy individuals. Leukemia. 2006;20:158-162.
32. Lanford RE, Chavez D, Chisari FV, Sureau C.Lack of detection of negative-strand hepatitis Cvirus RNA in peripheral blood mononuclear cellsand other extrahepatic tissues by the highlystrand-specific rTth reverse transcriptase PCR.J Virol. 1995;69:8079-8083.
33. Ni J, Hembrador E, Di Bisceglie AM, et al. Accu-mulation of B lymphocytes with a naive, restingphenotype in a subset of hepatitis C patients.J Immunol. 2003;170:3429-3439.
34. Kallemuchikkal U, Gorevic PD. Evaluation of
cryoglobulins. Arch Pathol Lab Med. 1999;123:119-125.
35. Gorevic PD and Galanakis D. Cryoglobulins,cryofibrinogenemia, and pyroglobulins. In: RoseNR, Hamilton RG, Detrick B, eds. Manual of Clini-cal Laboratory Immunology (ed 6). Washington,DC: ASM Press; 2002:97-106.
36. Scheuer PJ. Classification of chronic viral hepati-tis: a need for reassessment. J Hepatol. 1991;13:372-374.
37. De Vita S, Boiocchi M, Sorrentino D, et al. Char-acterization of prelymphomatous stages of B-celllymphoproliferation in Sjogren’s syndrome. Arthri-tis Rheum. 1997;40:318-331.
38. Ramasamy I, Brisco M, Morley A. Improved PCRmethod for detecting monoclonal immunoglobulinheavy chain rearrangement in B cell neoplasms.J Clin Pathol. 1992;45:770-775.
39. Abramoff MD, Magelhaes PJ, Ram SJ. ImageProcessing with ImageJ. Biophotonics Int. 2004;11:36-42.
40. Wardemann H, Yurasov S, Schaefer A, YoungJW, Meffre E, Nussenzweig MC. Predominantautoantibody production by early human B cellprecursors. Science. 2003;301:1374-1377.
41. International Immunogenetics Information Sys-tem. http://imgt.cines.fr. Accessed September 8,2007.
42. National Institute of Arthritis and Musculoskeletaland Skin Diseases. Joinsolver. http://joinsolver.niams.nih.gov. Accessed September 8, 2007
43. Lefranc MP. IMGT databases, web resources andtools for immunoglobulin and T cell receptor se-quence analysis, http://imgt.cines.fr. Leukemia.2003;17:260-266.
44. Chang B, Casali P. The CDR1 sequences of amajor proportion of human germline Ig VH genesare inherently susceptible to amino acid replace-ment. Immunol Today. 1994;15:367-373.
45. Lossos I. http://www-stat.stanford.edu/immuno-globulin. Accessed September 8, 2007.
46. Thompson JD, Higgins DG, Gibson TJ. CLUSTALW: improving the sensitivity of progressive mul-tiple sequence alignment through sequenceweighting, position-specific gap penalties andweight matrix choice. Nucleic Acids Res. 1994;22:4673-4680.
47. National Center for Biotechnology Information.GenBank. http://ncbi.nlm.nih.gov/Genbank. Ac-cessed October 30, 2007.
48. Monti G, Galli M, Invernizzi F, et al. Cryoglobuli-naemias: a multi-centre study of the early clinicaland laboratory manifestations of primary and sec-ondary disease. GISC. Italian Group for the Studyof Cryoglobulinaemias. QJM. 1995;88:115-126.
49. Klein U, Rajewsky K, Kuppers R. Human immu-noglobulin (Ig)M�IgD� peripheral blood B cellsexpressing the CD27 cell surface antigen carrysomatically mutated variable region genes: CD27as a general marker for somatically mutated(memory) B cells. J Exp Med. 1998;188:1679-1689.
50. Curry MP, Golden-Mason L, Doherty DG, et al.Expansion of innate CD5pos B cells expressinghigh levels of CD81 in hepatitis C virus infectedliver. J Hepatol. 2003;38:642-650.
51. Zuckerman E, Slobodin G, Kessel A, et al. Pe-ripheral B-cell CD5 expansion and CD81 overex-pression and their association with disease se-verity and autoimmune markers in chronichepatitis C virus infection. Clin Exp Immunol.2002;128:353-358.
52. Baumgarth N, Tung JW, Herzenberg LA. Inherent
CLONAL EXPANSION OF IgM�CD27� B CELLS IN HCV MC 1355BLOOD, 1 FEBRUARY 2008 � VOLUME 111, NUMBER 3
For personal use only.on December 6, 2018. by guest www.bloodjournal.orgFrom

specificities in natural antibodies: a key to im-mune defense against pathogen invasion.Springer Semin Immunopathol. 2005;26:347-362.
53. Youinou P, Jamin C, Lydyard PM. CD5 expres-sion in human B-cell populations. Immunol Today.1999;20:312-316.
54. Crouzier R, Martin T, Pasquali JL. MonoclonalIgM rheumatoid factor secreted by CD5-negativeB cells during mixed cryoglobulinemia: evidencefor somatic mutations and intraclonal diversity ofthe expressed VH region gene. J Immunol. 1995;154:413-421.
55. Monteverde A, Ballare M, Pileri S. Hepatic lym-phoid aggregates in chronic hepatitis C andmixed cryoglobulinemia. Springer Semin Immu-nopathol. 1997;19:99-110.
56. Bende RJ, Aarts WM, Riedl RG, de Jong D, PalsST, van Noesel CJ. Among B cell non-Hodgkin’slymphomas, MALT lymphomas express a uniqueantibody repertoire with frequent rheumatoid fac-tor reactivity. J Exp Med. 2005;201:1229-1241.
57. Casato M, Mecucci C, Agnello V, et al. Regres-sion of lymphoproliferative disorder after treat-ment for hepatitis C virus infection in a patientwith partial trisomy 3, Bcl-2 overexpression, andtype II cryoglobulinemia. Blood. 2002;99:2259-2261.
58. Tsuiji M, Yurasov S, Velinzon K, Thomas S, Nus-senzweig MC, Wardemann H. A checkpoint forautoreactivity in human IgM� memory B cell de-velopment. J Exp Med. 2006;203:393-400.
59. Shiow LR, Rosen DB, Brdickova N, et al. CD69acts downstream of interferon-alpha/beta to in-hibit S1P1 and lymphocyte egress from lymphoidorgans. Nature. 2006;440:540-544.
60. Hermine O, Lefrere F, Bronowicki JP, et al. Re-gression of splenic lymphoma with villous lym-
phocytes after treatment of hepatitis C virus infec-tion. N Engl J Med. 2002;347:89-94.
61. Carsetti R, Rosado MM, Wardmann H. Peripheraldevelopment of B cells in mouse and man. Immu-nol Rev. 2004;197:179-191.
62. Weller S, Braun MC, Tan BK, et al. Human bloodIgM “memory” B cells are circulating splenic mar-ginal zone B cells harboring a prediversified im-munoglobulin repertoire. Blood. 2004;104:3647-3654.
63. Tierens A, Delabie J, Pittaluga S, Driessen A, De-Wolf-Peeters C. Mutation analysis of the rear-ranged immunoglobulin heavy chain genes ofmarginal zone cell lymphomas indicates an originfrom different marginal zone B lymphocyte sub-sets. Blood. 1998;91:2381-2386.
64. Weller S, Faili A, Garcia C, et al. CD40-CD40Lindependent Ig gene hypermutation suggests asecond B cell diversification pathway in humans.Proc Natl Acad Sci U S A. 2001;98:1166-1170.
65. Klein U, Kuppers R, Rajewsky K. Evidence for alarge compartment of IgM-expressing memory Bcells in humans. Blood. 1997;89:1288-1298.
66. Moccia F, Tognoni E, Boccaccio P. The relation-ship between splenic marginal zone B-cell lym-phoma and chronic liver disease associated withhepatitis C virus infection. Ann Ital Med Int. 1999;14:288-293.
67. Kelaidi C, Rollot F, Park S, et al. Response to an-tiviral treatment in hepatitis C virus–associatedmarginal zone lymphomas. Leukemia. 2004;18:1711-1716.
68. Marasca R, Vaccari P, Luppi M, et al. Immuno-globulin gene mutations and frequent use ofVH1-69 and VH4-34 segments in hepatitis C vi-rus-positive and hepatitis C virus-negative nodal
marginal zone B-cell lymphoma. Am J Pathol.2001;159:253-261.
69. Wehr C, Eibel H, Masilamani M, et al. A newCD21low B cell population in the peripheral bloodof patients with SLE. Clin Immunol. 2004;113:161-171.
70. Moir S, Malaspina A, Ogwaro KM, et al. HIV-1induces phenotypic and functional perturbationsof B cells in chronically infected individuals. ProcNatl Acad Sci U S A. 2001;98:10362-10367.
71. Zabel MD, Weis JH. Cell-specific regulation of theCD21 gene. Int Immunopharmacol. 2001;1:483-493.
72. Segundo C, Medina F, Rodriguez C, Martinez-Palencia R, Leyva-Cobian F, Brieva JA. Surfacemolecule loss and bleb formation by human ger-minal center B cells undergoing apoptosis: role ofapoptotic blebs in monocyte chemotaxis. Blood.1999;94:1012-1020.
73. Adderson EE, Shackelford PG, Quinn A, et al.Restricted immunoglobulin VH usage andVDJ combinations in the human responseto Haemophilus influenzae type b capsularpolysaccharide: nucleotide sequences ofmonospecific anti-Haemophilus antibodiesand polyspecific antibodies cross-reactingwith self antigens. J Clin Invest. 1993;91:2734-2743.
74. Soulas P, Woods A, Jaulhac B, et al. Autoantigen,innate immunity, and T cells cooperate to break Bcell tolerance during bacterial infection. J Clin In-vest. 2005;115:2257-2267.
75. Leadbetter EA, Rifkin IR, Hohlbaum AM, Beau-dette BC, Shlomchik MJ, Marshak-Rothstein A.Chromatin-IgG complexes activate B cells bydual engagement of IgM and Toll-like receptors.Nature. 2002;416:603-607.
1356 CHARLES et al BLOOD, 1 FEBRUARY 2008 � VOLUME 111, NUMBER 3
For personal use only.on December 6, 2018. by guest www.bloodjournal.orgFrom

online October 17, 2007 originally publisheddoi:10.1182/blood-2007-07-101717
2008 111: 1344-1356
Ira M. Jacobson, Charles M. Rice and Lynn B. DustinEdgar D. Charles, Rashidah M. Green, Svetlana Marukian, Andrew H. Talal, Gerond V. Lake-Bakaar, HCV-associated mixed cryoglobulinemia
B cells in+CD27+Clonal expansion of immunoglobulin M
http://www.bloodjournal.org/content/111/3/1344.full.htmlUpdated information and services can be found at:
(5642 articles)Immunobiology and Immunotherapy (4866 articles)Clinical Trials and Observations
Articles on similar topics can be found in the following Blood collections
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
Copyright 2011 by The American Society of Hematology; all rights reserved.of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society
For personal use only.on December 6, 2018. by guest www.bloodjournal.orgFrom