Clinical Study Serum NGAL in Critically Ill Children in ICU from a...
8
Hindawi Publishing Corporation ISRN Nephrology Volume 2013, Article ID 140905, 7 pages http://dx.doi.org/10.5402/2013/140905 Clinical Study Serum NGAL in Critically Ill Children in ICU from a Single Center in Egypt Doaa Mohammed Youssef, 1 Asmaa Mohammed Esh, 2 Ebthag Helmy Hassan, 2 and Tahia Mohammed Ahmed 2 1 Pediatric Department, Zagazig University, Zagazig 44519, Egypt 2 Clinical Pathology Department, Zagazig University, Zagazig 44519, Egypt Correspondence should be addressed to Doaa Mohammed Youssef; [email protected] Received 4 December 2012; Accepted 26 December 2012 Academic Editors: M. L´ eone and D. Malhotra Copyright © 2013 Doaa Mohammed Youssef et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Introduction. e mortality and morbidity associated with acute kidney injury (AKI), unfortunately, remain unacceptably high. We aimed to detect the extent of serum neutrophil gelatinase-associated lipocalin (NGAL) to early detect AKI in critically ill children. Subjects and Methods. is is a case control study. It included 75 subjects that include 15 as controls and 60 critically ill children. Patients were further subdivided according to RIFLE criteria into two other categories: patients who developed AKI and patients who did not develop AKI. Serum NGAL assayed on admission and aſter 3 days. Results. ere was significant increase in the level of NGAL among patients group when compared with control group. Also, 21.7% of children admitted to PICU developed AKI from which 8.3% needed dialysis. e receiver operating characteristic curve of NGAL at day 0 revealed AUC of 0.63 with 95% CI of 0.50–0.77. At a cutoff value of 89.5 ng/mL, the sensitivity of NGAL was 84.6%, while specifcity was 59.6%, positive predictive value was 36.7%, negative predictive value was 68.4%, and accuracy was 93.3% in diagnosis of AKI. Conclusion. We found that NGAL acts as a sensitive marker rather than a specific one for AKI. At the same time, it presents as a negative predictive value more valuable than being a positive predictive value in detecting AKI. 1. Introduction Acute kidney injury (AKI), formerly known as acute renal failure, continues to represent a very common and potentially devastating problem in critically ill children and adults. e reported incidence of AKI in this population varies greatly due to the lack of a standard consensus definition. For example, AKI affects between 5% and 50% of critically ill patients in reported series [1]. Unfortunately, the mortality and morbidity associated with AKI remain unacceptably high (up to 80% mortality in critically ill children and adults with multiple organ dys- function syndrome (MODS)). While this dismal prognosis is partly attributable to other comorbid conditions, recent studies have revealed that AKI may be an independent risk factor for mortality in both critically ill children [2] and adults [3]. Acute kidney injury is typically diagnosed by measuring serum creatinine. However, it is well known that creatinine is an unreliable and insensitive indicator during early acute changes in kidney function. First, serum creatinine concen- trations may not change until about 50% of kidney function has already been lost. Second, serum creatinine does not accurately depict kidney function until a steady state has been reached, which may require several days [4]. Neutrophil gelatinase-associated lipocalin is a 25 kDa protein that is expressed at very low concentrations in several human tissues, including the kidney, lungs, and gastrointesti- nal tract [5]. e aim of this study was to detect the extent of serum neutrophil gelatinase-associated lipocalin (NGAL) to early detect acute kidney injury (AKI) in critically ill children and to evaluate its sensitivity and specificity in AKI detection.
Transcript of Clinical Study Serum NGAL in Critically Ill Children in ICU from a...

Hindawi Publishing CorporationISRN NephrologyVolume 2013 Article ID 140905 7 pageshttpdxdoiorg1054022013140905
Clinical StudySerum NGAL in Critically Ill Children in ICU from a SingleCenter in Egypt
Doaa Mohammed Youssef1 Asmaa Mohammed Esh2
Ebthag Helmy Hassan2 and Tahia Mohammed Ahmed2
1 Pediatric Department Zagazig University Zagazig 44519 Egypt2 Clinical Pathology Department Zagazig University Zagazig 44519 Egypt
Correspondence should be addressed to Doaa Mohammed Youssef dody5176yahoocom
Received 4 December 2012 Accepted 26 December 2012
Academic Editors M Leone and D Malhotra
Copyright copy 2013 Doaa Mohammed Youssef et al This is an open access article distributed under the Creative CommonsAttribution License which permits unrestricted use distribution and reproduction in any medium provided the original work isproperly cited
IntroductionThemortality andmorbidity associated with acute kidney injury (AKI) unfortunately remain unacceptably highWeaimed to detect the extent of serum neutrophil gelatinase-associated lipocalin (NGAL) to early detect AKI in critically ill childrenSubjects and Methods This is a case control study It included 75 subjects that include 15 as controls and 60 critically ill childrenPatients were further subdivided according to RIFLE criteria into two other categories patients who developed AKI and patientswho did not develop AKI Serum NGAL assayed on admission and after 3 days ResultsThere was significant increase in the levelof NGAL among patients group when compared with control group Also 217 of children admitted to PICU developed AKI fromwhich 83 needed dialysis The receiver operating characteristic curve of NGAL at day 0 revealed AUC of 063 with 95 CI of050ndash077 At a cutoff value of 895 ngmL the sensitivity of NGAL was 846 while specifcity was 596 positive predictive valuewas 367 negative predictive value was 684 and accuracy was 933 in diagnosis of AKIConclusionWe found that NGAL actsas a sensitive marker rather than a specific one for AKI At the same time it presents as a negative predictive value more valuablethan being a positive predictive value in detecting AKI
1 Introduction
Acute kidney injury (AKI) formerly known as acute renalfailure continues to represent a very common and potentiallydevastating problem in critically ill children and adults Thereported incidence of AKI in this population varies greatlydue to the lack of a standard consensus definition Forexample AKI affects between 5 and 50 of critically illpatients in reported series [1]
Unfortunately the mortality and morbidity associatedwith AKI remain unacceptably high (up to 80 mortalityin critically ill children and adults with multiple organ dys-function syndrome (MODS)) While this dismal prognosisis partly attributable to other comorbid conditions recentstudies have revealed that AKI may be an independent riskfactor formortality in both critically ill children [2] and adults[3]
Acute kidney injury is typically diagnosed by measuringserum creatinine However it is well known that creatinineis an unreliable and insensitive indicator during early acutechanges in kidney function First serum creatinine concen-trations may not change until about 50 of kidney functionhas already been lost Second serum creatinine does notaccurately depict kidney function until a steady state has beenreached which may require several days [4]
Neutrophil gelatinase-associated lipocalin is a 25 kDaprotein that is expressed at very low concentrations in severalhuman tissues including the kidney lungs and gastrointesti-nal tract [5]
The aim of this study was to detect the extent of serumneutrophil gelatinase-associated lipocalin (NGAL) to earlydetect acute kidney injury (AKI) in critically ill children andto evaluate its sensitivity and specificity in AKI detection
2 ISRN Nephrology
2 Subjects and Methods
This study had been carried out in Pediatric Intensive CareUnit (PICU) and Clinical Pathology Department Faculty ofMedicine Zagazig University Hospital
This study included (75) subjects They were classifiedinto group I (15) apparently healthy volunteers and their agesranged between 1 and 29 months with the median age of 6months and group II (60) children who were admitted atPICU and their ages ranged between 1 and 108 months withthe median age of 9 months
For group I routine investigations as liver functionkidney function and complete blood count were done toconfirm their healthy state
For group II serum creatinine was measured in the firstday of admission and then another sample was measured inthe 3rd day of admission to the PICU This group of patientswas further subdivided according to RIFLE criteria into twoother categories groupA patients who developedAKI (AKI)and group B patients who did not develop AKI (NAKI) TheRIFLE criteria include (risk of acute renal failure injury tothe kidney and failure of renal function)
Then the patients who developedAKI are further dividedinto two other groups according to the severity (dialysisdependence) as follow AKI with dialysis (AKI +D) and AKIwithout dialysis (AKIminusD)
All studied subjects included in this study were subjectedto the following full history taking including family historyof underlying kidney disease complete clinical examinationroutine laboratory investigations and serum NGAL assay
21 NGAL Assay
211 Sampling Five milliliters of venous blood were col-lected under complete aseptic precautions from each subjectThe collected blood was divided as the following
(i) 1mL was delivered into EDTA containing polypropy-lene tube and then gently inverted then CBC wasperformed
(ii) 4mL were collected in plain tube for serum sepa-ration After clotting samples were centrifuged at1000timesg for 15 minutes and sera were separated anddivided into two aliquots A fresh serum aliquotfrom each individual was used for assay of serumcreatinine blood urea nitrogen (BUN) and liverfunction tests The other aliquot was stored at minus20∘Cuntil the assay of neutrophil gelatinase-associatedlipocalin Hemolyzed samples were discarded andrepeated freezing and thawing was avoided
22 NGAL Assay by Enzyme-Linked Immunosorbent AssayAssay of NGALwas carried out by a sandwich enzyme-linkedimmunosorbent assay (ELISA) technique using reagents pro-vided by Quantikine RampD International Inc (RampD SystemsInc MN USA)
Principle This assay employs the quantitative sandwichenzyme immunoassay technique A monoclonal antibody
specific for NGAL has been precoated onto a microplateStandards and samples are pipetted into the wells and anyNGAL present is bound by the immobilized antibody Afterwashing away any unbound substances an enzyme-linkedmonoclonal antibody specific for NGAL is added to the wellsFollowing a wash step to remove any unbound antibodyenzyme reagent a substrate solution is added to thewells andcolor develops in proportion to the amount of NGAL boundin the initial step The color development is stopped and theintensity of the color is measured [6]
Reagents are as follows
(i) NGAL microplate 96-well polystyrene microplate(12 strips of 8 wells) coated with a rat monoclonalantibody against NGAL
(ii) NGAL conjugate 21mL of monoclonal antibodyagainst NGAL conjugated to horseradish peroxidasewith preservatives
(iii) NGAL standard 100 ng of recombinant humanNGAL in a buffer with preservatives lyophilizedNGAL standard was reconstituted with 10mL ofdeionized or distilled water This reconstitution pro-duces a stock solution of 100 ngmLThe standardwasmixed to ensure complete reconstitution and thestandard was allowed to sit for a minimum of 15 min-utes with gentle agitation prior to making dilutions
Serial dilution of standard was done to obtain the followingconcentrations 10 5 25 125 0625 0312 and 0156 ngmL900120583L of calibrator diluent were pipetted into the 10 ngmLtube 500120583L were pipetted into the remaining tubes Thestock solution was used to produce a dilution series (later)Each tube wasmixed thoroughly before the next transferThe10 ngmL standard served as the high standardThe calibratordiluent served as the zero standard (0 ngmL)
(iv) assay diluent RD1-52 11mL of a buffer with preserva-tives
(v) calibrator diluent RD5-24 concentrate 21mL of a 5-fold concentrated solution containing buffered pro-tein base with preservatives
(vi) wash buffer concentrate 21mL of a 25-fold concen-trated solution of buffered surfactant with preserva-tives
(vii) color reagent A 125mL of stabilized hydrogen per-oxide
(viii) color reagent B 125mL of stabilized chromogen(tetramethylbenzidine)
(ix) stop solution 6mL of 2N sulfuric acid
(x) plate covers 4 adhesive strips
Assay Procedure
(i) 100 120583L of assay diluent RD1-52 were dispensed intoeach well
ISRN Nephrology 3
(ii) 50 120583L of standards controls and samples were addedto each well
(iii) The plate was covered and incubated for 2 hours at 2ndash8∘C
(iv) Aspiration of each well was done and this was fol-lowed by a washing step which was repeated threetimes
(v) 200120583L of NGAL conjugate were added into each wellcovered with a new adhesive strip and incubated for 2hours at 2ndash8∘C
(vi) Aspirationwashing was repeated as in step (iii)
(vii) 200120583L of substrate solution were dispended into eachwell
(viii) Plate was covered and incubated for 30 minutes atroom temperature
(ix) 50 120583L of stop solution were added into each well
(x) Determination of the optical density of each wellwithin 30 minutes was done using a microplatereader set to 450 nm
Calculation of Results A standard curve was constructed byplotting themean absorbance for each standard on the 119910-axisagainst the concentration on the 119909-axis on log-log graph anda best fit line was drawn through the points on the graphConcentration of lipocaline-2 in each sample was determinedby finding the mean absorbance value of each one Fromthe 119910-axis of the standard curve graph a vertical line wasextended from this absorbance value to the standard curveAt the point of intersection a horizontal line was extended tothe 119909-axis and the corresponding concentration was read
3 Statistical Analysis
The data were tabulated and statistically analyzed usingStatistical Package for Social Sciences (SPSS Inc ChicagoIL USA) version 17 Comparison of continuous data wasperformed using student 119905-test and Mann-Whitney test fortwo groups while for more than two groups ANOVA testwas used ROC curves analysis (an efficient way to displaythe relationship between sensitivity (true positive rate) andspecificity (true negative rate) for tests with continuousoutcomes a point in the curve moves down and to the leftshowing lower sensitivity and high specificity while it movesup and to the right showing higher sensitivity and lowerspecificity) was used The cutoff value was selected from theROCcurve by choosing a point having the best sensitivity andconsiderable specificity 119875 value lt 005 was considered statis-tically significant Sensitivity is the proportion of true positivethat are correctly identified Specificity is the proportion oftrue negative that are correctly identified Positive predictiveValue (PPV) is probability of disease in a patient with anabnormal testNegative Predictive Value (NPV) is probabilityof a patient not having the disease when the test result isnegative
0 025 05 075 1
Sens
itivi
ty
ROC curve
0
025
05
075
1
1minus Specificity
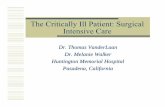
Figure 1 Receiver operating characteristic curve of NGAL
4 Results
The routine Laboratory results in our studies subjects werepresented on Table 1 We found that range of NGAL at dayzero was (34ndash210) with median of 885 and at 3rd day was(34ndash550) with median 114 urea at day zero ranged from 15to 116 with median of 355 and at 3rd day ranged from 27to 310 with median of 415 while creatinine at zero day was(X1015840 plusmn SD = 068plusmn022) while at 3rd day (X1015840 plusmn SD 118plusmn108)So there were statistical significance between NGAL ureaand creatinine at day zero and 3rd day (119875 = 0000) as shownin Table 2
A significant increase between two groups with and with-out AKI regarding NGAL urea and creatinine at admissionand at 3rd day (119875 lt 005) was shown in Table 3
There was no statistical significance among the 3 groupsregarding NGAL at admission and urea at 3rd day (119875 = 024and 076 resp) However there was statistical significanceamong the 3 groups regarding NGAL at 3rd day urea atadmission and creatinine at admission and at 3rd day (119875 =007 001 0004 and 0000 resp) as presented in Table 4
Table 5 described that applying the receiver operatingcharacteristic (ROC) curve of NGAL to early detectionof AKI revealed area under the curve of 063 with 95confidence interval (CI) of 050ndash077 A cutoff of 895 ngmLwas chosen for early detection of AKI presented in Figure 1
NGAL acts as a sensitive marker rather than a specificone At the same time it presents a negative predictivevalue more valuable than being a positive predictive valuein detecting AKI We described in Table 6 that at cutoff of895 ngmL NGAL was positive at 11 out of 13 patients withAKI the sensitivity of NGAL in diagnosis of AKI was 846Howerver 28 out of 47 had truly absent AKI with specificity596 The positive predictive value (11(11 + 19)) was 367and the negative predictive value (28(2 + 28)) was 933
4 ISRN Nephrology
Table 1 Laboratory investigations of study groups regarding liver and kidney functions
Parameter Control119873 = 15 Patients119873 = 60 Test of significance 119875
Total bilirubin (mgdL)Median 04 05 125b 0210Range (03ndash08) (03ndash234)
Direct bilirubin (mgdL)Median 01 05 099b 0321Range (01ndash02) (01ndash129)
ALT (UL)Median 31 455 111b 026Range (12ndash42) (9ndash133)
AST (UL)Median 38 556 3007b 0003lowastRange (5ndash55) (18ndash1207)
Albumin (gdL)X1015840plusmn SD (3907 plusmn 0371) (336 plusmn 0618) 3245a 0002lowast
TP (gdL)X1015840plusmn SD (68 plusmn 0442) (57 plusmn 0868) 447a 0001lowast
Urea (mgdL)Median 258 355 342b 0001lowastRange (15ndash37) (15ndash116)
Creatinine (mgdL)X1015840plusmn SD 065 plusmn 022 068 plusmn 022 038a 069
WBCs (times103cmm) 121 (61ndash141) 131 (21ndash562) 064b 051Hb (gdL ) 125 (95ndash155) 105 (66ndash18) 626b 0001lowast
Platelet (times109cmm) 250 (180ndash340) 222 (35ndash1008) 049b 062NGAL-0 (ngmL) 54 (44ndash141) 885 (34ndash210) 247b 001lowast
Test of significance at-test bMann-Whiney test lowastsignificant
Table 2 Acute kidney injury (AKI) markers at admission (day 0)and after 3 days (3rd day) among patients group
Parameter Day zero 3rd day Wilcoxonrsquosrank sum test 119875
NGAL (ngmL)Median 885 144 628 0000lowastRange (34ndash210) (34ndash550)
Urea (mgdL)Median 355 415 601 0000lowastRange (15ndash116) (27ndash310)
Creatinine(mgdL)
X1015840plusmn SD 068 plusmn 022 118 plusmn 108 41 0000lowastlowast
Significant
5 Discussion
Acute kidney injury is a common and serious conditionand the diagnosis of which depends on serum creatinineurea which is a delayed and unreliable indicator of AKIFortunately understanding the early stress response of thekidney to acute injuries has revealed a number of potentialbiomarkers [7]
Neutrophil gelatinase-associated lipocalin is a small pro-tein of the lipocalin superfamily and is expressed by immunecells hepatocytes and renal tubular cells [8]
In particular NGAL is emerging as an excellent biomark-er in the urine and plasma for several processes such as earlyprediction of AKI monitoring clinical trials in AKI and forthe prognosis of AKI in several common clinical scenarios[7]
The aim of the present work was to assess serum levels ofNGAL in critically ill children affected byAKI and to evaluateits clinical significance in diagnosis as well as assessment ofdisease severity in comparison with other markers as serumcreatinine and urea ratio in critically ill children
We prospectively measured serumNGAL concentrationsduring day zero and after the 3rd day of admission to thePICU in 60 critically ill children (28 males and 32 females)and 15 healthy children (8 males and 7 females)
In our prospective study there were no statistical sig-nificant differences between controls and patients groupregarding demographic data including age and gender 119875 =015 and 119875 = 064 respectively
The liver function (total bilirubin direct bilirubin andALT) showed that there was no statistical significance dif-ference between critically ill children and control groupHowever there was a significant increase in the level of AST
ISRN Nephrology 5
Table 3 Serum NGAL urea and creatinine at day zero and 3rd day among 2 groups of patients AKI (group A) and NAKI (group B)
Parameters AKI Test of significance119875
Absent119873 = 47 Present119873 = 13NGAL-0 (ngmL)
Median 76 110 264b 0008lowastRange (34ndash200) (66ndash210)
NGAL-3 (ngmL)Median 105 280 332b 0001lowastRange (34ndash530) (92ndash550)
Urea-0 (mgdL)Median 345 425 204b 0040lowastRange (15ndash116) (287ndash788)
Urea-3 (mgdL)Median 38 1134 300b 0003lowastRange (18ndash310) (7ndash228)
Creatinine-0 (mgdL)X plusmn SD 061 plusmn 023 086 plusmn 023 34a 0001lowast
Creatinine-3 (mgdL)X plusmn SD 073 plusmn 063 208 plusmn 124 101a 0000lowast
Test of significance at-test bMann-Whiney test lowastsignificant
and significant decrease in the levels of albumin and totalprotein among the two groups
Regarding kidney function there was significant increasein the level of urea in patients group compared to controlgroup (119875 = 0000) However creatinine value increased incritically ill children group showing no statistical significancewith control group (119875 = 069)
This is in agreement with Bagshaw et al (2006) [3] whoreported that urea is not produced at a constant rate and therate can be influenced by extrarenal factors Urea productioncan be increased by diet critical illness burns traumagastro intestinal bleeding and sepsis Also in patients withdecreased circulating blood volume due to volume depletionor low cardiac output resorption of urea increases because ofthe relationship between urea levels and water conservationmechanisms Therefore urea can be influenced by multiplefactors and does not represent real-time changes in GFR
In the present study the level of serum NGAL con-centration for control group ranged from 44 to 141 ngmLwith median of 54 ngmL and critically ill children groupranged from 34 to 210 ngmL with median of 885 ngmLat admission There was significant increase in the level ofNGAL in the critically ill children group compared to controlgroup 119875 lt 001
These findings are in agreement with Bailey et al (2007)who reported that there was a significant difference in serumNGAL between healthy children and critically ill children [1]
Critically ill children who developed AKI (by doublingof serum creatinine from baseline according to RIFLEclassification) had significantly elevated serum NGAL ureaand creatinine levels at 3rd-day compared to serum NGALurea and creatinine at day zero Also critically ill childrenwho developed AKI had significantly elevated serum NGAL
urea and creatinine levels at day zero and at 3rd day whencompared with critically ill children who did not developAKI
This goes hand in hand with Mishra et al (2005) [8]and Wheeler et al (2008) [9] who demonstrated that serumNGAL concentrations within 24 hours of PICU admissionwere significantly increased in these children who developedAKI compared to children who did not develop AKI Asecond sample was obtained on the third day of admissionto the PICU and the difference between critically ill childrenwith AKI and critically ill children without AKI remainedsignificant (119875 lt 0001)
AKI developed in 13 out of 60 (217) critically ill childrenincluded in this studymdashall but 5 of these critically ill children(83) had a greater severity of illness and need to dialysisPatients who developed AKI and need to dialysis showedhigher level of NGAL at day 0 compared to patients whodeveloped AKI without need to dialysis and patients who didnot develop AKI but with no statistical significance whileat 3rd day it markedly increased (median = 350 ngmL) andbecame highly significant (119875 = 004)
These findings are in agreement with Hoste et al (2003)[10] who found that AKI developed in 32 out of 69 (463)critically ill childrenmdashall but 8 of these critically ill children(115) had a greater severity of illness and need to dialysis
In our study the receiver operating characteristic curveof NGAL for early detection of AKI revealed area under thecurve of 063 with 95 (CI of 050ndash077) At cutoff value of895 ngmL the sensitivity ofNGALwas 846 the specificitywas 596 positive predictive value was 367 and negativepredictive value was 684
Close results were found by Akcan-Arikan et al (2007)[2] who had shown that at cutoff of 139 ngmL the receiver
6 ISRN Nephrology
Table 4 Comparative study of patients group according to NGAL Urea and creatinine at admission (day zero) and 3rd day and theirclassification according to severity to 3 subgroups NAKI AKI minus D and AKI + D
Parameter NAKI AKI minus D AKI + D Test of significance 119875
119873 = 47 119873 = 8 119873 = 5
NGAL-0 (ngmL)Median 84 1005 120 137b 024Range (34ndash210) (74ndash115) (66ndash148)
NGAL-3 (ngmL)Median 105 184 350 308b 004lowastRange (34ndash530) (42ndash395) (150ndash550)
Urea-0 (mgdL)Median 345 38 65 591b 001lowastRange (15ndash116) (28ndash57) (425ndash788)
Urea-3 (mgdL)Median 38 841 1134 008b 076Range (18ndash310) (40ndash228) (7ndash178)
Creatinine-0 (mgdL)X plusmn SD 06 plusmn 023 08 plusmn 027 094 plusmn 015 119865 = 622 0004lowast
Creatinine-3 (mgdL)X plusmn SD 073 plusmn 036 225 plusmn 101 37 plusmn 11 119865 = 779 0000lowast
bMann-Whitney test 119865 Fisher test lowastsignificant
Table 5 Area under the receiver operating characteristic curve(ROC-AUC) and cutoff value for NGAL
Parameter ROC-AUC 95 CI CutoffNGAL-0 063 050ndash077 895 ngmL
Table 6 Validity of NGAL in prediction of AKI
Parameter AKI TotalPresent Absent
NGAL ge 895 11 19 30NGAL le 895 2 28 30Total 13 47 60
operating characteristic curve of NGAL revealed area underthe curve of 0677 with 95 (CI of 0557ndash0786)The sensitiv-ity of NGALwas 86 specificity was 39 positive predictivevalue was 39 and negative predictive value was 94
Our results of early predictive sensitive nonspecificserum NGAL although of clear statistical significance willcertainly need to be validated in a larger trial includingpatients with preexisting chronic kidney disease and comorbid conditions that normally accumulate with impairedrenal function The ability of biomarkers such as NGAL todiscern both the onset and resolution of AKI will furthervalidate their use in the clinical setting and greatly enhanceour understanding of AKI in the pediatric population
6 Conclusion
In conclusion we found that NGAL acts as a sensitivemarkerrather than a specific for one AKI At the same time it
presents a negative predictive value more valuable than beinga positive predictive value in detecting AKI
References
[1] D Bailey V Phan C Litalien et al ldquoRisk factors of acute renalfailure in critically ill children a prospective descriptive epi-demiological studyrdquo Pediatric Critical Care Medicine vol 8 no1 pp 29ndash35 2007
[2] A Akcan-Arikan M Zappitelli L L Loftis K K WashburnL S Jefferson and S L Goldstein ldquoModified RIFLE criteria incritically ill children with acute kidney injuryrdquo Kidney Interna-tional vol 71 no 10 pp 1028ndash1035 2007
[3] S M Bagshaw C Langenberg and R Bellomo ldquoUrinary bio-chemistry and microscopy in septic acute renal failure a sys-tematic reviewrdquo American Journal of Kidney Diseases vol 48no 5 pp 695ndash705 2006
[4] S M Moran and B D Myers ldquoCourse of acute renal failurestudied by a model of creatinine kineticsrdquo Kidney Internationalvol 27 no 6 pp 928ndash937 1985
[5] L Kjeldsen A H Johnsen H Sengelov and N BorregaardldquoIsolation and primary structure of NGAL a novel proteinassociated with human neutrophil gelatinaserdquo The Journal ofBiological Chemistry vol 268 no 14 pp 10425ndash10432 1993
[6] K Mori and K Nakao ldquoNeutrophil gelatinase-associated lipo-calin as the real-time indicator of active kidney damagerdquoKidneyInternational vol 71 no 10 pp 967ndash970 2007
[7] P Devarajan ldquoBiomarkers for the early detection of acutekidney injuryrdquo Current Opinion in Pediatrics vol 23 no 2 pp194ndash200 2011
[8] J Mishra C Dent R Tarabishi et al ldquoNeutrophil gelatinase-associated lipocalin (NGAL) as a biomarker for acute renalinjury after cardiac surgeryrdquoThe Lancet vol 365 no 9466 pp1231ndash1238 2005
ISRN Nephrology 7
[9] D S Wheeler P Devarajan Q Ma et al ldquoSerum neutrophilgelatinase-associated lipocalin (NGAL) as a marker of acutekidney injury in critically ill children with septic shockrdquoCriticalCare Medicine vol 36 no 4 pp 1297ndash1303 2008
[10] E A J Hoste N H Lameire R C Vanholder D D Benoit JM A Decruyenaere and F A Colardyn ldquoAcute renal failurein patients with sepsis in a surgical ICU predictive factorsincidence comorbidity and outcomerdquo Journal of the AmericanSociety of Nephrology vol 14 no 4 pp 1022ndash1030 2003
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 ISRN Nephrology
2 Subjects and Methods
This study had been carried out in Pediatric Intensive CareUnit (PICU) and Clinical Pathology Department Faculty ofMedicine Zagazig University Hospital
This study included (75) subjects They were classifiedinto group I (15) apparently healthy volunteers and their agesranged between 1 and 29 months with the median age of 6months and group II (60) children who were admitted atPICU and their ages ranged between 1 and 108 months withthe median age of 9 months
For group I routine investigations as liver functionkidney function and complete blood count were done toconfirm their healthy state
For group II serum creatinine was measured in the firstday of admission and then another sample was measured inthe 3rd day of admission to the PICU This group of patientswas further subdivided according to RIFLE criteria into twoother categories groupA patients who developedAKI (AKI)and group B patients who did not develop AKI (NAKI) TheRIFLE criteria include (risk of acute renal failure injury tothe kidney and failure of renal function)
Then the patients who developedAKI are further dividedinto two other groups according to the severity (dialysisdependence) as follow AKI with dialysis (AKI +D) and AKIwithout dialysis (AKIminusD)
All studied subjects included in this study were subjectedto the following full history taking including family historyof underlying kidney disease complete clinical examinationroutine laboratory investigations and serum NGAL assay
21 NGAL Assay
211 Sampling Five milliliters of venous blood were col-lected under complete aseptic precautions from each subjectThe collected blood was divided as the following
(i) 1mL was delivered into EDTA containing polypropy-lene tube and then gently inverted then CBC wasperformed
(ii) 4mL were collected in plain tube for serum sepa-ration After clotting samples were centrifuged at1000timesg for 15 minutes and sera were separated anddivided into two aliquots A fresh serum aliquotfrom each individual was used for assay of serumcreatinine blood urea nitrogen (BUN) and liverfunction tests The other aliquot was stored at minus20∘Cuntil the assay of neutrophil gelatinase-associatedlipocalin Hemolyzed samples were discarded andrepeated freezing and thawing was avoided
22 NGAL Assay by Enzyme-Linked Immunosorbent AssayAssay of NGALwas carried out by a sandwich enzyme-linkedimmunosorbent assay (ELISA) technique using reagents pro-vided by Quantikine RampD International Inc (RampD SystemsInc MN USA)
Principle This assay employs the quantitative sandwichenzyme immunoassay technique A monoclonal antibody
specific for NGAL has been precoated onto a microplateStandards and samples are pipetted into the wells and anyNGAL present is bound by the immobilized antibody Afterwashing away any unbound substances an enzyme-linkedmonoclonal antibody specific for NGAL is added to the wellsFollowing a wash step to remove any unbound antibodyenzyme reagent a substrate solution is added to thewells andcolor develops in proportion to the amount of NGAL boundin the initial step The color development is stopped and theintensity of the color is measured [6]
Reagents are as follows
(i) NGAL microplate 96-well polystyrene microplate(12 strips of 8 wells) coated with a rat monoclonalantibody against NGAL
(ii) NGAL conjugate 21mL of monoclonal antibodyagainst NGAL conjugated to horseradish peroxidasewith preservatives
(iii) NGAL standard 100 ng of recombinant humanNGAL in a buffer with preservatives lyophilizedNGAL standard was reconstituted with 10mL ofdeionized or distilled water This reconstitution pro-duces a stock solution of 100 ngmLThe standardwasmixed to ensure complete reconstitution and thestandard was allowed to sit for a minimum of 15 min-utes with gentle agitation prior to making dilutions
Serial dilution of standard was done to obtain the followingconcentrations 10 5 25 125 0625 0312 and 0156 ngmL900120583L of calibrator diluent were pipetted into the 10 ngmLtube 500120583L were pipetted into the remaining tubes Thestock solution was used to produce a dilution series (later)Each tube wasmixed thoroughly before the next transferThe10 ngmL standard served as the high standardThe calibratordiluent served as the zero standard (0 ngmL)
(iv) assay diluent RD1-52 11mL of a buffer with preserva-tives
(v) calibrator diluent RD5-24 concentrate 21mL of a 5-fold concentrated solution containing buffered pro-tein base with preservatives
(vi) wash buffer concentrate 21mL of a 25-fold concen-trated solution of buffered surfactant with preserva-tives
(vii) color reagent A 125mL of stabilized hydrogen per-oxide
(viii) color reagent B 125mL of stabilized chromogen(tetramethylbenzidine)
(ix) stop solution 6mL of 2N sulfuric acid
(x) plate covers 4 adhesive strips
Assay Procedure
(i) 100 120583L of assay diluent RD1-52 were dispensed intoeach well
ISRN Nephrology 3
(ii) 50 120583L of standards controls and samples were addedto each well
(iii) The plate was covered and incubated for 2 hours at 2ndash8∘C
(iv) Aspiration of each well was done and this was fol-lowed by a washing step which was repeated threetimes
(v) 200120583L of NGAL conjugate were added into each wellcovered with a new adhesive strip and incubated for 2hours at 2ndash8∘C
(vi) Aspirationwashing was repeated as in step (iii)
(vii) 200120583L of substrate solution were dispended into eachwell
(viii) Plate was covered and incubated for 30 minutes atroom temperature
(ix) 50 120583L of stop solution were added into each well
(x) Determination of the optical density of each wellwithin 30 minutes was done using a microplatereader set to 450 nm
Calculation of Results A standard curve was constructed byplotting themean absorbance for each standard on the 119910-axisagainst the concentration on the 119909-axis on log-log graph anda best fit line was drawn through the points on the graphConcentration of lipocaline-2 in each sample was determinedby finding the mean absorbance value of each one Fromthe 119910-axis of the standard curve graph a vertical line wasextended from this absorbance value to the standard curveAt the point of intersection a horizontal line was extended tothe 119909-axis and the corresponding concentration was read
3 Statistical Analysis
The data were tabulated and statistically analyzed usingStatistical Package for Social Sciences (SPSS Inc ChicagoIL USA) version 17 Comparison of continuous data wasperformed using student 119905-test and Mann-Whitney test fortwo groups while for more than two groups ANOVA testwas used ROC curves analysis (an efficient way to displaythe relationship between sensitivity (true positive rate) andspecificity (true negative rate) for tests with continuousoutcomes a point in the curve moves down and to the leftshowing lower sensitivity and high specificity while it movesup and to the right showing higher sensitivity and lowerspecificity) was used The cutoff value was selected from theROCcurve by choosing a point having the best sensitivity andconsiderable specificity 119875 value lt 005 was considered statis-tically significant Sensitivity is the proportion of true positivethat are correctly identified Specificity is the proportion oftrue negative that are correctly identified Positive predictiveValue (PPV) is probability of disease in a patient with anabnormal testNegative Predictive Value (NPV) is probabilityof a patient not having the disease when the test result isnegative
0 025 05 075 1
Sens
itivi
ty
ROC curve
0
025
05
075
1
1minus Specificity
Figure 1 Receiver operating characteristic curve of NGAL
4 Results
The routine Laboratory results in our studies subjects werepresented on Table 1 We found that range of NGAL at dayzero was (34ndash210) with median of 885 and at 3rd day was(34ndash550) with median 114 urea at day zero ranged from 15to 116 with median of 355 and at 3rd day ranged from 27to 310 with median of 415 while creatinine at zero day was(X1015840 plusmn SD = 068plusmn022) while at 3rd day (X1015840 plusmn SD 118plusmn108)So there were statistical significance between NGAL ureaand creatinine at day zero and 3rd day (119875 = 0000) as shownin Table 2
A significant increase between two groups with and with-out AKI regarding NGAL urea and creatinine at admissionand at 3rd day (119875 lt 005) was shown in Table 3
There was no statistical significance among the 3 groupsregarding NGAL at admission and urea at 3rd day (119875 = 024and 076 resp) However there was statistical significanceamong the 3 groups regarding NGAL at 3rd day urea atadmission and creatinine at admission and at 3rd day (119875 =007 001 0004 and 0000 resp) as presented in Table 4
Table 5 described that applying the receiver operatingcharacteristic (ROC) curve of NGAL to early detectionof AKI revealed area under the curve of 063 with 95confidence interval (CI) of 050ndash077 A cutoff of 895 ngmLwas chosen for early detection of AKI presented in Figure 1
NGAL acts as a sensitive marker rather than a specificone At the same time it presents a negative predictivevalue more valuable than being a positive predictive valuein detecting AKI We described in Table 6 that at cutoff of895 ngmL NGAL was positive at 11 out of 13 patients withAKI the sensitivity of NGAL in diagnosis of AKI was 846Howerver 28 out of 47 had truly absent AKI with specificity596 The positive predictive value (11(11 + 19)) was 367and the negative predictive value (28(2 + 28)) was 933
4 ISRN Nephrology
Table 1 Laboratory investigations of study groups regarding liver and kidney functions
Parameter Control119873 = 15 Patients119873 = 60 Test of significance 119875
Total bilirubin (mgdL)Median 04 05 125b 0210Range (03ndash08) (03ndash234)
Direct bilirubin (mgdL)Median 01 05 099b 0321Range (01ndash02) (01ndash129)
ALT (UL)Median 31 455 111b 026Range (12ndash42) (9ndash133)
AST (UL)Median 38 556 3007b 0003lowastRange (5ndash55) (18ndash1207)
Albumin (gdL)X1015840plusmn SD (3907 plusmn 0371) (336 plusmn 0618) 3245a 0002lowast
TP (gdL)X1015840plusmn SD (68 plusmn 0442) (57 plusmn 0868) 447a 0001lowast
Urea (mgdL)Median 258 355 342b 0001lowastRange (15ndash37) (15ndash116)
Creatinine (mgdL)X1015840plusmn SD 065 plusmn 022 068 plusmn 022 038a 069
WBCs (times103cmm) 121 (61ndash141) 131 (21ndash562) 064b 051Hb (gdL ) 125 (95ndash155) 105 (66ndash18) 626b 0001lowast
Platelet (times109cmm) 250 (180ndash340) 222 (35ndash1008) 049b 062NGAL-0 (ngmL) 54 (44ndash141) 885 (34ndash210) 247b 001lowast
Test of significance at-test bMann-Whiney test lowastsignificant
Table 2 Acute kidney injury (AKI) markers at admission (day 0)and after 3 days (3rd day) among patients group
Parameter Day zero 3rd day Wilcoxonrsquosrank sum test 119875
NGAL (ngmL)Median 885 144 628 0000lowastRange (34ndash210) (34ndash550)
Urea (mgdL)Median 355 415 601 0000lowastRange (15ndash116) (27ndash310)
Creatinine(mgdL)
X1015840plusmn SD 068 plusmn 022 118 plusmn 108 41 0000lowastlowast
Significant
5 Discussion
Acute kidney injury is a common and serious conditionand the diagnosis of which depends on serum creatinineurea which is a delayed and unreliable indicator of AKIFortunately understanding the early stress response of thekidney to acute injuries has revealed a number of potentialbiomarkers [7]
Neutrophil gelatinase-associated lipocalin is a small pro-tein of the lipocalin superfamily and is expressed by immunecells hepatocytes and renal tubular cells [8]
In particular NGAL is emerging as an excellent biomark-er in the urine and plasma for several processes such as earlyprediction of AKI monitoring clinical trials in AKI and forthe prognosis of AKI in several common clinical scenarios[7]
The aim of the present work was to assess serum levels ofNGAL in critically ill children affected byAKI and to evaluateits clinical significance in diagnosis as well as assessment ofdisease severity in comparison with other markers as serumcreatinine and urea ratio in critically ill children
We prospectively measured serumNGAL concentrationsduring day zero and after the 3rd day of admission to thePICU in 60 critically ill children (28 males and 32 females)and 15 healthy children (8 males and 7 females)
In our prospective study there were no statistical sig-nificant differences between controls and patients groupregarding demographic data including age and gender 119875 =015 and 119875 = 064 respectively
The liver function (total bilirubin direct bilirubin andALT) showed that there was no statistical significance dif-ference between critically ill children and control groupHowever there was a significant increase in the level of AST
ISRN Nephrology 5
Table 3 Serum NGAL urea and creatinine at day zero and 3rd day among 2 groups of patients AKI (group A) and NAKI (group B)
Parameters AKI Test of significance119875
Absent119873 = 47 Present119873 = 13NGAL-0 (ngmL)
Median 76 110 264b 0008lowastRange (34ndash200) (66ndash210)
NGAL-3 (ngmL)Median 105 280 332b 0001lowastRange (34ndash530) (92ndash550)
Urea-0 (mgdL)Median 345 425 204b 0040lowastRange (15ndash116) (287ndash788)
Urea-3 (mgdL)Median 38 1134 300b 0003lowastRange (18ndash310) (7ndash228)
Creatinine-0 (mgdL)X plusmn SD 061 plusmn 023 086 plusmn 023 34a 0001lowast
Creatinine-3 (mgdL)X plusmn SD 073 plusmn 063 208 plusmn 124 101a 0000lowast
Test of significance at-test bMann-Whiney test lowastsignificant
and significant decrease in the levels of albumin and totalprotein among the two groups
Regarding kidney function there was significant increasein the level of urea in patients group compared to controlgroup (119875 = 0000) However creatinine value increased incritically ill children group showing no statistical significancewith control group (119875 = 069)
This is in agreement with Bagshaw et al (2006) [3] whoreported that urea is not produced at a constant rate and therate can be influenced by extrarenal factors Urea productioncan be increased by diet critical illness burns traumagastro intestinal bleeding and sepsis Also in patients withdecreased circulating blood volume due to volume depletionor low cardiac output resorption of urea increases because ofthe relationship between urea levels and water conservationmechanisms Therefore urea can be influenced by multiplefactors and does not represent real-time changes in GFR
In the present study the level of serum NGAL con-centration for control group ranged from 44 to 141 ngmLwith median of 54 ngmL and critically ill children groupranged from 34 to 210 ngmL with median of 885 ngmLat admission There was significant increase in the level ofNGAL in the critically ill children group compared to controlgroup 119875 lt 001
These findings are in agreement with Bailey et al (2007)who reported that there was a significant difference in serumNGAL between healthy children and critically ill children [1]
Critically ill children who developed AKI (by doublingof serum creatinine from baseline according to RIFLEclassification) had significantly elevated serum NGAL ureaand creatinine levels at 3rd-day compared to serum NGALurea and creatinine at day zero Also critically ill childrenwho developed AKI had significantly elevated serum NGAL
urea and creatinine levels at day zero and at 3rd day whencompared with critically ill children who did not developAKI
This goes hand in hand with Mishra et al (2005) [8]and Wheeler et al (2008) [9] who demonstrated that serumNGAL concentrations within 24 hours of PICU admissionwere significantly increased in these children who developedAKI compared to children who did not develop AKI Asecond sample was obtained on the third day of admissionto the PICU and the difference between critically ill childrenwith AKI and critically ill children without AKI remainedsignificant (119875 lt 0001)
AKI developed in 13 out of 60 (217) critically ill childrenincluded in this studymdashall but 5 of these critically ill children(83) had a greater severity of illness and need to dialysisPatients who developed AKI and need to dialysis showedhigher level of NGAL at day 0 compared to patients whodeveloped AKI without need to dialysis and patients who didnot develop AKI but with no statistical significance whileat 3rd day it markedly increased (median = 350 ngmL) andbecame highly significant (119875 = 004)
These findings are in agreement with Hoste et al (2003)[10] who found that AKI developed in 32 out of 69 (463)critically ill childrenmdashall but 8 of these critically ill children(115) had a greater severity of illness and need to dialysis
In our study the receiver operating characteristic curveof NGAL for early detection of AKI revealed area under thecurve of 063 with 95 (CI of 050ndash077) At cutoff value of895 ngmL the sensitivity ofNGALwas 846 the specificitywas 596 positive predictive value was 367 and negativepredictive value was 684
Close results were found by Akcan-Arikan et al (2007)[2] who had shown that at cutoff of 139 ngmL the receiver
6 ISRN Nephrology
Table 4 Comparative study of patients group according to NGAL Urea and creatinine at admission (day zero) and 3rd day and theirclassification according to severity to 3 subgroups NAKI AKI minus D and AKI + D
Parameter NAKI AKI minus D AKI + D Test of significance 119875
119873 = 47 119873 = 8 119873 = 5
NGAL-0 (ngmL)Median 84 1005 120 137b 024Range (34ndash210) (74ndash115) (66ndash148)
NGAL-3 (ngmL)Median 105 184 350 308b 004lowastRange (34ndash530) (42ndash395) (150ndash550)
Urea-0 (mgdL)Median 345 38 65 591b 001lowastRange (15ndash116) (28ndash57) (425ndash788)
Urea-3 (mgdL)Median 38 841 1134 008b 076Range (18ndash310) (40ndash228) (7ndash178)
Creatinine-0 (mgdL)X plusmn SD 06 plusmn 023 08 plusmn 027 094 plusmn 015 119865 = 622 0004lowast
Creatinine-3 (mgdL)X plusmn SD 073 plusmn 036 225 plusmn 101 37 plusmn 11 119865 = 779 0000lowast
bMann-Whitney test 119865 Fisher test lowastsignificant
Table 5 Area under the receiver operating characteristic curve(ROC-AUC) and cutoff value for NGAL
Parameter ROC-AUC 95 CI CutoffNGAL-0 063 050ndash077 895 ngmL
Table 6 Validity of NGAL in prediction of AKI
Parameter AKI TotalPresent Absent
NGAL ge 895 11 19 30NGAL le 895 2 28 30Total 13 47 60
operating characteristic curve of NGAL revealed area underthe curve of 0677 with 95 (CI of 0557ndash0786)The sensitiv-ity of NGALwas 86 specificity was 39 positive predictivevalue was 39 and negative predictive value was 94
Our results of early predictive sensitive nonspecificserum NGAL although of clear statistical significance willcertainly need to be validated in a larger trial includingpatients with preexisting chronic kidney disease and comorbid conditions that normally accumulate with impairedrenal function The ability of biomarkers such as NGAL todiscern both the onset and resolution of AKI will furthervalidate their use in the clinical setting and greatly enhanceour understanding of AKI in the pediatric population
6 Conclusion
In conclusion we found that NGAL acts as a sensitivemarkerrather than a specific for one AKI At the same time it
presents a negative predictive value more valuable than beinga positive predictive value in detecting AKI
References
[1] D Bailey V Phan C Litalien et al ldquoRisk factors of acute renalfailure in critically ill children a prospective descriptive epi-demiological studyrdquo Pediatric Critical Care Medicine vol 8 no1 pp 29ndash35 2007
[2] A Akcan-Arikan M Zappitelli L L Loftis K K WashburnL S Jefferson and S L Goldstein ldquoModified RIFLE criteria incritically ill children with acute kidney injuryrdquo Kidney Interna-tional vol 71 no 10 pp 1028ndash1035 2007
[3] S M Bagshaw C Langenberg and R Bellomo ldquoUrinary bio-chemistry and microscopy in septic acute renal failure a sys-tematic reviewrdquo American Journal of Kidney Diseases vol 48no 5 pp 695ndash705 2006
[4] S M Moran and B D Myers ldquoCourse of acute renal failurestudied by a model of creatinine kineticsrdquo Kidney Internationalvol 27 no 6 pp 928ndash937 1985
[5] L Kjeldsen A H Johnsen H Sengelov and N BorregaardldquoIsolation and primary structure of NGAL a novel proteinassociated with human neutrophil gelatinaserdquo The Journal ofBiological Chemistry vol 268 no 14 pp 10425ndash10432 1993
[6] K Mori and K Nakao ldquoNeutrophil gelatinase-associated lipo-calin as the real-time indicator of active kidney damagerdquoKidneyInternational vol 71 no 10 pp 967ndash970 2007
[7] P Devarajan ldquoBiomarkers for the early detection of acutekidney injuryrdquo Current Opinion in Pediatrics vol 23 no 2 pp194ndash200 2011
[8] J Mishra C Dent R Tarabishi et al ldquoNeutrophil gelatinase-associated lipocalin (NGAL) as a biomarker for acute renalinjury after cardiac surgeryrdquoThe Lancet vol 365 no 9466 pp1231ndash1238 2005
ISRN Nephrology 7
[9] D S Wheeler P Devarajan Q Ma et al ldquoSerum neutrophilgelatinase-associated lipocalin (NGAL) as a marker of acutekidney injury in critically ill children with septic shockrdquoCriticalCare Medicine vol 36 no 4 pp 1297ndash1303 2008
[10] E A J Hoste N H Lameire R C Vanholder D D Benoit JM A Decruyenaere and F A Colardyn ldquoAcute renal failurein patients with sepsis in a surgical ICU predictive factorsincidence comorbidity and outcomerdquo Journal of the AmericanSociety of Nephrology vol 14 no 4 pp 1022ndash1030 2003
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

ISRN Nephrology 3
(ii) 50 120583L of standards controls and samples were addedto each well
(iii) The plate was covered and incubated for 2 hours at 2ndash8∘C
(iv) Aspiration of each well was done and this was fol-lowed by a washing step which was repeated threetimes
(v) 200120583L of NGAL conjugate were added into each wellcovered with a new adhesive strip and incubated for 2hours at 2ndash8∘C
(vi) Aspirationwashing was repeated as in step (iii)
(vii) 200120583L of substrate solution were dispended into eachwell
(viii) Plate was covered and incubated for 30 minutes atroom temperature
(ix) 50 120583L of stop solution were added into each well
(x) Determination of the optical density of each wellwithin 30 minutes was done using a microplatereader set to 450 nm
Calculation of Results A standard curve was constructed byplotting themean absorbance for each standard on the 119910-axisagainst the concentration on the 119909-axis on log-log graph anda best fit line was drawn through the points on the graphConcentration of lipocaline-2 in each sample was determinedby finding the mean absorbance value of each one Fromthe 119910-axis of the standard curve graph a vertical line wasextended from this absorbance value to the standard curveAt the point of intersection a horizontal line was extended tothe 119909-axis and the corresponding concentration was read
3 Statistical Analysis
The data were tabulated and statistically analyzed usingStatistical Package for Social Sciences (SPSS Inc ChicagoIL USA) version 17 Comparison of continuous data wasperformed using student 119905-test and Mann-Whitney test fortwo groups while for more than two groups ANOVA testwas used ROC curves analysis (an efficient way to displaythe relationship between sensitivity (true positive rate) andspecificity (true negative rate) for tests with continuousoutcomes a point in the curve moves down and to the leftshowing lower sensitivity and high specificity while it movesup and to the right showing higher sensitivity and lowerspecificity) was used The cutoff value was selected from theROCcurve by choosing a point having the best sensitivity andconsiderable specificity 119875 value lt 005 was considered statis-tically significant Sensitivity is the proportion of true positivethat are correctly identified Specificity is the proportion oftrue negative that are correctly identified Positive predictiveValue (PPV) is probability of disease in a patient with anabnormal testNegative Predictive Value (NPV) is probabilityof a patient not having the disease when the test result isnegative
0 025 05 075 1
Sens
itivi
ty
ROC curve
0
025
05
075
1
1minus Specificity
Figure 1 Receiver operating characteristic curve of NGAL
4 Results
The routine Laboratory results in our studies subjects werepresented on Table 1 We found that range of NGAL at dayzero was (34ndash210) with median of 885 and at 3rd day was(34ndash550) with median 114 urea at day zero ranged from 15to 116 with median of 355 and at 3rd day ranged from 27to 310 with median of 415 while creatinine at zero day was(X1015840 plusmn SD = 068plusmn022) while at 3rd day (X1015840 plusmn SD 118plusmn108)So there were statistical significance between NGAL ureaand creatinine at day zero and 3rd day (119875 = 0000) as shownin Table 2
A significant increase between two groups with and with-out AKI regarding NGAL urea and creatinine at admissionand at 3rd day (119875 lt 005) was shown in Table 3
There was no statistical significance among the 3 groupsregarding NGAL at admission and urea at 3rd day (119875 = 024and 076 resp) However there was statistical significanceamong the 3 groups regarding NGAL at 3rd day urea atadmission and creatinine at admission and at 3rd day (119875 =007 001 0004 and 0000 resp) as presented in Table 4
Table 5 described that applying the receiver operatingcharacteristic (ROC) curve of NGAL to early detectionof AKI revealed area under the curve of 063 with 95confidence interval (CI) of 050ndash077 A cutoff of 895 ngmLwas chosen for early detection of AKI presented in Figure 1
NGAL acts as a sensitive marker rather than a specificone At the same time it presents a negative predictivevalue more valuable than being a positive predictive valuein detecting AKI We described in Table 6 that at cutoff of895 ngmL NGAL was positive at 11 out of 13 patients withAKI the sensitivity of NGAL in diagnosis of AKI was 846Howerver 28 out of 47 had truly absent AKI with specificity596 The positive predictive value (11(11 + 19)) was 367and the negative predictive value (28(2 + 28)) was 933
4 ISRN Nephrology
Table 1 Laboratory investigations of study groups regarding liver and kidney functions
Parameter Control119873 = 15 Patients119873 = 60 Test of significance 119875
Total bilirubin (mgdL)Median 04 05 125b 0210Range (03ndash08) (03ndash234)
Direct bilirubin (mgdL)Median 01 05 099b 0321Range (01ndash02) (01ndash129)
ALT (UL)Median 31 455 111b 026Range (12ndash42) (9ndash133)
AST (UL)Median 38 556 3007b 0003lowastRange (5ndash55) (18ndash1207)
Albumin (gdL)X1015840plusmn SD (3907 plusmn 0371) (336 plusmn 0618) 3245a 0002lowast
TP (gdL)X1015840plusmn SD (68 plusmn 0442) (57 plusmn 0868) 447a 0001lowast
Urea (mgdL)Median 258 355 342b 0001lowastRange (15ndash37) (15ndash116)
Creatinine (mgdL)X1015840plusmn SD 065 plusmn 022 068 plusmn 022 038a 069
WBCs (times103cmm) 121 (61ndash141) 131 (21ndash562) 064b 051Hb (gdL ) 125 (95ndash155) 105 (66ndash18) 626b 0001lowast
Platelet (times109cmm) 250 (180ndash340) 222 (35ndash1008) 049b 062NGAL-0 (ngmL) 54 (44ndash141) 885 (34ndash210) 247b 001lowast
Test of significance at-test bMann-Whiney test lowastsignificant
Table 2 Acute kidney injury (AKI) markers at admission (day 0)and after 3 days (3rd day) among patients group
Parameter Day zero 3rd day Wilcoxonrsquosrank sum test 119875
NGAL (ngmL)Median 885 144 628 0000lowastRange (34ndash210) (34ndash550)
Urea (mgdL)Median 355 415 601 0000lowastRange (15ndash116) (27ndash310)
Creatinine(mgdL)
X1015840plusmn SD 068 plusmn 022 118 plusmn 108 41 0000lowastlowast
Significant
5 Discussion
Acute kidney injury is a common and serious conditionand the diagnosis of which depends on serum creatinineurea which is a delayed and unreliable indicator of AKIFortunately understanding the early stress response of thekidney to acute injuries has revealed a number of potentialbiomarkers [7]
Neutrophil gelatinase-associated lipocalin is a small pro-tein of the lipocalin superfamily and is expressed by immunecells hepatocytes and renal tubular cells [8]
In particular NGAL is emerging as an excellent biomark-er in the urine and plasma for several processes such as earlyprediction of AKI monitoring clinical trials in AKI and forthe prognosis of AKI in several common clinical scenarios[7]
The aim of the present work was to assess serum levels ofNGAL in critically ill children affected byAKI and to evaluateits clinical significance in diagnosis as well as assessment ofdisease severity in comparison with other markers as serumcreatinine and urea ratio in critically ill children
We prospectively measured serumNGAL concentrationsduring day zero and after the 3rd day of admission to thePICU in 60 critically ill children (28 males and 32 females)and 15 healthy children (8 males and 7 females)
In our prospective study there were no statistical sig-nificant differences between controls and patients groupregarding demographic data including age and gender 119875 =015 and 119875 = 064 respectively
The liver function (total bilirubin direct bilirubin andALT) showed that there was no statistical significance dif-ference between critically ill children and control groupHowever there was a significant increase in the level of AST
ISRN Nephrology 5
Table 3 Serum NGAL urea and creatinine at day zero and 3rd day among 2 groups of patients AKI (group A) and NAKI (group B)
Parameters AKI Test of significance119875
Absent119873 = 47 Present119873 = 13NGAL-0 (ngmL)
Median 76 110 264b 0008lowastRange (34ndash200) (66ndash210)
NGAL-3 (ngmL)Median 105 280 332b 0001lowastRange (34ndash530) (92ndash550)
Urea-0 (mgdL)Median 345 425 204b 0040lowastRange (15ndash116) (287ndash788)
Urea-3 (mgdL)Median 38 1134 300b 0003lowastRange (18ndash310) (7ndash228)
Creatinine-0 (mgdL)X plusmn SD 061 plusmn 023 086 plusmn 023 34a 0001lowast
Creatinine-3 (mgdL)X plusmn SD 073 plusmn 063 208 plusmn 124 101a 0000lowast
Test of significance at-test bMann-Whiney test lowastsignificant
and significant decrease in the levels of albumin and totalprotein among the two groups
Regarding kidney function there was significant increasein the level of urea in patients group compared to controlgroup (119875 = 0000) However creatinine value increased incritically ill children group showing no statistical significancewith control group (119875 = 069)
This is in agreement with Bagshaw et al (2006) [3] whoreported that urea is not produced at a constant rate and therate can be influenced by extrarenal factors Urea productioncan be increased by diet critical illness burns traumagastro intestinal bleeding and sepsis Also in patients withdecreased circulating blood volume due to volume depletionor low cardiac output resorption of urea increases because ofthe relationship between urea levels and water conservationmechanisms Therefore urea can be influenced by multiplefactors and does not represent real-time changes in GFR
In the present study the level of serum NGAL con-centration for control group ranged from 44 to 141 ngmLwith median of 54 ngmL and critically ill children groupranged from 34 to 210 ngmL with median of 885 ngmLat admission There was significant increase in the level ofNGAL in the critically ill children group compared to controlgroup 119875 lt 001
These findings are in agreement with Bailey et al (2007)who reported that there was a significant difference in serumNGAL between healthy children and critically ill children [1]
Critically ill children who developed AKI (by doublingof serum creatinine from baseline according to RIFLEclassification) had significantly elevated serum NGAL ureaand creatinine levels at 3rd-day compared to serum NGALurea and creatinine at day zero Also critically ill childrenwho developed AKI had significantly elevated serum NGAL
urea and creatinine levels at day zero and at 3rd day whencompared with critically ill children who did not developAKI
This goes hand in hand with Mishra et al (2005) [8]and Wheeler et al (2008) [9] who demonstrated that serumNGAL concentrations within 24 hours of PICU admissionwere significantly increased in these children who developedAKI compared to children who did not develop AKI Asecond sample was obtained on the third day of admissionto the PICU and the difference between critically ill childrenwith AKI and critically ill children without AKI remainedsignificant (119875 lt 0001)
AKI developed in 13 out of 60 (217) critically ill childrenincluded in this studymdashall but 5 of these critically ill children(83) had a greater severity of illness and need to dialysisPatients who developed AKI and need to dialysis showedhigher level of NGAL at day 0 compared to patients whodeveloped AKI without need to dialysis and patients who didnot develop AKI but with no statistical significance whileat 3rd day it markedly increased (median = 350 ngmL) andbecame highly significant (119875 = 004)
These findings are in agreement with Hoste et al (2003)[10] who found that AKI developed in 32 out of 69 (463)critically ill childrenmdashall but 8 of these critically ill children(115) had a greater severity of illness and need to dialysis
In our study the receiver operating characteristic curveof NGAL for early detection of AKI revealed area under thecurve of 063 with 95 (CI of 050ndash077) At cutoff value of895 ngmL the sensitivity ofNGALwas 846 the specificitywas 596 positive predictive value was 367 and negativepredictive value was 684
Close results were found by Akcan-Arikan et al (2007)[2] who had shown that at cutoff of 139 ngmL the receiver
6 ISRN Nephrology
Table 4 Comparative study of patients group according to NGAL Urea and creatinine at admission (day zero) and 3rd day and theirclassification according to severity to 3 subgroups NAKI AKI minus D and AKI + D
Parameter NAKI AKI minus D AKI + D Test of significance 119875
119873 = 47 119873 = 8 119873 = 5
NGAL-0 (ngmL)Median 84 1005 120 137b 024Range (34ndash210) (74ndash115) (66ndash148)
NGAL-3 (ngmL)Median 105 184 350 308b 004lowastRange (34ndash530) (42ndash395) (150ndash550)
Urea-0 (mgdL)Median 345 38 65 591b 001lowastRange (15ndash116) (28ndash57) (425ndash788)
Urea-3 (mgdL)Median 38 841 1134 008b 076Range (18ndash310) (40ndash228) (7ndash178)
Creatinine-0 (mgdL)X plusmn SD 06 plusmn 023 08 plusmn 027 094 plusmn 015 119865 = 622 0004lowast
Creatinine-3 (mgdL)X plusmn SD 073 plusmn 036 225 plusmn 101 37 plusmn 11 119865 = 779 0000lowast
bMann-Whitney test 119865 Fisher test lowastsignificant
Table 5 Area under the receiver operating characteristic curve(ROC-AUC) and cutoff value for NGAL
Parameter ROC-AUC 95 CI CutoffNGAL-0 063 050ndash077 895 ngmL
Table 6 Validity of NGAL in prediction of AKI
Parameter AKI TotalPresent Absent
NGAL ge 895 11 19 30NGAL le 895 2 28 30Total 13 47 60
operating characteristic curve of NGAL revealed area underthe curve of 0677 with 95 (CI of 0557ndash0786)The sensitiv-ity of NGALwas 86 specificity was 39 positive predictivevalue was 39 and negative predictive value was 94
Our results of early predictive sensitive nonspecificserum NGAL although of clear statistical significance willcertainly need to be validated in a larger trial includingpatients with preexisting chronic kidney disease and comorbid conditions that normally accumulate with impairedrenal function The ability of biomarkers such as NGAL todiscern both the onset and resolution of AKI will furthervalidate their use in the clinical setting and greatly enhanceour understanding of AKI in the pediatric population
6 Conclusion
In conclusion we found that NGAL acts as a sensitivemarkerrather than a specific for one AKI At the same time it
presents a negative predictive value more valuable than beinga positive predictive value in detecting AKI
References
[1] D Bailey V Phan C Litalien et al ldquoRisk factors of acute renalfailure in critically ill children a prospective descriptive epi-demiological studyrdquo Pediatric Critical Care Medicine vol 8 no1 pp 29ndash35 2007
[2] A Akcan-Arikan M Zappitelli L L Loftis K K WashburnL S Jefferson and S L Goldstein ldquoModified RIFLE criteria incritically ill children with acute kidney injuryrdquo Kidney Interna-tional vol 71 no 10 pp 1028ndash1035 2007
[3] S M Bagshaw C Langenberg and R Bellomo ldquoUrinary bio-chemistry and microscopy in septic acute renal failure a sys-tematic reviewrdquo American Journal of Kidney Diseases vol 48no 5 pp 695ndash705 2006
[4] S M Moran and B D Myers ldquoCourse of acute renal failurestudied by a model of creatinine kineticsrdquo Kidney Internationalvol 27 no 6 pp 928ndash937 1985
[5] L Kjeldsen A H Johnsen H Sengelov and N BorregaardldquoIsolation and primary structure of NGAL a novel proteinassociated with human neutrophil gelatinaserdquo The Journal ofBiological Chemistry vol 268 no 14 pp 10425ndash10432 1993
[6] K Mori and K Nakao ldquoNeutrophil gelatinase-associated lipo-calin as the real-time indicator of active kidney damagerdquoKidneyInternational vol 71 no 10 pp 967ndash970 2007
[7] P Devarajan ldquoBiomarkers for the early detection of acutekidney injuryrdquo Current Opinion in Pediatrics vol 23 no 2 pp194ndash200 2011
[8] J Mishra C Dent R Tarabishi et al ldquoNeutrophil gelatinase-associated lipocalin (NGAL) as a biomarker for acute renalinjury after cardiac surgeryrdquoThe Lancet vol 365 no 9466 pp1231ndash1238 2005
ISRN Nephrology 7
[9] D S Wheeler P Devarajan Q Ma et al ldquoSerum neutrophilgelatinase-associated lipocalin (NGAL) as a marker of acutekidney injury in critically ill children with septic shockrdquoCriticalCare Medicine vol 36 no 4 pp 1297ndash1303 2008
[10] E A J Hoste N H Lameire R C Vanholder D D Benoit JM A Decruyenaere and F A Colardyn ldquoAcute renal failurein patients with sepsis in a surgical ICU predictive factorsincidence comorbidity and outcomerdquo Journal of the AmericanSociety of Nephrology vol 14 no 4 pp 1022ndash1030 2003
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 ISRN Nephrology
Table 1 Laboratory investigations of study groups regarding liver and kidney functions
Parameter Control119873 = 15 Patients119873 = 60 Test of significance 119875
Total bilirubin (mgdL)Median 04 05 125b 0210Range (03ndash08) (03ndash234)
Direct bilirubin (mgdL)Median 01 05 099b 0321Range (01ndash02) (01ndash129)
ALT (UL)Median 31 455 111b 026Range (12ndash42) (9ndash133)
AST (UL)Median 38 556 3007b 0003lowastRange (5ndash55) (18ndash1207)
Albumin (gdL)X1015840plusmn SD (3907 plusmn 0371) (336 plusmn 0618) 3245a 0002lowast
TP (gdL)X1015840plusmn SD (68 plusmn 0442) (57 plusmn 0868) 447a 0001lowast
Urea (mgdL)Median 258 355 342b 0001lowastRange (15ndash37) (15ndash116)
Creatinine (mgdL)X1015840plusmn SD 065 plusmn 022 068 plusmn 022 038a 069
WBCs (times103cmm) 121 (61ndash141) 131 (21ndash562) 064b 051Hb (gdL ) 125 (95ndash155) 105 (66ndash18) 626b 0001lowast
Platelet (times109cmm) 250 (180ndash340) 222 (35ndash1008) 049b 062NGAL-0 (ngmL) 54 (44ndash141) 885 (34ndash210) 247b 001lowast
Test of significance at-test bMann-Whiney test lowastsignificant
Table 2 Acute kidney injury (AKI) markers at admission (day 0)and after 3 days (3rd day) among patients group
Parameter Day zero 3rd day Wilcoxonrsquosrank sum test 119875
NGAL (ngmL)Median 885 144 628 0000lowastRange (34ndash210) (34ndash550)
Urea (mgdL)Median 355 415 601 0000lowastRange (15ndash116) (27ndash310)
Creatinine(mgdL)
X1015840plusmn SD 068 plusmn 022 118 plusmn 108 41 0000lowastlowast
Significant
5 Discussion
Acute kidney injury is a common and serious conditionand the diagnosis of which depends on serum creatinineurea which is a delayed and unreliable indicator of AKIFortunately understanding the early stress response of thekidney to acute injuries has revealed a number of potentialbiomarkers [7]
Neutrophil gelatinase-associated lipocalin is a small pro-tein of the lipocalin superfamily and is expressed by immunecells hepatocytes and renal tubular cells [8]
In particular NGAL is emerging as an excellent biomark-er in the urine and plasma for several processes such as earlyprediction of AKI monitoring clinical trials in AKI and forthe prognosis of AKI in several common clinical scenarios[7]
The aim of the present work was to assess serum levels ofNGAL in critically ill children affected byAKI and to evaluateits clinical significance in diagnosis as well as assessment ofdisease severity in comparison with other markers as serumcreatinine and urea ratio in critically ill children
We prospectively measured serumNGAL concentrationsduring day zero and after the 3rd day of admission to thePICU in 60 critically ill children (28 males and 32 females)and 15 healthy children (8 males and 7 females)
In our prospective study there were no statistical sig-nificant differences between controls and patients groupregarding demographic data including age and gender 119875 =015 and 119875 = 064 respectively
The liver function (total bilirubin direct bilirubin andALT) showed that there was no statistical significance dif-ference between critically ill children and control groupHowever there was a significant increase in the level of AST
ISRN Nephrology 5
Table 3 Serum NGAL urea and creatinine at day zero and 3rd day among 2 groups of patients AKI (group A) and NAKI (group B)
Parameters AKI Test of significance119875
Absent119873 = 47 Present119873 = 13NGAL-0 (ngmL)
Median 76 110 264b 0008lowastRange (34ndash200) (66ndash210)
NGAL-3 (ngmL)Median 105 280 332b 0001lowastRange (34ndash530) (92ndash550)
Urea-0 (mgdL)Median 345 425 204b 0040lowastRange (15ndash116) (287ndash788)
Urea-3 (mgdL)Median 38 1134 300b 0003lowastRange (18ndash310) (7ndash228)
Creatinine-0 (mgdL)X plusmn SD 061 plusmn 023 086 plusmn 023 34a 0001lowast
Creatinine-3 (mgdL)X plusmn SD 073 plusmn 063 208 plusmn 124 101a 0000lowast
Test of significance at-test bMann-Whiney test lowastsignificant
and significant decrease in the levels of albumin and totalprotein among the two groups
Regarding kidney function there was significant increasein the level of urea in patients group compared to controlgroup (119875 = 0000) However creatinine value increased incritically ill children group showing no statistical significancewith control group (119875 = 069)
This is in agreement with Bagshaw et al (2006) [3] whoreported that urea is not produced at a constant rate and therate can be influenced by extrarenal factors Urea productioncan be increased by diet critical illness burns traumagastro intestinal bleeding and sepsis Also in patients withdecreased circulating blood volume due to volume depletionor low cardiac output resorption of urea increases because ofthe relationship between urea levels and water conservationmechanisms Therefore urea can be influenced by multiplefactors and does not represent real-time changes in GFR
In the present study the level of serum NGAL con-centration for control group ranged from 44 to 141 ngmLwith median of 54 ngmL and critically ill children groupranged from 34 to 210 ngmL with median of 885 ngmLat admission There was significant increase in the level ofNGAL in the critically ill children group compared to controlgroup 119875 lt 001
These findings are in agreement with Bailey et al (2007)who reported that there was a significant difference in serumNGAL between healthy children and critically ill children [1]
Critically ill children who developed AKI (by doublingof serum creatinine from baseline according to RIFLEclassification) had significantly elevated serum NGAL ureaand creatinine levels at 3rd-day compared to serum NGALurea and creatinine at day zero Also critically ill childrenwho developed AKI had significantly elevated serum NGAL
urea and creatinine levels at day zero and at 3rd day whencompared with critically ill children who did not developAKI
This goes hand in hand with Mishra et al (2005) [8]and Wheeler et al (2008) [9] who demonstrated that serumNGAL concentrations within 24 hours of PICU admissionwere significantly increased in these children who developedAKI compared to children who did not develop AKI Asecond sample was obtained on the third day of admissionto the PICU and the difference between critically ill childrenwith AKI and critically ill children without AKI remainedsignificant (119875 lt 0001)
AKI developed in 13 out of 60 (217) critically ill childrenincluded in this studymdashall but 5 of these critically ill children(83) had a greater severity of illness and need to dialysisPatients who developed AKI and need to dialysis showedhigher level of NGAL at day 0 compared to patients whodeveloped AKI without need to dialysis and patients who didnot develop AKI but with no statistical significance whileat 3rd day it markedly increased (median = 350 ngmL) andbecame highly significant (119875 = 004)
These findings are in agreement with Hoste et al (2003)[10] who found that AKI developed in 32 out of 69 (463)critically ill childrenmdashall but 8 of these critically ill children(115) had a greater severity of illness and need to dialysis
In our study the receiver operating characteristic curveof NGAL for early detection of AKI revealed area under thecurve of 063 with 95 (CI of 050ndash077) At cutoff value of895 ngmL the sensitivity ofNGALwas 846 the specificitywas 596 positive predictive value was 367 and negativepredictive value was 684
Close results were found by Akcan-Arikan et al (2007)[2] who had shown that at cutoff of 139 ngmL the receiver
6 ISRN Nephrology
Table 4 Comparative study of patients group according to NGAL Urea and creatinine at admission (day zero) and 3rd day and theirclassification according to severity to 3 subgroups NAKI AKI minus D and AKI + D
Parameter NAKI AKI minus D AKI + D Test of significance 119875
119873 = 47 119873 = 8 119873 = 5
NGAL-0 (ngmL)Median 84 1005 120 137b 024Range (34ndash210) (74ndash115) (66ndash148)
NGAL-3 (ngmL)Median 105 184 350 308b 004lowastRange (34ndash530) (42ndash395) (150ndash550)
Urea-0 (mgdL)Median 345 38 65 591b 001lowastRange (15ndash116) (28ndash57) (425ndash788)
Urea-3 (mgdL)Median 38 841 1134 008b 076Range (18ndash310) (40ndash228) (7ndash178)
Creatinine-0 (mgdL)X plusmn SD 06 plusmn 023 08 plusmn 027 094 plusmn 015 119865 = 622 0004lowast
Creatinine-3 (mgdL)X plusmn SD 073 plusmn 036 225 plusmn 101 37 plusmn 11 119865 = 779 0000lowast
bMann-Whitney test 119865 Fisher test lowastsignificant
Table 5 Area under the receiver operating characteristic curve(ROC-AUC) and cutoff value for NGAL
Parameter ROC-AUC 95 CI CutoffNGAL-0 063 050ndash077 895 ngmL
Table 6 Validity of NGAL in prediction of AKI
Parameter AKI TotalPresent Absent
NGAL ge 895 11 19 30NGAL le 895 2 28 30Total 13 47 60
operating characteristic curve of NGAL revealed area underthe curve of 0677 with 95 (CI of 0557ndash0786)The sensitiv-ity of NGALwas 86 specificity was 39 positive predictivevalue was 39 and negative predictive value was 94
Our results of early predictive sensitive nonspecificserum NGAL although of clear statistical significance willcertainly need to be validated in a larger trial includingpatients with preexisting chronic kidney disease and comorbid conditions that normally accumulate with impairedrenal function The ability of biomarkers such as NGAL todiscern both the onset and resolution of AKI will furthervalidate their use in the clinical setting and greatly enhanceour understanding of AKI in the pediatric population
6 Conclusion
In conclusion we found that NGAL acts as a sensitivemarkerrather than a specific for one AKI At the same time it
presents a negative predictive value more valuable than beinga positive predictive value in detecting AKI
References
[1] D Bailey V Phan C Litalien et al ldquoRisk factors of acute renalfailure in critically ill children a prospective descriptive epi-demiological studyrdquo Pediatric Critical Care Medicine vol 8 no1 pp 29ndash35 2007
[2] A Akcan-Arikan M Zappitelli L L Loftis K K WashburnL S Jefferson and S L Goldstein ldquoModified RIFLE criteria incritically ill children with acute kidney injuryrdquo Kidney Interna-tional vol 71 no 10 pp 1028ndash1035 2007
[3] S M Bagshaw C Langenberg and R Bellomo ldquoUrinary bio-chemistry and microscopy in septic acute renal failure a sys-tematic reviewrdquo American Journal of Kidney Diseases vol 48no 5 pp 695ndash705 2006
[4] S M Moran and B D Myers ldquoCourse of acute renal failurestudied by a model of creatinine kineticsrdquo Kidney Internationalvol 27 no 6 pp 928ndash937 1985
[5] L Kjeldsen A H Johnsen H Sengelov and N BorregaardldquoIsolation and primary structure of NGAL a novel proteinassociated with human neutrophil gelatinaserdquo The Journal ofBiological Chemistry vol 268 no 14 pp 10425ndash10432 1993
[6] K Mori and K Nakao ldquoNeutrophil gelatinase-associated lipo-calin as the real-time indicator of active kidney damagerdquoKidneyInternational vol 71 no 10 pp 967ndash970 2007
[7] P Devarajan ldquoBiomarkers for the early detection of acutekidney injuryrdquo Current Opinion in Pediatrics vol 23 no 2 pp194ndash200 2011
[8] J Mishra C Dent R Tarabishi et al ldquoNeutrophil gelatinase-associated lipocalin (NGAL) as a biomarker for acute renalinjury after cardiac surgeryrdquoThe Lancet vol 365 no 9466 pp1231ndash1238 2005
ISRN Nephrology 7
[9] D S Wheeler P Devarajan Q Ma et al ldquoSerum neutrophilgelatinase-associated lipocalin (NGAL) as a marker of acutekidney injury in critically ill children with septic shockrdquoCriticalCare Medicine vol 36 no 4 pp 1297ndash1303 2008
[10] E A J Hoste N H Lameire R C Vanholder D D Benoit JM A Decruyenaere and F A Colardyn ldquoAcute renal failurein patients with sepsis in a surgical ICU predictive factorsincidence comorbidity and outcomerdquo Journal of the AmericanSociety of Nephrology vol 14 no 4 pp 1022ndash1030 2003
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

ISRN Nephrology 5
Table 3 Serum NGAL urea and creatinine at day zero and 3rd day among 2 groups of patients AKI (group A) and NAKI (group B)
Parameters AKI Test of significance119875
Absent119873 = 47 Present119873 = 13NGAL-0 (ngmL)
Median 76 110 264b 0008lowastRange (34ndash200) (66ndash210)
NGAL-3 (ngmL)Median 105 280 332b 0001lowastRange (34ndash530) (92ndash550)
Urea-0 (mgdL)Median 345 425 204b 0040lowastRange (15ndash116) (287ndash788)
Urea-3 (mgdL)Median 38 1134 300b 0003lowastRange (18ndash310) (7ndash228)
Creatinine-0 (mgdL)X plusmn SD 061 plusmn 023 086 plusmn 023 34a 0001lowast
Creatinine-3 (mgdL)X plusmn SD 073 plusmn 063 208 plusmn 124 101a 0000lowast
Test of significance at-test bMann-Whiney test lowastsignificant
and significant decrease in the levels of albumin and totalprotein among the two groups
Regarding kidney function there was significant increasein the level of urea in patients group compared to controlgroup (119875 = 0000) However creatinine value increased incritically ill children group showing no statistical significancewith control group (119875 = 069)
This is in agreement with Bagshaw et al (2006) [3] whoreported that urea is not produced at a constant rate and therate can be influenced by extrarenal factors Urea productioncan be increased by diet critical illness burns traumagastro intestinal bleeding and sepsis Also in patients withdecreased circulating blood volume due to volume depletionor low cardiac output resorption of urea increases because ofthe relationship between urea levels and water conservationmechanisms Therefore urea can be influenced by multiplefactors and does not represent real-time changes in GFR
In the present study the level of serum NGAL con-centration for control group ranged from 44 to 141 ngmLwith median of 54 ngmL and critically ill children groupranged from 34 to 210 ngmL with median of 885 ngmLat admission There was significant increase in the level ofNGAL in the critically ill children group compared to controlgroup 119875 lt 001
These findings are in agreement with Bailey et al (2007)who reported that there was a significant difference in serumNGAL between healthy children and critically ill children [1]
Critically ill children who developed AKI (by doublingof serum creatinine from baseline according to RIFLEclassification) had significantly elevated serum NGAL ureaand creatinine levels at 3rd-day compared to serum NGALurea and creatinine at day zero Also critically ill childrenwho developed AKI had significantly elevated serum NGAL
urea and creatinine levels at day zero and at 3rd day whencompared with critically ill children who did not developAKI
This goes hand in hand with Mishra et al (2005) [8]and Wheeler et al (2008) [9] who demonstrated that serumNGAL concentrations within 24 hours of PICU admissionwere significantly increased in these children who developedAKI compared to children who did not develop AKI Asecond sample was obtained on the third day of admissionto the PICU and the difference between critically ill childrenwith AKI and critically ill children without AKI remainedsignificant (119875 lt 0001)
AKI developed in 13 out of 60 (217) critically ill childrenincluded in this studymdashall but 5 of these critically ill children(83) had a greater severity of illness and need to dialysisPatients who developed AKI and need to dialysis showedhigher level of NGAL at day 0 compared to patients whodeveloped AKI without need to dialysis and patients who didnot develop AKI but with no statistical significance whileat 3rd day it markedly increased (median = 350 ngmL) andbecame highly significant (119875 = 004)
These findings are in agreement with Hoste et al (2003)[10] who found that AKI developed in 32 out of 69 (463)critically ill childrenmdashall but 8 of these critically ill children(115) had a greater severity of illness and need to dialysis
In our study the receiver operating characteristic curveof NGAL for early detection of AKI revealed area under thecurve of 063 with 95 (CI of 050ndash077) At cutoff value of895 ngmL the sensitivity ofNGALwas 846 the specificitywas 596 positive predictive value was 367 and negativepredictive value was 684
Close results were found by Akcan-Arikan et al (2007)[2] who had shown that at cutoff of 139 ngmL the receiver
6 ISRN Nephrology
Table 4 Comparative study of patients group according to NGAL Urea and creatinine at admission (day zero) and 3rd day and theirclassification according to severity to 3 subgroups NAKI AKI minus D and AKI + D
Parameter NAKI AKI minus D AKI + D Test of significance 119875
119873 = 47 119873 = 8 119873 = 5
NGAL-0 (ngmL)Median 84 1005 120 137b 024Range (34ndash210) (74ndash115) (66ndash148)
NGAL-3 (ngmL)Median 105 184 350 308b 004lowastRange (34ndash530) (42ndash395) (150ndash550)
Urea-0 (mgdL)Median 345 38 65 591b 001lowastRange (15ndash116) (28ndash57) (425ndash788)
Urea-3 (mgdL)Median 38 841 1134 008b 076Range (18ndash310) (40ndash228) (7ndash178)
Creatinine-0 (mgdL)X plusmn SD 06 plusmn 023 08 plusmn 027 094 plusmn 015 119865 = 622 0004lowast
Creatinine-3 (mgdL)X plusmn SD 073 plusmn 036 225 plusmn 101 37 plusmn 11 119865 = 779 0000lowast
bMann-Whitney test 119865 Fisher test lowastsignificant
Table 5 Area under the receiver operating characteristic curve(ROC-AUC) and cutoff value for NGAL
Parameter ROC-AUC 95 CI CutoffNGAL-0 063 050ndash077 895 ngmL
Table 6 Validity of NGAL in prediction of AKI
Parameter AKI TotalPresent Absent
NGAL ge 895 11 19 30NGAL le 895 2 28 30Total 13 47 60
operating characteristic curve of NGAL revealed area underthe curve of 0677 with 95 (CI of 0557ndash0786)The sensitiv-ity of NGALwas 86 specificity was 39 positive predictivevalue was 39 and negative predictive value was 94
Our results of early predictive sensitive nonspecificserum NGAL although of clear statistical significance willcertainly need to be validated in a larger trial includingpatients with preexisting chronic kidney disease and comorbid conditions that normally accumulate with impairedrenal function The ability of biomarkers such as NGAL todiscern both the onset and resolution of AKI will furthervalidate their use in the clinical setting and greatly enhanceour understanding of AKI in the pediatric population
6 Conclusion
In conclusion we found that NGAL acts as a sensitivemarkerrather than a specific for one AKI At the same time it
presents a negative predictive value more valuable than beinga positive predictive value in detecting AKI
References
[1] D Bailey V Phan C Litalien et al ldquoRisk factors of acute renalfailure in critically ill children a prospective descriptive epi-demiological studyrdquo Pediatric Critical Care Medicine vol 8 no1 pp 29ndash35 2007
[2] A Akcan-Arikan M Zappitelli L L Loftis K K WashburnL S Jefferson and S L Goldstein ldquoModified RIFLE criteria incritically ill children with acute kidney injuryrdquo Kidney Interna-tional vol 71 no 10 pp 1028ndash1035 2007
[3] S M Bagshaw C Langenberg and R Bellomo ldquoUrinary bio-chemistry and microscopy in septic acute renal failure a sys-tematic reviewrdquo American Journal of Kidney Diseases vol 48no 5 pp 695ndash705 2006
[4] S M Moran and B D Myers ldquoCourse of acute renal failurestudied by a model of creatinine kineticsrdquo Kidney Internationalvol 27 no 6 pp 928ndash937 1985
[5] L Kjeldsen A H Johnsen H Sengelov and N BorregaardldquoIsolation and primary structure of NGAL a novel proteinassociated with human neutrophil gelatinaserdquo The Journal ofBiological Chemistry vol 268 no 14 pp 10425ndash10432 1993
[6] K Mori and K Nakao ldquoNeutrophil gelatinase-associated lipo-calin as the real-time indicator of active kidney damagerdquoKidneyInternational vol 71 no 10 pp 967ndash970 2007
[7] P Devarajan ldquoBiomarkers for the early detection of acutekidney injuryrdquo Current Opinion in Pediatrics vol 23 no 2 pp194ndash200 2011
[8] J Mishra C Dent R Tarabishi et al ldquoNeutrophil gelatinase-associated lipocalin (NGAL) as a biomarker for acute renalinjury after cardiac surgeryrdquoThe Lancet vol 365 no 9466 pp1231ndash1238 2005
ISRN Nephrology 7
[9] D S Wheeler P Devarajan Q Ma et al ldquoSerum neutrophilgelatinase-associated lipocalin (NGAL) as a marker of acutekidney injury in critically ill children with septic shockrdquoCriticalCare Medicine vol 36 no 4 pp 1297ndash1303 2008
[10] E A J Hoste N H Lameire R C Vanholder D D Benoit JM A Decruyenaere and F A Colardyn ldquoAcute renal failurein patients with sepsis in a surgical ICU predictive factorsincidence comorbidity and outcomerdquo Journal of the AmericanSociety of Nephrology vol 14 no 4 pp 1022ndash1030 2003
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 ISRN Nephrology
Table 4 Comparative study of patients group according to NGAL Urea and creatinine at admission (day zero) and 3rd day and theirclassification according to severity to 3 subgroups NAKI AKI minus D and AKI + D
Parameter NAKI AKI minus D AKI + D Test of significance 119875
119873 = 47 119873 = 8 119873 = 5
NGAL-0 (ngmL)Median 84 1005 120 137b 024Range (34ndash210) (74ndash115) (66ndash148)
NGAL-3 (ngmL)Median 105 184 350 308b 004lowastRange (34ndash530) (42ndash395) (150ndash550)
Urea-0 (mgdL)Median 345 38 65 591b 001lowastRange (15ndash116) (28ndash57) (425ndash788)
Urea-3 (mgdL)Median 38 841 1134 008b 076Range (18ndash310) (40ndash228) (7ndash178)
Creatinine-0 (mgdL)X plusmn SD 06 plusmn 023 08 plusmn 027 094 plusmn 015 119865 = 622 0004lowast
Creatinine-3 (mgdL)X plusmn SD 073 plusmn 036 225 plusmn 101 37 plusmn 11 119865 = 779 0000lowast
bMann-Whitney test 119865 Fisher test lowastsignificant
Table 5 Area under the receiver operating characteristic curve(ROC-AUC) and cutoff value for NGAL
Parameter ROC-AUC 95 CI CutoffNGAL-0 063 050ndash077 895 ngmL
Table 6 Validity of NGAL in prediction of AKI
Parameter AKI TotalPresent Absent
NGAL ge 895 11 19 30NGAL le 895 2 28 30Total 13 47 60
operating characteristic curve of NGAL revealed area underthe curve of 0677 with 95 (CI of 0557ndash0786)The sensitiv-ity of NGALwas 86 specificity was 39 positive predictivevalue was 39 and negative predictive value was 94
Our results of early predictive sensitive nonspecificserum NGAL although of clear statistical significance willcertainly need to be validated in a larger trial includingpatients with preexisting chronic kidney disease and comorbid conditions that normally accumulate with impairedrenal function The ability of biomarkers such as NGAL todiscern both the onset and resolution of AKI will furthervalidate their use in the clinical setting and greatly enhanceour understanding of AKI in the pediatric population
6 Conclusion
In conclusion we found that NGAL acts as a sensitivemarkerrather than a specific for one AKI At the same time it
presents a negative predictive value more valuable than beinga positive predictive value in detecting AKI
References
[1] D Bailey V Phan C Litalien et al ldquoRisk factors of acute renalfailure in critically ill children a prospective descriptive epi-demiological studyrdquo Pediatric Critical Care Medicine vol 8 no1 pp 29ndash35 2007
[2] A Akcan-Arikan M Zappitelli L L Loftis K K WashburnL S Jefferson and S L Goldstein ldquoModified RIFLE criteria incritically ill children with acute kidney injuryrdquo Kidney Interna-tional vol 71 no 10 pp 1028ndash1035 2007
[3] S M Bagshaw C Langenberg and R Bellomo ldquoUrinary bio-chemistry and microscopy in septic acute renal failure a sys-tematic reviewrdquo American Journal of Kidney Diseases vol 48no 5 pp 695ndash705 2006
[4] S M Moran and B D Myers ldquoCourse of acute renal failurestudied by a model of creatinine kineticsrdquo Kidney Internationalvol 27 no 6 pp 928ndash937 1985
[5] L Kjeldsen A H Johnsen H Sengelov and N BorregaardldquoIsolation and primary structure of NGAL a novel proteinassociated with human neutrophil gelatinaserdquo The Journal ofBiological Chemistry vol 268 no 14 pp 10425ndash10432 1993
[6] K Mori and K Nakao ldquoNeutrophil gelatinase-associated lipo-calin as the real-time indicator of active kidney damagerdquoKidneyInternational vol 71 no 10 pp 967ndash970 2007
[7] P Devarajan ldquoBiomarkers for the early detection of acutekidney injuryrdquo Current Opinion in Pediatrics vol 23 no 2 pp194ndash200 2011
[8] J Mishra C Dent R Tarabishi et al ldquoNeutrophil gelatinase-associated lipocalin (NGAL) as a biomarker for acute renalinjury after cardiac surgeryrdquoThe Lancet vol 365 no 9466 pp1231ndash1238 2005
ISRN Nephrology 7
[9] D S Wheeler P Devarajan Q Ma et al ldquoSerum neutrophilgelatinase-associated lipocalin (NGAL) as a marker of acutekidney injury in critically ill children with septic shockrdquoCriticalCare Medicine vol 36 no 4 pp 1297ndash1303 2008
[10] E A J Hoste N H Lameire R C Vanholder D D Benoit JM A Decruyenaere and F A Colardyn ldquoAcute renal failurein patients with sepsis in a surgical ICU predictive factorsincidence comorbidity and outcomerdquo Journal of the AmericanSociety of Nephrology vol 14 no 4 pp 1022ndash1030 2003
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

ISRN Nephrology 7
[9] D S Wheeler P Devarajan Q Ma et al ldquoSerum neutrophilgelatinase-associated lipocalin (NGAL) as a marker of acutekidney injury in critically ill children with septic shockrdquoCriticalCare Medicine vol 36 no 4 pp 1297ndash1303 2008
[10] E A J Hoste N H Lameire R C Vanholder D D Benoit JM A Decruyenaere and F A Colardyn ldquoAcute renal failurein patients with sepsis in a surgical ICU predictive factorsincidence comorbidity and outcomerdquo Journal of the AmericanSociety of Nephrology vol 14 no 4 pp 1022ndash1030 2003
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
![NGAL protects against endotoxin-induced renal tubular cell … · 2018. 7. 6. · apoptotic and NGAL mRNA expression was increased [8]. However, the function of NGAL is unclear, so](https://static.fdocuments.net/doc/165x107/60a09378519508702b6b9e40/ngal-protects-against-endotoxin-induced-renal-tubular-cell-2018-7-6-apoptotic.jpg)