
Clinical Review Report - CADTH · CDR CLINICAL REVIEW REPORT FOR INVOKANA vii Common Drug Review...
68
September 2015 Drug canagliflozin (Invokana) Indications Indicated in combination with metformin and either a sulfonylurea or pioglitazone in adult patients with type 2 diabetes mellitus to improve glycemic control when diet, exercise, and dual therapy (with metformin plus either a sulfonylurea or pioglitazone) do not provide adequate glycemic control. Listing request Listed as a third-line therapy added on to metformin and a sulfonylurea for patients with inadequate glycemic control on metformin and a sulfonylurea. Manufacturer Janssen Inc. Common Drug Review Clinical Review Report
Transcript of Clinical Review Report - CADTH · CDR CLINICAL REVIEW REPORT FOR INVOKANA vii Common Drug Review...

September 2015
Drug canagliflozin (Invokana)
Indications
Indicated in combination with metformin and either a sulfonylurea or pioglitazone in adult patients with type 2 diabetes mellitus to improve glycemic control when diet, exercise, and dual therapy (with metformin plus either a sulfonylurea or pioglitazone) do not provide adequate glycemic control.
Listing request Listed as a third-line therapy added on to metformin and a sulfonylurea for patients with inadequate glycemic control on metformin and a sulfonylurea.
Manufacturer Janssen Inc.
Common Drug Review Clinical Review Report

This review report was prepared by the Canadian Agency for Drugs and Technologies in Health (CADTH). In addition to CADTH staff, the review team included a clinical expert in endocrinology who provided input on the conduct of the review and the interpretation of findings. Through the CADTH Common Drug Review (CDR) process, CADTH undertakes reviews of drug submissions, resubmissions, and requests for advice, and provides formulary listing recommendations to all Canadian publicly funded federal, provincial, and territorial drug plans, with the exception of Quebec. The report contains an evidence-based clinical and/or pharmacoeconomic drug review, based on published and unpublished material, including manufacturer submissions; studies identified through independent, systematic literature searches; and patient-group submissions. In accordance with CDR Update — Issue 87, manufacturers may request that confidential information be redacted from the CDR Clinical and Pharmacoeconomic Review Reports. The information in this report is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. The information in this report should not be used as a substitute for the application of clinical judgment with respect to the care of a particular patient or other professional judgment in any decision-making process, nor is it intended to replace professional medical advice. While CADTH has taken care in the preparation of this document to ensure that its contents are accurate, complete, and up-to-date as of the date of publication, CADTH does not make any guarantee to that effect. CADTH is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in the source documentation. CADTH is not responsible for any errors or omissions or injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the information in this document or in any of the source documentation. This document is intended for use in the context of the Canadian health care system. Other health care systems are different; the issues and information related to the subject matter of this document may be different in other jurisdictions and, if used outside of Canada, it is at the user’s risk. This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada. CADTH takes sole responsibility for the final form and content of this document, subject to the limitations noted above. The statements and conclusions in this document are those of CADTH and not of its advisory committees and reviewers. The statements, conclusions, and views expressed herein do not necessarily represent the views of Health Canada or any Canadian provincial or territorial government. Production of this document is made possible by financial contributions from Health Canada and the governments of Alberta, British Columbia, Manitoba, New Brunswick, Newfoundland and Labrador, Northwest Territories, Nova Scotia, Nunavut, Ontario, Prince Edward Island, Saskatchewan, and Yukon. You are permitted to make copies of this document for non-commercial purposes, provided it is not modified when reproduced and appropriate credit is given to CADTH. You may not otherwise copy, modify, translate, post on a website, store electronically, republish, or redistribute any material from this document in any form or by any means without the prior written permission of CADTH. Please contact CADTH’s Vice-President of Corporate Services at [email protected] with any inquiries about this notice or other legal matters relating to CADTH’s services.
CDR CLINICAL REVIEW REPORT FOR INVOKANA
iii
Common Drug Review September 2015
TABLE OF CONTENTS
ABBREVIATIONS ........................................................................................................................................... vi EXECUTIVE SUMMARY ................................................................................................................................ vii 1. INTRODUCTION ..................................................................................................................................... 1
1.1 Disease Prevalence and Incidence ............................................................................................... 1 1.2 Standards of Therapy .................................................................................................................. 1 1.3 Drug ............................................................................................................................................. 2
2. OBJECTIVES AND METHODS.................................................................................................................. 3
2.1 Objectives .................................................................................................................................... 3 2.2 Methods ...................................................................................................................................... 3
3. RESULTS................................................................................................................................................. 5
3.1 Findings From the Literature ....................................................................................................... 5 3.2 Included Studies .......................................................................................................................... 7 3.3 Patient Disposition .................................................................................................................... 13 3.4 Exposure to Study Treatments .................................................................................................. 15 3.5 Critical Appraisal ........................................................................................................................ 16 3.6 Efficacy ....................................................................................................................................... 19 3.7 Harms......................................................................................................................................... 24
4. DISCUSSION ......................................................................................................................................... 30
4.1 Summary of Available Evidence ................................................................................................ 30 4.2 Interpretation of Results ........................................................................................................... 31
5. CONCLUSIONS ..................................................................................................................................... 34 APPENDIX 1: PATIENT INPUT SUMMARY .................................................................................................... 35 APPENDIX 2: LITERATURE SEARCH STRATEGY ............................................................................................ 38 APPENDIX 3: EXCLUDED STUDIES ............................................................................................................... 40 APPENDIX 4: SUMMARY AND APPRAISAL OF MANUFACTURER-SUBMITTED MIXED-TREATMENT COMPARISION ....................................................................................................................... 41 APPENDIX 5: SUMMARY OF OTHER STUDIES .............................................................................................. 49 REFERENCES ............................................................................................................................................... 55
CDR CLINICAL REVIEW REPORT FOR INVOKANA
iv
Common Drug Review September 2015
Tables Table 1: Summary of Efficacy Results ........................................................................................................ viii Table 2: Summary of Harms Outcomes ....................................................................................................... ix Table 3: Inclusion Criteria for the Systematic Review .................................................................................. 3 Table 4: Details of Included Studies .............................................................................................................. 6 Table 5: Glycated Hemoglobin Eligibility Criteria........................................................................................ 10 Table 6: Daily Doses of Sulfonylurea Required for Randomization in DIA3015 and DIA3002 .................... 10 Table 7: Summary of Demographic and Baseline Characteristics from DIA3002 and DIA3015 ................. 11 Table 8: Glycemic Rescue Criteria and Withdrawal Criteria ....................................................................... 12 Table 9: Summary of Patient Disposition From DIA3002 and DIA3015 ...................................................... 14 Table 10: Duration of Exposure to Investigational Products ...................................................................... 15 Table 11: Metformin Usage at Baseline and During DIA3002 and DIA3015 .............................................. 16 Table 12: Sulfonylurea Usage at Baseline and During DIA3002 and DIA3015 ............................................ 17 Table 13: Within-Group Changes in Glycated Hemoglobin and Fasting Plasma Glucose From DIA3002 and DIA3015 ................................................................................................................. 20 Table 14: Changes in Body Weight From Study .......................................................................................... 22 Table 15: Summary of Harms From DIA3015 and DIA3002 ........................................................................ 24 Table 16: Summary of Adverse Events From DIA3002 and DIA3015 .......................................................... 25 Table 17: Summary of Withdrawals Due to Adverse Events From DIA3015 and DIA3002 ........................ 26 Table 18: Summary of Hypoglycemia From DIA3002 and DIA3015............................................................ 27 Table 19: Summary of Female Genital Infection Adverse Events From DIA3002 and DIA3015 ................. 28 Table 20: Summary of Male Genital Infection Adverse Events From DIA3002 and DIA3015..................... 28 Table 21: Summary of Renal Adverse Events ............................................................................................. 29 Table 22: Difference in Change from Baseline in Fasting Lipids (Last Observation Carried Forward) ......................................................................................................................... 30 Table 23: Base-Case Analysis — Results of Random-Effects Model for the Mean Difference in Glycated Hemoglobin ............................................................................................................. 44 Table 24: Base-Case Analysis – Results of Fixed-Effect Model for Odds Ratio of the Proportion of Patients Reaching A1C of Less Than 7% for Canagliflozin Versus Active Comparators .............. 44 Table 25: Base-Case Analysis — Results of Fixed-Effect Model for the Mean Difference in Fasting Plasma Glucose for Canagliflozin Versus Active Comparators ....................................... 45 Table 26: Base-Case Analysis — Results of Random-Effects Model for the Mean Difference in Weight for Canagliflozin Versus Active Comparators ................................................................. 45 Table 27: Base-Case Analysis — Results of Fixed-Effect Model for the Mean Difference in Systolic Blood Pressure for Canagliflozin Versus Active Comparators .................................................... 46 Table 28: Base-Case Analysis — Results of Fixed-Effect Model for Odds Ratio in all Hypoglycemic Events for Canagliflozin Versus Active Comparators .................................................................. 46 Table 29: Appraisal of Network Meta-analysis Using ISPOR Criteria .......................................................... 47 Table 30: Baseline Demographics and Disease Characteristics .................................................................. 50 Table 31: Summary of Changes in Blood Pressure and Fasting Plasma Lipids ........................................... 53 Table 32: Summary of Overall Safety and Selected Adverse Events Over 52 Weeks ................................. 54
CDR CLINICAL REVIEW REPORT FOR INVOKANA
v
Common Drug Review September 2015
Figures Figure 1: QUOROM Flow Diagram for Inclusion and Exclusion of Studies ................................................... 5 Figure 2: Trial Design of DIA3015 .................................................................................................................. 8 Figure 3: Trial Design of DIA3002 .................................................................................................................. 9 Figure 4: Changes in Glycated Hemoglobin From DIA3002 and DIA3015 at 26 and 52 Weeks ................. 20 Figure 5: Changes in Fasting Plasma Glucose From DIA3002 at 26 Weeks and DIA3015 at 52 Weeks ................................................................................................................................. 21 Figure 6: Changes in Glycated Hemoglobin (A) and Fasting Plasma Glucose (B) From DIA3015 Over 52 Weeks ............................................................................................................................ 21 Figure 7: Difference in Change from Baseline in Body Weight From DIA3002 and DIA3015 .................... 23 Figure 8: Difference in Percentage Changes in Systolic (A) and Diastolic (B) Blood Pressure From DIA3002 and DIA3015 ................................................................................................................. 24 Figure 9: Organizations and Foundations That Made Donations to the Canadian Diabetes Association Between September 2012 and August 2013 ........................................................... 37 Figure 10: Evidence Network Diagrams ...................................................................................................... 43 Figure 11: Mean Change in Glycated Hemoglobin Value (Percentage) Versus Placebo ............................ 46 Figure 12: Patient Disposition in DIA3012 .................................................................................................. 51 Figure 13: Changes in Glycemic Parameters ............................................................................................... 51 Figure 14: Percentage Change in Body Weight (Last Observation Carried Forward) ................................. 52
CDR CLINICAL REVIEW REPORT FOR INVOKANA
vi
Common Drug Review September 2015
ABBREVIATIONS
A1C glycated hemoglobin
AE adverse event
CDR CADTH Common Drug Review
CI confidence interval
DPP-4 dipeptidyl peptidase-4
eGFR estimated glomerular filtration rate
EMA European Medicines Agency
FPG fasting plasma glucose
GLP-1 glucagon-like peptide-1
ITT intention-to-treat
mITT modified intention-to-treat
n number of patients with event
N number of patients
NMA network meta-analysis
NPH neutral protamine Hagedorn
PP per-protocol
RCT randomized controlled trial
SBP systolic blood pressure
SGLT2 sodium-glucose cotransporter-2
WDAE withdrawal due to adverse event
CDR CLINICAL REVIEW REPORT FOR INVOKANA
vii
Common Drug Review September 2015
EXECUTIVE SUMMARY
Introduction Canagliflozin is the first sodium-glucose cotransporter-2 (SGLT2) inhibitor to be approved for use in Canada. Canagliflozin is indicated for patients with type 2 diabetes to improve glycemic control as monotherapy or in combination with metformin; a sulfonylurea; metformin and a sulfonylurea; metformin and pioglitazone; or insulin (with or without metformin) when these drugs do not provide adequate glycemic control. The recommended starting dose is 100 mg once daily. A dose of 300 mg once daily may be considered for patients who have tolerated a dose of 100 mg once daily and who need tighter glycemic control, provided they have an estimated glomerular filtration rate (eGFR) of ≥ 60 mL/min/1.73 m2 and have a low risk of adverse reactions associated with reduced intravascular volume.1 Canagliflozin is contraindicated in renally impaired patients who have an eGFR of less than 45 mL/min/1.73 m2, have end-stage renal disease, or are on dialysis. The current CADTH Common Drug Review (CDR) submission for canagliflozin is for use in combination with metformin and a sulfonylurea in adult patients with type 2 diabetes mellitus to improve glycemic control when diet, exercise, and dual therapy do not provide adequate glycemic control.
Results and Interpretation Included Studies The CDR review included two double-blind phase 3 randomized controlled trials investigating the efficacy and safety of canagliflozin in patients with type 2 diabetes and inadequate glycemic control with metformin and sulfonylurea combination therapy. DIA3015 (N = 756) randomized patients who were using metformin and a sulfonylurea to either canagliflozin 300 mg once daily or sitagliptin 100 mg once daily add-on therapy over a period of 52 weeks. DIA3002 (N = 469) randomized patients to either canagliflozin 100 mg once daily, canagliflozin 300 mg once daily, or matching placebo added on to their existing metformin and sulfonylurea therapy over a period of 26 weeks in the primary study, and an additional 26 weeks in an extension study. Adults with type 2 diabetes were eligible for these studies if they had poor glycemic control (i.e., glycated hemoglobin [A1C] ≥ 7% and ≤ 10.5%) despite using the maximum tolerated dose of metformin (≥ 1,500 mg/day) and using at least half the maximum recommended dose of a sulfonylurea. The primary efficacy end point in both studies was the difference in A1C levels from baseline to the end of the study period (52 weeks in DIA3015 and 26 weeks in DIA3002). Efficacy Active-Controlled Trial (DIA3015)
After 52 weeks, canagliflozin 300 mg once daily demonstrated non-inferiority and superiority compared with sitagliptin 100 mg once daily for change from baseline in A1C in both intention-to-treat (least squares mean difference [LSMD] –0.37%; 95% confidence interval [CI], –0.50% to –0.25%) and per-protocol data analyses (LSMD –0.21%; 95% CI, –0.34% to –0.08%) (Table 1). Compared with sitagliptin, canagliflozin 300 mg once daily demonstrated statistically significant reductions in fasting plasma glucose (FPG) (LSMD –1.34 mmol/L; 95% CI, –1.66 mmol/L to –1.01 mmol/L) and systolic blood pressure (LSMD –5.91 mm Hg; 95% CI, –7.64 mm Hg to –xxxx mm Hg) and resulted in a greater reduction in percentage body weight (LSMD –2.8%; 95% CI, –3.3% to –2.2%) (Table 1).

CDR CLINICAL REVIEW REPORT FOR INVOKANA
viii
Common Drug Review September 2015
Placebo-Controlled Trial (DIA3002)
Both doses of canagliflozin demonstrated statistically significant (P < 0.001) reductions in A1C, FPG, and body weight relative to placebo in DIA3002 (Table 1). Compared with placebo, the LSMD in change from baseline in A1C was –0.71% (95% CI, –0.90% to –0.52%) for 100 mg once daily and –0.92% (95% CI, –1.11% to –0.73%) for 300 mg once daily. The LSMD for changes in FPG was –1.24 mmol/L (95% CI, –1.75 mmol/L to –0.73 mmol/L) and –1.92 mmol/L (95% CI, –2.43 mmol/L to –1.41 mmol/L) for canagliflozin 100 mg and 300 mg, respectively. Compared with placebo, the percentage change in body weight favoured canagliflozin with an LSMD of –1.4% (95% CI, –2.1% to –0.7%) for 100 mg once daily and –2.0% (95% CI, –2.7% to –1.3%) for 300 mg once daily. Neither canagliflozin group demonstrated a statistically significant reduction in systolic blood pressure at week 26 compared with placebo.
TABLE 1: SUMMARY OF EFFICACY RESULTS
Efficacy End Points DIA3015 DIA3002
CANA 300 mg vs. SITA CANA 100 mg vs. PL CANA 300 mg vs. PL
Change from BL in A1C (%) LSMD (95% CI)
–0.37 (–0.50 to –0.25)
–0.71 (–0.90 to –0.52)
–0.92 (–1.11 to –0.73)
Change from BL in FPG (mmol/L) LSMD (95% CI)
–1.34 (–1.66 to –1.01)
–1.24 (–1.75 to –0.73)
–1.92 (–2.43 to –1.41)
Change from BL in body weight (%) LSMD (95% CI)
–2.8 (–3.3 to –2.2)
–1.42 (–2.1 to –0.7)
–2.02 (–2.7 to –1.3)
Change from BL in SBP (mm Hg) LSMD (95% CI)
–5.91 (–7.64 to –xxxx)
–2.24 (–xxxx to 0.24)
–1.62 (–4.11 to xxxx)
BL = baseline; CANA = canagliflozin; CI = confidence interval; FPG = fasting blood glucose; LSMD = least squares mean difference; PL = placebo; SITA = sitagliptin; vs = versus.
Harms In DIA3015, the proportion of patients who experienced at least one adverse event during the 52-week treatment period was similar in the canagliflozin (76.7%) and sitagliptin (77.5%) groups. The incidences of influenza, upper respiratory tract infection, and headache were higher in the canagliflozin group relative to the sitagliptin group. In DIA3002, the incidence of patients with at least one adverse event was 57.3% in the canagliflozin 100 mg group, 62.2% in the canagliflozin 300 mg group, and xxxxx in the placebo group. The proportion of patients with at least one serious adverse event was similar in the canagliflozin 300 mg group (6.4%) and the sitagliptin 100 mg group (5.6%). Serious adverse events were less commonly reported in the canagliflozin groups (3.2% to 3.8%), relative to the placebo group (5.8%) in DIA3002. The incidence of adverse events leading to discontinuation was higher in the canagliflozin groups in both of the included studies. In DIA3015, withdrawals due to adverse events (WDAE) were reported for 5.3% of the canagliflozin group versus 2.9% in the sitagliptin group. The proportion of WDAE in the canagliflozin groups was similar in DIA3002, with 5.8% in the 300 mg group and 5.7% in the 100 mg group, both of which numerically exceeded the proportion in the placebo group (3.2%).

CDR CLINICAL REVIEW REPORT FOR INVOKANA
ix
Common Drug Review September 2015
In DIA 3015, the incidence of hypoglycemia was similar in the canagliflozin 300 mg (43.2%) and sitagliptin 100 mg groups (40.7%). Events classified as severe hypoglycemia were reported for 4.0% of patients in the canagliflozin group and 3.4% in the sitagliptin group (Table 2). In DIA3002, hypoglycemia was more commonly reported in the canagliflozin 100 mg (27.4%) and canagliflozin 300 mg (30.1%) groups than in the placebo group (15.4%) (Table 2). The incidence of any hypoglycemia was 30.1% and 27.4% for canagliflozin 300 mg and canagliflozin 100 mg, respectively, compared with 15.4% in the placebo group. Severe hypoglycemia was rare in DIA3002 with just one event reported in each of the placebo and canagliflozin 100 mg groups and no events in the canagliflozin 300 mg group. Canagliflozin was associated with an increase in vulvovaginal adverse events in women and superficial genital infections in men relative to sitagliptin and placebo. Vulvovaginal adverse events were reported for 15.3% of patients in the canagliflozin 300 mg group compared with 4.3% in the sitagliptin group. In DIA 3015, the incidence of superficial genital infections in men was 9.2% in the canagliflozin 300 mg group compared with 0.5% in the sitagliptin 100 mg group. In the placebo-controlled trial (DIA3002), the incidence was 6.6% with canagliflozin 100 mg, 3.4% with canagliflozin 300 mg, and 1.3% with placebo. Nearly all of these adverse events were mild or moderate in severity. In DIA3015, canagliflozin 300 mg was shown to increase both high-density lipoprotein (HDL) cholesterol (LSMD: 6.99 mmol/L [95% CI, 4.6 to 9.3]) and low-density lipoprotein (LDL) cholesterol (6.44 mmol/L [95% CI, 1.7 to 11.2]) relative to sitagliptin 100 mg. In DIA3002, canagliflozin also appeared to increase HDL cholesterol (3.53 mmol/L [95% CI, 0.1 to 7.0]) and LDL cholesterol (4.58 mmol/L [95% CI, –1.8 to 10.9]) relative to placebo. There were no significant differences between canagliflozin 100 mg and placebo in DIA3002.
TABLE 2: SUMMARY OF HARMS OUTCOMES
Summary of AEs
DIA3015 DIA3002
CANA 300 mg (N = 377)
n (%)
SITA 100 mg (N = 378)
n (%)
Placebo (N = 156)
n (%)
CANA 100 mg (N = 157)
n (%)
CANA 300 mg (N = 156)
n (%)
Any AEs 289 (76.7) 293 (77.5) 99 (63.5) 90 (57.3) 97 (62.2)
WDAEs 20 (5.3) 11 (2.9) 5 (3.2) 9 (5.7) 9 (5.8)
SAEs 24 (6.4) 21 (5.6) 9 (5.8) 5 (3.2) 6 (3.8)
Any hypoglycemia 163 (43.2) 154 (40.7) 24 (15.4) 43 (27.4) 47 (30.1)
Severe hypoglycemia 15 (4.0) 13 (3.4) 1 (0.6) 1 (0.6) 0
Events per patient-year 4.14 3.81 1.04 2.58 3.38
AE = adverse event; CANA = canagliflozin; SAE = serious adverse event; SITA = sitagliptin; WDSAE = withdrawal due to serious adverse event. Source: Data from Clinical Study Reports for DIA3002
2 and DIA3015.
3

CDR CLINICAL REVIEW REPORT FOR INVOKANA
x
Common Drug Review September 2015
Conclusions The CDR systematic review included two phase 3 randomized controlled trials that investigated the comparative safety and efficacy of canagliflozin in patients with type 2 diabetes with inadequate glycemic control with metformin and a sulfonylurea. One 12-month, active-controlled study demonstrated that canagliflozin 300 mg once daily was superior to sitagliptin 100 mg once daily for improving glycemic control, reducing body weight, and lowering systolic blood pressure. One six-month study demonstrated that canagliflozin, at both the recommended starting dose of 100 mg once daily and the higher 300 mg once-daily dose, resulted in clinically relevant improvements in glycemic control compared with placebo. The improvements in glycemic control and blood pressure observed with canagliflozin were generally considered to be clinical relevant by regulatory authorities and the CDR clinical expert; however, publication of the longer-term studies will be required to determine any beneficial or harmful effects on cardiovascular end points. Canagliflozin is associated with an increased risk of developing urogenital adverse events and an increase in LDL cholesterol. When used in combination with a sulfonylurea, canagliflozin increases the risk of hypoglycemia relative to placebo. As with all new antihyperglycemic drugs, additional studies and clinical experience will be required to fully characterize the longer-term safety profile of canagliflozin.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
1
Common Drug Review September 2015
1. INTRODUCTION
1.1 Disease Prevalence and Incidence Diabetes is a chronic, metabolic disease with significant health impacts on individuals and societies. The incidence of diabetes is increasing at a dramatic rate around the world. The International Diabetes Federation estimates that 371 million people worldwide had diabetes in 2012, a figure that is expected to increase to 552 million by 2030.4 In Canada, the prevalence of diabetes in 2009 was 6.8% (2.4 million Canadians); this is expected to rise to 3.7 million people by 2019.5 People with diabetes are more likely to be hospitalized and to experience complications requiring specialist care. By 2020, diabetes-associated costs to the Canadian health care system will be an estimated $16.9 billion per year.6 Ninety per cent of people with diabetes have type 2 diabetes mellitus,7 a condition characterized by increased hepatic glucose output, reduced insulin secretion, and insulin resistance. It is generally diagnosed in adults older than 40 years, although increasingly it is being detected in adolescents and children. Diagnosis is based on a fasting plasma glucose (FPG) level of ≥ 7.0 mmol/L; a two-hour plasma glucose level with a 75 g oral glucose tolerance test of ≥ 11.1 mmol/L; or a glycated hemoglobin (A1C) of ≥ 6.5%. A diagnosis of type 2 diabetes based on A1C is restricted to adults without any of the factors that can affect the accuracy of A1C test results.4 These thresholds for diagnosis have been established because they predict the development of retinopathy, which is one of the common microvascular complications of diabetes.4 Other microvascular complications are nephropathy (which may progress to end-stage renal disease) and neuropathy (which may cause pain, tingling, gastroparesis, erectile dysfunction, or lower-extremity peripheral vascular disease, often resulting in the need for amputation). Type 2 diabetes is the leading cause of blindness, end-stage renal disease, and non-traumatic amputation in Canadian adults.4 Cardiovascular disease (i.e., heart disease, stroke, and peripheral vascular disease) is a major macrovascular complication of type 2 diabetes and is the leading cause of death in people with that disease.5
1.2 Standards of Therapy There are currently 11 classes of antihyperglycemic drugs approved for use in Canada: biguanides, sulfonylureas, meglitinides, alpha-glucosidase inhibitors, thiazolidinediones, dipeptidyl peptidase-4 (DPP-4) inhibitors, glucagon-like peptide-1 (GLP-1) analogues, sodium-glucose cotransporter-2 (SGLT2) inhibitors, basal insulins, bolus insulins, and biphasic insulins. In most patients with type 2 diabetes, metformin is recommended as the first-line oral antihyperglycemic drug when glycemic control cannot be achieved by lifestyle interventions alone.4 In 2013, CADTH published updated network meta-analyses (NMAs) and pharmacoeconomic analyses assessing the comparative safety, efficacy, and cost-effectiveness of all available classes of antihyperglycemic therapies in the following clinical situations: patients with type 2 diabetes with inadequate glycemic control on metformin monotherapy;8 and patients with type 2 diabetes with inadequate glycemic control on metformin and a sulfonylurea.9,10 Based on this evidence, the Canadian Drug Expert Committee recommended the following: 1. A sulfonylurea should be added to metformin for most adults with type 2 diabetes who are
inadequately controlled on metformin alone. 2. Neutral protamine Hagedorn (NPH) insulin should be added for most adults with type 2 diabetes
inadequately controlled on metformin and a sulfonylurea. 3. A DPP-4 inhibitor may be added to metformin and sulfonylurea therapy in circumstances where
patients with type 2 diabetes are unable to use insulin as a third-line option.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
2
Common Drug Review September 2015
These CADTH reviews predated the emergence of SGLT2 inhibitors in Canada; therefore, they were not included in the reviews or addressed in the recommendations.
1.3 Drug Canagliflozin is the first antihyperglycemic drug of the SGLT2 inhibitor class to be approved for use in Canada. This class of oral antihyperglycemic drugs has a novel insulin-independent mechanism of action, which results in reduced reabsorption of filtered glucose and a lower renal threshold for glucose. This increases urinary glucose excretion, which lowers elevated concentrations of plasma glucose. The product monograph also states that the increase in urinary glucose excretion produces a diuretic effect, leading to a reduction in systolic blood pressure (SPB), and results in a loss of calories, contributing to a reduction in body weight. Canagliflozin is indicated for use as monotherapy and in combination with other antihyperglycemic drugs as follows:
As an adjunct to diet and exercise to improve glycemic control in adult patients with type 2 diabetes
In combination with metformin or a sulfonylurea in adult patients with type 2 diabetes mellitus to improve glycemic control when diet and exercise plus monotherapy with one of these drugs does not provide adequate glycemic control
In combination with metformin and either a sulfonylurea or pioglitazone in adult patients with type 2 diabetes mellitus to improve glycemic control when diet, exercise, and dual therapy (with metformin plus either a sulfonylurea or pioglitazone) do not provide adequate glycemic control
As add-on combination therapy with insulin (with or without metformin) in adult patients with type 2 diabetes mellitus as an adjunct to diet and exercise to improve glycemic control when diet and exercise and therapy with insulin (with or without metformin) do not provide adequate glycemic control.
The recommended starting dose of canagliflozin is 100 mg once daily. In patients tolerating canagliflozin 100 mg once daily who need tighter glycemic control, the 300 mg dose may be considered for patients who have an estimated glomerular filtration rate (eGFR) of ≥ 60 mL/min/1.73 m2 and who have a low risk of adverse reactions associated with reduced intravascular volume due to canagliflozin treatment.1 Canagliflozin is contraindicated in renally impaired patients who have an eGFR of less than 45 mL/min/1.73 m2, have end-stage renal disease, or are on dialysis. No dose adjustment is needed for patients with mild renal impairment (eGFR of 60 mL/min/1.73 m2 to < 90 mL/min/1.73 m2 or greater). Canagliflozin should not be initiated in patients with an eGFR < 60 mL/min/1.73 m2. In patients tolerating canagliflozin whose eGFR persistently falls below 60 mL/min/1.73 m2, the dose of canagliflozin should be adjusted to or maintained at 100 mg once daily. Canagliflozin should be discontinued when eGFR is persistently below 45 mL/min/1.73 m2 as it is not expected to be sufficiently effective in these patients and adverse reactions are more frequent.1
Indication under review
Indicated in combination with metformin and either a sulfonylurea or pioglitazone in adult patients with type 2 diabetes mellitus to improve glycemic control when diet, exercise, and dual therapy (with metformin plus either a sulfonylurea or pioglitazone) do not provide adequate glycemic control.
Listing criteria requested by sponsor
Listed as a third-line therapy added on to metformin and a sulfonylurea for patients with inadequate glycemic control on metformin and a sulfonylurea.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
3
Common Drug Review September 2015
2. OBJECTIVES AND METHODS
2.1 Objectives To perform a systematic review of the beneficial and harmful effects of canagliflozin for the treatment of adults with type 2 diabetes who have experienced inadequate glycemic control on combination therapy with metformin and a sulfonylurea.
2.2 Methods Studies were selected for inclusion in the systematic review based on the selection criteria presented in Table 3.
TABLE 3: INCLUSION CRITERIA FOR THE SYSTEMATIC REVIEW
Patient Population Adults with type 2 diabetes who have experienced inadequate glycemic control on combination therapy with metformin and a sulfonylurea
Intervention Canagliflozin at a dose of 100 mg once daily or 300 mg once daily in combination with metformin and a sulfonylurea
Comparators DPP-4 inhibitors, basal insulin, or placebo in combination with metformin and a sulfonylurea
Outcomes Key efficacy outcomes • Mortality • Diabetes-related morbidity (macrovascular, microvascular) • Glycemic control (A1C, FPG) • Quality of life (measured by any validated scale) Body weight Blood pressure Harms outcomes Total adverse events Serious adverse events Withdrawals due to adverse events Hypoglycemia Urogenital adverse events Renal adverse events Lipids Other outcomes Health care resource utilization
Study Design Published and unpublished RCTs ≥ 12 weeks duration
A1C = glycated hemoglobin; DPP-4 = dipeptidyl peptidase-4; FPG = fasting plasma glucose; RCT = randomized controlled trial.
The literature search was performed by an information specialist using a peer-reviewed search strategy. Published literature was identified by searching the following bibliographic databases: MEDLINE (1946–) with in-process records and daily updates via Ovid; Embase (1974–) via Ovid; and PubMed. The search strategy consisted of both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was Invokana (canagliflozin). No filters were applied to limit the retrieval by study type. Where possible, retrieval was limited to the human population. Retrieval was not limited by publication year or by language. Conference abstracts
CDR CLINICAL REVIEW REPORT FOR INVOKANA
4
Common Drug Review September 2015
were excluded from the search results. The initial search was completed on August 20, 2014. Regular alerts were established to update the search until the meeting of the Canadian Drug Expert Committee on December 10, 2014. Regular search updates were performed on databases that do not provide alert services. Details regarding the search strategy are provided in Appendix 2. Grey literature (literature that is not commercially published) was identified by searching relevant websites from the following sections of the CADTH Grey Matters checklist (www.cadth.ca/en/resources/finding-evidence-is/grey-matters): Health Technology Assessment Agencies, Health Economics, Clinical Practice Guidelines, Databases (free), and Internet Search. Google and other Internet search engines were used to search for additional web-based materials. These searches were supplemented by reviewing the bibliographies of key papers and through contacts with appropriate experts. In addition, the manufacturer of the drug was contacted for information regarding unpublished studies.
Two CADTH Common Drug Review (CDR) clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least one reviewer were acquired. The reviewers independently made the final selection of studies to be included in the review; any differences were resolved through discussion. The included studies are presented in Table 4 and the excluded studies in Appendix 3.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
5
Common Drug Review September 2015
11 Reports included,
presenting data from 2 unique studies
289 Citations identified in literature search
7 Potentially relevant reports
identified and screened
13 Total potentially relevant reports identified and screened
2 Reports excluded
6 Potentially relevant reports
from other sources
3. RESULTS
3.1 Findings From the Literature Two studies were identified from the literature for inclusion in the systematic review (Figure 1).
FIGURE 1: QUOROM FLOW DIAGRAM FOR INCLUSION AND EXCLUSION OF STUDIES
QUOROM = Quality of Reporting of Meta-analyses.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
6
Common Drug Review September 2015
TABLE 4: DETAILS OF INCLUDED STUDIES DIA3015 (CANTATA-D2) DIA3002 (CANTATA-MSU)
De
sign
s &
Po
pu
lati
on
s
Study design Phase 3, DB active-controlled, two-group, parallel-group, multi-centre RCT
Phase 3, DB, three-group, parallel-group, placebo-controlled, multi-centre RCT
Locations 140 centres 85 centres
Randomized (N) 756 469
Inclusion criteria ≥ 18 years of age with T2DM and inadequately controlled with MET and an SU
Exclusion criteria Repeated FPG and/or fasting SMBG measurements ≥ 16.7 mmol/L (DIA3015) or 15 mmol/L (DIA3002) during the pre-treatment phase
History of diabetic ketoacidosis, T1DM, pancreas, or beta-cell transplantation, or diabetes secondary to pancreatitis or pancreatectomy
Receiving any antihyperglycemic except as specified in the inclusion criteria MI, unstable angina, revascularization procedure, or cerebrovascular accident
within three months of screening, or history of NYHA Class III or Class IV cardiac disease
Findings on 12-lead ECG that required urgent diagnostic evaluation or intervention Uncontrolled hypertension eGFR < 55 mL/min/1.73 m
2 (or < 60 mL/min/1.73 m
2 if based upon restriction of
MET use in the MET local label) or SCr 124 µmol/L (men) and ≥ 115 µmol/L (women)
Inte
rve
nti
on
s
Interventions
Canagliflozin 300 mg once daily Canagliflozin 100 mg once daily Canagliflozin 300 mg once daily
Comparator
Sitagliptin 100 mg once daily Placebo
Du
rati
on
Run-in Antihyperglycemic adjustment period: ≤ four-week MET and/or SU dose titration period eight-week MET and SU stable period
Two-week placebo run-in (single-blind)
Double-blind 52-week core study No extension phase
26-week core study 26-week extension phase
Follow-up 30 days after last dose of study drug
Ou
tco
me
s
Primary end point
Change in A1C from baseline to 52 weeks Change in A1C from baseline to 26 weeks
Secondary efficacy end points
Proportion of patients with A1C < 7.0% Change from baseline in FPG Change from baseline in fasting HDL-C and triglycerides Change from baseline body weight Change from baseline systolic blood pressure
Safety assessments
Adverse events, hypoglycemia, safety laboratory tests, 12-lead electrocardiograms, vital sign measurements

CDR CLINICAL REVIEW REPORT FOR INVOKANA
7
Common Drug Review September 2015
No
tes
Data sources Clinical study reports2,3
Common Technical Document
11
FDA Statistical Report12
Health Canada pharmaceutical safety and efficacy assessment
13
European public assessment report13,14
Clinicaltrials.gov
A1C = glycated hemoglobin; AE = adverse event; DB = double-blind; ECG = electrocardiogram; eGFR = estimated glomerular filtration rate; FPG = fasting plasma glucose; HDL-C = high-density lipoprotein cholesterol; MET = metformin; MI = myocardial infarction; NYHA = New York Heart Association; RCT = randomized controlled trial; SCr = serum creatinine; SMBG = self-monitoring of blood glucose; SU = sulfonylurea; T1DM = type 1 diabetes; T2DM = type 2 diabetes mellitus; TG = triglycerides.
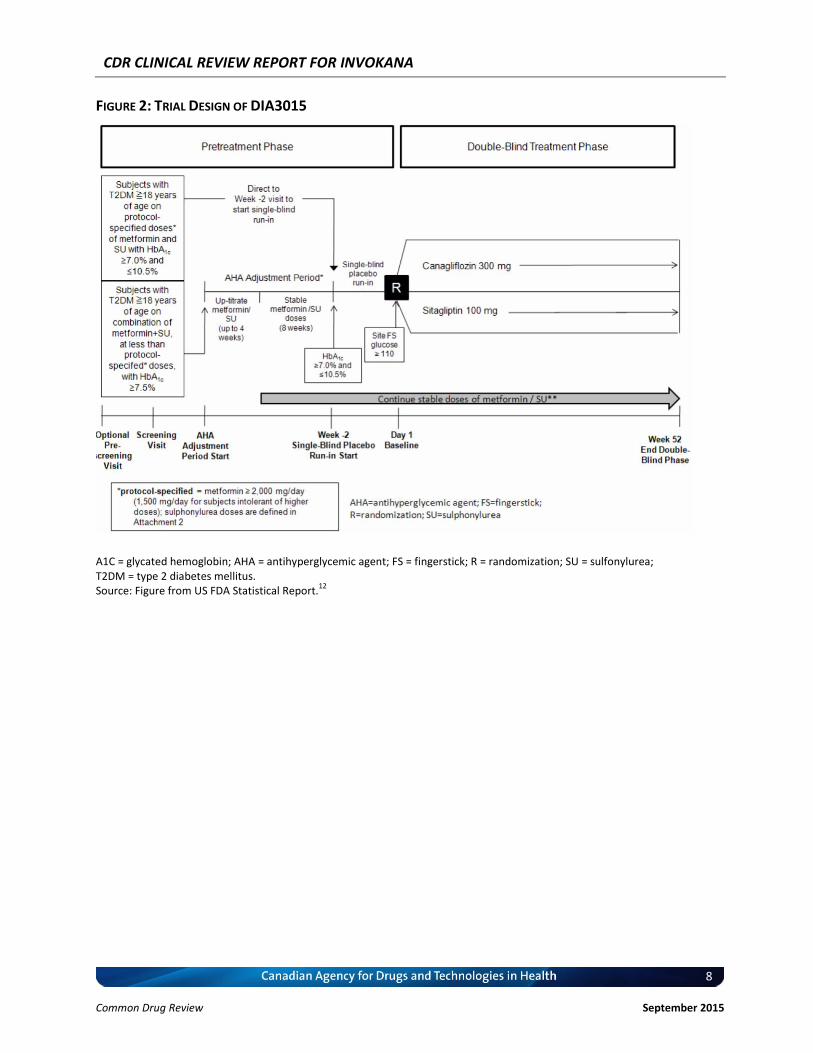
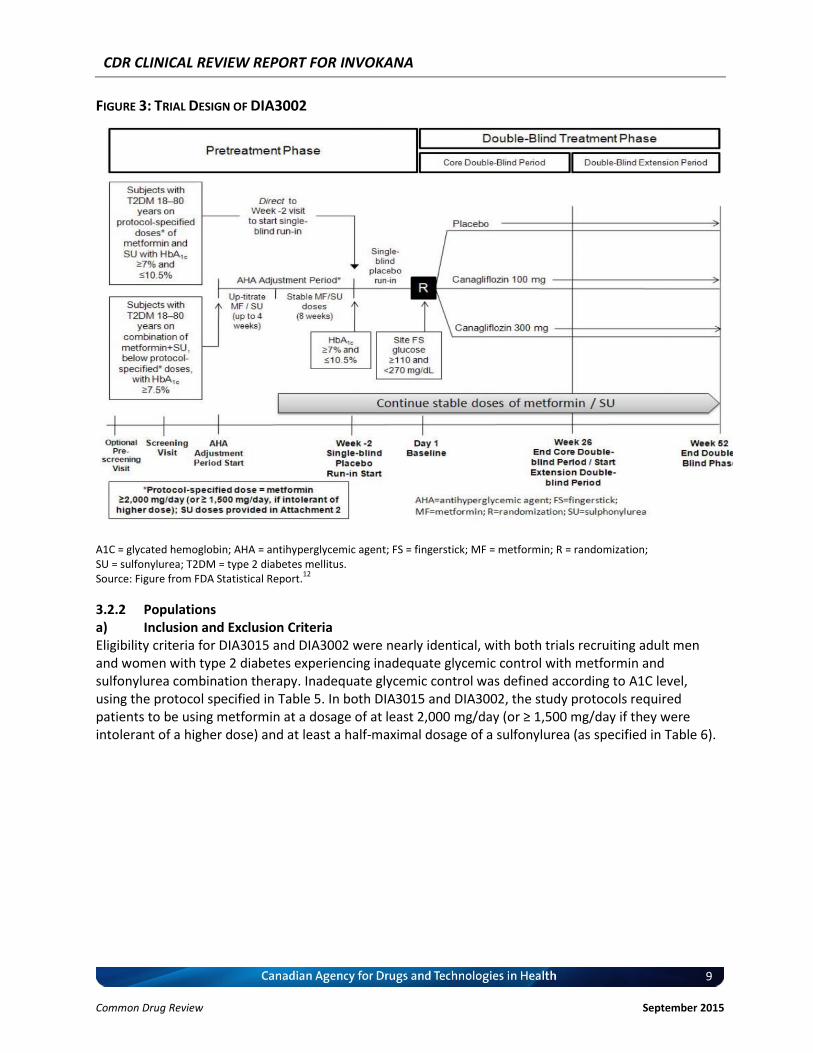
3.2 Included Studies 3.2.1 Description of Studies a) Active-Controlled Trial DIA3015 was a phase 3, double-blind, active-controlled, two-group, parallel-group, multi-centre randomized controlled trial (RCT). The study was conducted at 140 centres located primarily in North America (70 centres) and Europe (21 centres). The study randomized (1:1) 756 patients with type 2 diabetes experiencing inadequate glycemic control with metformin and a sulfonylurea to receive either canagliflozin 300 mg once daily or sitagliptin 100 mg once daily over a period of 52 weeks. Prior to randomization, all eligible participants were required to complete a two-week, single-blind, placebo run-in phase (Figure 2). The purpose of the run-in period was to assess whether participants would demonstrate compliance with study procedures and have no difficulty with administration of the study drugs. b) Placebo-Controlled Trial DIA3002 was a phase 3, double-blind, three-group, parallel-group, placebo-controlled, multi-centre RCT. The study was conducted at 85 centres located primarily in North America (42), Europe (24), and Central America (5). The study randomized (1:1:1) 469 patients with type 2 diabetes experiencing inadequate glycemic control with metformin and a sulfonylurea to receive either canagliflozin 100 mg once daily, canagliflozin 300 mg once daily, or matching placebo over a period of 26 weeks in the core study, and an additional 26 weeks in a double-blinded extension study. Similar to DIA3015, all eligible participants were required to complete a two-week, single-blind, placebo run-in phase prior to randomization (Figure 3).
CDR CLINICAL REVIEW REPORT FOR INVOKANA
8
Common Drug Review September 2015
FIGURE 2: TRIAL DESIGN OF DIA3015
A1C = glycated hemoglobin; AHA = antihyperglycemic agent; FS = fingerstick; R = randomization; SU = sulfonylurea; T2DM = type 2 diabetes mellitus. Source: Figure from US FDA Statistical Report.
12
CDR CLINICAL REVIEW REPORT FOR INVOKANA
9
Common Drug Review September 2015
FIGURE 3: TRIAL DESIGN OF DIA3002
A1C = glycated hemoglobin; AHA = antihyperglycemic agent; FS = fingerstick; MF = metformin; R = randomization; SU = sulfonylurea; T2DM = type 2 diabetes mellitus. Source: Figure from FDA Statistical Report.
12
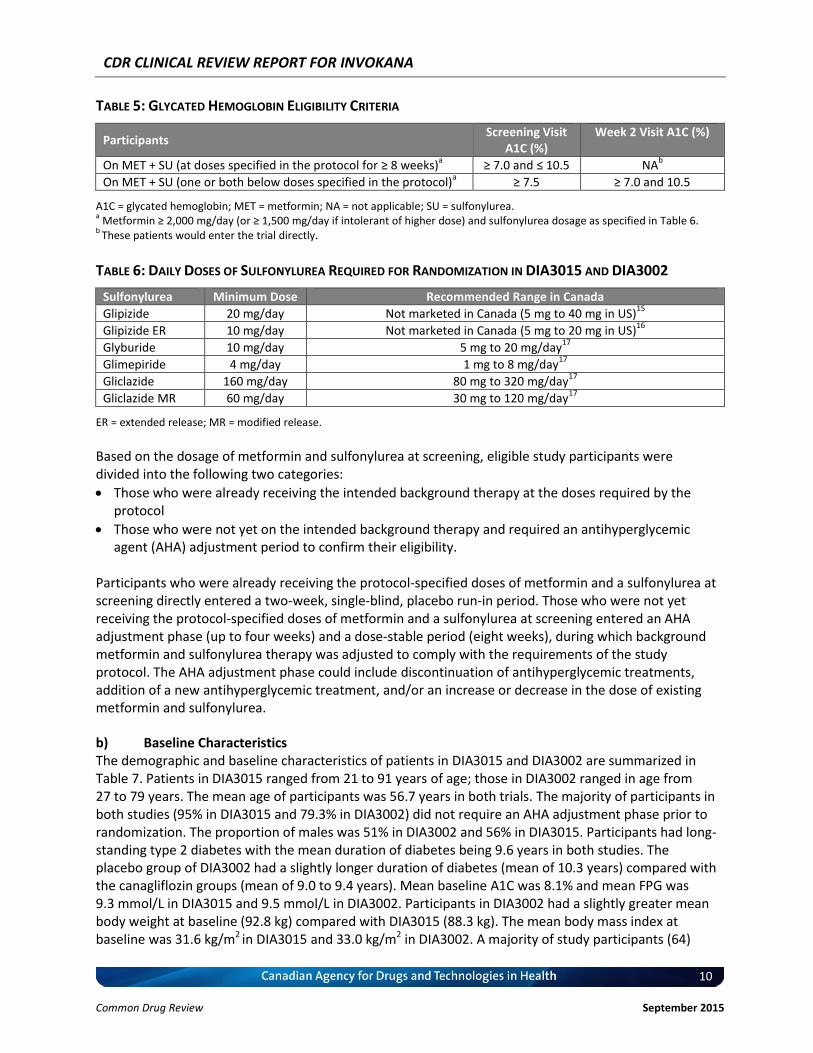
3.2.2 Populations a) Inclusion and Exclusion Criteria Eligibility criteria for DIA3015 and DIA3002 were nearly identical, with both trials recruiting adult men and women with type 2 diabetes experiencing inadequate glycemic control with metformin and sulfonylurea combination therapy. Inadequate glycemic control was defined according to A1C level, using the protocol specified in Table 5. In both DIA3015 and DIA3002, the study protocols required patients to be using metformin at a dosage of at least 2,000 mg/day (or ≥ 1,500 mg/day if they were intolerant of a higher dose) and at least a half-maximal dosage of a sulfonylurea (as specified in Table 6).
CDR CLINICAL REVIEW REPORT FOR INVOKANA
10
Common Drug Review September 2015
TABLE 5: GLYCATED HEMOGLOBIN ELIGIBILITY CRITERIA
Participants Screening Visit
A1C (%) Week 2 Visit A1C (%)
On MET + SU (at doses specified in the protocol for ≥ 8 weeks)a ≥ 7.0 and ≤ 10.5 NA
b
On MET + SU (one or both below doses specified in the protocol)a ≥ 7.5 ≥ 7.0 and 10.5
A1C = glycated hemoglobin; MET = metformin; NA = not applicable; SU = sulfonylurea. a Metformin ≥ 2,000 mg/day (or ≥ 1,500 mg/day if intolerant of higher dose) and sulfonylurea dosage as specified in Table 6.
b These patients would enter the trial directly.
TABLE 6: DAILY DOSES OF SULFONYLUREA REQUIRED FOR RANDOMIZATION IN DIA3015 AND DIA3002
Sulfonylurea Minimum Dose Recommended Range in Canada
Glipizide 20 mg/day Not marketed in Canada (5 mg to 40 mg in US)15
Glipizide ER 10 mg/day Not marketed in Canada (5 mg to 20 mg in US)16
Glyburide 10 mg/day 5 mg to 20 mg/day17
Glimepiride 4 mg/day 1 mg to 8 mg/day17
Gliclazide 160 mg/day 80 mg to 320 mg/day17
Gliclazide MR 60 mg/day 30 mg to 120 mg/day17
ER = extended release; MR = modified release.
Based on the dosage of metformin and sulfonylurea at screening, eligible study participants were divided into the following two categories:
Those who were already receiving the intended background therapy at the doses required by the protocol
Those who were not yet on the intended background therapy and required an antihyperglycemic agent (AHA) adjustment period to confirm their eligibility.
Participants who were already receiving the protocol-specified doses of metformin and a sulfonylurea at screening directly entered a two-week, single-blind, placebo run-in period. Those who were not yet receiving the protocol-specified doses of metformin and a sulfonylurea at screening entered an AHA adjustment phase (up to four weeks) and a dose-stable period (eight weeks), during which background metformin and sulfonylurea therapy was adjusted to comply with the requirements of the study protocol. The AHA adjustment phase could include discontinuation of antihyperglycemic treatments, addition of a new antihyperglycemic treatment, and/or an increase or decrease in the dose of existing metformin and sulfonylurea.
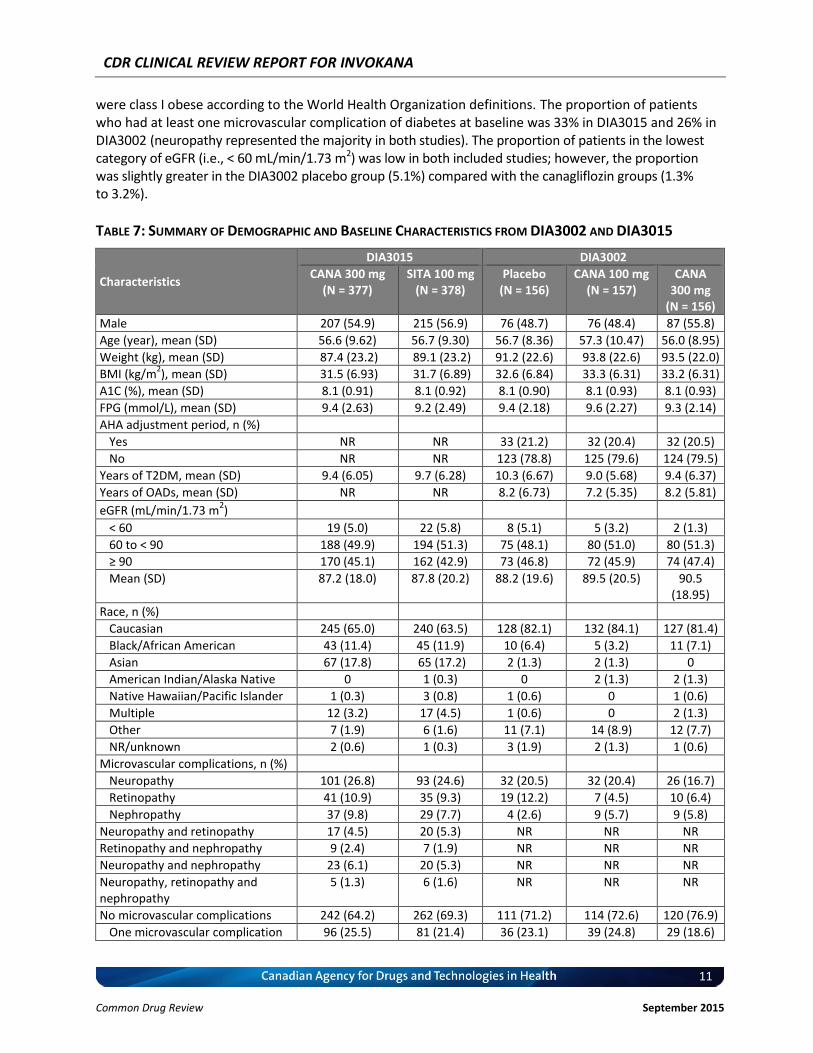
b) Baseline Characteristics The demographic and baseline characteristics of patients in DIA3015 and DIA3002 are summarized in Table 7. Patients in DIA3015 ranged from 21 to 91 years of age; those in DIA3002 ranged in age from 27 to 79 years. The mean age of participants was 56.7 years in both trials. The majority of participants in both studies (95% in DIA3015 and 79.3% in DIA3002) did not require an AHA adjustment phase prior to randomization. The proportion of males was 51% in DIA3002 and 56% in DIA3015. Participants had long-standing type 2 diabetes with the mean duration of diabetes being 9.6 years in both studies. The placebo group of DIA3002 had a slightly longer duration of diabetes (mean of 10.3 years) compared with the canagliflozin groups (mean of 9.0 to 9.4 years). Mean baseline A1C was 8.1% and mean FPG was 9.3 mmol/L in DIA3015 and 9.5 mmol/L in DIA3002. Participants in DIA3002 had a slightly greater mean body weight at baseline (92.8 kg) compared with DIA3015 (88.3 kg). The mean body mass index at baseline was 31.6 kg/m2 in DIA3015 and 33.0 kg/m2 in DIA3002. A majority of study participants (64)
CDR CLINICAL REVIEW REPORT FOR INVOKANA
11
Common Drug Review September 2015
were class I obese according to the World Health Organization definitions. The proportion of patients who had at least one microvascular complication of diabetes at baseline was 33% in DIA3015 and 26% in DIA3002 (neuropathy represented the majority in both studies). The proportion of patients in the lowest category of eGFR (i.e., < 60 mL/min/1.73 m2) was low in both included studies; however, the proportion was slightly greater in the DIA3002 placebo group (5.1%) compared with the canagliflozin groups (1.3% to 3.2%).
TABLE 7: SUMMARY OF DEMOGRAPHIC AND BASELINE CHARACTERISTICS FROM DIA3002 AND DIA3015
Characteristics
DIA3015 DIA3002
CANA 300 mg (N = 377)
SITA 100 mg (N = 378)
Placebo (N = 156)
CANA 100 mg (N = 157)
CANA 300 mg
(N = 156)
Male 207 (54.9) 215 (56.9) 76 (48.7) 76 (48.4) 87 (55.8)
Age (year), mean (SD) 56.6 (9.62) 56.7 (9.30) 56.7 (8.36) 57.3 (10.47) 56.0 (8.95)
Weight (kg), mean (SD) 87.4 (23.2) 89.1 (23.2) 91.2 (22.6) 93.8 (22.6) 93.5 (22.0)
BMI (kg/m2), mean (SD) 31.5 (6.93) 31.7 (6.89) 32.6 (6.84) 33.3 (6.31) 33.2 (6.31)
A1C (%), mean (SD) 8.1 (0.91) 8.1 (0.92) 8.1 (0.90) 8.1 (0.93) 8.1 (0.93)
FPG (mmol/L), mean (SD) 9.4 (2.63) 9.2 (2.49) 9.4 (2.18) 9.6 (2.27) 9.3 (2.14)
AHA adjustment period, n (%)
Yes NR NR 33 (21.2) 32 (20.4) 32 (20.5)
No NR NR 123 (78.8) 125 (79.6) 124 (79.5)
Years of T2DM, mean (SD) 9.4 (6.05) 9.7 (6.28) 10.3 (6.67) 9.0 (5.68) 9.4 (6.37)
Years of OADs, mean (SD) NR NR 8.2 (6.73) 7.2 (5.35) 8.2 (5.81)
eGFR (mL/min/1.73 m2)
< 60 19 (5.0) 22 (5.8) 8 (5.1) 5 (3.2) 2 (1.3)
60 to < 90 188 (49.9) 194 (51.3) 75 (48.1) 80 (51.0) 80 (51.3)
≥ 90 170 (45.1) 162 (42.9) 73 (46.8) 72 (45.9) 74 (47.4)
Mean (SD) 87.2 (18.0) 87.8 (20.2) 88.2 (19.6) 89.5 (20.5) 90.5 (18.95)
Race, n (%)
Caucasian 245 (65.0) 240 (63.5) 128 (82.1) 132 (84.1) 127 (81.4)
Black/African American 43 (11.4) 45 (11.9) 10 (6.4) 5 (3.2) 11 (7.1)
Asian 67 (17.8) 65 (17.2) 2 (1.3) 2 (1.3) 0
American Indian/Alaska Native 0 1 (0.3) 0 2 (1.3) 2 (1.3)
Native Hawaiian/Pacific Islander 1 (0.3) 3 (0.8) 1 (0.6) 0 1 (0.6)
Multiple 12 (3.2) 17 (4.5) 1 (0.6) 0 2 (1.3)
Other 7 (1.9) 6 (1.6) 11 (7.1) 14 (8.9) 12 (7.7)
NR/unknown 2 (0.6) 1 (0.3) 3 (1.9) 2 (1.3) 1 (0.6)
Microvascular complications, n (%)
Neuropathy 101 (26.8) 93 (24.6) 32 (20.5) 32 (20.4) 26 (16.7)
Retinopathy 41 (10.9) 35 (9.3) 19 (12.2) 7 (4.5) 10 (6.4)
Nephropathy 37 (9.8) 29 (7.7) 4 (2.6) 9 (5.7) 9 (5.8)
Neuropathy and retinopathy 17 (4.5) 20 (5.3) NR NR NR
Retinopathy and nephropathy 9 (2.4) 7 (1.9) NR NR NR
Neuropathy and nephropathy 23 (6.1) 20 (5.3) NR NR NR
Neuropathy, retinopathy and nephropathy
5 (1.3) 6 (1.6) NR NR NR
No microvascular complications 242 (64.2) 262 (69.3) 111 (71.2) 114 (72.6) 120 (76.9)
One microvascular complication 96 (25.5) 81 (21.4) 36 (23.1) 39 (24.8) 29 (18.6)

CDR CLINICAL REVIEW REPORT FOR INVOKANA
12
Common Drug Review September 2015
Characteristics
DIA3015 DIA3002
CANA 300 mg (N = 377)
SITA 100 mg (N = 378)
Placebo (N = 156)
CANA 100 mg (N = 157)
CANA 300 mg
(N = 156)
Two microvascular complications 34 (9.0) 29 (7.7) 8 (5.1) 3 (1.9) 5 (3.2)
Three microvascular complications
5 (1.3) 6 (1.6) 1 (0.6) 1 (0.6) 2 (1.3)
A1C = glycated hemoglobin; AHA = antihyperglycemic agent; BMI = body mass index; CANA = canagliflozin; eGFR = estimated glomerular filtration rate; FPG = fasting plasma glucose; NR = not reported; OADs = oral antidiabetes drugs; SD = standard deviation; SITA = sitagliptin; T2DM = type 2 diabetes mellitus. Note: Data from Clinical Study Reports for DIA3002
2 and DIA3015.
3
3.2.3 Interventions In DIA3002, canagliflozin was supplied as capsules containing active tablets (100 mg or 300 mg) and a filler. Placebo was supplied as capsules matching canagliflozin capsules in size and appearance, containing a filler only. In DIA3015, canagliflozin was supplied as capsules containing active tablets (100 mg or 300 mg) and a filler. Commercially available sitagliptin was supplied as capsules containing two 50 mg tablets and a filler, identical in appearance to that used for canagliflozin. 3.2.4 Outcomes a) Glycemic Control The primary efficacy end point was the change from baseline in A1C at 26 weeks (DIA3002) or 52 weeks (DIA3015).11 An analysis of covariance model was used in both studies for the primary end points, with treatment and stratification factors (e.g., whether or not a participant entered the AHA adjustment period) as fixed effects and A1C baseline value as a covariate. Subgroup analyses were conducted on a variety of patient characteristics, including participation in the AHA adjustment period, sex, age group (< 65 years or > 65 years), race, ethnicity, baseline body mass index (< 30 kg/m2 or ≥ 30 kg/m2), baseline A1C (< 8%, 8% to < 9%, or ≥ 9%), and baseline eGFR (< 90 mL/min/1.73 m2 or ≥ 90 mL/min/1.73 m2). DIA3015 and DIA3002 differed with regard to the handling of patients with poor glycemic control during the trial. In DIA3015, patients were to be withdrawn from the trial if they met the glycemic control criteria specified in Table 8. In DIA3002, patients meeting the criteria shown in Table 8 would be provided rescue medication and continued in the study.
TABLE 8: GLYCEMIC RESCUE CRITERIA AND WITHDRAWAL CRITERIA
Time Point Value
Day 1 through week 6 FPG > 270 mg/dL (15 mmol/L)
After week 6 through week 12 FPG > 240 mg/dL (13.3 mmol/L)
After week 12 through week 26 FPG > 200 mg/dL (11.1 mmol/L)
After week 26 A1C > 8.0%
A1C = glycated hemoglobin; FPG = fasting plasma glucose. Note: From DIA3002 and DIA3015 Clinical Study Reports.
3
b) Hypoglycemia Hypoglycemic events were classified as one of the following:
Severe hypoglycemia: defined as those events where the patient required the assistance of another person to recover, lost consciousness, or experienced a seizure (regardless of whether biochemical documentation of a low glucose value was obtained)1

CDR CLINICAL REVIEW REPORT FOR INVOKANA
13
Common Drug Review September 2015
Biochemically documented: events with a plasma glucose cut-off of < 3.9 mmol/L based on the guidelines on clinical investigation for diabetes products from the US FDA and European Medicines Agency (EMA)18,19
Any hypoglycemia: all events that were reported regardless of whether the episode met the criteria for biochemical confirmation and/or severe hypoglycemia.2,3
c) Patient-Reported Outcomes Both DIA3002 and DIA3015 included a number of exploratory patient-reported end points, including the Multidimensional Diabetes Questionnaire, Motivation for Exercise and Diet Questionnaire, Impact of Weight on Quality of Life-Lite, Current Health Satisfaction Questionnaire, Short-Form 36, EuroQol Five Dimensions Questionnaire, and the Diabetes Utility Index. However, all of these outcomes were considered exploratory by the manufacturer and no formal statistical hypotheses were tested as part of the manufacturer’s analysis plan. In the absence of any comparative statistics, these data have not been summarized in the CDR systematic review.
3.2.5 Statistical Analysis In study DIA3015, non-inferiority of canagliflozin 300 mg once daily relative to sitagliptin 100 mg once daily was established if the upper bound of the two-sided 95% confidence interval (CI) for the between-group difference was less than 0.3%. The manufacturer reported that the non-inferiority margin of 0.3% was selected with reference to the values suggested in the FDA and EMA guidance documents for diabetes.19,20 If non-inferiority was established, superiority was tested and concluded if the upper limit of the 95% CI for the difference in least squares means between canagliflozin and sitagliptin was less than 0%.11 The last observation carried forward (LOCF) method was applied when the week 26 values (DIA3002) or week 52 values (DIA3015) were missing. The analyses sets used in DIA3002 and DIA3015 included a modified intention-to-treat (mITT) set, a per-protocol (PP) analysis set, a completers analysis set, and a safety analysis set, as defined below:
mITT analysis set: This set included all randomized participants who took at least one dose of the double-blind study drug. All efficacy analyses were performed on the mITT analysis set.
PP analysis set: This included all mITT participants who completed 26 weeks of treatment in DIA3002 or 52 weeks of treatment in DIA3015 and had no major protocol deviations that may have affected the interpretation of the primary efficacy end point.
Completers analysis set: This included all mITT participants who completed 26 weeks of treatment in DIA3002 or 52 weeks of treatment in DIA3015.
Safety analysis set: This consisted of the same participants as in the mITT analysis set with respect to the allocation of treatment assignment.
Adjustments for multiplicity were conducted to control the type I error at 5% using a predetermined hierarchy. Statistical testing proceeded sequentially conditional on the statistical significance of the prior tests. The testing stopped as soon as any step of the testing sequence failed.
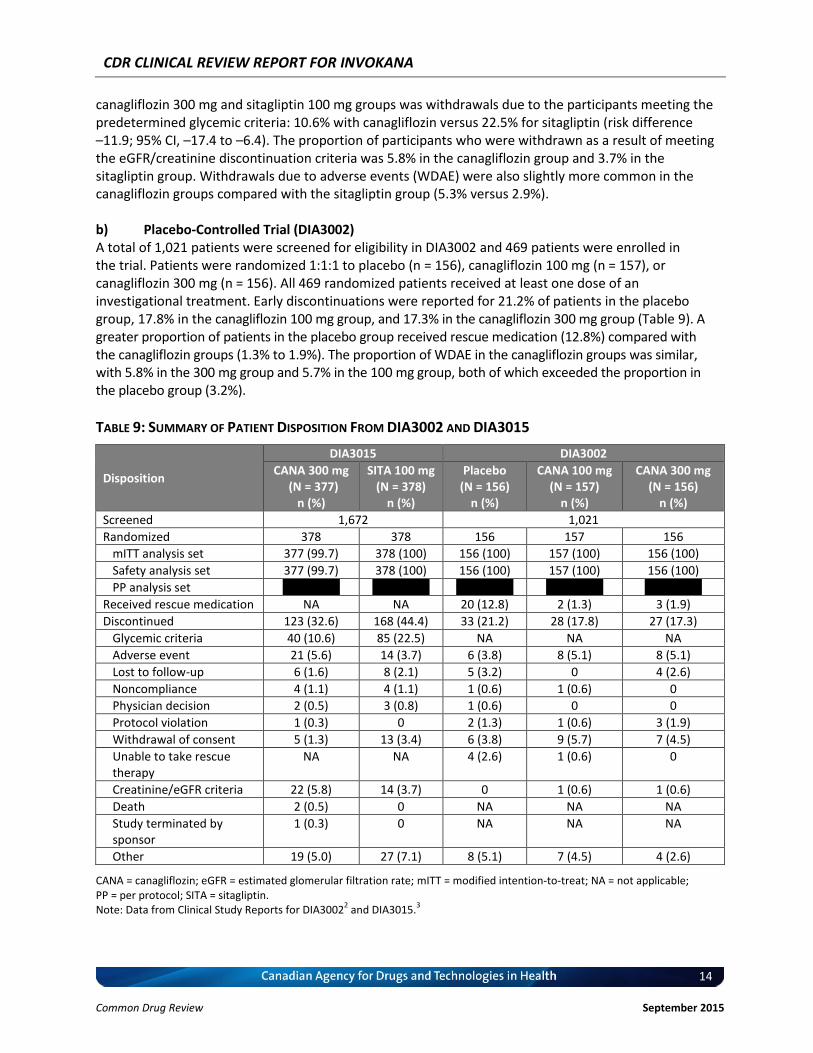
3.3 Patient Disposition a) Active-Controlled Trial (DIA3015) A total of 1,672 patients were screened for eligibility in DIA3015 and 756 patients were enrolled in the trial. Patients were randomized 1:1 to canagliflozin 300 mg (n = 378) or sitagliptin 100 mg (n = 378). Nearly all randomized patients received at least one dose of the investigational treatments (99.9%). Early discontinuations were common, with 32.6% of patients in the canagliflozin 300 mg group withdrawing and 44.4% in the sitagliptin group (Table 9). The largest difference between the
CDR CLINICAL REVIEW REPORT FOR INVOKANA
14
Common Drug Review September 2015
canagliflozin 300 mg and sitagliptin 100 mg groups was withdrawals due to the participants meeting the predetermined glycemic criteria: 10.6% with canagliflozin versus 22.5% for sitagliptin (risk difference –11.9; 95% CI, –17.4 to –6.4). The proportion of participants who were withdrawn as a result of meeting the eGFR/creatinine discontinuation criteria was 5.8% in the canagliflozin group and 3.7% in the sitagliptin group. Withdrawals due to adverse events (WDAE) were also slightly more common in the canagliflozin groups compared with the sitagliptin group (5.3% versus 2.9%). b) Placebo-Controlled Trial (DIA3002) A total of 1,021 patients were screened for eligibility in DIA3002 and 469 patients were enrolled in the trial. Patients were randomized 1:1:1 to placebo (n = 156), canagliflozin 100 mg (n = 157), or canagliflozin 300 mg (n = 156). All 469 randomized patients received at least one dose of an investigational treatment. Early discontinuations were reported for 21.2% of patients in the placebo group, 17.8% in the canagliflozin 100 mg group, and 17.3% in the canagliflozin 300 mg group (Table 9). A greater proportion of patients in the placebo group received rescue medication (12.8%) compared with the canagliflozin groups (1.3% to 1.9%). The proportion of WDAE in the canagliflozin groups was similar, with 5.8% in the 300 mg group and 5.7% in the 100 mg group, both of which exceeded the proportion in the placebo group (3.2%).
TABLE 9: SUMMARY OF PATIENT DISPOSITION FROM DIA3002 AND DIA3015
Disposition
DIA3015 DIA3002
CANA 300 mg (N = 377)
n (%)
SITA 100 mg (N = 378)
n (%)
Placebo (N = 156)
n (%)
CANA 100 mg (N = 157)
n (%)
CANA 300 mg (N = 156)
n (%)
Screened 1,672 1,021
Randomized 378 378 156 157 156
mITT analysis set 377 (99.7) 378 (100) 156 (100) 157 (100) 156 (100)
Safety analysis set 377 (99.7) 378 (100) 156 (100) 157 (100) 156 (100)
PP analysis set vvv vvvvvv vvv vvvvvv vvv vvvvvv vvv vvvvvv vvv vvvvvv
Received rescue medication NA NA 20 (12.8) 2 (1.3) 3 (1.9)
Discontinued 123 (32.6) 168 (44.4) 33 (21.2) 28 (17.8) 27 (17.3)
Glycemic criteria 40 (10.6) 85 (22.5) NA NA NA
Adverse event 21 (5.6) 14 (3.7) 6 (3.8) 8 (5.1) 8 (5.1)
Lost to follow-up 6 (1.6) 8 (2.1) 5 (3.2) 0 4 (2.6)
Noncompliance 4 (1.1) 4 (1.1) 1 (0.6) 1 (0.6) 0
Physician decision 2 (0.5) 3 (0.8) 1 (0.6) 0 0
Protocol violation 1 (0.3) 0 2 (1.3) 1 (0.6) 3 (1.9)
Withdrawal of consent 5 (1.3) 13 (3.4) 6 (3.8) 9 (5.7) 7 (4.5)
Unable to take rescue therapy
NA NA 4 (2.6) 1 (0.6) 0
Creatinine/eGFR criteria 22 (5.8) 14 (3.7) 0 1 (0.6) 1 (0.6)
Death 2 (0.5) 0 NA NA NA
Study terminated by sponsor
1 (0.3) 0 NA NA NA
Other 19 (5.0) 27 (7.1) 8 (5.1) 7 (4.5) 4 (2.6)
CANA = canagliflozin; eGFR = estimated glomerular filtration rate; mITT = modified intention-to-treat; NA = not applicable; PP = per protocol; SITA = sitagliptin.
Note: Data from Clinical Study Reports for DIA30022 and DIA3015.
3

CDR CLINICAL REVIEW REPORT FOR INVOKANA
15
Common Drug Review September 2015
3.4 Exposure to Study Treatments 3.4.1 Investigational Products A summary of exposure to study treatments during the double-blind treatment period is presented in Table 10. Exposure to the investigational treatments was slightly greater in the canagliflozin groups compared with the placebo group in DIA3002 and sitagliptin group in DIA3015.
TABLE 10: DURATION OF EXPOSURE TO INVESTIGATIONAL PRODUCTS
Exposure DIA3015 DIA3002
CANA 300 mg (N = 377)
SITA 100 mg (N = 378)
Placebo (N = 156)
CANA 100 mg (N = 157)
CANA 300 mg (N = 156)
Mean (SD; weeks) 42.6 (15.6) 41.4 (14.9) 22.2 (6.9) 23.7 (5.9) 23.6 (6.1)
Median (weeks) 51.1 51.0 26.0 26.1 26.0
Range (weeks) 0.1 to 55.3 0.1 to 54.7 0.1 to 28.1 0.7 to 28.0 1.4 to 28.9
Total (patient-years)
308.1 300.2 66.4 71.3 70.7
CANA = canagliflozin; SD = standard deviation; SITA = sitagliptin.
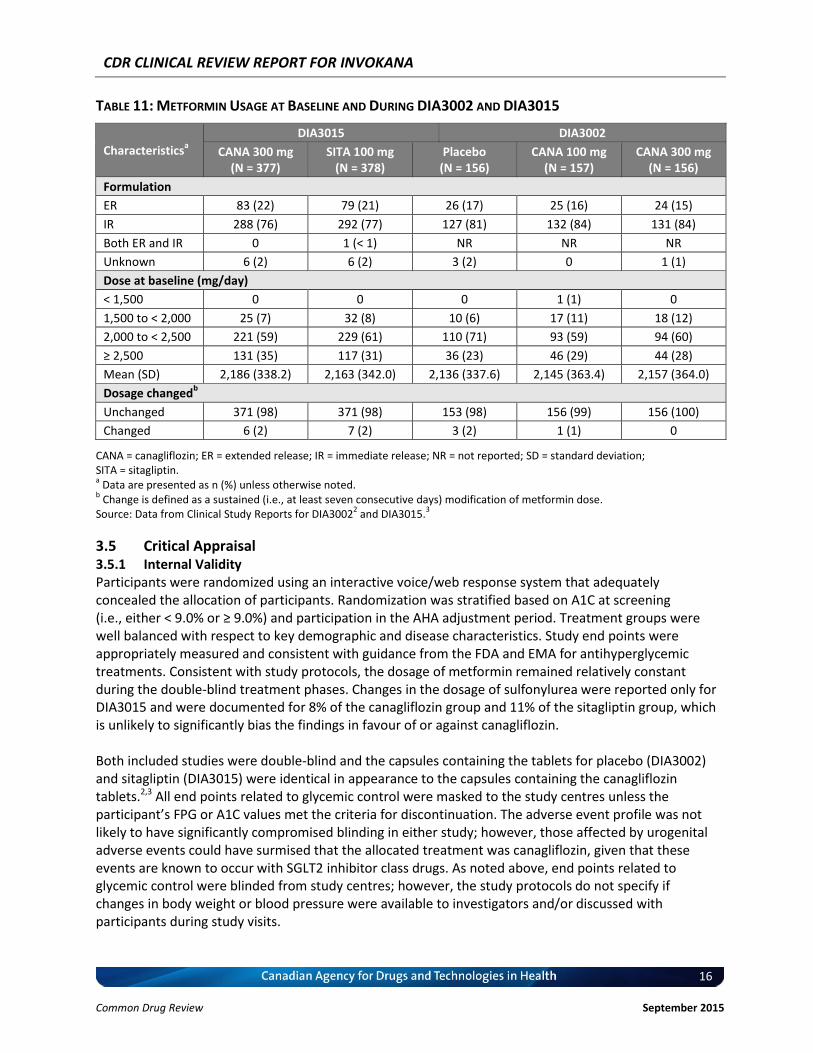
3.4.2 Concomitant Medications Patients were required to be on stable doses of metformin and a sulfonylurea for at least eight weeks prior to randomization in both DIA3002 and DIA3015. The dosages of metformin and sulfonylurea were to remain constant during the double-blind treatment phase; however, the dosage of metformin could be reduced or temporarily interrupted as a result of clinical intolerance, and the dosage of sulfonylurea could be reduced to manage hypoglycemia. The formulation and baseline dosage of metformin and the sulfonylureas are summarized in Table 11, as well as the proportion of patients who had their background therapy adjusted during the trials. In DIA3002 and DIA3015, glyburide (35%) and glimepiride (30%) were the most commonly used sulfonylureas, followed by gliclazide (17% to 19%, including the modified-release formulation) and glipizide (12% to 14%). Changes in background metformin were very rare in both DIA3002 and DIA3015, with 98% to 100% of patients remaining on a consistent dosage. Changes in the dosage of sulfonylurea were only reported for DIA3015 and were documented for 8% of the canagliflozin group and 11% of the sitagliptin group. Nearly all of these adjustments were reductions in the dosage.
CDR CLINICAL REVIEW REPORT FOR INVOKANA
16
Common Drug Review September 2015
TABLE 11: METFORMIN USAGE AT BASELINE AND DURING DIA3002 AND DIA3015
Characteristicsa
DIA3015 DIA3002
CANA 300 mg (N = 377)
SITA 100 mg (N = 378)
Placebo (N = 156)
CANA 100 mg (N = 157)
CANA 300 mg (N = 156)
Formulation
ER 83 (22) 79 (21) 26 (17) 25 (16) 24 (15)
IR 288 (76) 292 (77) 127 (81) 132 (84) 131 (84)
Both ER and IR 0 1 (< 1) NR NR NR
Unknown 6 (2) 6 (2) 3 (2) 0 1 (1)
Dose at baseline (mg/day)
< 1,500 0 0 0 1 (1) 0
1,500 to < 2,000 25 (7) 32 (8) 10 (6) 17 (11) 18 (12)
2,000 to < 2,500 221 (59) 229 (61) 110 (71) 93 (59) 94 (60)
≥ 2,500 131 (35) 117 (31) 36 (23) 46 (29) 44 (28)
Mean (SD) 2,186 (338.2) 2,163 (342.0) 2,136 (337.6) 2,145 (363.4) 2,157 (364.0)
Dosage changedb
Unchanged 371 (98) 371 (98) 153 (98) 156 (99) 156 (100)
Changed 6 (2) 7 (2) 3 (2) 1 (1) 0
CANA = canagliflozin; ER = extended release; IR = immediate release; NR = not reported; SD = standard deviation; SITA = sitagliptin. a Data are presented as n (%) unless otherwise noted.
b Change is defined as a sustained (i.e., at least seven consecutive days) modification of metformin dose.
Source: Data from Clinical Study Reports for DIA30022 and DIA3015.
3
3.5 Critical Appraisal 3.5.1 Internal Validity Participants were randomized using an interactive voice/web response system that adequately concealed the allocation of participants. Randomization was stratified based on A1C at screening (i.e., either < 9.0% or ≥ 9.0%) and participation in the AHA adjustment period. Treatment groups were well balanced with respect to key demographic and disease characteristics. Study end points were appropriately measured and consistent with guidance from the FDA and EMA for antihyperglycemic treatments. Consistent with study protocols, the dosage of metformin remained relatively constant during the double-blind treatment phases. Changes in the dosage of sulfonylurea were reported only for DIA3015 and were documented for 8% of the canagliflozin group and 11% of the sitagliptin group, which is unlikely to significantly bias the findings in favour of or against canagliflozin. Both included studies were double-blind and the capsules containing the tablets for placebo (DIA3002) and sitagliptin (DIA3015) were identical in appearance to the capsules containing the canagliflozin tablets.2,3 All end points related to glycemic control were masked to the study centres unless the participant’s FPG or A1C values met the criteria for discontinuation. The adverse event profile was not likely to have significantly compromised blinding in either study; however, those affected by urogenital adverse events could have surmised that the allocated treatment was canagliflozin, given that these events are known to occur with SGLT2 inhibitor class drugs. As noted above, end points related to glycemic control were blinded from study centres; however, the study protocols do not specify if changes in body weight or blood pressure were available to investigators and/or discussed with participants during study visits.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
17
Common Drug Review September 2015
TABLE 12: SULFONYLUREA USAGE AT BASELINE AND DURING DIA3002 AND DIA3015
Characteristicsa
DIA3015 DIA3002
CANA 300 mg (N = 377)
SITA 100 mg (N = 378)
Placebo (N = 156)
CANA 100 mg (N = 157)
CANA 300 mg (N = 156)
Formulation
Glipizide 47 (12) 40 (11) 18 (12) 21 (13) 24 (15)
Glipizide ER 16 (4) 18 (5) 10 (6) 3 (2) 5 (3)
Glyburide 128 (34) 133 (35) 51 (33) 54 (34) 61 (39)
Glimepiride 121 (32) 106 (28) 46 (29) 50 (32) 45 (29)
Gliclazide 26 (7) 30 (8) 5 (3) 4 (3) 3 (2)
Gliclazide MR 37 (10) 50 (13) 26 (17) 25 (16) 16 (10)
Glyburide micronized 2 (1) 0 NR NR NR
Tolazamide 0 1 (< 1) NR NR NR
Other NR NR 0 0 1 (1)
Dose at baseline
< minimum doseb 7 (2) 5 (1) NR NR NR
≥ minimum doseb 370 (98) 373 (99) NR NR NR
Dosage changed
Unchanged 345 (92) 338 (89) NR NR NR
Changed 32 (8) 40 (11) NR NR NR
Decreased 31 (8) 33 (9) NR NR NR
Increased 3 (1) 5 (1) NR NR NR
Interrupted 0 4 (1) NR NR NR
CANA = canagliflozin; ER = extended release; MR = modified release; NR = not reported; SD = standard deviation; SITA = sitagliptin.
a Data are presented as n (%) unless otherwise noted.
b Sulfonylurea minimum daily dose required was defined as follows: glipizide = 20 mg, glipizide ER = 10 mg, glyburide = 10 mg,
glimepiride = 4 mg, gliclazide = 160 mg, gliclazide MR = 60 mg, glyburide micronized = 6 mg. Source: Data from Clinical Study Reports for DIA3002
2 and DIA3015.
3
The statistical approach used in DIA3015 and DIA3002 was considered by regulatory authorities to be well described and appropriate. Consistent with guidance from regulatory authorities (e.g., EMA), baseline A1C was included as a covariate in the analysis of the primary end point. A number of sensitivity analyses were conducted to support the findings of the primary analysis. Both studies used an appropriate method to control type I error rate when performing multiple statistical analyses. The non-inferiority margin selected in DIA3015 (0.3%) is reflective of guidance from the FDA and EMA and is consistent with other trials conducted for antihyperglycemic treatments. Due to the demonstration of the superiority, the selection of the non-inferiority margin is not particularly relevant for this review. Both DIA3015 and DIA3002 used a modified ITT analysis as opposed to a true ITT analysis; however, only a small number of patients were excluded.
Early discontinuations were common in both DIA3002 and DIA3015. In the 52-week active-controlled trial, 32.6% of participants discontinued in the canagliflozin group and 44.4% discontinued in the sitagliptin group. The large difference between the canagliflozin 300 mg and the sitagliptin 100 mg groups was primarily due to a two-fold increase in withdrawals due to the participants meeting the predetermined glycemic criteria in the sitagliptin group (22.5% versus 10.6%). DIA3015 did not permit the use of rescue medication and those meeting the criteria for poor glycemic control had to be withdrawn from the study; hence, the completion rate in DIA3015 was lower compared with the other

CDR CLINICAL REVIEW REPORT FOR INVOKANA
18
Common Drug Review September 2015
phase 3 studies conducted for canagliflozin (e.g., a 14% completion rate across the 26-week placebo-controlled trial).11 Primary analyses for both DIA3002 and DIA3015 were conducted using LOCF. Given the large number of patients who discontinued early in DIA3015 and the imbalance in discontinuations between the two groups (i.e., 32.6% in the canagliflozin group versus 44.4% in the sitagliptin group), the use of LOCF may provide an explanation for the differences in the ITT and per-protocol analyses for A1C (i.e., –0.37% versus –0.21%). Reviewers for the FDA conducted reanalyses using a mixed-effect model repeat measurement and reported results that were generally consistent with the manufacturer’s LOCF analysis.12 The use of LOCF may have underestimated the effect of canagliflozin in the placebo-controlled trial, as some patients in the placebo group would be coded as being stable at the time of withdrawal rather than allowing their glycemic control to continue to deteriorate over the 26-week study period.
3.5.2 External Validity The patients enrolled in DIA3015 and DIA3002 are representative of the target Canadian population in terms of demography, comorbidities, and disease characteristics. The baseline dosages of metformin and sulfonylureas used in DIA3015 and DIA3002 (see Table 11 and Table 12) were consistent with the inclusion criteria of the trials and reflective of situations where third-line therapy would be considered by physicians in Canada. Patients who were taking metformin and a sulfonylurea at dosages below those specified in the protocol were still eligible for enrolment in DIA3002 and DIA3015 provided they completed the AHA adjustment period and then demonstrated inadequate glycemic control based on A1C. The AHA adjustment period consisted of a forced titration of the protocol-specified concomitant antihyperglycemic drugs for up to four weeks, followed by an eight-week maintenance period. Such forced titrations are unlikely to be reflective of routine clinical practice. Eight weeks of stable doses of medication is at the lower end of the range recommended by the EMA (8 to 12 weeks) to ensure the maximal effect of the previous medication has been achieved and that A1C is stabilized at baseline.20 In DIA3015, only a small minority of participants (approximately 5%) were required to complete the AHA adjustment phase prior to screening. In addition, randomization was stratified by whether or not the patient completed the AHA adjustment phase. The efficacy of canagliflozin was assessed using surrogate end points (e.g., A1C). Both DIA3015 and DIA3002 were of inadequate size or duration to assess the effect of canagliflozin on macrovascular or microvascular complications of diabetes, or on mortality. The relationship between glycemic control as measured by A1C and diabetes-related complications remains controversial, particularly for macrovascular events. These studies were up to 52 weeks in duration (including the extension of phase of DIA3002), which is sufficient to detect differences in the primary end point (i.e., A1C) and several of the key secondary end points (e.g., FPG, body weight, SBP). Although the findings of DIA3002 and DIA3015 may not be indicative of long-term efficacy and safety, the duration and design of these trials is consistent with similar published trials for other members of the classes of antihyperglycemic drugs, including DPP-4 inhibitors and GLP-1 analogues. In DIA3015, both sitagliptin and canagliflozin were provided at the maximum recommended dosages. The final product monograph recommends that the 300 mg dose of canagliflozin be considered for patients tolerating canagliflozin at a dosage of 100 mg once daily who need tighter glycemic control; therefore, the initial 300 mg dosage of canagliflozin used in DIA3015 may have resulted in a larger difference in A1C between canagliflozin and sitagliptin than would be expected in clinical practice when canagliflozin is likely to be initiated a lower dosage.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
19
Common Drug Review September 2015
CADTH’s recommendation for sequential therapy of diabetes is that a basal insulin (such as NPH insulin) be used as third-line therapy for patients whose hyperglycemia is inadequately controlled with metformin and a sulfonylurea. There is no evidence regarding the efficacy of canagliflozin versus a basal insulin for patients who are inadequately controlled using metformin and a sulfonylurea. Both trials involved extensive patient contact with health care professionals (i.e., nine visits in DIA3015 from randomization to end point). In addition, both trials included a single-blind two-week run-in period to ensure compliance with the study protocol and dosage regimen. This is not reflective of routine clinical practice in Canada and may, therefore, reduce generalizability of results to the general population with type 2 diabetes.
3.6 Efficacy 3.6.1 Diabetes-Related Complications and Mortality Neither DIA3015 nor DIA3002 evaluated outcomes related to macrovascular or microvascular complications of type 2 diabetes. 3.6.2 Glycemic Control a) Glycated Hemoglobin Active-Controlled Trial (DIA3015)
After 52 weeks, canagliflozin 300 mg once daily demonstrated non-inferiority and superiority compared with sitagliptin 100 mg once daily for change from baseline in A1C in both the mITT (least squares mean difference [LSMD] –0.37%; 95% CI, –0.50% to –0.25%) and per-protocol data sets (LSMD –0.21%; 95% CI, –0.34% to –0.08%). Differences between groups are presented in Figure 4 and differences within groups are presented in Table 13. For subgroups based on baseline A1C, numerically greater reductions from baseline in A1C were observed in the canagliflozin group compared with the sitagliptin group for patients with higher baseline A1C values, relative to those with lower baseline A1C values. The between-treatment differences were –0.54%, –0.41%, and –0.26% for those with an A1C value of ≥ 9%, 8% to < 9%, and < 8%, respectively. Subgroup analyses by age, sex, ethnicity, or eGFR (< 90 mL/min/1.73 m2 or ≥ 90 mL/min/1.73 m2) demonstrated results that were similar to the primary mITT analysis. A greater proportion of patients treated with canagliflozin 300 mg had an A1C value of less than 7% at week 52 compared with sitagliptin (47.6% versus 35.3%; odds ratio 1.80 [95% CI, 1.30 to 2.48]). The proportion of patients with an A1C of less than 6.5% was similar between the two groups (22.5% with canagliflozin and 18.9% with sitagliptin; odds ratio 1.27 [95% CI, 0.87 to 1.86]). Placebo-Controlled Trial (DIA3002)
Both doses of canagliflozin demonstrated statistically significant (P < 0.001) reductions in A1C relative to placebo in DIA3002. Compared with placebo, the LSMD in change from baseline in A1C was –0.71 (95% CI, –0.90 to –0.52) for canagliflozin 100 mg once daily and –0.92 (95% CI, –1.11 to –0.73) for canagliflozin 300 mg once daily. Results were similar in the per-protocol analysis; however, the effect sizes for canagliflozin compared with placebo were smaller (–0.54% [95% CI, –0.76% to –0.32%] for the 100 mg dose and –0.73% [95% CI, –0.96% to –0.51%] for the 300 mg dose). Compared with placebo (18.0%), a statistically significantly greater proportion of patients had an A1C of less than 7% in the canagliflozin 100 mg group (43.2%) and canagliflozin 300 mg group (56.6%); odds ratio 4.42 (95% CI, 2.48 to 7.87) and 8.80 (95% CI, 4.86 to 15.95), respectively.
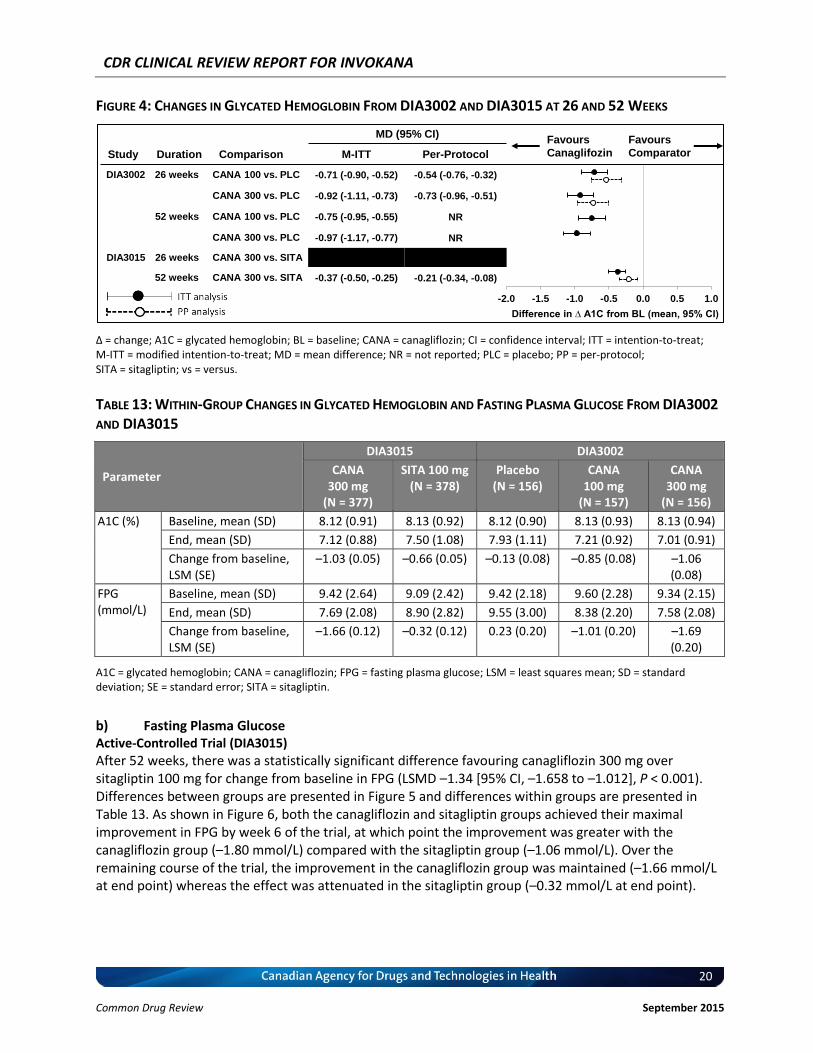
CDR CLINICAL REVIEW REPORT FOR INVOKANA
20
Common Drug Review September 2015
FIGURE 4: CHANGES IN GLYCATED HEMOGLOBIN FROM DIA3002 AND DIA3015 AT 26 AND 52 WEEKS
∆ = change; A1C = glycated hemoglobin; BL = baseline; CANA = canagliflozin; CI = confidence interval; ITT = intention-to-treat; M-ITT = modified intention-to-treat; MD = mean difference; NR = not reported; PLC = placebo; PP = per-protocol; SITA = sitagliptin; vs = versus.
TABLE 13: WITHIN-GROUP CHANGES IN GLYCATED HEMOGLOBIN AND FASTING PLASMA GLUCOSE FROM DIA3002
AND DIA3015
Parameter
DIA3015 DIA3002
CANA 300 mg
(N = 377)
SITA 100 mg (N = 378)
Placebo (N = 156)
CANA 100 mg
(N = 157)
CANA 300 mg
(N = 156)
A1C (%) Baseline, mean (SD) 8.12 (0.91) 8.13 (0.92) 8.12 (0.90) 8.13 (0.93) 8.13 (0.94)
End, mean (SD) 7.12 (0.88) 7.50 (1.08) 7.93 (1.11) 7.21 (0.92) 7.01 (0.91)
Change from baseline, LSM (SE)
–1.03 (0.05) –0.66 (0.05) –0.13 (0.08) –0.85 (0.08) –1.06 (0.08)
FPG (mmol/L)
Baseline, mean (SD) 9.42 (2.64) 9.09 (2.42) 9.42 (2.18) 9.60 (2.28) 9.34 (2.15)
End, mean (SD) 7.69 (2.08) 8.90 (2.82) 9.55 (3.00) 8.38 (2.20) 7.58 (2.08)
Change from baseline, LSM (SE)
–1.66 (0.12) –0.32 (0.12) 0.23 (0.20) –1.01 (0.20) –1.69 (0.20)
A1C = glycated hemoglobin; CANA = canagliflozin; FPG = fasting plasma glucose; LSM = least squares mean; SD = standard deviation; SE = standard error; SITA = sitagliptin.
b) Fasting Plasma Glucose Active-Controlled Trial (DIA3015)
After 52 weeks, there was a statistically significant difference favouring canagliflozin 300 mg over sitagliptin 100 mg for change from baseline in FPG (LSMD –1.34 [95% CI, –1.658 to –1.012], P < 0.001). Differences between groups are presented in Figure 5 and differences within groups are presented in Table 13. As shown in Figure 6, both the canagliflozin and sitagliptin groups achieved their maximal improvement in FPG by week 6 of the trial, at which point the improvement was greater with the canagliflozin group (–1.80 mmol/L) compared with the sitagliptin group (–1.06 mmol/L). Over the remaining course of the trial, the improvement in the canagliflozin group was maintained (–1.66 mmol/L at end point) whereas the effect was attenuated in the sitagliptin group (–0.32 mmol/L at end point).
Study Duration Comparison
MD (95% CI)
M-ITT Per-Protocol
DIA3002 26 weeks CANA 100 vs. PLC -0.71 (-0.90, -0.52) -0.54 (-0.76, -0.32)
CANA 300 vs. PLC -0.92 (-1.11, -0.73) -0.73 (-0.96, -0.51)
52 weeks CANA 100 vs. PLC -0.75 (-0.95, -0.55) NR
CANA 300 vs. PLC -0.97 (-1.17, -0.77) NR
DIA3015 26 weeks CANA 300 vs. SITA XXXXXXXXXXXX XXXXXXXXXXXX
52 weeks CANA 300 vs. SITA -0.37 (-0.50, -0.25) -0.21 (-0.34, -0.08)
Hemoglobin A1C (REDACTED VERSION)
Favours
Comparator
Favours
Canaglifozin
-2.0 -1.5 -1.0 -0.5 0.0 0.5 1.0
Difference in ∆ A1C from BL (mean, 95% CI)
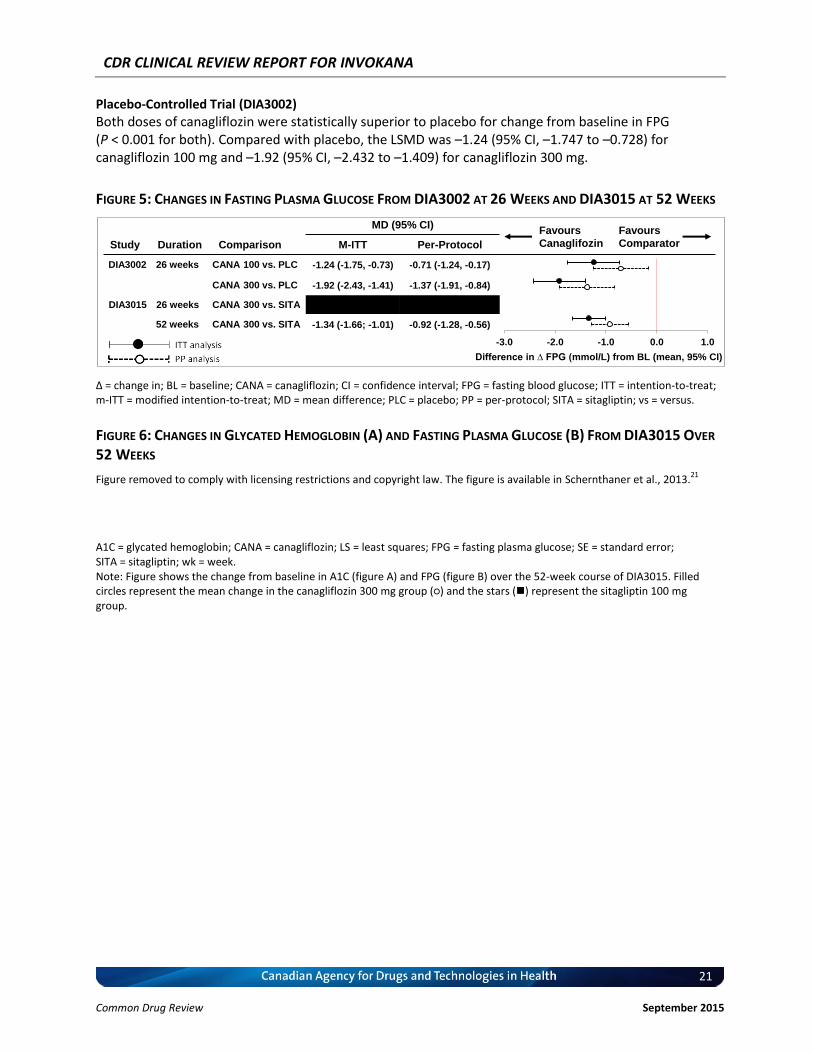
CDR CLINICAL REVIEW REPORT FOR INVOKANA
21
Common Drug Review September 2015
Placebo-Controlled Trial (DIA3002)
Both doses of canagliflozin were statistically superior to placebo for change from baseline in FPG (P < 0.001 for both). Compared with placebo, the LSMD was –1.24 (95% CI, –1.747 to –0.728) for canagliflozin 100 mg and –1.92 (95% CI, –2.432 to –1.409) for canagliflozin 300 mg.
FIGURE 5: CHANGES IN FASTING PLASMA GLUCOSE FROM DIA3002 AT 26 WEEKS AND DIA3015 AT 52 WEEKS
∆ = change in; BL = baseline; CANA = canagliflozin; CI = confidence interval; FPG = fasting blood glucose; ITT = intention-to-treat; m-ITT = modified intention-to-treat; MD = mean difference; PLC = placebo; PP = per-protocol; SITA = sitagliptin; vs = versus.
FIGURE 6: CHANGES IN GLYCATED HEMOGLOBIN (A) AND FASTING PLASMA GLUCOSE (B) FROM DIA3015 OVER
52 WEEKS
Figure removed to comply with licensing restrictions and copyright law. The figure is available in Schernthaner et al., 2013.21
A1C = glycated hemoglobin; CANA = canagliflozin; LS = least squares; FPG = fasting plasma glucose; SE = standard error; SITA = sitagliptin; wk = week. Note: Figure shows the change from baseline in A1C (figure A) and FPG (figure B) over the 52-week course of DIA3015. Filled circles represent the mean change in the canagliflozin 300 mg group (○) and the stars () represent the sitagliptin 100 mg group.
Study Duration Comparison
MD (95% CI)
M-ITT Per-Protocol
DIA3002 26 weeks CANA 100 vs. PLC -1.24 (-1.75, -0.73) -0.71 (-1.24, -0.17)
CANA 300 vs. PLC -1.92 (-2.43, -1.41) -1.37 (-1.91, -0.84)
DIA3015 26 weeks CANA 300 vs. SITA XXXXXXXXXXX XXXXXXXXXXX
52 weeks CANA 300 vs. SITA -1.34 (-1.66; -1.01) -0.92 (-1.28, -0.56)
Favours
Comparator
Favours
Canaglifozin
-3.0 -2.0 -1.0 0.0 1.0
Difference in ∆ FPG (mmol/L) from BL (mean, 95% CI)
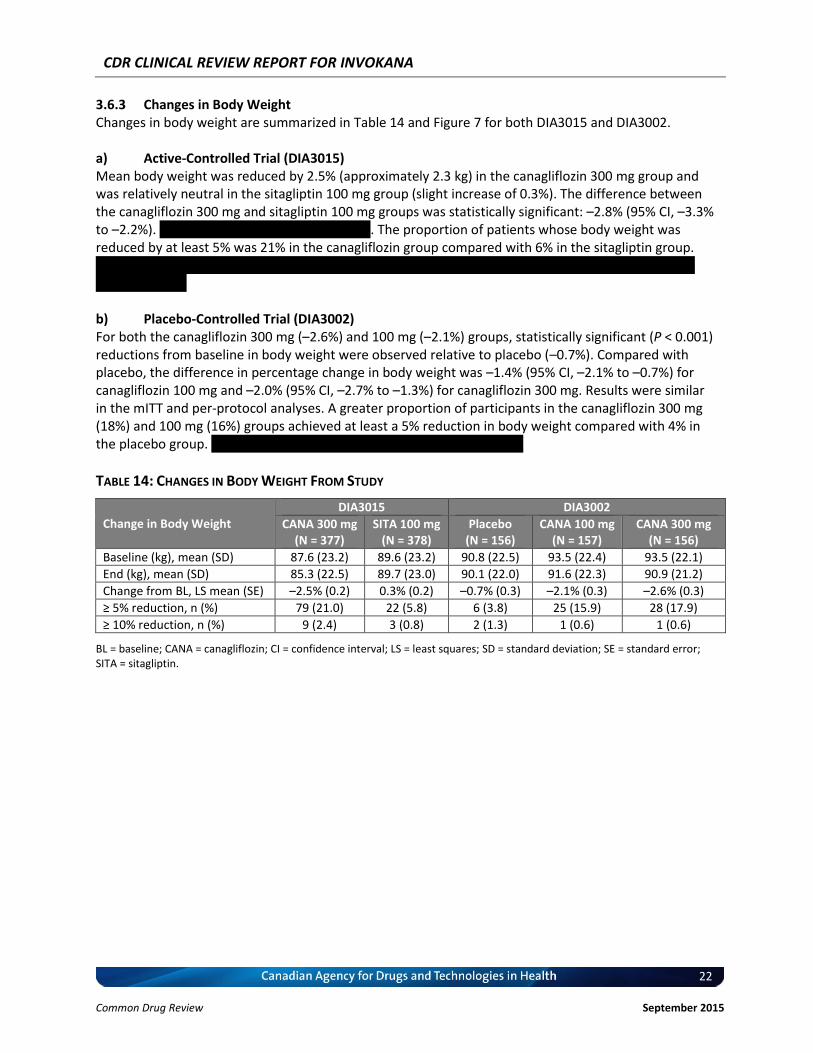
CDR CLINICAL REVIEW REPORT FOR INVOKANA
22
Common Drug Review September 2015
3.6.3 Changes in Body Weight Changes in body weight are summarized in Table 14 and Figure 7 for both DIA3015 and DIA3002. a) Active-Controlled Trial (DIA3015) Mean body weight was reduced by 2.5% (approximately 2.3 kg) in the canagliflozin 300 mg group and was relatively neutral in the sitagliptin 100 mg group (slight increase of 0.3%). The difference between the canagliflozin 300 mg and sitagliptin 100 mg groups was statistically significant: –2.8% (95% CI, –3.3% to –2.2%). ....... .... ....... .. ... .... ... ............ ......... The proportion of patients whose body weight was reduced by at least 5% was 21% in the canagliflozin group compared with 6% in the sitagliptin group. .......... .. .. ..... ... .... .... .. .... ....... ........ .......... .... ........ .. ... ............. ..... .. . .. ........ . .... ......... ........ .... ... ........... ..... .. . .. b) Placebo-Controlled Trial (DIA3002) For both the canagliflozin 300 mg (–2.6%) and 100 mg (–2.1%) groups, statistically significant (P < 0.001) reductions from baseline in body weight were observed relative to placebo (–0.7%). Compared with placebo, the difference in percentage change in body weight was –1.4% (95% CI, –2.1% to –0.7%) for canagliflozin 100 mg and –2.0% (95% CI, –2.7% to –1.3%) for canagliflozin 300 mg. Results were similar in the mITT and per-protocol analyses. A greater proportion of participants in the canagliflozin 300 mg (18%) and 100 mg (16%) groups achieved at least a 5% reduction in body weight compared with 4% in the placebo group. ....... .. ........ .......... .. .... ...... .. .. ..... ... .... .... .. ... .......
TABLE 14: CHANGES IN BODY WEIGHT FROM STUDY
Change in Body Weight
DIA3015 DIA3002
CANA 300 mg (N = 377)
SITA 100 mg (N = 378)
Placebo (N = 156)
CANA 100 mg (N = 157)
CANA 300 mg (N = 156)
Baseline (kg), mean (SD) 87.6 (23.2) 89.6 (23.2) 90.8 (22.5) 93.5 (22.4) 93.5 (22.1)
End (kg), mean (SD) 85.3 (22.5) 89.7 (23.0) 90.1 (22.0) 91.6 (22.3) 90.9 (21.2)
Change from BL, LS mean (SE) –2.5% (0.2) 0.3% (0.2) –0.7% (0.3) –2.1% (0.3) –2.6% (0.3)
≥ 5% reduction, n (%) 79 (21.0) 22 (5.8) 6 (3.8) 25 (15.9) 28 (17.9)
≥ 10% reduction, n (%) 9 (2.4) 3 (0.8) 2 (1.3) 1 (0.6) 1 (0.6)
BL = baseline; CANA = canagliflozin; CI = confidence interval; LS = least squares; SD = standard deviation; SE = standard error; SITA = sitagliptin.
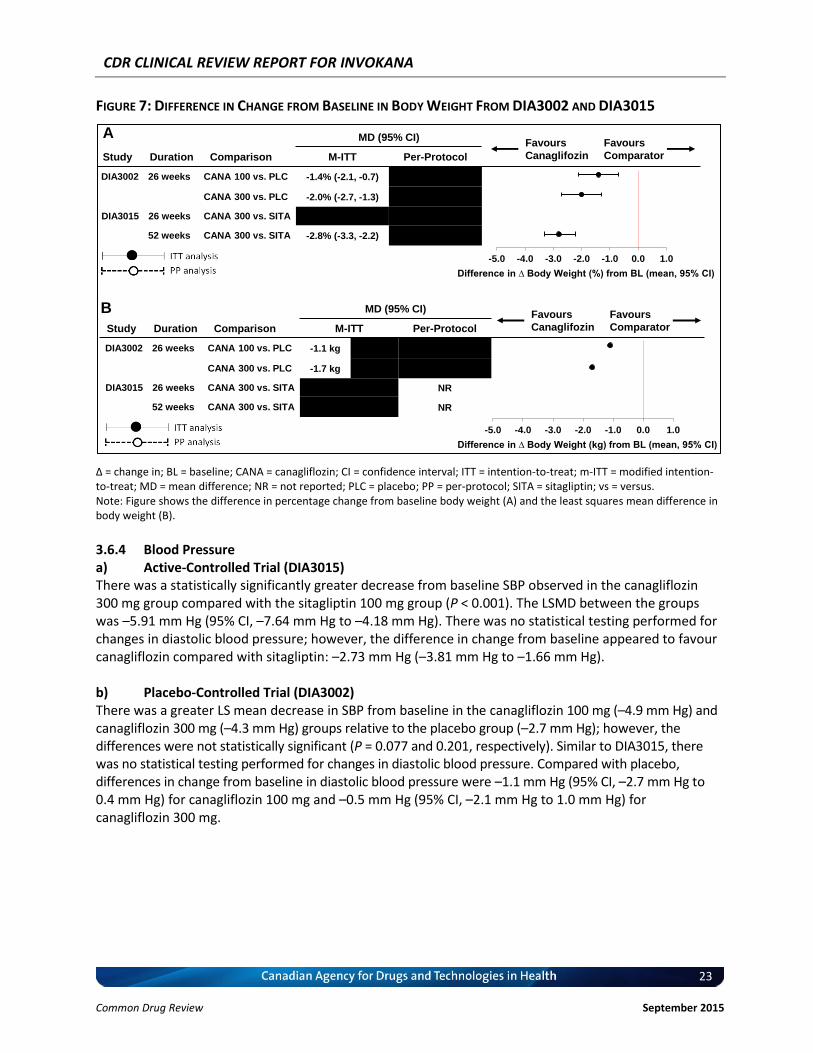
CDR CLINICAL REVIEW REPORT FOR INVOKANA
23
Common Drug Review September 2015
FIGURE 7: DIFFERENCE IN CHANGE FROM BASELINE IN BODY WEIGHT FROM DIA3002 AND DIA3015
∆ = change in; BL = baseline; CANA = canagliflozin; CI = confidence interval; ITT = intention-to-treat; m-ITT = modified intention-to-treat; MD = mean difference; NR = not reported; PLC = placebo; PP = per-protocol; SITA = sitagliptin; vs = versus. Note: Figure shows the difference in percentage change from baseline body weight (A) and the least squares mean difference in body weight (B).
3.6.4 Blood Pressure a) Active-Controlled Trial (DIA3015) There was a statistically significantly greater decrease from baseline SBP observed in the canagliflozin 300 mg group compared with the sitagliptin 100 mg group (P < 0.001). The LSMD between the groups was –5.91 mm Hg (95% CI, –7.64 mm Hg to –4.18 mm Hg). There was no statistical testing performed for changes in diastolic blood pressure; however, the difference in change from baseline appeared to favour canagliflozin compared with sitagliptin: –2.73 mm Hg (–3.81 mm Hg to –1.66 mm Hg). b) Placebo-Controlled Trial (DIA3002) There was a greater LS mean decrease in SBP from baseline in the canagliflozin 100 mg (–4.9 mm Hg) and canagliflozin 300 mg (–4.3 mm Hg) groups relative to the placebo group (–2.7 mm Hg); however, the differences were not statistically significant (P = 0.077 and 0.201, respectively). Similar to DIA3015, there was no statistical testing performed for changes in diastolic blood pressure. Compared with placebo, differences in change from baseline in diastolic blood pressure were –1.1 mm Hg (95% CI, –2.7 mm Hg to 0.4 mm Hg) for canagliflozin 100 mg and –0.5 mm Hg (95% CI, –2.1 mm Hg to 1.0 mm Hg) for canagliflozin 300 mg.
-5.0 -4.0 -3.0 -2.0 -1.0 0.0 1.0
Difference in ∆ Body Weight (kg) from BL (mean, 95% CI)
-5.0 -4.0 -3.0 -2.0 -1.0 0.0 1.0
Difference in ∆ Body Weight (%) from BL (mean, 95% CI)
Study Duration Comparison
MD (95% CI)
M-ITT Per-Protocol
DIA3002 26 weeks CANA 100 vs. PLC -1.4% (-2.1, -0.7) xxxxxxxxxxx
CANA 300 vs. PLC -2.0% (-2.7, -1.3) xxxxxxxxxxx
DIA3015 26 weeks CANA 300 vs. SITA xxxxxxxxxxxxxx xxxxxxxxxxx
52 weeks CANA 300 vs. SITA -2.8% (-3.3, -2.2) xxxxxxxxxxxx
Favours
Comparator
Favours
Canaglifozin
Study Duration Comparison
MD (95% CI)
M-ITT Per-Protocol
DIA3002 26 weeks CANA 100 vs. PLC -1.1 kg (xxxxx) xxxxxxxxxxxx
CANA 300 vs. PLC -1.7 kg (xxxxx) xxxxxxxxxxxx
DIA3015 26 weeks CANA 300 vs. SITA xxxxxxxxxxxx NR
52 weeks CANA 300 vs. SITA xxxxxxxxxxxx NR
Favours
Comparator
Favours
Canaglifozin
A
B
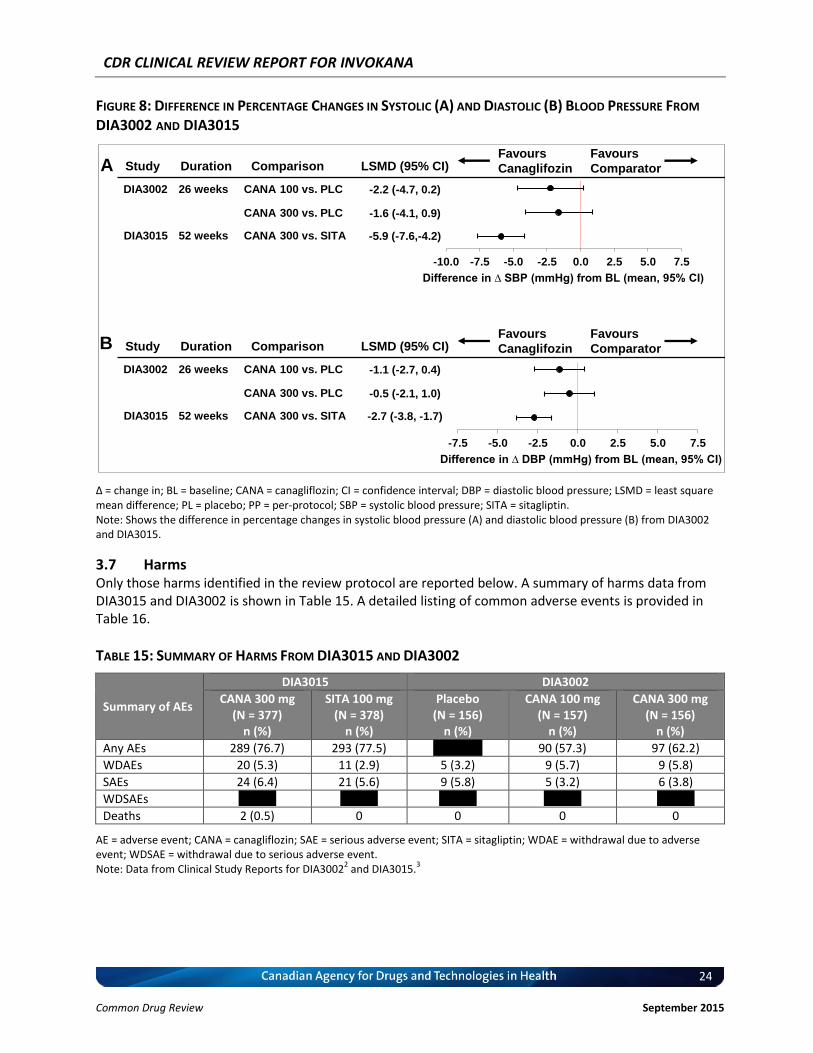
CDR CLINICAL REVIEW REPORT FOR INVOKANA
24
Common Drug Review September 2015
FIGURE 8: DIFFERENCE IN PERCENTAGE CHANGES IN SYSTOLIC (A) AND DIASTOLIC (B) BLOOD PRESSURE FROM
DIA3002 AND DIA3015
∆ = change in; BL = baseline; CANA = canagliflozin; CI = confidence interval; DBP = diastolic blood pressure; LSMD = least square mean difference; PL = placebo; PP = per-protocol; SBP = systolic blood pressure; SITA = sitagliptin. Note: Shows the difference in percentage changes in systolic blood pressure (A) and diastolic blood pressure (B) from DIA3002 and DIA3015.
3.7 Harms Only those harms identified in the review protocol are reported below. A summary of harms data from DIA3015 and DIA3002 is shown in Table 15. A detailed listing of common adverse events is provided in Table 16.
TABLE 15: SUMMARY OF HARMS FROM DIA3015 AND DIA3002
Summary of AEs
DIA3015 DIA3002
CANA 300 mg (N = 377)
n (%)
SITA 100 mg (N = 378)
n (%)
Placebo (N = 156)
n (%)
CANA 100 mg (N = 157)
n (%)
CANA 300 mg (N = 156)
n (%)
Any AEs 289 (76.7) 293 (77.5) xx xxxxxx 90 (57.3) 97 (62.2)
WDAEs 20 (5.3) 11 (2.9) 5 (3.2) 9 (5.7) 9 (5.8)
SAEs 24 (6.4) 21 (5.6) 9 (5.8) 5 (3.2) 6 (3.8)
WDSAEs x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Deaths 2 (0.5) 0 0 0 0
AE = adverse event; CANA = canagliflozin; SAE = serious adverse event; SITA = sitagliptin; WDAE = withdrawal due to adverse event; WDSAE = withdrawal due to serious adverse event.
Note: Data from Clinical Study Reports for DIA30022 and DIA3015.
3
Study Duration Comparison LSMD (95% CI)
DIA3002 26 weeks CANA 100 vs. PLC -2.2 (-4.7, 0.2)
CANA 300 vs. PLC -1.6 (-4.1, 0.9)
DIA3015 52 weeks CANA 300 vs. SITA -5.9 (-7.6,-4.2)
Favours
Comparator
Favours
Canaglifozin
-10.0 -7.5 -5.0 -2.5 0.0 2.5 5.0 7.5
Difference in ∆ SBP (mmHg) from BL (mean, 95% CI)
Study Duration Comparison LSMD (95% CI)
DIA3002 26 weeks CANA 100 vs. PLC -1.1 (-2.7, 0.4)
CANA 300 vs. PLC -0.5 (-2.1, 1.0)
DIA3015 52 weeks CANA 300 vs. SITA -2.7 (-3.8, -1.7)
Favours
Comparator
Favours
Canaglifozin
-7.5 -5.0 -2.5 0.0 2.5 5.0 7.5
Difference in ∆ DBP (mmHg) from BL (mean, 95% CI)
A
B
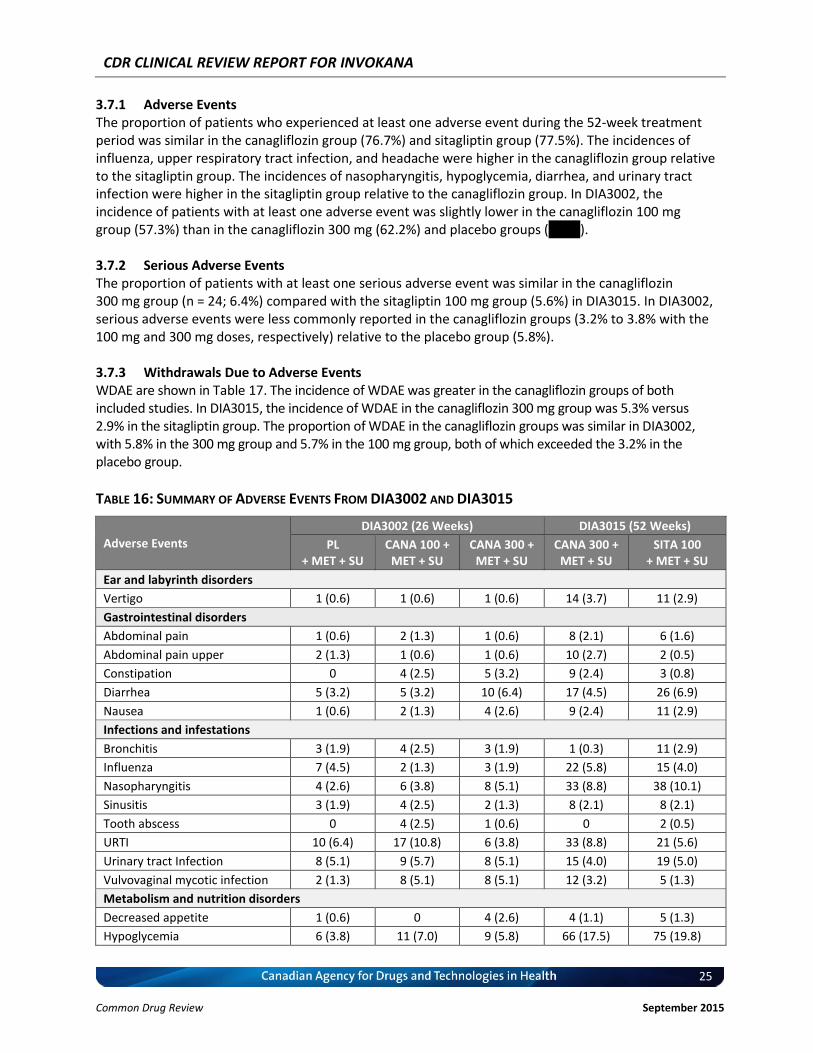
CDR CLINICAL REVIEW REPORT FOR INVOKANA
25
Common Drug Review September 2015
3.7.1 Adverse Events The proportion of patients who experienced at least one adverse event during the 52-week treatment period was similar in the canagliflozin group (76.7%) and sitagliptin group (77.5%). The incidences of influenza, upper respiratory tract infection, and headache were higher in the canagliflozin group relative to the sitagliptin group. The incidences of nasopharyngitis, hypoglycemia, diarrhea, and urinary tract infection were higher in the sitagliptin group relative to the canagliflozin group. In DIA3002, the incidence of patients with at least one adverse event was slightly lower in the canagliflozin 100 mg group (57.3%) than in the canagliflozin 300 mg (62.2%) and placebo groups (xxxxx). 3.7.2 Serious Adverse Events The proportion of patients with at least one serious adverse event was similar in the canagliflozin 300 mg group (n = 24; 6.4%) compared with the sitagliptin 100 mg group (5.6%) in DIA3015. In DIA3002, serious adverse events were less commonly reported in the canagliflozin groups (3.2% to 3.8% with the 100 mg and 300 mg doses, respectively) relative to the placebo group (5.8%). 3.7.3 Withdrawals Due to Adverse Events WDAE are shown in Table 17. The incidence of WDAE was greater in the canagliflozin groups of both included studies. In DIA3015, the incidence of WDAE in the canagliflozin 300 mg group was 5.3% versus 2.9% in the sitagliptin group. The proportion of WDAE in the canagliflozin groups was similar in DIA3002, with 5.8% in the 300 mg group and 5.7% in the 100 mg group, both of which exceeded the 3.2% in the placebo group.
TABLE 16: SUMMARY OF ADVERSE EVENTS FROM DIA3002 AND DIA3015
Adverse Events
DIA3002 (26 Weeks) DIA3015 (52 Weeks)
PL + MET + SU
CANA 100 + MET + SU
CANA 300 + MET + SU
CANA 300 + MET + SU
SITA 100 + MET + SU
Ear and labyrinth disorders
Vertigo 1 (0.6) 1 (0.6) 1 (0.6) 14 (3.7) 11 (2.9)
Gastrointestinal disorders
Abdominal pain 1 (0.6) 2 (1.3) 1 (0.6) 8 (2.1) 6 (1.6)
Abdominal pain upper 2 (1.3) 1 (0.6) 1 (0.6) 10 (2.7) 2 (0.5)
Constipation 0 4 (2.5) 5 (3.2) 9 (2.4) 3 (0.8)
Diarrhea 5 (3.2) 5 (3.2) 10 (6.4) 17 (4.5) 26 (6.9)
Nausea 1 (0.6) 2 (1.3) 4 (2.6) 9 (2.4) 11 (2.9)
Infections and infestations
Bronchitis 3 (1.9) 4 (2.5) 3 (1.9) 1 (0.3) 11 (2.9)
Influenza 7 (4.5) 2 (1.3) 3 (1.9) 22 (5.8) 15 (4.0)
Nasopharyngitis 4 (2.6) 6 (3.8) 8 (5.1) 33 (8.8) 38 (10.1)
Sinusitis 3 (1.9) 4 (2.5) 2 (1.3) 8 (2.1) 8 (2.1)
Tooth abscess 0 4 (2.5) 1 (0.6) 0 2 (0.5)
URTI 10 (6.4) 17 (10.8) 6 (3.8) 33 (8.8) 21 (5.6)
Urinary tract Infection 8 (5.1) 9 (5.7) 8 (5.1) 15 (4.0) 19 (5.0)
Vulvovaginal mycotic infection 2 (1.3) 8 (5.1) 8 (5.1) 12 (3.2) 5 (1.3)
Metabolism and nutrition disorders
Decreased appetite 1 (0.6) 0 4 (2.6) 4 (1.1) 5 (1.3)
Hypoglycemia 6 (3.8) 11 (7.0) 9 (5.8) 66 (17.5) 75 (19.8)

CDR CLINICAL REVIEW REPORT FOR INVOKANA
26
Common Drug Review September 2015
Adverse Events
DIA3002 (26 Weeks) DIA3015 (52 Weeks)
PL + MET + SU
CANA 100 + MET + SU
CANA 300 + MET + SU
CANA 300 + MET + SU
SITA 100 + MET + SU
Musculoskeletal and connective tissue disorders
Arthralgia 4 (2.6) 7 (4.5) 7 (4.5) 17 (4.5) 8 (2.1)
Back pain 4 (2.6) 2 (1.3) 5 (3.2) 8 (2.1) 15 (4.0)
Musculoskeletal pain 1 (0.6) 0 3 (1.9) 8 (2.1) 6 (1.6)
Nervous system disorders
Headache 4 (2.6) 5 (3.2) 2 (1.3) 29 (7.7) 27 (7.1)
Renal and urinary disorders
Pollakiuria 1 (0.6) 4 (2.5) 3 (1.9) 6 (1.6) 5 (1.3)
Reproductive system and breast disorders
Vulvovaginal pruritus 0 1 (0.6) 3 (1.9) 15 (4.0) 1 (0.3)
CANA = canagliflozin; MET = metformin; PL = placebo; SITA = sitagliptin; SU = sulfonylurea. Note: Data from canagliflozin product monograph.
1
TABLE 17: SUMMARY OF WITHDRAWALS DUE TO ADVERSE EVENTS FROM DIA3015 AND DIA3002
WDAEs by SOC
DIA3015 DIA3002
CANA 300 mg
(N = 377) n (%)
SITA 100 mg (N = 378)
n (%)
Placebo (N = 156)
n (%)
CANA 100 mg (N = 157)
n (%)
CANA 300 mg
(N = 156) n (%)
Total WDAEs 20 (5.3) 11 (2.9) 5 (3.2) 9 (5.7) 9 (5.8)
Cardiac disorders x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Ear and labyrinth disorders x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Gastrointestinal disorders x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
General disorders x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Hepatobiliary disorders x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Infections and infestations x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Investigations x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Metabolism/nutrition disorders x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Neoplasms x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Nervous system disorders x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Psychiatric disorders x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Renal and urinary disorders x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Reproductive/breast disorders x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Skin/subcutaneous tissue disorders x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
CANA = canagliflozin; SITA = sitagliptin; WDAE = withdrawal due to adverse event.
3.7.4 Hypoglycemia a) Active-Controlled Trial (DIA3015) The incidence of hypoglycemia was similar between the canagliflozin 300 mg and sitagliptin 100 mg groups. At least one episode of overall hypoglycemia was reported for 43.2% of patients in the canagliflozin group and 40.7% in the sitagliptin group. Events classified as severe hypoglycemia were reported for 4.0% of patients in the canagliflozin group and 3.4% in the sitagliptin group.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
27
Common Drug Review September 2015
b) Placebo-Controlled Trial (DIA3002) Hypoglycemia was more commonly reported in the canagliflozin groups than in the placebo group. The incidence of any hypoglycemia was 30.1% and 27.4% for the canagliflozin 300 mg and 100 mg groups, respectively, compared with 15.4% in the placebo group. Severe hypoglycemia was rare in DIA3002 with just one event reported in the placebo and canagliflozin 100 mg groups, and no events in the canagliflozin 300 mg group.
TABLE 18: SUMMARY OF HYPOGLYCEMIA FROM DIA3002 AND DIA3015
Hypoglycemia
DIA3015 DIA3002
CANA 300 mg
(N = 377) n (%)
SITA 100 mg (N = 378)
n (%)
Placebo (N = 156)
n (%)
CANA 100 mg
(N = 157) n (%)
CANA 300 mg (N = 156)
n (%)
Any hypoglycemia 163 (43.2) 154 (40.7) 24 (15.4) 43 (27.4) 47 (30.1)
Severe hypoglycemia 15 (4.0) 13 (3.4) 1 (0.6) 1 (0.6) 0
Patients with 1 episode 45 (11.9) 46 (12.2) 13 (8.3) 12 (7.6) 15 (9.6)
Patients with 2 episodes 14 (3.7) 20 (5.3) 3 (1.9) 10 (6.4) 9 (5.8)
Patients with ≥ 3 episodes 104 (27.6) 88 (23.3) 8 (5.1) 21 (13.4) 23 (14.7)
Events per patient-year 4.14 3.81 1.04 2.58 3.38
CANA = canagliflozin; SITA = sitagliptin.
Note: Data from Clinical Study Reports for DIA30022 and DIA3015.
3
3.7.5 Urogenital Adverse Events The incidence and duration of urogenital adverse events are summarized in Table 19 for women and Table 20 for men. a) Active-Controlled Trial (DIA3015) The incidences of vulvovaginal adverse events were higher in the canagliflozin 300 mg group compared with the sitagliptin group (15.3% versus 4.3%). xxxxxxxxx xx xx xxxxx xxxxx xx xxx xxxxxxxxxxxxx xxxxx xxxx
xxxxxxxxxxxxxx xxxxxxx xxxxxx xxx xx xxxxx xxxxxxx xx xxxxxxx xxxxx xxxxxxxxxx xx xxx xxxxxxxxxxxxx xxxxxx xxx xxxxxxxxxxxxxx xxxxxxx xxxxxxx xxx xxxx xxxx xx xxxxx xxxxxxxxxxxxxxxxxx xxx xx xxxxx xxxx xxxx xxxxxx xxxxxxxx xxxxxx xxx xxxxx x xxxxx xx xxxxxxxxx xxxx xxxxxxxxxxxxxx xxx xxxxx xxxxxxx xxxxxxx xxx xxxx xxxxxxxx xx xxxxxxx xxxxxxxx xxx xx xxxx
xxxxxxx xx xx xxxxxx xxx xxxx xxxxxxxx xx xxx xxxxxxxxxxxxxx xxxxxxx xxxxxx xxx xx xxxx xxxxxxx xx xx xxxxxx xxx xx xxx xxxxxxx
xxxxxx xx xxxxxx xxxxxxx xxxxxxxxxx xxxx xxxx xx xxxxxxxx xx xxxxxxxx xxxx xxx xxxxxxxxx xx xxx xxxxxx xxxxxx None of the 26 patients in the canagliflozin group withdrew as a result of these adverse events. There was a higher incidence of superficial genital infections in men in the canagliflozin 300 mg group compared with the sitagliptin 100 mg group (9.2% versus 0.5%). xxxxxxx xx xxx xx xxx xxxxxxx xx xxx xxxxxxxxxxxxx xxxxx xxxx xx xxxxxxx xxxxx xx xxxxxxxxxxx xxxxxxx xxxxxxxxx xxxx xxxxxxxxxxxxx xxx x xx xx xxxxx xxx x xxxxxxx xxxxxxx xx xxxxxxxxx xx xxxxxxxxxxxxxxx xxxxxx xxx x xxxxx xxxxx xx xxxxxxxx xxx xxxxxx xxx xxxx xxxx xx xxx
xxxxx xxxxx xxx xxxxxxxxxxxxx xx xxxxx xxxx xxxx xxxxxxx xxxxxx xxxxxxxx xx xxxxx xx xx xxxxx xxx xxxx x xxxx xxxxxxxx xx xxx
xxxxxxx xxxxxx xx xx xxxx xxxxxxx xx xx xxxxxx xxx xxxx xxxxxxxx xx xxxxxxxx xxx xx xxxx xxxxxxx xx x xxxxx All adverse events were reported as mild or moderate in severity; however, one patient in the canagliflozin group discontinued due to an adverse event of balanoposthitis. b) Placebo-Controlled Trial (DIA3002) The incidences of vulvovaginal adverse events were higher in the two canagliflozin groups compared with the placebo group, with a higher incidence in the canagliflozin 300 mg group compared with the
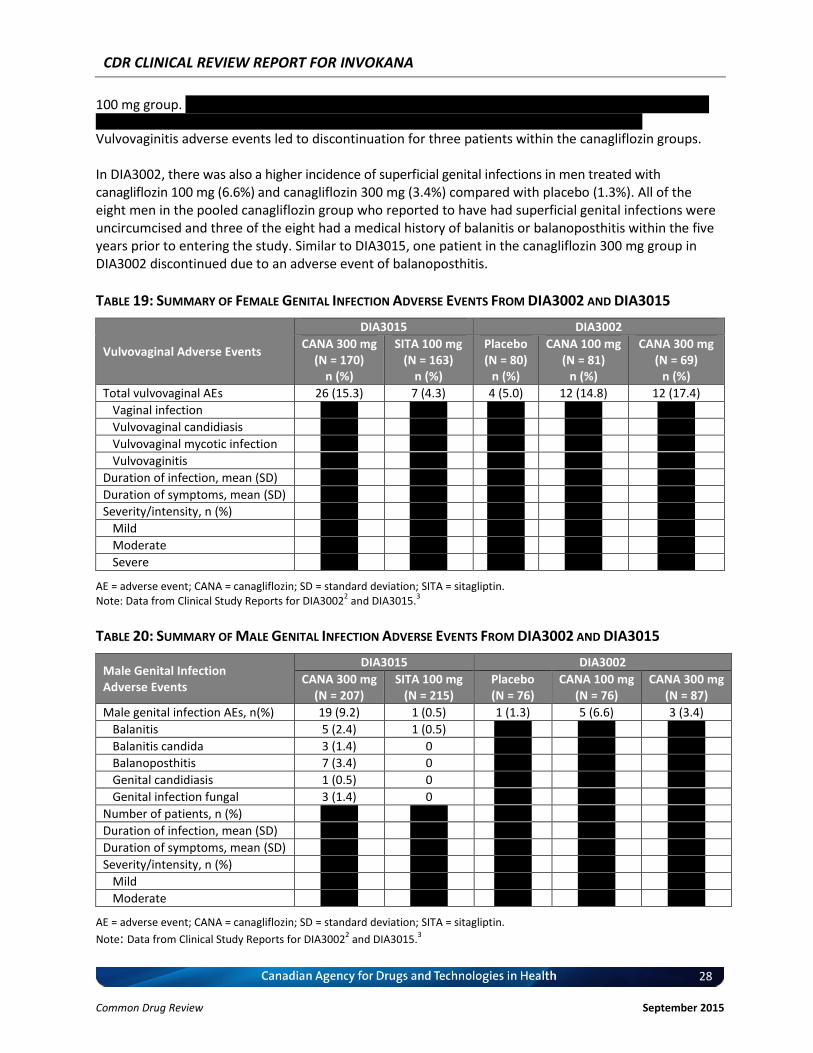
CDR CLINICAL REVIEW REPORT FOR INVOKANA
28
Common Drug Review September 2015
100 mg group. xxx xxxxxxxxxxxxxx xxxxxxx xxxxxxx xxx xxxx xxxxxxxx xx xxxxxxx xxxxxxxx xxx xx xxxx xxxxxxx xx xx
xxxxxx xxx xxx xxx xx xxx xxxxxxx xxxxxx xx xxxxxx xxxxxxx xxxxxxxxxx xxxx xxxx xx xxxxxxxx xx xxxxxxxx Vulvovaginitis adverse events led to discontinuation for three patients within the canagliflozin groups. In DIA3002, there was also a higher incidence of superficial genital infections in men treated with canagliflozin 100 mg (6.6%) and canagliflozin 300 mg (3.4%) compared with placebo (1.3%). All of the eight men in the pooled canagliflozin group who reported to have had superficial genital infections were uncircumcised and three of the eight had a medical history of balanitis or balanoposthitis within the five years prior to entering the study. Similar to DIA3015, one patient in the canagliflozin 300 mg group in DIA3002 discontinued due to an adverse event of balanoposthitis.
TABLE 19: SUMMARY OF FEMALE GENITAL INFECTION ADVERSE EVENTS FROM DIA3002 AND DIA3015
Vulvovaginal Adverse Events
DIA3015 DIA3002
CANA 300 mg (N = 170)
n (%)
SITA 100 mg (N = 163)
n (%)
Placebo (N = 80)
n (%)
CANA 100 mg (N = 81)
n (%)
CANA 300 mg (N = 69)
n (%)
Total vulvovaginal AEs 26 (15.3) 7 (4.3) 4 (5.0) 12 (14.8) 12 (17.4)
Vaginal infection x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Vulvovaginal candidiasis x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Vulvovaginal mycotic infection x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Vulvovaginitis x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Duration of infection, mean (SD) x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Duration of symptoms, mean (SD) x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Severity/intensity, n (%) x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Mild x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Moderate x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Severe x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
AE = adverse event; CANA = canagliflozin; SD = standard deviation; SITA = sitagliptin. Note: Data from Clinical Study Reports for DIA3002
2 and DIA3015.
3
TABLE 20: SUMMARY OF MALE GENITAL INFECTION ADVERSE EVENTS FROM DIA3002 AND DIA3015
Male Genital Infection Adverse Events
DIA3015 DIA3002
CANA 300 mg (N = 207)
SITA 100 mg (N = 215)
Placebo (N = 76)
CANA 100 mg (N = 76)
CANA 300 mg (N = 87)
Male genital infection AEs, n(%) 19 (9.2) 1 (0.5) 1 (1.3) 5 (6.6) 3 (3.4)
Balanitis 5 (2.4) 1 (0.5) x xxxxx x xxxxx x xxxxx
Balanitis candida 3 (1.4) 0 x xxxxx x xxxxx x xxxxx
Balanoposthitis 7 (3.4) 0 x xxxxx x xxxxx x xxxxx
Genital candidiasis 1 (0.5) 0 x xxxxx x xxxxx x xxxxx
Genital infection fungal 3 (1.4) 0 x xxxxx x xxxxx x xxxxx
Number of patients, n (%) x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Duration of infection, mean (SD) x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Duration of symptoms, mean (SD) x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Severity/intensity, n (%) x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Mild x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Moderate x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
AE = adverse event; CANA = canagliflozin; SD = standard deviation; SITA = sitagliptin.
Note: Data from Clinical Study Reports for DIA30022 and DIA3015.
3
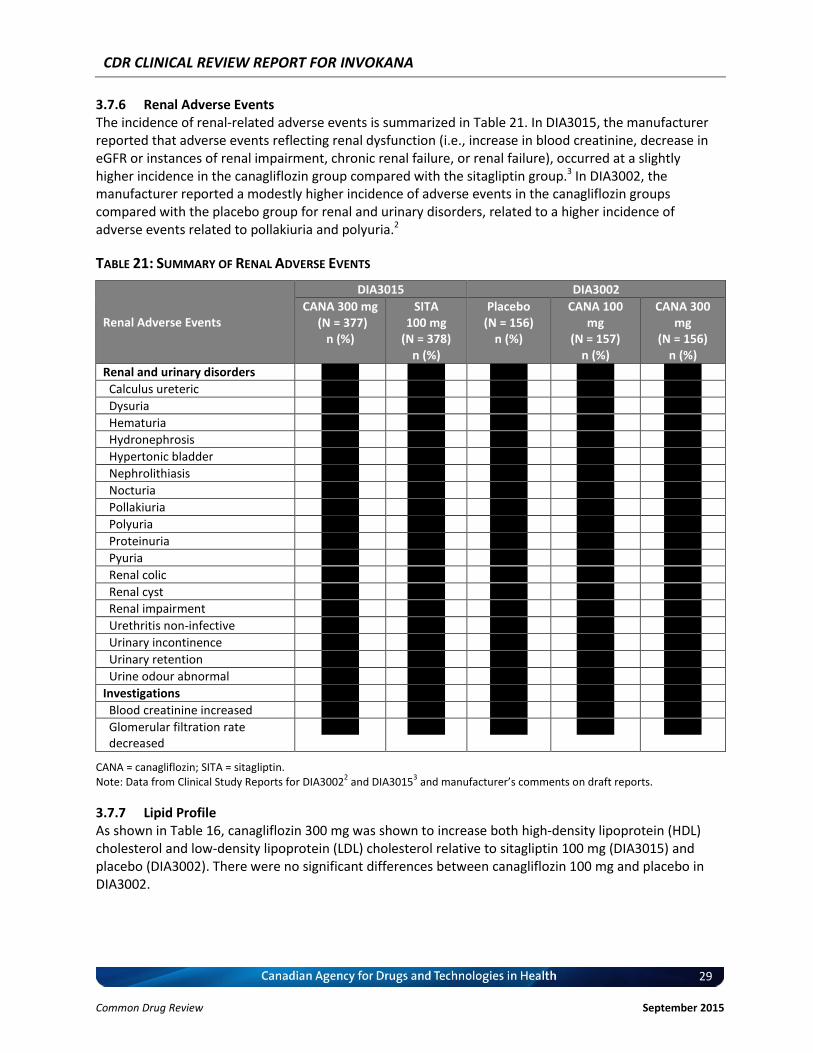
CDR CLINICAL REVIEW REPORT FOR INVOKANA
29
Common Drug Review September 2015
3.7.6 Renal Adverse Events The incidence of renal-related adverse events is summarized in Table 21. In DIA3015, the manufacturer reported that adverse events reflecting renal dysfunction (i.e., increase in blood creatinine, decrease in eGFR or instances of renal impairment, chronic renal failure, or renal failure), occurred at a slightly higher incidence in the canagliflozin group compared with the sitagliptin group.3 In DIA3002, the manufacturer reported a modestly higher incidence of adverse events in the canagliflozin groups compared with the placebo group for renal and urinary disorders, related to a higher incidence of adverse events related to pollakiuria and polyuria.2
TABLE 21: SUMMARY OF RENAL ADVERSE EVENTS
Renal Adverse Events
DIA3015 DIA3002
CANA 300 mg (N = 377)
n (%)
SITA 100 mg
(N = 378) n (%)
Placebo (N = 156)
n (%)
CANA 100 mg
(N = 157) n (%)
CANA 300 mg
(N = 156) n (%)
Renal and urinary disorders x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Calculus ureteric x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Dysuria x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Hematuria x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Hydronephrosis x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Hypertonic bladder x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Nephrolithiasis x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Nocturia x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Pollakiuria x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Polyuria x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Proteinuria x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Pyuria x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Renal colic x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Renal cyst x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Renal impairment x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Urethritis non-infective x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Urinary incontinence x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Urinary retention x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Urine odour abnormal x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Investigations x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Blood creatinine increased x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
Glomerular filtration rate decreased
x xxxxx x xxxxx x xxxxx x xxxxx x xxxxx
CANA = canagliflozin; SITA = sitagliptin. Note: Data from Clinical Study Reports for DIA3002
2 and DIA3015
3 and manufacturer’s comments on draft reports.
3.7.7 Lipid Profile As shown in Table 16, canagliflozin 300 mg was shown to increase both high-density lipoprotein (HDL) cholesterol and low-density lipoprotein (LDL) cholesterol relative to sitagliptin 100 mg (DIA3015) and placebo (DIA3002). There were no significant differences between canagliflozin 100 mg and placebo in DIA3002.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
30
Common Drug Review September 2015
TABLE 22: DIFFERENCE IN CHANGE FROM BASELINE IN FASTING LIPIDS (LAST OBSERVATION CARRIED FORWARD)
Serum Fasting Lipids
DIA3015 DIA3002
CANA 300 – SITA LSMD (95% CI)
CANA 100 – PL LSMD (95% CI)
CANA 300 – PL LSMD (95% CI)
Percentage change from baseline
Cholesterol 4.88 (2.1 to 7.7) –0.91 (–4.5 to 2.6) 2.19 (–1.4 to 5.8)
HDL-C 6.99 (4.6 to 9.3) 2.60 (–0.8 to 6.0) 3.53 (0.1 to 7.0)
LDL-C 6.44 (1.7 to 11.2) 0.52 (–5.8 to 6.8) 4.58 (–1.8 to 10.9)
LDL-C/HDL-C –1.08 (–6.3 to 4.2) –2.66 (–8.9 to 3.6) 0.31 (–6.0 to 6.6)
Triglycerides –2.28 (–9.8 to 5.3) –6.19 (–16.9 to 4.5) –3.08 (–13.8 to 7.7)
Change from baseline
Cholesterol (mmol/L) vvvv vvvvv vv vvvvv vvvv vvvvv vv vvvvv vvvv vvvvv vv vvvvv
HDL-C (mmol/L) vvvv vvvvv vv vvvvv vvvv vvvvv vv vvvvv vvvv vvvvv vv vvvvv
LDL-C (mmol/L) vvvv vvvvv vv vvvvv vvvv vvvvv vv vvvvv vvvv vvvvv vv vvvvv
LDL-C/HDL-C vvvv vvvvv vv vvvvv vvvv vvvvv vv vvvvv vvvv vvvvv vv vvvvv
Triglycerides (mmol/L) vvvv vvvvv vv vvvvv vvvv vvvvv vv vvvvv vvvv vvvvv vv vvvvv
CANA = canagliflozin; CI = confidence interval; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol; LOCF = last observation carried forward; LSMD = least squares mean difference; PL = placebo; SITA = sitagliptin.
4. DISCUSSION
4.1 Summary of Available Evidence Canagliflozin is the first SGLT2 inhibitor to be approved for use in Canada. The manufacturer has requested a “list with clinical criteria” recommendation for the use of canagliflozin after failure of metformin and a sulfonylurea. CADTH’s therapeutic review of third-line antihyperglycemic drugs, which predated the emergence of the SGLT2 inhibitor class, recommended NPH insulin as the preferred option for patients with type 2 diabetes and inadequate glycemic control with metformin and a sulfonylurea. This has been reflected in previous Canadian Expert Drug Advisory Committee and Canadian Drug Expert Committee recommendations for DPP-4 inhibitors (i.e., sitagliptin, linagliptin, and saxagliptin)22-24 that were recommended for use in the third-line setting “when insulin is not an option.” The objective of this review was to evaluate the beneficial and harmful effects of canagliflozin for the treatment of adults with type 2 diabetes who have experienced inadequate glycemic control on combination therapy with metformin and a sulfonylurea. There was one 12-month active-controlled RCT (DIA3015) and one six-month placebo-controlled RCT (DIA3002) identified in this review that investigated the use of canagliflozin in the target patient population. The trial design of these RCTs is consistent with current advice from the FDA and EMA regarding registration trials for new antihyperglycemic drugs, which states that while confirmatory studies are typically six months in duration, at least one trial, preferably active-controlled, should demonstrate maintenance of effect over at least 12 months.18,19 There were no studies comparing the addition of canagliflozin against a basal insulin for patients with inadequate control on metformin and a sulfonylurea. The Canadian, European, and US product monographs for canagliflozin all recommend a starting dose of 100 mg once daily and state that the dosage may be increased to 300 mg once daily for patients who require more stringent glycemic control and who have a low risk of adverse reactions.1 The CDR review did not identify any clinical studies in the population of interest that investigated dose escalation of canagliflozin from 100 mg to 300 mg once daily. It is currently unclear what proportion of patients would
CDR CLINICAL REVIEW REPORT FOR INVOKANA
31
Common Drug Review September 2015
be expected to receive a 300 mg dosage in Canadian clinical practice; however, the clinical expert consulted by CDR noted that, given the progressive nature of type 2 diabetes, it is likely that a majority of patients who tolerate a 100 mg dosage of canagliflozin would eventually progress to the higher dosage in order to maintain glycemic control. The National Institute for Health and Care Excellence (NICE) technology appraisal guidance for canagliflozin noted similar uncertainty in the United Kingdom setting and reported that data from the US, provided during their consultation period, suggested that 50% of people who had received canagliflozin 100 mg once daily escalated to the 300 mg once daily regimen.25 The NICE appraisal also indicated the manufacturer provided observational data reporting that 25% of patients escalated to the 300 mg once daily regimen.25
4.2 Interpretation of Results 4.2.1 Efficacy There was no evidence related to macrovascular or microvascular complications of type 2 diabetes for canagliflozin used in combination with metformin and a sulfonylurea. This is consistent with the paucity of evidence found in CADTH’s therapeutic review of third-line diabetes pharmacotherapy9 and with other systematic reviews of oral antihyperglycemic drugs.26-29 The manufacturer is currently conducting two longer-term studies to satisfy US FDA post-marketing requirements for canagliflozin: CANVAS (N = 4,335) will investigate the cardiovascular risk for major adverse cardiac events and CANVAS-R (N = 5,700) will assess the progression of albuminuria in participants receiving standard care but with inadequate glycemic control and at elevated risk of cardiovascular events.30,31 Similar to the majority of RCTs conducted with antihyperglycemic drugs, change in A1C from baseline was the primary end point across all nine phase 3 studies in the canagliflozin development program. Although glycemic control may not be fully responsible for differences in clinical outcomes, A1C is considered an appropriate primary outcome in clinical trials of antihyperglycemic drugs. The placebo-controlled trial demonstrated that both the 100 mg and 300 mg doses of canagliflozin effectively lowered A1C. The change from baseline within the canagliflozin 300 mg group was approximately 1% and was greater than the –0.85% observed within the canagliflozin 100 mg group. Reviewers for Health Canada13 and the EMA14 concluded that the improvement in glycemic control with both doses of canagliflozin was clinically meaningful. NICE and the US FDA have indicated that reductions from baseline in A1C as small as ‒0.5% and ‒0.7%, respectively, have clinical importance.18,32 The active-controlled trial demonstrated that canagliflozin 300 mg once daily was non-inferior and superior to sitagliptin 100 mg over a 52-week treatment period. Within this trial, both groups demonstrated meaningful improvements from baseline (–0.66% with sitagliptin and –1.03% with canagliflozin). The difference between the canagliflozin and sitagliptin groups was –0.37% with the mITT analysis set and –0.21% with the per-protocol analysis set. Although statistically significant, this difference falls below most commonly cited thresholds for clinically relevant differences in A1C. However, reviewers for Health Canada concluded that canagliflozin 300 mg provided clinically and statistically significant glycemic improvements relative to sitagliptin.13 Reports from the FDA and the EMA14 did not comment on the clinical relevance of the difference. The onset of the glycemic response in DIA3015 was similar between the canagliflozin and sitagliptin groups, with the maximal effects being reported at approximately week 12. From this point in the study, the response in the sitagliptin group began to deteriorate, whereas the patients treated with canagliflozin demonstrated a more sustained glycemic response. At the end of the 52-week study, the A1C of patients in the sitagliptin group had increased by approximately 0.4% from the nadir observed at week 12 (i.e., the values had increased from –1.05 to –0.66% in the mITT data set). In contrast, the A1C

CDR CLINICAL REVIEW REPORT FOR INVOKANA
32
Common Drug Review September 2015
of patients in the canagliflozin group was relatively constant, with only a minor deterioration of approximately 0.1% from week 12 to week 52 in the mITT data set. A similar deterioration of glycemic control was observed for FPG in the sitagliptin group, with the end-of-study FPG measurements nearly approaching baseline, in addition to a lower initial response to treatment with sitagliptin relative to canagliflozin. The clinical expert consulted by CDR noted that the deterioration of glycemic control reported for sitagliptin in DIA3015 is relatively consistent with observations made in clinical practice for patients who are treated with a DPP-4 inhibitor following failure with metformin and a sulfonylurea. Many patients with type 2 diabetes, including a majority of those in DIA3002 and DIA3015, are overweight or obese. Therefore, changes in body weight associated with antihyperglycemic therapy may be important for both patients and health care professionals. Canagliflozin has been shown to be associated with a decrease in body weight of approximately 2 kg when provided in combination with metformin and a sulfonylurea. Relative to placebo, the mean difference in percentage change from baseline in body weight was –1.4% and –2.0% for canagliflozin 100 mg and 300 mg, respectively. Across the full study population, this difference is not likely to be clinically relevant, based on the 2006 Canadian clinical practice guidelines on the management and prevention of obesity in adults and children, which define a clinically important weight change as being at least 5% of total body weight; however, a greater proportion of canagliflozin-treated patients did achieve an improvement of at least 5% of total body weight compared with sitagliptin and placebo. The EMA reported the body weight reduction with canagliflozin was attributable to a greater decrease in body fat mass (two-thirds) relative to lean body mass (one-third) and suggested that the weight loss was predominantly due to loss of calories rather than dehydration.14 The mechanism of action for canagliflozin and other SGLT2 inhibitors results in osmotic diuresis and can lead to a reduction in SBP.1 This effect was observed in DIA3015, where canagliflozin was shown to result in a statistically significant reduction in SBP relative to sitagliptin, with a mean difference of –5.91 mm Hg between the canagliflozin and sitagliptin groups. The reduction in SBP with canagliflozin was not statistically significant relative to placebo in DIA3002; however, the results were numerically in favour of canagliflozin. Across the short-term phase 3 trials that have been reported for canagliflozin, the reduction in SBP has been consistently observed and relatively well characterized. It should be noted that the product monograph indicates caution should also be exercised in other patients for whom a decrease in blood pressure could pose a risk of harm. Reviewers for the EMA and the FDA generally concluded that the magnitude of reduction in blood pressure with canagliflozin is clinically relevant and could have a beneficial effect on patients with type 2 diabetes, noting that such patients are often hypertensive. Similarly, the clinical expert consulted during the review indicated that this reduction in blood pressure would likely be beneficial for the patient population of interest for this review (i.e., those with long-standing type 2 diabetes) as the majority of these patients have hypertension and would therefore not be at significant risk of becoming hypotensive as a result of the reduction in blood pressure observed with canagliflozin. 4.2.2 Harms The mechanism of action for SGLT2 inhibitors results in an increase in glucose excretion in the patient’s urine, which favours the development of urogenital infections.1,14 As a result, treatment-emergent urogenital adverse events were more frequently reported with canagliflozin than with placebo or any of the active comparators used in the phase 3 trials. A similar result has been observed with dapagliflozin (Forxiga), another drug in the SGLT2 inhibitor class that has been approved for use by the EMA.33,34 The manufacturer’s investigation into those adverse events suggests that patients with a history of genital mycotic infections and uncircumcised males were more likely to develop genital mycotic infections. The
CDR CLINICAL REVIEW REPORT FOR INVOKANA
33
Common Drug Review September 2015
majority of events were mild to moderate in severity and patients were provided with oral or topical treatment; in a pooled analysis of the 2,313 canagliflozin-treated patients, just 0.7% withdrew as a result of mycotic vulvovaginitis.11 The majority of vulvovaginal candidiasis occurred within the first four months of initiating treatment with canagliflozin.1 A pooled safety analysis of phase 3 studies demonstrated that 2.3% of women treated with canagliflozin experienced more than one infection. NICE noted that the clinical specialists consulted during their review indicated that the infections had generally been resolved by topical treatment and that recurrence rates were low. It is currently unclear to what extent these infections would influence prescribing by physicians and adherence by patients in Canadian clinical practice. The included trials demonstrated there is an increased risk of hypoglycemia with canagliflozin relative to placebo when patients are receiving background treatment with metformin and a sulfonylurea. In the absence of concomitant treatment with insulin or an insulin secretagogue (e.g., a sulfonylurea), canagliflozin treatment has a minimal risk of hypoglycemia. The product monograph states that when canagliflozin is used as add-on therapy with a sulfonylurea, a lower dose of the sulfonylurea may be considered to reduce the risk of hypoglycemia. The increased risk in the presence of a sulfonylurea is consistent with what has been observed with DPP-4 inhibitors and GLP-1 analogues, two classes of antihyperglycemic drugs that are not typically associated with hypoglycemia in the absence of insulin or an insulin secretagogue. In the active-controlled trial, there was a slightly higher event rate per patient-year with canagliflozin (4.14) compared with sitagliptin (3.81); however, regulatory authorities concluded that this difference was not clinically important.14 Consistent with most short-term studies of antihyperglycemic drugs, events of severe hypoglycemia were rare in the placebo-controlled trial (range 0% to 0.6%); however, the rates of severe hypoglycemia in DIA3015 were relatively large in both the canagliflozin (4.0%) and sitagliptin groups (3.4%) compared with the 26-week DIA3002 data and many other trials conducted in third-line settings.9 Given the similarity in the design of DIA3002 and DIA3015, it is unclear why the rates of severe hypoglycemia were so much greater in DIA3015. The product monograph states that canagliflozin is contraindicated in renally impaired patients who have an eGFR of less than 45 mL/min/1.73 m2, have end-stage renal disease, or are on dialysis, noting that canagliflozin should not be initiated in patients with an eGFR of less than 60 mL/min/1.73 m2, and should be discontinued when the eGFR is below 45 mL/min/1.73 m2. The product monograph recommends that renal function be assessed prior to initiating treatment with canagliflozin and regularly thereafter. As the patients of interest for this review are those already receiving metformin and a sulfonylurea, similar testing should already be in place in accordance with recommendations for metformin;35 therefore, the need to monitor renal function during treatment with canagliflozin is not likely to represent an additional burden for patients and physicians. As a result of the dose-dependent increases in LDL cholesterol observed with canagliflozin treatment, the product monograph recommends that LDL cholesterol levels be monitored for patients initiating treatment with canagliflozin. The clinical expert consulted during the review indicated that the patients of interest for this review would most likely be receiving annual lipid monitoring prior to initiating treatment with canagliflozin. It was noted that the magnitude of the increase in LDL cholesterol with canagliflozin was small and of uncertain clinical relevance. The clinical expert also suggested that such increases in LDL cholesterol would likely not be attributed to therapy with canagliflozin in clinical practice and would be unlikely to result in patients discontinuing treatment.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
34
Common Drug Review September 2015
5. CONCLUSIONS
The CDR systematic review included two phase 3 RCTs that investigated the comparative safety and efficacy of canagliflozin in patients with type 2 diabetes with inadequate glycemic control with metformin and a sulfonylurea. One 12-month, active-controlled study demonstrated that canagliflozin 300 mg once daily was superior to sitagliptin 100 mg once daily for improving glycemic control, reducing body weight, and lowering SBP. One six-month study demonstrated that canagliflozin, at both the recommended starting dose of 100 mg once daily and the higher 300 mg once-daily dose, resulted in clinically relevant improvements in glycemic control compared with placebo. The improvements in glycemic control and blood pressure observed with canagliflozin were generally considered to be clinically relevant by regulatory authorities and the clinical expert by CDR; however, publication of the longer-term studies will be required to determine any beneficial or harmful effects on cardiovascular end points. Canagliflozin is associated with an increased risk of developing urogenital adverse events and an increase in LDL cholesterol. When used in combination with a sulfonylurea, canagliflozin increases the risk of hypoglycemia relative to placebo. As with all new antihyperglycemic drugs, additional studies and clinical experience will be required to fully characterize the longer-term safety profile of canagliflozin.
CDR CLINICAL REVIEW REPORT FOR INVOKANA
35
Common Drug Review September 2015
APPENDIX 1: PATIENT INPUT SUMMARY
This section was summarized by CADTH Common Drug Review (CDR) staff based on the input provided by the patient group. It has not been systematically reviewed. It has been reviewed by the submitting patient group.
Brief Description of Patient Group(s) Supplying Input The Canadian Diabetes Association (CDA) provides education and services, advocates on behalf of people with diabetes, supports research, and translates research into practical applications. The CDA is supported in its efforts by a community-based network of volunteers, employees, health care professionals, researchers, and partners. The CDA solicits and receives unrestricted educational grants from multiple manufacturers and vendors of medications, supplies, and devices for diabetes and its complications and these are listed in Figure 9. These funds are used to help the CDA support community programs and services for people with diabetes and to fund research and advocacy across Canada. The CDA declared no conflicts of interest in the preparation of this submission.
Condition and Current Therapy-Related Information The CDA solicited patient input via a survey distributed through social media and email blasts. A total of 388 individuals participated in the survey and 93% identified themselves as patients with type 2 diabetes. This submission is based on 376 respondents who are either diabetics or caregivers. Of this group, 93% had taken (or are taking) anti-diabetic medication. Approximately 7.6% (13 of 171 respondents) had taken canagliflozin. Type 2 diabetes is a chronic (progressive) condition that occurs when the pancreas does not produce enough insulin or when the body does not effectively use the insulin that is produced. Common symptoms of diabetes include fatigue, thirst, and weight change. High blood-glucose levels can cause long-term complications such as blindness, heart disease, kidney problems, nerve damage, and erectile dysfunction. The majority of patients with type 2 diabetes indicated that daily fluctuations in blood sugar were the most important aspect of diabetes to control during the day and overnight. These fluctuations affect the ability to work and interactions with friends and family, cause stress and worry, and affect one’s ability to participate in the normal activities of daily living. Uncontrolled diabetes and the stigma associated with the disease can result in reduced quality of life. Respondents frequently emphasized the psychological and emotional impact of diabetes on their lives (effect on stress and anxiety, having to adjust to changes in diet and lifestyle, having to manage medication and treatment, the effects on relationships with family), as well as the physical impacts, such as fatigue and lack of energy. A patient noted: “It is a life-altering disease that impacts every aspect of life. There is constant blood monitoring, diet, level of activity, (and the) cost of expensive supplies and medication.” Management of diabetes includes lifestyle changes (diet, exercise, and stress management). Initial therapy is most often with metformin but, over time, most patients will require the addition of a second or third drug to reach glycemic targets. Many of the currently available second-line therapies cause significant weight gain while their ability to achieve optimal glycemic control may be limited by

CDR CLINICAL REVIEW REPORT FOR INVOKANA
36
Common Drug Review September 2015
hypoglycemia. “The most distressing side effect of all of the diabetes drugs is they make you gain weight or prevent weight loss. It is annoying to be told to lose weight then handed a drug that prevents weight loss.” Many patients with diabetes do not take oral glucose-lowering therapy as prescribed. Almost 30% of respondents found it somewhat difficult, difficult, or very difficult to take multiple medications through the day. Given that diabetes frequently occurs with other chronic conditions, this finding has significant implications for the diabetes population. Approximately 56% of all respondents indicated general satisfaction (satisfied or very satisfied) with their drug therapy.
Related Information About the Drug Being Reviewed The availability of canagliflozin as an alternative treatment option for stabilizing blood glucose is important to patients. It belongs to a new class of drugs that lowers blood glucose and also causes a reduction in blood pressure and weight loss through inhibition of SGLT2. Only 13 respondents had experience with canagliflozin. Of these, 10 people qualitatively described treatment. Four were very pleased with the glucose control and experienced no notable side effects. These patients described the relief of finally receiving treatment that controlled their blood glucose. A patient noted, “It has actually lowered my blood sugar levels to a range of readings that I haven’t seen in several years.” Three patients described increased urination and one patient discontinued canagliflozin as a result. One described persistent yeast infection. Survey respondents answered the following questions as follows:
How important is it to have new drug therapy for glucose lowering also reduce weight? About 78% said it was important to essential.
How important is it to have new drug therapy for glucose lowering also reduce blood pressure? About 80% said it was important to essential.
About 80% of respondents said the availability of canagliflozin is important. Patients stated that weight and hypertension are often problems for those living with diabetes and contribute towards many of the complications with this condition. In summary, diabetes is a very common chronic progressive condition that requires intensive self-management. The availability of canagliflozin provides an important option for patients who often have several comorbid conditions.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
37
Common Drug Review September 2015
FIGURE 9: ORGANIZATIONS AND FOUNDATIONS THAT MADE DONATIONS TO THE CANADIAN DIABETES
ASSOCIATION BETWEEN SEPTEMBER 2012 AND AUGUST 2013

CDR CLINICAL REVIEW REPORT FOR INVOKANA
38
Common Drug Review September 2015
APPENDIX 2: LITERATURE SEARCH STRATEGY
OVERVIEW
Interface: Ovid
Databases: Embase 1974 to present
MEDLINE Daily and MEDLINE 1946 to present
MEDLINE In-Process & Other Non-Indexed Citations
Note: Subject headings have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search:
August 20, 2014
Alerts: Weekly search updates until December 10, 2014
Study types: Randomized controlled trials; controlled clinical trials; multicenter studies; cohort studies; crossover studies; case control studies; comparative studies; epidemiologic studies; also costs and cost analysis studies, quality of life studies, and economic literature.
Limits: No date or language limits were used
Conference abstracts were excluded
SYNTAX GUIDE
/ At the end of a phrase, searches the phrase as a subject heading
MeSH Medical Subject Heading
exp Explode a subject heading
* Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings
.ti Title
.ab Abstract
.hw Heading word; usually includes subject headings and controlled vocabulary
.pt Publication type
.rn CAS registry number
.nm Name of substance word
pmez
Ovid database code; MEDLINE In-Process & Other Non-Indexed Citations, MEDLINE Daily and Ovid MEDLINE 1946 to Present
oemezd Ovid database code; Embase 1974 to present, updated daily
MULTI-DATABASE STRATEGY
Line # Strategy
1 (Invokana or canagliflozin or Prominad or TA7284 or TA 7284 or JNJ28431754 or JNJ 28431754 or JNJ24831754AAA or JNJ 24831754AAA or JNJ24831754ZAE or JNJ 24831754ZAE or JNJ 24831754 AAA or UNII6S49DGR869 or UNII 6S49DGR869 or "842133 18 0" or "842133180"). ti,ab,ot,sh,hw,rn,nm.
2 ("842133180" or "842133 18 0" or "84213318 0" or 842133 180 or UNII6S49DGR869 or UNII 6S49DGR869 or TA7284 or TA 7284 or JNJ28431754 or JNJ 28431754 or JNJ24831754AAA or JNJ 24831754AAA or JNJ24831754ZAE or JNJ 24831754ZAE or JNJ 24831754 AAA).rn,nm.
3 1 or 2
4 3 use pmez
5 exp canagliflozin/
6 (Invokana or canagliflozin or Prominad or TA7284 or TA 7284 or JNJ28431754 or JNJ 28431754 or JNJ24831754AAA or JNJ 24831754AAA or JNJ24831754ZAE or JNJ 24831754ZAE or JNJ 24831754 AAA or

CDR CLINICAL REVIEW REPORT FOR INVOKANA
39
Common Drug Review September 2015
MULTI-DATABASE STRATEGY
Line # Strategy
UNII6S49DGR869 or UNII 6S49DGR869 or "842133 18 0" or "842133180").ti,ab.
7 5 or 6
8 7 use oemezd
9 3 or 8
10 9 not conference abstract.pt.
11 exp animals/
12 exp animal experimentation/ or exp animal experiment/
13 exp models animal/
14 nonhuman/
15 exp vertebrate/ or exp vertebrates/
16 animal.po.
17 or/11-16
18 exp humans/
19 exp human experimentation/ or exp human experiment/
20 human.po.
21 or/18-20
22 17 not 21
23 10 not 22
OTHER DATABASES
PubMed Same MeSH, keywords, limits, and study types used as per MEDLINE search, with appropriate syntax used.
Trial registries (Clinicaltrials.gov and others)
Same keywords, limits used as per MEDLINE search.
Grey Literature
Dates for search: To August 20, 2014 Keywords: Invokana, canagliflozin, Prominad, TA7284, JNJ28431754 Limits: No date or language limits used
Relevant websites from the following sections of the CADTH grey literature checklist, “Grey matters: a practical tool for evidence-based searching” (http://www.cadth.ca/en/resources/finding-evidence-is/grey-matters) were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Databases (free)
Internet Search

CDR CLINICAL REVIEW REPORT FOR INVOKANA
40
Common Drug Review September 2015
APPENDIX 3: EXCLUDED STUDIES
Study Population Not of Interest Forst T, Guthrie R, Goldenberg R, Yee J, Vijapurkar U, Meininger G, et al. Efficacy and safety of canagliflozin over 52 weeks in patients with type 2 diabetes on background metformin and pioglitazone. Diabetes Obes Metab. 2014 May;16(5):467-77. Yale JF, Bakris G, Cariou B, Nieto J, vid-Neto E, Yue D, et al. Efficacy and safety of canagliflozin over 52 weeks in patients with type 2 diabetes mellitus and chronic kidney disease. Diabetes Obes Metab. 2014 Jun 25.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
41
Common Drug Review September 2015
APPENDIX 4: SUMMARY AND APPRAISAL OF MANUFACTURER-SUBMITTED MIXED-TREATMENT COMPARISION
Objective To summarize and critically appraise the manufacturer’s network meta-analysis (NMA)36,37 comparing the relative efficacy and safety of canagliflozin against other antihyperglycemic drugs as add-on therapy to metformin and a sulfonylurea.
Summary of Network Meta-analysis There is a lack of head-to-head clinical data for comparison of canagliflozin (100 mg and 300 mg) to other antihyperglycemic drugs (except sitagliptin) as third-line treatment (in addition to background therapy of metformin and a sulfonylurea). Because of this lack of data, an NMA was conducted by the manufacturer to assess the comparative clinical effectiveness of canagliflozin versus all relevant comparators on the following outcomes: change in glycated hemoglobin (A1C) from baseline; proportion of patients reaching an A1C of less than 7%; fasting plasma glucose (FPG) change from baseline; body weight change from baseline; and systolic blood pressure (SBP) change from baseline. Methods a) Eligibility Criteria Clinical data for the NMA were derived from a systematic review of randomized controlled trials (RCTs). Eligible studies included those involving adults with type 2 diabetes mellitus who had inadequate glycemic control on metformin and a sulfonylurea. Intervention and comparators included canagliflozin (100 mg or 300 mg once daily), dipeptidyl peptidase-4 (DPP-4) inhibitors, GLP-1 analogues, thiazolidinediones, dapagliflozin, and neutral protamine Hagedorn (NPH) insulin (intermediate-acting), long-acting insulin (glargine, detemir), biphasic/pre-mixed insulin, and short-acting insulin (lispro, aspart). b) Network Meta-analysis A Bayesian hierarchical model, which preserves the randomization of each trial, was used for the NMA.38 For the modelling of binary outcomes, the manufacturer assumed that the number of events in each treatment group followed a binomial likelihood where parameters are the probability of events under each treatment and the number of patients in each group. As the probabilities can only vary between 0 and 1, a transformation was used to map these probabilities into a continuous measure. For a binomial likelihood, the standard link function is the logit, which was based on the assumption of the linearity of effects. For continuous outcomes, the meta-analysis was based on the sample means, which can be assumed as being approximately normally distributed. Moreover, this parameter was not constrained in an interval, as consequence identity was used as link function. The model selection (fixed- or random-effects model) was based on how well the model fit (“goodness of fit”). Fitness was assessed using the deviance information criterion (DIC). The fixed-effect and random-effects models were developed, and the one associated with the smallest DIC was selected (with a difference of at least three points in DIC). The model with the smallest DIC is the model with the best compromise between adequacy and complexity. For each loop of the network, an indirect comparison (Bucher method39) was conducted and compared with the direct evidence from the NMA.40 The ratio of the point estimates obtained from indirect versus direct evidence was calculated, together with the 95% confidence interval. Inconsistency was suspected
CDR CLINICAL REVIEW REPORT FOR INVOKANA
42
Common Drug Review September 2015
if the confidence interval excluded 1. For each treatment, the probability of being ranked first, second, etc. was calculated. In addition, the surface under the cumulative ranking (SUCRA) was estimated. The NMA was performed with WinBUGS version 1.4 using the Markov Chain Monte Carlo simulation method. In addition to the base-case analyses conducted at 26 weeks, various sensitivity analyses were also conducted to handle potential heterogeneity. Results a) Study and Patient Characteristics Nine studies were included in the NMA (three open-label and six double-blind). Insulin was the most frequently used treatment class, followed by glucagon-like peptide 1 (GLP-1) analogues, DPP-4 inhibitors, and SGLT2 inhibitors. No studies were included that investigated the use of thiazolidinediones. The primary outcome in all nine trials was change in A1C from baseline. The network of evidence is showed in Figure 10. Treatment duration ranged from 22 weeks to 56 weeks. One RCT was a crossover study comparing insulin glargine with NPH insulin. The inclusion criteria for baseline A1C were 7% to 11%; however, three studies did not report this criteria. Critical appraisal of the RCTs was conducted in alignment with National Institute for Health and Care Excellence methodology; however, the results were not reported. b) Glycemic Control (A1C, A1C of less than 7%, Fasting Plasma Glucose) The evidence networks for A1C, an A1C of less than 7%, and FPG are presented in Figure 10 (A, B, and C). The comparative effectiveness of canagliflozin (100 mg once daily and 300 mg once daily) with other antihyperglycemic drugs (including biphasic insulin, long-acting insulin, sitagliptin 100 mg once daily, exenatide 10 mcg twice daily, exenatide 5 mcg twice daily, and linagliptin 5 mg once daily) are presented in Table 23, Table 24, and Table 25. xxxxxxx, xxxxx xx xx xxxxxxxxxxxxx xxxxxxxxxxx xxxxxxx-xxxxx xxxxxxxxxx xx xxx xx xxxx xx, xx xxx xxxxxxxxxx xx xxxxxxxx xxxxxxxx xx xxx xx xxxx xxxx x%, xx xx xxx xxxxxx xx xxx, xxxx xxx xxxxxxxxx xxxx xxxxxxxx xxxxxxx xxxxxx x xxxxxxxxxxxxx xxxxxxxxxxx xxxxx xxx xxxxxxxx xxxx xxxxxxxxxxxxx xxx xx xxxx xxxxx (xxxxxx xxxxxxxxxx, x.xxx xx% xxxxxxxx xxxxxxxx xxxxx, x.xx xx x.xx) xxx xxxxxxxxxxxxx xxx xx xxxx xxxxx (xxxxxx xxxxxxxxxx, x.xxx xx% xxx, x.xx xx x.xx). Canagliflozin 300 mg was associated with probabilities higher than xx% in terms of A1C compared with the DPP-4 inhibitors (sitagliptin 100 mg and linagliptin 5 mg). In terms of FPG, both canagliflozin 100 mg and 300 mg were associated with probabilities higher than xx% compared with the DPP-4 inhibitors. When comparing canagliflozin 100 mg and 300 mg with insulin, biphasic insulin ranked first in terms of glycemic control on the basis of the SUCRA. Compared with GLP-1 agonists, canagliflozin 300 mg was associated with probabilities higher than xx% of achieving glycemic control compared with exenatide 10 mcg and 5 mcg. c) Body Weight The evidence network for body weight is presented in Figure 10D. The comparative effectiveness of canagliflozin (100 mg once daily and 300 mg once daily) with other antihyperglycemic drugs is presented in Table 26. xxxxxxx, xxxxx xx xx xxxxxxxxxxxxx xxxxxxxxxxx xxxxxxxxxx xx xxxx xxxxxx xx xxxx xx. xxxxxxxxxxxxx xxx xx xxxxxx xxxxx xx xxx xxxxx xx xxx xxxxx xxxx xxxxxxx xx xxx xxxxxxxx xx xxxx xxxxxx. Canagliflozin 100 mg and 300 mg were associated with probabilities higher than xx% of reducing weight compared with biphasic and long-acting insulin, with differences (versus insulin) ranging from –x.xx xx to –x.xx xx. Canagliflozin 100 mg and 300 mg were associated with probabilities higher than xx% of reducing weight compared with the DPP-4 inhibitors (sitagliptin 100 mg and linagliptin 5 mg). Canagliflozin 300 mg was associated with probabilities of xx% in reducing weight compared with the GLP-1 agonists (exenatide 5 mcg and 10 mcg). Canagliflozin 100 mg was associated with probabilities of xx% in reducing weight compared with exenatide 10 mcg and 5 mcg, respectively.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
43
Common Drug Review September 2015
FIGURE 10: EVIDENCE NETWORK DIAGRAMS
Figure removed to comply with licensing restrictions and copyright law. A1C = glycated hemoglobin; BID = twice daily; CANA = canagliflozin; DPP-4; dipeptidyl peptidase-4; GLP-1 = glucagon-like peptide 1; LINA = linagliptin; QD = once daily; SGLT2 = sodium-glucose cotransporter-2; SITA = sitagliptin; SU = sulfonylurea; TZD = thiazolidinedione. Note: Network diagrams are shown for the following: A) Change from baseline in A1C; B) Proportion of patients with A1C < 7%; C) Change from baseline in FPG; D) Change from baseline body weight; E) Change from baseline in SBP; and F) Hypoglycemia.
d) Systolic Blood Pressure The evidence network for SBP is presented in Figure 10E. The comparative effectiveness of canagliflozin (100 mg once daily and 300 mg once daily) with other antihyperglycemic drugs in terms of SBP is presented in Table 27. xxxxxxxx xxxx xxxxxxxxxxx xxx xx, xxxxxxxxxxxxx (xxx xx xx xxx xx) xxx xxxxxxxxxx xxxx x xxxxxxxxxxxxx xxxxxxxxxxx xxxxxxxx xx xxx. Canagliflozin 100 mg and 300 mg were associated with probabilities higher than xx% of lowering SBP compared with long-acting insulin and the DPP-4 inhibitor sitagliptin 100 mg. xxxxxxxxxxxxx xxx xx xxxxxx xxxxx xx xxx xxxxx xx xxx xxxxx xxx xxxxxxxxxxxxx xxx xx xxxxxx xxxxxx. e) Hypoglycemia The evidence network for hypoglycemia is presented in Figure 10F. The comparative effectiveness of canagliflozin (100 mg once daily and 300 mg once daily) with other antihyperglycemic drugs in terms of hypoglycemic events is presented in Table 28. Canagliflozin 100 mg and 300 mg were associated with probabilities higher than xx% of reducing the risk of all hypoglycemic events compared with long-acting and biphasic insulin, with odds ratios ranging from x.xx (xx% xxx, x.xx xx x.xx) to x.xx (xx% xxx, x.xx xx x.xx). Canagliflozin 100 mg was associated with a probability of xx% of reducing the risk of all hypoglycemic events compared with exenatide 10 mcg, and xx% compared with exenatide 5 mcg. Canagliflozin 300 mg was associated with probabilities lower than xx% of reducing the risk of all hypoglycemic events compared with exenatide 10 mcg, and probabilities lower than x% compared with exenatide 5 mcg. Both canagliflozin 100 mg and 300 mg were associated with probabilities higher than xx% of reducing the risk of all hypoglycemic events compared with sitagliptin 100 mg. These probabilities were lower than xx% compared with linagliptin 5 mg. Sensitivity Analysis Various sensitivity analyses were conducted to ensure robustness of the results. The sensitivity analysis was done by excluding studies that were a potential source of heterogeneity or inconsistency or were of lower quality (such as an open-label study), and by adding conference abstracts. All sensitivity analyses showed a decrease in A1C levels in the active treatment group when compared with placebo. A greater treatment dose resulted in a greater decrease in A1C levels following treatment with xxxxxxxxxxxxx xxx xxxxxxxxx. The greatest change in A1C from baseline when compared with placebo was a decrease of –x.xx% following treatment with xxxxxxxxxxx x.x xx xxxxx and the lowest being treatment with xxxxxxxxxxxx (see Figure 11). All sensitivity analyses showed no or minimal impact on the findings from the base-case analysis.
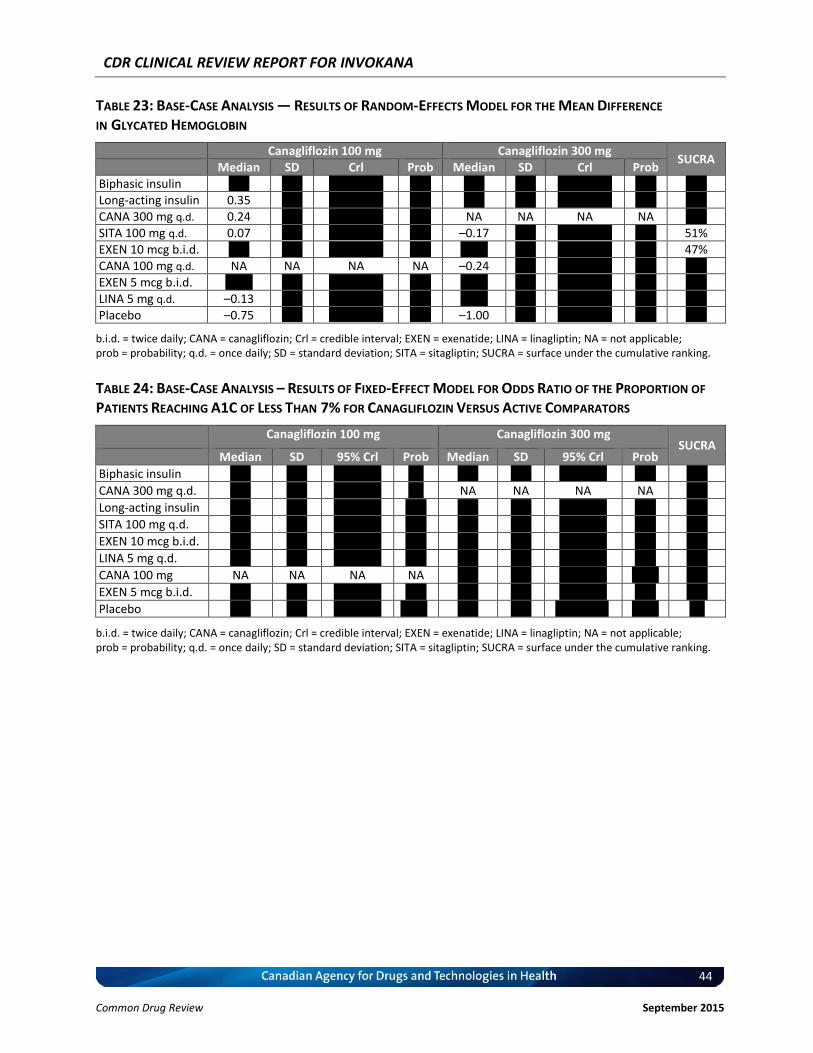
CDR CLINICAL REVIEW REPORT FOR INVOKANA
44
Common Drug Review September 2015
TABLE 23: BASE-CASE ANALYSIS — RESULTS OF RANDOM-EFFECTS MODEL FOR THE MEAN DIFFERENCE
IN GLYCATED HEMOGLOBIN
Canagliflozin 100 mg Canagliflozin 300 mg SUCRA
Median SD Crl Prob Median SD Crl Prob Biphasic insulin x.xx x.xx –x.xx, x.xx xx% x.xx x.xx –x.xx, x.xx xx% xx% Long-acting insulin 0.35 x.xx –x.xx, x.xx xx% x.xx x.xx –x.xx, x.xx xx% xx% CANA 300 mg q.d. 0.24 x.xx –x.xx, x.xx xx% NA NA NA NA xx% SITA 100 mg q.d. 0.07 x.xx –x.xx, x.xx xx% –0.17 x.xx –x.xx, x.xx xx% 51% EXEN 10 mcg b.i.d. x.xx x.xx –x.xx, x.xx xx% –x.xx x.xx –x.xx, x.xx xx% 47% CANA 100 mg q.d. NA NA NA NA –0.24 x.xx –x.xx, x.xx xx% xx% EXEN 5 mcg b.i.d. –x.xx x.xx –x.xx, x.xx xx% –x.xx x.xx –x.xx, x.xx xx% xx% LINA 5 mg q.d. –0.13 x.xx –x.xx, x.xx xx% –x.xx x.xx –x.xx, x.xx xx% xx% Placebo –0.75 x.xx –x.xx, x.xx xx% –1.00 x.xx –x.xx, x.xx xx% xx%
b.i.d. = twice daily; CANA = canagliflozin; Crl = credible interval; EXEN = exenatide; LINA = linagliptin; NA = not applicable; prob = probability; q.d. = once daily; SD = standard deviation; SITA = sitagliptin; SUCRA = surface under the cumulative ranking.
TABLE 24: BASE-CASE ANALYSIS – RESULTS OF FIXED-EFFECT MODEL FOR ODDS RATIO OF THE PROPORTION OF
PATIENTS REACHING A1C OF LESS THAN 7% FOR CANAGLIFLOZIN VERSUS ACTIVE COMPARATORS
Canagliflozin 100 mg Canagliflozin 300 mg SUCRA
Median SD 95% Crl Prob Median SD 95% Crl Prob
Biphasic insulin x.xx x.xx x.xx, x.xx x% x.xx x.xx x.xx, x.xx xx% xx%
CANA 300 mg q.d. x.xx x.xx x.xx, x.xx x% NA NA NA NA xx%
Long-acting insulin x.xx x.xx x.xx, x.xx xx% x.xx x.xx x.xx, x.xx xx% xx%
SITA 100 mg q.d. x.xx x.xx x.xx, x.xx xx% x.xx x.xx x.xx, x.xx xx% xx%
EXEN 10 mcg b.i.d. x.xx x.xx x.xx, x.xx xx% x.xx x.xx x.xx, x.xx xx% xx%
LINA 5 mg q.d. x.xx x.xx x.xx, x.xx xx% x.xx x.xx x.xx, x.xx xx% xx%
CANA 100 mg NA NA NA NA x.xx x.xx x.xx, x.xx xxx% xx%
EXEN 5 mcg b.i.d. x.xx x.xx x.xx, x.xx xx% x.xx x.xx x.xx, x.xx xx% xx%
Placebo x.xx x.xx x.xx, x.xx xxx% x.xx x.xx x.xx, xx.xx xxx% x%
b.i.d. = twice daily; CANA = canagliflozin; Crl = credible interval; EXEN = exenatide; LINA = linagliptin; NA = not applicable; prob = probability; q.d. = once daily; SD = standard deviation; SITA = sitagliptin; SUCRA = surface under the cumulative ranking.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
45
Common Drug Review September 2015
TABLE 25: BASE-CASE ANALYSIS — RESULTS OF FIXED-EFFECT MODEL FOR THE MEAN DIFFERENCE IN
FASTING PLASMA GLUCOSE FOR CANAGLIFLOZIN VERSUS ACTIVE COMPARATORS
Canagliflozin 100 mg Canagliflozin 300 mg SUCRA
Mediana SD 95% Crl Prob Median
a SD 95% Crl Prob
Biphasic insulin x.xx x.xx x.xx, x.xx x% x.xx x.xx x.xx, x.xx x% xxx%
Long-acting insulin
x.xx x.xx x.xx, x.xx x% x.xx x.xx –x.xx, x.xx xx% xx%
CANA 300 mg q.d.
x.xx x.xx x.xx, x.xx x% NA NA NA NA xx%
EXEN 10 µg b.i.d. x.xx x.xx –x.xx, x.xx xx% –x.xx x.xx –x.xx, x.xx xx% xx%
EXEN 5 µg b.i.d. x.xx x.xx –x.xx, x.xx xx% –x.xx x.xx –x.xx, x.xx xx% xx%
CANA 100 mg q.d.
NA NA NA NA –x.xx x.xx –x.xx, –x.xx xxx% xx%
SITA 100 mg q.d. –x.xx x.xx –x.xx, x.xx xx% –x.xx x.xx –x.xx, –x.xx xxx% xx%
LINA 5 mg q.d. –x.xx x.xx –x.xx, x.xx xx% –x.xx x.xx –x.xx, –x.xx xxx% xx%
Placebo –x.xx x.xx –x.xx, –x.xx xxx% –x.xx x.xx –x.xx, –x.xx xxx% x%
b.i.d. = twice daily; CANA = canagliflozin; Crl = credible interval; EXEN = exenatide; LINA = linagliptin; NA = not applicable; prob = probability; q.d. = once daily; SD = standard deviation; SITA = sitagliptin; SUCRA = surface under the cumulative ranking. a The median value indicates the between-group difference of differences, that is (active 1 – placebo) – (active 2 – placebo).
TABLE 26: BASE-CASE ANALYSIS — RESULTS OF RANDOM-EFFECTS MODEL FOR THE MEAN DIFFERENCE IN
WEIGHT FOR CANAGLIFLOZIN VERSUS ACTIVE COMPARATORS
Canagliflozin 100 mg Canagliflozin 300 mg SUCRA
Median SD 95% Crl Prob Median SD 95% Crl Prob
CANA 300 mg q.d.
x.xx x.xx –x.xx, x.xx x% NA NA NA NA xx%
CANA 100 mg q.d.
NA NA NA NA –x.xx x.xx –x.xx, x.xx xx% xx%
EXEN 10 mcg b.i.d.
–x.xx x.xx –x.xx, x.xx xx% –x.xx x.xx –x.xx, –x.xx xx% xx%
EXEN 5 mcg b.i.d. –x.xx x.xx –x.xx, x.xx xx% –x.xx x.xx –x.xx, –x.xx xx% xx%
Placebo –x.xx x.xx –x.xx, –x.xx xxx% –x.xx x.xx –x.xx, –x.xx xxx% xx%
LINA 5 mg q.d. –x.xx x.xx –x.xx, –x.xx xxx% –x.xx x.xx –x.xx, –x.xx xxx% xx%
SITA 100 mg q.d. –x.xx x.xx –x.xx, –x.xx xxx% –x.xx x.xx –x.xx, –x.xx xxx% xx%
Long-acting insulin
–x.xx x.xx –x.xx, –x.xx xxx% –x.xx x.xx –x.xx, –x.xx xxx% xx%
Biphasic insulin –x.xx x.xx –x.xx, –x.xx xxx% –x.xx x.xx –x.xx, –x.xx xxx% x%
b.i.d. = twice daily; CANA = canagliflozin; Crl = credible interval; EXEN = exenatide; LINA = linagliptin; NA = not applicable; prob = probability; q.d. = once daily; SD = standard deviation; SITA = sitagliptin; SUCRA = surface under the cumulative ranking.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
46
Common Drug Review September 2015
TABLE 27: BASE-CASE ANALYSIS — RESULTS OF FIXED-EFFECT MODEL FOR THE MEAN DIFFERENCE IN SYSTOLIC
BLOOD PRESSURE FOR CANAGLIFLOZIN VERSUS ACTIVE COMPARATORS
Canagliflozin 100 mg Canagliflozin 300 mg SUCRA
Median SD 95% Crl Prob Median SD 95% Crl Prob
CANA 100 mg q.d. NA NA NA NA 0.61 1.38 –2.07, 3.34 33% 89%
CANA 300 mg q.d. –0.61 1.38 –3.34, 2.07 67% NA NA NA NA 78%
Placebo –2.26 1.39 –5.01, 0.47 95% –1.66 1.39 –4.35, 1.10 88% 50%
Long-acting insulin
–4.17 2.47 –9.06, 0.69 95% –3.56 2.47 –8.43, 1.25 93% 26%
SITA 100 mg q.d. –5.76 1.66 –9.02, –2.53 100% –5.16 0.91 –6.94, –3.38 100% 7%
CANA = canagliflozin; Crl = credible interval; NA = not applicable; prob = probability; q.d. = once daily; SD = standard deviation; SITA = sitagliptin; SUCRA = surface under the cumulative ranking.
TABLE 28: BASE-CASE ANALYSIS — RESULTS OF FIXED-EFFECT MODEL FOR ODDS RATIO IN ALL HYPOGLYCEMIC
EVENTS FOR CANAGLIFLOZIN VERSUS ACTIVE COMPARATORS
Canagliflozin 100 mg Canagliflozin 300 mg SUCRA
Median SD 95% Crl Prob Median SD 95% Crl Prob
Placebo x.xx x.xx x.xx, x.xx 0% x.xx 0.91 x.xx, x.xx 0% 100%
EXEN 5 mcg b.i.d. x.xx x.xx x.xx, x.xx xx% x.xx 0.80 x.xx, x.xx 3% xx%
LINA 5 mg q.d. x.xx x.xx x.xx, x.xx xx% x.xx 0.68 x.xx, x.xx 2% 78%
CANA 100 mg NA NA NA NA x.xx 0.33 x.xx, x.xx 15% 56%
EXEN 10 mcg b.i.d.
x.xx 0.40 x.xx, x.xx xx% x.xx x.xx x.xx, x.xx xx% xx%
CANA 300 mg q.d.
0.78 0.20 x.xx, x.xx 85% NA NA NA NA 38%
SITA 100 mg q.d. 0.75 0.22 x.xx, x.xx 85% 0.96 0.14 x.xx, x.xx 60% 35%
Long-acting insulin
x.xx 0.19 x.xx, x.xx 99% x.xx 0.23 x.xx, x.xx 97% xx%
Biphasic insulin 0.24 0.13 0.10, 0.60 100% 0.31 0.16 x.xx, x.xx 100% 1%
b.i.d. = twice daily; CANA = canagliflozin; Crl = credible interval; EXEN = exenatide; LINA = linagliptin; NA = not applicable; prob = probability; q.d. = once daily; SD = standard deviation; SITA = sitagliptin; SUCRA = surface under the cumulative ranking.
FIGURE 11: MEAN CHANGE IN GLYCATED HEMOGLOBIN VALUE (PERCENTAGE) VERSUS PLACEBO
Confidential figure removed at manufacturer’s request.
CANA = canagliflozin; EXEN = LINA = linagliptin; LIRA = liraglutide; PIO = pioglitazone; q.d. = once daily; SITA = sitagliptin.
Critical Appraisal of Network Meta-analysis The quality of the manufacturer-submitted NMA was assessed according to recommendations provided by the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) Task Force on Indirect Treatment Comparisons.41 Details and commentary for each of the relevant items identified by ISPOR are provided in Table 29.
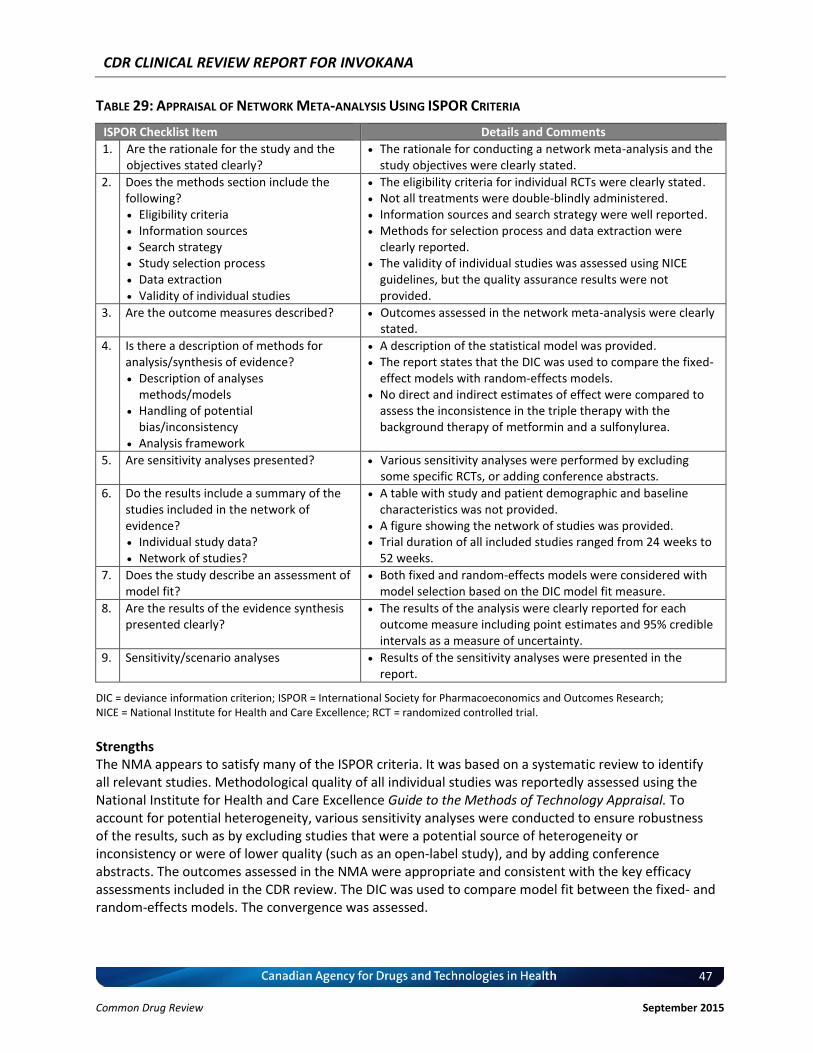
CDR CLINICAL REVIEW REPORT FOR INVOKANA
47
Common Drug Review September 2015
TABLE 29: APPRAISAL OF NETWORK META-ANALYSIS USING ISPOR CRITERIA
ISPOR Checklist Item Details and Comments
1. Are the rationale for the study and the objectives stated clearly?
The rationale for conducting a network meta-analysis and the study objectives were clearly stated.
2. Does the methods section include the following? Eligibility criteria Information sources Search strategy Study selection process Data extraction Validity of individual studies
The eligibility criteria for individual RCTs were clearly stated. Not all treatments were double-blindly administered. Information sources and search strategy were well reported. Methods for selection process and data extraction were
clearly reported. The validity of individual studies was assessed using NICE
guidelines, but the quality assurance results were not provided.
3. Are the outcome measures described? Outcomes assessed in the network meta-analysis were clearly stated.
4. Is there a description of methods for analysis/synthesis of evidence? Description of analyses
methods/models Handling of potential
bias/inconsistency Analysis framework
A description of the statistical model was provided. The report states that the DIC was used to compare the fixed-
effect models with random-effects models. No direct and indirect estimates of effect were compared to
assess the inconsistence in the triple therapy with the background therapy of metformin and a sulfonylurea.
5. Are sensitivity analyses presented? Various sensitivity analyses were performed by excluding some specific RCTs, or adding conference abstracts.
6. Do the results include a summary of the studies included in the network of evidence? Individual study data? Network of studies?
A table with study and patient demographic and baseline characteristics was not provided.
A figure showing the network of studies was provided. Trial duration of all included studies ranged from 24 weeks to
52 weeks.
7. Does the study describe an assessment of model fit?
Both fixed and random-effects models were considered with model selection based on the DIC model fit measure.
8. Are the results of the evidence synthesis presented clearly?
The results of the analysis were clearly reported for each outcome measure including point estimates and 95% credible intervals as a measure of uncertainty.
9. Sensitivity/scenario analyses Results of the sensitivity analyses were presented in the report.
DIC = deviance information criterion; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; NICE = National Institute for Health and Care Excellence; RCT = randomized controlled trial.
Strengths The NMA appears to satisfy many of the ISPOR criteria. It was based on a systematic review to identify all relevant studies. Methodological quality of all individual studies was reportedly assessed using the National Institute for Health and Care Excellence Guide to the Methods of Technology Appraisal. To account for potential heterogeneity, various sensitivity analyses were conducted to ensure robustness of the results, such as by excluding studies that were a potential source of heterogeneity or inconsistency or were of lower quality (such as an open-label study), and by adding conference abstracts. The outcomes assessed in the NMA were appropriate and consistent with the key efficacy assessments included in the CDR review. The DIC was used to compare model fit between the fixed- and random-effects models. The convergence was assessed.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
48
Common Drug Review September 2015
Limitations Although some patient characteristics in the individual studies were briefly presented in figures, the main patient demographic and study baseline characteristics were not provided; therefore, it is not clear whether they were comparable at baseline. The actual quality-assessment results were not provided in the report. The potential limitations included heterogeneity in terms of variable trial duration and baseline A1C, methodological quality of the individual study and definition of hypoglycemia. However, various sensitivity analysis results by excluding some specific RCTs showed no or minimal impact on the findings from base-case analysis; therefore, significant clinical impact of the heterogeneity on the overall findings in the NMA is unlikely.
Summary The manufacturer conducted a Bayesian NMA analysis based on a systematic review of RCTs comparing canagliflozin (100 mg once daily or 300 mg once daily) with other antihyperglycemic drugs, including biphasic and long-acting insulin, DPP-4 inhibitors (sitagliptin 100 mg and linagliptin 5 mg) and GLP-1 agonists (exenatide 5 mcg twice daily and 10 mcg twice daily) as third-line therapy for patients not adequately controlled with metformin and a sulfonylurea. It was reported that canagliflozin (100 mg once daily and 300 mg once daily) and biphasic insulin, long-acting insulin, sitagliptin 100 mg, exenatide 10 mcg, exenatide 5 mcg, and linagliptin 5 mg generally had similar effects on A1C, FPG, body weight, SBP, and hypoglycemia. Biphasic insulin showed statistically significantly lower FPG compared with canagliflozin (100 mg once daily and 300 mg once daily). Canagliflozin achieved a statistically significant lower body weight compared with insulin aspart. Compared with sitagliptin, treatment with canagliflozin demonstrated statistically significant and clinically meaningful reductions in SBP. The findings from this NMA appear to be reliable, although some methodological limitations exist.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
49
Common Drug Review September 2015
APPENDIX 5: SUMMARY OF OTHER STUDIES
Objective To summarize the findings of DIA3012: Efficacy and Safety of Canagliflozin Over 52 Weeks in Patients With Type 2 Diabetes on Background Metformin and Pioglitazone Therapy.42,43
Findings Study Characteristics DIA3012 was a randomized, double-blind, multi-centre, placebo-controlled trial. The objective of the trial was to assess the efficacy and safety of canagliflozin in patients with type 2 diabetes mellitus inadequately controlled with metformin and pioglitazone. The study consisted of a two-week run-in period and a 26-week placebo-controlled and double-blind core treatment period, followed by a 26-week, active-controlled, double-blind extension period. Inclusion criteria for the randomized controlled trial (RCT) included adults aged 18 to 80 years with type 2 diabetes on metformin (≥ 2,000 mg/day) and pioglitazone (30 mg/day or 45 mg/day) with a glycated hemoglobin (A1C) of ≥ 7.0% to ≤ 10.5% and a fasting plasma glucose (FPG) of < 15 mmol/L. Patients with an FPG of ≥ 15.0 mmol/L or higher or a history of type 1 diabetes were excluded. Patients (N = 342) were randomized to receive canagliflozin 100 mg, canagliflozin 300 mg, or placebo added onto their background therapy of metformin and pioglitazone. During the entire study, glycemic rescue therapy with glimepiride was initiated if required. During the 26-week extension period, patients who received placebo in the RCT phase were switched to sitagliptin 100 mg; the blinded switch from placebo to sitagliptin was performed to maintain the study’s double-blinding, but not to support active efficacy comparison at week 52 as treatments were not concurrently initiated. The primary outcome was change from baseline in A1C at week 26. Key secondary outcomes included A1C at 52 weeks; the proportion of patients reaching an A1C < 7.0%; FPG; systolic blood pressure (SBP); and body weight. Adverse events (AEs) over the 52-week treatment period were evaluated. Pre-specified AEs included urinary tract infections and genital mycotic infection, osmotic diuresis, volume depletion, and hypoglycemia. Sample size determination was based on showing the superiority of canagliflozin over placebo in reducing A1C from baseline to week 26. Efficacy outcomes were assessed using the modified intention-to-treat (mITT) population based on last observation carried forward. For patients who received glycemic rescue therapy, the last post-baseline value prior to initiation of rescue was used for analysis. An analysis of covariance model with treatment and stratification factors as fixed effects, and the corresponding baseline value for each end point as a covariate, was used to assess primary and continuous secondary end points. The dichotomous outcomes were analyzed with a logistic model with treatment and stratification factors as fixed effects and baseline A1C as a covariate. Patient Disposition A total of 342 patients were randomized and 296 (86.5%) completed the 26-week period. Study discontinuation rates were 8.0%, 11.4%, and 20.9% in the canagliflozin 100 mg, canagliflozin 300 mg, and placebo/sitagliptin groups, respectively. Of those who completed the study at 26 weeks, 289 entered the extension period and 263 completed 52 weeks of treatment. Discontinuation rates were 15.0%, 21.9%, and 32.2% over 52 weeks in the canagliflozin 100 mg, canagliflozin 300 mg, and placebo/sitagliptin groups, respectively (Figure 12).
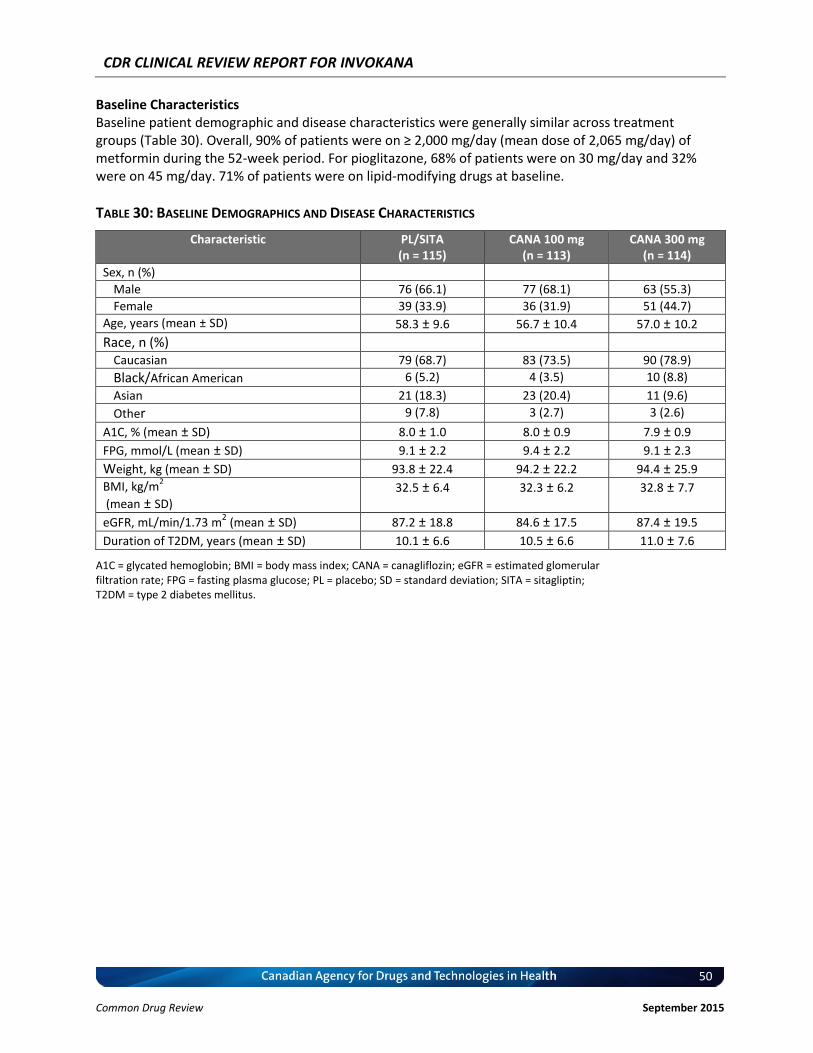
CDR CLINICAL REVIEW REPORT FOR INVOKANA
50
Common Drug Review September 2015
Baseline Characteristics Baseline patient demographic and disease characteristics were generally similar across treatment groups (Table 30). Overall, 90% of patients were on ≥ 2,000 mg/day (mean dose of 2,065 mg/day) of metformin during the 52-week period. For pioglitazone, 68% of patients were on 30 mg/day and 32% were on 45 mg/day. 71% of patients were on lipid-modifying drugs at baseline.
TABLE 30: BASELINE DEMOGRAPHICS AND DISEASE CHARACTERISTICS
Characteristic PL/SITA (n = 115)
CANA 100 mg (n = 113)
CANA 300 mg (n = 114)
Sex, n (%)
Male 76 (66.1) 77 (68.1) 63 (55.3)
Female 39 (33.9) 36 (31.9) 51 (44.7)
Age, years (mean ± SD) 58.3 ± 9.6 56.7 ± 10.4 57.0 ± 10.2
Race, n (%)
Caucasian 79 (68.7) 83 (73.5) 90 (78.9)
Black/African American 6 (5.2) 4 (3.5) 10 (8.8)
Asian 21 (18.3) 23 (20.4) 11 (9.6)
Other 9 (7.8) 3 (2.7) 3 (2.6)
A1C, % (mean ± SD) 8.0 ± 1.0 8.0 ± 0.9 7.9 ± 0.9
FPG, mmol/L (mean ± SD) 9.1 ± 2.2 9.4 ± 2.2 9.1 ± 2.3
Weight, kg (mean ± SD) 93.8 ± 22.4 94.2 ± 22.2 94.4 ± 25.9
BMI, kg/m2
(mean ± SD) 32.5 ± 6.4 32.3 ± 6.2 32.8 ± 7.7
eGFR, mL/min/1.73 m2 (mean ± SD) 87.2 ± 18.8 84.6 ± 17.5 87.4 ± 19.5
Duration of T2DM, years (mean ± SD) 10.1 ± 6.6 10.5 ± 6.6 11.0 ± 7.6
A1C = glycated hemoglobin; BMI = body mass index; CANA = canagliflozin; eGFR = estimated glomerular filtration rate; FPG = fasting plasma glucose; PL = placebo; SD = standard deviation; SITA = sitagliptin; T2DM = type 2 diabetes mellitus.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
51
Common Drug Review September 2015
FIGURE 12: PATIENT DISPOSITION IN DIA3012
Figure removed to comply with licensing restrictions and copyright law. The figure is available in Forst et al., 201443 CANA = canagliflozin; eGFR = estimated glomerular filtration rate; LOCF = last observation carried forward; mITT = modified intention-to-treat; PBO = placebo; SITA = sitagliptin. Efficacy a) Hemoglobin A1C At week 26, canagliflozin 100 mg and 300 mg significantly reduced A1C from baseline compared with placebo, with between-group differences of −0.62% and −0.76% with canagliflozin 100 mg and 300 mg, respectively (P < 0.001 for both). Reductions in A1C with canagliflozin 100 mg and 300 mg were sustained over 52 weeks of treatment (Figure 13B), with least squares mean (LSM) changes from baseline of −0.92% (95% confidence interval [CI], −1.06 to −0.79) and −1.03% (95% CI, −1.17 to −0.89), respectively, at week 52. A greater proportion of patients treated with canagliflozin 100 mg and 300 mg versus placebo achieved a A1C of < 7.0% at week 26 (P < 0.01 and P < 0.001, respectively), with additional modest increases observed at week 52 (Figure 13C).
FIGURE 13: CHANGES IN GLYCEMIC PARAMETERS
Figure removed to comply with licensing restrictions and copyright law. The figure is available in Forst et al., 201443
CANA = canagliflozin; CI = confidence interval; FPG = fasting plasma glucose; LOCF = last observation carried forward; LS = least squares; PBO = placebo; SE = standard error; wk = week. *P < 0.01 versus placebo; †P < 0.001 versus placebo. (A) Change in glycated hemoglobin (A1C) at week 26, (B) change in A1C at week 52, (C) proportion of patients achieving A1C < 7.0% at weeks 26 and 52, (D) change in FPG at week 26; and (E) change in FPG at week 52.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
52
Common Drug Review September 2015
b) Fasting Plasma Glucose Significant improvements from baseline in FPG were observed at week 26 with canagliflozin 100 mg and 300 mg compared with placebo; differences in the LSM change versus placebo were −1.6 mmol/L (−29.4 mg/dL) and −2.0 mmol/L (−35.7 mg/dL), respectively (P < 0.001 for both; Figure 13D). LSM changes (95% CI) in FPG from baseline at week 52 were −1.5 mmol/L (−1.8 to –1.2) and −1.8 mmol/L (−2.1 to −1.4) with canagliflozin 100 mg and 300 mg, respectively (Figure 13E). Mean FPG decreased from 9.3 mmol/L at week 26 to 8.6 mmol/L at week 52 in the placebo/sitagliptin group. c) Body Weight At week 26, significant dose-related reductions from baseline in body weight were observed with canagliflozin 100 mg and 300 mg compared with placebo; LSM percentage changes compared with placebo were −2.7% (−2.5 kg) and −3.7% (−3.5 kg), respectively (P < 0.001 for both; Figure 14A). LSM percentage changes (95% CI) in body weight from baseline at week 52 were −2.7% (−3.6 to –1.9) and −3.7% (−4.6 to −2.9) with canagliflozin 100 mg and 300 mg, respectively; mean absolute changes (95% CI) were −2.5 kg (−3.3 to −1.7) and−3.6 kg (−4.4 to −2.7) (Figure 14B). During the extension period from weeks 26 to 52, sitagliptin treatment was associated with a minimal change in body weight from 93.8 kg to 94.1 kg. At week 26, 28%, 39%, and 6% of patients achieved ≥ 5% body weight reduction with canagliflozin 100 mg, canagliflozin 300 mg, and placebo, respectively. At week 52, 26% and 36% of patients achieved ≥ 5% body weight reduction with canagliflozin 100 mg and canagliflozin 300 mg, respectively.
FIGURE 14: PERCENTAGE CHANGE IN BODY WEIGHT (LAST OBSERVATION CARRIED FORWARD)
Figure removed to comply with licensing restrictions and copyright law. The figure is available in Forst et al., 201443
CANA = canagliflozin; CI = confidence interval; LS = least squares; PBO = placebo; SE = standard error; wk = week. Note: (A) at week 26; (B) at week 52.
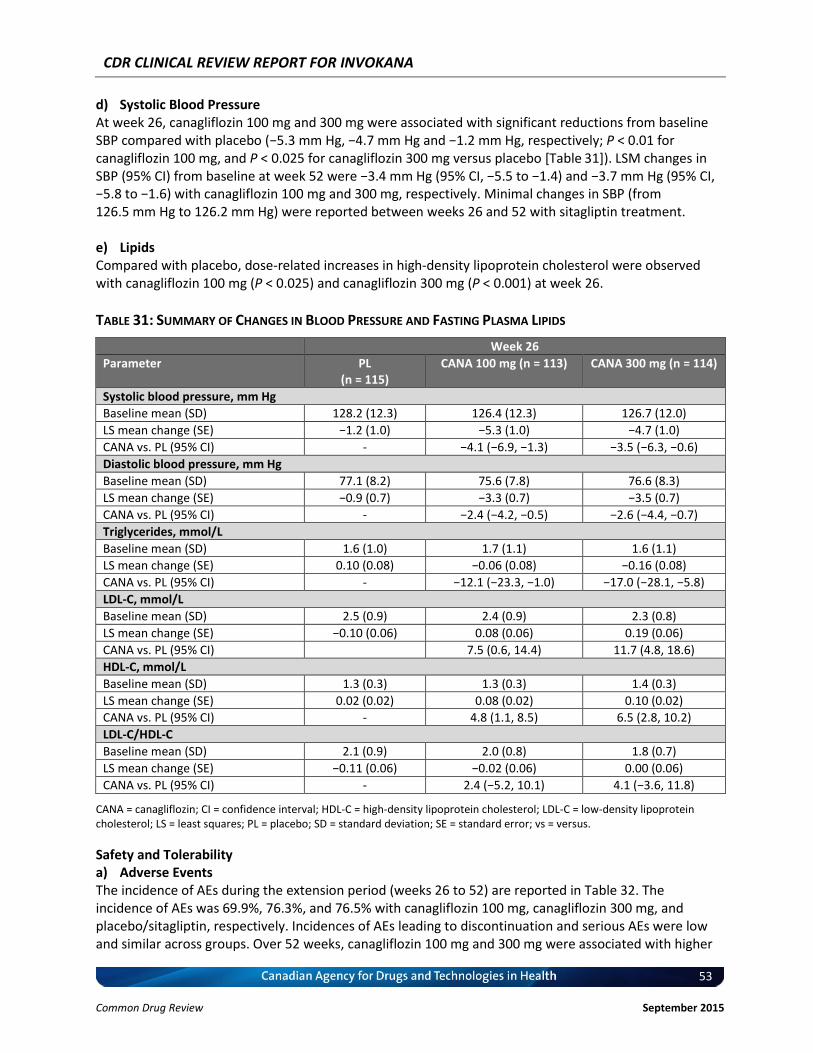
CDR CLINICAL REVIEW REPORT FOR INVOKANA
53
Common Drug Review September 2015
d) Systolic Blood Pressure At week 26, canagliflozin 100 mg and 300 mg were associated with significant reductions from baseline SBP compared with placebo (−5.3 mm Hg, −4.7 mm Hg and −1.2 mm Hg, respectively; P < 0.01 for canagliflozin 100 mg, and P < 0.025 for canagliflozin 300 mg versus placebo [Table 31]). LSM changes in SBP (95% CI) from baseline at week 52 were −3.4 mm Hg (95% CI, −5.5 to −1.4) and −3.7 mm Hg (95% CI, −5.8 to −1.6) with canagliflozin 100 mg and 300 mg, respectively. Minimal changes in SBP (from 126.5 mm Hg to 126.2 mm Hg) were reported between weeks 26 and 52 with sitagliptin treatment. e) Lipids Compared with placebo, dose-related increases in high-density lipoprotein cholesterol were observed with canagliflozin 100 mg (P < 0.025) and canagliflozin 300 mg (P < 0.001) at week 26.
TABLE 31: SUMMARY OF CHANGES IN BLOOD PRESSURE AND FASTING PLASMA LIPIDS
Week 26
Parameter PL (n = 115)
CANA 100 mg (n = 113) CANA 300 mg (n = 114)
Systolic blood pressure, mm Hg
Baseline mean (SD) 128.2 (12.3) 126.4 (12.3) 126.7 (12.0)
LS mean change (SE) −1.2 (1.0) −5.3 (1.0) −4.7 (1.0)
CANA vs. PL (95% CI) - −4.1 (−6.9, −1.3) −3.5 (−6.3, −0.6)
Diastolic blood pressure, mm Hg
Baseline mean (SD) 77.1 (8.2) 75.6 (7.8) 76.6 (8.3)
LS mean change (SE) −0.9 (0.7) −3.3 (0.7) −3.5 (0.7)
CANA vs. PL (95% CI) - −2.4 (−4.2, −0.5) −2.6 (−4.4, −0.7)
Triglycerides, mmol/L
Baseline mean (SD) 1.6 (1.0) 1.7 (1.1) 1.6 (1.1)
LS mean change (SE) 0.10 (0.08) −0.06 (0.08) −0.16 (0.08)
CANA vs. PL (95% CI) - −12.1 (−23.3, −1.0) −17.0 (−28.1, −5.8)
LDL-C, mmol/L
Baseline mean (SD) 2.5 (0.9) 2.4 (0.9) 2.3 (0.8)
LS mean change (SE) −0.10 (0.06) 0.08 (0.06) 0.19 (0.06)
CANA vs. PL (95% CI) 7.5 (0.6, 14.4) 11.7 (4.8, 18.6)
HDL-C, mmol/L
Baseline mean (SD) 1.3 (0.3) 1.3 (0.3) 1.4 (0.3)
LS mean change (SE) 0.02 (0.02) 0.08 (0.02) 0.10 (0.02)
CANA vs. PL (95% CI) - 4.8 (1.1, 8.5) 6.5 (2.8, 10.2)
LDL-C/HDL-C
Baseline mean (SD) 2.1 (0.9) 2.0 (0.8) 1.8 (0.7)
LS mean change (SE) −0.11 (0.06) −0.02 (0.06) 0.00 (0.06)
CANA vs. PL (95% CI) - 2.4 (−5.2, 10.1) 4.1 (−3.6, 11.8)
CANA = canagliflozin; CI = confidence interval; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol; LS = least squares; PL = placebo; SD = standard deviation; SE = standard error; vs = versus.
Safety and Tolerability a) Adverse Events The incidence of AEs during the extension period (weeks 26 to 52) are reported in Table 32. The incidence of AEs was 69.9%, 76.3%, and 76.5% with canagliflozin 100 mg, canagliflozin 300 mg, and placebo/sitagliptin, respectively. Incidences of AEs leading to discontinuation and serious AEs were low and similar across groups. Over 52 weeks, canagliflozin 100 mg and 300 mg were associated with higher
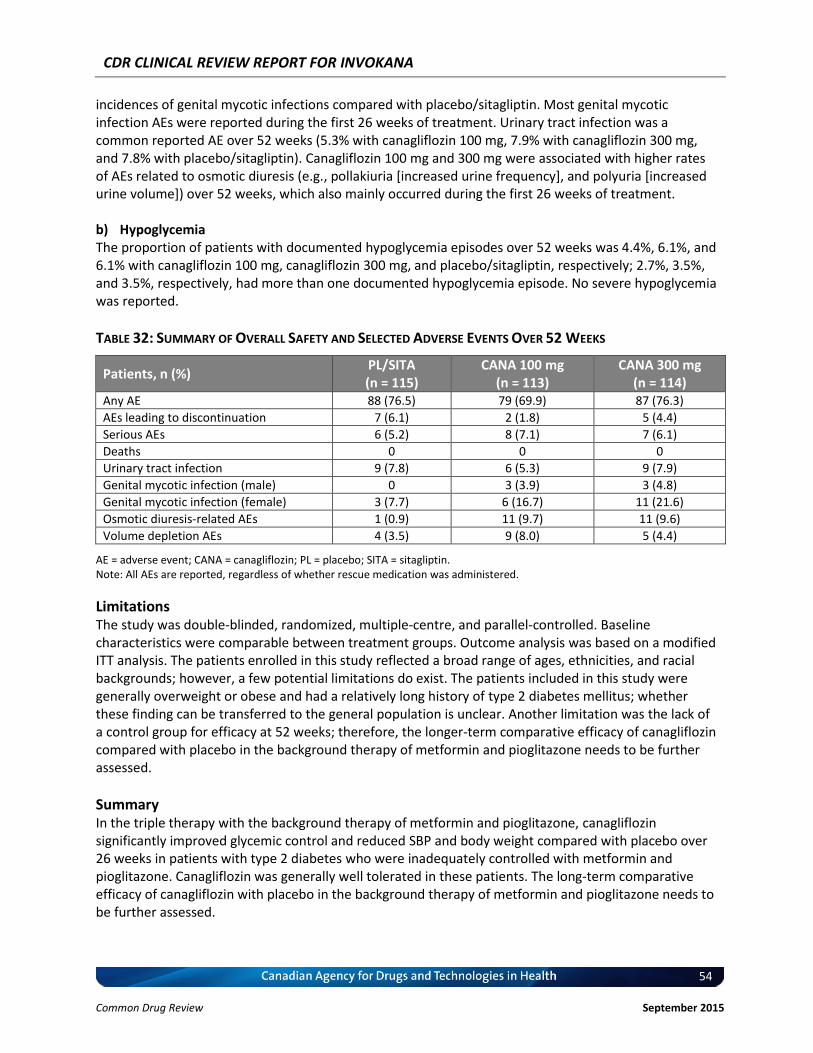
CDR CLINICAL REVIEW REPORT FOR INVOKANA
54
Common Drug Review September 2015
incidences of genital mycotic infections compared with placebo/sitagliptin. Most genital mycotic infection AEs were reported during the first 26 weeks of treatment. Urinary tract infection was a common reported AE over 52 weeks (5.3% with canagliflozin 100 mg, 7.9% with canagliflozin 300 mg, and 7.8% with placebo/sitagliptin). Canagliflozin 100 mg and 300 mg were associated with higher rates of AEs related to osmotic diuresis (e.g., pollakiuria [increased urine frequency], and polyuria [increased urine volume]) over 52 weeks, which also mainly occurred during the first 26 weeks of treatment. b) Hypoglycemia The proportion of patients with documented hypoglycemia episodes over 52 weeks was 4.4%, 6.1%, and 6.1% with canagliflozin 100 mg, canagliflozin 300 mg, and placebo/sitagliptin, respectively; 2.7%, 3.5%, and 3.5%, respectively, had more than one documented hypoglycemia episode. No severe hypoglycemia was reported.
TABLE 32: SUMMARY OF OVERALL SAFETY AND SELECTED ADVERSE EVENTS OVER 52 WEEKS
Patients, n (%) PL/SITA (n = 115)
CANA 100 mg (n = 113)
CANA 300 mg (n = 114)
Any AE 88 (76.5) 79 (69.9) 87 (76.3)
AEs leading to discontinuation 7 (6.1) 2 (1.8) 5 (4.4)
Serious AEs 6 (5.2) 8 (7.1) 7 (6.1)
Deaths 0 0 0
Urinary tract infection 9 (7.8) 6 (5.3) 9 (7.9)
Genital mycotic infection (male) 0 3 (3.9) 3 (4.8)
Genital mycotic infection (female) 3 (7.7) 6 (16.7) 11 (21.6)
Osmotic diuresis-related AEs 1 (0.9) 11 (9.7) 11 (9.6)
Volume depletion AEs 4 (3.5) 9 (8.0) 5 (4.4)
AE = adverse event; CANA = canagliflozin; PL = placebo; SITA = sitagliptin. Note: All AEs are reported, regardless of whether rescue medication was administered.
Limitations The study was double-blinded, randomized, multiple-centre, and parallel-controlled. Baseline characteristics were comparable between treatment groups. Outcome analysis was based on a modified ITT analysis. The patients enrolled in this study reflected a broad range of ages, ethnicities, and racial backgrounds; however, a few potential limitations do exist. The patients included in this study were generally overweight or obese and had a relatively long history of type 2 diabetes mellitus; whether these finding can be transferred to the general population is unclear. Another limitation was the lack of a control group for efficacy at 52 weeks; therefore, the longer-term comparative efficacy of canagliflozin compared with placebo in the background therapy of metformin and pioglitazone needs to be further assessed.
Summary In the triple therapy with the background therapy of metformin and pioglitazone, canagliflozin significantly improved glycemic control and reduced SBP and body weight compared with placebo over 26 weeks in patients with type 2 diabetes who were inadequately controlled with metformin and pioglitazone. Canagliflozin was generally well tolerated in these patients. The long-term comparative efficacy of canagliflozin with placebo in the background therapy of metformin and pioglitazone needs to be further assessed.

CDR CLINICAL REVIEW REPORT FOR INVOKANA
55
Common Drug Review September 2015
REFERENCES
1. PrInvokana™ (canagliflozin tablets): 100 mg and 300 mg as anhydrous canagliflozin [product monograph]. Toronto (ON): Janssen, Inc.; 2014 May 22.
2. Clinical Study Report: 28431754DIA3002; Phase 3. A randomized, double-blind, placebo-controlled, 3-arm, parallel-group, multicenter study, to evaluate the efficacy, safety, and tolerability of canagliflozin in the treatment of subjects with Type 2 Diabetes Mellitus with inadequate glycemic control on metformin and sulphonylurea therapy [CONFIDENTIAL internal manufacturer's report]. Toronto (ON): Janssen Inc.; 2012 Apr 18.
3. Clinical Study Report: 28431754DIA3015; Phase 3. A randomized, double-blind, active-controlled, multicenter study to evaluate the efficacy, safety, and tolerability of canagliflozin versus sitagliptin in the treatment of subjects with Type 2 Diabetes Mellitus with inadequate glycemic control on Metformin and Sulphonylurea therapy [CONFIDENTIAL internal manufacturer's report]. Toronto (ON): Janssen Inc.; 2012 May 7.
4. Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Canadian Diabetes Association 2013 clinical practice guidelines for the prevention and management of diabetes in Canada. Can J Diabetes [Internet]. 2013 Apr [cited 2014 Oct 27];37(suppl 1):S1-S212. Available from: http://guidelines.diabetes.ca/App_Themes/CDACPG/resources/cpg_2013_full_en.pdf
5. Public Health Agency of Canada. Diabetes in Canada: facts and figures from a public health perspective: report highlights [Internet]. Ottawa: PHAC; 2011. [cited 2014 Oct 27]. Available from: http://www.phac-aspc.gc.ca/cd-mc/publications/diabetes-diabete/facts-figures-faits-chiffres-2011/highlights-saillants-eng.php
6. Canadian Diabetes Association. The prevalence and costs of diabetes [Internet]. Ottawa: CDA; 2012. [cited 2014 Oct 27]. Available from: http://www.diabetes.ca/documents/about-diabetes/PrevalanceandCost_09.pdf
7. Health: type 2 diabetes [Internet]. Ottawa: Government of Canada; 2013. [cited 2014 Oct 27]. Available from: http://healthycanadians.gc.ca/diseases-conditions-maladies-affections/disease-maladie/diabete-eng.php
8. Canadian Agency for Drugs and Technologies in Health. Second-line pharmacotherapy for type 2 diabetes - update [Internet]. Ottawa (ON): The Agency; 2013. (CADTH optimal use report; vol.3, no. 1a). [cited 2014 Oct 27]. Available from: http://www.cadth.ca/media/pdf/OP0512_DiabetesUpdate_Second-line_e.pdf
9. Canadian Agency for Drugs and Technologies in Health. Third-line pharmacotherapy for type 2 diabetes — Update [Internet]. Ottawa (ON): The Agency; 2013. [cited 2014 Aug 14]. (CADTH optimal use report; vol. 3, no. 1b). Available from: www.cadth.ca/media/pdf/OP0512_Diabetes%20Update_Third-line_e.pdf
10. Canadian Agency for Drugs and Technologies in Health. Third-line pharmacotherapy for type 2 diabetes — Erratum [Internet]. Ottawa (ON): The Agency; 2014 May. [cited 2014 Aug 14]. Available from: www.cadth.ca/media/pdf/Diabetes%20Update%20-%20Erratum%20-%20Third-line.pdf
11. CDR submission: Invokanatm (canagliflozin) 100mg and 300mg once-daily (q.d) tablets. Company: Janssen, Inc. [CONFIDENTIAL manufacturer's submission]. Toronto (ON): Janssen, Inc; 2014.
CDR CLINICAL REVIEW REPORT FOR INVOKANA
56
Common Drug Review September 2015
12. Center for Drug Evaluation and Research, U.S. Food and Drug Administration. Statistical review(s) [Internet]. In: Invokana (Canagliflozin). Company: Janssen Research & Development, LLC. Application no.: NDA 204042. Approval date: 29/03/2013. Rockville (MD): FDA; 2013 [cited 2014 Aug 6]. (FDA drug approval package). Available from: www.accessdata.fda.gov/drugsatfda_docs/nda/2013/204042Orig1s000StatR.pdf.
13. Health Canada reviewer's report: Invokana (canagliflozin) [CONFIDENTIAL internal report]. Ottawa: Therapeutics Products Directorate, Health Canada; 2014 May 22.
14. Committee for Medicinal Products for Human Use (CHMP). European Public Assessment Report (EPAR): Canagliflozin [Internet]. London: European Medicines Agency; 2013 Sep 19. [cited 2014 Sep 11]. Available from: www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/002649/WC500156457.pdf
15. Glucotrol® (glipizide) tablets for oral use [product monograph]. New York (NY): Pfizer Inc; 2013 Oct.
16. Glucotrol XL® (glipizide) extended release tablets for oral use [product monograph]. New York (NY): Pfizer Inc.; 2013 Oct.
17. Sulfonylureas. 2012 [cited 2014 Aug 14]. In: e-CPS [Internet]. Ottawa (ON): Canadian Pharmacists Association; 2009 - . Available from: https://www.e-therapeutics.ca Subscription required.
18. Advisory committee briefing document Pargluva™ (Muraglitazar, BMS-298585): NDA 21-865 [Internet]. Silver Spring (MD): Endocrinologic and Metabolic Drugs Advisory Committee, U.S. Food and Drug Administration; 2005 Sep 9. [cited 2014 Aug 14]. Available from: http://www.fda.gov/ohrms/dockets/ac/05/briefing/2005-4169B2_01_01-BMS-Pargluva.pdf
19. Center for Drug Evaluation and Research. Guidance for industry. Diabetes Mellitus: developing drugs and therapeutic biologics for treatment and prevention (draft guidance) [Internet]. Silver Spring (MD): Food and Drug Administration; 2008 Feb. [cited 2014 Aug 14]. Available from: www.fda.gov/downloads/Drugs/Guidances/ucm071624.pdf
20. Committee for Medicinal Products for Human Use (CHMP). Guideline on clinical investigation of medicinal products in the treatment or prevention of diabetes mellitus. London: European Medicines Agency; 2012 May 14. [cited 2014 Aug 14]. Available from: www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2012/06/WC500129256.pdf
21. Schernthaner G, Gross JL, Rosentock J, Guarisco M, Fu M, Yee J, et al. Canagliflozin compared with sitagliptin for patients with type 2 Diabetes who do not have adequate glycemic control with metformin plus sulfonylurea: a 52-week randomized trial. Diabetes Care. 2013;36:2508-15.
22. Common Drug Review. CEDAC final recommendation: sitagliptin resubmission (Januvia – Merck Frosst Canada Ltd.). Indication: Type 2 Diabetes Mellitus [Internet]. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2010. [cited 2014 Aug 13]. Available from: http://www.cadth.ca/media/cdr/complete/cdr_complete_Januvia%20Resubmission_June-29-2010.pdf
23. Common Drug Review. CEDAC final recommendation: linagliptin (Trajenta - Boehringer Ingelheim Canada). Indication: Type 2 Diabetes Mellitus [Internet]. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2012. [cited 2014 Aug 13]. Available from: http://www.cadth.ca/media/cdr/complete/cdr_complete_Trajenta_February_18_2012.pdf
CDR CLINICAL REVIEW REPORT FOR INVOKANA
57
Common Drug Review September 2015
24. Common Drug Review. CEDAC final recommendation: saxagliptin (Onglyza -- Bristol-Myers Squibb Canada and AstraZeneca Canada). Indication: Type 2 Diabetes Mellitus [Internet]. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2013. [cited 2014 Aug 13]. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/complete_SR0329_Onglyza-preNOC_19-Nov-13_e.pdf
25. Canagliflozin in combination therapy for treating type 2 diabetes [Internet]. London (UK): National Institute for Health and Care Excellence; 2014 Jun. [cited 2014 Sep 11]. (NICE technology appraisal guidance 315). Available from: www.nice.org.uk/guidance/ta315/resources/guidance-canagliflozin-in-combination-therapy-for-treating-type2-diabetes-pdf
26. Bolen S, Feldman L, Vassy J, Wilson L, Yeh HC, Marinopoulos S, et al. Systematic review: comparative effectiveness and safety of oral medications for type 2 diabetes mellitus. Ann Intern Med. 2007 Sep 18;147(6):386-99.
27. Selvin E, Bolen S, Yeh HC, Wiley C, Wilson LM, Marinopoulos SS, et al. Cardiovascular outcomes in trials of oral diabetes medications: a systematic review. Arch Intern Med [Internet]. 2008 Oct 27 [cited 2014 Oct 27];168(19):2070-80. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2765722
28. Edwards KL, Alvarez C, Irons BK, Fields J. Third-line agent selection for patients with type 2 diabetes mellitus uncontrolled with sulfonylureas and metformin. Pharmacotherapy. 2008 Apr;28(4):506-21.
29. Richter B, Bandeira-Echtler E, Bergerhoff K, Lerch CL. Dipeptidyl peptidase-4 (DPP-4) inhibitors for type 2 diabetes mellitus. Cochrane Database Syst Rev. 2008;(2):CD006739.
30. Neal B, Perkovic V, de Zeeuw D, Mahaffey KW, Fulcher G, Stein P, et al. Rationale, design, and baseline characteristics of the Canagliflozin Cardiovascular Assessment Study (CANVAS)--a randomized placebo-controlled trial. Am Heart J. 2013 Aug;166(2):217-23.
31. ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US); 2000 -. NCT01989754, A Study of the Effects of Canagliflozin (JNJ-28431754) on Renal Endpoints in Adult Participants With Type 2 Diabetes Mellitus (CANVAS-R); 2014 [cited 2014 Aug 13]. Available from: http://clinicaltrials.gov/ct2/show/NCT01989754?term=canvas-R&rank=1
32. National Institute for Health and Clinical Excellence. Newer agents for blood glucose control in Type 2 Diabetes (supplement) [Internet]. London (UK): NICE; 2009. [cited 2014 Aug 14]. (NICE Clinical Guidelines, No. 87S). Available from: http://www.ncbi.nlm.nih.gov/books/NBK61930/
33. Committee for Medicinal Products for Human Use (CHMP). European Public Assessment Report (EPAR): Forxiga (dapaglifozin) [Internet]. London: European Medicines Agency; 2012 Sep 8. [cited 2014 Aug 13]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/002322/WC500136024.pdf
34. Committee for Medicinal Products for Human Use (CHMP). Forxiga: product information [Internet]. London: European Medicines Agency; 2014. [cited 2014 Aug 13]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/002322/WC500136024.pdf
35. e-CPS [Internet]. Ottawa: Canadian Pharmacists Association; 2009 -. MetforminPr; 2012 Jun [cited 2014 Sep 23]. Available from: https://www.e-therapeutics.ca Subscription required.
36. Systematic literature review and meta-analysis of treatments of type 2 diabetes: study report [CONFIDENTIAL report]. Vernier, Switzerland: Amaris; 2013 Oct.
https://www.cadth.ca/sites/default/files/cdr/complete/complete_SR0329_Onglyza-preNOC_19-Nov-13_e.pdf

CDR CLINICAL REVIEW REPORT FOR INVOKANA
58
Common Drug Review September 2015
37. Systematic literature review and meta-analysis of treatments of type 2 diabetes: update of MET + SU analysis [CONFIDENTIAL report]. Vernier, Switzerland: Amaris; 2014 Feb.
38. Lu G, Ades AE. Combination of direct and indirect evidence in mixed treatment comparisons. Stat Med. 2004 Oct 30;23(20):3105-24.
39. Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J Clin Epidemiol. 1997 Jun;50(6):683-91.
40. Dias S, Welton NJ, Sutton AJ, Caldwell DM, Lu G, Ades AE. NICE DSU technical support document 4: inconsistency in networks of evidence based on randomised controlled trials [Internet]. Sheffield (UK): National Institute for Health and Clinical Excellence, Decision Support Unit; 2011 May. [cited 2014 Apr 22]. Available from: http://www.nicedsu.org.uk/TSD4%20Inconsistency.final.15April2014.pdf
41. Jansen JP, Fleurence R, Devine B, Itzler R, Barrett A, Hawkins N, et al. Interpreting indirect treatment comparisons and network meta-analysis for health-care decision making: report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: part 1. Value Health. 2011 Jun;14(4):417-28.
42. Clinical Study Report: 28431754DIA3012; Phase 3. A randomized, double-blind, placebo-controlled, 3-arm, parallel-group, 26-week multicenter study with a 26-week extension to evaluate the efficacy, safety, and tolerability of JNJ-28431754 (canagliflozin) compared with placebo in the treatment of subjects with Type 2 Diabetes Mellitus with inadequate glycemic control on metformin and pioglitazone therapy [CONFIDENTIAL internal manufacturer's report]. Raritan, NJ: Janssen Research & Development, LLC; 2012 Apr 5.
43. Forst T, Guthrie R, Goldenberg R, Yee J, Vijapurkar U, Meininger G, et al. Efficacy and safety of canagliflozin over 52 weeks in patients with type 2 diabetes on background metformin and pioglitazone. Diabetes Obes Metab. 2014 May;16(5):467-77.


















