Clinical Reasoning and Proof of Value in Acute Care ... · Clinical Reasoning and Proof of Value in...
23
3/19/2018 1 Clinical Reasoning and Proof of Value in Acute Care Physical Therapy Practice Michael Bang PT, OCS Ryan Elliott PT, OCS, FAAOMPT Cristen Clark PT, OCS, FAAOMPT Michael Ross PT, DHSc, OCS Objectives (Part 1) • Encourage • Continue using the Fundamentals of Practice • Chart Review • History • Examination • Continuum of Care • Challenge • Synthesize and Act on Exam Findings • Enhance Clinical Reasoning • Know & Articulate your VALUE Objectives: Acute Care PT (Part 2) • Describe the current state of clinical practice • Analyze the clinical impact of PT intervention in the acute space • Describe redesign of acute care PT within a major medical system • Highlight acute care PT value through clinical reasoning • Case Vignettes Why US?? • Senior Faculty: Manual Therapy Fellowship • 8-12 hours/week of Acute Care Practice • Clinical Reasoning>>OMT technique • Emphasize patient care across the continuum • “Be a great PT” • Fellowship graduates: • Academia • Acute care supervisors • Pediatrics • Fellowship Coordinators • Embedded into special operations in the military A Battle is Being Waged • Early Mobility • YES, and we are SO much more than mobility • Multidisciplinary Collaboration • System Change is Required • How? • Extreme variation in practice Acute Care PT is a Career • Acute care PT has often been ill-defined & under-studied • Limited data: • Outcomes? • Efficiencies? • Staffing? • Acute care PT positions are historically difficult to recruit/retain • Acute is a “stepping stone” to other PT positions • Pay your dues…
Transcript of Clinical Reasoning and Proof of Value in Acute Care ... · Clinical Reasoning and Proof of Value in...

3/19/2018
1
Clinical Reasoning and Proof of Value in Acute Care Physical
Therapy Practice Michael Bang PT, OCS
Ryan Elliott PT, OCS, FAAOMPT Cristen Clark PT, OCS, FAAOMPT
Michael Ross PT, DHSc, OCS
Objectives (Part 1)
• Encourage • Continue using the Fundamentals of Practice
• Chart Review • History • Examination • Continuum of Care
• Challenge • Synthesize and Act on Exam Findings • Enhance Clinical Reasoning • Know & Articulate your VALUE
Objectives: Acute Care PT (Part 2)
• Describe the current state of clinical practice
• Analyze the clinical impact of PT intervention in the acute space
• Describe redesign of acute care PT within a major medical system
• Highlight acute care PT value through clinical reasoning • Case Vignettes
Why US??
• Senior Faculty: Manual Therapy Fellowship • 8-12 hours/week of Acute Care Practice
• Clinical Reasoning>>OMT technique • Emphasize patient care across the continuum • “Be a great PT”
• Fellowship graduates: • Academia • Acute care supervisors • Pediatrics • Fellowship Coordinators • Embedded into special operations in the military
A Battle is Being Waged
• Early Mobility • YES, and we are SO much more than mobility
• Multidisciplinary Collaboration
• System Change is Required • How?
• Extreme variation in practice
Acute Care PT is a Career
• Acute care PT has often been ill-defined & under-studied • Limited data:
• Outcomes? • Efficiencies?
• Staffing?
• Acute care PT positions are historically difficult to recruit/retain
• Acute is a “stepping stone” to other PT positions • Pay your dues…

3/19/2018
2
What we’re not…
• Assist with RASS
• CAM-ICU
• PEEP
• Spontaneous breathing trials
Value in PT
• Kaiser Permanente: REDESIGN Northern California Rehab Services
• How do we show Value in Acute Care PT? • Literature Review
• Clinician Engagement
• Academy of Acute Care’s 2015 Core Competencies
Value in Physical Therapy…
• Research emphasis has been dominated by outpatient orthopedics
• Timing of PT intervention matters • Cost of LBP management are exploding • Patient education is imperative early in the episode of care • Practice paradigms vary widely
• Ramifications of Reduced Fear/Anxiety
• Improved Patient Outcomes
• Reduced Downstream Healthcare Utilization
Grandpa Elliott: circa 2002
• After his 2nd PT session in the hospital
• “Oh, so you’re like a dog-walker for humans”…
Current Role
• Discharge Disposition…
What do we have to offer…
• Rehabilitation Excellence • FUNDAMENTALS
• Chart Review • History • Physical Exam
• Differential Diagnosis
• Champions of Mobility • PT/RN partnership • Multidisciplinary Mobility Training
• Continuum of Care/Discharge Disposition
• Clinical Reasoning

3/19/2018
3
RISK/BENEFIT…
• Mobility
• Empowers patients
• Reduces delirium & HAP
• Promotes functional independence • (+) predictor of returning home
• Shorter LOS
• Has almost no negative side effects
• In contrast…
• Immobility makes every organ system worse
• Skin breakdown
• Weakness & loss of muscle mass depression
• Poor circulation/risk of DVT
• Glucose intolerance
• Weak cough & respiratory muscles
• Constipation
Recovery…Happily Ever After?
• FIM score after 7 days of Vent: • Independent risk factor for 1 year mortality rate
• Severe disability at 1 and 5 years after Critical Illness
• PICS
• ARDS
• ICU-AW
• Sepsis
• Kyle Ridgeway…2/23 • Outcomes after Critical Care
Hospital Readmission Studies Hospital Associated Deconditioning (HAD)
• 68% of patients discharged from postacute care settings are below PLOF
• Functional mobility? • >85% of time lying in bed
• Hospitalized adults 61 times more likely to have ADL limitation compared to non-hospitalized adults
Post Hospital Syndrome (PHS) • Older adults with poor physical function have 3x the odds
of readmission compared to medically complex patients that have high physical function
• Falvey et al, 2016
Importance of Mobility
• 10 year study of 22,289 participants • 15% readmission rate within 30 days
• 16.9% with no functional impairment • 18.8% with ≥1 ADL difficulty
• 18.4% with dependence in 1–2 ADLs
• 25.7% with dependence in ≥3 ADLs
Greyson et al. Functional Impairment and Hospital Readmission in Medicare Seniors (2015)
Why is Patient Mobility SO Important?
• 449 participants >70 years old • Patients fully independent in ADLs 2 weeks prior to hospitalization
• Dependence in >1 ADL at discharge • Dependence=needing assistance from another person for that task
• 1 year prospective study regarding recovery, dependence & mortality • 27% still had dependence in ADLs
• 37% mortality rate
• Barnes et al. Prediction of Recovery, Dependence or Death in Elders Who Become Disabled During Hospitalization, 2012

3/19/2018
4
SUMMARY
• This is not adhesive capsulitis…
• Disability s/p hospitalization is not “self limiting”
“Don’t people already know this?” Jenna Elliott, non-PT, wife, harsh critic
You may know…
• This conference defines selection bias
• What is the standard of care across this country?
• Do your colleagues know? • Every patient?
• Disclosure: • Proof of value never stops—and shouldn’t
• Kaiser Permanente: Engaged in mobility and clinical reasoning culture shift • Imperfectly
Kaiser Permanente Northern California: Rehabilitation Redesign • Quality Patient Care
• Sustainable Practice
• Consistent Patient Care Experience
To Know our Value is Important… To Show Value is Imperative • How do we define our practice?
• Rehabilitative vs Consultative?
• Reimbursement-driven care
• How do we demonstrate this value to senior hospital leadership? • What is the optimal frequency and duration of care in the acute space?
Engagement: Regional Decision-Makers
• Previously: Limited/No PT representation
• Regional Director of Rehabilitation Services
• Clinician Directors
• Average PT is concerned over the state of practice • What do we DO about it?
3/19/2018
5
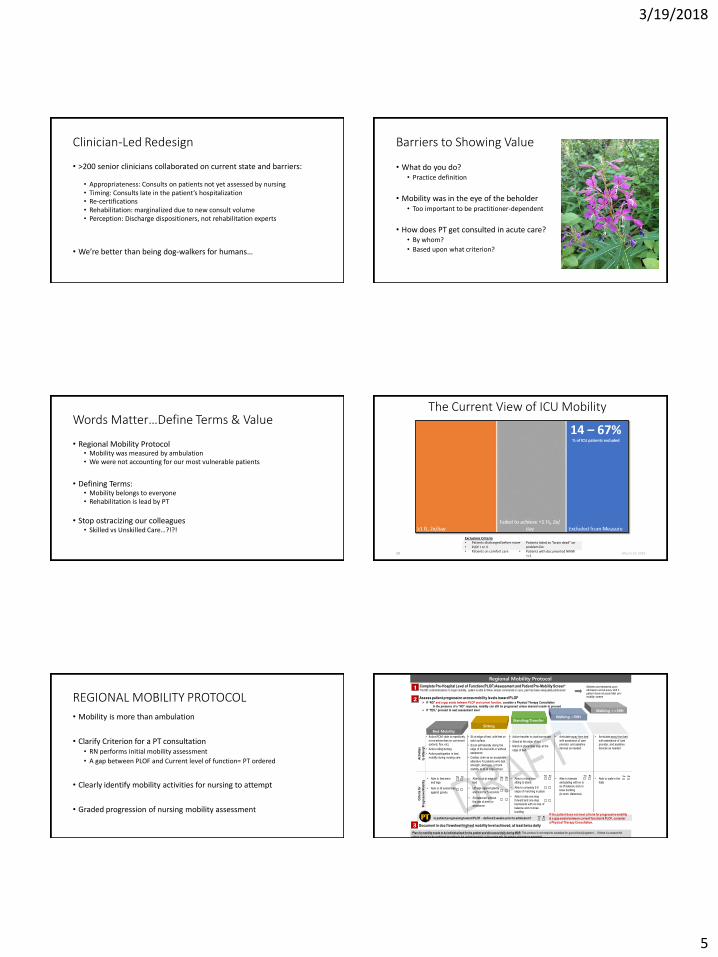
Clinician-Led Redesign
• >200 senior clinicians collaborated on current state and barriers:
• Appropriateness: Consults on patients not yet assessed by nursing • Timing: Consults late in the patient’s hospitalization • Re-certifications • Rehabilitation: marginalized due to new consult volume • Perception: Discharge dispositioners, not rehabilitation experts
• We’re better than being dog-walkers for humans…
Barriers to Showing Value
• What do you do? • Practice definition
• Mobility was in the eye of the beholder • Too important to be practitioner-dependent
• How does PT get consulted in acute care? • By whom?
• Based upon what criterion?
Words Matter…Define Terms & Value
• Regional Mobility Protocol • Mobility was measured by ambulation • We were not accounting for our most vulnerable patients
• Defining Terms: • Mobility belongs to everyone • Rehabilitation is lead by PT
• Stop ostracizing our colleagues • Skilled vs Unskilled Care…?!?!
28 March 19, 2018
The Current View of ICU Mobility
Exclusions Criteria • Patients discharged before noon • PLOF I or II • Patients on comfort care
• Patients listed as “brain dead” on problem list
• Patients with documented NMW <=1
14 – 67% % of ICU patients excluded
REGIONAL MOBILITY PROTOCOL
• Mobility is more than ambulation
• Clarify Criterion for a PT consultation • RN performs initial mobility assessment
• A gap between PLOF and Current level of function= PT ordered
• Clearly identify mobility activities for nursing to attempt
• Graded progression of nursing mobility assessment
Bed Mobility
Sitting
Standing/Transfer Walking <50ft
Walking >=50ft
Regional Mobility Protocol
Ac
tiv
itie
s
to A
tte
mp
t
• Active ROM: able to repetitively
move extremities on command
(extend, flex, etc)
• Active rolling/turning
• Active participation in bed
mobility during nursing care
• Sit at edge of bed, with feet on
solid surface.
• Scoot self laterally along the
edge of the bed with or without
assistance
• Cardiac chair as an acceptable
alterative for patients who lack
strength, alertness, or trunk
stability to sit at edge of bed
• Active transfer to chair/commode
• Stand at the edge of bed
• March in place/Side step at the
edge of bed
• Ambulate away from bed
with assistance of care
provider, and assistive
devices as needed
• Ambulate away from bed
with assistance of care
provider, and assistive
devices as needed
Cri
teri
a fo
r
Pro
gre
ss
ive
Mo
bil
ity
• Able to feel arms
and legs
• Able to lift extremities
against gravity
• Able to sit at edge of
bed
• Lift legs against gravity
and hold for 5 seconds
• Sit balanced without
the use of arms or
assistance
• Able to move from
sitting to stand
• Able to complete 3-5
steps of marching in place
• Able to take one step
forward and one step
backwards with no loss of
balance and no knee
buckling
• Able to tolerate
ambulating with no lo
ss of balance and no
knee buckling
(in-room distances)
• Able to walk in the
halls
Is patient progressing toward PLOF – defined 2 weeks prior to admission?
*Plan for mobility needs to be individualized for the patient and discussed daily during MDR. This protocol is not meant to substitute for good clinical judgment — If there is a reason the
patient should not be mobilized according to the ordered protocol, a discussion with the primary physician is warranted.
1 Complete Pre-Hospital Level of Function (PLOF) Assessment and Patient Pre-Mobility Screen*
2 Assess patient progression across mobility levels toward PLOF
PT Document in doc flowsheet highest mobility level achieved, at least twice daily 3
Address and reassess upon admission and at every shift if patient does not pass initial pre-mobility screen
If “NO” and a gap exists between PLOF and current function, consider a Physical Therapy Consultation
In the presence of a “NO” response, mobility can still be progressed unless deemed unsafe to proceed
If “YES,” proceed to next assessment level
Yes No Yes No Yes No Yes No Yes No
*No MD contraindications to begin mobility, patient is able to follow simple commands or cues, pain has been adequately addressed
Yes No If the patient does not meet criteria for progressive mobility
& a gap exists between current function & PLOF, consider
a Physical Therapy Consultation.

3/19/2018
6
PT/Nursing Partnership
• NURSING PARTNERS: Do the right thing for the patient • FUNDAMENTALS OF ASSESSMENT & TREATMENT
• It will be measured
• It will be credited
• Early PT engagement • FUNDAMENTALS
• PT provides Mobility Recommendations
• Clear Visibility across disciplines
• PT responsible for setting frequency/duration of rehabilitative care
PT LEADERSHIP IN EARLY MOBILITY
OPENED DOORS
• PT leadership in multidisciplinary mobility programs
• Improved transparency of documentation between disciplines
• Improved collaboration regarding hospital based falls
• Improved Workplace Safety
• Improvement in the continuum of care • Fall prevention classes • Outpatient PT follow-up • HHPT and SNF communication
Back to Grandpa Elliott…
• Is “walking a patient” skilled?
• Do we treat based upon diagnosis?
• Are our PTs bored?
• A Reminder • CLINICAL REASONING WITHIN ACUTE CARE
• Preaching to the choir…cream of the crop
Are we overpaid discharge dispositioners?
• Our jobs our on the line…
• Patients suffer in our absence…
• Clinical Reasoning is one of our differentiators
• We collect data, but do we ACT upon it? • Perform the FUNDAMENTALS of the PT evaluation
• The synthesis and application of facts into action
• COMMUNICATE these findings across disciplines
Academy of Acute Care Section: Core Competencies • “Acute care practice encompasses the knowledge and skills suitable
to thoroughly examine and appropriately intervene with patients in medically compromised situations encountered in any acute care hospital environment across the lifespan, from children to adults”.
• A great honor to have patients entrust their care to us in their most vulnerable state.

3/19/2018
7
IS THIS PATIENT APPRORIATE FOR PT INTERVENTION? • Bill Bouissonnault:
• TREAT • Do we assess mere function, or assist with the differential?
• Are we treating a diagnosis?
• Are we treating the right diagnosis?
• TREAT AND REFER • Do we assist with the why, not just the what?
• REFER • Sometimes most difficult to collaborate in the acute setting
• We all can too often assess/treat the “admitting diagnosis”
Continuum of Care
• Patient education regarding mobility and safety • Best motivators in acute care
• Family education
• Patient advocacy
• Interdisciplinary Communication • Years of RELATIONSHIP development
Clinical Reasoning in Acute Care: Case Discussions
• Highlighting: • Fundamentals of Clinical Practice
• Clinical Reasoning
• Differential Diagnosis
• Treatment
• Continuum of Care
58 y/o female s/p R THA • Algorithm or Assessment…
Chart Review
• Right Hemiplegia x 1 year
• Expressive aphasia
• Chronic low back pain
• Anemia
• Alcohol dependence • Drinks 1/5 vodka per day
• Moderate Tobacco User
• Colitis
• L ankle ORIF • Daily norco: (1-2 10 mg/day)
• Methadone: 3-4 tabs/4 times/day
PRE/POST OPERATIVE RADIOGRAPHS: (Anterior THA)

3/19/2018
8
HISTORY
• 1 year ago admitted for Left CVA • Right hemiparesis and expressive aphasia
• Discharged to SNF
• HHPT: ambulatory household distances supervised with quad cane
• Mod A for transfers & bed mobility
• Outpatient Chart Review
• 58 year old female referred to outpatient PT • R sided weakness/deconditioning
• R knee pain s/p fall • Non-ambulatory since the fall
Patient Profile
Past History: 7 months prior… • Son witnessed patient trip and fall
• Impact to her right knee
• Complaints of right knee pain and inability to ambulate
• Per ED physician:
• Mild swelling R knee
• Mild tenderness medial aspect of knee.
• No laxity on stress but tenderness with ROM and stress of MCL.
• Ordered right knee x-rays: (-), assessment: knee sprain • Patient not safe ambulating due to CVA
• Issued knee brace and wheelchair
• DC: Home
PRIMARY CARE VISITS: 4x in 4.5 months
• Knee sleeve, APAP and PT
• SUMMARY: • Worsening pain
• Difficult exam due to aphasia • Patient still non-ambulatory
• Physical Exam: • No joint tenderness, deformity or swelling
• No muscular tenderness
• Full ROM without pain, no crepitus
PT Visit #1: 7 months s/p fall
• Objective:
• Observation: WC dependent
• Dependent transfer to treatment table
• Unable to bear weight on R LE
• Knee AROM: 10-100—limited by pain
• Hip PROM: severely limited in all planes with guarding & pain • Internal rotation or flexion reproduced primary pain
• Tearful and high level of pain
• Assessment: advised MD regarding further work up of hip
• Plan: referred back to PCP for further workup
Acute Care: which mindset will we choose?
• “Simple” post-operative dx
• “Algorithm” of care
• “Boring protocol”
• Functional Assessment
• Discharge Disposition
• Holistic patient care
• Expressive aphasia
• Non-elective THA
• No assumptions
• ASK WHY?

3/19/2018
9
Ramifications of Standard Care
• Patient initially refused PT intervention
• Discharge destination and quality of life at risk • Patient was at “PLOF”
• Patient Care Coordinator: Board & Care discharge for custodial care
• Wheelchair bound 7 months for a reason!
PT IMPACT: Acute Care Rehabilitation
• Fear of all mobility
• High levels of pain
• Initially refused PT intervention
• Patient education regarding rehab potential
• Pain Science Education
• Family education
• Patient Advocacy regarding COC • Discussions with DC planners
• HBS
• SNF coordinator
Outcome
• Seen by Acute PT daily x 6 days • Reiteration of goals • Progressive rehab • HOPE!
• SNF x 7 days • Max A bed mobility • Mod A stand/pivot transfers • “Non Ambulatory at baseline”
• HHPT: 2 months x 15 visits • Renewed hope • Modified Independent Bed Mob/Transfers • Gait: 100 feet with SBA and Quad Cane
Importance of Your Role
• Worldwide, approximately 1.5 million people sustain Hip Fractures/year • Increase incidence to 2.6 million by 2025
• 4.5 million by 2050 • (Sterling R. S. (2011). Gender and race/ethnicity differences in hip fracture incidence, morbidity, mortality, and function. Clinical Orthopaedics and Related Research® , 469 (7), 1913 – 1918)
• One year mortality rate in patients >65: 8-36% • (Michaëlsson K. Nordström P. Nordström A. Garmo H. Byberg L. Pedersen N. L. Melhus H. (2014). Impact of hip fracture on mortality: A cohort study in hip fracture discordant identical twins. Journal of Bone an d Mineral
Research , 29 (2), 424 – 431)
SUMMARY: REMEMBER THE FUNDAMENTALS
• Chart Review: Why the non-elective THA?
• Why a hip fracture?
• History: PLOF—why did the patient decline?
• Detailed chart review
• Examine your patient
• Coordination of Care:
• Patient education/encouragement
• Patient advocacy
• Multidisciplinary engagement
DIZZINESS

3/19/2018
10
Dizziness in the Emergency Department • 15 million people develop dizziness every year
• ED visits for dizziness are on the rise:
• Annual ED visits from 1995 to 2011:
• All visits: increased by 44%
• Dizziness visits: increased by 97%
• From 2 million to 3.9 million • 3.5% of all ED visits
(Kattah ’09, Newman-Toker ’08 & ‘16, Cheung ’10, Saber Tehrani ‘13)
Dizziness in the Emergency Department
• Cost estimate for ED visits: ~$4 billion
• Total health care related costs: estimated > $10 billion
(Kattah ’09, Newman-Toker ’08 & ‘16, Cheung ’10, Saber Tehrani ‘13)
Dizziness in the Emergency Department
Compared to patients without dizziness in the ED, dizzy patients:
• Undergo more testing
• Undergo more imaging
• Have higher ED lengths of stay
• Are more likely to be admitted
(Newman-Toker ’08, Dallara ‘94, Kerber ‘10)
Acute Vestibular Syndrome (AVS) in the ED
• PERSISTENT DIZZINESS
• NAUSEA/VOMITING
• GAIT INSTABILITY
• NYSTAGMUS
• HEAD MOTION INTOLERANCE
Acute Vestibular Syndrome (AVS) in the ED MOST LIKELY DIFFERENTIAL:
• Vestibular Neuritis or Labyrinthitis • Very commonly misdiagnosed
• Stroke
• Posterior fossa (cerebellum or brainstem) • 96% of these strokes are ischemic
• When a stroke is the cause of dizziness, there is almost always other associated symptoms
• Other: Multiple Sclerosis, vertebral dissection, thiamine deficiency, autoimmune,
infections, metabolic conditions, etc.
(Hall ’16; Kerber ‘09, Tarnutzer ’11, Kerber ’12)
Dizziness in the Emergency Department:
• Posterior circulation strokes can mimic peripheral causes of dizziness
• In strokes with primary symptom of dizziness: • 3% are missed • 5% of those with an untreated TIA suffer a stroke within 48 hours
• Proper diagnosis is crucial • Prompt treatment lowers CVA risk after TIA by ~80%
• Neuroimaging is on the rise…
(Casani ’13)

3/19/2018
11
Neuroimaging • CT scans to rule out stroke:
• Increased from 10% in 1995 to ~40% in 2011
• Ineffective at ruling out stroke
• 16% sensitivity for all patients with dizziness • <1% sensitivity for dizziness in patients lacking clear neurological signs
• Cost of CT for dizziness in ED in 2013: $360 million
• Contributes to misdiagnosis and false sense of security
• Not without risk
Neuroimaging • MRI with Diffusion Weighted Imaging (DWI):
• Miss 10-20% of strokes presenting with AVS in the first 48 hours
• Take longer and cost 4x as much as CT scans
• Cost estimates in 2013: $110 million
• Used in 1-2% of dizzy patients
Neuroimaging • Increase in neuroimaging:
• Has led to an increase in length of stay • Has NOT led to a greater diagnostic yield of CNS diagnosis
• Suggestions:
• Stop unnecessary CT scans • Increase MRI in APPROPRIATE patients (6% of all dizzy visits)
• This would save ~half a billion dollars/year • Improve diagnostic accuracy in CNS patients • Reduce hospital admissions in benign peripheral inner ear disorders
• Focus on what is more accurate…history and physical examination
(Newman-Toker ’16)
CHALLENGE ACCEPTED?
• We should be called on each one of these dizzy patients
• Value? • Reliance on costly false negative imaging
• Merely performing gross functional assessment
Physical Therapy Role
• History and physical exam are more accurate than imaging
• Assist with determining peripheral vs central issue
• Assist with treatment and discharge plan
• Perform appropriate maneuver if BPPV
• Early mobilization
Physical Therapy Role
Fundamentals of Practice
• THOROUGH CHART REVIEW:
• Patient’s evolving condition over time
• Understand stroke risk factors
3/19/2018
12
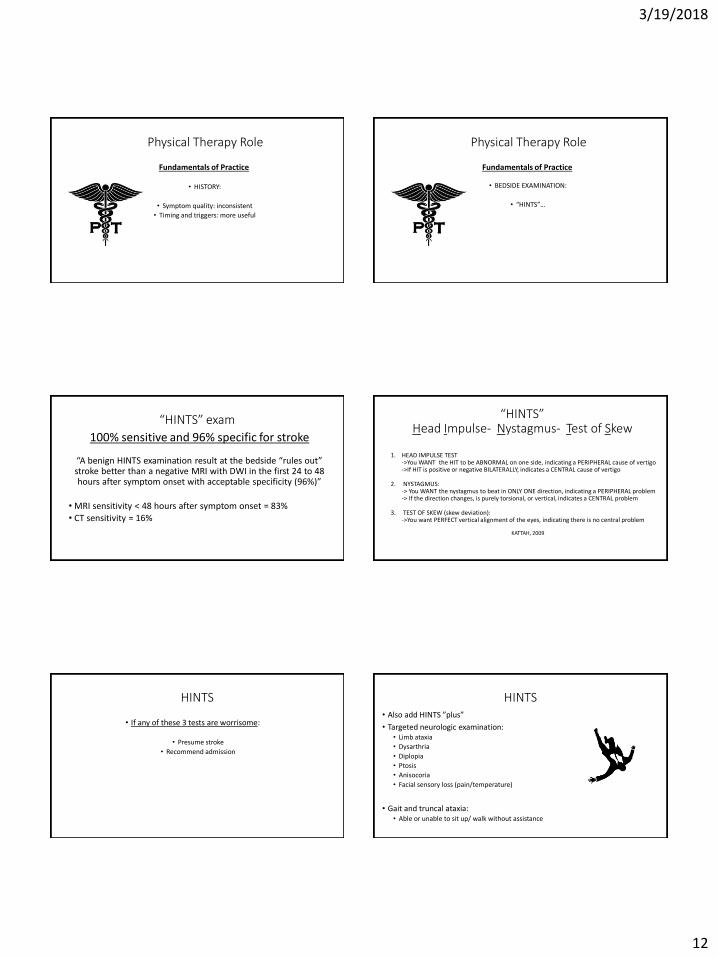
Physical Therapy Role
Fundamentals of Practice
• HISTORY:
• Symptom quality: inconsistent
• Timing and triggers: more useful
Physical Therapy Role
Fundamentals of Practice
• BEDSIDE EXAMINATION:
• “HINTS”…
“HINTS” exam
100% sensitive and 96% specific for stroke
“A benign HINTS examination result at the bedside “rules out” stroke better than a negative MRI with DWI in the first 24 to 48 hours after symptom onset with acceptable specificity (96%)”
• MRI sensitivity < 48 hours after symptom onset = 83% • CT sensitivity = 16%
“HINTS” Head Impulse- Nystagmus- Test of Skew
1. HEAD IMPULSE TEST ->You WANT the HIT to be ABNORMAL on one side, indicating a PERIPHERAL cause of vertigo ->If HIT is positive or negative BILATERALLY, indicates a CENTRAL cause of vertigo
2. NYSTAGMUS: -> You WANT the nystagmus to beat in ONLY ONE direction, indicating a PERIPHERAL problem -> If the direction changes, is purely torsional, or vertical, indicates a CENTRAL problem 3. TEST OF SKEW (skew deviation): ->You want PERFECT vertical alignment of the eyes, indicating there is no central problem
KATTAH, 2009
HINTS
• If any of these 3 tests are worrisome:
• Presume stroke
• Recommend admission
HINTS • Also add HINTS ”plus”
• Targeted neurologic examination: • Limb ataxia
• Dysarthria
• Diplopia
• Ptosis
• Anisocoria
• Facial sensory loss (pain/temperature)
• Gait and truncal ataxia: • Able or unable to sit up/ walk without assistance

3/19/2018
13
Case Example
• 67 year old female • NICU nurse Kaiser Oakland, lives alone, enjoys traveling, no regular exercise routine
• Past medical history: • HTN (currently untreated)
• Diverticulosis
• Hypothyroidism
• Adjustment disorder w/ depressed mood
• Vitamin D deficiency
• Medications: vitamin D3
Case Example
• 9 days after patient returned from vacation in Europe, she developed cough, congestion, bilateral ear fullness.
• Within 1 week of symptoms, developed dizziness, nausea/vomiting, headache, and imbalance. Called EMS, brought to ED by ambulance.
Case Example
• In ED, negative workup including: • CT of head and sinus
• Chest x-ray
• EKG
• NIHSS total: 0
• Given posterior CVA risk (age and untreated HTN), physician ordered: • Brain MRI w/ DWI
• Placed patient on observation
• PT evaluation
Bedside PT Examination
• CERVICAL AROM: wnl, guarded, increases subjective dizziness each direction
• MODIFIED VBI: (-)
• GAZE STABILITY ASSESSMENT • SPONTANEOUS NYSTAGMUS: right beating
• GAZE EVOKED NYSTAGMUS: direction fixed right beating nystagmus
• Saccades and Smooth Pursuit testing: intact
• HEAD IMPULSE TEST: (+) left
• SKEW DEVIATION: (-)
• Gait: moderate veering without walker
Evidence for Early Vestibular Rehabilitation in Neuritis
• Improved postural stability (Strupp ‘98)
• Less perception of disability and handicap (Banious ‘00)
• Dizziness and unsteadiness while walking are significantly decreased (Bjerlemo ‘06)
• Reduced duration of symptoms and need for medications (Venosa ‘07)
• Reduced perception of handicap, decreased symptom, and better performance (Teggi ’09)

3/19/2018
14
Case Example
• Patient education
• Gait training (80 ft w/ SBA and FWW)
• Recommendation: ambulate frequently throughout the day w/ FWW
• Discussed and demonstrated VOR stabilization exercise as soon as tolerable
• Recommendation: outpatient PT
• Physician and patient decline prednisone suggestion from PT
CASE EXAMPLE
• Patient with high anxiety
• Seen 3 days later in outpatient physical therapy
• Remains in acute stage as expected
CASE EXAMPLE
• Attempted to progress VOR and VSR
• Patient education: • decrease vigor of HEP
• reduce anxiety regarding condition
• Seen for 4 sessions: • Once/week for 2 weeks
• Once every 2 weeks for the next 2 weeks
• All symptoms resolved within 2 months
SUMMARY: OUR VALUE
• Dizziness is an extremely common symptom
• Causes are numerous
• Diagnosis is difficult
• Resource overutilization and misdiagnoses are common
• History and physical exam are more accurate than imaging
OUR ROLE:
Identify benign inner ear conditions:
• Discharge planning for home
• Early mobilization and treatment
• Fast-track to outpatient
• Reduce healthcare costs
Identify serious signs and symptoms:
• Save lives
• Reduce healthcare costs
References
Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418–1428.
Hines AL, Barrett ML, Jiang HJ, Steiner CA. Conditions with the Largest Number of Adult Hospital Readmissions by Payer, 2011. HCUP Statistical Brief #172. Rockville: Healthcare Research and Quality; 2014
Smith BA, Fields CJ, Fernandez N. Physical therapists make accurate and appropriate discharge recommendations for patients who are acutely ill. Phys Ther. 2010;90:693–703.
Falvey JR, Magione KK, Stevens-Lapsley. Rethinking Hospital-Associated Deconditioning: Proposed Paradigm Shift. Phys Ther. 2015;95(9):1307-1315.
Shih SL, Gerrard P, Goldstein R, et al. Functional status outperforms comorbidities in predicting acute care readmissions in medically complex patients. J Gen Intern Med. 2015;30:1688–1695.
Shih GL, Gerrard P, Goldstein R, et al. Functional Status Outperforms Comorbidities as a Predictor of 30-Day Acute Care Readmissions in the Inpatient Rehabilitation Population. 2016;10(17):921-926.
Falvey JR, Burke RE, Malone D et al. Role of Physical Therapists in Reducing Hospital Readmissions: Optimizing Outcomes for Older Adults During Care Transitions From Hospital to Community. Phys Ther. 2016;96(8):1125-1134.
Greyson SR, Cenzer IS, Auerbach AD, Covinsky KE. Functional Impairment and Hospital Readmission in Medicare Seniors. JAMAInternMed.2015;175(4):559-565
Barnes DE, Mehta KM, Boscardin WJ, Fortinsky RH, Palmer RM, Kirby KA, Landefeld, CS. Prediction of Recovery, Dependence or Death in Elders Who Become Disabled During Hospitalization. J Gen Intern Med 28(2):261–8.

3/19/2018
15
References • Casani, et al: Cerebellar infarctions mimicking acute peripheral vertigo: how to avoid misdiagnosis? Otolaryngol Head Neck Surg; 2013; 32:
pp. 1518-1521.
• Cheung CS: Predictors of important neurological causes of dizziness among patients presenting to the emergency department. Emerg Med J 2010; 27: pp. 517-521.
• Dallara J, Lee C, McIntosh L, Sloane PD, Morris D. ED length-of-stay and illness severity in dizzy and chest-pain patients. Am J Emerg Med. 1994; 12:421–4.Edlow JA, Newman-Toker DE, Savitz SI. Diagnosis and initial management of cerebellar infarction. Lancet Neurol. 2008; 7:951–64.
• Edlow, J, Newman-Toker: A new diagnostic approach to the adult patient with acute dizziness. Journal of Emerg Med; 2017: pp 1-35.
• Hall CD, Herdman SJ, Whitney SL, et al. Vestibular Rehabilitation for Peripheral Vestibular Hypofunction: An Evidence-Based Clinical Practice Guideline: Journal of Neurologic Physical Therapy. 2016;40(2):124-155.
• Kattah JC, Talkad AV, Wang DZ, Hsieh YH, Newman-Toker DE. HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke. 2009; 40:3504–10.Kerber KA, Meurer WJ, West BT, Fendrick AM. Dizziness presentations in U.S. emergency departments, 1995-2004. Acad Emerg Med. 2008; 15:744–50.Kerber, 09
• Kerber KA, Schweigler L, West BT, Fendrick AM, Morgenstern LB. Value of computed tomography scans in ED dizziness visits: analysis from a nationally-representative sample. Am J Emerg Med. 2010; 28:1030–6.Kerber ’12
• Newman-Toker DE. Charted records of dizzy patients suggest emergency physicians emphasize symptom quality in diagnostic assessment. Ann Emerg Med. 2007; 50:204–5.
• Newman-Toker DE, Kattah JC, Alvernia JE, Wang DZ. Normal head impulse test differentiates acute cerebellar strokes from vestibular neuritis. Neurology. 2008; 70:2378–85.Newman-Toker ‘13
• Newman-Toker: Missed stroke in acute vertigo a time for action, not debate. Ann Neurol 2016; 79: pp. 27-31.
• Saber Tehrani: Rising annual costs of dizziness presentations to U.S. emergency departments. Acad Emerg Med 2013. 20: pp. 689-696.
• Tarnutzer AT, Berkowitz AL, Robinson KA, Hsieh YH, Newman-Toker DE. Acute vestibular syndrome: does my patient have a stroke? A systematic and critical review of bedside diagnostic predictors. CMAJ. 2011; in press.
Medical Screening and Referral In Older
Adults
Michael D. Ross, PT, DHSc, OCS
Daemen College
Amherst, NY
Thank you!
• Academy of Acute Care Physical Therapy
• To all of you for attending!
• Michael Bang, PT
For your patients……
Do you Treat, Treat and Refer, or
Refer Only?
Differential diagnosis
….is the comparison of symptoms of similar diseases and medical diagnostics
(laboratory and test procedures performed) so that a correct assessment of
the patient/client’s actual problem can be made
Hypothetico-deductive reasoning model to facilitate diagnosis
Goodman and Snyder, 2013
Fundamental Principles of Evidence-Based
Practice
Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS. BMJ. 1996;312: 71-72.

3/19/2018
16
Patient’s Values and Expectations
respect for the patient’s values, preferences, and expressed needs
coordinated and integrated care
clear, high-quality information and education for the patient/family
physical comfort, including pain management
emotional support and alleviation of fear and anxiety
involvement of family members and friends, as appropriate
continuity, including through care-site transitions
access to care
N Engl J Med 366;9, March 1, 2012
Michael J. Barry, and Susan Edgman-Levitan
Manary et al, N Engl J Med Dec 26, 2012
Core Competencies
The Lancet 2016 388, 1545-1602DOI: (10.1016/S0140-6736(16)31678-6)
Copyright © 2016 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY license Terms and Conditions
Leading ten causes of global age-specific
years lived with disability in 2015
The Lancet 2016 388, 1545-1602DOI: (10.1016/S0140-6736(16)31678-6)
Copyright © 2016 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY license Terms and Conditions

3/19/2018
17
Case Discussion
53 year-old woman
2 wks s/p lumbar spinal fusion revision
surgery
– 6 surgeries over 3 years
CC: LBP, B shoulder (L>R), L upper
extremity, and upper back/neck pain
– B LE pain as well
PMHx: CAD, depression and suicidal
ideations
– 18 pack-year smoking history
Meds: Neurontin, Percocet, Soma, and
Xanax
Physical Exam
Pulse: 82 beats per minute
Blood pressure: 160/100 mmHg
Respiration rate: 22 breaths per minute
Moderate assist to transfer from a supine to
sitting position and from a seated to standing
position
Moderate assistance to ambulate 9-m with a
walker
SOB, lightheadedness, and fatigue with
activity
Physical Exam
Moderate assist to transfer from a supine to
sitting position and from a seated to standing
position
Moderate assistance to ambulate 9-m with a
walker
SOB, lightheadedness, and fatigue with
activity
NEXT STEP?
Treatment
Due to concern over a progressively worsening cardiac
condition, the PT immediately consulted the cardiologist, who
agreed to see the patient the next day

3/19/2018
18
Outcome
Cardiac catheterization revealed 75% blockage of her left
anterior descending coronary artery, 50% blockage of her left
circumflex artery and 99% blockage of her right coronary
artery
Outcome
Cardiac catheterization revealed 75% blockage of her left
anterior descending coronary artery, 50% blockage of her left
circumflex artery and 99% blockage of her right coronary
artery
Outcome
The patient was subsequently treated with coronary artery
bypass grafting (CABG)
Ten days following her CABG, cardiac rehabilitation was
started in her home with the same PT
Outcome
CC: post-surgical chest pain and low back soreness, which
was now greatly improved
Independent with transfers and ADLs
Ambulated 300-m with a SPC without LE pain
No longer complained of SOB or lightheadedness
Outcome
No longer taking her Percocet, Soma, or Xanax
Started on Lipitor and continued with the use of Neurontin
She was treated by the home health physical therapist for 8
weeks and then discharged to an advanced cardiac
rehabilitation program at a community hospital
Concerns
Multiple lumbar surgeries
History of cardiac disease
– Elev BP, SOB, dizziness, lightheadedness
– Meds (beta blocker, diuretic)
Pain pattern presentation (?)
Prevention (?)
3/19/2018
19
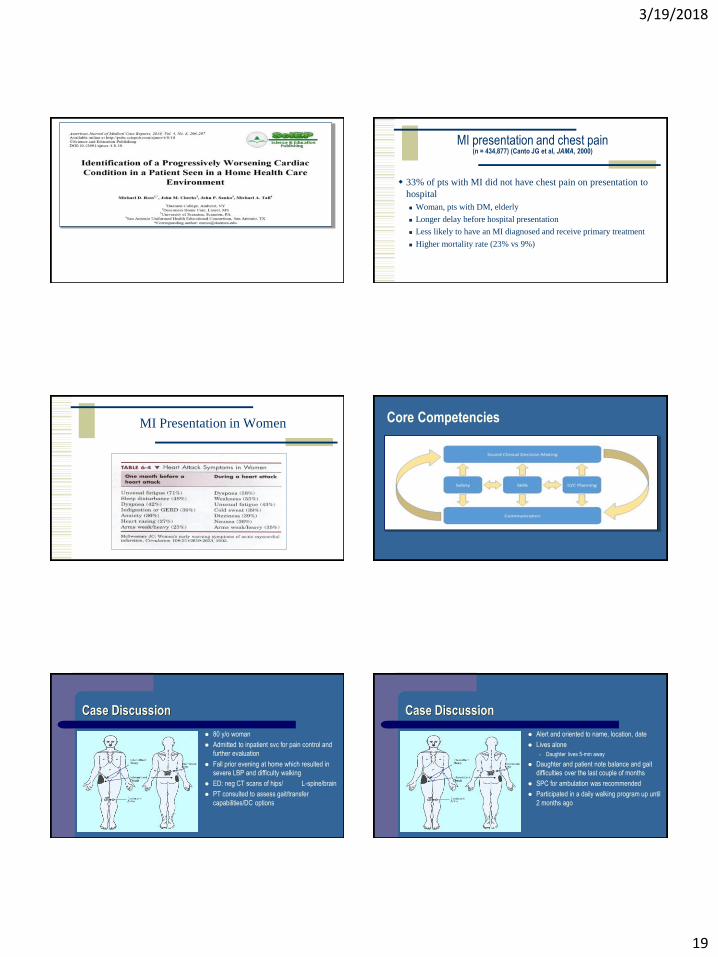
MI presentation and chest pain (n = 434,877) (Canto JG et al, JAMA, 2000)
33% of pts with MI did not have chest pain on presentation to
hospital
Woman, pts with DM, elderly
Longer delay before hospital presentation
Less likely to have an MI diagnosed and receive primary treatment
Higher mortality rate (23% vs 9%)
MI Presentation in Women Core Competencies
Case Discussion
80 y/o woman
Admitted to inpatient svc for pain control and
further evaluation
Fall prior evening at home which resulted in
severe LBP and difficulty walking
ED: neg CT scans of hips/ L-spine/brain
PT consulted to assess gait/transfer
capabilities/DC options
Case Discussion
Alert and oriented to name, location, date
Lives alone
– Daughter lives 5-min away
Daughter and patient note balance and gait
difficulties over the last couple of months
SPC for ambulation was recommended
Participated in a daily walking program up until
2 months ago

3/19/2018
20
Case Discussion
Meds: Norvasc, Diovan, Actonel, Pravachol
Goal is to get back home
Tests & Measures
Pulse: 76 beats per minute
Blood pressure: 135/88 mmHg
Respiration rate: 17 breaths per minute
Fair upper and lower extremity strength – Weakness more pronounced weakness in the UEs and on the R
Poor to fair bed mobility and transfer capabilities – Able to transfer from bed to chair with a use of a walker
– Mod assist due to pain/weakness
Tests & Measures
Fair upper and lower extremity strength – Weakness more pronounced weakness in the UEs and on the R
Fair bed mobility and transfer capabilities – Able to transfer from bed to chair with a use of a walker
– Mod assist due to pain/weakness
What’s the next step?
Tests & Measures
General hyperreflexia was noted – hyperactive deep tendon reflexes
– Hoffman reflex and Babinski sign are present
Patient also reported bilateral hand numbness and tingling/decreased fine motor skills prior to admission
Positive Hoffman’s Reflex Babinski Sign

3/19/2018
21
Hoffman and Babinski sign: clinical significance
A Hoffman and Babinski sign generally indicates cord involvement in the
cervical spine or intracranial pathology
Advanced diagnostic imaging is indicated—especially prior to mechanical
intervention
(Cook et al, 2007)
Patient Disposition
Examination findings were discussed with the patient’s physician
Magnetic resonance imaging of the brain and cervical spine were ordered to assess for a cerebrovascular accident and cervical myelopathy
T2 Weighted MRI – Sagittal View
C3 C3
T2 sagittal MR image reveals marked narrowing of the spinal canal at C3/C4 to C4/5 (arrows) secondary to posterior disc protrusions, degenerative osteophyte formation, and buckling of ligamentum flavuum. A small area of myelomalacia is also present within cord is present at the C5 level.
C3
Patient Disposition
The patient was subsequently referred to neurosurgery for evaluation
It was determined that the patient was a surgical candidate
The patient subsequently underwent surgical decompression laminoplasty from C3 to C6

3/19/2018
22
Outcome
At two months following surgery, the patient ambulated with an age-appropriate gait pattern with a SPC
Demonstrated a 5/5 lower extremity and 4+/5 upper extremity strength with manual muscle testing
At one year following surgery, the patient was living independently and had returned to her daily walking program
Description of Compressive Cervical Myelopathy
Spinal cord compression caused by narrowing of the cervical spinal canal
Cord Compression Signs
– Paresthesia
– Weakness
– Ataxia
– Babinski
– Clonus
– Hoffman’s
– Romberg
Description of CSM
In cases of progressive CSM, improved outcomes are reported if surgical
treatment is initiated earlier in the course of the disorder
– Therefore, early diagnosis is critical for optimal condition management and patient
outcomes
Because the early signs of CSM are often subtle and overshadowed by other
medical conditions, the diagnosis can be missed
Central Neurologic Exam
Examining for upper motor neuron or long tract signs – Subjective Exam
N/T
Balance
– Neuro Exam
Strength, sensation, DTRs
– Pathologic Reflexes
Hoffman’s Test
Babinski’s test
Clonus
Balance assessment: Gait, Tandem walking, Romberg
Chronic Anterior Cervical Cord Compression (Bohlman et al, 1979; Ono et al, 1977)
Histological alterations in the cord
– demyelination of the lateral columns
– ascending necrosis and degeneration of the dorsal columns

3/19/2018
23
Cervical Cord - Functional Review
Dorsal Columns
Corticospinal Tract
Spinothalamic Tract
Take home messages
Differential diagnosis in patients with a history of falls
– Early recognition of signs and symptoms of progressive CSM
– Appropriate referrals for diagnostic imaging and surgical evaluation when indicated
Physical therapists have a unique skill set in the acute care setting:
– maximize outcomes, with a particular emphasis on determining the appropriate
frequency and intensity of therapeutic interventions, optimizing physical function, and
reducing readmission rates
Thank you!