
Clinical protocol and the role of teh eye care practitioner
10
2 2 / 0 5 / 0 9 C E T 32 Spons ored by: Ap pr ov ed for Optometris ts Approv ed for DOs CONTINUING EDUCATION & TRAINING C ET THIS ISSUE CET: PA Y AS YOU LEARN ✔ To gain more standard CET points for this year’s PAYL series, purchase your credits at www.otbookshop.co.uk and then enter online at: www.otcet.co.uk to take your exams ✔ ✔ The busy eye care practitioner often finds that decisions on patient management must be made qu ickly and effectively. This can be especially challenging when patients present with less commonly encountered visual difficulties. This article uses the information described previously in this series to produce a clinical protocol that can allow th e practitioner to determine the best course of action for their patients with reading difficulties. The protocol is summ arised in Figure 1. 1 Eye care practitioners, particularly community optometrists, will have a typical ‘routine sight test/eye examination procedure’ that they use for patients. It is clear from this series of articles that they will need to use a more extensive protocol for people with Specific Learning Difficulties (SpLD), and those who might benefit from precision tinted lenses. This is sometimes called a ‘special investigation’ and it starts with a detailed investigation of the presenting symptoms, as outlined in Part 1 of this series of articles. (SUSPECTED) LEARNING DIFFICULTIES IS THERE A SIGNIFICANT REFRACTIVE ERROR? IS THERE A SIGNIFICANT ORTHOPTIC ANOMALY? TEST WITH INTUITIVE OVERLAYS IS THERE A SIGNIFICANT BENEFIT? INTUITIVE COLORIMETRY PREC ISION TINTS referral to optometrist yes no no positive yes positive no negative yes yes optometric correction correction/ treatment monitor monitor monitor MONITOR ANNUALLY < Figure 1 A clinical protocol for the management of patients with reading difficulties ARE EYES HEALTHY? no negative refer The eye examination The present series of articles has discussed several visual problems that can be associated with reading difficulties. The various cond itions can cause symptoms that are similar to one another, so the eye care practitioner is faced with a challenge of differential diagnosis. It is recommended that before visual stress is diagnosed, other optometric factors should be excluded with an extensive eye examination. The eye examination would typically include the components listed in Table 1 . Most of the tests in Table 1 will be familiar to optometrists, but a few of the less common ones will be described later. Diagnostic criteria and th e decision as to when to treat are discussed in parts 2-4 of this series of articles. What refractive correction should be worn during ocular motor tests During binocular vision and accommodative (ocular motor) tests a question th at sometimes arises is " wh at refractive correction, if any, shou ld th e V I S I O N & R E A DI NG DI F F I C U L TI E S P A R T 5 C O U R S E C O DE : C - 11112 Clinical protocol and the role of the eye care practitioner Dr Peter Allen, Prof Bruce Evans, Prof Arnold Wilkins This series of articles has described various aspects of visual characteristics of reading d iff iculties and the backgroun d behind techniques such as the use of coloured filters in h elping to reduce the d ifficulties that are experienced. The p resent article, which is the last of this series, aims to describe a clinical protocol that can be used by the busy eye care practitioner for the investigation and management of such patients. It also describes the testing techniques th at can be u sed for the various assessments. Warning: DO NOT LOOK AT FIGURE 7 IF YOU HAVE MIGRAINE OR EPILEPSY. CONFUSED ABOUT CET REQUIREMENTS? www.cetoptics.com/cetusers/faqs/ IMPORTANT I NFOR MATION Under the new Vantage rules, all OT CET points awarded will be uploaded to its website by us. All participants must confirm these results on www.cetoptics.com so that they can move their points from the “Pending Points record” into their “Final CET points record”. Full instructions on how to do this are available on their website.
Transcript of Clinical protocol and the role of teh eye care practitioner

8/7/2019 Clinical protocol and the role of teh eye care practitioner
http://slidepdf.com/reader/full/clinical-protocol-and-the-role-of-teh-eye-care-practitioner 1/10
2 2 / 0 5 / 0 9 C E T
2
Sponsored by:
Approved for Optometrists Approved for DOs
CONTINUINGEDUCATION &TRAININGCET
THIS ISSUE CET: PAY AS YOU LEARN✔
To gain more standard CET points for this year’s PAYL series, purchase your credits atwww.otbookshop.co.uk and then enter online at: www.otcet.co.uk to take your exams
✔
✔
The busy eye care practitioner oftenfinds that decisions on pat ientmanagement must be made qu ickly andeffectively. This can be especially
challenging when patients present withless commonly encountered visualdiff icul t ies . This ar t icle uses theinformation described previously inthis ser ies to produce a cl inicalprotocol that can allow th e practitionerto determine the best course of actionfor their pat ients with readingdifficulties. The protocol issumm arised in Figure 1. 1
Eye care practitioners, particularlycommunity optometrists, will have atypical ‘rout ine s ight test /eye
examination procedure’ that they usefor patients. It is clear from this seriesof articles that they will need to use amore extensive protocol for peoplewith Specific Learning Difficulties(SpLD), and those who might benefitfrom precision tinted lenses. This issometimes cal led a ‘specialinvest igat ion’ and i t s tar ts with adetailed investigation of the presentingsymptoms, as outlined in Part 1 of thisseries of articles.
(SUSPECTED) LEARNING DIFFICULTIES
IS THERE A SIGNIFICANT REFRACTIVE ERROR?
IS THERE A SIGNIFICANT ORTHOPTIC ANOMALY?
TEST WITH INTUITIVE OVERLAYS
IS THERE A SIGNIFICANT BENEFIT?
INTUITIVE COLORIMETRY
PRECISION TINTS
referral to optometrist
yes
no
no
positive
yes
positive
no
negative
yes
yes
optometric correction
correction/ treatment
monitor
monitor
monitor
MONITOR ANNUALLY
< Figure 1A clinical protocol for the management ofpatients with reading difficulties
ARE EYES HEALTHY?no
negative
refer
The eye examinationThe present ser ies of ar t icles hasdiscussed several visual problems thatcan be associated with reading
difficulties. The various cond itions cancause symptoms that are similar to oneanother, so the eye care practitioner isfaced with a challenge of differentialdiagnosis . I t is recommended thatbefore visual stress is diagnosed, otheroptometric factors should be excludedwith an extensive eye examination.The eye examination would typicallyinc lude the components l i s t ed inTable 1 .
Most of the tests in Table 1 will befamiliar to optometrists, but a few of
the less common ones wil l bedescribed later. Diagnostic criteriaand th e decision as to when to treat arediscussed in parts 2-4 of this series of articles.
What refractive correction should beworn during ocular motor testsDuring binocular vis ion andaccommodative (ocular motor) tests aquestion th at sometimes arises is "wh atrefractive correction, if any, shou ld th e
VISION & READING DIFFICULTIES PART 5 COURSE CODE: C-11112
Clinical protocol and the role ofthe eye care practitioner
Dr Peter Allen, Prof Bruce Evans, Prof Arnold Wilkins
This series of articles has described various aspects of visualcharacteristics of reading d ifficulties and the backgroun d behind
techniques such as the use of coloured filters in h elping to reducethe d ifficulties that are experienced. The p resent article, which isthe last of this series, aims to describe a clinical protocol that canbe used by the busy eye care practitioner for the investigation andmanagement of such patients. It also describes the testingtechniques th at can be u sed for the various assessments.
Warning: DO NOT LOOK AT FIGURE 7 IF YOU HAVE MIGRAINE OR EPILEPSY.
CONFUSED ABOUT CET REQUIREMENTS?www.cetoptics.com/cetusers/faqs/IMPORTANT INFORMATION
Under the new Vantage rules, allOT CET points awarded will be uploaded to its website by us. All participants must confirm these results onwww.cetoptics.comso that they can move their points from the “Pending Points record” into their “Final CET points record”. Full instructions on how to do this are available on their website.

8/7/2019 Clinical protocol and the role of teh eye care practitioner
http://slidepdf.com/reader/full/clinical-protocol-and-the-role-of-teh-eye-care-practitioner 2/10
2 2 / 0 5 / 0 9
C E T
33
Sponsored by:
Approved for Optometrists Approved for DOs
CONTINUINGEDUCATION &TRAININGCET
THIS ISSUE CET: PAY AS YOU LEARN✔
To gain more standard CET points for this year’s PAYL series, purchase your credits atwww.otbookshop.co.uk and then enter online at: www.otcet.co.uk to take your exams
✔
✔
General Description Details
Refractive error and visual acuity Presenting vision at distance and near; Retinoscopy; Subjective refraction;Corrected visual acuity
Health assessment Pupil reactions; Ophthalmoscopy; Visual fields (if old enough);Colour vision (Ishihara Plates)
Ocular motor assessment Cover-uncover test at distance and near; Dissociation test at distance andnear (e.g., alternating cover test, Maddox rod, Maddox wing); Aligningprism at distance and near (Mallett fixation disparity test); Ocular motility;Near point of convergence; Stereoacuity; Amplitude of accommodation;Accommodative lag (MEM retinoscopy); Facility of accommodation;Fusional reserves at near (possibly distance); AC/A ratio
Coloured filter screening Intuitive overlays; Rate of reading test; Pattern glare test
Coloured filter prescribing Intuitive colorimeter; Precision tinted lenses
instability and can cause symptomsincluding diplopia, blur, visualperceptual distortions and headaches.The best cl inical method forinvestigating binocular stability is touse the “OXO” test on the near Mallett
unit (Figure 2). During this test, theeyes are fused in a manner similar tothat when the patient is reading. Inaddit ion to the normal quest ionsregarding the alignment of the Nonius(green) lines whilst the patient fixatesthe X, a supplemen tary question of “doone or both lines ever move?” shouldbe asked. 2 Any movement of theNonius marker(s) should then beel iminated with ei ther prisms orspheres (base-in or negative sphere foran exo-slip), starting with 0.5 Δ an d
progressing in 0.5 Δ steps unti l themovement disappears. 3
Fusional reserves should be assessedat near using a prism bar or phoropter.Results can differ according to theprocedure used, so it is important tonote which method was used whenrecording the results. A prism bar isprobably the best method because thepatien t’s eyes can be w atched . Base-outpr i sm i s used to measure theconvergent fusional reserve and base-inprism is used to measure the divergent
fusional reserve. The fusional reservethat opposes the heterophoria shouldbe measu red first (ie convergent reservefor exophoria). The blur, break andrecovery points for both are required.
The p atient is asked to fixate a detailed
target whilst the optometrist increasesthe prism before one eye. The prismpower is gradually increased un til thetarget first becomes blurred (blurpoint), then first becomes double ormoves to the side (break point), andthen, as the prism power is reduced,when the target becomes single again(recovery point); the prism value ateach of these points should berecorded.
If the ampli tude of the fusionalreserve (from divergent to convergent
break points) is less than 20 Δ then thepatien t may have binocular instability. 3
If the fusional reserve is less than twicethe heterophoria it opposes, then thepa t ien t may have decompensa tedheterophoria (Sheard’s criterion).Binocular instability can be treatedwith fusional reserve exercises, or withspheres or prisms if associated withdecompensated heterophoria .Decompensated heterophoria can betreated or corrected with eye exercises,prisms, or spheres.
Accommodative lagMeasurement of the ampli tude of accommodation is perhaps the mostroutine assessment of accommodativefunction. An addit ional test of accommodative function, monocularestimation m ethod (MEM) retinoscop y,is part icular ly useful in pre-presbyopes with SpLD because i tprovides an objective assessment of accommodative accuracy ( ie thepresence of any lag or lead of
accommodation). The pat ientbinocu larly fixates a detailed target onthe retinoscope and is asked to keepthis in clear focus. Retinoscopy iscarr ied out along the horizontalmeridian and lenses are very brieflyheld in front of each eye to neutralisethe ret inoscope ref lex. Each lensshould on ly be presented mon ocularlyand for a split second so as not todisrupt the s tatus of the pat ient 'saccommodative and binocularresponse. The accommodative lag is
usually about +0.50D (although this isdependant on refract ive errorstability); 4 values of greater than+1.00D lag may representaccommodative insuff iciency. 3 If a
patient wear?” Most commonly, thepurpose of these tests is to determinethe significance of any visual p roblemsthat the patient may have with nearwork. So, if glasses are worn for nearwork at the ap propriate distance more
than 50% of the time, then the p atientshould wear their glasses du ring ocularmotor tests at the same distance. Anexception is ocular moti l i ty, whenspectacles are not usually worn unlessthere is a very high refractive error, inwhich case the test should be donewith an d w ithout glasses.
It is also useful to repeat somebinocular vis ion tests when apract i t ioner proposes to make asignificant change to the refractivecorrection (eg prescribing glasses for
the first time), to check that the newrefractive correction is not going toworsen the situation. This can also besensible if there is a significant ch ancethat the pat ient may ‘change’ therefract ive correct ion, by stoppingwearin g their glasses. For example, if ahypermetropic chi ld rapidly breaksdown to an esotropia without theirglasses, then p arents should be w arnedto have a spare p air of spectacles and toavoid periods where the child wouldbe without them.
Binocular stability assessment andfusional reservesBinocular instability is characterisedby low fusional reserves and vergence
< Table 1Components of the eye examination for people with specific learning difficulties (SpLD). Not alltests may be appropriate in every case

8/7/2019 Clinical protocol and the role of teh eye care practitioner
http://slidepdf.com/reader/full/clinical-protocol-and-the-role-of-teh-eye-care-practitioner 3/10
2 2 / 0 5 / 0 9 C E T
4
Sponsored by:
Approved for Optometrists Approved for DOs
CONTINUINGEDUCATION &TRAININGCET
THIS ISSUE CET: PAY AS YOU LEARN✔
To gain more standard CET points for this year’s PAYL series, purchase your credits atwww.otbookshop.co.uk and then enter online at: www.otcet.co.uk to take your exams
✔
✔
one minute. This number divided by
two gives the accommodative facilityrate in cycles per minute.
A suppression check should beincluded for any binocularmeasurements. The “OXO” letters andNonius lines on a n ear Mallett unit canbe used in con junc t ion wi th thepolarising filters for binocularaccommodative facility testing. Thevertical OXO target is recommendedbecause the patient is less likely to bedistracted by m ovement of the Noniusmarkers than if the h orizontal OXO test
is used.Normative values for children and
youn g adults are sometimes given as 11cycles per minute (cpm) for monocularfacility and 8 cp m for binocu lar facility.But these figures are the mean valuereported in a normative s tudy byZellers and colleagues 6 as opposed tothe 95% confidence interval, which isthe mean ±2 standard deviations (SDs).Data from Zellers et al. 6 indicated avery wide SD range, which may bebecause the test is confound ed by man y
variables other than accommodativefacility, such as verbal response,attention, and interpretation of blur. Arecent s tudy of s tudent volunteershowever, demonstrated that objectivemeasures of accommodative functionwere highly correlated with thesubject ive responses of personsundergoing the accommodative facilitytest. 7 Patients with low accommodativefacility rates may benefit from anaccommodative facility training regimein order to improve their dynamic
accommodation function. 8
Coloured filtersIf symp toms or read ing difficulties stillpersis t af ter the detect ion andtreatment of any refract ive and/orocular motor problems, thenoptometris ts should invest igate theeffect of coloured filters. It is best,when ever possible, to test the patientsin lighting conditions similar to thoseused when patients experience theirsymptoms. Note that l ight ing
conditions in school are far brighterthan the recommend ed level of 300-500lux (often in excess of 1,000 lux). Thelighting is usu ally fluorescent an d 80%of schools continue to be lit with low
frequency fluorescent lighting that emits
100Hz flicker.9
Testing usually starts by screeningwith coloured overlays. Sometimes, ateacher wil l have carr ied this outalready, but commonly the eye carepractitioner will be the first person tocarry this out. Th e Intuitive Overlays area range of coloured overlays that havebeen designed to sample colourssystematically, 10 are of an adequate sizeto be effective, 11 and have a sufficientrange of colours. 12 The Intuitive Overlayconsists of twenty A5 sized overlays
(two sets of ten different colouredoverlays). One su rface of the overlay h asa matt finish whereas the other side isgloss. A Test Page incorporating twopassages of text (visible in Figure 4)should be used.
Procedure for Intuitive OverlayassessmentThe procedure for Intuitive Overlayassessment is given in Table 2.
It is always worth confirming theconsistency of choice of the overlay or
overlay combinat ion. If the pat ientconsistently ch ooses a particular overlayor combination of overlays then it ispossible to measure the effects of theoverlays on reading speed (see later) –this can be a helpful indicator of wh ether or not the overlay is likely to beused.
A computerised version of theIntuitive Overlay test is also available,and this includes the Wilkins Rate of Reading Test (see later) and a meth od of individually printing coloured overlays.
< Figure 3Accommodative facility testing using binocularflippers
negative lens is required to neutralisethe reflex this suggests that the patientmay be over-accommod ating (lead).
The test may give useful additionalinformation if the ampli tude of accommodation is low, and in thosepat ients that are uncooperat ive. Asl ight ly different approach to thistechnique (Nott retinoscopy) involves
the fixation target being held in aconstant position and the retinoscopebeing moved to and fro to obtainreversal. Typically, this reveals aslightly lower degree of accommodative lag. 5
Accommodative facilityThe ability to alter accommodationrapidly and accurately is cal ledaccommodative faci l i ty and can beassessed using the ±2.00DSaccommodative flipper test (Figure 3).
The f l ipper consists of a pair of +2.00DS lenses moun ted on one side of a flipper bar and a pair of -2.00DSlenses mounted on the opposite side.The patient fixates a near target (at40cm) while the optometrist alters theaccommodative stimulus by placingeither the plus lens pair (stimulus of 0.50D) or the negative lens pair(stimulus of 4.50D) in front of thepatient’s eyes. The test should alwaysbegin with the +2.00DS lenses over thepatient’s up-to-date refractive
correction. The patient reports whenthe n ear target is seen clearly after eachalteration in accommodative stimulus,whils t the optometr is t counts thenumber of times clarity is obtained in
< Figure 2
Mallett near vision fixation disparity test,which is used to determine the aligning prism(associated heterophoria) or aligning sphere

8/7/2019 Clinical protocol and the role of teh eye care practitioner
http://slidepdf.com/reader/full/clinical-protocol-and-the-role-of-teh-eye-care-practitioner 4/10
2 2 / 0 5 / 0 9 C E T
35
Whether this provides a colour suitablefor overlays, how ever, has n ot yet beenevaluated.
Intuitive Overlays are a rapid andeasy method of screening for thebenefi t of colour on readingperformance, but they have somedrawbacks. Only a limited range of colours can be tested and prescribed,
and the overlays can only be used forreadin g and are not suitable for writing,white boards, or computer use. If aperson ben efits from a coloured overlaythen they are likely to be helped moreby precision tinted lenses since thesecan be prescribed individually, withgreater precision; they can also helpwith wri t ing, computer use, andwhiteboards as well as reading. Asdescribed in part 3 of this series of articles, precision tinted lenses aretypically prescribed on the basis of
testing with the Intuitive Colorimeter. 13
Children are generally only testedwith the Intuitive Colorimeter if theyhave show n a significant benefit from acoloured overlay. There are two ways
Sponsored by:
Approved for Optometrists Approved for DOs
CONTINUINGEDUCATION &TRAININGCET
THIS ISSUE CET: PAY AS YOU LEARN✔
To gain more standard CET points for this year’s PAYL series, purchase your credits atwww.otbookshop.co.uk and then enter online at: www.otcet.co.uk to take your exams
✔
✔
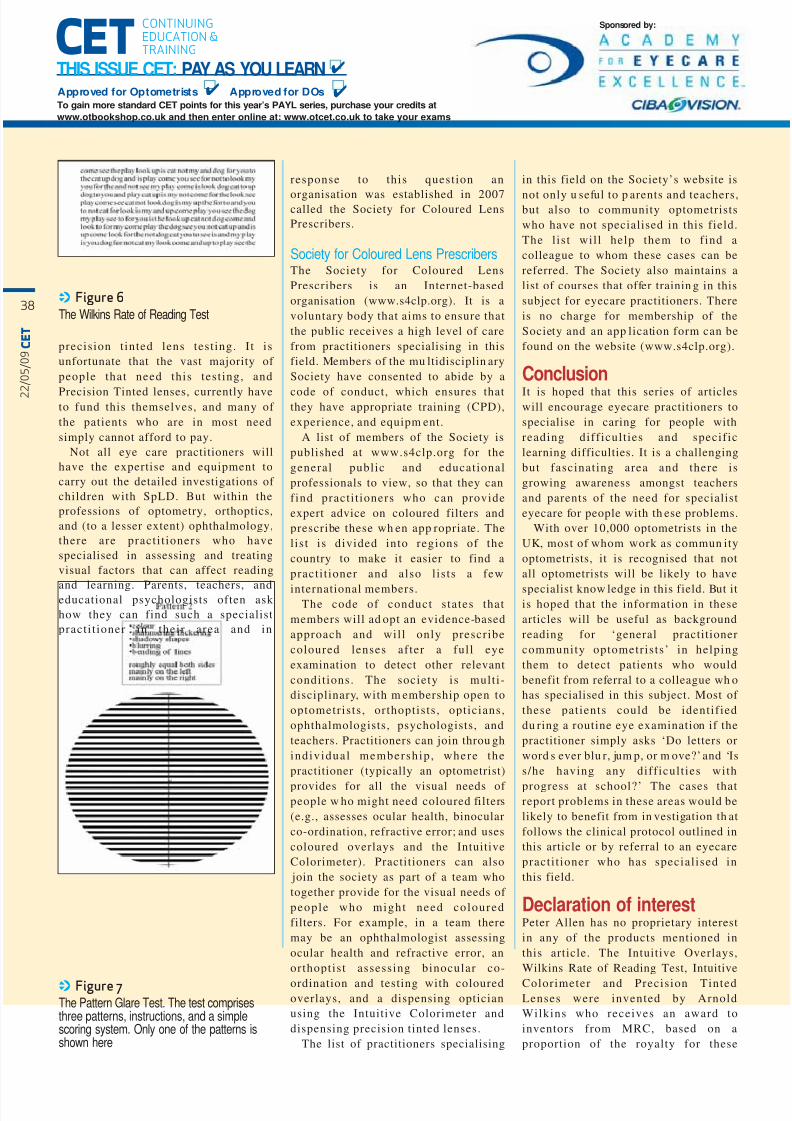
in a small closely spaced font (Figure6). There are four p assages (labelled Ato D) of random words includ ed in thetest pack.
First, the patient is asked to readpassage D to familiarise themselveswith the test. They can be stoppedafter 30 seconds, or earlier, if this iseffortful. Their preferred overlay
should then be p laced over passage Aand the patients asked to read theword s aloud as fast as possible, for oneminute, while t rying not to makemistakes. Time them with astopwatch, or an interval timer. Therecord sheet should be used to scoretheir reading; place a stroke throughomitted words and ignore words readaloud that are not in the text. If a lineis missed out then place the wholeline in brackets (more discrete thancrossing it through). Use a double
stroke (//) to indicate the final wordspoken by the patient. Note the totalnumber of words correct ly read,subtracting omitted words and lines. If a pair of words has been reversed in
of determining this. The first approach(‘sustained use’) is to dispen se the ch ildwith an overlay to use for a few weeksand to invite them to return for testingwith the Colorimeter i f the chi ld,parent, and/or teacher feel that theoverlay is helping. An al ternat iveapproach is to test the immediate effectof the coloured overlay on the child’s
performance. The most commonmethod of doing this is to use theWilkins Rate of Reading Test (WRRT),which is described later. Practitionersneed to be flexible and be prepared touse either of these methods, or both,when determining whether to progressto testing with the Colorimeter. Forsome children, the main benefit fromthe overlay is in reading performance,so the WRRT will be the best approach;for others, the main benefit from theoverlay is in visual comfort, so the
sustained use app roach will work best.
The Wilkins Rate of Reading Test (WRRT)The WRRT 14 consists of ten simplewords arranged in a random order and
< Figure 4Intuitive Overlays. The left side of the figure shows the overlay test underway. The right side of the figure shows the spectral reflectance of theoverlays; these surround the Uniform Chromaticity Scale diagram of the International Lighting Commission (CIE 1976). The inner ring of whitepoints, and the central point (grey overlay) show the chromaticities of the nine Intuitive Overlays, when in contact with a white (spectrally uniform)page. The chromaticities of double overlays formed by placing one overlay on top of another are shown by the outer ring of points. The filledpoints are the chromaticites of two overlays of identical colour. The crosses mark the chromaticities of two overlays of neighbouring colours. Thelines connect the chromaticities of the double overlays with those of constituent single overlays. Note that the reflectance functions take noaccount of the level of the illumination.
8/7/2019 Clinical protocol and the role of teh eye care practitioner
http://slidepdf.com/reader/full/clinical-protocol-and-the-role-of-teh-eye-care-practitioner 5/10
2 2 / 0 5 / 0 9 C E T
6
Sponsored by:
Approved for Optometrists Approved for DOs
CONTINUINGEDUCATION &TRAININGCET
THIS ISSUE CET: PAY AS YOU LEARN✔
To gain more standard CET points for this year’s PAYL series, purchase your credits atwww.otbookshop.co.uk and then enter online at: www.otcet.co.uk to take your exams
✔
✔
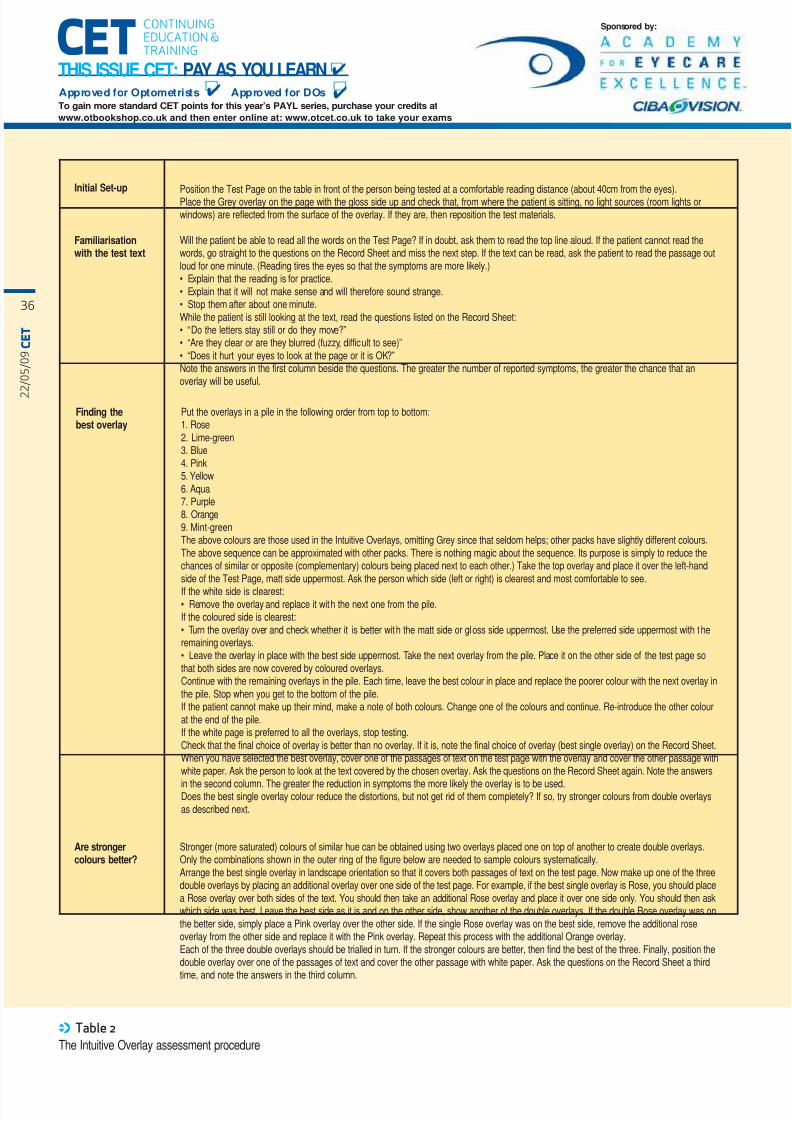
Initial Set-up Position the Test Page on the table in front of the person being tested at a comfortable reading distance (about 40cm from the eyes).Place the Grey overlay on the page with the gloss side up and check that, from where the patient is sitting, no light sources (room lights orwindows) are reflected from the surface of the overlay. If they are, then reposition the test materials.
Familiarisationwith the test text
Will the patient be able to read all the words on the Test Page? If in doubt, ask them to read the top line aloud. If the patient cannot read thewords, go straight to the questions on the Record Sheet and miss the next step. If the text can be read, ask the patient to read the passage outloud for one minute. (Reading tires the eyes so that the symptoms are more likely.)• Explain that the reading is for practice.• Explain that it will not make sense and will therefore sound strange.• Stop them after about one minute.While the patient is still looking at the text, read the questions listed on the Record Sheet:• “Do the letters stay still or do they move?”• “Are they clear or are they blurred (fuzzy, difficult to see)”• “Does it hurt your eyes to look at the page or it is OK?”Note the answers in the first column beside the questions. The greater the number of reported symptoms, the greater the chance that anoverlay will be useful.
Finding thebest overlay
Put the overlays in a pile in the following order from top to bottom:1. Rose2. Lime-green3. Blue4. Pink5. Yellow6. Aqua7. Purple8. Orange9. Mint-greenThe above colours are those used in the Intuitive Overlays, omitting Grey since that seldom helps; other packs have slightly different colours.The above sequence can be approximated with other packs. There is nothing magic about the sequence. Its purpose is simply to reduce thechances of similar or opposite (complementary) colours being placed next to each other.) Take the top overlay and place it over the left-handside of the Test Page, matt side uppermost. Ask the person which side (left or right) is clearest and most comfortable to see.If the white side is clearest:• Remove the overlay and replace it with the next one from the pile.If the coloured side is clearest:• Turn the overlay over and check whether it is better with the matt side or gloss side uppermost. Use the preferred side uppermost with theremaining overlays.• Leave the overlay in place with the best side uppermost. Take the next overlay from the pile. Place it on the other side of the test page sothat both sides are now covered by coloured overlays.Continue with the remaining overlays in the pile. Each time, leave the best colour in place and replace the poorer colour with the next overlay inthe pile. Stop when you get to the bottom of the pile.If the patient cannot make up their mind, make a note of both colours. Change one of the colours and continue. Re-introduce the other colourat the end of the pile.If the white page is preferred to all the overlays, stop testing.Check that the final choice of overlay is better than no overlay. If it is, note the final choice of overlay (best single overlay) on the Record Sheet.When you have selected the best overlay, cover one of the passages of text on the test page with the overlay and cover the other passage withwhite paper. Ask the person to look at the text covered by the chosen overlay. Ask the questions on the Record Sheet again. Note the answers
in the second column. The greater the reduction in symptoms the more likely the overlay is to be used.Does the best single overlay colour reduce the distortions, but not get rid of them completely? If so, try stronger colours from double overlaysas described next.
Are strongercolours better?
Stronger (more saturated) colours of similar hue can be obtained using two overlays placed one on top of another to create double overlays.Only the combinations shown in the outer ring of the figure below are needed to sample colours systematically.Arrange the best single overlay in landscape orientation so that it covers both passages of text on the test page. Now make up one of the threedouble overlays by placing an additional overlay over one side of the test page. For example, if the best single overlay is Rose, you should placea Rose overlay over both sides of the text. You should then take an additional Rose overlay and place it over one side only. You should then askwhich side was best. Leave the best side as it is and on the other side, show another of the double overlays. If the double Rose overlay was onthe better side, simply place a Pink overlay over the other side. If the single Rose overlay was on the best side, remove the additional roseoverlay from the other side and replace it with the Pink overlay. Repeat this process with the additional Orange overlay.Each of the three double overlays should be trialled in turn. If the stronger colours are better, then find the best of the three. Finally, position thedouble overlay over one of the passages of text and cover the other passage with white paper. Ask the questions on the Record Sheet a thirdtime, and note the answers in the third column.
< Table 2The Intuitive Overlay assessment procedure

8/7/2019 Clinical protocol and the role of teh eye care practitioner
http://slidepdf.com/reader/full/clinical-protocol-and-the-role-of-teh-eye-care-practitioner 6/10
2 2 / 0 5 / 0 9 C E T
37
order, count only one of the pair.
This procedure is repeated w ith thecoloured overlay removed and usingPassage B and again, without theoverlay, with Passage C. Theprocedure is then repeated, now withthe overlay, using Passage D. Thepractitioner should then calculate theaverage percentage increase inreading speed w ith the overlay.
If a percentage increase in readingspeed of 5% or more is shown, thenthe patient may benefit from testingwith the Intui t ive Colorimeter,
part icular ly i f they reportedsymp toms. If a percen tage increase inreading speed of 10% or more isshown with th e overlay, then they arevery likely to benefit from precisiontinted lenses and should definitely betested with the Intuitive Colorimeter.
The Pattern Glare TestAnother test that can provide usefulinformation that can help to predictreading performance, particularly inpat ients where the main problem
seems to be headaches or discomfort,is the Pattern Glare Test (Figure 7).The fourth article of this seriesdiscussed the mechanism for thebenefi t f rom coloured lenses andnoted th at the m ost likely explanationrelates to a hyperexcitability of thevisual cortex. The hyp erexcitability islikely to result in sen sitivity to certainvisual p atterns. 15 Pattern glare can bedetected with the Pattern Glare Test. 16
With this very simple test, the patientdescribes their symptoms (in answer
to a list of questions) whilst viewingeach of three visual patterns, and theirresponses indicate their susceptibilityto pattern glare. The test can be u sefulfor determining the cases most likelyto benefit from coloured filters. 17
The Pattern Glare Test comprisesthree gratings of differing spatialfrequencies: low SF (Pattern 1),medium SF (Pattern 2), and high SF(Pattern 3). A normative study of thePattern Glare Test showed that p eoplehave an abnormal degree of pattern
glare if they achieve a score of >3 onthe medium SF grating or a score of >1 when the score for the high SFpattern is subtracted from the scorefor the medium SF pattern 27 . Such
Sponsored by:
Approved for Optometrists Approved for DOs
CONTINUINGEDUCATION &TRAININGCET
THIS ISSUE CET: PAY AS YOU LEARN✔
To gain more standard CET points for this year’s PAYL series, purchase your credits atwww.otbookshop.co.uk and then enter online at: www.otcet.co.uk to take your exams
✔
✔
< Figure 5Intuitive Overlay colours. Each single overlay(inner ring) is associated with stronger colours(outer ring) formed by combining the overlaywith another of the same or similar colour
people are likely to benefit from
coloured filters26
.
The Intuitive ColorimeterIntui t ive Overlays are a usefulscreening tool but are not particularlygood as a long-term solution forreading difficulties, due to a limitedrange of colours and theinconvenience of having to beremoved and replaced every time apage is turned. Patients are almostalways helped more by the use of Precision Tinted lenses, since they are
present in front of the eyes and cantherefore be used for board work,writing, and compu ter work.
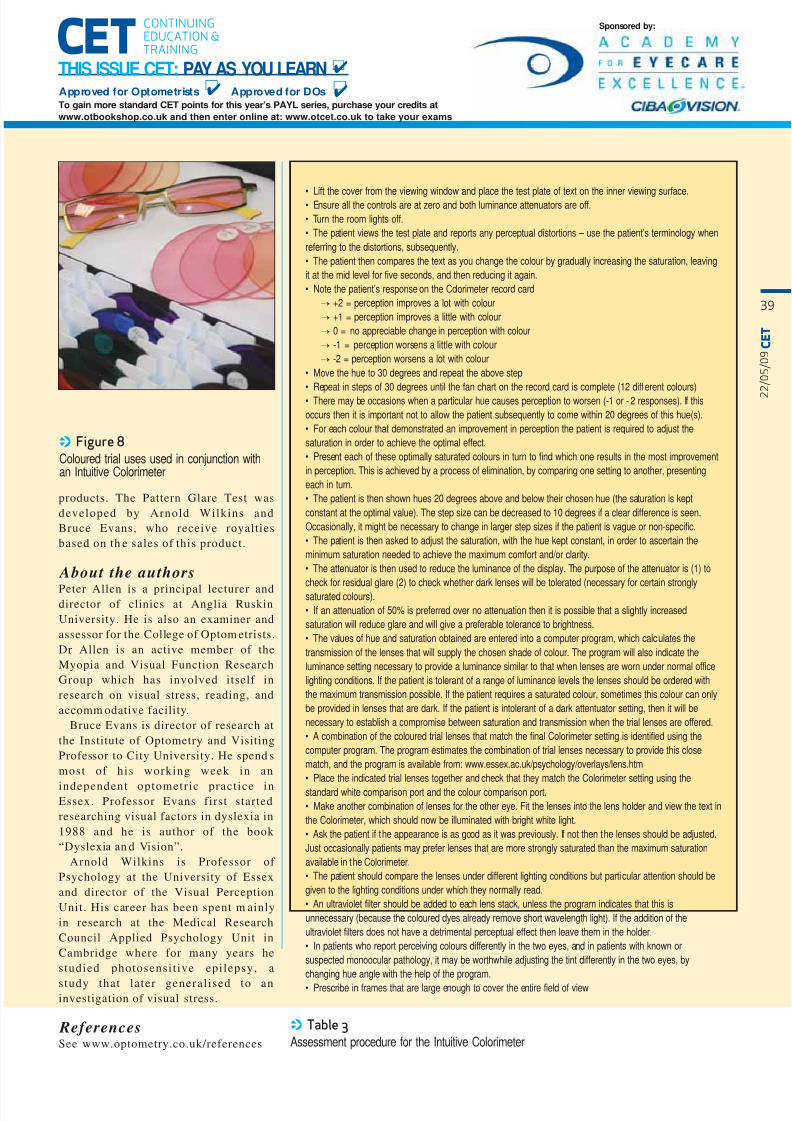
The Intu itive Colorimeter, describedin the third article in this series, is aninstrument that illuminates a page of text with coloured light and it can beused to prescribe individually specifictinted lenses (Figure 8). It enablesseparate variation in hue (colour) andsaturation (depth of colour) withoutan associated change in luminance(brightness). The hue, saturation and
luminance can al l be adjustedindependently. One major advantageof the Intuitive Colorimeter over theIntuitive Overlays is that the variationin colour is continuous rather than indiscrete steps. The entire visual fieldis stimulated with coloured light, aswhen tinted spectacles are worn. Thetest procedure is described in Table 3.
Prescribing advice for precisiontinted lensesChildren should be advised to wear
their precision t inted lenses forschoolwork, including homework, if they find them helpful. For adults,they are likely to be helpful for officework and reading. Often users findthem valuable for computer use,sometimes for television, and forenvironments where there are highlevels of fluorescent lighting, such assupermarkets. But patients should beadvised not to wear them outdoors assunglasses since they are not likely toprotect the eyes from sunlight in the
way that sunglasses will. Precisiontinted lenses should usually not beworn w hen driving or riding a bicycle,i f they are l ikely to impair theperception of traffic signals. The
computer program that is providedwith the colorimeter al lowspractitioners to check this, as well asthe safety for use in daylight, for therare cases where a p atient may wish towear th e lenses constantly (eg migraine
sufferer). The wearing of any tints fordriving at night is prohibited.
Funding and finding anappropriate practitionerThe most accepted mainstreamintervention for children with SpLD isspecialist teaching, ideally on a one-to-one basis. This is justified since themain cause of the commonest SpLD,dyslexia, is poor phonologicaldecod ing (see Part 1 of this series). Butmany children w ith reading difficulties
or other SpLD will also have visualproblems. In some cases, children maybe misdiagnosed as having SpLDswhen in fact al l they need is anoptometric intervention.
The most common visual problem inpeople with reading difficulties seemsto be visual stress, but before this canbe diagnosed practitioners need to ruleout a variety of other visual disorders(Figure 1). This requires a detailed eyeexamination, which, including thetesting for coloured filters, typically
takes about an hour. For communityoptom etrists, the NHS sight test fee willnot cover this detailed investigationwhilst there are very few secondarycare NHS hospitals that currently fund
8/7/2019 Clinical protocol and the role of teh eye care practitioner
http://slidepdf.com/reader/full/clinical-protocol-and-the-role-of-teh-eye-care-practitioner 7/10
2 2 / 0 5 / 0 9 C E T
8
Sponsored by:
Approved for Optometrists Approved for DOs
CONTINUINGEDUCATION &TRAININGCET
THIS ISSUE CET: PAY AS YOU LEARN✔
To gain more standard CET points for this year’s PAYL series, purchase your credits atwww.otbookshop.co.uk and then enter online at: www.otcet.co.uk to take your exams
✔
✔
precision t inted lens test ing. I t isunfortunate that the vast majority of people that need this test ing, and
Precision Tinted lenses, currently haveto fund this themselves, and many of the patients who are in most needsimply cannot afford to pay.
Not all eye care practitioners willhave the expertise and equipment tocarry out the detailed investigations of children with SpLD. But within theprofessions of optometry, orthoptics,and (to a lesser extent) ophthalmology,there are pract i t ioners who havespecialised in assessing and treatingvisual factors that can affect reading
and learning. Parents, teachers, andeducational psychologists often ask how they can find such a specialistpract i t ioner in their area and in
in this field on the Society’s website is
not only u seful to p arents and teachers,but also to community optometristswho have not specialised in this field.The l is t wil l help them to f ind acolleague to whom these cases can bereferred. The Society also maintains alist of courses that offer trainin g in thissubject for eyecare practitioners. Thereis no charge for membership of theSociety and an app lication form can befound on the website (www.s4clp.org).
ConclusionIt is hoped that this series of articleswill encourage eyecare practitioners tospecialise in caring for people withreading diff icul t ies and specif iclearning difficulties. It is a challengingbut fascinat ing area and there isgrowing awareness amongst teachersand parents of the need for specialisteyecare for people with th ese problems.
With over 10,000 optometrists in theUK, most of whom work as commun ityoptometrists, it is recognised that notall optometrists will be likely to have
specialist know ledge in this field. But itis hoped that the information in thesearticles will be useful as backgroundreading for ‘general practitionercommunity optometr is ts’ in helpingthem to detect patients who wouldbenefit from referral to a colleague wh ohas specialised in this subject. Most of these pat ients could be identif ieddu ring a routine eye examination if thepractitioner simply asks ‘Do letters orword s ever blu r, jum p, or m ove?’ and ‘Iss/he having any diff icul t ies with
progress at school?’ The cases thatreport problems in these areas would belikely to benefit from in vestigation th atfollows the clinical protocol outlined inthis article or by referral to an eyecarepract i t ioner who has special ised inthis field.
Declaration of interestPeter Allen has no proprietary interestin any of the products mentioned inthis article. The Intuitive Overlays,Wilkins Rate of Reading Test, Intuitive
Colorimeter and Precision TintedLenses were invented by ArnoldWilkins who receives an award toinventors from MRC, based on aproportion of the royalty for these
response to this quest ion an
organisation was established in 2007called the Society for Coloured LensPrescribers.
Society for Coloured Lens PrescribersThe Society for Coloured LensPrescribers is an Internet-basedorganisation (www.s4clp.org). It is avoluntary body that aims to ensure thatthe public receives a high level of carefrom practitioners specialising in thisfield. Members of the mu ltidisciplin arySociety have consented to abide by a
code of conduct, which ensures thatthey have appropriate training (CPD),experience, and equipm ent.
A list of members of the Society ispublished at www.s4clp.org for thegeneral public and educat ionalprofessionals to view, so that they canfind pract i t ioners who can provideexpert advice on coloured filters andprescribe these wh en app ropriate. Thelis t is divided into regions of thecountry to make it easier to find apract i t ioner and also l is ts a few
international members.The code of conduct s tates that
members will ad opt an evidence-basedapproach and wil l only prescribecoloured lenses af ter a ful l eyeexamination to detect other relevantcondit ions. The society is mult i -disciplinary, with m embership open tooptometris ts , or thoptis ts , opt icians,ophthalmologists, psychologists, andteachers. Practitioners can join throu ghind iv idua l membersh ip , where thepractitioner (typically an optometrist)
provides for all the visual needs of people w ho might need coloured filters(e.g., assesses ocular health, binocularco-ordination, refractive error; and usescoloured overlays and the IntuitiveColorimeter). Practitioners can also
join the society as part of a team whotogether provide for the visual needs of people who might need co louredfilters. For example, in a team theremay be an ophthalmologist assessingocular health and refractive error, anorthoptis t assessing binocular co-
ordination and testing with colouredoverlays, and a dispensing opticianusing the Intuitive Colorimeter anddispensing precision tinted lenses.
The list of practitioners specialising
< Figure 6The Wilkins Rate of Reading Test
< Figure 7The Pattern Glare Test. The test comprisesthree patterns, instructions, and a simplescoring system. Only one of the patterns isshown here
8/7/2019 Clinical protocol and the role of teh eye care practitioner
http://slidepdf.com/reader/full/clinical-protocol-and-the-role-of-teh-eye-care-practitioner 8/10
2 2 / 0 5 / 0 9 C E T
39
Sponsored by:
Approved for Optometrists Approved for DOs
CONTINUINGEDUCATION &TRAININGCET
THIS ISSUE CET: PAY AS YOU LEARN✔
To gain more standard CET points for this year’s PAYL series, purchase your credits atwww.otbookshop.co.uk and then enter online at: www.otcet.co.uk to take your exams
✔
✔
products. The Pattern Glare Test wasdeveloped by Arnold Wilkins andBruce Evans, who receive royaltiesbased on th e sales of this product.
About the authorsPeter Allen is a principal lecturer anddirector of clinics at Anglia RuskinUniversity. He is also an examiner andassessor for the College of Optom etrists.Dr Allen is an active member of theMyopia and Visual Function ResearchGroup which has involved itself inresearch on visual stress, reading, andaccomm odative facility.
Bruce Evans is director of research atthe Institute of Optometry and VisitingProfessor to City University. He spend smost of his working week in an
independent optometr ic pract ice inEssex. Professor Evans first startedresearching visual factors in dyslexia in1988 and he is author of the book “Dyslexia an d Vision”.
Arnold Wilkins is Professor of Psychology at the University of Essexand director of the Visual PerceptionUnit. His career has been spent m ainlyin research at the Medical ResearchCouncil Applied Psychology Unit inCambridge where for many years hestudied photosensi t ive epi lepsy, a
study that la ter general ised to aninvestigation of visual stress.
ReferencesSee www.optometry.co.uk/references
• Lift the cover from the viewing window and place the test plate of text on the inner viewing surface.• Ensure all the controls are at zero and both luminance attenuators are off.• Turn the room lights off.• The patient views the test plate and reports any perceptual distortions – use the patient’s terminology whenreferring to the distortions, subsequently.• The patient then compares the text as you change the colour by gradually increasing the saturation, leavingit at the mid level for five seconds, and then reducing it again.• Note the patient’s response on the Colorimeter record card
→ +2 = perception improves a lot with colour→ +1 = perception improves a little with colour→ 0 = no appreciable change in perception with colour→ -1 = perception worsens a little with colour→ -2 = perception worsens a lot with colour
• Move the hue to 30 degrees and repeat the above step• Repeat in steps of 30 degrees until the fan chart on the record card is complete (12 different colours)• There may be occasions when a particular hue causes perception to worsen (-1 or - 2 responses). If thisoccurs then it is important not to allow the patient subsequently to come within 20 degrees of this hue(s).• For each colour that demonstrated an improvement in perception the patient is required to adjust thesaturation in order to achieve the optimal effect.• Present each of these optimally saturated colours in turn to find which one results in the most improvementin perception. This is achieved by a process of elimination, by comparing one setting to another, presentingeach in turn.• The patient is then shown hues 20 degrees above and below their chosen hue (the saturation is keptconstant at the optimal value). The step size can be decreased to 10 degrees if a clear difference is seen.Occasionally, it might be necessary to change in larger step sizes if the patient is vague or non-specific.• The patient is then asked to adjust the saturation, with the hue kept constant, in order to ascertain theminimum saturation needed to achieve the maximum comfort and/or clarity.• The attenuator is then used to reduce the luminance of the display. The purpose of the attenuator is (1) tocheck for residual glare (2) to check whether dark lenses will be tolerated (necessary for certain stronglysaturated colours).• If an attenuation of 50% is preferred over no attenuation then it is possible that a slightly increasedsaturation will reduce glare and will give a preferable tolerance to brightness.• The values of hue and saturation obtained are entered into a computer program, which calculates thetransmission of the lenses that will supply the chosen shade of colour. The program will also indicate theluminance setting necessary to provide a luminance similar to that when lenses are worn under normal officelighting conditions. If the patient is tolerant of a range of luminance levels the lenses should be ordered withthe maximum transmission possible. If the patient requires a saturated colour, sometimes this colour can onlybe provided in lenses that are dark. If the patient is intolerant of a dark attentuator setting, then it will benecessary to establish a compromise between saturation and transmission when the trial lenses are offered.• A combination of the coloured trial lenses that match the final Colorimeter setting is identified using thecomputer program. The program estimates the combination of trial lenses necessary to provide this closematch, and the program is available from: www.essex.ac.uk/psychology/overlays/lens.htm• Place the indicated trial lenses together and check that they match the Colorimeter setting using thestandard white comparison port and the colour comparison port.• Make another combination of lenses for the other eye. Fit the lenses into the lens holder and view the text inthe Colorimeter, which should now be illuminated with bright white light.• Ask the patient if the appearance is as good as it was previously. If not then the lenses should be adjusted.Just occasionally patients may prefer lenses that are more strongly saturated than the maximum saturationavailable in the Colorimeter.• The patient should compare the lenses under different lighting conditions but particular attention should begiven to the lighting conditions under which they normally read.• An ultraviolet filter should be added to each lens stack, unless the program indicates that this isunnecessary (because the coloured dyes already remove short wavelength light). If the addition of theultraviolet filters does not have a detrimental perceptual effect then leave them in the holder.• In patients who report perceiving colours differently in the two eyes, and in patients with known orsuspected monoocular pathology, it may be worthwhile adjusting the tint differently in the two eyes, bychanging hue angle with the help of the program.• Prescribe in frames that are large enough to cover the entire field of view
< Table 3Assessment procedure for the Intuitive Colorimeter
< Figure 8Coloured trial uses used in conjunction withan Intuitive Colorimeter

8/7/2019 Clinical protocol and the role of teh eye care practitioner
http://slidepdf.com/reader/full/clinical-protocol-and-the-role-of-teh-eye-care-practitioner 9/10
2 2 / 0 5 / 0 9 C E T
0
Module questions Course code: c-11112Please note, there is only one correct answer. Enter online or by the form provided
An answer return form is included in this issue. It should be completed and returned to CET initiatives (c-11112)OT , Ten Alps plc, 9 Savoy Street, London WC2E 7HR by July 22 2009
Please complete online by midnight on July 22 2009 - You will be unable to submit exams after this date – answers to the module will be published on www.optometry.co.uk
7) Which statement about coloured filters is MOST accurate?a. Coloured filters are the best long term solution for reading problemsb. Precision tinted lenses help the patient less than coloured overlaysc. A major advantage of the Colorimeter is that the variation in colour is
continuous rather than in discrete steps.d. The Colorimeter allows variation in hue and luminance.
8) Which statement about the attenuator on the IntuitiveColorimeter is FALSE?
a. It is used to check for residual glareb. It is used to check whether the saturation is sufficientc. It is used to check whether a dark tint will be toleratedd. It is used to check whether the addition of a grey dye is necessary
9) Which statement about the tinted trial lenses of the IntuitiveColorimeter is TRUE?
a. The tint can be checked under usual lighting conditions encounteredb. A compromise between the saturation of tint desired and the darkness of
tint necessary is establishedc. They allow examination of the effects of a different tint in each eye,
where indicatedd. All of the above
10) Which statement about Precision Tinted lenses is TRUE?a. The tint can be checked under usual lighting conditions encounteredb. The lens colour will be the same as the overlay colourc. The lens colour will not need to be changedd. Normal colour vision is required for testing with Precision Tinted lenses
11) Which statement about wearing Precision Tinted lenses is TRUE?a. They should only be worn under fluorescent lightingb. They are usually worn indoorsc. They are usually worn outdoorsd. They will not interfere with colour perception
12) Which statement about the Society of Coloured Lens Prescribersis FALSE?
a. It is based in Sloughb. It is an Internet based organisationc. It has members from a variety of disciplinesd. It encourages specialist practitioners to provide high levels of care
1) Which statement is MOST accurate about the clinical protocol formanaging children with reading difficulties?
a. If overlays help, Precision Tinted lenses are needed but binocular visiondoes not have to be assessed
b. The Intuitive Colorimeter should be used before screening with overlaysc. Ocular health does not need to be assessedd. Once Precision Tinted lenses are prescribed, the colour should be
checked annually
2) Which statement is MOST accurate about eye examinations requiredfor children with reading difficulties?
a. They can only be carried out by a community optometristb. They can only be carried out in the hospital eye servicec. They are likely to include tests over and above the usual NHS sight testd. They are likely to include tests that are unfamiliar to optometrists and
orthoptists
3) Which statement about fusional reserves is FALSE?a. The fusional reserve opposing the heterophoria should be measured firstb. Base-in prism is used to measure the convergent fusional reservec. The blur, break and recovery points should be notedd. Fusional reserve exercises can be used to treat binocular instability
4) Which statement about lag of accommodation is FALSE?a. It is usually +0.50D in magnitudeb. A value of less than +1.00D may represent accommodative insufficiencyc. A value of more than +1.00D may represent accommodative insufficiencyd. It can be measured using MEM Retinoscopy
5) Which statement about the Pattern Glare Test is TRUE?a. It comprises four gratings of differing spatial frequenciesb. A score of under 3 on the medium SF grating indicates abnormal
pattern glarec. Reading speed is measured during the Pattern Glare Testd. It can be useful for determining patients most likely to benefit from
coloured lenses
6) Which of the following is NOT useful for deciding who needs testing withthe Intuitive Colorimeter?
a. The Pattern Glare Testb. Issuing a coloured overlay to see if a person uses it for a sustained periodc. Investigating the effect of the coloured overlay on the rate of reading testd. The 100 hue test
Sponsored by:
Approved for Optometrists Approved for DOs
CONTINUINGEDUCATION &TRAININGCET
THIS ISSUE CET: PAY AS YOU LEARN✔
To gain more standard CET points for this year’s PAYL series, purchase your credits atwww.otbookshop.co.uk and then enter online at: www.otcet.co.uk to take your exams
✔
✔

8/7/2019 Clinical protocol and the role of teh eye care practitioner
http://slidepdf.com/reader/full/clinical-protocol-and-the-role-of-teh-eye-care-practitioner 10/10
2 2 / 0 5 / 0 9 C E T
39
Sponsored by:
Approved for Optometrists Approved for DOs
CONTINUINGEDUCATION &TRAININGCET
THIS ISSUE CET: PAY AS YOU LEARN✔
To gain more standard CET points for this year’s PAYL series, purchase your credits atwww.otbookshop.co.uk and then enter online at: www.otcet.co.uk to take your exams
✔
✔


















