
Clinical Policy Title: Intra-articular hyaluronic acid ... · 1 Clinical Policy Title:...
15
1 Clinical Policy Title: Intra-articular hyaluronic acid injection for osteoarthritis Clinical Policy Number: 00.02.08 Effective Date: October 1, 2014 Initial Review Date: April 16, 2014 Most Recent Review Date: July 20, 2016 Next Review Date: July 2017 Related policies: CP# 14.02.08 Prolotherapy ABOUT THIS POLICY: Keystone First has developed clinical policies to assist with making coverage determinations. Keystone First’s clinical policies are based on guidelines from established industry sources, such as the Centers for Medicare & Medicaid Services (CMS), state regulatory agencies, the American Medical Association (AMA), medical specialty professional societies, and peer-reviewed professional literature. These clinical policies, along with other sources, such as plan benefits and state and federal laws and regulatory requirements, including any state- or plan-specific definition of “medically necessary,” and the specific facts of the particular situation are considered by Keystone First when making coverage determinations. In the event of conflict between this clinical policy and plan benefits and/or state or federal laws and/or regulatory requirements, the plan benefits and/or state and federal laws and/or regulatory requirements shall control. Keystone First’s clinical policies are for informational purposes only and not intended as medical advice or to direct treatment. Physicians and other health care providers are solely responsible for the treatment decisions for their patients. Keystone First’s clinical policies are reflective of evidence-based medicine at the time of review. As medical science evolves, Keystone First will update its clinical policies as necessary. Keystone First’s clinical policies are not guarantees of payment. Coverage policy Keystone First considers the use of intra-articular injection with hyaluronic acid (HA) to be clinically proven and, therefore, medically necessary when all of the following criteria are met: Criteria for Medical Necessity (Criteria A,B,C,D,E and F must be met) A. Documented symptomatic mild to moderate knee osteoarthritis. B. Patient reports pain interfering with functional activities, such as ambulation or prolonged standing. C. One of the following criteria: 1. Conservative therapy (oral medications) over the past four months has not resulted in functional improvement after at least three months; 2. Patient cannot tolerate other treatments (e.g., non-steroidal anti-inflammatory drugs [NSAIDs]) because of adverse effects; 3. Other therapy is contraindicated because of other medical problems; 4. Steroid injection therapy was administered within the prior two months and aspiration for effusion was unsuccessful, per affected knee; or 5. There is a medical reason for not being able to utilize steroid injections. D. The pain cannot be attributed to other forms of joint disease. Policy contains: Hyaluronic acid. Viscosupplementation. Osteoarthritis of the knee. Chondromalacia.
Transcript of Clinical Policy Title: Intra-articular hyaluronic acid ... · 1 Clinical Policy Title:...

1
Clinical Policy Title: Intra-articular hyaluronic acid injection for osteoarthritis
Clinical Policy Number: 00.02.08
Effective Date: October 1, 2014
Initial Review Date: April 16, 2014
Most Recent Review Date: July 20, 2016
Next Review Date: July 2017
Related policies:
CP# 14.02.08 Prolotherapy
ABOUT THIS POLICY: Keystone First has developed clinical policies to assist with making coverage determinations. Keystone First’s clinical policies are based on guidelines from established industry sources, such as the Centers for Medicare & Medicaid Services (CMS), state regulatory agencies, the American Medical Association (AMA), medical specialty professional societies, and peer-reviewed professional literature. These clinical policies, along with other sources, such as plan benefits and state and federal laws and regulatory requirements, including any state- or plan-specific definition of “medically necessary,” and the specific facts of the particular situation are considered by Keystone First when making coverage determinations. In the event of conflict between this clinical policy and plan benefits and/or state or federal laws and/or regulatory requirements, the plan benefits and/or state and federal laws and/or regulatory requirements shall control. Keystone First’s clinical policies are for informational purposes only and not intended as medical advice or to direct treatment. Physicians and other health care providers are solely responsible for the treatment decisions for their patients. Keystone First’s clinical policies are reflective of evidence-based medicine at the time of review. As medical science evolves, Keystone First will update its clinical policies as necessary. Keystone First’s clinical policies are not guarantees of payment.
Coverage policy
Keystone First considers the use of intra-articular injection with hyaluronic acid (HA) to be clinically proven and,
therefore, medically necessary when all of the following criteria are met:
Criteria for Medical Necessity
(Criteria A,B,C,D,E and F must be met)
A. Documented symptomatic mild to moderate knee osteoarthritis.
B. Patient reports pain interfering with functional activities, such as ambulation or prolonged standing.
C. One of the following criteria:
1. Conservative therapy (oral medications) over the past four months has not resulted in functional
improvement after at least three months;
2. Patient cannot tolerate other treatments (e.g., non-steroidal anti-inflammatory drugs [NSAIDs])
because of adverse effects;
3. Other therapy is contraindicated because of other medical problems;
4. Steroid injection therapy was administered within the prior two months and aspiration for
effusion was unsuccessful, per affected knee; or
5. There is a medical reason for not being able to utilize steroid injections.
D. The pain cannot be attributed to other forms of joint disease.
Policy contains:
Hyaluronic acid.
Viscosupplementation.
Osteoarthritis of the knee.
Chondromalacia.

2
Criteria for Medical Necessity
(Criteria A,B,C,D,E and F must be met)
E. A single course of treatment is given as described in the package insert of each product
F. Specific prior authorization criteria in Appendix A are met.
Limitations:
All other uses of intra-articular injection with hyaluronic acid are not medically necessary.
Other uses include, but are not limited to:
Lateral epidcondyltis (“tennis elbow”), as the condition is frequently self-limiting.
Glenohumeral joint arthritis.
Any tendinitis diagnosis.
Chondromalacia.
Coverage of specific pharmaceuticals and/or treatments is subject to prior authorization by plan
criteria. Prior authorization criteria for the pharmaceuticals listed in this policy is set forth in Appendix
A.
Alternative covered services:
Simple analgesics, nonsteroidal anti-inflammatory drugs (NSAIDs), and corticosteroid injections.
Background
Osteoarthritis (OA) is a chronic and progressive disease resulting from failure of joint cartilage repair after
breakdown or wear, accompanied by changes in synovial fluid, pain, and joint movement limitations. OA is the
most common type of arthritis, particularly in the elderly, and is associated with high rates of disability. Aging
populations and the risk factor of obesity contribute to increasing prevalence in developed countries — U.S.
(United States) prevalence is expected to nearly double by 2020. The most commonly affected joints include
cervical and lumbosacral spine, hip, knee, and first metatarsal-phalangeal (base of thumb); in other words, joints
ill-suited by evolution for prolonged weight bearing or other bipedal locomotion uses, while others (wrist and
elbow) are usually spared.
OA is diagnosed by structural abnormalities (loss of joint space) on imaging studies and associated symptoms
(activity-related joint pain and disability). Pharmacologic treatment includes acetaminophen, NSAIDs, and COX-2
inhibitors. Other options are intra-articular injections with corticosteroids or hyaluronic acid. Optimal therapy
tends to the idiosyncratic and is achieved by trial and error for each patient. When medical therapy fails and
patients find unacceptable reduction in quality of life, knee or hip total arthroplasty (arthroscopic debridement
and lavage) may be considered.
Sodium hyaluronate HA is a viscoelastic substance occurring naturally in synovial fluid and extracellular matrices of
many tissues, including cartilage and skin. It plays a role in joint lubrication, protection, and cartilage maintenance.
Commercially available preparations, administered as intra-articular injections, are used to relieve pain, improve
synovial fluid quantity or quality, and to modify disease progression in osteoarthritis and other joint diseases.
Other medical uses of HA include:
Dry, scaly skin, such as that caused by atopic dermatitis or eczema, in a prescription skin lotion
containing sodium hyaluronate as its active ingredient.

3
As a tumor marker for prostate and breast cancer. In some cancers, HA levels correlate well with
malignancy and poor prognosis. It may also be used to monitor the progression of the disease.
Postoperatively to induce tissue healing, notably after cataract surgery. Current models of wound
healing propose the larger polymers of HA appear in the early stages of healing to physically make
room for white blood cells, which mediate the immune response.
In the synthesis of biological scaffolds for wound-healing applications. These scaffolds typically have
proteins such as fibronectin attached to the HA to facilitate cell migration into the wound. This
application is particularly important for individuals with diabetes suffering from chronic wounds, such
as foot or leg ulcers.
Searches
Keystone First searched PubMed and the databases of:
UK National Health Services Centre for Reviews and Dissemination.
Agency for Healthcare Research and Quality Guideline Clearinghouse and evidence-based practice
centers.
The Centers for Medicare & Medicaid Services.
We conducted searches on June 22, 2016. Searched terms were “hyaluronic acid,” “injection therapies” and
“osteoarthritis.”
We included:
Systematic reviews, which pool results from multiple studies to achieve larger sample sizes and
greater precision of effect estimation than in smaller primary studies. Systematic reviews use
predetermined transparent methods to minimize bias, effectively treating the review as a scientific
endeavor, and are thus rated highest in evidence-grading hierarchies.
Guidelines based on systematic reviews.
Economic analyses, such as cost-effectiveness, and benefit or utility studies (but not simple cost
studies), reporting both costs and outcomes — sometimes referred to as efficiency studies — which
also rank near the top of evidence hierarchies.
Findings
The evidence supporting the efficacy and safety of HA intra-articular injection for improving pain and function in
osteoarthritis and other musculoskeletal conditions has recently improved. Prior to 2010, most reviewers cited
insufficient evidence; since then, reviewers generally agree on HA’s effectiveness. However, experts continue to
cite small study sizes and the need for larger randomized controlled trials (RCTs) to support selection criteria and
cost-utility. This information, along with the safety profiles and relative costs of included treatments, will be
helpful for individualized patient care decisions.
Keystone First identified one systematic review from the Blue Cross Blue Shield Technology Evaluation Center for
the Agency for Healthcare Research and Quality (Samson 2014); one analysis of Medicare utilization data
(Schmajuk 2014); and one clinical practice guideline from the American Academy of Orthopedic Surgeons (AAOS
2013).

4
Results of the two systematic reviews reflect some continued uncertainty regarding the effectiveness of intra-
articular HA for treatment of knee osteoarthritis. Indirect comparisons suggest some improvement in pain and
function relative to other available treatments, but comparisons to placebo have yielded conflicting results. An
analysis of Medicare utilization data found frequent use of intra-articular HA among Medicare beneficiaries despite
its higher cost, uncertain effectiveness, lack of optimal patient selection criteria, and variations in
recommendations from evidence-based guidelines. Therefore, it is reasonable to offer intra-articular HA for
individuals who have failed to respond adequately to conservative nonpharmacologic therapy, simple analgesics
and anti-inflammatories.
Policy updates
An RCT (Askari 2016) inclusive of 140 patients with knee OA randomized subjects to receive intra-articular injection
of either HA or corticosteroid. The mean age of the patients in the corticosteroid group was 57 ± 1.9 years and in
the HA group was 58.5 ± 8.3 years. Pain and stiffness did not improve in either of the groups at any time points
after the intervention (p > 0.05). However, a different pain scale suggested that symptoms improved after 3
months in both corticosteroid and HA groups, and daily activity improved in both groups (p < 0.05). The most
important difference between the two intervention groups was the duration of effectiveness: HA could be
administered intra-articularly every three months for knee joint OA, while corticosteroids needed to be injected
every two months to maintain symptom control.
Strand (2016) evaluated an injectable viscoelastic hydrogel composed of a cross-linked hyaluronate (Gel-200®) in a
13-week trial and demonstrated statistically significant improvements in patients treated with a single injection of
Gel-200 compared with a saline control. Improvements in pain score were evident as early as 3 weeks following
injection with more than 40 percent improvement from baseline. Adverse events were not significantly different
between the intervention group and saline controls. No unanticipated treatment-related serious adverse events
were reported.
A systematic review (Chandrasekaran 2016) of 72 RCTs assessed the use of corticosteroid, HA and platelet rich
plasma (PRP) in the non-operative management of OA and femoroacetabular impingement. The authors affirmed
the efficacy of diagnostic intra-articular hip injections, finding them sensitive and specific for differentiating
between intra-articular, extra-articular and spinal causes of hip symptoms. With regard to therapy, corticosteroids
were more effective than HA and PRP in alleviating pain from hip OA. A higher dose of corticosteroids produced a
longer benefit.
Summary of clinical evidence:
Citation Content, Methods, Recommendations
Askari (2016)
Hyaluronic acid compared with
corticosteroid injections for the
treatment of osteoarthritis of the
knee: a randomized control trail.
Key points:
An RCT inclusive of 140 patients with knee OA.
Randomized subjects to receive intra-articular injection of either HA or
corticosteroid.
Mean age in the corticosteroid group was 57 ± 1.9 years and in the HA group
was 58.5 ± 8.3 years.
Pain and stiffness did not improve in either of the groups at any time points
after the intervention (p > 0.05).

5
Citation Content, Methods, Recommendations
A different pain scale suggested that symptoms improved after 3 months in
both corticosteroid and HA groups (p < 0.05).
The most important difference between the two intervention groups was the
duration of effectiveness:
HA 3 months.
Corticosteroids 2 months.
Strand (2016)
Evidence for safety of retreatment
with a single intra-articular
injection of Gel-200 for treatment
of osteoarthritis of the knee from
the double-blind pivotal and open-
label retreatment clinical trials.
Key points:
An RCT evaluated Gel-200 in a 13-week trial.
Statistically significant improvements were noted compared with a saline
control.
Improvements in pain score were evident as early as 3 weeks.
Adverse events were not significantly different between the intervention group
and saline controls.
No unanticipated treatment-related serious adverse events were reported.
Chandrasekaran (2016)
Symposium: evidence for the use
of intra-articular cortisone or
hyaluronic acid injection in the
hip.
Key points:
A systematic review of 72 RCTs
Assessed the use of corticosteroid, HA and platelet rich plasma (PRP).
Affirmed the efficacy of diagnostic intra-articular hip injections.
Corticosteroids were more effective than HA and PRP in alleviating pain from
hip OA.
A higher dose of corticosteroids produced a longer benefit.
Bannuru (2015)
Therapeutic trajectory following
intra-articular hyaluronic acid
injection in knee osteoarthritis--
meta-analysis.
Key points:
Systematic review evaluated treatments for primary knee OA:- Aug 2014.
Network meta-analysis of 137 studies (33,243 subjects).
HA most efficacious treatment: effect size 0.63 (95% credible interval [CrI],
0.39 to 0.88) for pain control; acetaminophen least efficacious: effect size 0.18
(CrI, 0.04 to 0.33).
For function, all interventions except IA corticosteroids superior to oral placebo.
For stiffness, NS differences among treatments.
Limitations: Lack of long-term data, inadequate reporting of safety data,
possible publication bias, and few head-to-head comparisons.
Bannuru (2014)
Relative efficacy of hyaluronic
acid in comparison with NSAIDs
for knee osteoarthritis: a
systematic review and meta-
analysis.
Key points:
HA v. NSAIDs for knee osteoarthritis:
RCTs, - Feb 2013;
5 trials (712 subjects);
No significant differences at 4 and 12 weeks;
No safety concerns from review but limited by short follow-up
Samson (2014) Key points:

6
Citation Content, Methods, Recommendations
Treatment of Primary and
Secondary Osteoarthritis of the
Knee.
Systematic review of outcomes of three treatments for osteoarthritis (OA) of the
knee: intra-articular viscosupplementation; oral glucosamine, chondroitin or the
combination; and arthroscopic lavage or debridement.
Included 42 RCTs of viscosupplementation, all but one synthesized among six
meta-analyses; 21 RCTs of glucosamine/chondroitin, 16 synthesized among 6
meta-analyses; and 23 articles on arthroscopy.
Viscosupplementation trials generally report positive effects on pain and
function scores compared to placebo
The evidence on clinical benefit is uncertain, due to variable trial quality,
potential publication bias, and unclear clinical significance of the changes
reported.
The best available evidence does not clearly demonstrate clinical benefit.
Schmajuk (2014)
Using Medicare Data to
Understand Low-Value Health
Care: The Case of Intra-articular
Hyaluronic Acid Injections.
Key points:
Study reviewed 1,161,924 injections with intra-articular hyaluronic acid among
423,669 patients by 12,761 physicians or other clinicians.
Most formulations of hyaluronic acid consisted of 3 injections given 1 week
apart. The average cost per injection paid by Medicare was $179 for the drug
and $69 for the injection.
An analysis by regions showed that rates of intra-articular hyaluronic acid
injections were clustered (p < .001).
Higher rates of injection of intra-articular hyaluronic acid were associated with
higher numbers of physicians, surgeons, and rheumatologists.
AAOS (2013)
Clinical practice guideline on the
treatment of osteoarthritis of the
knee.
Key points:
Knee osteoarthritis
Strong recommendation against using IAHA for patients with symptomatic knee
osteoarthritis.
Based on 14 studies (3 high-strength studies and 11 moderate-strength
studies) indicating a low likelihood that IAHA provides minimum clinically
important improvement to patients.
Chang (2013)
Effectiveness of intra-articular
hyaluronic acid for ankle
osteoarthritis treatment: a
systematic review and meta-
analysis.
Key points:
Ankle osteoarthritis:
RCTs (4); CCTs (1) or prospective cohort (4): vs. saline, exercise or
arthroscopy 345 subjects total; 1995 – 2012;
Significant reduction in pain versus before treatment;
Molecular weight of preparation not associated with magnitude of pain relief but
increases in total doses and active ingredients may be.
Increased injection volume may be associated with reduced effect;
Extremely high molecular weight preparations frequently caused early post-
injection pain;
Multiple doses and appropriate injection volume recommended.

7
Citation Content, Methods, Recommendations
Hayes (2013)
Viscosupplementation for
chondromalacia.
Key points:
Chondromalacia.
Searches — July 2013;
Mostly animal studies; very limited human clinical data;
No products are specifically FDA-approved for chondromalacia.
Hayes (2013)
Preoperative
viscosupplementation for the
treatment of knee conditions.
Key points:
Preoperative viscosupplementation for knee conditions:
Products used in included studies: Orthovisc; Synvisc; Adant; Viscoseal;
Suplasyn; Synochrom;
6 RCTs, 1 CCT: anterior cruciate ligament tear or rupture; osteoarthritis;
meniscal tear;
30 to 80 subjects/study; FU, 6 weeks to 2 years;
Heterogeneity precluded meta-analysis but “several” studies reported benefits
in pain reduction, range of motion/function, cartilage volume;
No or few significant side effects reported.
Krogh (2013)
Comparative effectiveness of
injection therapies in lateral
epicondylitis: a systematic review
and network meta-analysis of
randomized controlled trials.
Key points:
Injection therapies for lateral epicondylitis:
17 RCTs (1381 subjects);overall low risk of bias;
8 treatments assessed: glucocorticoids (10 trials); botulinum toxin (4);
autologous blood (3); PRP (2); HA (1) and prolotherapy;
Beyond 8 weeks: glucocorticoids no more effective than placebo; botulinum
toxin had marginal benefit with temporary paralysis of finger extension;
Superior to placebo: autologous blood; plasma; hyaluronic acid; and
prolotherapy but all trials subject to bias;
Additional research is needed.
Miller (2013)
Systematic Review and Meta-
Analysis of Randomized, Saline-
Controlled Trials.
Key points:
Knee osteoarthritis:
Full-text English-language RCTs — 2013: Hyalgan; Synvisc; Supartz/Artzal;
Orthovisc; Gel-One; Euflexxa were most commonly studied;
29 trials (4866 subjects); most of moderate quality although with substantial
heterogeneity;
Significant improvements in knee pain and function at 4 to 26 weeks; no
differences in safety outcomes (inconsistently reported).
Pichon-Riviere (2013)
Intra-articular use of hyaluronic
acid in the treatment of knee
osteoarthritis.
Key points:
Knee osteoarthritis.
Available evidence of high quality; .
Intra-articular injection in patients for whom non-pharmacological treatments or

8
Citation Content, Methods, Recommendations
simple analgesics were ineffective slightly reduces pain and improves mobility
vs placebo or intra-articuar corticosteroids in 3 to 6 month evaluation period.
Evidence lacking for: benefit to repeated doses or impact on joint replacement.
Most guidelines and insurers cover for knees which have not responded to
other treatments.
Trigkilidas (2013)
The effectiveness of hyaluronic
acid intra-articular injections in
managing osteoarthritic knee
pain.
Key points:
Osteoarthritic knee pain.
14 RCTS.
HA has modest effect on early-to-moderate knee OA.
Effect peaks at 6 to 8 weeks and by 6 months is doubtful.
American College of
Rheumatology (2012)
Recommendations for the use of
nonpharmacologic and
pharmacologic therapies in
osteoarthritis of the hand, hip, and
knee.
Key points:
Osteoarthritis: does not cover HA.
Rutjes (2012)
Viscosupplementation for
osteoarthritis of the knee: a
systematic review and meta-
analysis.
Key points:
Osteoarthritis of knee.
RCTs or quasi — Jan 2012.
89 moderate quality trials (12,667 subjects).
Viscosupplementation has minimal or no benefit to patients with symptomatic
OA of the knee.
Serious adverse effects argue against use.
Bannuru (2011)
Therapeutic trajectory following
intra-articular hyaluronic acid
injection in knee osteoarthritis--
meta-analysis.
Key points:
Therapeutic trajectory after injection for knee osteoarthritis.
RCTs — Mar 2010.
54 studies (7545 subjects).
HA better than placebo, peaking at 8 weeks, residual detectable effect at 24
weeks.
HA modestly effective for knee OA pain over six months from injection.
Cost-utility analyses are needed.
Coombes (2010)
Efficacy and safety of
corticosteroid injections and other
injections for management of
tendinopathy.
Key points:
Corticosteroid and other injections ( prolotherapy, glycosaminoglycan
polysulfate, proteinase, HA, PRP, botulinum toxin, NSAID) for tendinopathy
(lateral or medial epicondyle, rotator cuff, Achilles,or patellar):
RCTs without language restriction — Mar 2010.

9
Citation Content, Methods, Recommendations
41 studies (2672 subjects) .
Corticosteroids: improvements on all outcomes in short-term treatment; better
than prolotherapy or no treatment for all tendinopathies.
Non-corticosteroid injection: some improvements for some tendinopathies for
varying periods.
Challenged long-term use of corticosteroid injections as less effective than
more conservative therapies.
Additional large high-quality studies supporting subgroup analyses needed.
Hayes (2009)
Sodium hyaluronate for
osteoarthritis.
Key points:
Osteoarthritis.
Moderate to strong evidence that intra-articular injection reduces pain and
improves. function in patients who did not respond to or cannot tolerate
conservative therapy.
Magnitude of effect similar to corticosteroids.
HA may be an option when steroids fail.
Hayes rating “B”:
Single course of treatment for OA of knee with goal of improving
symptoms and function.
Conflicting results from mixed boy of evidence (efficacy and safety)
for hip OA.
Fernandez-Lopez (2005)
Efficacy and safety of hyaluronic
acid in the treatment of
osteoarthritis of the hip.
Key points:
Osteoarthritis of the hip — insufficient evidence.
Glossary
Chondromalacia — Also known as patello-femoral pain syndrome or chondromalacia patellae. A painful repetitive
trauma- or overuse-related condition, in which joint cartilage softens and breaks down, becoming unable to
perform its usual functions of cushioning and protecting opposing bones within the joint. While any joint cartilage
may be involved, the most common site is the underside of the patella (kneecap) and the individuals most
commonly affected are athletes and the elderly.
Glenohumeral — Related to the shoulder joint, which is a multiaxial synovial ball and socket joint. Involves
articulation between the glenoid fossa of the scapula (shoulder blade) and the head of the humerus (upper arm
bone). Due to the very limited interface of the humerus and scapula, it is the most mobile joint of the human body.
Lateral epicondylitis — Also known as “tennis elbow.” An idiopathic and generally self-limiting condition in which
the outer part of the elbow becomes tender. It is usually due to over-exertion, a sudden forceful pull, or incorrect
tennis technique, any of which can result in micro-or macroscopic tears to tendons in the joint.
Non-steroidal anti-inflammatory drugs (NSAIDs) — A class of drugs with both analgesic and anti-inflammatory

10
effects. They include ibuprofen (Advil®) and naproxen (Aleve®), and are available over the counter in the United
States. They are used for acute and chronic conditions involving pain and inflammation, such as osteoarthritis,
rheumatoid arthritis, low back pain, headache, and toothache. Since gastrointestinal side effects are prominent,
they should be avoided by people with dyspepsia or other existing gastrointestinal conditions, such as diarrhea or
bleeding.
Prolotherapy — Also known as proliferation or regenerative injection therapies. Involves injecting a non-
pharmacologic or inactive but irritant substance (e.g., dextrose or glycerin) into a joint or surrounding tissues to
promote healing and resolve symptoms.
Synovial joint — Bony intersection in which the ends of the articulating bones are separated by a joint cavity and
enclosed in a joint capsule containing synovial fluid.
References
Professional society guidelines/other:
American Academy of Orthopedic Surgeons (AAOS). Clinical practice guideline on the treatment of osteoarthritis of
the knee. Second edition. Rosemont (IL): American Academy of Orthopedic Surgeons. 2013.
Hayes Inc., Hayes Medical Technology Report. Preoperative viscosupplementation for the treatment of knee
conditions. Lansdale, Pa. Hayes Inc.; 2013.
Hayes Inc., Hayes Medical Technology Report. Sodium hyaluronate for osteoarthritis. Lansdale, Pa. Hayes Inc.;
2009.
Hayes Inc., Hayes Medical Technology Report. Synovisc®(hylanG-F 20) (Genzyme Corp) for arthritis of the ankle.
Lansdale, Pa. Hayes Inc.; 2009; reviewed 2011; archived as outdated July 2012.
Hayes Inc., Hayes Medical Technology Report. Viscosupplementation for chondromalacia. Lansdale, Pa. Hayes Inc.;
2013.
Hochberg MC, Altman RD, April KT, et al. American College of Rheumatology 2012 recommendations for the use of
nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis care &
research. 2012;64(4):465-474.
Michigan Quality Improvement Consortium. Medical management of adults with osteoarthritis. Southfield (MI);
Michigan Quality Improvement Consortium. 2013.
Pichon-Riviere A, Augustovski F, Garcia Marti S, et al. Intra-articular use of hyaluronic acid in the treatment of knee
osteoarthritis. Institute for Clinical Effectiveness and Health Policy (IECS) Report No.305. Buenos Aires; IECS. 2013.
Samson DJ, Grant MD, Ratko TA, Bonnell CJ, Ziegler KM, Aronson N. Treatment of Primary
and Secondary Osteoarthritis of the Knee. Evidence Report/Technology Assessment No. 157
(Prepared by Blue Cross and Blue Shield Association Technology Evaluation Center Evidencebased

11
Practice Center under Contract No. 290-02-0026). AHRQ Publication No. 07-E012. Rockville, MD: Agency for
Healthcare Research and Quality. 2007.
Peer-reviewed references:
Askari A, Gholami T, NaghiZadeh MM, Farjam M, Kouhpayeh SA, Shahabfard Z. Hyaluronic acid compared with
corticosteroid injections for the treatment of osteoarthritis of the knee: a randomized control trail. SpringerPlus.
2016;5:442.
Bannuru RR, Natov NS, Dasi UR, Schmid CH, McAlindon TE. Therapeutic trajectory following intra-articular
hyaluronic acid injection in knee osteoarthritis--meta-analysis. Osteoarthritis and cartilage / OARS, Osteoarthritis
Research Society. 2011;19(6):611-619.
Bannuru RR, Vaysbrot EE, Sullivan MC, McAlindon TE. Relative efficacy of hyaluronic acid in comparison with
NSAIDs for knee osteoarthritis: a systematic review and meta-analysis. Seminars in arthritis and rheumatism.
2014;43(5):593-599.
Brander VA, Stadler TS. Functional improvement with hylan G-F 20 in patients with knee osteoarthritis. The
Physician and sportsmedicine. 2009;37(3):38-48.
Chang KV, Hsiao MY, Chen WS, Wang TG, Chien KL. Effectiveness of intra-articular hyaluronic acid for ankle
osteoarthritis treatment: a systematic review and meta-analysis. Archives of physical medicine and rehabilitation.
2013;94(5):951-960.
Cianflocco AJ. Viscosupplementation in patients with osteoarthritis of the knee. Postgraduate medicine.
2013;125(1):97-105.
Chandrasekaran S, Lodhia P, Suarez-Ahedo C, Vemula SP, Martin TJ, Domb BG. Symposium: evidence for the use of
intra-articular cortisone or hyaluronic acid injection in the hip. Journal of Hip Preservation Surgery. 2016;3(1):5-15.
Coombes BK, Bisset L, Vicenzino B. Efficacy and safety of corticosteroid injections and other injections for
management of tendinopathy: a systematic review of randomised controlled trials. Lancet. 20
2010;376(9754):1751-1767.
Fernandez-Lopez JC, Ruano-Ravina A. Efficacy and safety of hyaluronic acid in the treatment of osteoarthritis of the
hip. Santiago de Campostela: Galician Agency for Health Technology Assessment (AVALIA-T); 2005.
Henrotin Y, Hauzeur JP, Bruel P, Appelboom T. Intra-articular use of a medical device composed of hyaluronic acid
and chondroitin sulfate (Structovial CS): effects on clinical, ultrasonographic and biological parameters. BMC
research notes. 2012;5:407.
Hochberg MC, Altman RD, April KT, et al. American College of Rheumatology 2012 recommendations for the use of
nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis care &
research. 2012;64(4):465-474.
Iannitti T, Lodi D, Palmieri B. Intra-articular injections for the treatment of osteoarthritis: focus on the clinical use

12
of hyaluronic acid. Drugs in R&D. 2011;11(1):13-27.
Krogh TP, Bartels EM, Ellingsen T, et al. Comparative effectiveness of injection therapies in lateral epicondylitis: a
systematic review and network meta-analysis of randomized controlled trials. The American journal of sports
medicine. 2013;41(6):1435-1446.
Miller LE, Block JE. US-Approved Intra-Articular Hyaluronic Acid Injections are Safe and Effective in Patients with
Knee Osteoarthritis: Systematic Review and Meta-Analysis of Randomized, Saline-Controlled Trials. Clinical
medicine insights. Arthritis and musculoskeletal disorders. 2013;6:57-63.
Rutjes AW, Juni P, da Costa BR, Trelle S, Nuesch E, Reichenbach S. Viscosupplementation for osteoarthritis of the
knee: a systematic review and meta-analysis. Annals of internal medicine. 7 2012;157(3):180-191.
Schmajuk G, Bozic KJ, Yazdany J. Using Medicare Data to Understand Low-Value Health Care: The Case of Intra-
articular Hyaluronic Acid Injections. JAMA Intern Med. 2014;174(10):1702-1704.
Strand V, Lim S, Takamura J. Evidence for safety of retreatment with a single intra-articular injection of Gel-200 for
treatment of osteoarthritis of the knee from the double-blind pivotal and open-label retreatment clinical trials.
BMC Musculoskeletal Disorders. 2016;17:240.
Trigkilidas D, Anand A. The effectiveness of hyaluronic acid intra-articular injections in managing osteoarthritic
knee pain. Annals of the Royal College of Surgeons of England. 2013;95(8):545-551.
Clinical trials
Searched ClinicalTrials.gov on June 28, 2016 using terms: Open Studies | hyaluronic acid. Nineteen studies found; 5
relevant.
NuCel, LLC. An Investigation of ReNu™ Knee Injection in Patients With Osteoarthritis. ClinicalTrials.gov Web site.
http://clinicaltrials.gov/show/NCT02318511. Published December 9, 2014. Updated November 2015. Accessed
June 28, 2016.
University of California, San Francisco. To Look at the Characteristics of Synovial Fluid and Cartilage Matrix in
Osteoarthritic Knee After Hyaluronic Acid Injection. ClinicalTrials.gov Web site.
http://clinicaltrials.gov/show/NCT01895959. Published July 5, 2013. Updated September 2015. Accessed June 28,
2016.
New York University School of Medicine. Effectiveness Trial for Evaluating IAHA for PFPS (PFPS). ClinicalTrials.gov
Web site. http://clinicaltrials.gov/show/NCT02318511. Published February 15, 2013. Updated April 2016. Accessed
June 28, 2016.
Laval University. Daily Activity and Gait Analysis After Viscosupplement Injection Among Hip Osteoarthritis
Patients. ClinicalTrials.gov Web site. http://clinicaltrials.gov/show/NCT02086474. Published March 7, 2014.
Updated March 2016. Accessed June 28, 2016.
ProCore Ltd. A Phase I, Prospective, Randomized, Open-label, Active-Controlled Clinical Trial for Safety Evaluation

13
of Intra-articular Injection of RegenoGel-SP for the Treatment of Moderate to Severe Osteoarthritis.
ClinicalTrials.gov Web site. https://ClinicalTrials.gov/show/NCT02188771. Published July 10, 2014. Updated July
2014. Accessed June 28, 2016.
Centers for Medicare & Medicaid Services (CMS) national coverage determinations (NCDs).
No NCDs found at this time.
Local coverage determinations (LCDs)
Hyaluronan acid therapies for osteoarthritis of the knee (L32237). Available at: http://www.cms.gov/medicare-
coverage-database/details/lcd-
details.aspx?LCDId=32237&ContrId=314&ver=24&ContrVer=1&SearchType=Advanced&CoverageSelection=Both&
NCSelection=NCD&PolicyType=Final&s=All&KeyWord=Hyaluronan&KeyWordLookUp=Title&KeyWordSearchType=
Exact&kq=true&bc=IAAAABAAAAAAAA%3d%3d&. Accessed June 28, 2015.
Intra-articular Injections of hyaluronan (L30149). Available at: http://www.cms.gov/medicare-coverage-
database/details/lcd-
details.aspx?LCDId=30149&ContrId=143&ver=39&ContrVer=1&SearchType=Advanced&CoverageSelection=Both&
NCSelection=NCD&PolicyType=Final&s=All&KeyWord=Hyaluronan&KeyWordLookUp=Title&KeyWordSearchType=
Exact&kq=true&bc=IAAAABAAAAAAAA%3d%3d&. Accessed June 28, 2015.
Commonly submitted codes
Below are the most commonly submitted codes for the service(s)/item(s) subject to this policy. This is not an
exhaustive list of codes. Providers are expected to consult the appropriate coding manuals and bill accordingly.
CPT Code Description Comment
20610 Arthrocentesis, aspiration and/or injection; major joint or bursa (eg, shoulder,
hip, knee, subacromial bursa); without ultrasound guidance
20611 Arthrocentesis, aspiration and/or injection; major joint or bursa (eg, shoulder,
hip, knee, subacromial bursa); without ultrasound guidance
ICD-10 Code Description Comment
M17.0 Bilateral primary osteoarthritis of knee
M17.10 Unilateral primary osteoarthritis, unspecified knee
M17.11 Unilateral primary osteoarthritis, right knee
M17.12 Unilateral primary osteoarthritis, left knee
M17.2 Bilateral post-traumatic osteoarthritis of knee

14
ICD-10 Code Description Comment
M17.30 Unilateral post-traumatic osteoarthritis, unspecified knee
M17.31 Unilateral post-traumatic osteoarthritis, right knee
M17.32 Unilateral post-traumatic osteoarthritis, left knee
M17.4 Other bilateral secondary osteoarthritis of knee
M17.5 Other unilateral secondary osteoarthritis of knee
M17.9 Osteoarthritis of knee, unspecified
HCPCS Level
II Description Comment
J7321 Hyaluronan or derivative:(Hylgan or Supartz) for intra-articular injection.
J7323 Hyaluronan or derivative: (Euflexxa)for intra-articular injection.
J7324 Hyaluronan or derivative: (Orthovisc) for intra-articular injection.
J7325 Hyaluronan or derivative: (ynvisc or SynviscOne) for intra-articular injection.
J7326 Hyaluronan or derivative: (Gel-One) for intra-articular injection.
APPENDIX A
PerformRx criteria:
Field Name Field Description
Prior Authorization Group HYALURONIC ACID DERIVATIVES.
Drug(s) EUFLEXXA is PREFERRED agent.
Gel-One
Hyalgan
Monovisc
Orthovisc
Supartz
Covered Uses *Medically accepted indications are defined using the following sources: the Food
and Drug Administration (FDA), Micromedex, American Hospital Formulary
Service (AHFS), United States Pharmacopeia Drug Information for the
Healthcare
Professional (USP DI), or the Drug Package Insert (PPI).
Exclusion Criteria None.
Required Medical Information See other criteria.
Age Restrictions None.
Prescriber Restrictions None.
Coverage Duration If all of the criteria is met, the request will be approved for one complete course
15
Field Name Field Description
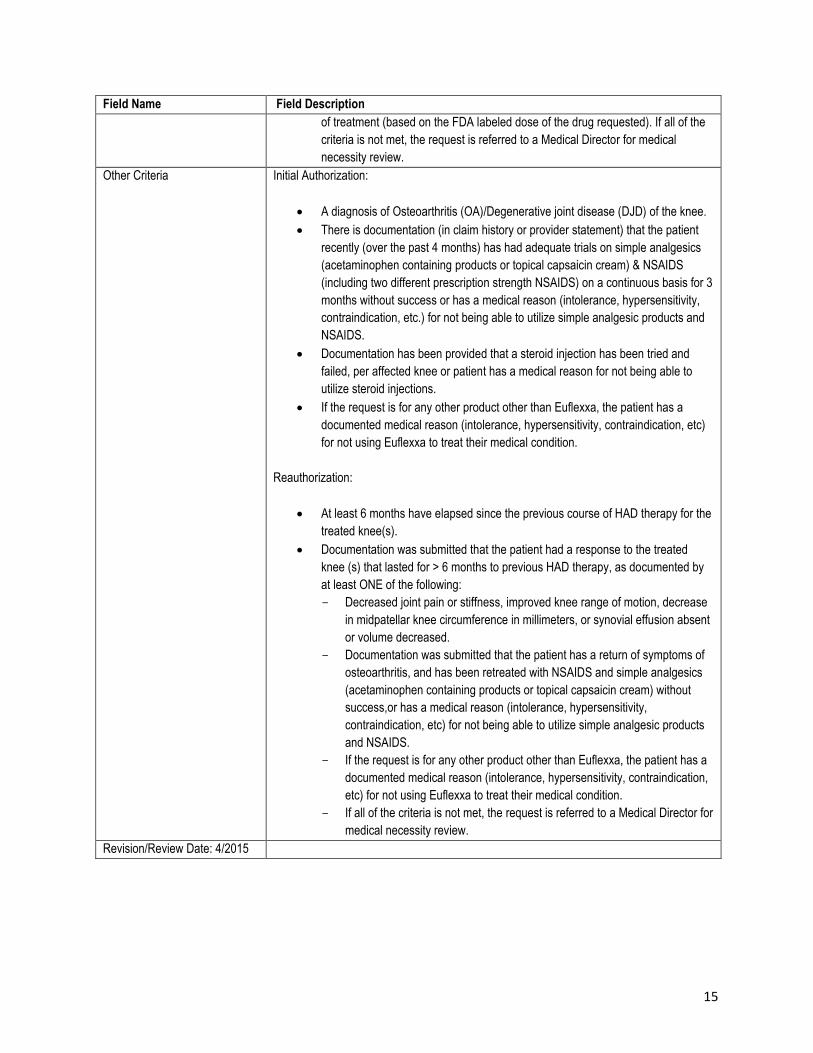
of treatment (based on the FDA labeled dose of the drug requested). If all of the
criteria is not met, the request is referred to a Medical Director for medical
necessity review.
Other Criteria Initial Authorization:
A diagnosis of Osteoarthritis (OA)/Degenerative joint disease (DJD) of the knee.
There is documentation (in claim history or provider statement) that the patient
recently (over the past 4 months) has had adequate trials on simple analgesics
(acetaminophen containing products or topical capsaicin cream) & NSAIDS
(including two different prescription strength NSAIDS) on a continuous basis for 3
months without success or has a medical reason (intolerance, hypersensitivity,
contraindication, etc.) for not being able to utilize simple analgesic products and
NSAIDS.
Documentation has been provided that a steroid injection has been tried and
failed, per affected knee or patient has a medical reason for not being able to
utilize steroid injections.
If the request is for any other product other than Euflexxa, the patient has a
documented medical reason (intolerance, hypersensitivity, contraindication, etc)
for not using Euflexxa to treat their medical condition.
Reauthorization:
At least 6 months have elapsed since the previous course of HAD therapy for the
treated knee(s).
Documentation was submitted that the patient had a response to the treated
knee (s) that lasted for > 6 months to previous HAD therapy, as documented by
at least ONE of the following:
Decreased joint pain or stiffness, improved knee range of motion, decrease
in midpatellar knee circumference in millimeters, or synovial effusion absent
or volume decreased.
Documentation was submitted that the patient has a return of symptoms of
osteoarthritis, and has been retreated with NSAIDS and simple analgesics
(acetaminophen containing products or topical capsaicin cream) without
success,or has a medical reason (intolerance, hypersensitivity,
contraindication, etc) for not being able to utilize simple analgesic products
and NSAIDS.
If the request is for any other product other than Euflexxa, the patient has a
documented medical reason (intolerance, hypersensitivity, contraindication,
etc) for not using Euflexxa to treat their medical condition.
If all of the criteria is not met, the request is referred to a Medical Director for
medical necessity review.
Revision/Review Date: 4/2015


















