Clinical Policy Title: Genetic testing for rare diseases · Clinical Policy Title: Genetic testing...
18
1 Clinical Policy Title: Genetic testing for rare diseases Clinical Policy Number: 02.01.09 Effective Date: January 1, 2016 Initial Review Date: October 16, 2013 Most Recent Review Date: October 19, 2016 Next Review Date: October 2017 Related policies: CP# 02.01.01 Maternal genetic testing CP# 02.01.02 Genetic testing for breast and ovarian cancer CP# 02.01.03 Array comparative genomic hybridization testing CP# 02.01.13 Pharmacogenetic testing for warfarin CP# 02.01.07 Genetic testing for cystic fibrosis CP# 02.01.08 Familial polyposis gene testing CP# 02.01.10 Colaris test for Lynch syndrome CP# 02.01.11 Afirma gene expression classifier for indeterminate thyroid nodules CP# 02.01.12 Corus coronary artery disease (CAD) for genomic expression CP# 02.01.14 Gene expression profile testing for breast cancer CP# 05.01.04 Molecular analysis for targeted therapy of non-small cell lung cancer ABOUT THIS POLICY: Keystone First has developed clinical policies to assist with making coverage determinations. Keystone First’s clinical policies are based on guidelines from established industry sources, such as the Centers for Medicare & Medicaid Services (CMS), state regulatory agencies, the American Medical Association (AMA), medical specialty professional societies, and peer-reviewed professional literature. These clinical policies along with other sources, such as plan benefits and state and federal laws and regulatory requirements, including any state- or plan-specific definition of “medically necessary,” and the specific facts of the particular situation are considered by Keystone First when making coverage determinations. In the event of conflict between this clinical policy and plan benefits and/or state or federal laws and/or regulatory requirements, the plan benefits and/or state and federal laws and/or regulatory requirements shall control. Keystone First’s clinical policies are for informational purposes only and not intended as medical advice or to direct treatment. Physicians and other health care providers are solely responsible for the treatment decisions for their patients. Keystone First’s clinical policies are reflective of evidence-based medicine at the time of review. As medical science evolves, Keystone First will update its clinical policies as necessary. Keystone First’s clinical policies are not guarantees of payment. Coverage policy Keystone First considers the once-per-lifetime use of genetic testing for rare disease to be clinically proven and, therefore, medically necessary when the following criteria are met: Policy contains: Inherited breast, ovarian, colorectal cancers. Cardiomyopathies, channelopathies.
Transcript of Clinical Policy Title: Genetic testing for rare diseases · Clinical Policy Title: Genetic testing...

1
Clinical Policy Title: Genetic testing for rare diseases
Clinical Policy Number: 02.01.09
Effective Date: January 1, 2016
Initial Review Date: October 16, 2013
Most Recent Review Date: October 19, 2016
Next Review Date: October 2017
Related policies:
CP# 02.01.01 Maternal genetic testing
CP# 02.01.02 Genetic testing for breast and ovarian cancer
CP# 02.01.03 Array comparative genomic hybridization testing
CP# 02.01.13 Pharmacogenetic testing for warfarin
CP# 02.01.07 Genetic testing for cystic fibrosis
CP# 02.01.08 Familial polyposis gene testing
CP# 02.01.10 Colaris test for Lynch syndrome
CP# 02.01.11 Afirma gene expression classifier for indeterminate thyroid nodules
CP# 02.01.12 Corus coronary artery disease (CAD) for genomic expression
CP# 02.01.14 Gene expression profile testing for breast cancer
CP# 05.01.04 Molecular analysis for targeted therapy of non-small cell lung cancer
ABOUT THIS POLICY: Keystone First has developed clinical policies to assist with making coverage determinations. Keystone First’s clinical policies are based on guidelines from established industry sources, such as the Centers for Medicare & Medicaid Services (CMS), state regulatory agencies, the American Medical Association (AMA), medical specialty professional societies, and peer-reviewed professional literature. These clinical policies along with other sources, such as plan benefits and state and federal laws and regulatory requirements, including any state- or plan-specific definition of “medically necessary,” and the specific facts of the particular situation are considered by Keystone First when making coverage determinations. In the event of conflict between this clinical policy and plan benefits and/or state or federal laws and/or regulatory requirements, the plan benefits and/or state and federal laws and/or regulatory requirements shall control. Keystone First’s clinical policies are for informational purposes only and not intended as medical advice or to direct treatment. Physicians and other health care providers are solely responsible for the treatment decisions for their patients. Keystone First’s clinical policies are reflective of evidence-based medicine at the time of review. As medical science evolves, Keystone First will update its clinical policies as necessary. Keystone First’s clinical policies are not guarantees of payment.
Coverage policy
Keystone First considers the once-per-lifetime use of genetic testing for rare disease to be clinically
proven and, therefore, medically necessary when the following criteria are met:
Policy contains:
Inherited breast, ovarian, colorectal
cancers.
Cardiomyopathies, channelopathies.

1
The test results will directly impact management (i.e., as a result of the test, effective
treatment may be offered that will alter the course of disease or outcomes).
The test is an analytically and clinically valid test (i.e., supported by peer-reviewed published
research).
The test results will be discussed with the patient or guardian (including the limitations of
the testing method, the risks and benefits of either continuing or stopping the therapy
based on the test, and current cancer management guidelines).
There is a care-coordinating, multidisciplinary team available for genetic and behavioral
counseling for a tiered evaluation, which includes (a.) a primary care provider and (b.) a
geneticist (who is a physician or a licensed genetic counselor). If access to a genetic
counselor or medical geneticist is not possible, genetic counseling may be initiated by a
physician with relevant genetic expertise.
The patient or guardian has a desire for engagement with the integrated multidisciplinary
team that is documented in the clinical record.
Consideration has been given to standard diagnostic evaluation and use of tiered panel or
targeted test sequence for minimal number of genes to establish the diagnosis.
The genetic test includes, but is not limited to, testing for any of the disorders listed below
where there is a family history or defined high risk:
Huntington’s disease.
HFE-associated hemochromatosis.
Heritable cancers — breast, ovarian, colorectal, or myeloproliferative.
Cardiomyopathy.
Channelopathy.
Hemoglobinopathy — sickle cell or thalassemia.
Hemophilia.
Duchenne muscular dystrophy.
Mitochondrial disease.
Chondrodystrophy.
Fragile X.
Down syndrome.
Limitations:
All other uses of once-per-lifetime genetic testing for rare disease are not medically necessary.
Note: The following CPT/HCPCS codes are not listed in the Pennsylvania Medicaid fee schedule:
81265 - Comparative analysis using Short Tandem Repeat (STR) markers: patient and comparative
specimen (e.g., pre-transplant recipient and donor germline testing, post transplant non-hematopoietic
recipient germline and donor testing, twin zygosity testing or maternal cell contamination of fetal cells.
2
81401 - HTT (huntingtin) (eg, Huntington disease), evaluation to detect abnormal (eg, expanded) alleles
81479 - Unlisted molecular pathology procedure.
Alternative covered services:
Laboratory evaluation with karyotyping, fluorescence in situ hybridization (FISH) assay.
Clinical evaluation by an appropriately trained in-network provider and standard laboratory
testing.
Background
Genetic testing for mutations in the human chromosome is used to determine whether an individual has
an increased risk for disease, including cancer, and in many cases to establish with certainty the medical
diagnosis (e.g., persons at high risk of inherited illness but whose genotype by traditional investigative
methods is inconclusive). Children who inherit mutations are at increased risk of congenital disorders,
treatable illnesses, and early onset of cancers, and carry these proclivities into adulthood. Adults with
genetic code derangements can be predictably counseled regarding risk and causes of morbidity and
mortality.
Genetic testing (or genomic testing as it is sometimes called) includes a variety of laboratory tests
(analysis of deoxyribonucleic acid [DNA], ribonucleic acid [RNA], and genes or gene products) performed
to diagnose disease, assist in treatment decisions, predict future disease, identify carriers of disease, and
conduct prenatal testing.
Searches
Keystone First searched PubMed and the databases of:
UK National Health Services Center for Reviews and Dissemination.
Agency for Healthcare Research and Quality’s National Guideline Clearinghouse and other
evidence-based practice centers.
The Centers for Medicare & Medicaid Services (CMS).
We conducted searches on October 4, 2016. Search terms were: "genetic testing (MeSH)," "genomic
tests (MeSH)," and "rare diseases (MeSH)."
We included:
Systematic reviews, which pool results from multiple studies to achieve larger sample sizes and
greater precision of effect estimation than in smaller primary studies. Systematic reviews use
predetermined transparent methods to minimize bias, effectively treating the review as a
scientific endeavor, and are thus rated highest in evidence-grading hierarchies.

3
Guidelines based on systematic reviews.
Economic analyses, such as cost-effectiveness, and benefit or utility studies (but not simple cost
studies), reporting both costs and outcomes — sometimes referred to as efficiency studies —
which also rank near the top of evidence hierarchies.
Findings
There is a great deal of evidence regarding genetic testing for diagnosis, but the vast majority of it has
been done in the closed cohort of risk-dense individuals (infants, children, and adults) in whom the
presumptive diagnosis has been made but not confirmed by karyotype or other laboratory assessment.
As such, the evidence can lead to an overestimate of risk attributable entirely due to the high
concentration of mutations in this group of people. Moreover, there are doubtless mutations that lead
to disease that have yet to be discovered or imagined, leading to the potential of false-negative results
due to undetected mutations.
Evidence regarding the impact of genetic testing on clinical decision-making is limited, although the
available data suggest that a positive genetic test can induce people to participate in surveillance
programs or to elect a primary prevention strategy (such as surgery or chemoprevention). In addition,
even those with negative tests may benefit from a higher level of understanding and awareness of
disease for which they face risk, leading to earlier diagnosis and greater survival.
Policy updates:
Okazaki (2016) studied next-generation sequencing (NGS) using the TruSight® one gene panel for the
diagnosis of Mendelian disorders in 17 families and 20 patients. The authors detected causative
mutations in six (35 percent) of 17 families. In particular, 11 (65 percent) of the families had syndromic
diagnosis and six (35 percent) had no syndromic diagnosis before NGS testing. The number of positive
diagnoses was five (45 percent) of 11 in the syndromic group and one (17 percent) of six among patients
of the no syndromic diagnosis group. Diagnostic yields were higher than in previous reports of whole
exome sequencing (WES).
Daoud (2016) conducted a pilot project in which the authors assessed the feasibility of NGS as a tool to
improve the diagnosis of rare diseases in newborns in the neonatal intensive care unit (NICU). Subjects
were retrospectively identified and newborns and infants prospectively recruited. Blood samples were
evaluated using the MiSeq® sequencing platform. Of 20 newborns studied, eight received a diagnosis on
the basis of NGS (40 percent) as varied as renal tubular dysgenesis, SCN1A-related encephalopathy
syndrome, myotubular myopathy, FTO deficiency syndrome, cranioectodermal dysplasia, congenital
myasthenic syndrome, autosomal dominant intellectual disability syndrome type 7, and Denys-Drash
syndrome.
NGS offers an opportunity to locate mutations associated with genetic and infectious diseases, as well as
tumorigenesis. Carrigan (2016) presented results from the Target 5000 project, a NGS study aimed at

4
identifying causative mutations in inherited retinal degenerations (IRDs). DNA samples were sequenced
using a capture panel consisting of all coding exons for genes previously implicated in retinopathies.
Candidate mutations were identified in 57 percent of pedigrees, many of which were novel and
previously unreported mutations identified in the IRD cohort, as were new ocular disease phenotypes
associated with genes previously implicated in other retinal disorders.
Pellicani (2016) reviewed the main clinical effects of ion channel mutations associated with migraine
headaches and presented convincing evidence of an increasing and evolving use of genetic analysis in
migraine research. The authors also showed how novel information in rare monogenic forms of migraine
might help to clarify the disease mechanisms in the general population of migraineurs.
Simeoni (2016) studied inherited bleeding, thrombotic, and platelet disorders (BPDs) with a high-
throughput sequencing platform targeting 63 genes relevant for BPDs. The platform identified single-
nucleotide variants, short insertions and deletions, and large copy number variants (though not
inversions), resulting in an average of 5.34 candidate variants per individual. The authors sequenced 159
and 137 samples, respectively, from cases with and without previously known causal variants. Among
the latter group, 61 cases had clinical and laboratory phenotypes indicative of a particular molecular
etiology, whereas the remainder had an uncertain etiology. A molecular diagnosis was reached in 56 of
61 and eight of 76 cases, respectively.
Pangalos (2016) reported an expanded exome sequencing-based test, coupled to a bioinformatics-
driven prioritization algorithm, targeting gene disorders presenting with abnormal prenatal ultrasound
findings. The authors applied the testing strategy to14 euploid fetuses, from 11 ongoing pregnancies
and three products of abortion, all with various abnormalities or malformations detected through
prenatal ultrasound examination. WES was followed by variant prioritization, utilizing a custom Fetalis
algorithm targeting 758 genes associated with genetic disorders. A definitive or highly likely diagnosis
was made in six of 14 cases (43 percent), among them Ellis-van Creveld syndrome, Ehlers-Danlos
syndrome and Nemaline myopathy, citrullinemia, Noonan syndrome, and PROKR2-related Kallmann
syndrome. In eight ongoing pregnancy cases, a ZIC1 variant of unknown clinical significance was
detected in one case, while in seven cases testing did not reveal any pathogenic variants. The authors
concluded the expanded targeted exome sequencing-based approach provided strong evidence of a
definite and beneficial increase in prenatal diagnosis.
A contemporary review (Hussein, 2015) sought evidence of efficacy of pre-conception testing for
thalassemia, sickle cell disease, cystic fibrosis, and Tay-Sachs disease in couples at genetic risk of the
conditions before pregnancy. The available evidence (mostly nonrandomized studies of limited power)
was insufficient to make a recommendation regarding the practice.
A study of the efficacy of screening the newborn population with genetic testing for homocysteinuria
failed to identify sufficient evidence to support a variance from the routine chemical testing (i.e., serum
methionine) that is now a legally mandated standard practice nationwide.

5
Summary of clinical evidence:
Citation Content, Methods, Recommendations
Okazaki (2016) Clinical Diagnosis of Mendelian Disorders Using a Comprehensive Gene-Targeted Panel Test for Next-Generation Sequencing
Key points:
NGS using the TruSight one gene panel for the diagnosis of Mendelian disorders in 17 families and 20 patients was evaluated.
The authors detected causative mutations in six (35 percent) of 17 families.
In particular, 11 (65 percent) of the families had syndromic diagnosis and six (35 percent) had no syndromic diagnosis before NGS testing.
The number of positive diagnoses was five (45 percent) of 11 in the syndromic group and one (17 percent) of six among patients in the non-syndromic diagnosis group.
Diagnostic yields were higher than in previous reports of WES.
Daoud (2016) Next-generation sequencing for diagnosis of rare diseases in the neonatal intensive care unit
Key points:
Pilot project assessed the feasibility of NGS as a tool to improve the diagnosis of rare diseases in newborns in the NICU.
Subjects were retrospectively identified and newborns and infants prospectively recruited.
Blood samples were evaluated using the MiSeq sequencing platform.
Of 20 newborns studied, eight received a diagnosis on the basis of NGS (40 percent) as varied as renal tubular dysgenesis, SCN1A-related encephalopathy syndrome, myotubular myopathy, FTO deficiency syndrome, cranioectodermal dysplasia, congenital myasthenic syndrome, autosomal dominant intellectual disability syndrome type 7, and Denys-Drash syndrome.
Carrigan (2016) Panel-Based Population Next-Generation Sequencing for Inherited Retinal Degenerations.
Key points:
Narrative review presented results from the Target 5000 project, an NGS study of causative mutations in IRDs.
DNA samples were sequenced using a capture panel consisting of all coding exons for genes previously implicated in retinopathies.
Candidate mutations were identified in 57 percent of pedigrees, many of which were novel and previously unreported mutations identified in the IRD cohort, as were new ocular disease phenotypes associated with genes previously implicated in other retinal disorders.
Pellacani (2016) The Revolution in Migraine Genetics: From Aching Channels Disorders to a Next-Generation Medicine
Key points:
Narrative review of the effects of ion channel mutations associated with migraine headaches.
Presented convincing evidence of an increasing and evolving use of genetic analysis in migraine research.
The authors also showed how novel information in rare monogenic forms of migraine might help to clarify the disease mechanisms in the general population of migraineurs.

6
Simeoni (2016) A high-throughput sequencing test for diagnosing inherited bleeding, thrombotic, and platelet disorders
Key points:
Project studied inherited BPDs with a high-throughput sequencing platform.
The platform identified single-nucleotide variants, short insertions and deletions, and large copy number variants (though not inversions), resulting in an average of 5.34 candidate variants per individual.
The authors sequenced 159 and 137 samples, respectively, from cases with and without previously known causal variants.
Among the latter group, 61 cases had clinical and laboratory phenotypes indicative of a particular molecular etiology, whereas the remainder had an uncertain etiology.
A molecular diagnosis was reached in 56 of 61 and eight of 76 cases, respectively.
Pangalos (2016) First applications of a targeted exome sequencing approach in fetuses with ultrasound abnormalities reveals an important fraction of cases with associated gene defects
Key points:
Reported an expanded exome sequencing-based test, coupled to a bioinformatics-driven prioritization algorithm.
The authors applied the testing strategy to14 euploid fetuses, from 11 ongoing pregnancies and three products of abortion.
WES was followed by variant prioritization, utilizing a custom Fetalis algorithm targeting 758 genes associated with genetic disorders.
A definitive or highly likely diagnosis was made in six of 14 cases (43 percent), among them Ellis-van Creveld syndrome, Ehlers-Danlos syndrome and Nemaline myopathy, citrullinemia, Noonan syndrome, and PROKR2-related Kallmann syndrome.
In eight ongoing pregnancy cases, a ZIC1 variant of unknown clinical significance was detected in one case, while in seven cases testing did not reveal any pathogenic variants.
The authors concluded the expanded targeted exome sequencing-based approach provided strong evidence of a definite and beneficial increase in prenatal diagnosis.
Hussein (2015) Preconception risk assessment for thalassemia, sickle cell disease, cystic fibrosis, and Tay-Sachs disease
Key points:
Systematic review of 13 randomized controlled trials (RCTs) looked for evidence of efficacy of pre-conception testing for thalassemia, sickle cell disease, cystic fibrosis, and Tay-Sachs disease in couples at genetic risk of the conditions before pregnancy.
Authors concluded the research evidence for policy recommendations is limited to nonrandomized studies.
Further evaluation from additional controlled studies is needed before definitive statements of clinical efficacy can be made about pre-conception testing.
Walters (2015) Newborn screening for homocystinuria
Key points:
Searched for evidence indicating newborn population screening with genetic tests for homocysteinuria can prevent or reduce the severity of disease.
No studies were identified for inclusion in the review.
The authors were unable to draw any conclusions based on controlled studies and deferred recommendation for its routine clinical practice.
Berardelli (2013) EFNS/MDS-ES recommendations for the diagnosis of Parkinson’s disease
Key points:
Concluded that the diagnosis of Parkinsonism is still largely based on the correct identification of its clinical features.
Genetic testing recommended for the diagnosis of Parkinsonism on an individual basis.
Family history and age of onset were determined to be key indicators of likelihood of disease.
7
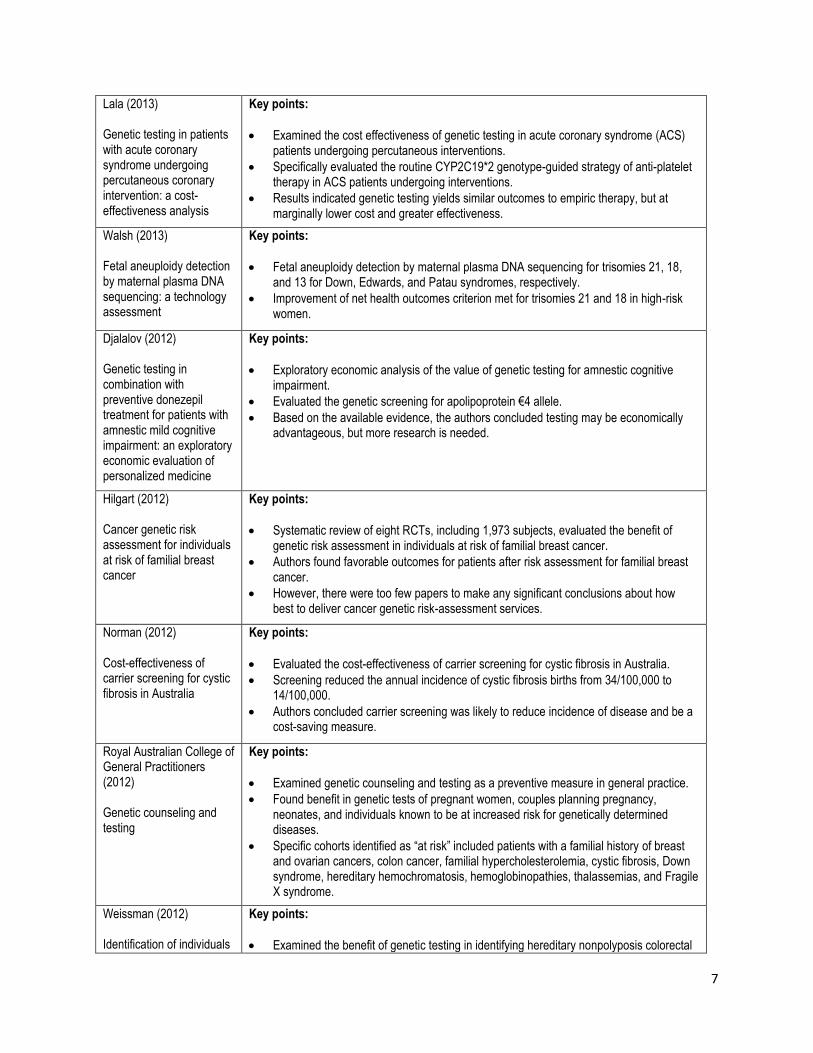
Lala (2013) Genetic testing in patients with acute coronary syndrome undergoing percutaneous coronary intervention: a cost-effectiveness analysis
Key points:
Examined the cost effectiveness of genetic testing in acute coronary syndrome (ACS) patients undergoing percutaneous interventions.
Specifically evaluated the routine CYP2C19*2 genotype-guided strategy of anti-platelet therapy in ACS patients undergoing interventions.
Results indicated genetic testing yields similar outcomes to empiric therapy, but at marginally lower cost and greater effectiveness.
Walsh (2013) Fetal aneuploidy detection by maternal plasma DNA sequencing: a technology assessment
Key points:
Fetal aneuploidy detection by maternal plasma DNA sequencing for trisomies 21, 18, and 13 for Down, Edwards, and Patau syndromes, respectively.
Improvement of net health outcomes criterion met for trisomies 21 and 18 in high-risk women.
Djalalov (2012) Genetic testing in combination with preventive donezepil treatment for patients with amnestic mild cognitive impairment: an exploratory economic evaluation of personalized medicine
Key points:
Exploratory economic analysis of the value of genetic testing for amnestic cognitive impairment.
Evaluated the genetic screening for apolipoprotein €4 allele.
Based on the available evidence, the authors concluded testing may be economically advantageous, but more research is needed.
Hilgart (2012) Cancer genetic risk assessment for individuals at risk of familial breast cancer
Key points:
Systematic review of eight RCTs, including 1,973 subjects, evaluated the benefit of genetic risk assessment in individuals at risk of familial breast cancer.
Authors found favorable outcomes for patients after risk assessment for familial breast cancer.
However, there were too few papers to make any significant conclusions about how best to deliver cancer genetic risk-assessment services.
Norman (2012) Cost-effectiveness of carrier screening for cystic fibrosis in Australia
Key points:
Evaluated the cost-effectiveness of carrier screening for cystic fibrosis in Australia.
Screening reduced the annual incidence of cystic fibrosis births from 34/100,000 to 14/100,000.
Authors concluded carrier screening was likely to reduce incidence of disease and be a cost-saving measure.
Royal Australian College of General Practitioners (2012) Genetic counseling and testing
Key points:
Examined genetic counseling and testing as a preventive measure in general practice.
Found benefit in genetic tests of pregnant women, couples planning pregnancy, neonates, and individuals known to be at increased risk for genetically determined diseases.
Specific cohorts identified as “at risk” included patients with a familial history of breast and ovarian cancers, colon cancer, familial hypercholesterolemia, cystic fibrosis, Down syndrome, hereditary hemochromatosis, hemoglobinopathies, thalassemias, and Fragile X syndrome.
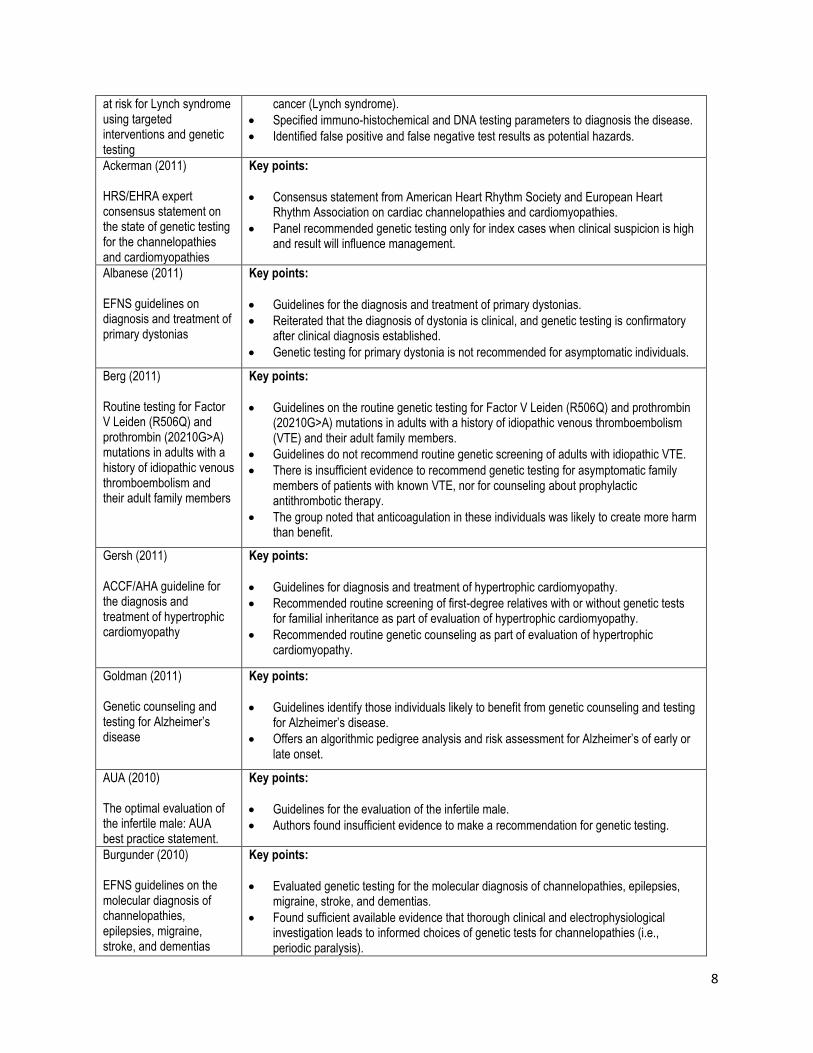
Weissman (2012) Identification of individuals
Key points:
Examined the benefit of genetic testing in identifying hereditary nonpolyposis colorectal
8
at risk for Lynch syndrome using targeted interventions and genetic testing
cancer (Lynch syndrome).
Specified immuno-histochemical and DNA testing parameters to diagnosis the disease.
Identified false positive and false negative test results as potential hazards.
Ackerman (2011) HRS/EHRA expert consensus statement on the state of genetic testing for the channelopathies and cardiomyopathies
Key points:
Consensus statement from American Heart Rhythm Society and European Heart Rhythm Association on cardiac channelopathies and cardiomyopathies.
Panel recommended genetic testing only for index cases when clinical suspicion is high and result will influence management.
Albanese (2011) EFNS guidelines on diagnosis and treatment of primary dystonias
Key points:
Guidelines for the diagnosis and treatment of primary dystonias.
Reiterated that the diagnosis of dystonia is clinical, and genetic testing is confirmatory after clinical diagnosis established.
Genetic testing for primary dystonia is not recommended for asymptomatic individuals.
Berg (2011) Routine testing for Factor V Leiden (R506Q) and prothrombin (20210G>A) mutations in adults with a history of idiopathic venous thromboembolism and their adult family members
Key points:
Guidelines on the routine genetic testing for Factor V Leiden (R506Q) and prothrombin (20210G>A) mutations in adults with a history of idiopathic venous thromboembolism (VTE) and their adult family members.
Guidelines do not recommend routine genetic screening of adults with idiopathic VTE.
There is insufficient evidence to recommend genetic testing for asymptomatic family members of patients with known VTE, nor for counseling about prophylactic antithrombotic therapy.
The group noted that anticoagulation in these individuals was likely to create more harm than benefit.
Gersh (2011) ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy
Key points:
Guidelines for diagnosis and treatment of hypertrophic cardiomyopathy.
Recommended routine screening of first-degree relatives with or without genetic tests for familial inheritance as part of evaluation of hypertrophic cardiomyopathy.
Recommended routine genetic counseling as part of evaluation of hypertrophic cardiomyopathy.
Goldman (2011) Genetic counseling and testing for Alzheimer’s disease
Key points:
Guidelines identify those individuals likely to benefit from genetic counseling and testing for Alzheimer’s disease.
Offers an algorithmic pedigree analysis and risk assessment for Alzheimer’s of early or late onset.
AUA (2010) The optimal evaluation of the infertile male: AUA best practice statement.
Key points:
Guidelines for the evaluation of the infertile male.
Authors found insufficient evidence to make a recommendation for genetic testing.
Burgunder (2010) EFNS guidelines on the molecular diagnosis of channelopathies, epilepsies, migraine, stroke, and dementias
Key points:
Evaluated genetic testing for the molecular diagnosis of channelopathies, epilepsies, migraine, stroke, and dementias.
Found sufficient available evidence that thorough clinical and electrophysiological investigation leads to informed choices of genetic tests for channelopathies (i.e., periodic paralysis).

9
Evidence supported electrophysiologic testing to establish muscular dystonia phenotype as a guide to informed choice of molecular genetic testing for these conditions.
Authors concluded that, “Molecular investigations are possible and may help in some cases to diagnose the condition, but cannot be considered routine procedure with the large number of mutations in different genes.” They give one exception: severe myoclonic epilepsy of infancy in which SCN1A mutations are found in 80 percent of those tested.
Bushby (2010) Diagnosis and management of Duchenne muscular dystrophy
Key points:
Guidelines for the diagnosis and management of Duchenne muscular dystrophy (DMD).
Genetic testing for mutation is necessary to confirm diagnosis.
Testing should be performed by a neuromuscular specialist, with support from geneticist and genetic counselors.
Palomaki (2010) Use of Genomic Profiling to Assess Risk for Cardiovascular Disease (CVD) and Identify Individualized Prevention Strategies
Key points:
Genomic profiling to assess cardiovascular risk results is a small improvement at best.
Authors found insufficient evidence to recommend it as a routine screening practice for cardiovascular risk.
Gasser (2010) EFNS guidelines on the molecular diagnosis of ataxias and spastic paraplegias
Key points:
Guidelines for the molecular diagnosis of ataxias and spastic paraplegias.
Authors found moderate-to-good evidence to support genetic testing for diagnosis of hereditary spastic paraplegias and hereditary ataxias (i.e., autosomal dominant and autosomal recessive cerebellar ataxias).
Lees (2010) Neonatal screening for sickle cell disease
Key points:
Searched for evidence indicating newborn population screening with genetic tests for sickle cell anemia can reduce the adverse effects of the disease.
No studies were identified for inclusion in the review.
The authors were unable to draw any conclusions based on controlled studies and deferred recommendation for its routine clinical practice.
Glossary
Acute coronary syndrome — Any group of symptoms related to coronary artery obstruction: most
commonly pressure-like chest pain, often radiating to the left arm or jaw; associated with nausea and
sweating; diagnosed by characteristic electrocardiogram patterns.
Alzheimer’s disease — Named for the German psychiatrist who described it in the early 20th century,
Alzheimer’s disease is the most common form of dementia. It usually occurs in people over age 65,
although an early onset type can be diagnosed much earlier. Diagnosis by standardized memory and
thinking tests is usually sufficient, although it is sometimes supplemented by brain scans. Causation and
risk factors (including any genetic component) and prevention remain incompletely defined. No
treatments to stop or reverse disease progression are yet available.

10
Cardiomyopathy — Literally, “disease of the heart muscle,” cardiomyopathy refers to deteriorated
heart function for any reason and ultimately results in heart failure. The most common form is dilated
cardiomyopathy. The cardiomyopathies are diagnosed by symptoms and electrocardiogram. Specific
causes, including any genetic contributors, are not always well-defined, although coronary artery
disease should be ruled out.
Channelopathy — Disease of the ion-channel sub-units of cell membranes or of the proteins that
regulate them. Channelopathies may be congenital/genetic or acquired. Those involving skeletal muscle
result in forms of paralysis.
Duchenne muscular dystrophy — Recessive, X-linked disease found in one of 3,600 boys before age 6
years and producing muscle degeneration eventually leading to death. Females may be carriers, but
rarely show symptoms. Genetic testing in symptomatic boys (muscle weakness in legs and pelvis, low
endurance and difficulty with stairs) confirms diagnosis. Leg braces may assist walking initially, but most
patients become wheelchair-dependent. Mean life expectancy is 25 years of age.
Fragile X — The second most common form of intellectual delay (after Down syndrome) and the most
common inherited form, Fragile X results from a dynamic mutation in a gene on the long arm of the X
chromosome. Various strategies are used for prenatal screening.
Genetic testing — A variety of laboratory tests (analysis of DNA, RNA, genes, or gene products)
performed to diagnose disease, assist in treatment decisions, predict future disease, and identify
carriers of disease.
Hereditary nonpolyposis colorectal cancer — Also known as Lynch syndrome, hereditary non-polyposis
colorectal cancer, familial adenomatous polyposis (FAP), attenuated familial polyposis (AFAP), inherited
mutation-associated polyposis (MAP), and adenomatous polyposis coli (APC), this condition is no longer
considered an exclusively autosomal dominant syndrome, since some patients show autosomal
recessive inheritance due to mutations in the same gene (MUTYH).
Mitochondrial diseases — A group of diseases caused by dysfunctional mitochondria, the subcellular
organelles responsible for energy production. Approximately 15 percent of the group is related to
mutations in mitochondrial DNA. These disorders include mitochondrial myopathies; diabetes mellitus
and deafness; Leber’s hereditary neuropathy; Wolff-Parkinson-White syndrome; Leigh syndrome;
neuropathy, ataxia, retinitis pigmentosa, and ptosis (NARP); myoneurogenic gastrointestinal
encephalopathy (MNGIE); myoclonic epilepsy with ragged red fibers (MERRF); mitochondrial myopathy,
encephalomyopathy, lactic acidosis, and stroke-like symptoms (MELAS); and others. Symptoms include
poor growth, muscle weakness and loss of coordination; visual and hearing problems; learning
disabilities; and dysfunction in other organs or systems. Approximately 1 in 4,000 U.S. children are
affected. Treatment options are limited.

11
Parkinson’s disease — A degenerative disease of the central nervous system resulting from dopamine-
generating cell death in a region of the mid-brain, causing characteristic clinical motor problems initially,
then eventually cognitive and behavioral ones. Many risk factors have been investigated, but no single
causative exposure or agent has been established. Diagnosis is clinical, and treatment with dopamine
agonists, MAO-B inhibitors, surgery, or rehabilitation is variably effective in compensating for deficits.
Sickle-cell disease — An inherited blood disorder characterized by rigid, abnormally shaped red blood
cells that can “log jam” at narrow or branch points in the vascular system, resulting in various acute and
chronic complications and shortened life expectancy. A mutation in the gene controlling hemoglobin
production produces co-dominant inheritance. Individuals with a single copy (carriers) of the gene have
both normal and abnormal hemoglobins, and experience symptoms only in certain circumstances (e.g.,
oxygen deprivation or severe dehydration). Individuals with two copies of the mutated gene are more
likely to experience painful vaso-occlusive crises that can lead to tissue or organ damage.
X-linked hemophilia (hemophilia A and B) — X-linked recessive bleeding disorders caused by
deficiencies in factors VIII and IX. Affected males are symptomatic with a range of clinical severities,
while females usually are asymptomatic carriers. Worldwide incidence is 1 in 5,000 newborn males for
hemophilia A and 1 in 30,000 for hemophilia B. Patients and families experience uncertain and excessive
bleeding episodes, transfusion-associated infection risks, frequent outpatient visits or hospitalizations,
financial and quality-of-life costs, and emotional burdens.
References
Professional society guidelines/other:
American Urological Association Education and Research Inc. The optimal evaluation of the infertile
male: AUA best practice statement. Linthicum, MD: American Urological Association Education and
Research Inc.; 2010.
Association of Comprehensive Cancer Centres (ACCC). Hereditary colorectal cancer. Amsterdam: NL:
ACCC; 2009.
Hayes Inc., Hayes Medical Technology Report. Genetic Testing for Susceptibility to Breast Cancer.
Lansdale, PA: Hayes Inc.; January 2008.
New Zealand Guidelines Group (NZGG). Management of early breast cancer. Wellington, NZ: NZGG;
2009: 149 – 59.
Royal Australian College of General Practitioners (RACGP). Genetic counseling and testing. In: Guidelines
for preventive activities in general practice, eighth edition. East Melbourne, AU: RACGP; 2012: 14 – 16.

12
Sturgeon CM, Diamandis EP (eds). Use of tumor markers in testicular, prostate, colorectal, breast, and
ovarian cancers. Washington, DC: National Academy of Clinical Biochemistry of the American
Association for Clinical Chemistry; 2009.
Peer-reviewed references:
Ackerman MJ, Priori SG, Willems S, et al. HRS/EHRA expert consensus statement on the state of genetic
testing for the channelopathies and cardiomyopathies. Heart Rhythm. 2011; 8(8): 1308 – 1339.
Albanese A, Asmus F, Bhatia KP, et al. EFNS guidelines on diagnosis and treatment of primary dystonias.
Eur J Neurol. 2011; 18(1): 5 – 18.
Berardelli A, Wenning GK, Antonini A, et al. EFNS/MDS-ES recommendations for the diagnosis of
Parkinson’s disease. Eur J Neurol. 2013; 20(1): 16 – 34.
Berg AO, Botkin J, Calone N, et al. Evaluation of Genomic Applications in Practice and Prevention
(EGAPP) Working Group. Routine testing for Factor V Leiden (R506Q) and prothrombin (20210G>A)
mutations in adults with a history of idiopathic venous thromboembolism and their adult family
members. Genet Med. 2011; 13(1): 67-76. doi: 10.1097/GIM.0b013e3181fbe46f.
Burgunder JM, Finisterer J, Szolnoki Z, et al. European Federation of Neurological Societies. EFNS
guidelines on the molecular diagnosis of channelopathies, epilepsies, migraine, stroke, and dementias.
Eur J Neurol. 2010; 17(5): 641 – 648.
Bushby K, Finkel R, Birnkrant DJ, et al. DMD Care Considerations Working Group. Diagnosis and
management of Duchenne muscular dystrophy, part 1: diagnosis, and pharmacological and psychosocial
management. Lancet Neurol. 2010; 9(1): 77 – 93.
Carrigan M, Duignan E, Malone CPG, et al. Panel-Based Population Next-Generation Sequencing for
Inherited Retinal Degenerations. Scientific Reports. 2016;6:33248.
Daoud H, Luco S, Li R, et al. Next-generation sequencing for diagnosis of rare diseases in the neonatal
intensive care unit. CMAJ. 2016 Aug 9; 188(11): E254–E260.
Djalalov S, Yong J, Beca J, et al. Genetic testing in combination with preventive donezepil treatment for
patients with amnestic mild cognitive impairment: an exploratory economic evaluation of personalized
medicine. Mol Diagn Ther. 2012; 16(6): 389 – 399.
Finsterer J, Harbo HF, Baets J, et al. European Federation of Neurological Sciences (EFNS) guidelines on
the molecular diagnosis of mitochondrial disorders. Eur J Neurol. 2009; 16(12): 1255 – 1264.

13
Gasser T, Baets J, van Broeckhoven C, et al. EFNS guidelines on the molecular diagnosis of ataxias and
spastic paraplegias. Eur J Neurol. 2010; 17(2): 179 – 88.
Gersh BJ, Maron BJ, Bonow RO, et al. 2011 American College of Cardiology Foundation/American Heart
Association (ACCF/AHA) guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: a
report of the ACCF/AHA Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2011; 58(25): e212 –
e260.
Goldman JS, Hahn SE, Catania JW, et al. American College of Medical Genetics and the National Society
of Genetic Counselors. Genetic counseling and testing for Alzheimer disease. Genet Med. 2011; 13(6):
597 – 605.
Hilgart JS, Coles B, Iredale R. Cancer genetic risk assessment for individuals at risk of familial breast
cancer. Cochrane Database of Systematic Reviews 2012, Issue 2. Art. No.: CD003721. DOI:
10.1002/14651858.CD003721.pub3.
Hussein N, Weng SF, Kai J, Kleijnen J, Qureshi N. Preconception risk assessment for thalassaemia, sickle
cell disease, cystic fibrosis and Tay-Sachs disease. Cochrane Database Syst Rev. 2015, Issue 8. Art. No.:
CD010849. DOI: 10.1002/14651858.CD010849.pub2.
Kornman LH, Nisbet DL, Liebelt J. Preconception and antenatal screening for the fragile site on the X-
chromosome. Cochrane Database Syst Rev. 2003, Issue 1. Art. No.: CD001806. DOI:
10.1002/14651858.CD001806.
LaLa A, Berger S, Sharma G, Hochman JS, Braithwaite RS, Ladapo A. Genetic testing in patients with
acute coronary syndrome undergoing percutaneous coronary intervention: a cost-effectiveness analysis.
Thromb Haemost. January 2013; 11(1): 81 – 91. doi: 10.1111/jth.12059.
Lees C, Davies SC, Dezateux C. Neonatal screening for sickle cell disease. Cochrane Database Syst Rev.
2000, Issue 1. Art. No.: CD001913. DOI: 10.1002/14651858.CD001913.
Lindenfeld J, Albert NM, Boehmer JP, et al. Genetic evaluation of cardiomyopathy: HFSA 2010
comprehensive heart failure practice guideline. J Card Fail. 2010; 16(6): e180 – e194.
Norman R, van Gool K, Hall J, Delatycki M, Massie J. Cost-effectiveness of carrier screening for cystic
fibrosis in Australia. J Cyst Fibros. 2012; 11(4): 281 – 287.
Okazaki T, Murata M, Kai M, et al. Clinical Diagnosis of Mendelian Disorders Using a Comprehensive
Gene-Targeted Panel Test for Next-Generation Sequencing. Yonago Acta Med. 2016 Jun; 59(2): 118–
125.
Palomaki GE, Melillo S, Neveux L, et al. Evaluation of Genomic Applications in Practice and Prevention
(EGAPP) Working Group. Use of Genomic Profiling to Assess Risk for Cardiovascular Disease (CVD) and

14
Identify Individualized Prevention Strategies. Genet Med. December 2010; 12(12): 772 – 784. doi:
10.1097/GIM.0b013e3181f8728d.
Pangalos C, Hagnefelt B, Lilakos K, Konialis C. First applications of a targeted exome sequencing
approach in fetuses with ultrasound abnormalities reveals an important fraction of cases with
associated gene defects.
PeerJ. 2016; 4: e1955.
Pellacani S, Sicca F, Di Lorenzo C, et al. The Revolution in Migraine Genetics: From Aching Channels
Disorders to a Next-Generation Medicine. Front Cell Neurosci. 2016; 10: 156.
Riley BD, Culver JO, Skrzynia C, et al. Essential elements of genetic cancer risk assessment, counseling,
and testing: updated recommendations of the National Society of Genetic Counselors. J Genet Couns.
2012; 21(2): 151 – 161.
Simeoni I, Stephens JC, Hu F, et al. A high-throughput sequencing test for diagnosing inherited bleeding,
thrombotic, and platelet disorders. Blood. 2016;127(23):2791-2803.
Southern KW, Mérelle MME, Dankert-Roelse JE, Nagelkerke A. Newborn screening for cystic fibrosis.
Cochrane Database Syst Rev. 2009; Issue 1. Art. No.: CD001402. DOI:
10.1002/14651858.CD001402.pub2.
Walsh, J. M. E. and Goldberg, J. D. Fetal aneuploidy detection by maternal plasma DNA sequencing: a
technology assessment. Prenat Diagn. 2013; 33(6): 514 – 520. doi: 10.1002/pd.4109.
Walter JH, Jahnke N, Remmington T. Newborn screening for homocystinuria. Cochrane Database Syst
Rev. 2015; Issue 10. Art. No.: CD008840. DOI: 10.1002/14651858.CD008840.pub4.
Weissman SM, Burt R, Church J, et al. Identification of individuals at risk for Lynch syndrome using
targeted interventions and genetic testing: National Society of Genetic Counselors and the Collaborative
Group of the Americas on Inherited Colorectal Cancer joint practice guideline. J Genet Couns. 2012;
21(4): 484 – 493.
Clinical trials:
Searched clinicaltrials.gov on September 30, 2016 using terms items | Open Studies. 943 studies found,
3 relevant.
Cure CMD. Myotubular Myopathy Genetic Testing Study. ClinicalTrials.gov Web site.
http://clinicaltrials.gov/show/NCT01817946. Published March 19, 2013. Updated July 2016. Accessed
September 30, 2016.

15
University of Utah. Genetic Analysis of Congenital Diaphragmatic Disorders. ClinicalTrials.gov Web site.
http://clinicaltrials.gov/show/NCT01243229. Published November 16, 2010. Updated March 2016.
Accessed September 30, 2016.
Medical College of Wisconsin. Genetic Analysis of PHACE Syndrome (Hemangioma With Other
Congenital Anomalies) (PHACE). ClinicalTrials.gov Web site. http://clinicaltrials.gov/show/NCT01016756.
Published November 18, 2009. Updated March 2016. Accessed September 30, 2016.
CMS National Coverage Determinations (NCDs):
No NCDs identified as of the writing of this policy, with the following technology assessment:
Update on Mapping the Landscape of Genetic Tests for Non-Cancer Diseases/Conditions.
https://www.cms.gov/Medicare/Coverage/DeterminationProcess/Downloads/id86TA.pdf. Accessed
September 30, 2015.
Local Coverage Determinations (LCDs):
No LCDs identified as of the writing of this policy.
Commonly submitted codes
Below are the most commonly submitted codes for the service(s)/item(s) subject to this policy. This is
not an exhaustive list of codes. Providers are expected to consult the appropriate coding manuals and
bill accordingly.
CPT Code Description Comment
81161 DMD (dystrophin) (E.g., Duchenne/Becker muscular dystrophy) deletion analysis, and duplication analysis, if performed.
81256 HFE (hemochromatosis) (e.g., hereditary hemochromatosis) gene analysis, common variants (e.g., C282Y, H63D).
81243 FMR1 (Fragile X mental retardation 1) (eg, fragile X mental retardation) gene analysis; evaluation to detect abnorma (eg, expanded) alleles
81244 FMR1 (Fragile X mental retardation 1) (eg, fragile X mental retardation) gene analysis; characterization of alleles (eg, expanded size and methylation status)
81265 Comparative analysis using Short Tandem Repeat (STR) markers: patient and comparative specimen (e.g., pre-transplant recipient and donor germline testing, post transplant non-hematopoietic recipient germline and donor testing, twin zygosity testing or maternal cell contamination of fetal cells.
81401 HTT (huntingtin) (eg, Huntington disease), evaluation to detect abnormal (eg, expanded) alleles
81479 Unlisted molecular pathology procedure.
ICD-10 Code Description Comment

16
C18.0 Malignant neoplasm of cecum
C18.1 Malignant neoplasm of appendix
C18.2 Malignant neoplasm of ascending colon
C18.3 Malignant neoplasm of hepatic flexure
C18.4 Malignant neoplasm of transverse colon
C18.5 Malignant neoplasm of splenic flexure
C18.6 Malignant neoplasm of descending colon
C18.7 Malignant neoplasm of sigmoid colon
C18.8 Malignant neoplasm of overlapping sites of colon
C18.9 Malignant neoplasm of colon, unspecified
C19 Malignant neoplasm of rectosigmoid junction
C20 Malignant neoplasm of rectum
C21.0 Malignant neoplasm of anus, unspecified
C50.011 Malignant neoplasm of nipple and areola, right female breast
C50.012 Malignant neoplasm of nipple and areola, left female breast
C50.019 Malignant neoplasm of nipple and areola, unspecified female breast
C50.111 Malignant neoplasm of central portion of right female breast
C50.112 Malignant neoplasm of central portion of left female breast
C50.119 Malignant neoplasm of central portion of unspecified female breast
C50.211 Malignant neoplasm of upper-inner quadrant of right female breast
C50.212 Malignant neoplasm of upper-inner quadrant of left female breast
C50.219 Malignant neoplasm of upper-inner quadrant of unspecified female breast
C50.311 Malignant neoplasm of lower-inner quadrant of right female breast
C50.312 Malignant neoplasm of lower-inner quadrant of left female breast
C50.319 Malignant neoplasm of lower-inner quadrant of unspecified female breast
C50.411 Malignant neoplasm of upper-outer quadrant of right female breast
C50.412 Malignant neoplasm of upper-outer quadrant of left female breast
C50.419 Malignant neoplasm of upper-outer quadrant of unspecified female breast
C50.511 Malignant neoplasm of lower-outer quadrant of right female breast
C50.512 Malignant neoplasm of lower-outer quadrant of left female breast
C50.519 Malignant neoplasm of lower-outer quadrant of unspecified female breast
C50.611 Malignant neoplasm of axillary tail of right female breast
C50.612 Malignant neoplasm of axillary tail of left female breast
C50.619 Malignant neoplasm of axillary tail of unspecified female breast
C50.811 Malignant neoplasm of overlapping sites of right female breast
C50.812 Malignant neoplasm of overlapping sites of left female breast
C50.819 Malignant neoplasm of overlapping sites of unspecified female breast
C50.911 Malignant neoplasm of unspecified site of right female breast
C50.912 Malignant neoplasm of unspecified site of left female breast
C50.919 Malignant neoplasm of unspecified site of unspecified female breast
C56.1 Malignant neoplasm of right ovary
C56.2 Malignant neoplasm of left ovary
C56.9 Malignant neoplasm of unspecified ovary
D56.4 Hereditary persistence of fetal hemoglobin [HPFH]
D56.8 Other thalassemias
D57.00 Hb-SS disease with crisis, unspecified
D57.01 Hb-SS disease with acute chest syndrome
D57.02 Hb-SS disease with splenic sequestration
D57.1 Sickle-cell disease without crisis
D57.20 Sickle-cell/Hb-C disease without crisis
D57.211 Sickle-cell/Hb-C disease with acute chest syndrome
D57.212 Sickle-cell/Hb-C disease with splenic sequestration
D57.219 Sickle-cell/Hb-C disease with crisis, unspecified
D57.80 Other sickle-cell disorders without crisis

17
D57.811 Other sickle-cell disorders with acute chest syndrome
D57.812 Other sickle-cell disorders with splenic sequestration
D57.819 Other sickle-cell disorders with crisis, unspecified
D58.2 Other hemoglobinopathies
D66 Hereditary factor VIII deficiency
D67 Hereditary factor IX deficiency
D68.0 Von Willebrand's disease
D68.1 Hereditary factor XI deficiency
D68.2 Hereditary deficiency of other clotting factors
E83.110 Hereditary hemochromatosis
E88.40 Mitochondrial metabolism disorder, unspecified
E88.41 MELAS syndrome
E88.42 MERRF syndrome
E88.49 Other mitochondrial metabolism disorders
G10 Huntington's disease
G71.0 Muscular dystrophy
G71.13 Myotonic chondrodystrophy
G72.3 Periodic paralysis
H49.811 Kearns-Sayre syndrome, right eye
H49.812 Kearns-Sayre syndrome, left eye
H49.813 Kearns-Sayre syndrome, bilateral
H49.819 Kearns-Sayre syndrome, unspecified eye
I42.0 Dilated cardiomyopathy
I42.4 Endocardial fibroelastosis
I42.5 Other restrictive cardiomyopathy
I42.8 Other cardiomyopathies
I42.9 Cardiomyopathy, unspecified
Q77.0 Achondrogenesis
Q77.1 Thanatophoric short stature
Q77.4 Achondroplasia
Q77.5 Diastrophic dysplasia
Q77.7 Spondyloepiphyseal dysplasia
Q77.8 Other osteochondrodysplasia with defects of growth of tubular bones and spine
HCPCS Level II
Description Comment