Clinical Policy Bulletin: Parenteral ImmunoglobulinsThere are several brands of parenteral...
56
Parenteral Immunoglobulins Page 1 of 56 04/15/2015 Aetna Better Health® 2000 Market Suite Ste. 850 Philadelphia, PA 19103 AETNA BETTER HEALTH® Clinical Policy Bulletin: Parenteral Immunoglobulins Number: 0206 Policy I. Aetna considers the use of intravenous immunoglobulin (IVIG) therapy medically necessary in members with the conditions specified below: ■ Acquired red cell aplasia ■ Acute disseminated encephalomyelitis (see Appendix) ■ Autoimmune mucocutaneous blistering diseases: IVIG is considered medically necessary for members with pemphigus vulgaris, pemphigus foliaceus, bullous pemphigoid, mucous membrane pemphigoid (a.k.a., cicatrical pemphigoid), and epidermolysis bullosa acquisita if the member has either failed or has contraindications to conventional therapy, or the member has rapidly progressive disease in which a clinical response could not be affected quickly enough using conventional agents. When indicated for rapidly progressive disease, accepted guidelines indicate that IVIG should be given along with conventional treatment(s) and IVIG should be used only until conventional therapy could take effect. (See Appendix) Note: IVIG for the treatment of autoimmune mucocutaneous blistering disease is considered medically necessary only for short-term therapy and not as a maintenance therapy ■ B-cell chronic lymphocytic leukemia (CLL): For persons with hypogammaglobulinemia associated with CLL and recurrent infections or specific antibody deficiency (see Appendix) ■ Birdshot (vitiligenous) retinochoroidopathy (see Appendix) ■ Chronic inflammatory demyelinating polyneuropathy (see Appendix) ■ Churg-Strauss Syndrome (CSS) (allergic granulomatosis), adjunctive therapy for persons with severe active illness for whom other interventions have been unsuccessful, have become intolerable, or are contraindicated ■ Dermatomyositis, adjunctive therapy in persons who have had an inadequate response to first and second line therapies (see Appendix) ■ Enteroviral meningoencephalitis (see Appendix) ■ Guillain-Barré syndrome (GBS) and GBS variants: IVIG is generally accepted as the treatment of choice for persons with Guillain-Barre syndrome, provided that they are so severely affected that they at least require aid to walk, that the disorder is diagnosed during the first 2 weeks of the illness, and that there are no contraindications to IVIG (see Appendix) ■ Hemolytic disease of newborn, to decrease need for exchange transfusion (see Appendix) ■ HIV infected children: Bacterial control or prevention (see Appendix)
Transcript of Clinical Policy Bulletin: Parenteral ImmunoglobulinsThere are several brands of parenteral...
Parenteral Immunoglobulins Page 1 of 56
04/15/2015
Aetna Better Health® 2000 Market Suite Ste. 850 Philadelphia, PA 19103
AETNA BETTER HEALTH® Clinical Policy Bulletin: Parenteral Immunoglobulins
Number: 0206
Policy
I. Aetna considers the use of intravenous immunoglobulin (IVIG) therapy medically necessary in
members with the conditions specified below:
■ Acquired red cell aplasia
■ Acute disseminated encephalomyelitis (see Appendix)
■ Autoimmune mucocutaneous blistering diseases: IVIG is considered medically necessary
for members with pemphigus vulgaris, pemphigus foliaceus, bullous pemphigoid, mucous membrane pemphigoid (a.k.a., cicatrical pemphigoid), and epidermolysis bullosa acquisita if the member has either failed or has contraindications to conventional therapy, or the member has rapidly progressive disease in which a clinical response could not be affected quickly enough using conventional agents. When indicated for rapidly progressive disease, accepted guidelines indicate that IVIG should be given along with conventional treatment(s) and IVIG should be used only until conventional therapy could take effect. (See Appendix) Note: IVIG for the treatment of autoimmune mucocutaneous blistering disease is considered medically necessary only for short-term therapy and not as a maintenance therapy
■ B-cell chronic lymphocytic leukemia (CLL): For persons with hypogammaglobulinemia
associated with CLL and recurrent infections or specific antibody deficiency (see Appendix)
■ Birdshot (vitiligenous) retinochoroidopathy (see Appendix)
■ Chronic inflammatory demyelinating polyneuropathy (see Appendix)
■ Churg-Strauss Syndrome (CSS) (allergic granulomatosis), adjunctive therapy for persons with severe active illness for whom other interventions have been unsuccessful, have become intolerable, or are contraindicated
■ Dermatomyositis, adjunctive therapy in persons who have had an inadequate response to
first and second line therapies (see Appendix)
■ Enteroviral meningoencephalitis (see Appendix)
■ Guillain-Barré syndrome (GBS) and GBS variants: IVIG is generally accepted as the treatment of choice for persons with Guillain-Barre syndrome, provided that they are so severely affected that they at least require aid to walk, that the disorder is diagnosed during the first 2 weeks of the illness, and that there are no contraindications to IVIG (see Appendix)
■ Hemolytic disease of newborn, to decrease need for exchange transfusion (see Appendix)
■ HIV infected children: Bacterial control or prevention (see Appendix)
Parenteral Immunoglobulins Page 2 of 56
04/15/2015
■ HIV-associated thrombocytopenia, pediatric or adult: Considered medically necessary when criteria in Appendix are met (see Appendix)
■ Hyperimmunoglobulinemia E syndrome: For treatment of severe infection (see Appendix)
■ Immune or idiopathic thrombocytopenic purpura (ITP) when a rapid rise in the platelet
count is required, such as prior to surgery, to control excessive bleeding, or to defer or avoid splenectomy (see Appendix for criteria for ITP in adults, ITP in children, chronic ITP, and ITP in pregnancy)
■ Kawasaki disease (see Appendix)
■ Lambert-Eaton myasthenic syndrome (see Appendix)
■ Moersch-Woltmann (Stiff-man) syndrome (unresponsive to other therapies) (see Appendix)
■ Multifocal motor neuropathy: For persons who have progressive, symptomatic multifocal
motor neuropathy that has been diagnosed on the basis of electrophysiologic findings that rule out other possible conditions that may not respond to this treatment (see Appendix)
■ Multiple myeloma (see Appendix)
■ Myasthenia gravis (see Appendix)
■ Neonatal alloimmune thrombocytopenia (NAIT) (also known as fetal alloimmune
thrombocytopenia or FAIT) (see Appendix)
■ Neonatal hemochromatosis, prophylaxis (see Appendix)
■ Opsoclonus-myoclonus (see Appendix)
■ Paraneoplastic opsoclonus-myoclonus-ataxia associated with neuroblastoma (see Appendix)
■ Parvovirus B19 infection, chronic, with severe anemia (see Appendix)
■ Polymyositis in persons who are resistant to first and second line therapies
■ Post-transfusion purpura (see Appendix)
■ Primary humoral immunodeficiency diseases (such as congenital agammaglobulinemia (X-
linked agammaglobulinemia), hypogammaglobulinemia, common variable immunodeficiency, X-linked immunodeficiency with hyperimmunoglobulin M, Wiscott- Aldrich syndrome, immunodeficiency with thymoma (Good syndrome), hyper IgM syndromes, and severe combined immunodeficiency) (see Appendix)
■ Rasmussen encephalitis (Rasmussen's syndrome) (see Appendix)
■ Refractory autoimmune hemolytic anemia (see Appendix)
■ Relapsing-remitting multiple sclerosis (MS) when standard approaches (i.e., interferons)
have failed, become intolerable, or are contraindicated (see Appendix) (See also CPB 0264 - Multiple Sclerosis)
■ Respiratory syncytial virus infection
■ Renal transplantation from live donor with ABO incompatibility or positive cross-match,
where a suitable non-reactive live or cadaveric donor is unavailable (preparative regimen)
■ Secondary immunosuppression associated with major surgery (such as cardiac transplants) and certain diseases (extensive burns, or collagen-vascular diseases) (see Appendix)
■ Selective IgG subclass deficiencies with severe infection for persons meeting selection
criteria (see Appendix)
Parenteral Immunoglobulins Page 3 of 56
04/15/2015
■ Solid organ transplantation, for suppression of panel reactive anti-HLA antibodies in persons with high panel reactive antibody (PRA) levels to human leukocyte antigens (HLA) prior to transplantation, and for treatment of antibody mediated rejection of solid organ transplants
■ Staphylococcal toxic shock syndrome (see Appendix)
■ Stem cell or bone marrow transplantation: IVIG is indicated for prophylaxis in allogeneic or
syngeneic transplant recipients within the first 100 days post-transplant; after 100 days post-transplant IVIG is indicated for recipients who are markedly hypogammaglobinemic (IgG level less than 400 mg/dL), who have primary immunodeficiency diseases, or who have CMV, EBV, or RSV infection (see Appendix and CPB 0544 - Immune Globulins for Post-exposure Prophylaxis). IVIG is also indicated for steroid-resistant graft-versus-host disease in bone marrow transplant recipients 20 years of age or older, in the first 100 days post-transplant, and who are hypogammaglobinemic (IgG level less than 400 mg/dL).
■ Systemic lupus erythematosus (SLE), for persons with severe active SLE for whom other
interventions have been unsuccessful, have become intolerable, or are contraindicated (see Appendix)
■ Toxic epidermal necrolysis and Steven-Johnson syndrome (see Appendix)
■ Toxic shock syndrome or toxic necrotizing fasciitis due to group A streptococcus (see
Appendix).
II. Aetna considers subcutaneously administered immunoglobulins as an alternative to intravenous
immunoglobulin therapy medically necessary for members who meet the criteria for IVIG set forth above.
III. Aetna considers intramuscularly administered immunoglobulins (e.g., GamaSTAN S/D) medically
necessary as an alternative to intravenous immunoglobulin therapy for conditions associated with hypogammaglobulinemia that meet the criteria for IVIG set forth above. Intramuscular formulations of immune globulin are also considered medically necessary for the following indications: prophylaxis of hepatitis A; prevention or modification of measles (rubeola) in persons exposed fewer than 6 days previously; passive immunization against varicella in immunosuppressed patients; and prophylaxis of rubella in pregnancy when therapeutic abortion is not an option. See CPB 0544 - Immune Globulins for Post-exposure Prophylaxis.
IV. Aetna considers the use of IVIG experimental and investigational for all other clinical conditions
because its effectiveness for indications other than the ones listed above has not been established. See Appendix for a current list of such indications (not an all-inclusive list).
V. Least Cost Medically Necessary Brands of Parenteral Immunoglobulins:
There are several brands of parenteral immunoglobulins on the market (see appendix). There is a lack of reliable evidence that any one brand of parenteral immunoglobulin is superior to other brands for medically necessary indications. Gammaplex brand of parenteral immunoglobulin ("least cost brand of parenteral immunoglobulin") is less costly to Aetna. Consequently, because other brands (e.g., Bivigam, Carimune, Glebogamma, Gammagard, Gammaked, Gammar, Gamunex, Hizentra, HyQvia, Iveegam, Octogam, Panglobin, Polygam, Privigen) of parenteral immune globulin are more costly than the alternative least cost brand of parenteral immune globulin that is at least as likely to produce equivalent therapeutic results as to the treatment of the member's disease, under some Aetna plans, other brands of parenteral immune globulin will be considered not medically necessary unless the member has a contraindication or intolerance to the least cost brand of parenteral immune globulin. If the least cost brand of parenteral immune globulin does not have the labeled indication (see appendix), then Aetna considers medically necessary another brand of parenteral immune globulin that has the required labeling indication. Other brands of Parenteral Immune globulin will be allowed to be grandfathered with their previous use history.
Notes: The following criteria are considered in assessing the medical necessity of IVIG for the indications listed above.
Parenteral Immunoglobulins Page 4 of 56
04/15/2015
1. Clinical monitoring takes clear precedence over laboratory monitoring. IVIG therapy should primarily be guided by clinical improvement.
2. In some situations, IVIG may be used for medically necessary indications listed above for a person that has rapidly progressive disease in which a clinical response could not be effected quickly enough using conventional agents. In these situations, IVIG therapy would be given along with conventional treatment(s) and continued administration of IVIG is not considered medically necessary once conventional therapy takes effect and the patient is stabilized.
3. Once treatment is initiated, there must be adequate documentation of progress. If there is initial improvement, and continued treatment is necessary, then some type of objective quantitative assessment to monitor the progress is required, when applicable. Any accepted metric assessment may be used for objective monitoring of progress, such as the Inflammatory Neuropathy Cause and Treatment (INCAT) scale*, the Medical Research Council (MRC) scale ** and activities of daily living (ADL) measurements. Changes in these measures should be clearly documented. Subjective or experiential improvement alone is generally insufficient to either continue IVIG, except for diseases where there is no accepted objective metric.
4. Previous treatment failures must be documented. (This would not apply to primary immunodeficiencies diagnosed at birth.)
5. The diagnosis of the disorder must be reasonably certain, and based on a thorough history and examination, and appropriate laboratory testing (e.g., electromyography (EMG), spinal fluid tests, serum tests and biopsy findings).
6. There should be, depending on the diagnosis and clinical circumstances, an attempt made to decrease/wean the dosage when improvement has occurred. There should be, when clinically appropriate for the diagnosis, an attempt to stop the IVIG infusion if improvement is sustained with dosage reduction. If improvement does not occur with IVIG, continued infusion may not be considered medically necessary. (This does not apply to persons with primary immune deficiency diseases.)
* The Inflammatory Neuropathy Cause and Treatment (INCAT) scale is used to access functional disability of both upper and lower extremity components in chronic inflammatory demyelinating polyneuropathy (CIDP). The INCAT scale has upper and lower extremity components, with a maximum of 5 points for the upper extremity (arm disability) and a maximum of 5 points for the lower extremity (leg disability), which add up to a maximum of 10 points (where 0 is normal and 10 is severely incapacitated). The INCAT scores may be used to evaluate the effectiveness and need for IVIG. IVIG may be discontinued when there is a lack of clear clinical improvement (i.e., a decline in INCAT disability score or failure to improve by 1 point at 6 weeks following the initial infusion or return to baseline at anytime following initial improvement of 1 point).
** The Medical Research Council (MRC) scale is used to grade muscle strength. Scale: 0 = no muscle movement; 1 = flicker of muscle movement; 2 = trace movement but not able to fully overcome gravity; 3 = just able to overcome gravity, but not against resistance; 4 = moves against resistance, but weak; 5 = full strength against resistance.
For IVIG for rubella (German measles), see CPB 0544 - Immune Globulins for Post-exposure Prophylaxis.
Background
Intravenous immunoglobulin (IVIG) has been shown to be ineffective for the prophylaxis of, and as a treatment adjunct in, infections in some high-risk, preterm, low-birth-weight neonates (USPDI, 2002). Studies published before 1990 suggested that prophylactic IVIG reduced nosocomial infections in low- birth-weight infants. However, these studies enrolled small numbers of patients; employed varied designs, preparations, and doses; and included diverse study populations. The National Institute of Child Health and Human Development (NICHHD) Neonatal Research Network therefore performed a prospective, multi-center, randomized trial to test the hypothesis that the intravenous administration of immune globulin to infants with birth weights between 501 and 1,500 grams would reduce the incidence of nosocomial infections (Fanaroff et al, 1994). In this trial, the repeated prophylactic administration of IVIG failed to reduce the incidence of nosocomial infections significantly in premature infants weighing 501 to 1,500 grams at birth. Furthermore, there were no significant differences in morbidity, mortality, or

Parenteral Immunoglobulins Page 5 of 56
04/15/2015
the duration of hospitalization between infants given IVIG and infants given no infusion or an infusion and placebo.
For a discussion of IVIG for recurrent spontaneous abortion, see CPB 0348 - Recurrent Pregnancy Loss.
Several brands of IVIG have been approved by the Food and Drug Adminsitration (FDA) (see table in Appendix). There is a lack of reliable evidence that any one brand of IVIG is more effective than other brands. However, immune globulin products may differ from each other in ways that may be important in a particular patient. Different manufacturers then use various combinations of precipitation and/or chromatography steps to obtain a final preparation that consists of greater than 95 % IgG in all currently available products. The various manufacturers also use different final purification steps and stabilizers to obtain their final products, which may then vary in storage requirement and shelf life. In several currently available products, stabilizers include sugars, such as sucrose, glucose, or maltose. Other products contain amino acids such as glycine and proline. The sodium content of different products also varies.
Most products approximate the distribution of IgG subclasses found in normal plasma. However, products are neither standardized nor routinely tested for their content of specific antibodies against different pathogens, except for measles, poliovirus, and hepatitis B surface antigen.
Thus, product-to-product and lot-to-lot variation in specific antibody titers is likely. There are also product -to-product and lot-to-lot variations in adverse effects in individual patients. Thus, generic substitution is not acceptable for many patients. In contrast, the different preparations are generally assumed to have overall equivalent therapeutic efficacy in protecting antibody deficient patients against infection.
Specific patients may require, or do better with, IGIV products with certain characteristics. Most patients tolerate most products with a minimum of adverse events, or with simple premedications. Thus, for many patients, selection of a product to conform with local dispensing or formulary preferences may not pose problems. However, some patients experience a different range and/or severity of adverse effects from different products, which may be impossible to predict.
If a patient is having adverse effects that interfere with IgG replacement, different products should be tried in the hope of finding a product that will be more acceptable. However, adverse effects may be more frequent and/or more severe whenever a patient is first started on IGIV and whenever a new product is used. For this reason, extra caution should be used when starting a naïve patient or changing the specific product used by any individual patient.
Some patients require products low in IgA, or products with relatively lower osmolarity, sucrose, or sodium. Patients with diabetes who use certain types of glucose meters must use caution with maltose- containing products, since that sugar may give false readings for glucose. Some preparations may have as much as 30 mg/ml (3 %) albumin, in addition to the IgG itself. This may be undesirable in patients who might have trouble tolerating increased intravascular volume.
The first type of IgG preparation to be used for antibody replacement, 16 % Immune Serum Globulin (ISG) for intra-muscular (IM) administration is still available. However, the IM route is rarely used at the present time because the injections are painful, the amount given is limited by the volumes that can be administered, and there is risk of local injury, such as nerve damage.
Immune globulin may also been given by the subcutaneous route. Immune globulin may be administered by a subcutaneous injection via a small, portable pump for the prevention of serious infection in children and adults with primary immunodeficiency. Many patients can be readily taught to infuse themselves at home, or parents may administer the infusions to their children.
In April 2006, the American Academy of Asthma, Allergy and Immunology (Orange et al, 2006) published evidence based guidelines on indications for intravenous immunoglobulins.
Darabi et al (2006) noted that IVIG has been approved by the FDA for use in 6 conditions: (i) immune thrombocytopenic purpura (ITP), (ii) primary immunodeficiency, (iii) secondary immunodeficiency, (iv) pediatric HIV infection, (v) Kawasaki disease, and (vi) prevention of graft-versus-host disease (GVHD) and infection in bone marrow transplant recipients. IVIG has subsequently been approved by the FDA for chronic inflammatory demyelinating polyneuropathy (CIDP). However, most usage of IVIG is for off- label indications, and for some of these comprehensive guidelines have been published. Common off- labeled uses for IVIG include chronic neuropathy (e.g., multi-focal motor neuropathy), hypogammaglobulinemia, renal transplant rejection, myasthenia gravis, Guillain-Barre syndrome,

Parenteral Immunoglobulins Page 6 of 56
04/15/2015
necrotizing fasciitis, and autoimmune hemolytic anemia. The authors concluded that only a few indications account for most of the usage for IVIG. Reports concerning IVIG continue to grow at a tremendous pace but few high-quality randomized controlled studies have been reported.
In a review on autism, Levy et al (2009) stated that popular biologically based treatments include anti- infectives, chelation medications, gastrointestinal medications, hyperbaric oxygen therapy, and IVIGs. Non-biologically based treatments include auditory integration therapy, chiropractic therapy, cranio- sacral manipulation, interactive metronome, and transcranial stimulation. However, few studies have addressed the safety and effectiveness of most of these treatments.
Whitington and Kelly (2008) stated that neonatal hemochromatosis (NH) is the result of severe fetal liver injury that seems to result from maternal-fetal alloimmunity. Women who have had an infant affected with NH are at high-risk in subsequent pregnancies for having another affected infant. This study was designed to examine if therapy directed at limiting the severity of gestational alloimmunity can reduce the occurrence of severe NH in infants of women at risk. A secondary objective was to use a prospectively collected data set to examine questions of vital interest about NH. Women with a history of pregnancy ending in documented NH were treated with IVIG at 1 g/kg of body weight weekly from the 18th week until the end of gestation. Extensive data were prospectively collected regarding the gestational histories of the subjects. The outcomes of treated pregnancies were compared with those of previous affected pregnancies, which were used as historical controls. A total of 48 women were enrolled to be treated during 53 pregnancies. The gestational histories of these women demonstrated the high-risk of occurrence of NH: 92 % of pregnancies at risk resulted in intrauterine fetal demise, neonatal death, or liver failure necessitating transplant. In contrast, with gestational therapy, the 53 at-risk gestations resulted in 3 failures and 52 infants who survived intact with medical therapy alone. When compared on a per-woman or per-infant basis, the outcome of gestation at risk for NH was improved by gestational therapy. The authors concluded that NH seems to be the result of a gestational alloimmune disease, and occurrence of severe NH in at-risk pregnancies can be significantly reduced by treatment with high- dose IVIG during gestation.
In this regard, the Australian National Blood Authority (Gibson et al, 2007) listed NH as one of the conditions for which IVIG has an established therapeutic role. According to the Australian agency, women who are pregnant or attempting to conceive and their most recent pregnancy ended in delivery of a fetus shown to have had NH are qualified for IVIG therapy. Dosage should be 1g/kg body weight weekly from the 18th week until the end of gestation.
Anderson et al (2007) noted that to help ensure IVIG use is in keeping with an evidence-based approach to the practice of medicine, the National Advisory Committee on Blood and Blood Products of Canada (NAC) and Canadian Blood Services convened a panel of national experts to develop an evidence- based practice guideline on the use of IVIG for hematologic conditions. The mandate of the expert panel was to review evidence regarding use of IVIG for 18 hematologic conditions and formulate recommendations on IVIG use for each. A panel of 13 clinical experts and 1 expert in practice guideline development met to review the evidence and reach consensus on the recommendations for the use of IVIG. The primary sources used by the panel were 3 recent evidence-based reviews. Recommendations were based on interpretation of the available evidence and where evidence was lacking, consensus of expert clinical opinion. A draft of the practice guideline was circulated to hematologists in Canada for feedback. The results of this process were reviewed by the expert panel, and modifications to the draft guideline were made where appropriate. This practice guideline provided the NAC with a basis for making recommendations to provincial and territorial health ministries regarding IVIG use management. Specific recommendations for routine use of IVIG were made for 7 conditions including acquired red cell aplasia; acquired hypogammaglobulinemia (secondary to malignancy); fetal- neonatal alloimmune thrombocytopenia; hemolytic disease of the newborn; HIV-associated thrombocytopenia; idiopathic thrombocytopenic purpura; and post-transfusion purpura. Intravenous immune globulin was not recommended for use, except under certain life-threatening circumstances, for 8 conditions including acquired hemophilia; acquired von Willebrand disease; autoimmune hemolytic anemia; autoimmune neutropenia; hemolytic transfusion reaction; hemolytic transfusion reaction associated with sickle cell disease; hemolytic uremic syndrome/thrombotic thrombocytopenic purpura; and viral-associated hemophagocytic syndrome. Intravenous immune globulin was not recommended for 2 conditions (aplastic anemia and hematopoietic stem cell transplantation) and was contraindicated for 1 condition (heparin-induced thrombocytopenia). For most hematologic conditions reviewed by the expert panel, routine use of IVIG was not recommended.

Parenteral Immunoglobulins Page 7 of 56
04/15/2015
Goebel et al (2010) evaluated the effectiveness of IVIG in patients with longstanding complex regional pain syndrome (CRPS) under randomized, controlled conditions. Patients who had pain intensity greater than 4 on an 11-point (0 to 10) numerical rating scale and had CRPS for 6 to 30 months that was refractory to standard treatment were enrolled in this study. Subjects received IVIG (0.5 g/kg) and normal saline in separate treatments, divided by a washout period of at least 28 days. The primary outcome was pain intensity 6 to 19 days after the initial treatment and the cross-over treatment. A total of 13 eligible participants were randomly assigned and 12 completed the trial. The average pain intensity was 1.55 units lower after IVIG treatment than after saline (95 % confidence interval [CI]: 1.29 to 1.82; p < 0.001). In 3 patients, pain intensity after IVIG was less than after saline by 50 % or more. No serious adverse reactions were reported. The drawbacks of this study were that the trial was small, and recruitment bias and chance variation could have influenced results and their interpretation. The authors concluded that IVIG (0.5 g/kg) can reduce pain in refractory CRPS. They stated that confirmatory trials are required to ascertain the best immunoglobulin dose, the duration of effect, the need for repeat treatment, and whether treatment response varies with disease duration.
Diabetic amyotrophy usually occurs in patients with poorly controlled diabetes, either as an initial presentation or in a patient with longstanding disease. The mechanism of diabetic amyotrophy is uncertain, although peri-vascular inflammation and secondary nerve infarction are thought responsible. A recent consensus statement from the American Academy of Neurology (AAN) concluded that there is "no convincing data" to substantiate the treatment of diabetic amyotrophy using IVIG (Donofrio et al, 2009).
O'Horo and Safdar (2009) stated that clostridium difficile (C. difficile) is the most common infectious cause of nosocomial healthcare-associated diarrhea. The increasing prevalence of C difficile, spread in the community, virulence and frequent relapse has created an urgent need to identify new effective treatments for C. difficile infection. Among these, IVIG is used for cases of severe C. difficile infection. These investigators undertook a systematic review to examine the published literature pertaining to the use of immunoglobulin for C. difficile infection. Four retrospective studies and 5 case reports that addressed the use of IVIG for the treatment of C. difficile infection were identified. One study on the use of oral immunoglobulin was identified. Although overall there appear to be benefits to using IVIG in recurrent severe disease, the small sample sizes and lack of control groups in 3 of the 4 studies do not allow recommendations to be made regarding the use of immunoglobulin in C. difficile infection. The authors stated that further research is urgently needed to clarify the role of immunoglobulin -- intravenous or oral -- for the treatment of C. difficile infection.
Abougergi et al (2010) stated that C. difficile colitis (CDC) is the most common cause of hospital- acquired diarrhea. The increase in the incidence and fatality rate of CDC over the past decade has stimulated a search for new therapies, including IVIG. These researchers reported their experience with IVIG for the treatment of 21 patients with severe CDC. The existing literature on IVIG infusion for severe CDC was also reviewed. Twenty-one of 1,230 patients with CDC were treated with IVIG. The mean age was 68 (range of 35 to 98) years, with mean hospital stay of 23 (range of 9 to 64) days. Conventional treatment was used for an average of 8 (range of 1 to 25) days before IVIG infusion. All patients had evidence of pancolitis (radiologically) or ileus (clinically). The mean Acute Physiological Assessment and Chronic Health Evaluation (APACHE II) score was 25 (range of 6 to 39) at day 1 of IVIG infusion. Nine patients (43 %) survived their hospitalization with colitis resolution while 12 (57 %) died. One patient developed pulmonary edema after IVIG infusion. Symptoms resolved after an average of 10 (range of 2 to 20) days for survivors. Two patients underwent urgent colectomy. The authors concluded that this is the largest case series describing IVIG use for patients with severe CDC and the one with the highest mortality rate to date. The use of IVIG in this setting does not seem to benefit all patients. Benefit appears to depend on the extent of systemic involvement. They stated that further studies are needed before adopting IVIG as routine treatment for severe CDC.
Diaz-Manera and colleagues (2009) noted that advances in the treatment of myasthenia gravis (MG) have reduced mortality rates due to the disease and improved patients' quality of life. Nowadays, attending neurologists can choose among different treatment strategies for MG patients. An exhaustive revision of published data on the efficacy of the different therapeutic options for MG indicates that there are insufficient evidence-based results. However, recommendations based on expert opinion can be provided. Thymectomy is indicated in all patients with a thymoma or for generalized acetylcholine receptor-sero-positive patients aged 18 to 55 years. Steroids are the most widely used immunosuppressive drug for MG. They are recommended as the first-line drug in all patients with
Parenteral Immunoglobulins Page 8 of 56
04/15/2015
generalized MG without response to thymectomy, or in those patients who do not fulfill criteria for the surgery. The selection of second-line drugs may vary between protocols. The authors recommended starting with azathioprine if insufficient remission is achieved with steroids, followed by ciclosporin, mycophenolate and others. They use rituximab or cyclophosphamide only in severely drug-resistant patients. Finally, the authors recommend IVIG or plasma exchange (PE) in MG crisis, or for unstable patients before thymectomy or in clinical exacerbations.
Tranchant (2009) stated that the purpose of the treatment of MG is to improve neuromuscular transmission, and to reduce the production or presence of the nicotinic acetylcholine receptor (achR). Acetylcholinesterase inhibitors are the first line treatment with the rapid onset of effect, for all types of MG (ocular, generalized MG, sero-negative or sero-positive patients). Plasmapheresis or IVIG is the treatment for exacerbations. Their main advantage is the rapid onset of the effect; 3 to 5 PE or IVIG infusions (1.2 to 2 g/body weight administered over 2 to 5 days) are usually recommended. In case of suspected thymoma, thymectomy should be always performed. The option of thymectomy was discussed in young patients less than 50 years old with unstable MG, even if thymoma lesions are not suspected. Corticosteroids and/or immunosuppressive agents are used in severe forms of the disease. A few randomized studies have shown the effectiveness of the therapeutic agents. Corticosteroids are considered a major treatment of MG but the doses and periods of time are still being debated. The combination of corticosteroids and immunosuppressive agents are recommended early to spare corticosteroids. The treatment of MG should be modulated regularly (minimal doses for example). The use of IVIG prior to thymectomy was not discussed.
The European Federation of Neurological Societies' task force on the use of IVIG in treatment of neurological diseases (Elovaara et al, 2008) stated that IVIG is an effective treatment for acute exacerbations of MG and for short-term treatment of severe MG (level A); and IVIG is similar to PE regarding effect. This treatment is safe also for children, during pregnancy, and for elderly patients with complicating disorders. There is not sufficient evidence to recommend IVIG for chronic maintenance therapy in MG alone or in combination with other immunoactive drugs. Furthermore, the use of IVIG before thymectomy was not discussed.
Morozumi and associates (2009) evaluated the effect of IVIG therapy in the treatment of neuropathic pain associated with Sjogren's syndrome. These investigators examined 5 patients affected by painful sensory neuropathy associated with Sjögren's syndrome. All patients were treated with IVIG (0.4 g/kg/day for 5 days) and pain rating was assessed by the visual analog scale (VAS). All 5 patients showed a remarkable improvement in neuropathic pain following IVIG therapy. Pain, assessed by the determination of mean VAS score, was reduced by 73.4 % from days 2 to 14 following treatment. The observed clinical improvement persisted for 2 to 6 months. One patient, examined by quantitative sensory testing, showed an improvement of superficial sensory deficit accompanied by pain relief. The authors concluded that IVIG might be an effective treatment for pain in Sjögren's syndrome-associated neuropathy. They stated that further studies should be done in a controlled, blind study.
Ishii et al (1994) examined the clinical effects of PE and high dose IVIG in a 41-year old woman with Isaacs' syndrome. After double filtration PE, symptoms almost disappeared for 2 to 3 weeks and the recorded continuous muscle action potentials were considerably decreased. Symptoms recurred within a few months. On the other hand, IVIG worsened the symptoms of the disorder: during and after IVIG at a dose of 0.2 g/kg/day (total 50 g), widespread myokymia, pseudomyotonia, and muscle cramps gradually increased. Symptoms improved after another course of PE.
Myers and Baker (2009) noted that acquired neuromyotonia, also known as Isaacs' syndrome, has been described in combination with a variety of other autoimmune disorders; however there has never been a report of sero-positive Isaacs' syndrome in a patient with a history of Guillain-Barre syndrome (GBS). Both conditions involve antibody-mediated autoimmune effects on the peripheral nervous system, although the clinical manifestations are quite different. These researchers presented a man who experienced an episode of GBS at the age of 21 and subsequently developed Isaacs' syndrome at the age of 24 which was positive for anti-voltage-gated potassium channel (VGKC) antibodies. When treated with IVIG, he developed an eczematous rash that differed markedly in pattern and duration from the usual presentation for this IVIG reaction.
Aries and colleagues (2005) stated that initially IVIGs were used as replacement therapy in primary and secondary antibody-deficiency syndromes. The clinical use of IVIG has been extended during the past decade to a wide variety of clinical conditions, such as infectious processes, neuroimmunological

Parenteral Immunoglobulins Page 9 of 56
04/15/2015
diseases, and different systemic autoimmune diseases. The mode of action of IVIG is complex, involving modulation of the Fc receptors, interference with the complement and cytokine network, and effects on the activation and differentiation of T and B-cells. Kawasaki disease (KD) was one of the first diseases within the group of primary vasculitides in which IVIG were used. Today, there is a clear evidence of benefit for IVIG in the treatment of coronary artery abnormalities related to KD. Subsequently, various reports have suggested a beneficial effect in other vasculitides; however, there are few data from controlled studies. For anti-neutrophil cytoplasmic antibody-associated vasculitis (AAV), 1 placebo- controlled and several open-label studies have shown a beneficial effect on the disease activity in patients with Wegener's granulomatosis or microscopic polyangiitis refractory to standard therapy with prednisone and cyclophosphamide. For other vasculitides, such as polyarteritis nodosa or Henoch- Schonlein purpura, only case reports have described an inhibition of a disease progression by IVIG so far. However, the effect was partly only temporary. The authors concluded that KD and AAV are the only vasculitides with a definite beneficial use of IVIG. For other vasculitides, the efficacy of IVIG has not been proven properly but may be useful in single cases.
Eleftheriou and Brogan (2009) stated that primary systemic vasculitides of the young are relatively rare diseases, but can have a significant morbidity and mortality. The purpose of this review was to provide an overview of the pediatric vasculitides. Vasculitides that predominantly affect children will be considered in more detail than vasculitic diseases that although are seen in children affect adults more commonly, such as the ANCA associated vasculitides. New classification criteria for childhood vasculitis have recently been proposed and are currently undergoing validation. Epidemiological clues continue to implicate infectious triggers in KD and Henoch Schönlein purpura. Several genetic polymorphisms have now been described in the vasculitides that may be relevant in terms of disease predisposition or development of disease complications. Treatment regimens continue to improve, with the use of different immunosuppressive medications and newer therapeutic approaches such as biologic agents. However new challenges are looming in regards to the role of inflammation in endothelial health and the long term cardiovascular morbidity for children with primary systemic vasculitis. International multi-center collaboration is of utmost importance in order for us to further advance the understanding and improve the treatment and outcome of systemic vasculitis in the young. Furthermore, an UpToDate review on "Management of Henoch-Schönlein purpura" (Dedeoglu et al, 2010) did not mention the use of IVIG as a therapeutic option.
Ishii and associates (2010) stated that treatment of autoimmune bullous skin diseases can often be challenging and primarily consists of systemic corticosteroids and a variety of immunosuppressants. Current treatment strategies are effective in most cases but hampered by the side effects of long-term immunosuppressive treatment. I ntravenous immunoglobulin is one potential promising therapy for patients with autoimmune bullous skin diseases, and evidence of its effectiveness and safety is increasing. A number of autoimmune bullous skin diseases have been identified in which IVIG treatment may be beneficial. However, experience with IVIG in patients with autoimmune skin blistering disease is limited, where it is recommended for patients not responding to conventional therapy. The mode of action of IVIG in autoimmune diseases, including bullous diseases is far from being completely understood. These researchers summarized the clinical evidence supporting the notion, that IVIG is a promising therapeutic agent for the treatment of patients with autoimmune bullous skin disease. In addition, they reviewed the proposed modes of action. In the future, randomized controlled trials are necessary to better determine the efficacy and adverse effects of IVIG in the treatment of autoimmune bullous skin diseases.
Jolles (2011) noted that high-dose IVIG (hdIVIG) is being used increasingly for dermatological indications. Its mode of action is via a number of proposed mechanisms and it is not associated with the many side-effects of steroids and other immunosuppressive agents. The evidence for using hdIVIG in the treatment of autoimmune bullous disorders is based on uncontrolled trials and case reports. However, there are now 62 reported patients and this review aimed to make a critical assessment of the current data. This has been obtained from a Medline search of the English literature from 1966 to 2000 for pemphigus vulgaris, pemphigus foliaceus, bullous pemphigoid, pemphigoid gestationis, cicatricial pemphigoid, epidermolysis bullosa acquisita and linear IgA disease. Taken together hdIVIG was effective in 81 % of the patients with blistering disease. Patients appear to be more likely to respond when hdIVIG is used as adjunctive therapy (91 % response rate) than as monotherapy (56 % response rate). The authors concluded that hdIVIG may offer a safe potential therapeutic avenue for resistant cases of the autoimmune bullous disorders but should be further assessed using double-blind placebo- controlled trials.

Parenteral Immunoglobulins Page 10 of 56
04/15/2015
Parambil et al (2011) stated that small fiber neuropathy (SFN) is commonly associated with sarcoidosis and can cause significant morbidity to afflicted patients. The appropriate treatment of this condition, when associated with sarcoidosis, is not well established. These investigators described case series of 3 patients with sarcoidosis and SFN; the presenting clinical features, skin biopsy results, autonomic reflex screen and quantitative sudomotor axon reflex testing (QSART) findings, and response to therapy were delineated. They described 3 patients with biopsy-proven sarcoidosis who developed intractable neuropathic pain and/or symptoms related to associated autonomic dysfunction despite treatment with various immunosuppressive medications and narcotic analgesics. QSART showed evidence of a post- ganglionic sudomotor abnormality in 1 patient and was normal in the other 2. Skin biopsy findings were abnormal, demonstrating a non-length-dependent sensory SFN in all 3 patients. Painful neuropathic symptoms, as well as symptoms related to dysautonomia from SFN responded significantly to treatment with IVIG. The authors concluded that IVIG appears to be effective in relieving symptoms from SFN associated with sarcoidosis, suggesting an underlying immune mechanism. Moreover, they stated that larger prospective, controlled studies are needed to confirm this response to IVIG and to further elucidate the underlying pathobiology behind this association with sarcoidosis.
Isobe et al (2004) described the case of a 40-year old female diagnosed with follicular lymphoma who was treated with rituximab-combined chemotherapy. Although she achieved complete remission, she developed progressive anemia and reticulocytopenia. Bone marrow examination revealed features of pure red cell aplasia and hemophagocytosis. In addition, the appearance of large pronormoblasts suggested that she was infected with parvovirus B19. Excess viral DNA in her bone marrow confirmed that her illness was caused by persistent parvovirus B19 infection. Serum immunoglobulin levels decreased beyond the lower normal limit, which indicated that her humoral immunity was impaired after rituximab-combined chemotherapy. Although she had been infected with parvovirus B19, she was re- infected and failed to control the viral expansion. High-titer immunoglobulin against parvovirus B19 was intravenously administrated and resulted in remarkable reticulocytosis and improvement of anemia. High -titer immunoglobulin, which contained a sufficient amount of neutralizing antibodies against parvovirus B19, likely inactivated most viruses in vivo. These investigators successfully eradicated the virus after 2 courses of high-dose therapy at 0.5 g/kg/day every week followed by 8 courses of maintenance therapy at 0.1 g/kg/day every other week. It is important to consider that parvovirus B19 infection is a possible cause of progressive anemia in B-cell lymphoma patients treated with rituximab-combined chemotherapy. The authors proposed that the use of high-titer immunoglobulin against parvovirus B19 may enable such immunocompromised patients to eradicate the virus before sufficient immune system reconstruction. Also, UpToDate reviews on "Initial treatment of follicular lymphoma" (Freedman and Friedberg, 2011) and "Treatment of relapsed or refractory follicular lymphoma" (Freedman and Friedberg, 2011) do not mention the use of IVIG.
Perlmutter et al (1999) examined if plasma exchange or IVIG would be better than placebo (sham IVIG) in reducing severity of neuropsychiatric symptoms in children, exacerbations of tics and obsessive symptoms. Children with severe, infection-triggered exacerbations of obsessive-compulsive disorder (OCD) or tic disorders, including Tourette syndrome, were randomly assigned treatment with plasma exchange (5 single-volume exchanges over 2 weeks), IVIG (1 g/kg daily on 2 consecutive days), or placebo (saline solution given in the same manner as IVIG). Symptom severity was rated at baseline, and at 1 month and 12 months after treatment by use of standard assessment scales for OCD, tics, anxiety, depression, and global function. A total of 30 children entered the study and 29 completed the trial. Ten received plasma exchange, 9 IVIG, and 10 placebo. At 1 month, the IVIG and plasma exchange groups showed striking improvements in obsessive-compulsive symptoms (mean improvement on children's Yale-Brown obsessive compulsive scale score of 12 [45 %] and 13 [58 %], respectively), anxiety (2.1 [31 %] and 3.0 [47 %] improvement on National Institute of Mental Health anxiety scale), and overall functioning (2.9 [33 %] and 2.8 [35 %] improvement on National Institute of Mental Health global scale). Tic symptoms were also significantly improved by plasma exchange (mean change on Tourette syndrome unified rating scale of 49 %). Treatment gains were maintained at 1 year, with 14 (82 %) of 17 children "much" or "very much" improved over baseline (7 of 8 for plasma exchange, 7 of 9 for IVIG). The authors concluded that plasma exchange and IVIG were both effective in lessening of symptom severity for children with infection-triggered OCD and tic disorders. They stated that further studies are needed to determine the active mechanism of these interventions, and to determine which children with OCD and tic disorders will benefit from immunomodulatory therapies.
In a double-blind placebo-controlled study, Hoekstra et al (2004) studied the effects of IVIG on tics. A total of 30 patients with a DSM-IV tic disorder were randomly assigned to IVIG (1 g/kg on 2 consecutive
Parenteral Immunoglobulins Page 11 of 56
04/15/2015
days; mean age = 28.71 years; range of 14 to 53 years) or placebo (mean age = 30.73 years; range of 14 to 63 years). Symptoms were rated with the Yale Global Tic Severity Scale, the Yale-Brown Obsessive Compulsive Scale, and the Clinical Global Impressions scale of symptom change with regard to tic severity. These were used at baseline and on weeks 2, 4, 6, 10, and 14 post-treatment, after which blinding was broken. The study was conducted from March through August 2002. These researchers observed no significant differences between both treatment groups regarding post-treatment changes in tic severity. Severity of obsessions and compulsions, which was in the subclinical range, decreased significantly in the IVIG group compared with the placebo group at week 6 (p = 0.02). Then, there was a 32.3 % improvement in the IVIG group compared with baseline. Though this improvement was maintained over the following 8 weeks, no statistically significant differences between the IVIG and the placebo group with regard to improvements in obsessions and compulsions were detected at subsequent assessments. IVIG treatment was associated with significantly more side effects than placebo, most notably headache. The authors concluded that based on the present results, IVIG can not be recommended in tic disorders.
Trucco et al (2011) evaluated the outcome of maternal autoantibody-mediated fetal cardiomyopathy/endocardial fibroelastosis following IVIG and corticosteroid therapy. These researchers have previously shown that 85 % of fetuses and infants with maternal autoantibody-mediated fetal cardiomyopathy/endocardial fibroelastosis suffer demise or need for transplant. In an attempt to improve this outcome, in 1998, they began to empirically treat affected patients with IVIG and corticosteroids. These investigators reviewed the clinical records and echocardiograms of 20 affected patients encountered in their institutions and treated with IVIG and corticosteroids from 1998 to 2009. All 20 were initially referred at a median gestational age of 23 weeks (range of 18 to 38 weeks); 19 mothers were anti-Ro antibody positive, 8 anti-La antibody positive, and 7 had clinical autoimmune disease. Endocardial fibroelastosis was seen in 16 and was not obvious in 4 others with reduced ventricular function, and 16 (80 %) had reduced or borderline ventricular shortening fraction (less than or equal to 30 %) before or after birth. Eighteen had atrioventricular block at referral (16 in 3°). During pregnancy, maternal IVIG was given in 9 and dexamethasone in 17. After birth, 17 infants received IVIG (n = 14) and/or corticosteroids (n = 15). Twelve underwent pacemaker implantation. Four with hydrops at presentation died perinatally, despite initial improvement in function in 3. At a median follow-up of 2.9 years (1.1 to 9.8 years), 16 (80 %) patients are currently alive with normal systolic ventricular function and 6 are not paced. The authors concluded that treatment of maternal autoantibody-mediated fetal cardiomyopathy/endocardial fibroelastosis with IVIG and corticosteroids potentially improves the outcome of affected fetuses. They stated that further studies (prospective, multi-center randomized trials including the evaluation of maternal and neonatal titers before and after therapy) are needed to determine the optimal dose and timing of IVIG administration.
In a Cochrane review, Ohlsson et al (2010) evaluated the effect of IVIG on mortality/morbidity caused by suspected infection in neonates and in those neonates who had suspected infection on study entry and later were confirmed as being infected. These investigators searched MEDLINE, EMBASE, The Cochrane Library, the reference lists of identified studies, meta-analyses and personal files in December 2009. They selected randomized or quasi-randomized controlled trials of IVIG for the treatment of suspected bacterial/fungal infection compared to placebo or no intervention in newborn infants (less than 28 days old). Statistical analyses included Typical Relative Risk (RR), Risk Difference (RD), weighted mean difference (WMD), the number needed to treat to benefit (NNTB) (all with with 95 % CI and the I(2) statistic to examine statistical heterogeneity. The updated search identified 1 new study; 10 studies of variable quality undertaken in 8 countries are included in this review. Mortality in infants with clinically suspected infection was reduced following IVIG treatment [7 studies (n = 378); typical RR 0.58 (95 % CI: 0.38, 0.89); typical RD -0.10 (95 % CI: - 0.18, -0.03); NNTB 10 (95 % CI: 6, 33); I(2) = 0 %]. Mortality in cases of subsequently proven infection was reduced [7 trials (n = 262); typical RR 0.55 (95 % CI: 0.31, 0.98); I(2) = 0 %]. The authors concluded that because of concerns about study quality, there is still insufficient evidence to support the routine administration of IVIG to prevent mortality in infants with suspected or subsequently proved neonatal infection. A large study of the effectiveness of IVIG in neonates with suspected infection has recently been completed. Results of the International Neonatal Immunotherapy Study (INIS trial), which enrolled 3,493 infants, are expected to be published in 2010. The results of that trial should establish the usefulness of IVIG for suspected infection in newborns.
The INIS Collaborative Group (2011) stated that neonatal sepsis is a major cause of death and complications despite antibiotic treatment. Effective adjunctive treatments are needed. Newborn infants are relatively deficient in endogenous immunoglobulin. Meta-analyses of trials of IVIG for suspected or proven neonatal sepsis suggest a reduced rate of death from any cause, but the trials have been small
Parenteral Immunoglobulins Page 12 of 56
04/15/2015
and have varied in quality. At 113 hospitals in 9 countries, these investigators enrolled 3,493 infants receiving antibiotics for suspected or proven serious infection and randomly assigned them to receive 2 infusions of either polyvalent IgG immune globulin (at a dose of 500 mg/kg body weight) or matching placebo 48 hours apart. The primary outcome was death or major disability at the age of 2 years. There was no significant between-group difference in the rates of the primary outcome, which occurred in 686 of 1,759 infants (39.0 %) who received IVIG and in 677 of 1,734 infants (39.0 %) who received placebo (relative risk, 1.00; 95 % CI: 0.92 to 1.08). Similarly, there were no significant differences in the rates of secondary outcomes, including the incidence of subsequent sepsis episodes. In follow-up of 2-year-old infants, there were no significant differences in the rates of major or non-major disability or of adverse events. The authors concluded that therapy with IVIG had no effect on the outcomes of suspected or proven neonatal sepsis.
Kim and colleagues (2011) stated that the prognosis of MG has improved dramatically due to advances in critical-care medicine and symptomatic treatments. Its immunopathogenesis is fundamentally a T-cell- dependent autoimmune process resulting from loss of tolerance toward self-antigens in the thymus. Thymectomy is based on this immunological background. For MG patients who are inadequately controlled with sufficient symptomatic treatment or fail to achieve remission after thymectomy, remission is usually achieved through the addition of other immunotherapies. These immunotherapies can be classified into 2 groups: (i) rapid induction and (ii) long-term maintenance. Rapid induction therapy includes IVIG and PE. These produce improvement within a few days after initiation, and so are useful for acute exacerbation including myasthenic crisis or in the peri-operative period. High-dose prednisone has been more universally preferred for remission induction, but it acts more slowly than IVIG and PE, commonly only after a delay of several weeks. Slow tapering of steroids after a high-dose pulse offers a method of maintaining the state of remission. However, because of significant side effects, other immunosuppressants (ISs) are frequently added as "steroid-sparing agents". The currently available ISs exert their immunosuppressive effects by 3 mechanisms: (i) blocking the synthesis of DNA and RNA, (ii) inhibiting T-cell activation and (iii) depleting the B-cell population. In addition, newer drugs including antisense molecule, tumor necrosis factor alpha receptor blocker and complement inhibitors are currently under investigation to confirm their effectiveness. Until now, the treatment of MG has been based primarily on experience rather than gold-standard evidence from randomized controlled trials. It is hoped that well-organized studies and newer experimental trials will lead to improved treatments.
A review of treatment of IgG subclass deficiencies (Lemmon & Knutsen, 2012) explains that, “in patients receiving immune globulin replacement therapy, treatment should periodically be held after one to two years for immunologic and clinical reassessment. When discontinuing immune globulin, it is advisable to do so during the spring months to minimize exposure to viral infections. We generally wait three or four months after discontinuation before performing immune testing.” The authors explain, as a rationale for this reassessment, that some people do not respond to IgG replacement therapy, and also that, especially in younger patients, immune responsiveness and IgG subclass levels may normalize over time.
The American College of Obstetricians and Gynecologists’ practice bulletin on “Antiphospholipid syndrome” (ACOG, 2011) indicated that IVIG was considered but not recommended for pregnant women with APS.
Also, the British Committee for Standards in Haematology’s guidelines on “The investigation and management of antiphospholipid syndrome” (Keeling et al, 2012) does not mention the use of IVIG.
Alijotas-Reig (2013) stated that currently there are no reliable data regarding the actual treatment received by women with refractory obstetric APS (OAPS). These researchers evaluated current clinical evidence and new trends in the treatment of refractory OAPS. A non-systematic but comprehensive literature search using relevant keywords was made to identify relevant articles published in English from different computerized databases: PubMed (Medline), Google Scholar electronic database search and The Cochrane Library, from January 2000 to March 2012. Studies on the treatment of poor obstetric outcomes in women with OAPS were included. Prospective randomized clinical trials, cohort studies, reviews, systematic reviews and meta-analysis were retrieved. A total of 130 articles were finally selected for this review, including 17 randomized clinical trials and 4 meta-analyses. The majority of articles were non-randomized original papers and basic and clinical reviews. The authors concluded that up to 20 % of women with OAPS do not receive the currently recommended therapeutic regimen. Unfortunately, well-designed studies regarding the usefulness of new drugs in refractory OAPS are
Parenteral Immunoglobulins Page 13 of 56
04/15/2015
scarce. Hydroxychloroquine and low-dose prednisolone appear to be useful when added to standard therapy. Current data do not support the use of IVIG in this field.
The American Academy of Child and Adolescent Psychiatry’s practice parameter for the assessment and treatment of children and adolescents with obsessive-compulsive disorder (AACAP, 2012) stated that “Therapeutic plasma exchange and intravenous immunoglobulin remain experimental interventions with substantial risk and potential morbidity”.
Also, UpToDate reviews on “Attention deficit hyperactivity disorder in children and adolescents: Treatment with medications” (Krull, 2012a), “Attention deficit hyperactivity disorder in children and adolescents: Overview of treatment and prognosis” (Krull, 2012b), and “Adult attention deficit hyperactivity disorder” (Searight and Burke, 2012) do NOT mention the use of IVIG as a therapeutic option.
UpToDate reviews on “Initial treatment of depression in adults” (Katon and Ciechanowski, 2012a) and “Treatment of resistant depression in adults” (Katon and Ciechanowski, 2012b) do NOT mention the use of IVIG as a therapeutic option.
An UpToDate review on “The diffuse alveolar hemorrhage syndromes” (Schwarz, 2012) states that “The possible role of intravenous immunoglobulin (IVIG) in patients with DAH due to vasculitis or other connective tissue disease is unknown”.
An UpToDate review on “PANDAS: Pediatric autoimmune neuropsychiatric disorder associated with group A streptococci” (Pichichero, 2012) states that “Routine administration of immunomodulatory therapy (e.g., glucocorticoids, plasma exchange, intravenous immunoglobulin [IVIG]) is not indicated for children who meet PANDAS criteria”.
Perlmutter et al (1999) reported on 29 children who were randomized to one of three groups: plasma exchange (n = 10), IVIG (n = 9), or placebo (n = 10). They found that at 1 month, the IVIG and plasma- exchange groups showed striking improvements in obsessive-compulsive symptoms (mean improvement on children’s Yale-Brown obsessive compulsive scale score of 12 [45 %] and 13 [58 %], respectively), anxiety (2·1 [31 %] and 3·0 [47 %] improvement on National Institute of Mental Health anxiety scale), and overall functioning (2·9 [33 %] and 2·8 [35 %] improvement on National Institute of Mental Health global scale). The investigators concluded that plasma exchange and IVIG were both effective in lessening of symptom severity for children with infection triggered OCD and tic disorders. The investigators stated that further studies are needed to determine the active mechanism of these interventions, and to determine which children with OCD and tic disorders will benefit from immunomodulatory therapies. This 3- armed trial with 10 or less participants per arm has limited statistical power.
Martino et al (2009) stated that despite their empirical use in community settings, there is still a lack of conclusive, evidence-based data regarding the usefulness of antibiotic and immuno-modulatory treatments in children with PANDAS.
Shulman (2009) noted that the relationship between obsessive-compulsive disorder (OCD) or tics/Tourette's syndrome in childhood to antecedent group A streptococci (GAS) is unclear. One recent prospective cohort study found that more than 85 % of clinical exacerbations in OCD/tic behavior in patients who met criteria for PANDAS had no relationship to GAS infection. Another study found no correlation between clinical exacerbations and changes in a variety of markers of brain autoimmunity, the proposed pathogenesis of PANDAS. A third recent study concluded that, compared with specialty clinic diagnoses, patients diagnosed with tics or Tourette's by physicians in the community were significantly more likely to be diagnosed with PANDAS without meeting the proposed criteria, most lacked supporting laboratory evidence of GAS infection, and they were more likely to be treated with unjustified short-term to chronic antibiotic and/or immuno-modulatory therapy.
Marconi et al (2009) stated that the use of treatment strategies, such as therapeutic plasmapheresis or IVIG, has been proposed to explain the autoimmune process responsible for the pathogenesis of PANDAS. Moreover, they stated that further research is still necessary in order to understand the role of streptococcal infection in the pathogenesis of PANDAS.
Tan et al (2012) posed the question “I have heard about children who have tic disorders that seem to be exacerbated by group A β-hemolytic streptococcal infection. Should children presenting with this phenomenon receive treatment with antibiotics, receive prophylactic treatment, or use
Parenteral Immunoglobulins Page 14 of 56
04/15/2015
immunomodulators to treat the symptoms?” They noted the answer to be: “Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS) constitute a condition that includes neuropsychiatric symptoms, mainly obsessive-compulsive disorder or tic disorders, temporally associated with an immune-mediated response to streptococcal infections. The actual existence of PANDAS as a unique clinical entity is still up for debate, as a temporal association between group A β- hemolytic streptococcal infections and symptom exacerbations has been difficult to prove thus far. Based on only a few studies, positive results have been found using antibiotic prophylaxis and immunomodulatory therapy in children with PANDAS. At this time, however, evidence does not support a recommendation for long-term antibiotic prophylaxis or immunomodulatory therapy.”
The AAN’s evidence-based guideline on “Intravenous immunoglobulin in the treatment of neuromuscular disorders” (Patwa et al, 2012) states that IVIG is as efficacious as plasmapheresis and should be offered for treating Guillain-Barré syndrome (GBS) in adults (Level A). IVIG is effective and should be offered in the long-term treatment of chronic inflammatory demyelinating polyneuropathy (Level A). IVIG is probably effective and should be considered for treating moderate-to-severe myasthenia gravis and multifocal motor neuropathy (Level B). IVIG is possibly effective and may be considered for treating non- responsive dermatomyositis in adults and Lambert-Eaton myasthenic syndrome (Level C). Evidence is insufficient to support or refute use of IVIG in the treatment of immunoglobulin M paraprotein-associated neuropathy, inclusion body myositis, polymyositis, diabetic radiculoplexoneuropathy, or Miller Fisher syndrome, or in the routine treatment of post-polio syndrome or in children with GBS (Level U). IVIG combined with plasmapheresis should not be considered for treating GBS (Level B). More data are needed regarding IVIG efficacy as compared with other treatments/treatment combinations.
In a Cochrane review, Gajdos et al (2012) examined the effectiveness of IVIG for treating exacerbations of MG or for chronic MG. These investigators searched the Cochrane Neuromuscular Disease Group Specialized Register (October 11, 2011), CENTRAL (2011, Issue 3), MEDLINE (January 1966 to September 2011) and EMBASE (January 1980 to September 2011) using 'myasthenia gravis' and 'intravenous immunoglobulin' as the search terms. All randomized controlled trials (RCTs) or quasi- RCTs in which IVIG was compared with no treatment, placebo or plasma exchange, in people with MG. One review author extracted the data and 2 others checked these data. For methodological reasons, no formal meta-analysis was performed. These researchers identified 7 RCTs. These trials differ in inclusion criteria, comparison with alternative treatment and outcomes. In a trial comparing IVIG with placebo, including 51 participants with MG worsening, the mean difference (MD) in quantitative MG score (QMGS) (MD 95 % CI) after 14 days was: -1.60 (95 % CI: - 3.23 to 0.03) this result being borderline statistically significant in favor of IVIG. In an unblinded study of 87 participants with exacerbation comparing IVIG and PE there was no difference in myasthenic muscle score (MMS) after 15 days (MD -1.00; 95 % CI: -7.72 to 5.72). In a study of 84 participants with worsening MG there was no difference in change in QMGS 14 days after IVIG or PE (MD -1.50; 95 % CI: -3.43 to 0.43). In a study of 12 participants with moderate or severe MG, which was at high-risk of bias from skewed allocation, the mean fall in QMGS both for IVIG and PE after 4 weeks was significant (p < 0.05). A study with 15 participants with mild or moderate MG found no difference in change in QMGS 42 days after IVIG or placebo (MD 1.60; 95 % CI: -1.92 to 5.12). A study included 33 participants with moderate exacerbations of MG and showed no difference in change in QMGS 14 days after IVIG or methylprednisolone (MD -0.42; 95 % CI: -1.20 to 0.36). All these 3 smaller studies were under- powered. The last trial, including 168 people with exacerbations, showed no evidence of superiority of IVIG 2 g/kg over IVIG 1 g/kg on the change of MMS after 15 days (MD 3.84; 95 % CI: -0.98 to 8.66). Adverse events due to IVIG were moderate (fever, nausea, headache), self-limiting and subjectively less severe than with PE (although, given the available data, no statistical comparison was possible). Other than where specific limitations were mentioned the trials were generally at low-risk of bias. The authors concluded that in exacerbation of MG, 1 RCT of IVIG versus placebo showed some evidence of the efficacy of IVIG and 2 did not show a significant difference between IVIG and PE. Another showed no significant difference in efficacy between 1 g/kg and 2 g/kg of IVIG. A further, but under-powered, trial showed no significant difference between IVIG and oral methylprednisolone. They stated that in chronic MG, there is insufficient evidence from RCTs to determine whether IVIG is effective.
The Ad Hoc Committee of the Croatian Society for Neurovascular Disorders/Croatian Medical Association’s guidelines for the use of IVIG in the treatment of neurologic diseases (Bascic-Kes et al, 2012) stated that the use of IVIG in the management of patients with neuroimmune disorders has shown a progressive trend over the last few years. Despite the wide use of IVIG, consensus on its optimal use is deficient. The European Federation of Neurological Societies (EFNS) guidance regulations offered consensus recommendations for optimal use of IVIG. The effectiveness of IVIG has been proven in
Parenteral Immunoglobulins Page 15 of 56
04/15/2015
Guillain-Barre syndrome (level A), chronic inflammatory demyelinating polyradiculoneuropathy (level A), multi-focal mononeuropathy (level A), acute exacerbations of MG and short-term treatment of severe MG (level A). As a second-line treatment, the use of IVIG is recommended in dermatomyositis in combination with prednisone (level B) and is considered as a treatment option in polymyositis (level C). As a 2nd- or even 3rd-line therapy, the use of IVIG should be considered in patients with RRMS if conventional immunomodulatory therapies are not tolerated (level B) and in relapses during pregnancy or post-partum period (good clinical practice point). Finally, it appears that the use of IVIG has a beneficial effect also in stiff-person syndrome (level A), some paraneoplastic neuropathies (level B), and some acute-demyelinating diseases and childhood refractory epilepsy (good practice point). The guideline did not mention the use of IVIG as a maintenance therapy for MG.
Also, an UpToDate review on "Treatment of myasthenia gravis" (Bird, 2013) did not mention the use of IVIG as maintenance therapy for MG.
In a Cochrane review, Lunn and Nobile-Orazio (2012) evaluated the effects of immunotherapy for IgM anti-myelin-associated glycoprotein paraprotein-associated demyelinating peripheral neuropathy. These investigators searched the Cochrane Neuromuscular Disease Group Specialized Register June 6, 2011), CENTRAL (2011, Issue 2), MEDLINE (January 1966 to May 2011) and EMBASE (January 1980 to May 2011) for controlled trials. They also checked bibliographies and contacted authors and experts in the field. These researchers included randomized or quasi-randomized controlled trials involving participants of any age treated with any type of immunotherapy for anti-myelin-associated glycoprotein antibody-associated demyelinating peripheral neuropathy with monoclonal gammopathy of undetermined significance and of any severity. The primary outcome measure was change in the Neuropathy Impairment Scale or Modified Rankin Scale at 6 months after randomization. Secondary outcome measures were: Neuropathy Impairment Scale or the Modified Rankin Score at 12 months after randomization; 10-meter walk time, subjective clinical scores and electrophysiological parameters at 6 and 12 months after randomization; IgM paraprotein levels and anti-myelin-associated glycoprotein antibody titers at 6 months after randomization; and adverse effects of treatments. The 2 authors independently selected studies; and 2 authors independently assessed the risk of bias in included studies. These investigators identified 7 eligible trials (182 participants), which tested IVIG, alfa- interferon alfa-2a, PE, cyclophosphamide and steroids, and rituximab. Only 2 trials, of IVIG (with 33 participants, including 20 with antibodies against myelin-associated glycoprotein), had comparable interventions and outcomes, but both were short-term trials. There were no clinical or statistically significant benefits of the treatments used on the outcomes pre-defined for this review, but not all the predefined outcomes were used in every included trial. Intravenous immunoglobulin showed a statistical benefit in terms of improvement in Modified Rankin Scale at 2 weeks and 10-meter walk time at 4 weeks. Cyclophosphamide failed to show any benefit in the trial's primary outcome, and showed a barely significant benefit in the primary outcome specified here, but some toxic adverse events were identified. A trial of rituximab was of poor methodological quality with a high risk of bias and a further larger study is awaited. Serious adverse events were few in the other trials. The authors concluded that there is inadequate reliable evidence from trials of immunotherapies in anti-myelin-associated glycoprotein paraproteinemic neuropathy to form an evidence base supporting any particular immunotherapy treatment. There is very low quality evidence of benefit from rituximab. They stated that large, well-designed, randomized trials of at least 6 to 12 months duration are needed to evaluate existing or novel therapies, preferably employing unified, consistent, well-designed, responsive and valid outcome measures.
Furthermore, in a review on “Intravenous immunoglobulin for treatment of neuromuscular disease”, Ruzhansky and Brannagan (2013) stated that “Clinical trials in amyotrophic lateral sclerosis, inclusion body myositis, and anti–myelin-associated glycoprotein neuropathy have been negative”.
Drulovic et al (2011) noted that Hashimoto's encephalopathy (HE) is a rare autoimmune syndrome characterized by various neuropsychiatric manifestations, responsive to steroid treatment and associated with Hashimoto's thyroiditis. There are only a few reports suggesting that IVIG might represent an effective treatment modality for the severe steroid-resistant HE cases. These investigators presented a patient with HE who developed a complete recovery after the IVIG therapy followed by a long-lasting remission. After detailed examinations, the diagnosis of HE was established. Two years later, in June 2001, new manifestations (unsteadiness in gait, personality changes, seizures, and persistent headache) gradually developed during a 6-month period. Response to steroids was unsatisfactory and partial, since headaches and personality changes had continuously worsened. In January 2002, the patient received IVIG (0.4 g/kg body weight daily for 5 days). Gradual improvement was noticed and a complete recovery
Parenteral Immunoglobulins Page 16 of 56
04/15/2015
developed over the following weeks. Up to March 2009, during a 7-year follow-up period, remission persisted. The authors concluded that to their best knowledge, this was the first report of a long-lasting remission of HE after IVIG therapy. Therefore, this case further supported administration of IVIG, as a potentially beneficial treatment modality, in severe cases of HE that are completely or partially resistant to steroids.
Olmez et al (2013) shared their experience on clinical presentation and management of patients diagnosed with HE. These researchers identified 13 patients who met the criteria for the diagnosis of HE. The median age was 49 years (range of 2 to 66) and all except 1 were women. Encephalopathy in the form of altered mental status, stroke-like symptoms or seizures, with prompt resolution of symptoms upon receiving steroids, was the commonest presentation, seen in 7 patients. The second commonest presentation was subacute progressive decrease in cognitive function, which reversed within days to weeks after steroid therapy, seen in 4 patients. Electroencephalogram (EEG) was available in 12 patients and was abnormal in 8, showing non-specific cerebral dysfunction in all 8 and epileptiform activity in 3. Treatment consisted of steroids in the acute phase for 12 of 13 patients with rapid improvement in symptoms. Maintenance therapy was rituximab in 7 patients, IVIG in 7, azathioprine in 4, mycophenolate mofetil in 3, and methotrexate in 1 (some patients received sequential therapy with different agents). There was complete or near complete resolution of symptoms in 12 of the 13 patients. The authors concluded that they presented a cohort of patients in whom central nervous system dysfunction was associated with elevated anti-thyroid antibodies and reversal of disease followed immunomodulatory therapies. This was a small study and the findings were confounded by sequential therapies with different agents.
He and colleagues (2013) reported the findings of a case of a 61-year old man presented with unconsciousness, spasms and a previous misdiagnosis as viral encephalitis. Response to anti-viral and steroid therapy was unsatisfactory, but treatment with immunoglobulin combined with corticosteroid therapy achieved rapid and complete recovery. The authors concluded that any patient presenting with acute or subacute unexplained encephalopathy should be considered HE, even if the thyroid function is normal. Thyroid antibody testing should be performed because this may be the most important clue to diagnosis. As soon as the diagnosis is made, steroid therapy is the first choice. If the steroid therapy does not lead to immediate improvement, IVIG is an effective alternative treatment.
An UpToDate review on “Hashimoto's encephalopathy” (Rubin, 2013) stated that “Clinical improvement with intravenous immunoglobulin, and plasmapheresis has been reported in individual cases”. However, IVIG is not mentioned in the “Summary and Recommendations” of this review.
Since available evidence is based on single-case studies as well as small case-series studies, the role of IVIG for the treatment for autoimmune encephalopathy has yet to be established.
In a Cochrane review, Wong et al (2013) assessed the safety and effectiveness of the use of IVIG antenatally to women with severe fetal red blood cell alloimmunization. These investigators searched the Cochrane Pregnancy and Childbirth Group trials register (December 19, 2012), and reference lists of articles. Randomized trials assessing the antenatal use of IVIG administered at any dose, frequency or duration with a control group (using any other, or no treatment) in the management of fetal red blood cell alloimmunization were selected for analysis. Two review authors independently assessed the available evidence. There were no included studies. The authors concluded that no information is available from randomized trials to indicate whether the antenatal use of IVIG is effective in the management of fetal red blood cell alloimmunization. Several case series suggested a beneficial role in delaying the onset of fetal anemia requiring invasive intrauterine transfusion.
An UpToDate review on “Epidemiology, pathogenesis, treatment, and prevention of enterovirus and parechovirus infections” (Modlin, 2013) stated that “The therapeutic options for more serious infections are limited and none has been subjected to adequate evaluation by clinical trials. Intravenous immune globulin (IVIG) has been administered to B-cell deficient patients with persistent meningoencephalitis, on a case by case basis, with mixed results”.
Joao (2007) stated that human B cell immune deficiencies are associated with increased susceptibility to viral and fungi infections, which are T cell immunity related infections. Also, some viral infections occurring in immune depressed patients such as cytomegalovirus (CMV) infections are recommended to be treated with IVIG in combination with anti-viral therapy. This fact has no clear biological explanation but it has been shown to be successful. Recently, B cells and immunoglobulin were identified as essential elements driving T cell receptor (TCR) diversity generation. Idiotype peptides of B cell
Parenteral Immunoglobulins Page 17 of 56
04/15/2015
immunoglobulin may be the driving force for the antigen presenting function of B cells and other antigen presenting cells to influence the T cell repertoire. This seems to be another relevance of Jerne's idiotypic network and another function of immunoglobulin. Since T cells function depends on the diversity of the TCR repertoire, means to increase the diversity of the T cell repertoire may improve T cell function in situations characterized by a contracted TCR repertoire (e.g., AIDS, primary immunodeficiency, cancer, autoimmunity and following chemotherapy and hematopoietic precursors transplantation). The clinical hypothesis put forth by this researcher is that B cells and/or immunoglobulin may be used therapeutically aiming to increase and potentially to restore T cell repertoire diversity improving T cell function in situations implicating a contracted T cell repertoire. The fact that immunoglobulin influences the composition of T cell repertoire by increasing its diversity allows a much wider application of this molecule in the clinical practice. The author presented a novel reasoning for the use of IVIG in humans, which should be explored. All the situations where immune reconstitution occurs are potentially a target for this therapeutically mechanism, aiming to improve the diversity of the reconstituted immune repertoires. This new role of Ig molecule may help to explain several effects that IVIG have in the T cell compartment, such as modulation of the activation and function of effectors T cells. The idea that immunoglobulin is essential in the generation and maintenance of a diverse compartment of T cells, affecting T cell function via that mechanism suggests a promising approach to medical conditions involving immune reconstitution. Furthermore, it represents a new paradigm of understanding the immune system as a complex, interdependent web of cells/cell products that inter-affect each other generation, function and survival.
Schmidt-Hieber et al (2009) developed a novel algorithm to define the need for high-dose prophylactic IVIG in periods of high-risk for CMV to patients after allo-SCT. Intravenous immunoglobulins were administered only if at least one of the following, monthly-assessed, criteria was fulfilled: (i) IgG concentration less than 4 g/L, (ii) NK (natural killer) cell count less than 100/microl, (iii) CD4(+) cell count less than 100/microl, and (iv) acute or chronic GVHD. The primary end-point was to determine the cumulative incidence of CMV infection in patients who received prophylactic IVIG according to the algorithm (intervention group) and compare it with that of a sequentially assessed control group, to which prophylactic IVIG were not administered. The study included 79 patients (44 in the intervention and 35 in the control group). The estimated cumulative incidence of CMV infection in the intervention and control group did not differ significantly (44 and 36 %; p = 0.31). Additionally, prophylactic IVIG did not reduce the frequency of CMV infection episodes. Cytomegalovirus disease was rare in both cohorts (5 % and 9 %; p = 0.65). The authors concluded that prophylactic IVIG should not be administered after allo-SCT, even if administered selectively in a high-dose to patients with delayed immune reconstitution or GVHD.
Also, an UpToDate review on “Immune reconstitution inflammatory syndrome” (Sexton and Pien, 2013) noted that many synonyms exist for IRIS [immune reconstitution inflammatory syndrome]:
Immune recovery disease Immune reconstitution disease Immune reconstitution syndrome Immune restoration disease Immune rebound illness Steroid-withdrawal disease Immunorestitution disease Immune response reactions
There is no mentioning of IVIG as a therapeutic option for IRIS in this UpToDate review.
Gavhed et al (2011) stated that there is currently no well-accepted therapy for central nervous system Langerhans cell histiocytosis (CNS-LCH), a neuroinflammatory disease clinically characterized by often progressive, neurological symptoms including ataxia, dysarthria, dysphagia, hyper-tonicity, intellectual impairment and behavioral abnormalities. These investigators applied immunomodulative/anti- inflammatory treatment on a patient with progressive CNS-LCH disease – IVIG was administered monthly for 15 years to a patient with severe, image-verified neurodegenerative CNS-LCH. During the IVIG treatment, the neurological deterioration initially appeared to be haltered, but over time there was still some deterioration. The authors concluded that IVIG may be beneficial in partly haltering CNS-LCH neurodegeneration, but further studies are needed.
Edeer-Karaca et al (2010) stated that common variable immunodeficiency (CVID) is an immunodeficiency syndrome characterized by generalized defective antibody production and recurrent
Parenteral Immunoglobulins Page 18 of 56
04/15/2015
sino-pulmonary bacterial infections. Autoimmune disease is common in CVID, occurring in approximately 20 % of patients, with a slight female predominance. Familial inheritance of CVID is very rare, and these investigators reported 2 siblings with CVID presenting remarkable autoimmune manifestations such as relapsing polychondritis, juvenile idiopathic arthritis and chronic inflammatory bowel disease. Autoimmune and inflammatory complications showed minimal improvement under regular IVIG replacement therapy, prophylactic antibiotics and immunosuppressives in these patients.
Also, an UpToDate review on “Treatment of relapsing polychondritis” (Michet, 2013) did not mention IVIG as a therapeutic option.
Hughes et al (2009) noted that idiopathic solar urticaria (SU) is a rare, debilitating photodermatosis, which may be difficult to treat. First-line treatment with anti-histamines is effective in mild cases, but remission after phototherapeutic induction of tolerance is often short-lived. Other treatment options include PE, photopheresis and cyclosporine. These researchers presented 2 cases of severe, idiopathic SU, which were resistant to conventional treatment. Both patients achieved remission after administration of IVIG and have remained in remission at 13 months and 4 years, respectively. There were only 2 case reports of successful treatment of solar urticaria with IVIG. The authors concluded that in their experience IVIG given at a total dose of 2 g/kg over several 5-day courses about a month apart is an effective treatment option for severe idiopathic SU. It is also generally safe, even if certainly subject to significant theoretical risks, such as induction of viral infection or anaphylaxis.
Llamas-Velasco et al (2011) stated that the treatment of SU can be difficult. Only a few cases of SU have been treated with IVIG (as monotherapy or combined with phototherapy), with reported fast and durable increase of solar exposure tolerance. In this study, a 61-year old female with severe UVB- and UVA-induced SU and a 62-year old female with severe UVA and visible light-induced SU were both treated with a single course of IVIG (total dose of 2 g/kg), infused over 3 days. Photo-test, performed 3 months after the treatment, showed only a slight minimal urticating dose improvement, and both patients reported just a moderate and “transient” subjective improvement. The authors concluded that their patients’ poorer response, compared with previous reports, may be due to differences in IVIG treatment schedules.
Adamski et al (2011) reported on the effectiveness of IVIG in severe SU. These researchers performed a retrospective multi-centric study via the mailing of a questionnaire to the French photodermatology units to analyze all cases of patients with SU who were treated with IVIG. A total of 7 patients (5 women) with a mean age of 40 years (range of 32 to 55 years) and a mean disease duration of 5 years (range of 2 to 10 years) received IVIG. The administration schedule differed from one patient to another: 1.4 to 2.5 g/kg were infused over 2 to 5 days. Five of 7 patients obtained a complete remission. The number of courses necessary to obtain clinical remission varied from 1 to 3 courses. Complete remission was maintained during 4 to more than 12 months but anti-histamines were still required. In 1 case, PUVA photochemotherapy was administered. The authors concluded that the findings of this case series suggested a beneficial effect of IVIG in severe SU; but additional prospective trials including a larger number of patients are needed to demonstrate the effectiveness of IVIG and to specify the optimal modalities of their administration in this disease. Drawbacks of this study included its retrospective study design, limited number of patients, and variations in the IVIG administration schedule.
Also, an UpToDate review on “Photosensitivity disorders (photodermatoses): Clinical manifestations, diagnosis, and treatment” (Elmets, 2013) does not mention the use of IVIG as a therapeutic option.
In a Cochrane review, Ohlsson and Lacy (2013) examined the effects of IVIG on mortality/morbidity caused by suspected or proven infection at study entry in neonates. These researchers also assessed in a subgroup analysis the effects of IgM-enriched IVIG on mortality from suspected infection. MEDLINE, EMBASE, The Cochrane Library, CINAHL, trial registries, Web of Science, reference lists of identified studies, meta-analyses and personal files were searched in 2013. No language restrictions were applied. Randomized or quasi-randomized controlled trials; newborn infants (less than 28 days old); IVIG for treatment of suspected or proven bacterial/fungal infection compared with placebo or no intervention; one of the following outcomes was reported: mortality, length of hospital stay or psychomotor development at follow-up. Statistical analyses included typical risk ratio (RR), risk difference (RD), weighted mean difference (WMD), number needed to treat for an additional beneficial outcome (NNTB) or an additional harmful outcome (NNTH) (all with 95 % CIs and the I-squared (I(2)) statistic to examine for statistical heterogeneity). The updated search identified 1 published study and 1 ongoing study. A total of 8 studies evaluating 3,871 infants were included in this review. Mortality during
Parenteral Immunoglobulins Page 19 of 56
04/15/2015
hospital stay in infants with clinically suspected infection at trial entry was not significantly different after IVIG treatment (8 studies (n = 2,425); typical RR 0.94, 95 % CI: 0.80 to 1.12; typical RD -0.01, 95 % CI: - 0.04 to 0.02 I(2) = 28 % for RR and 32 % for RD). Death or major disability at 2 years corrected age was not significantly different in infants with suspected infection after IVIG treatment (1 study (n = 1,985); RR 0.98, 95 % CI: 0.88 to 1.09 RD -0.01, 95 % CI: -0.05 to 0.03). Mortality during hospital stay was not significantly different after IVIG treatment in infants with proven infection at trial entry (RR 0.95, 95 % CI: 0.74 to 1.21 RD -0.01, 95 % CI: -0.04 to 0.03). Death or major disability at 2 years corrected age was not significantly different after IVIG treatment in infants with proven infection at trial entry (RR 1.03, 95 % CI: 0.91 to 1.18; RD 0.01, 95 % CI: -0.04 to 0.06). Mortality during hospital stay in infants with clinically suspected or proven infection at trial entry was not significantly different after IVIG treatment (1 study (n = 3,493); RR 1.00, 95 % CI: 0.86 to 1.16; RD 0.00, 95 % CI: - 0.02 to 0.03). Death or major disability at 2 years corrected age was not significantly different after IVIG treatment in infants with suspected or proven infection at trial entry (1 study (n = 3,493); RR 1.00, 95 % CI: 0.92 to 1.09; RD -0.00, 95 % CI: - 0.03 to 0.03). Length of hospital stay was not reduced for infants with suspected/proven infection at trial entry (1 study (n = 3,493); mean difference (MD) 0.00 days, 95 % CI: -0.61 to 0.61). No significant difference in mortality during hospital stay after IgM-enriched IVIG treatment for suspected infection was reported at trial entry (3 studies (n = 164); typical RR 0.57, 95 % CI: 0.31 to 1.04; RD -0.12, 95 % CI: - 0.24 to 0.00; p = 0.06); I(2) = 2 % for RR and 0 % for RD). The authors concluded that in previous reviews, they encouraged researchers to undertake well-designed trials to confirm or refute the effectiveness of IVIG in reducing adverse outcomes in neonates with suspected infection. Such a trial has been undertaken. Results of the INIS trial, which enrolled 3,493 infants, carried a heavy weight in the current update of this review, and the undisputed results showed no reduction in death or major disability at 2 years of age. They stated that routine administration of IVIG to prevent mortality in infants with suspected or proven neonatal infection is not recommended.
Noguchi et al (2003) reported on the case of a 62-yearold woman who was admitted to the authors’ hospital because of muscle weakness and sensory disturbance in extremities. She showed weakness, muscle atrophy and sensory abnormality in 4 limbs with patchy distribution, suggesting involvement of multiple peripheral nerve trunks. Serum titers of anti-SS-A, SS-B, and antinuclear antibody were elevated. Sural nerve biopsy showed recanalization and lymphocytic infiltration in the epineural small vessels, suggesting the presence of vasculitis. She was diagnosed as having vasculitic neuropathy complicated with Sjogren's syndrome. Methylprednisolone pulse therapy followed by oral prednisolone was started and these symptoms gradually improved in 1 month. At age 63, she felt dysesthesia in the right lower limb and this sensory abnormality spread to upper limbs. Two years later, she was admitted again due to clumsiness of hands and gait disturbance. Neurological examination showed decreased vibration and position sense of lower limbs and limb ataxia in addition to dysesthesia. Electrophysiological studies demonstrated significant decrease in amplitude of sensory nerve action potentials and delayed somatosensory evoked potentials after N13, indicating impairment of dorsal root ganglions. She was treated with IVIG (400 mg/kg, total 15 g/day) for 5 days. One week later, sensory ataxia was improved. It has been known that Sjogren's syndrome is often complicate with various types of neuropathies including vasculitic neuropathy and sensory neuropathy. This patient developed these 2 different types of neuropathies, which were dramatically improved after 2 different therapeutic regimens; indicating the importance to select a suitable treatment regimen in accordance with the mechanism of neuropathy associated with Sjogren's syndrome.
De Toni Franceschini et al (2011) reported on the case of a 64-year old woman, with asthma and sinusal polyposis in her medical history, who suddenly developed a painful polyneuropathy with diplopia. Nerve conduction studies, performed at the very onset of the neuropathy, could not definitely rule out a Guillain- Barre syndrome (GBS) and high-dose IVIG was administered. Clinical and laboratory findings subsequently supported the diagnosis of Churg-Strauss syndrome; corticosteroid therapy was started and clinical stabilization of neuropathy was apparently achieved. No indicators of unfavorable outcome were present at that time. Nevertheless, 30 days after the onset the patient acutely worsened with severe polyneuropathy relapse and fatal systemic diffusion to heart, kidney and mesenteric district, which a single cyclophosphamide pulse failed to control. The authors stated that this case highlighted the possibility that a GBS-like onset of Churg-Strauss syndrome neuropathy should be regarded as a part of multi-organ, severe or even life-threatening vasculitic involvement, requiring the most aggressive treatments, regardless of the presence of recognized factors of poor outcome.
Moreover, an UpToDate review on “Diagnosis and treatment of vasculitic neuropathy” (Brass and Helfgott, 2013) did not mention the use of IVIG as a therapeutic option.
Parenteral Immunoglobulins Page 20 of 56
04/15/2015
Thus, there is insufficient evidence to support the use of IVIG for the treatment of vasculitic polyneuropathy.
An UpToDate review on “Treatment and prognosis of Waldenstrom macroglobulinemia” (Rajkumar, 2013) does not mention IVIG as a therapeutic option.
The Austrialian National IVIg Criteria Review Working Group (NICRWG)'s guideline on "Criteria for the clinical use of intravenous immunoglobulin" (2012) concluded that the evidence for IVIG for autonomic ganglionopathy is insufficient (level 4a evidence -- small case studies only) and should be used only in exceptional circumstances -- such as in urgent or life-threatening circumstances, or in circumstances in which significant morbidity would be expected and other clinically appropriate standard therapies have been either exhausted or are contraindicated.
Furthermore, a multi-center clinical trial of IVIG for autoimmune autonomic neuropathy is ongoing. https://clinicaltrials.gov/ct2/show/NCT01522235.
Simon et al (2013) evaluated the likelihood of response to IVIG by studying consecutive patients presenting with progressive, asymmetric, pure lower motor neuron (LMN) limb weakness, and determined the clinical phenotype of those who respond. A total of 31 consecutive patients with progressive, focal-onset LMN limb weakness, without evidence of clinical upper motor neuron signs; sensory, respiratory, or bulbar involvement; or evidence of motor nerve conduction block on electrodiagnostic studies, were prospectively included in this study. Each patient underwent treatment with IVIG (2 g/kg body weight) for a minimum of 3 months. Electrodiagnostic studies, a neuromuscular symptom score, and expanded Medical Research Council sum score were documented before and after IVIG treatment. The final diagnosis was determined after prolonged clinical follow-up. Only 3 of 31 patients (10 %) responded to IVIG. All responders demonstrated distal upper limb-onset weakness, EMG abnormalities confined to the clinically weak muscles, and a normal creatine kinase. This set of features was also identified in 31 % of non-responders presenting with distal upper limb weakness. Sex, age at onset, number of involved limb regions, and the duration of symptoms before treatment were not significantly different between groups. The authors concluded that the findings of this study do not support uniform use of IVIG in patients presenting with progressive asymmetric LMN limb weakness. It is suggested that IVIG treatment be limited to patients who demonstrate clinical and laboratory features suggestive of multifocal motor neuropathy. This study provided Class IV evidence that IVIG will not improve muscle function in 90 % of patients with progressive, asymmetric, pure LMN weakness.
McMahan et al (2014) highlighted novel therapies that are being used in SSc. Therapeutic interventions in SSc generally target at least 1 of 3 ongoing biological processes characteristic of the disease: vasculopathy, autoimmunity and tissue fibrosis. Treatment decisions in SSc are determined by the level of disease activity and the degree of specific organ involvement. Traditional therapy has primarily focused on organ-specific management without clear evidence of overall disease modification. The authors provided a review of a variety of agents, which are already used for other autoimmune diseases, that are now being used to treat active SSc skin or lung disease, including rituximab, tocilizumab and IVIG. Several agents studied in-vitro and in animal models of fibrosis have shown promise, including bortezomib, LPA-1 antagonists, anti-CCN2 therapy, anti-IL-13 and thrombin antagonists. The authors also provided details on targeting intracellular molecular pathways and matricellular proteins, which is another novel area of investigation. The authors concluded that combination therapy may be necessary to control the complex biological network active in SSc. They noted that most of the current evidence that suggest benefit of these agents is based on small population studies; ultimately well-designed clinical trials are needed to define the role of these agents in treating SSc.
An UpToDate review on “Overview of the treatment of acute lymphoblastic leukemia in children and adolescents” (Horton and Steuber, 2014) does not mention IVIG as a management tool. Furthermore, the National Comprehensive Cancer Network’s clinical practice guideline on “Acute Lymphoblastic Leukemia” (Version 1.2014) does not mention IVIG as a management toll.
Toledano et al (2014) evaluated a trial of immunotherapy (IT) as an aid to diagnosis in suspected autoimmune epilepsy. These investigators reviewed the charts of 110 patients seen at the authors’ autoimmune neurology clinic with seizures as a chief complaint. A total of 29 patients met the following inclusion criteria: (i) autoimmune epilepsy suspected based on the presence of greater than or equal to 1 neural autoantibody (n = 23), personal or family history or physical stigmata of autoimmunity, and frequent or medically intractable seizures; and (ii) initiated a 6- to 12-week trial of IV methylprednisolone

Parenteral Immunoglobulins Page 21 of 56
04/15/2015
(IVMP), IVIG, or both. Patients were defined as responders if there was a 50 % or greater reduction in seizure frequency. Eighteen patients (62 %) responded, of whom 10 (34 %) became seizure-free; 52 % improved with the first agent. Of those receiving a second agent after not responding to the first, 43 % improved. A favorable response correlated with shorter interval between symptom onset and treatment initiation (median 9.5 versus 22 months; p = 0.048). Responders included 14/16 (87.5 %) patients with antibodies to plasma membrane antigens, 2/6 (33 %) patients seropositive for glutamic acid decarboxylase 65 antibodies, and 2/6 (33 %) patients without detectable antibodies. Of 13 responders followed for more than 6 months after initiating long-term oral immunosuppression, response was sustained in 11 (85 %). The authors concluded that these retrospective findings justified consideration of a trial of IT in patients with suspected autoimmune epilepsy. This study provided Class IV evidence that in patients with suspected autoimmune epilepsy, IVMP, IVIG, or both improve seizure control. The main drawbacks of this study were its small sample size (n = 29), a retrospective design, and the lack of systematic cross-over (from IVMP to IVIG or vice versa). Furthermore, likely confounders such as anti- epileptic drug medication changes during the trial could not be controlled for and non-responders may have been lost to follow-up. The authors stated that a RCT with a cross-over design would help to further specify treatment effect and would limit confounders.
In an editorial that accompanied the afore-mentioned study, Ruegg and Panzer (2014) stated that “These results lay the foundation for a randomized controlled trial of IT in presumed autoimmune epilepsy, which would compare standardized treatment groups, thereby eliminating biases with regards to treatment choice and disease severity. This study should also pave the way for additional prospective studies regarding the natural history of autoimmune PRE [pharmaco-resistant epilepsy] and serves to raise awareness of the role of IT in the treatment of refractory epilepsies”.
Rogosnitzky and colleagues (2012) stated that Crohn's disease (CD) is a debilitating condition that still requires improvement in its management. There is a need for alternatives to anti-tumor necrosis factor (TNF) drugs that are costly and beneficial in less than 50 % of patients. Intravenous immunoglobulin (IVIG) has been used in the management of aminosalicylate- and steroid-resistant CD for more than 20 years, although the published literature available is limited. A literature search identified 17 relevant publications since 1969, including 5 case reports of single patients, 2 abstracts, 3 conference papers, 1 review paper and 6 book or journal articles. No randomized controlled trials (RCTs) of IVIG in CD have been published. A review of the evidence identified indicated that IVIG can induce a rapid and significant improvement in aminosalicylate- and steroid-resistant CD, often within days of the initial administration. Data from longer-term studies showed that maintenance of remission over the medium-term is also possible. The authors concluded that these encouraging findings provided a rationale for the initiation of larger RCTs of IVIG in CD with the aim of providing further treatment options for this difficult-to-manage condition.
Furthermore, UpToDate reviews on "Overview of the medical management of mild to moderate Crohn disease in adults" (Farrell and Peppercorn, 2014a), "Overview of the medical management of severe or refractory Crohn disease in adults" (Farrell and Peppercorn, 2014b) and "Immunomodulator therapy in Crohn disease" (MacDermott, 2014) do not mention the use of IVIG/intravenous immunoglobulin as a therapeutic option.
An UpToDate review on “Approach to the patient with colonic polyps” (Ahnen and Macrae, 2014) states that “Cronkhite-Canada syndrome is a rare, nonfamilial disorder of unknown etiology associated with alopecia, cutaneous hyperpigmentation, gastrointestinal polyposis, onychodystrophy, diarrhea, weight loss, and abdominal pain. The polyps are hamartomas and do not appear neoplastic pathologically. Characteristic features include myxoid expansion of the lamina propria and increased eosinophils in the polyps. There is some evidence that the disorder may be immune-mediated, since it may respond to immunosuppressive therapy and, in some patients, immunostaining of the polyps for IgG4 is positive. Five-year mortality rates as high as 55 percent have been reported with most deaths due to gastrointestinal bleeding, sepsis, and congestive heart failure. Treatment has included nutritional support, glucocorticoids, azathioprine, acid suppression, and antibiotics, but no specific treatment has proven to be consistently effective”. This review does not mention IVIG as a therapeutic option.
Louis et al (2014) stated that IVIG is used in neonates with isoimmune hemolytic disease to prevent exchange transfusion (ET). However, studies supporting IVIG had methodological issues. These researchers updated the systematic review of safety and effectiveness of IVIG in neonates with isoimmune hemolytic disease. MEDLINE, Embase databases and Cochrane Central Register of Controlled Trials (Cochrane Library) were searched (from inception to May 2013) for randomized or
Parenteral Immunoglobulins Page 22 of 56
04/15/2015
quasi-randomized controlled trials comparing IVIG with placebo/controls in neonates with isoimmune hemolytic disease without any language restriction. Three investigators assessed methodological quality of included trials. Meta-analyses were performed using random effect model and risk ratio (RR)/risk difference (RD) and mean difference with 95 % CI calculated. A total of 12 studies were included; 10 trials (n = 463) of Rh isoimmunization and 5 trials (n = 350) of ABO isoimmunization (3 studies had both population). Significant variations in risk of bias precluded an overall meta-analysis of Rh isoimmunization. Studies with high risk of bias showed that IVIG reduced the rate of ET in Rh isoimmunization (RR 0.23, 95 % CI: 0.13 to 0.40), whereas studies with low risk of bias that also used prophylactic phototherapy did not show statistically significant difference (RR 0.82, 95 % CI: 0.53 to 1.26). For ABO isoimmunization, only studies with high risk of bias were available and meta-analysis revealed efficacy of IVIG in reducing ET (RR 0.31, 95 % CI: 0.18 to 0.55). The authors concluded that the effectiveness of IVIG is not conclusive in Rh hemolytic disease of newborn with studies with low risk of bias indicating no benefit and studies with high risk of bias suggesting benefit. They stated that the role of IVIG in ABO disease is not clear as studies that showed a benefit had high risk of bias.
Beken et al (2014) noted that there is still no consensus on the use of IVIG in ABO hemolytic disease of the newborn routinely. These investigators examined if administration of IVIG to newborns with ABO incompatibility is necessary. A total of 117 patients with ABO hemolytic disease and positive Coombs test were enrolled into the study. The subjects were healthy except jaundice. Infants were divided into 2 groups: Group I (n = 71) received 1 dose of IVIG (1 g/kg) and LED phototherapy; and Group II (n = 46) received only LED phototherapy. One patient received erythrocyte transfusion in Group I, no exchange transfusion was performed in both groups. Mean duration of phototherapy was 3.1 ± 1.3 days in Group I and 2.27 ± 0.7 days in Group II (p < 0.05). Mean duration of hospital stay was 5.34 ± 2.2 days in Group I and 3.53 ± 1.3 days in Group II (p < 0.05). Mean duration of phototherapy was 4.0 ± 1.5 days and 2.73 ± 1.1 days in double and single doses of IVIG, respectively, and this was statistically significant (p < 0.05). The authors concluded that IVIG therapy didn't decrease neither phototherapy nor hospitalization duration in infants with ABO hemolytic disease. They stated that meticulous follow-up of infants with ABO hemolytic disease and LED phototherapy decreased morbidity; IVIG failed to show preventing hemolysis in ABO hemolytic disease.
An UpToDate review on “Brachial plexus syndromes” (Bromberg, 2014) does not mention the use of IVIG as a therapeutic option.
UpToDate reviews on “Diagnosis and management of solitary extramedullary plasmacytoma” (Rajkumar, 2014a) and “Diagnosis and management of solitary plasmacytoma of bone” (Rajkumar, 2014b) do not mention IVIG as a therapeutic option.
An UpToDate review on “Postural tachycardia syndrome” (Freeman and Kaufman, 2014) does not mention the use of IVIG as a therapeutic option for POTS.
Parambil and colleagues (2011) noted that small fiber neuropathy (SFN) is commonly associated with sarcoidosis and can cause significant morbidity to afflicted patients. The appropriate treatment of this condition, when associated with sarcoidosis, is not well -established. These investigators presented the findings of case series of 3 patients with sarcoidosis and SFN. The presenting clinical features, skin biopsy results, autonomic reflex screen and quantitative sudomotor axon reflex testing (QSART) findings, and response to therapy are delineated. They described 3 patients with biopsy-proven sarcoidosis who developed intractable neuropathic pain and/or symptoms related to associated autonomic dysfunction despite treatment with various immunosuppressive medications and narcotic analgesics. QSART showed evidence of a post-ganglionic sudomotor abnormality in 1 patient and was normal in the other 2. Skin biopsy findings were abnormal, demonstrating a non-length-dependent sensory SFN in all 3 patients. Painful neuropathic symptoms, as well as symptoms related to dysautonomia from SFN responded significantly to treatment with intravenous immunoglobulin (IVIG). The authors concluded that IVIG appears to be effective in relieving symptoms from SFN associated with sarcoidosis, suggesting an underlying immune mechanism. Moreover, they stated that larger prospective, controlled studies would be needed to confirm this response to IVIG and to further elucidate the underlying pathobiology behind this association with sarcoidosis
Tzekou and Fehlings (2014) stated that neuroinflammation plays an important role in the secondary pathophysiological mechanisms of spinal cord injury (SCI) and can exacerbate the primary trauma and thus worsen recovery. Although some aspects of the immune response are beneficial, it is thought that leukocyte recruitment and activation in the acute phase of injury results in the production of cytotoxic
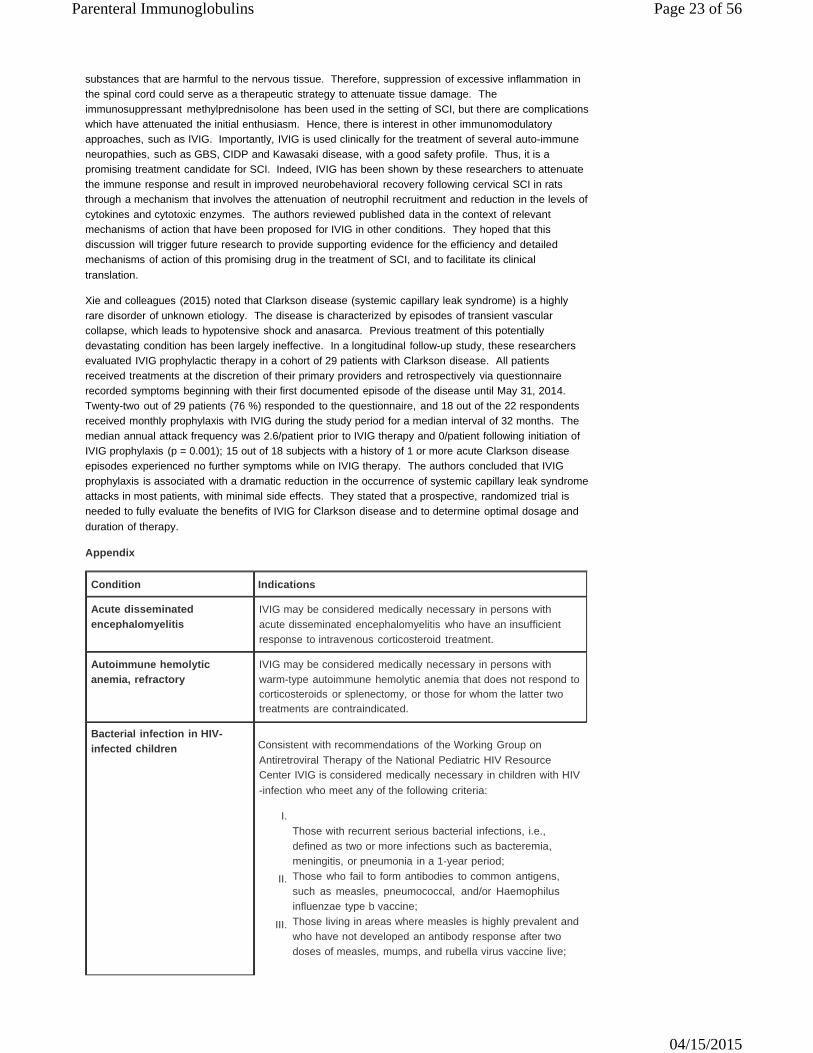
Parenteral Immunoglobulins Page 23 of 56
04/15/2015
substances that are harmful to the nervous tissue. Therefore, suppression of excessive inflammation in the spinal cord could serve as a therapeutic strategy to attenuate tissue damage. The immunosuppressant methylprednisolone has been used in the setting of SCI, but there are complications which have attenuated the initial enthusiasm. Hence, there is interest in other immunomodulatory approaches, such as IVIG. Importantly, IVIG is used clinically for the treatment of several auto-immune neuropathies, such as GBS, CIDP and Kawasaki disease, with a good safety profile. Thus, it is a promising treatment candidate for SCI. Indeed, IVIG has been shown by these researchers to attenuate the immune response and result in improved neurobehavioral recovery following cervical SCI in rats through a mechanism that involves the attenuation of neutrophil recruitment and reduction in the levels of cytokines and cytotoxic enzymes. The authors reviewed published data in the context of relevant mechanisms of action that have been proposed for IVIG in other conditions. They hoped that this discussion will trigger future research to provide supporting evidence for the efficiency and detailed mechanisms of action of this promising drug in the treatment of SCI, and to facilitate its clinical translation.
Xie and colleagues (2015) noted that Clarkson disease (systemic capillary leak syndrome) is a highly rare disorder of unknown etiology. The disease is characterized by episodes of transient vascular collapse, which leads to hypotensive shock and anasarca. Previous treatment of this potentially devastating condition has been largely ineffective. In a longitudinal follow-up study, these researchers evaluated IVIG prophylactic therapy in a cohort of 29 patients with Clarkson disease. All patients received treatments at the discretion of their primary providers and retrospectively via questionnaire recorded symptoms beginning with their first documented episode of the disease until May 31, 2014. Twenty-two out of 29 patients (76 %) responded to the questionnaire, and 18 out of the 22 respondents received monthly prophylaxis with IVIG during the study period for a median interval of 32 months. The median annual attack frequency was 2.6/patient prior to IVIG therapy and 0/patient following initiation of IVIG prophylaxis (p = 0.001); 15 out of 18 subjects with a history of 1 or more acute Clarkson disease episodes experienced no further symptoms while on IVIG therapy. The authors concluded that IVIG prophylaxis is associated with a dramatic reduction in the occurrence of systemic capillary leak syndrome attacks in most patients, with minimal side effects. They stated that a prospective, randomized trial is needed to fully evaluate the benefits of IVIG for Clarkson disease and to determine optimal dosage and duration of therapy.
Appendix
Condition Indications
Acute disseminated encephalomyelitis
IVIG may be considered medically necessary in persons with acute disseminated encephalomyelitis who have an insufficient response to intravenous corticosteroid treatment.
Autoimmune hemolytic anemia, refractory
IVIG may be considered medically necessary in persons with warm-type autoimmune hemolytic anemia that does not respond to corticosteroids or splenectomy, or those for whom the latter two treatments are contraindicated.
Bacterial infection in HIV- infected children Consistent with recommendations of the Working Group on
Antiretroviral Therapy of the National Pediatric HIV Resource Center IVIG is considered medically necessary in children with HIV -infection who meet any of the following criteria:
I.
II.
III.
Those with recurrent serious bacterial infections, i.e., defined as two or more infections such as bacteremia, meningitis, or pneumonia in a 1-year period; Those who fail to form antibodies to common antigens, such as measles, pneumococcal, and/or Haemophilus influenzae type b vaccine; Those living in areas where measles is highly prevalent and who have not developed an antibody response after two doses of measles, mumps, and rubella virus vaccine live;

Parenteral Immunoglobulins Page 24 of 56
04/15/2015
V.
VI.
Single dose for HIV-infected children who are exposed to measles; HIV-infected children with chronic bronchiectasis that is suboptimally responsive to antimicrobial and pulmonary therapy.
Birdshort (vitiligenous) retinochoroidopathy
IVIG is considered medically necessary for birdshot (vitiligenous) retinochoroidopathy that is not responsive to immunosuppressives (e.g., corticosteroids, cyclosporine).
Chronic Inflammatory Demyelinating Polyneuropathy (CIDP), also known as Chronic Relapsing Polyneuropathy, including diabetes mellitus-CIDP and multifocal acquired demyelinating sensory and motor neuropathy (MADSAM) variant
Symmetric or focal neurologic deficits with slowly progressive or relapsing course over 2 months or longer (with neurophysiological abnormalities). Note: A meta-analysis comparing the efficacy if IVIG, plasma exchange, and oral glucocorticoids found equivalence between all three, at least within the first 6 weeks of therapy (Van Schaik et al, 2002). IVIG is considered under accepted guidelines as the preferred treatment, particularly in children, when there is difficulty with venous access for plasmapheresis, and those susceptible to the complications of long-term corticosteroid therapy (Orange et al, 2006). Persons typically respond to IVIG or plasma exchange within the first several weeks of treatment and may demonstrate sustained improvement for many weeks or months. Relapses may require periodic isolated treatments with a single dose of IVIG or single plasma exchange. If a person responds successfully to infrequent booster treatments of either IVIG or plasma exchange, it is considered medically necessary to prescribe maintenance therapy with IVIG to prevent relapse, rather than adding corticosteroids or other immunosuppressants.
Chronic Lymphocytic Leukemia (CLL) in patients
IgG level less than 600 mg/dL; and:
with hypogamma- globulinemia
I. II.
1 severe bacterial infection within preceding 6 months or 2 or more bacterial infections in 1 year; or Evidence of specific antibody deficiency.
Dermatomyositis, Polymyositis(includes Juvenile)
I. Members presenting at least one item from the 1st criterion and four items from the 2nd through 9th criteria are said to have dermatomyositis. Patients presenting no items from the 1st criterion and at least four items from the 2nd through 9th criteria are said to have polymyositis.
A. Skin lesions
1. Heliotrope rash (red purple edematous
erythema on the upper palpebra) 2. Gottron's sign (red purple keratotic, atrophic
erythema, or macules on the extensor surface of finger joints)
3. Erythema on the extensor surface of
extremity joints: slightly raised red purple erythema over elbows or knees
B. Proximal muscle weakness (upper or lower extremity
and trunk)
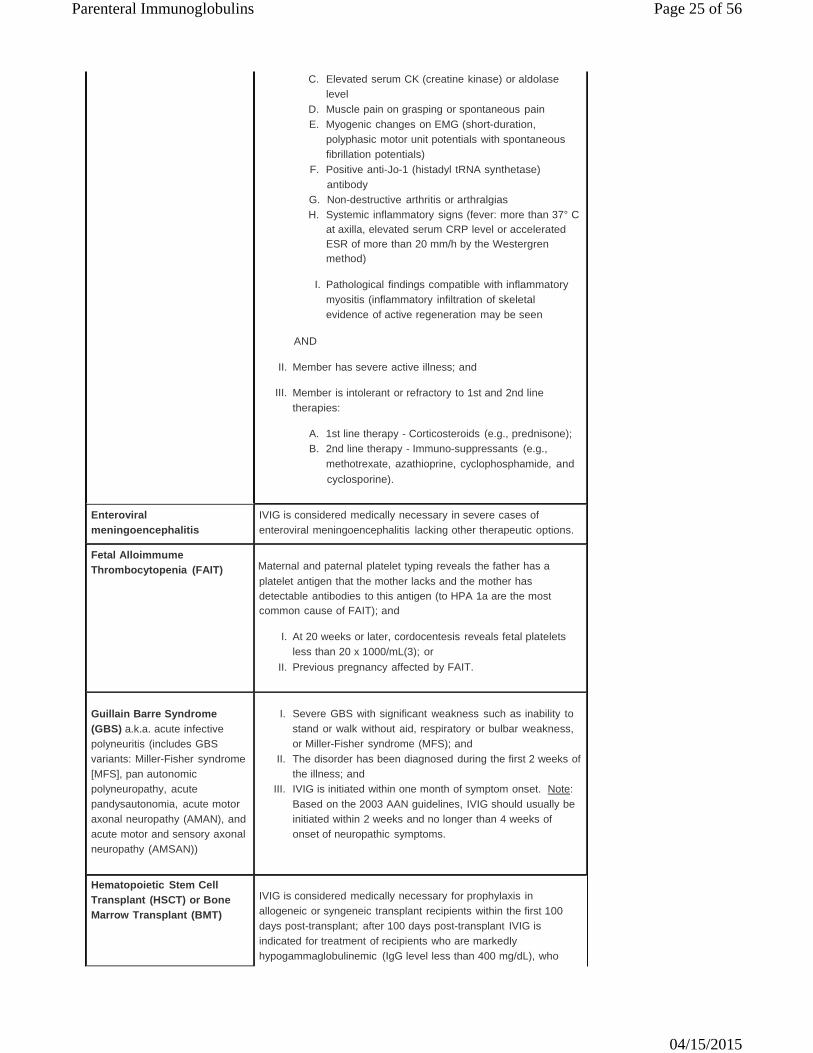
Parenteral Immunoglobulins Page 25 of 56
04/15/2015
C. Elevated serum CK (creatine kinase) or aldolase level
D. Muscle pain on grasping or spontaneous pain E. Myogenic changes on EMG (short-duration,
polyphasic motor unit potentials with spontaneous fibrillation potentials)
F. Positive anti-Jo-1 (histadyl tRNA synthetase) antibody
G. Non-destructive arthritis or arthralgias H. Systemic inflammatory signs (fever: more than 37° C
at axilla, elevated serum CRP level or accelerated ESR of more than 20 mm/h by the Westergren method)
I.
AND
Pathological findings compatible with inflammatory myositis (inflammatory infiltration of skeletal evidence of active regeneration may be seen
II. Member has severe active illness; and
III. Member is intolerant or refractory to 1st and 2nd line
therapies:
A. 1st line therapy - Corticosteroids (e.g., prednisone); B. 2nd line therapy - Immuno-suppressants (e.g.,
methotrexate, azathioprine, cyclophosphamide, and cyclosporine).
Enteroviral meningoencephalitis
IVIG is considered medically necessary in severe cases of enteroviral meningoencephalitis lacking other therapeutic options.
Fetal Alloimmume Thrombocytopenia (FAIT) Maternal and paternal platelet typing reveals the father has a
platelet antigen that the mother lacks and the mother has detectable antibodies to this antigen (to HPA 1a are the most common cause of FAIT); and
I.
II.
At 20 weeks or later, cordocentesis reveals fetal platelets less than 20 x 1000/mL(3); or Previous pregnancy affected by FAIT.
Guillain Barre Syndrome (GBS) a.k.a. acute infective polyneuritis (includes GBS variants: Miller-Fisher syndrome [MFS], pan autonomic polyneuropathy, acute pandysautonomia, acute motor axonal neuropathy (AMAN), and acute motor and sensory axonal neuropathy (AMSAN))
I. II.
III.
Severe GBS with significant weakness such as inability to stand or walk without aid, respiratory or bulbar weakness, or Miller-Fisher syndrome (MFS); and The disorder has been diagnosed during the first 2 weeks of the illness; and IVIG is initiated within one month of symptom onset. Note: Based on the 2003 AAN guidelines, IVIG should usually be initiated within 2 weeks and no longer than 4 weeks of onset of neuropathic symptoms.
Hematopoietic Stem Cell Transplant (HSCT) or Bone Marrow Transplant (BMT)
IVIG is considered medically necessary for prophylaxis in allogeneic or syngeneic transplant recipients within the first 100 days post-transplant; after 100 days post-transplant IVIG is indicated for treatment of recipients who are markedly hypogammaglobulinemic (IgG level less than 400 mg/dL), who
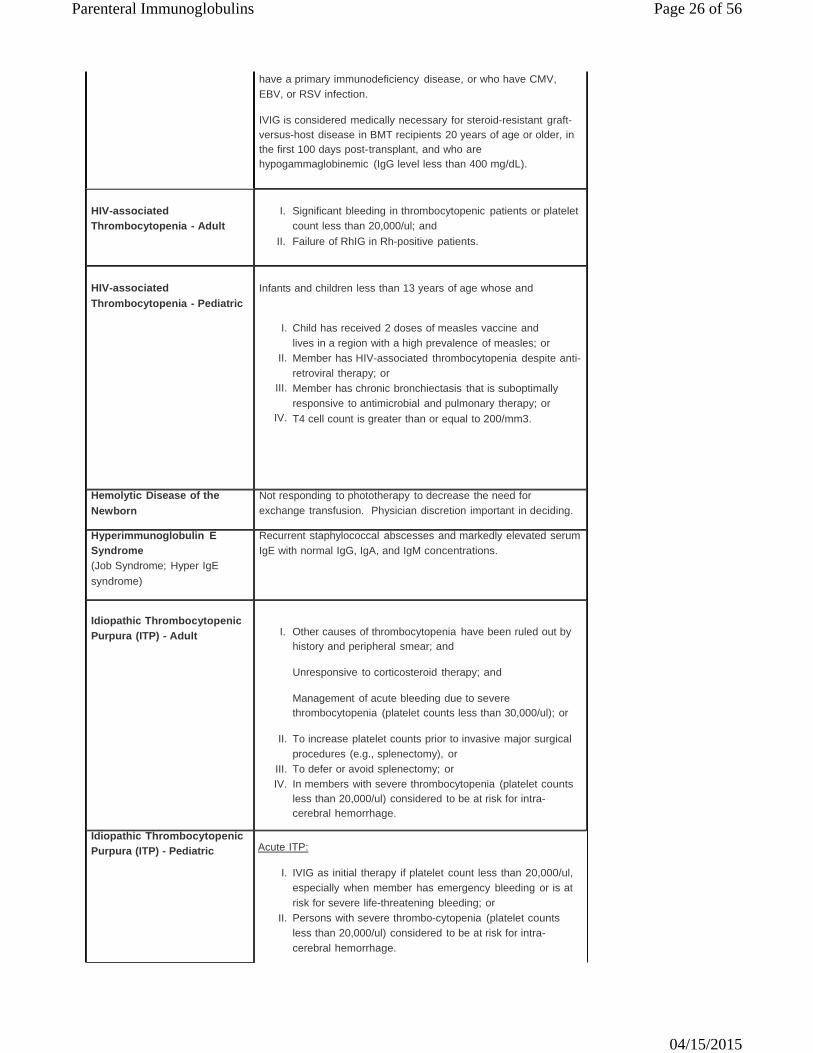
Parenteral Immunoglobulins Page 26 of 56
04/15/2015
have a primary immunodeficiency disease, or who have CMV, EBV, or RSV infection.
IVIG is considered medically necessary for steroid-resistant graft- versus-host disease in BMT recipients 20 years of age or older, in the first 100 days post-transplant, and who are hypogammaglobinemic (IgG level less than 400 mg/dL).
HIV-associated Thrombocytopenia - Adult
I. II.
Significant bleeding in thrombocytopenic patients or platelet count less than 20,000/ul; and Failure of RhIG in Rh-positive patients.
HIV-associated Thrombocytopenia - Pediatric
Infants and children less than 13 years of age whose and
I.
II.
III.
IV.
Child has received 2 doses of measles vaccine and lives in a region with a high prevalence of measles; or Member has HIV-associated thrombocytopenia despite anti- retroviral therapy; or Member has chronic bronchiectasis that is suboptimally responsive to antimicrobial and pulmonary therapy; or T4 cell count is greater than or equal to 200/mm3.
Hemolytic Disease of the Newborn
Not responding to phototherapy to decrease the need for exchange transfusion. Physician discretion important in deciding.
Hyperimmunoglobulin E Syndrome (Job Syndrome; Hyper IgE syndrome)
Recurrent staphylococcal abscesses and markedly elevated serum IgE with normal IgG, IgA, and IgM concentrations.
Idiopathic Thrombocytopenic Purpura (ITP) - Adult
I. Other causes of thrombocytopenia have been ruled out by
history and peripheral smear; and
Unresponsive to corticosteroid therapy; and
Management of acute bleeding due to severe thrombocytopenia (platelet counts less than 30,000/ul); or
II.
III. IV.
To increase platelet counts prior to invasive major surgical procedures (e.g., splenectomy), or To defer or avoid splenectomy; or In members with severe thrombocytopenia (platelet counts less than 20,000/ul) considered to be at risk for intra- cerebral hemorrhage.
Idiopathic Thrombocytopenic Purpura (ITP) - Pediatric Acute ITP:
I.
II.
IVIG as initial therapy if platelet count less than 20,000/ul, especially when member has emergency bleeding or is at risk for severe life-threatening bleeding; or Persons with severe thrombo-cytopenia (platelet counts less than 20,000/ul) considered to be at risk for intra- cerebral hemorrhage.
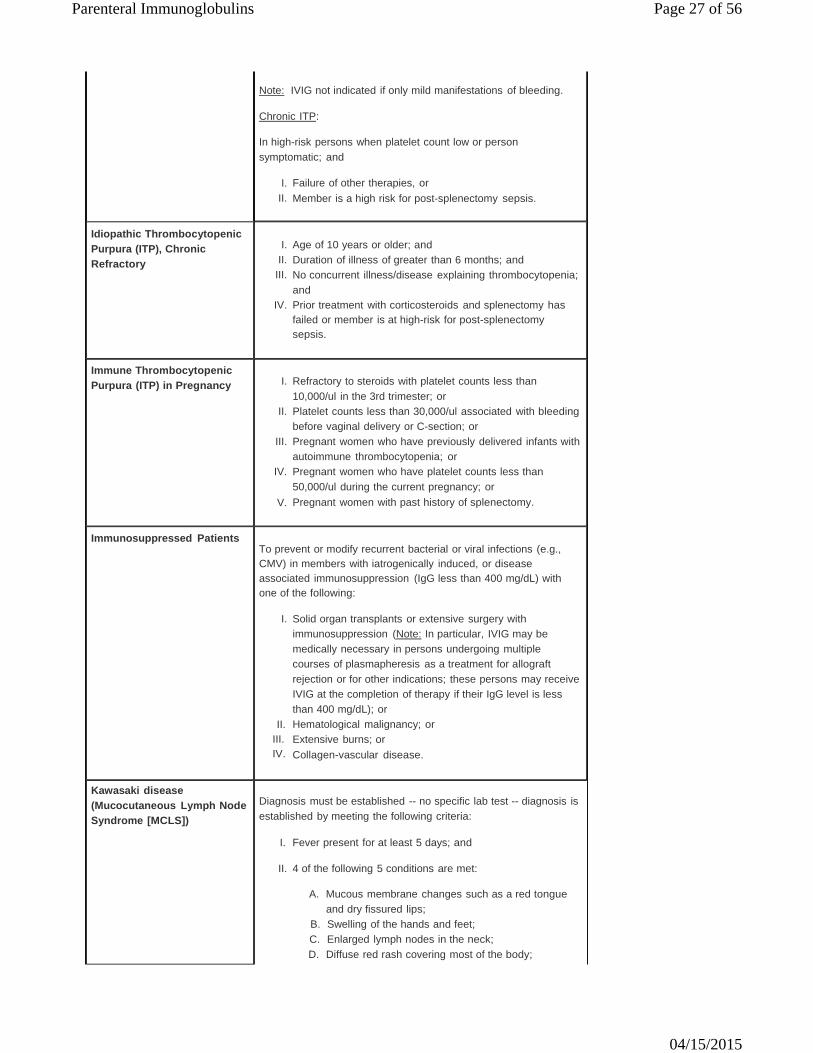
Parenteral Immunoglobulins Page 27 of 56
04/15/2015
Note: IVIG not indicated if only mild manifestations of bleeding.
Chronic ITP:
In high-risk persons when platelet count low or person symptomatic; and
I.
II. Failure of other therapies, or Member is a high risk for post-splenectomy sepsis.
Idiopathic Thrombocytopenic Purpura (ITP), Chronic Refractory
I.
II. III. IV.
Age of 10 years or older; and Duration of illness of greater than 6 months; and No concurrent illness/disease explaining thrombocytopenia; and Prior treatment with corticosteroids and splenectomy has failed or member is at high-risk for post-splenectomy sepsis.
Immune Thrombocytopenic Purpura (ITP) in Pregnancy
I.
II.
III.
IV.
V.
Refractory to steroids with platelet counts less than 10,000/ul in the 3rd trimester; or Platelet counts less than 30,000/ul associated with bleeding before vaginal delivery or C-section; or Pregnant women who have previously delivered infants with autoimmune thrombocytopenia; or Pregnant women who have platelet counts less than 50,000/ul during the current pregnancy; or Pregnant women with past history of splenectomy.
Immunosuppressed Patients
To prevent or modify recurrent bacterial or viral infections (e.g., CMV) in members with iatrogenically induced, or disease associated immunosuppression (IgG less than 400 mg/dL) with one of the following:
I.
II. III. IV.
Solid organ transplants or extensive surgery with immunosuppression (Note: In particular, IVIG may be medically necessary in persons undergoing multiple courses of plasmapheresis as a treatment for allograft rejection or for other indications; these persons may receive IVIG at the completion of therapy if their IgG level is less than 400 mg/dL); or Hematological malignancy; or Extensive burns; or Collagen-vascular disease.
Kawasaki disease (Mucocutaneous Lymph Node Syndrome [MCLS])
Diagnosis must be established -- no specific lab test -- diagnosis is established by meeting the following criteria:
I. Fever present for at least 5 days; and
II. 4 of the following 5 conditions are met:
A. Mucous membrane changes such as a red tongue
and dry fissured lips; B. Swelling of the hands and feet; C. Enlarged lymph nodes in the neck; D. Diffuse red rash covering most of the body;

Parenteral Immunoglobulins Page 28 of 56
04/15/2015
E. Redness of the eyes.
Lambert-Eaton Myasthenic Syndrome (LEMS) No response to anti-cholinesterases and dalfampridine (Ampyra);
and
I.
II.
Used as an alternative to plasma exchange if weakness is severe; or When there is difficulty with venous access for plasmapheresis.
Myasthenia Gravis
Treatment of acute myasthenic crisis with decompensation (respiratory failure, or disabling weakness requiring hospital admission); and other treatments have been unsuccessful or are contraindicated (e.g., azathioprine, cyclosporine, and cyclophosphamide).
Note: For management of myasthenic crises, IVIG is administered over 2 to 5 days. Use of IVIG as maintenance therapy is considered experimental and investigational.
Moersch-Woltmann (Stiff- man) Syndrome
I.
II.
Presence of anti-GAD antibody; and Benzodiazepines (e.g., Valium) and/or baclofen, phenytoin, clonidine, tizanidine have failed.
Multifocal Motor Neuropathy with Conduction Block
Progressive, symptomatic multifocal motor neuropathy that has been diagnosed on the basis of electrophysiologic findings that rule out other possible conditions that may not respond to IVIG treatment.
Multiple Myeloma (MM)
I. II.
III.
"Plateau Phase" MM (greater than 3 months since diagnosis); and IgG level less than 600 mg/dL; and 2 or more significant infections in last year or a single life threatening infection; or
Evidence of specific antibody deficiency.
Multiple Sclerosis (MS) - Relapsing-remitting (not primary or secondary progressive MS)
I.
II.
Severe manifestations of relapsing-remitting MS (not primary or secondary progressive MS); and Standard approaches (i.e., interferons – Betaseron, Avonex, Rebif) have failed, become intolerable, or are contraindicated.
Neonatal Hemochromatosis Treatment of pregnant women who have a history of pregnancy
ended in documented neonatal hemochromatosis. (Note: Dosage should be 1g/kg body weight weekly from the 18th week until the end of gestation).
Neuroblastoma associated paraneoplastic opsoclonus- myoclonus-ataxia syndrome
Treatment of opsoclonus-myoclonus-ataxia associated with neuroblastoma.
Opsoclonus-myoclonus Medically necessary as last-resort treatment for refractory
opsoclonus-myoclonus.
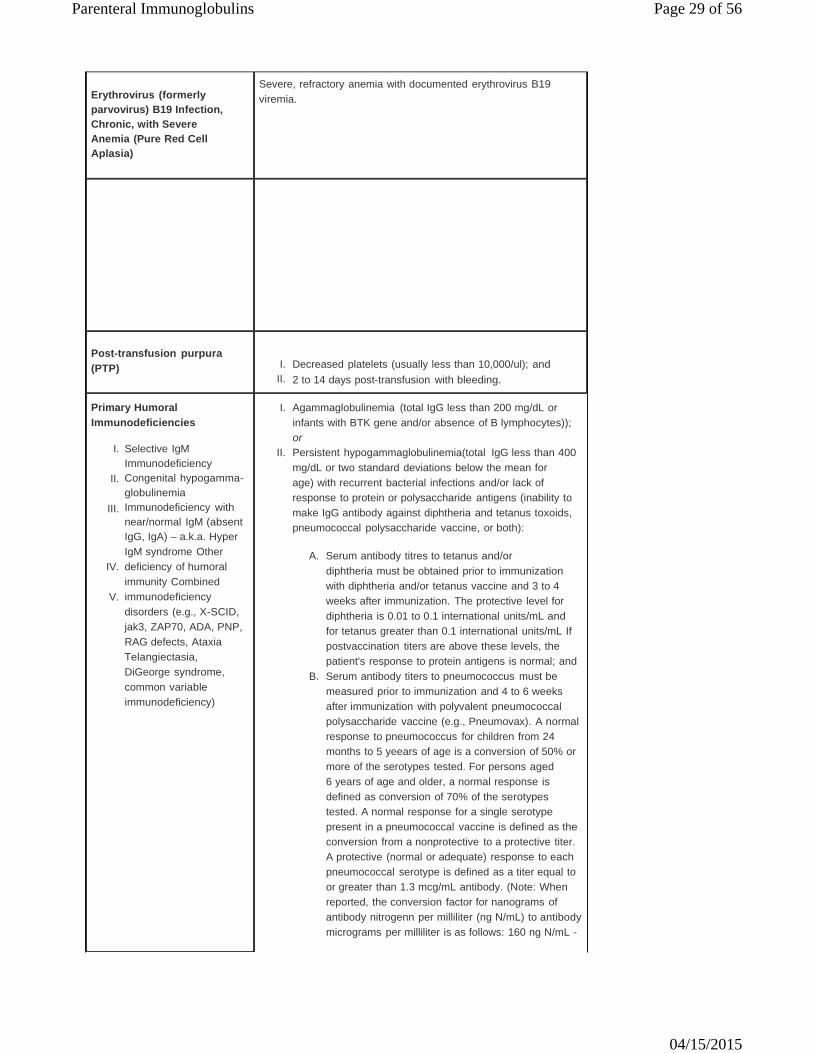
Parenteral Immunoglobulins Page 29 of 56
04/15/2015
Erythrovirus (formerly parvovirus) B19 Infection, Chronic, with Severe Anemia (Pure Red Cell Aplasia)
Severe, refractory anemia with documented erythrovirus B19 viremia.
Post-transfusion purpura (PTP)
I.
II.
Decreased platelets (usually less than 10,000/ul); and 2 to 14 days post-transfusion with bleeding.
Primary Humoral Immunodeficiencies
I. Agammaglobulinemia (total IgG less than 200 mg/dL or infants with BTK gene and/or absence of B lymphocytes)); or
I.
II.
III.
Selective IgM Immunodeficiency Congenital hypogamma- globulinemia Immunodeficiency with near/normal IgM (absent IgG, IgA) – a.k.a. Hyper
II. Persistent hypogammaglobulinemia(total IgG less than 400 mg/dL or two standard deviations below the mean for age) with recurrent bacterial infections and/or lack of response to protein or polysaccharide antigens (inability to make IgG antibody against diphtheria and tetanus toxoids, pneumococcal polysaccharide vaccine, or both):
IV.
V.
IgM syndrome Other deficiency of humoral immunity Combined immunodeficiency disorders (e.g., X-SCID, jak3, ZAP70, ADA, PNP, RAG defects, Ataxia Telangiectasia, DiGeorge syndrome, common variable immunodeficiency)
A. Serum antibody titres to tetanus and/or diphtheria must be obtained prior to immunization with diphtheria and/or tetanus vaccine and 3 to 4 weeks after immunization. The protective level for diphtheria is 0.01 to 0.1 international units/mL and for tetanus greater than 0.1 international units/mL If postvaccination titers are above these levels, the patient's response to protein antigens is normal; and
B. Serum antibody titers to pneumococcus must be measured prior to immunization and 4 to 6 weeks after immunization with polyvalent pneumococcal polysaccharide vaccine (e.g., Pneumovax). A normal response to pneumococcus for children from 24 months to 5 yeears of age is a conversion of 50% or more of the serotypes tested. For persons aged 6 years of age and older, a normal response is defined as conversion of 70% of the serotypes tested. A normal response for a single serotype present in a pneumococcal vaccine is defined as the conversion from a nonprotective to a protective titer. A protective (normal or adequate) response to each pneumococcal serotype is defined as a titer equal to or greater than 1.3 mcg/mL antibody. (Note: When reported, the conversion factor for nanograms of antibody nitrogenn per milliliter (ng N/mL) to antibody micrograms per milliliter is as follows: 160 ng N/mL -

Parenteral Immunoglobulins Page 30 of 56
04/15/2015
1.0 mcg/mL); or
III.
IV.
Selective IgG subclass deficiencies (see criteria in section of selective IgG subclass deficiency below); or Normal total IgG levels with severe polysaccharide non- responsiveness and evidence of recurrent severe difficult-to -treat infections (e.g., recurrent otitis media, bronchiectasis, recurrent infections requiring IV antibiotics, multiple antibiotic hypersensitivities, chronic or recurrent sinusitis) (see table below) with a documented requirement for antibiotic therapy:
A. Member has unexplained recurrent or persistent
severe bacterial infections despite adequate treatment, including all of the following:
1. Aggressive management of other conditions
predisposing to recurrent sinopulmonary infections (e.g., asthma, allergic rhinitis);
2. Prophylactic antibiotics; 3. Increased vigilance and appropriate antibiotic
therapy for infections; and 4. Immunization with conjugate vaccines in
patients who have not responded to polysaccharide vaccines.
B. Serum antibody titers to pneumococcus must be
measured prior to immunization and 4 to 6 weeks after immunization with polyvalent pneumococcal polysaccharide vaccine (e.g., Pneumovax); at least 14 polysaccharide antigens must be tested.
C. Polysaccharide non-responsiveness is defined as lack of protective antibody titer (specific IgG antibody titer less than 1.3 mcg/ml) in greater than 70 % of antigens tested (more than 50 % in children aged 2 to 5 years).
D. Further evidence of infection, including sinus and lung imaging, complete blood counts, C-reactive protein measurement, and erythrocyte sedimentation rate determination, may be required to support the need for IVIG supplementation.
E. For children 12 years of age or younger with normal total IgG levels and severe polysaccharide nonresponsiveness, IVIG must be discontinued and the medical necessity of IVIG re-evaluated 1 year after initiating therapy and every 2 years thereafter by reassessing immune response to protein and polysaccharide antigens. Immune response must be re-evaluated at least 3 months after discontinuation of IVIG. IVIG must also be discontinued at that time if the number and/or severity of infections have not been reduced, as not all persons with polysaccharide nonresponsiveness benefit from IVIG.
The use of IVIG may not be medically necessary in certain secondary immunodeficiency states; correction of the underlying condition is the preferred approach.
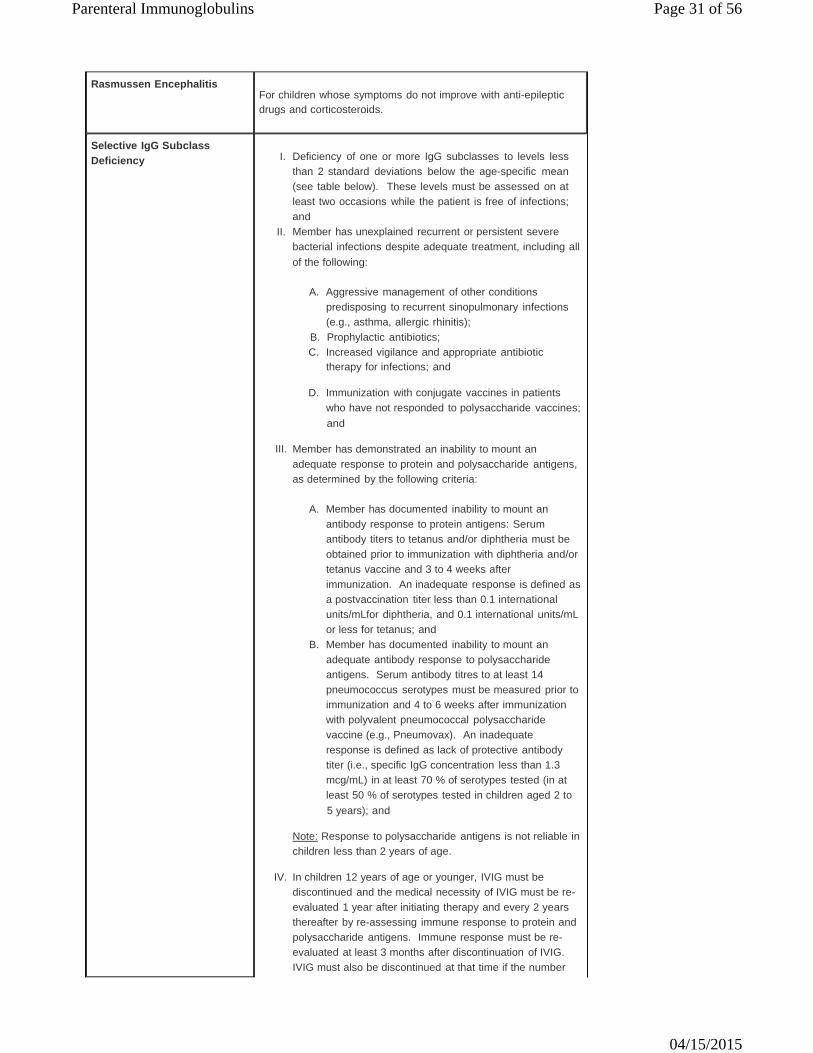
Parenteral Immunoglobulins Page 31 of 56
04/15/2015
Rasmussen Encephalitis For children whose symptoms do not improve with anti-epileptic drugs and corticosteroids.
Selective IgG Subclass Deficiency
I.
II.
Deficiency of one or more IgG subclasses to levels less than 2 standard deviations below the age-specific mean (see table below). These levels must be assessed on at least two occasions while the patient is free of infections; and Member has unexplained recurrent or persistent severe bacterial infections despite adequate treatment, including all of the following:
A. Aggressive management of other conditions
predisposing to recurrent sinopulmonary infections (e.g., asthma, allergic rhinitis);
B. Prophylactic antibiotics; C. Increased vigilance and appropriate antibiotic
therapy for infections; and
D. Immunization with conjugate vaccines in patients who have not responded to polysaccharide vaccines; and
III. Member has demonstrated an inability to mount an
adequate response to protein and polysaccharide antigens, as determined by the following criteria:
A. Member has documented inability to mount an
antibody response to protein antigens: Serum antibody titers to tetanus and/or diphtheria must be obtained prior to immunization with diphtheria and/or tetanus vaccine and 3 to 4 weeks after immunization. An inadequate response is defined as a postvaccination titer less than 0.1 international units/mLfor diphtheria, and 0.1 international units/mL or less for tetanus; and
B. Member has documented inability to mount an adequate antibody response to polysaccharide antigens. Serum antibody titres to at least 14 pneumococcus serotypes must be measured prior to immunization and 4 to 6 weeks after immunization with polyvalent pneumococcal polysaccharide vaccine (e.g., Pneumovax). An inadequate response is defined as lack of protective antibody titer (i.e., specific IgG concentration less than 1.3 mcg/mL) in at least 70 % of serotypes tested (in at least 50 % of serotypes tested in children aged 2 to 5 years); and
Note: Response to polysaccharide antigens is not reliable in children less than 2 years of age.
IV. In children 12 years of age or younger, IVIG must be
discontinued and the medical necessity of IVIG must be re- evaluated 1 year after initiating therapy and every 2 years thereafter by re-assessing immune response to protein and polysaccharide antigens. Immune response must be re- evaluated at least 3 months after discontinuation of IVIG. IVIG must also be discontinued at that time if the number
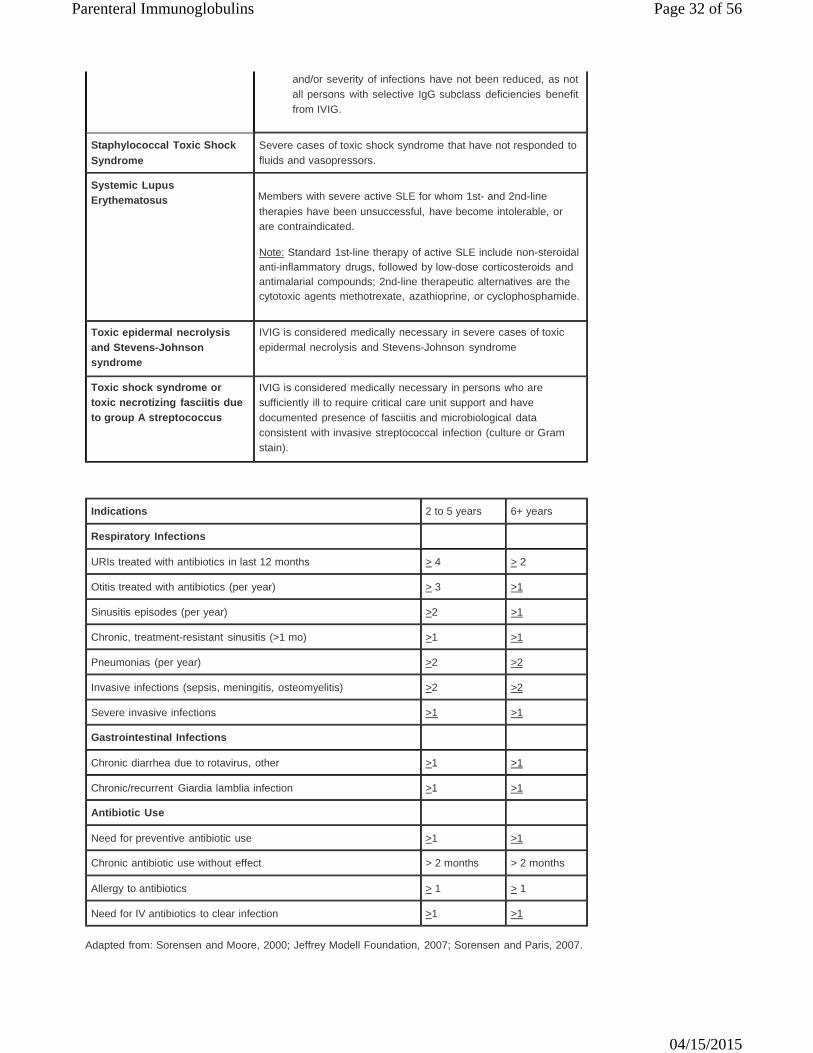
Parenteral Immunoglobulins Page 32 of 56
04/15/2015
and/or severity of infections have not been reduced, as not all persons with selective IgG subclass deficiencies benefit from IVIG.
Staphylococcal Toxic Shock Syndrome
Severe cases of toxic shock syndrome that have not responded to fluids and vasopressors.
Systemic Lupus Erythematosus Members with severe active SLE for whom 1st- and 2nd-line
therapies have been unsuccessful, have become intolerable, or are contraindicated.
Note: Standard 1st-line therapy of active SLE include non-steroidal anti-inflammatory drugs, followed by low-dose corticosteroids and antimalarial compounds; 2nd-line therapeutic alternatives are the cytotoxic agents methotrexate, azathioprine, or cyclophosphamide.
Toxic epidermal necrolysis and Stevens-Johnson syndrome
IVIG is considered medically necessary in severe cases of toxic epidermal necrolysis and Stevens-Johnson syndrome
Toxic shock syndrome or toxic necrotizing fasciitis due to group A streptococcus
IVIG is considered medically necessary in persons who are sufficiently ill to require critical care unit support and have documented presence of fasciitis and microbiological data consistent with invasive streptococcal infection (culture or Gram stain).
Indications 2 to 5 years 6+ years
Respiratory Infections
URIs treated with antibiotics in last 12 months > 4 > 2
Otitis treated with antibiotics (per year) > 3 >1
Sinusitis episodes (per year) >2 >1
Chronic, treatment-resistant sinusitis (>1 mo) >1 >1
Pneumonias (per year) >2 >2
Invasive infections (sepsis, meningitis, osteomyelitis) >2 >2
Severe invasive infections >1 >1
Gastrointestinal Infections
Chronic diarrhea due to rotavirus, other >1 >1
Chronic/recurrent Giardia lamblia infection >1 >1
Antibiotic Use
Need for preventive antibiotic use >1 >1
Chronic antibiotic use without effect > 2 months > 2 months
Allergy to antibiotics > 1 > 1
Need for IV antibiotics to clear infection >1 >1
Adapted from: Sorensen and Moore, 2000; Jeffrey Modell Foundation, 2007; Sorensen and Paris, 2007.
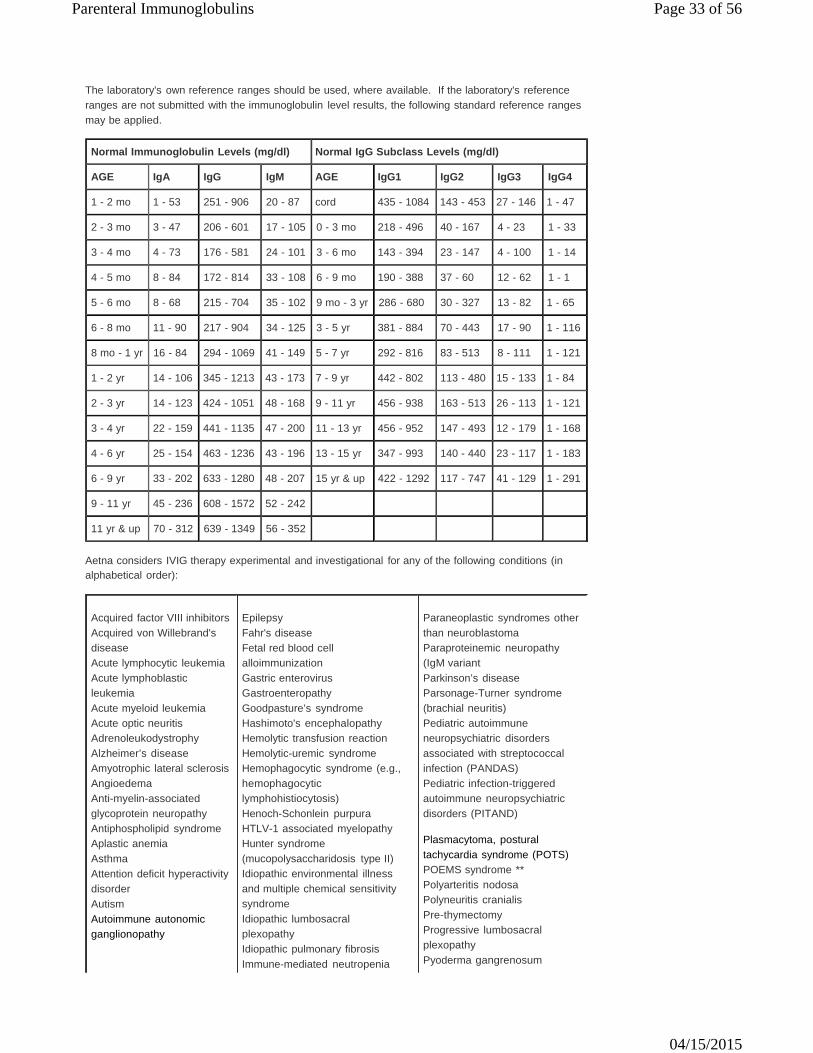
Parenteral Immunoglobulins Page 33 of 56
04/15/2015
The laboratory's own reference ranges should be used, where available. If the laboratory's reference ranges are not submitted with the immunoglobulin level results, the following standard reference ranges may be applied.
Normal Immunoglobulin Levels (mg/dl) Normal IgG Subclass Levels (mg/dl)
AGE IgA IgG IgM AGE IgG1 IgG2 IgG3 IgG4
1 - 2 mo 1 - 53 251 - 906 20 - 87 cord 435 - 1084 143 - 453 27 - 146 1 - 47
2 - 3 mo 3 - 47 206 - 601 17 - 105 0 - 3 mo 218 - 496 40 - 167 4 - 23 1 - 33
3 - 4 mo 4 - 73 176 - 581 24 - 101 3 - 6 mo 143 - 394 23 - 147 4 - 100 1 - 14
4 - 5 mo 8 - 84 172 - 814 33 - 108 6 - 9 mo 190 - 388 37 - 60 12 - 62 1 - 1
5 - 6 mo 8 - 68 215 - 704 35 - 102 9 mo - 3 yr 286 - 680 30 - 327 13 - 82 1 - 65
6 - 8 mo 11 - 90 217 - 904 34 - 125 3 - 5 yr 381 - 884 70 - 443 17 - 90 1 - 116
8 mo - 1 yr 16 - 84 294 - 1069 41 - 149 5 - 7 yr 292 - 816 83 - 513 8 - 111 1 - 121
1 - 2 yr 14 - 106 345 - 1213 43 - 173 7 - 9 yr 442 - 802 113 - 480 15 - 133 1 - 84
2 - 3 yr 14 - 123 424 - 1051 48 - 168 9 - 11 yr 456 - 938 163 - 513 26 - 113 1 - 121
3 - 4 yr 22 - 159 441 - 1135 47 - 200 11 - 13 yr 456 - 952 147 - 493 12 - 179 1 - 168
4 - 6 yr 25 - 154 463 - 1236 43 - 196 13 - 15 yr 347 - 993 140 - 440 23 - 117 1 - 183
6 - 9 yr 33 - 202 633 - 1280 48 - 207 15 yr & up 422 - 1292 117 - 747 41 - 129 1 - 291
9 - 11 yr 45 - 236 608 - 1572 52 - 242
11 yr & up 70 - 312 639 - 1349 56 - 352
Aetna considers IVIG therapy experimental and investigational for any of the following conditions (in alphabetical order):
Acquired factor VIII inhibitors Acquired von Willebrand's disease Acute lymphocytic leukemia Acute lymphoblastic leukemia Acute myeloid leukemia Acute optic neuritis Adrenoleukodystrophy Alzheimer’s disease Amyotrophic lateral sclerosis Angioedema Anti-myelin-associated glycoprotein neuropathy Antiphospholipid syndrome Aplastic anemia Asthma Attention deficit hyperactivity disorder Autism Autoimmune autonomic ganglionopathy
Epilepsy Fahr's disease Fetal red blood cell alloimmunization Gastric enterovirus Gastroenteropathy Goodpasture’s syndrome Hashimoto's encephalopathy Hemolytic transfusion reaction Hemolytic-uremic syndrome Hemophagocytic syndrome (e.g., hemophagocytic lymphohistiocytosis) Henoch-Schonlein purpura HTLV-1 associated myelopathy Hunter syndrome (mucopolysaccharidosis type II) Idiopathic environmental illness and multiple chemical sensitivity syndrome Idiopathic lumbosacral plexopathy Idiopathic pulmonary fibrosis Immune-mediated neutropenia
Paraneoplastic syndromes other than neuroblastoma Paraproteinemic neuropathy (IgM variant Parkinson’s disease Parsonage-Turner syndrome (brachial neuritis) Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS) Pediatric infection-triggered autoimmune neuropsychiatric disorders (PITAND) Plasmacytoma, postural tachycardia syndrome (POTS) POEMS syndrome ** Polyarteritis nodosa Polyneuritis cranialis Pre-thymectomy Progressive lumbosacral plexopathy Pyoderma gangrenosum

Parenteral Immunoglobulins Page 34 of 56
04/15/2015
Autoimmune autonomic neuropathy Autoimmune bullous skin diseases Autoimmune chronic urticaria Autoimmune encephalopathy
Autoimmune epilepsy Autoimmune inner ear disease Autoimmune liver disease Behçet's syndrome Burkitt’s lymphoma Cardiomyopathy, acute Chronic fatigue syndrome Chronic myelogenous leukemia Chronic sinusitis Clarkson disease (systemic capillary leak syndrome)
Clostridium difficile colitis Complex regional pain syndrome Congenital factor VII deficiency Congenital heart block Convulsive syndromes Critical illness polyneuropathy Crohn's disease
Cronkhite-Canada syndrome
Cystic fibrosis Degos disease Depression Dermatosis, autoimmune blistering Diabetes mellitus Diabetic amyotrophy Diffuse alveolar hemorrhage Dravet's syndrome Diamond-Blackfan anemia Dysautonomia, acute idiopathic Eczema Encephalopathy Endotoxemia
Immune reconstitution Inclusion body myositis Infertility Intractable seizures Isaacs syndrome Isoimmune hemolytic disease Landau-Kleffner syndrome Langerhans cell histiocytosis Leukemia, acute lymphoblastic Limbic encephalitis Lipidosis Lower motor neuron syndrome Malignancy, non-hematologic Mannose-binding lectin deficiency Maternal autoantibody-mediated cardiomyopathy Mitochondrial encephalopathy Multiple sclerosis - primary progressive or secondary types Myalgia, myositis, unspecified Myalgic encephalomyelitis Myelopathy, HTLV-I associated Necrotizing enterocolitis Neonatal lupus syndromes Neonatal sepsis (treatment) Neonatal sepsis (prophylaxis) Nephritic syndrome Nephropathy, membranous Nephrotic syndrome Neuromyelitis optica (Devic’s disease) Neuromyotonia (Isaacs’ syndrome) Neurosarcoidosis Nodular (follicular) lymphoma Obsessive-compulsive disorder Ophthalmopathy, euthyroid Oral use of IVIG for any indication Orthostatic tachycardia syndrome Otitis media, recurrent Paraneoplastic cerebellar degeneration
Radiculoneuritis, Lyme Recurrent otitis media Recurrent fetal/pregnancy loss Red cell aplasia not due to erythrovirus B19 Reducing the risk of post-partum exacerbation of multiple sclerosis Relapsing polychondritis Rheumatic fever, carditis Refractoriness to platelet transfusion Reiter's syndrome Renal failure, acute Rheumatoid arthritis (adult and juvenile) Scleroderma Selective isolated IgA immunodeficiency Sensory neuropathy SICCA syndrome/Sjogren's syndrome Small fiber neuropathy associated with sarcoidosis Solar urticaria Spinal cord injury Still's disease Suspected or proven infection in neonates Sydenham's chorea Systemic vasculitides Thrombocytopenia (non- immune, e.g., heparin-induced) Thrombotic thrombocytopenic purpura (TTP) Tic disorders Transverse myelopathy/myelitis Uveitis Vasculitic polyneuropathy Vasculitis associated with other connective tissue diseases Viral myocarditis Vogt-Koyanagi-Harada syndrome Waldenstrom macroglobulinemia Wegener’s granulomatosis
** The term "POEMS" is actually an acronym for the most common symptoms and signs of the syndrome: "P" - peripheral neuropathy (numbness, tingling, and weakness of the feet and hands); “O” - organomegaly (large organs, like the liver, lymph nodes and spleen); "E" - endocrinopathy (abnormal hormone levels including sex hormones, thyroid hormones, etc.); "M" - monoclonal plasma-proliferative disorder (a collection of abnormal bone marrow cells, called plasma cells); most patients will have at least on abnormal bone x-ray associated with these plasma cells; "S" - skin changes (increased skin pigment, increased body hair, thickening of the skin, etc).
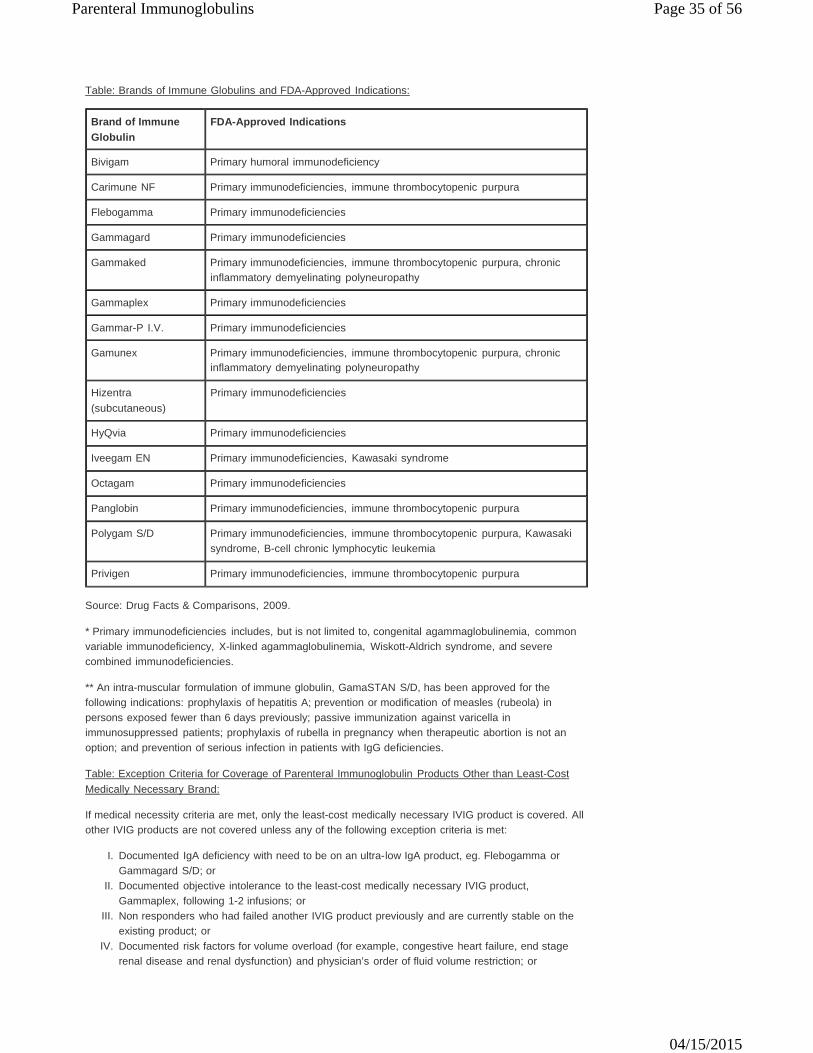
Parenteral Immunoglobulins Page 35 of 56
04/15/2015
Table: Brands of Immune Globulins and FDA-Approved Indications:
Brand of Immune Globulin
FDA-Approved Indications
Bivigam Primary humoral immunodeficiency
Carimune NF Primary immunodeficiencies, immune thrombocytopenic purpura
Flebogamma Primary immunodeficiencies
Gammagard Primary immunodeficiencies
Gammaked Primary immunodeficiencies, immune thrombocytopenic purpura, chronic
inflammatory demyelinating polyneuropathy
Gammaplex Primary immunodeficiencies
Gammar-P I.V. Primary immunodeficiencies
Gamunex Primary immunodeficiencies, immune thrombocytopenic purpura, chronic inflammatory demyelinating polyneuropathy
Hizentra (subcutaneous)
Primary immunodeficiencies
HyQvia Primary immunodeficiencies
Iveegam EN Primary immunodeficiencies, Kawasaki syndrome
Octagam Primary immunodeficiencies
Panglobin Primary immunodeficiencies, immune thrombocytopenic purpura
Polygam S/D Primary immunodeficiencies, immune thrombocytopenic purpura, Kawasaki
syndrome, B-cell chronic lymphocytic leukemia
Privigen Primary immunodeficiencies, immune thrombocytopenic purpura
Source: Drug Facts & Comparisons, 2009.
* Primary immunodeficiencies includes, but is not limited to, congenital agammaglobulinemia, common variable immunodeficiency, X-linked agammaglobulinemia, Wiskott-Aldrich syndrome, and severe combined immunodeficiencies.
** An intra-muscular formulation of immune globulin, GamaSTAN S/D, has been approved for the following indications: prophylaxis of hepatitis A; prevention or modification of measles (rubeola) in persons exposed fewer than 6 days previously; passive immunization against varicella in immunosuppressed patients; prophylaxis of rubella in pregnancy when therapeutic abortion is not an option; and prevention of serious infection in patients with IgG deficiencies.
Table: Exception Criteria for Coverage of Parenteral Immunoglobulin Products Other than Least-Cost Medically Necessary Brand:
If medical necessity criteria are met, only the least-cost medically necessary IVIG product is covered. All other IVIG products are not covered unless any of the following exception criteria is met:
I.
II.
III.
IV.
Documented IgA deficiency with need to be on an ultra-low IgA product, eg. Flebogamma or Gammagard S/D; or Documented objective intolerance to the least-cost medically necessary IVIG product, Gammaplex, following 1-2 infusions; or Non responders who had failed another IVIG product previously and are currently stable on the existing product; or Documented risk factors for volume overload (for example, congestive heart failure, end stage renal disease and renal dysfunction) and physician’s order of fluid volume restriction; or
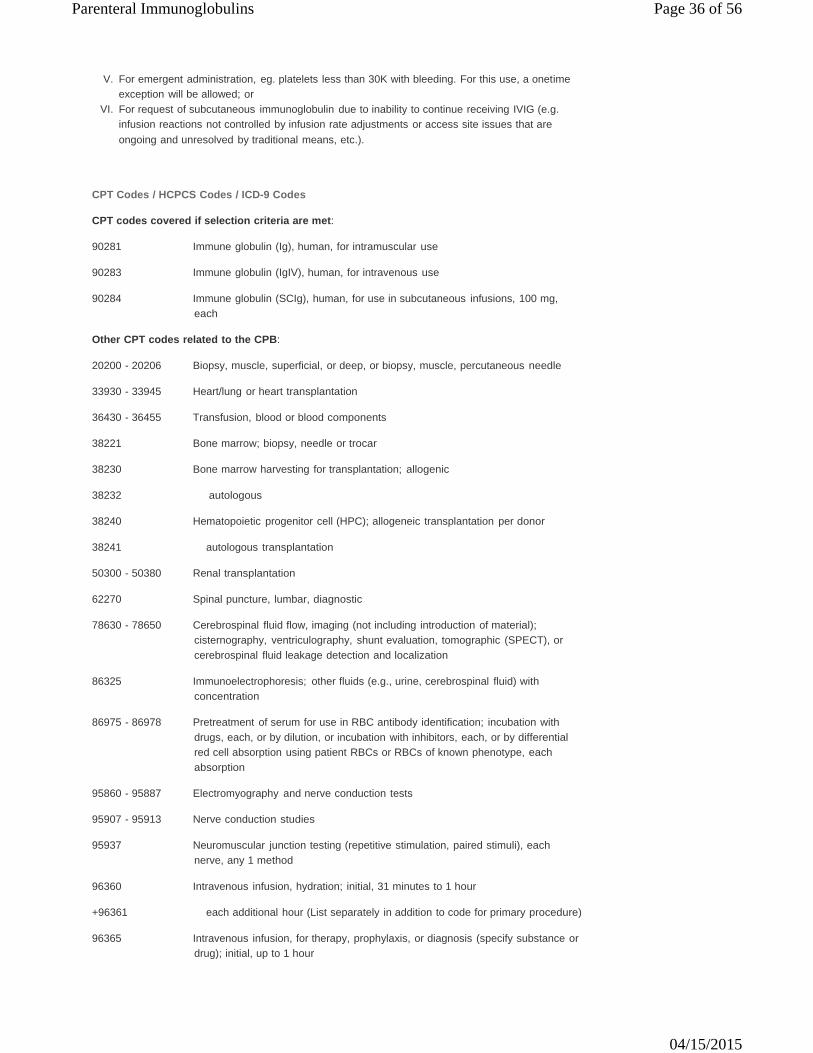
Parenteral Immunoglobulins Page 36 of 56
04/15/2015
V.
VI.
For emergent administration, eg. platelets less than 30K with bleeding. For this use, a onetime exception will be allowed; or For request of subcutaneous immunoglobulin due to inability to continue receiving IVIG (e.g. infusion reactions not controlled by infusion rate adjustments or access site issues that are ongoing and unresolved by traditional means, etc.).
CPT Codes / HCPCS Codes / ICD-9 Codes
CPT codes covered if selection criteria are met:
90281 Immune globulin (Ig), human, for intramuscular use
90283 Immune globulin (IgIV), human, for intravenous use
90284 Immune globulin (SCIg), human, for use in subcutaneous infusions, 100 mg, each
Other CPT codes related to the CPB:
20200 - 20206 Biopsy, muscle, superficial, or deep, or biopsy, muscle, percutaneous needle
33930 - 33945 Heart/lung or heart transplantation
36430 - 36455 Transfusion, blood or blood components
38221 Bone marrow; biopsy, needle or trocar
38230 Bone marrow harvesting for transplantation; allogenic
38232 autologous
38240 Hematopoietic progenitor cell (HPC); allogeneic transplantation per donor
38241 autologous transplantation
50300 - 50380 Renal transplantation
62270 Spinal puncture, lumbar, diagnostic
78630 - 78650 Cerebrospinal fluid flow, imaging (not including introduction of material);
cisternography, ventriculography, shunt evaluation, tomographic (SPECT), or cerebrospinal fluid leakage detection and localization
86325 Immunoelectrophoresis; other fluids (e.g., urine, cerebrospinal fluid) with
concentration
86975 - 86978 Pretreatment of serum for use in RBC antibody identification; incubation with drugs, each, or by dilution, or incubation with inhibitors, each, or by differential red cell absorption using patient RBCs or RBCs of known phenotype, each absorption
95860 - 95887 Electromyography and nerve conduction tests
95907 - 95913 Nerve conduction studies
95937 Neuromuscular junction testing (repetitive stimulation, paired stimuli), each
nerve, any 1 method
96360 Intravenous infusion, hydration; initial, 31 minutes to 1 hour
+96361 each additional hour (List separately in addition to code for primary procedure)
96365 Intravenous infusion, for therapy, prophylaxis, or diagnosis (specify substance or drug); initial, up to 1 hour

Parenteral Immunoglobulins Page 37 of 56
04/15/2015
+96366 each additional hour (List separately in addition to code for primary procedure)
+96367 additional sequential infusion of a new drug/substance, up to 1 hour (list separately in addition to code for primary procedure)
+96368 concurrent infusion (List separately in addition to code for primary procedure
96369 Subcutaneous infusion for therapy or prophylaxis (specify substance or drug);
initial, up to 1 hour, including pump set-up and establishment of subcutaneous infusion site(s)
+96370 each additional hour (List separately in addition to code for primary procedure
+96371 additional pump set-up with establishment of new subcutaneous infusion site
(s) (List separately in addition to code for primary procedure)
HCPCS codes covered if selection criteria are met:
J1459 Injection, immune globulin (Privigen), intravenous, nonlyophilized (e.g., liquid), 500 mg
J1556 Injection, immune globulin (bivigam), 500 mg
J1557 Injection, immune globulin, (gammaplex), intravenous, non-lyophilized (e.g.,
liquid), 500 mg
J1559 Injection, immune globulin (hizentra), 100 mg
J1561 Injection, immune globulin, (Gamunex/Gamunex-C/Gammaked), nonlyophilized (e.g., liquid), 500 mg
J1566 Injection, immune globulin, intravenous, lyophilized (e.g., powder), not otherwise
specified, 500 mg
J1568 Injection, immune globulin, (Octagam), intravenous, nonlyophilized (e.g., liquid), 500 mg
J1569 Injection, immune globulin, (Gammagard liquid), nonlyophilized, (e.g., liquid),
500 mg
J1572 Injection, immune globulin, (Flebogamma / Flebogamma Dif), intravenous, nonlyophilized (e.g., liquid), 500 mg
J1599 Injection, immune globulin, intravenous, non-lyophilized (eg, liquid), not
otherwise specified, 500 mg
Other HCPCS codes related to the CPB:
J1830 Injection interferon beta-1b, 0.25 mg
J9212 - J9216 Injection, interferon alfacon-1, recombinant, 1 mcg, interferon alfa-2a, recombinant, 3 million units, interferon alfa-2b, recombinant, 1 million units, interferon alfa-N3, (human leukocyte derived), 250,000 IU, or interferon gamma- 1b, 3 million units
Q3027 Injection, interferon beta-1a, 1 mcg for intramuscular use
S9338 Home infusion therapy, immunotherapy, administrative services, professional
pharmacy services, care coordination, and all necessary supplies and equipment (drugs and nursing visits coded separately), per diem
ICD-9 codes covered if selection criteria are met:
040.82 Toxic shock syndrome
041.01 Infection streptococcus, group A
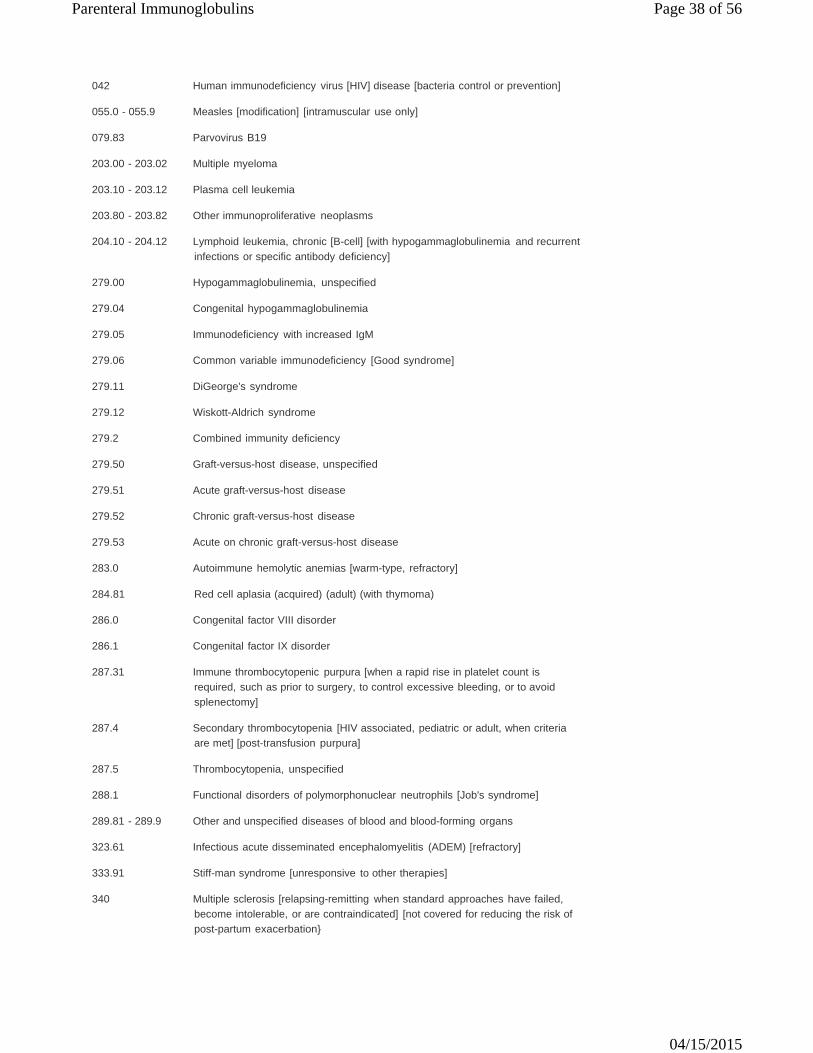
Parenteral Immunoglobulins Page 38 of 56
04/15/2015
042 Human immunodeficiency virus [HIV] disease [bacteria control or prevention]
055.0 - 055.9 Measles [modification] [intramuscular use only]
079.83 Parvovirus B19
203.00 - 203.02 Multiple myeloma
203.10 - 203.12 Plasma cell leukemia
203.80 - 203.82 Other immunoproliferative neoplasms
204.10 - 204.12 Lymphoid leukemia, chronic [B-cell] [with hypogammaglobulinemia and recurrent infections or specific antibody deficiency]
279.00 Hypogammaglobulinemia, unspecified
279.04 Congenital hypogammaglobulinemia
279.05 Immunodeficiency with increased IgM
279.06 Common variable immunodeficiency [Good syndrome]
279.11 DiGeorge's syndrome
279.12 Wiskott-Aldrich syndrome
279.2 Combined immunity deficiency
279.50 Graft-versus-host disease, unspecified
279.51 Acute graft-versus-host disease
279.52 Chronic graft-versus-host disease
279.53 Acute on chronic graft-versus-host disease
283.0 Autoimmune hemolytic anemias [warm-type, refractory]
284.81 Red cell aplasia (acquired) (adult) (with thymoma)
286.0 Congenital factor VIII disorder
286.1 Congenital factor IX disorder
287.31 Immune thrombocytopenic purpura [when a rapid rise in platelet count is
required, such as prior to surgery, to control excessive bleeding, or to avoid splenectomy]
287.4 Secondary thrombocytopenia [HIV associated, pediatric or adult, when criteria
are met] [post-transfusion purpura]
287.5 Thrombocytopenia, unspecified
288.1 Functional disorders of polymorphonuclear neutrophils [Job's syndrome]
289.81 - 289.9 Other and unspecified diseases of blood and blood-forming organs
323.61 Infectious acute disseminated encephalomyelitis (ADEM) [refractory]
333.91 Stiff-man syndrome [unresponsive to other therapies]
340 Multiple sclerosis [relapsing-remitting when standard approaches have failed, become intolerable, or are contraindicated] [not covered for reducing the risk of post-partum exacerbation}
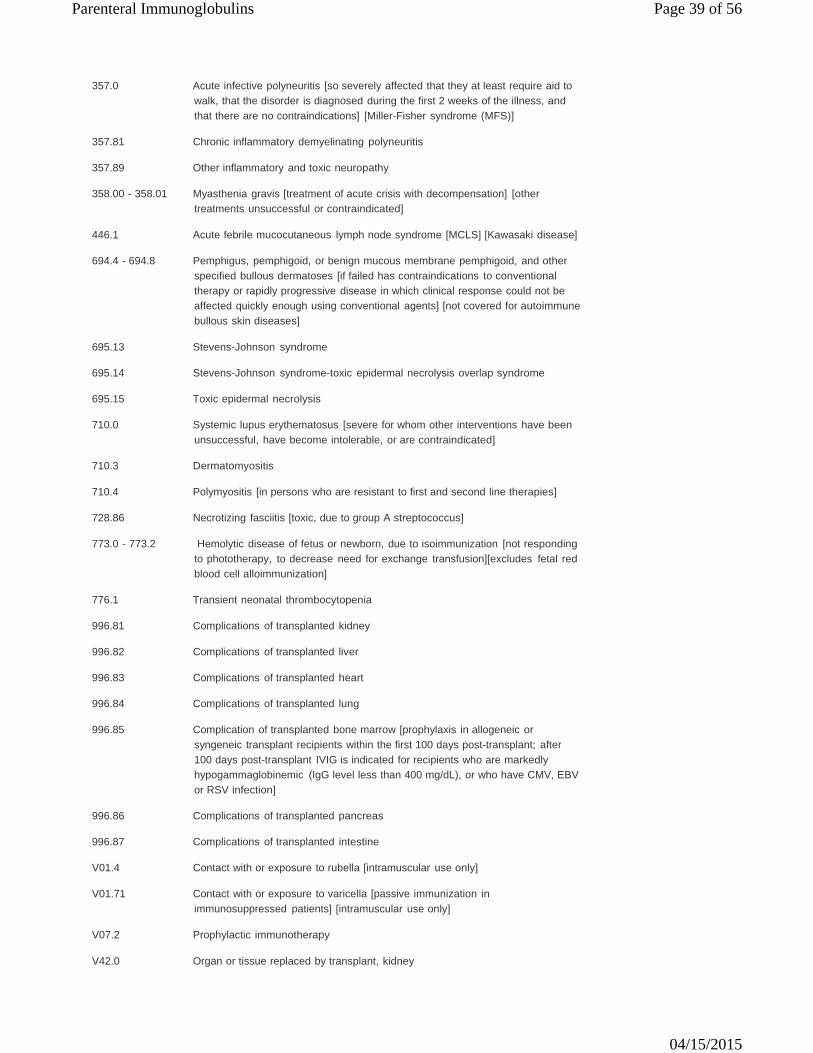
Parenteral Immunoglobulins Page 39 of 56
04/15/2015
357.0 Acute infective polyneuritis [so severely affected that they at least require aid to walk, that the disorder is diagnosed during the first 2 weeks of the illness, and that there are no contraindications] [Miller-Fisher syndrome (MFS)]
357.81 Chronic inflammatory demyelinating polyneuritis
357.89 Other inflammatory and toxic neuropathy
358.00 - 358.01 Myasthenia gravis [treatment of acute crisis with decompensation] [other
treatments unsuccessful or contraindicated]
446.1 Acute febrile mucocutaneous lymph node syndrome [MCLS] [Kawasaki disease]
694.4 - 694.8 Pemphigus, pemphigoid, or benign mucous membrane pemphigoid, and other specified bullous dermatoses [if failed has contraindications to conventional therapy or rapidly progressive disease in which clinical response could not be affected quickly enough using conventional agents] [not covered for autoimmune bullous skin diseases]
695.13 Stevens-Johnson syndrome
695.14 Stevens-Johnson syndrome-toxic epidermal necrolysis overlap syndrome
695.15 Toxic epidermal necrolysis
710.0 Systemic lupus erythematosus [severe for whom other interventions have been
unsuccessful, have become intolerable, or are contraindicated]
710.3 Dermatomyositis
710.4 Polymyositis [in persons who are resistant to first and second line therapies]
728.86 Necrotizing fasciitis [toxic, due to group A streptococcus]
773.0 - 773.2 Hemolytic disease of fetus or newborn, due to isoimmunization [not responding to phototherapy, to decrease need for exchange transfusion][excludes fetal red blood cell alloimmunization]
776.1 Transient neonatal thrombocytopenia
996.81 Complications of transplanted kidney
996.82 Complications of transplanted liver
996.83 Complications of transplanted heart
996.84 Complications of transplanted lung
996.85 Complication of transplanted bone marrow [prophylaxis in allogeneic or
syngeneic transplant recipients within the first 100 days post-transplant; after 100 days post-transplant IVIG is indicated for recipients who are markedly hypogammaglobinemic (IgG level less than 400 mg/dL), or who have CMV, EBV or RSV infection]
996.86 Complications of transplanted pancreas
996.87 Complications of transplanted intestine
V01.4 Contact with or exposure to rubella [intramuscular use only]
V01.71 Contact with or exposure to varicella [passive immunization in immunosuppressed patients] [intramuscular use only]
V07.2 Prophylactic immunotherapy
V42.0 Organ or tissue replaced by transplant, kidney
Parenteral Immunoglobulins Page 40 of 56
04/15/2015
V42.1 Organ or tissue replaced by transplant, heart
V42.6 Organ or tissue replaced by transplant, lung
V42.7 Organ or tissue replaced by transplant, liver
V42.81 Organ or tissue replaced by transplant, bone marrow [prophylaxis in allogeneic or syngeneic transplant recipients within the first 100 days post-transplant; after 100 days post-transplant IVIG is indicated for recipients who are markedly hypogammaglobinemic (IgG level less than 400 mg/dL), or who have CMV, EBV or RSV infection
V42.82 Organ or tissue replaced by transplant, peripheral stem cells replaced by
transplant [prophylaxis in allogeneic or syngeneic transplant recipients within the first 100 days post-transplant; after 100 days post-transplant IVIG is indicated for recipients who are markedly hypogammaglobinemic (IgG level less than 400 mg/dL), or who have CMV, EBV or RSV infection]
V42.83 Pancreas replaced by transplant
V42.84 Intestines replaced by transplant
V49.83 Awaiting organ transplant status
ICD-9 codes not covered for indications listed in the CPB (not all-inclusive):
008.45 Clostridium difficile intestinal infection
011.20 - 011.26 Tuberculosis of lung with cavitation
032.82 Diphtheritic myocarditis
036.43 Meningococcal myocarditis
074.23 Coxsackie myocarditis
078.89 Other specified diseases due to viruses [gastric enterovirus]
088.81 Lyme disease
093.82 Syphilitic myocarditis
099.3 Reiter's disease
130.3 Myocarditis due to toxoplasmosis
135 Sarcoidosis
136.9 Unspecified infectious and parasitic diseases
140.0 - 199.2 Malignant neoplasm (except hematologic)
200.20 - 200.28 Burkitt's tumor or lymphoma
202.00 - 202.08 Nodular (follicular) lymphoma
202.50 - 202.58 Letterer-Siwe disease [Langerhans cell histiocytosis]
204.00 - 204.02 Lymphoid leukemia, acute
205.00 - 205.02 Acute myeloid leukemia
205.10 - 205.12 Chronic myelogenous leukemia
209.00 - 209.30 Malignant carcinoid tumor
249.00 - 249.91 Secondary diabetes mellitus
Parenteral Immunoglobulins Page 41 of 56
04/15/2015
250.00 - 250.93 Diabetes mellitus
272.7 Lipidoses
273.1 - 273.3, 273.9
Monoclonal paraproteinemia, other paraproteinemias, macroglobulinemia, or unspecified disorder of plasma protein metabolism [Waldenstrom]
277.00 - 277.09 Cystic fibrosis
277.2 Other disorders of purine and pyrimidine metabolism
277.5 Mucopolysaccharidosis (Hunter's syndrome)
277.6 Other deficiencies of circulating enzymes
279.49 Autoimmune disease, not elsewhere classified [autoimmune encephalopathy]
283.11 Hemolytic-uremic syndrome
284.01 - 284.9 Aplastic anemia
286.3 Congenital deficiency of other clotting factors [congenital factor VII deficiency]
286.4 von Willebrand's disease
287.0 Allergic purpura (Henoch-Schonlein)
288.00 - 288.09 Neutropenia
288.4 Hemophagocytic syndromes [hemophagocytic lymphohistiocytosis]
296.20 - 296.36 Major depression
299.00 - 299.01 Autistic disorder
300.3 Obsessive-compulsive disorder
307.20 - 307.23 Tics
311 Depression
314.01 Attention deficit disorder with hyperactivity
320.0 - 322.9 Meningitis [infection in neonates]
323.0 - 323.9 Encephalitis/myelitis and encephalomyelitis [limbic]
330.0 Leukodystrophy
331.0 Alzheimer's disease
332.0 - 332.1 Parkinson's disease
333.4 Huntington's chorea
335.20 Amyotrophic lateral sclerosis
337.1 Peripheral autonomic neuropathy in disorders classified elsewhere [vasculitic
polyneuropathy]
337.20 - 337.29 Reflex sympathetic dystrophy [complex regional pain syndrome]
337.9 Unspecified disorder of autonomic nervous system [autoimmune autonomic neuropathy]
341.0 Neuromyelitis optica [Devic's syndrome]
345.00 - 345.91 Epilepsy and recurrent seizures
Parenteral Immunoglobulins Page 42 of 56
04/15/2015
348.30 - 348.39 Encephalopathy, not elsewhere classified [mitochondrial encephalopathy] [autoimmune encephalopathy]
352.6 Multiple cranial nerve palsies
353.5 Neuralgic amyotrophy [diabetic] [Parsonage-Turner syndrome]
356.8 - 356.9 Other specified idiopathic peripheral neuropathy [anti-myelin associated
glycoprotein neuropathy]
357.4 Polyneuropathy in other diseases classified elsewhere [small fiber neuropathy]
358.8 Other specified myoneural disorders [Isaacs syndrome]
364.00 - 364.3 Acute and subacute iridocyclitis, chronic iridocyclitis, certain types of iridocyclitis, and unspecified iridocyclitis
377.30 - 377.32 Optic neuritis
390 Rheumatic fever without mention of heart involvement
391.0 - 391.9 Rheumatic fever with heart involvement
392.9 Rheumatic chorea without mention of heart involvement [Sydenham's chorea]
422.0 Acute myocarditis in diseases classified elsewhere
425.4 Other primary cardiomyopathies
446.0 Polyarteritis nodosa
446.21 Goodpasture's syndrome
446.4 Wegener's granulomatosis
446.6 Thrombotic microangiopathy
447.8 Other specified disorders of arteries and arterioles [Degos disease]
473.0 - 473.9 Chronic sinusitis
480.0 - 486 Pneumonia [not related to RSV]
493.00 - 493.92 Asthma
516.3 Idiopathic fibrosing alveolitis [idiopathic pulmonary fibrosis]
516.5 Adult pulmonary Langerhans cell histiocytosis
531.00 - 538 Diseases of stomach and duodenum
555.0 - 558.9 Non-infectious enteritis and colitis
560.0 - 564.9 Other diseases of intestines
557.0 Acute vascular insufficiency of intestine
580.0 - 581.9 Nephritis and nephrotic syndrome
582.2 Chronic glomerulonephritis, with lesion of membranoproliferative
glomerulonephritis
583.1 Nephritis and nephropathy, not specified as acute or chronic, with lesion of membranous glomerulonephritis
584.5 - 584.9 Acute renal failure
628.0 - 628.9 Infertility, female
Parenteral Immunoglobulins Page 43 of 56
04/15/2015
686.01 Pyoderma gangrenosum
692.72 Acute dermatitis due to solar radiation [solar urticarial]
692.9 Eczema
694.4 - 694.8 Bullous dermatoses
708.8 Other specified urticaria
710.1 Systemic sclerosis
710.2 Sicca syndrome [Sjogren's syndrome]
714.0 - 714.9 Rheumatoid arthritis
729.1 Myalgia and myositis, unspecified
733.99 Other disorders of bone and cartilage [relapsing polychondritis]
746.86 Congenital heart block
771.81 - 771.89 Other infections specific to the perinatal period
780.39 Other convulsions
780.71 Chronic fatigue syndrome
785.0 Tachycardia, unspecified [orthostatic tachycardia syndrome]
785.59 Other shock without mention of trauma
786.30 Hemoptysis, unspecified [diffuse alveolar hemorrhage]
795.79 Other and unspecified nonspecific immunological findings
995.1 Angioneurotic edema
995.90 Systemic inflammatory response syndrome (SIRS), unspecified, NOS [immune reconstitution]
V13.29 Other genital system and obstetric disorders
Other ICD-9 codes related to the CPB:
075 Infectious mononucleosis [Epstein Barr virus]
078.5 Cytomegaloviral disease
079.6 Respiratory syncytial virus (RSV)
466.11 Acute bronchiolitis due to RSV
480.1 Pneumonia due to RSV
771.1 Congenital Cytomegalovirus Infection
200.00 - 202.98 Lymphosarcoma and reticulosarcoma
204.20 - 208.91 Subacute, other, and unspecified lymphoid leukemia, myeloid leukemia,
monocytic leukemia, other specified leukemia, and leukemia of unspecified cell type
323.81 Other causes of encephalitis and encephalomyelitis [noninfectious acute
disseminated encephalomyelitis (ADEM)] [Rasmussen's encepahlitis or syndrome]
333.2 Myoclonus
Parenteral Immunoglobulins Page 44 of 56
04/15/2015
336.3 Myelopathy in other diseases classified elsewhere
336.8 Other myelopathy
357.82 Critical illness polyneuropathy [acute motor axonal neuropathy (AMAN), acute motor and sensory axonal neuropathy (AMSAN)]
358.1 Myasthenic syndromes in diseases classified elsewhere [Eaton-Lambert
syndrome]
379.59 Other irregularities of eye movement
446.20 - 446.29 Hypersensitivity angiitis
728.85 Spasm of muscle
728.87 Muscle weakness (generalized)
780.66 Febrile nonhemolytic transfusion reaction
781.3 Lack of coordination
999.89 Other transfusion reaction
V42.82 Peripheral stem cells replaced by transplant
The above policy is based on the following references:
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11. 12.
13.
14. 15.
16.
Jongen JL, van Doorn PA, van der Meche FG. High-dose intravenous immunoglobulin therapy for myasthenia gravis. J Neurol. 1998;245(1):26-31. Bradley DJ, Glode MP. Kawasaki disease. The mystery continues. West J Med. 1998;168(1):23- 29. Sicherer SH, Winkelstein JA. Primary immunodeficiency diseases in adults. JAMA. 1998;279 (1):58-61. Tangel M, Hartung HP, Marx P, Gold R. Intravenous immunoglobulin treatment of neurological autoimmune diseases. J Neurol Sci. 1998;153(2):203-214. Otten A, Bossuyt PM, Vermeulen M, Brand A. Intravenous immunoglobulin treatment in hematological diseases. Eur J Haematol. 1998;60(2):73-85. Fabris F, Cordiano I, Girolami A. High-dose intravenous immune globulin and the response to splenectomy in patients with idiopathic thrombocytopenic purpura. N Engl J Med. 1997;337 (15):1088-1089. Comi G, Nemni R, Amadio S, et al. Intravenous immunoglobulin treatment in multifocal motor neuropathy and other chronic immune-mediated neuropathies. Mult Scler. 1997;3(2):93-97. Stiehm ER. Human intravenous immunoglobulin in primary and secondary antibody deficiencies. Pediatr Infect Dis J. 1997;16(7):696-707. Dalakas MC. Intravenous immune globulin therapy for neurologic diseases. Ann Intern Med. 1997;126(9):721-730. Dickler HB, Gelfand EW. Current perspectives on the use of intravenous immunoglobulin. Adv Intern Med. 1996;41:641-680. Rosti L. High-dose intravenous immunoglobulins. J Perinat Med. 1996;24(5):539. Cunningham-Rundles C. Established and new uses of intravenous immunoglobulin. Mt Sinai J Med. 1992;59(4):335-340. Klassen LW, Calabrese LH, Laxer RM. Intravenous immunoglobulin in rheumatic disease. Rheum Dis Clin North Am. 1996;22(1):155-173. National Institutes of Health. Intravenous Immunoglobulin Consens Statement. 1990;8(5):1-23. Canadian Paediatric Society, Infectious Diseases and Immunization Committee. Intravenous immune globulin use in children. Can Med Assoc J. 1992;146(2):121-124. Garvey MA, Giedd J, Swedo SE. PANDAS: The search for environmental triggers of pediatric neuropsychiatric disorders. Lessons from rheumatic fever. J Child Neurol. 1998;13(9):413-423.
Parenteral Immunoglobulins Page 45 of 56
04/15/2015
17.
18.
19.
20.
21.
22. 23.
24.
25. 26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
Swedo SE, Leonard HL, Mittleman BB, et al. Identification of children with pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections by a marker associated with rheumatic fever. Am J Psychiatry. 1997;154(1):110-112. Bril V, Allenby K, Midroni G, et al. IVIG in neurology--evidence and recommendations. Can J Neurol Sci. 1999;26(2):139-152. Horiuchi I, Yamada T, Imaiso Y, et al. [A case of stiff-man syndrome with an antineuronal autoantibody against an 80 kDa protein]. Rinsho Shinkeigaku. 1998;38(10-11):936-940. Liblau R, Benyahia B, Delattre JY. The pathophysiology of paraneoplastic neurological syndromes. Ann Med Interne (Paris). 1998;149(8):512-520. Sevrin C, Moulin T, Tatu L, et al. 'Stiff-man' syndrome treated with intravenous immunoglobulins (letter). Rev Neurol (Paris). 1998;154(5):431. Stayer C, Meinck HM. Stiff-man syndrome: An overview. Neurologia. 1998;13(2):83-88. Saiz A, Arias M, Fernandez-Barreiro A, et al. Diagnostic usefulness of glutamic acid decarboxylase antibodies in stiff-man syndrome. Med Clin (Barc). 1998;110(10):378-381. Liguori R, Cordivari C, Lugaresi E, Montagna P. Botulinum toxin A improves muscle spasms and rigidity in stiff-person syndrome. Mov Disord. 1997;12(6):1060-1063. Levin KH. Paraneoplastic neuromuscular syndromes. Neurol Clin. 1997;15(3):597-614. Fonseca LF, Noce TR, Teixeira ML, Early-onset acute transverse myelitis following hepatitis B vaccination and respiratory infection: Case report. Arq Neuropsiquiatr. 2003;61(2A):265-268. Barker RA, Marsden CD. Successful treatment of stiff man syndrome with intravenous immunoglobulin. J Neurol Neurosurg Psychiatry. 1997;62(4):426-427. Centers for Disease Control and Prevention (CDC). Availability of immune globulin intravenous for treatment of immune deficient patients -- United States, 1997-1998. MMWR Morb Mortal Wkly Rep. 1999;48(8):159-162. Lisak RP. Intravenous immunoglobulins in multiple sclerosis. Neurology. 1998;51(6 Suppl 5):S25- S29. Sorensen PS, Wanscher B, Jensen CV, et al. Intravenous immunoglobulin G reduces MRI activity in relapsing multiple sclerosis. Neurology. 1998;50(5):1273-1281. Achiron A, Gabbay U, Gilad R, et al. Intravenous immunoglobulin treatment in multiple sclerosis. Effect on relapses. Neurology. 1998;50(2):398-402. Sorensen PS. Intravenous immunoglobulin G therapy: Effects of acute and chronic treatment in multiple sclerosis. Mult Scler. 1996;1(6):349-352. Poehlau D, Federlein J, Postert T, et al. Intravenous immunoglobulin (IVIG) treatment for patients with primary or secondary progressive multiple sclerosis -- outline of a double- blind randomized, placebo-controlled trial. Mult Scler. 1997;3(2):149-152. Sorensen PS, Wanscher B, Schreiber K, et al. A double-blind, cross-over trial of intravenous immunoglobulin G in multiple sclerosis: Preliminary results. Mult Scler. 1997;3(2):145-148. Fazekas F, Deisenhammer F, Strasser-Fuchs S, et al. Treatment effects of monthly intravenous immunoglobulin on patients with relapsing-remitting multiple sclerosis: Further analyses of the Austrian Immunoglobulin in MS study. Mult Scler. 1997;3(2):137-141. Fazekas F, Deisenhammer F, Strasser-Fuchs S, et al. Randomised placebo-controlled trial of monthly intravenous immunoglobulin therapy in relapsing-remitting multiple sclerosis. Austrian Immunoglobulin in Multiple Sclerosis Study Group. Lancet. 1997;349(9052):589-593. American College of Obstetricians and Gynecologists (ACOG), Committee on Practice Bulletins -- Obstetrics. Thrombocytopenia in pregnancy. ACOG Practice Pattern No. 6. Washington, DC: ACOG; September 1999. Ohlsson A, Lacy JB. Intravenous immunoglobulin for suspected or subsequently proven infection in neonates. Cochrane Database Syst Rev. 2010;(3):CD001239. Ohlsson A, Lacy JB. Intravenous immunoglobulin for preventing infection in preterm and/or low- birth-weight infants. Cochrane Database Syst Rev. 2004;(1):CD000361. University HealthSystem Consortium (UHC), Technology Assessment Program of the Clinical Practice Advancement Center. Technology assessment: Intravenous immunoglobulin preparations. Oak Brook, IL: UHC; March 1999. University HealthSystem Consortium (UHC). Immune globulin intravenous (IGIV) - update. Drug Monograph. Oak Brook, IL: UHC; 2006. University of Michigan Health Center (UMHC), Department of Pediatrics and Communicable Diseases. Intravenous Immunoglobulin is effective therapy for acute idiopathic thrombocytopenic purpura. Evidence-Based Pediatrics Website. Ann Arbor, MI: UMHC; January 25, 1999. Available at: http://www.med.umich.edu/pediatrics/ebm/cats/itp.htm. Accessed June 24, 2002. .
Parenteral Immunoglobulins Page 46 of 56
04/15/2015
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
University of Pittsburgh Medical Center, Department of Pharmacy Services. IVIG Guidelines for Use. Pittsburgh, PA: University of Pittsburgh Medical Center; 1998. Available at: http://www.upmc.edu/druginfo/InternalAccess/Documents/ ShortForms/iv_immunoglobulin_products.htm. Accessed June 24, 2002. Association of British Neurologists (ABN). Guidelines for the Use of Intravenous Immunoglobulin in Neurologic Diseases. London, UK: ABN; March 2002. Available at: http://www.theabn.org/downloads/IVIgGuidelines.pdf. Accessed June 24, 2002. European Agency for the Evaluation of Medicinal Products, Committee for Proprietary Medicinal Products (CPMP), Blood Products Working Party. Core SPC for human normal immunoglobulin for intravenous administration (IVIg). London, UK: CPMP; June 2000. Available at: http://www.emea.eu.int/pdfs/human/bpwg/085995en.pdf. Accessed June 24, 2002. American Society for Reproductive Medicine (ASRM). Intravenous immunoglobulin (IVIG) and recurrent spontaneous pregnancy loss. A Practice Committee Report. Washington, DC: ASRM; July 1998. Available at: http://www.asrm.org/Media/Practice/ivig.html. Accessed June 24, 2002. Chapel HM, Spickett GP, Ericson D, et al. The comparison of the efficacy and safety of intravenous versus subcutaneous immunoglobulin replacement therapy. J Clin Immunol. 2000;20 (2):94-100. Gaspar J, Gerritsen B, Jones A. Immunoglobulin replacement treatment by rapid subcutaneous infusion. Arch Dis Child. 1998;79(1):48-51. Stiehm ER, Casillas AM, Finkelstein JZ, et al. Slow subcutaneous human intravenous immunoglobulin in the treatment of antibody immunodeficiency: Use of an old method with a new product. J Allergy Clin Immunol. 1998;101(6 Pt 1):848-849. Nigro G, D'Eufemia P, Zervini M, et al. Parvovirus B19 infection in a hypogammaglobulinemic infant with neurologic disorders and anemia: Successful immunoglobulin therapy. Pediatr Infect Dis J. 1994;13:1019-1021. American Academy of Pediatrics (AAP), Committee on Infectious Diseases. Immune globulin intravenous. In: 2006 Red Book: Report of the Committee on Infectious Diseases. 27th ed. Elk Grove Village, IL: AAP; 2006:57-60. Kimata H. High-dose intravenous gammaglobulin treatment of hyperimmunoglobulinemia E syndrome. J Allergy Clin Immunol. 1995;95:771-774. Bain PG, Motomura M, Newsom-Davis J, et al. Effects of intravenous immune globulin on muscle weakness and calcium-channel autoantibodies in the Lambert-Eaton myasthenic syndrome. Neurology. 1996;47:678-683. Fasano MB. Risks and benefits of intravenous immunoglobulin treatment in children. Curr Opin Pediatr. 1995;7:688-694. Clegg A, Bryant J, Milne R. Disease modifying agents in multiple sclerosis. Health Technol Assess. 2000;4(9):1-101. Center for Medicare and Medicaid Services (CMS). Intravenous immune globulin for autoimmune mucocutaneous blistering diseases. Decision Memorandum. CPG-00109N. Baltimore, MD: CMS; January 22, 2002. Available at: http://cms.hhs.gov/coverage.8b3-kkk2.asp. Accessed July 1, 2002. Fanaroff AA, Korones SB, Wright LL, et al. A controlled trial of intravenous immune globulin to reduce nosocomial infections in very-low-birth-weight infants. N Engl J Med. 1994;330(16):1107- 1113. Plasma Exchange/Sandoglobulin Guillain-Barré Syndrome Trial Group. Randomized trial of plasma exchange, intravenous immunoglobulin, and combined treatments in Guillain-Barré syndrome. Lancet. 1997;349:225-230. Oates-Whitehead RM, Baumer JH, Haines L, et al. Intravenous immunoglobulin for the treatment of Kawasaki disease in children. Cochrane Database Syst Rev. 2003;(4):CD004000. Wu HM, Tang JL, Sha ZH, et al. Interventions for preventing infection in nephrotic syndrome. Cochrane Database Syst Rev. 2004;(2):CD003964. Hughes RAC, Swan AV, van Doorn PA. Intravenous immunoglobulin for Guillain-Barré syndrome. Cochrane Database Syst Rev. 2010;(6):CD002063. Alejandria MM, Lansang MA, Dans LF, Mantaring JBV. Intravenous immunoglobulin for treating sepsis and septic shock. Cochrane Database Syst Rev. 2002;(1):CD001090. Gray O, McDonnell GV, Forbes RB. Intravenous immunoglobulins for multiple sclerosis. Cochrane Database Syst Rev. 2003;(3):CD002936. Brocklehurst P. Interventions for reducing the risk of mother-to-child transmission of HIV infection. Cochrane Database Syst Rev. 2002;(1):CD000102.
Parenteral Immunoglobulins Page 47 of 56
04/15/2015
65.
66.
67.
68.
69.
70.
71.
72.
73. 74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
85.
86.
87.
88.
89.
Gajdos P, Chevret S, Toyka K. Intravenous immunoglobulin for myasthenia gravis. Cochrane Database Syst Rev. 2008;(1):CD002277. Alcock GS, Liley H. Immunoglobulin infusion for isoimmune haemolytic jaundice in neonates. 2002;(3):CD003313. Bain PG, Motomura M, Newsom-Davis J, et al. Effects of intravenous immunoglobulin on muscle weakness and calcium-channel autoantibodies in the Lambert-Eaton myasthenic syndrome. Neurology. 1996;47:678-683. Maddison P, Newsom-Davis J. Treatment for Lambert-Eaton myasthenic syndrome. Cochrane Database Syst Rev. 2005;(2):CD003279. Daya S, Gunby J, Clark D A. Intravenous immunoglobulin therapy for recurrent spontaneous abortion: A meta-analysis. Am J Reprod Immunol. 1998;39(2):69-76. Jenson HB, Pollock BD. Meta-analyses of the effectiveness of intravenous immune globulin for prevention and treatment of neonatal sepsis. Pediatrics. 1997:99(2):E2. Ballow M. Primary immunodeficiency disorders: Antibody deficiency. J Allergy Clin Immunol. 2002;109(4):581-591. U.S. Pharmacopoeial Convention. Immune globulin intravenous (human) (systemic). USP-DI. Drug Information for the Healthcare Professional. Greenwood Village, CO: Micromedex; 2007. Schuval SJ. Treatment of antibody deficiency syndromes. Pediatrics Rev. 2000;21(10):358-359. Sorensen RU, Moore C. Antibody deficiency syndromes. Pediatr Clin North Am. 2000;47(6):1225- 1252. American Academy of Pediatrics, Committee on Children with Disabilities. Technical report: The pediatrician's role in the diagnosis and management of autistic spectrum disorder in children. Pediatrics. 2001;107(5):e85. Available at: http://www.pediatrics.org/cgi/content/full/107/5/e85. Accessed July 9, 2002. American Academy of Pediatrics (AAP). Immune globulins. In: 2000 Red book: Report of the Committee on Infectious Diseases. 25th ed. G Peter, ed. Elk Grove Village, IL: AAP;2000:39-41. Gajdos P, Chevret S, Clair B, et al. Clinical trial of plasma exchange and high dose immunoglobulin in myasthenia gravis. Ann Neurol. 1997;41(6):789-796. Ronager J, Ravnborg M, Hermansen I, Vorstrup S. Immunoglobulin treatment versus plasma exchange in patients with chronic moderate to severe myasthenia gravis. Artif Organs. 2001;25 (12):967-973. Wolfe GI, Barohn RJ, Foster BM, et al. Randomized, controlled trial of intravenous immunoglobulin in myasthenia gravis. Muscle Nerve. 2002;26(4):549-552. Cilliers AM, Manyemba J, Saloojee H. Anti-inflammatory treatment for carditis in acute rheumatic fever. Cochrane Database Syst Rev. 2003;(2):CD003176. Jordan S, Cunningham-Rundles C, McEwan R. Utility of intravenous immune globulin in kidney transplantation: Efficacy, safety, and cost implications. Am J Transplant. 2003;3(6):653-664. Glotz D, Antoine C, Julia P, et al. Desensitization and subsequent kidney transplantation of patients using intravenous immunoglobulins (IVIg). Am J Transplant. 2002;2(8):758-760. Jordan SC. Management of the highly HLA- sensitized patient. A novel role for intravenous gammaglobulin. Am J Transplant. 2002;2(8):691-692. Sonnenday CJ, Ratner LE, Zachary AA, et al. Preemptive therapy with plasmapheresis/intravenous immunoglobulin allows successful live donor renal transplantation in patients with a positive cross-match. Transplant Proc. 2002;34(5):1614-1616. Al-Uzri AY, Seltz B, Yorgin PD, et al. Successful renal transplant outcome after intravenous gamma-globulin treatment of a highly sensitized pediatric recipient. Pediatr Transplant. 2002;6 (2):161-165. Glotz D, Antoine C, Haymann JP, et al. Intravenous immunoglobulins and kidney transplantation in patients with anti-HLA antibodies. Adv Nephrol Necker Hosp. 2000;30:221-233. Montgomery RA, Zachary AA, Racusen LC, et al. Plasmapheresis and intravenous immune globulin provides effective rescue therapy for refractory humoral rejection and allows kidneys to be successfully transplanted into cross-match-positive recipients. Transplantation. 2000;70(6):887 -895. Jordan SC, Quartel AW, Czer LS, et al. Posttransplant therapy using high-dose human immunoglobulin (intravenous gammaglobulin) to control acute humoral rejection in renal and cardiac allograft recipients and potential mechanism of action. Transplantation. 1998;66(6):800- 805. Wadstrom J, Gannedahl G, Bersztel A, et al. Successful kidney transplantation after suppression of HLA alloantibodies with intravenous immunoglobulin in a highly sensitized patient. Transplant Proc. 1995;27(6):3463-3464.
Parenteral Immunoglobulins Page 48 of 56
04/15/2015
90.
91.
92.
93.
94.
95.
96.
97.
98.
99.
100.
101.
102.
103.
104.
105.
106.
107.
108.
109.
110.
111.
112.
Glotz D, Haymann JP, Niaudet P, et al. Successful kidney transplantation of immunized patients after desensitization with normal human polyclonal immunoglobulins. Transplant Proc. 1995;27 (1):1038-1039. Glotz D, Haymann JP, Sansonetti N, et al. Suppression of HLA-specific alloantibodies by high- dose intravenous immunoglobulins (IVIg). A potential tool for transplantation of immunized patients. Transplantation. 1993;56(2):335-337. Mouthon L. [Treatment of ANCA-positive systemic vasculitis with intravenous immunoglobins] Rev Med Interne. 1999;20 Suppl 4:431s-435s. Levy Y, George J, Fabbrizzi F, et al. Marked improvement of Churg-Strauss vasculitis with intravenous gammaglobulins. South Med J. 1999;92(4):412-414. Jordan SC. Treatment of systemic and renal-limited vasculitic disorders with pooled human intravenous immune globulin. J Clin Immunol. 1995;15(6 Suppl):76S-85S. Reinhold-Keller E, Tatsis E, Gross WL. [ANCA-associated vasculitis (Wegener's granulomatosis, Churg-Strauss syndrome, microscopic polyangiitis). 3. Therapeutic Procedure] Z Rheumatol. 1995;54(5):303-309. Armentia A, Fernandez A, Sanchez P, et al. Asthma and vasculitis. Response to intravenous immunoglobulins. Allergol Immunopathol (Madr). 1993;21(2):47-52. Hamilos DL, Christensen J. Treatment of Churg-Strauss syndrome with high-dose intravenous immunoglobulin. J Allergy Clin Immunol. 1991;88(5):823-824. Levy Y, Sherer Y, George J, et al. Serologic and clinical response to treatment of systemic vasculitis and associated autoimmune disease with intravenous immunoglobulin. Int Arch Allergy Immunol. 1999;119(3):231-238. Cordonnier C, Chevret S, Legrand M, et al. Should immunoglobulin therapy be used in allogeneic stem-cell transplantation? A randomized, double-blind, dose effect, placebo-controlled, multicenter trial. Ann Intern Med. 2003;139:8-18. British Columbia Ministry of Health Services, Provincial Blood Coordinating Office. IVIG utilization management handbook. 1st ed. Vancouver, BC: British Columbia Ministry of Health Services; April 2002. Available at: http://www.bloodlink.bc.ca/documents/ivighandbook2.pdf. Accessed June 30, 2003. Larcombe J. Urinary tract infection in children. In: BMJ Clinical Evidence. London, UK: BMJ Publishing Group; July 2009. Nicholas R, Chataway J. Multiple sclerosis. In: BMJ Clinical Evidence. London, UK: BMJ Publishing Group; June 2008. Hughes RAC, Wijdicks EFM, Barohn R, et al. Practice parameter: Immunotherapy for Guillian- Barre syndrome. Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2003;61:736-740. Available at: http://www.neurology.org/cgi/content/abstract/61/6/736. Accessed March 10, 2004. Massachusetts General Hospital, Transfusion Committee. Consensus indications for IV IgG. Boston, MA: Massachusetts General Hospital; February 2003. Available at: http://www.mgh.harvard.edu/labmed/lab/bts/IV%20IgG%20Guidelines.pdf. Accessed April 29, 2004. Buckley RH. Immunoglobulin G subclass deficiency: Fact or fancy? Curr Allergy Asthma Rep. 2002;2(5):356-360. Buckley RH. IgG subclass deficiency. In: Clinical Focus on Primary Immune Deficiencies. Issues and Information on Current Topics. Towson, MD: Immune Deficiency Foundation; December 1998;1(3):1-4. Fleisher TA. Evaluation of suspected immunodeficiency. Med Lab Observ. 2003;35(2):1- 2,12,14,19. Maguire GA, Kumararatne DS, Joyce HJ. Are there any clinical indications for measuring IgG subclasses? Ann Clin Biochem. 2002;39:374-377. Salcedo J, Keates S, Pothoulakis C, et al. Intravenous immunoglobulin therapy for severe Clostridium difficile colitis. Gut. 1997;41(3):366-370. Leung DY, Kelly CP, Boguniewicz M, et al. Treatment with intravenously administered gamma globulin of chronic relapsing colitis induced by Clostridium difficile toxin. J Pediatr. 1991;118(4 ( Pt 1)):633-637. Ohlsson A, Lacy J. Intravenous immunoglobulin for preventing infection in preterm and/or low- birth-weight infants. Cochrane Database Syst Rev. 2004;(1):CD000361. Fanaroff AA, Korones SB, Wright LL, et al. A controlled trial of intravenous immune globulin to reduce nosocomial infections in very-low-birth-weight infants. National Institute of Child Health and Human Development Neonatal Research Network. N Engl J Med. 1994;330(16):1107-1013.
Parenteral Immunoglobulins Page 49 of 56
04/15/2015
113.
114.
115.
116.
117.
118.
119.
120.
121.
122.
123.
124.
125.
126.
127.
128.
129.
130.
131.
132.
133.
134.
135.
136.
Kinney J, Mundorf L, Gleason C, et al. Efficacy and pharmacokinetics of intravenous immune globulin administration to high-risk neonates. Am J Dis Child. 1991;145(11):1233-1238. Malik S, Giacoia GP, West K. The use of intravenous immunoglobulin (IVIG) to prevent infections in bronchopulmonary dysplasia: Report of a pilot study. J Perinatol. 1991;11(3):239-244. Buemi M, Pettinato G, Palella S, et al. Treatment of the nephritic syndrome in elderly with human intravenous immunoglobulins. Contrib Nephrol. 1993;105:172-179. Hebert AA, Bogle MA. Intravenous immunoglobulin prophylaxis for recurrent Stevens-Johnson syndrome. J Am Acad Dermatol. 2004;50(2):286-288. Campione E, Marulli GC, Carrozzo AM, et al. High-dose intravenous immunoglobulin for severe drug reactions: efficacy in toxic epidermal necrolysis. Acta Derm Venereol. 2003;83(6):430-432. Metry DW, Jung P, Levy ML. Use of intravenous immunoglobulin in children with Stevens- Johnson syndrome and toxic epidermal necrolysis: Seven cases and review of the literature. Pediatrics. 2003;112(6 Pt 1):1430-1436. Sidwell RU, Swift S, Yan CL, et al. Treatment of toxic epidermal necrolysis with intravenous immunoglobulin. Int J Clin Pract. 2003;57(7):643-645. Mayorga C, Torres MJ, Corzo JL, et al, Posadas S, Jurado A, Blanca M. Improvement of toxic epidermal necrolysis after the early administration of a single high dose of intravenous immunoglobulin. Ann Allergy Asthma Immunol. 2003;91(1):86-91. Bachot N, Roujeau JC. Intravenous immunoglobulins in the treatment of severe drug eruptions. Curr Opin Allergy Clin Immunol. 2003;3(4):269-274. Prins C, Vittorio C, Padilla RS, et al, Saurat JH, French LE. Effect of high-dose intravenous immunoglobulin therapy in Stevens-Johnson syndrome: A retrospective, multicenter study. Dermatology. 2003;207(1):96-99. Tan A, Tan HH, Lee CC, Ng SK. Treatment of toxic epidermal necrolysis in AIDS with intravenous immunoglobulins. Clin Exp Dermatol. 2003;28(3):269-271. Wolff K, Tappeiner G. Treatment of toxic epidermal necrolysis: The uncertainty persists but the fog is dispersing. Arch Dermatol. 2003;139(1):85-86. Trent JT, Kirsner RS, Romanelli P, Kerdel FA. Analysis of intravenous immunoglobulin for the treatment of toxic epidermal necrolysis using SCORTEN: The University of Miami Experience. Arch Dermatol. 2003;139(1):39-43. Bachot N, Revuz J, Roujeau JC. Intravenous immunoglobulin treatment for Stevens-Johnson syndrome and toxic epidermal necrolysis: A prospective noncomparative study showing no benefit on mortality or progression. Arch Dermatol. 2003;139(1):33-36. Prins C, Kerdel FA, Padilla RS, et al. TEN-IVIG Study Group. Toxic epidermal necrolysis- intravenous immunoglobulin. Treatment of toxic epidermal necrolysis with high-dose intravenous immunoglobulins: Multicenter retrospective analysis of 48 consecutive cases. Arch Dermatol. 2003;139(1):26-32. Tristani-Firouzi P, Petersen MJ, Saffle JR, et al. Treatment of toxic epidermal necrolysis with intravenous immunoglobulin in children. J Am Acad Dermatol. 2002;47(4):548-552. Umapathi T, Hughes RAC, Nobile-Orazio E, Léger JM. Immunosuppressive treatment for multifocal motor neuropathy. Cochrane Database Syst Rev. 2005;(3):CD003217. Reid S, Chalder T, Cleare A, et al. Chronic fatigue syndrome. In: BMJ Clinical Evidence. London, UK: BMJ Publishing Group; September 2007. Karussis D. Abramsky O. Is the routine use of intravenous immunoglobulin treatment in neurologic disorders justified? Arch Neurol. 1999;56(8):1028-1032. Rodnitzky RL. Is IVIG effective in myasthenia gravis? Summary and Comment. Journal Watch Neurology. 2002;6. Available at: http://neurology.jwatch.org/cgi/content/full/2002/1206/6. Accessed October 27, 2004. Bussiere M, and the University of Western Ontario (UWO) Evidence Based Neurology Group. There is no difference in the functional outcome of patients with a myasthenic exacerbation treated with either IVIg or plasma exchange. London, ON: UWO; December 2001. Available at: http://www.uwo.ca/cns/ebn/CATs/nm-mg-ivig-pe-therapy.htm. Accessed October 27, 2004. American Academy of Pediatrics (AAP), Committee on Infectious Diseases. Immune globulin
intravenous. In: Red Book: 2003 Report of the Committee on Infectious Diseases. 26th ed. LK Pickering, ed. Elk Grove Village, IL: AAP; 2003:56-59. Majumdar S, Mockenhaupt M, Roujeau J-C, Townshend A. Interventions for toxic epidermal necrolysis. Cochrane Database Syst Rev. 2002;(4):CD001435. Kirtschig G, Murrell D, Wojnarowska F, Khumalo N. Interventions for mucous membrane pemphigoid/cicatricial pemphigoid and epidermolysis bullosa acquisita: A systematic literature review. Archiv Dermatol. 2002;138(3):380-384.
Parenteral Immunoglobulins Page 50 of 56
04/15/2015
137.
138.
139.
140.
141. 142.
143.
144.
145.
146.
147.
148.
149.
150.
151.
152.
153.
154.
155.
156.
157.
158.
159.
160.
161.
NHS Centre for Reviews and Dissemination. The effectiveness of interventions used in the treatment/management of chronic fatigue syndrome and/or myalgic encephalomyelitis in adults and children. York, UK: Centre for Reviews and Dissemination; 2002. Gottstein R, Cooke RW. Systematic review of intravenous immunoglobulin in haemolytic disease of the newborn. Arch Dis Child Fetal Neonatal Ed. 2003;88(1):F6-F10. van Koningsveld R, Schmitz PI, Meche FG, et al. Effect of methylprednisolone when added to standard treatment with intravenous immunoglobulin for Guillain-Barre syndrome: Randomised trial. Lancet. 2004;363(9404):192-196. Dalakas MC. Intravenous immunoglobulin in autoimmune neuromuscular diseases. JAMA. 2004;291(19):2367-2375. Buyon JP, Rupel A, Clancy RM. Neonatal lupus syndromes. Lupus. 2004;13(9):705-712. Hoekstra PJ, Minderaa RB, Kallenberg CG. Lack of effect of intravenous immunoglobulins on tics: A double-blind placebo-controlled study. J Clin Psychiatry. 2004;65(4):537-542. Robinson J, Hartling L, Vandermeer B, et al. Intravenous immunoglobulin for presumed viral myocarditis in children and adults. Cochrane Database Syst Rev. 2005;(1):CD004370. Tanimoto K, Nakano K, Kano S, et al. Classification criteria for polymyositis and dermatomyositis. J Rheumatol. 1995;22(4):668-674. Cernadas C, Pichon Riviere A, Augustovski F. Assessment of treatment with immunoglobulines in recurrent miscarriage [summary]. Report ITB No. 5. Buenos Aires, Argentina: Institute for Clinical Effectiveness and Health Policy (IECS); 2003. Dodel RC, Du Y, Depboylu C, et al. Intravenous immunoglobulins containing antibodies against beta-amyloid for the treatment of Alzheimer's disease. J Neurol Neurosurg Psychiatry. 2004;75 (10):1472-1474. Broughton SS, Meyerhoff WE, Cohen SB. Immune-mediated inner ear disease: 10-year experience. Semin Arthritis Rheum. 2004;34(2):544-548. Roed HG, Langkilde A, Sellebjerg F, et al. A double-blind, randomized trial of IV immunoglobulin treatment in acute optic neuritis. Neurology. 2005;64:804-810. Bartolomei F, Boucraut J, Barrie M, et al. Cryptogenic partial epilepsies with anti-GM1 antibodies: A new form of immune-mediated epilepsy? Epilepsia. 1996;37(10):922-926. Bakker J, Metz L. Devic's neuromyelitis optica treated with intravenous gamma globulin (IVIG). Can J Neurol Sci. 2004;31(2):265-267. Mutch LS, Johnston DL. Late presentation of opsoclonus-myoclonus-ataxia syndrome in a child with stage 4S neuroblastoma. J Pediatr Hematol Oncol. 2005;27(6):341-343. Garvey MA, Snider LA, Leitman SF, et al. Treatment of Sydenham's chorea with intravenous immunoglobulin, plasma exchange, or prednisone. J Child Neurol. 2005;20(5):424-429. Bearden CM, Agarwal A, Book BK, et al. Rituximab inhibits the in vivo primary and secondary antibody response to a neoantigen, bacteriophage phiX174. Am J Transplant. 2005;5(1):50-57. Jordan SC, Vo AA, Tyan D, et al. Current approaches to treatment of antibody-mediated rejection. Pediatr Transplant. 2005;9(3):408-415. Asia-Pacific IVIG Advisory Board. Expert consensus statements on the use of IVIG in neurology.
1st ed. Singapore: Asia-Pacific IVIG Advisory Board Inc.; November 2004. Fergusson D, Hutton B, Sharma M, et al. Use of intravenous immunoglobulin for treatment of neurologic conditions: A systematic review. Transfusion. 2005;45(10):1640-1657. Rayment R, Brunskill SJ, Stanworth S, et al. Antenatal interventions for fetomaternal alloimmune thrombocytopenia. Cochrane Database Syst Rev. 2005;(1):CD004226. Empson M, Lassere M, Craig J, Scott J. Prevention of recurrent miscarriage for women with antiphospholipid antibody or lupus anticoagulant. Cochrane Database Syst Rev. 2005; (2):CD002859. van Schaik IN, van den Berg LH, de Haan R, Vermeulen M. Intravenous immunoglobulin for multifocal motor neuropathy. Cochrane Database Syst Rev. 2005;(2):CD004429. Choy EHS, Hoogendijk JE, Lecky B, Winer JB. Immunosuppressant and immunomodulatory treatment for dermatomyositis and polymyositis. Cochrane Database Syst Rev. 2005; (3):CD003643. Liu Z, Albon E, Hyde C. The effectiveness and cost effectiveness of immunoglobulin replacement therapy for primary immunodeficiency and chronic lymphocytic leukaemia: A systematic review and economic evaluation. DPHE Report No. 54. Birmingham, UK: West Midlands Health Technology Assessment Collaboration, Department of Public Health and Epidemiology, University of Birmingham (WMHTAC); 2005.
Parenteral Immunoglobulins Page 51 of 56
04/15/2015
162.
163.
164.
165.
166.
167.
168.
169.
170.
171.
172. 173.
174.
175.
176.
177.
178.
179.
180.
181.
182.
183.
184.
185.
Orange JS, Hossny EM, Weiler CR, et al. Use of intravenous immunoglobulin in human disease: A review of evidence by members of the Primary Immunodeficiency Committee of the American Academy of Allergy, Asthma and Immunology. J Allergy Clin Immunol 2006;117:S525-S553. Darabi K, Abdel-Wahab O, Dzik WH. Current usage of intravenous immune globulin and the rationale behind it: The Massachusetts General Hospital data and a review of the literature. Transfusion. 2006;46(5):741-753. Porter TF, LaCoursiere Y, Scott JR. Immunotherapy for recurrent miscarriage. Cochrane Database Syst Rev. 2006;(2):CD000112. Overell JR, Hsieh ST, Odaka M, et al. Treatment for Fisher syndrome, Bickerstaff's brainstem encephalitis and related disorders. Cochrane Database Syst Rev. 2007:(1):CD004761. Allen D, Lunn MPT, Niermeijer J, Nobile-Orazio E. Treatment for IgG and IgA paraproteinaemic neuropathy. Cochrane Database Syst Rev. 2007;(1):CD005376. Orellana JC, Pogonza RE, Lopez-Olivo MA, et al. Intravenous immunoglobulin for juvenile idiopathic arthritis. Cochrane Database Syst Rev. 2006;(4):CD006191. Lunn MPT, Nobile-Orazio E. Immunotherapy for IgM anti-myelin-associated glycoprotein paraprotein-associated peripheral neuropathies. Cochrane Database Syst Rev. 2006; (2):CD002827. Volmink J, Marais B. HIV: Mother-to-child transmission. In: BMJ Clinical Evidence. London, UK: BMJ Publishing Group; January 2007. Alejandra M. Dengue haemorrhagic fever or dengue shock syndrome in children. In: BMJ Clinical Evidence. London, UK: BMJ Publishing Group; updated June 2008. Madjok R, Wu O. Systemic lupus erythematosus. In: BMJ Clinical Evidence. London, UK: BMJ Publishing Group; December 2008. Parr J. Autism. In: BMJ Clinical Evidence. London, UK: BMJ Publishing Group; May 2009. Duckitt K, Qureshi A. Recurrent miscarriage. In: BMJ Clinical Evidence. London, UK: BMJ Publishing Group; April 2007. Comite d' Evaluation et de Diffusion des Innovations Technologiques (CEDIT). Intravenous immunoglobulines - systematic review, primary research, expert panel, working group. Update. Paris, France; CEDIT; 2007. Meyer N, Ferraro V, Mignard MH, Adamski H, Chevrant-Breton J. Pyoderma gangrenosum treated with high-dose intravenous immunoglobulins: Two cases and review of the literature. Clin Drug Investig. 2006;26(9):541-546. Jolles S, Hughes J. Use of IGIV in the treatment of atopic dermatitis, urticaria, scleromyxedema, pyoderma gangrenosum, psoriasis, and pretibial myxedema. Int Immunopharmacol. 2006;6 (4):579-591. Feasby T, Banwell B, Benstead T, et al. Guidelines on the use of intravenous immune globulin for neurologic conditions. Transfus Med Rev. 2007;21(2 Suppl 1):S57-S107. Mikati MA, Shamseddine AN. Management of Landau-Kleffner syndrome. Paediatr Drugs. 2005;7 (6):377-389. Kang HC, Kim HD, Lee YM, Han SH. Landau-Kleffner syndrome with mitochondrial respiratory chain-complex I deficiency. Pediatr Neurol. 2006;35(2):158-161. de Menezes MS. Landau-kleffner syndrome. eMedicine Pediatric Neurology. San Francisco, CA: eMedicine.com; updated March 20, 2007. Available at: http://www.emedicine.com/neuro/topic182.htm. Accessed August 18, 2008. Whitington PF, Kelly S. Outcome of pregnancies at risk for neonatal hemochromatosis is improved by treatment with high-dose intravenous immunoglobulin. Pediatrics. 2008;121(6):e1615 -e1621. Chen S, Pi D, Ansari M, et al. Polyclonal intravenous immunoglobulin in patients with immune thrombocytopenic purpura: Clinical systematic review. Technology Report. HTA Issue 108. Ottawa, ON: Canadian Agency for Drugs and Technologies in Health (CADTH); 2008. Ho C, Membe S, Cimon K, et al. Subcutaneous versus intravenous immunoglobulin for primary immunodeficiencies: Systematic review and economic evaluation. Technology Report. HTA Issue 98. Ottawa, ON: Canadian Agency for Drugs and Technologies in Health (CADTH); 2008. Blackhouse G, Xie F, Campbell K, et al. Intravenous immunoglobulin for treatment of idiopathic thrombocytopenic purpura: Economic and health service impact analyses. Technology Report. HTA Issue 112. Ottawa, ON: Canadian Agency for Drugs and Technologies in Health (CADTH); 2008. Elovaara I, Apostolski S, van Doorn P, et al. EFNS guidelines for the use of intravenous immunoglobulin in treatment of neurological diseases: EFNS task force on the use of intravenous immunoglobulin in treatment of neurological diseases. Eur J Neurol. 2008;15(9):893-908.
Parenteral Immunoglobulins Page 52 of 56
04/15/2015
186.
187.
188.
189.
190.
191.
192.
193. 194.
195.
196.
197.
198.
199.
200.
201.
202.
203.
204.
205.
206.
207.
208.
209.
210.
Hughes RA, Donofrio P, Bril V, et al.; ICE Study Group. Intravenous immune globulin (10% caprylate-chromatography purified) for the treatment of chronic inflammatory demyelinating polyradiculoneuropathy (ICE study): A randomised placebo-controlled trial. Lancet Neurol. 2008;7 (2):136-144. Jann S, Bramerio MA, Facchetti D, Sterzi R. Intravenous immunoglobulin is effective in patients with diabetes and with chronic inflammatory demyelinating polyneuropathy: Long term follow-up. J Neurol Neurosurg Psychiatry. 2009;80(1):70-73. Achiron A, Kishner I, Dolev M, et al. Effect of intravenous immunoglobulin treatment on pregnancy and postpartum-related relapses in multiple sclerosis. J Neurol. 2004;251(9):1133-1137. Dudesek A, Zettl UK. Intravenous immunoglobulins as therapeutic option in the treatment of multiple sclerosis. J Neurol. 2006;253 Suppl 5:V50-V58. Haas J, Hommes OR. A dose comparison study of IVIG in postpartum relapsing-remitting multiple sclerosis. Mult Scler. 2007;13(7):900-908. Anderson D, Ali K, Blanchette V, et al. Guidelines on the use of intravenous immune globulin for hematologic conditions. Transfus Med Rev. 2007;21(2 Suppl 1):S9-S56. Osborne BJ, Volpe NJ. Optic neuritis and risk of MS: Differential diagnosis and management. Cleve Clin J Med. 2009;76(3):181-190. Levy SE, Mandell DS, Schultz RT. Autism. Lancet. 2009;374(9701):1627-1638. Gupta AA, Tyrrell P, Valani R, et al. Experience with hemophagocytic lymphohistiocytosis/macrophage activation syndrome at a single institution. J Pediatr Hematol Oncol. 2009;31(2):81-84. Eftimov F, Winer JB, Vermeulen M, et al. Intravenous immunoglobulin for chronic inflammatory demyelinating polyradiculoneuropathy. Cochrane Database Syst Rev. 2009;(1):CD001797. Fortin PM, Tejani AM, Bassett K, Musini VM. Intravenous immunoglobulin as adjuvant therapy for Wegener's granulomatosis. Cochrane Database Syst Rev. 2009;(3):CD007057. Goebel A, Baranowski A, Maurer K, et al. Intravenous immunoglobulin treatment of the complex regional pain syndrome: A randomized trial. Ann Intern Med. 2010;152(3):152-158. Raanani P, Gafter-Gvili A, Paul M, et al. Immunoglobulin prophylaxis in hematological malignancies and hematopoietic stem cell transplantation. Cochrane Database Syst Rev. 2008; (4):CD006501. Liu JP, Nikolova D, Fei Y. Immunoglobulins for preventing hepatitis A. Cochrane Database Syst Rev. 2009:(2):CD004181. Díaz-Manera J, Rojas-García R, Illa I. Treatment strategies for myasthenia gravis. Expert Opin Pharmacother. 2009;10(8):1329-1342. Tranchant C. Therapeutic strategy in myasthenia gravis. Rev Neurol (Paris). 2009;165(2):149- 154. Morozumi S, Kawagashira Y, Iijima M, et al. Intravenous immunoglobulin treatment for painful sensory neuropathy associated with Sjögren's syndrome. J Neurol Sci. 2009;279(1-2):57-61. Donofrio PD, Berger A, Brannagan TH 3rd, et al. Consensus statement: The use of intravenous immunoglobulin in the treatment of neuromuscular conditions report of the AANEM ad hoc committee. Muscle Nerve. 2009;40(5):890-900. O'Horo J, Safdar N. The role of immunoglobulin for the treatment of Clostridium difficile infection: A systematic review. Int J Infect Dis. 2009;13(6):663-667. Abougergi MS, Broor A, Cui W, Jaar BG. Intravenous immunoglobulin for the treatment of severe Clostridium difficile colitis: An observational study and review of the literature. J Hosp Med. 2010;5 (1):E1-E9. Stephenson MD, Kutteh WH, Purkiss S, et al. Intravenous immunoglobulin and idiopathic secondary recurrent miscarriage: A multicentered randomized placebo-controlled trial. Hum Reprod. 2010;25(9):2203-2209. Abougergi MS, Kwon JH. Intravenous immunoglobulin for the treatment of Clostridium difficile infection: A review. Dig Dis Sci. 2011;56(1):19-26. Ishii A, Hayashi A, Ohkoshi N, et al. Clinical evaluation of plasma exchange and high dose intravenous immunoglobulin in a patient with Isaacs' syndrome. J Neurol Neurosurg Psychiatry. 1994;57(7):840-842. Perlmutter SJ, Leitman SF, Garvey MA, et al. Therapeutic plasma exchange and intravenous immunoglobulin for obsessive-compulsive disorder and tic disorders in childhood. Lancet. 1999;354(9185):1153-1158. Hoekstra PJ, Minderaa RB, Kallenberg CG. Lack of effect of intravenous immunoglobulins on tics: A double-blind placebo-controlled study. J Clin Psychiatry. 2004;65(4):537-542.
Parenteral Immunoglobulins Page 53 of 56
04/15/2015
211.
212.
213.
214.
215.
216.
217.
218.
219.
220.
221.
222.
223.
224.
225.
226.
227.
228.
229.
230.
231.
232.
233.
234.
235.
236.
Isobe Y, Sugimoto K, Shiraki Y, et al. Successful high-titer immunoglobulin therapy for persistent parvovirus B19 infection in a lymphoma patient treated with rituximab-combined chemotherapy. Am J Hematol. 2004;77(4):370-373. Aries PM, Hellmich B, Gross WL. Intravenous immunoglobulin therapy in vasculitis: Speculation or evidence? Clin Rev Allergy Immunol. 2005;29(3):237-245. Myers KA, Baker SK. Late-onset seropositive Isaacs' syndrome after Guillain-Barré syndrome. Neuromuscul Disord. 2009;19(4):288-290. Eleftheriou D, Brogan PA. Vasculitis in children. Best Pract Res Clin Rheumatol. 2009;23(3):309- 323. Ishii N, Hashimoto T, Zillikens D, Ludwig RJ. High-dose intravenous immunoglobulin (IVIG) therapy in autoimmune skin blistering diseases. Clin Rev Allergy Immunol. 2010;38(2-3):186-195. Jolles S. A review of high-dose intravenous immunoglobulin (hdIVIg) in the treatment of the autoimmune blistering disorders. Clin Exp Dermatol. 2011;26(2):127-131. Kim JY, Park KD, Richman DP. Treatment of myasthenia gravis based on its immunopathogenesis. J Clin Neurol. 2011;7(4):173-183. Bird SJ. Treatment of myasthenia gravis. UpToDate [online serial]. Waltham, MA: UpToDate; last reviewed January 2012. Barker AF. Treatment of bronchiectasis in adult. UpToDate [online serial]. Waltham, MA: UpToDate; last reviewed September 2011. Dedeoglu F, Kim S, Sundel R. Management of Henoch-Schönlein purpura. UpToDate [online serial]. Waltham, MA: UpToDate; last reviewed September 2011. . Parambil JG, Tavee JO, Zhou L, et al. Efficacy of intravenous immunoglobulin for small fiber neuropathy associated with sarcoidosis. Respir Med. 2011;105(1):101-105. Freedman AS, Friedberg JW. Initial treatment of follicular lymphoma. UpToDate [online serial]. Waltham, MA: UpToDate; updated September 2011. Freedman AS, Friedberg JW. Treatment of relapsed or refractory follicular lymphoma. UpToDate [online serial]. Waltham, MA: UpToDate; updated September 2011. Trucco SM, Jaeggi E, Cuneo B, et al. Use of intravenous gamma globulin and corticosteroids in the treatment of maternal autoantibody-mediated cardiomyopathy. J Am Coll Cardiol. 2011;57 (6):715-723. INIS Collaborative Group, Brocklehurst P, Farrell B, King A, et al. Treatment of neonatal sepsis with intravenous immune globulin. N Engl J Med. 2011;365(13):1201-1211. Lemmon JK, Knutsen AP. IgG subclass deficiency. UpToDate [online serial]. Waltham, MA: UpToDate; May 11, 2012. American College of Obstetricians and Gynecologists (ACOG). Antiphospholipid syndrome. ACOG Practice Bulletin No. 118. Washington, DC: American College of Obstetricians and Gynecologists (ACOG); January 2011. Keeling D, Mackie I, Moore GW, et al, British Committee for Standards in Haematology. Guidelines on the investigation and management of antiphospholipid syndrome. Br J Haematol 2012;157(1):47–58. American Academy of Child and Adolescent Psychiatry. Practice parameter for the assessment and treatment of children and adolescents with obsessive-compulsive disorder. J Am Acad Child Adolesc Psychiatry 2012;51(1):98-113. Krull KR. Attention deficit hyperactivity disorder in children and adolescents: Treatment with medications. UpToDate [online serial]. Waltham, MA: UpToDate; updated December 2012a. Krull KR. Attention deficit hyperactivity disorder in children and adolescents: Overview of treatment and prognosis. UpToDate [online serial]. Waltham, MA: UpToDate; updated December 2012b. Searight HR, Burke JM. Adult attention deficit hyperactivity disorder. UpToDate [online serial]. Waltham, MA: UpToDate; updated December 2012. Katon W, Ciechanowski P. Initial treatment of depression in adults. UpToDate [online serial]. Waltham, MA: UpToDate; updated December 2012a. Katon W, Ciechanowski P. Treatment of resistant depression in adults. UpToDate [online serial]. Waltham, MA: UpToDate; updated December 2012b. Schwarz MI. The diffuse alveolar hemorrhage syndromes. UpToDate [online serial]. Waltham, MA: UpToDate; updated December 2012. Patwa HS, Chaudhry V, Katzberg H, et al. Evidence-based guideline: Intravenous immunoglobulin in the treatment of neuromuscular disorders: Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. 2012;78(13):1009 -1015.
Parenteral Immunoglobulins Page 54 of 56
04/15/2015
237.
238.
239.
240.
241.
242.
243.
244.
245.
246.
247.
248.
249.
250.
251.
252.
253.
254.
255.
256.
257.
258.
259.
260.
261.
262.
263.
264.
Pichichero ME. PANDAS: Pediatric autoimmune neuropsychiatric disorder associated with group A streptococci. UpToDate [online serial]. Waltham, MA: UpToDate; updated October 2012. Tan J, Smith CH, Goldman RD. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections. Can Fam Physician. 2012;58(9):957-959. Perlmutter SJ, Leitman SF, Garvey MA, et al. Therapeutic plasma exchange and intravenous immunoglobulin for obsessive-compulsive disorder and tic disorders in childhood. Lancet. 1999;354(9185):1153-1158. Martino D, Defazio G, Giovannoni G. The PANDAS subgroup of tic disorders and childhood-onset obsessive-compulsive disorder. J Psychosom Res. 2009;67(6):547-557. Shulman ST. Pediatric autoimmune neuropsychiatric disorders associated with streptococci (PANDAS): Update. Curr Opin Pediatr. 2009;21(1):127-130. Marconi D, Limpido L, Bersani I, et al. PANDAS: A possible model for adult OCD pathogenesis. Riv Psichiatr. 2009;44(5):285-298. Horton TM, Steuber CP. Overview of the treatment of acute lymphoblastic leukemia in children. UpToDate [online serial]. Waltham, MA: UpToDate; updated October 2012. Larson RA. Treatment of relapsed or refractory acute lymphoblastic leukemia in adults. UpToDate [online serial]. Waltham, MA: UpToDate; updated October 2012. Kakkis E, Wraith E. Complications and management of the mucopolysaccharidoses. UpToDate [online serial]. Waltham, MA: UpToDate; updated October 2012. Bronkhorst MW, Bouwman LH. Mannose-binding lectin deficiency. UpToDate [online serial]. Waltham, MA: UpToDate; updated October 2012. Alijotas-Reig J. Treatment of refractory obstetric antiphospholipid syndrome: The state of the art and new trends in the therapeutic management. Lupus. 2013;22(1):6-17. Hughes R, Cusack C, Murphy GM, Kirby B. Solar urticaria successfully treated with intravenous immunoglobulin. Clin Exp Dermatol. 2009;34(8):e660-e662. Llamas-Velasco M, Argila DD, Eguren C, et al. Solar urticaria unresponsive to intravenous immunoglobulins. Photodermatol Photoimmunol Photomed. 2011;27(1):53-54. Adamski H, Bedane C, Bonnevalle A, et al. Solar urticaria treated with intravenous immunoglobulins. J Am Acad Dermatol. 2011;65(2):336-340. Elmets CA. Photosensitivity disorders (photodermatoses): Clinical manifestations, diagnosis, and treatment. UpToDate [online serial]. Waltham, MA: UpToDate; reviewed December 2013. Gajdos P, Chevret S, Toyka KV. Intravenous immunoglobulin for myasthenia gravis. Cochrane Database Syst Rev. 2012;12:CD002277. Bascic-Kes V, Kes P, Zavoreo I, et al Ad Hoc Comittee of the Croatian Society for Neurovascular Disorders, Croatian Medical Association. Guidelines for the use of intravenous immunoglobulin in the treatment of neurologic diseases. Acta Clin Croat. 2012;51(4):673-683. Bird SJ. Treatment of myasthenia gravis. UpToDate [online serial]. Waltham, MA: UpToDate; reviewed December 2013. Fortin PM, Tejani AM, Bassett K, Musini VM. Intravenous immunoglobulin as adjuvant therapy for Wegener's granulomatosis. Cochrane Database Syst Rev. 2013;1:CD007057. Lunn MP, Nobile-Orazio E. Immunotherapy for IgM anti-myelin-associated glycoprotein paraprotein-associated peripheral neuropathies. Cochrane Database Syst Rev. 2012;5:CD002827. Ruzhansky K, Brannagan TH. Intravenous immunoglobulin for treatment of neuromuscular disease. Neurol Clin Pract. 2013;3(5):440-445. Drulovic J, Andrejevic S, Bonaci-Nikolic B, Mijailovic V. Hashimoto's encephalopathy: A long- lasting remission induced by intravenous immunoglobulins. Vojnosanit Pregl. 2011;68(5):452-454. Olmez I, Moses H, Sriram S, et al. Diagnostic and therapeutic aspects of Hashimoto's encephalopathy. J Neurol Sci. 2013;331(1-2):67-71. He L, Li M, Long XH, et al. A case of Hashimoto's encephalopathy misdiagnosed as viral encephalitis. Am J Case Rep. 2013;14:366-369. Rubin DI. Hashimoto's encephalopathy. UpToDate [online serial]. Waltham, MA: UpToDate; reviewed December 2013. Wong KS, Connan K, Rowlands S, et al. Antenatal immunoglobulin for fetal red blood cell alloimmunization. Cochrane Database Syst Rev. 2013;5:CD008267. Modlin JF. Epidemiology, pathogenesis, treatment, and prevention of enterovirus and parechovirus infections. UpToDate [online serial]. Waltham, MA: UpToDate; reviewed December 2013. Joao C. Immunoglobulin is a highly diverse self-molecule that improves cellular diversity and function during immune reconstitution. Med Hypotheses. 2007;68(1):158-161.
Parenteral Immunoglobulins Page 55 of 56
04/15/2015
265.
266.
267.
268.
269.
270.
271.
272.
273.
274.
275.
276.
277.
278.
279.
280.
281.
282.
283.
284.
285.
286.
287.
288.
289.
290.
Schmidt-Hieber M, Schwarck S, Stroux A, et al. Prophylactic i.v. Igs in patients with a high risk for CMV after allo-SCT. Bone Marrow Transplant. 2009;44(3):185-192. Sexton DJ, Pien BC. Immune reconstitution inflammatory syndrome. UpToDate [online serial]. Waltham, MA: UpToDate; reviewed December 2013. Gavhed D, Laurencikas E, Akefeldt SO, Henter JI. Fifteen years of treatment with intravenous immunoglobulin in central nervous system Langerhans cell histiocytosis. Acta Paediatr. 2011;100 (7):e36-e39. Edeer-Karaca N, Gulez N, Aksu G, Kutukculer N. Common variable immunodeficiency: Familial inheritance and autoimmune manifestations in two siblings. Turk J Pediatr. 2010;52(1):89-93. Michet CJ. Treatment of relapsing polychondritis. UpToDate [online serial]. Waltham, MA: UpToDate; reviewed December 2013. Ohlsson A, Lacy JB. Intravenous immunoglobulin for suspected or proven infection in neonates. Cochrane Database Syst Rev. 2013;7:CD001239. Noguchi Y, Tsuchiyama T, Matsumoto T, et al. Two distinct types of neuropathy associated with Sjogren's syndrome developed in one patient. The importance of the selection of an appropriate therapeutic regimen. Rinsho Shinkeigaku. 2003;43(9):539-543. De Toni Franceschini L, Amadio S, Scarlato M, et al. A fatal case of Churg-Strauss syndrome presenting with acute polyneuropathy mimicking Guillain-Barre syndrome. Neurol Sci. 2011;32 (5):937-940. Brass SD, Helfgott SM. Diagnosis and treatment of vasculitic neuropathy. UpToDate [online serial]. Waltham, MA: UpToDate; reviewed December 2013. Rajkumar SV. Treatment and prognosis of Waldenstrom macroglobulinemia. UpToDate [online serial]. Waltham, MA: UpToDate; reviewed December 2013. Orange JS, Ballow M, Stiehm ER, et al. Use and interpretation of diagnostic vaccination in primary immunodeficiency: A working group report of the Basic and Clinical Immunology Interest Section of the American Academy of Allergy, Asthma & Immunology. J Allergy Clin Immunol. 2012;130(3 Suppl):S1-S24. Parambil JG, Tavee JO, Zhou L, et al. Efficacy of intravenous immunoglobulin for small fiber neuropathy associated with sarcoidosis. Respir Med. 2011;105(1):101-105. Jurisdictional Blood Committee, for and on behalf of the Australian Health Ministers’ Conference. Criteria for the clinical use of intravenous immunoglobulin in Australia. 2nd ed. Canberra, ACT: Commonwealth of Australia; 2012. Simon NG, Ayer G, Lomen-Hoerth C. Is IVIg therapy warranted in progressive lower motor neuron syndromes without conduction block? Neurology. 2013;81(24):2116-2120. Puli L, Tanila H, Relkin N. Intravenous immunoglobulins for Alzheimer's disease. Curr Alzheimer Res. 2014;11(7):626-636. Goebel A, Shenker N, Padfield N, et al. Low-dose intravenous immunoglobulin treatment for complex regional pain syndrome (LIPS): Study protocol for a randomized controlled trial. Trials. 2014;15(1):404. McMahan ZH, Wigley FM. Novel investigational agents for the treatment of scleroderma. Expert Opin Investig Drugs. 2014;23(2):183-198. Akdag A, Dilmen U, Haque K, et al. Role of pentoxifylline and/or IgM-enriched intravenous immunoglobulin in the management of neonatal sepsis. Am J Perinatol. 2014;31(10):905-912. Horton TM, Steuber CP. Overview of the treatment of acute lymphoblastic leukemia in children and adolescents. UpToDate [online serial], Waltham, MA: UpToDate; reviewed October 2014. National Comprehensive Cancer Network (NCCN). Acute lymphoblastic leukemia. NCCN Clinical Practice Guidelines in Oncology. Version 1.2014. Fort Washington, PA: NCCN; 2014. Toledano M, Britton JW, McKeon A, et al. Utility of an immunotherapy trial in evaluating patients with presumed autoimmune epilepsy. Neurology. 2014;82(18):1578-1586. Ruegg S, Panzer JA. Immune therapy for pharmacoresistant epilepsy: Ready to go? Neurology. 2014;82(18):1572-1573. Rogosnitzky M, Danks R, Holt D. Intravenous immunoglobulin for the treatment of Crohn's disease. Autoimmun Rev. 2012;12(2):275-280. Farrell RJ, Peppercorn MA. Overview of the medical management of mild to moderate Crohn disease in adults. UpToDate [online serial], Waltham, MA: UpToDate; reviewed October 2014a. Farrell RJ, Peppercorn MA. Overview of the medical management of severe or refractory Crohn disease in adults. UpToDate [online serial]. Waltham, MA: UpToDate; reviewed October 2014b. MacDermott RP. Immunomodulator therapy in Crohn disease. UpToDate [online serial], Waltham, MA: UpToDate; reviewed October 2014.
Parenteral Immunoglobulins Page 56 of 56
04/15/2015
291.
292.
293.
294.
295.
296.
297.
298.
299.
300.
Ahnen DJ, Macrae FA. Approach to the patient with colonic polyps. UpToDate [online serial]. Waltham, MA: UpToDate; reviewed October 2014. Louis D, More K, Oberoi S, Shah PS. Intravenous immunoglobulin in isoimmune haemolytic disease of newborn: An updated systematic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed. 2014;99(4):F325-F331. Beken S, Hirfanoglu I, Turkyilmaz C, et al. Intravenous immunoglobulin G treatment in ABO hemolytic disease of the newborn, is it myth or real? Indian J Hematol Blood Transfus. 2014;30 (1):12-15. Rajkumar SG. Diagnosis and management of solitary extramedullary plasmacytoma. UpToDate [online serial]. Waltham, MA: UpToDate; reviewed October 2104a. Rajkumar SG. Diagnosis and management of solitary plasmacytoma of bone. UpToDate [online serial], Waltham, MA: UpToDate; reviewed October 2104b. Freeman R, Kaufman H. Postural tachycardia syndrome. UpToDate [serial online], Waltham, MA: UpToDate; reviewed October 2014. Bromberg MB. Brachial plexus syndromes. UpToDate [online serial], Waltham, MA: UpToDate; reviewed November 2014. Tzekou A, Fehlings MG. Treatment of spinal cord injury with intravenous immunoglobulin G: Preliminary evidence and future perspectives. J Clin Immunol. 2014;34 Suppl 1:S132-S138. Aubin F, Porcher R, Jeanmougin M, et al; Societe Française de Photodermatologie. Severe and refractory solar urticaria treated with intravenous immunoglobulins: A phase II multicenter study. J Am Acad Dermatol. 2014;71(5):948-953. Xie Z, Chan E, Long LM, et al. High dose intravenous immunoglobulin therapy of the systemic capillary leak syndrome (Clarkson disease). Am J Med. 2015;128(1):91-95.
Copyright Aetna Inc. All rights reserved. Clinical Policy Bulletins are developed by Aetna to assist in administering plan benefits and
constitute neither offers of coverage nor medical advice. This Clinical Policy Bulletin contains only a partial, general description of plan or
program benefits and does not constitute a contract. Aetna does not provide health care services and, therefore, cannot guarantee any
results or outcomes. Participating providers are independent contractors in private practice and are neither employees nor agents of
Aetna or its affiliates. Treating providers are solely responsible for medical advice and treatment of members. This Clinical Policy Bulletin
may be updated and therefore is subject to change.