
CLINICAL PHARMACY IN ENDOCRINOLOGY. COMMON ENDOCRINE DISORDERS Type 1 Diabetes Type 2 Diabetes...
31
CLINICAL PHARMACY IN ENDOCRINOLOGY
-
Upload
maurice-dawson -
Category
Documents
-
view
221 -
download
3
Transcript of CLINICAL PHARMACY IN ENDOCRINOLOGY. COMMON ENDOCRINE DISORDERS Type 1 Diabetes Type 2 Diabetes...

CLINICAL PHARMACY IN ENDOCRINOLOGY

COMMON ENDOCRINE DISORDERS
Type 1 Diabetes Type 2 Diabetes Osteoporosis Thyroid Cancer Addison's Disease Cushing's Syndrome Gestational Diabetes Graves' Disease Hashimoto's Thyroiditis
Hyperglycemia· Hyperparathyroidism
Hyperthyroidism Hypoglycemia Hypoparathyroidism Hypothyroidism Menopause Obesity Pre-diabetes Thyroid Nodules
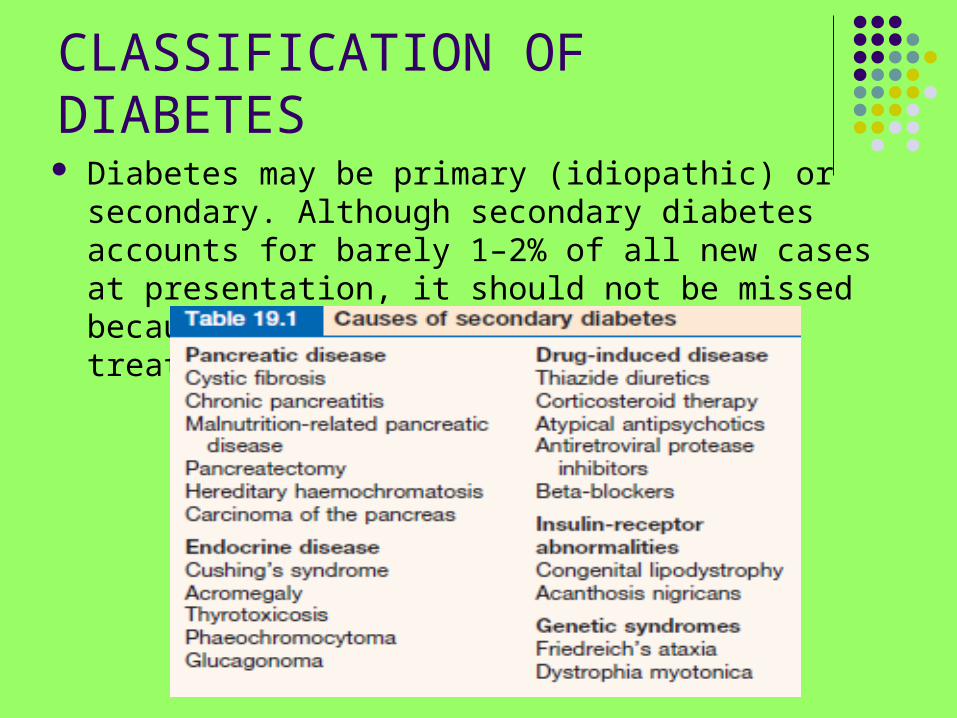
CLASSIFICATION OF DIABETES Diabetes may be primary (idiopathic) or secondary.
Although secondary diabetes accounts for barely 1–2% of all new cases at presentation, it should not be missed because the cause can sometimes be treated.

The spectrum of diabetes: a comparison of type 1 and type 2 diabetes mellitus

Type 1 diabetes
Type 1 diabetes (which used to be called juvenile diabetes) can be overwhelming; symptoms seem to develop suddenly: something triggers the development of type 1 diabetes (a viral infection)

Symptoms can rapidly develop:
Extreme weakness and/or tiredness Extreme thirst—dehydration Increased urination Abdominal pain Nausea and/or vomiting Blurry vision Wounds that don’t heal well Irritability or quick mood changes Changes to (or loss of) menstruation


There are also signs of type 1 diabetes. Signs are different from symptoms in that they can be measured objectively; symptoms are experienced and reported by the patient. Signs of type 1 diabetes include:
Weight loss—despite eating more Rapid heart rate Reduced blood pressure (falling below 90/60) Low body temperature (below 97º F)

Type 2 diabetes The symptoms of type 2 diabetes (type 2 diabetes
mellitus) develop gradually—so gradually, in fact, that it’s possible to miss them or to not connect them as related symptoms. Some people are actually surprised when they are diagnosed with type 2 diabetes because they’ve gone to the doctor for something else (eg, fatigue or increased urination). The symptoms develop gradually because, if you have the insulin resistant form of type 2, it takes time for the effects of insulin resistance to show up.

The common symptoms of type 2 diabetes: Fatigue Extreme thirst: No matter how much the patient drink, it feels
like the patient is still dehydrated. Tissues (such as muscles) are, in fact, dehydrated when there’s too much glucose (sugar) in blood. The body pulls fluid from the tissues to try to dilute the blood and counteract the high glucose, so the tissues will be dehydrated.
Frequent urination: This is related to drinking so much more in an attempt to satisfy thirst. Since the patient is drinking more, he’ll have to urinate more. Additionally, the body will try to get rid of the excess glucose through urination.
Extreme hunger: Even after the person eat, he may still feel very hungry.

The common symptoms of type 2 diabetes (cont’d): Weight loss. Infections: The effects of type 2 diabetes make it harder for the body to
fight off an infection. Women may have frequent vaginal (yeast) and/or bladder infections. That’s because bacteria can flourish when there are high levels of glucose in the blood.
Slow wound healing: Similar to the body’s inability to fight off infections, it might take longer for wounds (even small cuts) to heal. The high blood glucose level affects how well the white blood cells (which are in charge of healing wounds) work.
Blurry vision: In an attempt to get more fluid into the blood to counteract the high blood glucose level, the body may pull fluid from the eyes. The person may have trouble focusing then, leading to blurry vision.


Gestational diabetes
This term refers to glucose intolerance that develops in thecourse of pregnancy and usually remits following delivery.The condition is typically asymptomatic. Women who havea previous history of gestational diabetes, older or overweightwomen, those with a history of large for gestationalage babies and women from certain ethnic groups are atparticular risk, but many cases occur in women who are notin any of these categories. For this reason some advocatescreening of all pregnant women on the basis of randomplasma glucose testing in each trimester and by oral glucosetolerance testing if the glucose concentration is, for example,7 mmol/L or more.

THE ADRENAL MEDULLAPhaeochromocytoma (tumours of the sympathetic nervoussystem. Ninety per cent arise in the adrenal, while 10% occur elsewhere in the sympathetic chain.)
Symptoms Anxiety or panic attacks Palpitations Tremor Sweating Headache Flushing Nausea and/or vomiting Weight loss Constipation or diarrhoea Raynaud’s phenomenon Chest pain Polyuria/nocturia
Signs Hypertension Tachycardia/arrhythmias Bradycardia Orthostatic hypotension Pallor or flushing Glycosuria Fever (Signs of hypertensive
damage)

Phaeochromocytoma
Diagnosis Specific tests are:■ Measurement of urinary catecholamines andmetabolites (metanephrines are most sensitive andspecific) is a useful screening test; normallevels on three 24-hour collections of metanephrinesvirtually exclude the diagnosis.■ Resting plasma catecholamines are raised.■ Plasma chromogranin A (a storage vesicle protein) israised.■ Clonidine suppression test may be appropriate, butshould only be performed in specialist centres.■ CT scans, initially of the abdomen, are helpful tolocalize the tumours which are often large.■ MRI usually shows the lesion clearly.

Treatment
Tumours should be removed if this is possible; 5-year survivalis about 95% for non-malignant tumours. Medical preoperativeand perioperative treatment is vital and includescomplete alpha- and beta-blockade with phenoxybenzamine(20–80 mg daily initially in divided doses), then propranolol(120–240 mg daily), plus transfusion of whole blood to reexpandthe contracted plasma volume. The alpha-blockademust precede the beta-blockade, as worsened hypertensionmay otherwise result.

ADDISON’S DISEASE
Addison’s disease is a rare disorder that affects men and women of all ages. Addison’s disease is also referred to as primary adrenal insufficiency. Adrenal insufficiency develops when adrenal glands do not produce enough of the hormone cortisol.

Diseases of the Adrenal Cortex: Cushing's Syndrome
In 1932, a physician named Harvey Cushing described 8 patients with central body obesity, glucose intolerance, hypertension, excess hair growth, osteoporosis, kidney stones, menstrual irregularity, and emotional liability. It is now known that these symptoms characterize Cushing's syndrome, which is the result of excess production of cortisol by the adrenal glands.

Cushing's Syndrome Since cortisol production by the adrenal glands
is normally under the control of the pituitary, overproduction can be caused by a tumor in the pituitary or within the adrenal glands themselves. When a pituitary tumor secretes too much ACTH (adrenocorticotropic hormone), it causes the otherwise normal adrenal glands to produce too much cortisol. This type of Cushing's syndrome is termed Cushing's disease, and it is diagnosed like other endocrine disorders (by measuring hormone production). In this case, serum cortisol will be elevated, and serum ACTH will also be elevated

Cushing's Syndrome
When the adrenal glands develop a tumor, like any other endocrine gland, they usually produce excess amounts of the hormone normally produced by these cells. If the adrenal tumor is composed of cortisol-producing cells, excess cortisol will be produced.
Cushing's Syndrome
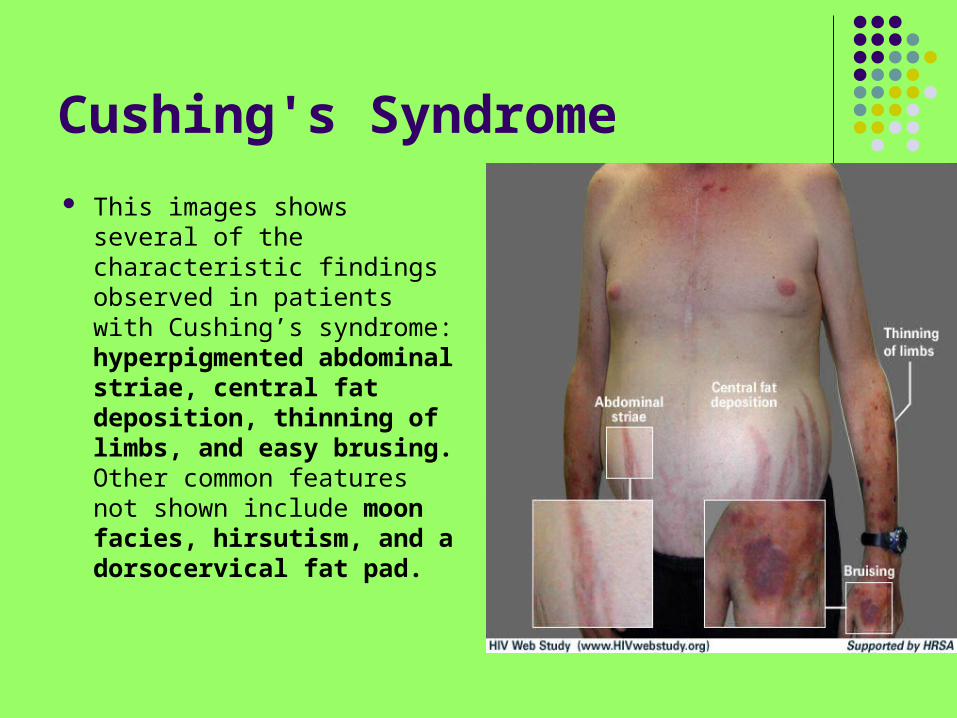
This images shows several of the characteristic findings observed in patients with Cushing’s syndrome: hyperpigmented abdominal striae, central fat deposition, thinning of limbs, and easy brusing. Other common features not shown include moon facies, hirsutism, and a dorsocervical fat pad.

Treatment of Cushing's Syndrome
The treatment of this disease depends on the cause. Pituitary tumors are usually removed surgically and often treated with radiation therapy. Neurosurgeons specialize in these tumors. If the cause is determined to be within a single adrenal gland, this is treated by surgical removal. If the tumor has characteristics of cancer on any of the x-ray tests, then a larger, conventional operation is in order. If a single adrenal gland possesses a small, well-defined tumor, it can usually be removed with a laparoscopic adrenalectomy.

Osteoporosis Osteoporosis means
"porous bone," and it's a disorder characterized by "holey" bones, meaning that bones aren't as strong as they should. Though post-menopausal women are most commonly associated with osteoporosis, men also experience it, so everyone should pay attention to their bone health.

Osteoporosis

Osteoporosis Osteoporosis is a condition
characterized by a decrease in the density of bone, decreasing its strength and resulting in fragile bones. Osteoporosis literally leads to abnormally porous bone that is compressible, like a sponge. This disorder of the skeleton weakens the bone and results in frequent fractures (breaks) in the bones. Osteopenia is a condition of bone that is slightly less dense than normal bone but not to the degree of bone in osteoporosis.

Prevention of Osteoporosis
The prevention of osteoporosis is made up of general lifestyle preferences and other more specific treatments. Regular and frequent activity of reasonable intensity is recommended and very helpful at all ages. No one seems to know just how exercise is too much or too little, but most physicians recommend about 30 minutes of vigorous exercise about 3 to 5 times per week. During the growing years of adolescence and teen years, attention must be paid to dietary calcium if peak bone mass is to be achieved.

Prevention of Osteoporosis
Specific attention to dietary calcium intake may also be warranted beyond age 60 which may come in the form of increased food calcium or from specific calcium and vitamin D supplements. For women at menopause, the appropriate administration of estrogen (or some of the new synthetic estrogens) is the most potent means by which bone mass may be preserved, thereby preventing fractures in the future. In fact, correction of low reproductive hormone levels at any age is important if proper bone mass is to be maintained.
There is no one treatment, or combination of treatments which can guarantee zero risk of fractures due to osteoporosis. The best prevention, however, is a life-long commitment to physical activity, good nutrition, and normal reproductive hormone status.

Treatment of Osteoporosis patients with proven osteoporosis (by fracture
history or BMD > 2.5 SD below average) generally need some of specific drug therapy. All patients, osteoporosis and osteopenia, need the lifestyle and dietary therapies
Drugs which are used to treat osteoporosis can be grouped into two groups. The first category is comprised of agents which limit the rate of bone loss. These drugs decrease the rate at which osteoclasts reabsorb bone and are referred to as "anti-resorption drugs".

Anti-resorption drugs
Calcium and Vitamin D Estrogen Calcitonin Biophosphonates

Hyperparathyroidism Under normal conditions, a
normal calcium level will be associated with a normal parathyroid hormone level. Also under normal conditions, a low serum calcium level will be associated with a high parathyroid hormone level; a high calcium level will be associated with a low parathyroid hormone level. These are all appropriate ways in which a parathyroid gland will react to calcium that is circulating in the blood as they attempt to regulate calcium in the narrow normal range.

Symptoms of Hypothyroidism Fatigue Weakness Weight gain or increased difficulty losing weight Coarse, dry hair Dry, rough pale skin Hair loss Cold intolerance (can't tolerate cold temperatures like those
around) Muscle cramps and frequent muscle aches Constipation Depression Irritability Memory loss Abnormal menstrual cycles Decreased libido


















