Clinical pharmacy COPD
17
Respiratory system Respiratory system Chronic obstructive pulmonary Chronic obstructive pulmonary disease (COPD disease (COPD ( (
-
Upload
aldawaa -
Category
Health & Medicine
-
view
72 -
download
7
Transcript of Clinical pharmacy COPD

Respiratory systemRespiratory systemChronic obstructive pulmonary Chronic obstructive pulmonary
disease (COPDdisease (COPD((

COPD: is defined as chronic slowly COPD: is defined as chronic slowly progressive disorder characterized by progressive disorder characterized by airway obstruction, which does not change airway obstruction, which does not change markedly by several months. Which is markedly by several months. Which is includingincluding::
11--Chronic bronchitisChronic bronchitis22--EmphysemaEmphysema


Chronic bronchitisChronic bronchitis
Is a clinical condition characterized by Is a clinical condition characterized by excessive mucus production result ing in excessive mucus production result ing in airways obstruction on most days for at airways obstruction on most days for at least 3 months of the year during at least least 3 months of the year during at least 2 consecutive years.2 consecutive years.
Etiology:Etiology:-Air pollution-Air pollution -Cigarette smoking -Cigarette smoking-Coal, gold mining, cement, grain handling -Coal, gold mining, cement, grain handling
and farming.and farming.


Clinical manifestations:Clinical manifestations:
-Excessive mucus production-Excessive mucus production-Bronchospasm, dyspnea and wheezing -Bronchospasm, dyspnea and wheezing -Hypoxia and hypercapnia (Blue in color)-Hypoxia and hypercapnia (Blue in color)-Productive cough-Productive cough-Increase body weight -Increase body weight
Complications:Complications:
Cor-pulmonaleCor-pulmonale
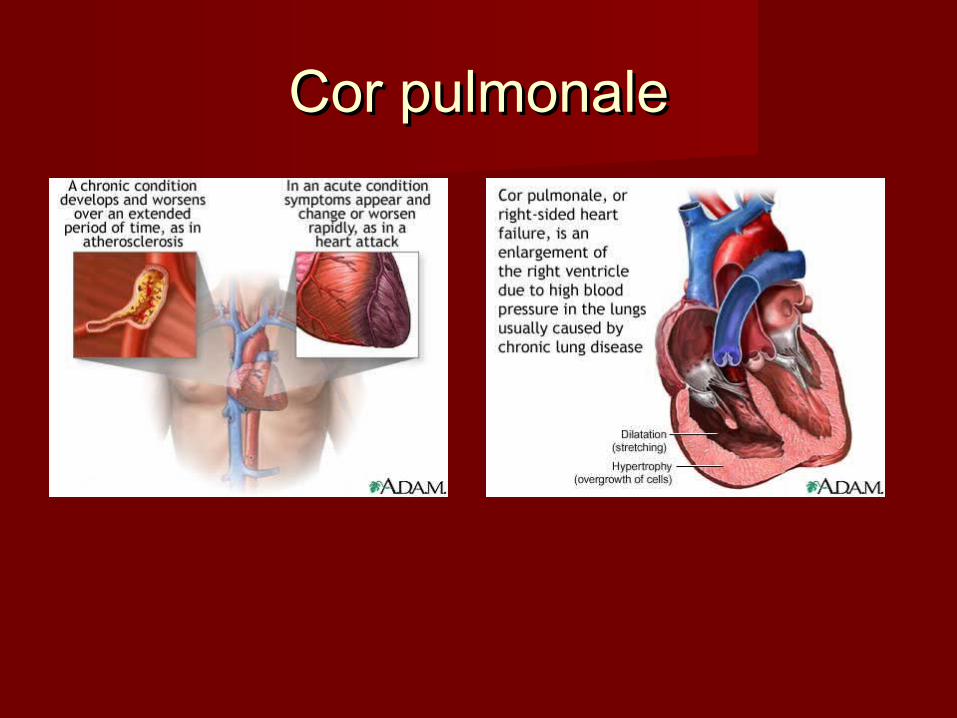
Cor pulmonaleCor pulmonale

EmphysemaEmphysema
An abnormal permanent enlargement of air spaces An abnormal permanent enlargement of air spaces distal to the terminal bronchioles, accompanied distal to the terminal bronchioles, accompanied by destruction of their walls.by destruction of their walls.
Etiology:Etiology:Cigarette smokingCigarette smoking
Clinical manifestat ions:Clinical manifestat ions:-Dyspnea at rest -Tachypnea (f lushed -Dyspnea at rest -Tachypnea (f lushed
appearance)appearance)-Patient wil l be thin-Patient wil l be thin


Investigations:Investigations:
1-Spirometer1-Spirometer2-Arterial blood gases 2-Arterial blood gases 3-Blood test (Polycythemia)3-Blood test (Polycythemia)4-X-ray to differentiate between two 4-X-ray to differentiate between two
diseases.diseases.

Emphysema
Bronchit is

Treatment:Treatment:
-Stop smoking-Stop smoking1-Antibiot ics1-Antibiot ics2-Bronchodilator 2-Bronchodilator -- Salbutamol (200-800ug/d inhalation) orSalbutamol (200-800ug/d inhalation) or-Ipratropium (80-120 ug/d inhalation)-Ipratropium (80-120 ug/d inhalation)3-Predinsolone tab. 30mg/d for 2 weeks if there is 3-Predinsolone tab. 30mg/d for 2 weeks if there is
improvement 200-500ug twice daily should be improvement 200-500ug twice daily should be taken.taken.
4-Mucolyt ic (Bromhexin 16mg t id oral) or 4-Mucolyt ic (Bromhexin 16mg t id oral) or expectorant (Guaifenesin 200mg tid oral)expectorant (Guaifenesin 200mg tid oral)
5-Inf luenza vaccination5-Inf luenza vaccination

Case studiesCase studiesCase 1Case 1::
M.R is a 60-year man, who is heavy smoker for the past 40 M.R is a 60-year man, who is heavy smoker for the past 40 years. He has had a chronic cough for the past 6 years, years. He has had a chronic cough for the past 6 years, often producing grey sputum. He is overweight and often producing grey sputum. He is overweight and
occasionally becomes breathlessoccasionally becomes breathless. . M.R was admitted to hospital with increasing M.R was admitted to hospital with increasing breathlessness, wheeze and productive cough. His breathlessness, wheeze and productive cough. His sputum was thick & green and he had a temperature of sputum was thick & green and he had a temperature of 39 C39 C°°. His present medication includes. His present medication includes::
--Salbutamol + Ipratropium combined inhaler 2 puffs four Salbutamol + Ipratropium combined inhaler 2 puffs four times a daytimes a day..
--Belomethasone inhaler 500ug twice a dayBelomethasone inhaler 500ug twice a day..--aminophylline slow release tab. 225 mg twice a dayaminophylline slow release tab. 225 mg twice a day..

QuestionsQuestions::
11--What is the probable diagnosis for this patientWhat is the probable diagnosis for this patient??
22--What factors lead to this caseWhat factors lead to this case??
33--Does this patient require antibiotics therapy? If Does this patient require antibiotics therapy? If so what would your recommended? Whyso what would your recommended? Why??
44--What other measures could be used to prevent What other measures could be used to prevent further exacerbationsfurther exacerbations??
55--Are there any particular precautions necessary if Are there any particular precautions necessary if influenza vaccination is administered to this influenza vaccination is administered to this
patientpatient??
66--What is the complication of chronic bronchitisWhat is the complication of chronic bronchitis? ?

Case 2Case 2::
H.C is a 68-year old male who presents to H.C is a 68-year old male who presents to emergency room (ER) with chief complaints of emergency room (ER) with chief complaints of fatigue and shortness of breath that has become fatigue and shortness of breath that has become progressively worse over the past two weeks. progressively worse over the past two weeks. He was seen by his local physician one week He was seen by his local physician one week ago, and treated with ampicillin for a presumed ago, and treated with ampicillin for a presumed upper respiratory infections. Over the past week upper respiratory infections. Over the past week dyspnea developed & worsened especially at dyspnea developed & worsened especially at rest. The past medical history is pertinent rest. The past medical history is pertinent EmphysemaEmphysema..
QuestionsQuestions::
11--What are signs& symptoms of EmphysemaWhat are signs& symptoms of Emphysema??
22--What are its etiology and investigationsWhat are its etiology and investigations??
33--What are the differences between COPD What are the differences between COPD underlying typesunderlying types??
44--What is the strategy in treatment acute COPDWhat is the strategy in treatment acute COPD??
55--What is the role of expectorant & mucolytic What is the role of expectorant & mucolytic agents in COPDagents in COPD??

ReferencesReferences
Walker and Edwards (eds). Clinical Walker and Edwards (eds). Clinical Pharmacy and Therapeutics. Third edition Pharmacy and Therapeutics. Third edition (2003).(2003).
Rang, Dale and Ritter Pharmacology Rang, Dale and Ritter Pharmacology (2009) (2009)
Katzung Katzung ––Basic and Clinical Basic and Clinical Pharmacology (2009)Pharmacology (2009)
British National Formulary (BNF) (2009)British National Formulary (BNF) (2009)