
Congestive Heart Failure Case Study. Congestive Heart Failure.

Randall C. Starling, MD, MPH, FACC,FESCProfessor Of Medicine
Heart Failure and Cardiac Transplant Medicine
Heart and Vascular Institute
Cleveland Clinic Lerner College of Medicine, CWRU
Cleveland Clinic
Cleveland OH USA
Clinical Pathways
Heart Failure Webinar
AMGA
May 31 2016

Survey Results
• Survey with 13 questions sent to AMGA
listserve n=50
• Survey designed to determine use of
clinical pathways in HF care
• Data represents 13 of 50 responses
26%
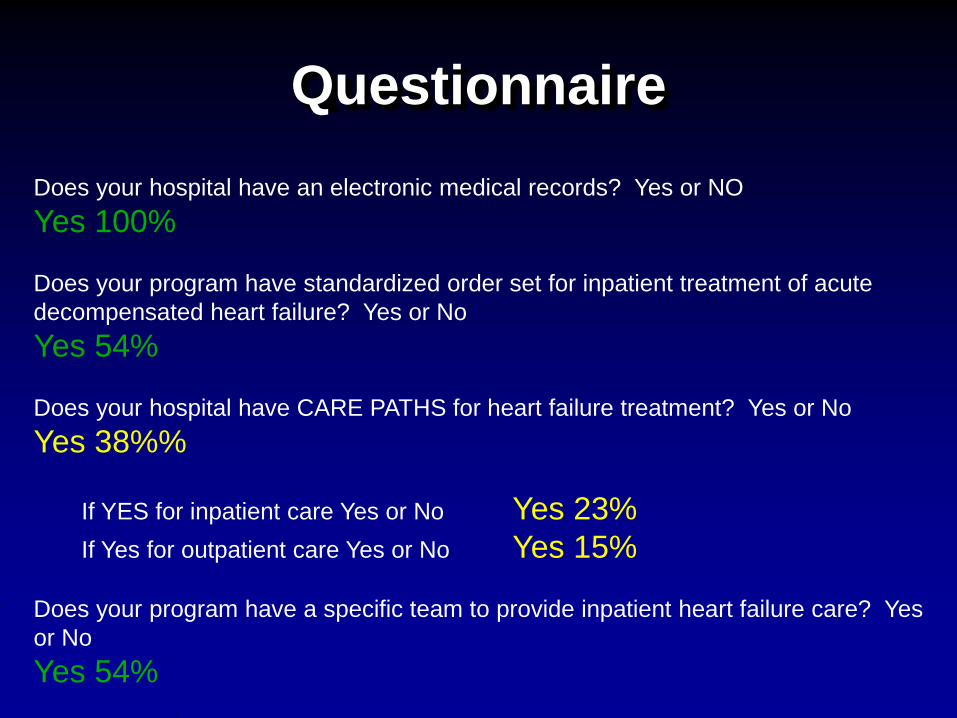
Questionnaire
Does your hospital have an electronic medical records? Yes or NO
Yes 100%
Does your program have standardized order set for inpatient treatment of acute
decompensated heart failure? Yes or No
Yes 54%
Does your hospital have CARE PATHS for heart failure treatment? Yes or No
Yes 38%%
If YES for inpatient care Yes or No Yes 23%
If Yes for outpatient care Yes or No Yes 15%
Does your program have a specific team to provide inpatient heart failure care? Yes
or No
Yes 54%

QuestionnaireDoes your program have a Heart Failure Disease Management Clinic with
dedicated staffing with expertise in HF care? Yes or No
Yes 69%
Does your HF program have a committee that reviews data periodically on HF
admissions demographics and readmission metrics. Yes or No
Yes 85%
Does your HF program have a standardized process for discharging HF
patients from the hospital? Yes or No
Yes 46%
Does your HF program require follow up visits within 1 week of hospital
discharge? Yes or No
Yes 92%

Questionnaire
Does your HF program require follow up visits at specific intervals after hospital
discharge? Yes or No
Yes 46%
Does your HF program offer home visits for homebound HF patients? Yes or No
Yes 85%
Does your HF program work directly with Skilled Nursing Facilities to optimize
care of HF patients? Yes or No
Yes 85%
Does your HF program offer structured HF education classes and or via written or
electronic media? Yes or No
62%

Questionnaire
Question: Please indicate the 30 day ALL CAUSE readmission rate for heart failure at your hospital
Number Who Answered: 13
25-30% 0 0%
20-25% 1 8%
15-20% 5 38%
10-15% 6 46%
less than 10% 1 8%
Question: Does your program offer heart transplant and or LVAD therapy?
Number Who Answered: 13
Yes No
5 8
38 % 62 %

Survey Take Aways
• EMR common
• Care Paths <50%
• Discharge Process not standardized
• Discharge Follow up very common
• Education materials provided
• GAPS: common practices to optimize
care and value?
- Risk Stratification

Introduction
• Accurate risk assessment tools to
predict readmission are needed
- Predicting risk of readmission and
reducing readmissions are two
separate challenges
• Validated care paths to reduce
readmissions or Episode of Care (EOC)
are needed
Kociol R et al. Am H Jour 2013;165:987-994.

Hypothesis
HF Clinical Pathways will:
improve quality of care
Reduce variability of care
Improve value and Reduce cost

We asked the question?
Are readmissions a sign
of poor quality care?

Are all readmissions bad
readmissions?
• Conclusions:
- Readmissions could be “adversely”
affected by a competing risk of
death.
- One simple measure isn’t enough?
Gorodeski, Starling, Blackstone. N Engl J Med 2010: 363:297-298.
Heidenreich P et al. J Am Coll Cardiol. 2010 Jul 27;56(5):362-8.
Krumholz H et al. JAMA. 2013;309(6):587-593

Kaplan-Meier curves for freedom from A, all-cause mortality, and B, all-cause rehospitalization stratified by discharge status.
Allen L A et al. Circ Heart Fail 2011;4:293-300
Copyright © American Heart Association
SNF: skilled nursing facility
N=15.459 Medicare
24.1% to SNF
Adjusted HR 1.75
Adjusted HR 1.08
OPPORTUNITY: PROCESS OF CARE FOR SNF

Ong MK et al. Circ Cardiovasc Qual Outcomes 2009;2:548-57.
From: Association of Hospital Spending Intensity With Mortality and Readmission Rates in Ontario Hospitals
JAMA. 2012;307(10):1037-1045. doi:10.1001/jama.2012.265
End-of-life expenditure index (EOL-EI) ranges, in Canadian dollars, are <$30 000 (US $29 970) for the low EOL-EI category,
$30 000 to $35 000 (US $29 970-$34 965) for the medium EOL-EI category, and >$35 000 (US $34 965) for the high EOL-EI
category. AMI indicates acute myocardial infarction; CHF, congestive heart failure.
Figure Legend:
Reducing
Readmissions
Labor intensive
EXPENSIVE
Mortality
Reduced Also
OPPORTUNITY:
TEAM WORK TO
IMPROVE OUTCOMES

“One thing is certain:
Rehospitalization after heart
failure admission is complex,
multifactorial, and not clearly
related to quality.”
O’Connor and Fiuzat. Editorial Comment.
JACC Vol. 56, No. 5, 2010.

WHY PATIENTS ARE READMITTED FOR HEART
FAILURE
Severe heart failure Polypharmacy
Inadequate treatment Healthcare illiteracy
End-of-life Poverty, social issues
Shortened LOS Medical noncompliance
Multiple co-morbidities Don’t purchase meds
Elderly, frail, confused Don’t take meds
Lack of followup Don’t call when sick

HVI Readmission Chart Review

Concept diagram
30-day HF
Readmission
Rate
All Cause:
HF related
other
Unavoidable
Planned,
Appropriate
Unplanned,
Avoidable (?)Poor care
CRT implant
Appendectomy
opportunity

Number of selected strategies implemented and risk-standardized readmission rates (RSRRs).
Bradley E et al. Circ Cardiovasc Qual Outcomes 2013;6:444-450
Copyright © American Heart Association

Discharge Checklist PilotJ72 Heart Failure Discharge Checklist PILOT
Sticker
Admission Date: ______________________
Nursing Date / Initials
? Care Partner Identified
? Nursing HF Education with Booklet
?Disease Education
?Daily Weights (patient calendar)
?Activity level
?I & Os
?Low Sodium Diet
?Fluid Restriction
?Medications
- Hand-outs given
- Initial Introduction
- Reinforcement
- Teach Back
? Survival Skills Class/EMMI TV Education (Course 560)
Multidisciplinary Consults Date / Initials
? Transitional Coach Consult
? age >65 years
? if needed, consult for high risk
? Seen by Transitional Coach
? If identified on Nursing Assessment: Nutrition consult placed
? If Nutrition consult not needed: Place Nutrition Screen
? Seen by Nutrition
? Pharmacy Education Consult placed for patients admitted w/ primary diagnosis heart failure
? EXCEPT post-CTS patient
? Seen by Pharmacy
Physicians/Nurse Practitioners Date / Initials
? Order for social support services/home care services/Heart Care at Home, if indicated
? Near optimal pharmacologic therapy initiated or achieved and any intolerances documented
? No symptomatic supine or standing hypotension (Orthostatic BPs require order)
? " Dry Weight" established and patient/caregiver informed of this goal
? Near optimal volume status achieved
? Stable renal function and acceptable electrolyte panel
? Core Measure Status Completed: Yellow Triangles Cleared
? Discharge medication reconciliation completed
MD/NP: PLEASE LIST PROVIDER PATIENT IS TO FOLLOW UP WITH (below and on blue appt. sheet)
Identify Primary Care Physician - Name ___________________________________________________________
7 Day LIP Appt/30 Day Cardiology MD Appt **BLUE APPT. SHEET COMPLETED**
7 Day LIP Appt/30 Day Cardiology MD Appt SCHEDULED (per HUC)
Case Management Date / Initials
? Discharge Needs identified
? Home Care visit offered
? Final post-discharge arrangements made

Explanation
•Comprehensive Domains: Nursing, Case
Management, Pharmacy, and
Physician/Mid-Level Provider
•Addresses Continuum of Care: Inpatient
Care, Transition, and Followup Care
Circ Heart Fail. 2012 Nov;5(6):680-7.

HF 30 Day Readmissions
All Cause 30 Day Readmissions
January 2014 to February 2016

Heart Failure 30 Day
Readmission RatesPatients on HF Electronic Checklist
Source: EBI Tableau 2015.
Quarterly Performance Goal 20%
* Through February 2016
10%
15%
20%
25%
30%
Q2.2014 Q3.2014 Q4.2014 Q1.2015 Q2.2015 Q3.2015 Q4.2015 Q1. 2016*

HF YTD 30 Day Readmission
Rates
Source: Outcomes Review 2016.04.06 *The most recent quarter may not contain the full three months

Heart Failure 30 Day
Readmission RatesPatients on HF Electronic Checklist
Source: EBI Tableau 2016.
Monthly Performance Goal 20%
19.6% 18.2%
JAN. '16 FEB. '16
2016

All Cause 30 Day Readmission
Rate Heart & Vascular Institute
Source: Outcomes Review 2016.04.06
Office of Clinical
Transformation
•Develop Care Paths to standardize care,
reduce variability, improve value
•System wide order sets
•System wide education tools
•Dedicated in patient HF team
•Dedicated out patient HF team
•Dedicated HF NPs both inpt and outpt
and transitional care

References Care Processes
1: Fonarow GC, Albert NM. Preface. Team-based Care for Heart Failure. Heart Fail Clin. 2015 Jul;11(3):xi-
xii.
2: Albert NM, Barnason S, Deswal A, Hernandez A, Kociol R, Lee E, Paul S, Ryan CJ, White-Williams C;
American Heart Association Complex Cardiovascular Patient and Family Care Committee of the Council on
Cardiovascular and Stroke Nursing, Council on Clinical Cardiology, and Council on Quality of Care and
Outcomes Research. Transitions of care in heart failure: a scientific statement from the American Heart
Association. Circ Heart Fail. 2015 Mar;8(2):384-409.
3: Fonarow GC, Albert NM, Curtis AB, Stough WG, Gheorghiade M, Heywood JT, McBride ML, Inge PJ,
Mehra MR, O'Connor CM, Reynolds D, Walsh MN, Yancy CW. Improving evidence-based care for heart
failure in outpatient cardiology practices: primary results of the Registry to Improve the Use of Evidence-
Based Heart Failure Therapies in the Outpatient Setting (IMPROVE HF). Circulation. 2010 Aug
10;122(6):585-96.
4: Albert NM, Fonarow GC, Yancy CW, Curtis AB, Stough WG, Gheorghiade M, Heywood JT, McBride M,
Mehra MR, O'Connor CM, Reynolds D, Walsh MN. Outpatient cardiology practices with advanced practice
nurses and physician assistants provide similar delivery of recommended therapies (findings from
IMPROVE HF). Am J Cardiol. 2010 Jun 15;105(12):1773-9.
5: Walsh MN, Yancy CW, Albert NM, Curtis AB, Stough WG, Gheorghiade M, Heywood JT, McBride ML,
Mehra MR, O'Connor CM, Reynolds D, Fonarow GC. Electronic health records and quality of care for heart
failure. Am Heart J. 2010 Apr;159(4):635-642.e1.
6: Albert NM, Fonarow GC, Yancy CW, Curtis AB, Stough WG, Gheorghiade M, Heywood JT, McBride M,
Mehra MR, O'Connor CM, Reynolds D, Walsh MN. Influence of dedicated heart failure clinics on delivery of
recommended therapies in outpatient cardiology practices: findings from the Registry to Improve the Use of
Evidence-Based Heart Failure Therapies in the Outpatient Setting (IMPROVE HF). Am Heart J. 2010
Feb;159(2):238-44.


















