Clinical Outcome in Aortic Regurgitation with ... - .pdfAortic regurgitation (AR) remains an...
27
Jane M. Francis, Adrian P. Banning, Jonathan P. Christiansen and Stefan Neubauer Saul G. Myerson, Joanna d'Arcy, Raad Mohiaddin, John P. Greenwood, Theodoros D. Karamitsos, Clinical Outcome in Aortic Regurgitation with Cardiovascular Magnetic Resonance Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2012 American Heart Association, Inc. All rights reserved. is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Circulation published online August 9, 2012; Circulation. http://circ.ahajournals.org/content/early/2012/08/09/CIRCULATIONAHA.111.083600 World Wide Web at: The online version of this article, along with updated information and services, is located on the http://circ.ahajournals.org//subscriptions/ is online at: Circulation Information about subscribing to Subscriptions: http://www.lww.com/reprints Information about reprints can be found online at: Reprints: document. Permissions and Rights Question and Answer available in the Permissions in the middle column of the Web page under Services. Further information about this process is Once the online version of the published article for which permission is being requested is located, click Request can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Circulation Requests for permissions to reproduce figures, tables, or portions of articles originally published in Permissions: at Ohio State University--Columbus on September 4, 2012 http://circ.ahajournals.org/ Downloaded from
Transcript of Clinical Outcome in Aortic Regurgitation with ... - .pdfAortic regurgitation (AR) remains an...

Jane M. Francis, Adrian P. Banning, Jonathan P. Christiansen and Stefan NeubauerSaul G. Myerson, Joanna d'Arcy, Raad Mohiaddin, John P. Greenwood, Theodoros D. Karamitsos,
Clinical Outcome in Aortic Regurgitation with Cardiovascular Magnetic Resonance
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2012 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation published online August 9, 2012;Circulation.
http://circ.ahajournals.org/content/early/2012/08/09/CIRCULATIONAHA.111.083600World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Circulation Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCULATIONAHA.111.083600
1
Clinical Outcome in Aortic Regurgitation with
Cardiovascular Magnetic Resonance
Running title: Myerson et al.; Aortic Regurgitation: Outcome with CMR
Saul G. Myerson, MBChB, MD, MRCP, FESC1; Joanna d’Arcy, MBChB, MRCP1;
Raad Mohiaddin, PhD, FRCR, FRCP, FESC2; John P. Greenwood, MBChB, PhD3; Theodoros D.
Karamitsos, MD, PhD1; Jane M. Francis, DCR(R), DNM1; Adrian P. Banning, MBBS, MD,
FRCP, FESC1; Jonathan P. Christiansen, MBChB, MD, FRACP, FACC, FCSANZ4;
Stefan Neubauer, MD, FRCP, FACC, FMedSci1
1Depts. of Cardiology & Cardiovascular Medicine; University of Oxford Centre for Clinical Magnetic Resonance Research, John Radcliffe Hospital, Oxford, 2CMR Unit, Royal Brompton Hospital and the National Heart and Lung Institute, London; 3Multidisciplinary Cardiovascular Research Centre (MCRC) & Leeds Institute of Genetics, Health and Therapeutics, University of
Leeds, Leeds, United Kingdom; 4North Shore Hospital, Auckland, New Zealand
Address for Correspondence:
Dr. Saul Myerson
Dept. of Cardiovascular Medicine
John Radcliffe Hospital
Headley Way
Oxford OX3 9DU, United Kingdom
Tel: +44 1865 222770
Fax: +44 1865 740449
E-mail: [email protected]
Journal Subject Codes: [30] CT and MRI; [124] Cardiovascular imaging agents/Techniques; [38] CV surgery: valvular disease
Karamitsos, MD, PhD ; Jane M. Francis, DCR(R), DNM ; Adrian P. Banning, MMBBBBB S,S, MMD,D
FRCP, FESC1; Jonathan P. Christiansen, MBChB, MD, FRACP, FACC, FCFCFCSASASANZNZNZ444; ;;
Stefan Neubauer, MD, FRCP, FACC, FMedSci1
11DDeDeptp s. oof f f CaCardrdioiolologygygy && CCarardidiovovaascsculularar MMedediciccinnne; UUniniveversitityy y oofof OOxfxforo d CeCentntrere fforor CClilinicacal fMaMagnetic Resesonono aaancecece RRReseseseaeaearcrcrchh,h, JJJohohohnn RRaRadcdclil fffffe HoHoHospitititalalal, , OxOxOxfofordrdr ,, 222CMCMCMRRR UnUnUnititit,, RoRoRoyayayall l BrBrBromomomptptptoon HoHoosps ital andnd thhee NNattiionnal l HeHeHeart t annd d LuLuung IInnnstituuutee,, LoLoondndndononon; 3MuMuMultidiiisccciplpllinnnarry CCaCardrdiiiovvvascccuullar ReReReseseearara chch CCCeneentrtreee ((M(MCRCRCRC)C) &&& LLLeeeeeedsdsds IInnsnstitiitutuutetete ooof f GGGennnettiticscss, , , HeHHealalalththh aaandndnd TTThheerarapepep ututu icics,s,s, UUnnnivveversrsiiityy y ofo
LLeLeeeds,s LLLeeeedsdsd , UUnUniti edd KKKiininggdomm;; 444NNoNortrthh ShShShorree HoHHospspiititaal, AuAuA ckckkllala dndnd, NeNew w ZZZealallana dd d
AdAddd ff CC dd
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.083600
2
Abstract:
Background - Current indications for surgery in patients with significant aortic regurgitation
(AR) focus on symptoms and left ventricular (LV) dilation/dysfunction. However, prognosis is
already reduced by this stage and earlier identification of patients for surgery could be beneficial.
Quantifying the regurgitation may help, but there is limited data on its link with outcome.
Cardiovascular magnetic resonance (CMR) can accurately quantify AR, and we examined
whether this was associated with the future need for surgery.
Methods and Results - 113 patients with echocardiographic moderate or severe AR were
monitored for up to 9 years (mean 2.6±2.1 years) following a CMR scan, and the progression to
symptoms or other indications for surgery was monitored. AR quantification identified outcome
with high accuracy: 85% of the 39 subjects with regurgitant fraction >33% progressed to surgery
(mostly within 3 years) compared to 8% of 74 subjects with regurgitant fraction 33%
(p<0.0001); area under the curve on receiver operating characteristic analysis 0.93 (p<0.0001).
This ability remained strong on time-dependent Kaplan-Meier survival curves. CMR-derived
end-diastolic volume (LVEDV) >246ml had good, though lower, discriminatory ability (AUC
0.88) but the combination of this with regurgitant fraction provided the best discriminatory
power.
Conclusions - High degrees of CMR-quantified AR were associated with the development of
symptoms or other indications for surgery. Quantifying AR showed slightly better discriminatory
ability than ‘Gold-standard’ CMR ventricular volume assessment. This could provide a new
paradigm for the timing of surgical intervention but requires confirmation in a clinical trial.
Key words: aortic regurgitation; aortic valve replacement; cardiovascular magnetic resonance imaging; outcome; prognosis
monitored for up to 9 years (mean 2.6±2.1 years) following a CMR scan, and thehe ppprororogrgrgresesessisisiononon tto
ymptoms or other indications for surgery was monitored. AR quantification identified outcome
withth hhhigigighhh acaca cucuc raaacycycy:: 85% of the 39 subjects with h rereregugg rgitant fraction >>333333%% progressed to surgery
mmmoosostly withhiniin 333 yyeaearsrsrs))) cococompmpmparararededed tttooo 8%8%8% oof ff 747474 ssubbbjeects s s wiwiwiththth rrregeggururu gigigitatatanntnt ffractcttioioionn n 33333 % % %
ppp<0<0<0.0. 000 1));; ararareaea uuundndeer ttthe cccururrvevev oon n n rereeceeeiviveerer ooopeperrarattitingngg ccchaharraractctererrissttic aannaalalysyssiss 00.99333 (p(p(p<<0..0000001))).
ThThThisisis aaabibibilililitytyty rrremememaiaiaineneneddd stststrororongngng ooonnn tititimememe d-d-depepepenenendededentntnt KaKaKaplplplananan M-M-Meieieiererer sssurururvivivivavavalll cucucurvrvrveseses. CMCMCMRR-R-dedederiririveveveddd
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCULATIONAHA.111.083600
3
Background
Aortic regurgitation (AR) remains an important cardiac condition,1, 2 although substantial chronic
regurgitation can be tolerated for many years, with patients remaining asymptomatic. Aortic
valve replacement is usually reserved for when symptoms or significant left ventricular (LV)
dilation or dysfunction occur,3, 4 but prognosis is already reduced by this stage.5-7 Earlier surgery
has been advocated,3, 8 but it is also important to avoid the increased risks associated with
premature surgery. Optimising the timing of surgery in these patients can therefore be difficult.
Quantifying the AR could be valuable for guiding management, especially in asymptomatic
patients with significant regurgitation, and might be used for the early identification of patients
requiring aortic valve surgery.
Cardiovascular magnetic resonance (CMR) is able to directly quantify aortic
regurgitation with high accuracy and reproducibility, using the technique of phase contrast
velocity mapping.9-11
As CMR also provides highly accurate measurements of left ventricular (LV) mass,
volumes and function12-15 (and is considered the ‘Gold-standard’ for measuring these), it would
appear to be an ideal technique for the assessment of aortic regurgitation, but the utility of CMR
to guide clinical management has not been evaluated. We sought to examine whether CMR
quantitation of aortic regurgitation and LV indices could identify which asymptomatic patients
with significant aortic regurgitation were likely to progress to symptoms or other established
indications for surgery in the near future. We also aimed to compare the CMR quantitation of
aortic regurgitation and LV volume/function indices for their relative predictive ability.
Methods
Subjects and follow up
equiring aortic valve surgery.
Cardiovascular magnetic resonance (CMR) is able to directly quantify aortic
eegugugurgrgrgitititatatatioioionn wiiththth hhigh accuracy and reproducibbbilililittyy, using the teechchc niiquququeee of phase contrast
vvelooocic ty mappipingngg.99-19-1111
AsAs CCCMRMRMR aallslsoo prprovovo ididesese hhhigigighlhlhlyy aacaccucucurararateee mmmeeaeassurrrememmenenentsss ooof f f leeeftftft vveenenttrtriciccululu arara (((LVLVLV)) mamamassss, ,
volumes and d fufufuncncn tititionono 121212-151515 (((ananand d isisis cconononsiiidededererered d d thththe e e ‘GGGololo d-d-stststaaandndndararrd’dd fororor mmmeaeaeasususuririr ngngng ttthehehesesese),)) it would
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCULATIONAHA.111.083600
4
Patients at least 18 years of age were recruited from four high-volume CMR centres in Oxford,
London, Leeds (UK) and Auckland (New Zealand). All asymptomatic patients with moderate or
severe chronic aortic regurgitation on echocardiography by standard (semi-quantitative)
assessment16 were eligible for inclusion and had a baseline CMR scan. Exclusion criteria
included the presence of other significant valve disease or clinical and/or angiographic evidence
for coronary disease.
Patients had a baseline CMR scan and were followed for up to 9 years. Those who
remained asymptomatic and under conservative management were designated the ‘conservative’
group, while those that developed symptoms or other established indications for surgery3 were
designated the ‘crossover’ group, with the decision for surgery taken as the point of censoring.
All clinical decisions were taken by the treating physician. In Oxford, patients participated in a
research study, with annual CMR scans, and clinical decisions were made without knowledge of
the CMR data. In the other three centres, study patients were identified from the clinical CMR
databases (though were initially diagnosed with echocardiography) and clinicians had access to
the CMR data. Events were only counted however if the reason for aortic valve surgery was for
established indications (primarily symptoms, excess LV dilation or LV dysfunction). Patients
undergoing aortic valve replacement for indications outside the established criteria3 (which do
not include CMR assessment), or when surgery was primarily for other surgery (e.g. aortic root
replacement) were considered to be in the conservative group but censored at the time of surgery.
In addition, a minimum period of two months was required between the CMR scan and the
decision for surgery, to avoid the potential bias of patients having a CMR scan ‘en-route’ to
surgery that had already been planned.
A third group was also included to compare CMR parameters with both the conservative
designated the ‘crossover’ group, with the decision for surgery taken as the poinnt t t ofoff cenenensososoririringngn ..
All clinical decisions were taken by the treating physician. In Oxford, patients participated in a
eeseseearararchchch ssstututudydyd , wiwiwitthth annual CMR scans, and clinnnicici aaal decisions wwerere e mamaaddede without knowledge of
hhhe CCMR dataa. InInIn ttthee ooththhererr tthrhrhreeee cccenenntrtreses,, stuududyyy paaatiieenttss wwwererre idideeenttitififiededed ffrorommm tththee clclc inininicici alal CCCMRMRMR
dadatatatabababaseses ss (t(t(thohohougugghh wewerrre iininitiialala lylyy dddiaiaiagngnososo ededed wwwititth hh eecechhohoccacardrdrdioioiogrgrrapapa hhyhy))) anana ddd cclclininnicici iaiaiansnss hhhadad aacccccesesss ttoto
he CMR datataa.. EvEvEvenenentstss wwwerrreee onono lylyy cccououountttededed hhhowowoweveve ererer iifff tthehee rreaeaeasososon n n fofof r r r aoaoaortrtrticicic vvvalala veveve sssurururgegegeryr was for ff
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCULATIONAHA.111.083600
5
and crossover groups. This group included patients already due for aortic valve replacement (the
‘surgical’ group), having developed established indications for surgery.3
The research study was approved by the Oxfordshire Central Research Ethics Committee
(Project code C02.020) and the Waitemata District Health Board “Knowledge Centre” in New
Zealand (Project number RM0980711302); all research subjects gave written informed consent.
CMR scanning
All scans were performed on 1.5 Tesla scanners (either Siemens Avanto [Siemens Medical
Solutions, Erlangen, Germany] or Philips Achieva scanners [Philips Healthcare, Best, The
Netherlands]) and analysed in each centre using the manufacturers’ software (Siemens Argus and
Philips ViewForum respectively) for both volumes and flow. All images were electrocardiogram
(ECG)-gated and most were obtained during an 8-16 second breath-hold to remove cardiac
motion due to the respiratory cycle. Subjects underwent a left ventricular function study as
previously described,14 consisting of a stack of contiguous short axis cine images from base to
apex, from which left ventricular end-diastolic and end-systolic volumes (LVEDV and LVESV
respectively) and mass were measured. Each value was also indexed to body surface area. Cine
image sequences were steady-state free precession (Siemens ‘TrueFISP’ or Philips ‘balanced fast
field echo’); temporal resolution 45msec; echo time 1.40-1.54msec; repetition time 2.80-
3.08msec; field of view 380x380mm; flip angle 50-60o).
Forward and regurgitant aortic flow were quantified using through-plane phase-contrast
velocity-mapping. This involves placing an image slice perpendicular to the direction of flow in
the aortic root, and measuring the velocity of flow through the image plane within each voxel.
From the resulting images, a region of interest identifying the aortic root is defined, and flow is
integrated for the whole cardiac cycle to provide forward and regurgitant flow through the aortic
Philips ViewForum respectively) for both volumes and flow. All images were eleleeectrtrtrocccararardididiogogograram
ECG)-gated and most were obtained during an 8-16 second breath-hold to remove cardiac n
momotititiononon dddueueue tttooo thheee rrerespiratory cycle. Subjects unnnddderrrwent a left venenntricucuulalalar r function study as
prevvvioi usly desscrcribibededd,,1411 ccconononsisiiststtining g g oofof aa ssttackkk oof cooonnttiguououousus sshhhorortt axxxisis ccininee imimmaagageses ffroroommm bababasese tooo
apapexexex, frfrf omomm wwwhihichchh lllefeft t veveentntriccuculalalarrr enenend-d-didid asasastototoliccc ananandd enend-d-d sysysysststolollicici vvvooolululummmess (L(LLVEVEVEDVDVV aaanddd LLLVEVEESVVV
espectivelyy) ) ) ananand d mamamasssss wwwererre e e mememeasasasururredede ... EaEaEachchch vvvalala uuue e e wawaw ss alala sososo iindndndexexe ededed ttto o o bobobodydyd sssurururfafafacecece aarea. Cine
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCULATIONAHA.111.083600
6
valve per cardiac cycle. The image plane was placed ~0.5cm above the aortic valve at end-
diastole, but maintaining a position in the aortic root throughout the cardiac cycle (Figure 1).
Imaging closer to the valve reduces the underestimation of regurgitation that can occur,17, 18 and
although increased turbulent flow can occur close to the valve,19 we have not found this to be a
problem in practice. If significant turbulence or aliasing was seen in the velocity image, the
acquisition was repeated a few millimetres further from the valve, and/or with a higher velocity
window. The original flow sequences9-11 acquire data over many cardiac cycles, taking
approximately two minutes with patients breathing freely, while newer magnetic resonance
sequences20 can acquire flow data within a single breath-hold (12-16 heart beats). Others have
suggested that the older free-breathing techniques may be more accurate for flow
quantification,19 as the newer sequences may be more prone to background flow offset errors
from the faster switching of magnetic field gradients (which can potentially cause significant
errors in flow quantification), but this has not been systematically examined. Free-breathing flow
sequences were used in Oxford and Leeds, while breath-hold flow sequences were used in the
other two centres. In all centres, the potential for background flow offset errors was reduced19 by
i) ensuring all flow sequences were acquired with the region of interest in the image slice located
at the isocentre of the magnet to minimise any inhomogeneities in the magnetic field, and ii)
using retrospective ECG-gating for all flow sequences, which also helps to ensure coverage of
the entire cardiac cycle. Image parameters: temporal resolution 25-55msec; echo time 2.6-
3.2msec; repetition time 4.3-7.8msec; field of view 320x320mm; velocity window 2.5-4.0m/sec;
signal averages: 1 for breath-hold sequences, 3 for free-breathing sequences; typical acquisition
time 12-16 seconds for breath-hold sequences, 2-3 minutes for free-breathing sequences. From
these images, forward and regurgitant aortic flow were measured by integrating the flow in each
uggested that the older free-breathing techniques may be more accurate for floww w
quantification,19 as the newer sequences may be more prone to background flow offset errors
frromomm ttthehehe fffasasasteteter swswwiititchc ing of magnetic field graddieieienntts (which can pppoto enntititiaalally cause significant
errrooorsr in flow qquuuannntififficici atatatioioion)n)n), bbubut t thththisi hhaaas nooot beeenn sysssteteemamaatiicacallllly exxamammiinnededd. FFrFreeeee-b-bbrerer aaathihihingngg ffflllow
eequququenenencecess wewewerere uuusseed d iinin OOxfxfoorord dd ananand d d LeLeeededdss,s, wwwhihihilelel bbrrereatatth-h--hohoholdldd fffloloow w sesesequququeenncecees s wewew rerere uuuseeed inin tthehehe
other two centnttrereres.s. IIIn n n alala l l l ceentntn rrreses,,, thththeee popootetetentntntiaiaiall fofoforr bababackckc grgrrouououndndnd flflflowowow oooffffffseseset t t erererroror rsrsrs wwwasasas rrrede uced191919 byyy
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.083600
7
frame over one cardiac cycle as previously described.9, 11 Regurgitant fraction (regurgitant
volume/forward volume x 100%) was also calculated.
Echocardiography
Clinical echocardiograms were acquired a mean of 22.9 ±81.5 days from the baseline CMR scan,
according to standard protocols.21 Assessment of the grade of AR on echocardiography was
based on multiple semi-quantitative and qualitative two-dimensional imaging parameters, as
suggested in the American Society of Echocardiography guidelines,16 with senior advice sought
in difficult cases. The echocardiograms were not performed specifically for the research study
however, and did not include the quantification of LV volumes or aortic regurgitation as current
guidelines recommend. Because of this limitation, LV end-diastolic and end-systolic diameters
and the semi-quantitative echocardiographic grading were not included in the predictive analysis
for comparison with CMR parameters.
Data assessment and statistical analysis
Receiver operating characteristic (ROC) analysis was used to determine the ability of the various
parameters to discriminate patients who would develop symptoms or other indications for
surgery during follow up, from those that remained asymptomatic. Differences in ROC area were
compared using the method of DeLong et al.22 Cox proportional hazards and multiple logistic
regression analyses were applied to any parameters with reasonable discriminatory ability (area
under the curve (AUC) on ROC analysis >0.70) to determine if any of these were independent
predictors. Cox proportional hazard analysis was performed in a binary fashion, comparing
groups above & below the optimal threshold identified on ROC analysis. Multiple logistic
regression analysis was performed using continuous variables, with subsequent binary analysis
for independent variables, again based on the thresholds identified from ROC analysis. Kaplan-
guidelines recommend. Because of this limitation, LV end-diastolic and end-syssttotoliliicc dididiammameteteterers s
and the semi-quantitative echocardiographic grading were not included in the predictive analysis
foor r cococommpmparararisisisooon wwwititith h CMR parameters.
DDattata assessmmenent aanandd d ststtatatatiisisttiticcacal l anananalalysysis
ReRececec iviviverer oopepeperaratitingngg cchhaararaactcterrisisi tititiccc (R(R(ROCOCC) ) anananaaalysysysisis wwwaas usussededed tooo dededetetermrmrmininne ththe e ababbililititty y y oof tttheee vvaraariooousu
parameters to o dididiscsccriririmimiminananatee pppatata ieeentntnts s whwhwhooo wowowoulululd d d dedeevevevelolol pp sysysympmpmptototomsmm ooor r otototheheher r r inindidid cacacatititiononons s for
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.083600
8
Meier survival curves are better for time-dependent events, and these were generated for any
independent parameters to illustrate their association with the progression to symptoms/surgery.
For group comparisons of CMR parameters, including the surgical group, one-way analysis of
variance (ANOVA) was used, with Bonferroni post-hoc analysis, after confirming normal
distributions of the variables using the Kolmogorov-Smirnov test. All analyses were performed
with SPSS version 17.0 (SPSS Inc., Chicago, USA) with the exception of the ROC and Cox
regression analyses which were performed with MedCalc version 9.3.1 (MedCalc Software,
Mariakerke, Belgium). Values shown are means standard deviation and a p-value of <0.05 was
considered the threshold for statistical significance.
Results
118 asymptomatic patients were considered for inclusion in the study, who had at least moderate
AR on echocardiography. Five were excluded because aortic valve surgery occurred within two
months of the CMR scan, leaving 113 patients, who were followed for up to 9 years (mean 2.6
±2.1 years). Thirty nine patients (35%) underwent aortic valve replacement during the follow-up
period, having developed symptoms (n=19) or other established echocardiographic indications
for surgery (excessive LV dilation [EDD >7.5cm or ESD >5.5cm], n=17); or reduced LV
function [echocardiographic ejection fraction <50%], n=3). These were designated the
‘crossover’ group. The mean time from CMR scan to the decision on surgery in this group was
21 months (median: 11 months), with 90% of events occurring within three years. Eight patients
underwent surgery primarily for aortic dilation and remained in the ‘conservative’ group but
censored at the time of surgery; mean regurgitant fraction in this group was 19% (range 5-30%).
One patient underwent aortic valve replacement surgery without conventional established
Results
111888 asasasymymptptptomommataticicic ppatients were considered for inininccllusion in the sstututudyy,, wwhwho had at least moderate
ARAR oon echocaardrdiioi grgrapapphyhyy. FiFiFivevee wwererereee eexcxccludeeeddd beccacauuse e e aaoaortrticic vvalallvee suurrrgeeery y oocccucurrrrrededd wwwitthihhin n twtwwo
momontntn hshshs ooofff thththee CMCMMRR R scscscanann,,, lel avavavining gg 11111 33 papapatititienenentsss,, , wwhwhooo wwewererere fffololo lololowwewed dd fofof rr r upupp tto o o 9 9 9 yeyeyeararars s (m(m(meaeaean n 222.66 6
±2.1 years).. TTThihihirtrtr y y y ninin nenene ppatatatieieientntn s s s (3(3( 5%5%5%) ) ) ununundedederwrwrwenenent t aoaoaortr icicc vvvalalalveveve rrrepee lalalacececememementntnt ddurururinining g g thththe e follow-uppp
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCULATIONAHA.111.083600
9
indications3 and was also retained in the conservative group. This patient was asymptomatic and
had surgery for LV ‘dilation’, but the echocardiographic end-diastolic diameter was 6.5cm; his
regurgitant fraction on CMR was 19%, and EDV 222ml.
Association with events
The ability of CMR parameters to identify patients at baseline who would develop indications for
surgery is shown in table 1 (ROC analyses). Quantitative measures of AR showed excellent
discriminatory power, with aortic regurgitant volume having an area under the curve (AUC) of
0.96 (p<0.0001), and regurgitant fraction an AUC of 0.93 (p<0.0001), with no statistical
difference between the two. CMR LV volumetric indices also showed good discriminatory
ability, though slightly lower than regurgitation quantification, with an AUC of 0.88 for LVEDV
and AUC 0.78 for LVESV (both p 0.01 vs. regurgitant volume). On multivariate analyses (table
2), only regurgitant fraction, regurgitant volume and LVEDV remained as independent
predictors. Binary analyses (comparing groups above/below the threshold identified on ROC
analysis) showed higher hazard ratios for regurgitant volume and fraction than LVEDV. The
differences in AUC and hazard ratios were small however, with some overlap of the confidence
limits, the latter likely due to the binary nature of the analyses and moderate sample size. In
general, regurgitant volume and fraction showed very similar discriminatory power; regurgitant
fraction has the modest advantage of being a body size-independent variable.
Regurgitant fraction >33% had high sensitivity (85%) and specificity (92%) for
identifying patients who progressed to symptoms and surgery (Figure 2). A single threshold
value may not provide all information however, and the data showed further useful thresholds:
all patients with a regurgitant fraction >51% (n=8) progressed to surgery (100% positive
predictive value), while all but two patients with a regurgitant fraction >43% (n=20) progressed
ability, though slightly lower than regurgitation quantification, with an AUC of 00.0.88888 ffforor LLLVEVEVEDDV
and AUC 0.78 for LVESV (both p 0.01 vs. regurgitant volume). On multivariate analyses (table
2)), , onononlylyly rregegegururrgitataanntnt fraction, regurgitant volumeee aaanndd LVEDV remmmaia needd d aaas independent
predddici tors. Binanarrry ananaalylyysesesesss (c(c(coomompapaparirir nngg ggrouupups abbbovve/bebebelolowww ththee ththhreeshshshololdd ididdeenentitifififiededed oonnn ROROROCC C
annalalalysysysisisi )) ) shshhowoowededd hhhigighhherr r hahazaaardrdd rrratatatioioios s fofoforrr rerereguguurrrgigitttannnt vvvolollumumumee anana ddd frfrfracaca ttitiononn tthhahan n n LVLVVEEDEDVV.V. TThehee
differences inin AAAUCUCUC aandndnd hazazazararard rararatitiososo wwwererreee smsmsmaaallll hhhowowwevvvererer,, wiwiwiththth ssommmeee ovovoverererlalal pp ofofof ttthehehe cconfidence
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.083600
10
to surgery (90% positive predictive value). At the other end of the scale, no patients with a
regurgitant fraction <26% (n=45) progressed to surgery (100% negative predictive value).
Survival curves are however better for assessing the effect of time on events (to account for the
fact that some events require adequate follow up to occur). There was significant separation of
the groups over time, with survival without surgery at the median time point (2.0 years) of 95%
for patients with regurgitant fraction 33% compared to 33% for patients with regurgitant
fraction >33% (p<0.0001 by logrank test). The data were also analysed using the highest
regurgitant fraction during follow up (there were 20 patients with serial CMR scans). This may
allow for increasing values over time and may also be closer to clinical practice (waiting until a
threshold is reached). Using the highest regurgitant fraction showed similar discriminatory power
on ROC analysis (AUC 0.93), and similar separation of survival curves at the median time point
of 1.9 years: surgery-free survival was 93% and 34% for regurgitant fractions 33% and >33%
respectively (Figure 3). In patients with highest regurgitant fraction 33%, longer term surgery-
free survival at 8 years showed a slight increase compared to analysis using the first recorded
regurgitant fraction (91% and 83% respectively), indicating the few patients that developed
higher degrees of regurgitation over time and were moved to the crossover group. All patients
with a regurgitant fraction >33% eventually had surgery over 8-9 years of follow up, but subject
numbers were small in the later years. The average time to surgery when using the highest
regurgitant fraction was slightly reduced, as would be expected (mean: 2.4 years, median: 1.9
years).
The association of aortic regurgitant fraction with outcome remained robust in sub-group
analyses. There was no significant difference between Oxford and the other participating centres;
table 3, p=0.59 by logrank test on Kaplan-Meier survival analysis (Figure 3c). Comparing
hreshold is reached). Using the highest regurgitant fraction showed similar disccriririmimim naaatototoryryry pppowowe
on ROC analysis (AUC 0.93), and similar separation of survival curves at the median time point
off 111.9.9.9 yyyeaeaarsrsrs:: ssurgrggeereryy-free survival was 93% and d 34343 %% for regurgittanaa t frfrracacactit ons 33% and >33%
eespppece tively (FiFiiggugurere 333).. IIn nn pappatititienentstst wwwiitthh higghheeest rregeggurgigigittatanntnt fffraraccttiooon n 33333 %,%, llloonongegeer rr tetetermrmm sssururggegerrry-
frreeeee sssurururvivivavaval l l atat 888 yyyeaearrss ssshohoweweed dd aaa slslsligiighthtt iincncncrerereasasse e e ccocompmpmpararededed tto o anana aaalysysysisisi uuussiingng tthehehe ffiririrststst reeecoorordedeedd
egurgitant frfracacactitit ononon (((91919 % %% ananand dd 83833%%% rrrese pepepectctctivivivelelely)y)y),,, ininndidid caaatititingngng ttthehehe fefef w w w papapatititienenentststs thahahat t t dededevevev loped
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCULATIONAHA.111.083600
11
centres using free-breathing CMR flow sequences (Oxford and Leeds) with the other two centres
using breath-hold sequences also showed no difference in the association of regurgitant fraction
with outcome (p=0.84 by logrank test on Kaplan-Meier survival analysis). Restricting the
analyses to only those patients that developed LV dilation or dysfunction as an indication for
surgery (excluding patients for whom symptoms developed) again showed a similar association
with outcome to the whole group. The area under the curve on ROC analysis was 0.91, and
survival without surgery to 2.0 years (the median time point) was 97% for those with regurgitant
fractions 33%, and 39% for those with regurgitant fraction >33% (p<0.0001 by logrank test).
The association of LVEDV with outcome appeared slightly lower than regurgitation
quantification, though the differences were slight and confidence limits overlap. Combining LV
end-diastolic volume with regurgitant fraction provided further improvement on either parameter
alone however (Figure 3d). The combination may thus provide the most robust discrimination,
especially given that both parameters are measured in one CMR examination. LV ejection
fraction was not able to predict events (AUC 0.55; p=0.43). CMR LV mass showed some
predictive power (AUC 0.74; p<0.0001), but this parameter is closely related to LVEDV, and the
similar mass:volume ratios in all groups (table 4) suggests that LVEDV is likely to be a
significant confounding factor.
Comparison with the surgical group
Data from the surgical group are shown in table 4. This showed similar mean aortic regurgitation
and LV volumetric indices to the crossover group and both were significantly larger than in the
conservative group. Ejection fraction was lower in the surgical group (mean 57.1% versus 62.9%
and 63.6% for the crossover and conservative groups respectively; p<0.01 for both comparisons),
perhaps reflecting a more advanced stage of the disease. The higher proportion of bicuspid
quantification, though the differences were slight and confidence limits overlap.. CoCoCombmbbininininining g g LVLV
end-diastolic volume with regurgitant fraction provided further improvement on either parameter
allononne e hohohoweweweveveer ((FiFiFiggugure 3d). The combination mmmayaya tthus provide ththhe e momooststst robust discrimination,
espeeecic ally givvenen thhhat t bobob ththth pppaararaamametettererrs s araree meeeaassureeded in ononone e CMCMCMRR exxamaminii aatatioioon.n. LLV VV ejejejecectit oonon
frracacctitiiononon wwasasas nnotot abblblee ttto pppreredidiictct eeeveveventnnts s (A(AAUCUCUC 000.5.5. 555; ppp==00.4.443)3)3).. CMCMCMR R R LVLVLV mmasasa s s shshshowowowededed somomome e
predictive ppowowwerere (((AUAUAUCCC 0.747474;;; p<<<0.0.0 0000000111))),, bububut t thththisiss ppparararamammetete ererer iiis s s clclclosoo elelely y y rererelalalateteted d tototo LLLVEVEVEDVD , and thhee
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCULATIONAHA.111.083600
12
valves in the crossover group (0.55, compared to 0.29 in the conservative group, p=0.003 by Chi-
squared analysis), might be explained by the slightly higher mean regurgitant fraction (mean
33.4% vs. 25.8% for tricuspid valves; p=0.004).
Discussion
The association of aortic regurgitation quantitation with outcome
Our data demonstrate the potential value of quantifying aortic regurgitation with CMR, which
showed a significant association with the future need for surgery, including patients who
developed asymptomatic LV dilation or dysfunction. Patients already destined for surgery (the
‘surgical’ group) also had measures of aortic regurgitation that were not significantly different
from the ‘crossover’ group, suggesting that a similar threshold of regurgitation had been reached
in the surgical group before symptoms occurred. These CMR parameters might thus be
predictors of future events, but this requires testing in a future prospective study.
Comparison with LV volumetric indices
Quantifying the regurgitation showed a slightly better association with events than CMR-derived
LV indices, despite highly accurate measurements of LV volumes and function by CMR.
LVEDV still had good discriminatory power however, and was an independent predictor on
multivariate analyses. The combination of LVEDV with regurgitant fraction provided a slight
enhancement over aortic regurgitation alone, and LV volumes and function are important in the
overall assessment of the patient. Given these factors, and that both are readily available from a
standard CMR scan, the combination of CMR quantification of aortic regurgitation and LV
volumes could be a valuable component of the work-up in patients with aortic regurgitation. The
slightly stronger association of outcome with aortic regurgitation indices compared to LV
surgical’ group) also had measures of aortic regurgitation that were not significacaa tntlylyl dddifififfefeferererentnt
from the ‘crossover’ group, suggesting that a similar threshold of regurgitation had been reached
nn tthehehe sssururgigigicacacal grgrrouououpp before symptoms occurredd. ThThhese CMR pararaameeteteersrsrs might thus be
predddici tors of fufututuurree eevvvenntnts,s,s bbbututut tthihiiss rerer qququiires teeestinnngg in aaa ffututuuurree pprrorospspecctit vveve ssstututudydy..
CoCoompmpmparara isissononon wwititthh LVLVV vvvololummmetetetririricc c iininddidicececesss
Quantifying g ththhe e e rereegugugurgrgrgitititatioioion n n shhhowowowedede aaa sslililighghghtltltly y y bebebettttt erere aaassssssococociaiai tititiononon wwwititth h h evevevenenentsts ttthahahan n n CMCMC R-derivedddd
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCULATIONAHA.111.083600
13
volumes, and the ability of regurgitant fraction to identify patients who would develop excess
LV dilation or dysfunction as indications for surgery, suggests that increases in regurgitation
may occur before LV dilation. This would be logical given that regurgitation is the physiological
stimulus for LV dilation in this patient group, though is not conclusively proven with our data.
LV mass showed reasonable discriminatory ability in identifying patients likely to
progress to surgery (AUC 0.74). It is however closely related to LV volume, and was not an
independent predictor on multivariate analysis. Other studies have not shown any predictive
power of wall thickness23 and the LV mass to volume ratios were similar for all three subject
groups in our study, suggesting that there is no excess increase in mass over that required for the
chamber volume increase, and that the apparent association of LV mass with outcome is likely to
be confounded by its close link to LV volume.
Comparison with echocardiography and other CMR studies
Echocardiographic techniques for quantifying aortic regurgitation also exist,24, 25 although there
are potential inaccuracies from the calculations and assumptions involved. Quantitative AR
assessment by echocardiography is primarily used to aid the grading of regurgitation severity,
and may have improved grading from the semi-quantitative assessment used to identify patients
in our study. It has also shown an association with the need for surgery,26 though in that paper
43% of patients with moderate AR on echocardiography progressed to surgery, suggesting a
lower ability of quantitative echocardiographic AR grading to identify patients at risk of events.
Previous studies comparing CMR with echocardiographic grading27, 28 suggest only a moderate
correlation, with significant overlap of CMR-quantified AR values across the echocardiographic
grades, particularly between moderate and severe grades. It is of interest that in the Gabriel
paper27 the AR groups defined as ‘truly severe’ had regurgitant volumes & fractions
chamber volume increase, and that the apparent association of LV mass with ouutctccommmee isisis lllikikikeleely y to
be confounded by its close link to LV volume.
CoCompmpmpaararisisisonono wititthh h eechocardiography and othererer CCCMR studies
EEchhohocardiograpaphhih ccc tetechchc nininiquqqueseses ffororr qqquauau ntntiifyingngng aorrrtiicc reeeggugurgrggittatatioioonn alalsoo exixiststt,24,24,24, 25255 aaaltltthohohougugugh hh thththererre
arre e e popopotetet ntntiaiaal l l ininacacccucuuraracccieeses ffrooom m m thththe ee ccacalclcculululatatatiioionsnsns aandndnd asssssumumumppptioioonsnsns invnvnvololvveved.d. QQQuauauantntiititaatativvvee AARAR
assessment bby y y ecece hohohocacac rdrdrdioi grgrgrapapaphyhyhy iiiss prpp imimmarararililly y y usususedede totoo aaididd tthehehe gggrararadidd ngngng ooof f f rereregugugurgrggitititatatatioioon n n ses verity,
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCULATIONAHA.111.083600
14
predominantly above the thresholds we identified in our study. Other CMR studies of AR
quantitation11, 28, 29 also showed significant overlap between quantitative values and AR grades
by other techniques, but none have examined the potential value of AR quantitation in clinical
management.
Comparison with previous studies of outcome in aortic regurgitation
Bonow et al’s 1991 study23 had similar methodology to our own, in a similar sized group of
patients, and examined the prediction of clinical events in initially asymptomatic patients who
underwent echocardiography. Both this and the 1995 Tornos study4 showed a predictive ability
for end-diastolic diameter (>7.0cm) and end-systolic diameter (>4.0cm but especially >5.0cm).
These findings are in keeping with our data which showed an association with outcome for end-
diastolic and end-systolic volumes, though the addition of CMR measurements of LV volume
and quantification of AR adds to these existing studies with more modern imaging techniques.
Other studies have examined the prediction of outcome post-surgery in patients with aortic
regurgitation,5, 6, 30 or in a mixed asymptomatic and pre-surgical group of patents,31 and
confirmed that symptoms, reduced ejection fraction and excess LV dilation are associated with
worse long term outcome. These studies helped inform the current guidelines for surgery in
aortic regurgitation,3 but also highlight the value in identifying patients prior to symptoms or
significant LV dilation or dysfunction, as this study aims to do.
Clinical utility
The ability to identify patients prior to symptoms or excess LV dilation/dysfunction would be
clinically important. These patients might be considered for early surgery, and at the very least
could be followed more closely. Our sample size was modest however, and to support a change
in clinical practice, particularly where cardiac surgery is concerned, requires better
These findings are in keeping with our data which showed an association with oouuutcocoomememe fffororor eeendnd-
diastolic and end-systolic volumes, though the addition of CMR measurements of LV volume
annd d d quququaanantititififificaationonon oof AR adds to these existing stststududdies with moree mmodddererernn imaging techniques.
OOOthheher studies hahaveveve eexxaamimiminenened d d thththe e prprpredede iicttiion offf outtctcomome e e popossts --ssururgegeeryy iiinnn ppapatitiienenentsts wwwititth h h aoaortrttiicic
eegugugurgrgrgititi atatioioon,nn,5, 5, 6,6, 300 oor r inin aa mmixixixededed aaasysysympmpptototomamamatiiicc c aandndnd pprrere-s-ssurururgigigicacacal l grgrgrouououpp p offf ppatatatenenntsts,,,3331 andndd
confirmed thhatatat sssymymymptptp omomoms, rrredededucuccededed eeejejej ctctctioioon n n frfrracacactitiiononn aaandndd eeexcxcxcesesess s s LVLVLV dddilililatatatioioion n n ararre ee asasassososocicic ated with
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCULATIONAHA.111.083600
15
demonstration of patient benefit in a randomised trial comparing early surgery with surgery
based on conventional indications. Quantitative CMR indices may provide the appropriate tool
for identifying suitable patients for such a trial. Conversely, patients with lower quantities of
aortic regurgitation and LV end-diastolic volume might be reassured of the good medium term
prognosis, and may require less frequent follow-up, aiding the efficient use of healthcare
resources.
Limitations
The moderate sample size and relatively small number of events limit the strength of our
conclusions, though follow up was for a reasonable period of time (mean 2.6 years, and up to 9
years).
The lack of blinding to the CMR data in three of the centres may also have biased results.
There are however no current CMR criteria/thresholds for recommending surgery, and we
attempted to minimise any bias where possible, and confirmed that there were no significant
differences in the association with the progression to surgery between centres. It is possible
however that some bias remains, particularly given the subjective nature of symptom assessment.
The CMR sequence for flow measurement also differed between centres, as did the analysis
software, but the associations with outcome were no different between sub-groups, which
suggests the results may be generalizable for both types of sequence and different vendor
software.
There remain a limited number of contra-indications to MRI, including most pacemakers
and other implanted metallic devices, and a few patients are unsuitable for CMR. Prosthetic heart
valves are not a contra-indication, however.
years).
The lack of blinding to the CMR data in three of the centres may also have biased results
Thhererere e e aararee hohohowwweveveverrr nno current CMR criteria/threeeshshshooolds for recommmemm ndddininingg surgery, and we
attteempm ted to mminininimmmisiseee anananyy bibibiaasas wwheheherere ppoossiiblblee, andndnd conononfifirmrmmeeded tthahat t ththheeeree weweereree nno o sisiigngng ifii iciccanant tt
didifffffferererenenencecesss ininin tthehee aaassssooociiaatitionnn wwwititithhh thththe e prprprogogogrreressssssioioi nnn ttoto sssururrgegegerryry bebeb twtwtweeeeeen n cecentntrerees.s. IIt t iisis pppossssiiblblb e e
however thatt sssomomomee e bibib asasa remmmaiaiainsss, , papapartrtr icccululu arararlylyly gggiiiveveen n n thththe sususubjbjbjecece tititivevev nnnatatatururureee ofofof ssymymymptptptomomom assessmenttt
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.083600
16
Conclusions
Quantification of aortic regurgitation with CMR showed significant associations with outcome,
particularly when combined with CMR-derived LV volume. The study was of moderate size
however and not all clinicians were blinded to the CMR results. These CMR parameters might
prove useful for identifying suitable patients for early aortic valve replacement, but a clinical
trial is recommended to confirm this and determine clinical benefit.
Acknowledgements: The authors would like to thank Jacqueline Birks for expert statistical
advice.
Funding Sources: The research study was funded by a project grant from the Garfield-Weston
Trust, London, UK (PMS/MMS – 02/03-620). The work was also supported by the Oxford
National Institute for Health Research (NIHR) Biomedical Research Centre programme, and the
NIHR Cardiovascular Biomedical Research Unit of the Royal Brompton and Harefield NHS
Foundation Trust and Imperial College London. SN acknowledges support from the Oxford
British Heart Foundation Centre of Research Excellence.
Conflict of Interest Disclosures: None.
References:
1. Iung B, Baron G, Butchart EG, Delahaye F, Gohlke-Barwolf C, Levang OW, Tornos P, Vanoverschelde JL, Vermeer F, Boersma E, Ravaud P, Vahanian A. A prospective survey of patients with valvular heart disease in europe: The euro heart survey on valvular heart disease. Eur Heart J. 2003;24:1231-1243. 2. Singh JP, Evans JC, Levy D, Larson MG, Freed LA, Fuller DL, Lehman B, Benjamin EJ. Prevalence and clinical determinants of mitral, tricuspid, and aortic regurgitation (the framingham heart study). Am J Cardiol. 1999;83:897-902. 3. Bonow RO, Carabello BA, Kanu C, de Leon AC, Jr., Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O'Gara PT, O'Rourke RA, Otto CM, Shah PM, Shanewise JS, Smith SC, Jr., Jacobs AK, Adams CD, Anderson JL, Antman EM, Faxon DP, Fuster V, Halperin JL, Hiratzka LF, Hunt SA, Lytle BW, Nishimura R, Page RL, Riegel B. Acc/aha 2006 guidelines for
Funding Sources: The research study was funded by a project grant from the GGaaarfifiieleld-d-d-WeWeWestststonon
Trust, London, UK (PMS/MMS – 02/03-620). The work was also supported by the Oxford
National Institute for Health Research (NIHR) Biomedical Research CeCentre programme, and the
NINIIHRHRHR CCarrdididiooovasascuculalar BiB omomeddicical RResseaarcr h UnU itit offf the RoRoyay l BrBrromoo ptptonon andd HHara efieeldld NNHS
FFouunundation Trurussst aaandndd Impmpmpeereriaiaialll CoCoolllllegege ee LLLonnddooon. SNSNSN ackckcknonowlwlwlededgggess susuppppoorort t frfrfromom ttthehehe OOOxfxffoorord dd
BrBrrititisisi h h Hearrtt t FoFoF ununundadattiionn CCeenentrtrtre e ofoff RRReeseeaearcrchhh EExExceellllenenncecee..
Conflict of InInIntetetererereststst DDDisissclclosososuuureses::: NoNoN nenene.
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCULATIONAHA.111.083600
17
the management of patients with valvular heart disease: A report of the american college of cardiology/american heart association task force on practice guidelines (writing committee to revise the 1998 guidelines for the management of patients with valvular heart disease): Developed in collaboration with the society of cardiovascular anesthesiologists: Endorsed by the society for cardiovascular angiography and interventions and the society of thoracic surgeons. Circulation. 2006;114:e84-231. 4. Tornos MP, Olona M, Permanyer-Miralda G, Herrejon MP, Camprecios M, Evangelista A, Garcia del Castillo H, Candell J, Soler-Soler J. Clinical outcome of severe asymptomatic chronic aortic regurgitation: A long-term prospective follow-up study. Am Heart J. 1995;130:333-339. 5. Hwang MH, Hammermeister KE, Oprian C, Henderson W, Bousvaros G, Wong M, Miller DC, Folland E, Sethi G. Preoperative identification of patients likely to have left ventricular dysfunction after aortic valve replacement. Participants in the veterans administration cooperative study on valvular heart disease. Circulation. 1989;80:I65-76. 6. Turina J, Milincic J, Seifert B, Turina M. Valve replacement in chronic aortic regurgitation. True predictors of survival after extended follow-up. Circulation. 1998;98:II100-106; discussion II106-107. 7. Chaliki HP, Mohty D, Avierinos JF, Scott CG, Schaff HV, Tajik AJ, Enriquez-Sarano M. Outcomes after aortic valve replacement in patients with severe aortic regurgitation and markedly reduced left ventricular function. Circulation. 2002;106:2687-2693. 8. Enriquez-Sarano M, Tajik AJ. Clinical practice. Aortic regurgitation. N Engl J Med. 2004;351:1539-1546. 9. Dulce MC, Mostbeck GH, O'Sullivan M, Cheitlin M, Caputo GR, Higgins CB. Severity of aortic regurgitation: Interstudy reproducibility of measurements with velocity-encoded cine mr imaging. Radiology. 1992;185:235-240. 10. Honda N, Machida K, Hashimoto M, Mamiya T, Takahashi T, Kamano T, Kashimada A, Inoue Y, Tanaka S, Yoshimoto N. Aortic regurgitation: Quantitation with mr imaging velocity mapping. Radiology. 1993;186:189-194. 11. Sondergaard L, Lindvig K, Hildebrandt P, Thomsen C, Stahlberg F, Joen T, Henriksen O. Quantification of aortic regurgitation by magnetic resonance velocity mapping. Am Heart J. 1993;125:1081-1090. 12. Bellenger NG, Burgess MI, Ray SG, Lahiri A, Coats AJ, Cleland JG, Pennell DJ. Comparison of left ventricular ejection fraction and volumes in heart failure by echocardiography, radionuclide ventriculography and cardiovascular magnetic resonance; are they interchangeable? Eur Heart J. 2000;21:1387-1396. 13. Hudsmith LE, Petersen SE, Francis JM, Robson MD, Neubauer S. Normal human left and right ventricular and left atrial dimensions using steady state free precession magnetic resonance
True predictors of survival after extended follow-up. Circulation. 1998;98:II100-101006;6;6 ddisiscucussssioi nI106-107.
7. Chaliki HP, Mohty D, Avierinos JF, Scott CG, Schaff HV, Tajik AJ, Enriquez-Sarano M.Outcomes after aortic valve replacement in patients with severe aortic regug rgitation and mamarkrkrkedededllyly rrredededuucededed llefe t ventricular function. Circccuululaattion. 2002;10666:2: 6887-7-7-22693.
88.. EEEnrn iquez-Saararaanooo MMM, TaTaTajijijik k k AJAAJ.. ClClClininii acaal prrracccticeee. AoAorrrtitiic c rreeggugurgrggittatatioionnn. NN N EnEnEngglgl JJJ MMMededed... 2020004044;351:153539-1151546.
9. DDululce MMC,C MMosstbtbece k GHG , O'O'SuSulll ivann MM, ChCheieitlin MM, CaCapuputot GGR,R, HHiggiginsns CCB.B. Seveveritity y ofo aortic regurgigig tatatatitit ononon::: InInnteteersstututudydyd rrreeeprprp ododo ucucucibibbilillititi yy y ofofof mmmeaeae suuurererememementntntsss wwititith h h vevevelololocicicityty-e-eencncncodododedee cine mr mmagaginingg RaRadidiolologogyy 19199292;1;18585:2:23535 2-24040
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCULATIONAHA.111.083600
18
imaging. J Cardiovasc Magn Reson. 2005;7:775-782. 14. Lorenz CH, Walker ES, Morgan VL, Klein SS, Graham TP, Jr. Normal human right and left ventricular mass, systolic function, and gender differences by cine magnetic resonance imaging. J Cardiovasc Magn Reson. 1999;1:7-21. 15. Myerson SG, Bellenger NG, Pennell DJ. Assessment of left ventricular mass by cardiovascular magnetic resonance. Hypertension. 2002;39:750-755. 16. Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD, Levine RA, Nihoyannopoulos P, Otto CM, Quinones MA, Rakowski H, Stewart WJ, Waggoner A, Weissman NJ. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and doppler echocardiography. J Am Soc Echocardiogr. 2003;16:777-802. 17. Chatzimavroudis GP, Walker PG, Oshinski JN, Franch RH, Pettigrew RI, Yoganathan AP. Slice location dependence of aortic regurgitation measurements with mr phase velocity mapping. Magn Reson Med. 1997;37:545-551. 18. Myerson SG. Heart valve disease: Investigation by cardiovascular magnetic resonance. JCardiovasc Magn Reson. 2012;14:7. 19. Kilner PJ, Gatehouse PD, Firmin DN. Flow measurement by magnetic resonance: A unique asset worth optimising. J Cardiovasc Magn Reson. 2007;9:723-728. 20. Sakuma H, Kawada N, Kubo H, Nishide Y, Takano K, Kato N, Takeda K. Effect of breath holding on blood flow measurement using fast velocity encoded cine mri. Magn Reson Med. 2001;45:346-348. 21. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise JS, Solomon SD, Spencer KT, Sutton MS, Stewart WJ. Recommendations for chamber quantification: A report from the american society of echocardiography's guidelines and standards committee and the chamber quantification writing group, developed in conjunction with the european association of echocardiography, a branch of the european society of cardiology. J Am Soc Echocardiogr. 2005;18:1440-1463. 22. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics. 1988;44:837-845. 23. Bonow RO, Lakatos E, Maron BJ, Epstein SE. Serial long-term assessment of the natural history of asymptomatic patients with chronic aortic regurgitation and normal left ventricular systolic function. Circulation. 1991;84:1625-1635. 24. Enriquez-Sarano M, Seward JB, Bailey KR, Tajik AJ. Effective regurgitant orifice area: A noninvasive doppler development of an old hemodynamic concept. J Am Coll Cardiol. 1994;23:443-451.
18. Myerson SG. Heart valve disease: Investigation by cardiovascular magnetic rrresesonono anana cecece. JJJCardiovasc Magn Reson. 2012;14:7.
19. Kilner PJ,J, GGatehouse PD, Firmin DN. Flow measurement by magnetic resonance: A uniqueassseseettt wwowortrtrth h h opoptimimimisising. J Cardiovasc Magn Resosoonn. 2007;9:723-772822 .
2200. SSakuma HH, KaKaKawawadadad NNN, KuKuKubbobo HHH,, NNisshhideee YYY, TTakkkannoo KK,, KKaKatoto NNN, TaTaT kekeedada KKK.. EfEfffefefectctc ooof brbrbreaeaathhh hohoholdddini g on bblolooddd ffflowww mmmeasasururrememennt t t uussininng ffafasst veellooccitity y y enenencccodddeddd cciine mmmrrii.. MaMaMagngn RRResssononn MMMedd. 200001010 ;4;4;45:5:343446-6-6-3434888.
21. Lang RM,M,M, BBBieieeriririg gg M,M,M DDDeveveverere eueueuxx x RBRBRB, , FlFlFlacacchshshskakakampmpmpfff FFA,A,A FFFososo teteter r r E,E,, PPPelele lililikkkkkka aa PAPAA,, PiPiPicacacardr MH, ffRoRomamann MJMJ SeSewawardrd JJ ShShananewewisisee JSJS SoSololommonon SSDD SSpepencncerer KKTT SSututtotonn MSMS StStewewarartt WJWJ
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCULATIONAHA.111.083600
19
25. Tribouilloy CM, Enriquez-Sarano M, Fett SL, Bailey KR, Seward JB, Tajik AJ. Application of the proximal flow convergence method to calculate the effective regurgitant orifice area in aortic regurgitation. J Am Coll Cardiol. 1998;32:1032-1039. 26. Detaint D, Messika-Zeitoun D, Maalouf J, Tribouilloy C, Mahoney DW, Tajik AJ, Enriquez-Sarano M. Quantitative echocardiographic determinants of clinical outcome in asymptomatic patients with aortic regurgitation: A prospective study. JACC Cardiovasc Imaging. 2008;1:1-11. 27. Gabriel RS, Renapurkar R, Bolen MA, Verhaert D, Leiber M, Flamm SD, Griffin BP, Desai MY. Comparison of severity of aortic regurgitation by cardiovascular magnetic resonance versus transthoracic echocardiography. Am J Cardiol. 2011;108:1014-1020. 28. Kutty S, Whitehead KK, Natarajan S, Harris MA, Wernovsky G, Fogel MA. Qualitative echocardiographic assessment of aortic valve regurgitation with quantitative cardiac magnetic resonance: A comparative study. Pediatr Cardiol. 2009;30:971-977. 29. Ambrosi P, Faugere G, Desfossez L, Habib G, Bory M, Luccioni R, Bernard P. Assessment of aortic regurgitation severity by magnetic resonance imaging of the thoracic aorta. Eur Heart J. 1995;16:406-409. 30. Klodas E, Enriquez-Sarano M, Tajik AJ, Mullany CJ, Bailey KR, Seward JB. Optimizing timing of surgical correction in patients with severe aortic regurgitation: Role of symptoms. J Am Coll Cardiol. 1997;30:746-752. 31. Dujardin KS, Enriquez-Sarano M, Schaff HV, Bailey KR, Seward JB, Tajik AJ. Mortality and morbidity of aortic regurgitation in clinical practice. A long-term follow-up study. Circulation. 1999;99:1851-1857.
of aortic regurgitation severity by magnetic resonance imaging of the thoracic aortrta.a.a. EuEur r HeHearart J1995;16:406-409.
30. Klodas E, Enriquez-Sarano M, Tajik AJ, Mullany CJ, Bailey KR, Seward JB. Optimizing imingg of surggical correction in patients with severe aortic regurgitation: Role of symptoms. J Am
CoCollllll CCCaarardididiololol.. 199979797;3;30:746-752.
331. DDujardin KKS,S,S EEEnrnriqiqi uueuez-z-SaSaSarraranonoo MMM, SScchaffff HHVV,, BBBaillleyeyey KKKRR,R, SSewewwararddd JBBB, TaTaTajjijik k AJAJAJ.. MMMortrtrtalalititi yy anannd d mom rbiditity yy offf aaaortiicc rreguguurgrggiti atatioon n n iinn cccliniiicaaal prraractcticicce.e.e. AAA looong--teeerm fffolllloow-w-w-upup sttutuddydy.. CiCiircrcrculululatata ioionnn.. 119199999;9;999:9:18185151-11858585777.
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCULATIONAHA.111.083600
20
Table 1. Receiver operating characteristic (ROC) data. Comparison of the ability of each CMR parameter to identify the initially asymptomatic patients who would develop indications for surgery, using receiver operating characteristic (ROC) analysis.
AUC Threshold p Sens (%) Spec (%)
Regurgitant fraction (%) 0.93 (0.87-0.97) > 33 <0.0001 85 92
Regurgitant volume (ml) 0.96 (0.90-0.99) > 42 <0.0001 92 85
Regurgitant volume index (ml/m2) 0.95 (0.89-0.98) > 23 <0.0001 82 92
LVEDV (ml) 0.88 (0.80-0.93) > 246 <0.0001 87 77
LVEDV index (ml/m2) 0.86 (0.79-0.92) > 129 <0.0001 85 82
LVESV (ml) 0.78 (0.70-0.86) > 88 <0.0001 77 70
LVESV index (ml/m2) 0.77 (0.68-0.84) > 45 <0.0001 74 72
Ejection fraction (%) 0.55 (0.45-0.65) < 59 0.43 38 77
LV mass (g) 0.74 (0.64-0.81) > 187 <0.0001 72 68
LV mass index (g/m2) 0.73 (0.63-0.81) > 90 <0.0001 74 64 AUC = area under the curve; LVEDV = left ventricular end-diastolic volume; LVESV = left ventricular end-systolic volume; p = p value for ROC curve; Sens = sensitivity; Spec = specificity; threshold = value for each parameter which best identified the ‘crossover’ group.
Ejection fraction (%) 0.55 (0.45-0.65) < 59 0.43 383838 777777
LV mass (g) 0.74 (0.64-0.81) > 187 <0.0001 72722 6688
LV mass index (gg/m2) 0.73 (0.63-0.81) > 90 <0.0001 74 64 AUAUCCC === aareaa uuundndnder tthehehe ccurve; LVEDV = left ventricular endndnd-dddiastolic volume;; LLLVEESVSVV == left ventricular end-systolicvovoolulummme; p = p vavavaluee fofoorr ROROCCC cucuurvrve;e; SSenene ss == sesensnsititivivitity;y;y; SSpeeec == spepecicifificicityt ; ththhrereshsholold d == vav luue e fofoorr eaeachch ppararamama etetterer wwhiccchh best identififieieied d ttthe e ‘c‘c‘ rooossssssovovovererer’ grgroououpp.p.
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.083600
21
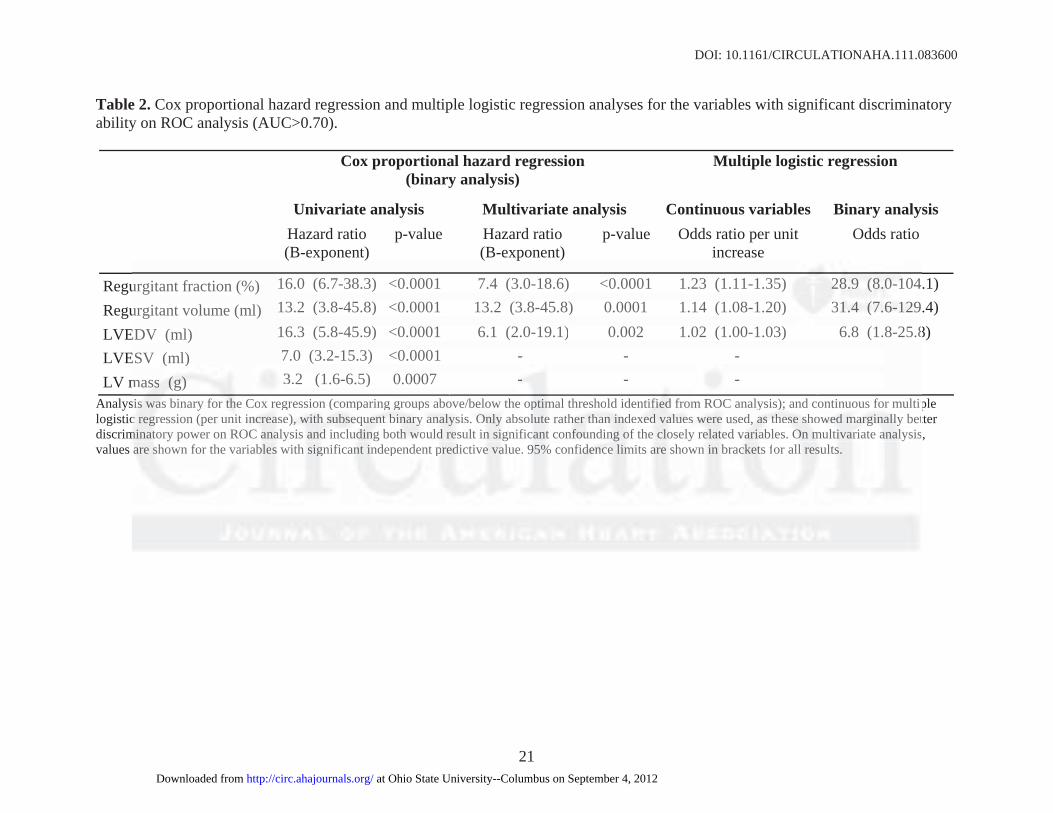
Table 2. Cox proportional hazard regression and multiple logistic regression analyses for the variables with significant discriminatory ability on ROC analysis (AUC>0.70).
Cox proportional hazard regression (binary analysis)
Multiple logistic regression
Univariate analysis Multivariate analysis Continuous variables Binary analysis Hazard ratio
(B-exponent) p-value Hazard ratio
(B-exponent) p-value Odds ratio per unit
increase Odds ratio
Regurgitant fraction (%) 16.0 (6.7-38.3) <0.0001 7.4 (3.0-18.6) <0.0001 1.23 (1.11-1.35) 28.9 (8.0-104.1)
Regurgitant volume (ml) 13.2 (3.8-45.8) <0.0001 13.2 (3.8-45.8) 0.0001 1.14 (1.08-1.20) 31.4 (7.6-129.4)
LVEDV (ml) 16.3 (5.8-45.9) <0.0001 6.1 (2.0-19.1) 0.002 1.02 (1.00-1.03) 6.8 (1.8-25.8) LVESV (ml) 7.0 (3.2-15.3) <0.0001 - - -
LV mass (g) 3.2 (1.6-6.5) 0.0007 - - - Analysis was binary for the Cox regression (comparing groups above/below the optimal threshold identified from ROC analysis); and continuous for multiple logistic regression (per unit increase), with subsequent binary analysis. Only absolute rather than indexed values were used, as these showed marginally better discriminatory power on ROC analysis and including both would result in significant confounding of the closely related variables. On multivariate analysis, values are shown for the variables with significant independent predictive value. 95% confidence limits are shown in brackets for all results.
urgitant fraction (%) 16.0 (6.7-38.3) <0.0001 7.4 (3.0-18.6) <0.0001 1.23 (1.11-1.35)) 2228.8.8 9 99 (((8.8.8.0-0-0 101 4
urgitant volume (ml) 13.2 (3.8-45.8) <0.0001 13.2 (3.8-45.8) 0.0001 1.14 (1.08-1.20)) 331.1.1 4 4 4 (((7.7.6-6-6 121212999
EDV (ml) 16.3 (5.8-45.9) <0.0001 6.1 (2.0-19.1) 0.002 1.02 (1.00-1.03) 6.8 (1.8-25.8ESV ((ml) 7.0 (3.2-15.3) <0.0001 - - -
mmasasssss (((g)g)g) 3.3 2 (1.6-6.5) 0.0007 -- - - ssisiss wasasa bbininary fofor r thththe Coox x reregrgrese siionon ((cocompm arrining g grgrououpsps aaboboveve/b/bele owow tthehe optpp mmi al thrhreseshoholdld identntififfieiei d d d frf omm RROCOC anaalyysisis)s); ; aandnd cconntitinunuouous for r mum ltipcc r ggegreression (per uuninit t ininncrcrc aaea ese),),, wwiti hh h sus sbseqeqe ueueuentntnt bbbinini rarary yy anananalal sysy isis. OnOnO lyly aabsb llolute e rathherere ttthahahan nn ninindedexexexed d d vaaalululuesese wweree usedd, , , aaass thththesese ee shshs owwowededed mmmarara gigig nan lllllly y bet
mim anatotory power on ROROC C ana alaa yssisis aa ddnd iincncluludidd ngngn bbotothh h wowow ulu d dd eresult in nn isigng if cicanant t co fnfnfouououndnd nining ofoo tthehe c ooloselyl rrelee tateded vvaraa aiaiablblees.s OOOn mumum ltltivi rarariaiatee aaa analylysisaaare ssshown for the variablblb es ss wi hth s ggignificacantnn iindn eppendedentn pppredid ctiveee aavalue. 9599 % %% confnfididdenenencecece l mmimits araa e shs own n in bbrackcc tets s for a llll r sesulu ssts. ff
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCULATIONAHA.111.083600
22
Table 3. Proportion of asymptomatic patients developing indications for surgery over time, according to CMR regurgitant fraction, and stratified by CMR centre.
Proportion developing indications for surgery
CMRCentre n
Highest CMR regurgitant fraction 33%
Highest CMR regurgitant fraction >33%
Kaplan-Meierp-value for difference
by logrank test Oxford 39 0.04 (n=24) 0.80 (n=15) Other centers 74 0.08 (n=48) 0.81 (n=26)
0.59
Table 4. CMR parameters by group. Comparison of CMR parameters between the three groups of patients with aortic regurgitation.
Conservative Crossover Surgical p-value Number in group 74 39 45 Age (years) 50.8 16.8 45.7 18.7 55.6 16.5* 0.04 Height (cm) 173.4 10.0 176.6 9.0 173.8 8.1 0.24 Proportion of male subjects 0.69 0.92† 0.91† 0.002 Weight (kg) 79.1 16.4 83.0 13.0 83.2 18.4 0.30 Body surface area (m2) 1.94 0.22 2.00 0.18 1.98 0.25 0.31 Bicuspid valve frequency 0.29 0.55† 0.24 0.006 Systolic BP (mmHg) 132.9 19.3 134.2 16.0 135.1 21.4 0.82 Diastolic BP (mmHg) 68.8 15.0 59.4 13.5 63.5 16.3 0.17 Regurgitant volume (ml) 27.5 15.5 74.7 28.5†† 80.5 38.7†† <0.0001 Regurgitant volume index (ml/m2) 14.1 7.6 37.4 14.5 †† 41.4 21.0†† <0.0001 Regurgitant fraction (%) 21.8 9.8 42.0 9.5 †† 45.6 11.0†† <0.0001 LVEDV (ml) 209.5 54.7 301.1 61.6 †† 315.8 91.1†† <0.0001 LVEDV index (ml/m2) 108.0 25.3 151.6 31.6 †† 160.6 48.6†† <0.0001 LVESV (ml) 78.7 35.5 113.0 33.0 †† 138.4 59.4††* <0.0001 LVESV index (ml/m2) 40.5 17.8 57.1 17.3† 70.3 31.8††* <0.0001 LV Ejection fraction (%) 63.6 8.7 62.9 6.4 57.1 10.9†* <0.0001 Echo LVEDD (cm) 5.9 0.6 6.6 0.7 †† 6.6 0.8†† <0.0001 Echo LVESD (cm) 3.7 0.6 4.1 0.6† 4.4 0.8†† <0.0001 LV mass (g) 173.2 73.1 232.2 80.1†† 277.4 77.8††* <0.0001 LV mass index (g/m2) 88.5 34.8 117.1 40.0† 143.7 41.1††* <0.0001 LV mass/LVEDV ratio (g/ml) 0.83 0.26 0.78 0.25 0.91 0.24 0.69
Abbreviations same as for table 1. Values are means ±standard deviation; p-values shown for one-way ANOVA with the exception of bicuspid valve frequency and proportion of male subjects which were by chi-squared analysis; bold figures indicate p<0.05. Individual group comparisons using Bonferroni correction are also shown: †p<0.01, †p<0.001 and ††p<0.0001 vs. the conservative group; *p<0.05 surgical vs. crossover groups.
Height (cm) 173.4 10.0 176.6 9.0 173.8 8.11 00.0.242424 Proportion of male subjects 0.69 0.92† 0.91† 000.000020202 Weight (kg) 79.1 16.4 83.0 13.0 83.2 18.4 0.30 Bodydy suru facece areea a ((mm2) 1.94 0.22 2.00 0.18 11.9.98 0.25 0.31 BiBiBicuuuspspid vvalalalvvve ffrereququencyy 0.29 0.55† 0.24 0.006 SySyststolic BPP (m(mmHmHmHg)g) 13131 2.22 99 9 1911 ..33 133434.2.2.2 16161 .0.00 113355.1 22121.4.4.4 00.0.828282 DDiD aasastolic BPP ((mmmmHHHg) 6868.8.8 155.000 59.9.9.444 1333.5 633.3.55 166.3 0.1717 ReReegugugurgrgrgitititananant t t vovolululumemee (((mmml) ) 2727.5.5. 11515.555 77744.4.7 7 28282 .5.5.5†††† 8880.55 5 383838 7.7.7††††† <<0<0.0.00000011ReReRegugugurgrgrgitititanananttt vovovolululumememe iiindndndexexex (((mlmlml/m/m/m22))) 141414 11.1 777.666 373737 44.4 141414 55.5 †† 444111.444 212121 00.0†† <0<0<0 00.0000000111ReRegugurgrgititanant t frfrf acactitit onon (((%)%)%) 2121.88.8 9.9.88 44242.0.0 9.9.9 55 ††††† 4445.5.6 6 11111.0.0††††† <00.0.0000011
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCULATIONAHA.111.083600
23
Figure Legends:
Figure 1. CMR flow measurement in aortic regurgitation. Top: still frame from steady-state free
precession cine showing left ventricular outflow tract view in diastole with the aortic
regurgitation jet (arrowed) and the slice location for through-plane flow measurement (parallel
lines). Middle: example through-plane flow images; left – anatomical (magnitude) image in
systole, middle – flow (phase) image in systole showing forward flow in white, right – flow
(phase) image in diastole showing regurgitant flow in black. Bottom: resulting flow-time curve
showing volume of regurgitation. LV = left ventricle, LA = left atrium, Ao = aorta.
Figure 2. Discriminatory ability of aortic regurgitant fraction. Top: receiver operating
characteristic (ROC) curve for the ability of aortic regurgitant fraction to identify asymptomatic
patients who would develop symptoms or other indications for surgery. Bottom: dot plot
showing regurgitant fraction in the conservative and crossover groups, with the optimal threshold
of 33% shown.
Figure 3. Surgery-free survival by aortic regurgitant fraction. Kaplan-Meier graphs for survival
without surgery in 113 asymptomatic subjects with at least moderate aortic regurgitation initially
treated conservatively and followed for up to 9 years. a) Stratified by the highest aortic
regurgitant fraction measured by CMR during follow up 33% (n=74) and >33% (n=39), with
the time of the scan with highest regurgitant fraction used as the baseline. b) Similar graph
stratified by CMR-derived LV end-diastolic volume 246ml (n=60) and >246ml (n=53). c) Same
graph as in a), stratified by both highest CMR regurgitant fraction and CMR centre. d) Similar
graph stratified by both highest CMR regurgitant fraction and LV end-diastolic volume.
Figure 2. Discriminatory ability of aortic regurgitant fractif on. Top: receiver operating
chararacacacteteteriririststs icicc (ROROOC)CC curve for the ability of aorrtitiiccc rerr gurgitant fractionn tttooo identify asymptomatic rrr
ppaatiienents whoo wwoououlddl dddeveve elelelopopop sssymymymptptptomomomss ooror ooothththeer r innnddiicaatititiononons s s fofofor r susus rgrgrgerereryy.y. BBBotttototom:m:m: dddototo ppplololot t t
hhhowowowining g regugugurgrgr itttannnt t frfrraccctionnn inn n ththe e cocconnsnserervavaatiiveve aanandd ccrcroosossosooveeer ggrgroooupspp ,, wwiwiththh theheh oopptptimimmaaal tthrhreeshhhold
ofofof 3333%3%3% ssshohohownwnwn.
at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from

at Ohio State University--Columbus on September 4, 2012http://circ.ahajournals.org/Downloaded from